aic orientation course - vbems · aic orientation course manual and reference document for vbems...
TRANSCRIPT

2/16/2017
1
AIC Orientation Course
Manual and Reference Document for VBEMS Members 11/16/16
Welcome to VBEMS This course will help to get you
started in your exciting and rewarding adventure with VBEMS. There is a lot of information included in these pages and the document will be updated and added to over time.
We look
forward to
working with
you!
2
New Member Introduction Course Objectives
Review VBEMS chain of command
Understand your current status and the Trainee process
Discuss VBEMS staffing and scheduling
Understand the scheduling process and OSCAR
Examine basic duty expectations
Learn how to log into the MDT
Review the Virginia Beach ERS system
Understand special responses
Log into the Electronic Medical Record system
Understand the Protocols
3
2/16/2017
2
Virginia Beach Emergency Medical Services
EMS Administration
477 Viking Dr Suite 130
Virginia Beach, VA 23452
Phone: (757) 385-1999
Fax (757) 431-3019
EMS Training
927 South Birdneck Rd
Virginia Beach, VA 23451
Phone: (757) 385-2970
Fax: (757) 437-6560
Routine Hours of Operation: 8:00-5:00, Monday -Friday
4
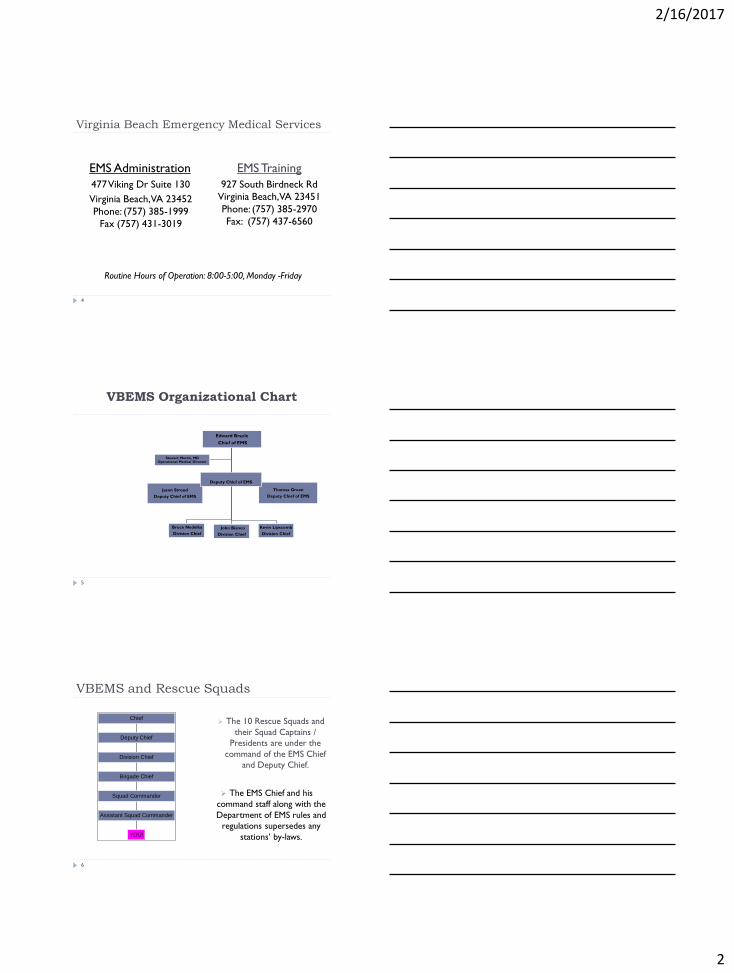
VBEMS Organizational Chart
5
Thomas Green
Deputy Chief of EMS
Jason Stroud
Deputy Chief of EMS
Edward Brazle
Chief of EMS
Bruce Nedelka
Division Chief
John Bianco
Division Chief
Kevin Lipscomb
Division Chief
Stewart Martin, MD Operational Medical Director
Deputy Chief of EMS
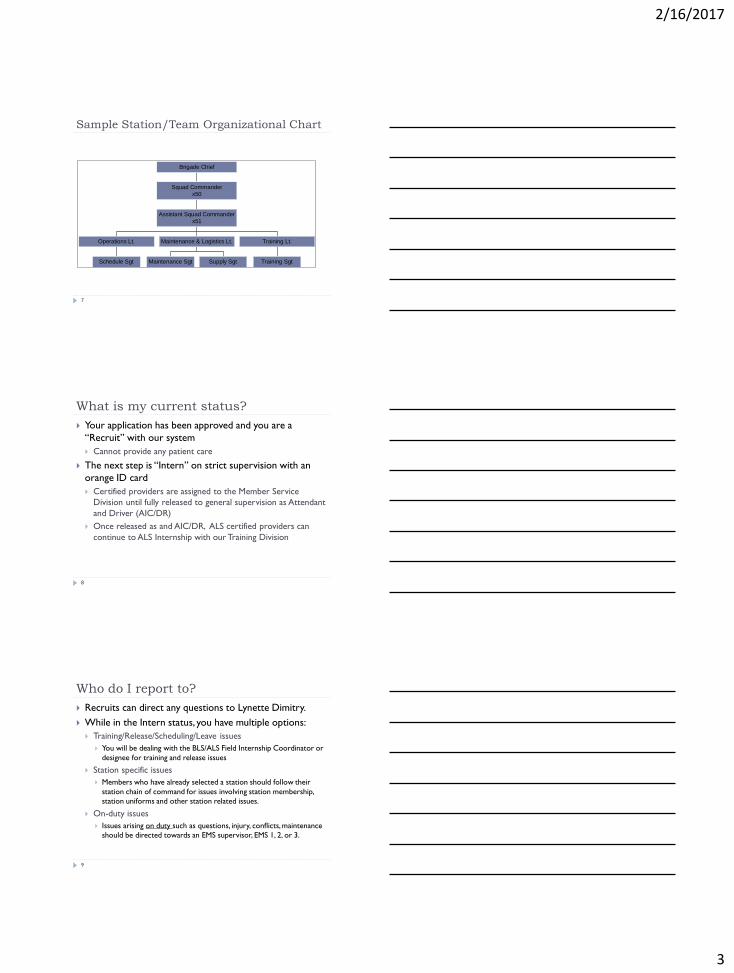
VBEMS and Rescue Squads
6
YOU!
Assistant Squad Commander
Squad Commander
Brigade Chief
Division Chief
Deputy Chief
Chief
The 10 Rescue Squads and
their Squad Captains /
Presidents are under the
command of the EMS Chief
and Deputy Chief.
The EMS Chief and his
command staff along with the
Department of EMS rules and
regulations supersedes any
stations’ by-laws.
2/16/2017
3
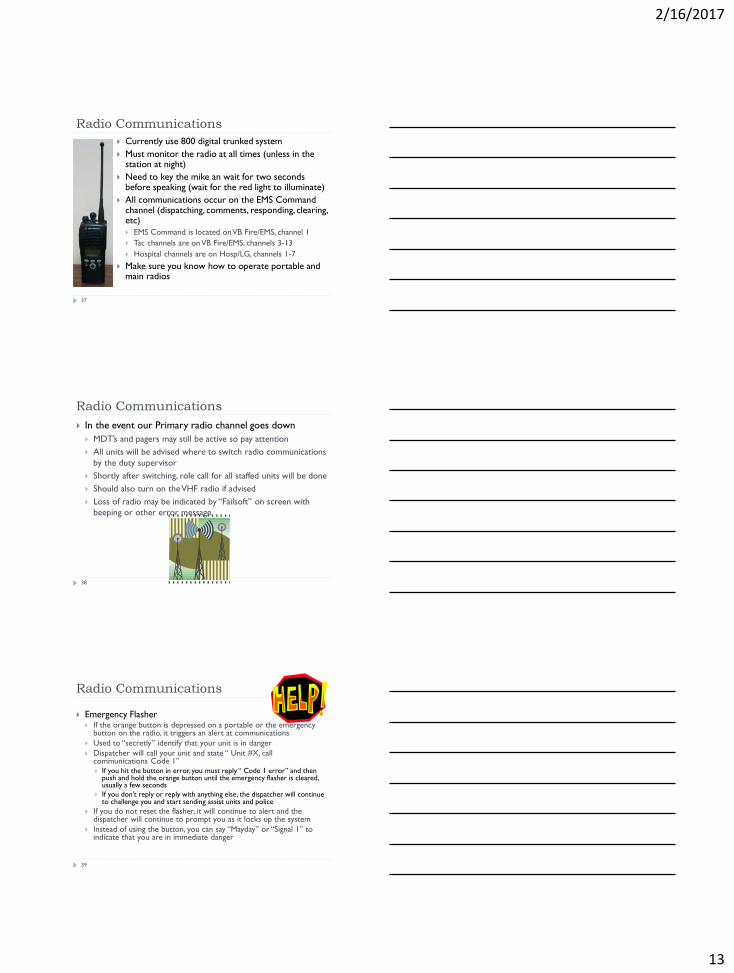
Sample Station/Team Organizational Chart
Schedule Sgt
Operations Lt.
Maintenance Sgt Supply Sgt
Maintenance & Logistics Lt.
Training Sgt
Training Lt.
Assistant Squad Commander
x51
Squad Commander
x50
Brigade Chief
7
What is my current status?
Your application has been approved and you are a
“Recruit” with our system
Cannot provide any patient care
The next step is “Intern” on strict supervision with an
orange ID card
Certified providers are assigned to the Member Service
Division until fully released to general supervision as Attendant
and Driver (AIC/DR)
Once released as and AIC/DR, ALS certified providers can
continue to ALS Internship with our Training Division
8
Who do I report to?
Recruits can direct any questions to Lynette Dimitry.
While in the Intern status, you have multiple options:
Training/Release/Scheduling/Leave issues
You will be dealing with the BLS/ALS Field Internship Coordinator or
designee for training and release issues
Station specific issues
Members who have already selected a station should follow their
station chain of command for issues involving station membership,
station uniforms and other station related issues.
On-duty issues
Issues arising on duty such as questions, injury, conflicts, maintenance
should be directed towards an EMS supervisor, EMS 1, 2, or 3.
9

