alarm management: understanding and addressing the...
TRANSCRIPT
Samantha Jacques, PhD, FACHEDirector, Biomedical EngineeringTexas Children’s Hospital
Alarm Management: Understanding and Addressing the Ecosystem
Page 2
xxx00.#####.ppt 7/29/2015 2:51:41 PMPage 2
Texas Children’s Hospital• Hospital System
• Tertiary Care Hospital• Community Hospital• 4 Health Centers• 5 MFM/OBGyn clinics• 50+ primary care pediatric practices
• 650 Licensed Beds• 173 NICU beds• 118 ICU (including CVICU)• 289 Acute Care/IMU/Rehab• 70 L&D/MBU
• FY 2014 Stats• 117,275 EC Visits• 32,446 Admissions• 189,057 Patient Days• 27,945 Surgeries

Page 3
xxx00.#####.ppt 7/29/2015 2:51:41 PMPage 3

Hurdles in the Long Distance Race
4
Data is not easy to come by
Little Literature or Evidence Based Guidelines on Alarms
One Size Solutions do NOT fit all situations/ units/ institutions
Culture isn’t easy to change
Page 5
xxx00.#####.ppt 7/29/2015 2:51:42 PMPage 5
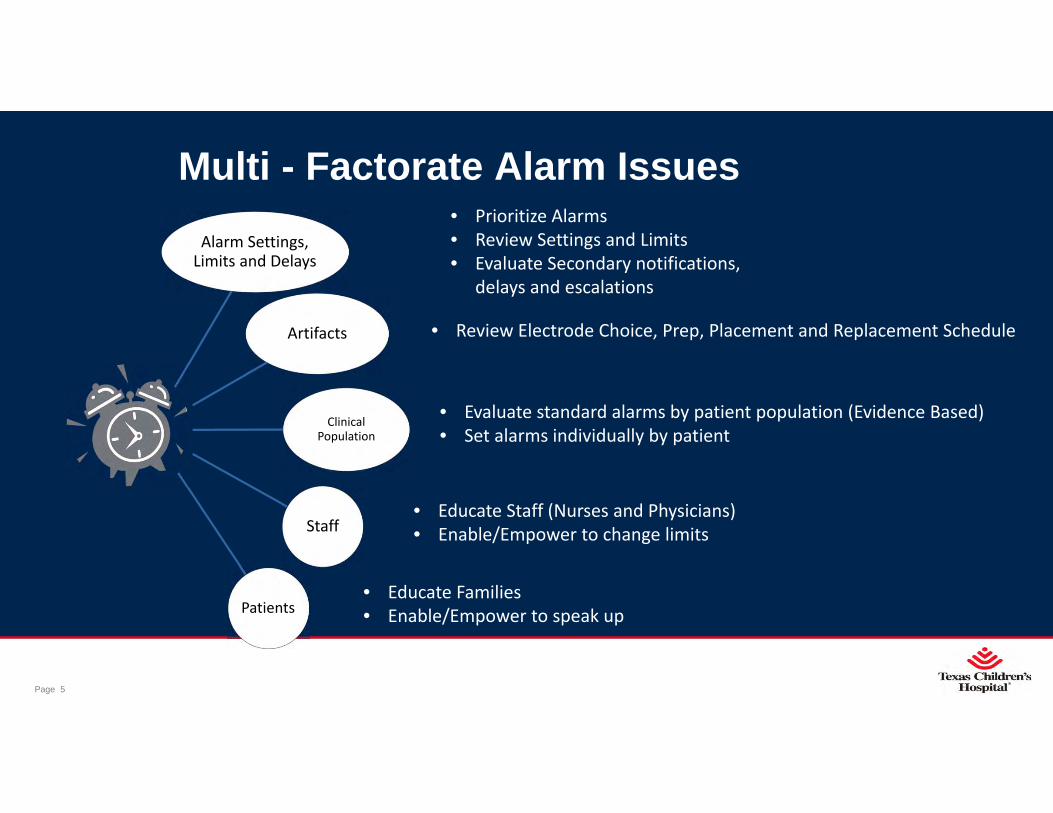
Multi - Factorate Alarm IssuesAlarm Settings, Limits and Delays
Artifacts
Clinical Population
Staff
Patients
• Prioritize Alarms• Review Settings and Limits• Evaluate Secondary notifications,
delays and escalations
• Review Electrode Choice, Prep, Placement and Replacement Schedule
• Evaluate standard alarms by patient population (Evidence Based)• Set alarms individually by patient
• Educate Staff (Nurses and Physicians)• Enable/Empower to change limits
• Educate Families• Enable/Empower to speak up

Page 6
xxx00.#####.ppt 7/29/2015 2:51:42 PMPage 6
TCH Alarm Management Journey
• High• Medium • Low
Priorities
• Limits by Age and Unit
Thresholds• Delays• Escalations
Secondary Notifications
Reduced Quantity of Alarms by 66%

Page 7
xxx00.#####.ppt 7/29/2015 2:51:42 PMPage 7
Meet Nurse Nancy• Nancy is a Progressive Care (Step down unit) nurse with
15 years experience‐ She is assigned three patients for her 12 hour shift by the unit
charge nurse
• 8yo Cystic Fibrosis patient post lung transplant
• 2 year old on renal patient post pheresis
• 11 month old post heart surgery
‐ Monitors are set with following alarm parameters:
SPO2 HR RR
8 year old 93 – 100% 55 – 85 bpm 12 – 18 brpm
2 year old 93 – 100% 70 – 110 bpm 20 – 30 brpm
11 month old 93 – 100% 80 – 120 bpm 25 – 40 brpm

