aha medical/scientific statement specialcirc.ahajournals.org/content/90/4/2180.full.pdf · upper...
TRANSCRIPT

2180
AHA Medical/Scientific StatementSpecial Report
Guidelines for Evaluation and Management ofCommon Congenital Cardiac Problems in
Infants, Children, and AdolescentsA Statement for Healthcare Professionals
From the Committee on Congenital Cardiac Defects ofthe Council on Cardiovascular Disease in the Young,
American Heart Association
David Driscoll, MD, Chair; Hugh D. Allen, MD; Dianne L. Atkins, MD; Joel Brenner, MD;Ann Dunnigan, MD; Wayne Franklin, MD; Howard P. Gutgesell, MD; Paul Herndon, MD;
Robert E. Shaddy, MD; Kathryn A. Taubert, PhD; Kenneth Zahka, MD, Members;Arthur Garson, Jr, MD; David J. Skorton, MD; Gordon K. Danielson, MD, Consultants
Appropriate use of diagnostic and therapeutictechniques is important to ensure optimumand efficient treatment of patients in a cost-
effective manner. Ideally, guidelines for appropriate,cost-effective care of patients should be based on out-come studies of management strategies. In the absenceof reliable outcome studies, the conventional wisdom ofexperienced pediatric cardiologists can be used to de-velop guidelines. However, such guidelines must besubjected to review when outcome studies becomeavailable. In addition, the guidelines should change asdiagnostic and therapeutic technologies change.Approximately 50 years of experience in evaluation of
patients with congenital cardiac defects has accumu-lated. Outcome analyses are now available for severalconditions and defects, and others are being published.Knowledge of pediatric cardiology is sufficient to allowthe development of diagnostic and treatment guidelinesfor relatively simple but common problems. Recogniz-ing that critical analysis of diagnostic and treatmentpractices improves patient care and could reduce thecost of medical care, the Committee on CongenitalCardiac Defects of the American Heart AssociationCouncil on Cardiovascular Disease in the Young devel-oped the following sets of management and treatmentguidelines.These guidelines are designed for use by board-
eligible/certified pediatric cardiologists (hereafter re-ferred to as pediatric cardiologists) and others who havea specialized cognitive knowledge of the clinical and
"Guidelines for Evaluation and Management of Common Con-genital Cardiac Problems in Infants, Children, and Adolescents"was approved by the American Heart Association SAC/SteeringCommittee on June 16, 1994.
Requests for reprints should be sent to Kathryn A. Taubert,PhD, Office of Scientific Affairs, American Heart Association,7272 Greenville Avenue, Dallas, TX 75231-4596.C 1994 American Heart Association, Inc.
natural history of congenital heart defects. Patients forwhom these guidelines have been designed should bescreened before referral to a pediatric cardiologist. Thisstatement represents recommended guidelines to sup-plement practitioners in their clinical judgment and isnot intended as a standard of care for all cases.These guidelines are restricted to relatively simple,
uncomplicated problems in infants, children, and ad-olescents. This is because 1) there are more patientswith these problems than those with complex defects,and 2) the diversity of the natural history and diag-nostic and therapeutic problems associated with com-plex defects preclude development of widely applica-ble useful guidelines.The following guidelines are the consensus of com-
mittee members and consultants to the committeeguided by results of published outcome studies or, whennot available, by current practice patterns.
Construction of AlgorithmsThe algorithms were constructed over 3 years during
several meetings of the Committee on Congenital Car-diac Defects of the Council on Cardiovascular Diseasein the Young. Ten board-certified pediatric cardiolo-gists and Kathryn Taubert, PhD, senior science consult-ant at the AHA, were members of the committee duringthe construction of these algorithms. One of the 10cardiologists, Howard Gutgesell, MD, represented thecardiology subsection of the American Academy ofPediatrics. Another pediatric cardiologist, Arthur Gar-son, Jr, MD, represented the American College ofCardiology. Input was also obtained from a cardiovas-cular surgeon, Gordon Danielson, MD, and an internistcardiologist, David Skorton, MD.The algorithms were reviewed and approved by the
appropriate scientific committees of the AHA.
by guest on May 17, 2018
http://circ.ahajournals.org/D
ownloaded from

AIIA Council on CVDY Guidelines for Pediatric Congenital Cardiac Problems
History and exarnTime O (ECG and cheat radiogram, clas 11)
Abnormal ECGTypical physical and/or chest x-ray Atypical findingsfindings of anInnocent murmur Optio yNNpoo
Echo 4 ECG +1- chest x-ray
Abnormal Norrnal _
Off Abnormal Nomal
No further cardiacevaluation
FIG 1. Algorithm for asymptomatic child with a cardiac murmur.ECG indicates electrocardiogram.
Classification of Testing ProceduresClass I: Conditions for which (or patients for whom)
there is general agreement that a specific evaluation or
test is useful and reliable. In this report, all evaluations,procedures, and tests are Class I unless stated otherwise.
Class II: Conditions for which (or patients for whom)there is a divergence of opinion with respect to theusefulness of an evaluation or test.
Definition of Defects, Exclusion Criteria, andAnnotation of Algorithms
Asymptomatic Child with a Systolic Murmur("Innocent Murmurs of Childhood") (Fig 1)Exclusion Criteria
1. The patient is 2 years old or younger.
2. The patient is symptomatic.3. The patient is uncooperative during the examination.
Definition of Type ofMurmurs1. Still's murmur: a low-frequency systolic murmur
less than or equal to grade 3/6 in intensity; heard bestalong left sternal border; normal second heart sound; noclick; no diastolic murmur.
2. Pulmonic flow murmur: a mid-frequency murmur
less than or equal to grade 3/6 in intensity; heard best atupper left sternal border; normal second heart sound;no click; no diastolic murmur.
3. Venous hum: a high-frequency murmur of grade3/6 or less in intensity; best heard in sitting or standingposition; best heard at base of the neck or the infraclav-icular or supraclavicular area; normal second heartsound; systolic and/or diastolic in timing; abolished bycompression of jugular vein, change of head position, or
assumption of supine position.4. Carotid bruit: grade 3/6 or less in intensity; heard
over carotid artery; no associated precordial ejectionclick; no clinical evidence for aortic stenosis; no diastolicmurmur; normal second heart sound.