2/16/2017
4
We are ONE Squad
10
Our organization is divided into 10 Rescue Squads with one
purpose….
Our mission of providing the
best, most timely patient
care.
Station Information Rescue 1/22 - Ocean Park - (757) -464-0594
Rescue 2 - Davis Corner - (757) -460-7574
Rescue 4 - Chesapeake Beach - (757) -460-7509
Rescue 5/21 - Princess Anne Courthouse - (757) -427-4688
Rescue 6 – Creeds - (757) -721-6389
Rescue 9/10/19 – Kempsville – (757) -340-5877
Rescue 13 – Blackwater - (757) -421-2200
Rescue 14/8 - Virginia Beach- (757) -437-4830
EMS Station 15 – Thalia – (757) 385-7307
Rescue 16 - Princess Anne Plaza - (757) -385-2864
Rescue 17 – Sandbridge - (757) -219-2917
Here’s a link to our website with additional information about our Volunteer Rescue Stations
http://www.vbems.com/about-us/rescue-stations/
11
Individual Rescue Squads
12
The city provides fuel, maintenance, radios and some
equipment as well as many other items and benefits to
the stations and members
The stations provide ambulances, soft goods and other
supplies as well as uniforms and many other items and
benefits to its members
Each station has it’s own bylaws, uniforms, policies and
procedures and traditions
The rules and regulations of the EMS Chief, his command staff
and the Department of EMS supersede any stations’ by-laws

2/16/2017
5
Policies, Procedures, Rules and Regulations
VBEMS falls under many regulatory agencies/departments
Federal
OSHA-required for each agency upon initial entry and annually
updated
State
VAOEMS- http://www.vdh.state.va.us/oems/
Virginia EMS rules and regulations
Local
City of Virginia Beach-city code and requirements
VBEMS Policies and Procedures are located on the VBEMS website
http://www.vbems.com/providers/department-policies/
Tidewater EMS Council
13
VBEMS Staffing and “optimized scheduling”
To meet full city coverage, ambulances and crews are
moved strategically throughout the city for coverage
The Optimized Scheduling Coordinator constantly monitors the master
schedule for cancellations, changes and existing gaps in coverage and
augments when necessary
If two stations have a half crew, the Scheduling Coordinator may
combine them
Field Supervisor may split ALS crews
Career medics may augment with a half crew or
may staff additional ambulances
14
What does that mean to me?
15
Sometimes, you will be required to pull duties with members from others squads
Sometimes, you maybe required to split up your duty crew.
Sometimes, you may be requested to pull duties at another station maybe even with members from others squads.

