agenda of the board of directors public board · provide valuable feedback and ensure the visits...
TRANSCRIPT

AGENDA OF THE BOARD OF DIRECTORS
PUBLIC BOARD To be held 10:30 - 13:00 on Wednesday 4 December 2019
Ruffwood Suite, Education Centre, Ormskirk Hospital L39 2AZ
V = Verbal D = Document P = Presentation
Ref No. Agenda Item Lead Duration
PRELIMINARY BUSINESS 10:30
TB197/19
(V)
Chair’s welcome & note of apologies
To note the apologies for absence Chair
10
TB198/19
(D)
Declaration of Directors’ Interests concerning
agenda items
To receive declarations of interest relating to
agenda items and/or any changes to the register
of directors’ declared interests
Chair
TB199/19
(D)
Minutes of the Meeting held on 6 November
2019
To approve the minutes of the Public Board of
Directors
Chair
TB200/19
(D)
Matters arising action Logs - Outstanding &
Completed Actions
To review the Action Logs and receive relevant
updates
Chair
TB201/19
(D/V)
(V/P)
Patients and Engagement Issues including:
• NEDs & Executive Visits/Walkabouts:
o NEDs: (verbal)
o Executives: (document/verbal)
• Patient Story:
Chaplaincy and Spiritual Care - the work and achievements from over the last year and its positive impact on the patient experience To receive the Patient Story and note lessons learnt
NEDs EDs
Michelle Kitson/Martin
Abrams
30
STRATEGIC CONTEXT 11:10
TB202/19
(D)
Chief Executive’s Report
To receive key issues and update from the CEO
CEO 10
Pub
lic B
oard
Age
nda
- 4
Dec
19
Page 1 of 210

Ref No. Agenda Item Lead Duration
QUALITY & SAFETY 11:20
TB203/19
(P/D/V)
Quality and Safety Reports:
a) Quality Improvement Plan Update
b) Summary of Complaints & Compliments
c) Learning from Deaths Report (formerly
Monthly Mortality Report)
d) Safe Staffing: Monthly
e) Medical Vacancy Rate: Monthly
f) CQC Inspection Update
To receive the presentation and reports
DoN/MD
30
PERFORMANCE & GOVERNANCE 11:50
TB204/19
(P/D)
Integrated Performance Report (IPR)
To receive the report COO 15
TB205/19
(D)
Financial Position at Month 7, 2019/20
To receive the report
DoF
15
TB206/19
(D)
Risk Management
Corporate Risk Register (CRR)
To receive the monthly reports.
DoN
5
TB207/19
(P/D)
Single Improvement Plan Update (SIP)
To receive the report
DCEO/ DoS
10
TB208/19
(P)
Workforce Directorate Presentation
To receive the presentation
DHR 10
TB209/19
(D)
Charity Update
• Name change for the Charity
• Investment Policy for the Charity
To receive the reports
DoF
ITEMS FOR APPROVAL/RATIFICATION 12:45
TB210/19
(V)
a) Learning Lessons to Improve our
People Practices Report
b) Workforce Disability Equality Standard
Information Report April 2019 – March
2020
c) Workforce Race Equality Standard
Information Report April 2018 – March
2019
Chair
10
Page 2 of 210

To approve the reports
CONCLUDING BUSINESS 12:55
TB211/19
(V)
Questions from Members of the Public
Public 10
TB212/19
(V)
Any Other Business
To receive/discuss any other business not on
the agenda, including items for forward agenda –
8 January 2020
Chair 10
TB213/19 (V)
Message from the Board
• To agree the key messages to be cascaded
throughout the organisation from the Board. Chair
5
TB214/19 (D)
Meeting Evaluation
To give members the opportunity to evaluate the
performance of the Board meeting. Chair 5
TB215/19 (V)
Date and time of next meeting:
10:30, Wednesday 8 January 2020
Seminar Room, Clinical Education Centre,
Southport District General Hospital, PR8 6PN
Chair
13:30
CLOSE
Chair: Neil Masom
ACTIONS REQUIRED:
Approve: To formally agree the receipt of a report and its recommendations OR a particular course of action
Receive: To discuss in depth a report, noting its implications for the Board or Trust without needing to formally approve it
Note: For the intelligence of the Board without the in-depth discussion as above
Assure: To apprise the Board that controls and assurances are in place
For Information: Literally, to inform the Board
Pub
lic B
oard
Age
nda
- 4
Dec
19
Page 3 of 210


1
Re
gis
ter
of
Inte
rests
De
cla
red
by t
he B
oard
of
Dir
ecto
rs 2
01
9/2
0 A
S A
T 1
0 N
OV
EM
BE
R 2
019
N
AM
E
PO
SIT
ION
/RO
LE
D
irecto
rsh
ip,
inc
lud
ing
no
n-
execu
tive
dir
ecto
rsh
ip
he
ld in
pri
vate
co
mp
an
ies o
r P
LC
s (
wit
h t
he
excep
tio
n o
f th
os
e d
orm
an
t co
mp
an
ies)
Ow
ne
rsh
ip, o
r p
art
ow
ners
hip
o
f p
rivate
co
mp
an
ies,
bu
sin
esses o
r co
ns
ult
an
cie
s
likely
or
po
ssib
ly
seekin
g t
o d
o
bu
sin
ess w
ith
th
e N
HS
Ma
jori
ty o
r co
ntr
ollin
g
sh
are
ho
ldin
gs
in
org
an
isati
on
s
likely
or
po
ssib
ly
seekin
g t
o d
o
bu
sin
ess w
ith
th
e N
HS
A p
os
itio
n o
f au
tho
rity
in
a
ch
ari
ty o
r vo
lun
tary
b
od
y in
th
e
field
of
he
alt
h a
nd
so
cia
l care
An
y c
on
ne
cti
on
w
ith
a v
olu
nta
ry
or
oth
er
bo
dy
co
ntr
acti
ng
fo
r N
HS
serv
ices
Rela
ted
to
an
yb
od
y
tha
t w
ork
s
in t
he
Tru
st
Lo
yalt
y:
An
off
icer
wit
h
clo
se t
ies t
o a
d
ecis
ion
m
akin
g
co
lleag
ue
fro
m
an
o
rga
nis
ati
on
w
ho
may s
eek
to d
o b
usin
ess
wit
h t
he T
rust
Oth
er
Date
of
en
try
on
reg
iste
r o
r am
en
dm
en
t
BIR
RE
LL
, M
r J
im
No
n-E
xecu
tive
D
ire
cto
r N
il
Nil
N
il
Nil
N
il
Nil
N
il
Nil
25
S
ep
tem
be
r 2
01
7
BR
ICK
NE
LL
, D
r D
av
id
No
n-E
xecu
tive
Dir
ecto
r
Pil
kin
gto
n
Fa
mil
y T
rus
t S
t J
os
ep
h’s
H
os
pic
e
Th
e W
orl
d o
f G
las
s
Pil
kin
gto
n
Gla
ss
C
oll
ec
tio
n
Nil
N
il
Dir
ec
tor,
S
t J
os
ep
h’s
H
os
pic
e
Dir
ec
tor,
P
ilk
ing
ton
F
am
ily
Tru
st
Dir
ec
tor,
S
t J
os
ep
h’s
H
os
pic
e
Nil
N
il
Nil
9
Ap
ril
201
8
CH
RIS
TIA
N,
M
r S
tev
en
Ch
ief
Op
era
ting
O
ffic
er
Nil
N
il
Nil
N
il
Nil
N
il
Nil
N
il
28
Ju
ne
201
8
CO
SG
RO
VE
M
s J
uli
ett
e
Dir
ecto
r o
f N
urs
ing
, M
idw
ife
ry &
T
he
rapie
s
Nil
N
il
Nil
N
il
Nil
N
il
Nil
N
il
7
May
201
8
TB
198_
19 D
ecla
ratio
ns o
f Int
eres
t Boa
rd o
f Dire
ctor
s 20
19-2
020
- N
ov 1
9
Page 4 of 210

2
NA
ME
P
OS
ITIO
N/R
OL
E
Dir
ecto
rsh
ip,
inc
lud
ing
no
n-
execu
tive
dir
ecto
rsh
ip
he
ld in
pri
vate
co
mp
an
ies o
r P
LC
s (
wit
h t
he
excep
tio
n o
f th
os
e d
orm
an
t co
mp
an
ies)
Ow
ne
rsh
ip, o
r p
art
ow
ners
hip
o
f p
rivate
co
mp
an
ies,
bu
sin
esses o
r co
ns
ult
an
cie
s
likely
or
po
ssib
ly
seekin
g t
o d
o
bu
sin
ess w
ith
th
e N
HS
Ma
jori
ty o
r co
ntr
ollin
g
sh
are
ho
ldin
gs
in
org
an
isati
on
s
likely
or
po
ssib
ly
seekin
g t
o d
o
bu
sin
ess w
ith
th
e N
HS
A p
os
itio
n o
f au
tho
rity
in
a
ch
ari
ty o
r vo
lun
tary
b
od
y in
th
e
field
of
he
alt
h a
nd
so
cia
l care
An
y c
on
ne
cti
on
w
ith
a v
olu
nta
ry
or
oth
er
bo
dy
co
ntr
acti
ng
fo
r N
HS
serv
ices
Rela
ted
to
an
yb
od
y
tha
t w
ork
s
in t
he
Tru
st
Lo
yalt
y:
An
off
icer
wit
h
clo
se t
ies t
o a
d
ecis
ion
m
akin
g
co
lleag
ue
fro
m
an
o
rga
nis
ati
on
w
ho
may s
eek
to d
o b
usin
ess
wit
h t
he T
rust
Oth
er
Date
of
en
try
on
reg
iste
r o
r am
en
dm
en
t
GIB
SO
N,
Mrs
Pa
ulin
e
No
n-E
xecu
tive
D
ire
cto
r D
esig
na
te
D
ire
cto
r;
Ex
ce
l C
oa
ch
ing
&
Co
ns
ult
an
cy
. P
rov
isio
n o
f c
oa
ch
ing
s
erv
ices
to
D
ire
cto
rate
a
nd
sen
ior
NH
S
Ma
na
ge
men
t p
ers
on
nel
Nil
N
il
Nil
N
il
Nil
N
il
25
Ju
ly 2
01
7
GO
RR
Y,
Mrs
Ju
lie
No
n-E
xecu
tive
D
ire
cto
r C
ata
lys
t C
ho
ice
s C
.I.C
.
Nil
N
il
Nil
P
roje
ct
Ad
vis
er:
H
os
pic
e o
f th
e G
oo
d
Sh
ep
he
rd
20
17
to
date
Sp
ec
ialis
t A
dv
ise
r C
QC
2
01
5 to
date
Ma
cm
illa
n
Ca
nc
er
Info
rma
tio
n &
S
up
po
rt
Sp
ec
ialis
t
20
17
to
date
Nil
N
il
NE
D
Re
pre
se
nta
tiv
e
on
th
e N
ort
h
We
st
Co
as
t S
tra
teg
ic
Cli
nic
al
Ne
two
rk f
or
Pa
llia
tive
an
d
En
d o
f L
ife
C
are
9
Ju
ly
20
19
HA
NK
IN
Dr
Te
ren
ce
Me
dic
al D
irecto
r
Nil
N
il
Nil
N
il
Nil
N
il
Nil
N
il
7 J
an
ua
ry
20
19
Page 5 of 210

3
NA
ME
P
OS
ITIO
N/R
OL
E
Dir
ecto
rsh
ip,
inc
lud
ing
no
n-
execu
tive
dir
ecto
rsh
ip
he
ld in
pri
vate
co
mp
an
ies o
r P
LC
s (
wit
h t
he
excep
tio
n o
f th
os
e d
orm
an
t co
mp
an
ies)
Ow
ne
rsh
ip, o
r p
art
ow
ners
hip
o
f p
rivate
co
mp
an
ies,
bu
sin
esses o
r co
ns
ult
an
cie
s
likely
or
po
ssib
ly
seekin
g t
o d
o
bu
sin
ess w
ith
th
e N
HS
Ma
jori
ty o
r co
ntr
ollin
g
sh
are
ho
ldin
gs
in
org
an
isati
on
s
likely
or
po
ssib
ly
seekin
g t
o d
o
bu
sin
ess w
ith
th
e N
HS
A p
os
itio
n o
f au
tho
rity
in
a
ch
ari
ty o
r vo
lun
tary
b
od
y in
th
e
field
of
he
alt
h a
nd
so
cia
l care
An
y c
on
ne
cti
on
w
ith
a v
olu
nta
ry
or
oth
er
bo
dy
co
ntr
acti
ng
fo
r N
HS
serv
ices
Rela
ted
to
an
yb
od
y
tha
t w
ork
s
in t
he
Tru
st
Lo
yalt
y:
An
off
icer
wit
h
clo
se t
ies t
o a
d
ecis
ion
m
akin
g
co
lleag
ue
fro
m
an
o
rga
nis
ati
on
w
ho
may s
eek
to d
o b
usin
ess
wit
h t
he T
rust
Oth
er
Date
of
en
try
on
reg
iste
r o
r am
en
dm
en
t
CO
SG
RO
VE
M
rs J
ulie
tte
Dir
ecto
r o
f N
urs
ing
, M
idw
ife
ry a
nd
T
he
rapie
s
Nil
N
il
Nil
N
il
Nil
N
il
Nil
G
ov
ern
or
–
So
uth
po
rt
Co
lle
ge
04
Oc
tob
er
20
19
MA
SO
M
Mr
Ne
il
Ch
air
ma
n &
Non
- E
xe
cu
tive
Dir
ecto
r In
du
str
ial &
F
ina
nc
ial
Sy
ste
ms (
IFS
) A
B
ND
LM
Ltd
J
SS
H L
td
CQ
C H
old
ing
s
Ltd
(m
an
ufa
ctu
rer
of
textile
p
rod
ucts
)
Nil
N
il
Nil
N
il
Nil
N
il
9 J
uly
2
01
9
PA
TT
EN
, M
s T
he
res
e
Acting
Ch
ief
Exe
cu
tive
/Dir
ecto
r o
f S
tra
teg
y
Nil
N
il
Nil
N
il
Nil
N
il
Nil
T
rus
tee
-
Bla
ck
bu
rn
Ho
us
e G
rou
p
3 O
cto
be
r 2
01
5
RO
YD
S,
Mrs
Jan
e
Dir
ecto
r o
f H
um
an
Re
so
urc
es
Nil
N
il
Nil
N
il
Nil
N
il
Nil
V
ice
Ch
air
of
Go
ve
rno
rs,
Fa
rnb
oro
ug
h
Ro
ad
Ju
nio
r S
ch
oo
l,
So
uth
po
rt
25
S
ep
tem
be
r 2
01
7
SH
AN
AH
AN
, M
r S
tev
e
Dir
ecto
r o
f F
ina
nce
Nil
N
il
Nil
N
il
Mr
Sh
an
ah
an
’s
bro
the
r, M
r P
ete
r S
ha
na
han
is
a
n E
xe
cu
tiv
e
Dir
ec
tor,
A
dv
iso
ry o
n
the
Ern
st
&
Yo
un
g A
&E
P
erf
orm
an
ce
Imp
rov
em
en
t P
roje
ct
at
So
uth
po
rt &
Nil
N
il
Tru
ste
e –
Ag
e
Co
nc
ern
4
Oc
tob
er
20
19
TB
198_
19 D
ecla
ratio
ns o
f Int
eres
t Boa
rd o
f Dire
ctor
s 20
19-2
020
- N
ov 1
9
Page 6 of 210

4
NA
ME
P
OS
ITIO
N/R
OL
E
Dir
ecto
rsh
ip,
inc
lud
ing
no
n-
execu
tive
dir
ecto
rsh
ip
he
ld in
pri
vate
co
mp
an
ies o
r P
LC
s (
wit
h t
he
excep
tio
n o
f th
os
e d
orm
an
t co
mp
an
ies)
Ow
ne
rsh
ip, o
r p
art
ow
ners
hip
o
f p
rivate
co
mp
an
ies,
bu
sin
esses o
r co
ns
ult
an
cie
s
likely
or
po
ssib
ly
seekin
g t
o d
o
bu
sin
ess w
ith
th
e N
HS
Ma
jori
ty o
r co
ntr
ollin
g
sh
are
ho
ldin
gs
in
org
an
isati
on
s
likely
or
po
ssib
ly
seekin
g t
o d
o
bu
sin
ess w
ith
th
e N
HS
A p
os
itio
n o
f au
tho
rity
in
a
ch
ari
ty o
r vo
lun
tary
b
od
y in
th
e
field
of
he
alt
h a
nd
so
cia
l care
An
y c
on
ne
cti
on
w
ith
a v
olu
nta
ry
or
oth
er
bo
dy
co
ntr
acti
ng
fo
r N
HS
serv
ices
Rela
ted
to
an
yb
od
y
tha
t w
ork
s
in t
he
Tru
st
Lo
yalt
y:
An
off
icer
wit
h
clo
se t
ies t
o a
d
ecis
ion
m
akin
g
co
lleag
ue
fro
m
an
o
rga
nis
ati
on
w
ho
may s
eek
to d
o b
usin
ess
wit
h t
he T
rust
Oth
er
Date
of
en
try
on
reg
iste
r o
r am
en
dm
en
t
Orm
sk
irk
H
os
pit
al
Tru
st.
SIN
GH
, M
r G
urp
ree
t N
on
-Execu
tive
Dir
ecto
r N
il
GS
Uro
log
y
Ltd
: p
rov
idin
g
pra
cti
ce
&
G
MC
wo
rk
Nil
N
il
Pri
va
te
pra
cti
ce
at
Ra
ms
ay
H
ea
lth
M
em
be
r o
f th
e
Me
dic
al
Ed
uc
ati
on
C
ha
rity
at
So
uth
po
rt &
O
rms
kir
k
Ho
sp
ita
l N
HS
T
rus
t
Nil
N
il
Nil
9
Ap
ril
201
8
6
No
ve
mb
er
20
19
Page 7 of 210

1
Minutes of the Public Section of the Board of Directors’ Meeting
Wednesday, 6 November 2019
Seminar Room, Clinical Education Centre, Southport Hospital (Subject to the approval of the Board on 4 Dec 2019)
Members Present
Mr J Birrell, Non-Executive Director
Mr D Bricknell, Non-Executive Director
Mrs J Cosgrove, Executive Director of Nursing,
Midwifery & Therapies
Mrs J Gorry, Non-Executive Director
Mrs T Patten, Acting Chief Executive / Executive
Director of Strategy
Mr S Shanahan, Executive Director of Finance
Mr G Singh, Non-Executive Director
In Attendance
Mr S Christian, Chief Operating Officer
Mrs A Davenport, Interim Associate Director for Corporate Governance
Mr T Ellis, PR & Communications Manager
Mrs P Gibson, Non-Executive Director Designate
Mrs C Griffiths, NHSE/I Improvement Director
Mrs A Marshall, PA to the Chief Executive & Chair
Mrs J Royds, Director of Human Resources & Organisational Development
Apologies:
Dr T Hankin, Executive Medical Director
Neil Masom, Chair
AGENDA
ITEM
ACTION LEAD
PRELIMINARY BUSINESS
TB180/19 Chair’s Welcome and Note of Apologies
Mr Birrell opened the meeting by welcoming members of the public who were in attendance. He reminded them that although this is a meeting held in public it is not a public meeting. Therefore he would give those in attendance an opportunity to ask questions at the end of the meeting. Apologies noted from Mr Masom, Dr Hankin and Mrs Roberts.
TB181/19 Declaration of Directors’ Interests Concerning Agenda Items
The Chair asked that members declare any interests in relation to the agenda items and asked that any changes or additions to the Register of Interests declared by the Board of Directors should be submitted to the Company Secretary. Mr Singh confirmed that he had been asked to become a member of
TB
199_
19 D
RA
FT
Pub
lic T
rust
Boa
rd M
inut
es 6
Nov
19
Page 8 of 210

2
the Medical Education Charity at Southport & Ormskirk Hospital NHS Trust.
TB182/19 Minutes of the Meeting Held On 6 March 2019
The minutes of the meeting held on 2 October were agreed as a correct record and were approved. . RESOLVED: The Board approved the minutes as an accurate record.
TB183/19 Matters Arising Action Log
The Board considered the following matters arising in turn: January 2019, Min No. TB028/19 Monthly Mortality Report/External Mortality Review Dr Hankin to provide a progress update to provide Board assurance. September 2019, Min No. TB149/19 Quality Improvement Plan Awaiting final CQC report
MD
DON
TB184/19 Patient and Engagement Issues including:
• NEDs & Executive Visits/Walkabouts
• Patient/Staff Story: Surgical Assessment Unit – How they improved the patient journey
NEDs & Executive Visits/Walkabouts Mrs Gorry & The Director of Finance had visited Spinal Injuries Unit (SIU)on 23 October. The SIU had recently been refurbished following the Klebsiella outbreak. The visit went well with engaging feedback from the staff, who were proud of the patient centred team, the standard of work and care and the comprehensive induction programme in place. It was noted however the staff on SIU felt frustrated with overall communications which came from the management team of the hospital and were unsure how they fitted into the strategic plans for the future. There are elements of the IT systems which do not align. Some of the staff felt the profile of SIU should be raised and run as a separate Clinical Business Unit (CBU). There was a suggestion to link the NEDs with designated wards. The Acting Chief Executive & Director of Strategy will provide a summary of actions from the NED and Executive visits which would provide valuable feedback and ensure the visits are viewed as a meaningful exercise. It was noted that both the Chief Operating Officer and the Director of
Nursing, Midwifery & Therapies were providing support and visibility around the wards during this period of overwhelming demand. The Director of Human Resources & Operational Development confirmed there were dates in the diary for her and Gurpreet Singh to arrange ward visits during the next couple of months. Back to the floor visits for all of the Executive Team were also being arranged. Patient/Staff Story: Surgical Assessment Unit – How they improved the patient journey The Board were apprised of the background of the opening of the
Page 9 of 210

3
Surgical Assessment Unit (SAU). The SAU was 18 months in the planning and opened in October 2018. It is a purpose built area for ambulatory patients who require surgical review. The process of embedding the new service into practice has taken 12 months. There were some initial teething issues but these have now been resolved. The aim of the unit is to reduce avoidable admissions. Some of the achievements to date include: ➢ March 2019 - Cohort 4 NHS Elect Programme: Trust
commitment to best practice and developing ambulatory models of care. The team have been asked to coach Cohort 5 and asked to share their data template
➢ May - Acute Abdomen Pathway formalised
➢ June - Pilot of Hot clinic
➢ July - Formalisation of Standard Operating Policy for Hot Clinic and Ward Attender Referral Process
The work continues to provide excellent safe and appropriate care. Improvements to service provision adapt in relation to feedback received. There is further work underway with NHS Elect to ringfence the unit and increase revenue from Best Practice Tariff. There had been some HRG coding issues which had indicated under-costing however this issue has been resolved and should be reflected in the August data. The staff on SAU are very proud of this service and are looking forward to the future development of the unit. The next 12 months will be looking at developing a 7 day service.
Patient Story – Sally’s Story
The outcome from Sally’s story was very positive. Sally had given
permission to use both her story and her name. Following a 3 year
history of a cyst to her back Sally’s GP referred her to SAU for
assessment. As a result of the review Sally was listed by the
Surgeon for same day ‘see and treat’. This process allowed Sally to
attend the hospital on the morning of her procedure. Her husband
who required a carer was able to attend with her and was looked
after by the staff on duty. The procedure was completed and Sally
was discharged home. There was no capacity within the
Community to provide a wound check the following day so Sally
returned to the unit for wound care and no follow up appointment
was required.
Mr Birrell thanked Gemma for attending the meeting offered his praise for the development of the service and encouraged Board members to visit the area. The Chief Operating Officer praised Gemma and her team for their hard work and dedication noting that Gemma was an exemplar colleague.
RESOLVED: The Board received the presentation and noted the excellent progress being made
STRATEGIC CONTEXT
TB1850/19 Chief Executive’s Report
TB
199_
19 D
RA
FT
Pub
lic T
rust
Boa
rd M
inut
es 6
Nov
19
Page 10 of 210

4
The Chief Executive’s Report was presented to the Board, with key issues being highlighted as follows: ➢ Ormskirk hospital is the key to winter planning.
The Trust plans to make better use of the excellent facilities at Ormskirk hospital following extensive clinical consultations.
➢ Visit by the Secretary of State for Health and Social Care Matt Hancock, the Secretary of State for Health and Social Care, visited Southport hospital visited the Trust on 9 October. He was visiting at the invitation of Southport MP Damien Moore.
➢ Time to Shine Awards Nearly 250 staff and guests gathered at Formby Hall Golf Resort and Spa last month to celebrate our annual staff awards, the Time to Shine Awards. Congratulations to be offered to the Time to Shine winners and moninees.
➢ Bed reopening in Spinal Injuries Centre North West Regional Spinal Injuries Centre at Southport hospital has begun to reopen after closing to admissions in the summer following an increase in the incidence of patients colonised with the Klebsiella bacteria.
➢ Flu Campaign at week 5 – 73% ➢ Winter Plan approved at Private Board subject to a
clinical conversation. ➢ Electronic Medical Prescribing.
£700k funding approved to support implementation of Electronic Medical Prescribing, this is a major investment into IT systems it is hoped this will be mobilised by the beginning of January 2020.
RESOLVED: The Board noted the report.
QUALITY & SAFETY
TB186/19 QUALITY & SAFETY REPORTS
The key issues from the 5 comprehensive reports provided in relation to this agenda item (Summary of Complaints & Compliments, Learning from Deaths Report (formerly Monthly Mortality Report), Quality Improvement Plan, Safe Staffing, CQC update, and Freedom to Speak Up Quarterly Update and Relaunch of Strategy) were highlighted in a presentation to the Board, as follows: Quality Improvement Priorities Complaints & Compliments This month’s report shows a breakdown of the number of compliments, complaints and concerns received for the month of September and the improvements now in place following the closure of complaints in August. It was noted the number of complaints and concerns had appeared to stabilise, however plans to address the backlogs will be managed by the newly appointed Deputy Directors of Nursing.
Action: Director of Nursing, Midwifery & Therapies By: January Board
Learning from Deaths Report (formerly Monthly Mortality
Page 11 of 210

5
Report) It was noted the Monthly Mortality Report to the Board is now a
Learning from Deaths Report. In April the HSMR increased to 118
from 82.8 the previous month. There had been no significant spikes
in any disease specific areas and the main primary diagnoses of
these patients were similar to previous months. Fortnightly Mortality
Meetings are now in place to support the delivery of a responsive
and learning approach to the screening of deaths.
Mortality Screening Following a review of the process the screening rate has shown an
improvement. Structured Judgement Reviews and potential
avoidance of death reviews are in place. There are still a
percentage of patients receiving poor care. Director of Nursing,
Midwifery & Therapies noted these cases would be managed
through the Mortality Operational Group and the themes would be
consolidated.
Quality Improvement Plan Training is being delivered on the Older Peoples Care Training
Programme to include Nutrition, Hydration & Mouth Care, Dementia
& Delirium, Continence, End of Life Care, Falls, Care of the
Deteriorating Patient, Infection Prevention and Control (IPC) and
Medicines Management. There are some issues around nutrition
due to the lack of ability to release Dietitians from clinical duties in
the absence of a Dietetic lead. The Falls Strategy is being
developed with a view to launch in November. A new Neck of
Femur (NOF) Pathway has been approved and will be reviewed and
audited.
IPC Update
The Team is working across the Community in conjunction with
AQUA. There is a focus on reducing antimicrobial use. The C.Diff
target is more challenging this year due to a change in how cases
are attributed to the Trust. There had been an MRSA bacteraemia
in August which was the first one in almost 2 years and was a result
of cannulation, relevant learning identified. To date there have been
3 cases of flu but no transmission noted and a table top exercise
has been completed. Klebsiella outbreak on Spinal Injuries Unit had
been handled effectively.
Medicines Management
Following the issues raised by the CQC and the information
provided by the Model Hospital Team which identified the
department was under resourced a Business Case for additional
staffing had been completed and was approved at Private Board on
6 November 2019.
Safe Staffing There has been an overall improvement to the fill rate which is as a result of an increase in the number of allocate on arrival shifts which attract an enhanced rate. There have been a number of recruitment events but the Trust is only just managing to maintain
Comms
TB
199_
19 D
RA
FT
Pub
lic T
rust
Boa
rd M
inut
es 6
Nov
19
Page 12 of 210

6
safe staffing levels. The Trust has one of the highest vacancy rates across Cheshire & Merseyside. International recruitment is a consideration. There is no central point for the management of medical vacancies and these are managed within the individual CBUs. The Executive Medical Director will be asked to provide a paper update to the Board which will provide details of the medical vacancy rate across the Trust, it was noted this would be a complex piece of work and would require discussion at Workforce Committee.
Action: Executive Medical Director By: December Board
Improving Criteria Led Discharge Important for the Trust to ensure there are nurses available to support Criteria Led Discharge, work is progressing in this area but not something that will be fully established this year. The Red to Green multi-disciplinary approach will also support patient flow. CQC Update The Trust received the draft report for factual accuracy checking on 8 October 2019 the Quality Team worked with the Core Service leads to identify any inaccuracies and the report was returned by the deadline 29 October 2019. The CQC have been asked to consider amendment to some key ratings. The date for official publication of the report is yet unclear due to the process of Purdah. Freedom to Speak Up Quarterly Update During October the Freedom To Speak Up Champions engaged in different activities, plans for November include drop-in sessions to recruit more Champions. It had been noted within the Freedom To Speak Up Index Report that the Trust had been listed in the bottom 10 but there was no indication as to why this is the case. Martin Abrams is meeting with the Regional Liaison Lead for the North West to discuss the potential to ‘buddy up’ with an organisation which has shown improvement. RESOLVED: The Board received the Complaints & Compliments Report, the Learning from Deaths Report (formerly Monthly Mortality Report) and the Monthly Safe Staffing Report and was assured by the Quality Improvement Report and the CQC Preparation Update
PERFORMANCE & GOVERNANCE
TB187/19 Assurance & Performance
INTEGRATED PERFORMANCE REPORT The Chief Operating Officer provided an overview of this report which identified an improvement of 31 indicators and a deterioration of 24. Key areas: 12 hour DTA breaches 5 declared for the month of September 4 of which were attributed to patient flow and 1 a delay in securing a mental health bed. Assurance given that all patients did receive senior review during this time. Currently showing as an outlier for the region which is also bringing scrutiny from the Regulators.
Page 13 of 210

7
RTT Remains above the 92% target however performance is currently being impacted by anaesthetics and various workforce issues. C.Diff Mr Birrell asked for clarification of the Trust target as there appeared to be conflicting information within the description and narrative columns.
Action: Executive Medical Director By: December Board
Friends & Family Test Performance has shown a significant deterioration in comparison to the previous month. LOS Interventions in place are showing an improvement, with continued work around embedding the Home First solution.
Theatre Productivity July – September 2019 showed an improvement of 5%
Agency Staff Costs continue to remain high due to the reliance on agency staff to provide safe patient care in both medical and nursing areas. The Director of Human Resources & Organisational Development noted there are 4 consultant panel interviews taking place over the next 3 weeks and there have recently been 3 appointments within the Anaesthetics Department which is a positive step.
Diagnostic Waits There was a demonstrable improvement for the third month in a row however Radiology and Endoscopy are key services which are impacting on performance. The Trust has improvement plans in place to address the issues. Mr Birrell noted that the sickness rate was currently at the lowest level for some time however the staff turnover rate was the highest. The Director of Human Resources & Organisational Development advised there was a focused piece of work underway looking at staff retention issues. For noting there are currently over 450 recruitment opportunities in various stages of progression. The Executive Assurance Reports were noted. RESOLVED: The Board received the IPR
TB188/19 Financial Position at Month 6, 2019/20
The report for month 6 of 2019/20 was received and noted by the Board. The Director of Finance noted the Trust had delivered the Quarter 2 plan and assured the Board that accounting adjustments had been made in conjunction with the Regulators. However he noted the financial position was set to get more challenging in the forthcoming months. The Trust currently has an unmitigated risk of £5m to the delivery of the control total. Agency spend had increased to above £1m which is a significant risk heading into
TB
199_
19 D
RA
FT
Pub
lic T
rust
Boa
rd M
inut
es 6
Nov
19
Page 14 of 210

8
winter. The use of Thornbury Agency has reduced but there was still a reliance on Tier 2 nursing agency and an increase in the use of allocate on arrival which is paid at an enhanced rate. RESOLVED: The Board received the report
TB189/19 Risk Management: Risk Register
The Risk Management Risk Register was received and noted by the Board. A more detailed discussion took place relating the following risks:
• Risk 1688 – Inadequate Staffing Levels in Anaesthetic Department. This is for discussion at Risk & Compliance Group to consider the potential to reduce the risk score.
• Risk 2056 – Lost to Follow Up. Work continues following the identification of a number of individual incidents where patients were not on the RTT pathway. 98% of pathways closed down the remaining 2% required clinical review following which they were also closed down. Comprehensive overview will take place at the next Quality & Safety Committee.
RESOLVED: The Board received the Risk Register report.
OTHER REPORTS FOR RECEIVING
TB190/19 SINGLE IMPROVEMENT PLAN UPDATE (SIP)
The Board received the Single Improvement Plan Board update. The Acting Chief Executive & Director of Strategy advised that following a recent Southport & Ormskirk Improvement Board the Trust had been asked to review the detail contained within the narrative of the assurance reports to ensure a clear and comprehensive progress update was provided. Business Planning Session arranged for 7 November to agree quality and operational priorities for next year. The outline Pre Consultation Business Case has been completed and unlikely to be circulated until after the General Election on 13 December. RESOLVED: The Board received the paper.
TB191/19 ITEMS FOR APPROVAL/RATIFICATION
a) To ratify the decision taken under Emergency Powers Section 4.3 of the Standing Orders on 25 October 2019 to approve application for an uncommitted Revenue Support Loan for November 2019
RESOLVED: The Board noted and approved the request.
CONCLUDING BUSINESS
TB192/19 Questions from Members of the Public
Ms Wright - Could the Trust confirm where the company was based that covered the out-sourcing of Radiology.
Page 15 of 210

9
There being no other business, the meeting was adjourned
In view of the high numbers of vacancy rates especially within Radiology the Trust had developed a solution to ensure the timely review of patient assessments was provided. The service has been outsourced via the national framework to Telemedicine who are an internationally based company with their head office in Australia. Ms Wright - Clarity around Criteria Led Discharge Juliette Cosgrove, Director of Nursing advised that the Multi-Disciplinary Team decides a criteria for discharge for individual patients and when this is met then the patient can go home. This is normally led by a nurse. This process is designed to prevent discharge delays when Therapies are required. It is not an alternative to using doctors.
TB193/19 ANY OTHER BUSINESS
To receive/discuss any other business not on the agenda.
TB194/19 Message from the Board
Messages which the Board wished to communicate to the wider Trust were:
• SAU – Spotlight on positive achievements
• Thank you - Time to Shine award winners and nominees
• More patients treated – less Theatres used
• Achievement of Quarter 2 Finance Plan
• EPMA Funding
• Approval of Winter Plan Business Case
• Sickness at lowest level since September 2014
Communications
TB195/19 Meeting Evaluation
To give members the opportunity to evaluate the performance of the Board meeting
• Clear presentations to support discussions
• Willingness to respond to questions
• Would be helpful if Board members introduced themselves
• Page direction would be helpful
• Time Management of meeting – some items rushed, insufficient time to cover items
TB196/19 DATE, TIME AND VENUE OF THE NEXT MEETING
Wednesday 4 December 2019, 10:30am Ruffwood Suite, Education Centre, Ormskirk District General Hospital
TB
199_
19 D
RA
FT
Pub
lic T
rust
Boa
rd M
inut
es 6
Nov
19
Page 16 of 210

10
Board Attendance 2019/20
Members Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Neil Masom (Chair) ✓
Jim Birrell ✓
David Bricknell ✓
Ged Clarke ✓
Juliette Cosgrove ✓
Julie Gorry ✓
Terry Hankin ✓
Silas Nicholls ✓
Therese Patten ✓
Steve Shanahan ✓
Gurpreet Singh A
In Attendance Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Pauline Gibson ✓
Audley Charles ✓
Steve Christian ✓
Jane Royds ✓
A = Apologies ✓ = In attendance
Page 17 of 210

Pu
blic
Bo
ard
Mat
ters
Ari
sin
g A
ctio
n L
og
as a
t 6
No
vem
be
r 2
01
9
1
OU
TS
TA
ND
ING
AC
TIO
NS
A
ge
nd
a
Re
f M
ee
tin
g
Da
te
Ag
en
da
Ite
m
Ag
reed
Ac
tio
n
L
ead
O
rig
ina
l D
ea
dli
ne
F
ore
ca
st
Co
mp
leti
on
S
tatu
s O
utc
om
es
B
RA
G
ST
AT
US
TB
02
8/1
9
Ja
n
2019
M
on
thly
Mo
rta
lity
R
ep
ort
, in
clu
din
g
a s
um
ma
ry r
ep
ort
o
f th
e E
xte
rna
l M
ort
ali
ty R
ev
iew
Th
e
15
0
ca
se
s
revie
we
d
ha
d
ide
ntifie
d
11
ke
y
reco
mm
en
da
tio
ns
and
se
ve
n
ca
se
s
of
ve
ry p
oo
r ca
re.
Fro
m
a
qu
alit
y
pers
pective
, th
e
Bo
ard
sh
ou
ld
rece
ive
fu
rth
er
assu
ran
ce
if
the
a
ctio
ns
agre
ed
a
nd
th
e t
ime
line t
o
ach
ieve
th
ose
w
ere
id
en
tifie
d
MD
M
ay
2019
Ju
l 2019
M
arc
h 2
01
9
Dr
Ha
nkin
an
d D
r G
od
dard
to
re
vie
w t
ime
line
an
d
upd
ate
Tru
st
Bo
ard
M
ay
201
9
On
tra
ck t
o b
e c
om
ple
ted b
y J
uly
201
9
No
vem
be
r 2
01
9
Re
vie
we
d m
on
thly
as p
art
of M
ort
alit
y O
pera
tio
na
l G
roup
(M
OG
).
B
LU
E
BR
AG
Sta
tus
Key
Red
Sig
nific
antly d
ela
yed a
nd/o
r of hig
h r
isk
Am
be
r S
lig
htl
y d
ela
yed
an
d/o
r o
f lo
w r
isk
Gre
en
P
rog
ressin
g o
n s
ch
ed
ule
Blu
e
Co
mp
lete
d
TB
200_
19 M
atte
rs A
risin
g P
ublic
Boa
rd N
ov fo
r D
ec 1
9
Page 18 of 210

Pu
blic
Bo
ard
Mat
ters
Ari
sin
g A
ctio
n L
og
as a
t 6
No
vem
be
r 2
01
9
2
B
oard
aw
aitin
g
co
nfirm
atio
n t
hat
all
actio
ns h
ave
b
ee
n c
om
ple
ted.
MD
M
ay
2019
D
ec
2019
O
cto
be
r U
pd
ate
: D
r H
ankin
to
mee
t w
ith
Dr
Go
dd
ard
/Mrs
Po
we
r/M
rs
Flo
od
-Jo
nes t
o s
ign o
ff E
xte
rna
l M
ort
alit
y R
evie
w
(RA
M)
Pro
ject.
N
ov
em
be
r U
pd
ate
: M
ee
tin
g w
as h
eld
on
10
th
Octo
be
r 2
01
9.
Th
e E
xte
rna
l M
ort
alit
y B
oard
A
ssu
ran
ce
Re
port
(E
MB
AR
) A
ctio
n P
lan
un
derw
en
t a
fu
ll re
vie
w.
De
cem
be
r 2
01
9
Dr
Ha
nkin
to
giv
e a
pro
gre
ss u
pd
ate
to
pro
vid
e
Bo
ard
assu
ran
ce
GR
EE
N
TB
14
9/1
9
Se
pt
2019
Q
ua
lity
Im
pro
vem
en
t P
lan
T
o
un
dert
ake
a
m
ap
pin
g
exe
rcis
e
to
cla
rify
w
here
a
nd
how
all
are
as
for
imp
rove
me
nt
are
b
ein
g
add
resse
d
an
d
ensu
re
focu
s
on
co
ntin
ua
l im
pro
ve
me
nt
will
b
e m
ain
tain
ed
Do
N
Oct
2019
D
ec
2019
O
cto
be
r U
pd
ate
: M
ap
pin
g u
nde
rwa
y,
pe
ndin
g r
esu
lts o
f C
QC
in
sp
ectio
n r
epo
rt,
wh
ich
ma
y p
ossib
ly r
eq
uire
re
co
nsid
era
tio
n
No
vem
be
r U
pd
ate
: A
wa
itin
g f
ina
l C
QC
re
port
D
ec
em
be
r U
pd
ate
:
GR
EE
N
TB
17
4/1
9
Oct
2019
It
em
s f
or
Ap
pro
va
l o
r R
ati
fic
ati
on
L
ea
rnin
g L
esso
ns t
o
Impro
ve
our
Pe
ople
P
ractice
s
Re
po
rt
(Do
HR
)
All
thre
e r
ep
ort
s
are
to
be r
etu
rne
d
to th
e B
oard
in
a
more
use
r fr
ien
dly
fo
rma
t, t
o in
clu
de
a
n E
xe
cu
tive
S
um
mary
Do
HR
O
ct
2019
D
ec
2019
GR
EE
N
Wo
rkfo
rce
Dis
ab
ility
E
qu
alit
y
Sta
nd
ard
In
form
atio
n
Re
po
rt
Ap
ril
201
9 – M
arc
h
202
0 (
Do
HR
)
Do
HR
O
ct
2019
D
ec
2019
GR
EE
N
Page 19 of 210

Pu
blic
Bo
ard
Mat
ters
Ari
sin
g A
ctio
n L
og
as a
t 6
No
vem
be
r 2
01
9
3
Wo
rkfo
rce
R
ace
E
qu
alit
y
Sta
nd
ard
In
form
atio
n
Re
po
rt
Ap
ril
201
8 – M
arc
h
201
9 (
Do
HR
)
Do
HR
O
ct
201
9
De
c
2019
GR
EE
N
TB
18
6/1
9
No
v
20
19
Q
ualit
y
&
Sa
fety
R
ep
ort
s
Co
mp
lain
ts
&
Co
mp
limen
ts
Pro
vid
e a
n u
pd
ate
to
th
e B
oard
on
resp
on
se
tim
es f
or
co
mp
lain
ts
DO
N
Ja
n
2020
Ja
n
2020
GR
EE
N
TB
18
6/1
9
No
v
2019
Q
ualit
y
&
Sa
fety
R
ep
ort
s
Sa
fe S
taff
ing
Pa
pe
r to
th
e
Bo
ard
wh
ich
will
p
rovid
e d
eta
ils o
f m
ed
ica
l va
ca
ncy
rate
acro
ss t
he
T
rust
MD
D
ec
2019
D
ec
2019
D
ec
em
be
r U
pd
ate
:
TB
200_
19 M
atte
rs A
risin
g P
ublic
Boa
rd N
ov fo
r D
ec 1
9
Page 20 of 210

Pu
blic
Bo
ard
Mat
ters
Ari
sin
g A
ctio
n L
og
as a
t 6
No
vem
be
r 2
01
9
4
CO
MP
LE
TE
D A
CT
ION
S
Ag
en
da
R
ef
Mee
tin
g
Da
te
Ag
en
da
Ite
m
Ag
reed
Ac
tio
n
L
ead
O
rig
ina
l D
ea
dli
ne
F
ore
ca
st
Co
mp
leti
on
S
tatu
s O
utc
om
es
B
RA
G
ST
AT
US
TB
18
7/1
9
No
v
2019
In
tegra
ted
Pe
rfo
rma
nce
R
ep
ort
C.D
iff
Tru
st
Ta
rge
t
Cla
rifica
tio
n o
f th
e
Tru
st
targ
et
16 o
r 36
MD
D
ec
2019
D
ec
2019
D
ec
em
be
r U
pd
ate
:
An
nu
al T
rus
t ta
rge
t is
16 –
IP
R a
me
nd
ed
B
LU
E
Page 21 of 210

PUBLIC TRUST BOARD 4 DECEMBER 2019
Agenda Item TB202/19 Report Title Acting Chief Executive report
to Board
Executive Lead Acting Chief Executive
Lead Officer
Action Required
(Definitions below)
To Approve ✓ To Note
To Assure To Receive
For Information
Executive Summary
• Care Quality Commission report published
• £1.4m investment in electronic prescribing
• Further improvement is mortality performance
• CQC Children’s and young people’s survey
• Honorary professorship for Dr May Ng
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
Strategic Objective Principal Risk
✓ SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
✓ SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
✓ SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
✓ SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
✓ SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
✓ SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
If the system does not have an agreed acute services strategy it may lead to non-alignment of partner organisations plans resulting in the inability to develop and deliver sustainable services
TB
202_
19 F
S C
EO
Rep
ort D
ec 1
9
Page 22 of 210

Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
✓ Caring Statutory Requirement
✓ Effective Annual Business Plan Priority
✓ Responsive Best Practice
✓ Safe Service Change
✓ Well Led
Impact (is there an impact arising from the report on any of the following?)
Compliance Legal
✓ Engagement and Communication Quality & Safety
Equality Risk
Finance Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Board/Committee/Group)
N/A
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
GUIDE TO ACTIONS REQUIRED (TO BE REMOVED BEFORE ISSUE):
Approve: To formally agree the receipt of a report and its recommendations OR a particular course of action
Receive: To discuss in depth a report, noting its implications for the Board or Trust without needing to formally approve
Note: For the intelligence of the Board without the in-depth discussion as above
Assure: To apprise the Board that controls and assurances are in place
For Information: Literally, to inform the Board
Page 23 of 210

ACTING CHIEF EXECUTIVE’S REPORT TO BOARD – December 2019 Care Quality Commission report published Improvements to care and leadership were recognised in the Trust’s latest Care Quality Commission report published on 29 November. It was our first full inspection since November 2017.
Across many of the Trust’s services, the inspectors found staff to be kind, treated people with compassion and respected their privacy and dignity.
They said leaders were approachable, experienced and capable, and were helping staff to develop their skills. There was active engagement between patients, staff and leaders alongside external stakeholders and equality groups to further develop collaboration and improve services.
Eight areas of inspection were rated as improving: six at Southport hospital in urgent and emergency care, surgery and end of life care, and two in the children’s and young people’s services at Ormskirk.
End of life care and Sefton Sexual Health were both rated “good”. This is the first time they have been inspected as individual services. Overall the Trust remains rated “requires improvement”.
The report reflects the significant progress the Trust is making. While we recognise there is still much work to do, it also shows us on track to meet our ambition of being rated “good” by 2020.
“I want to thank all our staff for their dedication and hard work that made these improvements to patient care possible.”
£1.4m investment in electronic prescribing Our staff will move away from handwritten prescriptions next year thanks to a £1.4m investment in electronic prescribing. The Department of Health will give £700,000 to make the scheme possible. The new system will be provided by our existing electronic patient record provider and interface with the pharmacy system. Electronic prescribing will be phased in over 18 months with the first areas going live by the early summer. Working this way saves time and benefits patients by:
• Reducing medication errors by up to 30% compared with paper systems • Ensuring fast access to potentially lifesaving information on prescribed
medicines • Building up a complete, single electronic record to reduce duplication of
information-gathering
TB
202_
19 C
EO
Rep
ort D
ec 1
9
Page 24 of 210

Electronic prescribing will also mean information about patients’ medicines can be more easily and reliably shared between all the clinical professionals a patient comes into contact with, including general practitioners. Further improvement is mortality performance I am pleased to report the latest national figure for SHMI, the Standardised Hospital Mortality Indicator, showed the Trust performing better than expected at 99.62.
SHMI is the ratio between the actual number of patients who die following hospitalisation and number who would be expected to die on the basis of average England figures. It also includes deaths in hospital and deaths 30 days after discharge.
The result is particularly pleasing given the Trust was a national outlier for SHMI less than a year ago. It is also a tribute to the dedication, commitment and hard work of staff across organisation that we have made such a dramatic improvement to patient care.
The fall reflects a rapid decline in the other national mortality indicator, HSMR (Hospital Standardised Mortality Ratio), which tracks the ratio of observed to expected deaths.
CQC Children’s and young people’s survey The latest Care Quality Commission (CQC) children and young people’s survey shows what our patients already know – we have a great team caring for children at Ormskirk hospital. One hundred and fifty-three patients responded to the annual national survey. It found the children’s team provided care that was as good or better than the other trusts surveyed. Staff introducing themselves to patients, giving them sufficient privacy and explaining procedures were particularly noted in the survey. Honorary professorship for Dr May Ng Congratulations to Dr May Ng who has been awarded the title of Honorary Associate Professor from the University of Liverpool. This is in recognition of her commitment to reduce variation in care for diabetes and her outstanding delivery of education and training in paediatric endocrinology and diabetes. Dr Ng, a Consultant Paediatrician who is Associate Medical Director for Specialist Services, has received numerous national awards for her leadership roles and has a wide research portfolio of more than 120 publications as well a best-selling book, A Journey With Brendan, documenting an autism journey with her son. Page 25 of 210

In brief … Chief Executive. Trish Armstrong-Child joined the Trust as Chief Executive on Monday 2 December. Flu vaccinations. As we approached the end of November, 83% of frontline staff had been vaccinated – this includes 98% of all allied health professionals such as therapists. Many non-clinical colleagues have also received their jab. Thanks a Bunch. Each month staff nominate colleagues for our Thanks a Bunch Award for someone who’s gone the extra mile and deserves recognition. The most recent awards were made to:
• The Anaesthetic team
• Lynne Finnigan, diabetic nurse
• Matt Parry, casting manager Therese Patten Acting Chief Executive December 2019
TB
202_
19 C
EO
Rep
ort D
ec 1
9
Page 26 of 210


PUBLIC TRUST BOARD 4 December 2019
Agenda Item TB203/19a Report Title Quality Improvement Report
Executive Lead Juliette Cosgrove, Director of Nursing, Midwifery, Therapy & Governance
Lead Officer Jo Simpson, Assistant Director of Quality
Bridget Lees, Deputy Director of Nursing
Action Required
(Definitions below)
To Approve To Note
To Assure To Receive
For Information
Executive Summary
This paper provides the Board with an update on the progress of the Quality Improvement Plan and progress made in relation to actions and recommendations relating to the Quality Priorities The Board is asked to note progress identified in this report in relation to the Quality Improvements and the proposed single reporting template which will be used for assurance for both internal and external requirements.
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
Strategic Objective Principal Risk
SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
Absence of clear direction, engagement and leadership across the system is a risk to the sustainability of the Trust and will lead to declining clinical standards.
TB
203_
19a
FS
QI U
pdat
e D
ec 1
9
Page 27 of 210

Linked to Regulation & Governance
CQC KLOEs
GOVERNANCE
Caring Statutory Requirement
Effective Annual Business Plan Priority
Responsive Best Practice
Safe Service Change
Well Led
Impact (is there an impact arising from the report on any of the following?)
Compliance Legal
Engagement and Communication Quality & Safety
Equality Risk
Finance Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Board/Committee/Group)
Board of Directors
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
Page 28 of 210

1
QUALITY IMPROVEMENT PLAN UPDATE DECEMBER 2019
1. PURPOSE OF REPORT
This paper provides the Board of Directors with an update on the progress of the Quality Improvement Plan and progress made in relation to actions and recommendations relating to the Quality Priorities
2. QUALITY IMPROVEMENT
The Quality Improvement Plan (QIP) is an integral component of the Trust’s Vision 2020 Programme. This means that in terms of the governance arrangements, the delivery of the QIP is monitored through Trust Board in the following way:
• The delivery of the programme is managed and monitored through the Hospital Management Board via the Hospital Improvement Board. Programme governance of the plan is managed through the Quality and Safety Group (QSG). Day to day management is delivered through the work streams.
• Reports feed into the Quality and Safety Committee to ensure appropriate assurance as part of the Trust’s Quality and Safety Integrated Performance Report and Quality Improvement Plan Update.
• External governance is provided through the Southport and Ormskirk Improvement Board
• Quality Priorities will also be reported through the annual Quality Account.
The Quality and Safety group operationally monitor delivery of the Quality Priorities:
• Care of the Older Patient
• Care of the Deteriorating Patient
• Infection Prevention and Control
• Medicines Management
In addition to the four identified Trust Quality Priorities, another four quality areas have been
identified and are reported to Hospital Improvement Board (HIB) based on the Vision 20/20
Single Improvement Plan, the work streams include:
• Clinical Workforce Development (incorporating clinical education, medical staffing numbers and professional standards)
• Quality Standards Compliance (Quality Improvement and CQC preparation and delivery of Quality Improvement Plan)
• Patient Experience and Engagement
• Patient Safety (complaints and Risk Management)
• Safeguarding (Improve training compliance and documentation regarding Mental Capacity Act (MCA) and Deprivation of Liberty Safeguards (DoLS)
• Safe and Effective Discharge
• Documentation
The work streams will be reviewed again following publication of the 2019 CQC Report.
TB
203_
19a
QI R
epor
t Dec
19
Page 29 of 210

2
3. FUTURE REPORTING POSITION
The Quality Priority Programme Leads have been allocated a dedicated programme resource, the PMO support are developing full standardised suite of programme documentation including Driver Diagrams, Programme Initiation Documentation (PID), Highlight Report and Gantt Charts, these will be completed and signed off ready for committees in January 2020. For each of the four quality priorities, the Programme Leads are developing improvement measures to monitor improvement and provide assurance, these will include structure, process and outcomes. Any areas for improvement identified during the recent CQC inspections associated to the four quality priorities will be incorporated into the reporting framework.
The Deteriorating Patient summary below provides as example of how the new Quality
Priority reporting dashboard will As advised at the meeting this report template for quality
improvement is being modified to provide assurance and demonstrate a continuous cycle of
improvement.
Page 30 of 210

