aha/hret hen 2.0 falls webinar, finding balance ... · • 2015 ags beers criteria that address...
TRANSCRIPT
August 4, 201611:00 a.m. – 12:00 p.m. CT
AHA/HRET HEN 2.0 FALLS WEBINAR
FINDING BALANCE: PREVENTING MEDICATION RELATED FALLS

WELCOME AND INTRODUCTIONSEmily Koebnick, Program Manager, HRET | 11:00 – 11:05
• Quality of audio (if listening through your computer) depends on your internet connection.
• To maximize the size of any one “pod,” simply press the four-way arrow icon in the top right corner.
ADDITIONAL REMINDERS

AGENDA FOR TODAY11:00-11:05 AM Welcome and Introductions
Open and housekeeping information, including review of relevant HRET HEN resources, change packages and Listserv®.
Emily KoebnickProgram Manager, HRET
11:05-11:10 AM HEN Data Update Topic-specific data update – not limited to national percent reduction and percent reporting.
Rich Rodriguez, MPHData Analyst, HRET
11:10-11:30 AM Finding Balance Through Appropriate Medication Use
Certain medications are commonly implicated is falls, especially in the elderly. Learn about screening tools specifically designed to identify medication related falls risk and explore methodologies to address the risks.
Joseph T. Hanlon, PharmD, MSProfessor, Department of Medicine (Geriatrics), University of PittsburghHealth Scientist, Pittsburgh VAHS
11:30-11:45 AM Hospital StoriesHospitals will share how they developed an interprofessional approach that engages all departments in fall prevention.
Ruth Zimmerman, RN, MSN, CPPSPatient Safety ManagerSummit Health Care Regional Medical Center
11:45-11:55 AM Discussion and ReflectionFacilitated discussion with the presenters and nurse reactor. Patricia Ducklow, MSN, CNS
Acute Care Clinical Nurse Specialist,Memorial Hospital Jackie Conrad RN MBAImprovement Advisor, Cynosure
11:55 AM-12:00 PM Bring it HomeAction items and tying together of didactic, hospital-level and improvement science information.
Emily KoebnickProgram Manager, HRET

• Falls With Injury driver diagrams and change ideas
• Adverse Event Area definition and scope
• Example PDSA cycles• Descriptions and guidance
on how to use change package effectively
• Referenced appendices
ChaFALLS WITH INJURY CHANGE PACKAGE
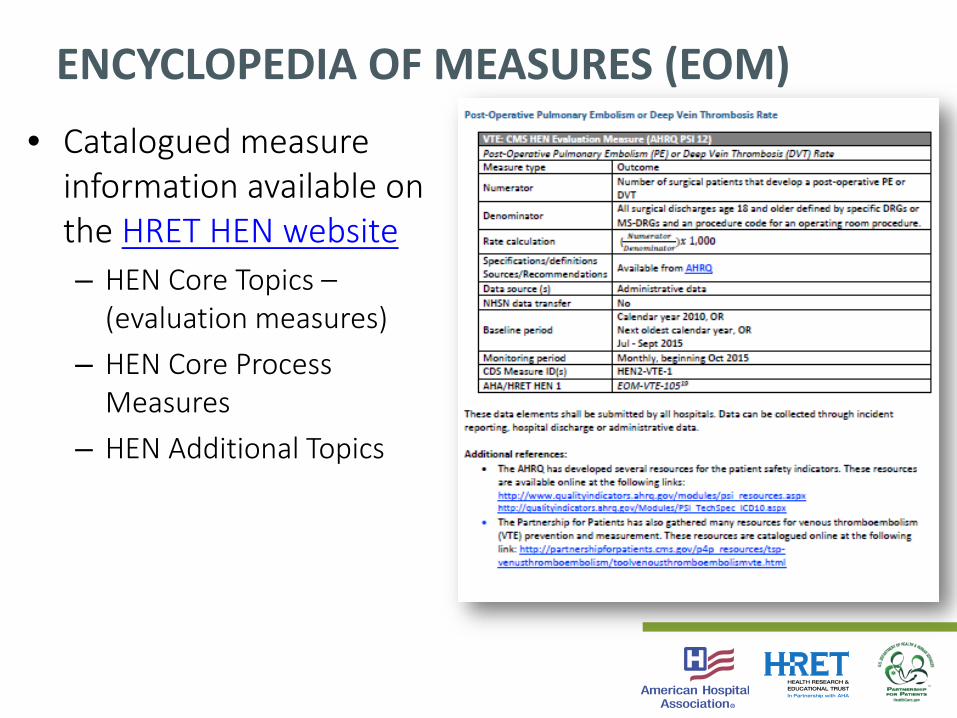
ENCYCLOPEDIA OF MEASURES (EOM)• Catalogued measure
information available on the HRET HEN website– HEN Core Topics –
(evaluation measures)– HEN Core Process
Measures– HEN Additional Topics
• Falls Analytics Listserv® is available for:– Sharing of:
• HRET Resources• Publically Available Resources• Best Practices• Learnings from Subject Matter Experts
– Troubleshooting for Data Reporting and Analysis
SIGN UP TODAY: FALLS LISTSERV®
Sign Up Here