Algorithm for Asymptomatic Child With a
Systolic MurmurThis algorithm is intended to address the evaluation of
the innocent murmur of childhood. Since "Time 0" is theinitial evaluation by a pediatric cardiologist, the murmurwill not have been classified as innocent. Hence, thealgorithm is directed at the evaluation of a systolic mur-
Time 0 History, exam, ECG, echo, chest x-rayOption2 ~~~1,>,_4
Time 0+0-12 months
Option 1
History and exam
Typical findings Atypical findings
Echo
PDA foundo/\ ;*DX other th
0 Close PDA(preoperativeecho, class 11) OfT pro
han PDA
)tocol
Time: Postoperative History and exam (chest x-ray, ECGoutpatient if not done postoperatively in hospital;visit echo class 11)
Normal Abnormal
No further Off protocolcardiacevaluation
FIG 2. Algorithm for patent ductus arteriosus in a patientyounger than 6 months. History, physical examination, chestradiogram, electrocardiogram, and echocardiographic studieswill be performed in postoperative period before patient hasentered postoperative phase of this protocol. It is assumed thatdocumentation of resolution of all perioperative problems suchas pleural and pericardial effusion or postoperative woundinfections will be obtained before patient is enrolled in thisprotocol. ECG indicates electrocardiogram; PDA, patent ductusarteriosus; DX, diagnosis.
mur in an asymptomatic child 2 years of age or older.While many pediatric cardiologists are comfortable diag-nosing an innocent murmur on the basis of the history andphysical examination alone, some pediatric cardiologistsobtain a chest radiogram and/or electrocardiogram. Thus,an ECG and a chest radiogram have been designated asClass II tests at the time of the initial evaluation. Becausethere are cases for which the history and physical findingsare atypical for an innocent murmur, the algorithm pro-vides for echocardiography* in selected cases. Once amurmur is determined to be innocent, further cardiacevaluation is unnecessary.
Patent Ductus Arteriosus (Figs 2 and 3)Exclusion Criteria
1. The patient has associated cardiovascular anomalies.2. The patient has symptoms or signs of congestive
heart failure.3. The patient was born prematurely.4. The patient has pulmonary vascular obstructive
disease.
Algorithms for Patent Ductus ArteriosusTwo algorithms are provided for the management of
patent ductus arteriosus. For the first, "Time 0" is the
*An echocardiogram is a two-dimensional study with Dopplerand color flow evaluation used at the discretion of the examiningpediatric echocardiographer. It is assumed that all echocardio-grams will be performed by, or by someone directly responsible to,a pediatric cardiologist with expertise in the echocardiographicevaluation of children and patients with congenital heart disease.
2181
by guest on May 17, 2018
http://circ.ahajournals.org/D
ownloaded from

2182 Circulation Vol 90, No 4 October 1994
Time O History and exam,ECG, echo, chest x-ray
Close PDA
Time: Postoperative History and exam (chest x-ray, ECGoutpatient if not done postoperatively in hospital;visit echo, class 11)
Normal Abnormal
No further Off protocolcardiacevaluation
FIG 3. Algorithm for patent ductus arteriosus in a patient olderthan 6 months. History, physical examination, chest radiogram,electrocardiogram, and echocardiographic studies will be per-formed in postoperative period before patient has entered postop-erative phase of this protocol. It is assumed that documentation ofresolution of all perioperative problems such as pleural and peri-cardial effusion or postoperative wound infections will be obtainedbefore patient is enrolled in this protocol. ECG indicates electro-cardiogram; PDA, patent ductus arteriosus.
initial evaluation by a pediatric cardiologist and thepatient is less than 6 months old, and for the second thepatient is 6 months old or older at the time of thatevaluation. The algorithms provide for an initial history,physical examination, electrocardiogram, and echocar-diogram. In patients with a patent ductus arteriosus thathas been documented echocardiographically, surgicalclosure of the defect can be done without additionalechocardiographic studies if the physical findings re-main typical for an uncomplicated patent ductus arte-riosus. If the findings become atypical, one additionalechocardiographic study is considered necessary. Thealgorithm provides for elective closure of the patentductus arteriosus sometime within the first year of life.
After surgery, successful ligation/division of the duc-tus arteriosus can be documented by physical examina-tion. The algorithm provides for a posthospital outpa-tient evaluation, usually within 3 months of surgery. Achest radiogram may be necessary to exclude persistentperioperative problems. Echocardiography to confirmductal closure is a class II test and is intended todemonstrate complete closure of the patent ductusarteriosus. It is recognized that additional postoperativestudies may be needed for treatment of individualpatients in the perioperative period. The evaluationprovides for detection of additional perioperative prob-lems such as wound infection, pleural effusion, etc.After documentation of successful ligation/division ofthe ductus arteriosus and resolution of all perioperativeproblems, further cardiac evaluation is unnecessary.The algorithm for patent ductus arteriosus in patients
older than 6 months differs from that for patientsyounger than 6 months only in that surgical closure canbe performed shortly after diagnosis.
Ostium Secundum Atrial Septal Defect(unoperated) (Figs 4 and 5)Exclusion Criteria
1. The patient is older than 21 years.2. The patient has congestive heart failure.
Time 0 History and exam, chest radiogram, ECG, echo
Small shunt Large shuntAsymptomatic
Asymptomatic Symptomatic -Off+ ~~~~~~~~~~~~protocolTime 0+2 yr History and
exam
Small shunt Large shuntAsymptomatic
Time 0+5 yr History andexam
Small shunt Large shunt
Asymptomatfc History of CNS emboll, atiialarrhythmia, exercise Intolerance
SX not secondary SX secondary toto ASD AS
Time 0+8 yr History,and every 5 yr exam and
chest x-ray, and ECG
Close ASD withSmall shunt and Large shunt or _-preoperatve ECG,asymptomatic SXsecondary to chest x-ray and echo
Reevaluate at 1 yr, close ASD between2-5 yr of age if shunt still largeor symptoms develop from ASD.Preoperative chest x-ray, ECG, andecho as class 11 evaluations
FIG 4. Algorithm for atrial septal defect for a patient 5 years oldor younger. ECG indicates electrocardiogram; CNS, centralnervous system; SX, symptoms; ASD, atrial septal defect.
3. The patient has pulmonary vascular obstructivedisease.Definition of Shunt Size
1. Small shunt: Absence of diastolic flow rumble,normal chest x-ray, echocardiographic evidence of nor-mal right ventricular dimension, and normal interven-tricular septal motion or a pulmonary to systemic flowratio (QP/QS) <1.5.
