alcohol and its medical complications
TRANSCRIPT
ALCOHOL AND ITS MEDICAL
COMPLICATIONSATWIINE CISSY TIBAYUNGWA
BYONANUWE SIMON
PRESENTATION OUTLINE
• Introduction• Definitions• Aspects of alcohol metabolism• Acute and chronic complications of alcohol
INTRODUCTION• Alcohol: An organic compound derived from hydrocarbons and
contains one or more hydroxyl groups (-OH)• Ethanol (C2H5OH: Is the main psychoactive ingredient in alcoholic
beverages. It is a result of the fermentation of yeast.• Consumed all over the world in large quantities• Global consumption~6.2L/capita/yr, WHO 2011.• ~1.8m deaths/yr(3.2% of all deaths)
Cont…Uganda• Commonest substance of abuse• world's leading consumer(WHO 2004, 2005)• Per capita consumption 19.5L(2004), 23.7L(2014) annually• 89% unregulated, home brewed and illegally sold.
DEFINITIONS
• Abstainers-individuals who consume no alcohol. • Moderate drinking-average number of drinks consumed daily that
places an adult at low risk for alcohol problems.• At-risk drinking-level of alcohol consumption that imparts health risksMen: ≥15/week or ≥5 drinks/day Women: ≥8/week or ≥4 drinks/day

Cont…• Binge drinking or heavy drinking-episodic consumption of large
amounts of alcohol, usually ≥5drinks/occasion(men), ≥4drinks(F).• Problem drinking- level of alcohol consumption that causes any
problems for the patient (medical, psychiatric, behavioral, or social—alcohol problems).
ALCOHOL ABUSE • Maladaptive pattern of alcohol use leading to clinically significant
impairment or distress, manifested within a 12-month period by ≥1 of the following:
Failure to fulfill role obligations at work, school, or home Recurrent use in hazardous situations Legal problems related to alcohol Continued use despite alcohol-related social or interpersonal
problems Symptoms have never met criteria for alcohol dependence
ALCOHOL DEPENDENCE • Maladaptive pattern of alcohol use leading to clinically significant
impairment or distress, manifested within a 12-month period by ≥3of the following:
Tolerance Withdrawal (withdrawal symptoms or use to relieve or avoid symptoms) Use of larger amounts for a longer period than intended Persistent desire or unsuccessful attempts to cut down or control use Great deal of time spent obtaining, using, or recovering from use Important social relationships, occupations, or recreational activities given
up or reduced Use despite knowledge of alcohol-related physical or psychological problems
Cont…• Alcoholism- repetitive intake of alcoholic beverages to an extent that
the drinker is harmed. Harm may be mental, physical, social, economic, political.Person has lost control over his/her drinking and life.
PK• Contains ethanol, a small water soluble molecule.• Absorbed unaltered in stomach and small intestines(20%, 80% resp)• Readily crosses all biological membranes• Distributed to all tissues and fluids.• >90% metabolized in the liver• Remainder-urine, lungs, sweat.• Amount exhaled is proportional to blood level, forms basis of the
breath test used by law enforcement agencies
METABOLISM• 3 enzyme systemsADH------Cytosol MEOS------SER, and Catalase( abt 5%)…...Peroxisomes
ADH• Is the primary pathway• Cytosol of hepatocytes• But also in brain and stomach.• Uses NAD+ as cofactor• H+ transferred from etOH to NAD+ to form NADH.