3
TB
203_
19a
QI R
epor
t Dec
19
Page 31 of 210

4
Page 32 of 210

5
TB
203_
19a
QI R
epor
t Dec
19
Page 33 of 210

6
Page 34 of 210

7
4. CURRENT POSITION
Whilst improvement measures are being developed, the table below provides a summary update in relation to the four quality priorities
Care of the Older Patient:
Mouth Care Matters launched on Ward 14B 04/11/19 Falls bundle now on all wards at both Southport and Ormskirk sites. Cognitive impairment risk assessment and care plan now on all wards at Southport and Ormskirk sites. Revised nutritional screening policy has been rolled out on Ward 10B with demonstrable improvement. Dietetic lead now in post and will continue this piece of work. The training programme for Care of Older People has continued to be delivered with excellent feedback. 170 people are booked to undertake the programme by the end of 2019. The first member of the Dementia and Delirium Team in post 04.11.19 and the Admiral Nurse due in post 16.12.19 Continence project is being revised with a focus on 1 specific ward (7b) to enable greater focus and pace.
Infection Prevention and Control (IPC): Priorities in relation to policy updates is ongoing E Coli Bacteraemia: YTD reduction by 2 cases in September when compared with last year’s data. The trust has enrolled with AQuA: Action on Anti-Microbial reduction programme starting in November which will further support E coli reduction Spinal Centre refurbishments and deep cleaning: - Patient room and bathroom refurbishment nearing completion - Domestic hours increased to correspond with national guidelines - A Public Health England (PHE) Assurance visit of national experts took place on 12 November to provide advice and verify adequacy of processes undertaken, the Trust are awaiting the final report Influenza: 14B Influenza cases x 3 - all contacts reviewed and no transmission and minimal impact on operational capacity Management of Seasonal Influenza policy passed by policy group Table top exercise completed in Oct 19 using the influenza policy conducted by Emergency Planning Point of care Influenza testing analyser now installed in Southport lab; staff currently being trained, but should come on-line mid-November
Medicines Management: Medicines Management Business Case approved at Board 6 November 2019 Serious Incident RCA in relation to the CQC concern has been completed and
TB
203_
19a
QI R
epor
t Dec
19
Page 35 of 210

8
recommendations have been incorporated into Medicine management development plan, after been through SIRG Focus remains on improving 7 day working, staffing and Electronic prescribing Two new additions to the improvement plan include a 6 month plan and assurance tracker. Ward checklists now in place, however anecdotal feedback is that compliance is poor. Weekly audits commenced 21 October and outcomes are to be fed into the tracker to provide assurance against compliance and identify any gaps. The funding application of £700,000 for EPMA (Electronic Prescribing and Medicines Administration) has been approved by NHSE/I
5. RECOMMENDATION
The Board are asked discuss progress identified in this report in relation to the Quality Improvement and to approve a single reporting template which will be used for assurance for both internal and external requirements.
Page 36 of 210

PUBLIC TRUST BOARD 4 December 2019
Agenda Item TB203/19b Report Title Complaints & Compliments
Executive Lead Juliette Cosgrove, Director of Nursing, Midwifery & Therapies
Lead Officer Mandy Power, Associate Director of Integrated Governance
Action Required
(Definitions below)
To Approve To Note
To Assure ✓ To Receive
For Information
Executive Summary
This report provides a breakdown on the number of compliments, complaints, concerns received in
the month of September and the improvements put in place following closure of complaints in
September 2019.
The numbers of complaints and concerns are decreasing; some of the same themes are coming
through but discharge has featured this month within the themes.
• Clinical Treatment – in particularly co-ordination of medical treatment
• Staff attitude/behaviour
• End of life
• Admission/transfers/discharge procedure
• Communication
• Date for appointment
The themes are subject to going improvement work within the Trust.
Recommendation
The Board is asked to receive the report
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
Strategic Objective Principal Risk
✓ SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
✓ SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact
TB
203_
19b
FS
Com
plai
nts
& C
ompl
imen
ts D
ec 1
9
Page 37 of 210

on clinical outcomes and patient experience.
✓ SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
If the system does not have an agreed acute services strategy it may lead to non-alignment of partner organisations plans resulting in the inability to develop and deliver sustainable services
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
✓ Caring ✓ Statutory Requirement
✓ Effective Annual Business Plan Priority
✓ Responsive Best Practice
✓ Safe Service Change
✓ Well Led
Impact (is there an impact arising from the report on any of the following?)
✓ Compliance Legal
Engagement and Communication ✓ Quality & Safety
Equality Risk
Finance Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Board/Committee/Group)
Continue to monitor complaints and compliments. Weekly complaints review meeting to review all complaints over 40 day response target.
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
Page 38 of 210

Complaints & Compliments
October 2019
1.0 Introduction
This report provides a breakdown on the number of compliments, complaints, concerns received in the month of October, it does not relate to care or experience received in Month.
2.0 Compliments
The compliments received across the trust related to the quality of care received by Patients, Communications with relatives & patients, staff behaviour, attitude, staff availability & competence, cleanliness & hospital facilities, transport and also related to Privacy & dignity.
Planned care received the most compliments with 43 in total and General Surgery – Colorectal (11A) receiving 15 compliments in the month.
The Urgent Care Business Unit received 19 Compliments, with the Short Stay Unit reporting 6 compliments.
The Women & Children’s Business Unit received 6 compliments, of which all 6 related to Paediatric ward.
2.1 Complaints
The complaints data has been split in to low level concerns and formal complaints graded 3 or above using the trust grading tool. The formal complaints often include more than one area of complaint.
A total of 30 formal complaints were received in October.
Urgent Care received 16 complaints, with Ward 10A (EAU) accounting for 4 and A&E 2. Planned Care received 6 complaints, in 3 different areas. Specialist Services received 7 complaints, of which 2 related to Maternity. 1 complaint was received by Estates and Facilities and related to Security.
The following themes were identified:
• Clinical Treatment – in particularly co-ordination of medical treatment
• Staff attitude/behaviour
• End of life
• Admission/transfers/discharge procedure
• Communication
• Date for appointment
All complaints are currently being reviewed within the Business Units and response and relevant actions are being put in place.
TB
203_
19b
Sum
mar
y of
Com
plai
nts
& C
ompl
imen
ts D
ec 1
9
Page 39 of 210

Improvements identified
There have been 18 complaints closed during the month of September, there has been some key areas of improvement work been identified through the complaints process. The following are areas were improvement has been highlighted Urgent Care
Following the closure of complaints the Urgent Care Business Unit have met with a number of complainants and offered apologies for nursing care and attitude of staff. The changes in practice are limited this month but are as follows:-
• Following a complaint about feeling rushed and wasting the physiotherapist time, the physiotherapy department are reviewing their communication processes.
• A complaint has been received from a patient’s son who is complaining about the care given to his father and disagrees with the clinician’s assessment that he patient requires a PEG feeding tube. After several meeting with the family the Trust is pursuing a Court of Protection order in the patient’s best interest for a PEG tube to be placed.
Planned care Prior to the closure of complaints the Business Unit have met with complainants and apologised for the poor care and pressure ulcers a patient experienced. A review of discharge processes is underway across the Trust. Specialist Services
Following the closure of a complaint the Specialist Service Business Unit has implemented the following changes in practice:-
• Review of environment and processes with parents when seeing children in
the community paediatrics.
• Matron and Lead midwife is liaising and supporting a patient who complained
about the attitude of a midwife. The concerns have eben shared with the
midwife.
Concerns
There have been a total number of 57 concerns raised this month. 11 were requests for information, 8 related to oral communication and 13 related to appointment dates.
3.0 Conclusion
There has been an increase in the number of complaints received this month but they are comparable with the numbers received last year in October, overall the complaints and concerns are decreasing. The same themes are coming through. The themes are subject to going key areas of improvement work within the Trust.
Page 40 of 210

1
PUBLIC TRUST BOARD 4 December 2019
Agenda Item
TB203/19c Report Title Learning from Deaths Monthly Report
(Formerly The Mortality Report)
Executive Lead Dr Terry Hankin, Medical Director
Lead Officer
Dr. Chris Goddard, Associate Medical Director of Patient Safety
Authors Rachel Flood-Jones, Project Delivery Manager
Mike Lightfoot, Head of Information
Action Required
(Definitions below)
To Approve To Note
To Assure ✓ To Receive
For Information
Executive Summary
The Committee is asked to receive the report for assurance the measures for mortality
alongside detail of the activity supporting the improvement of quality of care and performance.
1.0 Executive Summary
2.0 Mortality Indicators
• Summary Hospital-level Mortality Indicator (SHMI) – 12 month rolling published up to
May 2019
• Hospital Standardised Mortality Ratio (HSMR) – Rolling 12 month and in month for
June 2019
• Disease-Specific Mortality Ratios – April 2019
3.0 Mortality Improvement Activity
4.0 Learning from Deaths: Structured Judgement Reviews (SJRs)
5.0 National Learning
6.0 Conclusions & Recommendations 7. 0 Appendices:
Appendix 1: The External Mortality Review Board Assurance Action Plan: November 2019 Appendix 2: Recognition and Care of the Deteriorating Patient Project Highlight Report
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 41 of 210

2
Appendix 3: Mortality Dashboard.(Dr Foster Mortality Data) November 2019
Appendix 4: Distribution Performance Graph, May 2019
Appendix 5: Mortality Indicators
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
Strategic Objective Principal Risk
SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
✓ SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
Absence of clear direction, engagement and leadership across the system is a risk to the sustainability of the Trust and will lead to declining clinical standards.
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
✓ Caring ✓ Statutory Requirement
✓ Effective ✓ Annual Business Plan Priority
✓ Responsive ✓ Best Practice
✓ Safe ✓ Service Change
✓ Well Led
Impact (is there an impact arising from the report on any of the following?)
✓ Compliance Legal
Engagement and Communication ✓ Quality & Safety
Equality Risk
Finance Workforce
Equality Impact Assessment Policy
Page 42 of 210

3
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Board/Committee/Group)
Previously Presented at:
Audit Committee ✓ ✓ Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 43 of 210

4
1. Executive Summary
• The Month by Month HSMR is inherently unstable. It is affected by the number of
deaths in that month and the case mix, which changes. It does however allow
analysis of what the underlying contributors are. These are the causes of demand
capacity mismatch. This month (HSMR 61.5) discharge and AED flow improved
dramatically – thus the system could cope better with demand.
• The Rolling HSMR and SHMI give a better indication of direction of travel. The trend
of both is towards improvement, again reflecting the investment made in quality.
• Capacity and Demand must be actively managed, should demand increase,
commensurate increases in capacity are required to maintain safety. This is not just
attendance at AED, but can be across different parts of the system including
inpatient wards – what is our surge plan and how is it governed / activated?
• Mortality screening rates remain around 90%, 117 SJRs were performed in 2018-
2019, which is the target and has been met. The challenge now is using this
information to identify and propose improvement work. The first areas will be end of
life care, AKI and fractured Neck of Femur.
• The Board is asked to receive the report for assurance, the measures for mortality
alongside detail of the activity supporting the improvement of quality of care and
performance.
2. Mortality indicators
2.1 Performance Indicator Chart: Key National and Local Mortality Indicators
2018/19 2019/20
Target
Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
Rolling 12 Month
HSMR 112.8 112.3 112.0 102.9 98.7 94.8 96.3 97.4 94.4 100.0
Monthly HSMR 75.7 91.3 105.3 84.7 81.5 82.8 121.0 96.8 61.5 100.0
SHMI 111.1 101.9 101.3 101.1 100.0
Local HSMR
Bronchitis 136.6 136.6 138.1 133.0 118.4 105.9 116.2 111.4 108.7 100.0
Local HSMR
LRTI 137.6 137.4 138.9 134.1 119.5 106.8 120.8 112.3 109.6 100.0
Local HSMR
Pneumonia 121.7 122.1 120.1 112.6 104.8 103.7 110.2 107.1 102.6 100.0
Local HSMR
Septicemia 89.9 89.7 90.2 81.1 79.1 80.0 79.5 75.0 74.6 100.0
Local HSMR
Stroke 107.9 110.1 112.0 100.3 100.2 103.5 105.5 96.8 94.9 100.0
Page 44 of 210

5
Local HSMR UTI 114.9 123.5 120.0 106.2 109.0 80.0 84.2 91.2 85.2 100.0
Local HSMR
Acute Renal
Failure 96.1 107.4 128.8 126.8 115.0 101.3 112.8 112.4 116.2 100.0
Mortality
Screens - % 300.00% 150.00% 151.85% 249.46% 113.33% 425.00% 105.49% 121.95% 312.50% 528.81% 253.85% 88.89% 90.00%
SJRs 21.0 13.0 7.0 13.0 4.0 9.0 6.0 4.0 10.0 11.0 13.0 12.0 0.0
2nd Review 2.0 2.0 0.0 2.0 1.0 0.0 0.0 0.0 1.0 1.0 1.0 0.0 0.0
In Hospital
Deaths 59.0 69.0 81.0 94.0 60.0 72.0 91.0 82.0 48.0 60.0 52.0 63.0 77.0
In Hospital
Deaths Crude
Rate 17.5 20.6 24.5 27.5 19.2 21.6 30.2 25.6 16.0 17.8 15.4 19.4 31.0
LD Deaths 0.0 0.0 0.0 0.0 0.0 0.0 2.0 0.0 0.0 1.0 0.0 0.0 1.0
Steis Incidents 10.0 2.0 3.0 4.0 6.0 3.0 4.0 5.0 5.0 6.0 8.0 4.0 5.0
Explicit values for a rolling 12 month period, when no national target is available a baseline from last year has been used
2.2 SHMI (to May 19)
The SHMI is now being reported monthly by NHS digital and is therefore now presented as
such. SHMI is calculated as observed deaths over expected deaths as predicted by a risk
adjustment model. This figure includes deaths within 30 days of discharge and deaths of
patients receiving palliative care. Compared to the same time period in previous years, we
have less deaths in total and more deaths are ‘expected’ on the SHMI risk adjustment.
The trusts SHMI is within the expected range, meaning that our mortality rate as measured
in this model is ‘as expected’.
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 45 of 210

6
2.3 HSMR - Hospital Standardised Mortality Ratio (Monthly June 19)
The in-month HSMR for June (most recent month with data available) is 61.5 (previous two
months 96.8 and 121) This reflects the inherent volatility in mortality rates when viewed
monthly in isolation. Comparing May to June, the data suggests that the improved figure is
driven by improved harm free care (i.e. increased clinical quality) reduced time spent in the
A&E department - which implies more efficient diagnosis and treatment, and a reduction in
deaths after discharge and days spent waiting for discharge once clinically stable. HSMR
is also produced as an observed mortality over expected. This model excludes patient
deaths of those receiving palliative care. Palliative care rates are currently around 40% of
all deaths. This will influence the HSMR figure, but not the SHMI.
2.4 HSMR - Hospital Standardised Mortality Ratio (Rolling to June 19)
Rolling HSMR to June 2019 is 94.4. This is again within the expected range. Rolling HSMR
is averaged over 12 months and is therefore less prone to in-month variation. Consistent
factors affecting HSMR over the past 12 months are metrics of AED flow – particularly
arrival to departure times. This probably reflects clinical teams being able to assess,
diagnose and treat better and more effectively when clinical capacity and demand is
matched across the organisation from admission to departure. It is important to realise that
Page 46 of 210

7
deterioration in AED flow my represent issues that have not been dealt with further down
the inpatient or community pathways.
2.5 Diagnosis Groups
Respiratory: LRTI and Acute bronchitis have a low risk of death. Analysis of these cases
shows that these patients frequently have high co-morbidity burdens and this is not being
captured as the primary diagnosis. These are now subject to clinical review to ascertain the
appropriate diagnosis. Pneumonia continues to be the subject of improvement work,
establishing and embedding the pneumonia clinical pathway and performing appropriate
diagnostics are the foci.
Renal Failure: A task and finish group is operational to lead AKI work. This is following the
AQ indicators of clinical quality, supported by the AKI pathway and 12 hourly AKI alerts.
3. Mortality Improvement Activity
The Deteriorating Patient Project is the second phase of the Reducing Avoidable Mortality
Project and is one of the Trust’s four key Quality Priorities in line with Vision 2020.
A more detailed update on the project can be found under Appendix 1 in the form of the
monthly project highlight report.
3.1 Update on Recognition and Care of the Deteriorating Patient Programme
Primary Driver Progress and achievements this month
Appropriate Assessment & Admission
The Surgical Ambulatory Emergency Care Project Group are working on a pathway for improved, appropriate GP referrals to the Surgical Assessment Unit. Members of the Emergency Department are working with Strata Networking Solutions to design an electronic GP referral system directly into the Ambulatory Care Unit.
Senior Ownership The Electronic Board Round is in the final iteration of the PDSA cycle. The pilot has been well received by the Consultants and Drs on Ward 10A (Gastro). The tool captures the level of escalation (ward care, critical care or end of life care) for each patient and records the direct or remote senior review of all Daily Board Rounds. There is a currently delay in securing resource from the IT Team to complete the fixes required to finalise the electronic functionality for roll out.
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 47 of 210

8
Primary Driver Progress and achievements this month
Correct Pathways of Care The AKI Steering Group is now driving the required activity to improve compliance to best practice. Linking into the Deteriorating Patient Group ensures the triangulation with business intelligence and the Critical Care Outreach Team. The scoping session of the 1st November was supported by attendance and input from the Advanced Quality Alliance (AQUA). New areas of focus have been incorporated into the work stream include: IV and Fluid Balance, Insulin, Abdominal Pain Pathway, Fractured Neck of Femur and Gastro-Intestinal Bleed.
Observations & Escalations The Observations QI Project continues on Ward 9A (Short Stay Unit). Iterations of the PDSA cycle are continuing with the use of business intelligence to identify when and why patients are being taken off protocol for observations and how compliance with the Trust Track and Trigger Policy can be improved. Changes to reporting are with System C to realign ‘breach’ and ‘overdue’ parameters with Trust protocol to produce accurate reporting in line with revised timeframes. Training requirements are being scoped in order to ensure that all relevant employees have the most up to date training in management of the deteriorating patient. (Acute Illness Management Training (AIMS) and Red Day Training in particular for which funding will be required to deliver.
Future Care Planning Strata Networking Solutions have undertaken process mapping with key stakeholders from the Trust, Queenscourt Hospice and community service providers to design a tool with which Anticipatory Clinical Management Plans can be shared. This will ensure that there is one version of the truth and a single plan that can be accessed for each relevant patient at any access point. The project team is yet to understand from Strata to what level the model will be delivered under the existing contract.
Learning from Deaths The Trust has a total of 40 SJR level one reviewers across all specialities that are key to the success of the process. An increased focus of thematic reviewing of deaths from the SJR process will support the dissemination of learnings. The first thematic presentation to the Grand Round will be given on 29th November by Dr MacDonald on End of Life deaths. The revised Learning from Deaths Board Report along with high level fortnightly Mortality Meetings will support the delivery of a responsive and learning focused approach to the screening of deaths and the findings of the Structured Judgement Review.
Page 48 of 210

9
4. Learning from Deaths: Structured Judgement Reviews (SJR)
4.1 Screening
The above table details the screening process and rates. This demonstrates improved
screening with September and October 2019 meeting the 90% target.
Within 3 months, on average 80% of reviews have been completed. There are delays in
terms of the availability of case notes for review, and the timeliness of allocation of a
reviewer. These process issues are under investigation to try and make reviewing more
timely.
4.2 First Structured Judgement Review
The number of reviews completed is gradually increasing. 117 reviews have been
completed for 2018/19, meeting our target of 10% of all inpatient deaths.
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 49 of 210

10
Graphical presentation of all reviews performed demonstrates that ongoing (or ward
based) care, in the opinion of our reviewers, is where a patient is most likely to
experience ‘poor’ or at best ‘adequate’ care. Improvement focus should be targetted at
this area of the patients journey, which is reflected in the senior ownership and correct
pathways of care aspects of the Deteriorating Patient Project.
Page 50 of 210

11
When broken down further by clinical areas with 18 or more reviews it can be seen that
the situation with ongoing care is most acute in the general medical population. Also of
note is a higher proportion than overall of adequate, poor or very poor end of life care.
Critical Care reviews have a higher proportion of excellence overall, but have 3 cases of
poor care around a procedure, which is a higher proportion than other clinical areas.
Analysis of individual cases in individual clinical areas is required for further insights.
4.3 Second Structured Judgement Review
This table shows the conversion rate by specialty from 1st to 2nd SJR. The criteria for
this is ‘poor’ or ‘very poor’ care in the overall category. To date 8 second reviews have
been completed. All second reviews are presented to the Mortality Operational
Committee.
T
B20
3_19
c Lf
D R
epor
t Dec
19
Page 51 of 210

12
The data above demonstrates the change in the assessment of overall care and the
change in avoidability judgement between first and second SJR. In 5/9 cases the care
judgement remains the same, in 3 further cases the judgement has changed by one
category, and in a further case the judgement has changed dramatically from, ‘very
poor’ to ‘good’. These cases are all discussed at MOG to allow the rationale to be
presented by the reviewers.
An avoidability assessment is made by the first reviewer using the Hogan scale. This
assessment is then made again by the second reviewer. The case is presented at the
MOG and a committee decision is made on avoidability. Should the committee agree
that the death is more likely than not to be avoidable (definite or probable) then this
case is referred to SIRG for appropriate action. To date 2 cases have been identified
as avoidable by first reviewers, this judgement has been upheld in one case, which
was referred to SIRG, underwent a full RCA, and the findings have been shared with
the Sefton Coroner’s office.
4.6 Lessons Learned: Process & Activity
The trust will hold 3 Grand Rounds a year based on the finding from SJRs. The first of these will
be held on the 29th of November and facilitated by Dr McDonald. The discussion will focus
around decision making at the end of life using case examples from the past 12 months.
A Lessons Learned Bulletin is produced in order to communicate out important points from the
MOG, including relevant findings from SJRs. This is produced on a monthly basis by Janette
Mills, Head of Audit and Effectiveness.
We have cross referenced data from coding and SJR to identify ten cases of death from AKI.
These cases will be reviewed for learning to add extra information to the AKI improvement
work.
Further work is planned to use our SJR database to provide an information source to design
improvements going forward such as in the case of femoral neck fractures.
Page 52 of 210

13
5. Conclusions & Recommendations
Successive mortality reports have stressed the link between AED flow and mortality
rates. This report also makes this point. However, the association is with the whole
system and not just AED. AED flow deteriorates when whole system capacity is
outstripped by demand. When this occurs the system becomes less safe and mortality
rates rise.
Our hospital population is a population which does not have a large degree of
physiological resilience, either due to frailty or multi-morbidity, thus, variations in the
capacity / demand equation are particularly dangerous.
The equation is affected by the number of patients arriving, the number departing and
the capacity of the staff within the system (vacancies, stress, sickness, training and
experience in the organisation).
Better balancing these demands by increasing staffing and their skill set, standardising
processes of care and working to provide alternatives to hospital admission - were
appropriate, has reduced our headline mortality figures and improved the safety of our
care.
Recent events demonstrate that sudden increases in demand, without commensurate
increases in capacity threaten safe patient care. This can either be predictable (winter)
or unpredictable.
Recommendations
Proactive monitoring of capacity and demand within the system occurs; those
performing this monitoring must be clear that decisions taken to manage surges in
demand have real consequence on patient mortality.
Continue to evaluate and invest in activity which provides capacity to manage serious
illness quickly and aggressively to reduce complications and length of stay.
Encourage and support interventions which support staff to work reliably and
consistently, with minimal variation, such as through the adoption of appropriate IT or
best practice pathways which are clear and available.
Support ward processes and ward care with the same intention as supporting AED in
order to improve the quality of patient care and thereby improve flow and improve
safety. Start by engaging with ward teams such as junior medical staff and junior nurses
to understand the issues they face.
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 53 of 210

14
6.
7.0
Ap
pen
dic
es
Ap
pen
dix
1 -
Ex
tern
al
Mo
rtali
ty A
cti
on
Pla
n (
inc
lud
ing
7 R
CA
Ca
se
s)
– B
oa
rd P
rog
res
s A
ss
ura
nc
e R
ep
ort
(EM
BA
R)
EM
BA
R
Th
e E
xte
rnal
Mo
rtali
ty A
cti
on
Pla
n (
Inclu
din
g 7
RC
A C
ases)
Bo
ard
Pro
gre
ss A
ssu
ran
ce R
ep
ort
2019-2
1
Ori
gin
Re
co
mm
en
da
tio
n D
eta
il
Pro
gra
mm
e /
Pro
jec
t
Le
ad
(s)
Sta
rt
Da
te
Pro
jec
ted
Co
mp
leti
o
n D
ate
Co
mp
leti
o
n %
BR
AG
U
pd
ate
21
st
Oc
tob
er
20
19
Impro
ve
pa
tie
nt flo
w s
o tha
t
pa
tie
nts
re
quir
ing a
dm
issio
n d
o n
ot
ha
ve
to
wa
it f
or
an a
ppro
pri
ate
be
d
and a
re n
ot nurs
ed o
n c
orr
ido
rs.
Fo
cusin
g o
n:
50
%G
The
Pa
tie
nt F
low
Im
pro
ve
me
nt P
rogra
mm
e (
PF
IP)
co
nsis
ts o
f 4
Wo
rkstr
ea
ms:
1. Im
pro
ve
Em
erg
ency D
epa
rtm
ent a
nd A
sse
ssm
ent U
nits S
erv
ice
s
2. S
tanda
rdis
atio
n o
f B
est P
ractice
Wa
rd P
roce
sse
s (
to r
educe
length
of
sta
y)
3. S
urg
ica
l Am
bula
tory
Em
erg
ency C
are
Im
pro
ve
me
nt P
roje
ct (i
n a
sso
cia
tio
n w
ith N
HS
E A
EC
)
4. S
tra
ta E
lectr
onic
Ne
two
rkin
g S
olu
tio
ns to
im
pro
ve
Pa
tie
nt F
low
pa
thw
ays
The
Pro
gra
mm
e d
rive
s the
im
ple
me
nta
tio
n o
f th
e N
HS
I S
AF
ER
Pa
tie
nt F
low
Im
pro
ve
me
nt bundle
; th
e f
ive
ele
me
nts
of
the
SA
FE
R p
atie
nt flo
w b
undle
are
:
S –
Se
nio
r re
vie
w. A
ll pa
tie
nts
will
ha
ve
a s
enio
r re
vie
w b
efo
re m
idda
y b
y a
clin
icia
n a
ble
to
ma
ke
ma
na
ge
me
nt a
nd d
ischa
rge
de
cis
ions.
A –
All
pa
tie
nts
will
ha
ve
an e
xpe
cte
d d
ischa
rge
da
te a
nd c
linic
al c
rite
ria
fo
r dis
cha
rge
. T
his
is s
et a
ssum
ing ide
al r
eco
ve
ry
and a
ssum
ing n
o u
nne
ce
ssa
ry w
aitin
g.
F –
Flo
w o
f pa
tie
nts
will
co
mm
ence
at th
e e
arlie
st o
ppo
rtunity f
rom
asse
ssm
ent units to
inpa
tie
nt w
ard
s. W
ard
s tha
t ro
utine
ly
rece
ive
pa
tie
nts
fro
m a
sse
ssm
ent units w
ill e
nsure
the
fir
st pa
tie
nt a
rriv
es o
n the
wa
rd b
y 1
0 a
m.
E –
Ea
rly d
ischa
rge
. 3
3%
of
pa
tie
nts
will
be
dis
cha
rge
d f
rom
ba
se
inpa
tie
nt w
ard
s b
efo
re m
idda
y.
R –
Re
vie
w. A
syste
ma
tic m
ulti
-dis
cip
lina
ry te
am
re
vie
w o
f pa
tie
nts
with e
xte
nde
d le
ngth
s o
f sta
y (
>7
da
ys –
‘str
ande
d
pa
tie
nts
’) w
ith a
cle
ar
‘ho
me
fir
st’ m
indse
t.
a.
Alt
ern
ati
ve
to
ad
mis
sio
n
Avo
ida
ble
adm
issio
ns w
ith
turn
aro
und a
t fr
ont do
or
or
within
12
ho
urs
unde
r ca
re o
f spe
cia
list
tea
ms
20
%G
The
Pa
tie
nt F
low
Im
pro
ve
me
nt P
rogra
mm
e (
PF
IP)
is c
urr
ently
re
vie
win
g D
r F
oste
r a
nd M
ode
l Ho
spita
l da
ta to
ide
ntify
pa
thw
ays r
equir
ing m
odific
atio
n to
avo
id ina
ppro
pri
ate
atte
nda
nce
s a
t A
&E
and ina
ppro
pri
ate
adm
issio
ns.
Le
ngth
of
Sta
y ta
rge
ts a
nd r
epo
rtin
g a
re b
ein
g r
evie
we
d in the
co
nte
xt o
f a
sig
nific
ant in
cre
ase
in y
ea
r o
n y
ea
r A
&E
atte
nda
nce
s.
Wo
rk is o
ngo
ing w
ith S
tra
ta N
etw
ork
ing S
olu
tio
ns a
nd c
om
munity p
art
ne
rs to
de
sig
n p
ath
wa
ys to
suppo
rt the
im
ple
me
nt IT
functio
na
lity f
or:
1. G
P r
efe
rra
ls into
Am
bula
tory
Ca
re
2. F
railt
y P
ath
wa
y: sha
red P
atie
nt A
nticip
ato
ry C
linic
al M
ana
ge
me
nt P
lans (
AC
MP
)
3. D
ischa
rge
to
Asse
ss
4. E
lectr
onic
Re
ferr
al t
o S
ocia
l Ca
re
b.
Cri
teri
a l
ed
dis
ch
arg
e
Ea
rly d
ischa
rge
pla
nnin
g f
or
adm
itte
d p
atie
nts
with a
gre
ed
pe
rmis
sio
ns f
or
nurs
e a
nd A
llie
d
He
alth
Pro
fessio
na
ls (
AH
P)
led
dis
cha
rgin
g.
50
%G
Impro
vin
g C
rite
ria
Le
d D
ischa
rge
to
suppo
rt f
low
and r
educe
length
of
sta
y is a
ke
y d
eliv
era
ble
of
the
Wo
rk S
tre
am
2 (
of
PF
IP).
Cri
teri
a L
ed D
ischa
rge
is d
rive
n b
y c
lea
r m
edic
al d
ocum
enta
tio
n a
nd p
lannin
g a
nd s
tart
s w
ith the
Expe
cte
d D
ate
of
Dis
cha
rge
(E
DD
) w
hic
h is a
lloca
ted b
y a
clin
icia
n a
t th
e o
uts
et o
f th
e p
atie
nt's
tim
e in h
opsita
l. T
he
pa
tie
nt is
to
kno
w the
ir
ED
D w
ith a
nsw
ers
to
4 o
the
r ke
y q
ue
stio
ns:
1. W
ha
t is
wro
ng w
ith m
e o
r w
ha
t a
re y
ou try
ing to
exclu
de
?
2. W
ha
t ha
ve
we
agre
ed tha
t w
ill b
e d
one
and w
he
n to
'so
rt m
e o
ut'?
3. W
ha
t do
I n
ee
d to
achie
ve
to
ge
t m
e h
om
e?
4. A
ssum
ing m
y r
eco
ve
ry is 'i
de
al'
and the
re is n
o u
nne
ce
ssa
ry w
aitin
g, w
he
n s
ho
uld
I e
xpe
ct to
go
ho
me
?
The
Re
d to
Gre
en m
ulti
-dis
cip
lina
ry a
ppro
ach s
uppo
rts p
atie
nt flo
w b
y e
nsuri
ng tha
t a
ll pa
tie
nts
ha
ve
a 'g
ree
n d
ay' w
he
re it is
po
ssib
le (
a d
ay o
f va
lue
fo
r th
e p
atie
nt’s p
rogre
ss to
wa
rds d
ischa
rge
) a
s o
ppo
se
d to
a 'r
ed d
ay' (
a d
ay w
he
re the
re is li
ttle
or
no
va
lue
addin
g c
are
).
c.
Pro
ac
tiv
e
es
ca
lati
on
pla
nn
ing
Co
mpre
he
nsiv
e tre
atm
ent pla
ns
de
taili
ng e
sca
latio
n a
nd c
eili
ngs o
f
ca
re inclu
din
g D
o N
ot A
tte
mpt
Ca
rdio
pulm
ona
ry R
esuscita
tio
n
(DN
AC
PR
) o
rde
rs.
80
%G
The
Ele
ctr
onic
Bo
ard
Ro
und r
equir
es c
onfirm
atio
n f
or
ea
ch d
aily
pa
tie
nt re
vie
w o
f th
e le
ve
l of
esca
latio
n r
equir
ed (
whe
the
r th
e
pa
tie
nt re
quir
es W
ard
Ca
re, In
tensiv
e C
are
or
End o
f L
ife
Ca
re).
The
Tru
st's
late
st D
NA
CP
R A
udit r
esults
we
re p
ublis
he
d in J
uly
20
19
and s
ho
we
d a
n 1
00
% o
f pa
tie
nt re
co
rds r
evie
we
d h
ad a
rea
so
n c
ode
, 9
2%
ha
d a
ori
gin
ato
r da
te a
nd 9
5%
ha
d a
ppro
pri
ate
info
rma
tio
n r
ega
rdin
g w
hy the
de
cis
ion h
as b
ee
n m
ade
.
d.
Mu
lti-
Sp
ec
ialt
y
Te
am
Wo
rkin
g
Te
am
wo
rkin
g to
im
pro
ve
pa
tie
nt
ma
na
ge
me
nt th
rough the
pa
thw
ay
inclu
din
g in-r
ea
ch to
em
erg
ency
de
pa
rtm
ent a
nd c
ritica
l ca
re
outr
ea
ch to
all
are
as.
90
%G
A m
ulti
-dis
cip
lina
ry te
am
(M
DT
) a
ppro
ach is the
co
rne
rsto
ne
of
the
da
ily R
ed to
Gre
en B
oa
rd R
ounds. M
ini a
udits a
re
curr
ently
be
ing u
nde
rta
ke
n f
or
two
we
eks to
ensure
the
co
rre
ct a
nd c
om
ple
te M
DT
atte
nda
nce
in li
ne
with n
ew
'Re
d to
Gre
en
Bo
ard
Ro
und' S
tanda
rd O
pe
rating P
roce
dure
. W
ard
s a
re b
ein
g a
ske
d to
fo
cus o
n k
ey a
ctivity:
• E
nsuri
ng bo
ard
ro
unds h
appe
n -
with a
fir
m f
ocus o
n a
gre
ein
g the
ne
ce
ssa
ry a
ctio
ns to
ensure
eve
ry p
atie
nt ha
s a
pla
n to
pro
gre
ss the
ir c
are
to
wa
rds d
ischa
rge
• E
arly s
enio
r re
vie
w o
f a
ll in
pa
tie
nt ca
re p
lans –
cle
arly c
om
munic
ate
d a
nd d
ocum
ente
d w
ith the
wa
rd M
DT
on the
re
quir
ed
cri
teri
a f
or
dis
cha
rge
• U
se
the
dis
cha
rge
lounge
to
cre
ate
flo
w a
nd w
ork
ha
rd to
ge
t th
ose
pa
tie
nts
tha
t ca
n g
o h
om
e to
da
y a
wa
y a
s s
oo
n a
s
po
ssib
le
• E
arly c
om
ple
tio
n o
f T
TO
s a
nd b
oo
kin
g o
f tr
anspo
rt f
or
dis
cha
rge
• R
efe
rra
ls m
ade
by w
ard
MD
T te
am
s a
re a
ctio
ne
d p
rom
ptly
(e
.g. th
era
py, ra
dio
logy, pha
rma
cy)
• D
ela
ys to
dis
cha
rge
to
be
esca
late
d to
the
Be
d M
ana
ge
me
nt T
ea
m
Lo
ng S
tay T
ue
sda
ys: a
multi
-dis
cip
lina
ry a
nd m
ulti
-age
ncy a
ppro
ach to
re
vie
w p
atie
nts
with a
length
of
sta
y o
f 7
da
ys o
r o
ve
r
to f
ind s
olu
tio
ns to
de
lays a
nd e
xpe
dite
dis
cha
rage
are
ongo
ing.
Blu
e
Re
d
Am
be
r
Gre
en
Im
pro
ve
Pa
tie
nt
Flo
wActivity c
om
ple
ted
Sig
nific
antly d
ela
yed a
nd/o
r of hig
h r
isk -
not exp
ecte
d to r
ecover
Slig
htly d
ela
yed a
nd / o
r of lo
w r
isk -
can b
e r
ecovere
d
Pro
gre
ssin
g o
n s
chedule
Ma
r-2
0
Are
a R
eq
uir
ing
Imp
rov
em
en
t
Pa
tie
nt F
low
Impro
ve
me
nt
Pro
gra
mm
e
(De
teri
ora
ting
Pa
tie
nt P
roje
ct:
'Appro
pri
ate
Asse
ssm
ent &
Adm
issio
n')
Exe
cutive
Le
ad:
Chie
f
Ope
rating
Off
ice
r
Patient Flow
EM
R
Actio
n 1
No
v-1
8
Page 54 of 210

15
Exte
rnal M
ort
ality
Acti
on
Pla
n, B
oard
Assu
ran
ce R
ep
ort
– P
ag
e 2
EM
BA
R
Th
e E
xte
rna
l M
ort
ali
ty A
cti
on
Pla
n (
Inc
lud
ing
7 R
CA
Ca
se
s)
Bo
ard
Pro
gre
ss
As
su
ran
ce
Re
po
rt 2
01
9-2
1
Ori
gin
Re
co
mm
en
da
tio
n D
eta
il
Pro
gra
mm
e /
Pro
jec
t
Le
ad
(s)
Sta
rt
Da
te
Pro
jec
ted
Co
mp
leti
o
n D
ate
Co
mp
leti
o
n %
BR
AG
U
pd
ate
21
st
Oc
tob
er
20
19
d.
Mu
lti-
Sp
ec
ialt
y
Te
am
Wo
rkin
g
Te
am
wo
rkin
g to
im
pro
ve
pa
tie
nt
ma
na
ge
me
nt th
rough the
pa
thw
ay
inclu
din
g in-r
ea
ch to
em
erg
ency
de
pa
rtm
ent a
nd c
ritica
l ca
re
outr
ea
ch to
all
are
as.
90
%G
A m
ulti
-dis
cip
lina
ry te
am
(M
DT
) a
ppro
ach is the
co
rne
rsto
ne
of
the
da
ily R
ed to
Gre
en B
oa
rd R
ounds. M
ini a
udits a
re
curr
ently
be
ing u
nde
rta
ke
n f
or
two
we
eks to
ensure
the
co
rre
ct a
nd c
om
ple
te M
DT
atte
nda
nce
in li
ne
with n
ew
'Re
d to
Gre
en
Bo
ard
Ro
und' S
tanda
rd O
pe
rating P
roce
dure
. W
ard
s a
re b
ein
g a
ske
d to
fo
cus o
n k
ey a
ctivity:
• E
nsuri
ng bo
ard
ro
unds h
appe
n -
with a
fir
m f
ocus o
n a
gre
ein
g the
ne
ce
ssa
ry a
ctio
ns to
ensure
eve
ry p
atie
nt ha
s a
pla
n to
pro
gre
ss the
ir c
are
to
wa
rds d
ischa
rge
• E
arly s
enio
r re
vie
w o
f a
ll in
pa
tie
nt ca
re p
lans –
cle
arly c
om
munic
ate
d a
nd d
ocum
ente
d w
ith the
wa
rd M
DT
on the
re
quir
ed
cri
teri
a f
or
dis
cha
rge
• U
se
the
dis
cha
rge
lounge
to
cre
ate
flo
w a
nd w
ork
ha
rd to
ge
t th
ose
pa
tie
nts
tha
t ca
n g
o h
om
e to
da
y a
wa
y a
s s
oo
n a
s
po
ssib
le
• E
arly c
om
ple
tio
n o
f T
TO
s a
nd b
oo
kin
g o
f tr
anspo
rt f
or
dis
cha
rge
• R
efe
rra
ls m
ade
by w
ard
MD
T te
am
s a
re a
ctio
ne
d p
rom
ptly
(e
.g. th
era
py, ra
dio
logy, pha
rma
cy)
• D
ela
ys to
dis
cha
rge
to
be
esca
late
d to
the
Be
d M
ana
ge
me
nt T
ea
m
Lo
ng S
tay T
ue
sda
ys: a
multi
-dis
cip
lina
ry a
nd m
ulti
-age
ncy a
ppro
ach to
re
vie
w p
atie
nts
with a
length
of
sta
y o
f 7
da
ys o
r o
ve
r
to f
ind s
olu
tio
ns to
de
lays a
nd e
xpe
dite
dis
cha
rage
are
ongo
ing.
RC
A
Actio
n 1
Ensure
tha
t pa
thw
ays o
f ca
re f
or
ke
y c
ause
s o
f clin
ica
l de
teri
ora
tio
n
are
; up to
da
te, a
va
ilable
, cle
ar
and
use
d a
cro
ss the
org
anis
atio
n.
The
se
must in
clu
de
Se
psis
,
Pne
um
onia
and A
KI. T
rain
ing g
aps
on the
se
pro
ce
sse
s f
or
do
cto
rs
and n
urs
es m
ust be
ide
ntifie
d a
nd
clo
se
d o
rga
nis
atio
n-w
ide
, to
inclu
de
the
ba
sic
inve
stiga
tive
and
the
rape
utic s
tra
tegie
s f
or
the
fir
st
ho
urs
of
ca
re a
nd c
rite
ria
fo
r
refe
rra
l.
Ma
r-1
8O
ngo
ing
until e
nd o
f
pro
ject
Ma
rch
20
20
40
%A
The
Tru
st's
Clin
ica
l Educa
tio
n L
ea
d ha
s inclu
de
d the
re
vis
ed A
KI P
ath
wa
y (
Apri
l 20
19
) in
to the
Tru
st's
'Do
cto
rs in T
rain
ing:
Wo
rkin
g H
andbo
ok'
AK
I is
big
ge
st is
sue
fro
m a
n A
Q p
ers
pe
ctive
. T
he
Tru
st no
w h
as a
de
dlc
ate
d A
KI S
tee
ring G
roup w
hic
h m
ee
ts o
nce
a m
onth
to d
rive
ta
rge
ted a
ctivity.
Sin
ce
Ja
nua
ry, da
ily a
uto
ma
ted a
lert
s o
f ne
w c
ase
s o
f A
KI a
re s
ent by the
Me
dw
ay T
ea
m to
bo
th the
Cri
tica
l Ca
re O
utr
ea
ch
Te
am
and the
Pha
rma
cy T
ea
m.
The
ne
w 2
4/7
Cri
tica
l Ca
re O
utr
ea
ch T
ea
m is n
ow
re
vie
win
g p
atie
nts
with A
KI le
ve
l 3. T
he
se
im
pro
ve
me
nts
sho
uld
be
refle
cte
d in the
ne
xt bia
nnua
l re
po
rt f
rom
the
Adva
ncin
g Q
ua
lity A
llia
nce
(A
QU
A)
in O
cto
be
r 2
01
9. It is e
xpe
cte
d tha
t
impro
ve
me
nts
will
be
vis
ible
in N
ove
mbe
r 2
01
9 r
epo
rtin
g o
n O
cto
be
r da
ta.
Jul-1
81
00
%B
Ma
r-2
06
0%
A
EM
R
Actio
n 3
Re
vie
w a
nd/o
r e
sta
blis
h a
pne
um
onia
pa
thw
ay to
ensure
tha
t
it m
ee
ts n
atio
na
l guid
elin
es.
De
teri
ora
ting
Pa
tie
nt P
roje
ct
No
v-1
8M
ay-1
99
0%
GT
he
Pne
um
onia
Ca
re P
ath
wa
y is r
ea
dily
ava
ilable
acro
ss the
Tru
st a
nd h
as b
ee
n g
ive
n a
dditio
na
l fo
cus b
y the
Co
nsulta
nt in
Acute
Me
dic
ine
in the
Em
erg
ency A
mbula
tory
Unit.
The
Asso
cia
te D
ire
cto
r fo
r P
atie
nt S
afe
ty a
nd the
Tru
st's
Clin
ica
l Educa
tio
n L
ea
d a
re inco
rpo
rating the
Pne
um
onia
Ca
re
Pa
thw
ay into
the
junio
r do
cto
rs' t
rain
ing p
rogra
mm
e.
Blu
e
Re
d
Am
be
r
Gre
en
Activity c
om
ple
ted
Sig
nific
antly d
ela
yed a
nd/o
r of hig
h r
isk -
not exp
ecte
d to r
ecover
Slig
htly d
ela
yed a
nd / o
r of lo
w r
isk -
can b
e r
ecovere
d
Pro
gre
ssin
g o
n s
chedule
Ma
r-2
0
Are
a R
eq
uir
ing
Imp
rov
em
en
t
Pa
tie
nt F
low
Impro
ve
me
nt
Pro
gra
mm
e
(De
teri
ora
ting
Pa
tie
nt P
roje
ct:
'Appro
pri
ate
Asse
ssm
ent &
Adm
issio
n')
Exe
cutive
Le
ad:
Chie
f
Ope
rating
Off
ice
r
Impro
ve
aw
are
ne
ss o
f S
epsis
6
guid
elin
es a
nd m
onito
r a
dhe
rence
.
Es
tab
lis
h
Pn
eu
mo
nia
Pa
thw
ay
Imp
rov
e D
eli
ve
ry
of
Pa
thw
ays
of
Ca
re
Patient Flow
Imp
rov
e
co
mp
lia
nc
e w
ith
Se
ps
is 6
Gu
ide
lin
es
/
Mo
nit
or
Co
mp
lain
ce
Wit
h
Se
ps
is P
ath
wa
y
Imp
rov
e
aw
are
ne
ss
of
Se
ps
is
Correct Pathways of Care
EM
R
Actio
n 2
EM
R
Actio
n 1
Apr-
18
Asso
cia
te
Me
dic
al
Dir
ecto
r o
f
Pa
tie
nt
Sa
fety
Co
mplia
nce
with o
f th
e S
epsis
Six
(th
ree
dia
gno
stic a
nd thre
e the
rape
utic s
teps to
be
de
live
red w
ithin
one
ho
ur
of
the
initia
l
dia
gno
sis
of
se
psis
) is
ingra
ine
d a
cro
ss the
Tru
st.
In li
ne
with the
AQ
UA
AQ
da
ta s
et; w
e a
re p
erf
orm
ing w
ell
in r
ela
tio
n to
our
pe
ers
ho
we
ve
r o
ngo
ing a
rea
s o
f cha
llenge
inclu
de
:
pe
rfo
rma
nce
of
blo
od c
ultu
res w
ithin
an h
our
of
dia
gno
sis
and s
enio
r re
vie
w w
ithin
tw
o h
ours
. T
he
mo
st up to
da
te A
Q d
ata
repo
rts o
n a
citvity u
p to
Fe
bru
ary
20
19
; w
e e
xpe
ct to
se
e im
pro
ve
me
nt go
ing f
orw
ard
re
fle
cting the
im
pa
ct o
f th
e incre
ase
d
co
ve
r o
f th
e 2
4/7
Cri
tica
l Ca
re O
utr
ea
ch T
ea
m.
The
Tru
st's
Co
nsulta
nt M
icro
bio
logis
t ha
s p
roduce
d g
uid
ance
on b
est pra
ctice
fo
r ta
kin
g b
loo
d c
ultu
res to
re
duce
co
nta
min
atio
n r
ate
s. T
his
ha
s r
ece
ntly
be
en s
igne
d o
ff a
nd is n
ow
be
ing e
mbe
dde
d thro
ugh tra
inin
g.
No
v-1
8
De
teri
ora
ting
Pa
tie
nt P
roje
ct:
'Co
rre
ct
Pa
thw
ays o
f
Ca
re'
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 55 of 210

16
Exte
rnal M
ort
ality
Acti
on
Pla
n, B
oard
Assu
ran
ce R
ep
ort
– P
ag
e 3
EM
BA
R
Th
e E
xte
rnal
Mo
rtali
ty A
cti
on
Pla
n (
Inclu
din
g 7
RC
A C
ases)
Bo
ard
Pro
gre
ss A
ssu
ran
ce R
ep
ort
2019-2
1
Ori
gin
Re
co
mm
en
da
tio
n D
eta
il
Pro
gra
mm
e /
Pro
jec
t
Le
ad
(s)
Sta
rt
Da
te
Pro
jec
ted
Co
mp
leti
o
n D
ate
Co
mp
leti
o
n %
BR
AG
U
pd
ate
21
st
Oc
tob
er
20
19
EM
R
Actio
n 4
Re
vie
w d
octo
rs’ ro
tas to
ensure
suff
icie
nt
da
ily s
enio
r co
ve
r a
nd tha
t ju
nio
r do
cto
rs a
re
no
t unsuppo
rte
d o
r w
ork
ing b
eyo
nd the
ir
ca
pa
bili
tie
s.
AM
Ds o
f
Clin
ica
l
Busin
ess
Units
Ma
r-1
9M
ar-
20
20
%A
The
re
quir
em
ent to
re
vie
w d
octo
rs r
ota
s to
ensure
da
ily s
enio
r co
ve
r o
rigin
ate
d f
rom
re
po
rts tha
t ju
nio
r do
cto
rs w
ere
wo
rkin
g
unsupe
rvis
ed o
n w
ard
s. A
udits to
asse
ss s
taff
ing le
ve
ls h
ave
sho
we
d tha
t th
e issue
is n
ot a
sho
rta
ge
of
do
cto
rs b
ut th
e p
oo
r
ma
na
ge
me
nt o
f ro
tas a
nd the
mis
allo
ca
tio
n o
f sta
ff (
for
exa
mple
co
ho
rts o
f sta
ff a
ll a
tte
ndin
g tra
inin
g a
t th
e s
am
e tim
e).
The
audit is to
be
re
run in N
ove
mbe
r to
asce
rta
in w
he
the
r cha
nge
s in jo
b p
lannin
g a
nd the
mo
dific
atio
n o
f ju
nio
r do
cto
r ro
tas in
August ha
s im
pro
ve
d c
ove
r a
nd s
uppo
rt f
or
junio
r do
cto
rs.
RC
A
Actio
n 2
Ensure
tha
t it is c
lea
r to
eve
ry p
atie
nt, f
am
ily
and s
taff
me
mbe
r w
hic
h c
onsulta
nt te
am
is
the
lea
d p
rovid
er
of
ca
re f
or
eve
ry p
atie
nt,
inclu
din
g w
he
n c
are
is s
ha
red b
etw
ee
n te
am
s
and s
pe
cia
lism
s. D
epa
rtm
enta
l po
licie
s a
nd
wo
rkin
g p
ractice
s m
ust pro
mo
te a
nd s
uppo
rt
co
nsulta
nt le
ade
rship
of
pa
tie
nt ca
re a
nd
co
nsis
tent ha
ndo
ve
r o
f ca
re o
f pa
tie
nts
be
twe
en s
hifts
AM
D o
f
Pa
tie
nt
Sa
fety
with A
MD
s
of
Clin
ica
l
Busin
ess
Units
Apr-
19
Ma
r-2
02
5%
GT
he
Ele
ctr
onic
Wa
rd B
oa
rd P
ilot ha
s e
nte
red into
its
fin
al P
DS
A ite
ratio
n. T
he
to
ol h
as b
ee
n w
ell
rece
ive
d b
y C
onsulta
nts
and
Drs
on W
ard
10
A (
Ga
str
o)
and is s
ucce
ssfu
lly r
eco
rdin
g s
enio
r o
wne
rship
/ invo
lve
me
nt (i
n r
espo
nse
to
Exte
rna
l Mo
rta
lity
Re
vie
w 2
01
8 a
nd the
He
alth
Educa
tio
n E
ngla
nd r
epo
rt w
hic
h s
tate
d tha
t Junio
r D
rs w
ere
n't
be
ing s
uppo
rte
d. A
ltho
ugh w
e w
ere
unde
rta
kin
g D
aily
Bo
ard
Ro
unds o
r re
vie
ws a
fte
r Jnr
Dr
Bo
ard
Ro
unds, e
vid
ence
wa
s r
equir
ed to
pro
ve
this
).
The
Ele
ctr
onic
Bo
ard
Ro
und r
equir
es a
n e
sca
latio
n le
ve
l to
be
ide
ntifie
d f
or
ea
ch p
atie
nt (a
s s
tipula
ted in the
NE
WS
2 P
olic
y):
wa
rd c
are
, cri
tica
l ca
re o
r e
nd o
f lif
e c
are
. T
he
be
ne
fits
of
the
syste
m a
re tha
t: w
e c
an c
orr
ela
te N
EW
S2
Sco
res a
ga
inst th
e
Esca
latio
n s
tatu
s / p
lan, w
e w
ill b
e a
ble
to
pro
duce
a li
st o
f pa
tie
nts
who
ne
ed to
be
se
en b
y the
Tra
nsfo
rm T
ea
m a
nd w
e w
ill
ha
ve
a li
st o
f pa
tie
nts
who
are
at ri
sk.
The
pilo
t ha
s h
ow
eve
r sho
wn tha
t th
e a
lloca
ted c
onsulta
nt fo
r e
ach p
atie
nt is
oft
en u
ncle
ar,
(T
he
re
spo
nsib
le c
onsulta
nt sho
uld
be
do
cum
ente
d a
bo
ve
the
pa
tie
nt's
be
d, in
the
nurs
ing h
ando
ve
r no
tes a
nd o
n M
edw
ay. T
he
sta
nda
rdis
ed n
urs
ing
do
cum
enta
tio
n tha
t w
as u
se
d to
ca
ptu
re this
info
rma
tio
n is n
o lo
nge
r in
co
nsis
tent use
and n
ee
ds to
be
fa
cto
red into
the
Do
cum
enta
tio
n P
roje
ct.)
EM
R
Actio
n 5
Re
vie
w s
tanda
rds o
f do
cum
enta
tio
n to
ensure
tha
t sta
ff a
lwa
ys s
ign a
nd d
ate
the
ir
entr
ies a
nd tha
t ha
ndo
ve
r o
f ca
re is c
lea
rly
do
cum
ente
d inclu
din
g the
re
spo
nsib
le
Co
nsulta
nt.
Ma
r-2
17
%R
De
dic
ate
d P
rogra
mm
e M
ana
ge
me
nt suppo
rt is n
ow
allo
ca
ted to
the
Tru
st's
Do
cum
enta
tio
n P
roje
ct in
ord
er
to e
nsure
tha
t th
e
sco
pe
of
wo
rk c
onsid
ers
all
of
the
long te
rm r
equir
em
ents
fo
r m
edic
s, nurs
ing a
nd the
rapie
s in li
ne
with the
IT
Ro
adm
ap.
Clin
ica
l No
ting is a
long w
ay o
ff o
n the
IT
Ro
adm
ap a
nd s
o d
iscussio
ns a
re u
nde
rwa
y w
ith the
Me
dw
ay T
ea
m to
add thre
e k
ey
do
cum
ents
to
the
ele
ctr
onic
Me
dw
ay (
Pa
tie
nt A
dm
inis
tra
tio
n S
yste
m)
to
suppo
rt the
nurs
ing te
am
s w
ith the
co
mple
tio
n o
f
do
cum
enta
tio
n.
To
da
te, a
sco
pin
g s
essio
n to
loo
k a
t nurs
ing d
ocum
enta
tio
n to
ok p
lace
on the
16
th J
uly
with w
ard
ma
na
ge
rs a
nd s
taff
nurs
es
fro
m a
cro
ss U
rge
nt C
are
and P
lanne
d C
are
. to
re
vie
w n
urs
ing r
isk a
sse
ssm
ent bo
okle
ts a
nd c
are
pla
ns. F
ee
dba
ck f
rom
the
gro
up w
as tha
t tim
e to
co
mple
te d
ocum
enta
tio
n w
as the
ma
in b
locka
ge
.
RC
A
Actio
n 3
Publis
h a
nd r
egula
rly a
udit a
ga
inst a
gre
ed
sta
nda
rds f
or
clin
ica
l do
cum
enta
tio
n; to
inclu
de
the
co
mple
tio
n o
f pa
thw
ays o
f ca
re
for
ke
y m
edic
al c
onditio
ns a
nd le
gib
le
pre
scri
bin
g. T
his
sho
uld
fo
rm p
art
of
str
uctu
red f
ee
dba
ck to
me
dic
al s
taff
.
Ongo
ing
50
%G
The
Tru
st pa
rtic
ipa
tes in the
re
gio
na
l be
nchm
ark
ing e
xe
cis
e A
dva
ncin
g Q
ua
lity. E
ve
ry m
onth
we
co
llect in
form
atio
n o
n c
are
for
the
fo
llow
ing c
onditio
ns: A
KI, A
RL
D, P
ne
um
onia
, D
iabe
tes, H
ip a
nd K
ne
e r
epla
ce
me
nt a
nd S
epsis
, H
ospita
l acquir
ed
pne
um
onia
(pilo
t).
The
me
asure
s f
or
adva
ncin
g q
ua
lity a
re b
ase
d o
n N
ICE
guid
elin
es f
or
be
st pra
ctice
.
EM
R
Actio
n 6
Re
vie
w n
urs
ing a
nd A
HP
do
cum
enta
tio
n to
ensure
tha
t it is f
it f
or
purp
ose
in f
ocusin
g a
nd
pro
mo
ting e
sse
ntia
l ca
re, pa
rtic
ula
rly f
luid
ba
lance
and n
utr
itio
na
l ne
eds.
Ma
r-2
15
%R
Upda
te a
s p
er
'Re
vie
w S
tanda
rds o
f D
ocum
enta
tio
n' a
bo
ve
.
EM
R
Actio
n 7
Ensure
pre
scri
bin
g is le
gib
le, cle
arly s
igne
d
and in li
ne
with n
atio
na
l exis
ting g
uid
elin
es f
or
ca
re. F
ocus initia
lly o
n o
pia
te p
rescri
bin
g in
line
with r
ece
nt G
ospo
rt r
epo
rt.
Ma
r-2
01
5%
RT
he
Go
spo
rt a
udits c
om
ple
ted w
ithin
So
uth
po
rt a
nd O
rmskir
k H
ospita
l Tru
st sho
we
d s
ignific
ant le
ve
ls o
f a
ssura
nce
apa
rt f
rom
the
do
cum
enta
tio
n o
f clin
ica
l indic
atio
ns f
or
dru
gs (
apa
rt f
rom
tho
se
who
are
actu
ally
dyin
g w
hic
h is b
ette
r) a
nd the
hig
h
incid
ence
of
pne
um
onia
as c
ause
of
de
ath
.
The
Tru
st is
de
dic
ate
d to
a M
edic
ine
s M
ana
ge
me
nt Im
pro
ve
me
nt a
nd O
ptim
isa
tio
n P
roje
ct w
hic
h is c
urr
ently
be
ing d
rive
n b
y a
de
taile
d a
ctio
n p
lan w
hic
h is s
ubje
ct to
we
ekly
scru
tiny a
nd p
lannin
g m
ee
tings. C
lea
r a
nd le
gib
le d
ocum
enta
tio
n in li
ne
with
na
tio
na
l guid
elin
es is to
be
inco
rpo
rate
d into
the
Do
cum
enta
tio
n P
roje
ct.
RC
A
Actio
n 4
Ongo
ing a
udit o
f physio
logic
al o
bse
rva
tio
n
co
mplia
nce
and f
luid
ba
lance
co
mple
tio
n m
ust
be
re
po
rte
d to
CB
U a
nd c
entr
ally
. A
ll C
BU
s
must cle
arly d
em
onstr
ate
ho
w the
y w
ill
impro
ve
obse
rva
tio
n c
om
plia
nce
and f
luid
ba
lance
co
mple
tio
n o
n the
ir w
ard
s a
nd
de
mo
nstr
ate
tha
t th
is is o
ccurr
ing.
Ja
n-1
9M
ar-
20
40
%G
As p
art
of
the
NH
SI Q
ua
lity Im
pro
ve
me
nt P
rogra
mm
e, a
PD
SA
im
pro
ve
me
nt cycle
ha
s b
ee
n u
nde
rta
ke
n o
n W
ard
9A
(S
ho
rt
Sta
y U
nit);
to
re
vie
w a
nd im
pro
ve
the
wa
y tha
t o
bse
rva
tio
ns a
re ta
ke
n, do
cum
ente
d a
nd r
evie
we
d.
Wo
rk is c
ontinuin
g to
re
duce
obse
rva
tio
n b
rea
che
s a
nd to
im
pro
ve
obse
rva
tio
ns c
om
plia
nce
aga
inst th
e T
rust's
The
Tru
st's
NE
WS
2 P
olic
y (
CL
IN C
OR
P 8
1 E
arly W
arn
ing T
rack &
Tri
gge
r S
yste
m O
pe
ratio
na
l Po
licy.)
The
Tru
st ha
s inve
ste
d in a
Flu
id B
ala
nce
mo
dule
on V
ita
lPa
c (
Syste
m C
) w
hic
h w
ill e
lectr
onic
ally
re
co
rd f
luid
ba
lance
che
cks
and p
rovid
e r
epo
rtin
g b
y w
ard
to
me
asure
co
mplia
nce
leve
ls a
ga
inst sta
nda
rds. T
he
ro
ll o
ut o
f th
e p
roduct is
expe
cte
d in the
ne
ar
futu
re w
ith a
sta
rt d
ate
to
be
co
nfirm
ed.
Do
cto
rs’ R
ota
s t
o
be
Re
vie
we
d
(to
en
su
re
su
ffic
ien
t d
ail
y
se
nio
r c
ov
er
&
jun
ior
do
cto
r
su
pp
ort
)
Are
a R
eq
uir
ing
Imp
rov
em
en
t
On
go
ing
au
dit
of
ph
ys
iolo
gic
al
ob
se
rva
tio
n
co
mp
lia
nc
e a
nd
flu
id b
ala
nc
e
co
mp
leti
on
Senior Ownership
Cle
ar
Se
nio
r
Cli
nic
al
Le
ad
Re
vie
w S
tan
da
rds
of
Do
cu
me
nta
tio
n
Re
vie
w N
urs
ing
an
d A
HP
Do
cu
me
nta
tio
n
Documentation & Observations
En
su
re P
res
cri
bin
g
is l
eg
ible
, c
lea
rly
sig
ne
d a
nd
in
lin
e
wit
h n
ati
on
al
exis
tin
g g
uid
eli
ne
s
for
ca
re.
Cli
nic
al
Do
cu
me
nta
tio
n
Au
dit
s
Apr-
19
De
puty
Dir
ecto
r o
f
Nurs
ing
De
teri
ora
ting
Pa
tie
nt P
roje
ct
('S
enio
r
Ow
ne
rship
')
Do
cum
enta
tio
n'
Pro
ject
De
teri
ora
ting
Pa
tie
nt P
roje
ct
('O
bse
rva
tio
ns
&
Do
cum
enta
tio
n'
)
Page 56 of 210

