airway management the medic one way… by zachary wm. drathman
TRANSCRIPT
Airway Airway ManagementManagement
The Medic One Way…By Zachary Wm. Drathman
Our Role in Airway Management
Resuscitation:CPR, Intubation, epinephrine, shocks
Trauma: Airway, breathing, circulation
Medical:Airway, breathing, circulation, dysfunction

Room air: HyperventilationCannula: Basic exam, CP, Asthma, Minor Trauma, COPDNRB: CHF, Inhalation, Trauma, OB,
Pneumonia, Anaphylaxis, Severe COPD
BVM: CPR, Intoxicants, Seizure, Diabetic, CHF, Occlusion, Prep for ETT OPA: Just makes “Bagging” easier
Basic Airway Control
Equipment
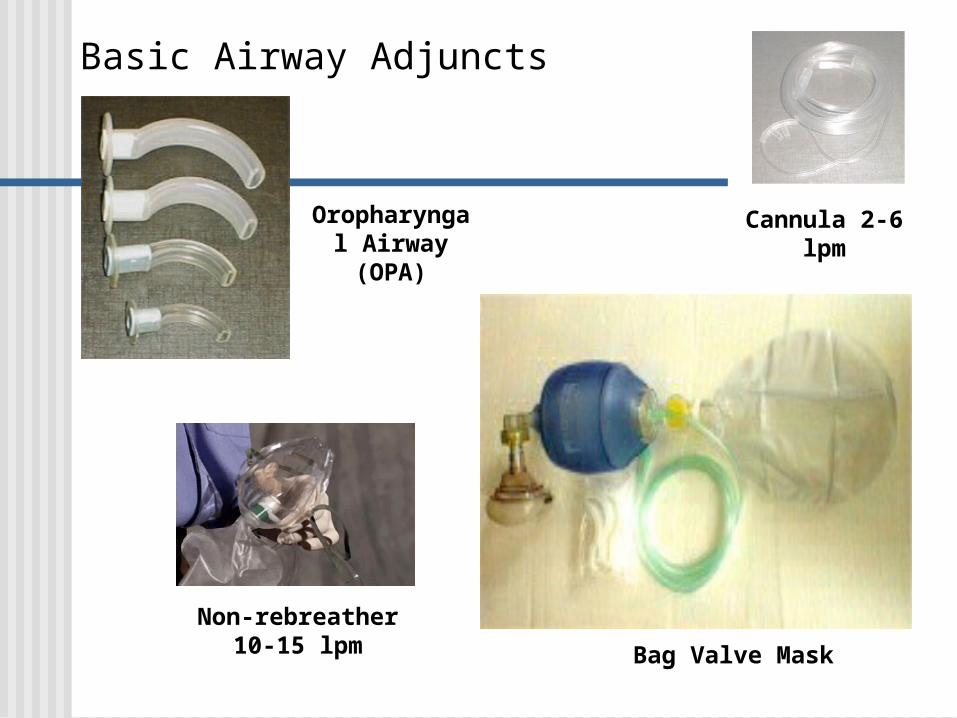
Basic Airway Adjuncts
Cannula 2-6 lpm
Non-rebreather10-15 lpm Bag Valve Mask
Oropharyngal Airway
(OPA)
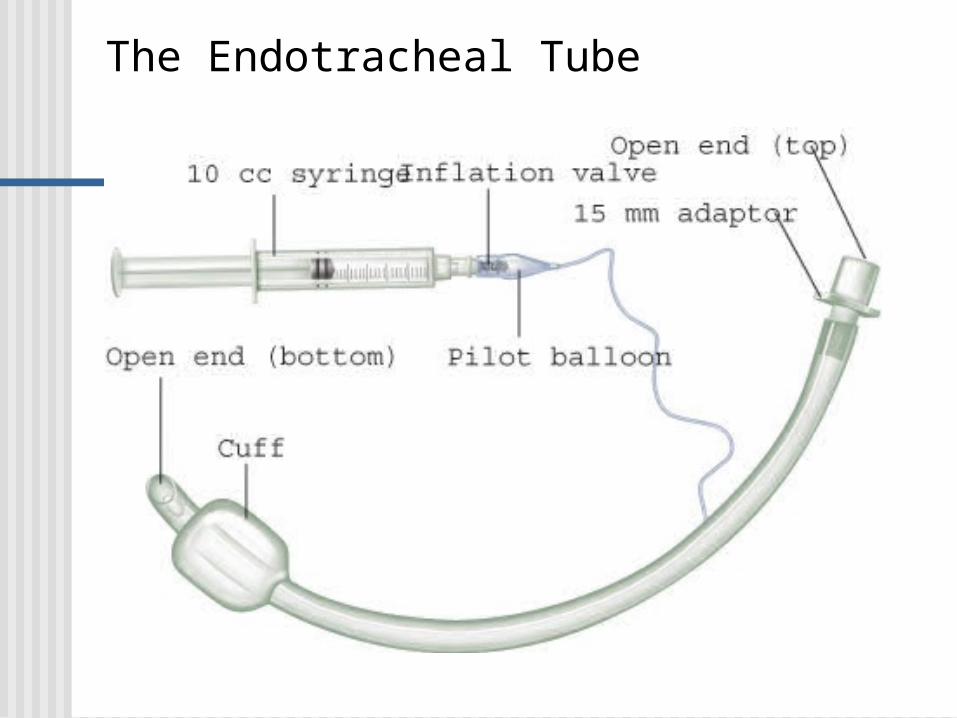
The Endotracheal Tube