HEN DATA UPDATERich Rodriguez, Data Analyst, HRET | 11:05 – 11:10
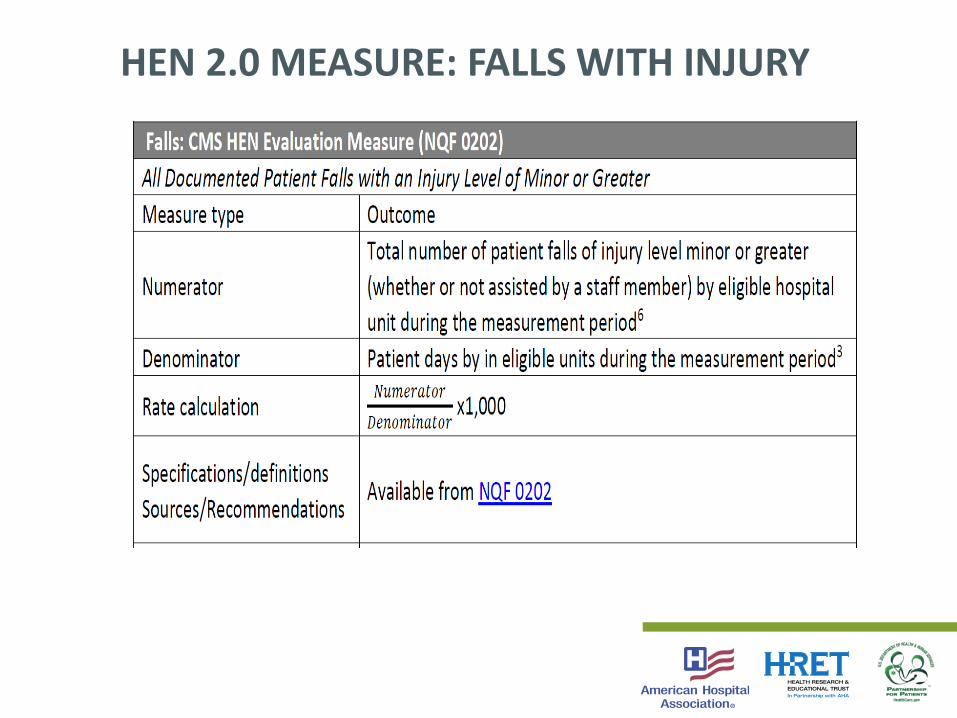
HEN 2.0 MEASURE: FALLS WITH INJURY
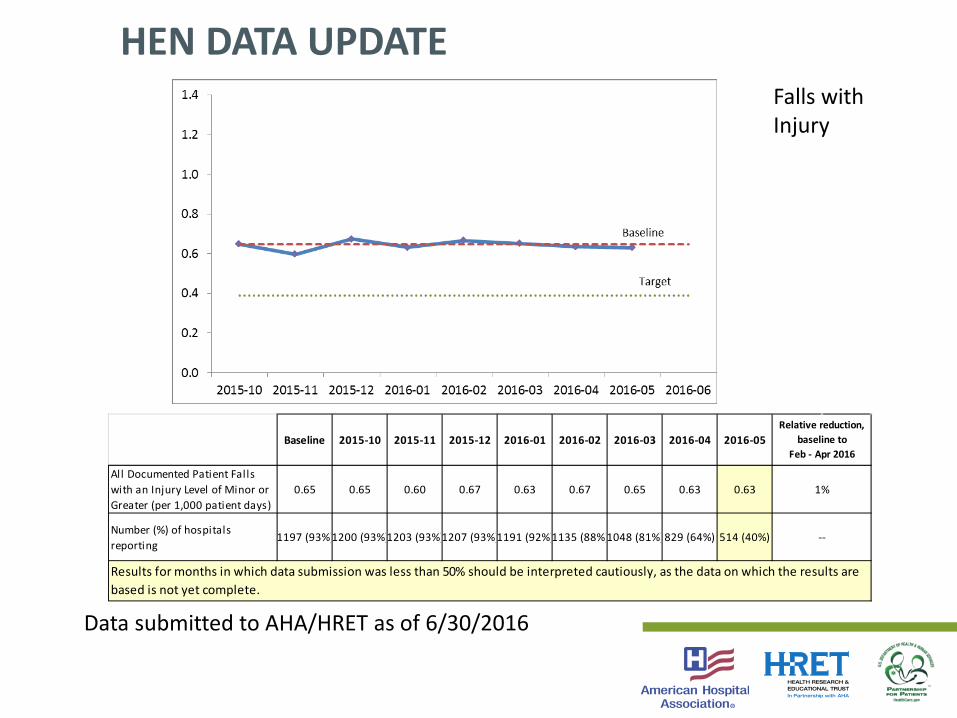
HEN DATA UPDATE
Baseline 2015-10 2015-11 2015-12 2016-01 2016-02 2016-03 2016-04 2016-05
All Documented Patient Falls with an Injury Level of Minor or Greater (per 1,000 patient days)
0.65 0.65 0.60 0.67 0.63 0.67 0.65 0.63 0.63
Number (%) of hospitals reporting
1197 (93%)1200 (93%)1203 (93%)1207 (93%)1191 (92%)1135 (88%)1048 (81%)829 (64%) 514 (40%)
Relative reduction, baseline to
Feb - Apr 2016
1%
--
Results for months in which data submission was less than 50% should be interpreted cautiously, as the data on which the results are based is not yet complete.
Data submitted to AHA/HRET as of 6/30/2016
Falls with Injury

FINDING BALANCE THROUGH APPROPRIATE MEDICATION USEJoseph T. Hanlon, PharmD, MS, Professor Department ofMedicine (Geriatrics), University of Pittsburgh | 11:10 – 11:30

TOPICS TO DISCUSS
• 2015 AGS Beers Criteria that address drug-induced falls/fractures
• Newer evidence about the risk of skeletal muscle relaxants (SMRs), Serotonin-norepinephrine reuptake inhibitors (SNRIs) and combined central nervous system (CNS) dosage and falls/fractures
• Evidence-based/practical interventions that can reduce drug-induced falls/fractures