MEOS• A.k.a mixed function oxidase system• Uses NADPH• Consists primarily CYP-2E1, 1A2, 3A4.• Little contribn at low etOH conc(100mg/dl or 22mmol/l)• Wn large amts consumed, ADH saturated owing to depletion of NAD+
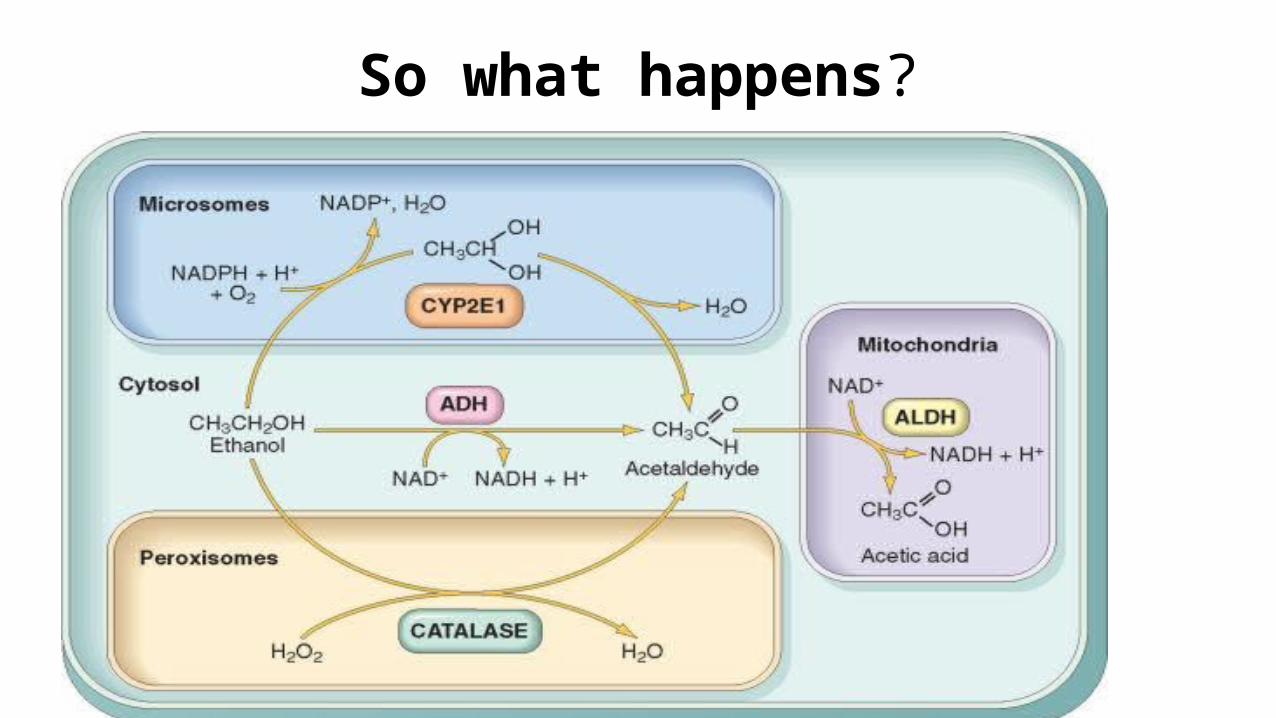
So what happens?
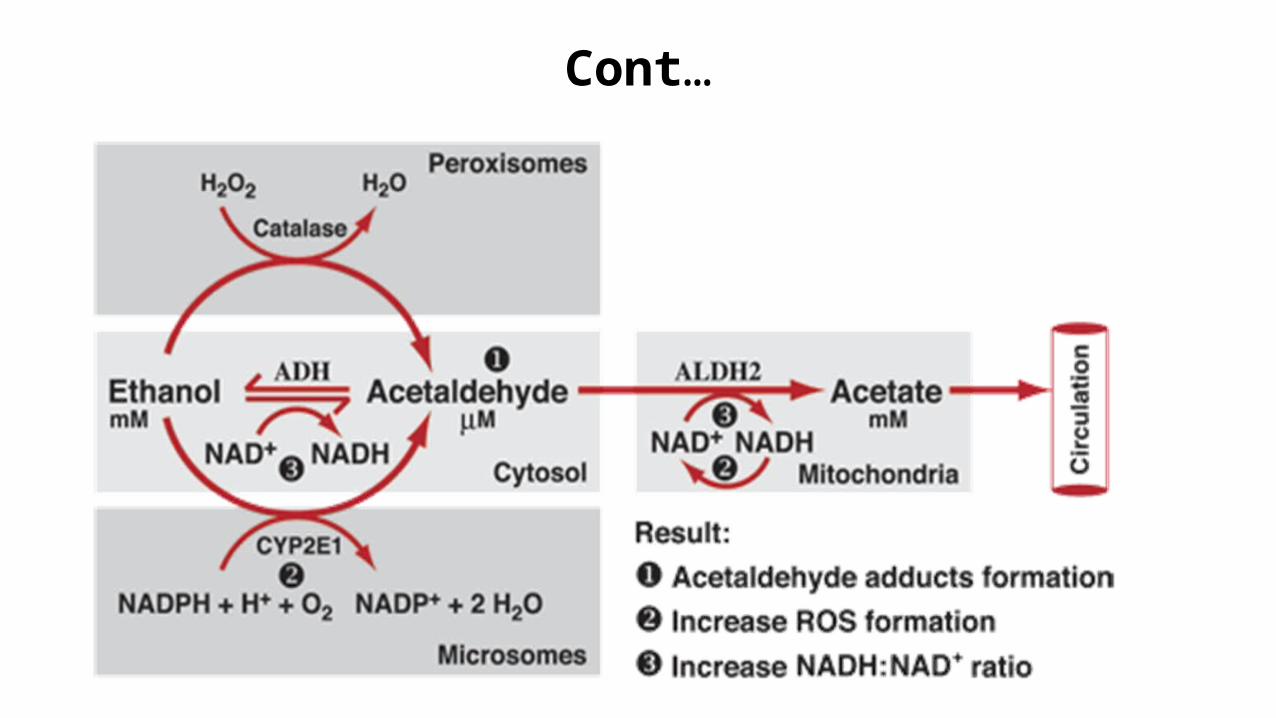
Cont…
Variations
• Food—Delayed absorption, slows gatric emptg.• Sex-F high etOH levels>>M• Genetic variation in ALDH----Inactive in 50% Asians.
MEDICAL COMPLICATIONS
• Can be acute or chronic• Acute ---most commonly: alcohol intoxication and alcohol withdrawal. • Chronic almost every organ system.
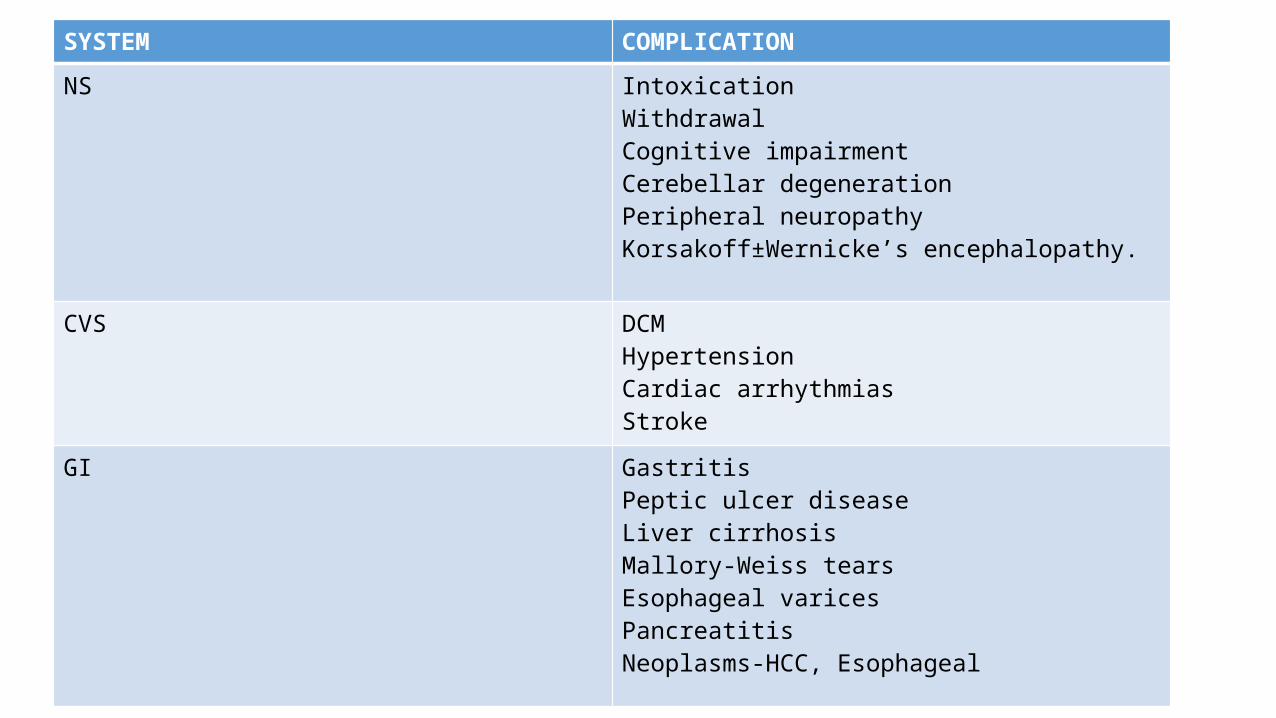
SYSTEM COMPLICATION
NS IntoxicationWithdrawalCognitive impairmentCerebellar degenerationPeripheral neuropathyKorsakoff±Wernicke’s encephalopathy.
CVS DCMHypertensionCardiac arrhythmiasStroke
GI GastritisPeptic ulcer diseaseLiver cirrhosisMallory-Weiss tearsEsophageal varicesPancreatitisNeoplasms-HCC, Esophageal