17
Exte
rnal M
ort
ality
Acti
on
Pla
n, B
oard
Assu
ran
ce R
ep
ort
– P
ag
e 4
EM
BA
R
Th
e E
xte
rnal
Mo
rtali
ty A
cti
on
Pla
n (
Inclu
din
g 7
RC
A C
ases)
Bo
ard
Pro
gre
ss A
ssu
ran
ce R
ep
ort
2019-2
1
Ori
gin
Re
co
mm
en
da
tio
n D
eta
il
Pro
gra
mm
e /
Pro
jec
t
Le
ad
(s)
Sta
rt
Da
te
Pro
jec
ted
Co
mp
leti
o
n D
ate
Co
mp
leti
o
n %
BR
AG
U
pd
ate
21
st
Oc
tob
er
20
19
EM
R
Actio
n 7
Ensure
pre
scri
bin
g is le
gib
le, cle
arly s
igne
d
and in li
ne
with n
atio
na
l exis
ting g
uid
elin
es f
or
ca
re. F
ocus initia
lly o
n o
pia
te p
rescri
bin
g in
line
with r
ece
nt G
ospo
rt r
epo
rt.
Ma
r-2
01
5%
RT
he
Go
spo
rt a
udits c
om
ple
ted w
ithin
So
uth
po
rt a
nd O
rmskir
k H
ospita
l Tru
st sho
we
d s
ignific
ant le
ve
ls o
f a
ssura
nce
apa
rt f
rom
the
do
cum
enta
tio
n o
f clin
ica
l indic
atio
ns f
or
dru
gs (
apa
rt f
rom
tho
se
who
are
actu
ally
dyin
g w
hic
h is b
ette
r) a
nd the
hig
h
incid
ence
of
pne
um
onia
as c
ause
of
de
ath
.
The
Tru
st is
de
dic
ate
d to
a M
edic
ine
s M
ana
ge
me
nt Im
pro
ve
me
nt a
nd O
ptim
isa
tio
n P
roje
ct w
hic
h is c
urr
ently
be
ing d
rive
n b
y a
de
taile
d a
ctio
n p
lan w
hic
h is s
ubje
ct to
we
ekly
scru
tiny a
nd p
lannin
g m
ee
tings. C
lea
r a
nd le
gib
le d
ocum
enta
tio
n in li
ne
with
na
tio
na
l guid
elin
es is to
be
inco
rpo
rate
d into
the
Do
cum
enta
tio
n P
roje
ct.
RC
A
Actio
n 4
Ongo
ing a
udit o
f physio
logic
al o
bse
rva
tio
n
co
mplia
nce
and f
luid
ba
lance
co
mple
tio
n m
ust
be
re
po
rte
d to
CB
U a
nd c
entr
ally
. A
ll C
BU
s
must cle
arly d
em
onstr
ate
ho
w the
y w
ill
impro
ve
obse
rva
tio
n c
om
plia
nce
and f
luid
ba
lance
co
mple
tio
n o
n the
ir w
ard
s a
nd
de
mo
nstr
ate
tha
t th
is is o
ccurr
ing.
Ja
n-1
9M
ar-
20
40
%G
As p
art
of
the
NH
SI Q
ua
lity Im
pro
ve
me
nt P
rogra
mm
e, a
PD
SA
im
pro
ve
me
nt cycle
ha
s b
ee
n u
nde
rta
ke
n o
n W
ard
9A
(S
ho
rt
Sta
y U
nit);
to
re
vie
w a
nd im
pro
ve
the
wa
y tha
t o
bse
rva
tio
ns a
re ta
ke
n, do
cum
ente
d a
nd r
evie
we
d.
Wo
rk is c
ontinuin
g to
re
duce
obse
rva
tio
n b
rea
che
s a
nd to
im
pro
ve
obse
rva
tio
ns c
om
plia
nce
aga
inst th
e T
rust's
The
Tru
st's
NE
WS
2 P
olic
y (
CL
IN C
OR
P 8
1 E
arly W
arn
ing T
rack &
Tri
gge
r S
yste
m O
pe
ratio
na
l Po
licy.)
The
Tru
st ha
s inve
ste
d in a
Flu
id B
ala
nce
mo
dule
on V
ita
lPa
c (
Syste
m C
) w
hic
h w
ill e
lectr
onic
ally
re
co
rd f
luid
ba
lance
che
cks
and p
rovid
e r
epo
rtin
g b
y w
ard
to
me
asure
co
mplia
nce
leve
ls a
ga
inst sta
nda
rds. T
he
ro
ll o
ut o
f th
e p
roduct is
expe
cte
d in the
ne
ar
futu
re w
ith a
sta
rt d
ate
to
be
co
nfirm
ed.
EM
R
Actio
n 8
Re
vie
w e
sca
latio
n a
nd c
eili
ngs o
f ca
re
po
licie
s to
inclu
de
tim
ely
acce
ss to
cri
tica
l
ca
re a
nd e
nd o
f lif
e c
are
. In
clu
de
a f
ocus o
n
tra
inin
g o
f a
ll sta
ff in a
ccura
te c
alc
ula
tio
ns o
f
Ea
rly W
arn
ing S
co
res (
EW
S),
inte
rpre
tatio
n
and c
onte
xtu
alis
atio
n o
f E
WS
and a
sha
red
unde
rsta
ndin
g o
f w
he
n to
esca
late
ca
re a
nd
co
nsid
er
a s
tructu
red c
om
munic
atio
n
appro
ach s
uch a
s S
itua
tio
n, B
ackgro
und,
Asse
ssm
ent, R
eco
mm
enda
tio
n (
SB
AR
).
Ja
n-1
9Jun-1
98
0%
G
RC
A
Actio
n 5
Imple
me
nt th
e R
CP
/NIC
E N
EW
S2
physio
logic
al m
onito
ring p
roce
ss, w
ith c
lea
r
pa
thw
ays f
or
the
mo
nito
ring a
nd e
sca
latio
n o
f
ele
va
ted s
co
res to
se
nio
r de
cis
ion m
ake
rs.
This
must in
clu
de
a r
egula
r se
nio
r re
vie
w o
f
the
appro
pri
ate
ne
ss o
f e
sca
latio
n p
lans f
or
eve
ry inpa
tie
nt a
s a
n inte
gra
l pa
rt o
f e
ve
ry
wa
rd a
nd b
oa
rd r
ound. A
ll clin
ica
l sta
ff s
ho
uld
be
aw
are
of
the
NE
WS
2 s
co
re f
or
esca
latio
n, w
ho
to
, a
nd w
ha
t sho
uld
be
expe
cte
d f
rom
the
se
nio
r de
cis
ion m
ake
r.
Ja
n-1
9Jun-1
98
0%
G
Are
a R
eq
uir
ing
Imp
rov
em
en
t
On
go
ing
au
dit
of
ph
ys
iolo
gic
al
ob
se
rva
tio
n
co
mp
lia
nc
e a
nd
flu
id b
ala
nc
e
co
mp
leti
on
Asso
cia
te
Me
dic
al
Dir
ecto
r o
f
Pa
tie
nt
Sa
fety
Ph
ys
iolo
gic
al
Mo
nit
ori
ng
Pro
ce
ss
Appropirate Escalation
Re
vie
w E
sc
ala
tio
n
an
d C
eil
ing
s o
f
Ca
re P
oli
cie
s
Documentation & Observations
En
su
re P
res
cri
bin
g
is l
eg
ible
, c
lea
rly
sig
ne
d a
nd
in
lin
e
wit
h n
ati
on
al
exis
tin
g g
uid
eli
ne
s
for
ca
re.
Apr-
19
De
puty
Dir
ecto
r o
f
Nurs
ing
De
teri
ora
ting
Pa
tie
nt P
roje
ct
('A
ppro
pri
ate
Esca
latio
n')
Do
cum
enta
tio
n'
Pro
ject
De
teri
ora
ting
Pa
tie
nt P
roje
ct
('O
bse
rva
tio
ns
&
Do
cum
enta
tio
n'
)
The
Tru
st's
NE
WS
2 P
olic
y (
CL
IN C
OR
P 8
1 E
arly W
arn
ing T
rack &
Tri
gge
r S
yste
m O
pe
ratio
na
l Po
licy)
ha
s b
ee
n r
atifie
d is
live
in the
Tru
st's
inte
rna
l on-lin
e P
olic
y P
ort
folio
.
Lin
k N
urs
es (
on e
ach w
ard
) ha
ve
be
en tra
ine
d w
ith the
re
mit to
ca
sca
de
tra
inin
g. A
n e
lectr
onic
tra
inin
g m
odule
is b
ein
g
inve
stiga
ted. T
rain
ing m
ode
ls a
re b
ein
g r
evie
we
d to
ensure
appro
pri
ate
suppo
rt o
f th
e li
nk n
urs
e p
rogra
me
.
As d
eta
iled a
bo
ve
, a
min
i im
pro
ve
me
nt pro
ject is
be
ing u
nde
rta
ke
n o
n W
ard
9A
(S
ho
rt S
tay U
nit)
to
incre
ase
obse
rva
tio
ns in
line
the
po
licy to
95
% b
y S
epte
mbe
r 2
01
9. O
nce
the
blu
epri
nt fo
r be
st pra
ctice
ha
s b
ee
n e
sta
blis
he
d, th
is w
ill b
e r
olle
d o
ut
acro
ss the
Tru
st to
ensure
tha
t co
mplia
nce
leve
ls a
re m
ain
tain
ed to
eff
ective
ly s
uppo
rt e
sca
latio
n o
f th
e d
ete
rio
rating p
atie
nt.
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 57 of 210

18
Exte
rnal M
ort
ality
Acti
on
Pla
n, B
oard
Assu
ran
ce R
ep
ort
– P
ag
e 5
EM
BA
R
Th
e E
xte
rnal
Mo
rtali
ty A
cti
on
Pla
n (
Inclu
din
g 7
RC
A C
ases)
Bo
ard
Pro
gre
ss A
ssu
ran
ce R
ep
ort
2019-2
1
Ori
gin
Re
co
mm
en
da
tio
n D
eta
il
Pro
gra
mm
e /
Pro
jec
t
Le
ad
(s)
Sta
rt
Da
te
Pro
jec
ted
Co
mp
leti
o
n D
ate
Co
mp
leti
o
n %
BR
AG
U
pd
ate
21
st
Oc
tob
er
20
19
EM
R
Actio
n 1
0
Ensure
tha
t in
div
idua
l end o
f lif
e c
are
pla
ns
are
co
mm
ence
d p
rom
ptly
and tha
t th
e c
are
pla
ns a
re w
ell
do
cum
ente
d inclu
din
g p
refe
rre
d
pla
ce
of
ca
re. C
onsid
er
wid
er
use
of
Em
erg
ency H
ea
lth C
are
Pla
ns to
pre
ve
nt
rea
dm
issio
n f
or
pa
tie
nts
appro
achin
g the
end
of
the
ir li
fe.
Se
p-1
8M
ar-
21
30
%G
Str
ata
He
alth
ca
re h
as p
rese
nte
d a
n e
lectr
onic
so
lutio
n to
suppo
rt the
de
live
ry o
f a
sin
gle
Pa
tie
nt A
nticip
ato
ry C
linic
al
Ma
na
ge
me
nt P
lan (
AC
MP
) a
cro
ss a
ll lo
ca
l he
alth
ca
re p
rovid
ers
.
A ta
rge
ted tra
inin
g p
rogra
mm
e is b
ein
g d
eve
lope
d a
s p
art
of
the
Futu
re C
are
Pla
nnin
g w
ork
str
ea
m o
f th
e O
lde
r P
eo
ple
s' C
are
Pro
gra
mm
e. T
he
fin
din
gs o
f th
e N
atio
na
l Audit o
f C
are
at E
nd o
f L
ife
are
info
rmin
g a
nd s
uppo
rtin
g the
ca
se
fo
r A
dva
nce
Ca
re
Pla
nnin
g a
nd the
Anticip
ato
ry C
linic
al M
ana
ge
me
nt P
lannin
g m
ode
l.
EM
R
Actio
n 1
1
Ensure
de
ve
lopm
ent o
f a
mo
re r
obust
mo
rta
lity r
evie
w p
roce
ss w
ith c
entr
al
repo
rtin
g. T
he
re s
ho
uld
be
an e
mpha
sis
on
dis
se
min
atio
n o
f le
arn
ing f
rom
de
ath
s a
cro
ss
all
spe
cia
ltie
s w
ith invo
lve
me
nt fr
om
me
dic
al,
nurs
ing a
nd a
llie
d h
ea
lthca
re p
rofe
ssio
na
ls.
and inclu
din
g c
olle
ague
s f
rom
Pri
ma
ry C
are
.
Jul-1
8M
ar-
20
50
%G
The
Scre
enin
g o
f de
ath
s incre
ase
d f
rom
32
.9%
in M
ay to
90
.5%
in S
epte
mbe
r. T
his
hig
h le
ve
l of
scre
enin
g w
as c
arr
ied
thro
ugh into
August w
he
n 8
4.6
% o
f de
ath
s w
ere
re
vie
we
d. T
he
incre
ase
d c
om
plia
nce
is a
ttri
bute
d to
im
pro
ve
d a
cce
ss to
IT
and e
ffe
ctive
co
mm
unic
atio
ns. T
he
AM
D f
or
pa
tie
nt sa
fety
ha
s b
ee
n m
ee
ting w
ith le
ads f
rom
ea
ch d
epa
rtm
ent to
dis
cuss
ba
rrie
rs to
the
co
mple
tio
n o
f S
JR
s.
Re
co
gnitio
n o
f th
ose
like
ly to
be
dyin
g incre
asin
g -
59
% h
ad a
n indiv
idua
l pla
n f
or
the
ca
re o
f th
ose
tho
ught lik
ely
to
be
dyin
g
de
ve
lope
d w
ith the
m a
nd tho
se
im
po
rta
nt to
the
m (
20
18
/19
). D
ocum
enta
tio
n o
f in
div
idua
l pla
ns f
or
ca
re o
f th
ose
tho
ught lik
ely
to b
e d
yin
g im
pro
vin
g, but still
a lo
ng w
ay to
go
- e
duca
tio
n is o
ngo
ing. 6
6%
pe
ople
who
die
in h
ospita
l ha
ve
do
cum
ente
d
pre
ferr
ed p
lace
of
ca
re a
nd f
or
the
se
70
% a
chie
ve
d it by d
yin
g in h
ospita
l (2
01
8/1
9).
12
7 p
eo
ple
who
PP
C w
as n
ot ho
spita
l
we
re tra
nsfe
rre
d in the
Ra
pid
End o
f L
ife
Tra
nsfe
r pro
ce
ss w
he
n d
yin
g w
as r
eco
gnis
ed a
nd a
che
ive
d the
ir P
PC
. (2
01
8/1
9).
Me
mbe
rs o
f th
e R
educin
g A
vo
ida
ble
Mo
rta
lity a
nd the
Old
er
Pe
ople
's C
are
Pro
ject G
roups a
re c
olla
bo
rating o
n F
utu
re C
are
Pla
nnin
g a
ctivity; in p
art
icula
r th
e c
ultu
ral s
hift to
wa
rds p
roa
ctive
Anticip
ato
ry C
linic
al M
ana
ge
me
nt P
lannin
g a
nd a
syste
m
wid
e a
ppro
ach to
Ca
re M
ana
ge
me
nt P
lans.
RC
A
Actio
n 6
Mo
rta
lity a
nd M
orb
idity r
evie
w m
ust o
ccur
in
de
pa
rtm
ents
with e
vid
ence
pro
duce
d o
f
agre
ed a
ctio
ns a
nd im
pro
ve
me
nt pro
jects
, a
s
de
fine
d b
y the
ca
se
s p
rese
nte
d. T
he
se
impro
ve
me
nts
, ge
ne
rate
d b
y c
linic
al t
ea
ms,
must ha
ve
evid
ence
of
revie
w b
y C
BU
and
se
nio
r m
ana
ge
me
nt to
de
mo
nstr
ate
ope
nly
ho
w c
ha
nge
is s
uppo
rte
d.
Jul-1
8M
ar-
20
50
%A
The
Tru
st's
Mo
rta
lity R
epo
rt h
as b
ee
n r
ede
sig
ne
d to
pro
vid
e m
onth
ly a
ssura
nce
aro
und L
ea
rnin
g f
rom
De
ath
s. L
ea
rnin
g f
rom
De
ath
s is a
lso
a s
tanda
lone
wo
rk s
tre
am
in the
ne
wly
re
vis
ed T
rust M
ort
alit
y P
roje
ct; R
eco
gnitio
n a
nd C
are
of
the
De
teri
ora
ting P
atie
nt. T
he
ove
rrid
ing o
bje
ctive
is to
ensure
the
mo
st e
ffe
ctive
dis
se
min
atio
n o
f le
sso
ns le
arn
ed w
ith
assura
nce
tha
t le
arn
ing h
as b
ee
n e
mbe
dde
d.
A s
tructu
re h
as b
ee
n a
gre
ed in p
rincip
le to
ide
ntify
a g
ove
rna
nce
lea
d c
linic
ian in e
ach C
BU
to
dri
ve
to
M&
M p
roce
sse
s a
nd
ide
ntify
the
ke
y w
ork
str
ea
ms f
or
impro
ve
me
nt w
hic
h w
ill in turn
be
re
po
rte
d to
the
Mo
rta
lity O
pe
ratio
na
l Gro
up. A
mo
nth
ly
lesso
ns le
arn
ed b
ulle
tin c
asca
de
s the
ge
ne
ral l
esso
ns f
rom
Le
ve
l 2 S
tructu
red J
udge
me
nt R
evie
ws tha
t a
re e
sca
late
d to
MO
G.
The
Asso
cia
te M
edic
al D
ire
cto
r fo
r P
atie
nt C
are
is w
ork
ing w
ith the
Clin
ica
l Le
ad f
or
Educa
tio
n to
inco
rpo
rate
lesso
ns
lea
rne
d d
isse
min
atio
n thro
ugh the
junio
r do
cto
rs tra
inin
g p
rogra
mm
e. T
he
AM
D f
or
Pa
tie
nt S
afe
ty, C
linic
al L
ea
d f
or
Educa
tio
n
and H
ea
d o
f R
isk a
re to
me
et to
dis
cuss the
de
ve
lopm
ent o
f be
st pra
ctice
.
RC
A
Actio
n 7
Re
vie
w a
nd u
pda
te the
tru
sts
po
licy a
nd
appro
ach to
the
ma
na
ge
me
nt o
f in
pa
tie
nt
dia
be
tes. E
nsure
ava
ilable
, cle
ar
guid
ance
exis
ts f
or
the
ma
na
ge
me
nt o
f dia
be
tic
Tbc
CD
Me
dic
ine
/
AM
D o
f
Urg
ent C
are
Apr-
19
Ma
r-2
15
0%
AR
ecru
itm
ent fo
r D
iabe
tes a
nd E
ndo
cro
no
logy C
onsulta
nt co
ve
r is
no
w u
nde
rwa
y a
nd w
ill a
ddre
ss the
long te
rm g
ap le
ft w
he
n
the
co
mm
unity s
erv
ice
s w
ere
co
ntr
acte
d o
ut in
20
17
. T
he
Me
dic
al D
ire
cto
r is
org
anis
ing a
re
vie
w o
f dia
be
tes s
erv
ice
.
RC
A
Actio
n 8
Re
vie
w a
nd u
pda
te the
tru
sts
appro
ach to
the
pro
vis
ion o
f a
cute
pa
in s
erv
ice
s, to
inclu
de
the
ava
ilable
guid
ance
to
no
n-s
pe
cia
list
do
cto
rs o
n a
ba
sic
pha
rma
co
logic
str
ate
gy,
Tbc
Acute
Pa
in
Le
ad / C
D
Ana
esth
etic
s
Apr-
19
Ma
r-2
13
0%
AT
he
Tru
st ha
s o
ne
Pa
in S
pe
cia
list N
urs
e w
ho
co
ve
rs b
oth
acute
and c
hro
nic
pa
in. D
r H
old
en, C
linic
al L
ea
d f
or
Educa
tio
n is
wo
rkin
g o
n a
ba
sic
sta
nda
rd f
or
the
adm
inis
tra
tio
n o
f a
na
lga
esic
s.
Are
a R
eq
uir
ing
Imp
rov
em
en
t
Mo
rta
lity
&
Mo
rbid
ity R
ev
iew
s
mu
st
oc
cu
r in
de
pa
rtm
en
ts w
ith
ev
ide
nc
e p
rod
uc
ed
of
ag
ree
d a
cti
on
s
an
d i
mp
rov
em
en
t
pro
jec
ts
Ma
na
ge
me
nt
of
Dia
be
tes
Ac
ute
Pa
in
Se
rvic
es
De
teri
ora
ting
Pa
tie
nt P
roje
ct
('F
utu
re C
are
Pla
nnin
g')
De
teri
ora
ting
Pa
tie
nt P
roje
ct
('F
utu
re C
are
Pla
nnin
g')
Specialist
En
su
re p
rom
pt
co
mm
en
ce
me
nt
of
we
ll d
oc
um
en
ted
ind
ivid
ua
l e
nd
of
life
ca
re p
lan
s
Learning from Deaths Future Care
Ro
bu
st
mo
rta
lity
rev
iew
pro
ce
ss
wit
h c
en
tra
l
rep
ort
ing
wit
h a
foc
us
of
dis
em
ina
tio
n o
f
lea
rnin
g f
rom
de
ath
s.
Asso
cia
te
Me
dic
al
Dir
ecto
r o
f
Pa
tie
nt
Sa
fety
with
Asso
cia
te
Dir
ecto
r o
f
Inte
gra
ted
Go
ve
rna
nce
Me
dic
al &
Educa
tio
n
Dir
ecto
r,
Que
ensco
ur
t H
ospic
e
Page 58 of 210

19
Ap
pen
dix
2 –
Re
co
gn
itio
n a
nd
Ca
re o
f th
e D
ete
rio
rati
ng
Pa
tien
t P
roje
ct
Hig
hlig
ht
Re
po
rt
Pro
gra
mm
e
Sta
rt D
ate
B
RA
G f
or
pro
gre
ss o
f acti
vit
y ag
ain
st
pro
jecte
d
tim
efr
am
es
A
En
d D
ate
31st
Marc
h 2
021
Pro
ject
Man
ag
er
Rach
el F
loo
d-J
on
es, P
roje
ct
Man
ag
er
Pro
gra
mm
e H
igh
lig
ht
Re
po
rt
Reco
gn
itio
n a
nd
Care
of
the D
ete
rio
rati
ng
Pati
en
t (R
CD
P)
(Form
erl
y 'R
ed
ucin
g A
void
ab
le M
ort
alit
y' P
roje
ct)
Re
co
gn
itio
n a
nd
Care
of
the
De
teri
ora
tin
g
Pati
en
tE
xe
cu
tiv
e S
po
nso
rD
r T
err
y H
an
kin
, M
ed
ical D
ire
cto
rB
RA
G f
or
KP
I actu
al v
ers
us in
mo
nth
targ
et
R
Info
rmati
on
Le
ad
M
ike
Lig
htf
oo
t, H
ead
of
Info
rmati
on
/
Am
an
da H
als
all In
form
ati
on
An
aly
st
Re
po
rtin
g T
oM
ort
ality
Op
era
tio
nal G
rou
p / Q
uality
& S
afe
ty
(Im
pro
ve
me
nt
Bo
ard
) G
rou
p
Re
po
rt D
ate
13th
No
ve
mb
er
2018 fo
r H
osp
ital M
an
ag
em
en
t B
oard
21st
No
ve
mb
er
2019
1st
Ap
ril 2019
Clin
ical L
ead
Dr
Ch
ris G
od
dard
, A
MD
Pati
en
t S
afe
ty
EX
EC
UT
IVE
SU
MM
AR
Y
(Wh
at
we
are
try
ing
to
ac
hie
ve
an
d w
he
re w
e a
re t
o t
arg
et)
The
Mo
nth
by M
onth
Ho
sp
ital S
tand
ard
Mo
rtalit
y R
atio
is inhe
rently u
nsta
ble
. It
is a
ffe
cte
d b
y the
num
be
r o
f d
eath
s in that m
onth
and
the
case
mix
, w
hic
h c
hang
es. It
do
es h
ow
eve
r allo
w a
naly
sis
of
what th
e u
nd
erlyin
g c
ontr
ibuto
rs a
re. T
he
se
are
the
cause
s o
f d
em
and
cap
acity m
ism
atc
h. T
his
mo
nth
(H
SM
R 6
1.5
) d
ischarg
e a
nd
AE
D f
low
im
pro
ve
d d
ram
atically
– thus the
syste
m c
ould
co
pe
be
tte
r w
ith d
em
and
.
The
Ro
lling
HS
MR
and
SH
MI
giv
e a
be
tte
r in
dic
atio
n o
f d
ire
ctio
n o
f tr
ave
l. T
he
tre
nd
of
bo
th is to
ward
s im
pro
ve
me
nt, a
gain
re
fle
cting
the
inve
stm
ent m
ad
e in q
ualit
y.
Cap
acity a
nd
De
mand
must b
e a
ctive
ly m
anag
ed
, sho
uld
de
mand
incre
ase
, co
mm
ensura
te incre
ase
s in c
ap
acity a
re r
eq
uire
d to
main
tain
safe
ty. T
his
is n
ot ju
st atte
nd
ance
at A
ED
, b
ut can b
e a
cro
ss d
iffe
rent p
art
s o
f th
e s
yste
m inclu
din
g inp
atie
nt
ward
s –
what is
our
surg
e p
lan a
nd
ho
w is it g
ove
rne
d / a
ctivate
d?
Mo
rtalit
y s
cre
enin
g r
ate
s r
em
ain
aro
und
90
%, 1
17
SJR
s w
ere
pe
rfo
rme
d in 2
01
8-2
01
9, w
hic
h is the
targ
et and
has b
ee
n m
et. T
he
challe
ng
e n
ow
is u
sin
g this
info
rmatio
n to
id
entify
and
pro
po
se
im
pro
ve
me
nt w
ork
. T
he
first are
as w
ill b
e e
nd
of
life
care
, A
KI
and
fra
ctu
red
Ne
ck o
f F
em
ur.
The
Bo
ard
is a
ske
d to
re
ce
ive
the
re
po
rt f
or
assura
nce
, th
e m
easure
s f
or
mo
rtalit
y a
long
sid
e d
eta
il o
f th
e a
ctivity s
up
po
rtin
g the
im
pro
ve
me
nt o
f q
ualit
y o
f care
and
pe
rfo
rmance
.
SM
AR
T O
BJ
EC
TIV
ES
(Sp
ec
ific
-Me
as
ura
ble
-Att
ain
ab
le-R
ele
va
nt-
Tim
e b
ou
nd
)
To
de
vis
e c
on
tin
uo
us
se
lf-
imp
rov
em
en
t s
tru
ctu
res
wh
ich
pro
ac
tiv
ely
id
en
tify
clin
ica
l d
ete
rio
rati
on
wit
hin
ou
r c
om
mu
nit
y s
o t
ha
t b
y M
arc
h 2
02
1:
Mo
rtalit
y ind
icto
rs s
it p
rem
ane
ntly w
ithin
co
nfid
ence
inte
rvals
(S
HM
I, H
SM
R &
Lo
cal S
MR
)
All
end
of
life
patie
nts
to
have
an A
nticip
ato
ry C
linic
al M
anag
em
ent P
lan
Ad
vance
Care
Pla
nnin
g is b
usin
ess a
s u
sual w
ith s
taff
co
nfid
ent to
have
co
nve
rsatio
ns w
ith p
atie
nts
and
fam
ilie
s
Jo
ine
d u
p w
ork
ing
and
se
em
less c
olla
bo
ratio
n b
etw
ee
n p
rim
ary
care
, acute
care
, co
mm
unity s
erv
ice
pro
vid
ers
and
care
ho
me
s to
de
live
r th
e m
ost ap
pro
priate
care
fo
r p
atie
nts
in lin
e w
ith A
CP
, A
CM
P a
nd
GS
F.
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 59 of 210

20
MIL
ES
TO
NE
/ W
OR
K S
TR
EA
M / K
EY
AC
TIV
ITY
Sta
rt d
ate
En
d d
ate
Ow
ne
r /
Le
ad
Co
mp
leti
on
%
BR
AG
Se
nio
r O
wn
ers
hip
& A
pp
rop
ria
te E
sc
ala
tio
n
Ele
ctr
on
ic W
ard
Bo
ard
Ro
un
d
PD
SA
Pilo
t on G
astr
o W
ard
03/0
6/2
019
30/0
3/2
020
AM
D P
atie
nt
Safe
ty
20%
RT
he
re r
em
ain
s a
blo
ckag
e w
hic
h h
as c
au
se
d a
2 m
on
th d
ela
y to
date
: IT
fix
es r
eq
uir
ed
to
mo
ve
th
e p
ilo
t fo
rward
are
on
ho
ld a
t th
e t
ime
of
rep
ort
ing
du
e t
o s
taff
ing
le
ve
ls in
th
e IT
de
ve
lop
me
nt
team
. (
Cf
Ris
k L
og
).
A s
cre
en is
bein
g s
ecure
d for
the fin
al c
ycle
of th
e p
ilot on W
ard
11B
whic
h w
ill la
st fo
r a furt
her
2 w
eeks
. T
he p
ilot is
als
o to b
e
ext
ended to w
ard
14A
(O
rthopaedic
Ward
- S
urg
ery
). O
nce a
robust and a
ppro
ved m
odel h
as b
een d
eve
loped, th
e p
lan is
to r
oll
out
acro
ss w
ard
s in
line w
ith the w
ard
refu
rbis
hm
ent pro
gra
mm
e (
a p
riva
te r
oom
and s
cre
ens w
ill b
e r
equired o
n e
very
ward
).
LA
TE
ST
UP
DA
TE
FO
R H
IGH
LIG
HT
RE
PO
RT
Pro
jec
t R
es
co
pin
g
21/1
0/2
019
15/1
1/2
019
R F
lood-J
ones
85%
A5 o
f 6 r
equired r
e-s
copin
g s
essio
ns h
ave
now
been h
eld
and d
ocum
ente
d.
Drive
r D
iagra
ms a
re w
ith w
ork
str
eam
gro
ups for
feedback
ahead o
f second s
essio
n for
feedback.
Th
ere
is a
re
qu
ire
me
nt
for
the
Tru
st
Do
cu
me
nta
tio
n P
rog
ram
me
to
be
sco
pe
d in
lin
e w
ith
th
e O
pe
rati
on
al S
trate
gy
in lin
e
wit
h V
isio
n 2
020
Concern
s r
ais
ed a
t D
ete
riora
ting P
atie
nt O
pera
tional G
roup r
egard
ing id
entif
icatio
n o
f C
onsulta
nt re
view
in m
edic
al n
ote
s –
Consulta
nts
are
to b
e e
ncoura
ged to c
arr
y and u
se n
am
e s
tam
ps. A
n u
pdate
is e
xpecte
d a
t th
e n
ext
Gro
up M
eetin
g o
n 1
5th
Octo
ber.
The T
rust's
Docum
enta
tion P
roje
ct is
bein
g r
evi
site
d b
y a n
ew
Pro
gra
mm
e O
ffic
e L
ead.
OB
SE
RV
AT
ION
S &
ES
CA
LA
TIO
NS
:
Tim
ely
Ob
se
rva
tio
ns
(P
DS
A -
Wa
rd 9
A)
(95
% o
f p
atie
nts
on W
ard
9A
to
have
the
ir o
bse
rvatio
ns p
erf
orm
ed
as p
er
Tru
st P
olic
y b
y S
ep
tem
be
r 2
01
9 (
mo
de
l to
be
de
sig
ne
d,
tria
lled
and
the
n to
be
ro
lled
out acro
ss o
the
r w
ard
s)
12/0
6/2
019
30/0
9/2
019
Clin
ical Q
ualit
y
Lead
25%
RO
bse
rvati
on
Bre
ach
es f
or
the
Tru
st
req
uir
e im
me
dia
te a
tte
nti
on
. T
he
PD
SA
cyc
le o
n W
ard
9A
is b
ein
g e
xte
nd
ed
on
to W
ard
14B
The fin
din
gs o
f th
e P
DS
A c
ycle
on W
ard
9A
pre
sente
d a
t th
e N
HS
I QI E
vent 12th
Septe
mber
report
ed s
uccess thro
ugh the follo
win
g
changes:
Move
fro
m b
edsid
e d
iscussio
n o
f patie
nts
observ
atio
ns to o
rganis
ed g
roup
Handove
r m
eeitn
gs (
with
access to the e
lectr
onic
data
on Ip
ads).
Incre
ased e
ducatio
n a
nd v
isib
ility
of O
bserv
atio
ns c
om
plia
nce le
vels
for
the w
ard
to d
rive
corr
ect activ
ty.
Dis
cuss N
EW
S2 S
core
s in
R2G
Board
Rounds to in
cre
ase u
niv
ers
al a
ware
ness o
f hig
h s
coring p
atie
nts
.
Set tim
es for
observ
atio
ns to b
e take
n 6
tim
es e
very
24 h
ours
.
Co
ns
ult
an
t R
ev
iew
(D
oc
um
en
tati
on
)23/0
7/2
019
30/1
0/2
019
Lead T
bc
10%
A
Le
arn
ing
fro
m D
ea
ths
S
tru
ctu
re J
ud
ge
me
nt
Re
vie
w M
eth
od
01/0
4/2
019
30/0
3/2
020
AM
D P
atie
nt
Safe
ty
70%
RT
he S
cre
enin
g o
f death
s in
cre
ased to
90.7
% for
Octo
ber
2019
. There
is a
n in
cre
asin
g b
ackl
og o
f S
JR r
evi
ew
s in
surg
ery
and o
rthopaedic
s, m
edic
ine a
nd IC
U a
re c
urr
ently
perf
orm
ing w
ell.
This
is
main
ly b
ein
g d
rive
n b
y clin
ical c
apacity
(re
view
s take
1-2
hours
) and the im
passe c
aused b
y th
e la
ck
of cla
rity
ove
r jo
b p
lannin
g.
Revi
ew
ers
do n
ot have
this
work
recognis
ed in
the c
urr
ent jo
b p
lannin
g s
tructu
re. A
meetin
g o
f m
ort
alit
y le
ads is
to b
e a
rranged to
addre
ss the is
sues.
Fu
ture
Ca
re P
lan
nin
g
Ad
va
nc
e C
are
Pla
nn
ing
: s
up
po
rtin
g d
isc
us
sio
ns
wit
h
Pa
tie
nts
an
d F
am
ilie
s
01/0
4/2
019
30/0
9/2
020
Pro
ject M
anager
/
Fra
ilty
Pra
ctit
ioner
5%
RS
trata
Netw
ork
ing S
olu
tions h
ave
pro
posed a
paperless s
olu
tion for
a s
ingle
ele
ctr
onic
AC
MP
- there
are
issues w
ith the g
ove
rnance
and p
ace u
nder
whic
h S
trata
are
curr
ently
slo
wly
deliv
ering p
rogre
ss. T
here
is c
oncern
that th
ey
will
only
pro
vide a
basis
pro
of of
concept by
the e
nd o
f th
e c
ontr
acte
d p
eriod a
nd that th
ere
will
be c
onsid
era
ble
cost to
the T
rust to
purc
hase the fully
required p
roduct
in li
ne w
ith e
xpecta
tions.
The topic
for
the G
rand R
ound o
n the 2
9th
Nove
mber
2019 is
based u
pon the S
tructu
red J
udgem
ent R
evi
ew
fin
din
gs for
End o
f Life
Death
s. T
his
them
atic
appro
ach w
ill c
ontin
ue to u
nderp
in L
earn
ing fro
m D
eath
s le
ssons le
arn
ed.
The m
onth
ly M
ort
alit
y R
eport
to the Q
ualit
y and S
afe
ty C
om
mitt
ee a
nd the T
rust B
oard
is c
hangin
g to a
Learn
ing fro
m D
eath
s R
eport
whic
h w
ill d
em
onstr
ate
the in
cre
ased o
f fo
cus o
f Lessons L
earn
ed.
Clin
ical A
udit
Lead is
pro
ducin
g a
month
ly n
ew
sle
tter
from
the M
ort
alit
y O
pera
tional G
roup (
MO
G)
calle
d 'L
essons to b
e L
earn
ed'
whic
h is
bein
g c
ircula
ted to F
oundatio
n, S
pecia
lty a
nd G
P d
octo
rs in
tra
inin
g a
s w
ell
as b
ein
g p
oste
d o
n T
rust N
ew
s a
nd o
n the
Meetin
g P
lace (
the T
rust's
clo
sed F
acebook
page).
Le
ss
on
s L
ea
rne
d
01/0
4/2
019
30/0
3/0
20
AM
D P
atie
nt
Safe
ty / D
irecto
r of
Medic
al E
ducatio
n
/ A
DO
Inte
gra
ted
Gove
rnance
40%
A
PM
O h
ave
met w
ith M
Pin
nin
gto
n w
ho is
lead for
the r
edesig
n o
f th
e n
urs
ing tra
inin
g p
lan. T
here
are
no funds to s
upport
the
coord
inatio
n o
r deliv
ery
of tr
ain
ing. A
ris
k paper
is to b
e w
ritten for
escala
tion thro
ugh the T
rust's
gove
rnance a
rrangem
ents
,
Dis
cussio
n r
equired w
ith W
ork
Str
eam
Gro
up to c
onfir
m w
heth
er
this
is to b
e b
rought in
to the s
cope o
f th
e P
roje
ct,
Re
d D
ay &
AIM
S T
rain
ing
01/1
1/2
019
30/1
2/2
020
M P
innin
gto
n5%
Page 60 of 210

21
Cu
rre
nt
PD
SA
Cy
cle
s
Le
ad
D
eta
il
Ite
rati
on
En
d
Date
Ne
xt
Ste
ps
Ele
ctr
on
ic W
ard
Bo
ard
Pilo
t (W
ard
11
B)
AM
D P
atie
nt
Safe
ty
Ele
ctr
onic
sta
nd
ard
isa
tio
n o
f B
oa
rd R
ound
to
ensure
do
cum
ente
d s
enio
r in
put a
nd
co
nsis
tent p
ractice
. 17/1
0/2
019
Tri
al t
o jo
in u
p w
ith R
ed
to
Gre
en d
id n
ot w
ork
. T
ria
l ha
s o
vera
ll g
one
we
ll. A
wa
itin
g
IT fix
es a
nd
a s
cre
en. T
o s
tart
on w
ard
14
A.
95
% T
ime
ly O
bs
erv
ati
on
s P
DS
A (
Wa
rd 9
A)
Clin
ical Q
ualit
y
Lead
95
% o
f p
atie
nts
on W
ard
9A
to
ha
ve the
ir o
bse
rva
tio
ns p
erf
orm
ed
as p
er
Tru
st P
olic
y b
y S
ep
tem
be
r 2
01
9
(the
n to
be
ro
lled
out a
cro
ss o
the
r w
ard
s)
17/1
0/2
019
Up
da
tes to
co
me
fro
m the
PD
SA
Te
am
fo
r W
ard
9A
. M
ea
sure
s ta
ke
n a
s b
elo
w
fro
m V
ItalP
ac r
ep
ort
s. T
ime
line
fo
r ro
ll o
ut to
be
dis
cusse
d a
t 'O
bse
rva
tio
ns a
nd
Esca
latio
n' M
ee
ting
in O
cto
be
r.
RIS
KS
(Po
tentia
l ris
k w
hic
h w
ill im
pa
ct th
e p
roje
ct; h
as n
ot ye
t o
ccurr
ed
whic
h w
ill
RA
GM
itig
ati
on
Acti
vit
yR
AG
Aft
er
Mit
igati
on
Co
mm
en
ts
Ele
ctr
on
ic W
ard
Bo
ard
s -
IT
De
ve
lop
me
nt
RA
t tim
e o
f re
po
rtin
g a
ll IT
sup
po
rt fo
r th
e E
lectr
onic
Wa
rd B
oa
rd P
SD
A h
as b
ee
n p
ut o
n h
old
due
to
sta
ffin
g
leve
ls. D
iscussio
ns a
nd
w
ork
aro
und
s a
re the
ne
xt s
tep
s.
RC
onfe
rence
ca
ll b
oo
ke
d to
dis
cuss n
ext
ste
ps fo
r p
roje
ct te
am
3rd
Octo
be
r.
Em
erg
en
cy
De
part
me
nt
Ph
arm
acis
t
(To id
entif
y m
orb
idity
and tim
ely
revi
ew
of A
KI P
atie
nts
)
RT
ria
ng
ula
tio
n o
f se
rio
us incid
ent re
vie
ws a
nd
lea
rnin
g fro
m d
ea
ths v
ia the
SJR
me
tho
do
log
y ha
s h
ighlig
hte
d the
ne
ed
fo
r a
n E
me
rge
ncy
De
pa
rtm
ent P
ha
rma
cis
t.T
his
po
sito
n m
ay
co
ntr
ibute
to
the
id
entifica
tio
n o
f p
atie
nt co
-
mo
rbid
ity
by
co
rre
latio
n o
f m
ed
ica
tio
n h
isto
ry w
ith d
iag
no
sis
, th
us c
ontr
ibuting
to
the
co
st o
f th
e p
ost. T
he
po
st
wo
uld
als
o im
pro
ve the
tim
elin
ess o
f p
ha
rma
cy
revi
ew
of p
atie
nts
with A
KI.
AA
busin
ess c
ase
whic
h inclu
de
s a
Pha
rma
cis
t fo
r A
&E
is b
ein
g s
ub
mitte
d thro
ug
h
the
Tru
st's
Go
vern
ance
ro
ute
fo
r co
nsid
era
tio
n c
om
me
ncin
g o
n 1
st O
cto
be
r.
Str
uctu
red
Ju
dg
em
en
t R
ev
iew
s
RT
he
re is a
n incre
asin
g b
acklo
g o
f S
JR
re
vie
ws in s
urg
ery
and
ort
ho
pa
ed
ics w
hic
h is a
ttri
buta
ble
in the
ma
in to
clin
ica
l ca
pa
city
(re
vie
ws ta
ke
1-2
ho
urs
) a
nd
the
im
pa
sse
ca
use
d b
y th
e la
ck o
f cla
rity
ove
r jo
b p
lannin
g.
Re
vie
we
rs d
o n
ot ha
ve this
wo
rk r
eco
gnis
ed
in the
curr
ent jo
b p
lannin
g s
tructu
re.
A m
ee
ting
of m
ort
alit
y le
ad
s is b
ein
g a
rra
ng
ed
to
ad
dre
ss the
issue
s.
AD
iscussio
ns w
ith s
taff to
em
be
d a
re o
ng
oin
g.
Mo
re info
rma
tio
n to
fo
llow
.
ISS
UE
S
(Issues h
ave
already
occurr
ed / a
re c
urr
ently
impactin
g u
pon the p
roje
ct)
RA
GA
cti
on
Take
nR
AG
Aft
er
Mit
igati
on
Co
mm
en
ts
Co
nsu
ltan
t E
ng
ag
em
en
t fo
r 'P
ne
um
on
ia a
s C
om
plicati
on
of
He
art
Failu
re'
Wo
rksh
op
.
RF
ace
to
fa
ce
dis
cussio
ns r
eq
uir
ed
with L
ea
d R
esp
ira
tory
and
Ca
rdia
c C
onsulta
nts
to
co
nfirm
re
pre
se
nta
tio
n fo
r
se
co
nd
atte
mp
t a
t 'P
ne
um
onia
as c
om
plic
atio
n o
f H
ea
rt F
ailu
re' W
ork
sho
p.
GT
his
is to
be
inco
rpo
rate
d into
the
Co
rre
ct C
are
Pa
thw
ays
me
eting
in O
cto
be
r.
Re
su
s r
eq
uir
e d
ed
icate
d t
rain
ing
ro
om
s t
o r
un
tra
inin
g f
rom
an
d s
tore
eq
uip
me
nt.
(D
ete
riora
ting P
atie
nt O
pera
tional G
roup 2
3/0
7/1
9)
AD
iscusse
d a
t th
e D
ete
rio
rating
Pa
tie
nt O
pe
ratio
na
l Gro
up
23
/07
/19
and
is b
ein
g ta
ke
n to
the
Mo
rta
lity
Op
era
tio
na
l Gro
up
13
/18
/19
G
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 61 of 210

22
A
pp
end
ix 3
: M
ort
alit
y M
on
thly
Dat
a R
epo
rt
Page 62 of 210

23
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 63 of 210

24
A
pp
en
dix
4:
Pefo
rman
ce D
istr
ibu
tio
n f
or
May &
Ju
ne 2
019
Page 64 of 210

25
Appendix
5 Mortality Indicators June 2019
SHMI - Summary Hospital Level Mortality Indicator
HSMR - Hospital Standardised Mortality Ratio (Rolling 12 month)
HSMR - Hospital Standardised Mortality Ratio (Monthly)
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 65 of 210

26
Local HSMR Bronchitis
Local HSMR Lower Respiratory Tract Infection
Local HSMR Pneumonia
Page 66 of 210

27
Local HSMR Septicemia
Local HSMR Stroke
Local HSMR Urinary Tract Infection
TB
203_
19c
LfD
Rep
ort D
ec 1
9
Page 67 of 210

28
Local HSMR Acute Renal Failure
Mortality Screens - % Deaths Screened
Crude Mortality Rate (Crude rate per 1000 discharges (excluding day cases))
Page 68 of 210

PUBLIC TRUST BOARD 4 December 2019
Agenda Item TB203/19d Report Title Monthly Safe Nurse & Midwifery
Staffing Report – October 2019
Executive Lead Juliette Cosgrove, Director of Nursing Midwifery Therapies and Governance
Lead Officer Claire Blackman-Deputy Director of nursing
Carol Fowler Assistant Director of Nursing – Workforce
Action Required
(Definitions below)
To Approve To Note
To Assure ✓ To Receive
For Information
Executive Summary
The Trust Board safe staffing highlight report for October 2019 is set out below:
The purpose of this report is to provide the Board with the current position of nursing staffing in line with National Quality Board, National Institute of Health & Care Excellence and NHS Improvement guidance. The report includes as a comparable metric, Care Hours per Patient Day (CHpPD) which supports the recording and reporting of nursing and care staff deployment. This report presents the safer staffing position for the month of October 2019. Alert
• For the month of October 2019 the Trust reports safe staffing against the national average (90%) at 92.3%.
Advise
• Care Hours per Patient Day (CHpPD) reporting remains under review to support accuracy of data reporting. Trust CHpPD reports at 8.3
• The Nursing Safe Staffing report is under reconstruction with a revised report anticipated in January 2020. The review includes workforce dashboard reporting and triangulation against clinical outcomes.
• The Trusts reporting to UNIFY has been reviewed to assure the Safe Staffing reporting includes the staff allocated on arrival of shift to clinical areas from the flexible workforce pool. Retrospective review has identified slight uplift to the trust safe staffing % reporting and an application to resubmit this data to UNIFY has therefore been requested by the trust.
Assure
• No harm events have occurred to our patients due to staffing levels
Recommendation
The Board is asked to receive the report
Strategic Objective(s) and Principal Risks(s)
Strategic Objective Principal Risk
✓ SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
TB
203_
19d
Saf
e N
urse
Sta
ffing
Rep
ort -
(O
ct d
ata)
Dec
19
Page 69 of 210

SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
✓ SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
If the system does not have an agreed acute services strategy it may lead to non-alignment of partner organisations plans resulting in the inability to develop and deliver sustainable services
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
✓ Caring ✓ Statutory Requirement
✓ Effective ✓ Annual Business Plan Priority
✓ Responsive ✓ Best Practice
✓ Safe ✓ Service Change
✓ Well Led
Impact (is there an impact arising from the report on any of the following?)
✓ Compliance Legal
✓ Engagement and Communication ✓ Quality & Safety
✓ Equality ✓ Risk
✓ Finance ✓ Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Committee)
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee ✓ Workforce Committee
GUIDE TO ACTIONS REQUIRED (TO BE REMOVED BEFORE ISSUE):
Approve: To formally agree the receipt of a report and its recommendations OR a particular course of action
Receive: To discuss in depth a report, noting its implications for the Board or Trust without needing to formally approve
Note: For the intelligence of the Board without the in-depth discussion as above
Assure: To apprise the Board that controls and assurances are in place
For Information: Literally, to inform the Board
Page 70 of 210

1. Introduction This report provides an overview of the staffing levels for October 2019. Overall fill rate for October 2019 was 92.3% (appendix 1).
• 91.01% Registered Nurses on days
• 86.04% Registered Nurses on nights
• 97.14% Care staff on days
• 98.72% Care staff on nights
The Board is advised the Trusts reporting to UNIFY has been reviewed to assure the Safe Staffing reporting includes the staff allocated on arrival of shift to clinical areas from the flexible workforce pool. Retrospective review has identified slight uplift to the trust safe staffing % reporting and an application to resubmit this data to UNIFY has therefore been requested by the trust. The Board will be kept appraised on this outcome and any change to the trusts Safe Staffing % reporting. The overall CHpPD for the Trust has remained static in month reporting at 8.3 hours (appendix 1) and remains slightly above the national average of 7 hours CHpPD, The Trust current reporting for CHpPD includes Registered Nurses/Registered Midwives. . Planned care clinical business unit (CBU) report overall 10.3, Urgent Care CBU 6.6 and Women’s and Children’s 13.0 overall. 2. October Safe Staffing Trust whole time equivalent (wte) funded establishment versus contracted for October 2019 below finance figures:
Funded WTE Contracted WTE Vacancy
Registered 950.41 791.46 158.95
Non-registered 447.71 367.03 80.68
Total 1,398.12 1,158.49 239.63
3. Staffing Related Reported Incidents October 2019
TB
203_
19d
Saf
e N
urse
Sta
ffing
Rep
ort -
(O
ct d
ata)
Dec
19
Page 71 of 210

27 staffing incidents/nursing red flags were reported in October, 12 less than the previous month. 13 of these incidents highlight insufficient nurses/midwives or nurse shortfalls, 16 less than September. 3 of these relate to Ward 14A (red flags) and a further 2 to Delivery Suite. No harm was caused to patients as a result of these incidents.
In October there were 4 nursing red flags reported in month, 3 on ward 14A, 1 on ward 7b. All incidents have been supported and managed through trust process and there has been no reported correlation with patient harm.
4. Non Framework Nurse Agency Usage
Page 72 of 210

The Trust continues to proactively review and consider options for additional staffing resource as an interim and longer term substantive position.
October reports a 3.7% increase in off framework agency usage compared to September.
5. Recommendations
The Board is asked to receive the content presented in this paper and support the on-going plans to
achieve and sustain compliance against Safe Staffing Plan.
Carol Fowler Assistant Director of Nursing – Workforce
TB
203_
19d
Saf
e N
urse
Sta
ffing
Rep
ort -
(O
ct d
ata)
Dec
19
Page 73 of 210

App
end
ix 1
: C
are
Hours
pe
r P
atient
Day (
CH
PP
D)
– O
cto
ber
20
19
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Wa
rd 7
A-S
DG
H3
00
- G
ENER
AL
MED
ICIN
E1
,47
6.7
51
,38
2.9
81
,51
2.5
01
,29
9.9
81
,10
6.5
01
,23
3.5
01
,13
9.5
01
,06
3.5
08
35
93
.65
%8
5.9
5%
11
1.4
8%
93
.33
%3
.12
.86
.0
A&
E O
bse
rva
tio
n W
ard
18
0 -
AC
CID
ENT
& E
MER
GEN
CY
73
9.5
07
26
.50
37
0.5
03
41
.00
73
2.0
07
41
.67
36
0.7
53
83
.25
26
39
8.2
4%
92
.04
%1
01
.32
%1
06
.24
%5
.62
.88
.3
E A
U3
00
- G
ENER
AL
MED
ICIN
E1
,74
8.9
81
,56
6.4
81
,31
8.7
51
,23
7.9
21
,08
6.5
31
,19
9.5
38
67
.50
96
7.2
55
95
89
.57
%9
3.8
7%
11
0.4
0%
11
1.5
0%
4.6
3.7
8.4
FESS
Wa
rd3
00
- G
ENER
AL
MED
ICIN
E1
,67
4.7
21
,30
2.2
21
,63
9.7
51
,48
7.2
01
,09
3.0
01
,12
6.0
07
89
.50
90
3.1
78
50
77
.76
%9
0.7
0%
10
3.0
2%
11
4.4
0%
2.9
2.8
5.7
Wa
rd 1
1B
-SD
GH
30
0 -
GEN
ERA
L M
EDIC
INE
1,5
56
.48
1,4
52
.48
1,6
89
.00
1,3
32
.00
1,0
96
.50
1,1
54
.50
1,2
18
.00
1,1
21
.50
79
69
3.3
2%
78
.86
%1
05
.29
%9
2.0
8%
3.3
3.1
6.4
Wa
rd 1
4B
-SD
GH
30
0 -
GEN
ERA
L M
EDIC
INE
1,7
85
.23
1,6
23
.23
1,6
36
.23
1,5
00
.07
1,4
61
.50
1,4
26
.00
1,1
62
.50
1,0
41
.00
89
49
0.9
3%
91
.68
%9
7.5
7%
89
.55
%3
.42
.86
.3
Sho
rt S
tay
Un
it3
00
- G
ENER
AL
MED
ICIN
E1
,50
9.9
21
,35
3.2
51
,52
6.0
01
,61
3.4
81
,09
8.0
01
,11
8.0
01
,11
4.5
01
,27
9.0
08
74
89
.62
%1
05
.73
%1
01
.82
%1
14
.76
%2
.83
.36
.1
Wa
rd 1
5a
Gen
era
l M
ed3
00
- G
ENER
AL
MED
ICIN
E1
,55
6.2
51
,36
1.2
51
,67
3.2
51
,51
1.1
71
,10
6.0
01
,08
3.5
01
,09
3.5
01
,24
7.1
77
33
87
.47
%9
0.3
1%
97
.97
%1
14
.05
%3
.33
.87
.1
Stro
ke W
ard
30
0 -
GEN
ERA
L M
EDIC
INE
1,2
72
.25
1,2
95
.58
1,5
23
.00
1,2
95
.98
1,0
98
.98
1,0
92
.00
73
3.0
07
99
.48
58
31
01
.83
%8
5.0
9%
99
.36
%1
09
.07
%4
.13
.67
.7
Reh
ab
& D
isch
arg
e Lo
un
ge3
14
- R
EHA
BIL
ITA
TIO
N1
,55
1.2
51
,26
4.0
01
,94
6.0
71
,69
0.8
21
,10
0.0
01
,09
8.0
01
,11
2.5
01
,13
4.5
08
26
81
.48
%8
6.8
8%
99
.82
%1
01
.98
%2
.93
.46
.3Y
x1 i
nci
den
ts r
ela
tin
g to
bel
ow
25
% o
r m
ore
th
an
8h
rs a
gain
st R
N -
Mit
iga
ted
at
tim
e in
vest
iga
tio
n o
ngo
ing
Wa
rd 1
4A
11
0 -
TR
AU
MA
&
OR
THO
PA
EDIC
S1
,84
1.2
51
,61
5.1
72
,46
7.7
51
,74
8.2
31
,10
9.2
51
,20
4.2
51
,58
7.5
01
,40
7.0
09
11
87
.72
%7
0.8
4%
10
8.5
6%
88
.63
%3
.13
.56
.6Y
x3 i
nci
den
t R
ela
ted
to
hig
h p
ati
ent
acu
ity
,sh
ort
ter
m s
ickn
ess-
ma
na
ged
wit
hin
tru
st p
roce
ss-
no
pa
tien
t h
arm
. In
cid
ent
clo
sed
.
Sho
rt S
tay
Surg
ica
l U
nit
10
0 -
GEN
ERA
L SU
RG
ERY
1,2
38
.25
1,2
46
.25
1,3
85
.25
1,2
23
.25
72
3.0
07
24
.00
36
7.5
03
78
.00
45
11
00
.65
%8
8.3
1%
10
0.1
4%
10
2.8
6%
4.4
3.6
7.9
Wa
rd H
11
0 -
TR
AU
MA
&
OR
THO
PA
EDIC
S7
43
.50
65
7.0
07
42
.00
39
1.5
07
30
.50
61
0.5
00
.00
15
3.5
01
23
88
.37
%5
2.7
6%
83
.57
%#D
IV/0
!1
0.3
4.4
14
.7
Surg
ica
l W
ard
10
0 -
GEN
ERA
L SU
RG
ERY
1,0
73
.25
1,0
15
.42
1,1
09
.00
99
2.5
07
37
.00
74
9.5
03
67
.00
36
7.0
04
74
94
.61
%8
9.5
0%
10
1.7
0%
10
0.0
0%
3.7
2.9
6.6
Spin
al
Inju
ries
Un
it4
00
- N
EUR
OLO
GY
2,9
83
.92
2,8
49
.25
3,1
25
.42
2,9
69
.92
2,5
97
.75
2,4
49
.75
1,4
43
.00
1,4
31
.00
72
09
5.4
9%
95
.02
%9
4.3
0%
99
.17
%7
.46
.11
3.5
Wa
rd G
10
1 -
UR
OLO
GY
1,0
95
.50
92
7.0
01
,06
9.0
07
73
.75
82
5.0
07
78
.00
37
9.5
03
55
.00
32
88
4.6
2%
72
.38
%9
4.3
0%
93
.54
%5
.23
.48
.6
TOTA
L2
3,8
47
.00
21
,63
8.0
62
4,7
33
.47
21
,40
8.7
61
7,7
01
.52
17
,78
8.7
01
3,7
35
.75
14
,03
1.3
21
02
56
90
.74
%8
6.5
6%
10
0.4
9%
10
2.1
5%
3.8
3.5
7.3
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
A&
E N
urs
ing
4,1
95
.25
4,2
87
.00
2,6
07
.25
1,6
07
.75
3,6
52
.00
3,5
83
.50
1,1
08
.00
74
8.0
00
10
2.1
9%
61
.66
%9
8.1
2%
67
.51
%
Am
bu
lato
ry C
are
Un
it7
27
.00
33
0.0
07
40
.00
40
0.9
80
.00
17
6.0
00
.00
92
.00
10
44
5.3
9%
54
.19
%#D
IV/0
!#D
IV/0
!
TOTA
L4
,92
2.2
54
,61
7.0
03
,34
7.2
52
,00
8.7
33
,65
2.0
03
,75
9.5
01
,10
8.0
08
40
.00
52
93
.80
%6
0.0
1%
10
2.9
4%
75
.81
%N
/AN
/AN
/A
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
ITU
/CC
U1
92
- C
RIT
ICA
L C
AR
E M
EDIC
INE
3,9
79
.75
3,3
31
.75
1,2
15
.00
1,0
01
.50
3,6
92
.00
3,1
88
.50
1,1
16
.00
53
8.7
53
86
83
.72
%8
2.4
3%
86
.36
%4
8.2
8%
16
.94
.02
0.9
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Del
iver
y Su
ite
50
1 -
OB
STET
RIC
S#D
IV/0
!#D
IV/0
!#D
IV/0
!
Ma
tern
ity
Wa
rd5
01
- O
BST
ETR
ICS
3,5
36
.25
3,3
38
.17
1,2
91
.00
1,1
23
.00
63
9.2
55
67
.75
1,0
98
.00
1,0
62
.50
42
59
4.4
0%
86
.99
%8
8.8
2%
96
.77
%9
.25
.11
4.3
MA
U5
01
- O
BST
ETR
ICS
#DIV
/0!
#DIV
/0!
#DIV
/0!
TOTA
L 3
,53
6.2
53
,33
8.1
71
,29
1.0
01
,12
3.0
06
39
.25
56
7.7
51
,09
8.0
01
,06
2.5
04
25
94
.40
%8
6.9
9%
88
.82
%9
6.7
7%
9.2
5.1
14
.3
War
d n
ame
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Tota
l
mo
nth
ly
pla
nn
ed
staf
f h
ou
rs
Tota
l
mo
nth
ly
actu
al s
taff
ho
urs
Neo
na
tal
Wa
rd -
OD
GH
42
0 -
PA
EDIA
TRIC
S1
,15
2.7
51
,18
4.5
03
07
.50
22
2.7
51
,15
3.6
81
,13
3.7
50
.00
0.0
02
29
10
2.7
5%
72
.44
%9
8.2
7%
#DIV
/0!
10
.11
.01
1.1
Pa
edia
tric
Un
it4
20
- P
AED
IATR
ICS
1,9
28
.50
1,8
54
.50
1,3
89
.00
1,1
39
.25
1,8
70
.00
1,6
60
.00
37
1.5
04
79
.50
40
39
6.1
6%
82
.02
%8
8.7
7%
12
9.0
7%
8.7
4.0
12
.7
TOTA
L 3
,08
1.2
53
,03
9.0
01
,69
6.5
01
,36
2.0
03
,02
3.6
82
,79
3.7
53
71
.50
47
9.5
06
32
.00
98
.63
%8
0.2
8%
92
.40
%1
29
.07
%9
.23
2.9
11
2.1
4
PLA
NN
ED1
2,9
55
.42
11
,64
1.8
41
1,1
13
.42
9,1
00
.65
10
,41
4.5
09
,70
4.5
05
,26
0.5
04
,63
0.2
53
,39
38
9.8
6%
81
.89
%9
3.1
8%
88
.02
%6
.34
.01
0.3
UR
GEN
T1
4,8
71
.33
13
,32
7.9
71
4,8
35
.05
13
,30
9.6
11
0,9
79
.02
11
,27
2.7
09
,59
1.2
59
,93
9.8
27
24
98
9.6
2%
89
.72
%1
02
.67
%1
03
.63
%3
.43
.26
.6
W&
C6
,61
7.5
06
,37
7.1
72
,98
7.5
02
,48
5.0
03
,66
2.9
33
,36
1.5
01
,46
9.5
01
,54
2.0
01
,05
79
6.3
7%
83
.18
%9
1.7
7%
10
4.9
3%
9.2
3.8
13
.0
TRU
ST T
OTA
LS3
4,4
44
.25
31
,34
6.9
82
8,9
35
.97
24
,89
5.2
62
5,0
56
.45
24
,33
8.7
01
6,3
21
.25
16
,11
2.0
71
1,6
99
91
.01
%8
6.0
4%
97
.14
%9
8.7
2%
4.8
3.5
8.3
Gre
en-
80
% a
nd
ab
ove
Red
- U
nd
er 8
0%
Spe
cial
tyR
ed
Flag
C
om
me
nts
Re
gist
ere
d n
urs
es
Car
e S
taff
Re
gist
ere
d n
urs
es
Car
e S
taff
Pat
ien
ts a
t
23
:59
eac
h
day
Re
gist
ere
d
nu
rse
sC
are
Sta
ffO
vera
ll
Ave
rage
fill
rate
-
regi
ste
red
nu
rse
s/
mid
wiv
es
(%
)
Ave
rage
fill
rate
- c
are
staf
f (%
)
Ave
rage
fill
rate
-
regi
ste
red
nu
rse
s/
mid
wiv
es
(%)
Ave
rage
fill
rate
- c
are
staf
f (%
)
Re
d
Flag
C
om
me
nts
Car
e S
taff
Ove
rall
Ave
rage
fill
rate
-
regi
ste
red
nu
rse
s/
mid
wiv
es
(%
)
Ave
rage
fill
rate
- c
are
staf
f (%
)
Re
gist
ere
d n
urs
es
Car
e S
taff
Spe
cial
ty
Re
gist
ere
d
nu
rse
s
Car
e S
taff
Re
gist
ere
d n
urs
es
Car
e S
taff
Re
gist
ere
d n
urs
es
Pat
ien
ts a
t
23
:59
eac
h
day
Ave
rage
fill
rate
-
regi
ste
red
nu
rse
s/
mid
wiv
es
(%)
Ave
rage
fill
rate
- c
are
staf
f (%
)
Spe
cial
ty
Ave
rage
fill
rate
- c
are
staf
f (%
)
Re
d
Flag
C
om
me
nts
Pat
ien
ts a
t
23
:59
eac
h
day
Re
gist
ere
d
nu
rse
sC
are
Sta
ffR
ed
Flag
C
om
me
nts
Ave
rage
fill
rate
-
regi
ste
red
nu
rse
s/
mid
wiv
es
Ave
rage
fill
rate
- c
are
staf
f (%
)
Re
gist
ere
d
nu
rse
sC
are
Sta
ffO
vera
ll
Ove
rall
Ave
rage
fill
rate
-
regi
ste
red
nu
rse
s/
mid
wiv
es
(%
)
Ave
rage
fill
rate
- c
are
staf
f (%
)
Ave
rage
fill
rate
-
regi
ste
red
nu
rse
s/
mid
wiv
es
(%)
Ove
rall
Ave
rage
fill
rate
- c
are
staf
f (%
)
Ave
rage
fill
rate
-
regi
ste
red
nu
rse
s/
mid
wiv
es
(%
)
Re
d
Flag
C
om
me
nts
Pat
ien
ts a
t
23
:59
eac
h
day
Ave
rage
fill
rate
- c
are
staf
f (%
)
Ave
rage
fill
rate
-
regi
ste
red
nu
rse
s/
mid
wiv
es
(%)
Re
gist
ere
d
nu
rse
sC
are
Sta
ffW
ard
nam
e
Car
e S
taff
Re
gist
ere
d n
urs
es
Re
gist
ere
d n
urs
es
Car
e S
taff
Spe
cial
ty
War
d n
ame
War
d n
ame
Spe
cial
ty
Re
gist
ere
d n
urs
es
Car
e S
taff
War
d n
ame
Re
gist
ere
d n
urs
es
Car
e S
taff
Re
gist
ere
d n
urs
es
Car
e S
taff
Pat
ien
ts a
t
23
:59
eac
h
day
Ave
rage
fill
rate
-
regi
ste
red
nu
rse
s/
mid
wiv
es
(%
)
Ave
rage
fill
rate
- c
are
staf
f (%
)
Page 74 of 210

PUBLIC TRUST BOARD 4 December 2019
Agenda Item TB204/19 Report Title Integrated Performance
Report
Executive Lead Steve Christian, Chief Operating Officer
Lead Officer Anita Davenport, Interim Performance Manager
Action Required
(Definitions below)
To Approve To Note
✓ To Assure ✓ To Receive
For Information
Executive Summary
The report highlights the indicators that require discussion at the board. Some of these indicators require corrective action to be taken. Executive assurance and action plans have been provided in order to provide assurance that corrective measures are in place. The reporting forms part of the Trust’s Performance and Accountability Framework, where governance is in place to drive and monitor both operational performance improvement and delivery of the Vision 2020 Single Improvement Plan. Update on development: The development of the IPR has been an ongoing process over the last year. To date, several improvements have been made to both the structure and content of the report to enable ease of use and clarity of understanding. The improvements include:
• SPC charts for each indicator in line with NHSI recommendations
• The inclusion of targets where these were previously not included
• The addition of trajectories of performance where this is practicable and appropriate (blue line on graph)
• The division of the ‘red/green’ box on the detailed report to enable a clear picture of where the Trust is performing against both target and trajectory – a white box indicates ‘no trajectory’
• Executive sign off, for their respective KPIs
• Ongoing data cleansing and data quality audits – data quality group set up
• HR Trajectories have been agreed and will be included going forward
• Continued support to colleagues in developing good quality and useful narrative - Peer review of IPR introduced
• Results of MIAA audit of IPR recommended stability in design to enable documentation of the data collection process, and a focus on data quality
The Board is asked to receive the report and highlight any further assurance necessary in relation to areas of poor performance.
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
Strategic Objective Principal Risk
TB
204_
19 1
FS
IPR
Dec
19
Page 75 of 210

✓ SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
✓ SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
✓ SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
✓ SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
✓ SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
✓ SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
If the system does not have an agreed acute services strategy it may lead to non-alignment of partner organisations plans resulting in the inability to develop and deliver sustainable services
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
✓ Caring ✓ Statutory Requirement
✓ Effective ✓ Annual Business Plan Priority
✓ Responsive ✓ Best Practice
✓ Safe ✓ Service Change
✓ Well Led
Impact (is there an impact arising from the report on any of the following?)
✓ Compliance ✓ Legal
✓ Engagement and Communication ✓ Quality & Safety
✓ Equality ✓ Risk
Finance ✓ Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Board/Committee/Group)
Continue to monitor complaints and compliments. Weekly complaints review meeting to review all complaints over 40 day response target.
Previously Presented at:
Audit Committee ✓ Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
✓ Finance, Performance & Investment ✓ Workforce Committee
Page 76 of 210

Committee
TB
204_
19 1
FS
IPR
Dec
19
Page 77 of 210


Inte
grat
ed
Per
form
ance
Re
po
rt E
xecu
tive
Su
mm
ary
Sep
tem
be
r 2
01
9, S
teve
Ch
rist
ian
(C
hie
f O
per
atin
g O
ffic
er)
Go
vern
ance
Fra
me
wo
rk
The
Inte
grat
ed
Per
form
ance
rep
ort
is r
evie
wed
mo
nth
ly b
y th
e Tr
ust
Bo
ard
an
d s
pec
ific
ind
icat
ors
are
rev
iew
ed
by
the
sub
co
mm
itte
es o
f th
e B
oar
d w
hic
h
rep
ort
ass
ura
nce
, ale
rts
and
ad
vice
to
th
e B
oar
d.
The
per
form
ance
rep
ort
incl
ud
es t
he
Tru
st in
dic
ato
rs r
elat
ing
to t
he
NH
S, C
on
stit
uti
on
al S
tan
dar
ds,
th
e 2
01
9/2
0 S
OF
and
inte
rnal
per
form
ance
ind
icat
ors
wh
ich
th
e Tr
ust
has
iden
tifi
ed a
s es
sen
tial
mea
sure
s o
f o
per
atio
nal
del
iver
y an
d a
ssu
ran
ce.
The
per
form
ance
ind
icat
ors
are
gro
up
ed a
cco
rdin
g to
th
e
do
mai
ns
use
d b
y re
gula
tors
in t
he
We
ll Le
d F
ram
ewo
rk.
Each
ind
icat
or
has
a S
tati
stic
al P
roce
ss C
on
tro
l Ch
art
(SP
C)
and
co
mm
enta
ry. W
hils
t th
is e
xecu
tive
su
mm
ary
pro
vid
es a
n o
vera
ll vi
ew o
f th
e o
rgan
isat
ion
al
imp
rove
men
ts a
nd
ris
ks, s
om
e in
dic
ato
rs a
re a
lso
incl
ud
ed a
s im
pro
vem
ent
mea
sure
s fo
r th
e fo
ur
QI p
rio
riti
es a
nd
are
co
vere
d in
det
ail i
n t
he
rele
van
t
rep
ort
s.
The
Exec
uti
ve S
um
mar
y h
igh
ligh
ts k
ey
chan
ges
in T
rust
per
form
ance
(im
pro
vem
ent
or
any
area
s o
f co
nce
rn)
and
ou
tlin
es s
pec
ific
act
ion
s lin
ked
to
th
e
Tru
st’s
Imp
rove
men
t P
lan
an
d k
ey p
rogr
amm
es o
f w
ork
Exec
uti
ve S
um
mar
y
Do
mai
n
Hig
h L
eve
l Su
mm
ary
(pri
ori
ty K
PIs
by
exe
mp
tio
n)
Cri
tica
l Act
ion
s (a
gain
st p
rio
rity
KP
Is)
Re
spo
nsi
ve
& E
ffic
ien
cy
Urg
en
t an
d E
me
rgen
cy C
are
(U
EC)
Dem
and
fo
r U
EC a
nd
th
e ab
ility
to
op
tim
ise
pat
ien
t fl
ow
re
mai
ns
a ch
alle
nge
fo
r th
e Tr
ust
an
d t
he
wid
er s
yste
m.
Th
e co
nti
nu
ed c
hal
len
ges
in U
EC w
ill h
ave
a n
egat
ive
imp
act
on
a n
um
ber
of
KP
Is w
ith
in t
he
IPR
giv
en t
he
sign
ific
ant
relia
nce
on
go
od
pat
ien
t fl
ow
. 4
ho
ur
per
form
ance
has
dec
reas
ed in
Oct
ob
er t
o 8
4.6
% f
rom
8
8.6
% in
Sep
tem
ber
, So
uth
po
rt a
chie
vin
g 6
9.9
4%
wh
ich
is a
si
gnif
ican
t d
rop
fro
m 7
7.5
8%
in S
epte
mb
er.
In a
dd
itio
n t
he
Sou
thp
ort
sit
e re
po
rted
27
x 1
2 h
ou
r D
TA B
reac
hes
. ED
at
ten
dan
ces
at S
ou
thp
ort
we
re 5
.6%
hig
her
th
an O
cto
ber
la
st y
ear
and
4.0
% h
igh
er t
han
th
e p
revi
ou
s m
on
th r
each
ing
UEC
W
inte
r P
lan
nin
g (s
yste
m w
ide)
: Sys
tem
win
ter
pla
ns
hav
e b
een
pu
lled
to
geth
er t
o a
dd
ress
th
e o
ut
of
ho
spit
al c
apac
ity
gap
iden
tifi
ed b
y V
enn
. Th
ere
are
risk
s ar
ou
nd
th
e ab
ility
fo
r th
ese
sch
emes
to
del
iver
aga
inst
th
e as
sum
pti
on
s d
ue
to w
ork
forc
e av
aila
bili
ty in
par
ticu
lar
wit
hin
th
e co
mm
un
ity
sett
ing
and
sp
ecif
ical
ly a
cro
ss t
he
Sou
thp
ort
& F
orm
by
loca
lity.
W
inte
r P
lan
nin
g (i
nte
rnal
): T
he
Tru
st h
as in
tro
du
ced
a w
eekl
y W
inte
r O
per
atio
nal
Gro
up
to
su
pp
ort
imp
lem
enta
tio
n o
f th
e h
osp
ital
win
ter
sch
emes
. Th
e sc
hem
es in
clu
de
the
op
enin
g o
f a
16
bed
ded
po
st -
op
erat
ive
Ort
ho
pae
dic
w
ard
to
su
pp
ort
ap
pro
pri
ate
tran
sfer
of
pat
ien
ts s
till
un
der
acu
te c
are
that
can
re
ceiv
e th
eir
reh
abili
tati
on
at
Orm
skir
k. T
his
in e
ffec
t w
ill r
elea
se 1
6 b
eds
at
Sou
thp
ort
as
this
cu
rren
t co
ho
rt o
f p
atie
nts
rem
ain
on
th
e So
uth
po
rt s
ite
un
til
TB
204_
19 2
IPR
Sum
mar
y D
ec 1
9
Page 78 of 210

a fi
gure
of
50
03. T
his
is t
he
fou
rth
tim
e th
is y
ear
wh
en
Sou
thp
ort
att
end
ance
s h
ave
bre
ach
ed t
he
50
00 m
ark.
7th
O
cto
ber
201
9 is
cu
rren
tly
the
bu
sies
t d
ay o
n r
eco
rd f
or
the
dep
artm
ent
wh
en 2
24
pat
ien
ts a
rriv
ed in
on
e d
ay.
In
add
itio
n, t
he
Med
ical
ly O
pti
mis
ed f
or
Dis
char
ge (
MO
fD)
rate
co
nti
nu
es t
o in
crea
se f
rom
51
pat
ien
ts in
Ap
ril t
o 7
3
pat
ien
ts in
Oct
ob
er, a
n in
crea
se o
f 4
3%
.
Can
cer
The
62 d
ay s
tan
dar
d w
as 8
2%
aga
inst
th
e 8
5%
co
nst
itu
tio
nal
req
uir
emen
t. W
hils
t th
is is
mar
ked
im
pro
vem
ent
agai
nst
th
e p
revi
ou
s m
on
th t
he
sust
ain
abili
ty
of
per
form
ance
ab
ove
80%
is a
ch
alle
nge
. E
nd
osc
op
y co
nti
nu
es t
o a
pp
oin
t at
th
e 1
4 d
ay p
oin
t. H
aem
ato
logy
an
d
Hea
d &
Nec
k se
rvic
es
un
der
inte
nse
pre
ssu
res
du
e to
w
ork
forc
e co
nst
rain
ts (
bo
th s
erv
ices
hav
e h
isto
rica
l SLA
s in
p
lace
wit
h o
ther
pro
vid
ers
that
are
no
t p
erfo
rmin
g)
18
Wee
k R
TT P
erfo
rman
ce
Sep
tem
ber
18
-we
ek R
TT p
erfo
rman
ce w
as 9
3.4
%.
Pre
dic
tio
ns
for
No
vem
ber
sh
ow
per
form
ance
will
rem
ain
ar
ou
nd
93
% a
nd
co
nti
nu
e to
be
abo
ve t
he
92%
th
resh
old
. Th
ere
are
curr
entl
y 7
pat
ien
ts w
aiti
ng
ove
r 4
0 w
eeks
, a
slig
ht
incr
ease
, h
ow
ever
th
e n
um
ber
of
30
+ w
eek
wai
ters
h
as d
rop
ped
fro
m 9
9 t
o 8
8 o
ver
the
pas
t 4
we
eks,
th
ese
lon
g w
aite
rs a
re la
rgel
y d
ue
to t
he
con
tin
uin
g ch
alle
nge
s in
C
om
mu
nit
y P
aed
iatr
ics
and
Gyn
aeco
logy
.
fit
for
dis
char
ge.
The
Tru
st B
oar
d h
as s
ign
ed o
ff t
he
bu
sin
ess
case
wit
h
recr
uit
men
t an
d e
stat
es
wo
rk c
om
men
ced
wit
h a
tar
get
dat
e o
f o
pen
ing
in t
he
firs
t w
eek
of
Jan
uar
y.
Pat
ien
t Fl
ow
Imp
rove
men
t p
rogr
amm
e: A
nu
mb
er o
f sc
hem
es a
re b
ein
g in
tro
du
ced
to
su
pp
ort
wee
ken
d p
erfo
rman
ce.
Th
ese
incl
ud
e en
han
cin
g p
har
mac
y p
rese
nce
, op
enin
g u
p a
mb
ula
tory
car
e an
d in
crea
sin
g se
nio
r d
ecis
ion
mak
ers
acro
ss t
he
inp
atie
nt
war
ds.
Pat
ien
t Fl
ow
Imp
rove
men
t P
rogr
amm
e (P
FIP
) co
nti
nu
es t
o w
ork
on
its
acti
on
s to
imp
rove
eff
icie
ncy
an
d
lead
ersh
ip o
f p
atie
nt
man
agem
ent
on
th
e w
ard
wit
h a
n a
spir
atio
n o
f es
tab
lish
ed r
edu
ce a
ll Em
erge
ncy
ALO
S b
y 0
.5 d
ays.
Th
e b
asel
ine
at t
he
star
t o
f th
is w
ork
str
eam
was
set
at
aver
age
LOS
7.4
day
s. T
he
resu
lts
for
Oct
ob
er
sho
w a
n im
pro
vem
ent
of
alm
ost
1 d
ay n
ow
at
6.5
day
s.
Can
cer
Fort
nig
htl
y C
ance
r Im
pro
vem
ent
mee
tin
gs w
ith
Ch
ief
Op
erat
ing
Off
icer
allo
w
hig
h le
vel i
mp
acts
an
d b
arri
ers
to b
e d
iscu
ssed
wit
h C
ance
r Se
rvic
es.
The
mee
tin
g p
rovi
des
ass
ura
nce
an
d e
scal
atio
n o
f is
sues
, wit
h r
epo
rtin
g o
f so
luti
on
s th
e m
ain
fo
cus.
In a
dd
itio
n, i
nd
ivid
ual
tu
mo
ur
site
s ar
e in
vite
d t
o
atte
nd
th
is m
eeti
ng
to d
iscu
ss in
dep
th t
he
risk
s, b
arri
ers
and
go
od
pra
ctic
e w
ith
in t
hei
r o
wn
are
as, w
hic
h s
up
po
rt t
hei
r im
pro
vem
ent
pla
n.
Ro
bu
st c
ance
r im
pro
vem
ent
pla
ns
for
eac
h in
div
idu
al t
um
ou
r si
te a
nd
ser
vice
s th
at a
ffec
t th
e ca
nce
r p
ath
way
s, w
ith
cle
arly
def
ined
KP
Is a
re n
ow
in p
lace
.
Form
al d
iscu
ssio
ns
are
un
der
way
wit
h o
ther
pro
vid
ers
rega
rdin
g H
aem
ato
logy
an
d H
ead
& N
eck
serv
ices
. 1
8 W
eek
RTT
Per
form
ance
Th
e G
ynae
colo
gy p
osi
tio
n is
pre
dic
ted
to
re
cove
r fr
om
Jan
uar
y 2
02
0 a
s th
e Tr
ust
has
rec
en
tly
app
oin
ted
4 c
on
sult
ants
. Th
e C
om
mu
nit
y P
aed
iatr
ics
per
form
ance
will
co
nti
nu
e to
be
com
pro
mis
ed u
nti
l we
can
ap
po
int
into
th
e va
can
t co
mm
un
ity
Pae
dia
tric
ian
po
st.
Page 79 of 210

Dia
gno
stic
s P
erfo
rman
ce f
or
Oct
ob
er a
gain
st t
he
6 w
eek
wai
t ta
rget
w
as 2
.16
% a
n im
pro
vem
ent
of
0.5
% o
ver
the
Sep
tem
ber
p
osi
tio
n a
nd
in li
ne
wit
h t
raje
cto
ry.
End
osc
op
y re
cord
ed
the
mo
st n
um
ber
of
sco
pes
in a
mo
nth
(o
n r
eco
rd)
in
Oct
ob
er a
t 6
53
wit
h z
ero
ses
sio
ns
can
celle
d d
ue
to n
o
nu
rses
. Th
eat
re U
tiliz
atio
n
Orm
skir
k im
pro
ved
in m
on
th t
o 7
3%
fo
r O
cto
ber
by
1%
ag
ain
st t
he
pre
vio
us
mo
nth
. H
ow
ever
So
uth
po
rt u
tiliz
atio
n
reco
rded
a d
eclin
e in
per
form
ance
du
e to
hig
h n
um
ber
s o
f ca
nce
llati
on
s at
trib
ute
d t
o p
oo
r p
atie
nt
flo
w.
Dia
gno
stic
s (U
ltra
sou
nd
) Th
e U
ltra
sou
nd
bac
klo
g re
du
ctio
n w
ill b
e d
eliv
ered
th
rou
gh a
n a
gree
d S
LA
wit
h R
en
acre
s, a
nd
will
co
nti
nu
e to
be
sup
po
rted
by
PD
S M
SK S
on
ogr
aph
ers
and
ext
ra in
-ho
use
co
nsu
ltan
t ac
tivi
ty.
Th
eat
re U
tiliz
atio
n
The
imp
rove
men
t p
rogr
amm
e co
nti
nu
es t
o s
ho
w p
rogr
ess
(5%
imp
rove
men
t in
uti
lizat
ion
sin
ce A
pri
l) t
hro
ugh
a f
ocu
s o
n t
hre
e w
ork
are
as: S
ched
ulin
g,
Avo
idin
g o
n-t
he-
day
can
cella
tio
ns
and
sta
rtin
g se
ssio
ns
on
tim
e (
the
Go
lden
P
atie
nt)
.
Wel
l Le
d
The
key
risk
s re
late
to
wo
rkfo
rce
cap
acit
y an
d c
apab
ility
. A
nu
mb
er o
f m
etri
cs in
clu
din
g va
can
cy r
ate
and
tu
rno
ver
as
we
ll as
sic
knes
s ab
sen
ce a
nd
ap
pra
isal
are
co
nsi
sten
tly
bel
ow
th
e re
qu
ired
leve
l. Th
is is
imp
acti
ng
sign
ific
antl
y o
n
the
fin
anci
al p
erfo
rman
ce a
s th
e Tr
ust
has
bee
n r
elia
nt
on
te
mp
ora
ry a
nd
hig
h c
ost
so
luti
on
s in
ord
er t
o m
ain
tain
saf
e
staf
fin
g an
d t
he
CH
PP
D le
vels
.
On
e su
ch im
pro
vin
g m
etri
c is
th
e Tr
ust
’s r
olli
ng
year
to
dat
e si
ckn
ess
abse
nce
rat
e w
hic
h h
as c
on
sist
en
tly
red
uce
d
mo
nth
on
mo
nth
fo
r 1
1 m
on
ths
and
rem
ain
s o
n t
rack
to
at
tain
bel
ow
5%
by
Mar
ch 2
02
0.
Ho
wev
er, t
he
Tru
st h
as
no
t fe
lt t
he
ben
efit
of
the
red
uci
ng
sick
nes
s ab
sen
ce r
ate
, d
ue
to a
n in
crea
sin
g va
can
cy r
ate,
wh
ich
is a
ttri
bu
ted
to
an
in
crea
sin
g st
aff
turn
ove
r ra
te.
Pri
ori
ty h
as b
een
giv
en t
o e
stab
lish
ing
a n
um
ber
of
task
an
d f
inis
h g
rou
ps
to
enga
ge w
ith
key
sta
keh
old
ers
to c
entr
e o
n: R
ecru
itm
ent
and
Re
ten
tio
n a
nd
al
so P
erfo
rman
ce D
evel
op
men
t an
d R
evie
w (
PD
R).
Th
eref
ore
, wit
hin
th
e n
ext
fou
r w
eeks
, tw
o t
ask
and
fin
ish
gro
up
s w
ill b
e es
tab
lish
ed, o
ne
gro
up
will
fo
cus
on
rec
ruit
men
t an
d r
eten
tio
n a
nd
th
e o
ther
on
per
form
ance
d
evel
op
men
t re
view
. In
ad
dit
ion
th
e Tr
ust
is c
on
tin
uin
g w
ork
wit
h a
n e
xte
rnal
co
mp
any,
Lia
iso
n, o
n d
evel
op
ing
thei
r W
ork
forc
e D
ash
bo
ard
s in
ord
er t
o
uti
lise
arti
fici
al a
nd
bu
sin
ess
inte
llige
nce
, in
ord
er t
hat
ho
tsp
ot
area
s ca
n b
e q
uic
kly
and
eas
ily id
enti
fied
an
d t
imel
y in
terv
enti
on
s p
ut
into
pla
ce.
W
ork
co
nti
nu
es o
n t
he
inte
rven
tio
ns
to r
edu
ce a
gen
cy s
pen
d b
elo
w w
hic
h
incl
ud
es a
n a
gree
d f
orm
al p
artn
ersh
ip a
rran
gem
ent
wit
h t
hir
d p
arty
o
rgan
isat
ion
s th
at c
an a
ssis
t w
ith
in-s
ou
rin
g to
mit
igat
e th
e ri
sk r
egar
din
g ta
x b
ills
on
pen
sio
n; T
he
dev
elo
pm
ent
of
a “m
edic
al”
ban
k -
to g
o li
ve 1
st
Dec
emb
er; T
he
on
goin
g u
se o
f th
e n
urs
ing
“tie
r 2
” fr
amew
ork
to
era
dic
ate
agen
cy u
sage
; A
sys
tem
wid
e re
view
of
Frag
ile s
ervi
ces
is in
pla
ce w
ith
th
e co
nsi
der
atio
n o
f w
ho
le s
yste
m s
olu
tio
ns.
TB
204_
19 2
IPR
Sum
mar
y D
ec 1
9
Page 80 of 210

Safe
P
osi
tive
pro
gres
s h
as b
een
ach
ieve
d a
gain
st t
he
falls
in
dic
ato
r (k
ey e
lem
ent
of
the
Car
e o
f O
lder
Peo
ple
Im
pro
vem
ent
Pri
ori
ty)
and
FN
OF
ind
icat
or
for
tim
e to
th
eatr
e. T
hes
e K
PIs
hav
e b
een
pre
vio
usl
y ra
ised
as
a co
nce
rn a
t SO
IB.
Del
iver
y o
f th
e fa
lls a
spec
t o
f th
e O
lder
Peo
ple
s Q
I pro
gram
me
has
ach
ieve
m
ajo
r m
ilest
on
es f
or
intr
od
uci
ng
new
ris
k as
sess
men
t, d
ocu
men
tati
on
, tr
ain
ing
and
un
der
taki
ng
RC
A r
evi
ews.
Th
e Fa
lls S
trat
egy
is o
n t
rack
fo
r th
e la
un
ch b
y th
e en
d o
f N
ove
mb
er 2
01
9.
Th
e O
rth
op
aed
ics
team
co
nti
nu
e to
imp
lem
ent
the
FNO
F p
ath
way
an
d
‘Go
lden
Pat
ien
t’ a
pp
roac
h t
o e
xped
ite
acce
ss t
o t
hea
tre
and
is a
imin
g to
ac
hie
ve t
he
targ
et b
y D
ecem
ber
20
19
. In
ad
dit
ion
we
hav
e im
pro
ved
ort
ho
-ge
riat
ric
sup
po
rt (
3 d
ays
per
wee
k).
The
Tru
sts
con
tin
ues
to
dem
on
stra
te
imp
rovi
ng
FNO
F m
ort
alit
y ra
tes.
Effe
ctiv
e
Co
nti
nu
ed im
pro
vem
ent
in p
erfo
rman
ce a
gain
st S
tro
ke a
nd
Se
psi
s in
dic
ato
rs h
as b
een
ach
ieve
d s
up
po
rted
by
the
Det
erio
rati
ng
Pat
ien
t Q
I Pri
ori
ty a
nd
Pat
ien
t Fl
ow
Im
pro
vem
ent
Pro
gram
me
(PFI
P).
In
ad
dit
ion
, th
ere
hav
e b
een
imp
rove
men
ts in
scr
een
ing
dea
ths
and
SJR
pro
cess
es
wh
ich
un
der
pin
th
e Le
arn
ing
fro
m D
eath
asp
ects
of
the
pro
gram
me.
Th
e H
MSR
an
d S
HM
I tra
ject
ory
co
nti
nu
e to
im
pro
ve.
The
nex
t im
pro
vem
ent
focu
s w
ill b
e o
n A
KI a
nd
LR
TI w
ith
lin
ks/i
nte
rdep
end
ency
wit
h t
he
Car
e o
f O
lder
Peo
ple
p
rogr
amm
e.
Imp
lem
enta
tio
n o
f ip
ad f
acili
ty f
or
scre
en
ing
dea
ths
and
mo
rtu
ary
enga
gem
ent
has
imp
rove
d r
ates
. A
pre
sen
tati
on
of
less
on
s le
arn
ed f
rom
SJR
s is
sch
edu
led
at
the
No
vem
ber
G
ran
d R
ou
nd
. Th
e Tr
ust
is a
lso
su
pp
ort
ing
two
acu
te T
rust
on
th
e d
evel
op
men
t o
f le
arn
ing
fro
m d
eath
s as
an
imp
rove
men
t ap
pro
ach
.
Car
ing
Th
e ke
y fo
cus
in t
his
do
mai
n is
to
incr
ease
th
e re
spo
nse
ra
te a
nd
use
of
info
rmat
ion
fro
m t
he
Frie
nd
s an
d F
amily
te
st. T
his
is e
sse
nti
al if
th
e Tr
ust
is t
o id
enti
fy k
ey a
spec
ts o
f p
atie
nt
exp
erie
nce
wh
ich
can
be
imp
rove
d.
Wh
ilst
the
traj
ecto
ry f
or
the
ove
rall
nu
mb
er o
f w
ritt
en
com
pla
ints
is p
osi
tive
th
e fu
ture
fo
cus
will
be
on
imp
rovi
ng
the
pro
cess
, th
emat
ic a
nal
ysis
an
d e
valu
atin
g th
e o
utc
om
e fr
om
th
e p
atie
nt/
care
r p
ersp
ecti
ve.
SMS
Text
an
d In
tera
ctiv
e V
oic
e m
essa
gin
g w
ent
live
on
th
e 1
st O
cto
ber
to
A+E
D
epar
tmen
ts, O
utp
atie
nts
an
d D
ay c
ase
area
s. T
his
has
dem
on
stra
ted
an
in
crea
se in
res
po
nse
rat
es
and
qu
alit
ativ
e co
mm
ents
acr
oss
th
ese
sett
ings
. Th
is w
ill p
rovi
de
mo
re r
epre
sen
tati
ve f
eed
bac
k to
iden
tify
are
as t
o f
ocu
s im
pro
vem
ents
.
The
corp
ora
te n
urs
ing
team
is u
nd
erta
kin
g a
revi
ew o
f th
e co
mp
lain
ts p
roce
ss
and
will
be
lead
ing
an im
pro
vem
ent
pro
gram
me.
Page 81 of 210

TB
204_
19 2
IPR
Sum
mar
y D
ec 1
9
Page 82 of 210


Wel
l-L
edT
arg
etA
ctu
alY
TD
A
ctu
alP
atie
nts
RA
GT
ren
dT
raj
RA
G
Dut
y of
Can
dour
- E
vide
nce
of
Dis
cuss
ion
100%
88.9
%96
.1%
1
Dut
y of
Can
dour
- E
vide
nce
of
Lette
r10
0%88
.9%
95.9
%1
I&E
sur
plus
or
defic
it/to
tal r
even
ue-1
%-7
.1%
-19%
N/A
Liqu
idity
-106
-129
-129
N/A
Dis
tanc
e fr
om C
ontr
ol T
otal
0%-0
.7%
-7.9
%N
/A
Cap
ital S
ervi
ce C
apac
ity0.
21-0
.144
-3.5
59N
/A
% A
genc
y S
taff
(cos
t)5.
45%
9.3%
8.5%
N/A
Use
of R
esou
rces
(F
inan
ce)
Sco
re3
43
N/A
Dis
tanc
e fr
om A
genc
y S
pend
Cap
0%14
2%14
2%N
/A
Sta
ff T
urno
ver
0.76
%1.
1%6.
8%N
/A
Sta
ff T
urno
ver
(Rol
ling)
10%
12.6
%N
/A
Vac
ancy
Rat
e -
Med
ical
5%16
.5%
N/A
Vac
ancy
Rat
e -
Nur
sing
8%17
.3%
N/A
Sic
knes
s R
ate
4%4.
9%4.
9%N
/A
Per
sona
l Dev
elop
men
t Rev
iew
85%
70.6
%71
.5%
N/A
Man
dato
ry T
rain
ing
85%
88.3
%87
.2%
N/A
Car
e H
ours
Per
Pat
ient
Day
(C
HP
PD
)7.
58.
38.
4N
/A
Tim
e to
Rec
ruit
3066
66N
/A
Eff
icie
ncy
Tar
get
Act
ual
YT
D
Act
ual
Pat
ien
tsR
AG
Tre
nd
Tra
j R
AG
MO
FD
(M
edic
ally
Opt
imis
ed fo
r D
isch
arge
) -
Ave
rage
Num
ber
of
Dai
ly B
eds
Lost
In M
onth
5073
6473
DT
OC
- N
umbe
r of
Bed
s lo
st p
er
mon
th21
821
8
Leng
th O
f Sta
y6.
56.
57
N/A
New
:Fol
low
Up
2.64
2.5
2.5
N/A
DN
A (
Did
Not
Atte
nd)
rate
8%7.
2%7.
1%18
37
Can
celle
d O
ps0.
61%
0.4%
0.3%
8
The
atre
Util
isat
ion
- S
DG
H80
%64
.9%
61.3
%N
/A
The
atre
Util
isat
ion
- O
DG
H90
%72
.3%
69.8
%N
/A
Str
ande
d P
atie
nts
(>6
Day
s LO
S)
170
179
1247
179
Sup
er S
tran
ded
Pat
ient
s (>
20 D
ays
LOS
)58
6948
669
Sou
thpo
rt A
&E
Con
vers
ion
Rat
e20
%21
%10
53
Saf
eT
arg
etA
ctu
alY
TD
A
ctu
alP
atie
nts
RA
GT
ren
dT
raj
RA
G
MR
SA
10
10
C-D
iff1.
335
195
Nev
er E
vent
s0
01
0
VT
E P
roph
ylax
is A
sses
smen
ts95
%96
.9%
97.7
%15
1
Har
m F
ree
(Saf
ety
The
rmom
eter
)95
%98
.9%
97.9
%4
Fal
ls -
Mod
erat
e/S
ever
e/D
eath
12
112
Pat
ient
Saf
ety
Inci
dent
s -
Low
, Nea
r M
iss
or N
o H
arm
814
5472
814
Saf
e S
taffi
ng90
%92
.3%
92%
N/A
Fra
ctur
ed N
eck
of F
emur
90%
79.3
%71
.4%
23
Eff
ecti
veT
arg
etA
ctu
alY
TD
A
ctu
alP
atie
nts
RA
GT
ren
dT
raj
RA
G
Per
cent
age
of D
eath
s S
cree
ned
100%
88.9
%60
%7
SH
MI (
Sum
mar
y H
ospi
tal-l
evel
M
orta
lity
Indi
cato
r)10
099
.610
0.7
N/A
HS
MR
- R
ollin
g 12
Mon
ths
(Hos
pita
l S
tand
ardi
sed
Mor
talit
y R
atio
)10
091
91N
/A
WH
O C
heck
list
100%
100%
100%
0
Str
oke
- 90
% S
tay
on S
trok
e W
ard
80%
94.1
%71
.8%
1
Sep
sis
- T
imel
y Id
entif
icat
ion
75%
100%
98.7
%N
/A
Sep
sis
- T
imel
y T
reat
men
t75
%80
%77
.9%
N/A
Car
ing
Tar
get
Act
ual
YT
D
Act
ual
Pat
ien
tsR
AG
Tre
nd
Tra
j R
AG
DS
SA
(D
eliv
erin
g S
ame
Sex
A
ccom
mod
atio
n) B
reac
hes
- T
rust
114
139
14
Writ
ten
Com
plai
nts
3530
151
30
Frie
nds
and
Fam
ily T
est -
% T
hat
Wou
ld R
ecom
men
d -
Tru
st O
vera
ll90
%91
.6%
92.7
%19
2
Boa
rd R
epor
t - O
ctob
er 2
019
RE
GU
LA
TO
RY
Tar
get
Act
ual
YT
D
Act
ual
Pat
ien
tsR
AG
Tre
nd
Tra
j R
AG
CQ
C R
egis
trat
ion
-
Mon
itor
Gov
erna
nce
Rat
ing
Gre
en-
--
-
Res
po
nsi
veT
arg
etA
ctu
alY
TD
A
ctu
alP
atie
nts
RA
GT
ren
dT
raj
RA
G
Acc
iden
t & E
mer
genc
y -
4 H
our
com
plia
nce
94.9
9%84
.6%
86.5
%16
35
Acc
iden
t & E
mer
genc
y -
12+
Hou
r tr
olle
y w
aits
127
6227
Am
bula
nce
Han
dove
rs <
=15
Min
s99
%48
.2%
53.1
%79
0
Dia
gnos
tic w
aits
1.
01%
2.2%
3.6%
61
14 d
ay G
P r
efer
ral t
o O
utpa
tient
s93
%96
.4%
94.4
%30
31 d
ay tr
eatm
ent
96%
95.3
%97
.5%
3
31 d
ay tr
eatm
ent (
Sur
gery
)94
%10
0%10
0%0
31 d
ay tr
eatm
ent (
Ant
i-can
cer
drug
s)98
%10
0%10
0%0
62 d
ay p
athw
ay A
naly
sis
85%
82%
78.6
%9
62 d
ay G
P r
efer
ral t
o tr
eatm
ent
85%
82%
77.4
%9
Ref
erra
l to
trea
tmen
t: on
-goi
ng92
%93
.3%
93.4
%75
0
Bed
Occ
upan
cy -
SD
GH
93%
90%
92.1
%N
/A
Bed
Occ
upan
cy -
OD
GH
60%
52%
48.3
%N
/A
Rep
ortin
g F
requ
ency
is m
onth
ly e
xcep
t for
SH
MI w
hich
is q
uart
erly
.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 1
of 1
TB
204_
19 3
IPR
Das
hboa
rd D
ecem
ber
2019
Oct
ober
Dat
a
Page 83 of 210


