ali fahir ozer m.d., murat cosar m.d. · ali fahir ozer m.d., murat cosar m.d. serrated bumps on...
TRANSCRIPT

Lumbar D
egenerative Disc D
isease and Dynam
ic Stabilization
257totAl DIsC
ReplACeMent
Ali fahir ozeR M.D., Murat CosAR M.D.29
Knowledge gathered from experiments and experi-ence grows like a tree, and we later begin to collect the tree’s fruit. Regarding the spine, we have started to obtain the products of rigid and dynamic stabi-lization from the synthesis of anatomy, physiology, biology, and mechanics. One of these products is the “disc prosthesis”.
1. Background
When we look at the development of disc replace-ment, we will see that it is not very dated. As the first person to perform a discectomy, Barr (1) de-clared in a later article, “Once a disc has been re-moved, we can no longer claim the spine to be ana-tomically or mechanically normal.” Barr, in keeping with my opinion, subsequently stated the problem further: “The disc can be removed, but this opera-tion is not sufficient, and I do not know what else can be performed.”
French van Steenbrugghe (2) were the first to receive a patent for placing a dynamic structure in the va-cated disc space. A dynamic prosthetic was first used in patient treatment by the Swedish spinal surgeon Fernström (3) in 1966. The prosthetic used by Fern-ström was a steel ball. He classified the ailments into two groups: “lumbar disc herniation” and “degen-erative disc disease”. His most notable finding was that the treatments of the patients in the disc herni-ation group were more successful, but the patients in the degenerative disc group only ceased to have lower back pain. However, Fernström’s method has not become prevalent. Because the steel ball is solid
and spherical, increased load on the point where the cartilage meets the vertebral end plates causes the cartilage to break and lodge into the vertebral body, and the prosthetic thus loses its dynamic property after a period of time.
In subsequent years, studies were performed mostly on the replacement of nuclear material. In 1973, Urbaniak et al. (4) injected silicon Dacron im-plants into chimpanzees and observed aberrant bone formation along with bone resorption. In 1974, Sch-neider and Oyen (5) injected liquid silicon into the disc space following discectomy and ensured that the silicon froze in the disc space. Froning (6) received a patent for an inter-disc device that remained in the vacated disc space that could collapse or expand and had a pocket, but he never applied this tech-nique to patients.
Fassio (7) made an elastic prosthetic that had a syn-thetic resin on the inside with a frame outside and, along with Ginestie (8), applied itfirst to monkeys and later to three patients.However, their results were not as good as expected; as disc height decreased, the material was displaced because it became squeezed, and movement was not observed.
In 1984, Germans Karin Büttner-Janz and Kurt Schelnack accomplished the process of total removal of a disc and replacement with an artificial disc. Af-ter intensive biomechanical material studies, they cre-ated a disc prosthetic made up of three parts. The first disc prosthetic was made of rigid metal plates as the top and bottom pieces with a plastic nuclear material connected to these metal plates. The car-tilage attached to the vertebrae by lodging to the

Lum
bar D
egen
erat
ive
Dis
c D
isea
se a
nd D
ynam
ic S
tabi
lizat
ion
258Ali Fahir OZER M.D., Murat COSAR M.D.
serrated bumps on the metal plates and to the ver-tebral end plates. Based on results in patients and the problems encountered after their application, the disc prosthetics were modified twice and took their final form as Charité III. The artificial disc came to be called Charité III because it was used at the Charité hospital connected to Humboldt University. In 1987, when Karin Büttner-Janz and Kurt Schelnack (9) pub-lished their first results, they emphasized that disc prosthetic surgery with a ventral approach was now an alternative treatment method. A year later, when these researchers published findings from a second set of patients, they were extremely pleased with their results. Compared to before surgery, 98% of patients improved after surgery (10). After this date, the use of the Charité III disc prosthetic spread throughout the world. Later, Marnay (11) devised the “ProDisc”, which is known as the “ball-socket” and has a slip-pery polythene substance between the plates. Mar-nay has published positive results from 11 years of clinical observations. Over the years, many disc pros-thetics have been made and used clinically. To treat degenerative disc disease today, prosthetic discs are often the best approach.
2. Indications
It should not be overlooked that of the lumbar disc prosthetic candidates, a majority of the patients have degenerative disc disease without neurologi-cal problems. The ultimate goal of the treatment is to increase the quality of life of the patient. For this reason, the primary goal should be to give the pa-tient the treatment that will provide the best chance for recovery or improvement, such as by performing back exercises to the extent that the patient can per-form them under the doctor’s guidance and achiev-ing medical health without surgery. Only those pa-tients who cannot sustain the medical treatment and exercise program should be candidates for surgery. Along these lines, Huang (50) has reported that only 5% of lumbar surgery patients have indications for total disc replacement (TDR).
Those patients with single-level degenerative disc disease form the best candidate group for lum-bar disc prosthesis surgery. A lumbar disc prosthe-sis can be made for two disc spaces by pushing in-dications; however, this approach is not practiced in our clinic, and we do not recommend such an
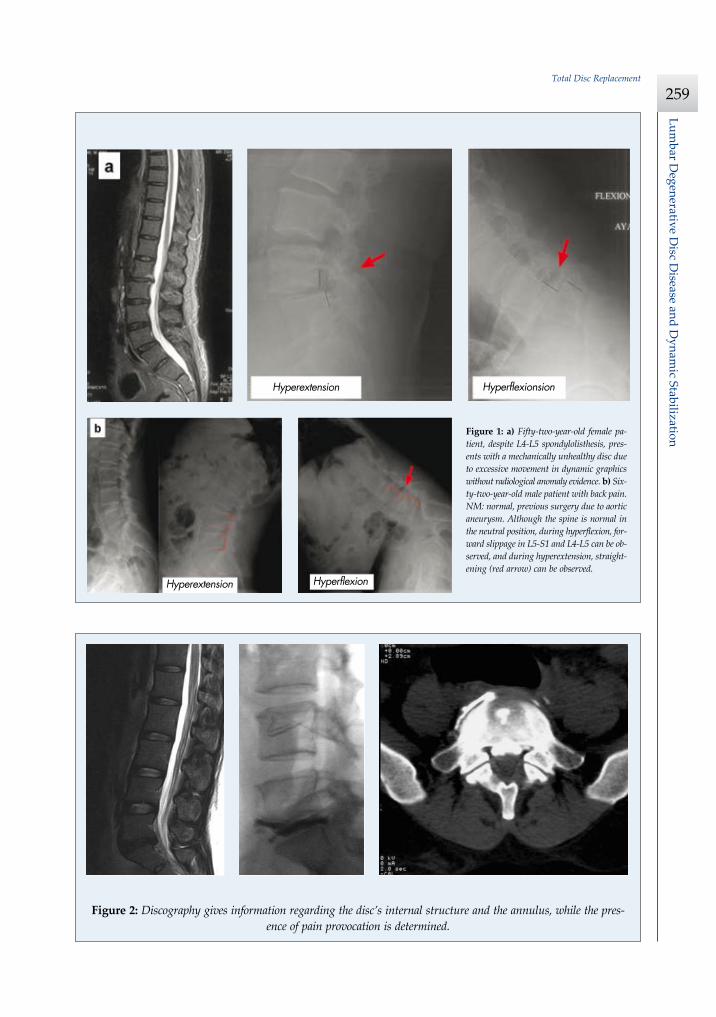
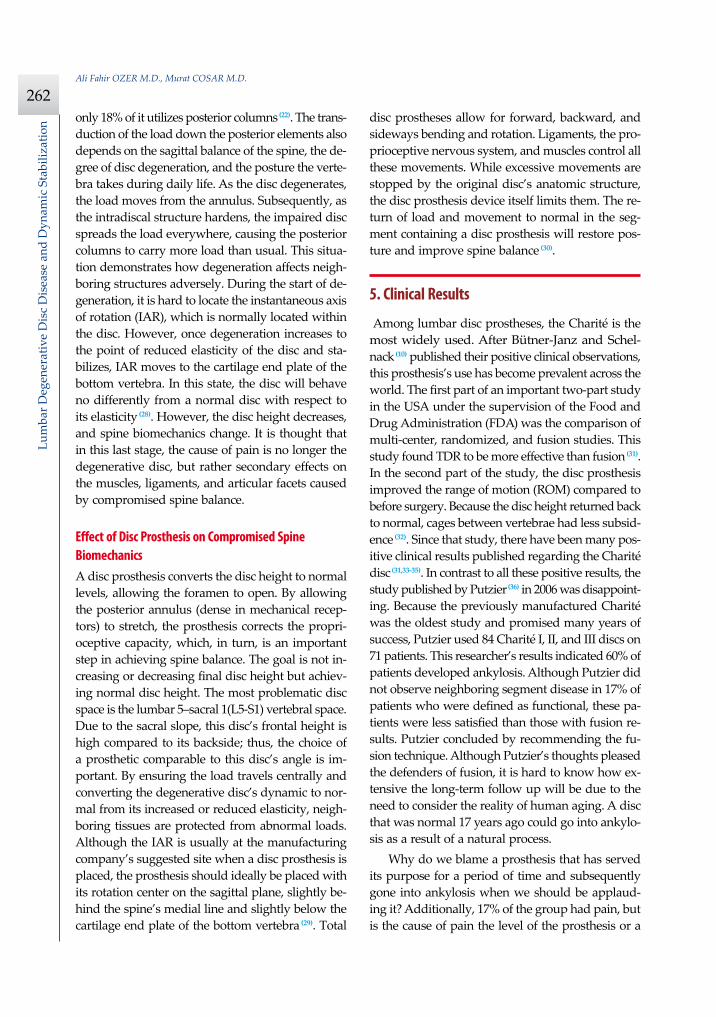
approach. For disc surgery, the patient needs to be complaining of pain, and instability of the disc needs to be detected radiologically (Figure 1). Although mag-netic resonance imaging (MRI) is a good method to detect disc status, MRI can give falsepositive re-sults (12,13). Even though many articles have recom-mended against it, to obtain as much information as possible from the patient, we use discography in our clinic (14-17). In discography, the presence of annu-lus tearing and pain provocation is observed (Figure 2). To better image the tears in the annulus, a disco-BT is recommended but not made mandatory. I believe there is benefit in emphasizing one point that does not receive much attention in the literature. Due to the increased pressure caused by the injections into the disc, the sides of a tear become mechanically ir-ritated. Additionally, the dye used can chemically irritate sensitive nerve endings. Both of these cause pain. If a tear is notably large or if there are many tears, pain provocation is not observed, due to the inability of the liquid to cause pressure in the disc, which yields falsenegative results.
In this case, we cannot say that the disc that the procedure is performed on is not the source of pain. If the patient is showing more than the expected re-action to the injection, it could be a sign that the pa-tient is psychologically unstable. In such patients, it is necessary to be careful in making the decision to perform surgery. The point to focus on with these procedures is the importance of the injection of in-tradiscal local anesthetic after the initial injection. Normally, the local anesthetic reduces the pain by blocking sensitive nerve endings. This situation also shows that this disc is the source of pain. For us, the ideal patient group is composed of adults ages 20-40, showing a problematic disc on MRI, with disc heights no less than 5 mm, with no facet joint prob-lems, and with good bone quality.
3. Contraindications
3.a. OsteoporosisBecause bone quality is compromised in patients with osteoporosis, the spine can fracture during the placement of the rigid metal disc. Even though most artificial discs are made of metals or nonmet-als, they are more rigid compared to normal discs. Therefore, they have little to no shock-absorbing qualities and transfer the load to a bottom segment.
Lumbar D
egenerative Disc D
isease and Dynam
ic Stabilization
259Total Disc Replacement
233Prof. Dr. Ali Fahir ÖZER
Önceki Spinal CerrahiDaha önce laminektomi ve diskektomi gibi hastal›klar› geçiren
hastalar, bu cerrahi için uygun de¤ildirler. Ancak, çok seçilmifl flavalligaman› korunmufl ve posterior cerrahi s›ras›nda faset eklemlerinedokunulmam›fl hastalar, daha sonra gerekirse önden disk protezi cer-rahisine aday olabilmektedirler(21).
