airway management, ventilation, oxygen...
TRANSCRIPT
OXYGEN THERAPY AND AIRWAY
MANAGEMENT, VENTILATOR
THERAPY
1
Dr.Dhaher JS Al-habbo
FRCP London UK
Assistant Professor in Medicine
DEPARTMENT OF MEDICINE

OXYGEN CONTENT OF BLOOD The theoretical maximum oxygen carrying capacity is
1.39 ml O2/g Hb, but direct measurement gives a
capacity of 1.34 ml O2/g Hb.1.34 is also known as
Hüfner’s constant.
The oxygen content of blood is the volume of oxygen
carried in each 100 ml blood.
It is calculated by: (O2 carried by Hb) + (O2 in
solution) = (1.34 x Hb x SpO2 x 0.01) + (0.023 x
PaO2)
10

OXYGEN DISSOCIATION CURVE (ODC)
3
Myocardial infarction
Acute pulmonary
disorders
Sepsis
Drug overdose
Liver failure
Head trauma
CHF
Hypovolemic shock
Blunt chest trauma
Acute neuromuscular disease
Acute abdomen (splinting)
Acute pancreatitis
Spinal cord injury
CLINICAL CONDITIONS WITH INCREASED
RISK OF HYPOXIA
Tachypnea
Cyanosis
Restlessness
Disorientation
Cardiac arrhythmias
Slow bounding pulse
Tachycardia
Hypertension
Dyspnea
Coma
Labored breathing (use of accessory muscles, nasal flaring)
Lethargy
Tremors/seizure activity
INDICATIONS FOR OXYGEN THERAPY
OXYGEN THERAPY
“Generally speaking”, a patient who is
breathing less than 12 and more than 24
/minute needs oxygen of some kind
6

OXYGEN THERAPY TO ENSURE SAFE AND
EFFECTIVE TREATMENT
Oxygen is required for the functioning and
survival of all body tissues and deprivation for
more than a few minutes is fatal.
In immediately life threatening situations oxygen
should be administered.
Hypoxaemia. Acute hypotension.
Breathing inadequacy. Trauma. Acute illness. CO
poisoning. Severe anaemia. During the peri-
operative period.
7
OXYGEN THERAPY TO ENSURE SAFE AND
EFFECTIVE TREATMENT
Oxygen is a prescription drug.
Prescriptions should include – Flow rate.
Delivery system.
Duration.
Instructions for monitoring.
Monitoring resps oxygen sats not definitive tool
need to be looking at other things acccessory
muscles etc
8

OXYGEN THERAPY
Oxygen therapy Humidification Is recommended
if more than 4 litres/min is delivered.
Helps prevent drying of mucous membranes.
Helps prevent the formation of tenacious
sputum.
Oxygen concentrations will be affected with all
delivery systems if not fitted correctly or tubing
becomes kinked and ports obstructed.
9

METHODS OF OXYGEN DELIVERY
Most common methods of oxygen delivery
include
Nasal Cannula
Venturi Mask
100% Non-Rebreather Mask
Mechanical Ventilation
HYPERBARIC OXYGEN THERAPY
(HBOT)

Nasal Cannula
Comfortable, convenient, mouth breathing will not effect % of O2 delivered
Liters/min = %
2 l/m = 24-28%
3 l/m = 28-30%
4 l/m = 32-36%
5 l/m = 36-40%
6 l/m = 40-44%
Cannot administer > 6 liters/minute (44%)
OXYGEN DELIVERY METHODS

NASAL CANNULA
Provides limited oxygen concentration
Used when patients cannot tolerate mask
Prongs and other uses
Concentration of 24 to 44%
Flow rate set between 1 to 6 liters
For every liter per minute of flow delivered, the
oxygen concentration the patient inhales increases
by 4%
12