More Tubes
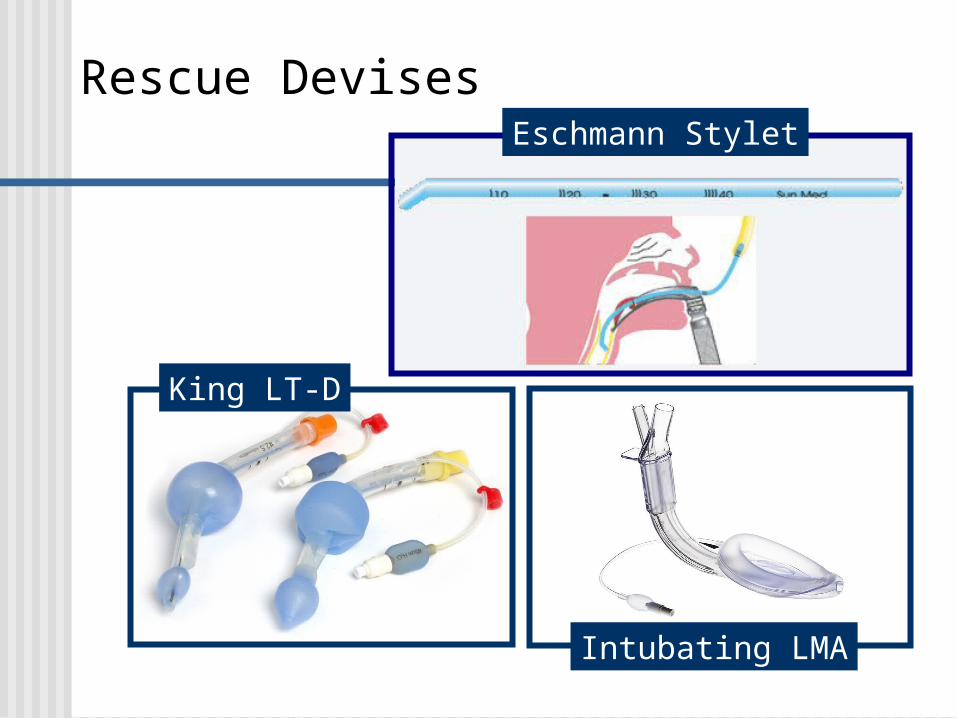
Rescue Devises
King LT-D
Intubating LMA
Eschmann Stylet
