aki and ckd: top ten facts for primary care physicians richard smith
TRANSCRIPT

AKI and CKD: Top ten facts for primary care physicians
Richard Smith

KIDNEYS

CKD: Does it really matter?
Richard SmithConsultant Nephrologist

www.renal.org/CKDguide/ckd.html http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4101902


Significant biochemical changes have no ‘immediate’ clinical correlate
CKD(3) and AKI are associated with significant risk
Recognise the patient at risk and manage this
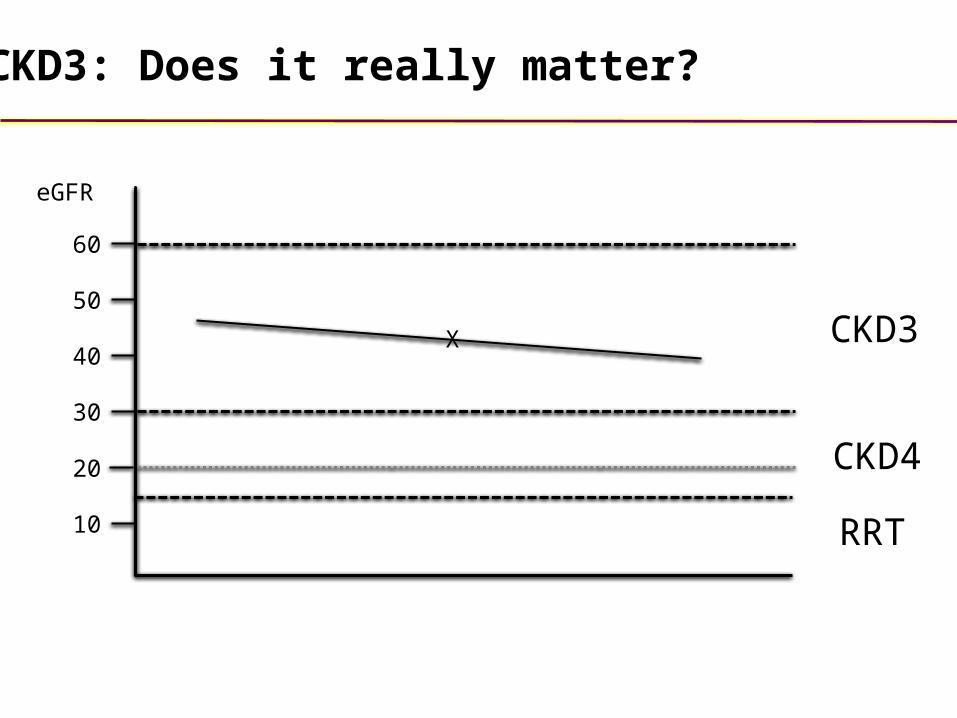
CKD(3):Confers significant cardiovascular risk and risk of AKIProgression to RRT is rare (1.3%)Progression to worse CKD (and therefore worse cardiovascular and AKI risk) is common
The talk in one slide: Risk management

RRT
60
50
40
30
20
10
eGFR
CKD3CKD3
CKD4CKD4
X
CKD: Does it really matter?
RRT
60
50
40
30
20
10
eGFR
CKD3
CKD4
X
CKD3: Does it really matter?

Risks associated with CKD
Cardiovascular Risk

(N=1,120,295)
1.0
1.4
2.0
2.8
3.4
Ha
zard
ra
tio fo
r C
V e
ven
t
0
1
2
3
4
Reduced kidney function is associated with a higher risk of CV events
≥60 45-59 30-44 15-29 <15
eGFR (mL/min/1.73m2)
Go et al. N Engl J Med 2004 351: 1296–1305 Tonelli et al. J Am Soc Nephrol 2006 17: 2034–2047Eeg-Olofsson et al. J Internal Medicine 2010 268: 471–482 Khaw Nature Reviews Endocrinology 2009 5: 130-131
8.0-8.9
9.0-9.9
CKD3

Age-related glomerulosclerosis is amplified by systemic atherosclerosis
Kasiske BL. Kidney Int 1987; 31: 1153-1159