LIST OF ABBREVIATIONSCI Confidence interval
OR Odds radio
TCA tricyclic antidepressants
SSRIs selective serotonin reuptake inhibitor
RR Relative risk
IRR Incident rate ratios
Mg Milligram
AEDs Antiepileptic drugs
DRR drug regimen review
FORTA criteria Fit for the ages
PIP Potentially inappropriate prescribing
Fs Functional status
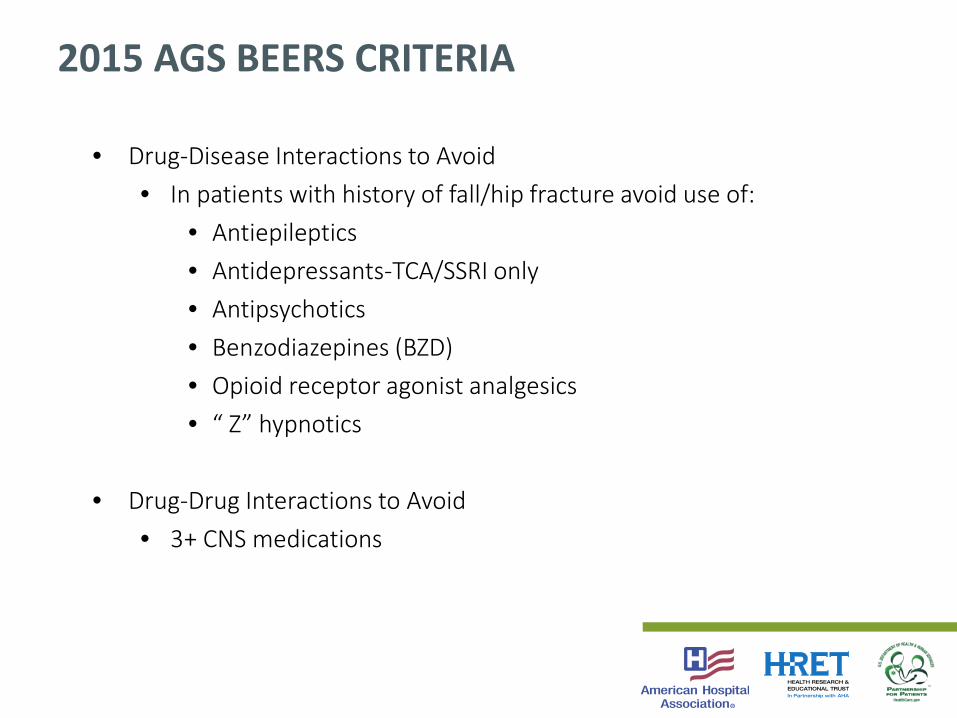
2015 AGS BEERS CRITERIA
• Drug-Disease Interactions to Avoid• In patients with history of fall/hip fracture avoid use of:
• Antiepileptics • Antidepressants-TCA/SSRI only• Antipsychotics• Benzodiazepines (BZD)• Opioid receptor agonist analgesics• “ Z” hypnotics
• Drug-Drug Interactions to Avoid• 3+ CNS medications

META-ANALYSES: 9 DRUG CLASSES AND FALLS
• Increased risk with CNS medications:
– SSRIs/TCAs (9 studies OR 1.68)
– Antipsychotics (5 studies OR 1.59)
– BZDs (11 studies OR 1.57)
– Sedative/hypnotics (7 studies OR 1.47)
Woolcott JC, et al. Arch Int Med 2009; 169:1952-60.
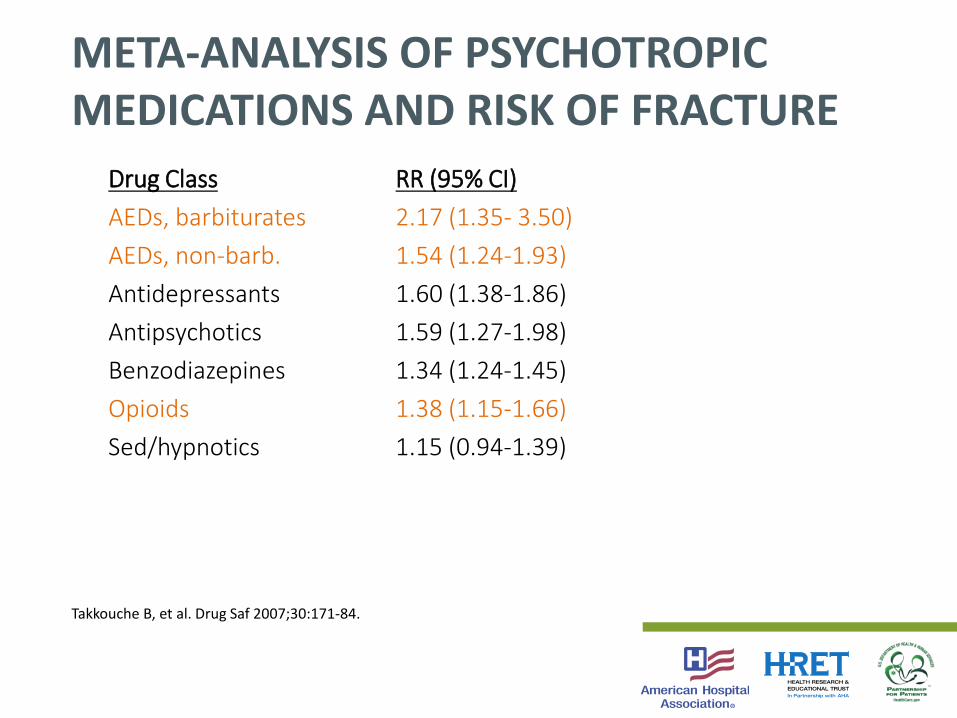
META-ANALYSIS OF PSYCHOTROPIC MEDICATIONS AND RISK OF FRACTURE
Drug Class RR (95% CI)AEDs, barbiturates 2.17 (1.35- 3.50)AEDs, non-barb. 1.54 (1.24-1.93)Antidepressants 1.60 (1.38-1.86)Antipsychotics 1.59 (1.27-1.98)Benzodiazepines 1.34 (1.24-1.45)Opioids 1.38 (1.15-1.66)Sed/hypnotics 1.15 (0.94-1.39)
Takkouche B, et al. Drug Saf 2007;30:171-84.