Boa
rd R
epor
t - O
ctob
er 2
019
S
afe
Ind
icat
or
Nam
e (C
olo
ur
- P
erf
| Tra
j)D
escr
ipti
on
Nar
rati
veM
on
th T
ren
d
MR
SA
The
num
ber
of M
ethi
cilli
n R
esis
tant
Sta
phyl
ococ
cus
Aur
eus
(MR
SA
) te
st s
ampl
es
that
wer
e po
sitiv
e.
The
thre
shol
d is
0.
The
re w
as z
ero
MR
SA
bac
tera
emia
in O
ctob
er -
Sin
ce th
e M
RS
A b
acte
raem
ia in
Aug
ust,
less
on
lear
ned
have
bee
n in
clud
ed in
Tru
st N
ews,
Man
dato
ry tr
aini
ng a
nd M
edic
al u
pdat
es. I
n ad
ditio
n th
e af
fect
ed w
ard
has
incl
uded
MR
SA
sup
pres
sion
Rxi
ng in
MD
T R
ed to
Gre
en r
evie
ws
and
hudd
les.
Als
o,
whe
n re
view
ing
MR
SA
pat
hway
s th
e IP
C te
am c
ross
ref
eren
ce th
e pa
tient
Rx
char
t and
adv
ise
clin
icia
ns to
con
side
r A
bxs
effe
ctiv
e ag
ains
t MR
SA
if th
e pa
tient
col
onis
ed w
ith M
RS
A a
nd is
bei
ng
trea
ted
for
an in
fect
ion.
C-D
iff
Num
ber
of C
lost
ridiu
m d
iffic
ile
(C. d
iff)
infe
ctio
ns fo
r pa
tient
s ag
ed 2
or
mor
e on
the
date
the
spec
imen
was
take
n.
Tru
st ta
rget
36
for
the
year
. G
ood
perf
orm
ance
is fe
wer
th
an 3
6 fo
r th
e ye
ar.
5 C
diff
cas
es in
Oct
ober
, how
ever
3 o
f the
se w
ill b
e ap
peal
able
as
no la
pses
in c
are
- R
egio
nally
C d
iff
rate
s ha
ve in
crea
sed
this
yea
r an
d S
outh
port
and
Orm
skirk
are
no
exce
ptio
n. T
he ta
rget
for
2019
/20
is
for
no m
ore
than
16
case
s an
d th
e T
rust
has
cur
rent
ly h
ad 2
0 ca
ses,
how
ever
7 o
f the
se c
ases
hav
e be
en s
ucce
ssfu
lly a
ppea
led
and
a fu
rthe
r 4
case
s ar
e el
igib
le fo
r ap
peal
.S
ome
of th
e is
sues
iden
tifie
d as
par
t of t
he R
CA
pro
cess
wer
e m
ultip
le p
resc
riptio
ns o
f Abx
s no
t onl
y in
th
e ho
spita
l but
als
o in
the
com
mun
ity p
rior
to a
dmis
sion
and
frai
l pat
ient
s w
ith fe
edin
g tu
bes
or lo
ng
term
cat
hete
rs.
The
Con
sulta
nt M
icro
biol
ogis
t and
the
Ant
imic
robi
al P
harm
acis
t are
rev
iew
ing
the
curr
ent A
ntim
icro
bial
gu
idel
ines
to r
ecom
men
d su
itabl
e al
tern
ativ
es to
the
freq
uent
use
of c
epha
losp
orin
's w
hich
hav
e an
in
crea
sed
risk
of C
diff
. O
ctob
er's
cas
es o
n w
ards
: SS
U, 1
4B, O
BS
, GP
and
FE
SS
(on
e on
the
FE
SS
cas
es w
as a
com
mun
ity
occu
rrin
g ho
spita
l ass
ocia
ted
case
- th
e ty
ping
of t
his
case
was
diff
eren
t to
the
othe
r F
ES
S c
ase)
Nev
er E
vent
s
Nev
er E
vent
s -
A p
artic
ular
ty
pe o
f ser
ious
inci
dent
that
is
who
lly p
reve
ntab
le a
nd h
as th
e po
tent
ial t
o ca
use
serio
us
patie
nt h
arm
or
deat
h.
The
re w
ere
no n
ever
eve
nts
in O
ctob
er -
The
Tru
st r
epor
ted
1 ne
ver
even
t in
the
last
12
mon
ths
- in
M
ay 2
019.
•
Sig
ns w
ere
imm
edia
tely
put
up
acro
ss a
ll T
heat
re a
reas
in th
e an
aest
hetic
Roo
ms,
follo
win
g th
e ev
ent
to a
lert
sta
ff to
’Sto
p B
efor
e Y
ou B
lock
’ •
The
inci
dent
was
dis
cuss
ed a
t dai
ly S
afet
y H
uddl
es•
Sta
ff aw
aren
ess
sess
ions
wer
e pu
t in
plac
e.•
Tra
inin
g ha
s no
w b
een
put i
n pl
ace
and
this
is in
clud
ed in
the
Clin
ical
Com
pete
ncy
trai
ning
pac
kage
s.•
We
have
a n
ew L
ocss
ip (
in th
e S
OP
tem
plat
e) ‘P
roce
dura
l Ver
ifica
tion
of S
ite M
arki
ng’ b
ased
on
Nat
ssip
s.•
We
have
com
men
ced
a m
onth
ly o
bser
vatio
nal a
udit
of S
top
Bef
ore
You
Blo
ck a
nd th
ere
have
bee
n no
oth
er e
piso
des.
• W
e ha
ve a
sec
tion
incl
uded
in In
duct
ion/
com
pete
ncy
pack
s ar
ound
Sto
p B
efor
e Y
ou B
lock
.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 1
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 84 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
S
afe
Ind
icat
or
Nam
e (C
olo
ur
- P
erf
| Tra
j)D
escr
ipti
on
Nar
rati
veM
on
th T
ren
d
VT
E P
roph
ylax
is A
sses
smen
ts
VT
E r
isk
asse
ssm
ent:
all
inpa
tient
Ser
vice
Use
rs
unde
rgoi
ng r
isk
asse
ssm
ent f
or
VT
E.
Thr
esho
ld 9
5%. G
ood
perf
orm
ance
is h
ighe
r.
Com
plia
nt -
The
Tru
st c
ontin
ues
to a
chie
ve a
bove
the
thre
shol
d of
95%
Har
m F
ree
(Saf
ety
The
rmom
eter
)
Saf
ety
The
rmom
eter
-
Per
cent
age
of P
atie
nts
With
H
arm
Fre
e C
are.
Thr
esho
ld 9
8%. H
ighe
r is
be
tter.
Per
form
ance
rem
ains
abo
ve ta
rget
- P
erfo
rman
ce fo
r O
ctob
er r
emai
ns g
ood
and
in to
tal t
he T
rust
re
port
ed 5
har
ms
durin
g O
ctob
er's
mon
thly
cen
sus.
2
x ca
thet
er a
ssoc
iate
d ur
inar
y tr
act i
nfec
tions
( 7
b an
d 9b
) an
d 3
x ne
w V
TE
's w
hich
wer
e 2
x ne
w
DV
T's
( N
WR
SIU
and
9a
) an
d 1x
new
PE
( 9
a)
Fal
ls -
Mod
erat
e/S
ever
e/D
eath
The
tota
l num
ber
of fa
lls w
ithin
th
e T
rust
wer
e th
e se
verit
y of
th
e ha
rm w
as e
ither
mod
erat
e,
seve
re o
r re
sulte
d in
dea
th.
Thr
esho
ld:0
Per
form
ance
is d
emon
stra
ting
stab
le n
umbe
rs o
f fal
ls w
ith h
arm
but
ear
ly d
emon
stra
tion
of a
red
uctio
n fo
r al
l fal
ls C
BU
spe
cific
- T
he fa
lls w
ith h
arm
are
low
num
bers
and
dem
onst
rate
a r
elat
ivel
y st
able
pi
ctur
e, h
owev
er th
e to
tal f
alls
par
ticul
arly
in U
rgen
t Car
e ap
pear
s to
be
in th
e ea
rly s
tage
s of
sho
win
g a
redu
ctio
n an
d th
is c
ontin
ues
to b
e w
orke
d on
. The
impr
ovem
ent i
s ex
pect
ed to
be
seen
now
eac
h m
onth
.
Wor
k is
und
erw
ay to
dev
elop
a ta
rget
for
all f
alls
map
ped
agai
nst a
traj
ecto
ry w
hich
will
pro
vide
mor
e ob
viou
s ev
iden
ce o
f im
prov
emen
t aga
inst
the
falls
impr
ovem
ent p
lan.
In
add
ition
, 'ba
ckgr
ound
wor
k' in
clud
es in
crea
sing
the
abili
ty to
iden
tify
patie
nts
at r
isk
of fa
lls a
s pe
r N
ICE
Clin
ical
Gui
danc
e 16
, whe
re th
e tr
ust h
as a
lread
y im
prov
ed fr
om 5
6% in
qua
rter
1, t
o 89
% in
qu
arte
r 2.
In
add
ition
we
mon
itor
the
impl
emen
tatio
n of
car
e pl
ans
for
thos
e id
entif
ied
as b
eing
at r
isk.
Thi
s w
as
72%
in Q
1 ris
ing
to 8
7% in
Q2
and
we
cont
inue
to s
triv
e to
war
ds th
e 95
% ta
rget
.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 2
of 2
3
Page 85 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
S
afe
Ind
icat
or
Nam
e (C
olo
ur
- P
erf
| Tra
j)D
escr
ipti
on
Nar
rati
veM
on
th T
ren
d
Pat
ient
Saf
ety
Inci
dent
s -
Low
, Nea
r M
iss
or N
o H
arm
The
num
ber
of in
cide
nts
rela
ting
to p
atie
nts
whe
re th
e se
verit
y w
as L
ow, N
ear
Mis
s or
N
o H
arm
cau
sed.
A h
ighe
r nu
mbe
r is
goo
d.
Incr
ease
in r
epor
ting
of N
o ha
rm/N
ear
mis
s/Lo
w h
arm
inci
dent
s by
71
- O
f thi
s in
crea
se 4
6 of
the
incr
ease
d in
cide
nts
are
attr
ibut
ed to
bed
man
agem
ent.
Thi
s re
late
s to
the
dela
y in
tran
sfer
of p
atie
nts
from
the
emer
genc
y ar
eas
to g
ener
al w
ards
and
from
thea
tre
and
Crit
ical
car
e to
gen
eral
war
ds to
en
able
new
pat
ient
s to
be
adm
itted
. Thi
s co
rrel
ates
with
the
pres
sure
on
A&
E/ E
AU
from
adm
issi
ons
thro
ugho
ut O
ctob
er.
Ano
ther
are
a sh
owin
g a
sign
ifica
nt in
crea
se is
Infe
ctio
n co
ntro
l with
an
incr
ease
of 1
5 re
latin
g to
the
batc
h im
port
of b
acte
raem
ia p
atie
nts
onto
dat
ix.
Saf
e S
taffi
ng
The
rat
io b
etw
een
the
prop
osed
num
ber
of n
ursi
ng
staf
f to
ensu
re a
saf
e st
affin
g le
vel a
nd th
e ac
tual
num
ber
of
nurs
es w
orki
ng th
ose
shift
s.
Thr
esho
ld: 9
5%, F
ail 9
0%.
The
Tru
st r
epor
ts a
n im
prov
ed p
ositi
on to
saf
e st
affin
g ag
ains
t the
nat
iona
l ave
rage
(90
%)
at 9
2.3%
. -
Sup
port
to im
prov
ed d
eliv
ery
agai
nst s
afe
staf
fing
perf
orm
ance
con
tinue
s th
roug
h fle
xibl
e w
orke
r op
port
uniti
es, c
onsi
dera
tion
of a
n ov
erse
as r
ecru
itmen
t pro
posa
l, lo
cal r
ecru
itmen
t ong
oing
.
Fra
ctur
ed N
eck
of F
emur
Per
cent
age
of F
NO
F o
pera
ted
on w
ithin
36
hour
s of
ad
mis
sion
.
Thr
esho
ld: 9
0%.
Per
form
ance
is s
how
ing
cont
inuo
us im
prov
emen
t fol
low
ing
bette
r us
e of
the
'gol
den
patie
nt' o
n th
e tr
aum
a lis
t - T
here
is n
ow b
ette
r us
e of
prio
ritis
ing
#NO
F p
atie
nts
as g
olde
n an
d si
lver
pat
ient
s on
the
thea
tre
list t
o en
sure
we
mee
t the
36h
rs to
thea
tre
targ
et.
Cur
rent
cap
acity
ena
bles
us
to o
pera
te o
n 3
NO
Fs
in 1
thea
tre
day.
Ofte
n th
ere
is m
ore
than
3 N
OF
pa
tient
s on
a th
eatr
e lis
t, as
wel
l as
othe
r pa
tient
s, th
eref
ore
whe
re o
ther
pat
ient
s ha
ve to
take
prio
rity,
th
is c
reat
es a
del
ay to
NO
F p
atie
nts
until
the
follo
win
g da
y.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 3
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 86 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
E
ffect
ive
Ind
icat
or
Nam
e (C
olo
ur
- P
erf
| Tra
j)D
escr
ipti
on
Nar
rati
veM
on
th T
ren
d
SH
MI (
Sum
mar
y H
ospi
tal-l
evel
M
orta
lity
Indi
cato
r)
Sum
mar
y H
ospi
tal-l
evel
M
orta
lity
Indi
cato
r (S
HM
I) is
the
stan
dard
ised
mor
talit
y bo
th in
ho
spita
l and
with
in 3
0 da
ys o
f di
scha
rge.
Sou
rce
= D
r. F
oste
r.
Ple
ase
note
: Thi
s in
dica
tor
is
repo
rted
qua
rter
ly (
rolli
ng 1
2 m
onth
s) a
nd is
6 m
onth
s be
hind
due
to w
hen
Dr
Fos
ter
publ
ish
the
data
.
Per
form
ance
with
in to
lera
nce,
figu
re is
with
in s
tatis
tical
nor
ms.
- N
HS
Dig
ital n
ow r
elea
se th
e S
HM
I m
onth
ly. P
erfo
rman
ce is
gen
eral
ly im
prov
ed.
As
SH
MI a
nd H
SM
R a
re b
oth
risk
adju
sted
mor
talit
y fig
ures
, the
act
ions
des
crib
ed in
the
HS
MR
na
rrat
ive,
als
o ap
ply
to S
HM
I.
HS
MR
- R
ollin
g 12
Mon
ths
(Hos
pita
l S
tand
ardi
sed
Mor
talit
y R
atio
)
The
rat
io o
f the
obs
erve
d nu
mbe
r of
in-h
ospi
tal d
eath
s w
ith a
Hos
pita
l Sta
ndar
dise
d M
orta
lity
Rat
io (
HS
MR
) di
agno
sis
to th
e ex
pect
ed
num
ber
of d
eath
s, m
ultip
lied
by
100.
Ple
ase
note
: Thi
s in
dica
tor
is
repo
rted
mon
thly
and
is 3
m
onth
s be
hind
due
to w
hen
Dr
Fos
ter
publ
ish
the
data
.
Per
form
ance
is w
ithin
acc
epte
d to
lera
nce
- -
In-m
onth
ach
ieve
men
t:1.
4/5
wor
ksho
ps fo
r th
e re
-sco
ping
of t
he d
eter
iora
ting
patie
nt p
roje
ct a
re c
ompl
ete.
6th
wor
kstr
eam
to
be s
cope
d (in
form
atio
n / d
ocum
enta
tion)
. Com
plet
ed r
e-sc
opin
g ex
pect
ed b
y ne
xt m
onth
.2.
Tw
o fu
rthe
r pr
ojec
ts to
red
uce
harm
from
nos
ocom
ial i
nfec
tion
are
bein
g de
vise
d3.
Dra
ft re
port
of p
robl
ems
in h
ealth
care
bei
ng d
evis
ed fr
om th
e 11
7 S
JR r
evie
ws
com
plet
ed s
o fa
r in
th
e tr
ust t
o al
low
targ
eted
ana
lysi
s of
this
ric
h da
ta. d
raft
repo
rt fo
r D
ecem
ber
MO
G.
Ong
oing
wor
k on
UT
I - th
is is
now
an
AQ
faci
litat
ed p
roje
ct to
red
uce
urin
ary
cath
eter
isat
ion.
Thi
s is
pr
edic
ted
to h
ave
mul
tiple
ben
efits
incl
udin
g im
prov
ed m
obili
ty, i
mpr
oved
con
tinen
ce a
nd a
red
uctio
n in
U
TI a
nd g
ram
-ve
infe
ctio
n.
A n
ew p
roje
ct h
as b
een
initi
ated
to r
educ
e va
riatio
n in
IV c
annu
la c
are
aim
ing
to r
educ
e as
soci
ated
st
aphy
loco
ccal
infe
ctio
n.
The
uni
fied
AC
MP
tem
plat
e to
sup
port
trai
ning
and
use
of A
CM
P to
rec
ord
deci
sion
s ab
out a
ppro
pria
te
ceili
ngs
of tr
eatm
ent i
s un
der
deve
lopm
ent.
Thi
s pr
ojec
t is
acro
ss m
ultip
le p
rovi
ders
in th
e he
alth
ec
onom
y an
d w
ill fa
cilit
ate
the
use
of A
ntic
ipat
ory
Clin
ical
Man
agem
ent P
lans
, pre
vent
ing
unw
ante
d ho
spita
l adm
issi
on a
nd im
prov
ing
the
achi
evem
ent o
f pre
ferr
ed p
lace
of d
eath
.
The
re is
dev
elop
men
t of a
pro
cess
to r
evie
w lo
wer
res
pira
tory
trac
t and
UT
I dea
ths
to e
nsur
e th
ese
are
in th
e co
rrec
t dia
gnos
tic g
roup
s. S
yste
m d
evis
ed to
allo
w c
o-m
orbi
dity
dat
a id
entif
ied
in c
odin
g re
view
s to
be
mad
e av
aila
ble
to c
linic
al s
taff
if pa
tient
Is r
e-ad
mitt
ed to
info
rm c
are
of th
e pa
tient
.
WH
O C
heck
list
WH
O C
heck
list.
W
HO
che
cklis
t com
plia
nce
cont
inue
s to
ach
ieve
100
% -
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 4
of 2
3
Page 87 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
E
ffect
ive
Ind
icat
or
Nam
e (C
olo
ur
- P
erf
| Tra
j)D
escr
ipti
on
Nar
rati
veM
on
th T
ren
d
Per
cent
age
of D
eath
s S
cree
ned
Per
cent
age
of D
eath
s S
cree
ned
- D
AT
IX
Sig
nific
ant i
mpr
ovem
ent i
s m
aint
aine
d -
Thi
s im
prov
emen
t fol
low
s th
e im
plem
enta
tion
of th
e iP
AD
sy
stem
and
the
rem
inde
r po
ster
s. T
here
rem
ains
a fo
cus
on th
is a
rea
in o
rder
to m
aint
ain
and
impr
ove
perf
orm
ance
.
Scr
eeni
ng o
f mor
talit
y is
impo
rtan
t to
allo
w th
e tr
ust m
orta
lity
revi
ewer
s to
focu
s th
eir
atte
ntio
ns o
n th
e ap
prop
riate
cas
es fo
r S
JR. W
e ai
m fo
r 90
%+
scr
eeni
ng to
ass
ure
that
the
vast
maj
ority
of d
eath
s ha
ve
a cl
inic
al r
evie
w.
We
cont
inue
to m
onito
r to
ens
ure
the
proc
ess
beco
mes
em
bedd
ed.
Str
oke
- 90
% S
tay
on S
trok
e W
ard
Pro
port
ion
of s
trok
e pa
tient
s w
ho h
ave
90%
of t
heir
hosp
ital
stay
on
a de
dica
ted
stro
ke
war
d. T
hres
hold
80%
. Goo
d pe
rfor
man
ce is
hig
her.
Ple
ase
note
: Ind
icat
or m
ay c
hang
e as
a
resu
lt of
del
ayed
val
idat
ion.
Str
oke
perf
orm
ance
ach
ieve
d ab
ove
the
80%
targ
et in
Oct
ober
at 9
4.12
% -
The
Tru
st h
as
dem
onst
rate
d an
impr
ovem
ent t
rend
sin
ce F
ebru
ary
of th
is y
ear
Sep
sis
- T
imel
y Id
entif
icat
ion
Sep
sis
Tim
ely
iden
tific
atio
n of
se
psis
in e
mer
genc
y de
part
men
ts a
nd a
cute
in
patie
nt s
ettin
gs -
Nat
iona
l ea
rly w
arni
ng s
core
(N
EW
s)
reco
rded
with
in 1
hou
r of
ho
spita
l arr
ival
.
The
trus
t con
tinue
s to
ach
ieve
the
targ
et fo
r id
entif
icat
ion
of S
epsi
s -
The
tota
l num
ber
of a
ttend
ance
to
A&
E n
atio
nally
in J
uly
2019
was
2,2
66,9
13 a
n in
crea
se o
f 4%
from
the
prev
ious
yea
r an
d th
e hi
ghes
t nu
mbe
r of
atte
ndan
ces
ever
rec
orde
d si
nce
colle
ctio
n of
figu
res
star
ted.
Sep
sis
- T
imel
y T
reat
men
t
Sep
sis
Tim
ely
trea
tmen
t for
se
psis
in e
mer
genc
y de
part
men
ts a
nd a
cute
in
patie
nt s
ettin
gs-
the
rate
of
rapi
d ad
min
istr
atio
n of
an
tibio
tics
with
in o
ne h
our
of
diag
nosi
s of
sep
sis.
Our
rol
ling
perf
orm
ance
bet
wee
n Ja
nuar
y 20
19 to
Aug
ust 2
019
for
antib
iotic
s w
ith 1
hou
r is
cur
rent
ly
achi
evin
g 80
%. -
Thi
s is
aga
inst
a b
ackd
rop
of th
e to
tal n
umbe
r of
atte
ndan
ces
to A
&E
nat
iona
lly in
Ju
ly 2
019
whi
ch w
as 2
,266
,913
rep
rese
ntin
g 4%
from
the
prev
ious
yea
r. T
his
is t
he h
ighe
st n
umbe
r of
at
tend
ance
sin
ce n
atio
nal d
ata
colle
ctio
n st
arte
d. T
he to
tal n
umbe
r of
atte
ndan
ce to
A&
E n
atio
nally
in
Aug
ust 2
019
was
2,1
25,4
45.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 5
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 88 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
C
arin
gIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
DS
SA
(D
eliv
erin
g S
ame
Sex
A
ccom
mod
atio
n) B
reac
hes
- T
rust
Thi
s in
dica
tor
mon
itors
the
Tru
st's
par
t in
the
NH
S
com
mitm
ent t
o el
imin
ate
mix
ed
sex
acco
mm
odat
ion.
Eac
h pa
tient
bre
ache
s ea
ch 2
4 ho
urs.
Bre
ache
s re
mai
n at
a s
tabl
e le
vel -
The
maj
ority
of b
reac
hes
are
in H
DU
and
Obs
war
d. T
here
is a
re
view
of a
ll pa
tient
s fo
r st
epdo
wn
from
crit
ical
car
e at
all
bed
mee
tings
and
the
plan
is d
epen
dent
on
the
over
all T
rust
pos
ition
; The
Crit
ical
Car
e M
anag
er a
ttend
s th
e 13
:30
bed
mee
ting
daily
; Obs
War
d w
ill c
ontin
ue to
follo
w p
olic
y an
d w
ork
with
all
team
s, a
nd r
epor
t bre
ache
s if
they
occ
ur; n
ew s
ingl
e se
x br
each
for
criti
cal c
are
is to
be
revi
ewed
Writ
ten
Com
plai
nts
The
tota
l num
ber
of c
ompl
aint
s re
ceiv
ed.
A lo
wer
num
ber
is g
ood.
The
re w
ere
30
com
plai
nts
in O
ctob
er -
The
num
ber
of c
ompl
aint
s re
ceiv
ed s
ugge
sts
that
pat
ient
s ar
e aw
are
of th
e co
mpl
aint
s pr
oced
ure.
the
com
plai
nts
cont
inue
to b
e re
port
ed in
to th
e Q
ualit
y an
d S
afet
y re
port
s fo
r ea
ch C
linic
al B
usin
ess
Uni
t and
in th
e in
tegr
ated
Gov
erna
nce
Rep
ort p
rese
nted
at Q
&S
C
omm
ittee
for
com
plai
nts
anal
ysis
suc
h as
tren
ds, t
hem
es a
nd r
espo
nsiv
enes
s.
The
com
plai
nts
data
has
bee
n sp
lit in
to lo
w le
vel c
once
rns
and
form
al c
ompl
aint
s gr
aded
3 o
r ab
ove
usin
g th
e tr
ust g
radi
ng to
ol. T
he fo
rmal
com
plai
nts
ofte
n in
clud
e m
ore
than
one
are
a of
com
plai
nt.
Urg
ent C
are
rece
ived
16
com
plai
nts,
with
War
d 10
A (
EA
U)
acco
untin
g fo
r 4
and
A&
E 2
. Pla
nned
Car
e re
ceiv
ed 6
com
plai
nts,
in 3
diff
eren
t are
as. S
peci
alis
t Ser
vice
s re
ceiv
ed 7
com
plai
nts,
of w
hich
2
rela
ted
to M
ater
nity
. 1 c
ompl
aint
was
rec
eive
d by
Est
ates
and
Fac
ilitie
s an
d re
late
d to
Sec
urity
.T
he fo
llow
ing
them
es w
ere
iden
tifie
d:•
Clin
ical
Tre
atm
ent –
in p
artic
ular
ly c
o-or
dina
tion
of m
edic
al tr
eatm
ent
• S
taff
attit
ude/
beha
viou
r•
End
of l
ife•
Adm
issi
on/tr
ansf
ers/
disc
harg
e pr
oced
ure
• C
omm
unic
atio
n•
Dat
e fo
r ap
poin
tmen
t
All
com
plai
nts
are
revi
ewed
with
in th
e B
usin
ess
Uni
ts a
nd r
espo
nse
and
rele
vant
act
ions
are
put
into
pl
ace.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 6
of 2
3
Page 89 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
C
arin
gIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
Frie
nds
and
Fam
ily T
est -
% T
hat
Wou
ld R
ecom
men
d -
Tru
st O
vera
ll
The
pro
port
ion
of p
atie
nts
over
all w
ho r
espo
nded
that
th
ey w
ould
be
likel
y or
ex
trem
ely
likel
y to
rec
omm
end
the
Tru
st to
Frie
nds
and
Fam
ily.
Per
form
ance
has
slig
htly
im
prov
ed o
n pr
evio
us m
onth
s da
ta b
ut r
emai
ls b
elow
targ
et o
f 94%
. -
Per
form
ance
impr
oved
on
prev
ious
mon
th b
ut r
emai
ns b
elow
targ
et o
f 94%
.
Oct
ober
was
the
first
mon
th im
plem
entin
g th
e E
NV
OY
sys
tem
and
the
Tru
st h
as s
een
a si
gnifi
cant
im
prov
emen
t in
resp
onse
rat
es (
6.48
% to
21.
18%
)an
d an
incr
ease
in q
ualit
ativ
e co
mm
ents
sup
port
ing
the
ratin
gs g
iven
.
Pla
nned
car
e -
thos
e th
at w
ould
rec
omm
end
has
incr
ease
d to
95.
81%
from
94.
34%
Urg
ent c
are-
thos
e th
at w
ould
rec
omm
end
has
incr
ease
d to
88.
96%
from
79.
67%
. (T
his
incl
udes
a
scor
e of
88%
that
wou
ld r
ecom
men
d fr
om th
e A
dult
Em
erge
ncy
Dep
artm
ent)
. .
Mat
erni
ty -
thos
e th
at w
ould
rec
omm
end
has
incr
ease
d to
100
% fr
om 9
7.09
.%.
Pae
diat
rics
- th
ose
that
wou
ld r
ecom
men
d ha
s de
crea
sed
to 9
2.24
% fr
om 9
3.33
% (
Thi
s in
clud
es a
sc
ore
of 9
1.92
% th
at w
ould
rec
omm
end
from
the
Pae
diat
ric E
mer
genc
y D
epar
tmen
t).
Fro
m q
ualit
ativ
e co
mm
ents
rec
eive
d al
ongs
ide
nega
tive
ratin
gs t
he to
p th
emes
iden
tifie
d w
ere
staf
f at
titud
e, c
omm
unic
atio
n, im
plem
enta
tion
of c
are
and
wai
ting
times
.
All
seni
or w
ard/
dept
sta
ff no
w h
ave
the
oppo
rtun
ity to
acc
ess
EN
VO
Y fo
r liv
e F
FT
dat
a to
ena
ble
timel
y ac
tion
to b
e ta
ken
at a
loca
l lev
el in
res
pons
e to
poo
r ra
tings
/com
men
ts a
nd th
e ab
ility
to id
entif
y po
sitiv
e/ne
gativ
e th
emes
to d
irect
loca
l im
prov
emen
ts. F
FT
dat
a is
als
o pr
esen
ted
on w
ard/
dept
da
shbo
ards
alo
ngsi
de th
e nu
mbe
r co
mpl
aint
s/co
ncer
ns to
sup
port
iden
tific
atio
n of
any
tren
ds.
Fro
m th
e 1s
t Nov
embe
r on
war
ds th
e m
atro
n fo
r pa
tient
exp
erie
nce
rece
ives
dai
ly a
lert
s fo
r ra
tings
of
unlik
ely
/ ext
rem
ely
unlik
ely
to m
onito
r th
emes
and
act
ion
any
resp
onse
s th
at r
equi
re im
med
iate
at
tent
ion
The
Tru
st h
as n
ow r
ecei
ved
resu
lts fr
om a
ll fo
ur N
atio
nal P
atie
nt E
xper
ienc
e S
urve
ys (
Mat
erni
ty
resu
lts a
wai
ting
rele
ase
from
CQ
C).
Loc
al a
ctio
n pl
ans
yet t
o be
dev
elop
ed b
y le
ads
with
in th
e P
aedi
atric
s, M
ater
nity
and
Adu
lt E
mer
genc
y C
are
depa
rtm
ents
. O
nce
deve
lope
d th
ese
will
be
pres
ente
d to
and
mon
itore
d th
roug
h th
e T
rust
Pat
ient
Exp
erie
nce
Gro
up.
The
202
0-20
21 T
rust
pat
ient
exp
erie
nce
stra
tegy
is c
urre
ntly
in d
raft
form
at. T
his
will
be
deliv
ered
for
cons
ulta
tion
at th
e Ja
n-20
pat
ient
exp
erie
nce
grou
p.
FF
T %
that
will
rec
omm
end
will
con
tinue
to b
e m
onito
red
and
repo
rted
to w
ards
/dep
ts. o
n a
mon
thly
ba
sis.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 7
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 90 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
R
espo
nsiv
eIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
Acc
iden
t & E
mer
genc
y -
4 H
our
com
plia
nce
Per
cent
age
of p
atie
nts
spen
ding
less
than
4 h
ours
in a
A
&E
dep
artm
ent f
rom
arr
ival
to
disc
harg
e, tr
ansf
er o
r ad
mis
sion
.
95%
targ
et. G
ood
perf
orm
ance
is
hig
her.
The
Sou
thpo
rt s
ite c
ontin
ues
to e
xper
ienc
e ch
alle
nges
in m
aint
aini
ng p
atie
nt fl
ow. T
his
a co
mbi
natio
n of
a 9
.4%
incr
ease
in a
ttend
ance
s on
the
Sou
thpo
rt s
ite (
an e
xtra
418
pat
ient
s) a
nd s
igni
fican
t bed
pr
essu
res.
- A
s a
resu
lt, th
ere
was
an
incr
ease
in th
e nu
mbe
r of
pat
ient
s w
ho w
aite
d lo
nger
than
4
hour
s in
ED
(15
04 p
atie
nts
com
pare
d to
114
3 pa
tient
s la
st y
ear)
. Rev
iew
s ha
ve b
een
unde
rtak
en to
un
ders
tand
the
reas
ons
for
the
brea
ches
(65
.82%
of 4
-hou
r br
each
es w
ere
attr
ibut
able
to b
ed d
elay
s;
15.3
5% w
ere
due
to E
D d
elay
s, 9
% w
ere
due
to s
peci
alty
del
ays,
8%
wer
e du
e to
clin
ical
del
ays)
. ED
co
ntin
ues
to tr
y an
d st
reng
then
sta
ffing
leve
ls. E
D n
ow h
as 7
wte
con
sulta
nts
in p
ost (
the
high
est
num
ber
to d
ate)
. M
iddl
e gr
ade
leve
l sta
ffing
rem
ains
a c
halle
nge.
Lat
e sh
ift s
taffi
ng c
ontin
ues
to b
e en
hanc
ed w
here
pos
sibl
e as
this
is w
hen
activ
ity le
vels
freq
uent
ly e
xcee
d ca
paci
ty. A
vac
ant E
NP
pos
t is
cur
rent
ly o
ut to
adv
ert,
whi
ch w
ill e
nabl
e th
e cu
rren
t ava
ilabi
lity
of a
n E
NP
min
ors
serv
ice
to b
e ex
tend
ed. T
he P
atie
nt F
low
Impr
ovem
ent P
rogr
amm
e co
ntin
ues
to w
ork
thro
ugh
high
impa
ct a
ctio
ns.
AC
U is
pilo
ting
Sun
day
open
ing
acro
ss a
num
ber
of d
ates
. A s
ucce
ssfu
l pilo
t was
hel
d at
the
end
of
Oct
ober
with
15
patie
nts
stre
amed
from
ED
and
0 r
equi
ring
adm
issi
on. T
he c
ontin
ued
bed
pres
sure
s re
sult
in o
ngoi
ng u
se o
f esc
alat
ion
area
s, w
hich
neg
ativ
ely
affe
cts
the
abili
ty to
max
imis
e st
ream
ing.
A
PD
SA
is p
lann
ed in
ED
to te
st im
prov
emen
ts in
red
ucin
g tr
iage
tim
es (
wc
18/1
1/19
)
Acc
iden
t & E
mer
genc
y -
12+
Hou
r tr
olle
y w
aits
The
num
ber
of p
atie
nts
wai
ting
mor
e th
an 1
2 ho
urs,
for
an
emer
genc
y ad
mis
sion
via
A&
E,
from
the
poin
t whe
n th
e de
cisi
on is
mad
e to
adm
it to
the
time
whe
n th
e pa
tient
is
adm
itted
.
The
thre
shol
d is
0.
The
re w
ere
x27
12-h
our
brea
ches
acr
oss
the
mon
th. T
hese
wer
e al
l rel
ated
to in
patie
nt b
ed p
ress
ures
. -
All
brea
ches
occ
urre
d du
ring
and
imm
edia
tely
follo
win
g w
eeke
nd p
ress
ures
. ED
saw
a 9
.4%
incr
ease
in
atte
ndan
ces
acro
ss th
e m
onth
(ad
ditio
nal 4
18 p
atie
nts)
and
90
addi
tiona
l adm
issi
ons.
Acr
oss
the
maj
ority
of t
he m
onth
, the
Tru
st w
orke
d ag
ains
t the
12
hour
sta
ndar
d w
ith a
ll es
cala
tion
area
s op
en a
nd
in u
se, h
igh
num
bers
of p
atie
nts
bedd
ed o
vern
ight
in E
D e
ach
nigh
t aw
aitin
g a
bed
and
corr
idor
car
e in
us
e du
e to
lack
of c
linic
al c
apac
ity in
the
depa
rtm
ent.
Tim
elin
es h
ave
been
com
plet
ed fo
r al
l 27
patie
nts
with
ass
uran
ce p
rovi
ded
that
all
patie
nts
rece
ived
tim
ely
and
appr
opria
te c
linic
al c
are
whi
lst i
n th
e de
part
men
t. T
he s
yste
m is
pro
vide
d co
ntin
ually
with
upd
ates
on
the
Tru
st's
esc
alat
ion
posi
tion.
Dai
ly
hudd
les
cont
inue
to ta
ke p
lace
with
sys
tem
par
tner
s to
ena
ble
the
redu
ctio
n of
leng
th o
f sta
y. Is
sues
ar
ound
leng
th o
f sta
y, IC
B a
nd c
omm
unity
cap
acity
con
tinue
to b
e ad
dres
sed
and
regu
lar
disc
ussi
ons
take
pla
ce w
ith th
e P
rogr
amm
e D
irect
or fo
r U
npla
nned
and
Em
erge
ncy
Car
e. D
isch
arge
team
co
ntin
ues
to h
ave
a pr
esen
ce a
t wee
kend
s to
try
and
supp
ort d
isch
arge
s ac
ross
the
wee
kend
, and
st
affin
g is
rou
tinel
y se
cure
d fo
r th
e us
e of
esc
alat
ion
area
s. T
he A
cute
team
hav
e id
entif
ied
a nu
mbe
r of
Sun
days
ove
r th
e co
min
g m
onth
s th
at th
ey a
re a
ble
to o
pen
AC
U to
sup
port
str
eam
ing
from
ED
in
effo
rts
to r
educ
e th
e nu
mbe
r of
pat
ient
s id
entif
ied
as r
equi
ring
beds
who
are
clin
ical
ly a
ppro
pria
te fo
r ad
mis
sion
.
Am
bula
nce
Han
dove
rs <
=15
Min
s
All
hand
over
s be
twee
n am
bula
nce
and
A&
E s
taff
to
occu
r w
ithin
15
min
utes
. Thi
s m
easu
re lo
oks
at th
e pe
rcen
tage
of h
ando
vers
with
in
15 m
inut
es.
Am
bula
nce
hand
over
s co
mpl
eted
with
in 1
5 m
ins
drop
ped
to 4
8.23
% -
Thi
s is
a r
efle
ctio
n of
the
incr
ease
of 9
.4%
in o
vera
ll at
tend
ance
s an
d th
e ch
alle
nges
in in
patie
nt fl
ow, r
esul
ting
in h
igh
num
bers
of
pat
ient
s aw
aitin
g be
ds in
ED
and
del
ays
in ti
mel
y ac
cess
to E
D c
ubic
les.
83.
63%
of p
atie
nts
arriv
ing
by a
mbu
lanc
e w
ere
hand
ed o
ver
with
in 3
0 m
inut
es fr
om a
rriv
al, c
ompa
red
to 7
2.91
% la
st O
ctob
er. T
he
Tru
st a
ttend
ed th
e 1s
t NW
AS
Han
dove
r C
olla
bora
tive
on 2
5/10
/19
and
is n
ow o
n a
90 d
ay
impr
ovem
ent p
rogr
amm
e. P
DS
A c
ycle
s ar
e pl
anne
d fo
r F
it to
Sit
(led
by N
WA
S)
and
Con
sulta
nt b
ased
in
tria
ge (
plan
ned
for
wc
18/1
1/19
.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 8
of 2
3
Page 91 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
R
espo
nsiv
eIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
Dia
gnos
tic w
aits
The
num
ber
of p
atie
nts
wai
ting
6 w
eeks
or
mor
e fo
r a
diag
nost
ic te
st e
xpre
ssed
as
a pe
rcen
tage
of a
ll pa
tient
s w
aitin
g.
Thr
esho
ld 1
%. G
ood
perf
orm
ance
is lo
wer
.
Per
form
ance
con
tinue
s to
impr
ove
for
the
four
th m
onth
in a
row
- B
reac
hes
are
as fo
llow
s:
Col
onos
copy
2 p
atie
nts
1.6%
ava
ilabi
lity/
patie
nt c
hoic
e
Com
pute
d T
omog
raph
y 1p
t 0.5
%
Cys
tosc
opy
13pt
s 12
.0%
Con
sulta
nt a
ctiv
ity -
spe
cial
ist s
ervi
ce -
spi
nal s
ervi
ce 2
pat
ient
cho
ice.
3
brea
ches
are
thea
tre
case
s du
e to
lack
of t
heat
re c
apac
ity d
ue to
the
incr
ease
in d
eman
d fo
r T
arge
t/Urg
ent c
ases
. 7 b
reac
hes
are
due
to E
mer
genc
y le
ave
take
n by
the
cons
ulta
nt in
Oct
ober
w
here
the
list h
ad to
be
canc
elle
d. 1
bre
ache
s ar
e du
e to
the
Uro
logy
/Spi
nal C
onsu
ltant
that
can
onl
y se
e th
e pa
tient
s. P
lan
to a
ccom
mod
ate
alte
rnat
e w
eekl
y se
ssio
n w
ith U
rolo
gy/S
pina
l Con
sulta
nt w
ithin
jo
b pl
an g
oing
forw
ard.
Cys
tosc
opy
(Gyn
aeco
logy
) 1p
t Cap
acity
issu
es. P
atie
nt h
as T
CI 2
0.11
.19
Fle
xi S
igm
oido
scop
y 2p
ts 2
.9%
2 p
atie
nt c
hoic
e 1
no in
terp
rete
r av
aila
ble.
G
astr
osco
py 2
pts
1.4%
1 p
atie
nt c
hoic
e 1
is d
ue to
pat
ient
dec
isio
n to
hav
e pr
oced
ure
unde
r G
A in
th
eatr
e.M
RI 2
pts
0.6%
2 b
reac
hes
both
at 6
wee
ks I
ssue
s co
ntac
ting
both
pat
ient
s N
on O
bs U
ltras
ound
34p
ts 3
.4%
cap
apci
ty is
sues
Uro
dyna
mic
s T
OT
AL
(S
PLI
T O
UT
BE
LOW
) 5p
ts 7
.5%
U
rody
nam
ics
(tre
atm
ent c
entr
e, U
rolo
gy)
17pt
s 1
Em
erge
ncy
leav
e ta
ken
via
spec
ialis
t nur
se -
on
the
day
8 pa
tient
cho
ice
Uro
dyna
mic
s (G
yn)
4pts
sta
ff si
ckne
ss
Inso
urci
ng h
as b
een
agre
ed b
y th
e tr
ust w
ith 'Y
our
Med
ical
' a c
ompa
ny w
ho a
re k
now
n to
the
trus
t and
ha
ve p
revi
ousl
y de
liver
ed w
ork
for
us. T
his
wor
k ha
s co
mm
ence
d an
d al
l pa
tient
s ha
ve b
een
offe
red
or
book
ed in
Nov
embe
r. N
umbe
rs h
ave
decr
ease
d an
d sh
ow c
ontin
ued
impr
ovem
ent g
oing
forw
ard.
14 d
ay G
P r
efer
ral t
o O
utpa
tient
s
Per
cent
age
of p
atie
nts
seen
w
ithin
two
wee
ks o
f an
urge
nt
GP
ref
erra
l for
sus
pect
ed
canc
er.
Tar
get 9
3%. G
ood
perf
orm
ance
is
hig
her.
Per
form
ance
has
rec
over
ed to
be
com
plia
nt in
Sep
tem
ber
- A
lthou
gh th
e de
man
d fo
r ap
poin
tmen
ts
rem
aine
d hi
gh in
som
e tu
mou
r gr
oups
, ove
rall
num
ber
of r
efer
rals
was
dow
n.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 9
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 92 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
R
espo
nsiv
eIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
31 d
ay tr
eatm
ent
Per
cent
age
of p
atie
nts
rece
ivin
g fir
st d
efin
itive
tr
eatm
ent w
ithin
one
mon
th (
31
days
) of
a c
ance
r di
agno
sis
(mea
sure
d fr
om 'd
ate
of
deci
sion
to tr
eat')
.
Tar
get 9
6%. G
ood
perf
orm
ance
is
hig
her.
3 br
each
es in
Aug
ust r
esul
ted
in fa
iled
targ
et -
Bre
ache
s w
ere
due
to c
apac
ity in
col
orec
tal t
heat
res
and
derm
atol
ogy
patie
nt c
hoic
e.
31 d
ay tr
eatm
ent (
Sur
gery
)
Per
cent
age
of p
atie
nts
rece
ivin
g fir
st d
efin
itive
sur
gica
l tr
eatm
ent w
ithin
one
mon
th (
31
days
) of
a c
ance
r di
agno
sis
(mea
sure
d fr
om 'd
ate
of
deci
sion
to tr
eat')
.
Per
form
ance
con
tinue
s to
be
mai
ntai
ned
at 1
00%
- T
hree
pat
ient
s w
ere
trea
ted
in th
e su
bseq
uent
su
rger
y ca
tego
ry in
Sep
tem
ber,
all
in ti
me.
31 d
ay tr
eatm
ent (
Ant
i-can
cer
drug
s)
Per
cent
age
of p
atie
nts
rece
ivin
g fir
st d
efin
itive
ant
i-ca
ncer
dru
g tr
eatm
ent w
ithin
on
e m
onth
(31
day
s) o
f a
canc
er d
iagn
osis
(m
easu
red
from
'dat
e of
dec
isio
n to
trea
t').
Com
plia
nce
mai
ntai
ned
at 1
00%
- O
nly
1 pa
tient
was
trea
ted
in th
is c
ateg
ory
in S
epte
mbe
r.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 10
of 2
3
Page 93 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
R
espo
nsiv
eIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
62 d
ay p
athw
ay A
naly
sis
All
Tru
st B
oard
s sh
ould
hav
e si
ght o
f tum
our
spec
ific
perf
orm
ance
aga
inst
the
62 d
ay
GP
ref
erra
l to
trea
tmen
t.
Som
e im
prov
emen
t see
n in
per
form
ance
- 5
0 ac
coun
tabl
e pa
tient
s w
ere
trea
ted
in S
epte
mbe
r. T
here
w
ere
9 br
each
es in
tota
l. th
is o
ccur
red
in th
e fo
llow
ing
tum
our
site
s;H
aem
atol
ogy
0.5
Hea
d &
Nec
k 0.
5C
olor
ecta
l 3O
ther
1U
rolo
gy 4
62 d
ay G
P r
efer
ral t
o tr
eatm
ent
Per
cent
age
of P
atie
nts
rece
ivin
g fir
st d
efin
itive
tr
eatm
ent f
or c
ance
r w
ithin
two
mon
ths
(62
days
) of
urg
ent G
P
refe
rral
for
susp
ecte
d ca
ncer
.
Tar
get 8
5%. G
ood
perf
orm
ance
is
hig
her.
Sep
tem
ber
clos
ed a
t 82%
- S
epte
mbe
r's p
erfo
rman
ce c
lose
d at
the
high
est p
ositi
on s
ince
Oct
ober
last
ye
ar. T
here
wer
e 50
acc
ount
able
trea
tmen
ts a
nd 9
bre
ache
s.
Ref
erra
l to
trea
tmen
t: on
-goi
ng
Per
cent
age
of p
atie
nts
on a
n in
com
plet
e pa
thw
ay w
ith a
cu
rren
t wai
t exp
erie
nce
of 1
8 w
eeks
or
less
.
Thr
esho
ld 9
2%. G
ood
perf
orm
ance
is h
ighe
r.
The
trus
t con
tinue
s to
mai
ntai
n co
mpl
ianc
e w
ith R
TT
- P
erfo
rman
ce is
cur
rent
ly b
eing
impa
cted
by
issu
es w
ithin
ana
esth
etic
s an
d va
rious
wor
kfor
ce is
sues
with
in s
peci
aliti
es. T
hese
wor
kfor
ce s
hort
falls
ha
ve h
isto
rical
ly b
een
addr
esse
d w
ith W
LIs.
Cur
rent
pen
sion
s ta
x is
sues
hav
e m
eant
this
is n
o lo
nger
a
solu
tion.
The
impa
ct is
bei
ng a
sses
sed
in o
rder
to a
ddre
ss th
is.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 11
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 94 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
R
espo
nsiv
eIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
Bed
Occ
upan
cy -
SD
GH
Per
cent
age
bed
occu
panc
y at
th
e S
outh
port
site
.
A lo
wer
per
cent
age
is g
ood.
T
hres
hold
is 9
3%.
Oct
ober
saw
a s
light
incr
ease
in o
ccup
ancy
for
Sou
thpo
rt s
ite b
ut th
e tr
ust a
chie
ved
targ
et fo
r th
e fo
urth
m
onth
in a
row
- ta
rget
leve
l was
ach
ieve
d at
89.
99%
- D
aily
bed
occ
upan
cy is
mon
itore
d th
roug
h th
e es
cala
tion
mee
tings
and
impr
ovem
ent w
ork
to r
educ
e oc
cupa
ncy
bein
g un
dert
aken
and
mon
itore
d vi
a th
e P
atie
nt F
low
Impr
ovem
ent G
roup
Bed
Occ
upan
cy -
OD
GH
Per
cent
age
bed
occu
panc
y at
th
e O
rmsk
irk s
ite, b
ased
on
open
bed
s. A
hig
her
perc
enta
ge is
goo
d. T
hres
hold
is
60%
.
Occ
upan
cy h
as r
emai
ned
stab
le in
mon
th 5
2.04
% a
nd is
slig
htly
bel
ow tr
ajec
tory
- -
Ele
ctiv
e ac
tivity
is
curr
ently
bei
ng im
pact
ed b
y th
e lo
ss o
f ana
esth
etic
s an
d th
e as
soci
ated
red
uctio
n in
cas
es.
Rec
ruitm
ent o
f ana
esth
etis
ts is
ong
oing
. Can
cella
tions
are
dis
trib
uted
am
ongs
t the
spe
cial
ties.
The
or
der
of p
riorit
y is
: mai
ntai
ning
crit
ical
car
e, th
en a
cute
car
e, th
en th
e O
rmsk
irk s
ite. T
his
is m
onito
red
thro
ugh
the
thea
tre
sche
dulin
g m
eetin
g an
d w
eekl
y P
TL.
HB
S c
ontr
act h
as a
lso
been
neg
otia
ted
to
enab
le a
naes
thet
ic c
over
. Oct
ober
saw
can
cella
tion
of li
sts
as a
res
ult o
f the
atre
sta
ff si
ckne
ss.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 12
of 2
3
Page 95 of 210
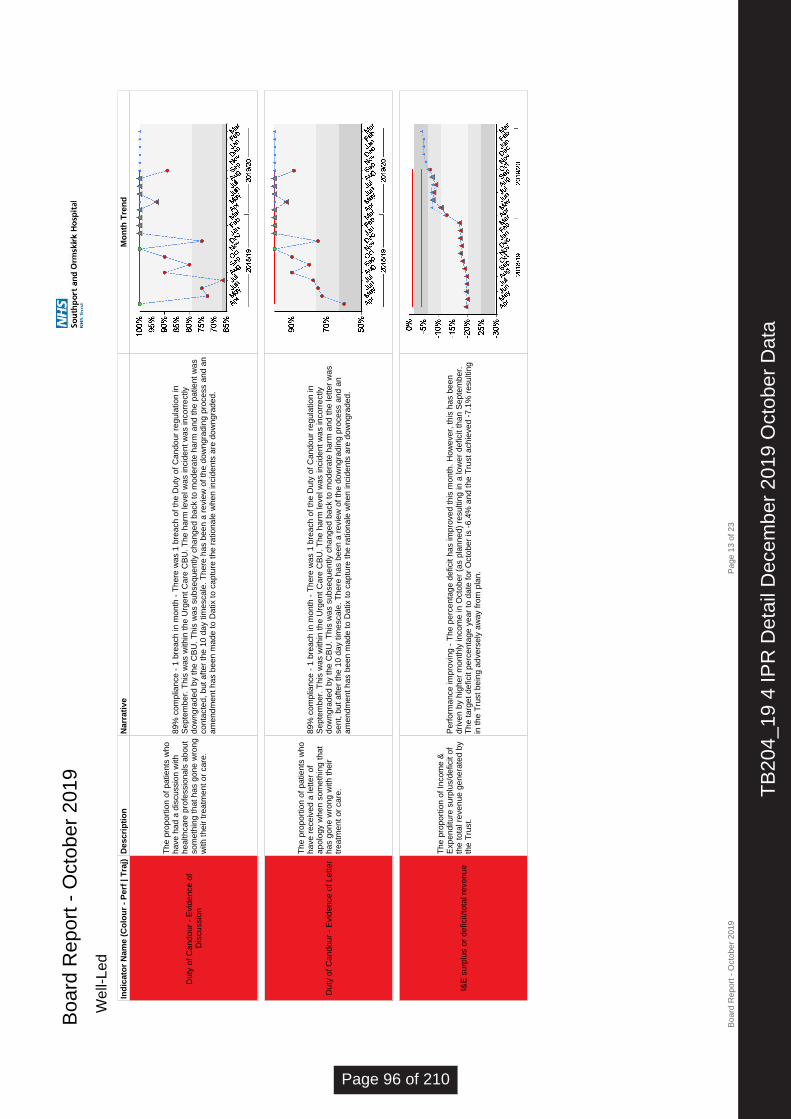
Boa
rd R
epor
t - O
ctob
er 2
019
W
ell-L
edIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
Dut
y of
Can
dour
- E
vide
nce
of
Dis
cuss
ion
The
pro
port
ion
of p
atie
nts
who
ha
ve h
ad a
dis
cuss
ion
with
he
alth
care
pro
fess
iona
ls a
bout
so
met
hing
that
has
gon
e w
rong
w
ith th
eir
trea
tmen
t or
care
.
89%
com
plia
nce
- 1
brea
ch in
mon
th -
The
re w
as 1
bre
ach
of th
e D
uty
of C
ando
ur r
egul
atio
n in
S
epte
mbe
r. T
his
was
with
in th
e U
rgen
t Car
e C
BU
. The
har
m le
vel w
as in
cide
nt w
as in
corr
ectly
do
wng
rade
d by
the
CB
U. T
his
was
sub
sequ
ently
cha
nged
bac
k to
mod
erat
e ha
rm a
nd th
e pa
tient
was
co
ntac
ted,
but
afte
r th
e 10
day
tim
esca
le. T
here
has
bee
n a
revi
ew o
f the
dow
ngra
ding
pro
cess
and
an
amen
dmen
t has
bee
n m
ade
to D
atix
to c
aptu
re th
e ra
tiona
le w
hen
inci
dent
s ar
e do
wng
rade
d.
Dut
y of
Can
dour
- E
vide
nce
of L
ette
r
The
pro
port
ion
of p
atie
nts
who
ha
ve r
ecei
ved
a le
tter
of
apol
ogy
whe
n so
met
hing
that
ha
s go
ne w
rong
with
thei
r tr
eatm
ent o
r ca
re.
89%
com
plia
nce
- 1
brea
ch in
mon
th -
The
re w
as 1
bre
ach
of th
e D
uty
of C
ando
ur r
egul
atio
n in
S
epte
mbe
r. T
his
was
with
in th
e U
rgen
t Car
e C
BU
. The
har
m le
vel w
as in
cide
nt w
as in
corr
ectly
do
wng
rade
d by
the
CB
U. T
his
was
sub
sequ
ently
cha
nged
bac
k to
mod
erat
e ha
rm a
nd th
e le
tter
was
se
nt, b
ut a
fter
the
10 d
ay ti
mes
cale
. The
re h
as b
een
a re
view
of t
he d
owng
radi
ng p
roce
ss a
nd a
n am
endm
ent h
as b
een
mad
e to
Dat
ix to
cap
ture
the
ratio
nale
whe
n in
cide
nts
are
dow
ngra
ded.
I&E
sur
plus
or
defic
it/to
tal r
even
ue
The
pro
port
ion
of In
com
e &
E
xpen
ditu
re s
urpl
us/d
efic
it of
th
e to
tal r
even
ue g
ener
ated
by
the
Tru
st.
Per
form
ance
impr
ovin
g -
The
per
cent
age
defic
it ha
s im
prov
ed th
is m
onth
. How
ever
, thi
s ha
s be
en
driv
en b
y hi
gher
mon
thly
inco
me
in O
ctob
er (
as p
lann
ed)
resu
lting
in a
low
er d
efic
it th
an S
epte
mbe
r.
The
targ
et d
efic
it pe
rcen
tage
yea
r to
dat
e fo
r O
ctob
er is
-6.
4% a
nd th
e T
rust
ach
ieve
d -7
.1%
res
ultin
g in
the
Tru
st b
eing
adv
erse
ly a
way
from
pla
n.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 13
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 96 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
W
ell-L
edIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
Liqu
idity
Liqu
idity
indi
cate
s w
heth
er th
e pr
ovid
er c
an m
eet i
ts
oper
atio
nal c
ash
oblig
atio
ns.
Dow
nwar
d tr
end
cont
inue
s -
Loan
s ar
e re
-cla
ssifi
ed a
s cu
rren
t lia
bilit
ies
whe
n th
ey a
re d
ue w
ithin
12
mon
ths.
Thi
s re
-cla
ssifi
catio
n ha
s oc
curr
ed in
Oct
ober
and
sig
nific
antly
affe
cts
the
calc
ulat
ion
of th
e m
etric
res
ultin
g in
a d
eter
iora
tion
in li
quid
ity.
Liqu
idity
day
s is
cal
cula
tes
as fo
llow
s:(C
urre
nt a
sset
s –
curr
ent l
iabi
litie
s –
inve
ntor
ies)
/(op
erat
ing
expe
nses
+ a
mor
tisat
ion
+ d
epre
ciat
ion)
X
num
ber
of d
ays
in th
e ye
ar to
dat
e re
port
ing.
Mon
th 7
liqu
idity
day
s is
-£6
9.25
8m /
£114
.573
m *
214
day
s =
-12
9.36
day
s
Dis
tanc
e fr
om C
ontr
ol T
otal
Dis
tanc
e fr
om C
ontr
ol T
otal
.
Per
form
ance
det
erio
rate
d in
Oct
ober
- T
he T
rust
ach
ieve
d th
e co
ntro
l tot
al a
t the
end
of Q
uart
er 2
with
no
n re
curr
ent s
uppo
rt. A
t mon
th 7
the
Tru
st is
cur
rent
ly b
ehin
d pl
an b
ut h
as p
lans
to m
itiga
te th
is r
isk
and
mee
t the
Qua
rter
3 c
ontr
ol to
tal.
Cap
ital S
ervi
ce C
apac
ity
The
leve
l of d
ebt t
he T
rust
is
requ
ired
to s
ervi
ce. T
his
indi
cato
r is
1 o
f 5 u
sed
to
deriv
e th
e 'U
se o
f Res
ourc
es
(Fin
ance
)' sc
ore.
Per
form
ance
impr
oved
in O
ctob
er -
The
mai
n re
ason
for
the
impr
ovem
ent i
n th
is m
etric
is th
at th
e T
rust
re
paid
DH
SC
loan
s fo
r £2
.741
mill
ion.
The
re's
no
chan
ge to
the
ratin
g of
this
met
ric w
hich
due
to it
be
ing
nega
tive
rem
ains
at a
4. P
erfo
rman
ce n
eeds
to b
e a
posi
tive
1.25
to a
chie
ve a
use
of r
esou
rces
sc
ore
of 3
for
this
asp
ect.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 14
of 2
3
Page 97 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
W
ell-L
edIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
% A
genc
y S
taff
(cos
t)
The
cos
t of a
genc
y st
aff a
s a
prop
ortio
n of
the
tota
l cos
t of
the
wor
kfor
ce.
Rel
iant
on
finan
ce s
yste
m to
m
onito
r sp
end
rath
er th
an th
e H
R s
yste
m.
Per
form
ance
det
erio
ratin
g -
Age
ncy
spen
d re
mai
ns h
igh
as a
per
cent
age
of to
tal p
ay c
ost.
Age
ncy
spen
d is
slig
htly
up
on S
epte
mbe
r (£
1.1m
aga
inst
£1.
05m
last
mon
th).
Tot
al p
ay s
pend
is a
lso
high
er
this
mon
th th
an la
st m
onth
. S
o bo
th th
e nu
mer
ator
and
den
omin
ator
in th
is c
alcu
latio
n ha
s in
crea
sed
but t
he o
vera
ll re
sult
is a
slig
ht r
educ
tion
in p
erce
ntag
e.P
erfo
rman
ce b
y st
aff g
roup
is:
Con
sulta
nts
16%
Oth
er m
edic
al 1
4%N
ursi
ng &
Mid
wife
ry 9
%S
cien
tific
/tech
/ther
apeu
tic 2
%O
ther
sta
ff 5%
Use
of R
esou
rces
(F
inan
ce)
Sco
re
A F
inan
cial
per
form
ance
sco
re
deriv
ed fr
om th
e N
HS
Im
prov
emen
t 'U
se o
f R
esou
rces
' ass
essm
ent
fram
ewor
k.
Per
form
ance
det
erio
rate
d in
Oct
ober
- O
vera
ll sc
ore
has
incr
ease
d fr
om a
3 la
st m
onth
to 4
this
mon
th.
The
mai
n ch
ange
has
bee
n on
the
dist
ance
from
pla
n m
etric
whi
ch is
now
a 2
(la
st m
onth
1)
as th
e T
rust
is a
dver
sely
aw
ay fr
om it
s pl
an a
t the
end
of O
ctob
er.
All
the
othe
r m
etric
s re
mai
n at
4-
Cap
ital
serv
ice
cove
r, L
iqui
dity
, I&
E m
argi
n an
d ag
ency
rat
ing.
Dis
tanc
e fr
om A
genc
y S
pend
Cap
Dis
tanc
e fr
om A
genc
y S
pend
C
ap.
Per
form
ance
det
erio
rate
d -
Alth
ough
the
Tru
st d
id n
ot a
gree
to th
e ag
ency
cap
the
targ
et fo
r m
onth
7
YT
D is
£2.
882
mill
ion.
The
act
ual m
onth
7 Y
TD
age
ncy
spen
d is
£6.
978
mill
ion.
Oct
ober
has
see
n th
e hi
ghes
t in
mon
th a
genc
y sp
end
with
mon
thly
nur
se a
genc
y at
its
high
est l
evel
. B
and
5 nu
rses
hav
e a
vaca
ncy
rate
of 2
5% a
nd n
ot a
ll th
ese
can
be fi
lled
with
ban
k st
aff w
hich
res
ults
in
the
Tru
st h
avin
g to
pay
a p
rem
ium
for
agen
cy n
urse
s.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 15
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 98 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
W
ell-L
edIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
Sta
ff T
urno
ver
Sta
ff T
urno
ver
is c
alcu
late
d by
ta
king
the
num
ber
of le
aver
s di
vide
d by
the
aver
age
head
coun
t fro
m th
e st
art a
nd
end
of th
e m
onth
.
Oct
ober
saw
a m
onth
ly d
ecre
ase
in tu
rnov
er to
1.1
2% h
owev
er th
e ro
lling
rat
e is
stil
l inc
reas
ing
due
to
the
over
all i
ncre
ase
in s
taff
turn
over
. - T
he n
umbe
r of
leav
ers
redu
ced
slig
htly
in m
onth
to 3
4 fr
om 3
8 in
S
epte
mbe
r an
d A
ugus
t. T
he T
rust
had
est
ablis
hed
a N
ursi
ng R
ecru
itmen
t and
Ret
entio
n gr
oup
whi
ch
initi
ally
saw
a s
igni
fican
t dec
reas
e in
nur
sing
turn
over
how
ever
the
grou
p is
und
er r
evie
w fo
llow
ing
the
appo
intm
ent o
f the
New
Dep
uty
Dire
ctor
of N
ursi
ng fo
r W
orkf
orce
. D
ue to
the
dete
riora
ting
Tru
st
posi
tion
in r
elat
ion
to s
taff
turn
over
(in
crea
sed
rolli
ng fi
gure
) a
new
wor
kfor
ce d
ashb
oard
is b
eing
cr
eate
d. T
he d
ashb
oard
will
pro
vide
gre
ater
bus
ines
s in
telli
genc
e in
to s
taff
turn
over
to id
entif
y ho
tpot
s in
ord
er th
at a
ppro
pria
te in
terv
entio
ns c
an b
e pu
t int
o pl
ace.
Wor
k w
ill b
e re
port
ed a
t a w
eekl
y W
orkf
orce
Impr
ovem
ent w
ork
stre
am w
hich
will
rep
ort i
nto
the
Tru
st’s
Wor
kfor
ce Im
prov
emen
t Gro
up.
A d
raft
dash
boar
d w
ill b
e av
aila
ble
for
revi
ew fr
om J
anua
ry 2
020.
Sta
ff T
urno
ver
(Rol
ling)
Sta
ff T
urno
ver
(Rol
ling)
is
calc
ulat
ed b
y ta
king
the
num
ber
of le
aver
s ov
er th
e pa
st
12 m
onth
s di
vide
d by
the
aver
age
head
coun
t fro
m th
e la
st 1
2 m
onth
s.
The
rol
ling
staf
f tur
nove
r ha
s in
crea
sed
in O
ctob
er 2
019
at 1
2.6%
com
pare
d to
12.
3% in
Sep
tem
ber
2019
. -
The
num
ber
of le
aver
s re
duce
d sl
ight
ly in
mon
th to
34
from
38
in S
epte
mbe
r an
d A
ugus
t. T
he
Tru
st h
ad e
stab
lishe
d a
Nur
sing
Rec
ruitm
ent a
nd R
eten
tion
grou
p w
hich
initi
ally
saw
a s
igni
fican
t de
crea
se in
nur
sing
turn
over
how
ever
the
grou
p is
und
er r
evie
w fo
llow
ing
the
appo
intm
ent o
f the
New
D
eput
y D
irect
or o
f Nur
sing
for
Wor
kfor
ce.
Due
to th
e de
terio
ratin
g T
rust
pos
ition
in r
elat
ion
to s
taff
turn
over
(in
crea
sed
rolli
ng fi
gure
) a
new
wor
kfor
ce d
ashb
oard
is b
eing
cre
ated
. T
he d
ashb
oard
will
pr
ovid
e gr
eate
r bu
sine
ss in
telli
genc
e in
to s
taff
turn
over
to id
entif
y ho
tpot
s in
ord
er th
at a
ppro
pria
te
inte
rven
tions
can
be
put i
nto
plac
e. W
ork
will
be
repo
rted
at a
wee
kly
Wor
kfor
ce Im
prov
emen
t wor
k st
ream
whi
ch w
ill r
epor
t int
o th
e T
rust
’s W
orkf
orce
Impr
ovem
ent G
roup
. A
dra
ft da
shbo
ard
will
be
avai
labl
e fo
r re
view
from
Jan
uary
202
0.
Vac
ancy
Rat
e -
Med
ical
The
pro
port
ion
of p
lann
ed
med
ical
est
ablis
hmen
t tha
t is
curr
ently
vac
ant.
The
med
ical
vac
ancy
rat
e sa
w a
furt
her
incr
ease
in O
ctob
er to
16.
5% -
App
licat
ions
to m
edic
al p
osts
ha
ve in
crea
sed
sinc
e th
e im
plem
enta
tion
of th
e B
MJ
adve
rtis
ing
cam
paig
n. F
urth
er p
lans
are
in
deve
lopm
ent t
o sc
ope
incr
ease
d ut
ilisa
tion
of s
ocia
l med
ia to
pro
mot
e ca
mpa
igns
. Con
trac
ting
com
plet
ed w
ith fr
amew
ork
agen
cy. E
ngag
ed w
ith h
ard
to r
ecru
it sp
ecia
lties
incl
udin
g R
adio
logy
and
A
naes
thet
ics.
Ana
esth
etic
PA
s re
crui
tmen
t in
prog
ress
; offe
rs m
ade
to g
row
alte
rnat
ive
futu
re w
orkf
orce
with
pla
ns in
pl
ace
to c
omm
ence
in Q
3/4.
Det
aile
d pr
ojec
t pla
n in
pla
ce to
sup
port
red
uctio
n in
tim
e to
hire
man
aged
thro
ugh
mod
el
hosp
italp
rogr
amm
e bo
ard
and
Wor
kfor
ce Im
prov
emen
t Gro
up.
Med
ical
est
ablis
hmen
t con
trol
impl
emen
tatio
n -
Pro
cess
to b
e im
plem
ente
d to
iden
tify
recr
uitm
ent
area
s
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 16
of 2
3
Page 99 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
W
ell-L
edIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
Vac
ancy
Rat
e -
Nur
sing
The
pro
port
ion
of p
lann
ed
nurs
ing
esta
blis
hmen
t tha
t is
curr
ently
vac
ant.
Nur
sing
Vac
ancy
rat
e re
mai
ns s
tatic
- A
lthou
gh th
e va
canc
y fig
ures
rem
ain
stat
ic th
e tr
ust h
as s
een
in
Oct
ober
25.
67 F
TE
new
sta
rter
s (R
N x
13 H
CA
x12
)Le
aver
s fo
r O
ct to
tals
13.
49 F
TE
(R
N X
6.8
HC
A X
6.69
). L
ocal
rec
ruitm
ent c
ontin
ues
to s
uppo
rt th
e tr
ust v
acan
cy p
ositi
on.
Sic
knes
s R
ate
The
pro
port
ion
of th
e su
bsta
ntiv
e W
TE
in m
onth
who
w
ere
unav
aila
ble
for
wor
k.
Thr
esho
ld: 4
%. L
ower
is b
ette
r.
Oct
ober
s 20
19's
mon
thly
sic
knes
s ab
senc
e ra
te h
as in
crea
sed
in m
onth
to 4
.94%
how
ever
rem
ains
un
der
the
5% tr
ajec
tory
for
the
year
- T
he r
ollin
g ye
ar to
dat
e si
ckne
ss a
bsen
ce r
ate
high
light
s pr
ogre
ss
mad
e to
dat
e an
d th
at th
ere
has
been
a m
onth
on
mon
th r
educ
tion
of th
e T
rust
’s r
ollin
g si
ckne
ss
abse
nce
rate
sin
ce D
ecem
ber
2018
whi
ch h
as b
een
sust
aine
d fo
r 11
mon
ths:
D
ec-1
8 -
5.95
%Ja
n-19
- 5
.89%
Feb
-19
- 5.
82%
Mar
-19
- 5.
76
Apr
-19
- 5.
72%
M
ay-1
9 -
5.70
%Ju
n-19
- 5
.65%
Ju
l-19
- 5.
61%
Aug
-19
– 5.
54%
Sep
t-19
– 5
.35%
Oct
-19
– 5.
20%
The
Tru
st m
onito
rs a
ttend
ance
leve
ls o
n a
mon
thly
bas
is a
nd r
emai
ns c
omm
itted
to s
uppo
rtin
g st
aff’s
at
tend
ance
to w
ork
to b
e ‘H
appy
, Hea
lthy
Her
e’. T
he T
rust
con
tinue
s to
be
part
of t
he N
HS
i Hea
lth a
nd
Wel
lbei
ng (
HW
B)
prog
ram
me
and
rece
ntly
atte
nded
the
NH
Si H
ealth
and
Wel
lbei
ng S
umm
it (R
educ
ing
sick
ness
abs
ence
) in
Nov
embe
r, w
here
all
trus
ts o
n th
e pr
ogra
mm
e sh
ared
thei
r ex
perie
nce
and
prog
ress
to d
ate.
Con
sequ
ently
the
HW
B a
ctio
n pl
an w
ill b
e re
view
ed in
ord
er to
eva
luat
e an
d co
nsid
er
the
good
pra
ctic
e an
d id
eas
that
wer
e sh
ared
at t
hat e
vent
. T
his
will
sup
port
the
Tru
sts
ongo
ing
assu
ranc
e to
del
iver
ing
the
HW
B a
ctio
n pl
an.
Per
form
ance
aga
inst
the
actio
n pl
an is
mon
itore
d at
W
orkf
orce
Com
mitt
ee a
nd W
orkf
orce
Impr
ovem
ent G
roup
to e
nsur
e pr
ogre
ss a
nd g
ive
assu
ranc
e.In
add
ition
to th
e ab
ove
The
Tru
st h
as e
mba
rked
upo
n a
6 m
onth
rev
iew
of t
he S
uppo
rtin
g A
ttend
ance
po
licy
with
sta
ff si
de a
nd k
ey s
take
hold
ers
with
in th
e T
rust
. An
initi
al m
eetin
g ha
s ta
ken
plac
e, w
ith a
fu
rthe
r m
eetin
g pl
anne
d be
fore
the
end
of th
e ye
ar to
agr
ee th
e re
view
of t
he p
olic
y. P
artn
ersh
ip h
as
flour
ishe
d du
ring
this
pie
ce o
f wor
k an
d di
scus
sion
s ha
ve b
een
wel
l str
uctu
red,
pro
duct
ive
and
mea
ning
ful.
Con
sequ
ently
ther
e is
a b
elie
f tha
t we
can
get t
o a
posi
tion
whe
re b
oth
staf
f sid
e an
d m
anag
emen
t sid
e co
nsid
er th
e T
rust
has
a p
olic
y in
pla
ce th
at s
uppo
rts
all s
taff.
Per
sona
l Dev
elop
men
t Rev
iew
Per
cent
age
of s
taff
with
an
up
to d
ate
Per
sona
l Dev
elop
men
t R
evie
w (
PD
R).
Rol
ling
12 m
onth
figu
re.
PD
R c
ompl
ianc
e in
crea
sed
slig
htly
in m
onth
to 7
0.56
% in
Oct
ober
. - C
BU
’s c
ontin
ue to
set
traj
ecto
ries
to in
crea
se a
ppra
isal
rat
es to
85%
but
hav
e be
en u
nabl
e to
mee
t the
m. O
ver
the
last
few
mon
ths
a ta
rget
ed a
ppro
ach
by th
e O
D te
am h
as b
een
take
n to
impr
ovin
g th
e qu
ality
of a
ppra
isal
s an
d a
myt
h bu
ster
has
bee
n de
velo
ped
and
shar
ed a
t dep
artm
enta
l/war
d vi
sits
in o
rder
to tr
y to
tack
le th
is is
sue.
T
his
wor
k ha
s se
en a
slig
ht im
prov
emen
t in
the
com
plia
nce
rate
by
near
ly 1
% s
ince
last
mon
th.
Mul
tiple
fact
ors
have
bee
n id
entif
ied
thro
ugho
ut th
e ye
ar in
und
erst
andi
ng th
e ba
rrie
rs to
impr
ovin
g co
mpl
ianc
e an
d su
bseq
uent
inte
rven
tions
hav
e be
en e
stab
lishe
d to
add
ress
the
mat
ter.
A c
olle
ctiv
e ta
rget
ed a
ppro
ach
is b
eing
take
n to
look
at h
ow b
est t
o ad
dres
s th
is K
PI i
n D
ecem
ber’s
Wor
kfor
ce
Impr
ovem
ent G
roup
.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 17
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 100 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
W
ell-L
edIn
dic
ato
r N
ame
(Co
lou
r -
Per
f | T
raj)
Des
crip
tio
nN
arra
tive
Mo
nth
Tre
nd
Man
dato
ry T
rain
ing
The
per
cent
age
of s
taff
with
up
to d
ate
Man
dato
ry T
rain
ing.
Thr
esho
ld: 8
5%.
Rol
ling
12 m
onth
figu
re.
Cor
e m
anda
tory
trai
ning
rem
ains
abo
ve th
e T
rust
's 8
5% a
t 88.
34%
- A
Tas
k &
Fin
ish
Gro
up in
N
ov/D
ec20
19 w
ill fo
cus
on a
rev
iew
of c
ore
man
dato
ry tr
aini
ng w
ith a
spe
cific
focu
s on
Res
usci
tatio
n T
rain
ing
at a
ll le
vels
.
Car
e H
ours
Per
Pat
ient
Day
(C
HP
PD
)
Num
ber
of n
ursi
ng c
are
hour
s w
orke
d pe
r pa
tient
day
. Thi
s in
dica
tor
is u
sed
to m
easu
re
nurs
e st
affin
g le
vels
.
The
ove
rall
CH
pPD
for
the
Tru
st h
as r
emai
ned
stat
ic i
n m
onth
rep
ortin
g at
8.3
hou
rs -
Cur
rent
re
port
ing
rem
ains
slig
htly
abo
ve th
e na
tiona
l ave
rage
of 7
hou
rs C
HpP
D, T
he T
rust
cur
rent
rep
ortin
g fo
r C
HpP
D in
clud
es R
egis
tere
d N
urse
s/R
egis
tere
d M
idw
ives
. .
Pla
nned
car
e cl
inic
al b
usin
ess
unit
(CB
U)
repo
rt o
vera
ll 10
.3, U
rgen
t Car
e C
BU
6.6
and
Wom
en’s
and
C
hild
ren’
s 13
.0 o
vera
ll.
Tim
e to
Rec
ruit
The
num
ber
of w
orki
ng d
ays
from
Adv
ert C
lose
to S
tart
D
ate.
Ple
ase
note
that
ca
ndid
ates
req
uirin
g a
Vis
a ar
e in
clud
ed.
-
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 18
of 2
3
Page 101 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
E
ffici
ency
Ind
icat
or
Nam
e (C
olo
ur
- P
erf
| Tra
j)D
escr
ipti
on
Nar
rati
veM
on
th T
ren
d
MO
FD
(M
edic
ally
Opt
imis
ed fo
r D
isch
arge
) -
Ave
rage
Num
ber
of D
aily
B
eds
Lost
In M
onth
Ave
rage
Num
ber
of D
aily
Bed
s Lo
st In
Mon
th.T
aken
from
A
Dai
ly S
naps
hot O
f Pat
ient
s M
edic
ally
Fit
For
Dis
char
ge.
Low
er is
bet
ter.
Incr
ease
in m
onth
- im
prov
emen
ts in
rec
ordi
ng o
f dat
a on
med
way
is g
ivin
g a
mor
e co
rrec
t mea
sure
to
wor
k w
ith. W
e co
ntin
ue to
wor
k w
ith c
omm
unity
and
LA
team
s to
sup
port
mov
emen
t of p
atie
nts
from
ac
ute
care
onc
e m
edic
ally
fit.
The
re r
emai
ns a
pro
port
ion
of p
atie
nts
who
req
uire
on-
goin
g th
erap
y w
hich
can
not
be
supp
orte
d in
the
com
mun
ity d
ue to
the
leve
l of d
epen
denc
y. D
aily
hud
dles
con
tinue
w
ith in
form
atio
n fr
om th
e di
scha
rge
faci
litat
ors
from
Red
2Gre
en b
oard
rou
nds;
SA
FE
R e
ngag
emen
t ev
ents
hav
e oc
curr
ed a
t war
d le
vel.
new
wee
kly
DT
OC
mee
ting
com
men
ced
to fo
rmal
ise
repo
rts;
ci
rcul
atio
n of
new
boa
rd r
ound
SO
P a
nd r
ed2g
reen
pos
ter
is h
elpi
ng to
focu
s al
l sta
ff on
flow
DT
OC
- N
umbe
r of
Bed
s lo
st p
er
mon
th
The
num
ber
of b
eds
lost
per
m
onth
from
pat
ient
s w
ho h
ave
expe
rienc
ed a
Del
ayed
T
rans
fer
of C
are
(DT
OC
).
The
se p
atie
nts
will
hav
e be
en
Med
ical
ly O
ptim
ised
for
Dis
char
ge (
MO
FD
) an
d th
e de
lay
conf
irmed
by
the
loca
l au
thor
ity.
218
bed
days
lost
- T
here
is c
ontin
ued
wor
k w
ith p
artn
ers
from
Com
mun
ity a
nd L
A s
uppo
rtin
g di
scha
rges
thro
ugh
daily
hud
dle
and
wee
kly
long
sta
y re
view
. Fro
m O
ctob
er o
f for
mal
DT
OC
mee
tings
ta
ke p
lace
with
bot
h LA
s to
agr
ee d
elay
s;
Leng
th O
f Sta
y
The
ave
rage
am
ount
of t
ime
in
days
that
pat
ient
s sp
ent a
s an
in
patie
nt fr
om a
n em
erge
ncy
adm
issi
on. E
xclu
des
ZE
RO
Le
ngth
of S
tay.
sust
aine
d at
<6.
5 da
ys -
wor
kstr
eam
s re
port
ing
thro
ugh
to P
atie
nt F
low
Impr
ovem
ent P
rogr
amm
e to
su
ppor
t util
isat
ion
of a
sses
smen
t are
as (
wor
k st
ream
1)
and
redu
cing
LoS
(w
orks
trea
m 2
);
enga
gem
ent e
vent
s w
ith a
ll in
-pat
ient
war
ds to
sup
port
SA
FE
R a
t war
d le
vel h
ave
been
com
plet
ed;
intr
oduc
tion
of b
oard
rou
nd S
OP
to s
uppo
rt im
plem
ent i
mpr
oved
red
2gre
en; c
ontin
ued
daily
rev
iew
th
roug
h di
scha
rge
hudd
le w
ith s
yste
m p
artn
ers
with
del
ays
iden
tifie
d th
roug
h w
ard
red2
gree
n bo
ard
roun
ds o
n al
l in-
patie
nt w
ards
; hea
d of
pat
ient
flow
and
CC
G fo
r S
efto
n w
orki
ng c
lose
ly to
geth
er to
su
ppor
t red
ucin
g Lo
S w
ith fo
cus
on s
uper
str
ande
d an
d st
rand
ed p
atie
nts
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 19
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 102 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
E
ffici
ency
Ind
icat
or
Nam
e (C
olo
ur
- P
erf
| Tra
j)D
escr
ipti
on
Nar
rati
veM
on
th T
ren
d
New
:Fol
low
Up
The
Tru
st's
ove
rall
ratio
be
twee
n ne
w o
utpa
tient
ap
poin
tmen
ts a
nd fo
llow
-up
outp
atie
nt a
ppoi
ntm
ents
.
Thr
esho
ld: m
onito
r.
The
trus
t con
tinue
s to
con
sist
ently
ach
ieve
targ
et -
DN
A (
Did
Not
Atte
nd)
rate
The
pro
port
ion
of p
atie
nts
of a
ll th
ose
offe
red
appo
intm
ents
or
trea
tmen
t dat
es th
at d
o no
t giv
e no
tice
of n
on-a
ttend
ance
irr
espe
ctiv
e of
how
sho
rt th
at
notic
e is
.
Low
er is
bet
ter.
Whi
lst t
he D
NA
rat
e re
mai
ns b
elow
targ
et, t
he tr
ust c
ontin
ues
to lo
ok fo
r so
lutio
ns to
impr
ove
- T
he
Tru
st is
cur
rent
ly r
evie
win
g el
ectr
onic
sol
utio
ns to
ass
ist i
n th
e m
anag
emen
t of t
his
and
the
asso
ciat
ed
prob
lem
s of
late
can
cella
tions
Can
celle
d O
ps
Can
celle
d E
lect
ive
Ope
ratio
ns
(with
in 2
4 ho
urs
of o
pera
tion)
-
% o
f Tot
al E
lect
ives
&
Day
case
s in
Mon
th
Dat
a re
port
ed is
in r
efer
ence
to c
ance
lled
emar
genc
y ca
ses
with
in 2
4hrs
. - O
n da
y ca
ncel
latio
ns o
f el
ectiv
e pa
tient
s is
45
at O
DG
H a
nd 1
3 at
SD
GH
.Is
sues
at S
DG
H a
re a
roun
d oc
cupa
ncy
on th
is s
ite a
nd e
lect
ive
adm
issi
ons
bein
g ca
ncel
led
due
to b
ed
pres
sure
s.A
t OD
GH
, the
issu
es a
re a
mix
of c
ance
llatio
ns w
ith 6
0% b
eing
due
to u
navo
idab
le c
linic
al r
easo
ns. 4
w
ere
due
to th
e ca
ncel
latio
n of
a li
st d
ue to
sur
geon
sic
knes
s. R
evie
w o
f can
cella
tions
due
to la
ck o
f th
eatr
e tim
e is
und
er r
evie
w a
nd is
gen
eral
ly a
s a
resu
lt of
the
late
sta
rt o
f afte
rnoo
n lis
ts.
KP
I for
can
celle
d el
ectiv
es b
eing
dev
elop
ed to
incl
ude
with
in IP
R
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 20
of 2
3
Page 103 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
E
ffici
ency
Ind
icat
or
Nam
e (C
olo
ur
- P
erf
| Tra
j)D
escr
ipti
on
Nar
rati
veM
on
th T
ren
d
The
atre
Util
isat
ion
- S
DG
H
The
pro
port
ion
of e
lect
ive
The
atre
slo
ts u
sed
over
the
tota
l ele
ctiv
e pl
anne
d ca
paci
ty
on th
e S
outh
port
site
.
Thi
s m
atrix
rep
orts
on
over
all t
heat
re u
tilis
atio
n at
SD
GH
incl
udin
g em
erge
ncy
and
trau
ma
lists
. -
Em
erge
ncy
and
trau
ma
list u
tilis
atio
n is
by
the
natu
re o
f the
term
var
iabl
e de
pend
ant o
n de
man
d.
Impr
ovem
ent o
f the
trau
ma
list c
ontin
ues
to b
e se
en w
ith th
e im
plem
enta
tion
of th
e go
ld a
nd s
ilver
pa
tient
pro
cess
intr
oduc
ed in
the
thea
tre
effic
ienc
y pr
ogra
mm
e. E
xclu
ding
trau
ma
and
emer
genc
y th
e th
eatr
e ut
ilisa
tion
is 6
8.37
%. T
his
was
impa
cted
with
13
on th
e da
y ca
ncel
latio
ns d
ue to
lack
of b
eds.
The
atre
Util
isat
ion
- O
DG
H
The
pro
port
ion
of e
lect
ive
The
atre
slo
ts u
sed
over
the
tota
l ele
ctiv
e pl
anne
d ca
paci
ty
on th
e O
rmsk
irk s
ite.
Slo
w im
prov
emen
t in
utili
satio
n w
hich
is c
urre
ntly
bei
ng im
pact
ed b
y on
day
can
cella
tions
. - T
heat
re
utili
satio
n w
as 7
3.06
%. T
his
was
impa
cted
by
45 o
n th
e da
y ca
ncel
latio
ns. F
ollo
win
g su
cces
sful
pilo
t of
the
48hr
pre
adm
issi
on c
alls
, the
se h
ave
now
com
men
ced
acro
ss a
ll sp
ecia
litie
s. C
ance
llatio
ns fo
r cl
inic
al r
easo
ns h
ave
incr
ease
d to
app
rox.
60%
, how
ever
, the
re is
a c
lear
impa
ct o
f lat
e ru
nnin
g af
tern
oon
lists
whi
ch is
und
er in
vest
igat
ion.
HB
S a
re o
fferin
g a
solu
tion
to th
e la
ck o
f ana
esth
etic
cov
er,
how
ever
sta
ff si
ckne
ss in
thea
tre
has
also
impa
cted
dur
ing
Oct
ober
.
Str
ande
d P
atie
nts
(>6
Day
s LO
S)
Pat
ient
s w
ho s
pend
7 d
ays
or
mor
e as
an
inpa
tient
.
Incr
ease
d no
ted
in s
tran
ded
in O
ctob
er -
The
SA
FE
R r
oll o
ut h
as b
een
revi
ewed
and
alth
ough
re
d2gr
een
com
plia
nce
has
impr
oved
it is
rec
ogni
sed
that
mor
e w
ork
is r
equi
red
to s
uppo
rt S
AF
ER
. S
OP
to s
uppo
rt r
ed2g
reen
boa
rd r
ound
s co
mpl
eted
and
pos
ter
deve
lope
d to
be
circ
ulat
ed;
red2
gree
n m
onito
ring
is im
prov
ing
and
wee
kly
audi
ts id
entif
y ar
eas
for
addi
tiona
l sup
port
. T
he d
evel
opm
ent o
f flo
w a
ctiv
ity r
epor
ts fo
r w
ards
is in
the
early
sta
ges
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 21
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 104 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
E
ffici
ency
Ind
icat
or
Nam
e (C
olo
ur
- P
erf
| Tra
j)D
escr
ipti
on
Nar
rati
veM
on
th T
ren
d
Sup
er S
tran
ded
Pat
ient
s (>
20 D
ays
LOS
)P
atie
nts
who
spe
nd 2
1 da
ys o
r m
ore
as a
n in
patie
nt.
incr
ease
in m
onth
con
tinue
s -
The
re r
emai
ns o
n-go
ing
wor
k w
ith #
long
stay
tues
day
with
the
com
mun
ity
and
LA a
t war
d le
vel a
nd c
ontin
ued
prog
ress
thro
ugh
the
Pat
ient
Flo
w Im
prov
emen
t pro
gram
me,
in
clud
ing
the
revi
ew o
f cur
rent
pro
cess
at w
ard
leve
l for
SA
FE
R,
enga
gem
ent e
vent
s w
ith M
DT
and
clin
icia
ns to
pro
mot
e S
AF
ER
, ac
ute
wor
king
to s
uppo
rt c
ompl
ex d
isch
arge
s in
to c
omm
unity
bed
s; r
elau
nch
of r
ed2g
reen
in
Nov
embe
r w
ith S
OP
to s
uppo
rt w
ards
; add
ition
al r
evie
ws
of s
tran
ded
patie
nts
to id
entif
y up
stre
am a
ny
com
plex
pat
ient
s
Sou
thpo
rt A
&E
Con
vers
ion
Rat
e
Pro
port
ion
of S
outh
port
A&
E
Atte
ndan
ces
that
are
mov
ed to
a
base
war
d. P
atie
nts
who
onl
y st
ay o
n an
Ass
essm
ent W
ard
are
not i
nclu
ded.
The
trus
t was
not
com
plia
nt in
Oct
ober
at 2
1.05
% -
The
Tru
st h
as w
orke
d ha
rd to
ens
ure
that
al
tern
ativ
e pa
thw
ays
to a
dmis
sion
whe
reve
r cl
inic
ally
app
ropr
iate
are
ado
pted
. Oct
ober
saw
an
addi
tiona
l 90
adm
issi
ons
via
ED
com
pare
d to
last
yea
r ag
ains
t an
incr
ease
of 4
18 a
ttend
ance
s.
Dem
and
for
side
roo
ms
durin
g O
ctob
er w
as h
igh
resu
lting
in p
atie
nts
adm
itted
str
aigh
t to
war
ds w
ithou
t go
ing
thro
ugh
asse
ssm
ent a
reas
. Thi
s w
as in
add
ition
to p
atie
nts
requ
iring
adm
issi
on to
ded
icat
ed
war
ds to
mee
t the
ir cl
inic
al n
eed
(par
ticul
arly
res
pira
tory
war
d fo
r N
IV, c
ardi
ac m
onito
ring
beds
on
SS
U
and
war
d 7A
). E
D c
ontin
ues
to h
ave
spec
ialty
in-r
each
into
ED
. Thi
s en
sure
s th
at p
atie
nts
iden
tifie
d as
re
quiri
ng a
bed
clin
ical
ly n
eed
adm
issi
on a
nd a
re n
ot s
uita
ble
for
alte
rnat
ive
path
way
s. T
he u
se o
f st
ream
ing
to C
DU
, SA
U a
nd A
CU
con
tinue
s. T
he m
odel
s ar
e in
line
with
bes
t pra
ctic
e an
d ha
ve b
een
desi
gned
in c
onju
nctio
n w
ith E
CIS
T (
natio
nal i
n-ho
use
NH
S e
xper
t con
sulta
ncy
for
UE
C).
Acr
oss
Oct
ober
, the
re w
as h
eavy
rel
ianc
e on
esc
alat
ion
bed
usag
e to
try
and
brid
ge th
e ga
p be
twee
n ad
mis
sion
s an
d di
scha
rges
, and
AC
U w
as u
sed
as a
n es
cala
tion
area
for
the
maj
ority
of t
he m
onth
, re
duci
ng o
ppor
tuni
ties
to m
axim
ise
stre
amin
g. A
s w
eeke
nds
are
a pa
rtic
ular
pre
ssur
e po
int,
AC
U h
as
open
ed o
n 3
Sun
days
str
eam
ing
a to
tal o
f 32
patie
nts
and
only
1 b
eing
adm
itted
. SA
U h
as p
rese
nted
a
mod
el to
red
esig
n th
e pa
thw
ay fo
r G
P r
efer
rals
and
are
look
ing
into
wee
kend
wor
king
, whi
ch w
ould
co
ntrib
ute
to r
educ
ing
the
conv
ersi
on r
ate
from
ED
.
Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 22
of 2
3
Page 105 of 210