Psikolojik De¤erlendirmeEn önemli de¤erlendirme kriterlerinden biri de psikolojik de¤er-
lendirmedir. Hastada psikolojik de¤erlendirme yap›lmamas›, ameli-yat› yapan cerrah için büyük sorunlara yol açmaktad›r. Bilerek veyabilmeyerek ikincil kazanç peflinde olanlar, kiflilik bozukluklar›, a¤›rdepresyon ve psikoz görülen hastalarda bu cerrahi ve acil d›fl›ndaher cerrahi kesinlikle kontraendikedir.
fiekil 2: Diskografi diskin iç yap›s› ve anulus hakk›nda bilgi vermekte, bu arada a¤r› provokasyonunun olup olmad›¤›na bak›lmaktad›r.
fiekil 3: MR ve BT anjiografi ile arter venin bifurkasyon ölçümü görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 233
233Prof. Dr. Ali Fahir ÖZER
Önceki Spinal CerrahiDaha önce laminektomi ve diskektomi gibi hastal›klar› geçiren
hastalar, bu cerrahi için uygun de¤ildirler. Ancak, çok seçilmifl flavalligaman› korunmufl ve posterior cerrahi s›ras›nda faset eklemlerinedokunulmam›fl hastalar, daha sonra gerekirse önden disk protezi cer-rahisine aday olabilmektedirler(21).
Psikolojik De¤erlendirmeEn önemli de¤erlendirme kriterlerinden biri de psikolojik de¤er-
lendirmedir. Hastada psikolojik de¤erlendirme yap›lmamas›, ameli-yat› yapan cerrah için büyük sorunlara yol açmaktad›r. Bilerek veyabilmeyerek ikincil kazanç peflinde olanlar, kiflilik bozukluklar›, a¤›rdepresyon ve psikoz görülen hastalarda bu cerrahi ve acil d›fl›ndaher cerrahi kesinlikle kontraendikedir.
fiekil 2: Diskografi diskin iç yap›s› ve anulus hakk›nda bilgi vermekte, bu arada a¤r› provokasyonunun olup olmad›¤›na bak›lmaktad›r.
fiekil 3: MR ve BT anjiografi ile arter venin bifurkasyon ölçümü görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 233
Figure 2: Discography gives information regarding the disc’s internal structure and the annulus, while the pres-ence of pain provocation is determined.
Figure 1: a) Fifty-two-year-old female pa-tient, despite L4-L5 spondylolisthesis, pres-ents with a mechanically unhealthy disc due to excessive movement in dynamic graphics without radiological anomaly evidence. b) Six-ty-two-year-old male patient with back pain. NM: normal, previous surgery due to aortic aneurysm. Although the spine is normal in the neutral position, during hyperflexion, for-ward slippage in L5-S1 and L4-L5 can be ob-served, and during hyperextension, straight-ening (red arrow) can be observed.
Hyperextension Hyperflexionsion
Hyperextension Hyperflexion
Lum
bar D
egen
erat
ive
Dis
c D
isea
se a
nd D
ynam
ic S
tabi
lizat
ion
260Ali Fahir OZER M.D., Murat COSAR M.D.
The spine can easily break in patients when the load is slightly above normal, especially in patients with two-disc prosthetics where the spine in between can break easily. For this reason, patients with calcium metabolism disorders or patients using cortisone are not suitable for disc prosthetic surgery.
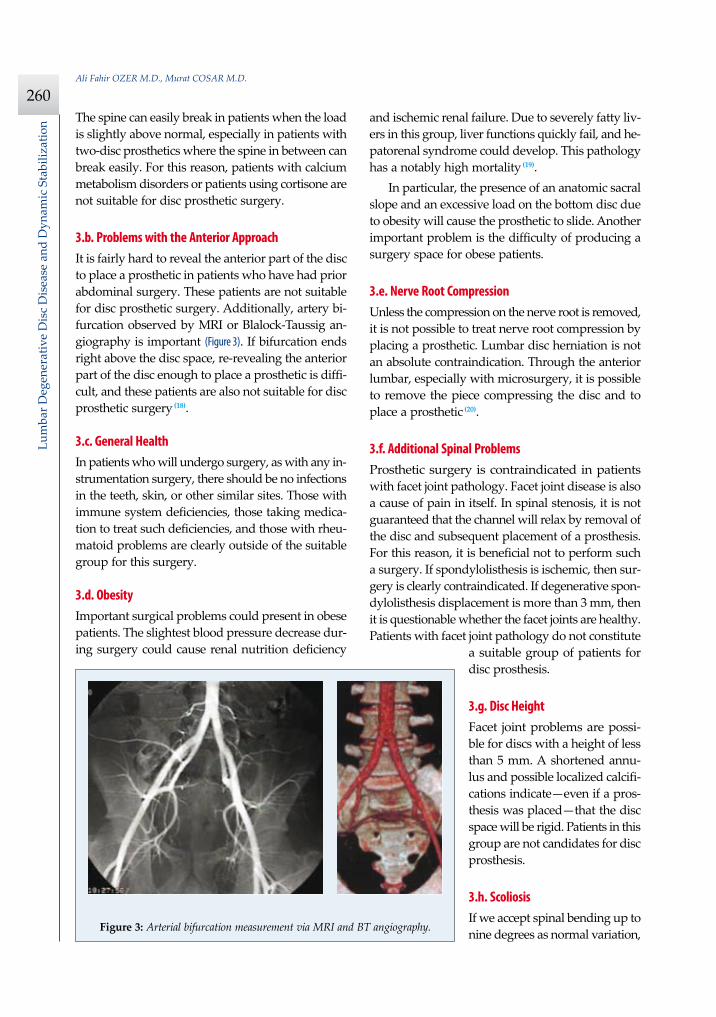
3.b. Problems with the Anterior Approach It is fairly hard to reveal the anterior part of the disc to place a prosthetic in patients who have had prior abdominal surgery. These patients are not suitable for disc prosthetic surgery. Additionally, artery bi-furcation observed by MRI or Blalock-Taussig an-giography is important (Figure 3). If bifurcation ends right above the disc space, re-revealing the anterior part of the disc enough to place a prosthetic is diffi-cult, and these patients are also not suitable for disc prosthetic surgery (18).
3.c. General HealthIn patients who will undergo surgery, as with any in-strumentation surgery, there should be no infections in the teeth, skin, or other similar sites. Those with immune system deficiencies, those taking medica-tion to treat such deficiencies, and those with rheu-matoid problems are clearly outside of the suitable group for this surgery.
3.d. ObesityImportant surgical problems could present in obese patients. The slightest blood pressure decrease dur-ing surgery could cause renal nutrition deficiency
and ischemic renal failure. Due to severely fatty liv-ers in this group, liver functions quickly fail, and he-patorenal syndrome could develop. This pathology has a notably high mortality (19).
In particular, the presence of an anatomic sacral slope and an excessive load on the bottom disc due to obesity will cause the prosthetic to slide. Another important problem is the difficulty of producing a surgery space for obese patients.
3.e. Nerve Root CompressionUnless the compression on the nerve root is removed, it is not possible to treat nerve root compression by placing a prosthetic. Lumbar disc herniation is not an absolute contraindication. Through the anterior lumbar, especially with microsurgery, it is possible to remove the piece compressing the disc and to place a prosthetic (20).
3.f. Additional Spinal ProblemsProsthetic surgery is contraindicated in patients with facet joint pathology. Facet joint disease is also a cause of pain in itself. In spinal stenosis, it is not guaranteed that the channel will relax by removal of the disc and subsequent placement of a prosthesis. For this reason, it is beneficial not to perform such a surgery. If spondylolisthesis is ischemic, then sur-gery is clearly contraindicated. If degenerative spon-dylolisthesis displacement is more than 3 mm, then it is questionable whether the facet joints are healthy. Patients with facet joint pathology do not constitute
a suitable group of patients for disc prosthesis.
3.g. Disc HeightFacet joint problems are possi-ble for discs with a height of less than 5 mm. A shortened annu-lus and possible localized calcifi-cations indicate—even if a pros-thesis was placed—that the disc space will be rigid. Patients in this group are not candidates for disc prosthesis.
3.h. ScoliosisIf we accept spinal bending up to nine degrees as normal variation,
233Prof. Dr. Ali Fahir ÖZER
Önceki Spinal CerrahiDaha önce laminektomi ve diskektomi gibi hastal›klar› geçiren
hastalar, bu cerrahi için uygun de¤ildirler. Ancak, çok seçilmifl flavalligaman› korunmufl ve posterior cerrahi s›ras›nda faset eklemlerinedokunulmam›fl hastalar, daha sonra gerekirse önden disk protezi cer-rahisine aday olabilmektedirler(21).
Psikolojik De¤erlendirmeEn önemli de¤erlendirme kriterlerinden biri de psikolojik de¤er-
lendirmedir. Hastada psikolojik de¤erlendirme yap›lmamas›, ameli-yat› yapan cerrah için büyük sorunlara yol açmaktad›r. Bilerek veyabilmeyerek ikincil kazanç peflinde olanlar, kiflilik bozukluklar›, a¤›rdepresyon ve psikoz görülen hastalarda bu cerrahi ve acil d›fl›ndaher cerrahi kesinlikle kontraendikedir.
fiekil 2: Diskografi diskin iç yap›s› ve anulus hakk›nda bilgi vermekte, bu arada a¤r› provokasyonunun olup olmad›¤›na bak›lmaktad›r.
fiekil 3: MR ve BT anjiografi ile arter venin bifurkasyon ölçümü görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 233
233Prof. Dr. Ali Fahir ÖZER
Önceki Spinal CerrahiDaha önce laminektomi ve diskektomi gibi hastal›klar› geçiren
hastalar, bu cerrahi için uygun de¤ildirler. Ancak, çok seçilmifl flavalligaman› korunmufl ve posterior cerrahi s›ras›nda faset eklemlerinedokunulmam›fl hastalar, daha sonra gerekirse önden disk protezi cer-rahisine aday olabilmektedirler(21).
Psikolojik De¤erlendirmeEn önemli de¤erlendirme kriterlerinden biri de psikolojik de¤er-
lendirmedir. Hastada psikolojik de¤erlendirme yap›lmamas›, ameli-yat› yapan cerrah için büyük sorunlara yol açmaktad›r. Bilerek veyabilmeyerek ikincil kazanç peflinde olanlar, kiflilik bozukluklar›, a¤›rdepresyon ve psikoz görülen hastalarda bu cerrahi ve acil d›fl›ndaher cerrahi kesinlikle kontraendikedir.
fiekil 2: Diskografi diskin iç yap›s› ve anulus hakk›nda bilgi vermekte, bu arada a¤r› provokasyonunun olup olmad›¤›na bak›lmaktad›r.
fiekil 3: MR ve BT anjiografi ile arter venin bifurkasyon ölçümü görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 233
Figure 3: Arterial bifurcation measurement via MRI and BT angiography.
Lumbar D
egenerative Disc D
isease and Dynam
ic Stabilization
261Total Disc Replacement
larger deformations will cause an asymmetrical load on the prosthesis and will cause the prosthe-sis to dislocate.
3.i. Prior Spinal Surgery Patients who have had prior laminectomy or dis-cectomy are not suitable for TDR. However, those patients with preserved flaval ligaments and those with unaffected facet joints after surgery could later become candidates for an anterior disc prosthesis if necessary (21).
3.j. Psychological EvaluationOne of the most important evaluation criteria is a psychological evaluation. Lack of a psychological evaluation can cause problems for the surgeon. Pa-tients who are, knowingly or unknowingly, pur-suing secondary gain and those with characteristic flaws, heavy depression, or psychosis are contrain-dicatory for this and any other type of surgery, ex-cept emergency cases.