ZOLPIDEM USE AND HIP FRACTURES IN ELDERS
Objectives: Determine if zolpidem is a safer alternative to benzodiazepines
Results: Zolpidem ↑ risk (OR 1.95; 95% CI 1.09-3.51)
BZDs ↑ risk (OR 1.46; 95%CI 1.21-1.76)
Conclusion: Zolpidem should be used with caution in older adults
Wang PS, et al. JAGS 2001;49:1685-1690.
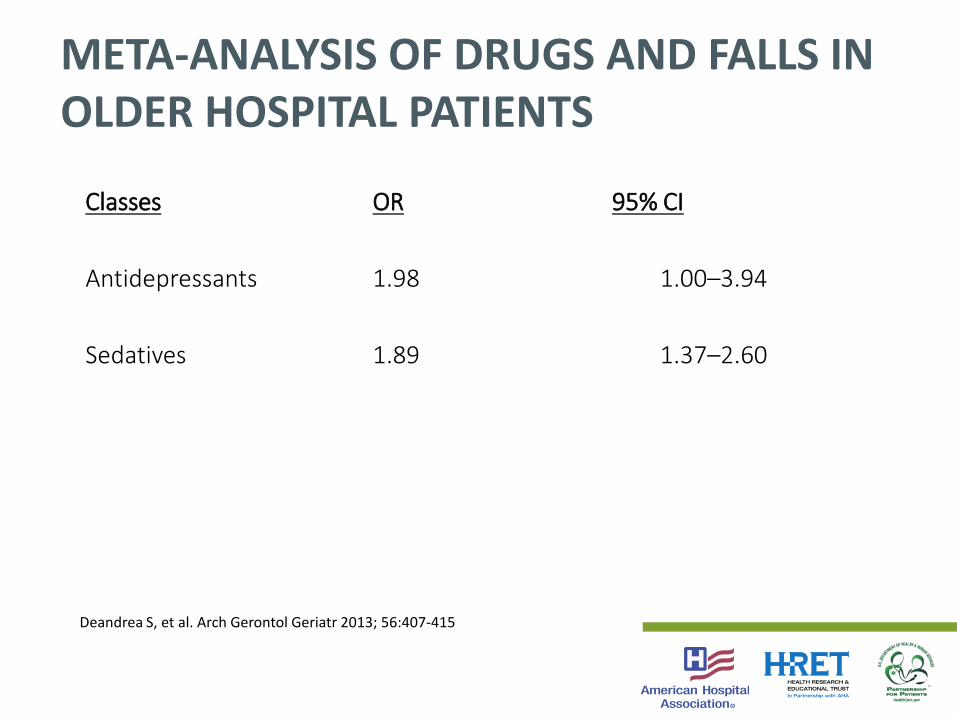
Classes OR 95% CI
Antidepressants 1.98 1.00–3.94
Sedatives 1.89 1.37–2.60
META-ANALYSIS OF DRUGS AND FALLS IN OLDER HOSPITAL PATIENTS
Deandrea S, et al. Arch Gerontol Geriatr 2013; 56:407-415

CNS POLYPHARMACY AND FALLS IN OLDER OUTPATIENT VETERANS
11.54
2.37
0
1
2
3
4
5A
djus
ted
odds
rat
io
0 1 >2CNS - active medications (n)
Weiner D, et al. Gerontol 1998;44:217-21.

CNS MEDICATION POLYPHARMACY AND RISK OF RECURRENT FALLS IN ELDERLY
CNS Medication Use Adjusted OR (95% Cl)
Use of 2+ agents 1.95 (1.35–2.81)
Use of 1 agent 1.55 (1.22–1.97)
Hanlon JT, et al. J Gerontol 2009; 64A(No.4):492-498

MULTIPLE PSYCHOACTIVE MEDICATIONS AND HOSPITALIZATION FOR FALLS
Design: Cohort study
Data: Australian Government Department of Veterans’ Affairs claims
Patients: 73,690 aged 65+
Results: ↑ incident rate ratios (IRRs) with ↑ psychoactive medicines (one-IRR 1.22 [(95 % CI 1.08–1.38]; two-IRR 1.70 [(95 % CI 1.45–1.99]; 3-4-IRR 1.96 [95 % CI 1.58–2.43]; 5+- IRR 3.15 [95 % CI 1.90–5.23]
Pratt NL et al. Drug Saf, 2014; 37:529-35.

