aggressive micro surgical resection
TRANSCRIPT

8/8/2019 Aggressive Micro Surgical Resection
http://slidepdf.com/reader/full/aggressive-micro-surgical-resection 1/8
CLINICAL STUDIES
PATIENT OUTCOME AT LONG-TERM FOLLOW-UP
AFTER AGGRESSIVE MICROSURGICAL RESECTION
OF CRANIAL BASE CHORDOMAS
Fortios Tzortzidis, M.D.
Department of Neurosurgery,
University of Washington,Seattle, Washington
Foad Elahi, M.D.
Department of Neurosurgery,
University of Washington,Seattle, Washington
Donald Wright, M.D.Department of Neurosurgery,Virginia Hospital Center,
Arlington, Virginia
Sabareesh K. Natarajan, M.S.,M.D.
Department of Neurosurgery,University of Washington,Seattle, Washington
Laligam N. Sekhar, M.D.
Department of Neurosurgery,University of Washington,
Seattle, Washington
Reprint requests:Laligam N. Sekhar, M.D., F.A.C.S.Department of Neurosurgery,
325 Ninth Avenue,Box 359924,Seattle, WA 98104.
Email: [email protected]
Received, August 1, 2005.
Accepted, April 10, 2006.
OBJECTIVE: In this study, we evaluated patients’ clinical outcome and recurrence rates atlong-term follow-up after aggressive microsurgical resection of cranial base chordomas.
METHODS: Seventy-four patients with chordomas underwent operations during a16-year period from 1988 to 2004. The philosophy was to perform complete resectionwhenever possible and to provide adjuvant radiotherapy for remnants. Staged opera-tions were performed for extensive tumors or if a sizable tumor remnant was notedafter the first resection. Patients included primary (previously untreated) and previouslyoperated or irradiated cases. Information was prospectively gathered concerning thepatients’ neurological condition, Karnofsky Performance Scale score, and tumor statuson magnetic resonance imaging scans.
RESULTS: There were 47 primarily operated patients (63.5%) and 27 patients (36.5%) whohad previously undergone surgery or radiotherapy. A total of 121 procedures were performedin 74 patients. The mean follow-up period was 96 months, with a range of 1 to 198 months.A single stage removal was performed in 41 (55.4%) of the patients and multiple stage removalwas performed in 33 (44.5%) of the patients. Gross total removal was accomplished in 53(71.6%) of the patients, and subtotal resection was accomplished in 21 (28.4%) of the patients.During the follow-up period, 24 (32%) of the patients had no evidence of disease, 37 (50%) of the patients were alive with evidence of disease, 11 (14.8%) of the patients died of disease, andtwo(2.7%) of the patients died of complications. Recurrence-free survival at 10 years was 31%for the whole group, 42% for the primarily operated patients, and 26% for the reoperationcases (P 0.0001). The average Karnofsky Performance Scale score was 80 11.7 preoper-atively, 84 8.9 at the 1-year follow-up, and 86 12.8 at the last follow-up in survivingpatients. No conclusion could be drawn regarding the value of radiotherapy because of thetreatment philosophy and the small number of patients.
CONCLUSION: Aggressive microsurgical resection of chordomas can be followed bylong-term, tumor-free survival with good functional outcome. A more conservativestrategy is recommended in reoperation cases, especially after previous radiotherapy,to reduce postoperative complications.
KEY WORDS: Chordoma, Clinical outcome, Follow-up
Neurosurgery 59:230-237, 2006 DOI: 10.1227/01.NEU.0000223441.51012.9D www.neurosurgery-online.com
Chordomas represent fewer than 0.1% ofall cranial base tumors. Chordomas de-velop from notochord remnants, which
exist in normal adults as the nucleus pulposusof the intervertebral discs. However, otherremnants may be found in the clival bonemarrow, accounting for the extradural loca-tion of most chordomas. Primary intraduralchordomas have been reported, but they arerare (11, 13, 22, 25, 26).