2. Large shunt: Presence of a diastolic flow rumble orECG evidence of right ventricular hypertrophy, chestradiographic evidence of cardiomegaly or increasedpulmonary vascular markings, or echocardiographic ev-idence of right ventricular enlargement or paradoxicalseptal motion or a QP/QS .1.5.Algorithm for Ostium Secundum AtrialSeptal Defect (unoperated)Two algorithms were developed for the management
of ostium secundum atrial septal defect. For one, "Time
Time 0 History and exam, chest radlogram, ECG, echo
Small shunt Large shunt - Off protocol ordclose ASD
Time 0+5 yr andevery 5 yr * History and exam, chest x-ray, ECG
Small shunt and Large shuntasymptomatc SX secondary to ---Off protocol
ASD or suspected or closepulmonary ASDhypertension
FIG 5. Algorithm for atrial septal defect in a patient older than 5years. ECG indicates electrocardiogram; SX, symptoms; ASD,atrial septal defect.
by guest on May 17, 2018
http://circ.ahajournals.org/D
ownloaded from
AHA Council on CVDY Guidelines for Pediatric Congenital Cardiac Problems
Time 0 History and exam
Normal history and Abnormal history andexam; cled ASD; exam; evidence ofno evidence of persistent ASD;arrhythmia or arrhythmia orconduction disturbance conduction disturbance
Off protocol
lnme 0+1 yr History and exam, EGG
Normal Abnormal
Appropriate evaluationlime 0+6 yr and of specific abnormalityevery5 yr
History and exam, ECG (postoperativeevery 5 yr echio, class II)
Normal Abnormal
Appropriate evaluationof specific abnomity
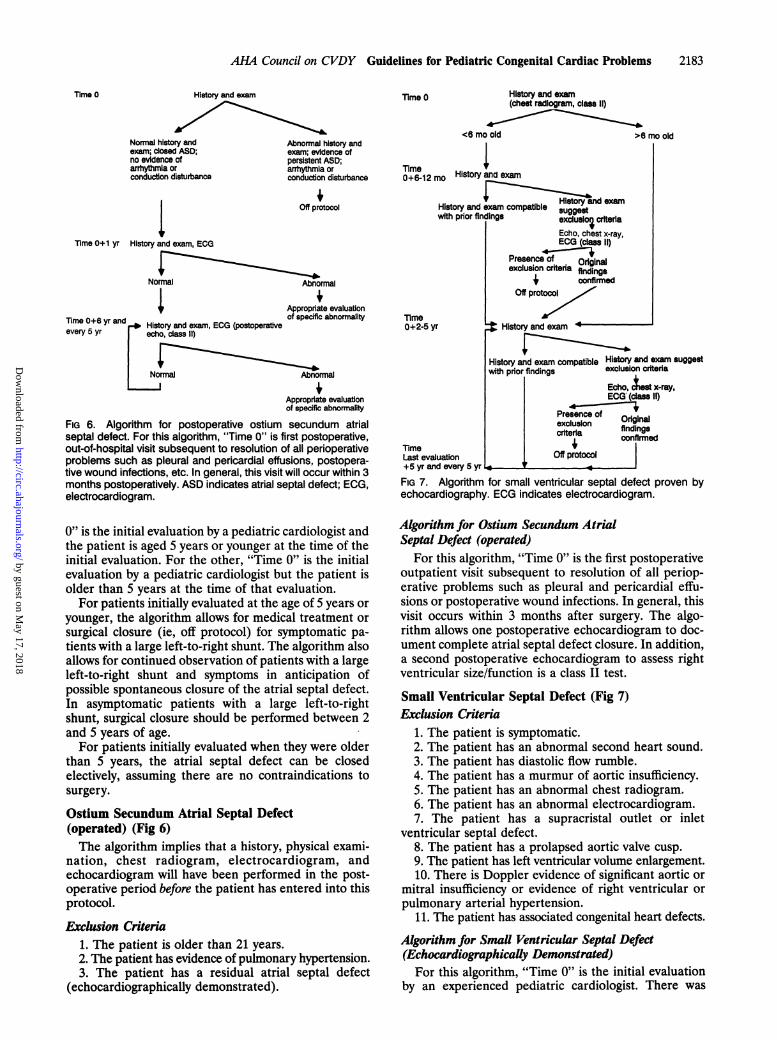
FIG 6. Algorithm for postoperative ostium secundum atrialseptal defect. For this algorithm, "Time 0" is first postoperative,out-of-hospital visit subsequent to resolution of all perioperativeproblems such as pleural and pericardial effusions, postopera-tive wound infections, etc. In general, this visit will occur within 3months postoperatively. ASD indicates atrial septal defect; ECG,electrocardiogram.
0" is the initial evaluation by a pediatric cardiologist andthe patient is aged 5 years or younger at the time of theinitial evaluation. For the other, "Time 0" is the initialevaluation by a pediatric cardiologist but the patient isolder than 5 years at the time of that evaluation.For patients initially evaluated at the age of 5 years or
younger, the algorithm allows for medical treatment orsurgical closure (ie, off protocol) for symptomatic pa-tients with a large left-to-right shunt. The algorithm alsoallows for continued observation of patients with a largeleft-to-right shunt and symptoms in anticipation ofpossible spontaneous closure of the atrial septal defect.In asymptomatic patients with a large left-to-rightshunt, surgical closure should be performed between 2and 5 years of age.For patients initially evaluated when they were older
than 5 years, the atrial septal defect can be closedelectively, assuming there are no contraindications tosurgery.
Ostium Secundum Atrial Septal Defect(operated) (Fig 6)The algorithm implies that a history, physical exami-
nation, chest radiogram, electrocardiogram, andechocardiogram will have been performed in the post-operative period before the patient has entered into thisprotocol.
Exclusion Criteria1. The patient is older than 21 years.2. The patient has evidence of pulmonary hypertension.3. The patient has a residual atrial septal defect
(echocardiographically demonstrated).
lime 0 History and exarn(cheat radlogram, class 11)
<6 mo old >6 mo old
Tlme Hso dea0+6-12 mo Historya
V~~7i~~b~~nd examnHistory and exam compatible sgetwith prior findings excluslo criteria
Echo, chest x-ray,ECG (class 11)
Presence of Originalexclusion criteda findings
4 confirrnedOff protocol
lime0+2-5 yr History and exarnm -
History and exam compatible History and exam suggestwit prior findings exclusion criteria
Echo, lest x-rY,ECG (cla 11)
Prsenc ofexclu31on Originalcriteria findings
lime confirmed
last evaluation Off protocol+5 yr and every 5 yr r
FIG 7. Algorithm for small ventricular septal defect proven byechocardiography. ECG indicates electrocardiogram.
