all of the presenters are employees of steris corporation
TRANSCRIPT

1
Care and Handling of
Endoscopes:Flexible and Rigid
• Participants must complete the entire presentation/seminar to
achieve successful completion and receive contact hour credit.
Partial credit will not be given.
• All of the presenters are employees of STERIS Corporation and
receive no direct compensation other than their normal salaries for
participation in this activity.
• STERIS Corporation is an approved provider of continuing nursing
education by the California Board of Registered Nursing, provider
number CEP11681 for 1 contact hour along with IAHCSMM and
CBSPD.
• STERIS Corporation is providing the speakers and contact hours for
this activity. However, products referred to or seen during this
presentation do not constitute a commercial support by the speakers.
Continuing Education Contact Hours
2
Learning ObjectivesUpon completion of this course, you will be able to:
• Discuss current healthcare trends in endoscopy
• Compare and contrast flexible and rigid endoscopes
• Name the major parts and functions of endoscopes
• Review key steps in point of use preparation,
transport, reprocessing and storage to prevent
endoscope damage
3
Current Trends in Endoscopy
• U.S. endoscope market valued at $2 billion
• Technology advances in diagnostics
• Advanced visualization for complex procedures
• Improved diagnostic and therapeutic capabilities
4
Learning ObjectivesUpon completion of this course, you will be able to:
• Discuss current healthcare trends in endoscopy
• Compare and contrast flexible and rigid endoscopes
• Name the major parts and functions of endoscopes
• Review key steps in point of use preparation,
transport, reprocessing and storage to prevent
endoscope damage
5
Flexible Endoscope
Suction and Air/
water channel ports
Distal tip
Biopsy port
Directional Lever
6

2
Camera –
approximately $15,000
Small Flexible Endoscope –
approximately $22,000
Robotic Scopes –
approximately $18,000
7
Flexible and Rigid Endoscope
Characteristics
• Delicate, complex,
expensive
• Require special care
and handling
• Access internal
structures/cavities
• Lens system for
image
• Fiberoptic cable for
light
• Internal lumens and
channels
• Insuffulation component
• Suction and irrigation
systems
• Monitors connected
through cable system to
carry signals
8
Types of Flexible Endoscopes
Fiberscope Videoscope
9
Flexible Endoscopes• Complex devices
− Mechanical, electrical, plumbing systems working in
unison
• Advanced visualization
• Delicate design
• Unique components
• Constant changing technology means:
− New endoscopes
− New design features
− New challenges
10
Flexible Endoscope Anatomy
• Mechanical system
− Control body, insertion and light guide tubes,
bending section
• Image
− Fiberoptic cable, video electronics,
connector, water resistant caps
• Channels
− Suction/biopsy, air/water, irrigation, water-jet, elevator
wire
• Accessories
− Valves, suction, air/water, biopsy port
− Biopsy forceps, snares, guide wires, irrigators, dilators
11
Effects on Repair Costs
• Level of care and handling
• Short turnover times
• Inadequate inventory
• Rush, skip steps during processing
• Cutting corners to please internal customers
• Lack of training/experience/expertise
• Poorly managed internal procedures and training
• Number of people handling and reprocessing
12

3
Mechanical System
• Control mechanism, insertion tube,
bending section
• Coiled wires connect to directional knobs
• Work together to angulate and move
bending section
13
Mechanical System, continued
• Insertion tube
− Portion inserted into patient
− Markings act as reference points
− Bending section covers end of insertion tube
Working component
14
Bending Section
• Flexible component for positioning
• Contains channels, lens, CCD chip
Outer rubber sheath
Metal spiral coil Steel mesh
Glue joints
Resin
15
Mechanical System
• Light guide tube
• Connects control body to light guide connector
• Houses wiring, tubing, fiber bundle, channels
• Incorporates connections
− suction, air/water bottle
− light fiber bundle
− electrical contacts
• ETO venting valve (fiberscopes)
• Electrical connector (video scopes)
16
Illumination - Fiberscope
• Fiber bundle carries light
• Image viewed directly through eyepiece
• Broken fibers diminish light
• New fiber bundle = total repair
Fiber bundle
Eye piece
17
Video Image System
• Chip located in distal tip
• Image bundle with video
camera unit
• Video lens system reduces
and focuses image onto
electronic chip
• Signals transmitted to
electrical connector/
processor
• Image viewed on video
screen
Load wires
CCD
Bending
Section
18