Risk factors for cardiovascular disease
Risk factors for chronic kidney disease
Hypertension
Smoking
Obesity
Diabetes
Dyslipidaemia
Reduced GFR
Proteinuria
Hypertension
Smoking
Obesity
Diabetes
Dyslipidaemia
Atherosclerosis
Heart failure

SHARP: Major Atherosclerotic Events5-year benefit per 1000 patients
http://www.ctsu.ox.ac.uk/~sharp/

Hemmelgarn BR. Kidney International 2006: 29: 2155
10,184 community-dwelling subjects aged 66 or over
Decline in eGFR greatest in diabetic patients (2.1 and 2.7 ml/min/1.73m2/year in F and M respectively)
Decline in eGFR in non-diabetic patients: 0.8 and 1.4 ml/min/1.73m2/year in F and M respectively
Decline more likely if baseline eGFR <30
Risk of decline of GFR in elderly people

CKD progression
Steps to identify progressive CKD
Obtain a minimum of three eGFR over not less than 90 days
In new cases of reduced eGFR repeat within 2 weeks
to exclude acute deterioration
Slow progression by treating BP
In CKD >140/90 mmHg
In CKD and diabetes or ACR 70mg/mmol > 130/80 mmHg
Risks associated with CKD
Acute Kidney Injury


NICE Guidance 28th August 2013
The National Confidential Enquiry into Patient Outcome and Death found that only half of patients with AKI had received 'good' care
Up to 30 per cent of cases of AKI can be prevented - that equates to at least 12,000 unnecessary deaths per year
Inadequate assessment of risk factors in 24% of patients admitted with AKI
Commonest risk factors not assessed were medication, co-morbidity and hypovolaemia

RRT
60
50
40
30
20
10
eGFR
CKD3
CKD4
X
CKD3: Is it really CKD?