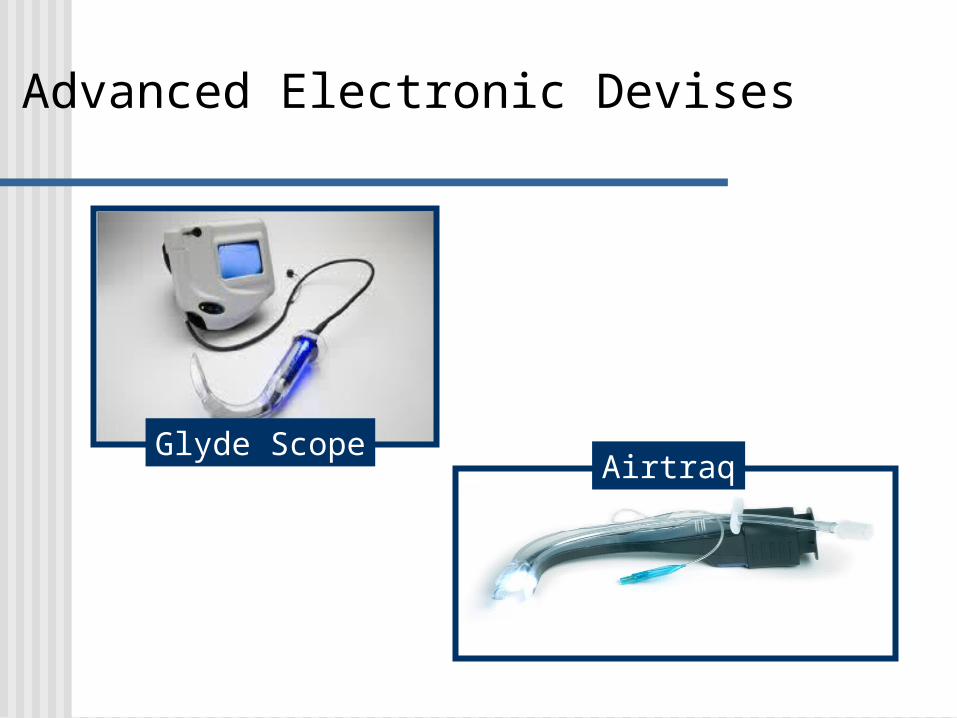
Advanced Electronic Devises
Glyde ScopeAirtraq
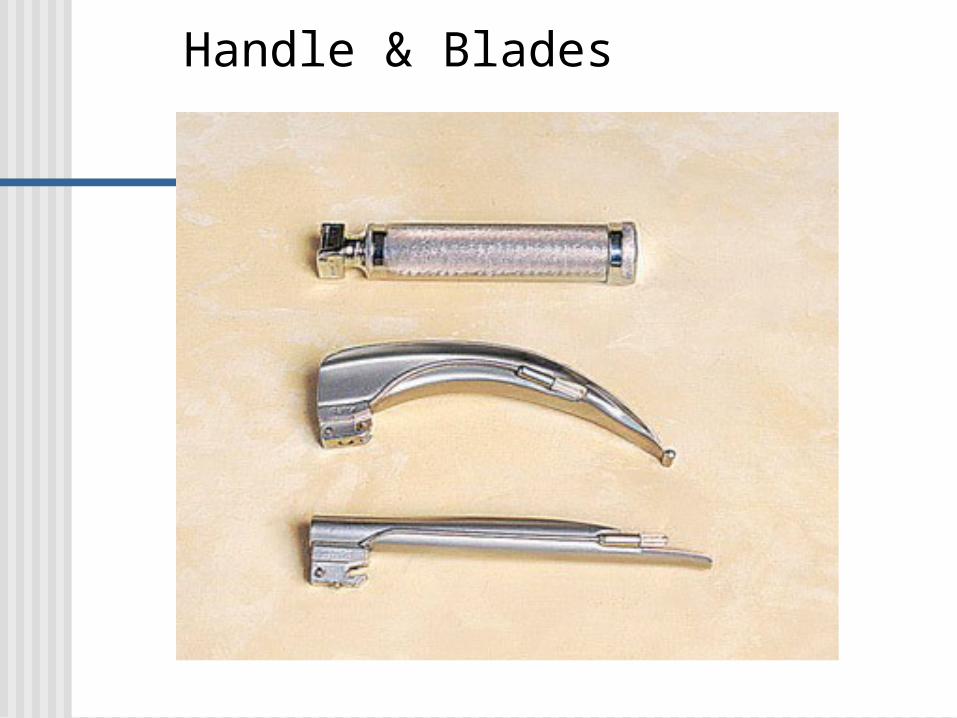
Handle & Blades