4. Biomechanics and Disc Prostheses
In humans, the spinal discs are under heavy me-chanical stress. Discs are more resilient to stress than bones, and discs deform only after bones are broken. Experimental studies have shown that a healthy disc can handle loads up to 17,000 N (22,23). Discs convert their compressive load into a tensile load on their annulus via the hydrostatic pressure formed by their internal interstitial fluid. While interior annulus fi-bers absorb the shock, stiffer outer fibers dissipate the compressive load (24). The high tensile strength of the annulus prevents the degenerative disc from bulging. As the nucleus dehydrates, swelling pres-sure decreases. When the strength of the annulus decreases, the effect of the load decreases in the load dissipation discussed above. The disc subse-quently transfers its entire load to the bone struc-ture (24). Pathological loads on the disc play an im-portant role on disc degeneration. In animals, static loads cause more degeneration compared to cy-clic loads (25). When a load is excessive, disc metab-olism is reduced proportionally to the intensity of the load, and catabolic enzyme production within the disc increases. In earlier stages of degeneration, temporary increases of dynamic disc cell number
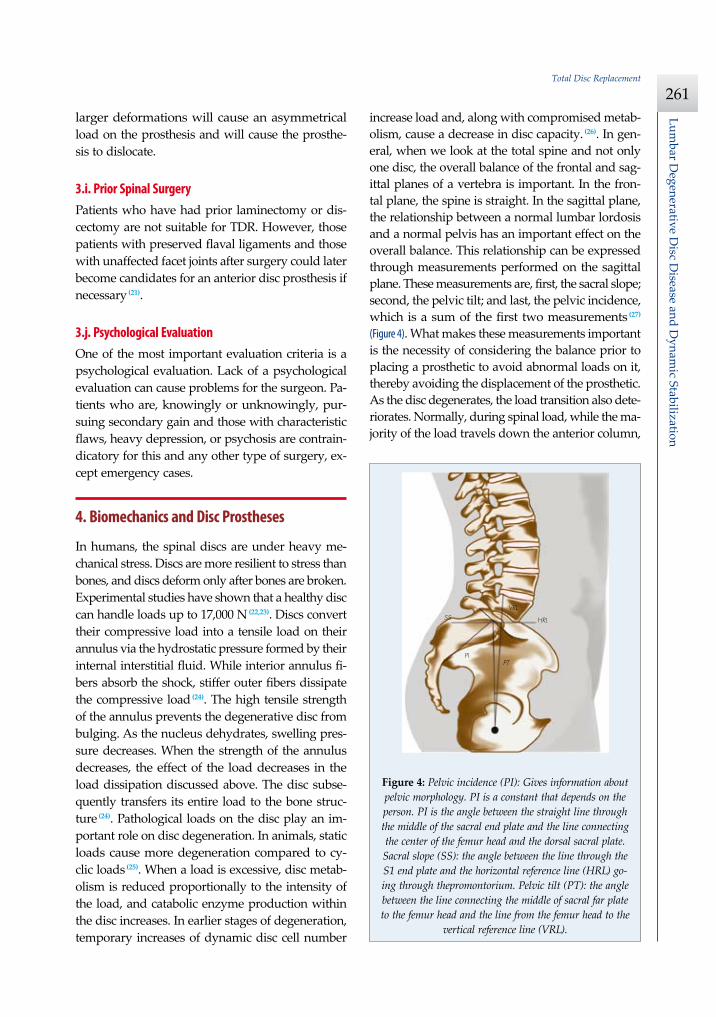
increase load and, along with compromised metab-olism, cause a decrease in disc capacity. (26). In gen-eral, when we look at the total spine and not only one disc, the overall balance of the frontal and sag-ittal planes of a vertebra is important. In the fron-tal plane, the spine is straight. In the sagittal plane, the relationship between a normal lumbar lordosis and a normal pelvis has an important effect on the overall balance. This relationship can be expressed through measurements performed on the sagittal plane. These measurements are, first, the sacral slope; second, the pelvic tilt; and last, the pelvic incidence, which is a sum of the first two measurements (27) (Figure 4). What makes these measurements important is the necessity of considering the balance prior to placing a prosthetic to avoid abnormal loads on it, thereby avoiding the displacement of the prosthetic. As the disc degenerates, the load transition also dete-riorates. Normally, during spinal load, while the ma-jority of the load travels down the anterior column,
234 Lomber Dejeneratif Disk Hastal›¤› ve Dinamik Stabilizasyon
26- TOTAL DİSK PROTEZİ
Biyomekanik ve Disk Protezi‹nsanlarda, diskin çok büyük mekanik stres alt›nda kald›¤› bilin-
mektedir. Diskin, strese kemikten daha fazla dayand›¤› ve kemik k›-r›ld›ktan sonra ancak yap›s›n›n bozuldu¤u gösterilmifltir. Deneyselçal›flmalar, 17000 N kadar olan yüklenmeleri sa¤l›kl› bir diskin kar-fl›layabildi¤ini göstermifltir(22,23). Disk üzerine gelen kompresif yüklen-meleri, içerisindeki interstisiyel s›v›da oluflan hidrostatik bas›nç yoluile anulus üzerinde gerilme (“tensile”) yüklenmelere çevirmektedir. ‹çanulus lifleri floku absorbe ederken, daha kat› olan d›fl lifler ise kom-presif yüklenmeyi çember fleklinde çevirerek da¤›tmaktad›r(24). Anulu-sun yüksek gerilim özelli¤i, dejenere diskteki kabarmay› (“bulging”)engellemektedir. Nükleustaki su kayb›na ba¤l› karfl› koyma bas›nc›(“swelling pressure”) azalmakta, anulusun sertli¤inin artmas›durumunda bahsi geçen yükün da¤›t›lmas› ile yükün etkisiazalmakta ve disk üzerine gelen tüm stresi kemik yap›ya ilet-mektedir(24). Diskin üzerine gelen patolojik yüklenmelerin, diskdejenerasyonunda önemli rol oynad›¤› ifade edilmektedir.Hayvanlarda yap›lan deneylerde statik yüklenmenin, siklikyüklenmeye göre daha çok dejenerasyona neden oldu¤ugösterilmifltir(25). Diske yap›lan afl›r› yüklenmelerde, yüklenme-nin fliddeti ile do¤ru orant›l› olarak disk metabolizmas›n›nazald›¤› ve içindeki katabolitik enzim yap›m›n›n artt›¤› orta-ya konulmufltur. Dejenerasyonun bafllang›c›nda, diskte geçiciolarak artan hareketli disk hücrelerinde daha çok yüklenme-ye neden oldu¤u ve metabolizman›n bozulmas›yla birliktedisk kapasitesinin de düflmeye bafllad›¤› görülmüfltür(26).
Genellikle tüm omurgaya bakt›¤›m›zda yaln›z bir diskinde¤il, tüm omurun frontal ve sagital plandaki dengesi deönem arz etmektedir. Frontal planda omurga düzdür. Sagitalplanda ise, normal bir lomber lordoz ile anatomik olarak nor-mal bir pelvisin sa¤l›kl› iliflkisinin tüm denge üzerinde önemlietkisi vard›r. Bu iliflkiyi sagital planda yapaca¤›m›z ölçümler-le ortaya koyabiliriz. ‹lki sakral e¤im (“slope”), di¤eri pelviktilt ve sonuncusu bu ikisinin toplam› olan pelvik insidans öl-çümleridir(27) (fiekil 4). Sözü edilen ölçümleri önemli k›lan un-sur; disk protezini yerlefltirmeden önce dengenin bu ölçümlergöz önüne al›narak ortaya konulmas› gereklili¤i, aksi haldeprotezin üzerine binen anormal yüklenmelerin protezin atma-s›na neden olmas›d›r.
Disk dejenere oldukça, üzerinden yük geçifli de bozul-maktad›r. Normalde omurgaya yap›lan bir yüklenmede, yü-kün büyük bir k›sm› anterior kolondan afla¤› inerken, sadece% 18’i posterior kolonlar› kullanmaktad›r(22). Posterior ele-mentlerden yükün afla¤› geçifli ayn› zamanda omurgan›n sa-gital dengesine, diskin dejenerasyon derecesine ve günlükyaflam s›ras›nda omurun ald›¤› postüre ba¤l›d›r.
Disk; dejenere oldukça yük anuluslardan tafl›nmaya bafl-lar ve diskin içindeki yap› sertlefltikçe, bozuk disk gelen yüküher tarafa da¤›tarak posterior kolonlar›n da normalden fazlayük tafl›mas›na neden olur. Bu durum, dejenerasyonun komfluyap›lar› nas›l y›prat›c› olarak etkiledi¤ini göstermektedir. Nor-malde diskin içinde olan anl›k rotasyon ekseni (instantenousaxis of rotation/IAR)’nin disk dejenere olmaya bafllad›¤›nda
yerini tespit etmek güçtür, ama iyice dejenere olup esnekli¤i azald›-¤›nda yani stabil döneme girdi¤inde alt vertebran›n k›k›rdak son pla-¤›na iner. Bu durumda iken, kinematik özelli¤ine bak›ld›¤›nda esnek-lik bak›m›ndan normal bir diskten fark› yokmufl gibi davranmakta-d›r(28). Ancak, disk yüksekli¤i azalmakta ve omurga biyomekani¤i de-¤iflmektedir. Bu son durumda a¤r›n›n nedeninin; art›k dejenere diskede¤il de, dejenere diskin omurga dengesinin bozulmas›na ba¤l› ola-rak adaleler, ligamanlar ve artiküler fasetler üzerine ikincil etkisindenkaynakland›¤› düflünülmelidir.
Disk Protezinin Bozuk Omurga Biyomekani¤ine EtkisiDisk protezi, disk yüksekli¤ini yeniden normale çevirmekte ve bu
flekilde foramenlerde aç›lma sa¤lamaktad›r.
fiekil 4: Pelvik insidans (PI): Pelvisin morfolojisi hakk›nda bilgi vermektedir. Kifliyeözel olup de¤iflmemekte, sakral son pla¤›n ortas›ndan geçen dik çizgi ile femur ba-fl›n›n merkezinin sakral uç pla¤›n›n orta noktas›n› birlefltiren çizgi aras›nda kalanaç›y› göstermektedir. Sakral slop (SS): S1 son pla¤›ndan geçen çizgi ile promontoriumdan geçen hori-zontal referans çizgi (horizontal reference line/HRL) aras›nda kalan aç›d›r. Pelvik tilt (PT): Sakral uç pla¤›n ortas›n›, femur bafl›na birlefltiren çizgi ile femur ba-fl›ndan geçen vertikal referans çizgi (vertical reference line/VRL) aras›ndaki aç›d›r.
HRL
PIPT
VRLSS
bolum26.qxp 4/18/11 2:12 PM Page 234
Figure 4: Pelvic incidence (PI): Gives information about pelvic morphology. PI is a constant that depends on the person. PI is the angle between the straight line through the middle of the sacral end plate and the line connecting the center of the femur head and the dorsal sacral plate. Sacral slope (SS): the angle between the line through the S1 end plate and the horizontal reference line (HRL) go-ing through thepromontorium. Pelvic tilt (PT): the angle between the line connecting the middle of sacral far plate to the femur head and the line from the femur head to the
vertical reference line (VRL).
Lum
bar D
egen
erat
ive
Dis
c D
isea
se a
nd D
ynam
ic S
tabi
lizat
ion
262Ali Fahir OZER M.D., Murat COSAR M.D.
only 18% of it utilizes posterior columns (22). The trans-duction of the load down the posterior elements also depends on the sagittal balance of the spine, the de-gree of disc degeneration, and the posture the verte-bra takes during daily life. As the disc degenerates, the load moves from the annulus. Subsequently, as the intradiscal structure hardens, the impaired disc spreads the load everywhere, causing the posterior columns to carry more load than usual. This situa-tion demonstrates how degeneration affects neigh-boring structures adversely. During the start of de-generation, it is hard to locate the instantaneous axis of rotation (IAR), which is normally located within the disc. However, once degeneration increases to the point of reduced elasticity of the disc and sta-bilizes, IAR moves to the cartilage end plate of the bottom vertebra. In this state, the disc will behave no differently from a normal disc with respect to its elasticity (28). However, the disc height decreases, and spine biomechanics change. It is thought that in this last stage, the cause of pain is no longer the degenerative disc, but rather secondary effects on the muscles, ligaments, and articular facets caused by compromised spine balance.
Effect of Disc Prosthesis on Compromised Spine BiomechanicsA disc prosthesis converts the disc height to normal levels, allowing the foramen to open. By allowing the posterior annulus (dense in mechanical recep-tors) to stretch, the prosthesis corrects the propri-oceptive capacity, which, in turn, is an important step in achieving spine balance. The goal is not in-creasing or decreasing final disc height but achiev-ing normal disc height. The most problematic disc space is the lumbar 5–sacral 1(L5-S1) vertebral space. Due to the sacral slope, this disc’s frontal height is high compared to its backside; thus, the choice of a prosthetic comparable to this disc’s angle is im-portant. By ensuring the load travels centrally and converting the degenerative disc’s dynamic to nor-mal from its increased or reduced elasticity, neigh-boring tissues are protected from abnormal loads. Although the IAR is usually at the manufacturing company’s suggested site when a disc prosthesis is placed, the prosthesis should ideally be placed with its rotation center on the sagittal plane, slightly be-hind the spine’s medial line and slightly below the cartilage end plate of the bottom vertebra (29). Total
disc prostheses allow for forward, backward, and sideways bending and rotation. Ligaments, the pro-prioceptive nervous system, and muscles control all these movements. While excessive movements are stopped by the original disc’s anatomic structure, the disc prosthesis device itself limits them. The re-turn of load and movement to normal in the seg-ment containing a disc prosthesis will restore pos-ture and improve spine balance (30).