OXYGEN THERAPY Simple facemask Easy to use.
Allows administration of variable concentration dependant on
flow of fresh gas up to 40%.
Nasal cannulae Easy to use. Well tolerated. Comfortable for long
periods. Patient can eat and talk easily.
Possible to deliver oxygen concentrations of 24-40% at flow rates
of 1-6 litres/min.
Flow rates in excess of 4 litres/min might cause discomfort
and drying of mucous membranes and are best avoided.
Flow Rate: 10 L/Min
O2 Conc.: 40 – 60 %
Use: moderate FiO2, mouth breathers
13
VENTURI MASK
Mostly used in the
hospital setting for
COPD patients
Concerns
Tight seal is a must
Interferes with
eating/drinking
Condensation
collection
14
FiO2 Delivery
Blue 24% Yellow 28%
White 31% Green
35%
Pink 40%
Provides precise
concentrations of oxygen
Entrainment valve to adjust
oxygen delivery
VENTURI MASK
15
Red 40% 10/L/M Blue 24% 2/L/M Yellow 35% 8/L/M
White28% 4/L/M Green 60% 15/L/M
Orange 31% 6/L/M
Delivery percentages
6 l/min = 55 – 60 %
8 l/min = 60 – 80 %
10 l/min = 80 – 90 %
>12 l/min = 90 + %
Benefit:
Has a one way expiratory
valve that prevents re-
breathing expired gases
Concern
May lead to O2 toxicity
OXYGEN DELIVERY METHODS
100% NON-REBREATHER

17
100% NON-REBREATHER MASK partial rebreather Mask

OXYGEN THERAPY
Non-rebreathing mask Allows the delivery of high
concentrations of oxygen (85% at 15
litres/min).
Has a reservoir bag to entrain oxygen. One way
valves prevent room and expired air from
diluting the oxygen concentration. A tight seal
is essential.
Reservoir bag must be seen to expand freely.
18
OXYGEN DELIVERY METHODS
MECHANICAL VENTILATION
Allows administration of 100% oxygen
Controls breathing pattern for patients who are unable to maintain adequate ventilation
Is a temporary support that “buys time” for correcting the primary pathologic process

INDICATIONS FOR MECHANICAL
VENTILATION Mechanical Failure
Ventilatory Failure
Oxygenation Failure
General Anesthesia
Post-Cardiac Arrest
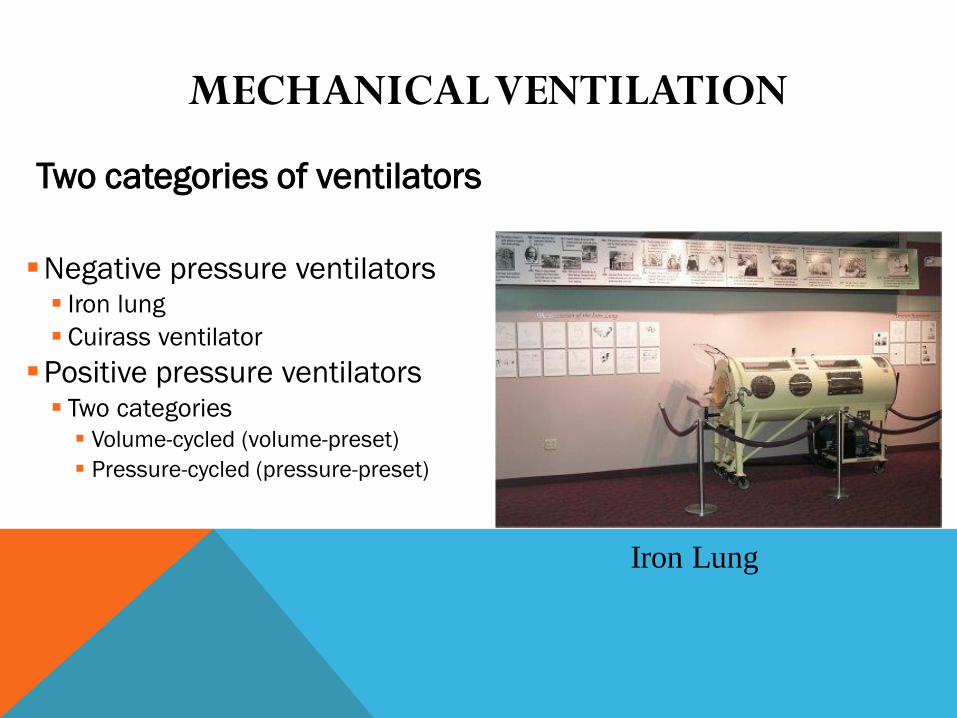
MECHANICAL VENTILATION
Two categories of ventilators
Negative pressure ventilators Iron lung
Cuirass ventilator
Positive pressure ventilators Two categories
Volume-cycled (volume-preset)
Pressure-cycled (pressure-preset)
Iron Lung

MECHANICAL VENTILATION PEEP
Description Maintains a preset positive airway pressure at the end of expiration
Increases PaO2 so that FiO2 can be decreased
Increases DO2 (amt of delivered O2 to tissue)
Maximizes pulmonary compliance
Minimized pulmonary shunting
Indications PaO2 < 60 on FiO2 > 60% by recruiting dysfunctional alveoli
Increases intrapulmonary pressure after cardiac surgery to decrease intrathoracic bleeding (research does not support this idea)