Miller (Straight) Blade

Machintosh (Curved) Blade

Semi-rigid stylet

McGuinty Equine Oral Retractor

Intubation
How to look like a star…
And avoid the parking lot.

This is a quest for perfection!
Every intubation is BIG deal!Assume each intubation will be a
difficult intubation.Give yourself every advantage.Control your stress level.Be “surgical”
Prepare your patient
Lateral alignment False teeth Sniffing position Suction
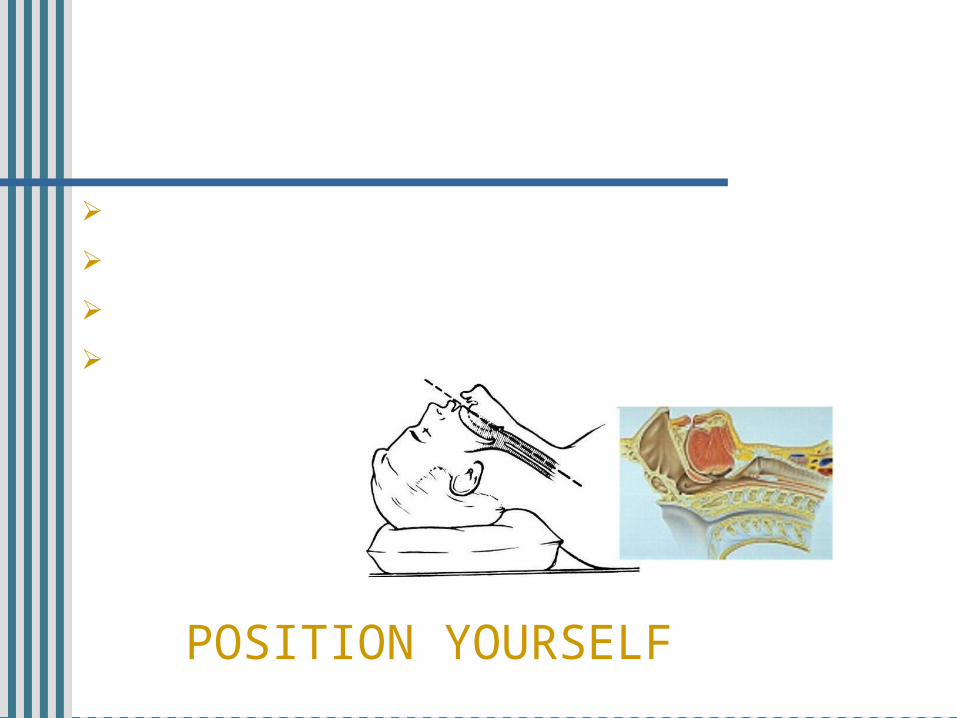
POSITION YOURSELF