2/16/2017
6
How is scheduling done?
OSCAR (Online Submission and Compilation of Availability
Records) is used by all members to submit their available dates
www.frompaper2web.com/oscartrack
Dates must be submitted by the 10th of the preceding
month
Station scheduling officers craft individual station schedules
using the availabilities submitted by their members
All stations meet around the 20th at a scheduling meeting to
maximize staffing
Interns are added after the scheduling meeting
Final schedules are posted and distributed via Oscar
16
First Time in
OSCAR/Log in
To create a new account:
Go to website and click on “New User?”
•Create a user name
•Create a password
•Enter your email address that you will want any scheduling items to be sent to
•Click “Submit”
17
First Time in
OSCAR/Log in
(cont)
If you have never logged in
before, OSCAR will prompt
you to establish membership
Since you are an EMS
member, enter your Officer
Code number in the space
provided and click “Submit”
The next screen will prompt
you to “Click Here to
Continue”
After this first time, just enter
your user name and password
on the login screen to log in
18

2/16/2017
7
How to enter dates
into OSCAR
When you log into
OSCAR, Select
the month you
wish to submit
duties for
19
How to enter dates
into OSCAR (cont)
As an intern, select EMS- Va Beach Dept of EMS as your Home squad.
You will choose This option until you are released.
The BLS Intern Scheduler will access this list to schedule your shifts.
Then scroll down……
20
How to enter dates
into OSCAR (cont)
Check all the shifts that you are
available for-days, nights or both.
Interns must submit a minimum
of 6 availabilities to maximize
the schedule.
If you are willing to run extra
shifts, you can enter the number
of additional shifts and also
submit any notes.
A note might read “can only do
one shift per week” or “can do
days or nights but not a 24 hour
shift”
Click submit!
Check dates
Extra shift
availability goes
here
Special Notes entered here
21

2/16/2017
8
How to enter dates
into OSCAR (cont)
When clicking on the
calendar, standard shifts are
selected (06-18 and 18-06).
There is no need to enter times if you are running standard shifts.
(Students and Interns are
not permitted to run partial
shifts without prior
approval so you shouldn’t
need to do anything with
this screen)
22
How to enter dates
into OSCAR (cont)
After you click “submit”, a
confirmation screen will appear.
Please take a moment to make sure
it is correct!
If it is not correct, or your schedule
changes after your submission (and
before the 10th), go back to the
OSCAR home page and click on
“Reconfirm or Retract” and follow
the instructions on the next screen.
**To make changes after
the 10th, you must contact
the BLS Intern scheduler.**
23
Log out
How to enter dates
into OSCAR (cont)
After you follow the retraction instructions, you will receive an email.
When you click on the link in the email, it will retract your current record (you will get the confirmation screen).
You will have to start all over to resubmit your proper dates.
24

2/16/2017
9
I am scheduled for duty!
After the availabilities have been submitted and schedules have been created, you will be notified of your assignments via an Oscar email
If you have a change in events, interns must trade/find coverage with another intern to make sure the shift is covered.
If you become suddenly ill and can not make your shift, you must contact EMS 1 at 274-2946 or EMS 2 at 635-7695 and notify the BLS Intern scheduler.
You should also notify the BLS Intern scheduler if you are late for duty or if you are moved to a new assignment.
If you find that your crew is not fully staffed, you must contact EMS 1 or EMS 2 for a new assignment (unless it will be staffed within 1-2 hours).
25
Shift assignments
As an intern, you may or
may not be scheduled at
your home station.
Shifts run from 0600-1800
and from 1800-0600
Schedules are always
changing so make sure you
monitor your email
You can verify your
schedule on the My
Assignments tab in Oscar
any time.
26
Important Intern Items to note-Duty
You must wear your EMS ID card whenever you are on
duty or in a city building
Wear the proper uniform while on duty
Shirt tucked in, pants not too loose/tight, shoes tied, belt, etc.
First impressions are important so look the part!
Remember to wear a watch
Try to arrive for duty15 - 30 minutes prior to the start of
shift and be ready to go
You may perform any skills authorized for the EMT BLS
level in the City of Virginia Beach while in the presence
of a released AIC or released ALS provider while on duty
27

2/16/2017
10
Professionalism and Accountability
28
Be Professional
Make deadlines (schedules, paperwork, projects, etc.)
Be on time or early
Wear the proper uniform
Keep others in the loop and informed
Be Accountable
Know when to ask for help
Take responsibility for your actions
Do the right thing!
Be a reliable member and partner
Driving an Emergency Vehicle
29
Members with Defensive Driving Class (DDC) can drive any city
insured vehicles
Only members with Emergency Vehicle Operations Course (EVOC) can drive in emergency mode (with lights and sirens) and interns must have a released driver in the front seat with them Driving lights and sirens is a big responsibility
“Nothing shall release the operator of any such vehicle from civil liability for failure to use reasonable care in such operation.”
Good Samaritan Law does NOT provide immunity from bad driving
Never Run a Red Light
You must be sure the intersection is clear before proceeding
You must slow down at red lights so you can stop before proceeding into the intersection
Members caught on a PhotoSafe red light camera can be subject to discipline and the fines
Members should wear a seatbelt at all times (unless required while
providing patient care in the back of the ambulance) All Patients and equipment should be secured at all times
Members are not permitted to use EMS vehicles to initiate traffic stops
Before the Call
At the start of shift your crew will log into the MDT, the
EMR and sign on over the radio
You must be added to both as part of the crew
MDT (Mobile Data Terminal) provides you with case information such
as the address and comments with updates as sent by dispatch
Can use for status changes, looking up cases, typing messages, etc
EMR (Electronic Medical Record) is how we document patient care
reports
Let your crew know what
your shift training
goals are!
30
Incident number

2/16/2017
11
MDT-Logging in
When you click on the “Logon”
screen, you will enter the following:
Unit ID: ambulance number such as
2222S
Vehicle #: vehicle bumper number
Password: of the person logging on
the vehicle – please have your AIC
help you establish a password ** your
Initial password is your Officer code
number**
Shift: if needed
Officer: officer code/800 number
(first officer # should match the
password)
Portable#: portable radio ID number
Enter subsequent officer codes and
matching portable radio numbers
Press “Logon to system” button or
“enter”
31
MDT Logon Troubleshooting
If you are having difficulty with your officer
code/password:
Ensure you are using the right combo of upper/lower case
letters—the MDT defaults to all caps
If it won’t work for you, let your partner try
You will want to have the dispatch supervisor reset your password
Make sure you staff up over the radio so they know you are
manned!
32
Emergency Response System
The ERS is an effort from the public safety agencies to
provide a coordinated response
Emergency Communications, EMS, Police and Fire work
together to respond the right units to all emergencies
33