5. Clinical Results
Among lumbar disc prostheses, the Charité is the most widely used. After Bütner-Janz and Schel-nack (10) published their positive clinical observations, this prosthesis’s use has become prevalent across the world. The first part of an important two-part study in the USA under the supervision of the Food and Drug Administration (FDA) was the comparison of multi-center, randomized, and fusion studies. This study found TDR to be more effective than fusion (31). In the second part of the study, the disc prosthesis improved the range of motion (ROM) compared to before surgery. Because the disc height returned back to normal, cages between vertebrae had less subsid-ence (32). Since that study, there have been many pos-itive clinical results published regarding the Charité disc (31,33-35). In contrast to all these positive results, the study published by Putzier (36) in 2006 was disappoint-ing. Because the previously manufactured Charité was the oldest study and promised many years of success, Putzier used 84 Charité I, II, and III discs on 71 patients. This researcher’s results indicated 60% of patients developed ankylosis. Although Putzier did not observe neighboring segment disease in 17% of patients who were defined as functional, these pa-tients were less satisfied than those with fusion re-sults. Putzier concluded by recommending the fu-sion technique. Although Putzier’s thoughts pleased the defenders of fusion, it is hard to know how ex-tensive the long-term follow up will be due to the need to consider the reality of human aging. A disc that was normal 17 years ago could go into ankylo-sis as a result of a natural process.
Why do we blame a prosthesis that has served its purpose for a period of time and subsequently gone into ankylosis when we should be applaud-ing it? Additionally, 17% of the group had pain, but is the cause of pain the level of the prosthesis or a

Lumbar D
egenerative Disc D
isease and Dynam
ic Stabilization
263Total Disc Replacement
spine that has aged 17 years? If these results had been observedthree to five years earlier, they might have been more meaningful, but 17 years is quite a long time! Freeman and Davenport (37), through literature searches involving a randomized dou-ble-blind study, two systematic studies, seven pro-spective studies, and eight retrospective studies, investigated the clinical outcomes of Charité and ProDisc II. These authors concluded through eval-uations of outcomes of TDR and lumbar fusion sur-gery that neither prosthesishas an advantage over the other. They also stated that long-term effects on neighboring segments and the complications that might arise later are not yet clear.
Punt et al. (38) determined that 75 patients in the Netherlands who received the SB Charité disc had continued, unexplained back and leg pain. These researchers stated that the sources of late compli-cations observed in 1000 patients who received a Charité disc prosthesis are chips, neighboring seg-ment degenerations, facet joint degenerations, and prosthesis migration. Researchers who applied fu-sion to 37 of these patients emphasized the danger-ous complications that could arise later from disc prosthesis surgery. The ProDisc, known as the “ball-socket” in the literature due to its structure, later came into use. In this mechanism, a hemisphere moves in its socket and includes a slippery poly-ethylene substance, which is also used in hip joint prostheses, between the plates that helps with move-ment and can prevent wear debris over time. Mar-nay (11) was the first to design and publish results of this disc in patients. ProDisc research groups have been formed with Marnay, and positive clinical re-sults have been published (39,40). A study under FDA supervision about ProDisc was published in 2007. While emphasizing the benefits of ProDisc in many parameters compared to fusion, the study was com-pleted with 0% complications (41).
The Maverick disc also works with a “ball-socket” mechanism. What makes it different from ProDisc is that it is made of two parts (male and female) and lacks a polyethylene piece in the middle to prevent wear debris. The center of motion, especially when placed in the disc space, is designed to fall behind the spinal medial line, and the disc is a metal-on-metal structure. The Maverick received approval for use in Europe in 2001. In 2003, after FDA approval in the United States, the Maverick has come under
close surveillance for material, strength, wear debris, and ease of surgical implementation. Successful re-sults from a series of clinical studies performed in France were published by Le Huec (42). In a separate study, these researchers applied the Maverick disc prosthesis to patients presenting with healthy facet joints who had first- and second-degree degenerated discs with fatty degenerated and thus weak mus-cles. While emphasizing the success of the study, these researchers reported the reduction of the load on facet joints, even with the presence of weakened muscle support (43).
Currently, clinical studies are being performed on MobiDisc, AcroSex, and Active-L, all of which had successful preliminary results. In our clinic, the Maverick disc has been used in a 20-patient series. To achieve objective results for pre- and post-sur-gery, the patients have been observed by the Phys-ical Therapy and Rehabilitation Department of the American Hospital. The visual analogue scale and Oswestry point system, performed pre- and post-surgery, have shown better results than single-level fusion in every aspect. In our meticulously chosen patient group, a complication rate of 0% has been observed (20,44). Together with the Physical Therapy and Rehabilitation Department, a treatment regimen has been developed for after surgery. To those pa-tients presenting to our clinic with disc herniations and nerve root ending compressions within chan-nels, disc prostheses are placed via anterior discec-tomy. It should be noted that lumbar disc hernia-tion is not contraindicatory (45).
Given these successes, why have we placed so few disc prostheses? The reason is that for those pa-tients previously indicating lumbar disc prostheses, we currently place posterior dynamic supports. By repairing these patients’ discs and providing dy-namic stabilization, we have observed that their discs almost return to normal within one year of fol-low-up. No prosthesis is as good as a patient’s own disc. In the United States and in Europe, many cen-ters place prostheses in patients’ discs if their poste-rior walls are torn, but the discs contain liquid ma-terial, and the disc heights are almost intact. Many of these discs can be preserved by strengthening via a dynamic system without the need to replace the discs. We should also remember that many of the prostheses used currently do not resemble the original and, at minimum, do not have the effect of

Lum
bar D
egen
erat
ive
Dis
c D
isea
se a
nd D
ynam
ic S
tabi
lizat
ion
264Ali Fahir OZER M.D., Murat COSAR M.D.
spreading the load or absorbing shock. These pros-theses provide movement within normal physio-logical limits and provide a healthy transfer of load downwards. It is not yet known what their effect on neighboring segments is (46).
6. Surgical Technique
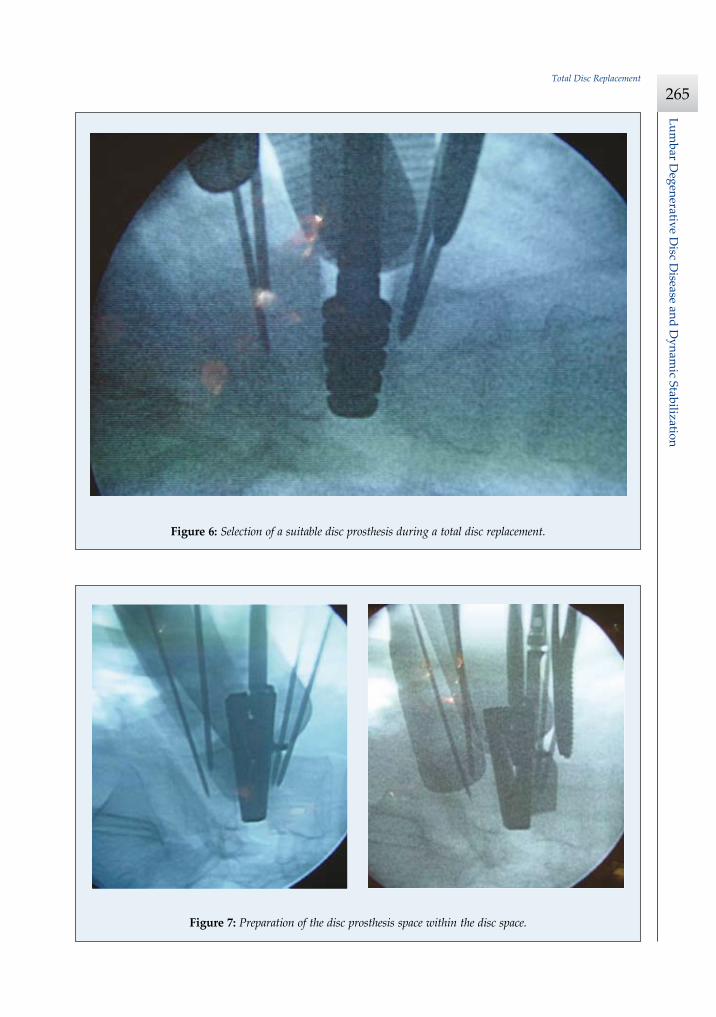
The anterior approach to the lumbar region is dis-cussed in another chapter of this book. The lumbar region is approached by following the minimally invasive method defined by Mayer (39). A modifica-tion is added to this approach to see the work field better, and the peritoneal leaves are sewn onto each other to prevent the intestines and the omentum from blocking the field of vision (18). The workspace is established by exposing the anterior part of the lumbar region and placing the right retractors. The size of the disc is determined with disc size mea-surement tools, and the median line is subsequently marked (Figure 5). Discectomy follows scope confirma-tion. Discectomy performed under a microscope re-duces possible complications. At this stage, with mea-surement tools in the prosthesis set, disc height and angle are measured, and a suitable prosthesis is se-lected (Figure 6). The posterior annulus is removed if necessary. If osteophytes are present, they should be cleared. At this point, it is possible to remove any previously detected disc material that causes herni-ation within the channel. Afterwards, the prosthe-sis site is prepared with the use of the device pro-vided to prepare the disc space under the microscope
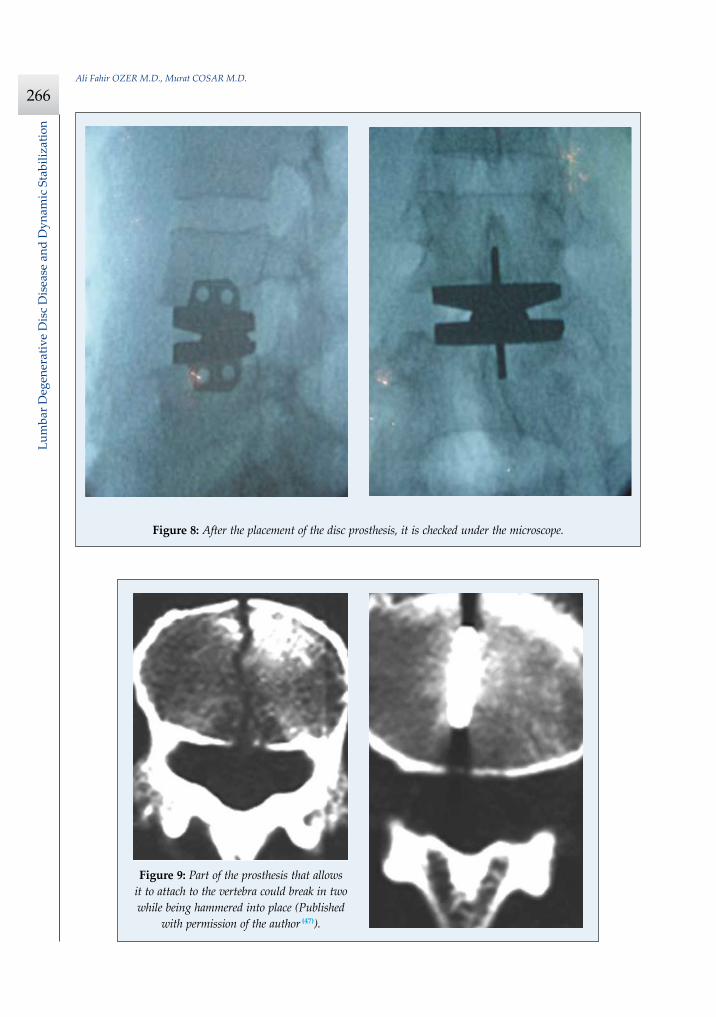
(Figure 7). The next step is to place the prosthesis un-der the microscope (Figure 8).