Do not ignore eGFR 30-59ml/min until know direction of travel and
significant causes ruled out
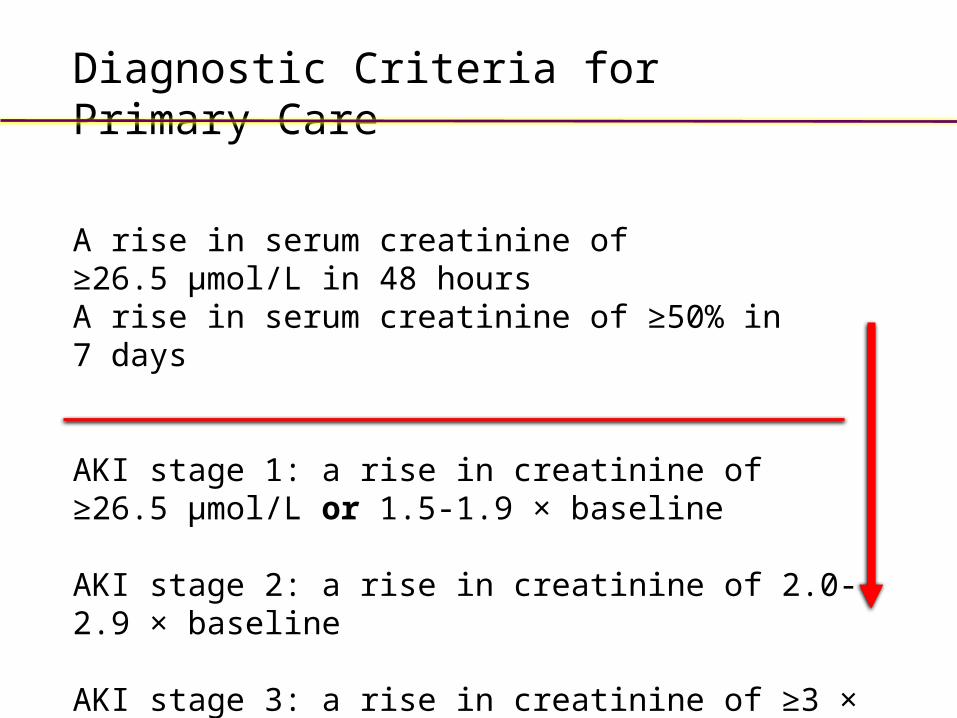
Diagnostic Criteria for Primary Care
A rise in serum creatinine of ≥26.5 μmol/L in 48 hoursA rise in serum creatinine of ≥50% in 7 days
AKI stage 1: a rise in creatinine of ≥26.5 μmol/L or 1.5-1.9 × baseline
AKI stage 2: a rise in creatinine of 2.0-2.9 × baseline
AKI stage 3: a rise in creatinine of ≥3 × baseline or increase in creatinine to ≥353 μmol/L
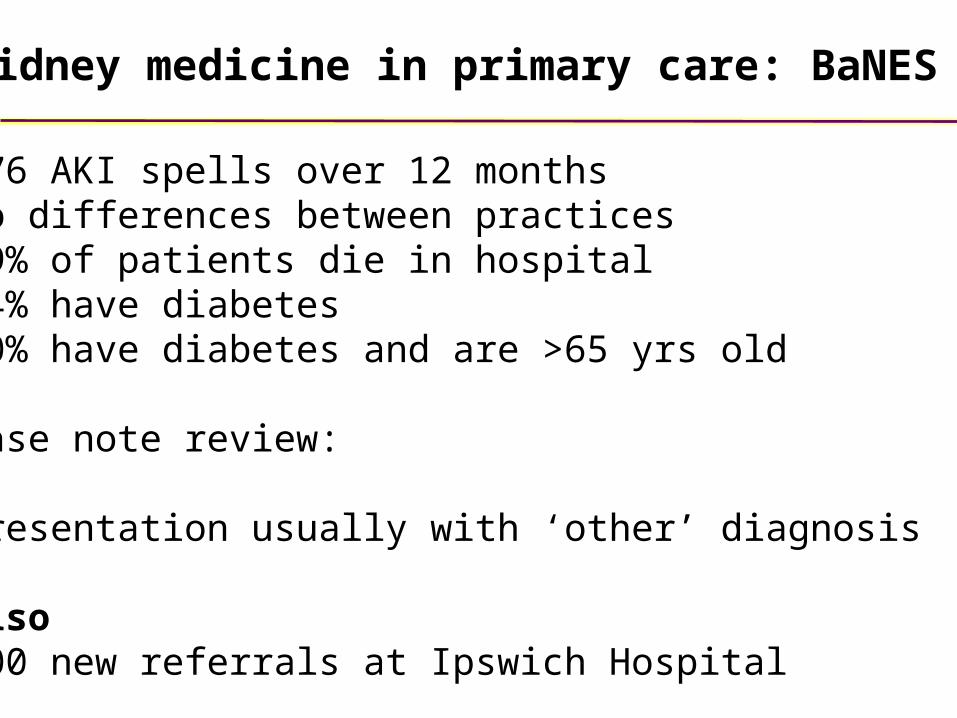
776 AKI spells over 12 monthsNo differences between practices19% of patients die in hospital24% have diabetes20% have diabetes and are >65 yrs old
Case note review:
Presentation usually with ‘other’ diagnosis
Also500 new referrals at Ipswich Hospital
Kidney medicine in primary care: BaNES

48 yr old man. Routine health check. Found to have eGFR of 35ml/minReferred for investigation of his “CKD 3”
No previous eGFRProtein ++++ No haematuriaBP 122/74
Case 1
Renal biopsy demonstrated FSGS

Mrs MA 74 year old eGFR 46ml/min/1.73m2
USS demonstrated ‘normal’ size kidneys
Serum electrophoresis revealed a paraprotein with urinary BJP
Case 2
Dipstick of urine revealed + protein
Fact 1: Haematuria and proteinuria are
flags for further investigation
Fact 2: Combined renal length <20cm
makes CKD likely Still need to exclude A/CKD

Mr PS 80 year old ‘Stable’ IHD Not diabetic No ACEI
Acutely SOB with possible rigor
Few crackles L base
Clarithromycin prescribed
Case 3

24 hours later confused and hypotensive
Emergency admission
Treated as CAP according to hospitalprotocol
Rx Vancomycin 1g x 2Gentamicin 160mg x 2