What is the “Sniffing Position?”
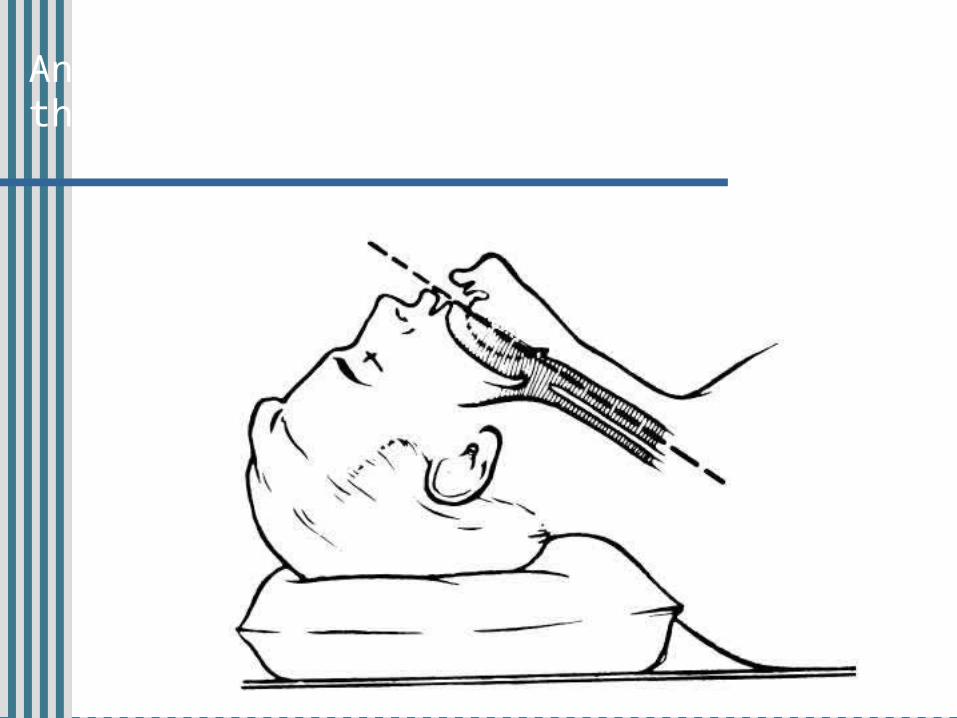
An attempt to align the three planes that form the airway.

Three planes in the airway:
Oral axis:The mouth
Pharyngeal axis:Back of the throat
Laryngeal axis:The trachea

Trying to bring the three planes as close to a parallel alignment as possible.

Patient Positioning
Optimal position: Elevate head to align the ear to the sternal notch.
Picture patients in respiratory distress: Head & neck forward, sitting upright.
Have “pillowing” material available

I’m hanging on your every
word!
Recognize trouble when it arrives.
Technique Nurse! Wipe my
forehead!
More than 90% of cases involving 3 or more attempts in the ED are ultimately
successfully intubated using laryngoscopy.
More than 90% of cases involving 3 or more attempts in the ED are ultimately
successfully intubated using laryngoscopy.
Most cases of “difficult” laryngoscopy in emergency settings are not truly difficult but instead, poorly performed at first and then subsequently managed with better technique.
Do it right the first time!

Proper grip on the Scope
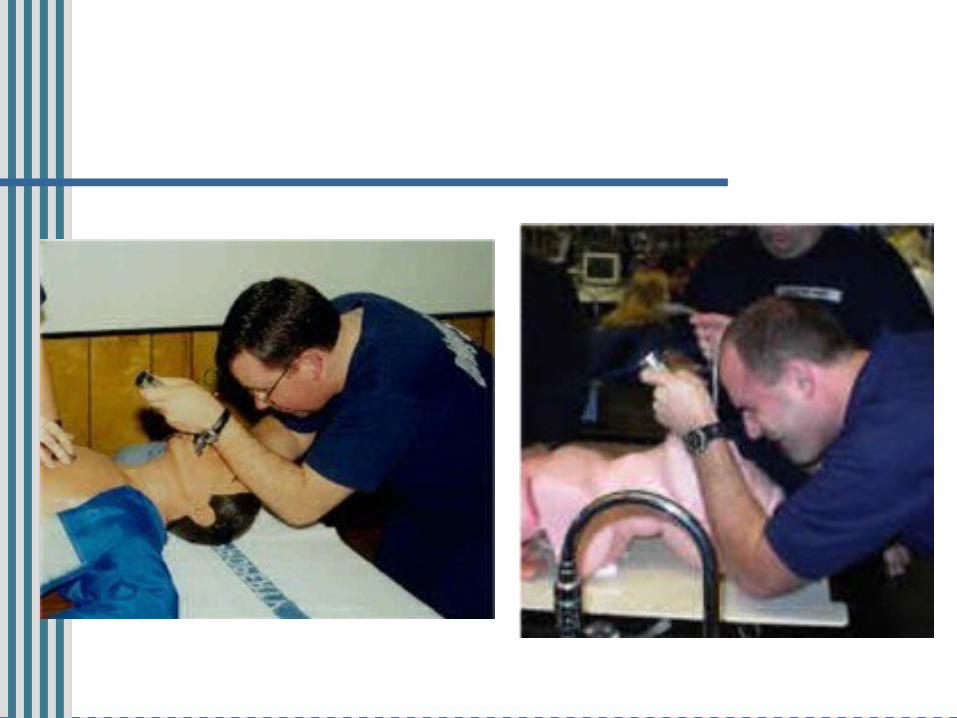
Proper body placement