Algorithm for Ostium Secundum AtrialSeptal Defect (operated)
For this algorithm, "Time 0" is the first postoperativeoutpatient visit subsequent to resolution of all periop-erative problems such as pleural and pericardial effu-sions or postoperative wound infections. In general, thisvisit occurs within 3 months after surgery. The algo-rithm allows one postoperative echocardiogram to doc-ument complete atrial septal defect closure. In addition,a second postoperative echocardiogram to assess rightventricular size/function is a class II test.
Small Ventricular Septal Defect (Fig 7)Exclusion Criteria
1. The patient is symptomatic.2. The patient has an abnormal second heart sound.3. The patient has diastolic flow rumble.4. The patient has a murmur of aortic insufficiency.5. The patient has an abnormal chest radiogram.6. The patient has an abnormal electrocardiogram.7. The patient has a supracristal outlet or inlet
ventricular septal defect.8. The patient has a prolapsed aortic valve cusp.9. The patient has left ventricular volume enlargement.10. There is Doppler evidence of significant aortic or
mitral insufficiency or evidence of right ventricular orpulmonary arterial hypertension.
11. The patient has associated congenital heart defects.
Algorithm for Small Ventricular Septal Defect(Echocardiographically Demonstrated)For this algorithm, "Time 0" is the initial evaluation
by an experienced pediatric cardiologist. There was
2183
by guest on May 17, 2018
http://circ.ahajournals.org/D
ownloaded from

2184 Circulation Vol 90, No 4 October 1994
Time 0 History and exam
Asymptomatic; exam Symptomatic; examconsistent with closed suggests hemodynamic orventricular septal defect rhythm abnormality, orand normal pulmonary pleural or pericardialartery pressure; no effusionevidence of pleural or 4percardial effusion Off protocol
1 2pooo
Time 0+6-12 mo - History and examand each (ECG and chest x-ray class 11)subsequent 2-5 yr
Asymptomatic; exam Symptomatic; examconsistent with closed suggests hemodynamicventricular septal defect or other abnormalityand normal pulmonary +artery pressure Ofl protocol
FIG 8. Algorithm for postoperative ventricular septal defect. Forthis algorithm, "Time O" is postoperative, out-of-hospital visitsubsequent to resolution of all perioperative problems such aspleural effusions, pericardial effusions, postoperative fevers, orwound infections. In general, this visit will occur within 3 monthsof hospital discharge. ECG indicates electrocardiogram.
considerable debate among committee members as towhether echocardiographic definition of a small ventric-ular septal defect was necessary to exclude other con-ditions that could mimic the physical findings of a smallventricular septal defect or associated problems such asprolapse of an aortic valve cusp. After considerablediscussion, it was decided to construct the algorithm forpatients with a small ventricular septal defect in whoman echocardiogram had been done. However, the com-mittee recognized that some pediatric cardiologists di-agnose a small ventricular septal defect without echo-cardiographic confirmation of the defect orechocardiographic exclusion of associated problems.The committee agreed that diagnosis and managementof patients with a small ventricular septal defect withoutechocardiographic confirmation was acceptable. Underthese circumstances, it is incumbent on the clinician toprovide appropriate ongoing evaluation to detect andmanage conditions that could mimic the physical find-ings of a small ventricular septal defect or the problemsassociated with it.
Postoperative Ventricular Septal Defect (Fig 8)The algorithm implies that a history, physical exami-
nation, chest radiogram, electrocardiogram, andechocardiogram are performed after surgery and beforethe patient has entered into this protocol.
Exclusion Criteria1. The patient is symptomatic.2. A residual ventricular septal defect of any size is
detected echocardiographically.3. The patient has an abnormal chest radiogram.4. The patient has an abnormal electrocardiogram
(except isolated right bundle branch block).5. The patient has transient perioperative second- or
third-degree atrioventricular block.6. The patient has evidence of persistent postopera-
tive pulmonary arterial hypertension.7. A left ventriculotomy is used for surgical closure of
the ventricular septal defect.8. The patient has a supracristal outlet or inlet
ventricular septal defect.
Time 0(patient <4yr old)
History and exam; ECG, echo
1 1Fulfills criteria formild pulmonary stenosisand <4 yr old
Time 0+ 6-12 mo History and exam, ECG
Exam and ECG Evidence forunchanged increased severity(echo class I1'
Echo
Gradient Gradier25-39 mm Hg <25 mr
Grai:.4C
nt Offim Hg
idlentmmHg
protocol
Time 0+24-36 mo History and exam, ECG(echo class 11)
Change
No change Gradient OffEcho-* ,40mm H-tprotocol
Gradient Gradient25-39 mm Hg <25 mm Hg
Fufills criteria formild pulmonary stenosisand .4 yr old
TimeG0 1(pTiment04 ~ _14 yr old Crime 0 evaluation includes echo as(patient >4 noted at Time 0+24-36 mo above)yr old)vTime 0+3-5 yr History and exam, ECG
No change Change
Echo
Gradient Gradient
Hstorydexam<40 mm Hg .40 mm Hg
Time and ECG 413-15 yr Off protocolof age and each5-10 yr thereafter
FIG 9. Algorithm for mild pulmonary valve stenosis. Two "TimeOs are shown, depending on the patient's age at initial evaluationby the pediatric cardiologist. ECG indicates electrocardiogram.
Algorithm for Postoperative Ventricular Septal DefectFor this algorithm, "Time 0" is the first postoperative,
out of hospital visit after resolution of all perioperativeproblems such as pleural effusions, pericardial effu-sions, and postoperative fevers or wound infections. Ingeneral, this visit will occur within 3 months of thehospital discharge.
Mild Pulmonary Valve Stenosis (Fig 9)Exclusion Criteria
1. Clinical findings are atypical.2. The Doppler peak instantaneous gradient is .40
mm Hg measured under resting conditions.3. The patient has an abnormal electrocardiogram
(except only mild right ventricular hypertrophy).4. The patient has a dysplastic pulmonary valve.