Page 8
xxx00.#####.ppt 7/29/2015 2:51:42 PMPage 8
• In ONE shift Her patients have a total of 336 alarms –• On average she spends 14% of her shift in ALARM FLOOD – (more than 10 alarms in 10 min)• This day she experienced 7 Floods – 2:25 hours of her shift
• Nancy cannot prioritize how to deliver care during a flood – high risk environment• Secondary notification – Greater than 50% of her messages are “warning” or “crisis”• She only has 70 min of alarm “silence”

Page 9
xxx00.#####.ppt 7/29/2015 2:51:42 PMPage 9
Lessons Learned
•Alarms Happen for unusual reasons – need to understand environmental factors
•Limits set by Age and Unit should be data driven – physiological “normal” based on literature may not be appropriate for the UNIT population – e.g. Respiratory Floor/ Cardiovascular Floor
•Limits by Age and Unit allow better baseline for UNIT, but don’t necessarily match INDIVIDUAL PATIENT NEED

Page 10
xxx00.#####.ppt 7/29/2015 2:51:43 PMPage 10
A New Way
•Real Time Analytics Dashboard Approach‐Unit‐Nurse‐Patient
•Uses‐Historical Information‐Track changes from PDSA cycles‐Nurse Assignments‐Leverage real time data to make clinical decisions on alarm settings on an INDIVUIDUAL PATIENT

Page 11
xxx00.#####.ppt 7/29/2015 2:51:43 PMPage 11
Unit Dashboard

Page 12
xxx00.#####.ppt 7/29/2015 2:51:43 PMPage 12
Unit Dashboard – Deep Dive

Page 13
xxx00.#####.ppt 7/29/2015 2:51:43 PMPage 13
Unit Dashboard – Bed View

Page 14
xxx00.#####.ppt 7/29/2015 2:51:43 PMPage 14
Unit Dashboard - Nurse Assignment

Page 15
xxx00.#####.ppt 7/29/2015 2:51:44 PMPage 15
Patient Specific Dashboard

Page 16
xxx00.#####.ppt 7/29/2015 2:51:44 PMPage 16
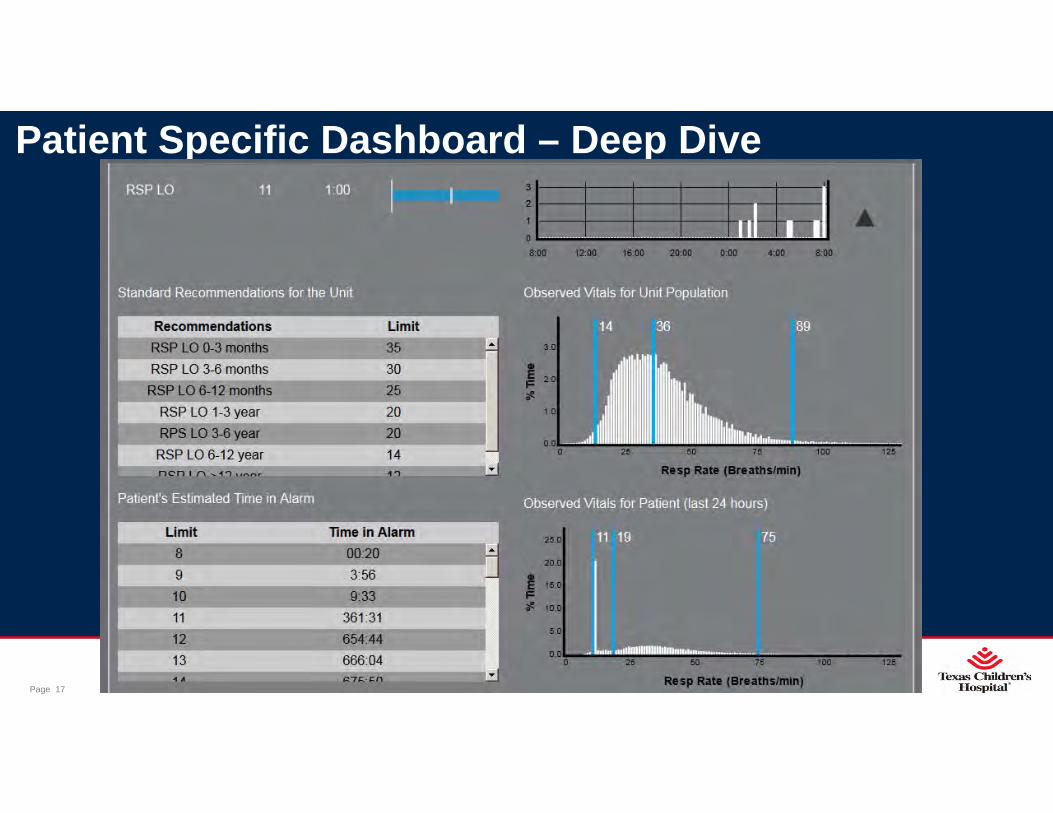
Patient Specific Dashboard – Deep Dive
Page 17
xxx00.#####.ppt 7/29/2015 2:51:44 PMPage 17
Patient Specific Dashboard – Deep Dive

Page 18
xxx00.#####.ppt 7/29/2015 2:51:45 PMPage 18
Workflow Nurse Manager uses report to Set Nurse
Assignments
Nurse Manager then highlights patients for
Rounds Review
During Rounds, Clinical team Reviews High Alarming Patients
Clinical Team makes decision
to keep or change alarm limits (orders updated)
At Shift Change: Nurse Manager
Runs Unit Report
Improves Safety –reducing likelihood of alarm floods
Reduces Alarm VolumeImproves Patient Satisfaction

Live Demo