MANUALLY OPEN THE MOUTH
Use the “scissor” technique.Manually opening the mouth allows control
of the bladeThe mouth tends to be as open as it will get
upon insertion of the blade. Opening it wide initially tends to provide greater success because it allows more room to pass the tube.
Opening the mouth with the blade is
UNACCEPTABLE!

FOCUS ON BLADE TIP
Treat the blade tip like a precision surgical instrument.
You are seeking the epiglotis.Mac blade: insertion into the
velecula.Miller blade: lifting of the epiglottis.
VISUALIZE ANATOMY AS YOU ADVANCE!
NOT a pry bar!
BLADE TIP PLACEMENT
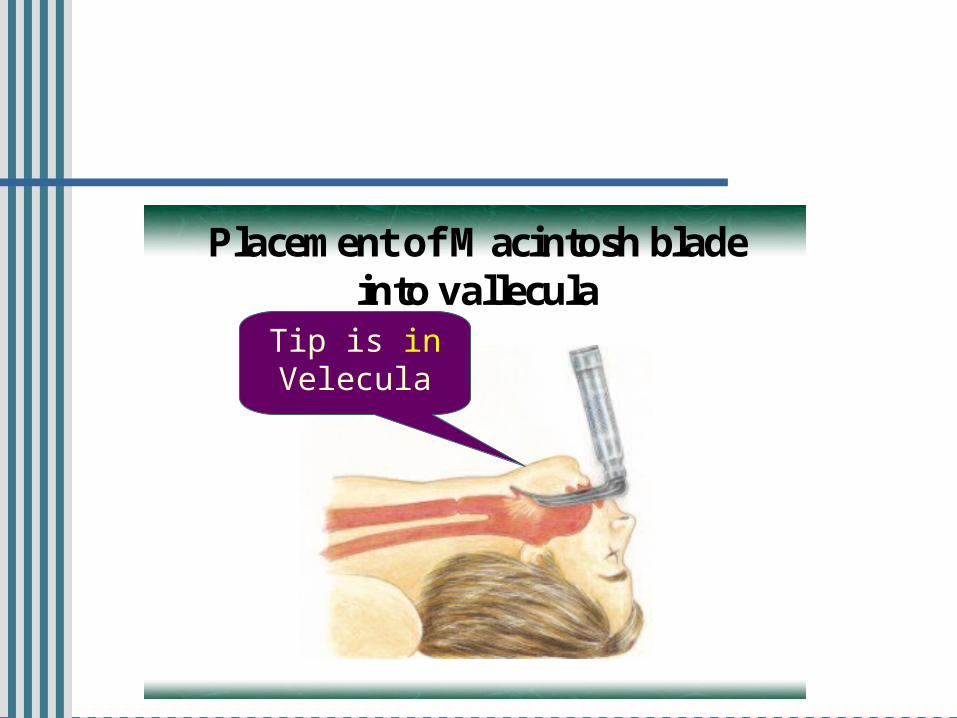
Placement of Macintosh bladeinto vallecula
Tip is in Velecula