TOPICS TO DISCUSS
• 2015 AGS Beers Criteria that address drug-induced falls/fractures
• Newer evidence about the risk of SMRs, SNRIs and combined CNS dosage and falls/fx
• Evidence-based/practical interventions that can reduce drug-induced falls/fractures
SMRS AND SNRI USE & ↑ RISK OF FALLS/FXS
• Alvarez CA, et al. Association of skeletal muscle relaxers and antihistamines on mortality, hospitalizations, and emergency department visits in elderly patients: a nationwide retrospective cohort study. BMC Geriatrics 2015;15:2.
• Coupland CA, et al. A study of the safety and harms of antidepressant drugs for older people: a cohort study using a large primary care database. Health Technol Assess 2011;15:1-202iii-iv.
• Gribbin J, et al. Serotonin-norepinephrine reuptake inhibitor antidepressants and the risk of falls in older people: case–control and case-series analysis of a large UK primary care database. Drugs Aging 2011;28:895-902.
• Lanteigne A, et al. Serotonin–norepinephrine reuptake inhibitor and selective serotonin reuptake inhibitor use and risk of fractures: a new-user cohort study among US adults aged 50 years and older. CNS Drugs 2015;28:79-88.
• Wang CY, et al. Serotonergic antidepressant use and the risk of fracture: a population-based nested case-control study. Osteoporos Int 2016;27:57-63.
CNS MEDICATION DOSAGE AND FALLS
Design: Longitudinal
Data: Health Aging Body Composition study
IV: 3+ Standardized Daily Doses (sdd) of BZD, Antidepressants, Antipsychotics, and Opioids
Outcome: 2+ falls in previous 12 months
Hanlon JT, et al. J Gerontol 2009; 64A(No.4):492-498.
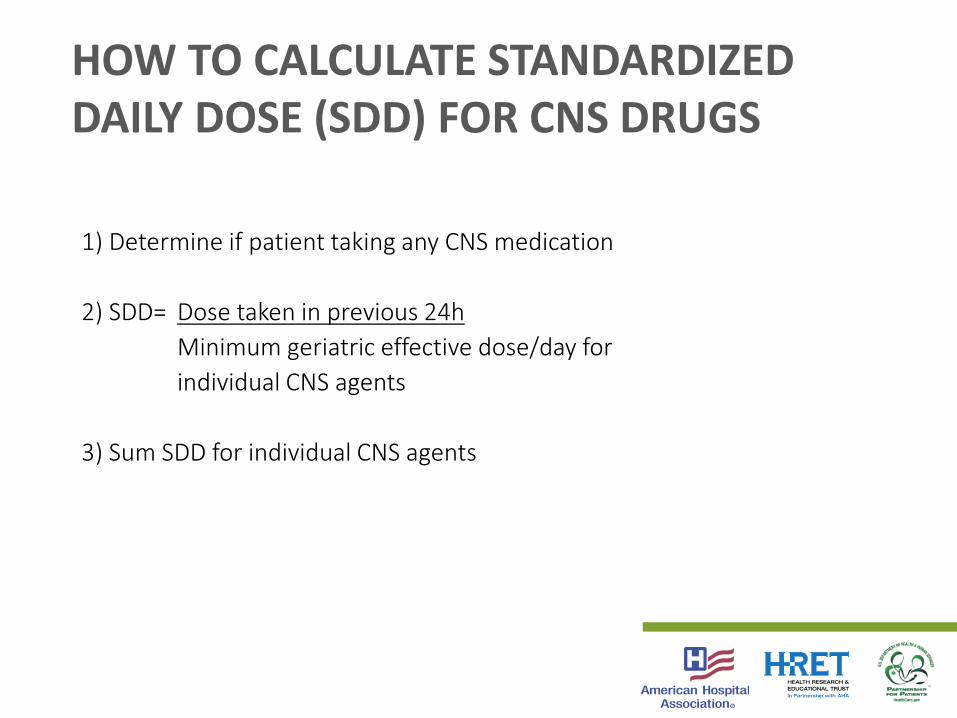
HOW TO CALCULATE STANDARDIZED DAILY DOSE (SDD) FOR CNS DRUGS
1) Determine if patient taking any CNS medication
2) SDD= Dose taken in previous 24hMinimum geriatric effective dose/day for individual CNS agents
3) Sum SDD for individual CNS agents

• Patient taking diazepam 5mg 3x/day and amitriptyline 50mg at bedtime• Diazepam minimum effective geriatric dose per day is 4mg• Amitriptyline minimum effective dose per day is 10 mg• Diazepam SDD— 15mg/4mg = 3.75• Amitriptyline SDD— 50mg/10mg = 5• Patient's total SDD = 8.75; total SDD >3 increases risk of falls/fractures
EXAMPLE OF CALCULATION OF CNS SDDS

CNS MEDICATION DOSAGE AND RISK OF RECURRENT FALLS IN ELDERLY PERSONS
Hanlon JT, et al. J Gerontol 2009; 64A(No.4):492-498.
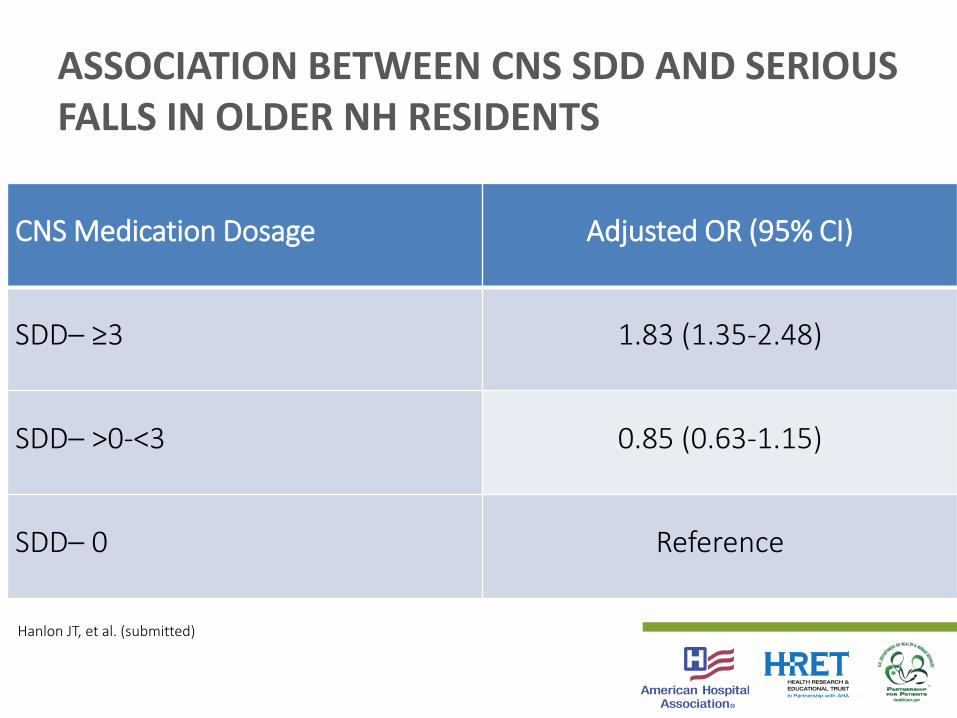
ASSOCIATION BETWEEN CNS SDD AND SERIOUS FALLS IN OLDER NH RESIDENTS
CNS Medication Dosage Adjusted OR (95% CI)
SDD– ≥3 1.83 (1.35-2.48)
SDD– >0-<3 0.85 (0.63-1.15)
SDD– 0 Reference
Hanlon JT, et al. (submitted)