4
Video Connector
Light Guide Connector Fluid Resistant Caps
Electrical Connector
Contact Pins
O-Ring
ScrewsLeak Tester Port
19
Rigid Endoscopes
20
Types of Rigid Endoscopes
• Arthroscopes
• Laparoscopes
• Cystoscopes
• Bronchoscopes
• Sinuscopes
• Hysterscopes
• Ureteroscopes
• Esophagoscopes
21
Learning ObjectivesUpon completion of this course, you will be able to:
• Discuss current healthcare trends in endoscopy
• Compare and contrast flexible and rigid endoscopes
• Name the major parts and functions of endoscopes
• Review key steps in point of use preparation,
transport, reprocessing and storage to prevent
endoscope damage
22
Rigid Endoscope Anatomy
Assembled View
Endoscopic Body & Shaft
Rod Lenses
Objective
Spacers
Light Post
Fiber Guide
Eye Piece
Focus Lens
Retainer
Ring/Spring
Alignment/Focus Mechanism
Expanded View
23
Rigid Endoscope Anatomy, continued
Objective
LensBody
Eye
Piece
Light Post
24

5
Scope Damage
• 30% scope damage = normal wear and tear
• 70% scope damage = within our control
25
Contributing Factors Towards
Repair Costs
• Improper care and handling
• Expedited room turnovers
• Insufficient inventory
• Pressure to quickly reprocess devices;
skipped steps
• Inadequate training/diminished competency
26
Effects on Repair Costs
• Routine use
• Fluid invasion
− Failed leak tests
• Mishandling/misuse
− During procedures
− Transport
− Cleaning, disinfection/sterilization
− Storage
• Broken fibers, cracked lenses
• Bent rods
• Punctures in internal lumens
27
Learning ObjectivesUpon completion of this course, you will be able to:
• Discuss current healthcare trends in endoscopy
• Compare and contrast flexible and rigid endoscopes
• Name the major parts and functions of endoscopes
• Review key steps in point of use preparation,
transport, reprocessing and storage to prevent
endoscope damage
28
Proper Handling
• Insertion tube coiled loosely
• Support control body, light guide
• Components separated
• No accessories
29
Poor Handling Practices
30

6
Poor Handling Practices, continued
31
Poor Practices • Avoid the “pretzel” syndrome
− Excessive coiling, twisting
− Not following natural curvature of endoscope
• Crushing injuries
• Stacking
• Buckling
32
Endoscope Damage • Most Vulnerable:
• Distal tip - houses CCD, light guide lens, air water nozzle
− Avoid striking or dropping
− Place tip down carefully, gently, avoid stacking
• Electronics and optics
− Keep fluid from internal workings
− No impact or trauma
• Channels
− Smaller have more kinds and curves
− More difficult to clean
33
Correct Handling Practices
• Protect eyepiece and body
• Avoid damage to lens
34
Endoscope Damage
• Routine use
• Fluid invasion
− Failed leak tests
• Mishandling/misuse
− During procedures
− Transport
− Cleaning, disinfection/sterilization
− Storage
• Broken fibers, cracked lenses
• Bent rods
• Punctures in internal lumens
35 36
7
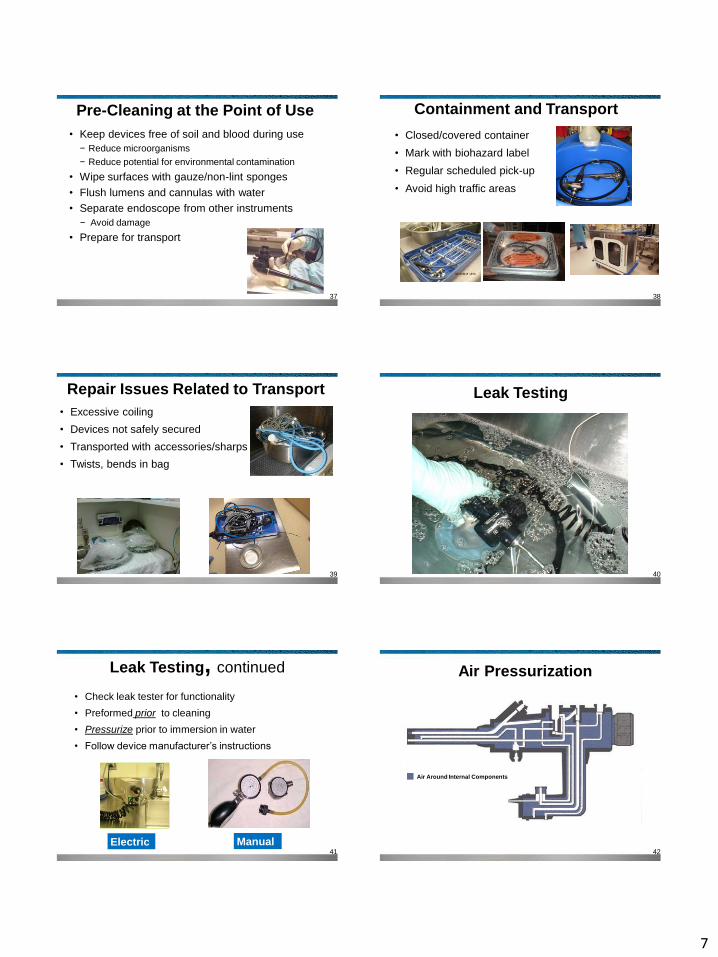
Pre-Cleaning at the Point of Use
• Keep devices free of soil and blood during use
− Reduce microorganisms
− Reduce potential for environmental contamination
• Wipe surfaces with gauze/non-lint sponges
• Flush lumens and cannulas with water
• Separate endoscope from other instruments
− Avoid damage
• Prepare for transport
37
Containment and Transport
• Closed/covered container
• Mark with biohazard label
• Regular scheduled pick-up
• Avoid high traffic areas
38
Repair Issues Related to Transport
• Excessive coiling
• Devices not safely secured
• Transported with accessories/sharps
• Twists, bends in bag
39
Leak Testing
40
Leak Testing, continued
• Check leak tester for functionality
• Preformed prior to cleaning
• Pressurize prior to immersion in water
• Follow device manufacturer’s instructions
Electric Manual41
Air Pressurization
Air Around Internal Components
42