2/16/2017
12
Situational Awareness
The public only sees us as one EMS system
The need to be aware of calls throughout the City while
on duty is your responsibility
One missed call, one unprofessional act, one improper
driving technique casts a bad light on the entire
organization
Everyone is watching
We are in a high profile, high risk profession
Dispatching
911 calls are received at the Communications Center (ECCS)
Dispatchers use Emergency Medical Dispatching (EMD) to determine the nature of the emergency with predefined questions
Offer basic first aid instructions if the caller
will accept them
EMS cases are either dispatched as
Priority 1 or Priority 2 based on the EMD
recommendation
Pri1 cases include chest pain, breathing
difficulty, entrapments, etc
Pri 2 cases include illnesses, minor injuries and
other minor situations
35
Dispatching (cont)
If in the station, your tones will go off and lights will turn on
If on the road, you will hear your unit dispatched over the
radio and your MDT will chirp
Always monitor the radio!
Units are dispatched based on preset run cards
If your unit is closer, you should offer to that information to the
dispatcher/EMS supervisor
Units may be reassigned by EMS supervisors based on many variables
If responding to calls with multiple units/departments, you may
be assigned a TAC channel-you need to switch to it as soon as
possible
36
2/16/2017
13
Radio Communications
Currently use 800 digital trunked system
Must monitor the radio at all times (unless in the station at night)
Need to key the mike an wait for two seconds before speaking (wait for the red light to illuminate)
All communications occur on the EMS Command channel (dispatching, comments, responding, clearing, etc)
EMS Command is located on VB Fire/EMS, channel 1
Tac channels are on VB Fire/EMS, channels 3-13
Hospital channels are on Hosp/LG, channels 1-7
Make sure you know how to operate portable and main radios
37
Radio Communications
38
In the event our Primary radio channel goes down
MDT’s and pagers may still be active so pay attention
All units will be advised where to switch radio communications
by the duty supervisor
Shortly after switching, role call for all staffed units will be done
Should also turn on the VHF radio if advised
Loss of radio may be indicated by “Failsoft” on screen with
beeping or other error message
Radio Communications
Emergency Flasher If the orange button is depressed on a portable or the emergency
button on the radio, it triggers an alert at communications
Used to “secretly” identify that your unit is in danger
Dispatcher will call your unit and state “ Unit #X, call communications Code 1” If you hit the button in error, you must reply “ Code 1 error” and then
push and hold the orange button until the emergency flasher is cleared, usually a few seconds
If you don’t reply or reply with anything else, the dispatcher will continue to challenge you and start sending assist units and police
If you do not reset the flasher, it will continue to alert and the dispatcher will continue to prompt you as it locks up the system
Instead of using the button, you can say “Mayday” or “Signal 1” to indicate that you are in immediate danger
39

2/16/2017
14
Radio Communications
40
Use plain talk Courtesy is assumed (“Can you please show unit x manned” can be
reduced to “Unit x is manned”)
Transmit direct questions and pertinent information, not reasons (“Our computer is broken, can you log us on?” becomes “Log on unit x.”)
When initiating communication over the radio say your Unit # to ___. Examples would be … Unit # to EMS01 or
Unit # to Virginia Beach - for raising the Dispatcher
“Air is restricted” Occurs frequently on police channels but means that no
communication should occur unless the crew requesting the restricted air has something to say
All other units should stay off the radio or use the fire channel until the restriction is lifted
What is a tiered response?
VBEMS uses a tiered response system Ambulances (BLS and ALS)
Ambulances can be BLS (R), Enhanced (S), or ALS (P)
All ambulances are ALS equipped
ALS zone cars-Intermediate/Paramedic A zone car may be dispatched with a BLS ambulance
If the patient does not require ALS transport, the zone car can clear
Fire first-response (BLS and ALS) Engines are dispatched for all Pri 1 cases, or if requested for time and
distance for Pri 2 cases
Engines should leave access on scene for units for best access to the residence
41
What to bring in with you on scene
Stretcher
Jumpbag with O2
Life Pack 15
42

2/16/2017
15
Specialty Responses-Cardiac Arrest
Police officers with an AED are dispatched
There are over 150 AED’s assigned to the police dept and we have had
many lives saved because of them
All officers are trained in CPR
An ambulance, engine, and EMS supervisor are dispatched
Supervisors and some ambulance carry LUCAS to be used for
compressions (LUCAS Training is included in the OPS II Class)
Dispatchers give CPR and choking instructions
if the caller wants them
Two zone cars are sent
Zone car may be cancelled by EMS supervisor
if ALS is on the engine or ambulance
43
Specialty Response-Working Fire
After the working fire is declared, automatic additional units
include an ambulance and an EMS supervisor
Responding units should switch to the assigned Tac channel
Units should be aware of egress from the scene (don’t get
blocked in by a hose)
If no assignment is given, check in with command on arrival
Crews should bring their stretcher, jump bag, monitor and a
back board to the rehab area and be prepared to rehab the
firefighters
If there are patients, additional
ambulances and possibly ALS are sent
as needed
44
Specialty Response-Hazmat
An ambulance is sent to all working hazmat cases
Responding units will switch to the assigned Tac channel
and report to command
Depending on the level of hazmat, crews may need to
perform entry and exit physicals on firefighters
EMS will not enter the warm or hot zone
Pay close attention
to staging directions
45

2/16/2017
16
Specialty Response-Airport Alert
Virginia Beach sends EMS and fire units to all Norfolk
International Airport Field emergencies
Units will be assigned a Tac channel
Units stage near Miller Store Rd and Burton Station Rd
Airport Fire is in command and works with Norfolk
Fire/Rescue and VB units
46
Specialty Response-Police Standby
Includes standbys for warrant service, hostage/barricade, and bomb scares
Unit will be assigned a staging location and unless otherwise notified, crews
need to stay with the vehicle until called in
If requested by SWAT medics, you should monitor the assigned Tac channel
for updates and evolving events
Standbys can be lengthy-the EMS supervisor will relieve crews as needed
47
Specialty Response-Entrapment
Standard response includes ambulance, zone car, EMS supervisor, fire engine, ladder and squad truck Alterations in response made
by command or EMS 1, 2 or 3
Personnel inside action area should be in protective gear There are a lot of sharp objects,
trip hazards and increased risk
Units are assigned a Tac channel and should switch upon dispatch
Most often, ambulance crews focus on preparing to receive the patient after extrication is complete
48

2/16/2017
17
Specialty Response-Water Rescue
VB has a lot of waterways!
Can include drownings and incidents with water craft
Reach, throw, row…..do not become a victim
Ambulance, zone car, EMS 1, 2 or 3 and marine rescue
team dispatched along with other resources from fire and
police—crews should switch to the assigned Tac channel
If you are the first unit, speak with
witnesses and obtain the point
last seen and gather as much
information as possible
49
Specialty Response-Medevac
The AIC on scene can request a helicopter due to time and
distance from the hospital
EMS 1, 2 or 3 may place one on standby prior to units being on scene
based on comments
EMS 1, 2 or 3 determines if Airmed or Nightingale will respond and then
makes request
VBEMS has a medevac helicopter staffed by medics
Airmed is a dual mission aircraft-police/medevac
Must be a paramedic to join
the Medevac team
50
Specialty Response-Military Installations
We often respond to military bases-stop at the gate
They will often provide a vehicle escort from gate
We often provide assistance for large events such as the
Oceana Air Show and drills
All units have VB radios and are listed in our CAD
No POV responses
They can request an
ALS only response
51