OTHER POSITIVE STUDIES SUGGESTING A CNS DOSE-RESPONSE RELATIONSHIP
• Sterke CS, et al. New insights: dose-response relationship between psychotropic drugs and falls: a study in nursing home residents with dementia. J Clin Pharmacol 2012;52:947-55.
• Wilson NM, et al. Associations between drug burden index and falls in older people in residential aged care. J Am Geriatr Soc 2011;59:875–880.

TOPICS TO DISCUSS
• 2015 AGS Beers Criteria that address drug-induced falls/fractures
• Newer evidence about the risk of standardized mortality ratios (SMR), SNRIs and combined CNS dosage and falls/fx
• Evidence-based/practical interventions that can reduce drug-induced falls/fractures

INTERVENTIONS DESIGNED TO IMPROVE SUBOPTIMAL PRESCRIBING AND REDUCE FALLS IN OLDER PTS
Methods: Identify systematic reviews of literature through 7/2016
Data Synthesis: 13 studies identified; 7 had ↓ risk of falls;Only one conducted in hospital
Iyer S. Drugs Aging 2008; Hill KD. Drugs Aging 2012; :29:1530;Patterson SM. Cochrane Rev 2012; CD008165; Tjia J. Drugs Aging 2013;30:285-307; Alldred DP. Cochrane Syst Rev 2013; CD009095; Coon JT. JAMDA 2014;15: 706–718; Salahudeen MS. Drugs Aging 2014;31:185-192; Gould RL. Br J Psych 2014;204:98-107.

RCTS DESIGNED TO ↓ FALLS AS SECONDARY OUTCOME IN OLDER ADULTS
Author/Year Intervention Sample Results
Crotty/ 2004
NH RPh. transit. coordinator
715 pts ↓ MAI;↓ hosp. use; ↔ADEs, Falls
Zermansky/2006
NH RPh. DRR 661 pts ↓ # drugs &falls; ↔ hospital use
Pit/2007
Clinic ed., assess med risk, feedback
20 MDs-749 pts
↑ med quality, ↓ falls ↔ Qol scores
Patterson/ 2010
NH RPh DRR 334 pts in22 NH
↓ inappropriate psycho-active meds; ↔ falls
Frankenthal/ 2014
NH RPh DRRusing STOPPcriteria
359 pts ↓ PIP, ↓ falls, ↔ FS, Qol, orhospitalizations
Michalek/2014
DRR withFORTA, MDfeedback
114 hosp pts ↓ PIP, ↓ falls↔ FS

PREVENTING DRUG-INDUCED FALLS/FXS IN OLDER ADULTS
• Educate patients/caregivers about potential risks of meds
• Use non-pharmacological approaches
• Do not initiate new prescribing of BZD receptor agonists, or SMRs
• Reduce dose of CNS agents to decrease total medication risk burden especially those at high risk (e.g., history of falls, cognitive impairment, depression)
• Taper d/c medication slowly over 4-8 weeks; exceptions are AEDs and BZDs which may require 6-12 months
SUMMARY
• 2015 AGS Beers Criteria that address drug-induced falls/fractures
• Newer evidence about the risk of SMRs, SNRIs and combined CNS dosage and falls/fx
• Evidence-based/practical interventions that can reduce drug-induced falls/fractures

HOSPITAL STORY: SUMMIT HEALTH CARE REGIONAL
Ruth Zimmerman, RN, MSN, CPPS, Patient Safety Manager | 11:30 – 11:45

38
SUMMIT HEALTHCARE REGIONAL MEDICAL CENTER
SHOW LOW, AZ
Insert a photo of your hospital and logo
here.
Jayne Simms, RN, MSN—M/S 2 DirectorCarolyn Jacobs, RN, MS, CPHQ—CQO
Daran Wilson, RN—M/S 1 DirectorNot pictured:
Stephanie Arellano, RNC—Quality Management Nurse Reviewer Ruth Zimmerman, RN, MSN, CPPS—Patient Safety Manager