Algorithm for Mild Pulmonary Valve StenosisFor this algorithm, "Time 0" is the initial evaluation
by a pediatric cardiologist. The algorithm provides for
by guest on May 17, 2018
http://circ.ahajournals.org/D
ownloaded from

AIM Council on CVDY Guidelines for Pediatric Congenital Cardiac Problems
lime O History and exam
Asymp ic and exam Symptoms or exam suggestsconsistent wfth gradient <40 mm Hg hemodynamic, rhythm, or otherand no evidence for pleural abnormat or pericardial oror pericardial effusion pleural effusin
Time 0+6-12 moHistory and exam,ECG, echo
Off protocol
Gradient9c40 mm Hg
Gradient<40 mm Hg Off protocol
lnme 0+5 yr, 0+10 yr, History and -Evidence for increasedand every 10 subsequent exam. ECG severity of pulmonary stenosisyears L
No evidence forincreased severity of Echopulmonary stenosis | Gradlent
I Hg40mm HgGiradbt<40 mm Hg 0 protocol
FIG 10. Algorithm for postoperative or post-balloon valvuloplastyfor pulmonary valve stenosis. For this algorithm, "Time 0" is firstpostoperative out-of-hospital visit subsequent to resolution of allperioperative problems such as pleural effusions, pericardial effu-sions, postoperative fevers, or wound infections. Entry of a patientat "Time O" assumes that a postoperative echocardiogram hasbeen performed and that the transpulmonary gradient was <40mm Hg. It also assumes that residual subvalvar pulmonary stenosishas resolved. ECG indicates electrocardiogram.
detection of an increasing transpulmonary gradient.The committee agreed that echocardiographic studieswere essential for assessing the severity of pulmonarystenosis. Since progressive severity is highly unlikely in a
patient with initially mild (<40 mm Hg) pulmonarystenosis, more than three echocardiographic studies of a
patient with a persistent transpulmonary gradient lessthan 40 mm Hg are probably unnecessary.
Postoperative Pulmonary Valve Stenosis (Fig 10)The algorithm implies that a history, physical exami-
nation, chest radiogram, electrocardiogram, and echo-cardiographic studies will be performed in the postop-erative period before the patient has entered into thisprotocol.
Exclusion Criteria1. The residual Doppler peak instantaneous gradient
is 240 mm Hg.
History and exam, ECGlime with 1-min rhythm
strip (echo, 24-hrambulatory ECG,exercise test, class II)
Normal exam and Normal exam and Abnormal exam or suspicious patientVno ECG (except nomal ECG (except family history or abnormal ECGfor isolated, single for isolated single (except for Iolated, single, uniform
uniform PVCs) unHom PVCs) and PVCs) or 24-hr ambuo ECGuniformvs) 24-hr ambulatory ECG with 250 PVCs per 24-hr, or
<50 PVCs per 24 hr, abnormal echo or exercise testand normal echo
Dismiss ORf protocol
FIG 11. Algorithm for isolated premature ventricular contrac-tions. ECG indicates electrocardiogram; PVCs, premature ven-tricular contractions.
2. The patient has preoperative critical pulmonary valvestenosis (suprasystemic right ventricular pressure).
3. The patient is younger than 1 year at the time ofballoon valvuloplasty or surgical valvotomy.
Algorithm for Postoperative (or Post-BalloonValvuloplasty) Pulmonary Valve StenosisFor this algorithm, "Time 0" is the first postoperative,
outpatient visit subsequent to resolution of all periop-erative problems such as pleural effusions, pericardialeffusions, postoperative fevers, or wound infections.Entry of a patient at Time 0 assumes that a postoper-ative echocardiogram has been performed and that thetranspulmonary valve gradient is <40 mm Hg. It alsoassumes that residual subvalvar pulmonary stenosis hasresolved at the time of the initial postoperative, out-of-hospital visit.
Premature Ventricular Contractions (Fig 11)The algorithm assumes that the patient is referred to
a pediatric cardiologist because of an irregular rhythmor symptoms of palpitations.
Exclusion Criteria1. The patient is aged 21 years or older.2. The patient has a family history of premature (less
than 40 years old) sudden death of presumed or estab-lished cardiac origin.
3. The patient has a family history of prolonged QT,interval syndrome.
4. The patient has a family history of cardiomyopathy.5. The patient has a history suggestive of myocarditis.6. The patient has a history of syncope, presyncope,
or seizures.7. The patient has a subjective history of sustained
tachycardia.8. The patient has cardiac symptoms in addition to
palpitations.9. The patient has undergone a cardiac examina-
tion that was designated "abnormal" by a pediatriccardiologist.
10. The patient has an abnormal electrocardiogram(except for associated premature ventricular contrac-tions.)
11. There is a prolonged QT, interval.
Algorithm for Isolated PrematureVentricular ContractionsFor this algorithm, "Time 0" is the initial evaluation
by a pediatric cardiologist. The committee debatedextensively about the need for 24-hour ambulatoryECG monitoring, echocardiography, and exercise test-ing. Thus, these were considered class II tests. Use ofthese studies is influenced by factors such as the pa-tient's age, frequency and intensity of palpitations, andprobability of an associated viral illness or other sys-temic diseases.
DiscussionInnocent Cardiac MurmursThree relatively recent studies have focused on the
usefulness of diagnostic tests in the initial evaluation ofmurmurs in children. Newburger et all assessed resultsof the initial evaluation of 280 children referred to a
2185
by guest on May 17, 2018
http://circ.ahajournals.org/D
ownloaded from

2186 Circulation Vol 90, No 4 October 1994
pediatric cardiologist because of a cardiac murmur.After the initial history and physical examination, 142 ofthe 280 children were deemed to have no heart disease.After further testing and follow-up evaluation, 5 of the142 patients were thought to have "possible" (2) or"definite" (3) heart disease. The two patients withpossible heart disease had ventricular hypertrophy asmeasured by ECG criteria, and one had a low-normalshortening fraction on M-mode echocardiography. Allthree patients with definite heart disease had mitralvalve prolapse based on a two-dimensional echocardio-graphic study. Smythe et a12 assessed the results of theinitial evaluation by pediatric cardiologists of 161 pa-tients with a cardiac murmur. After the initial historyand physical examination, 109 of the 161 patients werethought to have an innocent murmur. In two of the 109patients, a heart defect was detected by echocardiogra-phy: one small muscular ventricular septal defect andone small atrial septal defect. There was some questionas to whether the patient with an atrial septal defect hadin fact a patent foramen ovale. When the results ofthese were considered, a defect requiring care thatdiffered from the management of an innocent murmurwas ultimately discovered in only one patient (0.3% ofthe group), who had a small ventricular septal defect forwhich endocarditis prophylaxis would be recommended.Geva et a13 reviewed echocardiograms of 50 children
who, following physical examination, electrocardiogra-phy, and chest radiography, were thought to have aninnocent murmur. The echocardiogram was normal in48 patients, and the other two patients had a bicuspidaortic valve.Based on these three studies, examination alone
would have failed to identify three patients (1%) forwhom endocarditis prophylaxis should be recom-mended. Given the unestablished efficacy of endocardi-tis prophylaxis and its very low risk in patients with anatrial septal defect, it may not be cost-effective toperform echocardiographic studies in all patients withan innocent murmur to detect the 1% of patients whomight require endocarditis prophylaxis.