7. Complications
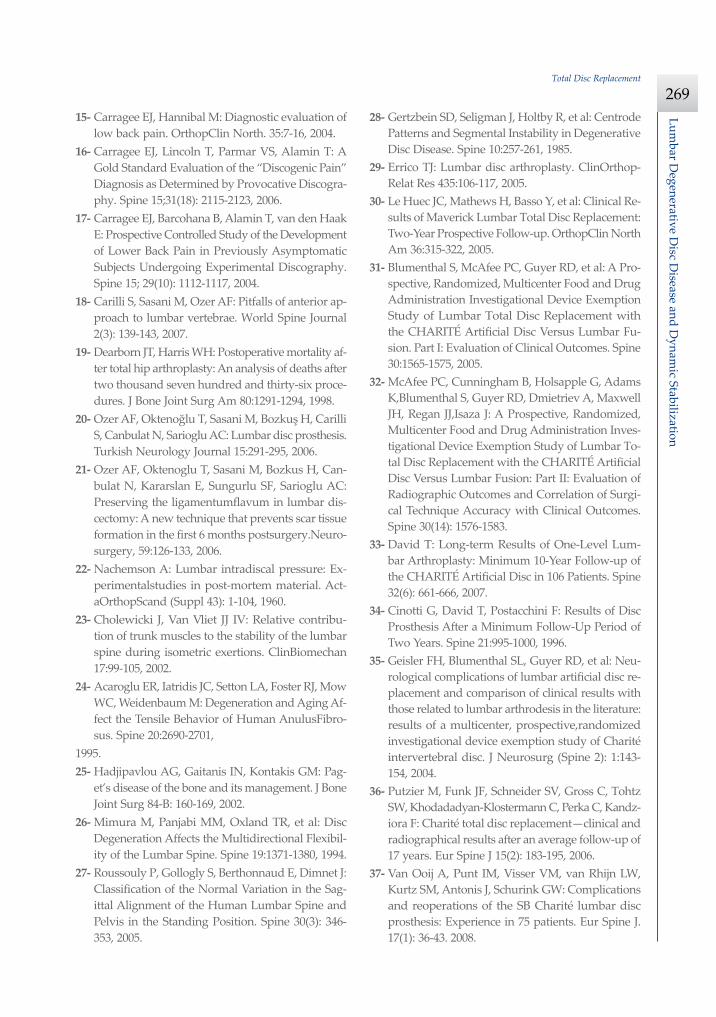
Internal organ damage, especially intestinal, can be observed. Vascular damage, especially venous damage, is important and could become fatal. It is quite possible to see vascular damage as more ves-sels are being slid off the top of the disc space. Ar-terial damage is less likely and is also easier to con-trol and fix. During discectomy, disc roots could be damaged, the dura could open, and a cerebro-spinal fluid (CSF) fistula could develop. The verte-bra could break while placing the prosthesis (47) (Fi-gure 9). The disc prosthesis could become embedded within the vertebra (48) (Figure 10), or the top part could slide off forward off the bottom part (49) (Figure 11). The prosthesis could also enter the disc space and com-press the neural tissue.
The most serious complications are infection and an unsuccessful operation. Since 1989, over 1000 pa-tients have had the SB Charité disc prosthesis ap-plied. These patients are not part of a partnered or planned study. Of these cases, 75 who have com-plained of back and leg pain were followed up for two years. While 34% of this group required a sec-ond surgery, 6% of the causes of discomfort were determined to be major complications.
The majority of complications in this patient group were caused by embedding of the prosthe-sis in to the vertebra, neighboring segment disease, facet joint disease, incompatibility of disc space size,
236 Lomber Dejeneratif Disk Hastal›¤› ve Dinamik Stabilizasyon
26- TOTAL DİSK PROTEZİ
fiu anda klinik seri sonuçlar› tam olarak aç›klanmayan, fakat önçal›flmalar› baflar›l› olan MobiDisc, AccuFlex ve Active-L disklerininde klinik çal›flmalar› yap›lmaktad›r.
Klini¤imizde Maverick diski kullan›lm›fl; yirmi hastal›k serimizde,sonuçlar ameliyat öncesi ve sonras› dönemde daha da objektif ola-bilmek amac›yla Amerikan Hastanesi Fizik Tedavi ve RehabilitasyonBölümü taraf›ndan de¤erlendirilip izlenmifltir. Görsel analog skalas›(visual analog scale/VAS) ve Oswestry puanlamas›, ameliyat öncesive sonras› dönemde yap›lm›fl ve sonuçlar her aç›dan tek seviye füz-yondan tart›fl›lmaz derecede baflar›l› bulunmufltur. Son derece özen-le seçilmifl hasta grubunda majör komplikasyon oran› % 0 görülmüfl-tür(20,44). Fizik Tedavi ve Rehabilitasyon Bölümü ile birlikte hastalar›nameliyat sonras› rehabilitasyonlar› için de bir tedavi ritüeli gelifltiril-mifltir. Kanal içinde sinir köküne bas› yapan disk herniasyonu ile kli-ni¤imize baflvuran hastalara, taraf›m›zdan anterior yolla diskektomiyap›larak protez konulmakta ve lomber disk herniasyonunun bir kon-traendikasyon olmad›¤› belirtilmektedir(45).
O halde, niçin lomber disk protezi uygulamalar›m›z bu denli azsay›da? Çünkü daha önce lomber disk protezi endikasyonu koydu-¤umuz hastalar›n büyük bir k›sm›na, flu anda posterior dinamik des-tek koymaktay›z. Bu hastalar›n disklerini tamir ederek, posterior di-namik stabilizasyonla destekledi¤imizde, disklerin bir sene sonraki kon-trollerinde neredeyse normale döndü¤ünü görmekteyiz. Hiçbir protez,hastan›n kendi diski kadar de¤erli de¤ildir. Amerika Birleflik Devletlerive Avrupa’n›n birçok merkezinde posterior duvar› y›rt›k ama neredey-se sa¤lama yak›n yüksekli¤i olan ve su muhtevas› içeren diske protezkonulmaktad›r. Bu disklerin ço¤unu ç›karmaya gerek kalmadan dina-mik sistemle destekleyerek korumak mümkündür. Yine unutmamal›y›zki, flu anda kullan›mda olan protezlerden hiçbiri orijinaline benzeme-mekte ve en az›ndan yükü da¤›tmak veya floku absorbe edici etkisi bu-lunmamaktad›r. Fizyolojik s›n›rlarda harekete olanak vermekte ve yü-kün afla¤› do¤ru sa¤l›kl› iletilmesini sa¤lamaktad›r. Komflu segmentüzerine etkisinin ne oldu¤u bile henüz bilinmemektedir(46).
Cerrahi TeknikAnterior yolla lomber bölgeye yaklafl›m, kitapta ayr› bir bölüm
olarak ele al›nm›flt›r. Mayer’in(39) tan›mlad›¤› minimal invaziv yakla-fl›mla lomber bölgeye inilmektedir. Bu yaklafl›ma sahay› daha iyi gör-mek için bir modifikasyon eklenmekte ve iç ve d›fl periton yapraklar›birbirine dikilerek ba¤›rsaklar›n ve omentumun sahay› kapatmas› en-gellenmektedir(18). Lomber bölgenin ön yüzü ortaya konulup ve uygunekartörler yerlefltirilip çal›fl›lacak mesafe belirlenerek, setin içindedisk büyüklüklerini gösteren ölçerlerle konulacak diskin büyüklü¤ütespit edilmekte ve takiben orta hat iflaretlenmektedir (fiekil 5). Skopiile teyit edildikten sonra, diskektomiye geçilmektedir. Diskektomininmikroskopla yap›lmas›, oluflacak komplikasyon olas›l›¤›n› düflürmek-tedir. Bu aflamada, protez setindeki ölçerleri kullanarak disk yüksek-li¤i ve aç›s› ölçülerek uygun disk protezi seçilmektedir (fiekil 6). Pos-terior anulus gerekirse al›nmakta ve osteofitler varsa mutlaka temiz-lenmesi gerekmektedir. Bu aflamada, ameliyat öncesi tespit edilmiflbir herniasyon varsa kanal içinde herniye olmufl disk materyalini deç›karmak mümkündür. Daha sonra, disk mesafesini haz›rlayan aletleskopi alt›nda protezin yeri haz›rlanmaktad›r (fiekil 7). Bundan sonra-ki aflama, yine skopi alt›nda protezi yerlefltirmek olacakt›r (fiekil 8).
KomplikasyonlarKar›n içi organ, özellikle ba¤›rsak yaralanmalar› görülebilmek-
tedir. Damar yaralanmas› özellikle venöz yaralanmalar çok önem-li olup, mortal seyredebilmektedir. Daha çok damar›n, disk mesafe-si üstünden s›yr›l›rken, zedelenme ihtimali çok yüksek olur. Arteryelyaralanmalar daha az görülmekte ve kontrol alt›na al›n›p tamiredilmesi daha kolay olmaktad›r. Diskektomi s›ras›nda sinir köklerizedelenebilmekte, dura aç›labilmekte ve bos fistülü geliflebilmekte-dir. Protez yerlefltirilirken omur k›r›labilmektedir(47) (fiekil 9). Diskprotezi omurun içine gömülebilmekte(48) (fiekil 10) veya üst parça
fiekil 5: Paramedian retroperitoneal yaklafl›mda cilt insizyonu görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 236
236 Lomber Dejeneratif Disk Hastal›¤› ve Dinamik Stabilizasyon
26- TOTAL DİSK PROTEZİ
fiu anda klinik seri sonuçlar› tam olarak aç›klanmayan, fakat önçal›flmalar› baflar›l› olan MobiDisc, AccuFlex ve Active-L disklerininde klinik çal›flmalar› yap›lmaktad›r.
Klini¤imizde Maverick diski kullan›lm›fl; yirmi hastal›k serimizde,sonuçlar ameliyat öncesi ve sonras› dönemde daha da objektif ola-bilmek amac›yla Amerikan Hastanesi Fizik Tedavi ve RehabilitasyonBölümü taraf›ndan de¤erlendirilip izlenmifltir. Görsel analog skalas›(visual analog scale/VAS) ve Oswestry puanlamas›, ameliyat öncesive sonras› dönemde yap›lm›fl ve sonuçlar her aç›dan tek seviye füz-yondan tart›fl›lmaz derecede baflar›l› bulunmufltur. Son derece özen-le seçilmifl hasta grubunda majör komplikasyon oran› % 0 görülmüfl-tür(20,44). Fizik Tedavi ve Rehabilitasyon Bölümü ile birlikte hastalar›nameliyat sonras› rehabilitasyonlar› için de bir tedavi ritüeli gelifltiril-mifltir. Kanal içinde sinir köküne bas› yapan disk herniasyonu ile kli-ni¤imize baflvuran hastalara, taraf›m›zdan anterior yolla diskektomiyap›larak protez konulmakta ve lomber disk herniasyonunun bir kon-traendikasyon olmad›¤› belirtilmektedir(45).
O halde, niçin lomber disk protezi uygulamalar›m›z bu denli azsay›da? Çünkü daha önce lomber disk protezi endikasyonu koydu-¤umuz hastalar›n büyük bir k›sm›na, flu anda posterior dinamik des-tek koymaktay›z. Bu hastalar›n disklerini tamir ederek, posterior di-namik stabilizasyonla destekledi¤imizde, disklerin bir sene sonraki kon-trollerinde neredeyse normale döndü¤ünü görmekteyiz. Hiçbir protez,hastan›n kendi diski kadar de¤erli de¤ildir. Amerika Birleflik Devletlerive Avrupa’n›n birçok merkezinde posterior duvar› y›rt›k ama neredey-se sa¤lama yak›n yüksekli¤i olan ve su muhtevas› içeren diske protezkonulmaktad›r. Bu disklerin ço¤unu ç›karmaya gerek kalmadan dina-mik sistemle destekleyerek korumak mümkündür. Yine unutmamal›y›zki, flu anda kullan›mda olan protezlerden hiçbiri orijinaline benzeme-mekte ve en az›ndan yükü da¤›tmak veya floku absorbe edici etkisi bu-lunmamaktad›r. Fizyolojik s›n›rlarda harekete olanak vermekte ve yü-kün afla¤› do¤ru sa¤l›kl› iletilmesini sa¤lamaktad›r. Komflu segmentüzerine etkisinin ne oldu¤u bile henüz bilinmemektedir(46).