On short repetition time (TR)/short echotime (TE) images, chordomas generally havea low-to-intermediate signal. On long TR/long TE images, chordomas generally have avery high signal that is heterogeneous inmore than two-thirds of the images (9, 18).After gadolinium administration, all chor-domas demonstrate some degree of contrastenhancement. The T2-weighted imaging sig-nal intensity of chordomas is significantly
230 | VOLUME 59 | NUMBER 2 | AUGUST 2006 www.neurosurgery-online.com

8/8/2019 Aggressive Micro Surgical Resection
http://slidepdf.com/reader/full/aggressive-micro-surgical-resection 2/8

8/8/2019 Aggressive Micro Surgical Resection
http://slidepdf.com/reader/full/aggressive-micro-surgical-resection 3/8
tient was treated with adjuvant radiotherapy. A more con-servative approach was used in recurrent cases. Such radio-therapy usually consisted of proton beam radiotherapy orradiosurgery. Although it was our goal to refer such pa-tients for proton beam radiotherapy, many patients couldnot afford the travel and the long-term stay that was re-
quired. Therefore, both radiosurgery and fractionated ra-diotherapy were used as adjuvants. In some patients, amultistage operative approach was planned preoperatively, based on the extent of tumor present in the initial MRIscans.
All tumors were examined pathologically with immunohis-tochemistry, especially for epithelial membrane antigen andcytokeratin (CK), to distinguish the tumor from chondrosar-coma.
Follow-up
Follow-up examinations were performed in patients annu-ally (whenever possible) by direct examination and MRI scan-
ning. At the conclusion of the study in December 2004, furtherfollow-up was conducted by a standardized questionnaire anda telephone interview by a nurse practitioner or physicians’assistant. Information was gathered regarding patients’ qual-ity of life, neurological deficits, and history of other treat-ments. The most recent MRI examination and/or the radiolo-gist’s report were obtained for review. The MRI scans werereviewed by radiologists who were not part of the study. If notumor was visible on MRI scans, the patient was consideredfree of tumor. Survival curves were plotted.
RESULTS
Postoperative complications in these patient series are sum-marized in Table 4. Two patients died postoperatively of com-plications. The mean follow-up period was 96 months, with arange of 1 to 198 months. A single stage removal was per-formed in 41 patients (55.4%) and multiple stage removal wasperformed in 33 patients (44.5%). Gross total resection wasaccomplished in 53 patients (71.6%), and subtotal resectionwas accomplished in 21 patients (28.4%). In primarily oper-ated patients, gross total re-section was accomplished in39 patients (83%), and, in re-operated patients, gross totalresection was accomplishedin 14 patients (30%) (Table 5).The average KPS score was80 11.7 preoperatively, 84 8.9 at the 1-year follow-upexamination, and 86 12.8 atthe last follow-up examina-tion (in surviving patients)(Table 6).
Twenty-six patients had re-currence after gross total re-
section. They were treated by irradiation only (six cases, 26%),resection followed by irradiation (19 cases, 73%), or no treat-ment (one case, 4%) (Table 5). The types of radiation adminis-tered include proton beam radiotherapy (38%), radiosurgery(43%), and fractionated external beam radiotherapy (19%) (Fig.1).
At the last follow-up examination, 24 patients (32%) had noevidence of disease, 37 patients (50%) were alive with evi-dence of disease, 11 patients (14.8%) died of disease, and twopatients (2.7%) died of complications (Table 5).
Recurrence-free survival was observed to be 1 to 36 monthsin 26 patients (56%), 37 to 84 months in 21 patients (45%), 85to 132 months in 19 patients (41%), and longer than 132months in 15 patients (31%). Recurrence-free survival for pre-viously treated cases was much less than for the primarypatients (log-rank significance, 0.0001) (Fig. 2). At 10 years, therecurrence-free survival for primarily operated patients was42%; for reoperation cases, it was 26% (Table 7).
This study was not designed to compare irradiated and
nonirradiated patients after complete tumor removal becausenone of the patients received irradiation after complete resec-tion. The number of patients irradiated was not large enoughto compare the different radiation modalities after subtotal
TABLE 4. Complications after surgerya
Complication No. of patients
CSF leakage 1
CN palsy, permanent 3
Hydrocephalus 1
Deep vein thrombosis 2
Pulmonary emboli 1
Hemiparesis 1Postoperative stroke 1
Sphenoid sinus infection 1
Hematoma at the fat graft harvesting site 1
Death 2
Total 12
a CSF, cerebrospinal fluid; CN, cranial nerve.
TABLE 5. Patients’ condition at the last follow-up examinationa
No. Recurrence NED AWD DOD DOC
Primary cases (n 47)
Gross total resection 39 17 21 17 — 1
Subtotal resection 8 — — 5 3 —
Reoperation cases (n 27)
Gross total resection 14 9 3 9 4 —
Subtotal resection 13 — — 6 4 1
Total 26 24 37 11 2
a NED, no evidence of disease; AWD, alive with evidence of disease DOD, died of disease; DOC, died of complications.