BLADE TIP PLACEMENT
Placement of Miller bladePlacement of Miller bladeunder epiglottisunder epiglottis
Tip supports epiglottis
The Storbakken Mantra
Lips
Teeth Tongue
Epiglottis
Vocal Cords
6 steps to success
1. Open mouth manually2. Lips3. Teeth 4. Tongue5. Epiglottis6. Vocal Cords
Verbalize these steps RELIGIOUSLY!
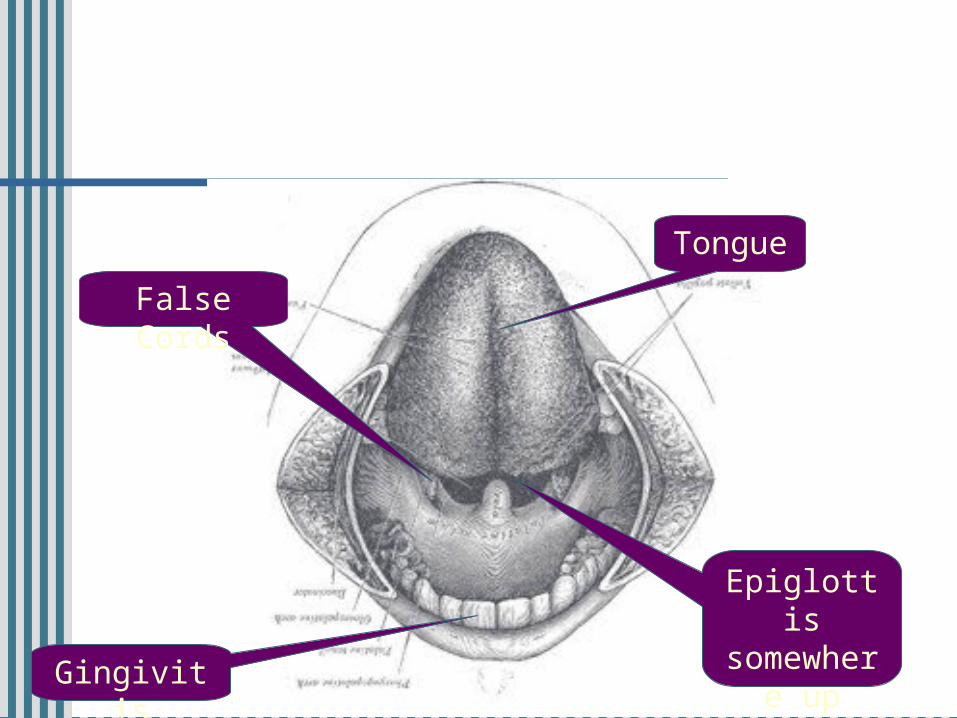
VISUALIZE ANATOMY
Tongue
False Cords
Epiglottis somewhe
re up there
Gingivitis