Cerrahi TeknikAnterior yolla lomber bölgeye yaklafl›m, kitapta ayr› bir bölüm
olarak ele al›nm›flt›r. Mayer’in(39) tan›mlad›¤› minimal invaziv yakla-fl›mla lomber bölgeye inilmektedir. Bu yaklafl›ma sahay› daha iyi gör-mek için bir modifikasyon eklenmekte ve iç ve d›fl periton yapraklar›birbirine dikilerek ba¤›rsaklar›n ve omentumun sahay› kapatmas› en-gellenmektedir(18). Lomber bölgenin ön yüzü ortaya konulup ve uygunekartörler yerlefltirilip çal›fl›lacak mesafe belirlenerek, setin içindedisk büyüklüklerini gösteren ölçerlerle konulacak diskin büyüklü¤ütespit edilmekte ve takiben orta hat iflaretlenmektedir (fiekil 5). Skopiile teyit edildikten sonra, diskektomiye geçilmektedir. Diskektomininmikroskopla yap›lmas›, oluflacak komplikasyon olas›l›¤›n› düflürmek-tedir. Bu aflamada, protez setindeki ölçerleri kullanarak disk yüksek-li¤i ve aç›s› ölçülerek uygun disk protezi seçilmektedir (fiekil 6). Pos-terior anulus gerekirse al›nmakta ve osteofitler varsa mutlaka temiz-lenmesi gerekmektedir. Bu aflamada, ameliyat öncesi tespit edilmiflbir herniasyon varsa kanal içinde herniye olmufl disk materyalini deç›karmak mümkündür. Daha sonra, disk mesafesini haz›rlayan aletleskopi alt›nda protezin yeri haz›rlanmaktad›r (fiekil 7). Bundan sonra-ki aflama, yine skopi alt›nda protezi yerlefltirmek olacakt›r (fiekil 8).
KomplikasyonlarKar›n içi organ, özellikle ba¤›rsak yaralanmalar› görülebilmek-
tedir. Damar yaralanmas› özellikle venöz yaralanmalar çok önem-li olup, mortal seyredebilmektedir. Daha çok damar›n, disk mesafe-si üstünden s›yr›l›rken, zedelenme ihtimali çok yüksek olur. Arteryelyaralanmalar daha az görülmekte ve kontrol alt›na al›n›p tamiredilmesi daha kolay olmaktad›r. Diskektomi s›ras›nda sinir köklerizedelenebilmekte, dura aç›labilmekte ve bos fistülü geliflebilmekte-dir. Protez yerlefltirilirken omur k›r›labilmektedir(47) (fiekil 9). Diskprotezi omurun içine gömülebilmekte(48) (fiekil 10) veya üst parça
fiekil 5: Paramedian retroperitoneal yaklafl›mda cilt insizyonu görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 236
Figure 5: Skin incision in the paramedian retroperitoneal approach.
Lumbar D
egenerative Disc D
isease and Dynam
ic Stabilization
265Total Disc Replacement
237Prof. Dr. Ali Fahir ÖZER
alttaki parçan›n üstünden öne kayabilmektedir(49) (fiekil 11). Mesafeiçine girilebilmekte ve nöral dokuya bas› oluflabilmektedir. En önem-li komplikasyon, enfeksiyon geliflmesi ve ifllemin tam bir felaketle so-nuçlanmas›d›r.
1989 y›l›ndan itibaren Hollanda’da 1000’in üzerinde olguya SBCharité disk protezi uygulanm›fl olup, bu olgular herhangi ortak plan-lanm›fl bir çal›flman›n parças› da de¤ildiler. Bu olgulardan bel ve ba-cak a¤r›s›ndan yak›nan 75 tanesi iki y›ll›k izleme al›nm›fl; % 34’ündeikinci ameliyata gerek görülürken, % 6’s›nda ise yak›nman›n nedeni
çok ciddi komplikasyonlar olarak tespit edilmifltir. Bu çal›flmada komp-likasyonlar irdelendi¤inde ise; en fazla protezin omura gömülmesi,komflu segment hastal›¤›, faset eklem dejenerasyonu, protez mesafe bü-yüklü¤ünün uyumsuzlu¤u ve dejeneratif skolyoz oldu¤u görülmüfltür. Te-davi olarak, olgular›n 22’sinde posterior füzyon yap›lm›fl ve 24’ündeise yaln›zca protez ç›kar›lm›fl ve bu grubun bile ameliyat öncesindendaha iyi oldu¤u vurgulanm›flt›r. TDR komplikasyonlar›na ba¤l› revizyoncerrahisinde mortalite oran› yüksektir. Büyük damarlar›n etraf›nda te-flekkül eden ba¤ dokusunun temizlenmesi en büyük sorundur.
fiekil 6: Total disk protezi cerrahisi s›ras›nda, uygun disk protezinin seçimi görülmektedir.
fiekil 7: Mesafe içinde disk protezi yuvas›n›n haz›rlanmas› görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 237
Figure 6: Selection of a suitable disc prosthesis during a total disc replacement.
237Prof. Dr. Ali Fahir ÖZER
alttaki parçan›n üstünden öne kayabilmektedir(49) (fiekil 11). Mesafeiçine girilebilmekte ve nöral dokuya bas› oluflabilmektedir. En önem-li komplikasyon, enfeksiyon geliflmesi ve ifllemin tam bir felaketle so-nuçlanmas›d›r.
1989 y›l›ndan itibaren Hollanda’da 1000’in üzerinde olguya SBCharité disk protezi uygulanm›fl olup, bu olgular herhangi ortak plan-lanm›fl bir çal›flman›n parças› da de¤ildiler. Bu olgulardan bel ve ba-cak a¤r›s›ndan yak›nan 75 tanesi iki y›ll›k izleme al›nm›fl; % 34’ündeikinci ameliyata gerek görülürken, % 6’s›nda ise yak›nman›n nedeni
çok ciddi komplikasyonlar olarak tespit edilmifltir. Bu çal›flmada komp-likasyonlar irdelendi¤inde ise; en fazla protezin omura gömülmesi,komflu segment hastal›¤›, faset eklem dejenerasyonu, protez mesafe bü-yüklü¤ünün uyumsuzlu¤u ve dejeneratif skolyoz oldu¤u görülmüfltür. Te-davi olarak, olgular›n 22’sinde posterior füzyon yap›lm›fl ve 24’ündeise yaln›zca protez ç›kar›lm›fl ve bu grubun bile ameliyat öncesindendaha iyi oldu¤u vurgulanm›flt›r. TDR komplikasyonlar›na ba¤l› revizyoncerrahisinde mortalite oran› yüksektir. Büyük damarlar›n etraf›nda te-flekkül eden ba¤ dokusunun temizlenmesi en büyük sorundur.
fiekil 6: Total disk protezi cerrahisi s›ras›nda, uygun disk protezinin seçimi görülmektedir.
fiekil 7: Mesafe içinde disk protezi yuvas›n›n haz›rlanmas› görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 237
237Prof. Dr. Ali Fahir ÖZER
alttaki parçan›n üstünden öne kayabilmektedir(49) (fiekil 11). Mesafeiçine girilebilmekte ve nöral dokuya bas› oluflabilmektedir. En önem-li komplikasyon, enfeksiyon geliflmesi ve ifllemin tam bir felaketle so-nuçlanmas›d›r.
1989 y›l›ndan itibaren Hollanda’da 1000’in üzerinde olguya SBCharité disk protezi uygulanm›fl olup, bu olgular herhangi ortak plan-lanm›fl bir çal›flman›n parças› da de¤ildiler. Bu olgulardan bel ve ba-cak a¤r›s›ndan yak›nan 75 tanesi iki y›ll›k izleme al›nm›fl; % 34’ündeikinci ameliyata gerek görülürken, % 6’s›nda ise yak›nman›n nedeni
çok ciddi komplikasyonlar olarak tespit edilmifltir. Bu çal›flmada komp-likasyonlar irdelendi¤inde ise; en fazla protezin omura gömülmesi,komflu segment hastal›¤›, faset eklem dejenerasyonu, protez mesafe bü-yüklü¤ünün uyumsuzlu¤u ve dejeneratif skolyoz oldu¤u görülmüfltür. Te-davi olarak, olgular›n 22’sinde posterior füzyon yap›lm›fl ve 24’ündeise yaln›zca protez ç›kar›lm›fl ve bu grubun bile ameliyat öncesindendaha iyi oldu¤u vurgulanm›flt›r. TDR komplikasyonlar›na ba¤l› revizyoncerrahisinde mortalite oran› yüksektir. Büyük damarlar›n etraf›nda te-flekkül eden ba¤ dokusunun temizlenmesi en büyük sorundur.
fiekil 6: Total disk protezi cerrahisi s›ras›nda, uygun disk protezinin seçimi görülmektedir.
fiekil 7: Mesafe içinde disk protezi yuvas›n›n haz›rlanmas› görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 237
Figure 7: Preparation of the disc prosthesis space within the disc space.
Lum
bar D
egen
erat
ive
Dis
c D
isea
se a
nd D
ynam
ic S
tabi
lizat
ion
266Ali Fahir OZER M.D., Murat COSAR M.D.
238 Lomber Dejeneratif Disk Hastal›¤› ve Dinamik Stabilizasyon
26- TOTAL DİSK PROTEZİ
Gerçekten de yaflamsal vasküler yap›la-r›n bulundu¤u bu bölgede yeniden bir ante-rior yaklafl›m›n yap›lmas› neredeyse imkân-s›zd›r(51). Özellikle öne kayan disklerde ma-jör damar komplikasyonlar› görülebilmekteve ameliyata mutlaka bir damar cerrahisiuzman› ile girilmesi önerilmektedir. Reviz-yon cerrahisi s›ras›nda damarlar›n y›rt›lmas›ve ameliyat sonras› trombüs teflekkülü nere-deyse kaç›n›lmaz olmaktad›r(52).
van Ooij ve arkadafllar›(37), 27 olgulukkomplikasyonlar› içeren serilerinde faset ek-lemlerinde ve komflu mesafede diskte dejene-rasyon ile protezin kaymas›n›n veya omur içi-ne çökmesinin en fazla memnuniyetsizlik ne-denleri oldu¤unu söylemifllerdir. Protez k›r›l-mas›n›n daha nadir görüldü¤ünü de söyleye-rek, disklerin biyomekani¤inin gözden geçiril-mesinin gereklili¤ini vurgulam›fllard›r. Uzunvadeli sonuçlar henüz tam olarak yay›mlan-mad›¤›ndan ne gibi komplikasyonlar›n gelifle-bilece¤inin de zamanla ortaya ç›kaca¤›n› ifa-de etmifllerdir.
fiekil 9: Protezin omur cismine tutunmas›n› sa¤la-yan parças›n›n, protez çak›l›rken omurga cisminik›rarak ikiye bölebildi¤i görülmektedir (Yazar›nizni ile yay›mlanm›flt›r(45)).
fiekil 8: Disk protezi yerlefltirildikten sonra skopi alt›ndaki kontrolünün yap›ld›¤› görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 238
238 Lomber Dejeneratif Disk Hastal›¤› ve Dinamik Stabilizasyon
26- TOTAL DİSK PROTEZİ
Gerçekten de yaflamsal vasküler yap›la-r›n bulundu¤u bu bölgede yeniden bir ante-rior yaklafl›m›n yap›lmas› neredeyse imkân-s›zd›r(51). Özellikle öne kayan disklerde ma-jör damar komplikasyonlar› görülebilmekteve ameliyata mutlaka bir damar cerrahisiuzman› ile girilmesi önerilmektedir. Reviz-yon cerrahisi s›ras›nda damarlar›n y›rt›lmas›ve ameliyat sonras› trombüs teflekkülü nere-deyse kaç›n›lmaz olmaktad›r(52).
van Ooij ve arkadafllar›(37), 27 olgulukkomplikasyonlar› içeren serilerinde faset ek-lemlerinde ve komflu mesafede diskte dejene-rasyon ile protezin kaymas›n›n veya omur içi-ne çökmesinin en fazla memnuniyetsizlik ne-denleri oldu¤unu söylemifllerdir. Protez k›r›l-mas›n›n daha nadir görüldü¤ünü de söyleye-rek, disklerin biyomekani¤inin gözden geçiril-mesinin gereklili¤ini vurgulam›fllard›r. Uzunvadeli sonuçlar henüz tam olarak yay›mlan-mad›¤›ndan ne gibi komplikasyonlar›n gelifle-bilece¤inin de zamanla ortaya ç›kaca¤›n› ifa-de etmifllerdir.
fiekil 9: Protezin omur cismine tutunmas›n› sa¤la-yan parças›n›n, protez çak›l›rken omurga cisminik›rarak ikiye bölebildi¤i görülmektedir (Yazar›nizni ile yay›mlanm›flt›r(45)).
fiekil 8: Disk protezi yerlefltirildikten sonra skopi alt›ndaki kontrolünün yap›ld›¤› görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 238
Figure 8: After the placement of the disc prosthesis, it is checked under the microscope.
Figure 9: Part of the prosthesis that allows it to attach to the vertebra could break in two while being hammered into place (Published
with permission of the author (47)).