TZORTZIDIS ET AL.
232 | VOLUME 59 | NUMBER 2 | AUGUST 2006 www.neurosurgery-online.com
8/8/2019 Aggressive Micro Surgical Resection
http://slidepdf.com/reader/full/aggressive-micro-surgical-resection 4/8
resection, particularly proton beam radiotherapy and radio-surgery.
Illustrative Cases
Patient 1This case is presented to illustrate the operative approach to exten-
sive tumors, with multistage surgery.A 43-year-old woman presented with facial numbness, VIth cranial
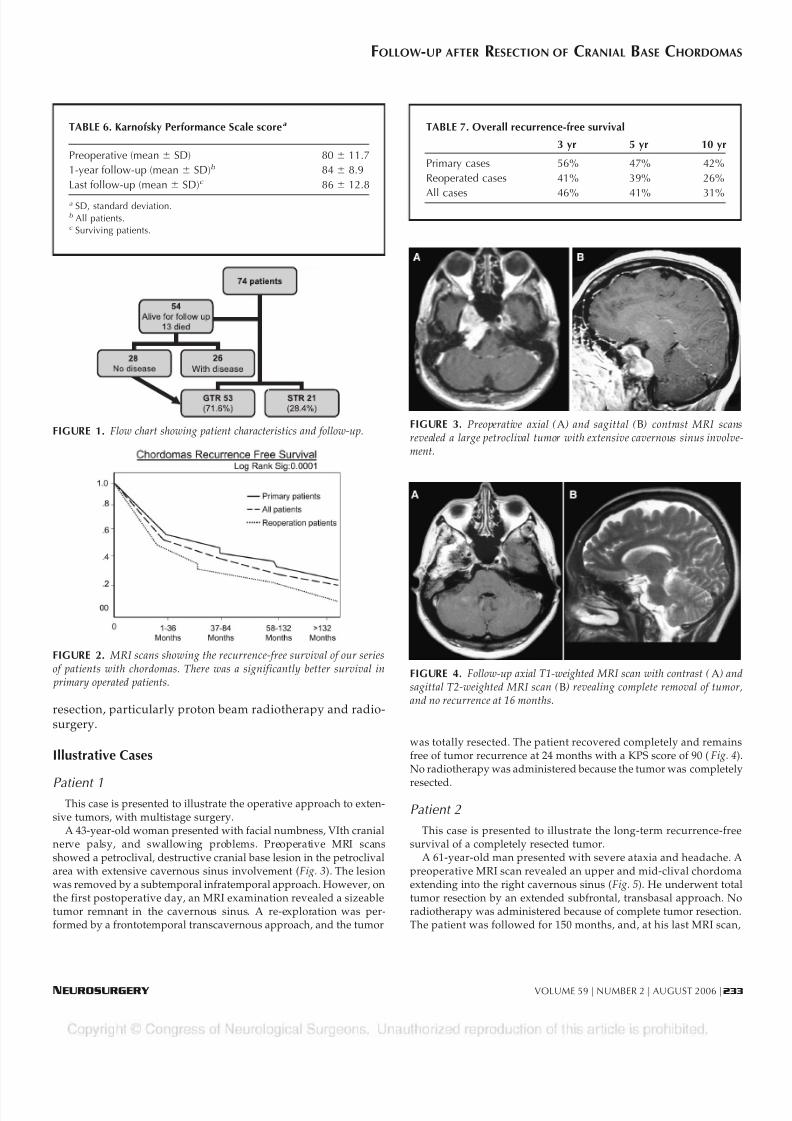
nerve palsy, and swallowing problems. Preoperative MRI scansshowed a petroclival, destructive cranial base lesion in the petroclivalarea with extensive cavernous sinus involvement (Fig. 3). The lesionwas removed by a subtemporal infratemporal approach. However, onthe first postoperative day, an MRI examination revealed a sizeabletumor remnant in the cavernous sinus. A re-exploration was per-formed by a frontotemporal transcavernous approach, and the tumor
was totally resected. The patient recovered completely and remainsfree of tumor recurrence at 24 months with a KPS score of 90 (Fig. 4).No radiotherapy was administered because the tumor was completely
resected.
Patient 2
This case is presented to illustrate the long-term recurrence-freesurvival of a completely resected tumor.