Boa
rd R
epor
t - O
ctob
er 2
019
Pag
e 23
of 2
3
TB
204_
19 4
IPR
Det
ail D
ecem
ber
2019
Oct
ober
Dat
a
Page 106 of 210


Ind
icat
or
Nam
eO
cto
be
r2
01
8Se
pte
mb
er
20
19
Oct
ob
er 2
01
9Tr
end
Ove
rall
Tru
st
A&
E a
tte
nd
an
ce
s1
0,0
60
10,4
29
10,3
27
SD
GH
A&
E A
tte
nd
an
ce
s4
,43
74
,79
54
,87
7
OD
GH
A&
E A
tte
nd
an
ce
s2
,48
02
,48
02
,47
3
SD
GH
Fu
ll A
dm
issio
ns
Ac
tua
l978
1,0
03
1,0
78
Str
an
de
d P
ati
en
ts A
VG
175
168
179
Su
pe
r S
tra
nd
ed
Pa
tie
nts
AV
G65
65
69
MO
FD
Avg
Pa
tie
nts
Pe
r D
ay
65
64
73
GP
Re
ferr
als
(E
xc.2
WW
)3
,01
22
,13
12
,32
4
2 W
ee
k W
ait
Re
ferr
als
770
752
777
Ele
cti
ve
Ad
mis
sio
ns
232
181
197
Act
ivit
y Su
mm
ary –
Oct
ob
er2
01
9
TB
204_
19 5
IPR
Act
ivity
Sum
mar
y D
ec 1
9
Page 107 of 210

Ind
icat
or
Nam
eO
cto
ber
20
18
Sep
tem
ber
20
19
Oct
ob
er 2
01
9Tr
end
Ele
cti
ve
Ca
nc
ell
ati
on
s38
20
24
Da
y c
as
e A
dm
issio
ns
1,9
35
1,9
44
1,8
90
Da
y C
ase
Can
ce
lla
tio
ns
50
51
45
To
tal C
an
cell
ati
on
s(o
n t
he d
ay)
15
40
Ou
tpa
tie
nts
Se
en
23,0
44
22,4
81
22,5
20
Ou
tpa
tie
nts
Ca
nc
ell
ati
on
s4
,28
64
,23
54
,05
0
Th
ea
tre
Ca
se
s678
637
617
Ge
ne
ral &
Ac
ute
Be
ds
Avg
. P
er
Da
y378
404
404
Es
ca
lati
on
Be
ds
Avg
. P
er
Da
y11
26
In H
osp
ita
l D
eath
s58
63
74
Act
ivit
y Su
mm
ary –
Oct
ob
er 2
01
9
Page 108 of 210

PUBLIC TRUST BOARD 4 December 2019
Agenda Item TB205/19 Report
Title
Director of Finance Report – Month 7
2019/20
Executive Lead Steve Shanahan, Director of Finance
Lead Officer Kevin Walsh, Deputy Director of Finance
Action Required
(Definitions below)
To Approve To Note
To Assure To Receive
For Information
Executive Summary
In the latest System Financial Recovery Plan the Trust is forecasting a year end overspend of £3.6
million against the deficit plan of £26.6 million (excluding PSF/FRF), after achieving the plan at the
end of Quarter 2 with non- recurrent assistance thus securing £3.654 million PSF/FRF funding.
The Month 7 financial plan was not achieved with expenditure higher than the trajectory allowed to
achieve the forecast outturn. The main reasons for this are; pay spend with both monthly agency
and bank levels at their highest levels; CIP delivery to date and a forecast gap at the end of the year
of £2.0 million (previous month was £1.7 million).
The overall System financial position is forecasting an over spend of £24.53 million against the
£25.6 million deficit control total (excluding PSF/FRF)
The Board is asked to receive the Finance Report – Month 7 2019/20.
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
Strategic Objective Principal Risk
SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
SO5 Enable all staff to be patient-centred leaders building
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
TB
205_
19 F
inan
ce R
epor
t Mon
th 7
Dec
19
Page 109 of 210

on an open and honest culture and the delivery of the Trust values
SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
If the system does not have an agreed acute services strategy it may lead to non-alignment of partner organisations plans resulting in the inability to develop and deliver sustainable services
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
Caring Statutory Requirement
Effective Annual Business Plan Priority
Responsive Best Practice
Safe Service Change
Well Led
Impact (is there an impact arising from the report on any of the following?)
Compliance Legal
Engagement and Communication Quality & Safety
Equality Risk
Finance Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Committee)
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
Page 110 of 210

Director of Finance Report – Month 7 2019/20
1. Purpose
1.1. This report provides the Board with the financial position for Month 7 (October 2019) and the
progress on delivery of the Trust’s control total.
1.2. It also provides an update on the Trusts’ forecast outturn alongside the overall System
position.
1.3. The Trust signed up to its 2019/20 deficit control total of £8.296 million (£26.567 million deficit
before non-recurrent funding of £18.271 million).
1.4. The non-recurrent funding consists of Provider Sustainability Funding (PSF) of £3.464 million
and Financial Recovery Fund (FRF) of £14.807 million.
2. Executive Summary
2.1. The month 7 (YTD) position is a deficit after PSF/FRF of £8.106 million against a plan of
£7.235 million resulting in £869,000 worse than plan. Before PSF/FRF the YTD deficit is
£16.328 million.
2.2. The month 7 (in month) positon is a deficit after PSF/FRF of £0.545 million against a surplus
plan of £0.315 million resulting in £0.861 million worse than plan. Before PSF/FRF the in-
month deficit is £2.372 million.
2.3. The Trust’s forecast outturn, based on month 6 performance and shared with NHSI/E on 1
November 2019, is £3.6 million overspend against the deficit plan.
2.4. Month 7 expenditure is higher than the trajectory used to achieve this forecast outturn.
2.5. The 2019/20 CIP programme is £1,350,000 behind plan at month 7; the forecast outturn is
£4.3 million against the £6.3 million plan leaving an unidentified gap of £2.0 million.
2.6. If material cash reducing CIP schemes cannot be transacted during the remainder of the year
then any pressure on the expenditure run rate will not be mitigated.
2.7. The table below is the I&E statement for October:
TB
205_
19 F
inan
ce R
epor
t Mon
th 7
Dec
19
Page 111 of 210

ANNUAL
I&E (Including R&D) Budget
£000
Budget
£000
Actual
£000
Variance
£000
Budget
£000 Actual £000
Variance
£000
Commissioning Income 165,513 97,340 97,208 (131) 14,463 14,279 (184)
PP, Overseas & RTA 1,094 640 453 (187) 92 53 (39)
Other Income 12,174 7,271 7,662 391 1,030 1,026 (3)
PSF & FRF 18,271 8,222 8,222 0 1,827 1,827 0
Total Operating Income 197,052 113,473 113,545 72 17,411 17,185 (226)
PAY (140,012) (82,273) (82,544) (271) (11,610) (11,961) (351)
NON PAY (53,220) (31,355) (32,032) (677) (4,453) (4,775) (322)
Total Operating Expenditure (193,232) (113,628) (114,577) (948) (16,064) (16,735) (673)
EBITDA 3,820 (155) (1,032) (876) 1,348 450 (899)
Net Financing Costs (12,149) (7,109) (7,112) (3) (1,019) (999) 20
Retained Surplus/Deficit (8,329) (7,264) (8,144) (879) 329 (549) (879)
Technical Adjustments 33 28 38 10 (14) 4 18
Break Even Surplus/(Deficit) (8,296) (7,235) (8,106) (869) 315 (545) (861)
Less PSF/FRF Funding (18,271) (8,222) (8,222) 0 (1,827) (1,827) 0
SURPLUS/(DEFICIT)
excluding PSF/FRF (26,567) (15,457) (16,328) (869) (1,512) (2,372) (861)
YEAR TO DATE IN MONTH
2.8. The YTD deficit in the above table (£16.328 million) equates to a monthly average of £2.3
million.
2.9. As previously highlighted a number of non recurrent items were actioned in Quarters 1 and 2.
2.10. It is estimated that the current underlying deficit remains in the region of £2.7 million per month
excluding PSF/FRF which is an underlying annualised deficit of £32.0 million.
3. 2019/20 Contract Position
3.1. The value of the Southport & Formby CCG contract is £74.9 million.
3.2. The contract is a “Cost based contract” which has a number of “conditional income” elements.
3.3. These conditional elements, and performance to date, are shown in the table below:
Annual M7 YTD M7 YTD M7 YTD
Plan Plan Actual Var
£ £ £ £
Repatriation 600,000 350,000 0 (350,000)
Business Cases 1,300,000 758,333 402,027 (356,306)
CQC Contingency 300,000 175,000 7,200 (167,800)
BPT 850,000 495,833 23,732 (472,101)
Contingency - Other Conditional 450,000 262,500 0 (262,500)
Total 3,500,000 2,041,667 432,959 (1,608,707)
3.4. The Trust is assuming that it will achieve the £3.5 million at the year end and, therefore, is
accruing the full £2.041 million in the above table in the month 7 YTD position.
3.5. An additional £200,000 has been accrued in the month 7 YTD position (current expected year
Page 112 of 210

end contract over performance of £1.1 million results in a contract payment of £76.0 million).
This is based on expected year end contract performance and is reviewed monthly.
3.6. Latest projections indicate that if Southport & Formby CCG was on a PbR contract value the
year end projection is in the region of £78.8 million.
3.7. Apart from the Sefton CCGs, all other CCG contracts are on a PbR type contract.
3.8. The commissioning income annual budget in the above table includes:-
• £51.0 million for West Lancashire CCG; based on month 7 activity performance, and
planned recovery of the elective plan, this is forecast to be achieved.
• £74.9 million for Southport & Formby CCG; the Trust is currently underperforming against
the conditional elements of the contract but the contract is expected to overachieve.
4. Income
4.1. Elective activity performance has been improving over the last few months. It should be noted
that this improvement has had an adverse impact on outpatient activity as cancelled elective
sessions were previously replaced with outpatient work.
4.2. Non elective activity has once again overperformed in month.
4.3. Trust activity and income performance at month 7 YTD is as follows:
• Elective – activity is 3.9% below plan; £435,000 loss of income.
• A&E – activity 5.5% above plan; £353,000 of additional income.
• Non Elective – activity is 2.4% below plan; £2,567,000 additional income due to case mix
• Outpatients – activity is 3.9% above plan; £627,000 of additional income
4.4. Not all of the above activity performance is payable in 2019/20 due to:
• the application of the “blended tariff” adjustment means that only a proportion of the non-
elective value is payable
• Sefton CCG’s contract applies the “blended tariff” to all points of delivery.
4.5. The Trust’s commissioning income for month 7 YTD position assumes the following:
• Southport & Formby CCG will overperform against the contract at the year end (full year
contract value is £74.9 million; overperformance of £1.1 million).
• £200,000 of this overperformance was bought into the month 6 income position and this
has also been accrued at month 7.
• All other commissioning income is paid in line with the agreed contract.
5. Expenditure
5.1. Please refer to attached appendices for more detailed information regarding expenditure and
Whole Time Equivalent (WTE).
5.2. Underlying expenditure levels over the last few months have been fairly consistent but have
increased in month 7.
TB
205_
19 F
inan
ce R
epor
t Mon
th 7
Dec
19
Page 113 of 210

5.3. The Board will recall that a number of non-recurrent expenditure reductions were applied in
month 3 in order to achieve the Quarter 1 control total.
5.4. No reductions were applied in months 4 and 5 but in month 6 a number of further adjustments
(mostly non-recurrent) were made which contributed to the achievement of the Quarter 2
control total.
5.5. In month 7 no adjustments have been made and this has contributed to a deteriorating
performance.
5.6. The most material increase in expenditure is within nursing staff with October 2019 seeing the
largest monthly nurse expenditure and WTE date. Although the substantive WTE has seen a
welcome increase this month (from 1,102 to 1,121 WTE) both bank and agency have also
increased.
5.7. It is important that substantive staff increase and vacancies reduce from both a quality and
finance perspective. Whilst bank is financially preferable to agency staff it is apparent that the
premium associated with bank is also significant as the majority of shifts covered are evenings
and weekends.
5.8. Further review of this will take place alongside the 2020/21 budget process.
5.9. Non pay areas have also seen a slight increase with some of this attributable to the additional
elective work now taking place.
6. Bank/agency spend
6.1. The Trust spent £2.052 million in October on bank and agency staff.
6.2. Monthly agency spend has increased in October to £1,109,000 (9.3% of the pay bill); Medical
staff £511,000; Nursing staff £458,000
6.3. Month 7 YTD agency spend is £6.978 million (8.4% of the pay bill); Medical staff £3.717
million; Nursing staff £2.619 million
6.4. The agency target cap of £4.891 million set by NHSI for 2019/20 was breached in month 6.
6.5. Bank spend is consistent with previous months; October is £944,000 (8.3% of the total pay bill)
bringing YTD spend to £6.533 million (7.9% of the total pay bill).
6.6. As referred to above both bank and agency attract a considerable premium element and is a
key area of focus for the Trust to improve its financial position.
7. Cost Improvement Plan (CIP)
7.1. The Trust’s I&E plan assumes a £6.3 million CIP is delivered in 2019/20 from both increased
income and reduced expenditure.
7.2. Following contract discussions the plan is mainly dependent on expenditure reduction.
7.3. The table below illustrates the targets with performance to date.
19/20 Plan - Expenditure (pay) 2,465 3,965 355 118 (237) 2,094 959 (1,135) 1,377 1,015
19/20 Plan - Expenditure (non pay) 1,724 1,724 160 83 (77) 910 737 (173) 1,143 996
19/20 Plan - Income (other op income) 325 325 39 25 (14) 128 242 114 343 66
19/20 Plan - Income (BPT) 1,800 300 26 (26) 156 (156)
19/20 Plan - Total 6,314 6,314 580 226 (354) 3,288 1,938 (1,350) 2,863 2,077
Annual
Plan
£000
Annual
Budget
£000
Month 6 YTD
CYE
£000
FYE
£000
Budget
£000
Actual
£000
Var
£000
Budget
£000
Actual
£000
Var
£000
Page 114 of 210

7.4. The forecast outturn against the £6.314 million target has reduced to is £4.359 million leaving
an unidentified gap of £1.955 million.
8. Forecast Outturn
8.1. The Trust has been signalling that it will not achieve its financial plan based on current
financial performance.
8.2. Despite the achievement of the Quarter 2 plan a large element of the income and expenditure
adjustments will impact in Quarter 4.
8.3. The Trust’s expenditure levels in the first half of the year, together with assumptions on CIP
delivery and future impact of agreed business cases, derived a predicted £5.1 million
overspend against the plan.
8.4. This was included in the System Recovery plan submitted to NHSI/E on 18th October 2019
and discussed at this Board’s October meeting.
8.5. Following review the System was instructed to find further schemes to reduce the forecast gap
from control totals.
8.6. The Trust has identified a further improvement of £1.49 million and is now predicting an
overspend of £3.61 million against the £26.6 million deficit plan. NHSI/E is monitoring the
Trust’s performance against this forecast on a weekly basis.
8.7. The table below shows the control total and current forecast for all System partners:
S&O
NHST
SS CCG SF CCG Winter Total
£m £m £m £m £m
2019/20 Control Total (excl PSF/FRF) (26.60) 1.00 0.00 0.00 (25.60)
Winter 0.00 0.00 0.00 (1.10) (1.10)
Forecast overspend (3.61) (9.12) (10.70) 0.00 (23.43)
Forecast Outturn (excl PSF/FRF) (30.21) (8.12) (10.70) (1.10) (50.13)
8.8. Month 7 expenditure levels were in the region of £0.2 million above the Trust’s trajectory to
achieve £3.61 million adverse against plan.
8.9. The pressure on the expenditure run rate as vacancies are filled (including agreed business
cases) is not being mitigated by real expenditure reductions form the CIP programme.
8.10. Based on current expenditure levels and CIP performance it is highly likely that the Trust will
not achieve the Quarter 3 deficit plan without significant CCG support and, therefore, will not
be in receipt of the PSF/FRF for that quarter (£5.481 million).
9. Cash
9.1. The previous large cash balance (October’s opening balance was £7 million) has now been
fully utilised with November closing cash balance £1.1million which is in line with the terms
and conditions of our revenue support loans..
9.2. Performance against the cash plan in October 2019 was on target overall, however, cash
outflows needed controlling to ensure the target was met.
TB
205_
19 F
inan
ce R
epor
t Mon
th 7
Dec
19
Page 115 of 210

9.3. Quarter 2 FRF funding of £2.961 million was received on 15th November 2019; it was not
forecast to be received until December 2019.
9.4. The uncertainty of timing around PSF and FRF funding has made forecasting a challenge
9.5. The Trust is not achieving the Better Payment Practice Code (BPPC) target, however, a focus
on delivering the e-invoicing target will help with both the BPPC and reduce the risk of
additional contractual penalty charges by NHS Shared Business Services.
10. Debtors
10.1. Debt levels have increased from £3.8 million at the end of September 2019 to £4.9 million at
the end of October 2019.
10.2. Greater than 90 day debt has increased from £1,466,998 last month to £2,021,405 this month.
10.3. The majority of this increase is in NHS debt and is linked mostly to a revoked credit note to
NHS England for -£364,000.
10.4. There has been some increase in non NHS debt and this is entirely due to Local Authority
invoices (Lancashire County Council) which are on SBS (Shared Business Services) dunning
levels.
10.5. A monthly debt management call takes place with SBS and this includes a review of the top 10
debtors (NHS and non-NHS) over 31 days and by dunning responsibility.
10.6. The majority of >90 day debt is NHS related (as per table above) and it can be difficult to
chase as this debt can’t be referred to external debt recovery.
11. Capital
11.1. Actual spend in month 7 was higher than month 6, at £535,000 bringing the cumulative actual
spend to date to £2,098,000 against a planned spend year to date of £4,027,000.
11.2. The low spend is more a reflection of an optimistic plan that schemes such as the ward
upgrades and library extension would have progressed further by this point in the year.
11.3. Commitments have increased in the month to £1,137,000, partly IT, but mainly Medical
Equipment on order which has recently been approved at Capital Investment Group (CIG).
11.4. Medical Equipment has the highest level of commitments, closely followed by IT which is
mostly connected with the Windows 10 rollout and Careflow Connect.
11.5. Taking actual and committed spend together at £3,087,000 (excluding donated and GE
radiology assets) and comparing this against the annual plan, £5,103,000, then the Trust is at
60.5% of the plan at the end of October 2019.
11.6. The first 5 wards of the Southport ward upgrade project will be completed before Christmas
with a 6th planned for completion before the end of the financial year.
11.7. Work is near completion in the Spinal Injuries Unit on the Isolation work and the bathroom
upgrades which were required as a result of the Klebsiella outbreak.
11.8. IM&T contingency scheme at £450,000 was originally intended for the datacentre, however,
this is unlikely to be implemented in 2019/20 and a re-utilisation of these monies to other IT
projects planned for next year is reflected in the revised plan.
11.9. The Trust has been successful in receiving £700,000 funding for ePMA (Electronic Prescribing
Page 116 of 210

and Medicines Administration) system.
11.10. NHSE/I has supported the Trust to apply for a capital loan of £935,000 to address the high risk
items identified in the six facet survey. This could be received in 2019/20.
11.11. The Board approved a revised capital plan on 6th November and included the authorisation to
proceed with the development of additional bed capacity at Ormskirk hospital as part of the
winter plan at a forecast cost of £350,000.
11.12. However, the full cost of these works is now £495,000 which includes backlog maintenance.
11.13. Under the new scheme of delegation Finance Performance and Investment Committee
approved the additional cost of the scheme.
11.14. This week confirmation was received that capital funding for winter planning of £500,000 had
been awarded; the relevant paperwork is awaited (Memorandum of Understanding) and once
signed off an application will be made to draw down public dividend capital.
11.15. Based on current information the MRI scanner project is back on track in and this scheme will
be delivered by the end of March 2020 as originally planned.
12. Recommendations
12.1. The Board is asked to receive the Finance Report – Month 7 2019/20.
TB
205_
19 F
inan
ce R
epor
t Mon
th 7
Dec
19
Page 117 of 210