238 Lomber Dejeneratif Disk Hastal›¤› ve Dinamik Stabilizasyon
26- TOTAL DİSK PROTEZİ
Gerçekten de yaflamsal vasküler yap›la-r›n bulundu¤u bu bölgede yeniden bir ante-rior yaklafl›m›n yap›lmas› neredeyse imkân-s›zd›r(51). Özellikle öne kayan disklerde ma-jör damar komplikasyonlar› görülebilmekteve ameliyata mutlaka bir damar cerrahisiuzman› ile girilmesi önerilmektedir. Reviz-yon cerrahisi s›ras›nda damarlar›n y›rt›lmas›ve ameliyat sonras› trombüs teflekkülü nere-deyse kaç›n›lmaz olmaktad›r(52).
van Ooij ve arkadafllar›(37), 27 olgulukkomplikasyonlar› içeren serilerinde faset ek-lemlerinde ve komflu mesafede diskte dejene-rasyon ile protezin kaymas›n›n veya omur içi-ne çökmesinin en fazla memnuniyetsizlik ne-denleri oldu¤unu söylemifllerdir. Protez k›r›l-mas›n›n daha nadir görüldü¤ünü de söyleye-rek, disklerin biyomekani¤inin gözden geçiril-mesinin gereklili¤ini vurgulam›fllard›r. Uzunvadeli sonuçlar henüz tam olarak yay›mlan-mad›¤›ndan ne gibi komplikasyonlar›n gelifle-bilece¤inin de zamanla ortaya ç›kaca¤›n› ifa-de etmifllerdir.
fiekil 9: Protezin omur cismine tutunmas›n› sa¤la-yan parças›n›n, protez çak›l›rken omurga cisminik›rarak ikiye bölebildi¤i görülmektedir (Yazar›nizni ile yay›mlanm›flt›r(45)).
fiekil 8: Disk protezi yerlefltirildikten sonra skopi alt›ndaki kontrolünün yap›ld›¤› görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 238
238 Lomber Dejeneratif Disk Hastal›¤› ve Dinamik Stabilizasyon
26- TOTAL DİSK PROTEZİ
Gerçekten de yaflamsal vasküler yap›la-r›n bulundu¤u bu bölgede yeniden bir ante-rior yaklafl›m›n yap›lmas› neredeyse imkân-s›zd›r(51). Özellikle öne kayan disklerde ma-jör damar komplikasyonlar› görülebilmekteve ameliyata mutlaka bir damar cerrahisiuzman› ile girilmesi önerilmektedir. Reviz-yon cerrahisi s›ras›nda damarlar›n y›rt›lmas›ve ameliyat sonras› trombüs teflekkülü nere-deyse kaç›n›lmaz olmaktad›r(52).
van Ooij ve arkadafllar›(37), 27 olgulukkomplikasyonlar› içeren serilerinde faset ek-lemlerinde ve komflu mesafede diskte dejene-rasyon ile protezin kaymas›n›n veya omur içi-ne çökmesinin en fazla memnuniyetsizlik ne-denleri oldu¤unu söylemifllerdir. Protez k›r›l-mas›n›n daha nadir görüldü¤ünü de söyleye-rek, disklerin biyomekani¤inin gözden geçiril-mesinin gereklili¤ini vurgulam›fllard›r. Uzunvadeli sonuçlar henüz tam olarak yay›mlan-mad›¤›ndan ne gibi komplikasyonlar›n gelifle-bilece¤inin de zamanla ortaya ç›kaca¤›n› ifa-de etmifllerdir.
fiekil 9: Protezin omur cismine tutunmas›n› sa¤la-yan parças›n›n, protez çak›l›rken omurga cisminik›rarak ikiye bölebildi¤i görülmektedir (Yazar›nizni ile yay›mlanm›flt›r(45)).
fiekil 8: Disk protezi yerlefltirildikten sonra skopi alt›ndaki kontrolünün yap›ld›¤› görülmektedir.
bolum26.qxp 4/18/11 2:12 PM Page 238

Lumbar D
egenerative Disc D
isease and Dynam
ic Stabilization
267Total Disc Replacement
239Prof. Dr. Ali Fahir ÖZER
fiekil 10: ‹ki veya daha fazla seviyede disk protezi kullan›ld›¤›nda protezlerin flok absorbe edici etkisi olmad›¤›ndandolay›, protezler aras›nda kalan omurun özellikle osteoporotikse kolayl›kla k›r›labildi¤i görülmektedir (Yazar›n izni ileyay›mlanm›flt›r (46)).
fiekil 11: Özellikle L5-S1 disklerinde L5 vertebras› s›yr›lma güçlerinin afl›r› etkisinde olup, ko-layl›kla üst protez parças›n›n, alt parçan›n üzerinden kaymas›na neden olabilir. Gözden ka-çan bir istmik defekt bu süreci h›zland›r›r (Yazar›n izni ile yay›mlanm›flt›r (47)).
SonuçTotal disk replasman›n›n endikasyonlar› limitlidir, tan›-n›n do¤rulu¤unda flüphe vard›r, k›sa süreli sonuçlar›-n›n füzyon cerrahisinden çok büyük bir fark› yoktur.TDR’nin ve di¤er füzyonsuz tekniklerin aksamadan ça-l›flmas› konusunda hâlâ flüpheler vard›r. Di¤er eklemreplasman sistemleri göz önüne al›nd›¤›nda bu siste-min bozulmayaca¤›n›n garantisi yoktur. Revizyon cer-rahisi çok ciddi risk teflkil etmektedir. Omurgada dina-mik sistem alan›nda önemli ölçüde pazar araflt›rmala-r› yapan Viscolgliosi Kardefller’in 2004 y›l›n›n May›say›nda yay›mlad›klar› rapor, TDR’nin 2010’lu y›llarakadar zirveye ç›kaca¤› ve 5 milyar dolarl›k bir rakam›yakalayaca¤›n› öngörürken, 2009 y›l›nda bu rakam›ngerçek karfl›l›¤› 1 milyar dolar olmufltur. Sonuçta dabeklenen öngörü gerçekleflmemifltir.Gelece¤in, total protezlerde mi yoksa nükleus replas-man› ya da tamirinde mi olaca¤›n› zaman gösterecek-tir.
bolum26.qxp 4/18/11 2:12 PM Page 239
239Prof. Dr. Ali Fahir ÖZER
fiekil 10: ‹ki veya daha fazla seviyede disk protezi kullan›ld›¤›nda protezlerin flok absorbe edici etkisi olmad›¤›ndandolay›, protezler aras›nda kalan omurun özellikle osteoporotikse kolayl›kla k›r›labildi¤i görülmektedir (Yazar›n izni ileyay›mlanm›flt›r (46)).
fiekil 11: Özellikle L5-S1 disklerinde L5 vertebras› s›yr›lma güçlerinin afl›r› etkisinde olup, ko-layl›kla üst protez parças›n›n, alt parçan›n üzerinden kaymas›na neden olabilir. Gözden ka-çan bir istmik defekt bu süreci h›zland›r›r (Yazar›n izni ile yay›mlanm›flt›r (47)).
SonuçTotal disk replasman›n›n endikasyonlar› limitlidir, tan›-n›n do¤rulu¤unda flüphe vard›r, k›sa süreli sonuçlar›-n›n füzyon cerrahisinden çok büyük bir fark› yoktur.TDR’nin ve di¤er füzyonsuz tekniklerin aksamadan ça-l›flmas› konusunda hâlâ flüpheler vard›r. Di¤er eklemreplasman sistemleri göz önüne al›nd›¤›nda bu siste-min bozulmayaca¤›n›n garantisi yoktur. Revizyon cer-rahisi çok ciddi risk teflkil etmektedir. Omurgada dina-mik sistem alan›nda önemli ölçüde pazar araflt›rmala-r› yapan Viscolgliosi Kardefller’in 2004 y›l›n›n May›say›nda yay›mlad›klar› rapor, TDR’nin 2010’lu y›llarakadar zirveye ç›kaca¤› ve 5 milyar dolarl›k bir rakam›yakalayaca¤›n› öngörürken, 2009 y›l›nda bu rakam›ngerçek karfl›l›¤› 1 milyar dolar olmufltur. Sonuçta dabeklenen öngörü gerçekleflmemifltir.Gelece¤in, total protezlerde mi yoksa nükleus replas-man› ya da tamirinde mi olaca¤›n› zaman gösterecek-tir.
bolum26.qxp 4/18/11 2:12 PM Page 239
Figure 10: Because the prostheses do not have shock-absorbing qualities, when two or more level prostheses are used, the vertebra between the prosthesis could easily break, especially if osteoporosis is present (Published with
permission of the author (46)).
239Prof. Dr. Ali Fahir ÖZER
fiekil 10: ‹ki veya daha fazla seviyede disk protezi kullan›ld›¤›nda protezlerin flok absorbe edici etkisi olmad›¤›ndandolay›, protezler aras›nda kalan omurun özellikle osteoporotikse kolayl›kla k›r›labildi¤i görülmektedir (Yazar›n izni ileyay›mlanm›flt›r (46)).
fiekil 11: Özellikle L5-S1 disklerinde L5 vertebras› s›yr›lma güçlerinin afl›r› etkisinde olup, ko-layl›kla üst protez parças›n›n, alt parçan›n üzerinden kaymas›na neden olabilir. Gözden ka-çan bir istmik defekt bu süreci h›zland›r›r (Yazar›n izni ile yay›mlanm›flt›r (47)).
SonuçTotal disk replasman›n›n endikasyonlar› limitlidir, tan›-n›n do¤rulu¤unda flüphe vard›r, k›sa süreli sonuçlar›-n›n füzyon cerrahisinden çok büyük bir fark› yoktur.TDR’nin ve di¤er füzyonsuz tekniklerin aksamadan ça-l›flmas› konusunda hâlâ flüpheler vard›r. Di¤er eklemreplasman sistemleri göz önüne al›nd›¤›nda bu siste-min bozulmayaca¤›n›n garantisi yoktur. Revizyon cer-rahisi çok ciddi risk teflkil etmektedir. Omurgada dina-mik sistem alan›nda önemli ölçüde pazar araflt›rmala-r› yapan Viscolgliosi Kardefller’in 2004 y›l›n›n May›say›nda yay›mlad›klar› rapor, TDR’nin 2010’lu y›llarakadar zirveye ç›kaca¤› ve 5 milyar dolarl›k bir rakam›yakalayaca¤›n› öngörürken, 2009 y›l›nda bu rakam›ngerçek karfl›l›¤› 1 milyar dolar olmufltur. Sonuçta dabeklenen öngörü gerçekleflmemifltir.Gelece¤in, total protezlerde mi yoksa nükleus replas-man› ya da tamirinde mi olaca¤›n› zaman gösterecek-tir.
bolum26.qxp 4/18/11 2:12 PM Page 239
Figure 11: Especially in the L5-S1 discs, the L5 vertebra is under a severe sliding force and could easily cause the top prosthesis to slip off of the bottom part. An overlooked ischemic effect will shorten this length of time (Pub-
lished with permission of the author (47)).

Lum
bar D
egen
erat
ive
Dis
c D
isea
se a
nd D
ynam
ic S
tabi
lizat
ion
268Ali Fahir OZER M.D., Murat COSAR M.D.
and degenerative scoliosis. As treatment, 22 of these cases underwent posterior fusion. In 24 cases, only the prostheses were removed, and even this group reported increased feeling compared to before sur-gery. Revision surgery due to TDR complications has a high mortality rate. The main complication is cleaning the connective tissue that forms around major vessels. In reality, in this region in which vital vascular structures are present, a repeat anterior ap-proach is nearly impossible (51). Major vascular com-plications are especially observedin discs that have slid forward, and surgery is recommended with a vascular surgeon present. It is almost inevitable for vessels to tear during revision surgery and for post-surgery thrombosis to arise (52).
In a 27-patient series involving complications, van Ooij et al. (37) observed that the major reasons for complaints were degeneration in facet joints and neighboring discs and sliding or embedding of the prosthesis. While acknowledging the rare occurrence of prosthesis breaks, these researchers emphasized the necessity to review disc biomechanics. Because long-term results are not yet published, these re-searchers stated that only time will tell what com-plications could develop.
8. Results
Indications of TDR are limited. The correctness of the diagnosis can be suspect, and short term outcomes are similar to those obtained from fusion surgery. There is still doubt as to whether TDR and other non-fusion techniques work without problems. When other joint replacement systems are considered, there is no guarantee as to whether this system will not fail. Revision surgery entails serious risks.