A 61-year-old man presented with severe ataxia and headache. Apreoperative MRI scan revealed an upper and mid-clival chordomaextending into the right cavernous sinus (Fig. 5). He underwent totaltumor resection by an extended subfrontal, transbasal approach. Noradiotherapy was administered because of complete tumor resection.The patient was followed for 150 months, and, at his last MRI scan,
TABLE 6. Karnofsky Performance Scale scorea
Preoperative (mean SD) 80 11.7
1-year follow-up (mean SD)b 84 8.9
Last follow-up (mean SD)c 86 12.8
a SD, standard deviation.b All patients.c Surviving patients.
FIGURE 1. Flow chart showing patient characteristics and follow-up.
TABLE 7. Overall recurrence-free survival
3 yr 5 yr 10 yr
Primary cases 56% 47% 42%
Reoperated cases 41% 39% 26%
All cases 46% 41% 31%
FIGURE 2. MRI scans showing the recurrence-free survival of our seriesof patients with chordomas. There was a significantly better survival in
primary operated patients.
FIGURE 3. Preoperative axial (A) and sagittal (B) contrast MRI scansrevealed a large petroclival tumor with extensive cavernous sinus involve-ment.
FIGURE 4. Follow-up axial T1-weighted MRI scan with contrast (A) andsagittal T2-weighted MRI scan (B) revealing complete removal of tumor,and no recurrence at 16 months.
FOLLOW-UP AFTER RESECTION OF CRANIAL BASE CHORDOMAS
NEUROSURGERY VOLUME 59 | NUMBER 2 | AUGUST 2006 | 233

8/8/2019 Aggressive Micro Surgical Resection
http://slidepdf.com/reader/full/aggressive-micro-surgical-resection 5/8
there was no evidence of recurrence (Fig. 6). He is not able to smelland has marked visual impairment in the right eye, but, until recently,worked as a university professor. He has now retired.
Patient 3
This case illustrates an example of an extremely aggressive chor-doma.
A 25-year-old man presented with severe headache, progressiveIIIrd nerve palsy, and complete VIth nerve palsy. He also had totalpituitary dysfunction. On MRI scans, a destructive tumor was re-vealed extending from the pituitary fossa to the upper and mid-clivus(Fig. 7). His preoperative KPS score was 90. In March 1994, the tumorwas partially removed using an extended subfrontal approach withresidual tumor in left cavernous sinus, which was inaccessiblethrough this approach. On the second stage surgery, the tumor wascompletely removed via a transsylvian approach. After 5 months fromhis first admission, a third operation was performed because of ag-gressive tumor recurrence.
Six months after the first operation, tumor recurred significantly inthe same area. He underwent reoperation for tumor excision, and hesubsequently underwent proton beam radiotherapy. In May 1995, hedeveloped back pain and urinary incontinence. The MRI scan revealeda sacral tumor, which was partially removed via a sacral laminectomy,and he received local radiotherapy (Fig. 8). In August of 1996, he had
a tumor recurrence in the lowerclival area (Fig. 9) with new on-set of hemiparesis. This tumorwas partially removed by atranscondylar approach for pal-liative purposes because he hadmaintained good function untilthen. In December 1996, the pa-tient died because of multipletumor recurrences.
DISCUSSION
Chordomas are locally ag-gressive tumors that arisefrom remnants of the noto-chord. The predominance ofthese tumors occurs in the sa-crococcygeal and cranial baseareas, although they do in-volve other spinal areas ( 6–8,10, 21). Their histological ap-pearance is typical, with areasof cartilage or bone destruc-tion and bubble-like or “phys-aliphorous” cells (25). A vari-ant of chordoma called the
“chondroid chordoma” is recognized with features resemblingchondrosarcoma (5, 25). Although some series have reported a better long-term outcome with chondroid chordoma, this wasnot borne out in other series (2, 4, 12, 19). On immunohistochem-istry, chordomas stain positively for S100, vimentin, epithelialmembrane antigen, and CK 8/18. They also express other CKs,such as CK 1/10, CK 7, CK 20, CK 19, and CK 12 to 17. Chon-drosarcomas of the cranial base do not stain positively for epi-thelial membrane antigen and CK. In reviewing any series ofthese tumors, it is important to elucidate whether the patients
FIGURE 5. Preoperative mid-sagittal (A) and axial (B) T2-weighted MRI scans with contrast revealing an upper clival tumor.
FIGURE 6. Follow-up mid-sagittal (A) and axial (B) T2-weighted MRI scans revealing complete removal of tumor and no recurrence at 138months after the operation.
FIGURE 7. Preoperative T2-weighted sagittal (A) and postcontrast coronalT1-weighted MRI scans (B) revealing a large tumor extending from the pituitary
fossa to the upper and mid-clival region.