Lis
t o
f A
pp
en
dic
es
1
. A
cti
vit
y r
un
ra
te b
y m
on
th
2.
Sta
tem
en
t o
f C
om
pre
he
ns
ive
In
co
me
(In
co
me
& E
xp
en
dit
ure
Acc
ou
nt)
3.
Ex
pe
nd
itu
re r
un
ra
te b
y m
on
th
4.
WT
E r
un
ra
te b
y m
on
th
5.
Sta
tem
en
t o
f F
ina
nc
ial
Po
sit
ion
(B
ala
nce
Sh
ee
t)
6.
Ca
pit
al
Ex
pe
nd
itu
re
7.
Ca
sh
flo
w F
ore
ca
st
TB
205_
19 F
inan
ce M
onth
7 R
epor
t App
endi
ces
Page 118 of 210

1.
Ac
tiv
ity
ru
n r
ate
by
mo
nth
Mo
nth
M
on
th
Mo
nth
M
on
th
Mo
nth
M
on
th
Mo
nth
M
on
th
Mo
nth
M
on
th
Mo
nth
M
on
thM
on
th
78
910
1112
12
34
56
7
Aan
dE
7,30
9
7,
328
6,89
6
7,
269
6,75
6
7,
595
7,17
6
7,
446
7,16
2
7,
783
7,22
4
7,
393
7,47
1
Day
Cas
e1,
906
1,98
4
1,
444
1,87
8
1,
731
1,85
4
1,
707
1,70
6
1,
605
1,81
5
1,
801
1,82
5
1,
849
Ele
ctiv
e21
2
18
9
13
8
18
0
17
5
17
9
14
4
18
7
18
3
17
7
17
5
15
3
19
4
No
n E
lect
ive
(In
clu
din
g Sh
ort
Sta
y)2,
654
2,67
9
2,
644
2,74
1
2,
480
2,64
6
2,
368
2,50
5
2,
340
2,66
2
2,
707
2,55
9
2,
781
No
n E
lect
ive
No
n E
me
rge
ncy
239
233
285
241
254
262
75
78
60
76
62
69
73
Ou
tpat
ien
ts (
Incl
ud
ing
Pro
ced
ure
s)16
,515
15,8
71
12
,855
14,9
26
14
,462
15,3
02
15
,075
15,6
15
14
,366
16,7
78
14
,066
15,2
28
15
,881
2019
/20
2018
/20
Page 119 of 210

2.
Sta
tem
en
t o
f C
om
pre
he
ns
ive
In
co
me
(In
co
me
& E
xp
en
dit
ure
Acc
ou
nt)
AN
NU
AL
I&E
(In
clu
din
g R
&D
) B
ud
get
£000
Bu
dge
t
£000
Act
ual
£000
Var
ian
ce
£000
Bu
dge
t
£000
A
ctu
al £
000
V
aria
nce
£000
Co
mm
issi
on
ing
Inco
me
165,
513
97,3
4097
,208
(131
)14
,463
14,2
79(1
84)
PP
, Ove
rse
as &
RTA
1,09
464
045
3(1
87)
9253
(39)
Oth
er
Inco
me
12,1
747,
271
7,66
239
11,
030
1,02
6(3
)
PSF
& F
RF
18,2
718,
222
8,22
20
1,82
71,
827
0
Tota
l Op
era
tin
g In
com
e19
7,05
211
3,47
311
3,54
572
17,4
1117
,185
(226
)
PA
Y(1
40,0
12)
(82,
273)
(82,
544)
(271
)(1
1,61
0)(1
1,96
1)(3
51)
NO
N P
AY
(53,
220)
(31,
355)
(32,
032)
(677
)(4
,453
)(4
,775
)(3
22)
Tota
l Op
era
tin
g Ex
pe
nd
itu
re(1
93,2
32)
(113
,628
)(1
14,5
77)
(948
)(1
6,06
4)(1
6,73
5)(6
73)
EBIT
DA
3,82
0(1
55)
(1,0
32)
(876
)1,
348
450
(899
)
Ne
t Fi
nan
cin
g C
ost
s(1
2,14
9)(7
,109
)(7
,112
)(3
)(1
,019
)(9
99)
20
Re
tain
ed
Su
rplu
s/D
efi
cit
(8,3
29)
(7,2
64)
(8,1
44)
(879
)32
9(5
49)
(879
)
Tech
nic
al A
dju
stm
en
ts33
2838
10(1
4)4
18
Bre
ak E
ven
Su
rplu
s/(D
efi
cit)
(8,2
96)
(7,2
35)
(8,1
06)
(869
)31
5(5
45)
(861
)
Less
PSF
/FR
F Fu
nd
ing
(18,
271)
(8,2
22)
(8,2
22)
0(1
,827
)(1
,827
)0
SUR
PLU
S/(D
EFIC
IT)
exc
lud
ing
PSF
/FR
F(2
6,56
7)(1
5,45
7)(1
6,32
8)(8
69)
(1,5
12)
(2,3
72)
(861
)
YEA
R T
O D
ATE
IN M
ON
TH
TB
205_
19 F
inan
ce M
onth
7 R
epor
t App
endi
ces
Page 120 of 210

3.
Ex
pe
nd
itu
re r
un
ra
te b
y m
on
th
RU
N R
AT
E M
on
th o
n M
on
th -
£(0
00
)A
s a
t 3
1st
Octo
be
r 2
01
9
Cla
ss
ST
AF
F G
RO
UP
ST
AF
F T
YP
EO
ct-
18
No
v-1
8D
ec-1
8Ja
n-1
9F
eb
-19
Ma
r-1
9A
pr-
19
Ma
y-1
9Ju
n-1
9Ju
l-1
9A
ug
-19
Se
p-1
9O
ct-
19
PA
YC
on
su
lta
nts
Su
bsta
nti
ve
(1,3
19
)(1
,29
9)
(1,3
19
)(1
,39
5)
(1,3
24
)(1
,11
8)
(1,2
38
)(1
,23
9)
(1,2
34
)(1
,32
1)
(1,2
35
)(1
,39
6)
(1,2
82
)
Ba
nk
(50
)(4
0)
(70
)(1
01
)(7
8)
(10
4)
(98
)(7
0)
(65
)(1
12
)(6
5)
(75
)(8
4)
Ag
en
cy
(11
0)
(15
4)
(18
7)
(17
9)
(20
6)
(27
2)
(27
9)
(27
9)
(20
1)
(27
5)
(26
6)
(34
1)
(26
4)
Co
nsu
lta
nts
To
tal
(1,4
79
)(1
,49
4)
(1,5
77
)(1
,67
5)
(1,6
08
)(1
,49
4)
(1,6
15
)(1
,58
7)
(1,5
00
)(1
,70
8)
(1,5
66
)(1
,81
2)
(1,6
30
)
Oth
er
Me
dic
al
Su
bsta
nti
ve
(1,2
43
)(1
,20
2)
(1,2
63
)(1
,31
9)
(1,3
07
)(1
,25
6)
(1,3
37
)(1
,30
5)
(1,3
27
)(1
,29
7)
(1,3
13
)(1
,43
1)
(1,3
28
)
Ba
nk
(12
9)
(16
3)
(14
2)
(13
7)
(11
5)
(16
7)
(16
5)
(16
7)
(19
5)
(15
5)
(17
4)
(17
1)
(14
6)
Ag
en
cy
(22
6)
(21
7)
(20
8)
(24
4)
(27
3)
(31
6)
(25
6)
(25
7)
(27
7)
(28
8)
(25
5)
(23
5)
(24
7)
Oth
er
Me
dic
al
To
tal
(1,5
97
)(1
,58
1)
(1,6
12
)(1
,69
9)
(1,6
95
)(1
,73
9)
(1,7
58
)(1
,73
0)
(1,7
99
)(1
,74
0)
(1,7
42
)(1
,83
7)
(1,7
22
)
Nu
rse
s &
Mid
wiv
es
Su
bsta
nti
ve
(3,6
28
)(3
,60
4)
(3,5
71
)(3
,70
4)
(3,6
72
)(3
,38
8)
(3,9
54
)(3
,81
8)
(3,7
97
)(3
,74
5)
(3,7
22
)(3
,77
1)
(3,7
49
)
Ba
nk
(52
9)
(56
5)
(54
3)
(59
5)
(58
8)
(68
4)
(60
9)
(63
7)
(64
5)
(63
2)
(67
1)
(65
6)
(68
4)
Ag
en
cy
(36
7)
(29
4)
(26
2)
(42
7)
(41
5)
(43
6)
(37
2)
(39
7)
(31
9)
(30
3)
(40
0)
(37
0)
(45
8)
Nu
rse
s &
Mid
wiv
es T
ota
l(4
,52
4)
(4,4
63
)(4
,37
5)
(4,7
26
)(4
,67
5)
(4,5
08
)(4
,93
5)
(4,8
52
)(4
,76
1)
(4,6
80
)(4
,79
3)
(4,7
96
)(4
,89
1)
Scie
nti
fic,
Te
ch
nic
al
&
Th
era
pu
tic
Su
bsta
nti
ve
(1,3
31
)(1
,33
0)
(1,3
07
)(1
,32
0)
(1,3
19
)(1
,26
0)
(1,4
37
)(1
,34
9)
(1,3
29
)(1
,32
3)
(1,3
48
)(1
,37
2)
(1,3
84
)
Ba
nk
(11
)(1
3)
(12
)(9
)(1
2)
(12
)(7
)(7
)(7
)(8
)(6
)(5
)(5
)
Ag
en
cy
(16
)(2
0)
(15
)(1
2)
(8)
(14
)(4
)(8
)(2
0)
(35
)(2
6)
(72
)(2
8)
Scie
nti
fic,
Te
ch
nic
al
& T
he
rap
uti
c T
ota
l(1
,35
8)
(1,3
63
)(1
,33
4)
(1,3
41
)(1
,33
9)
(1,2
86
)(1
,44
8)
(1,3
64
)(1
,35
5)
(1,3
66
)(1
,38
0)
(1,4
49
)(1
,41
7)
Oth
er
Sta
ffS
ub
sta
nti
ve
(2,0
10
)(2
,04
0)
(1,9
81
)(1
,96
5)
(2,0
08
)(1
,73
1)
(2,2
84
)(2
,15
6)
(2,1
47
)(2
,09
0)
(2,1
15
)(2
,15
0)
(2,1
20
)
Ba
nk
(31
)(7
)(2
8)
(27
)(1
9)
(34
)(3
8)
(17
)(2
7)
(34
)(4
0)
(28
)(2
4)
Ag
en
cy
(63
)(5
1)
(58
)(5
9)
(50
)(5
4)
(59
)(5
4)
(48
)(6
4)
(78
)(3
4)
(11
2)
Oth
er
Sta
ff T
ota
l(2
,10
5)
(2,0
98
)(2
,06
7)
(2,0
51
)(2
,07
7)
(1,8
18
)(2
,38
1)
(2,2
27
)(2
,22
3)
(2,1
88
)(2
,23
2)
(2,2
13
)(2
,25
6)
Pa
y R
ese
rve
sS
ub
sta
nti
ve
0
35
1
84
2
32
7
98
(1
76
)(5
7)
(56
)1
49
(1
91
)(5
4)
91
4
(0)
Pa
y R
ese
rve
s T
ota
l0
3
5
18
4
23
2
79
8
(17
6)
(57
)(5
6)
14
9
(19
1)
(54
)9
14
(0
)
Pa
y C
IPS
ub
sta
nti
ve
0
0
0
0
0
0
0
0
0
0
0
0
0
Pa
y C
IP T
ota
l0
0
0
0
0
0
0
0
0
0
0
0
0
Ap
pre
nti
ce
sh
ip L
ev
yS
ub
sta
nti
ve
(39
)(4
4)
(39
)(4
1)
(40
)(4
7)
(44
)(4
2)
(38
)(5
0)
(36
)(4
3)
(46
)
Ap
pre
nti
ce
sh
ip L
ev
y T
ota
l(3
9)
(44
)(3
9)
(41
)(4
0)
(47
)(4
4)
(42
)(3
8)
(50
)(3
6)
(43
)(4
6)
PA
Y T
ota
l(1
1,1
02
)(1
1,0
08
)(1
0,8
20
)(1
1,3
01
)(1
0,6
36
)(1
1,0
68
)(1
2,2
39
)(1
1,8
57
)(1
1,5
27
)(1
1,9
24
)(1
1,8
03
)(1
1,2
35
)(1
1,9
61
)
NO
N-P
AY
Su
pp
lie
s &
Se
rvic
es C
lin
ica
l(2
,31
7)
(2,2
90
)(2
,22
8)
(2,2
49
)(2
,22
7)
(2,4
13
)(2
,26
3)
(2,3
25
)(2
,25
9)
(2,4
20
)(2
,26
4)
(2,2
27
)(2
,38
2)
Su
pp
lie
s &
Se
rvic
es G
en
era
l(2
04
)(2
14
)(2
00
)(2
03
)(1
99
)(2
12
)(1
86
)(1
72
)(1
73
)(1
64
)(1
89
)(2
19
)(2
11
)
No
n-E
xe
cu
tiv
e D
ire
cto
rs(6
)(6
)(6
)(8
)(4
)(6
)(6
)
Esta
bli
sh
me
nt
Ex
pe
nse
s(2
88
)(3
52
)(2
95
)(2
98
)(2
92
)(2
68
)(1
91
)(2
26
)(2
32
)(2
21
)(2
45
)(2
42
)(2
37
)
Pre
mis
es &
Fix
ed
Pla
nt
(99
0)
(94
3)
(99
3)
(95
3)
(91
7)
(77
5)
(1,0
18
)(1
,03
5)
(99
1)
(98
5)
(1,0
55
)(9
48
)(1
,06
1)
Mis
ce
lla
ne
ou
s(6
16
)(6
32
)(6
59
)(6
38
)(6
54
)(5
95
)(7
17
)(7
20
)(7
16
)(7
35
)(7
17
)(6
66
)(7
40
)
Se
rvic
es F
rom
Oth
er
NH
S B
od
ies
(27
9)
(29
3)
(20
9)
(28
7)
(25
3)
(32
8)
(10
3)
(61
)(6
9)
(14
5)
(18
8)
(13
6)
(13
7)
No
n P
ay
Re
se
rve
0
0
0
0
0
0
(7)
7
0
0
0
0
0
No
n P
ay
CIP
0
0
0
0
0
0
0
0
0
0
0
0
0
NO
N-P
AY
To
tal
(4,6
95
)(4
,72
5)
(4,5
83
)(4
,62
8)
(4,5
43
)(4
,59
0)
(4,4
91
)(4
,53
8)
(4,4
46
)(4
,67
8)
(4,6
62
)(4
,44
3)
(4,7
75
)
NO
N-O
PE
RA
TIN
G E
XP
EN
DIT
UR
E(9
20
)(9
39
)(9
42
)(9
39
)(9
40
)(4
79
)(1
,03
1)
(1,0
23
)(1
,03
7)
(1,0
06
)(1
,04
2)
(1,0
16
)(9
98
)
Gra
nd
To
tal
(16
,71
7)
(16
,67
2)
(16
,34
6)
(16
,86
8)
(16
,11
9)
(16
,13
7)
(17
,76
1)
(17
,41
8)
(17
,00
9)
(17
,60
8)
(17
,50
6)
(16
,69
4)
(17
,73
3)
PA
Y S
UM
MA
RY
BY
ST
AF
F T
YP
E
PA
YS
ub
sta
nti
ve
(9,5
70
)(9
,48
5)
(9,2
96
)(9
,51
1)
(8,8
71
)(8
,97
5)
(10
,35
1)
(9,9
64
)(9
,72
3)
(10
,01
6)
(9,8
22
)(9
,24
8)
(9,9
08
)
Ba
nk
(74
9)
(78
8)
(79
5)
(86
9)
(81
3)
(1,0
01
)(9
18
)(8
98
)(9
40
)(9
42
)(9
56
)(9
36
)(9
44
)
Ag
en
cy
(78
2)
(73
5)
(73
0)
(92
0)
(95
2)
(1,0
92
)(9
70
)(9
95
)(8
64
)(9
66
)(1
,02
4)
(1,0
50
)(1
,10
9)
PA
Y T
ota
l(1
1,1
02
)(1
1,0
08
)(1
0,8
20
)(1
1,3
01
)(1
0,6
36
)(1
1,0
68
)(1
2,2
39
)(1
1,8
57
)(1
1,5
27
)(1
1,9
24
)(1
1,8
03
)(1
1,2
35
)(1
1,9
61
)
Page 121 of 210

4.
WT
E r
un
ra
te b
y m
on
th
WTE
wo
rke
dA
s at
31s
t O
cto
be
r 20
19
STA
FF G
RO
UP
STA
FF T
YP
EO
ct-1
8N
ov-
18D
ec-
18Ja
n-1
9Fe
b-1
9M
ar-1
9A
pr-
19M
ay-1
9Ju
n-1
9Ju
l-19
Au
g-19
Sep
-19
Oct
-19
Co
nsu
ltan
tsSu
bst
anti
ve
100
103
102
9
4
9
9
9
7
9
6
9
5
9
4
9
4
9
5
9
5
9
5
Ban
k
2
2
4
4
5
5
5
5
3
5
3
3
4
Age
ncy
25
8
9
8
10
12
12
12
9
12
12
13
14
Co
nsu
ltan
ts T
ota
l
127
114
115
107
114
114
114
111
106
111
110
111
113
Oth
er
Me
dic
alSu
bst
anti
ve
207
207
215
218
224
225
225
226
217
228
225
217
216
Ban
k
1
0
1
1
1
0
1
0
1
0
1
1
1
3
1
1
9
1
2
1
2
9
1
2
Age
ncy
65
19
18
21
24
28
20
23
24
22
20
20
21
Oth
er
Me
dic
al T
ota
l
281
236
242
249
258
264
258
260
250
263
257
246
249
Nu
rse
s &
Mid
wiv
es
Sub
stan
tive
1,0
97
1,1
01
1,0
98
1,0
94
1,1
01
1,1
10
1,1
06
1,1
21
1,1
10
1,1
09
1,1
07
1,1
02
1,1
21
Ban
k
161
171
161
172
176
208
178
185
186
189
196
187
197
Age
ncy
48
44
42
62
59
69
63
60
54
57
66
65
75
Nu
rse
s &
Mid
wiv
es
Tota
l
1
,305
1
,315
1
,302
1
,329
1
,336
1
,387
1
,347
1
,367
1
,350
1
,355
1
,369
1
,354
1
,394
Pay
Re
serv
es
Sub
stan
tive
-
-
-
-
-
-
-
-
-
-
-
-
-
Pay
Re
serv
es
Tota
l
-
-
-
-
-
-
-
-
-
-
-
-
-
Scie
nti
fic,
Te
chn
ical
& T
he
rap
uti
cSu
bst
anti
ve
410
403
402
402
407
402
405
400
387
395
400
408
406
Ban
k
3
2
2
2
3
2
2
2
1
2
2
1
1
Age
ncy
13
4
3
3
2
2
1
1
4
6
5
6
5
Scie
nti
fic,
Te
chn
ical
& T
he
rap
uti
c
Tota
l
426
410
407
406
411
407
408
403
392
403
407
415
412
Oth
er
Staf
fSu
bst
anti
ve
775
774
771
760
772
773
810
802
805
797
803
804
824
Ban
k
1
2
1
4
1
2
9
1
1
1
4
1
5
1
3
1
0
1
4
1
4
1
3
1
2
Age
ncy
11
15
11
7
10
8
8
10
13
10
12
9
11
Oth
er
Staf
f To
tal
7
99
8
03
7
93
7
77
7
93
7
95
8
33
8
25
8
28
8
21
8
29
8
26
8
48
Gra
nd
To
tal
2,9
38
2,8
78
2,8
60
2,8
68
2,9
12
2,9
67
2,9
59
2,9
66
2,9
26
2,9
52
2,9
72
2,9
52
3,0
15
SUM
MA
RY
BY
STA
FF T
YP
E
PA
YSu
bst
anti
ve
2
,589
2
,589
2
,588
2
,569
2
,603
2
,608
2
,642
2
,643
2
,613
2
,623
2
,630
2
,626
2
,663
Ban
k
187
200
190
198
205
240
213
215
210
222
227
213
226
Age
ncy
1
62
90
82
1
01
1
04
1
19
1
03
1
08
1
03
1
07
1
15
1
13
1
26
Gra
nd
To
tal
2,9
38
2,8
78
2,8
60
2,8
68
2,9
12
2,9
67
2,9
59
2,9
66
2,9
26
2,9
52
2,9
72
2,9
52
3,0
15
TB
205_
19 F
inan
ce M
onth
7 R
epor
t App
endi
ces
Page 122 of 210

5.
Sta
tem
en
t o
f F
ina
nc
ial
Po
sit
ion
(B
ala
nce
Sh
ee
t)
Op
en
ing
ba
lan
ce
Clo
sin
g
ba
lan
ce
Mo
ve
me
nt
Mvt
in
mo
nth
01/0
4/2
019
31/1
0/2
019
£'0
00s
£'0
00s
£'0
00s
£'0
00s
NO
N C
UR
RE
NT A
SS
ETS
Pro
pert
y p
lant
and e
quip
ment/
inta
ngib
les
123,0
67
121,0
87
(1,9
80)
(38)
Oth
er
assets
966
1,5
37
571
(31)
TO
TA
L N
ON
CU
RR
EN
T A
SS
ETS
124,0
33
122,6
24
(1,4
09)
(69)
CU
RR
EN
T A
SS
ETS
Inve
nto
ries
2,3
82
2,3
15
(67)
105
Tra
de a
nd o
ther
receiv
able
s11,6
78
13,8
68
2,1
90
2,7
33
Cash a
nd c
ash e
quiv
ale
nts
1,0
42
1,1
19
77
(6,1
00)
Non c
urr
ent
assets
held
for
sale
00
00
TO
TA
L C
UR
RE
NT A
SS
ETS
15,1
02
17,3
02
2,2
00
(3,2
62)
CU
RR
EN
T L
IAB
ILIT
IES
Tra
de a
nd o
ther
payable
s(2
2,7
71)
(22,3
58)
413
(1,9
31)
Pro
visio
ns
(199)
(212)
(13)
0
PF
I/F
inance lease lia
bilitie
s(1
,153)
(1,1
53)
00
DH
reve
nue loans
(20,4
87)
(53,5
47)
(33,0
60)
(2)
DH
Capital lo
an
(411)
(400)
11
0
Oth
er
liabilitie
s(1
,025)
(6,5
75)
(5,5
50)
1,1
08
TO
TA
L C
UR
RE
NT L
IAB
ILIT
IES
(46,0
46)
(84,2
45)
(38,1
99)
(825)
NE
T C
UR
RE
NT A
SS
ETS
/(LIA
BIL
ITIE
S)
(30,9
44)
(66,9
43)
(35,9
99)
(4,0
87)
TO
TA
L A
SS
ETS
LE
SS
CU
RR
EN
T L
IAB
ILIT
IES
93,0
89
55,6
81
(37,4
08)
(4,1
56)
NO
N C
UR
RE
NT L
IAB
ILIT
IES
Pro
visio
ns
(207)
(160)
47
20
DH
reve
nue loans
(82,9
53)
(55,0
26)
27,9
27
2,7
43
PF
I/F
inance lease lia
bilitie
s(1
3,8
31)
(12,9
38)
893
645
DH
Capital lo
an
(1,0
00)
(600)
400
200
TO
TA
L N
ON
CU
RR
EN
T L
IAB
ILIT
IES
(97,9
91)
(68,7
24)
29,2
67
3,6
08
TO
TA
L A
SS
ETS
EM
PLO
YE
D(4
,902)
(13,0
43)
(8,1
41)
(548)
FIN
AN
CE
D B
Y T
AXP
AY
ER
S E
QU
ITY
Public D
ivid
end C
apital
98,2
14
98,2
14
00
Reta
ined e
arn
ings
(112,4
32)
(120,5
73)
(8,1
41)
(548)
Reva
luation r
eserv
e9,3
16
9,3
16
00
TO
TA
L T
AXP
AY
ER
S E
QU
ITY
(4,9
02)
(13,0
43)
(8,1
41)
(548)
In m
onth
mate
rial
move
ments
are
as follow
s:
Cash h
as r
educed by £
6.1
million a
s it has b
een utilised
to p
ay d
ow
n som
e o
f th
e D
HS
C l
oans (
£2.7
43 m
illion)
and c
ope w
ith less m
onie
s f
rom
the C
om
mis
sio
ners
as
they a
re c
law
ing b
ack p
revi
ously
paid
monie
s o
ver
the
last 6 m
onth
s o
f th
e y
ear.
The in
cre
ase i
n t
rade a
nd o
ther
receiv
able
s is
a
com
bin
ation in
an incre
ase i
n a
ged debt
(£1.1
million)
and a
n incre
ase in
incom
e a
ccru
als
.
Tra
de and o
ther
payable
s h
as a
lso incre
ased w
ith t
he
majo
rity
(appro
x.
£1.5
million)
associa
ted w
ith u
npaid
purc
hase in
voic
es.
Page 123 of 210

6.
Ca
pit
al
CA
TEG
OR
Y
CA
PIT
AL
SCH
EME
DES
CR
IPTI
ON
S SC
HEM
E C
OD
ES
20
19
/20
M7
YTD
Ord
ers
no
t ye
t re
ceiv
ed
Ve
rbal
ly
agre
ed
/
lett
er
of
inte
nt
R
emai
nin
g B
ud
get
to Y
en
d
£'0
00
£'0
00
£'0
00
Ori
gin
al
Pla
n
Re
vise
d P
lan
A
ctu
al
Var
ian
ce
A
ctu
al
Act
ual
Re
vise
d P
lan
A
ctu
al
Var
ian
ce
MED
ICA
L D
EVIC
ES
Med
ical
Eq
uip
me
nt
fun
d
G0
09
0
1,0
00
1
25
2
87
(1
62
)
28
4
31
1,0
00
7
46
2
54
Bed
s /
Tro
lleys
G
00
60
3
1
31
(3
1)
Sub
to
tal M
EDIC
AL
DEV
ICES
1,0
00
1
25
2
87
(1
62
)
28
4
62
1,0
00
7
77
2
23
IM&
T
Elec
tro
nic
Pat
ien
t R
eco
rd B
lue
spie
r G
01
00
1
11
Elec
tro
nic
Pat
ien
t R
eco
rd P
DS
G0
10
1
69
69
69
Elec
tro
nic
Pat
ien
t R
eco
rd C
aref
low
G
01
02
1
49
1
27
12
7
27
7
4
62
2
77
1
85
Vit
alp
ac
G0
00
7
10
25
(2
5)
25
2
5
Pat
ien
t Se
rvic
e Si
gnp
ost
ing
G0
10
3
18
4
13
8
10
6
32
1
84
1
06
7
8
eDM
S Ev
olv
e F6
44
7
80
4
0
43
(3
)
4
3
43
SQL
Serv
er U
pgr
ade
s
95
95
Win
do
ws
10
Pro
ject
G
01
04
3
18
2
59
4
41
(1
82
)
5
7
4
73
4
98
(2
5)
Tele
ph
on
y Sy
stem
Re
pla
cem
ent
G0
05
9
50
50
50
Bab
y Ta
ggin
g G
01
05
5
0
50
50
4
8
5
0
48
2
Cyb
er S
ecu
rity
G
00
71
8
0
60
2
3
37
2
2
23
(1
)
Fixe
d N
etw
ork
Infr
astr
uct
ure
F6
49
8
12
0
70
4
3
27
1
20
4
3
77
PA
S R
epla
cem
en
t F6
40
9
6
(6)
1
7
(7)
Dat
a St
ora
ge In
fras
tru
ctu
re
G0
10
6
25
61
61
Wir
eles
s N
etw
ork
Up
grad
e
G0
07
3
2
(2)
2
(2
)
IM&
T C
on
tin
gen
cy
G0
10
7
45
0
22
0
99
1
21
5
6
4
2
15
5
(11
3)
Sub
to
tal I
M&
T
1,6
96
9
64
7
88
1
76
4
39
1,6
96
1
,22
7
46
9
ESTA
TES
GE
Turn
key
wo
rks
for
Rad
iolo
gy e
qu
ipm
ent
rep
lace
me
nt
pro
gram
me
G
00
61
3
50
3
50
35
0
1
3
50
1
3
49
6 F
acet
Su
rvey
G
01
50
9
0
90
4
9
41
9
0
49
4
1
Nu
rse
Cal
l Sys
tem
G
01
51
1
00
Up
grad
e V
enti
lati
on
Pla
nts
G
01
52
1
00
Fire
co
mp
artm
en
tati
on
G
00
52
1
00
4
(4)
4
(4
)
Fire
Pre
cau
tio
ns
- Fi
re D
oo
rs
G0
01
9
10
0
2
(2
)
2
(2)
Legi
on
ella
Pre
ven
tio
n
G0
15
3
50
Spin
al L
ift
& R
amp
G
01
54
8
5
Spin
al is
ola
tio
n w
ork
s G
00
99
1
50
2
01
2
95
(9
4)
4
2
52
2
99
(4
7)
TB
205_
19 F
inan
ce M
onth
7 R
epor
t App
endi
ces
Page 124 of 210

CA
TEG
OR
Y
CA
PIT
AL
SCH
EME
DES
CR
IPTI
ON
S SC
HEM
E C
OD
ES
20
19
/20
M7
YTD
Ord
ers
no
t ye
t re
ceiv
ed
Ve
rbal
ly
agre
ed
/
lett
er
of
inte
nt
R
emai
nin
g B
ud
get
to Y
en
d
£'0
00
£'0
00
£'0
00
Ori
gin
al
Pla
n
Re
vise
d P
lan
A
ctu
al
Var
ian
ce
A
ctu
al
Act
ual
Re
vise
d P
lan
A
ctu
al
Var
ian
ce
ESTA
TES
SDG
H W
ard
Up
grad
es
G0
15
5
60
0
69
3
20
6
48
7
34
97
2
24
0
73
2
Lib
rary
Ext
ensi
on
G
01
56
1
45
1
45
14
5
14
5
1
45
Cap
ital
Tea
m
F63
05
1
60
9
3
10
1
(8)
16
0
10
1
59
CC
TV
G0
15
7
50
Sub
to
tal E
STA
TE IM
PR
OV
EMEN
T SC
HEM
ES
2
,08
0
1,5
72
6
57
9
15
1
38
1,9
69
6
96
1
,27
3
ESTA
TES
CO
NTI
NG
ENC
Y
Esta
tes
Co
nti
nge
ncy
Fu
nd
45
45
War
d E
Y B
lock
(ap
pro
ved
CIG
07
/19
)
20
20
Do
cto
rs M
ess
(18
/19
) F6
42
0
(1)
1
(1)
(1)
Spin
al W
ard
Bat
hro
om
s &
Sto
rage
G
01
58
1
62
(1
62
)
2
22
18
8
18
6
2
UP
S Th
eatr
e
G0
05
3
1
5
15
15
1
5
Sou
thp
ort
A&
E G
00
68
13
1
3
1
3
13
Sexu
al H
ealt
h A
cco
mm
od
atio
n
G0
07
9
(1
) (1
)
(1)
(1)
Car
Par
kin
g Sc
hem
e
Was
te M
anag
emen
t G
00
80
EBM
E Li
ft
HR
Mo
ve -
Fu
rth
er A
lter
atio
ns
to L
RC
F6
30
1
2
5
13
1
2
34
1
3
21
Su
b t
ota
l EST
ATE
S C
ON
TIN
GEN
CY
SC
HEM
ES
52
2
01
(1
49
)
71
2
2
3
13
2
94
1
9
Su
b t
ota
l EST
ATE
S SC
HEM
ES
2
,08
0
1,6
24
8
58
7
66
72
6
0
2
,28
2
99
0
1,2
92
FAC
ILIT
IES
Cat
erin
g eq
uip
me
nt
G0
02
6
75
6
2
18
4
4
6
9
10
2
87
1
5
V
ehic
le R
epla
cem
ent
G0
14
5
50
(1
2)
(1
2)
23
23
Su
b t
ota
l FA
CIL
ITIE
S
12
5
50
1
8
32
69
1
25
8
7
38
C
ON
TIN
GEN
CY
F6
30
1
20
2
(1
) 1
8
7
(7
)
C
apit
al p
lan
exc
lud
ing
do
nat
ion
s an
d IF
RIC
12
5,1
03
2
,76
3
1,9
50
8
13
16
8
96
9
5
,10
3
3,0
88
2
,01
5
OTH
ER
Do
nat
ed a
sset
s 0
00
00
0
10
0
50
5
0
1
00
5
0
50
GE
Rad
iolo
gy e
qu
ipm
ent
rep
lace
men
t p
rogr
amm
e (I
FRIC
12
) F6
42
0
1,2
14
1
,21
4
98
1
,11
6
1,2
14
9
8
1,1
16
Su
b t
ota
l Do
nat
ion
s an
d IF
RIC
12
1,3
14
1
,26
4
14
8
1,1
16
1
,31
4
14
8
1,1
66
TO
TAL
CA
PIT
AL
SPEN
D
6
,41
7
4,0
27
2
,09
8
1,9
29
16
8
96
9
6
,41
7
3,2
36
3
,18
1
Page 125 of 210

7.
Ca
sh
flo
w F
ore
ca
st – 2
019
/20
Actu
al
Actu
al
Actu
al
Actu
al
Actu
al
Actu
al
Actu
al
Pla
nP
lan
Pla
nP
lan
Pla
n
Ap
r-19
Ma
y-1
9Ju
n-1
9Ju
l-19
Au
g-1
9S
ep
-19
Oct-
19
No
v-1
9D
ec-1
9Ja
n-2
0F
eb
-20
Ma
r-20
To
tal
£'0
00s
£'0
00s
£'0
00s
£'0
00s
£'0
00s
£'0
00s
£'0
00s
£'0
00s
£'0
00s
£'0
00s
£'0
00s
£'0
00s
£'0
00s
Ca
sh
Flo
ws f
rom
Op
era
tin
g A
cti
vit
ies
Opera
ting S
urp
lus/(
Deficit)
(1,5
93)
(1,0
05)
(26)
(1,0
93)
(1,3
91)
126
(122)
482
(89)
612
(15)
912
(3,2
02)
Incom
e r
ecognis
ed in r
espect
of capital donations (
cash a
nd n
on-c
ash)
(9)
10
(34)
00
(8)
0(3
3)
00
(17)
(100)
Depre
cia
tion a
nd A
mort
isation
594
593
601
571
572
572
573
581
581
598
598
599
7,0
33
Impairm
ents
and R
eve
rsals
00
00
0
(Incre
ase)
in Inve
nto
ries
59
(86)
200
(143)
(74)
216
(105)
(50)
30
25
18
30
120
(Incre
ase)
in T
rade a
nd O
ther
Receiv
able
s(9
49)
(2,0
96)
(1,1
15)
1,1
43
1,9
47
1,0
11
(2,7
02)
(2,4
54)
1,2
00
(2,7
58)
(2,7
58)
3,1
36
(6,3
95)
Incre
ase in T
rade a
nd O
ther
Payable
s3,5
17
(1,1
23)
(1,8
71)
(1,8
87)
5,8
22
(512)
514
(1,5
59)
(2,8
94)
(3,8
65)
170
(1,1
65)
(4,8
53)
Incre
ase in P
rovi
sio
ns
1(8
)(3
)10
0(1
4)
14
(25)
(42)
(67)
Ne
t C
ash
In
flo
w/(
Ou
tflo
w)
fro
m O
pe
rati
ng
Acti
vit
ies
1,6
20
(3,7
24)
(2,2
14)
(1,4
33)
6,8
76
1,3
99
(1,8
36)
(3,0
00)
(1,2
30)
(5,3
88)
(1,9
87)
3,4
53
(7,4
64)
Ca
sh
Flo
ws f
rom
In
ve
sti
ng
Acti
vit
ies
Inte
rest
Receiv
ed
34
55
817
(1)
66
66
772
(Paym
ents
) fo
r In
tangib
le A
ssets
(57)
0(2
)(1
52)
127
0(2
)(9
2)
(112)
(83)
(80)
(237)
(690)
(Paym
ents
) fo
r P
PE
and inve
stm
ent
pro
pert
y(1
90)
(117)
(186)
40
(1,1
44)
(325)
(189)
(391)
(570)
(667)
(291)
(1,0
70)
(5,1
00)
Receip
ts fro
m d
isposal of fixed a
ssets
00
00
0
Receip
t of cash d
onations t
o p
urc
hase c
apital
assets
9(1
)0
34
833
17
100
Ne
t C
ash
In
flo
w/(
Ou
tflo
w)
fro
m I
nve
sti
ng
Acti
vit
ies
(235)
(114)
(183)
(73)
(1,0
09)
(308)
(184)
(477)
(643)
(744)
(365)
(1,2
83)
(5,6
18)
Ca
sh
Flo
ws f
rom
Fin
an
cin
g A
cti
vit
ies
Public d
ivid
end c
apital re
ceiv
ed
00
00
0
Public d
ivid
end c
apital re
paid
00
00
0
Loans r
eceiv
ed fro
m D
H2,4
56
1,4
58
2,3
86
2,1
79
00
03,6
93
3,1
55
6,4
34
3,0
81
24,8
42
Loans r
epaid
to D
H(2
00)
00
00
0(2
,941)
(697)
(1,2
36)
(5,0
74)
Capital ele
ment
of finance leases
(8)
(8)
(8)
(8)
(8)
(8)
(596)
(24)
(240)
(24)
(932)
Capital ele
ment
of P
FI, L
IFT
(16)
(15)
(118)
(16)
(15)
(119)
(15)
(16)
(118)
(16)
(15)
(119)
(598)
Inte
rest
Paid
(190)
(234)
(225)
(195)
(228)
(545)
(207)
(238)
(234)
(205)
(236)
(540)
(3,2
77)
Inte
rest
ele
ment
of finance lease
00
00
(240)
(158)
(398)
Inte
rest
ele
ment
of P
FI, L
IFT
(80)
(81)
(209)
(80)
(81)
(209)
(81)
(81)
(209)
(81)
(80)
(209)
(1,4
81)
PD
C d
ivid
end (
paid
)/re
funded
00
00
0
Ne
t C
ash
In
flo
w/(
Ou
tflo
w)
fro
m F
ina
ncin
g
Acti
vit
ies
1,9
62
1,1
20
1,8
26
1,8
80
(332)
(881)
(4,0
80)
3,3
58
1,8
73
6,1
32
2,3
52
(2,1
28)
13,0
82
NE
T I
NC
RE
AS
E/(
DE
CR
EA
SE
) IN
CA
SH
3,3
47
(2,7
18)
(571)
374
5,5
35
210
(6,1
00)
(119)
00
042
0
Ca
sh
- B
eg
inn
ing
of
the
Pe
rio
d1,0
42
4,3
89
1,6
71
1,1
00
1,4
74
7,0
09
7,2
19
1,1
19
1,0
00
1,0
00
1,0
00
1,0
00
1,0
42
Ca
sh
- E
nd
of
the
Pe
rio
d4,3
89
1,6
71
1,1
00
1,4
74
7,0
09
7,2
19
1,1
19
1,0
00
1,0
00
1,0
00
1,0
00
1,0
42
1,0
42
TB
205_
19 F
inan
ce M
onth
7 R
epor
t App
endi
ces
Page 126 of 210


PUBLIC TRUST BOARD 4 December 2019
Agenda Item PB206/19 Report Title Risk Register
Executive Lead Juliette Cosgrove, Director of Nursing, Midwifery and Therapies
Lead Officer Katharine Martin, Interim Head of Risk
Mandy Power, Assistant Director of Integrated Governance
Action Required
(Definitions below)
To Approve To Note
To Assure ✓ To Receive
For Information
Executive Summary
Since the last meeting, one new risk has been added onto the risk register.
• 2122 – Medicines Management (15). This risk has been added as a result of concerns raised by CQC. A Medicines Management Improvement Plan has been developed with actions underway.
Discussions have taken place at Risk & Compliance Group to add an additional two risks onto this risk register. These relate to ‘Fragile Services’ and ‘Medical Staffing’. These will be drafted for approval at Risk & Compliance Group in December. Since the last meeting, no risks have been removed from the risk register. There are currently 8 risks on the High Level Risk register. These are:
• 1688 - Inadequate Staffing Levels in Anaesthetic Department (will be consolidated into Medical Staffing risk)
• 1902 - Failure to comply & improve governance of services in relation to the areas of non-compliance identified by CQC
• 2052 - Older Peoples Care
• 1862 - Maintaining safe quality nursing care with current level of nursing & HCA vacancies
• 1942 - Eradicating the Trust’s deficit by 2023/24
• 2072 - Failure to achieve 2019/20 financial control total
• 2056 - Missing Patient appointments/admissions
• 2122 – Medicines Management
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
TB
206_
19 F
S R
isk
Reg
iste
r D
ec 1
9
Page 127 of 210

Strategic Objective Principal Risk
✓ SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
✓ SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
✓ SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
✓ SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
✓ SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
✓ SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
Absence of clear direction, engagement and leadership across the system is a risk to the sustainability of the Trust and will lead to declining clinical standards.
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
✓ Caring Statutory Requirement
✓ Effective ✓ Annual Business Plan Priority
✓ Responsive Best Practice
✓ Safe Service Change
✓ Well Led
Impact (is there an impact arising from the report on any of the following?)
✓ Compliance Legal
Engagement and Communication ✓ Quality & Safety
Equality ✓ Risk
✓ Finance ✓ Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Board/Committee/Group)
This is a dynamic document and its structure and content may be updated as necessary.
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
Page 128 of 210

GUIDE TO ACTIONS REQUIRED (TO BE REMOVED BEFORE ISSUE):
Approve: To formally agree the receipt of a report and its recommendations OR a particular course of action
Receive: To discuss in depth a report, noting its implications for the Board or Trust without needing to formally approve
Note: For the intelligence of the Board without the in-depth discussion as above
Assure: To apprise the Board that controls and assurances are in place
For Information: Literally, to inform the Board
TB
206_
19 F
S R
isk
Reg
iste
r D
ec 1
9
Page 129 of 210


Page 1 of 14
NOVEMBER 2019 – SUMMARY OF HIGH LEVEL RISK REGISTER AS AT 26/11/2019
Risk ID Principle Objective(s) Risk Executive Lead Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19
1688
SO1 - Improve clinical outcomes and patient safety to ensure we deliver high quality
services
SO3 - Efficiently and productively provide care within agreed financial limits
SO4 - Develop a flexible, responsive workforce of the right size and with the right skills
who feel valued and motivated
SO6 - Engage strategic partners to maximise the opportunities to design and deliver
sustainable services for the population of Southport, Formby and West Lancashire
Inadequate Staffing Levels in
Anaesthetic Department
Chief
Operating
Officer
=15 20 =20 =20 =20 =20
1902
SO1 - Improve clinical outcomes and patient safety to ensure we deliver high quality
services
SO2 - Deliver services that meet NHS constitutional and regulatory standards
SO3 - Efficiently and productively provide care within agreed financial limits
SO4 - Develop a flexible, responsive workforce of the right size and with the right skills
who feel valued and motivated
SO5 - Enable all staff to be patient-centered leaders building on an open and honest
culture and the delivery of the Trust values
SO6 - Engage strategic partners to maximise the opportunities to design and deliver
sustainable services for the population of Southport, Formby and West Lancashire
Failure to comply & improve
governance of services in
relation to the areas of non
compliance identified by CQC
Director of
Nursing &
Quality
=16 =16 =16 =16 =16 =16
1862
SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality
services
SO2 - Deliver services that meet NHS constitutional and regulatory standards
Maintaining safe quality
nursing care with current level
of nursing & HCA vacancies
Director of
Nursing &
Quality =16 =16 =16 =16 =16 =16
1942 SO3 - Efficiently and productively provide care within agreed financial limitsEradicating the Trust's deficit
by 2023/24
Director of
Finance =16 =16 =16 =16 =16 =16
1987
SO1 - Improve clinical outcomes and patient safety to ensure we deliver high quality
services
SO2 - Deliver services that meet NHS constitutional and regulatory standards
SO3 - Efficiently and productively provide care within agreed financial limits
SO4 - Develop a flexible, responsive workforce of the right size and with the right skills
who feel valued and motivated
SO5 - Enable all staff to be patient-centered leaders building on an open and honest
culture and the delivery of the Trust values
SO6 - Engage strategic partners to maximise the opportunities to design and deliver
sustainable services for the population of Southport, Formby and West Lancashire
Haem / Oncology, reduction in
medical capacity following
resignation of consultant
Executive
Medical
Director
=16 =16 =16 12 =12 =12
2052
SO1 - Improve clinical outcomes and patient safety to ensure we deliver high quality
services
SO2 - Deliver services that meet NHS constitutional and regulatory standards
SO3 - Efficiently and productively provide care within agreed financial limits
SO6 - Engage strategic partners to maximise the opportunities to design and deliver
sustainable services for the population of Southport, Formby and West Lancashire
Older Peoples Care
Director of
Nursing &
Quality
!16 =16 =16 =16 =16 =16
2056
SO1 - Improve clinical outcomes and patient safety to ensure we deliver high quality
services
SO2 - Deliver services that meet NHS constitutional and regulatory standards
Missing Patient
appointments/admissions
Chief
Operating
Officer !16 20 =20 =20
2021
SO1 - Improve clinical outcomes and patient safety to ensure we deliver high quality
services
SO2 - Deliver services that meet NHS constitutional and regulatory standards
SO4 - Develop a flexible, responsive workforce of the right size and with the right skills
who feel valued and motivated
SO5 - Enable all staff to be patient-centered leaders building on an open and honest
culture and the delivery of the Trust values
SO6 - Engage strategic partners to maximise the opportunities to design and deliver
sustainable services for the population of Southport, Formby and West Lancashire
In Hospital Mortality
Executive
Medical
Director
!15 =15 =15 10 10
1977
SO1 - Improve clinical outcomes and patient safety to ensure we deliver high quality
services
SO3 - Efficiently and productively provide care within agreed financial limits
SO4 - Develop a flexible, responsive workforce of the right size and with the right skills
who feel valued and motivated
SO6 - Engage strategic partners to maximise the opportunities to design and deliver
sustainable services for the population of Southport, Formby and West Lancashire
Peadiatric Dietetics Band 6
Director of
Nursing &
Quality
!15 =15 16
Risk to be
amalgama
ted into
overarchi
ng Fragile
Services
risk
2072 SO3 - Efficiently and productively provide care within agreed financial limitsFailure to achieve 2019/20
financial control total
Director of
Finance !16 =16 =16
2122SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality
servicesMedicines Management
Executive
Medical
Director !15
TB
206_
19 R
isk
Reg
iste
r D
ec 1
9
Page 130 of 210

Pa
ge
2 o
f 1
4
TR
US
T R
ISK
PR
OF
ILE
AS
AT
26
/11
/20
19
C
ON
SEQ
UEN
CE
(im
pac
t/se
veri
ty)
LIK
ELIH
OO
D
(fre
qu
ency
) In
sign
ific
ant
(1)
Min
or
(2)
Mo
de
rate
(3
) M
ajo
r (4
) C
atas
tro
ph
ic (
5)
Alm
ost
Cer
tain
(5
)
Like
ly (
4)
194
2 –
Era
dic
atin
g th
e T
rust
’s d
efic
it b
y 2
023/
24
207
2 -
Fai
lure
to
ach
ieve
20
19/2
0 fi
nan
cial
co
ntr
ol t
ota
l 2
052
- O
lder
Pe
op
les
Car
e 1
862
- M
ain
tain
ing
safe
qu
alit
y n
urs
ing
care
wit
h c
urr
en
t le
vel o
f n
urs
ing
& H
CA
va
can
cies
1
902
- F
ailu
re t
o c
om
ply
& im
pro
ve
gove
rnan
ce o
f se
rvic
es in
rel
atio
n t
o t
he
area
s o
f n
on
-co
mp
lian
ce id
enti
fied
by
CQ
C
16
88
- In
adeq
uat
e
Staf
fin
g Le
vels
in
An
aest
het
ic D
ep
artm
ent
20
56
– M
issi
ng
Pat
ien
t ap
po
intm
ents
/ad
mis
sio
ns
Po
ssib
le (
3)
21
22
– M
edic
ines
M
anag
eme
nt
Un
likel
y (2
)
Rar
e (
1)
Page 131 of 210

Pa
ge
3 o
f 1
4
Board
/Sub-B
oard
C
om
mitte
e:
Tru
st
Board
R
isk R
eg
iste
r
Str
ate
gic
Ob
jecti
ve
SO
1 -
Im
pro
ve c
linic
al outc
om
es a
nd p
atie
nt safe
ty to e
nsure
we d
eliv
er
hig
h q
ualit
y s
erv
ices
Lin
k t
o B
AF
Op
en
ed
ID
AD
O/E
xec L
ead
Ris
k L
ead
Tit
le
14/1
1/2
019
2122
Executive M
edic
al D
irecto
r John W
illia
ms
Me
dic
ines M
anagem
ent
Descri
pti
on
If the tru
st cannot
guara
nte
e S
afe
and S
ecure
Handlin
g o
f M
edic
ines a
nd
Clin
ical P
harm
acy S
erv
ice then t
here
is a
ris
k o
f patie
nt harm
thro
ugh la
ck o
f tim
ely
me
dic
ines r
econcili
atio
n, supply
of
critical m
edic
ines t
o p
atie
nts
, corr
ect pre
scrib
ing a
nd a
dm
inis
tratio
n o
f m
edic
ines a
nd r
isk o
f patie
nts
goin
g h
om
e w
ithout th
e c
orr
ect ta
ke h
om
e m
edic
atio
n.
Co
ntr
ols
P
harm
acis
t clin
ical check f
or
all
non
-sto
ck ite
ms d
urin
g o
penin
g h
ours
. Late
nig
ht ro
ta for
Pharm
acy s
taff a
nd o
n-c
all
serv
ice.
Access t
o E
me
rgency S
tore
out of hours
W
eekend o
penin
g tim
es lim
ited t
o a
n e
me
rgency s
erv
ice
E
lectr
onic
dis
charg
e, in
clu
din
g lin
ks to P
harm
Ou
tcom
es
Locum
cover
for
som
e v
acancie
s
Patie
nts
ow
n m
edic
ines s
tore
d in b
ed s
ide lo
ckers
S
elf a
dm
inis
tratio
n of m
edic
ines, C
ontr
olle
d D
rug a
nd M
edic
ines O
ptim
isatio
n P
olic
ies
Weekly
top u
p a
nd d
ate
checkin
g fro
m p
harm
acy s
taff in
cupboard
s for
mo
st clin
ical are
as;
Ele
ctr
onic
Checklis
t fo
r re
sus t
rolle
ys t
o e
nsure
ite
ms a
re in
date
Gap
s i
n C
on
tro
ls
Insuffic
ient S
taff w
ithin
Pharm
acy D
epart
me
nt to
pro
vid
e
me
dic
ines r
econcili
atio
n w
ithin
24 h
ours
. U
nable
to e
nsure
tim
ely
dis
charg
e m
edic
atio
n d
ue t
o in
suff
icie
nt
sta
ff r
esultin
g in in
suff
icie
nt
openin
g t
ime
s
Imp
act
on p
atie
nt
flo
w d
ue to d
ela
yed d
ischarg
es a
s a
result o
f dela
yed d
ischarg
e m
edic
atio
n n
ot bein
g p
rescrib
ed in
a t
ime
ly
fashio
n
Insuffic
ient re
sourc
e f
or
in-p
atie
nt/dis
charg
e c
ounselli
ng
impactin
g p
oor
in-p
atie
nt surv
ey r
esults, and a
bili
ty for
patie
nts
to
self-a
dm
inis
ter.
R
isk o
f patie
nts
mis
sin
g c
ritical m
edic
ines/t
hera
py.
Unable
to e
nsure
contin
uity o
f supply
of critical m
edic
ines d
ue to
insuffic
ient
ward
based s
erv
ices inclu
din
g w
ard
based p
harm
acy
technic
ians.
Me
dic
ines T
rolle
ys u
nfit fo
r purp
ose.
Inadequate
syste
m for
pre
-pack m
edic
ines c
ontr
ol in
all
are
as
Lack o
f C
D d
estr
uctio
n a
t w
ard
level due t
o la
ck o
f w
ard
based
technic
ians.
Aseptic u
nit Q
CN
W e
xte
rnal audit n
ote
d m
ajo
r concern
s
regard
ing Q
ualit
y R
evie
w s
yste
ms
Lim
ited o
penin
g h
ours
of P
harm
acy M
onday-
Frid
ay 9
-5,
and
reduced s
erv
ice a
nd s
taff
ing 3
hours
Sat
and S
un.
Eff
ect
on P
harm
acy s
taff w
ell-
bein
g a
nd s
ickness r
ate
s d
ue t
o
work
load p
ressure
. Lack o
f centr
al w
irele
ss m
onitorin
g s
yste
m f
or
tem
pera
ture
s in
dru
g s
tora
ge a
reas.
Lack o
f E
PM
A (
ele
ctr
onic
pre
scrib
ing)
trust w
ide.
Anti-c
oagula
nt clin
ics r
un o
n m
inim
al sta
ffin
g
Unable
to u
pdate
to D
rug L
ibra
ry for
IV p
um
ps in a
tim
ely
ma
nner
Poor
upta
ke o
f m
edic
ines m
anagem
ent tr
ain
ing to
mu
ltid
iscip
linary
team
. P
oor
com
ple
tion o
f docum
enta
tio
n.
TB
206_
19 R
isk
Reg
iste
r D
ec 1
9
Page 132 of 210