Patent Ductus ArteriosusThe diagnosis of a patent ductus arteriosus can be
made on the basis of a history and physical examinationand confirmed by Doppler echocardiography. Cardiaccatheterization is necessary only in atypical cases, pri-marily those in which high pulmonary vascular resis-tance is suspected.
Complications of a patent ductus arteriosus includeinfective arteritis, aneurysm of the ductus, congestiveheart failure, pulmonary vascular obstructive disease,and calcification of the ductus.4-6 Therefore, the pres-ence of a clinically detectable ductus arteriosus isconsidered an indication for closure.7,8
Postoperative sequelae are uncommon, limited pri-marily to early postoperative complications of thoracot-omy, such as but not limited to wound infection, he-mothorax, or recurrent laryngeal nerve injury. Othersequelae include incomplete closure or recanalization.9
Ostium Secundum Atrial Septal DefectThe natural history of secundum atrial septal defect
includes development in adulthood of right ventricular
nary vascular obstructive disease. Investigators have founda greater mortality for patients with unoperated atrialseptal defect than for normal subjects or patients whohave had surgical closure of the defect.10 Although spon-taneous closure of an atrial septal defect is uncommon inolder children, adolescents, and adults, spontaneous clo-sure between 4% and 39.5% has been observed in infancyand early childhood.11-16 Most investigators agree thatspontaneous closure of an atrial septal defect is unlikelyafter the age of 2 years and very uncommon after the ageof 4 years. Thus, the rationale for conservative treatmentof asymptomatic patients with secundum atrial septaldefects who are younger than 4 years is justified.Treatment of symptomatic patients with secundum
atrial septal defects in infancy is controversial. Someinvestigators have demonstrated spontaneous closure ofatrial septal defects in infants who had congestive heartfailure.11,13 Whether it is better to surgically close anatrial septal defect in an infant with congestive heartfailure or to treat these patients with anticongestivetherapy is unclear. For this reason, these patients arenot considered in this algorithm.
Little is known about the fate of asymptomatic pa-tients with a small atrial septal defect. The incidence ofsmall atrial septal defects is unknown, and it is difficultto distinguish a "small" atrial septal defect from a"large" patent foramen ovale. In one study of smallatrial septal defect, progression of the left-to-right shuntoccurred in 15% of patients, and spontaneous closureoccurred in 11.5%.14 An additional risk of a small atrialseptal defect (or a patent foramen ovale) is paradoxicalembolization and stroke. Certainly it seems reasonableto close atrial septal defects if the left-to-right shuntbecomes progressively larger. For these reasons thealgorithm provides for continued follow-up evaluationof these patients. The efficacy of closing an atrial septaldefect (or patent foramen ovale) in a patient who hashad an unexplained stroke is unknown. However, thealgorithm allows the clinician to elect that course oftreatment.
Continued long-term follow-up of patients who havehad operative closure of an atrial septal defect seemsreasonable to detect the onset of new arrhythmias.17 Inone study, 2% of patients with an atrial septal defecthad arrhythmias before surgery, but 23% had them 0.1to 8.0 years after surgery.18
Ventricular Septal DefectThere have been several outcome studies of the
treatment of ventricular septal defect.19-21
Small Ventricular Septal DefectThe Second Joint Study on Natural History of Congen-
ital Heart Defects provided comprehensive data on 242young adults known to have a small ventricular septaldefect who were followed up medically from early child-hood. Spontaneous closure occurred in 13.7%. Five pa-tients (2.1%) developed clinical signs of congestive heartfailure, and 10 (4.1%) were taking digitalis, diuretics, orantiarrhythmic agents. Bacterial endocarditis occurred infive patients (7.1 per 10 000 person-years). In the entirecohort of 570 with ventricular septal defects of all sizes, 12(2%) developed aortic regurgitation.
Thus, although in most patients a small ventricularfailure, atrial arrhythmias, and in rare instances, pumeno- septal defect is a relatively benign condition, ongoing
by guest on May 17, 2018
http://circ.ahajournals.org/D
ownloaded from

AIIA Council on CVDY Guidelines for Pediatric Congenital Cardiac Problems
medical evaluation of these patients is necessary todetect and manage the relatively rare but importantcomplications of endocarditis, arrhythmias, aortic re-gurgitation, and subvalvular pulmonary stenosis anddiscrete subaortic stenosis.
Postoperative Ventricular Septal DefectSurgical closure of ventricular septal defects has been
done successfully for nearly 40 years. Surgical techniquesand timing and the mortality and morbidity of operationhave changed over time. Preoperative or postoperativehigh pulmonary vascular resistance and surgically ac-quired complete atrioventricular block are risk factors forlong-term morbidity and mortality. For the purposes ofthese guidelines, only children with isolated ventricularseptal defect and normal pulmonary vascular resistance,intact atrioventricular conduction, and complete closureor, at most, a small residual ventricular septal defect wereconsidered.
In the Second Natural History Study 226 young adultshad undergone ventricular septal defect closure inchildhood. Subsequent operations were performed in 31of 33 patients with a pulmonary artery band and 7 of193 patients with primary closure. Episodes of conges-tive heart failure were noted in 72 patients, and 6patients had cardiac pacemakers. Bacterial endocarditisoccurred in 10 patients.
Pulmonary StenosisThe algorithm for the management of patients with
mild pulmonary stenosis is based on the premise thatpatients 1) with a transpulmonary peak Doppler gradi-ent <40 mm Hg do not require operation or balloondilation; 2) with a transpulmonary gradient >40 mm Hgmay require surgery or balloon dilation; 3) withtranspulmonary gradients <40 mm Hg may progress togradients >40 mm Hg; 4) with gradients <25 mm Hgare less likely to progress to gradients >40 mm Hg thanpatients with gradients between 26 and 39 mm Hg.