FIGURE 8. Sagittal T2-weightedlumbar MRI revealing a sacral tumor.The patient experienced a seedingalong the neuraxis or de novo tumor
formation in the sacral area 14 monthsafter initial resection.
TZORTZIDIS ET AL.
234 | VOLUME 59 | NUMBER 2 | AUGUST 2006 www.neurosurgery-online.com

8/8/2019 Aggressive Micro Surgical Resection
http://slidepdf.com/reader/full/aggressive-micro-surgical-resection 6/8
were studied by immunohis-tochemistry. Chondrosarco-mas of the cranial base have amuch more benign coursethan chordomas, and mixingthese two types of tumors in
the report may give a falseidea regarding the long-termresults of a particular treat-ment modality used (11, 13,19). Chordomas seem to havetwo distinct biological behav-iors. The first group, whichcomprises the majority of tu-mors, are slow growing, and,in rare cases, may not evengrow at all (the senior author, LNS, is following two such pa-tients). Such tumors also remain locally confined rather thanmetastasize to other areas of the remains or other body areas (3,
6, 8). The second group has a more aggressive behavior, withrapid local recurrence spread to other areas of the neuroaxis ormetastasis to the lung, liver, or bone (as seen in Patients 3 and 4).Some primary tumors and many postradiation recurrent tumors behave in a more aggressive fashion (14, 16, 17).
The treatment of cranial base chordomas is based entirelyon Class III evidence, as there are no randomized trials re-garding the efficacy of surgery or radiotherapy (1). Becausechordomas are known to be minimally radiosensitive, high-dose therapy with proton beam radiation and radiosurgeryusing the gamma knife and CyberKnife have been used (4,19–21, 23, 24). There are no reports regarding long-term resultsafter gamma knife or CyberKnife radiosurgery, but there are
reports regarding proton beam radiotherapy (4, 19). On the basis of the results of treatment with proton beam radiother-apy, it seems that chondrosarcomas respond much better thanchordomas, and the results are better for chondroid chordo-mas.
The term “chondroid chordoma” is based on the findings oflarge amounts of cartilaginous material in the matrix of chor-domas, but not all pathologists are convinced regarding thisdistinction (5). In a previous report, we did not find a betterprognosis in “chondroid chordomas” (12). In this report, ourpatients were not classified into chondroid and nonchondroid
varieties. However, it is obvious that there is a distinct groupof chordomas with a more aggressive behavior, as exemplified by Patient 3. Most chordomas that have recurred after radio-therapy also belong to this group.
There are three different philosophies regarding the treat-ment of chordomas: aggressive surgical resection, with radio-therapy given only in patients who have remnants, aggressiveresection followed by radiotherapy, and partial resection fol-lowed by radiotherapy. After aggressive surgical resection, wehave also observed a third group of patients with delayedrecurrence that may do well for a number of years withreoperation. The senior author (LNS) and Crockard et al. (7)have followed the policy of aggressive surgical resection and
no radiotherapy unless distinct remnants remain. Al-Meftyand Borba (2) administer radiotherapy to all patients postop-eratively, regardless of resection. Other neurosurgeons haveadopted varying philosophies. Our series presents the infor-mation regarding long-term follow-up, which is not yet avail-able with other series (Table 8). None of the previously re-ported patient series have had the length of follow-up as ourseries. For a disease with low incidence and recurrence evenafter 10 years, it would be very difficult to conduct a random-ized trial to compare different treatment modalities.
In our series of patients, we have used a variety of cranial base approaches for the resection of tumors on the basis of thetumors’ location and the senior author’s (LNS) preference.
Certain approaches were used less frequently, in particular,the transphenoidal, transmaxillary, and transoral approaches.We also did not use endoscopic resection of these tumors as is being performed presently in some centers (endoscopic assis-tance was used during resection of some tumors). Frameless
FIGURE 9. T1-weighted postcon-trast MRI revealed the last recurrenceof this extremely aggressive tumor inthe upper and lower clival area in Au-
gust 1996.
TABLE 8. Previously published seriesa
Series(ref. no.)