We are a not-for-profit rural healthcare organization serving the White Mountains of Arizona since 1970. Our 89-bed hospital includes a 32-bed Emergency Department, Level II Nursery, 12-bed ICU, medical/surgical, and telemetry units, cardiac catheterization lab, Perioperative Services including a 4-suite OR, hybrid room, and special procedures rooms. We also have a strong presence in the community via outpatient clinics, physician offices, and various outreach programs.
39
ABOUT SUMMIT HEALTHCARE
2003 Restraints on general medical units were eliminated Fall rate was to 5/1000 patient days Targeted to decrease number of patient falls and the severity of
injury resulting from them Q1 2011 to Q4 2013
Fall rates sustained at <2.5 falls/1000 patient days with zero major injuries
Q1–Q2 2014 Fall rates spiked to >3/1000 patient days Major injuries (fractures) as high as 0.6/1000 patient days
40
PROJECT BACKGROUND AND GOALS
We recognized a need to address drift behavior on the part of staff Focus:
Leading circumstance surrounding falls (toileting) Develop a means of communicating patients’ fall risk house-wide
41
GETTING BACK ON COURSE
“Zero” is an attainable goal
Not just a nursing issue and not only on nursing units
House-wide effort involving all employees, clinical and non-clinical, as well as Security and Volunteer Services
Communicate liberally throughout the organization
Education—patients, families, staff, providers
All patients are at least a moderate risk
Leverage technology
42
STRATEGIES

Yellow arm bands, non-slip socks Falling Star program Gait belts in every room Bed and chair alarms Stryker I-Bed features White boards, hourly rounding, scripted language All patients at least moderate risk Monthly Fall Team meeting co-run by Med Surg directors Staff required to stay in room while patient in bathroom Standardized fall risk assessment at least once per shift Bromage scale post-spinal/epidural (OB) Periodic Fall Prevention policy and guideline revisions
43
MEASURES IN PLACE
Therapy Services, Diagnostic Imaging, ED Director, and invited guests added to Fall Team
Monthly fall stats posted on each unit with “photos” of “patients” PT/OT eval for strength, mobility, balance and to educate staff Orthostatic BP at least once per shift for high risk patients Patient/family education to “Call, don’t fall” Yellow gowns for patients at high risk Sitters as available Change of shift SBAR revised to include fall risk Post-Fall Huddle with notification of Director at time of fall EHR prompt to reassess at intervals post-fall Staff on units must stay in room with patient and be able to visualize
feet in bathroom
44
MEASURES ADDED
45
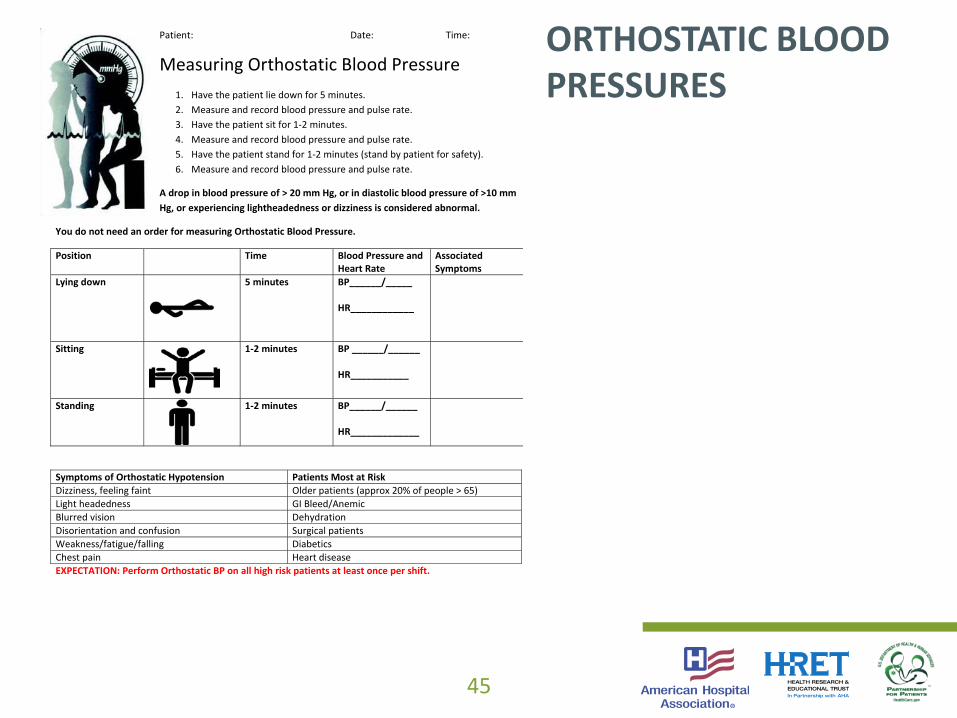
ORTHOSTATIC BLOOD PRESSURES
Patient: Date: Time:
Measuring Orthostatic Blood Pressure 1. Have the patient lie down for 5 minutes. 2. Measure and record blood pressure and pulse rate. 3. Have the patient sit for 1-2 minutes. 4. Measure and record blood pressure and pulse rate. 5. Have the patient stand for 1-2 minutes (stand by patient for safety). 6. Measure and record blood pressure and pulse rate.
A drop in blood pressure of > 20 mm Hg, or in diastolic blood pressure of >10 mm Hg, or experiencing lightheadedness or dizziness is considered abnormal.
You do not need an order for measuring Orthostatic Blood Pressure.
Position Time Blood Pressure and Heart Rate
Associated Symptoms
Lying down
5 minutes BP______/_____ HR____________
Sitting
1-2 minutes BP ______/______ HR___________
Standing
1-2 minutes BP______/______ HR_____________
Symptoms of Orthostatic Hypotension Patients Most at Risk Dizziness, feeling faint Older patients (approx 20% of people > 65) Light headedness GI Bleed/Anemic Blurred vision Dehydration Disorientation and confusion Surgical patients Weakness/fatigue/falling Diabetics Chest pain Heart disease EXPECTATION: Perform Orthostatic BP on all high risk patients at least once per shift.