In the First Natural History Study 14% of all patientswith valvular pulmonary stenosis had a significant in-crease of transpulmonary gradient at the conclusion ofthe study.22 For patients with an initial transpulmonarygradient <40 mm Hg, progression to a gradient >60mm Hg was rare. Gradients were unlikely to increase inpatients older than 12 years and were most likely toincrease significantly in patients younger than 4 years,particularly if the initial gradient was >40 mm Hg.There were 94 patients with pulmonary stenosis and atranspulmonary gradient <40 mm Hg on admission tothe First Natural History Study. Of these, 5 progressedto a gradient >40 mm Hg at the termination of that studyand an additional two patients progressed to a gradient>40 mm Hg at the time of the Second Natural HistoryStudy. None of the seven patients underwent surgery. Anadditional eight patients had an admission gradient <40mm Hg but had a pulmonary valvotomy. One of the eightprogressed to a gradient >40 mm Hg at the end of theFirst Natural History Study. Although the admissiongradient for the remaining seven was <40 mm Hg, theimmediate preoperative gradient was unknown. In theSecond Natural History Study, no cardiac-related deathsoccurred among the medically managed patients.23 For
mm Hg, 96.1% were free of cardiac operation over a25-year period.The results of operation (and presumably balloon
dilation) of pulmonary valve stenosis are excellent. Inthe Second Natural History Study, 349 patients optedfor relief of pulmonary valve stenosis.23 There were atotal of 19 deaths. Only 3.1% of patients required asecond operation within 10 years of the initial opera-tion. These data support an algorithm designed todetect the recurrence of significant pulmonary stenosisand detection of the rare patient who experiences latecomplications.
Isolated Uniform Premature Ventricular ContractionsBased on experience with older patients with isch-
emic heart disease, the notion that premature ventric-ular contractions lead to ventricular tachycardia that inturn leads to ventricular fibrillation has evolved. Thisperception has continued to evolve in the ischemic heartdisease model, but extrapolation of the adult experienceto the pediatric patient is difficult, in part becauseischemic heart disease is a rare cause of prematureventricular contractions in the pediatric patient. Never-theless, the possible association with occult heart dis-ease makes evaluation of premature ventricular con-tractions an important clinical problem.
Isolated premature ventricular contractions with uni-form ECG features are commonly found in older chil-dren and adolescents but are infrequently detected ininfants. For example, Southall and coworkers24 evalu-ated 134 healthy full-term infants using 24-hour ambu-latory ECG monitoring, and no premature ventricularcontractions were recorded in these newborn infants. Ina previous study Southall et a125 reported a prevalenceof premature ventricular contractions in newborns of0.9%. In children between 7 and 11 years of age, 1 of 92patients had premature ventricular contractions re-corded with 24-hour ambulatory ECG monitoring.26Scott et a127 evaluated 131 presumably healthy boys aged10 to 13 years and found that 26% had prematureventricular contractions. In a study of boys aged 14 to 16years, 41% had premature ventricular contractions and3% had nonsustained ventricular tachycardia.28 Brod-sky et a129 found that 50% of 50 male medical studentshad premature ventricular contractions. Based on thesestudies, it appears that the prevalence of prematureventricular contractions in otherwise healthy children isuncommon in infancy but increases with age. Thissuggests that the evaluation of a patient with prematureventricular contractions must be tempered by the pa-tient's age.Although it has been suggested24'30 that isolated
premature ventricular contractions in patients whoseem otherwise normal is a benign problem, the con-founding effects of age, number of premature ventricu-lar contractions, or variation in ECG features on thenatural history of these patients has not been thor-oughly addressed. Certainly there are conditions asso-ciated with ventricular ectopic activity that are relatedto increased risk of sudden death, such as myocarditis,myocardial tumors, prolonged QT interval syndromes,and arrhythmogenic right ventricular dysplasia. Theseare relatively rare and usually associated with otherphysical or ECG abnormalities. The necessity of exten-sively testing all patients with premature ventricular
2187
patients who had initial transpuhnonary gradients <25
by guest on May 17, 2018
http://circ.ahajournals.org/D
ownloaded from

2188 Circulation Vol 90, No 4 October 1994
TABLE. Bacterial EndocarditisProphylaxis Recommendations
Cardiac Conditions* Endocarditis prophylaxis is recommended for mostunoperated congenital cardiac malformations.* Endocarditis prophylaxis is not recommended for isolatedsecundum atrial septal defect.* Endocarditis prophylaxis is not recommended 6 monthsafter repair (without residua) of secundum atrial septal defect,ventricular septal defect, or patent ductus arteriosus.* Endocarditis prophylaxis is recommended for patients witha history of previous endocarditis, regardless of currentcardiac status.
Specific surgical and dental procedures needing coverageand the antibiotic regimens recommended by the AHA are givenin reference 31.
contractions to exclude these relatively rare problems isunclear. For these reasons, echocardiography and 24-hour ambulatory ECG monitoring are Class II tests. Athorough past medical history and family history areessential in the evaluation of these patients to alert theclinician to potentially important conditions.
Other ConsiderationsMany patients with congenital cardiac defects require
prophylaxis for bacterial endocarditis when undergoingcertain surgical and dental procedures (the Table). TheAHA has made specific recommendations concerningantibiotics.31Few patients with congenital heart defects are ever
truly "cured." Recommendations for endocarditis pro-phylaxis, sports participation, and genetic counselingchange as new information is acquired. Ongoing contactwith patients is necessary to communicate thesechanges to them. Maintaining contact with many pa-tients over a long period of time is difficult. It islogistically impossible for health providers alone toensure that this contact is maintained. Many patientswill eventually be followed up by an internist cardiolo-gist. It is important that internist cardiologists have asufficient level of expertise and experience to followthese patients into their adult years.
References1. Newburger JW, Rosenthal A, Williams RG, Fellows K, Miettinen
OS. Noninvasive tests in the initial evaluation of heart murmurs inchildren. N Engl J Med. 1983;308:61-64.
2. Smythe JF, Teixeira OH, Vlad P, Demers PP, Feldman W. Initialevaluation of heart murmurs: are laboratory tests necessary? Pedi-atrics. 1990;86:497-500.
3. Geva T, Hegesh J, Frand M. Reappraisal of the approach to thechild with heart murmurs: is echocardiography mandatory? Int JCardiol. 1988;19:107-113.
4. Campbell M. Natural history of persistent ductus arteriosus. BrHeart J. 1968;30:4-13.
5. Furuse A, Mizuno A, Nohara F, Ito K, Saigusa M. Calcified patentductus arteriosus. Jpn Heart J. 1968;9:316-320.
6. Fisher RG, Moodie DS, Sterba R, Gill CC. Patent ductus arte-riosus in adults -long-term follow-up: nonsurgical versus surgicaltreatment. JAm Coil Cardiol. 1986;8:280-284.