8
Indications of a Leak
Control body Channels
43
Fluid Invasion
• Frequent repair – over half of total repair costs
• Requires immediate identification and repair
• If undetected = greater damage
− Image stains
− Foggy images
− Transmission of infection
− Fluid, biologic materials, biofilm collect
44
Cleaning
• Multi-step process
• 2 sinks of adequate size for flexible
endoscopes
− First sink: soak/wash with cleaning
solution to remove soil
− Second sink: rinse
− Third sink for treated water rinse
• Work flow dirty to clean 45
Cleaning Methods
• Follow manufacturer IFUs
− Manual
− Mechanical
− Combination of both
− Mechanical friction
• Physically remove debris
− Wiping, brushing, spraying, flushing lumens
• Should not damage endoscope
• Safe for the worker performing the task
46
Manual Cleaning• Non-lint cloths
• Identify models and channels
• ALL channels accessed
• Channel irrigators used
• Brush inventory
− Correct brush sizes for
channels
− Varying diameters and lengths
− Single use are disposable!
− Disinfect reusable brushes
• Flush channels to remove
loosened soil47
Appropriate Cleaning Chemistry
• Fresh solution
• READ THE LABEL!
• Follow manufacturer IFUs
• Neutral pH
• Compatible with endoscopes
• Dilute correctly
• Check water temperature
• Mark water line on sink
• Soak time
48

9
Mechanical Cleaning Options
• Flushes internal channels
• Consistent process
49
Manual Cleaning:Rinse in Second Sink
• Clean, fresh, warm water
• Thorough rinsing
• Immersed in water
• Flush all instrument channels
• Rinse to irrigate the challenging design features
• Remove soil and cleaning chemistry
50
Manual Cleaning: Third Sink with treated water
for rinsing
51
Inappropriate Cleaning Chemistry
and Inadequate Rinsing
52
Mechanical Cleaning
53
Ultrasonic Cleaning
• Utilized for fine cleaning of rigid devices
• Gross debris removed
• Effective cleaning chemistry
• Cavitation process
− Sonic energy created bubbles
− Unstable bubbles implode
− Dislodges soil from surfaces
• Degas prior to use
• Change solution regularly
• No optical devices, mixed metals
54