2/16/2017
18
Specialty Response-Mass Casualty
52
MCI is an incident that overwhelms the resources
One crew could be overwhelmed by a few patients or a city could be
overwhelmed by hundreds of patients
If first onscene of multiple patients, assume command, perform triage and
share information
5 S’s-Safety, Size-up, Send, Setup, Start
A lot of units are coming so start thinking about staging and scene flow
VBEMS has 2 MCI trucks which can handle approx 50 patients with
supplies
Specialty Response-Interstate calls
53
An engine is sent to ALL cases on the interstate or off ramps to assist with traffic control
Ambulances and smaller vehicles should park IN FRONT of the engine
Enter Interstate well behind the reported accident to avoid missing it.
For example if the accident is 264 E/B at Witchduck, get on at Newtown
Wear safety vests, be cautious when
exiting vehicles and always be on
the lookout.
Switch to assigned TAC channel
Specialty Response-Large Scale/Major Events
54
There is a potential for unexpected major events
requiring many resources
If an event occurs, do not respond directly to the scene
If you can assist, respond to a station and staff a unit.
Those out on medical or other leave cannot respond
Must have released ID to respond
If there are no units available, stage at the station and
await further instruction.
2/16/2017
19
Other Items of Note
Declaring a patient deceased
Any released AIC can declare a pt deceased
Sometimes just one provider will enter at PD request to pronounce depending on circumstances
North Landing Bridge
You should call ahead and advise your ETA if using that route
Standbys
We have many large events throughout the year requiring standby units assigned to the event
Should be self-sufficient but may require a unit to stand-by while they are transporting or ALS assistance
Will often have a command structure established with a Tac channel
55
Other Items of Note (cont)
56
POV Responses
POV responses are not permitted while in intern status
Trainees should only respond to cases while in uniform and on duty
POV responses are never permitted to the interstate
The use of emergency lights in a POV is very highly
discouraged
Operators use them at their own risk and must obey traffic laws or
are subject to ticketing by police
Photography on Scene
You are not allowed to take photos or
recordings while on calls without advance
prior permission from the Chief for any reason
Other Items of Note (cont)
CISM-Critical Incident Stress Management
Contact a EMS supervisor if you feel you or your crew may benefit from CISM
Region has CISM team
Many of our members are very involved
Different levels of team involvement based on incident-from one-on-one to large groups
DNR (Do Not Resuscitate) and DDNR-Durable DNR
VA providers can honor a written DNR order signed by a physician in a licensed facility or the yellow original state DNR form/legible photocopy
DNR jewelry, original POST forms etc. can also be recognized
http://www.vdh.state.va.us/OEMS/Files_page/DDNR/DDNRFactSheet.pdf
Virginia EMS providers CANNOT honor a Living Will or a DNR from another state
If in doubt, contact medical control for advice on how to proceed
57

2/16/2017
20
Other Items of Note (cont) Child/Elder Abuse Reporting
VA EMS providers are mandated reporters meaning we are responsible to report the suspected abuse directly to APS/CPS within 24 hours Required to report suspected abuse, neglect, or exploitation of elders or
incapacitated adults.
When you suspect that a child is being abused or neglected (physically, mentally, emotionally, sexually)
If you have any doubt as to whether you should report or not, you should report it
Report must be made immediately EMS providers can report the situation directly to the receiving physician in lieu of
reporting
EMS supervisors cannot make a report on your behalf
Reporters should provide the name, age and address or location of the person who is suspected of being abused, and as much information about the abusive situation as possible
http://www.dss.virginia.gov/abuse/
58
Other Items of Note (cont)
Accidents involving vehicle insured by the city
Notify EMS supervisor, dispatch and PD immediately
If transporting a patient, request an additional unit for
transport
Do not move the vehicles unless absolutely necessary
Supervisor will determine if vehicle needs to be evaluated by
the city garage
The crew may be subject to a urine screen
Loss/Damage of property insured by the city
Notify squad commander or EMS supervisor as soon as the
loss/damage is noted
59
Other Items of Note (cont)
Personal Injury while on duty
If you are injured while on duty, contact EMS supervisor immediately
If proper and timely notification is not made, reimbursement by the
city is not guaranteed
You may be directed to an ER, occupational health or other facility
for emergency treatment
Depending on the injury, you may just complete the paperwork
You will be required to visit Occupational Health for permission to
return to duty
Illness on duty
Illnesses in which you need to go home should be reported to EMS 1
or 2 immediately so coverage for your position can be arranged
60
2/16/2017
21
Other Items of Note (cont)
Exposure to blood or body fluids while on duty
True exposure is: “A specific eye, mouth, other mucous membrane,
non-intact skin, or parenteral contact with blood or other potentially
infectious materials that results from the performance of an employee’s
duties”
Clean/flush the affected site immediately
Report the incident to EMS 1, 2 or 3 immediately
EMS supervisor will walk you through reporting steps until you
are handed over to Occupational Health
EMS Admin is notified of the exposure but Occupational
Health deals with all results and contact for your privacy
Your station is not notified unless you tell them
61
What if you are charged with a crime?
62
If you are charged with a crime involving off duty activities, you
must notify your immediate supervisor and DEMS Division
Chief of Support Services/Admin as per the Criminal Activity
and Traffic Offense Reporting Policy within 24 hours of the
citation/charge
Includes being served, arrested or cited for the following:
Traffic violations involving speed, DUI, reckless driving, suspension or loss of
license----any moving violation or loss of license
All alleged criminal activity that has or may lead to arrest, detainment or
conviction
Any activity that is alleged to be criminal in nature by law enforcement
personnel, including all misdemeanor offenses.
Charges need to be reported-not just convictions
Other Items of Note (cont)
63
Privacy and Protected Health Information (PHI)
Any information collected from an individual that is created or
received by a health care provider, relates to the past, present,
or future condition of an individual, and which can reasonably
used to identify an individual.
Includes things such as phone numbers, SSN, record numbers,
addresses, names, license plate number, DOB, email address, photos,
etc.
Must shred any notes containing this information and log out of Field
Bridge when not in use.
Information about calls should not be shared or discussed with
anyone who wasn’t on the case with you

2/16/2017
22
Other Items of Note (cont)
64
Patient Refusals
The legal age of consent in VA is 14 years or older
Use your judgment if no adult is readily available in anyone under age 18
Those under 18 who are emancipated or pregnant are also capable of refusing
Patients should be “competent” to refuse meaning alert, oriented, not under the influence and not suffering from an illness or injury that would alter their judgment
If you have concerns about allowing the patient to refuse, contact Medical Control and/or EMS supervisor
A report must be completed including vitals signs and all patient information
Don’t forget signatures and the AMA form
After the call
Patient care records are completed
Unit is put back together and cleaned
Crews will restock approved items from the hospital
Only take what you used (linen included)
Stations maintain stock for refusals and replacement
Some hospitals require the TEMS Exchange form to be completed
Hospitals provide drug and IV boxes for restock
Must leave a completed exchange slip with each box returned
If one item is used, entire box is exchanged
Contact EMS supervisor if you need to delay clearing for
important supplies
Advise over the air that your unit is available
65
Electronic Patient Care Reporting (ePCR)
66
Your reports
Are important to your patient and their treatment.
Are used at the local, state, and federal levels.
Are a reflection of your professionalism as a healthcare provider.
Hospitals have direct access to your posted reports and use
them daily.
In 2015, EMS Admin processed 758 requests for reports to
attorneys, medical examiners, patients, or the
City/Commonwealth Attorney.
2016 is on track to exceed those requests.