48 hours later AKI diagnosedBaseline eGFR 42ml/min/1.73m2
4 week hospital admission
Probably avoidable with recognition that patient likely to have CKD and risk conferred by this CKD
Admission eGFR 22ml/min/1.73m2
‘48h’ eGFR 12ml/min/1.73m2

74 year old male with 12 year history of T2DM presents to casualty unwell with lower abdominal pain. Known to have diverticular disease
Most recent HbA1c 7.4%
First thoughts?
Case 4
Rx Ramipril 5mg daily and Metformin 500mg bd

74 year old male with 12 year history of T2DM presents to casualty unwell with lower abdominal pain. Known to have diverticular disease
Rx Ramipril 5mg daily and Metformin 500mg bd
Pyrexial. BP 130/74. Euvolaemic
WCC 10.6x109/l CRP 48ng/ml
eGFR 42ml/min with a potassium of 4.2mmol/l
Case 5

92 year old is seen in clinic having been found by GP to have ‘CKD4’
She is well with an eGFR of 26ml/min
Rest of biochemistry is safe, urine reveals neither blood nor protein
What do I do?
Case 6
USS shows echobright kidneys of 8.2cm and 8.4cm with no evidence of obstruction
eGFR was 28ml/min in 2008

Fact 1: Haematuria and proteinuria are flags for further
investigation
Fact 2: Direction of travel is everything!
Fact 3: Risk factors for AKI include age >65, diabetes, CVD and
ACEI/ ARB
Fact 4: Infection is a trigger for AKI in at risk patients even if not
involvingurinary tract

Case 7
A 36 yr old woman who has been previously fit and well and who rarely attends the surgery presents complaining of increased tiredness. She is an active sportswoman who has noticed reduction in exercise tolerance over 3 weeks such that she has struggled on hills when jogging. For 3 days she has had a sore throat, ‘painful’ fingers and noticed a few ‘red spots’ on her right thigh. On examination you confirm that she has a palpable non-blanching purpuric rash on her thigh. BP is 164/90 but examination is otherwise unremarkable.
What do I do?

Case 7
A 36 yr old woman who has been previously fit and well and who rarely attends the surgery presents complaining of increased tiredness. She is an active sportswoman who has noticed reduction in exercise tolerance over 3 weeks such that she has struggled on hills when jogging. For 3 days she has had a sore throat, ‘painful’ fingers and noticed a few ‘red spots’ on her right thigh. On examination you confirm that she has a palpable non-blanching purpuric rash on her thigh. BP is 164/90 but examination is otherwise unremarkable.
What do I do
Dipstick of urine revealed blood ++ and protein ++

Fact 1: Dipstick of urine is your get out of jail free card.
Particularly if hypertension.

78 year old with stable CKD3. Rx Ramipril 5mg daily
eGFR June 2011 47ml/min April 2014 41ml/min
Cares for terminally ill husband therefore deferred R hip replacement
What pain killers would you recommend?
Case 8
Pharmacist recommended Ibuprofen 400mg daily
4th July 2014 16ml/min
Stopped Brufen
14th July 2014 39ml/min

Fact 5: NSAID/COX inhibitors/COX-2 inhibitorsXFact 6: Consider stopping ACEI/ARB
Even in patient with stable kidney function if ‘at risk’
Fact 7: Restart ACEI/ARB when acute event resolved
Patients who need ACEI/ARB should not be deprived of them because of undue concerns about AKI
Fact 8: Stop metformin if risk of AKI
Fact 9: Metformin can be used in CKD3
Avoid in CKD3b if significant risk of AKI

Recognition and Prevention of AKI
Is this an at risk patient?Age >65 yearsVascular diseaseDMACEI/ARBCKD
Is glomerular perfusion threatened ?Hypotension or sepsisNSAID/COXi/COX-2i
Kidney medicine in primary care: 7 minutes
Fact 10: Slides and more info available at www.clinimeded.co.uk Wales Deanery CPD for
GPs
http://gpcpd.walesdeanery.org/Clinical
Acute Kidney Injury
Quiz: http://www.doctors.net.uk