No. of patients
Sex(M/F)
Therapy GTR STR PR RTRecurrence-free survival Mean
follow-up(mo)
Tumor-related death
3 mo 3 yr 5 yr 7 yr 11 yr >11 yr
Al-Mefty and
Borba, 1997 (2)
25 15/10 Radical surgery
and proton-photonbeam therapy
43 48 9 17 16/21 25.4 2 (10%)
Gay et al., 1995(12)
46 Radical surgeryand RT for ST only
47 43 10 12 65% 46 5 (10.8%)
Forsyth et al.,1993 (11)
51 Surgery and RT 40 11 39 51% 35%
Current studies 74 36/38 Radical surgeryand RT for ST only
53 21 0 25 56% 45% 41% 32% 96 11 (14.9%)
a GTR, gross total resection; STR, subtotal resection; PR, partial resection; RT, radiotherapy.
FOLLOW-UP AFTER RESECTION OF CRANIAL BASE CHORDOMAS
NEUROSURGERY VOLUME 59 | NUMBER 2 | AUGUST 2006 | 235

8/8/2019 Aggressive Micro Surgical Resection
http://slidepdf.com/reader/full/aggressive-micro-surgical-resection 7/8
stereotactic guidance has been extensively used for extraduraltumors during the past 6 years and was found to be particu-larly useful for tumor removal from certain areas. The use ofan individual surgical approach is based on the experience ofthe surgeon and the surgeon’s confidence with the safety andefficacy of the approach for tumor resection. As such, there is
no correct or incorrect approach; one has to focus on theresults and complications.
On the basis of the experience gained from this series, it may be stated that tumor resections are much easier if the patient isseen initially, before the patient has had a previous resection orradiotherapy. Recurrent tumors are not only more difficult toremove, but also carry a higher complication rate. Thus, thesurgeon’s aim should be to administer the optional treatmentduring the initial treatment session, which may consist of tumorresection and/or radiotherapy. The senior author (LNS) thinksthat, whenever possible, radiotherapy should be reserved forrecurrences rather than initial therapy. However, the philosophyshould be tempered by not creating a significant disability in the
patient. In this series, better long-term results were obtained inprimary tumors than recurrent tumors. However, this may becaused by more aggressive biological behavior (recurrent tu-mors) rather than complete removal (in primary patients).
When a patient presents with recurrent tumors, the approachshould be different and more conservative. If the tumor can beremoved completely without causing disability, it should beremoved. However, the surgeon (and the patient) should beaware that the chances of long-term survival and the potential forcomplications (resulting in disability) are higher in reoperationcases. The treatment strategy should be planned appropriately.
CONCLUSIONA series of patients with chordomas treated by aggressive
surgical resection and long-term follow-up is presented. Thesurvival was better in primary operation patients than inreoperation cases. We could not draw any conclusions regard-ing the value of radiotherapy, particularly after complete re-moval. New approaches to treatment of aggressive chordomasare necessary. We also could not compare the different radi-ation modalities because of the small numbers.
REFERENCES
1. Anonymous: The periodic health examination: 2. 1987 update. Canadian
Task Force on the Periodic Health Examination. CMAJ 138:618–626, 1998.
2. Al-Mefty O, Borba LA: Skull base chordomas: A management challenge. J Neurosurg 86:182–189, 1997.
3. Arnautovic KI, Al-Mefty O: Surgical seeding of chordomas. J Neurosurg
95:798–803, 2001.
4. Austin-Seymour M, Munzenrider J, Goitein M, Verhey L, Urie M, Gentry R,
Birnbaum S, Ruotolo D, McManus P, Skates S, Ojemann RG, Rosenberg A,
Schiller A, Koehler A, Suit HD: Fractionated proton radiation therapy of
chordoma and low-grade chondrosarcoma of the base of the skull.
J Neurosurg 70:13–17, 1989.
5. Brooks JJ, LiVolsi VA, Trojanowski JQ: Does chondroid chordoma exist?
Acta Neuropathol (Berl) 72:229–235, 1987.
6. Colli B, Al-Mefty O: Chordomas of the craniocervical junction: Follow-up
review and prognostic factors. J Neurosurg 95: 933–943, 2001.
7. Crockard HA, Steel T, Plowman N, Singh A, Crossman J, Revesz T, Holton
JL, Cheeseman A: A multidisciplinary team approach to skull base chordo-
mas. J Neurosurg 95:175–183, 2001.
8. Dalpra L, Malgara R, Miozzo M, Riva P, Volonte M, Larizza L, Fuhrman
Conti AM: First cytogenetic study of a recurrent familial chordoma of the
clivus. Int J Cancer 81:24–30, 1999.9. Erdem E, Angtuaco EC, Van Hemert R, Park JS, Al-Mefty O: Comprehensive
review of intracranial chordoma. Radiographics 23:995–1009, 2003.