MECHANICAL VENTILATION PEEP
Advantages Improves PaO2 and SaO2 while allowing FiO2 to be
decreased Decreases the work of breathing Keeps airways from closing at end expiration (esp. in pts
with surfactant deficiency)
Disadvantages Increased functional residual capacity (increases risk for
barotrauma) Can cause increased dead space and increased ICP In pts with increased ICP, must assure CO2 elimination Contraindicated: hypovolemia, drug induced low cardiac
output, unilateral lung disease, COPD

24
MECHANICAL VENTILATION CPAP
Description
Constant positive pressure is applied throughout
the respiratory cycle to keep alveoli open
Indications
To wean without having to remove the ventilator
and having to connect to additional equipment

26
MECHANICAL VENTILATION CPAP
Advantages
Takes advantage of the ventilator alarm systems
providing psychological security of the ventilator being
there
Disadvantages
Patient may sense resistance as he breathes through the
ventilator tubing

Respiratory arrest from disconnection
Respiratory infection (VAP)
Acid-base imbalances
Oxygen toxicity
Pneumothorax
GI bleeding
Barotrauma
Decreased cardiac output
MECHANICAL VENTILATION
COMPLICATIONS

VENTILATOR WEANING
Vital Capacity at least 10 – 15 ml/kg
Tidal Volume > 5 ml/kg
Resting minute volume > 10 L per minute
ABG’s adequate on < 40% FiO2
Stable vital signs
Intact airway protective reflexes (strong cough)
Absence of dyspnea, neuromuscular fatigue, pain, diaphoresis, restlessness, use of accessory muscles

HYPERBARIC OXYGEN THERAPY
(HBOT)
30

HYPERBARIC OXYGEN THERAPY
(HBOT) Hyperbaric Oxygen Therapy
Uses a special chamber, sometimes called a pressure chamber, to allow a person to get high levels of oxygen in the blood.
This means that the air inside the pressurized chamber is typically 2 1/2 times greater than normal atmospheric pressure.
This leads to make the blood carrying larger amounts of oxygen, and bringing this oxygen to organs and tissues in the body.
By doing so, wounds, particularly infected wounds, can heal more readily.

HBOT— WHAT IS IT USED FOR?
Decompression sickness
Arterial gas embolism
Carbon monoxide
poisoning
Osteomyelitis
Skin grafts
Burns
Necrotizing fascitis
Anemia
Gas gangrene
Chronic non-healing wounds
Sports injuries
and more…

Analysis Arterial Blood Gas results:
If you can remember the following pyramid points and
steps, you will be able to analyze any blood gas report.
Pyramid points: In acidosis, the PH is down.
In alkalosis, the PH is high.
The respiratory function indicator is the PCO2.
The metabolic function indicator is the HCO3.
Normal blood gas value: PH: 7.35-7.45
PCO2: 35-45 mmHg
HCO3: 22-27meq/liter
PO2 : 80-100
Analysis Arterial Blood Gas results

Pyramid steps:
Pyramid step 1:- look at the blood gas report. Look at the PH, is it up or
down; if it is up; it reflects alkalosis. If it is down; it reflects
acidosis.
Pyramid step 2:- look at the PCO2, is it up or down; if it reflects an
opposite response to the PH, then you know that the
condition is a respiratory imbalance.
Analysis Arterial Blood Gas results

If it does not reflect an opposite response to the PH; then move on
to pyramid step 3.
Pyramid step 3:- look at the HCO3. Does the HCO3 reflect a corresponding
response with the PH; if it does, then the condition is a metabolic
imbalance.
Pyramid step 4:-
Remember, compensation has occurred if the PH is in a normal
range of 7.35-7.45. If the PH is not within normal range, look at
the respiratory or metabolic function indicators.
Analysis Arterial Blood Gas results

Respiratory Imbalances :
if the condition is a respiratory imbalance look at the HCO3
to determine the state of compensation.
if the HCO3 is normal, then the condition is uncompensated.
if the HCO3 is abnormal, then the condition is partial
compensation.
Analysis Arterial Blood Gas results

Metabolic Imbalance :
If the condition is metabolic imbalance, look at the PCO2
to determine the state of compensation.
If the PCO2 is normal, then the condition is
uncompensated.
If the PCO2 is abnormal, then the is partial compensation.
Analysis Arterial Blood Gas results