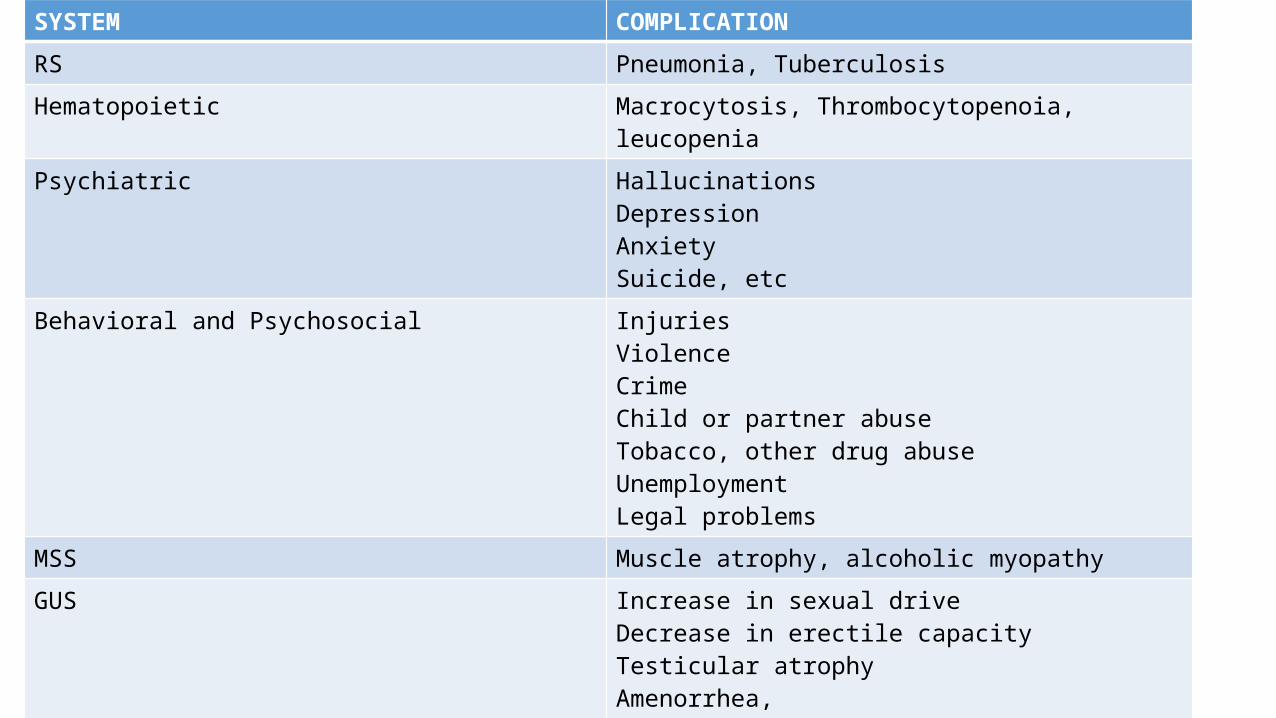
SYSTEM COMPLICATIONRS Pneumonia, TuberculosisHematopoietic Macrocytosis, Thrombocytopenoia, leucopeniaPsychiatric Hallucinations
DepressionAnxietySuicide, etc
Behavioral and Psychosocial InjuriesViolenceCrimeChild or partner abuseTobacco, other drug abuseUnemploymentLegal problems
MSS Muscle atrophy, alcoholic myopathy
GUS Increase in sexual driveDecrease in erectile capacityTesticular atrophyAmenorrhea,InfertilityFAS
• Characterized by substantial neurological impairmentsevere mental impairment ataxia. slurred speech and lack of coordination. coma, and death can occur at levels>60 mmol/L (non-tolerant
drinkers) and 90-120 mmol/L (tolerant drinkers) death may occur due to respiratory depression and hypotension.
ALCOHOL INTOXICATION
Mgt• A-reduced LOC -reduced clearance of pulmonary secretions -vomiting $ aspiration• B-depression of resp centre• C-dehydration/low BP/shock -myocardial depression -arrythmias