10. Eriksson B, Gunterberg B, Kindblom LG: Chordoma: A clinicopathologic
and prognostic study of a Swedish national series. Acta Othop Scand
52:49–58, 1981.
11. Forsyth PA, Cascino TL, Shae EG, Scheithauer BW, O’Fallon JR, Dozier JC,
Piepgras DG: Intracranial chordomas: A clinicopathological and prognostic
study of 51 cases. J Neurosurg 78:741–747, 1993.
12. Gay E, Sekhar LN, Rubinstein E, Wright DC, Sen C, Janecka IP, Snyderman
CH: Chordomas and chondrosarcomas of the cranial base: Results and
follow-up of 60 patients. Neurosurgery 36:887–897, 1995.
13. Heffelfinger MJ, Dahlin DC, MacCarty CS, Beabout JW: Chordomas and
cartilaginous tumors at the skull base. Cancer 32:410–420, 1973.
14. Holton JL, Steel T, Luxsuwong M, Crockard HA, Revesz T: Skull base
chordoma: Correlation of tumor doubling time with age, mitosis and Ki67
proliferation index. Neuropathol Appl Neurobiol 26:497–503, 2000.
15. Hug EB, Fitzek MM, Liebsch NJ, Munzenrider JE: Locally challenging osteo-
and chondrogenic tumors of the axial skeleton: Results of combined proton
and photon radiation therapy using three-dimensional treatment planning.
Int J Radiat Oncol and Biol Phys 31:467–476, 1995.
16. Kamrin RP, Potanos JN, Pool JL: An evaluation of the diagnosis and treat-
ment of chordoma. J Neurol Neurosurg Psychiatry 27:157–165, 1964.
17. Korten A, Berg H, Spincemaille GH, Laan RT, van de Wel AM: Intracranial
chondrosarcoma: Review of the literature and report of 15 cases. J Neurol
Neurosurg Psychiatry 65:88–92, 1998.
18. Meyers SP, Hirsch WL Jr, Curtin HD, Barnes L, Sekhar LN, Sen C: Chordo-
mas of the skull base: MR features. AJNR Am J Neuroradiol 13:1627–1636,
1992.
19. Munzenrider JE, Liebsch NJ: Proton therapy for tumors of the skull base.
Strahlenther Oncol 175 [Suppl 2]:57–63, 1999.
20. Muthukumar N, Kondziolka D, Lunsford LD, Flickinger JC: Stereotacticradiosurgery for chordoma and chondrosarcoma: Further experiences. Int J
Radiation Oncology Biol Phys 41:387–392, 1998.
21. Noel G, Feuvret L, Ferrand R, Boisserie G, Mazeron JJ, Habrand JL: Radio-
therapeutic factors in the management of cervical-basal chordomas and
chondrosarcomas. Neurosurgery 55:1252–1262, 2004.
22. Nishigaya K, Kaneko M, Ohashi Y, Nukui H: Intradural retroclival chor-
doma without bone involvement: No tumor regrowth 5 years after opera-
tion: Case report. J Neurosurg 88:764–768, 1998.
23. O’Connell JX, Renard LG, Liebsch NJ, Efird JT, Munzenrider JE, Rosenberg
AE: Base of skull chordoma: A correlative study and clinical features of 62
cases. Cancer 74:2261–2267, 1994.
24. Pearlman AW, Friedman M: Radical radiation therapy of chordoma. Am J
Roentgenol Radium Ther Nucl Med 108:333–341, 1970.
25. Russel DS, Rubinstein LJ (eds): Pathology of Tumors of the Nervous System.
London, Edward Arnold, 1989, pp 664–765.
26. Warnick RE, Raisanen J, Kaczmar T, Davis RL, Prados MD: Intraduralchordoma of the tentorium cerebelli: Case report. J Neurosurg 74:508–511,
1991.
27. Watkins L, Khudados ES, Kaleoglu M, Revesz T, Sacares P, Crockard HA:
Skull base chordomas: A review of 38 patients, 1958–1988. Br J Neurosurg
7:241–248, 1993.
Acknowledgments
We thank Ramin Rak, M.D., Susan Buchholtz, N.P., and Oleg Rivkin, P.A., for
their assistance with data collection.
TZORTZIDIS ET AL.
236 | VOLUME 59 | NUMBER 2 | AUGUST 2006 www.neurosurgery-online.com

8/8/2019 Aggressive Micro Surgical Resection
http://slidepdf.com/reader/full/aggressive-micro-surgical-resection 8/8
COMMENTS
A large series of 74 patients with chordomas who underwent a totalof 121 surgical procedures is presented in this study. With a mean
follow-up period of 96 months, the authors present 12 complicationsafter surgery and two deaths in previously operated and irradiated
patients.Chordomas present a challenging problem for the neurosurgeon.