2/16/2017
23
Electronic Patient Care Reporting (ePCR)
67
When do you need to complete a report?
For every dispatch, whether patient contact is made, including:
Transports, refusals, death pronouncements, public assists, standby
events, or cancellations/no patient contact.
For cancellations, if you are cleared:
By VBFD
VBFD is responsible for the report
By another VBEMS unit
That unit will complete the report
By anyone else (dispatcher, VBPD, etc.)
Ambulance crew is responsible for the report
Electronic Patient Care Reporting (ePCR)
68
Report Requirements
Per Virginia Law (12VAC5-31-1140. Provision of Patient Care Documentation)
Patient care reports are due to the receiving facility at the time of patient transfer.
If unable to provide a full report, an abbreviated (verbal) report is made at the hospital and the full report us due within 12 hours.
Required fields are established at the national, state, and local levels.
Reports must meet a minimum validation score of 98% to be considered complete.
Only complete reports are sent to Virginia or Sentara.
Expect to be contacted to finish an incomplete or missing report.
Electronic Patient Care Reporting (ePCR)
69
Computer Hardware
Keep your EMR charged.
Reboot it at the start of your shift.
Decon as needed, otherwise be gentle when cleaning the screen.
Shut down when not in use.
Shift supervisors are your first line of support
They have replacement computers, batteries, chargers, and styluses.
You may be asked to document damage or failures to help identify
and correct problems.
You won’t be in trouble if asked to fill this out. Accidents happen. But
issues can’t be fixed if they aren’t reported.

2/16/2017
24
Electronic Patient Care Reporting (ePCR)
70
Mobile Data Terminal (MDT)
Ambulance computer in the front of the ambulance, used to
interact with dispatch, receive call information, etc.
Call a Dispatch Supervisor to reset your password.
Broadcasts the CVB-EMERGENCY Wi-Fi network used by
EMRs.
Reboot the MDT if having problems connecting to the
internet.
Electronic Patient Care Reporting (ePCR)
71
Wi-Fi use
For EMRs, only connect to CVB-EMERGENCY and CARE4U
networks.
This includes your station’s Wi-Fi network.
Connecting to multiple networks has proven to cause connectivity
issues.
Electronic Patient Care Reporting (ePCR)
72
Elite
Our patient care reporting software from our vendor,
ImageTrend.
Is web-based, however it can work offline in Field Mode (away
from Wi-Fi)
You must be connected to Wi-Fi in order to
Login
Download CAD
Look up repeat patients
Zip code lookups
Posting or transferring reports

2/16/2017
25
Electronic Patient Care Reporting (ePCR)
73
Sign in with your username and password
If you lost your password, use self-service to reset it.
Shift supervisors can also reset your password if needed.
If you need additional assistance, email [email protected].
Electronic Patient Care Reporting (ePCR)
74
EKG transmission/download First step is ALWAYS to gently plug the USB cable from the LifePak into
the EMR.
If sending a 12-lead to the hospital Press TRANSMIT on the LifePak and select a HOSPITAL as the site.
Then press SEND.
If downloading 12-lead into the report Launch the Elite Desktop Client and click the Physio-Control
Transfer Wizard button.
Press TRANSMIT on the LifePak and select EMR NOTEBOOK as the site. Then press SEND.
From inside Elite, click the EKG button and find your downloaded data, then click Import Selected.
Electronic Patient Care Reporting (ePCR)
75
Quick reference instructions are available right on your
EMR desktop:

2/16/2017
26
Electronic Patient Care Reporting (ePCR)
76
Transferring Reports
Used to transfer a report in progress from one EMR to
another.
Be sure to download CAD data first.
View Transfers is keyed off Dispatch Time. Leaving this blank and
transferring will make it difficult to find your report.
It is your choice whether leave the report on the original EMR.
Just be sure you don’t post the report from two different devices or
you will lose data!
Electronic Patient Care Reporting (ePCR)
77
EliteBridge
Website where you can start or complete reports if the EMR
is unavailable.
http://www.vbems.com/elitebridge
Log in with the same username and password as on the EMR.
Also where you will receive CQI messages and patient
outcome information.
Electronic Patient Care Reporting (ePCR)
78
Review
Patient care reports are due within 12 hours of patient turnover.
Minimum validation score is 98% for all reports.
Use only the CVB-EMERGENCY Wi-Fi network.
You must be connected to Wi-Fi to log into Elite, download CAD data, or lookup repeat patients.
If you forget your password, use self-service features to reset it.
Sign into EliteBridge to access your reports after the incident, and, to view Inbox messages about your reports.
If you need assistance:
Contact a shift supervisor when on duty.
Otherwise, email [email protected].

2/16/2017
27
Tidewater EMS Council
TEMS integrates and coordinates resources
Coordinates between more than 70 local EMS agencies and 12 hospitals
EMS system planning, regional medical direction, standardized medication and IV exchange system, mass casualty planning, trauma triage planning and quality improvement
Implementation and sustainment of the Hampton Roads Metropolitan Medical Response Team
TEMS agrees on consistent protocols which are approved by the Operational Medical Directors committee
Individual medical directors may expand or limit the regional protocols
Where to find them-TEMS website
http://tidewater.vaems.org/tidewater-ems-council/protocols/2013-protocols/1679-tems-protocol-pocket-guide-2014-06-02/file
79
Protocols-Goals and Expectations
Goals
Establish minimum expectations for appropriate patient care
To relieve pain and suffering, improve patient outcomes and do no harm
To ensure a structure of accountability for operational medical directors, facilities, agencies and providers
Protocols are derived from a variety of sources
Expectations
Protocols are designed to be used in conjunction with each other- it is acceptable to use more than one protocol at a time
Providers will maintain a working knowledge of the protocols
Each patient should have a thorough assessment performed
BLS providers should request ALS assistance if any deficiencies are found on the initial assessment
80
Protocols-Format
Introduction
Legend of symbols, Skills delineation, Medication lists
Reference Sections
Adult and pediatric
Burn chart, drip charts, pain scale, APGAR, etc
Protocols
Adult Cardiac and Adult General
Peds Cardiac and Peds General
Each protocol includes flowchart and informational page
Performance Indicators-included for each protocol
81