Whereas the May 2004 report published by the Viscolgliosi brothers, who have performed a consid-erable amount of marketing research in the area of spinal dynamic systems, suggested TDR will peak after 2010 and will become a five-billion-dollar in-dustry, the actual number in 2009 was one billion dollars. Thus, these researchers’ prediction has not become reality. Time will tell whether total prosthe-ses, nucleus replacement, or repair will predomi-nate in the future.
References
1- Barr JS, Mixter WJ: Posterior protrusion of the lum-bar intervertebral discs. J Bone Joint Surg 23:444-456, 1941.
2- Van Steebrugghe D: French Patent FR1122634, 1956.
3- Fernström U: Arthroplasty with intercorporalendo-prosthesis in herniated disc and painful disc. Act-aChirScand 357 (Suppl):154-159, 1966.
4- Urbaniak JR, Bright DS, Hopkins JE: Replacement of intervertebral discs in chimpanzees by silicone-Dacron implants: a preliminary report. J Biomed Mater Res 7:165-186, 1973.
5- Schneider PG, Oyen R: Surgical replacement of intervertebral disc. First communication: Replace-ment of lumbar discs with silicon-rubber. Theoreti-cal and experimental investigations. Z OrthopIhre-Grenzgeb 112:1078-1086,1974.
6- Froning EC: Intervertebral disc prosthesis and in-struments for locating same. United States Patent 3,875,595 April 8, 1975.
7- Fassio B: French Patent 2372622,30-06, 1978.8- Fassio B, Ginestie JF: Discal prosthesis made of
silicone: experimental study and 1st clinical cases. Nouv Press Med 7(3):207, 1978.
9- Büttner-Janz K, Schelnack K, Zippel H: An alterna-tive treatment strategy for lumbar disc damage us-ing the SB Charité modular disc prosthesis. Z Or-thropIhreGrenzgeb 125:1-6, 1987.
10- Büttner-Janz K, Schelnack K. Zippel H, et al: Expe-rience and results with the SB Charité lumbar in-tervertebral endoprosthesis. Zeitschrift fur Klinis-cheMedizin 43:1785-1789, 1988.
11- Marnay T: ProDisc Retrospective Clinical Study: 7-11 year follow-up. New York: Spine Solutions, 2002.
12- Boden SD, Davis DO, Dina DS, et al: Abnormal magnetic resonance scans of the lumbar spine in asymptomatic subjects: A prospective investigation. J Bone Joint Surg Am 72;403-408, 1990.
13- Boos N, Rieder N, Schade, et al: The Diagnostic Accuracy of Magnetic Resonance Imaging, Work Perception, and Psychological Factors in Identify-ing Symptomatic Disc Herniation. Spine 20:2613-2625, 1995.
14- Carragee EJ, Paragioudakis SJ, Khurana S: Value Award winner in clinical studies. Lumbar High-In-tensity Zone and Discography in Subjects Without Low Back Problems. Spine 25:2987-2992, 2000.
Lumbar D
egenerative Disc D
isease and Dynam
ic Stabilization
269Total Disc Replacement
15- Carragee EJ, Hannibal M: Diagnostic evaluation of low back pain. OrthopClin North. 35:7-16, 2004.
16- Carragee EJ, Lincoln T, Parmar VS, Alamin T: A Gold Standard Evaluation of the “Discogenic Pain” Diagnosis as Determined by Provocative Discogra-phy. Spine 15;31(18): 2115-2123, 2006.
17- Carragee EJ, Barcohana B, Alamin T, van den Haak E: Prospective Controlled Study of the Development of Lower Back Pain in Previously Asymptomatic Subjects Undergoing Experimental Discography. Spine 15; 29(10): 1112-1117, 2004.
18- Carilli S, Sasani M, Ozer AF: Pitfalls of anterior ap-proach to lumbar vertebrae. World Spine Journal 2(3): 139-143, 2007.
19- Dearborn JT, Harris WH: Postoperative mortality af-ter total hip arthroplasty: An analysis of deaths after two thousand seven hundred and thirty-six proce-dures. J Bone Joint Surg Am 80:1291-1294, 1998.
20- Ozer AF, Oktenoğlu T, Sasani M, Bozkuş H, Carilli S, Canbulat N, Sarioglu AC: Lumbar disc prosthesis. Turkish Neurology Journal 15:291-295, 2006.
21- Ozer AF, Oktenoglu T, Sasani M, Bozkus H, Can-bulat N, Kararslan E, Sungurlu SF, Sarioglu AC: Preserving the ligamentumflavum in lumbar dis-cectomy: A new technique that prevents scar tissue formation in the first 6 months postsurgery.Neuro-surgery, 59:126-133, 2006.
22- Nachemson A: Lumbar intradiscal pressure: Ex-perimentalstudies in post-mortem material. Act-aOrthopScand (Suppl 43): 1-104, 1960.
23- Cholewicki J, Van Vliet JJ IV: Relative contribu-tion of trunk muscles to the stability of the lumbar spine during isometric exertions. ClinBiomechan 17:99-105, 2002.
24- Acaroglu ER, Iatridis JC, Setton LA, Foster RJ, Mow WC, Weidenbaum M: Degeneration and Aging Af-fect the Tensile Behavior of Human AnulusFibro-sus. Spine 20:2690-2701,
1995.25- Hadjipavlou AG, Gaitanis IN, Kontakis GM: Pag-
et’s disease of the bone and its management. J Bone Joint Surg 84-B: 160-169, 2002.
26- Mimura M, Panjabi MM, Oxland TR, et al: Disc Degeneration Affects the Multidirectional Flexibil-ity of the Lumbar Spine. Spine 19:1371-1380, 1994.
27- Roussouly P, Gollogly S, Berthonnaud E, Dimnet J: Classification of the Normal Variation in the Sag-ittal Alignment of the Human Lumbar Spine and Pelvis in the Standing Position. Spine 30(3): 346-353, 2005.
28- Gertzbein SD, Seligman J, Holtby R, et al: Centrode Patterns and Segmental Instability in Degenerative Disc Disease. Spine 10:257-261, 1985.
29- Errico TJ: Lumbar disc arthroplasty. ClinOrthop-Relat Res 435:106-117, 2005.
30- Le Huec JC, Mathews H, Basso Y, et al: Clinical Re-sults of Maverick Lumbar Total Disc Replacement: Two-Year Prospective Follow-up. OrthopClin North Am 36:315-322, 2005.
31- Blumenthal S, McAfee PC, Guyer RD, et al: A Pro-spective, Randomized, Multicenter Food and Drug Administration Investigational Device Exemption Study of Lumbar Total Disc Replacement with the CHARITÉ Artificial Disc Versus Lumbar Fu-sion. Part I: Evaluation of Clinical Outcomes. Spine 30:1565-1575, 2005.
32- McAfee PC, Cunningham B, Holsapple G, Adams K,Blumenthal S, Guyer RD, Dmietriev A, Maxwell JH, Regan JJ,Isaza J: A Prospective, Randomized, Multicenter Food and Drug Administration Inves-tigational Device Exemption Study of Lumbar To-tal Disc Replacement with the CHARITÉ Artificial Disc Versus Lumbar Fusion: Part II: Evaluation of Radiographic Outcomes and Correlation of Surgi-cal Technique Accuracy with Clinical Outcomes. Spine 30(14): 1576-1583.
33- David T: Long-term Results of One-Level Lum-bar Arthroplasty: Minimum 10-Year Follow-up of the CHARITÉ Artificial Disc in 106 Patients. Spine 32(6): 661-666, 2007.
34- Cinotti G, David T, Postacchini F: Results of Disc Prosthesis After a Minimum Follow-Up Period of Two Years. Spine 21:995-1000, 1996.
35- Geisler FH, Blumenthal SL, Guyer RD, et al: Neu-rological complications of lumbar artificial disc re-placement and comparison of clinical results with those related to lumbar arthrodesis in the literature: results of a multicenter, prospective,randomized investigational device exemption study of Charité intervertebral disc. J Neurosurg (Spine 2): 1:143-154, 2004.
36- Putzier M, Funk JF, Schneider SV, Gross C, Tohtz SW, Khodadadyan-Klostermann C, Perka C, Kandz-iora F: Charité total disc replacement—clinical and radiographical results after an average follow-up of 17 years. Eur Spine J 15(2): 183-195, 2006.
37- Van Ooij A, Punt IM, Visser VM, van Rhijn LW, Kurtz SM, Antonis J, Schurink GW: Complications and reoperations of the SB Charité lumbar disc prosthesis: Experience in 75 patients. Eur Spine J. 17(1): 36-43. 2008.

Lum
bar D
egen
erat
ive
Dis
c D
isea
se a
nd D
ynam
ic S
tabi
lizat
ion
270Ali Fahir OZER M.D., Murat COSAR M.D.
38- Freeman BJ, Davenport J: Total disc replacement in the lumbar spine: A systematic review of the litera-ture. Eur Spine J Suppl 3:S439-S447, 2006.
39- Mayer HM, Wiechert K, Korge A, Qose I: Minimally invasive total disc replacement: Surgical technique and preliminary clinical results. Eur Spine J Suppl 2:S124-S130, 2002.
40- Bertagloni R, Kumar S: Indication for full pros-thetic arthroplasty: A correlation of clinical outcome against a variety of indications. Eur Spine J (Suppl 2): S131-S136, 2002.
41- Zigler J, Delamarter R, Spivak JM, Linovitz RJ, Dan-ielson GO 3rd, Haider TT, Cammisa F, Zuchermann J, Balderston R, Kitchel S, Foley K, Watkins R, Brad-ford D, Yue J, Yuan H, Herkowitz H, Geiger D, Bendo J, Peppers T, Sachs B, Girardi F, Kropf M, Goldstein J: Results of the Prospective, Randomized, Multicenter Food and Drug Administration Investi-gational Device Exemption Study of the ProDisc-L Total Disc Replacement Versus Circumferential Fu-sion for the Treatment of 1-Level Degenerative Disc Disease. Spine 32(11): 1155-1162, 2007.
42- Le Huec JC, Mathews H, Basso Y, Aunoble S, Hoste D, Bley B, Friesem T: Clinical Results of Maverick Lumbar Total Disc Replacement: Two-Year Pro-spective Follow-up. OrthopClin North Am 36(3): 315-322, 2005.
43- Le Huec JC, Basso Y, Aunoble S, Friesem T, Bruno MB: Influence of Facet and Posterior Muscle De-generation on Clinical Results of Lumbar Total Disc Replacement: Two-Year Follow-Up. J Spinal Disord Tech 18(3): 219-223, 2005.
44- Canbulat N, Berker N, Cerezci O, Oktenoglu T, Sasani M, Berker E, Ozer AF: Lumbar disc pros-
theses: Is there a rehabilitation protocol? 6th Med-iterranean Congress of PRM, 18-21 October 2006, Portugal.
45- Sasani M, Ozer AF, Oktenoglu T, Canbulat N, Boz-kus, Carilli S, Sarioglu AC: Total disc replacement in the treatment of lumbar discogenic pain with disc herniation: A prospective clinical study. Turk-ish Neurosurgery J (19) 2:127-134, 2009.
46- German JW, Foley KT: Disc Arthroplasty in the Management of the Painful Lumbar Motion Seg-ment. Spine 30(Suppl 16): S60-S67, 2005.
47- Shim CS, Lee S, Maeng DH, Lee SH: Vertical Split Fracture of the Vertebral Body Following Total Disc Replacement Using ProDisc: Report of Two Cases. J Spinal Disord Tech 18(5): 465-469, 2005.
48- Murtagh RD, Quencer RM, Cohen DS, et al: Nor-mal and Abnormal Imaging Findings in Lumbar Total Disk Replacement: Devices and Complica-tions. Radiographics 29:105-118, 2009.
49- Mathew P, Blackman M, Redla S, Hussein AA: Bi-lateral Pedicle Fractures Following Anterior Dislo-cation of the Polyethylene Inlay of a ProDisc Artifi-cial Disc Replacement: A Case Report of an Unusual Complication. Spine 30(11): E311-E314, 2005.
50- Huang RC, et al: The Prevalence of Contraindications to Total Disc Replacement in a Cohort of Lumbar Surgical Patients. Spine 29:2538-2541, 2004.
51- Santos EG, et al: Disc Arthroplasty: Lessons Learned from Total Joint Arthroplasty. Spine 4:S182-S189, 2004.
52- Daly KJ, Ross ER, Norris H, McCollum CN: Vascu-lar complications of prosthetic intervertebral discs. Eur Spine J 15 Suppl 5:644-649, 2006.