The biological behavior of chordomas is not uniform, and two patientswith the same diagnosis may have a completely different prognosisindependent of the surgical strategy. In our experience, aggressively
growing chordomas can rarely be completely removed by microsur-gical means, and most will show a large recurrence within 1 year.
These patients will have a fatal outcome, even with repeated surgicalprocedures. Conversely, slow-growing chordomas present a betterprognosis after radical resection of the tumor. The crucial question
when treating the latter group is what amount of morbidity has to betaken into account for a radical resection. In cases of recurrent tumors,we agree with the authors to perform another resection. Afterwards,
radiation therapy should be performed in suspicious regions in which
surgeons could expect a recurrence.Recurrences after surgery and radiation present a difficult and
challenging problem for the neurosurgeon because these cases areprone to develop complications, such as cranial nerve and vascularinjuries. With increased experience, surgical removal of the tumors
can be more complete. In our opinion, we should not perform a radicalresection if it impedes on the patient’s quality of life. In this context,“aggressive” surgical treatments do not entail damaging important
structures, but they do require radical, yet gentle, microsurgical tech-niques.
Wolf LudemannMadjid Samii
Hannover, Germany
Tzortzidis et al. provide an important contribution for defining therole of surgery in the management of cranial base chordomas. The
authors report on a large cohort of 74 patients harboring cranial base
chordomas who underwent aggressive microsurgical resection be-tween 1988 and 2004. There is a long follow-up period (mean, 96 mo;range, 1–198 mo), and the results were unaffected by radiotherapy,
which was given only in two cases. Gross total resection was accom-plished in 53 patients (71.6%), and subtotal resection was accom-plished in 21 patients (28.4%). Twenty-six patients (35%) had recur-
rences after gross total resection. At the 10-year follow-upexamination, 19% of patients were disease free. The average Karnof-sky Performance Scale score was 80 11.7 preoperatively and 86 12.8 at the time of the last follow-up visit in surviving patients.
The authors’ results are comparable to previously reported findingsin which radiotherapy was administered (Table 8), thus supportingaggressive tumor resection to obtain long survival with good func-tional preservation.
The authors report the differences in the biological behavior ofchordomas. The majority are slow growing, some do not grow, and
some rare cases are aggressive, with rapid local recurrence and neuraland /or extra neural metastasis. There is currently no grading systemto define the malignancy of this type of tumor, and, in my opinion,with the absence of similar criteria, aggressive management of chor-domas is mandatory.
Giorgio Frank
Bologna, Italy
This article reports clinical outcome and rates of recurrence in alarge series of 74 patients managed with a consistent strategy of
attempted complete resection and reoperation or radiation for anyresidual tumor. Complete removal was achieved by one or moreoperation in 53 out of 74 patients (71.6%), with an operative mortalityrate of 2.7%. At the time of the last follow-up visit, 35% were alivewith disease, 38% were alive without disease, and 15% had died ofdisease. The median duration of postoperative survival was approx-imately 8 years.
This excellent outcome in a large series supports the authors’ con-tention that their strategy has merit. However, the data do not estab-lish the superiority of this approach compared with the alternatives ofaggressive surgery with postoperative radiation, even if radiograph-ically complete removal is achieved, conservative surgery with post-operative radiation, or either radiotherapy or radiosurgery alone.
Griffith R. Harsh IV
Stanford, California
The authors present a rather extensive cranial base experience in thesurgical treatment of chordomas in 74 patients. The authors note
that, although chordomas may look the same histologically, they may be biologically different and have a different clinical course. Theyclearly indicate the benefit of aggressive surgical resection in themajority of patients, irrespective of the type of tumor. We agree withthe authors that the best chance for a more radical resection is at thefirst surgery. For this reason, patients with the presumptive radiolog-ical diagnosis of chordoma are better served in specialized centers thathave a high volume and experience with these relatively uncommonlesions. It would have been interesting if the authors reported howtheir experience influenced the outcomes by comparing recentlytreated patients with those treated earlier.
Ali F. Krisht
Little Rock, Arkansas
FOLLOW-UP AFTER RESECTION OF CRANIAL BASE CHORDOMAS
NEUROSURGERY VOLUME 59 | NUMBER 2 | AUGUST 2006 | 237