7. Black LL, Goldman BS. Surgical treatment of the patent ductusarteriosus in the adult. Ann Surg. 1972;175:290-293.
8. Heymann M. Patent ductus arteriosus. In: Adams FH, Emman-ouilides GC, Riemenschneider TA, eds. Moss' Heart Disease inInfants, Children, andAdolescents. 4th ed. Baltimore, Md: Williams& Wilkins; 1989:221.
9. Sorensen KE, Kristensen B, Hansen OK. Frequency of occurrenceof residual ductal flow after surgical ligation by color-flowmapping. Am J Cardiol. 1991;67:653-654.
10. Ogawa K, Ito T, Ban M, Mizutani K, Nagashima M. Long-termresults of operated and non-operated patients with congenitalheart diseases. Jpn Circ J. 1981;45:238-242.
11. Mahoney LT, Truesdell SC, Krzmarzick TR, Lauer RM. Atrialseptal defects that present in infancy. Am J Dis Child. 1986;140:1115-1118.
12. Cockerham JT, Martin TC, Gutierrez FR, Hartmann AF Jr,Goldring D, Strauss AW. Spontaneous closure of secundum atrialseptal defect in infants and young children. Am J Cardiol. 1983;52:1267-1271.
13. Hoffman JI, Rudolph AM, Danilowicz D. Left to right atrial shuntsin infants. Am J Cardiol. 1972;30:868-875.
14. Andersen M, Moller I, Lyngborg K, Wennevold A. The naturalhistory of small atrial septal defects: long-term follow-up withserial heart catheterizations. Am Heart J. 1976;92:302-307.
15. Han L, Ettedgui J, Zuberbuhler J. Clinical course of atrial septaldefect in children. Cardiol Young. 1992;2:141-146.
16. Kavey R, Blackman M, Byrum C, Smith F. Spontaneous closurerate of atrial septal defects diagnosed in infancy. JAm Coll Cardiol.1988;11:249a. Abstract.
17. Meijboom F, Hess J, Szatmari A, Utens EM, McGhie J, DeckersJW, Roelandt JR, Bos E. Long-term follow-up (9 to 20 years) aftersurgical closure of atrial septal defect at a young age.Am J Cardiol.1993;72:1431-1434.
18. Bink-Boelkens MT, Velvis H, van der Heide JJ, Eygelaar A, Hard-jowijono RA. Dysrhythmias after atrial surgery in children. AmHeartJ. 1983;106(pt 1):125-130.
19. Kidd L, Driscoll DJ, Gersony WM, Hayes CJ, Keane JF, O'FallonWM, Pieroni DR, Wolfe RR, Weidman WH. Second natural historystudy of congenital heart defects: results of treatment of patients withventricular septal defects. Circulation. 1993;87(suppl I):I-38-I-51.
20. Moller JH, Patton C, Varco RL, Lillehei CW. Late results (30 to 35years) after operative closure of isolated ventricular septal defectfrom 1954 to 1960. Am J Cardiol. 1991;68:1491-1497.
21. Van Hare GF, Soffer LJ, Sivakoff MC, Liebman J. Twenty-five-year experience with ventricular septal defect in infants andchildren. Am Heart J. 1987;114:606- 614.
22. Nugent EW, Freedom RM, Nora JJ, Ellison RC, Rowe RD, NadasAS. Clinical course in pulmonary stenosis. Circulation. 1977;56(suppl I):I-38-I-47.
23. Hayes CJ, Gersony WM, Driscoll DJ, Keane JF, Kidd L, O'FallonWM, Pieroni DR, Wolfe RR, Weidman WH. Second natural historystudy of congenital heart defects: results of treatment of patients withpulmonary valvar stenosis. Circulation. 1993;87(suppl I):I-28-I-37.
24. Southall DP, Richards J, Mitchell P, Brown DJ, Johnston PG,Shinebourne EA. Study of cardiac rhythm in healthy newborninfants. Br Heart . 1980;43:14-20.
25. Southall DP, Orrell MJ, Talbot JF, Brinton RJ, Vulliamy DG,Johnson AM, Keeton BR, Anderson RH, Shinebourne EA. Studyof cardiac arrhythmias and other forms of conduction abnormalityin newborn infants. Br Med J. 1977;2:597-599.
26. Southall DP, Johnston F, Shinebourne EA, Johnston PG. 24-hourelectrocardiographic study of heart rate and rhythm patterns inpopulation of healthy children. Br Heart J. 1981;45:281-291.
27. Scott 0, Williams GJ, Fiddler GI. Results of 24-hour ambulatorymonitoring of electrocardiogram in 131 healthy boys age 10 to 13years. Br Heart J. 1980;44:304-308.
28. Dickinson DF, Scott 0. Ambulatory electrocardiographic moni-toring in 100 healthy teenage boys. Br Heart J. 1984;51:179-183.
29. Brodsky M, Wu D, Denes P, Kanakis C, Rosen KM. Arrhythmiasdocumented by 24 hour continuous electrocardiographic moni-toring in 50 male medical students without apparent heart disease.Am J Cardiol. 1977;39:390-395.
30. Jacobsen JR, Garson A Jr, Gillette PC, McNamara DG. Pre-mature ventricular contractions in normal children. JPediatr. 1978;92:36-38.
31. Dajani AS, Bisno AL, Chung KJ, Durack DT, Freed M, Gerber MA,Karchmer AW, Millard HD, Rahimtoola S, Shulman ST,Watakunakom C, Taubert KA. Prevention of bacterial endocarditis:recommendations by the American Heart Association. JAMA. 1990;264:2919-2922.
by guest on May 17, 2018
http://circ.ahajournals.org/D
ownloaded from

Herndon, R E Shaddy and K A TaubertD Driscoll, H D Allen, D L Atkins, J Brenner, A Dunnigan, W Franklin, H P Gutgesell, P
Young, American Heart Association.Committee on Congenital Cardiac Defects of the Council on Cardiovascular Disease in the
infants, children, and adolescents. A statement for healthcare professionals from the Guidelines for evaluation and management of common congenital cardiac problems in
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1994 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.90.4.2180
1994;90:2180-2188Circulation.
http://circ.ahajournals.org/content/90/4/2180.citationWorld Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 17, 2018
http://circ.ahajournals.org/D
ownloaded from