2/16/2017
28
Protocols-Legend of Symbols Teddy bear in the upper right corner of protocol
indicates a corresponding pediatric protocol (age 14 and younger/55 lbs)
Assessment Decision Point
Assessment or Action
Delivery
Treatment
Decision point that can occur independently of other actions or simultaneously
82
Protocols-Legend of Symbols (cont)
Next to “Treatment” boxes, you will note letters
EMT = EMT-Basic
A = EMT-Enhanced
I = EMT-Intermediate
P = EMT-Paramedic
MD = Physician
[Brackets] around the letters indicate PHYSICIAN ORDER
That level can perform the skill but must have permission from med control
Physician Orders require a signature from a receiving practitioner on the EMR
No brackets indicate STANDING ORDER
You can complete the task or skill up to your released level without calling med control for permission
83
Protocols-SO vs. PO Symbols [EMT]
A
I
P
A
I
P
[I]
[P]
Indicates EMT-B can administer the
subcutaneous epi with physician orders
only and all other levels can administer on
standing orders
(EMT-B’s can only use the patient’s Epi-pen)
Indicates EMT-Enhanced and above can
administer Benadryl on standing orders
Can only be administered by EMT-
Intermediate or above and with physician
orders
Epinephrine
1:1000 0.01 mg/kg
SQ/IM
Max dose 0.5 mg
Diphenhydramine
(Benadryl) 50 mg IV,
(IM if IV not available
Consider sedation
Haldol 5mg IM (Large muscle area)
and 2mg Ativan IM
84
2/16/2017
29
Protocol of note-
Airway/Oxygenation/Ventilation
Supplemental Oxygen
Many programs teach high flow oxygen for all patients
We base oxygen delivery on the individual patient
Goal for SpO2 (pulse ox) reading is 94% or higher
For patients with adequate respirations
For a pulse ox between 90-93%, consider a nasal cannula at 1-6L
For a pulse ox less than 90%, use a non-rebreather
Upgrade or downgrade as necessary
Provide oxygen for all patients with altered mental status,
hypoperfusion, chest pain, significant trauma, CO exposure or SOB
regardless of the pulse ox reading
85
86
87

2/16/2017
30
Protocol of note-Spinal Immobilization
To rule out the need for spinal immobilization, the patient must:
Have no positive mechanism
High speed MVC, age extremes, axial load, diving accident, loss of consciousness, etc
Low risk mechanisms can also produce spinal injuries (elderly falls)
Be reliable
Must be calm, cooperative, not impaired by drugs or alcohol, alert and oriented and have no distracting injuries
Distracting injuries can include fractures, dislocations, severe bruising or cuts
Have no spinal tenderness or pain
Have a normal motor and sensory exam
If there are any doubts or questions, immobilize!
88
89
90

2/16/2017
31
High-Performance CPR
High-Performance CPR (pit crew method) is becoming a
standard practice to better patient outcomes.
It’s a practical application of the science
In line with AHA 2010 ECC Guidelines
Standardize approach saves lives!
91
How we’re doing
An average survival rate (SCA) of 34-36%
We use the same measurement tool as Seattle, Wake,
CARES, etc.
National SCA Survival Rate is 30.2% (Valderamma, 2011).
Seattle 56%
Wake Co, NC. 45%
Rochester, MN 58%
Charlotte (Mecklenberg) 52%
While we’re doing good…we can always do better!
92
High Performance CPR
1. Own CPR!
2. Minimize interruptions in
CPR at ALL TIMES
3. Ensure proper depth of
compressions
4. Ensure full chest recoil
5. Ensure proper
compression rate (100-
120)
6. Rotate compressors every
2 minutes
7. Hover hands over chest
during shock
administration
8. Do NOT stop CPR to
place an advanced airway
9. Do NOT stop CPR to
obtain IV/IO access
10. Coordinate
care/movement between
BLS/ALS
93

2/16/2017
32
Pausing makes a difference
Pausing DOES make a
difference
Longer pauses in chest
compressions = lower
chances of positive outcome
The longer the pause
preceding shock or following
a shock, the lower the
chances of survival
94
95
96
2/16/2017
33
Trauma
Trauma
Assessment to Protocol
Protocol to Treatment
Spinal Immobilization Protocol
CAT Tourniquet
http://www.youtube.com/watch?v=3-WnRUi5UZI
98
99

2/16/2017
34
Medical 1 Breathing Difficulty
Assessment to Protocol Waveform Capnography
Protocol to Treatment
HHN Albuterol
Analyphalxis EMT may give Albuterol- MDI or Nebulized on Standing orders
Only one dose under standing orders
Breathing Difficulty Albuterol (MDI or HHN) x 2 (Standing orders)
Atrovent Breathing Difficulty
Atrovent (HHN) x 1 (standing orders)
CPAP for enhanced/advanced – coming soon
http://www.youtube.com/watch?v=Xre92Ap0vrA
101
102
2/16/2017
35
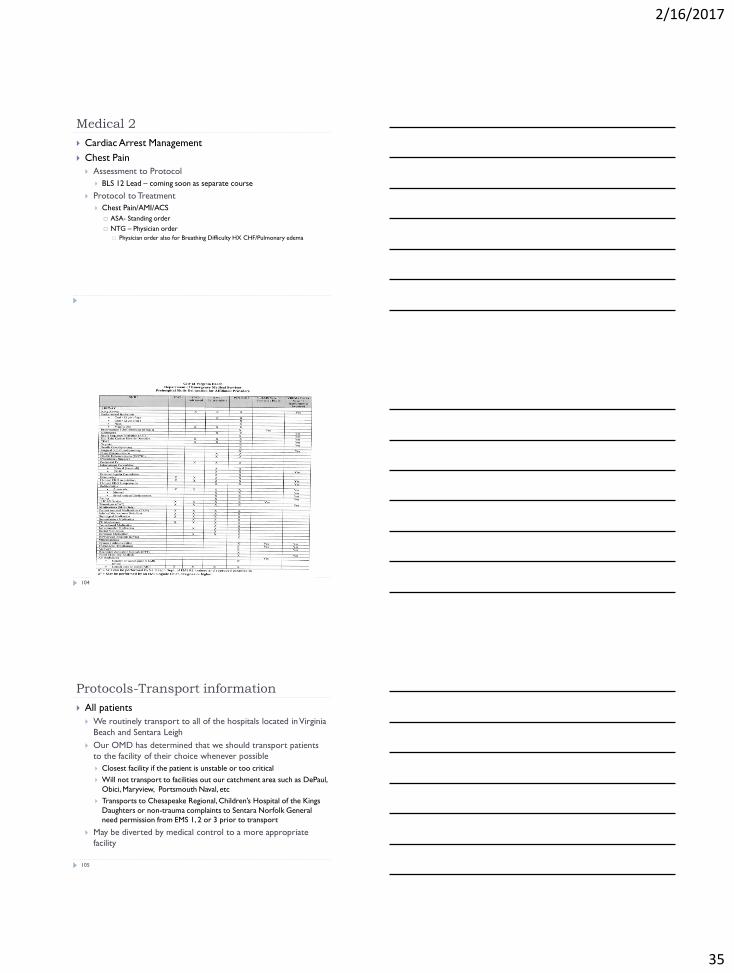
Medical 2
Cardiac Arrest Management
Chest Pain
Assessment to Protocol
BLS 12 Lead – coming soon as separate course
Protocol to Treatment
Chest Pain/AMI/ACS
ASA- Standing order
NTG – Physician order
Physician order also for Breathing Difficulty HX CHF/Pulmonary edema
104
Protocols-Transport information
All patients
We routinely transport to all of the hospitals located in Virginia
Beach and Sentara Leigh
Our OMD has determined that we should transport patients
to the facility of their choice whenever possible
Closest facility if the patient is unstable or too critical
Will not transport to facilities out our catchment area such as DePaul,
Obici, Maryview, Portsmouth Naval, etc
Transports to Chesapeake Regional, Children’s Hospital of the Kings
Daughters or non-trauma complaints to Sentara Norfolk General
need permission from EMS 1, 2 or 3 prior to transport
May be diverted by medical control to a more appropriate
facility
105