10
Mechanical CleaningAutomated Endoscope Reprocessor
• Wash phase during cycle
• Augments manual cleaning for consistent outcome
• Cleaning chemistry labeled for endoscopes
• FDA cleared wash phase with minimal pre-cleaning
− Pre-cleaning steps MUST be followed
• Follow endoscope manufacturer instructions
• Follow AER manufacturer instructions
• IFUs may be in conflict
55
Endoscope Accessories
• Reusable accessories, valves, tubing processed
per manufacturer instructions
• Disassembled and cleaned
• Inspect for integrity
• AER manufacturer validates processing
56
Inspection
• Examine line of shaft
• External damage
• Check vision
57
Disinfection vs. Sterilization
• Endoscope’s intended use
• Critical, semi-critical
• Sterilization preferred
− Vaporized Hydrogen
Peroxide
− Hydrogen Peroxide gas
plasma
− Liquid chemical
sterilization
• Follow manufacturer‘s
guidelines
• Individual facility policy
**Add Image of LCS
58
High Level Disinfection
• Follow manufacturer’s
instructions
• Manual soaking and
adequate rinsing
• Automated Endoscope
Reprocessor
− Careful placement in
Reprocessor
− Use validated
adapters as needed
59
Storage
• Remove residual water
• Purge all channels with alcohol and
(compressed) air
• Detach removable parts, valves, biopsy caps
• Angulation locks in free position
• Variable stiffness knob in neutral position
• Detach water resistant cap
• Well-ventilated cabinet
• Hang freely
• Distal tip not touching bottom of cabinet
• Processed scopes labeled as ‘patient ready’60

11
Incorrect Storage
61
Storage Time
Endoscope Shelf Life prior to reprocessing:
• AAMI ST 91: based on risk assessment
• AORN: based on risk assessment
• SGNA: up to 7 days
• CDC: based on risk assessment
62
Preventative Maintenance
for all Endoscopes
• Check for signs of wear and tear
• Scope intact after repairs
• Prevent damage
• Trained and qualified staff
63
Action Plan
• Continuing education to staff on proper care,
handling and maintenance of all scopes
• Refer to scope manufacturer’s instructions for
proper use and handling
64
References• Alfa, M. J. (2013). Monitoring and improving the effectiveness of
cleaning medical and surgical devices. American Journal of Infection
Control, 41(5), S56-S59. doi:10.1016/j.ajic.2012.12.006
• Association for the Advancement of Medical Instrumentation.
(2013). ANSI/AAMI ST58: 2013. Arlington, VA: Author.
Chemical sterilization and high-level disinfection in health care
facilities
• Association for the Advancement of Medical Instrumentation.
(2014). AAMI TIR34:2014. Arlington, VA: Author.
Water for the reprocessing of medical devices
• Association for the Advancement of Medical Instrumentation.
(2015). ANSI/AAMI ST91:2015. Arlington, VA: Author.
Flexible and semi-rigid endoscope processing in health care facilities
• Association of periOperative Registered Nurses, Burlingame, B.,
Denholm, B., Kovac, M., Link, T., Ogg, M. J., … Wood, A.
(2016). Guidelines For PERIOPERATIVE PRACTICE (2016 ed.).
Dever, CO: Author.
65
References• Endoscope care guide. (2015). HEALTHCARE PURCHASING
NEWS, 39(11), 34-57.
• Flood, A., Huslage, D. K., & Myers, F. (2015). Endoscope crosswalk:
Critical guideline review.Prevention Strategist, 8(4), 52-54.
• Herrin, A., Loyola, M., Bocian, S., Diskey, A., Friis, C., Herron-Rice, L.,
& Selking, S. (2015).Standards of infection prevention in reprocessing
flexible gastrointestinal endoscopes. Retrieved February 29, 2016,
from
http://www.sgna.org/Portals/0/Standards%20for%20reprocessing%20
endoscopes_FINAL_2.22.pdf
• Kulkarni, K. (2013). Endoscope care guide. HEALTHCARE
PURCHASING NEWS, 37(11), 10-29.
• McDonnell, G. (2014). Chemical disinfection and
sterilization. Healthcare Purchasing News,38(3), 50-53.
66

12
References• McDonnell, G. E., & Sheard, D. (2012). A practical guide to
decontamination in healthcare. Chichester, U.K: Wiley-Blackwell.
• Reprocessing medical devices in health care settings: Validation
methods and Labeling guidance for industry and food and drug
administration staff. (2015, March 17). Retrieved February 29, 2016,
from
http://www.fda.gov/downloads/medicaldevices/deviceregulationandgui
dance/guidancedocuments/ucm253010.pdf
• Society of Gastroenterology Nurses and Associates, Inc. (2014,
September). Position statement reprocessing of endoscopic
accessories and valves. Retrieved February 29, 2016, from
http://www.sgna.org/Portals/0/Education/PDF/Position-
Statements/Reprocessingvalvesdocument_FINAL.pdf
67
Summary
Now that you have completed this course, you can:
• Discuss current healthcare trends in endoscopy
• Compare and contrast flexible and rigid endoscopes
• Name the major parts and functions of endoscopes
• Review key steps in point of use preparation,
transport, reprocessing and storage to prevent
endoscope damage
68
Steris University
Go to: http://university.steris.comuniversity.steris.com
Playing a part in your professional development today
To help you achieve your career vision for tomorrow