VISUALIZE ANATOMY

VISUALIZE ANATOMY
TongueFalse Cords
Epiglottis somewhe
re up there

VISUALIZE ANATOMY
intubation final 13.mpg

LOCATE EPIGLOTTIS
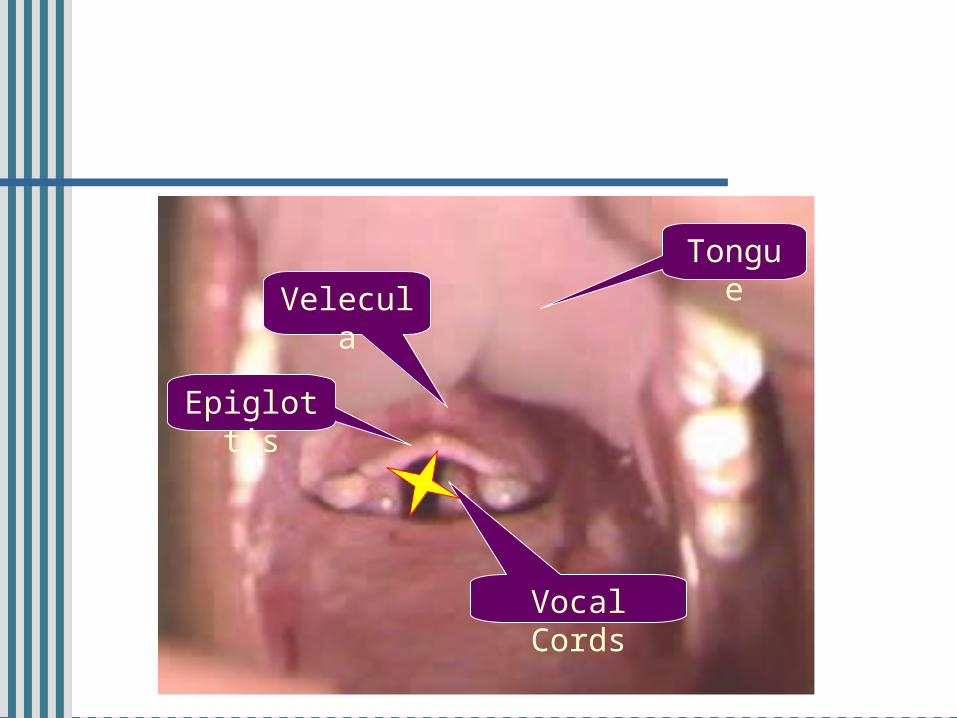
VISUALIZATION
Velecula
Epiglottis
Vocal Cords
Tongue
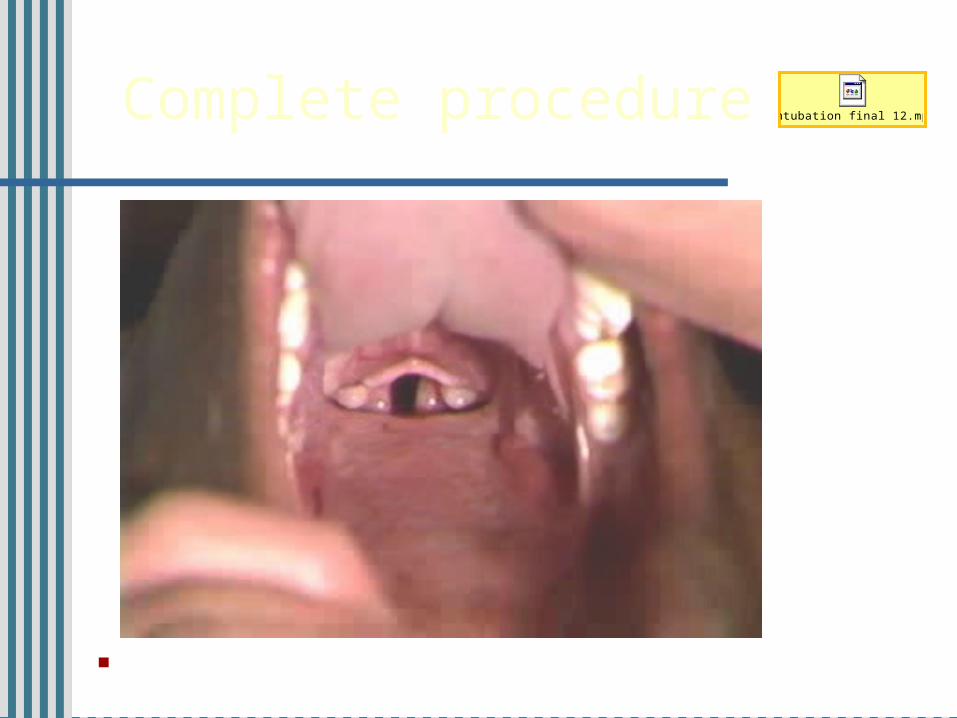
Complete procedure
Notice utilization of the Ukrainian two fisted method.
intubation final 12.mpg