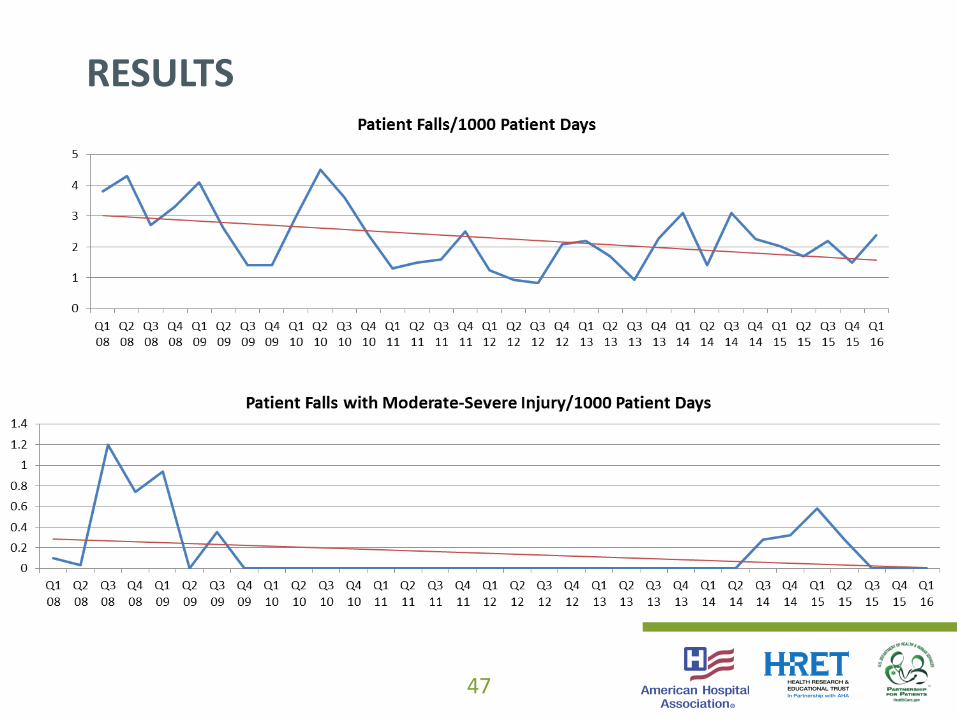
Although slower to address the increase in falls and injuries than we had hoped, the Fall Team has maintained an active role
Housekeepers and other non-clinical staff are reporting hazards Security staff monitor for patients in yellow gowns ambulating off the
nursing units, in walking rounds and via security cameras, intervene as necessary to return the patients to their rooms
Although initially reluctant to remain in the bathroom during toileting, staff will remain in the room and visualize the feet as a first clue when the patient moves toward standing
No patient has suffered a moderate to severe injury since Q2 2015
46
RESULTS
47
RESULTS

The journey does not end! We are continually evaluating falls/near misses for trends in type,
location, patient demographics, impact of staffing (numbers/skill mix/experience level)
Involve staff from as many disciplines as possible in developing the plan
Allow staff the ability to tailor interventions to patient needs Don’t be afraid to “put your foot down” on non-negotiables (in our
case, staying in the room during toileting) Empower ALL employees in preventing falls, and be sure to educate
every new employee who joins the organization
48
LESSONS LEARNED
Yellow gowns: one size fits most, inconsistent stocking between units Patients remaining in yellow gowns after they are no longer a risk Patients in yellow gowns ambulating independently off units (may or
may not still be a fall risk) Fall risk communication for ED patients impacted by triage process ED fall rates have been going up
49
BARRIERS AND CHALLENGES
Going forward, need to assess use of high-risk medications more fully How to communicate fall risk among different EMRs that don’t
interface with each other (Peri-Birth, McKesson/Paragon, T-System)
50
NEXT STEPS

DISCUSSION AND REFLECTIONPatricia Ducklow, MSN, CNS, Acute Care Clinical Nurse Specialist Memorial Hospital | 11:45 – 11:55

BRING IT HOMEEmily Koebnick, Program Manager, HRET| 11:50 – 11:55

What are you going to do by next Tuesday? Assess Standard Daily Dosing for CNS agents for elderly patients Utilize Beers criteria for prescribing new medications and evaluating
existing medications
What are you going to do in the next month? Work with pharmacy leadership to evaluate medication reconciliation
processes to assure fall risk increasing drugs are evaluated for discontinuation or tapering
PHYSICIAN LEADER ACTION ITEMS
What are you going to do by next Tuesday? Work with pharmacy staff to audit 5 medication records of patients
>65 to assess medication ordering practices Invite pharmacy to join the falls team
What are you going to do in the next month? Establish a process for triggering a medication review for fall risk
increasing drugs on high risk patients Include pharmacy in the post-fall review process
UNIT-BASED TEAM ACTION ITEMS

What are you going to do by next Tuesday? Assess clinical pharmacist resources for medication review for fall risk
increasing drugs on elderly patients
What are you going to do in the next month? Support clinical pharmacist’s building medication reconciliation into
work flow for high-risk patients Explore pharmacist availability in the community for medication
reconciliation post-discharge
HOSPITAL LEADERS ACTION ITEMS
What are you going to do by next Tuesday? Review patient education resources for medication side effects
What are you going to do in the next month? Develop a simple medication education resource to help patients
understand how medications can contribute to fall risk
PFE LEADS ACTION ITEMS

HRET/HEN 2.0 CAUTI WebinarAugust 9 | 11:00 a.m. – 12:00 p.m. CT
HRET/HEN 2.0 HAPU WebinarAugust 18 | 11:00 a.m. – 12:00 p.m. CT
HRET/HEN 2.0 Readmissions WebinarAugust 23 | 11:00 a.m. – 12:00 p.m. CT
View all upcoming events
UPCOMING WEBINARS

Find more information on our website: www.hret-hen.org
Questions/Comments: [email protected]
THANK YOU!