Cont…• Thiamine• Dextrose• Manage hypothermia• Gastric lavage
ALCOHOL WITHDRAWAL SYNDROME
• occurs within 12-48 h after prolonged heavy drinking• 4 stages described, however not all may be experienced1 (onset 12-18 h after last drink): “the shakes” tremor, sweating,
agitation, anorexia, cramps, diarrhea, sleep disturbance2 (onset 7-38 h): alcohol withdrawal seizures, usually GTC, brief3 (onset 48 h): visual, auditory, olfactory or tactile hallucinations4 (onset 3-5 d): delirium tremens, confusion, delusions,
hallucinations, agitation, tremors, autonomic hyperactivity (fever, tachycardia, hypertension)
Mgt
• monitor using the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-A) scoring system. • areas of assessment includenausea and vomiting, tactile disturbances, Tremor, auditory disturbancesAgitation, paroxysmal sweats, visual disturbances,
Cont…
Anxietyhaeadache, fullness in head, orientation and clouding of sensorium.• all categories are scored from 0-7 (except: orientation/sensorium 0-4),
maximum score of 67• mild <10• moderate 10-20• severe >20
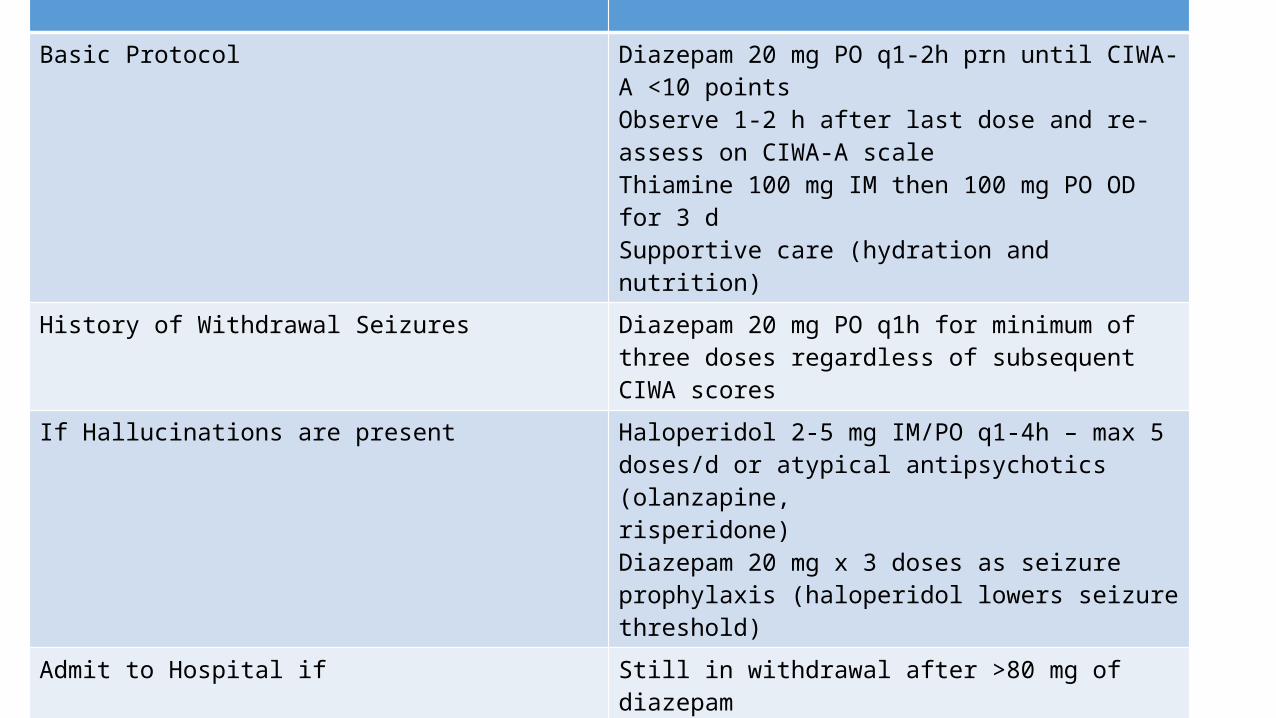
Cont…Basic Protocol Diazepam 20 mg PO q1-2h prn until CIWA-A <10 points
Observe 1-2 h after last dose and re-assess on CIWA-A scaleThiamine 100 mg IM then 100 mg PO OD for 3 dSupportive care (hydration and nutrition)
History of Withdrawal Seizures Diazepam 20 mg PO q1h for minimum of three doses regardless of subsequent CIWA scores
If Hallucinations are present Haloperidol 2-5 mg IM/PO q1-4h – max 5 doses/d or atypical antipsychotics (olanzapine,risperidone)Diazepam 20 mg x 3 doses as seizure prophylaxis (haloperidol lowers seizure threshold)
Admit to Hospital if Still in withdrawal after >80 mg of diazepamDelirium tremens, recurrent arrhythmias, or multiple seizuresMedically ill or unsafe to discharge home
DELIRIUM TREMENS• The most severe manifestation of alcohol withdrawal syndrome. • Charecterised by disorientation, confusion, hallucination, diaphoresis, fever, and tachycardia. • Begins after 2-4 days of abstinence• most severe form can result in death.
Mgt
• Diazepam 5-10mg per 5-15mins till patient is calm, then 1-4hrs PRN
WERNICKE-KORSAKOFF SYNDROME:Wernicke’s encephalopathy
• due to thiamine deficiency• Necrotic lesions: mammillary bodies, thalamus, brainstem• Wernicke’s encephalopathy (acute and reversible)• Triad of Othalmoplegia, ataxia and confusion
Mx
• Urgent Thiamine • Iv 2-3 pairs of high potency ampoules 8hx7/7,• Then oral.

Korsakoff’s syndrome • Chronic and only 20% reversible with treatment• Pt xtically fully conscious• BUT has profound impairement of memory recall(anterograde) and
new learning ability.• Striking feature is a tendency to confabulate• Confab probably results from inability to distinguish the temporal
sequence of past events
Mx• Thiamine 100 mg PO bid/tid x 3-12 mo
……been a long journey, …SDL on e rest!SucceSS.