2/16/2017
36
Protocols-Transport information (cont)
Trauma patients Trauma centers are Sentara Norfolk General (Level 1) and Sentara
Virginia Beach General (Level 3)
Can transport directly to a trauma center when they meet Trauma center transport criteria
Patients requiring a burn center will go to Norfolk General
Stable pregnant patients greater than 20 weeks should be taken to the Norfolk General trauma center (Unstable and/or less than 20 weeks can start to VBGH—when in doubt, contact Med Control)
Pregnant patients Should be transported to a facility with Labor and Delivery if more
than 20 weeks pregnant
Leigh, Princess Anne and Chesapeake have L& D
Specialty patients Some patients with specialized devices or conditions may require
transport to a specific facility
106
Ongoing Training
VBEMS has both ALS and BLS recertification programs
available throughout the year
Many courses online for annual recertification/refresher
Provide EVOC, CPR, ACLS and PALS on a regular basis
Multiple other sources of training from local hospitals,
TEMS, and other agencies
Contact the EMS Training center for information on
advancing to the next certification level
VBEMS offers specialty courses such
as RSI, extrication, medevac, ITLS
107
How do I get to the next step?
Complete the following to move to Intern status:
1. Complete this course
2. View the Lifepak 15 information
3. Complete Initial OSHA
4. Complete the new member and OSHA quizzes (bring them with you for step 5)
5. Make appointment with EMS Admin to obtain your Intern ID card
At the appointment, you can expect the following:
Review the quizzes
Review the training process
Questions and answers (Bring questions with you!)
Hands-on with Lifepak
Get your Intern ID!
108

2/16/2017
37
I am an Intern! Now what?
Your goal while on strict supervision is:
To demonstrate your ability to function as an EMT intern while
following the policies and protocols established by the City of
Virginia Beach Department of EMS.
That means you need to:
Perform assessments
Provide appropriate patient care
Demonstrate your knowledge of policies, protocols and procedures
Show the ability to drive an ambulance safely in both emergency and
non-emergency modes
Be in charge on calls
Be able to use the radios and computers
Show that you can handle a call “on your own”.
109
Intern process
1. As soon as you are issued your Intern ID, you will need to
submit your dates for scheduling in OSCAR
2. You will run four duties per month (12 hour shifts)
3. An evaluation must be completed for each shift/duty run and
turned in to the BLS Intern Coordinator at Admin
4. Ensure completion of all required courses
ICS-100, 200, 700, 800, EVOC, Hazmat, current CPR and EMT
5. After approximately 3-6 months (12-25 duties) your
internship should be complete or very near completion
6. Be recommended for release and feel comfortable being
released!
110
Links for other courses
Once you have passed the final exam, return to the
course completion page and print your certificate,
and provide a copy of the certificate to EMS Admin.
Hazmat-Terrorism Awareness for Emergency First Responders
[AWR160]-- http://www.teexwmdcampus.com/
ICS-100, 200b, 700, 800b-- http://training.fema.gov/IS/NIMS.asp
111

2/16/2017
38
Definitions
112
There are many terms and abbreviations used in EMS. Here are some that you may find in this document or may hear someone mention.
Admin-EMS Administration office
AIC (Attendant in Charge)-EMT or higher able to be in charge of patient care and calls
ALS-Advanced Life Support
BLS-Basic Life Support
CAD (Computer Aided Dispatch)-system used to send and record 911case information
EMD (Emergency Medical Dispatch)-process for dispatch to prioritize calls
EMR (Electronic Medical Record)-medical record
EMS 1, 2, 3 -EMS supervisor on duty
Entrapment-person can’t be removed from a car, machine, etc without special tools
ERS (Emergency Response System)-coordinated response to emergencies from multiple agencies
FTO (Field Training Officer)-AIC with specific qualifications to help new members progress
Image Trend-Company name of EMR and documentation system
Intern-certified member working on being released
LP (Lifepak 12/15 )-brand of EKG monitor/AED we use
Definitions (cont)
113
MDT (Mobile Data Terminal)-computer in vehicle that communicates with CAD
MRT (Marine Rescue Team)-certified divers and boat operators for water borne incidents
OMD (Operational Medical Director)-Physician who oversees our service
OSCAR-online schedule submission and management program
POV (Personal Operated Vehicle)-private vehicle
Recruit-brand new member who is awaiting class or a certification
Student-member in EMT class
TAC channel-special radio channel assigned for a specific incident
TEMS (Tidewater EMS Council)-our regional EMS council
Toughbook-computer for entering patient care reports
Trainee-non-released member (recruit, student or intern)
Training-EMS Training center
Zone car-sedan or truck that is staffed with an Intermediate or Paramedic
Thank you!
Thank you for joining VBEMS and reviewing the material.
We know this is a lot of information! You can review this
program anytime and we want you to ask questions all
along the way. You will master these items and so many
more in the coming months.
114