Pa
ge
4 o
f 1
4
Ris
k L
evels
L
ikelih
oo
d
Co
ns
eq
ue
nce
Ris
k R
ati
ng
(I
nit
ial)
Ris
k R
ati
ng
(C
urr
en
t)
Ris
k L
evel
(Cu
rren
t)
Ris
k R
ati
ng
(T
arg
et)
R
isk L
evel (T
arg
et)
D
ate
of
La
st
Rev
iew
D
ate
of
Next
Revie
w
P
ossib
le (
3)
Cata
str
ophic
(5)
20
15
Extr
em
e r
isk
4
Mo
dera
te r
isk
21/1
1/2
019
12/1
2/2
019
Assu
ran
ce
Dru
g a
nd T
hera
peutic C
om
mitte
e p
rovid
es M
edic
ines G
overn
ance
and m
eets
mo
nth
ly
Me
dic
ines S
afe
ty C
om
mitte
e m
eets
mo
nth
ly. R
evie
w o
f dru
g a
lert
s a
nd m
edic
ines in
cid
ents
. M
ost lo
w/n
o
harm
. P
harm
acis
t in
terv
entio
n m
onitoring
P
harm
acy G
overn
ance m
onth
ly m
eetin
g. R
evie
w o
f D
ispensin
g e
rrors
S
OC
CA
S w
ard
accre
ditatio
n s
yste
m h
ighlig
hts
are
as o
f good p
ractice a
nd a
reas for
imp
rovem
ent
in
me
dic
ines m
anagem
ent
CD
audits
Gap
s i
n A
ssu
ran
ce
Out
of date
me
dic
ines,
poor
dru
g s
tora
ge a
nd t
em
pera
ture
m
onitorin
g w
ithin
exis
tin
g t
reatm
ent
room
s.
Poor
me
dic
ines r
econcili
atio
n w
ithin
24 h
ours
. C
D P
olic
y r
equires r
evie
w
Poor
attendance a
t M
edic
ines M
anagem
ent
train
ing
Acti
on
Pla
n
PM
O s
upport
pro
vid
ed to the M
edic
al D
irecto
r, C
hie
f P
harm
acis
t, P
harm
acy a
nd N
urs
ing s
taff to c
om
ple
te
the M
edic
ines M
anagem
ent
Develo
pm
ent P
roje
ct
in lin
e w
ith N
HS
I, C
QC
and in
tern
al assessm
ents
to
clo
se t
he G
aps in
assura
nce
Acti
on
Pla
n D
ue
Date
01/1
1/2
021
A
cti
on
Pla
n R
ati
ng
Mo
dera
te
Pro
gre
ss M
ade
La
test
Mo
nth
P
rog
ress
Th
e p
harm
acy b
usin
ess c
ase for
work
forc
e w
as a
ppro
ved a
t th
e t
rust board
7th
Novem
ber2
019 (
for
exte
nded w
eekend w
ork
ing, A
ED
Consultant
pharm
acis
t and w
ard
pharm
acy a
ssis
tants
). A
ny
changes to w
ork
ing h
ours
will
be s
ubje
ct to
sta
ff c
onsultatio
n w
ith s
upport
of
HR
. T
he t
rust
has b
een s
uccessfu
l in
securin
g £
700k o
f fu
ndin
g f
rom
NH
S E
ngla
nd I
nte
gra
ted D
igital C
are
Fu
nd t
o
imple
me
nt an e
lectr
onic
pre
scrib
ing a
nd m
edic
ines a
dm
inis
tratio
n (
EP
MA
) syste
m o
ver
the n
ext
18 m
onth
s w
hic
h w
ill s
upport
patie
nt safe
ty a
nd t
he
dis
charg
e p
rocess.
Page 133 of 210

Pa
ge
5 o
f 1
4
Str
ate
gic
Ob
jecti
ve
SO
1 -
Im
pro
ve c
linic
al outc
om
es a
nd p
atie
nt safe
ty to e
nsure
we d
eliv
er
hig
h q
ualit
y s
erv
ices S
O2 -
Deliv
er
serv
ices t
hat m
eet N
HS
constitu
tio
nal
and r
egula
tory
sta
ndard
s
Lin
k t
o B
AF
Op
en
ed
ID
AD
O/E
xec L
ead
Ris
k L
ead
Tit
le
27/0
6/2
019
2056
Chie
f O
pera
tin
g O
ffic
er
Hele
n B
ayth
orp
e
Mis
sin
g P
atie
nt
appoin
tme
nts
/adm
issio
ns
Descri
pti
on
If w
e f
ail
to h
ave a
robust
pro
cess in
pla
ce t
o m
anage O
utp
atie
nt C
linic
and W
ard
outc
om
es then t
here
is a
ris
k w
e w
ill c
ause
harm
to p
atients
due t
o n
ot
pro
vid
ing a
ppro
priate
tre
atm
ent in
a t
ime
ly
ma
nner.
Co
ntr
ols
2 N
on R
TT
valid
ato
rs h
ave c
om
menced in
Tru
st
to r
evie
w h
igh r
isk p
ath
ways in
Uro
logy a
nd
Ophth
alm
olo
gy
Report
re m
issin
g o
utc
om
es in
suite o
f P
TL
report
s to allo
w m
onitoring
S
OP
's in
pla
ce for
ma
nagem
ent
of clin
ic o
utc
om
es
Patie
nt's
giv
en a
dvic
e a
nd c
onta
ct num
ber
to c
all
if n
ot
heard
within
a c
ert
ain
perio
d w
ithin
Uro
logy
GP
lett
ers
ale
rtin
g t
o loss t
o f
ollo
w u
p
Clin
ic o
utc
om
e s
heets
now
reta
ined a
nd o
utc
om
ed o
n t
he d
ay
Clin
ic o
utc
om
e s
heets
now
reta
ined a
nd o
utc
om
ed o
n t
he d
ay
Gap
s i
n C
on
tro
ls
No a
udit o
f pro
cess in p
lace f
or
bookin
g a
ppoin
tme
nts
and lis
tin
g
patie
nts
for
pro
cedure
s
Paper
based p
rocess w
hic
h is f
ragm
ente
d
Lack o
f ele
ctr
onic
syste
m
Logis
tical is
sues o
f clin
ics b
ein
g h
eld
acro
ss s
ites c
ausin
g issues
transfe
rrin
g p
aper
form
s in v
ario
us m
odes
Non R
TT
tra
ckers
la
ck c
apacity to r
evie
w p
ath
ways.
Th
e p
rocess p
uts
the o
nus o
n the p
atie
nt
GP
's m
ay n
ot
ale
rt the loss t
o f
ollo
w u
p in
all
cases.
Sta
ff c
om
ple
te tra
inin
g p
ackage E
nd D
ec 2
019 w
hic
h m
eans
pote
ntia
l fo
r fu
rther
issues c
urr
ently o
ngoin
g.
Ris
k L
evels
L
ikelih
oo
d
Co
ns
eq
ue
nce
Ris
k R
ati
ng
(I
nit
ial)
Ris
k R
ati
ng
(C
urr
en
t)
Ris
k L
evel
(Cu
rren
t)
Ris
k R
ati
ng
(T
arg
et)
R
isk L
evel (T
arg
et)
D
ate
of
La
st
Revie
w
Date
of
Next
Revie
w
Lik
ely
(4)
Cata
str
ophic
(5)
20
20
Extr
em
e r
isk
5
Mo
dera
te r
isk
18/1
1/2
019
18/1
2/2
019
Assu
ran
ce
Hig
hlig
hte
d t
o t
he B
oard
. P
atie
nts
lo
st to
follo
w-u
p r
eport
ed w
hen id
entifie
d v
ia D
atix
Gap
s i
n A
ssu
ran
ce
Lik
ely
to h
ave a
sig
nific
ant
dela
y p
rio
r to
gain
ing t
he r
ight solu
tio
n
As a
t 11/0
7/1
9 -
12 S
I's r
eport
ed r
ela
tin
g t
o U
rolo
gy a
nd
Ophth
alm
olo
gy
Acti
on
Pla
n
Deliv
ery
again
st th
e T
rust overa
rchin
g lo
st to
follo
w u
p a
ctio
n p
lan
A
cti
on
Pla
n D
ue
Date
31/0
1/2
020
A
cti
on
Pla
n R
ati
ng
Mo
dera
te
Pro
gre
ss M
ade
La
test
Mo
nth
P
rog
ress
Weekly
me
etin
gs c
ontin
ue to take p
lace to u
pdate
on t
he a
ctio
n p
lan w
ith C
CG
repre
senta
tio
n f
ort
nig
htly a
t th
ese m
eetin
gs.
CC
G c
onfirm
that
update
d a
ctio
n p
lan is p
resente
d a
t th
e J
oin
t Q
ualit
y a
nd
perf
orm
ance m
eetin
g.
SO
Ps h
ave b
een a
gre
ed a
nd c
ircula
ted.
Sta
ge 1
of tr
ain
ing h
as n
ow
been c
om
ple
ted w
ith S
tage 2
to b
e c
om
ple
ted b
y e
nd o
f D
ecem
ber
2019.
This
is r
ecord
ed o
n E
RS
to
enable
mo
nitorin
g.
Second tra
cker
is n
ow
tra
ined a
nd t
rackin
g r
eport
as a
bove is a
liv
e d
ocum
ent, w
ith d
aily
update
s.
Busin
ess c
ase h
as b
een w
ritt
en for
substa
ntive p
osts
and w
ill g
o to B
DIS
C D
ec
12th
.In lig
ht of curr
ent C
CG
engagem
ent
and r
eport
ing, T
rust re
quest
report
ing into
contr
act m
eetin
g b
y e
xceptio
n o
nly
.
TB
206_
19 R
isk
Reg
iste
r D
ec 1
9
Page 134 of 210

Pa
ge
6 o
f 1
4
Str
ate
gic
Ob
jecti
ve
SO
1 -
Im
pro
ve c
linic
al outc
om
es a
nd p
atie
nt safe
ty to e
nsure
we d
eliv
er
hig
h q
ualit
y s
erv
ices S
O2 -
Deliv
er
serv
ices t
hat m
eet N
HS
constitu
tio
nal
and r
egula
tory
sta
ndard
s
Lin
k t
o B
AF
SO
2
Op
en
ed
ID
AD
O/E
xec L
ead
Ris
k L
ead
Tit
le
20/0
6/2
018
1862
Directo
r of N
urs
ing &
Qualit
y
Caro
l F
ow
ler
Ma
inta
inin
g s
afe
qualit
y n
urs
ing c
are
with c
urr
ent
level of
nurs
ing &
HC
A v
acancie
s
Descri
pti
on
If le
vels
of
Regis
tere
d N
urs
e &
HC
A s
taff
ing r
em
ain
s b
elo
w funded e
sta
blis
hm
ent
due to v
acancie
s then p
atie
nts
ma
y e
xperie
nce
poor
qualit
y o
f care
(safe
ty &
patie
nt
experie
nce).
Co
ntr
ols
S
afe
Care
mo
nitore
d d
aily
M-F
ri
Daily
sta
ffin
g h
uddle
s w
ith M
atr
ons &
Senio
r nurs
e
Revie
w H
ealth r
oste
r P
olic
y &
com
plia
nce r
atifie
d J
uly
2019
N
HS
P c
ontr
act
Nurs
ing e
sta
blis
hm
ents
ratifie
d a
t T
rust B
oard
Ma
y 2
019
Sta
ffin
g d
ata
revie
ws
See r
isks 1
132 , 2
78 a
nd h
igh r
isk 1
368
D
atix s
yste
m t
o id
entify
if th
ere
has b
een a
harm
of
patie
nts
due to s
taffin
g levels
D
atix s
yste
m in
pla
ce t
o id
entify
if th
ere
has b
een a
harm
of
patie
nts
due t
o s
taff
ing le
vels
in
accord
ance
with N
ICE
're
d' f
lags
Safe
sta
ffin
g r
eport
to W
Fo
rce C
om
m. &
Tru
st B
oard
on a
mo
nth
ly b
asis
T
ier
2 n
urs
e a
gency in p
lace
R
ete
ntio
n g
roup w
ith a
focus o
n R
ecru
itm
ent, s
upport
ed b
y N
HS
I C
ontr
act bookin
g for
RN
agency t
o s
upport
fill
rate
on d
ay s
hifts
during w
inte
r pre
ssure
d m
onth
s
Gap
s i
n C
on
tro
ls
No f
orm
al S
afe
ty H
uddle
at
w/e
nds
Esta
blis
hm
ent re
vie
w n
ot
undert
aken o
n a
6 m
onth
ly b
asis
with
recom
mendatio
ns t
o the T
B
NH
SP
contr
act fo
r re
vie
w in 6
mo
nth
s
Clin
ical w
ork
forc
e P
lan to b
e d
evelo
ped f
ollo
win
g E
sta
blis
hm
ent
revie
w
See r
isks 1
132, 278 a
nd h
igh r
isk 1
368.
Ris
k L
evels
L
ikelih
oo
d
Co
ns
eq
ue
nce
Ris
k R
ati
ng
(I
nit
ial)
Ris
k R
ati
ng
(C
urr
en
t)
Ris
k L
evel
(Cu
rren
t)
Ris
k R
ati
ng
(T
arg
et)
R
isk L
evel (T
arg
et)
D
ate
of
La
st
Revie
w
Date
of
Next
Revie
w
Lik
ely
(4)
Ma
jor
(4)
20
16
Extr
em
e r
isk
8
Hig
h R
isk
18/1
1/2
019
16/1
2/2
019
Assu
ran
ce
Mo
nth
ly s
taff
ing r
eport
C
QC
in
spectio
n
Qualit
y a
nd s
afe
ty r
eport
s
Com
pla
ints
In
cid
ent re
port
ing
Bi annual sta
ffin
g r
eport
s
ma
ndato
ry tra
inin
g
Work
forc
e d
ata
(sic
kness &
AL)
D
edic
ate
d H
roste
r Lead f
or
N&
M
Esta
blis
hm
ent re
vie
w p
rocess S
OP
ratifie
d b
y H
MB
- M
ay 2
019
Mo
nth
ly E
roste
r m
eetin
gs &
dashboard
in
pla
ce
E-R
oste
r polic
y
QI m
eth
odolo
gy in
pla
ce to s
upport
E-R
oste
r perf
orm
ance
Gap
s i
n A
ssu
ran
ce
Work
forc
e P
lan (
inclu
din
g R
ete
ntion &
Recru
itm
ent)
U
pdate
d E
roste
r polic
y
Ma
trons d
ashboard
/Clin
ical m
etr
ics n
eeds t
o b
e d
evelo
ped
furt
her
Ma
ndato
ry tra
inin
g n
ot
bein
g a
t T
rust re
quired s
tandard
M
anagin
g P
erf
orm
ance F
ram
ew
ork
pro
cess
Acti
on
Pla
n
Fu
ll deta
ils in
sm
art
-sheets
- E
roste
r com
plia
nce
P
rio
ritise tem
pla
te u
plo
ad
Cla
rify
capacity to u
plo
ad t
em
pla
tes for
new
NE
R
Contin
ue 2
weekly
me
etin
g w
ith H
oN
/M &
Ma
trons
NE
R -
deta
iled p
lans o
n s
ma
rt s
heets
- M
odel H
ospital
Unders
tand c
urr
ent data
su
bm
issio
n
Revie
w M
odel hospital fo
r S
&O
data
A
ssess o
pport
unity for
savin
gs b
ased o
n n
ew
data
S
ma
rt s
heets
has d
eta
iled p
lan -
Fin
ance.
Uplo
ad b
udgets
In
form
Wd m
anagers
/Matr
ons o
f final e r
oste
r ro
ta
Acti
on
Pla
n D
ue
Date
27/1
2/2
019
27/1
2/2
019
31/1
2/2
020
31/1
2/2
020
31/1
2/2
020
29/0
6/2
018
31/0
1/2
019
29/0
3/2
019
31/0
5/2
019
Acti
on
Pla
n R
ati
ng
Com
ple
ted
Mo
dera
te
Pro
gre
ss M
ade
Com
ple
ted
Mo
dera
te
Pro
gre
ss M
ade
Mo
dera
te
Pro
gre
ss M
ade
Com
ple
ted
Com
ple
ted
Com
ple
ted
Com
ple
ted
Page 135 of 210

Pa
ge
7 o
f 1
4
Uplo
ad n
ew
tem
pla
tes
Sm
art
sheets
has d
eta
iled p
lan -
Recru
itm
ent
Identify
HR
recru
itm
ent te
am
to s
upport
recru
itm
ent pro
cess
Advert
ise r
ele
vant posts
(R
N,
HC
A, B
4)
Mo
nth
ly r
evie
w o
f vacancie
s, tu
rnover
& p
rogre
ss t
hro
ugh R
&R
Ste
erin
g g
roup
R
evie
w w
ork
forc
e d
ashboard
s to a
ssure
again
st positio
n
Ta
ble
top e
sta
blis
hm
ent re
vie
w O
ct/
Nov 2
019
Sm
art
sheets
have d
eta
iled p
lan -
New
Role
s (
tNA
) P
rocess m
ap c
urr
ent
path
way
Confirm
JD
& P
spec
Cla
rify
tra
inin
g p
rogra
mm
e
Cla
rify
QIA
role
s &
Responsib
ilities
Senio
r nurs
ing s
taff d
eplo
yed t
o identifie
d a
reas to r
evie
w c
urr
ent
nurs
ing p
ractice a
nd c
are
deliv
ery
. D
eplo
ym
ent of senio
r sta
ff t
o w
ard
s id
entifie
d.
Qualit
y im
pro
vem
ent
appro
ach o
f th
e t
hem
es to a
ddre
ss a
ctio
ns f
orm
CQ
C inspectio
n, com
pla
ints
and
incid
ents
C
om
ple
te N
urs
e E
sta
blis
hm
ent
revie
w b
ased o
n n
atio
nal guid
ance
La
test
Mo
nth
P
rog
ress
Contr
act bookin
g for
RN
agency t
o s
upport
fill
rate
on d
ay s
hifts
during w
inte
r pre
ssure
d m
onth
s s
tart
ed w
/c 1
8/1
1/1
9-
appro
xim
ate
ly 2
0 W
TE
. T
able
top e
sta
blis
hm
ent
revie
ws h
ave c
om
menced.
TB
206_
19 R
isk
Reg
iste
r D
ec 1
9
Page 136 of 210

Pa
ge
8 o
f 1
4
Str
ate
gic
Ob
jecti
ve
SO
1 -
Im
pro
ve c
linic
al outc
om
es a
nd p
atie
nt safe
ty to e
nsure
we d
eliv
er
hig
h q
ualit
y s
erv
ices S
O2 -
Deliv
er
serv
ices t
hat m
eet N
HS
constitu
tio
nal
and r
egula
tory
sta
ndard
s S
O3 -
Effic
iently a
nd p
roductively
pro
vid
e c
are
within
agre
ed fin
ancia
l lim
its S
O4 -
Develo
p a
fle
xib
le,
responsiv
e
work
forc
e o
f th
e r
ight siz
e a
nd w
ith t
he r
ight skill
s w
ho feel valu
ed a
nd m
otivate
d S
O5 -
Enable
all
sta
ff t
o b
e p
atie
nt-
cente
red le
aders
build
ing o
n
an o
pen a
nd h
onest culture
and t
he d
eliv
ery
of
the T
rust valu
es S
O6 -
Engage s
trate
gic
part
ners
to m
axim
ise t
he o
pport
unitie
s to d
esig
n a
nd
deliv
er
susta
inable
serv
ices for
the p
opula
tio
n o
f S
outh
port
, F
orm
by a
nd W
est Lancashire
Lin
k t
o B
AF
Op
en
ed
ID
AD
O/E
xec L
ead
Ris
k L
ead
Tit
le
19/0
9/2
018
1902
Directo
r of N
urs
ing &
Qualit
y
Brid
get
Lees
Fa
ilure
to c
om
ply
& im
pro
ve g
overn
ance o
f serv
ices in
rela
tio
n to t
he a
reas o
f non-c
om
plia
nce id
entified b
y
CQ
C
Descri
pti
on
If w
e f
ail
to c
om
ply
with r
egula
tory
fra
me
work
then t
his
will
result in
bre
ach o
f th
e T
rust re
gula
tio
n a
nd p
ote
ntia
l le
gal
actio
n,
poor
patie
nt
experie
nce, unsafe
and p
oor
qualit
y o
f care
, and lack o
f public
confid
ence in t
he T
rust
Co
ntr
ols
enhanced t
eam
to s
upport
DoN
deliv
er
expecta
tio
ns
Imp
rovem
ent
pla
ns d
evelo
ped a
nd a
gre
ed w
ith tru
st B
oard
Im
pro
vem
ent
gro
ups d
evelo
ped a
cro
ss T
rusts
, in
clu
din
g C
BU
s
Identifie
d E
xecutive a
nd m
anagem
ent
leads f
or
Perf
orm
ance, qualit
y, people
and u
se o
f re
sourc
es
develo
pm
ent of a s
hare
d d
rive t
o e
nable
evid
ence t
o b
e u
plo
aded
develo
pm
ent of aw
are
ness r
ais
ing a
nd p
repara
tion
for
key le
aders
at B
oard
and C
BU
level
identifie
d s
upport
fro
m P
MO
with p
roje
ct m
anagem
ent
Well-
led w
ork
ongoin
g w
ith A
QU
A
PIR
com
ple
ted a
nd s
ubm
itte
d 0
3.0
5.1
9
Board
Info
rma
tio
n P
acks d
evelo
ped a
nd E
xecutive a
nd N
on-E
xecutive C
oachin
g p
lanned
Sta
ff a
ware
ness b
ookle
ts d
istr
ibute
d
Depart
me
nta
l aw
are
ness s
essio
ns p
lanned f
or
all
sta
ff
Use o
f R
esourc
es p
lannin
g p
repara
tio
n le
t by I
nte
rim
Tu
rn A
round D
irecto
r
Fa
ctu
al A
ccura
cy C
heckin
g C
om
ple
ted a
nd s
ubm
itte
d w
ithin
tim
escale
s a
nd s
igned o
ff b
y I
nte
rim
Chie
f E
xecutive
Gap
s i
n C
on
tro
ls
CQ
C id
entifie
d 9
6 M
US
T A
ND
SH
OU
LD
DO
actio
ns f
ollo
win
g
Novem
ber
and D
ecem
ber
2017 inspectio
n
Lack o
f pace a
nd a
ssura
nce r
egard
ing p
rogre
ss o
f actio
n p
lan
Ris
k L
evels
L
ikelih
oo
d
Co
ns
eq
ue
nce
Ris
k R
ati
ng
(I
nit
ial)
Ris
k R
ati
ng
(C
urr
en
t)
Ris
k L
evel
(Cu
rren
t)
Ris
k R
ati
ng
(T
arg
et)
R
isk L
evel (T
arg
et)
D
ate
of
La
st
Revie
w
Date
of
Next
Revie
w
Lik
ely
(4)
Ma
jor
(4)
16
16
Extr
em
e r
isk
12
Hig
h R
isk
18/1
1/2
019
23/1
2/2
019
Assu
ran
ce
com
mitte
e s
tructu
re
regula
r engagem
ent
me
etin
gs
assura
nce a
t qualit
y a
nd s
afe
ty &
com
mitte
e
CB
U m
onth
ly g
overn
ance m
eetin
gs
develo
pm
ent of a s
ingle
qualit
y im
pro
vem
ent
actio
n p
lan
engage a
nd g
ain
support
for
valid
atio
n f
rom
HealthW
atc
h,
CC
G a
nd o
ther
regula
tors
C
ore
serv
ice r
evie
w id
entifie
d s
om
e a
reas o
f im
pro
vem
ent
inclu
din
g o
penness o
f sta
ff, S
taff a
re c
arin
g,
com
passio
nate
and there
are
exam
ple
s o
f good p
ractice, sta
bili
ty o
f le
aders
hip
and n
o a
reas w
ere
consid
ere
d to b
e ‘in
adequate
’ on b
oth
days
Inte
rnal assura
nce p
anels
F
ollo
win
g s
ubm
issio
n o
f P
IR -
Pre
para
tio
n P
lan U
pdate
d a
nd K
LO
Es id
entifie
d
QID
Me
etin
g re
-esta
blis
hed
First unannounced inspectio
n w
/c 0
8.0
7.1
9
Second u
nannounced in
spectio
n w
/c 3
0.0
7.1
9
Me
dic
ines m
anagem
ent im
pro
vem
ent
pla
n d
evelo
ped &
agre
ed w
ith N
HS
E &
I &
share
d w
ith C
QC
Lett
er
subm
itte
d to C
QC
id
entify
ing im
pro
vem
ents
ma
de s
ince in
spectio
ns
Fa
ctu
al A
ccura
cy C
heckin
g C
om
ple
ted a
nd s
ubm
itte
d w
ithin
tim
escale
s a
nd s
igned o
ff b
y I
nte
rim
Chie
f E
xecutive
Gap
s i
n A
ssu
ran
ce
Engagem
ent
of key le
aders
fro
m 'w
ard
to b
oard
' re
duced u
nders
tandin
g o
f expecta
tio
ns o
f re
gula
tor
prio
r, d
urin
g
and a
fter
inspectio
ns
A n
um
ber
of
gaps id
entifie
d d
urin
g c
ore
serv
ices r
evie
w, th
ese
are
bein
g a
ddre
ssed t
hro
ugh Q
ualit
y Im
pro
vem
ent P
lan.
C
QC
Inspectio
n J
uly
id
entifie
d issues w
ith M
edic
ines
Ma
nagem
ent, M
CA
/ D
oLs a
nd o
ther
are
as f
or
furt
her
impro
vem
ent
F
eedback r
eceiv
ed fro
m C
QC
facili
tie
s f
ocus g
roup h
ighlig
htin
g
dis
conte
nt
in team
and issues w
ith c
ulture
and c
om
mu
nic
atio
n
Acti
on
Pla
n
Incorp
ora
te a
ny R
ed M
ust
Do A
ctions into
CB
U R
isk R
egis
ter
M
onitor
facili
ties f
ocus g
roup a
ction p
lan t
hro
ugh q
ualit
y a
ssura
nce p
anels
A
cti
on
Pla
n D
ue
Date
17/0
7/2
019
28/0
2/2
020
A
cti
on
Pla
n R
ati
ng
Com
ple
ted
Little o
r N
o
Page 137 of 210

Pa
ge
9 o
f 1
4
Fa
ctu
al accura
cy t
o b
e c
om
ple
ted w
ithin
agre
ed tim
e s
cale
s o
f 10 d
ays.
w
ork
with c
om
munic
atio
ns team
to e
ngage w
idely
with s
taff
develo
p t
rain
ing f
or
sta
ff a
cro
ss t
he o
rganis
atio
n
Key le
aders
to a
ccess tra
inin
g w
ith le
ad C
QC
executive/m
anager
Esta
blis
h c
onfirm
and c
halle
nge s
essio
ns for
each a
ctio
n a
nd c
ore
serv
ice t
o e
xpedite p
rogre
ss a
gain
st
actio
n P
lan,
and lo
ok a
t re
-esta
blis
hin
g t
he Q
ualit
y Im
pro
vem
ent D
evelo
pm
ent
(QID
)Gro
up
To
deliv
er
again
st th
e 9
6 M
US
T a
nd S
HO
ULD
DO
CQ
C r
ecom
me
ndatio
ns o
utlin
ed in
the o
vera
rchin
g
CQ
C A
ctio
n P
lan.
29/1
1/2
019
30/0
9/2
019
28/0
6/2
019
22/1
0/2
019
29/1
1/2
019
Pro
gre
ss M
ade
Com
ple
ted
Com
ple
ted
Com
ple
ted
Actio
ns A
lmost
Com
ple
ted
Mo
dera
te
Pro
gre
ss M
ade
La
test
Mo
nth
P
rog
ress
Th
e T
rust
is c
urr
ently a
waitin
g the C
QC
report
whic
h is e
xpecte
d b
y the e
nd o
f N
ovem
ber.
Th
is r
isk w
ill b
e u
pdate
d o
n r
eceip
t of th
is r
eport
.
TB
206_
19 R
isk
Reg
iste
r D
ec 1
9
Page 138 of 210

Pa
ge
10
of
14
Str
ate
gic
Ob
jecti
ve
SO
1 -
Im
pro
ve c
linic
al outc
om
es a
nd p
atie
nt safe
ty to e
nsure
we d
eliv
er
hig
h q
ualit
y s
erv
ices S
O2 -
Deliv
er
serv
ices t
hat m
eet N
HS
constitu
tio
nal
and r
egula
tory
sta
ndard
s S
O3 -
Effic
iently a
nd p
roductively
pro
vid
e c
are
within
agre
ed fin
ancia
l lim
its S
O6 -
Engage s
trate
gic
part
ners
to
ma
xim
ise t
he o
pport
unitie
s to d
esig
n a
nd d
eliv
er
susta
inable
serv
ices for
the p
opula
tio
n o
f S
outh
port
, F
orm
by a
nd W
est
Lancas
hire
Lin
k t
o B
AF
Op
en
ed
ID
AD
O/E
xec L
ead
Ris
k L
ead
Tit
le
13/0
6/2
019
2052
Directo
r of N
urs
ing &
Qualit
y
Me
gan L
angle
y
Old
er
People
s C
are
Descri
pti
on
If there
is c
ontin
ued p
oor
qualit
y c
are
deliv
ere
d in p
art
icula
r to
old
er
people
in
South
port
& O
rmskirk N
HS
Tru
st, c
ontin
ue t
hen h
arm
may b
e c
aused to o
ur
old
er
patie
nts
im
pactin
g n
egatively
on their
qualit
y o
f lif
e, fu
nctio
n a
nd e
xperience. T
he a
reas o
f concern
rela
te to s
pecific
pra
ctices:
•Deconditio
nin
g o
f patie
nts
•T
he in
appro
pria
te u
se o
f bed r
ails
•P
oor
mo
uth
care
•P
oor
nutr
itio
n a
ssessm
ent
and m
anagem
ent
•Poor
hydra
tio
n m
anagem
ent
•Poor
contin
ence a
ssessm
ent
and m
anagem
ent
•Lack o
f in
tera
ctio
n a
nd s
ocia
l/cognitiv
e s
tim
ula
tion in
cre
asin
g c
onfu
sio
n a
nd d
elir
ium
•
A lack o
f educatio
n a
nd tra
inin
g s
pecific
ally
in c
arin
g f
or
old
er
people
•
A lack o
f end o
f lif
e c
are
education s
trate
gy w
ithin
the T
rust
•Lim
ited a
vaila
bili
ty o
f G
eria
tric
ians to p
rovid
e h
olis
tic c
om
pre
hensiv
e a
ssessm
ent
and a
dvanced c
are
ma
nagem
ent
pla
ns for
pa
tie
nts
in a
dditio
n t
o lim
ited c
linic
al support
for
the F
railt
y P
ractitio
ners
•I
nabili
ty to d
ischarg
e p
atie
nts
hom
e d
ue to lack o
f re
sourc
e t
o s
upport
at hom
e p
art
icula
rly c
are
and r
ehabili
tatio
n p
rovis
ions in t
he c
om
mu
nity
•Poorly e
sta
blis
hed p
ath
way for
patie
nts
with s
pin
al fr
actu
res
•An e
nvironm
ent
not conduciv
e to s
tim
ula
ting p
eople
and e
nablin
g t
hem
to m
ain
tain
and m
axim
ise their f
unctio
n
•Th
e la
ck o
f a form
ally
agre
ed f
railt
y p
ath
way a
nd m
odel
Co
ntr
ols
R
ed2G
reen r
olle
d o
ut
- T
hera
py d
evelo
pin
g a
com
pete
ncy a
nd t
rain
ing f
or
sta
ff to b
e e
quip
ped t
o c
hair a
nd
challe
nge in a
consis
tent
way s
usta
inin
g t
he R
ed2G
reen p
rincip
les a
t board
rounds a
cro
ss t
he T
rust.
N
utr
itio
n -
New
polic
y a
ppro
ved, N
ew
E-le
arn
ing m
odule
pro
vid
ed to R
Ns o
n w
ard
10B
with n
ew
care
pla
ns
bein
g t
este
d -
in
additio
n t
o t
his
, additio
nal D
iete
tic s
upport
is b
ein
g o
ffere
d t
o t
his
ward
while
they
imple
me
nt th
e n
ew
pra
ctices. B
usin
ess I
nte
llig
ence a
re w
ork
ing o
n a
new
colle
ctio
n o
f K
PIs
to m
easure
and m
onitor
impro
vem
ent.
Mo
uth
Care
- 5 s
taff c
om
ple
ted M
outh
Care
Matt
ers
Tra
in t
he T
rain
er
pro
gra
mm
e-
curr
ently d
evelo
pin
g
new
polic
y, care
pla
ns a
nd p
roduct
availa
bili
ty.
Dem
entia
& D
elir
ium
- N
ew
cognitiv
e r
isk a
ssessm
ent and c
are
pla
n b
ein
g t
ria
led o
n 6
ward
s w
ith n
ew
patie
nt
info
rma
tio
n le
afle
ts a
nd r
eport
ing o
f F
AIR
natio
nally
on a
new
pro
form
a a
s t
he s
cre
enin
g t
ool has
been c
hanged. T
his
is b
ein
g r
evie
wed a
fter
1 m
onth
(end o
f June)
for
any a
me
ndm
ents
and f
urt
her
roll
out.
F
alls
- 6
ward
s u
sin
g n
ew
ris
k a
ssessm
ent, c
are
pla
n a
nd d
aily
checklis
t w
ith n
ew
e-le
arn
ing m
odule
accessib
le to s
taff f
or
com
ple
tio
n. T
his
is b
ein
g r
evie
wed a
fter
1 m
onth
(end o
f June)
for
any a
me
ndm
ents
and f
urt
her
roll
out.
B
edra
ils-
6 w
ard
s tria
ling n
ew
ris
k a
ssessm
ent, c
are
pla
n a
nd d
aily
check -
bein
g r
evie
wed a
fter
1 m
onth
(e
nd o
f June)
for
any a
me
ndm
ents
and f
urt
her
roll
out. (
Educatio
n inclu
ded in
falls
e-le
arn
ing m
odule
) F
railt
y T
eam
deliv
erin
g s
erv
ice M
-F in
AE
D a
nd in
-reachin
g -
contin
uin
g t
o w
ork
on c
om
pete
ncie
s
part
icula
rly a
round C
GA
com
ple
tion.
As p
art
of th
e R
ed2G
reen, E
ndP
Jpara
lysis
Get
Up,
Get
Dre
ssed, K
eep M
ovin
g w
as in
troduced -
this
will
be f
orm
ally
la
unched a
s a
pro
ject
in J
uly
as p
art
of th
e T
rust's
QI
work
.
Gap
s i
n C
on
tro
ls
Care
pla
ns n
ot alw
ays u
sed a
ppro
pria
tely
and n
ot all
care
pla
ns
are
appro
pria
te -
these a
re b
ein
g r
evie
wed b
y t
he d
ocum
enta
tio
n
gro
up
F
alls
and b
ed r
ails
new
ris
k a
ssessm
ent and c
are
pla
ns in 6
w
ard
s b
ein
g t
riale
d -
need to c
ontinue r
oll-
out.
Inabili
ty to c
onsis
tently s
taff a
dditio
nal care
bay
Tra
inin
g f
or
sta
ff r
e:
old
er
people
ris
ks n
ot curr
ently p
rovid
ed -
N
ew
Tra
inin
g P
rogra
mm
e t
o b
e launched e
nd o
f July
. E
nvironm
ent
not conduciv
e to r
eablin
g p
atie
nts
and m
ain
tain
ing
functio
n, socia
l in
tera
ctio
n o
r orie
nta
tio
n.
Environm
ent
not
wholly
adapte
d f
or
additio
nal/enhanced c
are
needs e
g d
em
entia
Lack o
f unders
tandin
g o
f th
e im
pact of
patie
nts
rem
ain
ing in b
ed,
in p
ads, w
ith c
ot sid
es, not eatin
g/d
rin
kin
g -
New
Tra
inin
g
Pro
gra
mm
e to b
e la
unched e
nd o
f July
. Lack o
f path
way/s
erv
ice a
vaila
bili
ty to s
upport
patie
nts
with
enhanced n
eeds r
etu
rnin
g h
om
e-
i.e. la
ck o
f 24hour
care
in
com
mu
nity to s
tep d
ow
n -
Work
underw
ay w
ith C
CG
, C
om
mu
nity
and L
A c
olle
agues t
o r
edesig
n p
ath
way,
Hom
efirs
t and
Delir
ium
/Dem
entia
. N
ot
yet com
me
nced m
outh
care
roll-
out
Docum
enta
tio
n n
ot conduciv
e to p
rovid
ing p
ers
on
-centr
ed c
are
, th
is is to b
e r
evie
wed a
s a
n e
ntity
July
2019 (
part
icula
rly c
are
pla
ns a
nd r
isk a
ssessm
ents
) C
linic
al superv
isio
n f
or
the fra
ilty team
lackin
g-
explo
rin
g u
se o
f Leeds B
uddy a
rrangem
ent to
support
. C
ontin
ence p
roje
ct not yet com
menced
- scopin
g s
essio
n 2
5/6
/19
to p
lan im
pro
vem
ent
work
Page 139 of 210

Pa
ge
11
of
14
Ris
k L
evels
L
ikelih
oo
d
Co
ns
eq
ue
nce
Ris
k R
ati
ng
(I
nit
ial)
Ris
k R
ati
ng
(C
urr
en
t)
Ris
k L
evel
(Cu
rren
t)
Ris
k R
ati
ng
(T
arg
et)
R
isk L
evel (T
arg
et)
D
ate
of
La
st
Revie
w
Date
of
Next
Revie
w
Lik
ely
(4)
Ma
jor
(4)
16
16
Extr
em
e r
isk
8
Hig
h R
isk
18/1
1/2
019
18/1
2/2
019
Assu
ran
ce
CQ
C R
evie
w
G
ap
s i
n A
ssu
ran
ce
Need t
o d
evelo
p in
tern
al assura
nce o
f im
pro
ved q
ualit
y a
round
all
dom
ain
s lis
ted in t
he h
azard
. N
eed t
o d
evelo
p a
ctio
n p
lan a
nd
RA
G r
ate
, id
entify
pro
jects
and le
ads for
the im
pro
vem
ents
whic
h
have b
een id
entifie
d.
Need t
o c
om
mence a
udits o
f old
er
people
incid
ents
, harm
, im
pact
of
adm
issio
n, causes o
f 'red d
ays' and d
ela
ys b
etw
een
bein
g f
it t
o le
ave a
nd le
avin
g h
ospital.
Acti
on
Pla
n
Esta
blis
h a
nd d
evelo
p s
taff k
now
ledge,
focus a
nd e
ducatio
n o
n p
atient
functio
n. E
nsu
re a
ppro
pria
te
equip
me
nt
availa
ble
, develo
p r
esourc
e b
oxes s
pecific
ally
for
patie
nts
with c
ognitiv
e im
pairm
ent, d
evelo
p
actio
n p
lanners
for
engagin
g a
nd s
tim
ula
tin
g a
ctivitie
s o
n the w
ard
s.
Fa
lls p
olic
y e
xpired.
Fa
lls E
ducatio
n n
ot
esta
blis
hed/p
rovid
ed.
Falls
docum
enta
tio
n r
evie
w.
Fa
lls r
eport
ing a
nd K
PIs
to b
e r
evie
wed.
Fa
lls s
trate
gy to b
e d
evelo
ped.
Pre
vio
us p
olic
y for
nutr
itio
n s
cre
enin
g d
id n
ot com
ply
with b
est
pra
ctice o
r natio
nal guid
ance. P
ractices
there
fore
did
not alig
n e
ither.
E
sta
blis
h T
rain
ing P
rogra
mm
e f
or
Old
er
People
s C
are
M
outh
Care
pro
vis
ion o
f care
- r
evie
w o
f polic
y, care
pla
n,
educatio
n a
nd c
are
pro
vis
ion r
equired.
Esta
blis
h a
clin
ical path
way a
nd p
ractice for
the a
ssessm
ent and m
anagem
ent
of contin
ence f
or
patie
nts
. T
his
will
in
volv
e w
ritin
g a
path
way/p
olic
y, care
pla
ns, educatio
n p
ackage a
nd c
ham
pio
ns o
n t
he w
ard
s w
ith
a r
oll
out pla
n for
the n
ew
pra
ctices.
To
esta
blis
h a
path
way f
or
adults in t
he a
cute
sett
ing t
o p
rovid
e tim
ely
scre
enin
g f
or
delir
ium
/dem
entia
, ask
the c
ase fin
din
g q
uestio
n,
ensure
appro
pria
te f
urt
her
assessm
ent, c
are
, fo
llow
-up a
nd s
upport
for
the
patie
nt, c
are
r and f
am
ily. T
o e
nable
this
- p
rovid
e s
taff t
he a
ppro
pria
te e
ducatio
n.
Acti
on
Pla
n D
ue
Date
28/0
2/2
020
31/0
1/2
020
30/0
4/2
020
31/1
2/2
019
31/0
3/2
020
31/0
3/2
020
28/0
2/2
020
Acti
on
Pla
n R
ati
ng
Mo
dera
te
Pro
gre
ss M
ade
Actio
ns A
lmost
Com
ple
ted
Actio
ns A
lmost
Com
ple
ted
Com
ple
ted
Mo
dera
te
Pro
gre
ss M
ade
Mo
dera
te
Pro
gre
ss M
ade
Mo
dera
te
Pro
gre
ss M
ade
La
test
Mo
nth
P
rog
ress
Date
s h
ave b
een s
et fo
r 2020 f
or
the O
lder
People
’s C
are
Tra
inin
g P
rogra
mm
e.
Falls
ris
k a
ssessm
ent and c
are
bundle
on a
ll w
ard
s e
xcept
Inte
nsiv
e C
are
and w
ill b
e in
Inte
nsiv
e C
are
by t
he e
nd o
f N
ovem
ber,
when the o
ld c
are
pla
ns w
ill b
e r
em
oved fro
m t
he in
tranet. T
he n
ew
post-
falls
assessm
ent
is s
till
bein
g t
este
d o
n 2
ward
s w
ith the in
tentio
n o
f la
unchin
g o
n a
ll w
ard
s a
t th
e e
nd o
f N
ovem
ber.
A F
alls
report
ing d
ashboard
is b
ein
g d
evelo
ped, fo
llow
ing t
his
the d
ata
will
need t
o b
e r
evie
wed a
nd t
hen c
leansed.
Th
e F
alls
Str
ate
gy w
as r
evie
wed a
t N
MG
and f
ollo
win
g a
few
am
endm
ents
will
be a
ppro
ved a
nd la
unched in
the f
orm
of an 'I
mp
rovem
ent P
lan' by the e
nd o
f N
ovem
ber.
Th
e D
em
entia
resourc
e b
oxes a
re b
ein
g d
iscussed w
ith p
rocure
me
nt
and in
fectio
n c
ontr
ol,
once a
gre
ed a
charita
ble
funds b
id w
ill b
e c
reate
d t
o m
ake the p
urc
hases.
Th
ese w
ill then b
e u
sed in c
onju
nctio
n w
ith the a
ctivity p
lanners
and the e
ndP
Jpara
lysis
in
itia
tive to
get patie
nts
up,
dre
ssed
and m
ovin
g. T
his
pie
ce o
f w
ork
has b
een initia
ted o
n o
ne w
ard
and a
roll
out pla
n is b
ein
g d
evelo
ped.
Dem
entia
and D
elir
ium
Te
am
appro
ved in b
usin
ess c
ase,
one m
em
ber
in p
ost, A
dm
iral N
urs
e t
o
sta
rt 1
6/1
2/1
9 a
nd fin
al post to
com
mence b
efo
re e
nd o
f F
ebru
ary
2020.
Te
am
com
mencin
g im
media
te w
ork
on id
entify
ing c
ognitiv
e im
pairm
ent, a
nd r
olli
ng o
ur
risk a
ssessm
ent and c
are
pla
n -
this
is
in a
ll are
as w
ith t
he e
xceptio
n o
f In
tensiv
e C
are
and w
ill b
e in
all
are
as b
y the e
nd o
f N
ovem
ber
2019. 8 M
em
bers
of sta
ff h
ave n
ow
com
ple
ted t
he H
ealth E
ducatio
n E
ngla
nd T
rain
the T
rain
er
cours
e
for
Mo
uth
Care
. T
he p
roje
ct te
am
are
testin
g the n
ew
assessm
ent, e
ducatio
n, care
pla
n a
nd p
roduct
range o
n w
ard
14B
with a
roll-o
ut
pla
n e
sta
blis
hed for
the r
em
ain
ing w
ard
s. E
ducatio
n b
ein
g
pro
vid
ed a
t w
ard
le
vel durin
g w
ard
out
and a
lso m
onth
ly o
n t
he O
lder
People
s C
are
Tra
inin
g P
rogra
mm
e.
Refr
esh o
f th
e C
ontin
ence p
roje
ct is
underw
ay w
ith n
ew
focus o
f ta
rgetin
g o
ne w
ard
(7A
&B
)
to t
est new
range o
f pro
ducts
, assessm
ent, c
are
pla
n a
nd o
nw
ard
refe
rral/path
way.
Dem
onstr
able
im
pro
vem
ent on d
ashboard
for
MU
ST
scre
enin
g feedback to the w
ard
. F
urt
her
roll-
out
now
bein
g
schedule
d a
s t
he n
ew
Die
tetic le
ad h
as c
om
me
nced in
post and is p
rio
ritisin
g t
his
pie
ce o
f w
ork
. P
rio
r to
furt
her
roll-o
ut how
ever
their inte
ntio
n is to tw
eak the c
are
pla
n to a
lign a
gain
to b
est
pra
ctice
and t
he n
ew
tem
pla
tes b
ein
g u
sed o
n t
he w
ard
s c
urr
ently. S
taff a
re r
eceiv
ing e
ducatio
n o
n t
he O
lder
People
s C
are
Tra
inin
g P
rogra
mm
e a
nd a
TN
A is u
nde
rway to a
dd t
he e
-le
arn
ing m
odule
for
BA
PE
N N
utr
itio
n t
o a
ppro
pria
te p
rofile
s f
or
sta
ff t
o c
om
mence c
om
ple
tio
n.
TB
206_
19 R
isk
Reg
iste
r D
ec 1
9
Page 140 of 210

Pa
ge
12
of
14
Str
ate
gic
Ob
jecti
ve
SO
1 -
Im
pro
ve c
linic
al outc
om
es a
nd p
atie
nt safe
ty to e
nsure
we d
eliv
er
hig
h q
ualit
y s
erv
ices S
O3 -
Effic
iently a
nd p
roductively
pro
vid
e c
are
w
ithin
agre
ed fin
ancia
l lim
its S
O4 -
Develo
p a
fle
xib
le,
responsiv
e w
ork
forc
e o
f th
e r
ight siz
e a
nd w
ith the r
ight skill
s w
ho feel valu
ed a
nd
mo
tivate
d S
O6 -
Engage s
trate
gic
part
ners
to m
axim
ise t
he o
pport
unitie
s t
o d
esig
n a
nd d
eliv
er
susta
inable
serv
ices for
the p
opula
tio
n o
f S
outh
port
, F
orm
by a
nd W
est
Lancashire
Lin
k t
o B
AF
Op
en
ed
ID
AD
O/E
xec L
ead
Ris
k L
ead
Tit
le
13/1
1/2
017
1688
Chie
f O
pera
tin
g O
ffic
er
Ma
ndy M
ars
h
Inadequate
Sta
ffin
g L
evels
in A
naesth
etic D
epart
me
nt
Descri
pti
on
Sta
ffin
g L
evels
of
anaesth
etic d
epart
me
nt
aff
ectin
g c
apacity a
nd s
afe
ty o
f em
erg
ency/IC
U/M
ate
rnity c
over.
Lack o
f em
erg
ency c
over
for
on c
all
/ IC
U / m
ate
rnity b
oth
sites. T
his
would
result in t
he c
losure
of
hig
h r
isk p
atie
nts
pre
sentin
g to A
&E
for
both
adult a
nd c
hild
ren a
nd the inabili
ty t
o s
taff IT
U.
Co
ntr
ols
In
tern
al/exte
rnal Locum
s a
naesth
etists
to c
over
short
fall
caused b
y v
acancie
s
People
to w
ork
additio
nal hours
to fill
extr
a s
essio
ns
Ele
ctive lis
ts c
ancelle
d to e
nsure
cover
when n
eeded
Change t
o o
n-c
all
syste
m to e
nsure
full
covera
ge;
1st on c
all
onsite &
2nd o
n c
all
support
ing w
ithin
core
hours
In
terim
support
fro
m s
taff p
ain
managem
ent short
fall
Agency locum
s b
ein
g s
ought to
support
gaps
Gap
s i
n C
on
tro
ls
Availa
bili
ty o
f sta
ff t
o c
over
vacant shifts
at a m
inim
um
due to
burn
out/
sic
kness/a
nnual le
ave
Lack o
f agency s
taff
within
capped r
ate
10 v
acancie
s r
em
ain
in s
erv
ice
1 c
onsultant taken o
ut of core
theatr
e s
essio
ns t
o r
un p
ain
activity;
back fill
ing those s
essio
ns w
ith W
LI's
whic
h h
as b
een
appro
ved t
o the e
nd o
f th
e y
ear
by S
S
Ris
k L
evels
L
ikelih
oo
d
Co
ns
eq
ue
nce
Ris
k R
ati
ng
(I
nit
ial)
Ris
k R
ati
ng
(C
urr
en
t)
Ris
k L
evel
(Cu
rren
t)
Ris
k R
ati
ng
(T
arg
et)
R
isk L
evel (T
arg
et)
D
ate
of
La
st
Revie
w
Date
of
Next
Revie
w
Lik
ely
(4)
Cata
str
ophic
(5)
20
20
Extr
em
e r
isk
5
Mo
dera
te r
isk
13/1
1/2
019
13/1
2/2
019
Assu
ran
ce
Mo
nth
ly P
lanned C
are
govern
ance m
eetin
gs
PC
ris
k r
evie
w m
eetin
g w
ith A
DO
/HoN
Gap
s i
n A
ssu
ran
ce
Acti
on
Pla
n
Revie
win
g jo
b d
escrip
tio
ns to b
e in lin
e w
ith n
atio
nal re
quirem
ents
. C
ontin
ue t
o a
dvert
ise to r
ecru
it t
o p
osts
. W
ork
forc
e s
trate
gy m
eetings s
et up w
ith C
OO
& M
D in
support
to
addre
ss. 1st m
eetin
g h
eld
on 0
6/1
1/1
8 w
ith t
he n
ext m
eetin
g s
chedule
d f
or
29/1
1/1
8. T
eam
are
actively
seekin
g s
olu
tio
ns t
o a
ddre
ss g
aps in
the w
ork
forc
e a
nd lo
okin
g a
t new
ways o
f w
ork
ing t
o b
oth
the o
n c
all
rota
(s)
and s
taff
ing e
sta
blis
hm
ent.
Update
29.0
1.1
9 -
Busin
ess c
ase c
urr
ently w
ith f
inance follo
win
g w
ork
forc
e r
evie
w.
Imp
lem
ent
new
ways
of
work
ing u
sin
g s
upport
sta
ff to m
ain
tain
safe
sta
ffin
g levels
and r
obust successio
n p
lan in
vie
w o
f extr
em
e r
ecru
itm
ent and r
ete
ntio
n issues.
12.0
2.1
9 -
Busin
ess C
ase p
resente
d a
t B
DIS
C, fo
r H
MB
next w
eek. If
appro
ved,
recru
itm
ent
drive to
advert
ise/a
ppoin
t to
posts
- f
ore
cast 6 m
onth
s t
o r
ecru
it -
full
qualif
icatio
n o
f som
e s
taff in
post w
ill b
e 2
years
. A
wait o
utc
om
e o
f H
MB
next w
eek.
17.0
4.1
9 S
till
aw
aitin
g fin
al appro
val
Update
;16.0
5.1
9 -
Busin
ess c
ase for
fin
al sig
n o
ff a
t H
MB
on 2
2.0
5.1
9
Update
01.0
7.1
9 -
still
aw
aitin
g f
inal sig
n o
ff -
back t
o H
MB
B
usin
ess c
ase a
ppro
ved a
nd a
ll advert
s w
ill g
o o
ut.
Acti
on
Pla
n D
ue
Date
18/1
2/2
017
13/1
2/2
019
Acti
on
Pla
n R
ati
ng
Com
ple
ted
Mo
dera
te
Pro
gre
ss M
ade
La
test
Mo
nth
P
rog
ress
Recru
ited to 1
substa
ntive C
onsultant
and 2
Tru
st
locum
Consultant fixed term
posts
. S
ubsta
ntive c
om
me
nced 1
1.1
1.1
9 a
nd 1
of th
e T
rust lo
cum
s c
om
menced o
n 0
4.1
1.1
9.
Th
e 3
rd T
rust
locum
was
only
appoin
ted 1
2/1
1 (
inte
rnal),
but
this
will
cre
ate
a furt
her
SA
S D
r post. W
e h
ave a
ppoin
ted 3
x S
AS
Dr's a
nd p
re -
em
plo
ym
ent checks u
nderw
ay.
We s
till
have 3
x I
CU
Consultant and 1
Pain
M
anagem
ent vacancie
s, 3 x
SA
S D
r V
acancie
s a
nd 1
Clin
ical F
ello
w.
Th
e r
isk is t
o r
em
ain
extr
em
e u
ntil all
posts
are
recru
ited
to a
s the I
CU
ele
me
nt is
still
extr
em
e.
Page 141 of 210

Pa
ge
13
of
14
Str
ate
gic
Ob
jecti
ve
SO
3 -
Effic
iently a
nd p
roductively
pro
vid
e c
are
within
agre
ed f
inancia
l lim
its
Lin
k t
o B
AF
Op
en
ed
ID
AD
O/E
xec L
ead
Ris
k L
ead
Tit
le
15/0
1/2
019
1942
Directo
r of F
inance
Ste
ve S
hanahan
Era
dic
atin
g t
he T
rust's
deficit b
y 2
023/2
4
Descri
pti
on
If the T
rust does n
ot re
config
ure
serv
ices a
nd in
vest in
its
infr
astr
uctu
re t
hen it w
ill n
ot m
ake s
ignific
ant fin
ancia
l im
pro
vem
ents
again
st th
e c
urr
ent
deficit. It w
ill then b
e u
nable
to c
om
ply
with N
HS
O
pera
tio
nal P
lannin
g a
nd C
ontr
actin
g G
uid
ance 2
019/2
0 w
hic
h s
tate
s that
all
Tru
st deficits s
hould
be e
radic
ate
d b
y 2
023/2
4.
Co
ntr
ols
S
yste
m B
oard
set
up t
o m
anage fin
ancia
l re
covery
of th
e h
ealth e
conom
y
Mo
nth
ly r
un r
ate
report
s,
Tru
st and C
BU
T
urn
aro
und D
irecto
r re
vie
w o
f fin
ancia
l govern
ance
PM
O in
pla
ce to a
ssis
t th
e d
rive f
or
inte
rnal effic
iencie
s id
entifie
d thro
ugh M
odel H
ospital
GIR
FT
pro
gra
mm
e c
om
me
nced w
ith f
utu
re r
oll
out to
oth
er
specia
ltie
s p
roposed
Gap
s i
n C
on
tro
ls
Fu
ture
clin
ical m
odel still
to b
e fin
alis
ed a
nd c
oste
d
Accura
cy o
f P
LIC
S a
nd M
odel H
ospital data
F
ive y
ear
fin
ancia
l re
covery
pla
n (
NH
SI to
publis
h g
uid
ance)
not
in p
lace
No W
ave 4
Capital fu
ndin
g
West Lancs C
CG
me
mb
er
of
Healthie
r Lancashire a
nd S
C
um
bria
ST
P
Ris
k L
evels
L
ikelih
oo
d
Co
ns
eq
ue
nce
Ris
k R
ati
ng
(I
nit
ial)
Ris
k R
ati
ng
(C
urr
en
t)
Ris
k L
evel
(Cu
rren
t)
Ris
k R
ati
ng
(T
arg
et)
R
isk L
evel (T
arg
et)
D
ate
of
La
st
Revie
w
Date
of
Next
Revie
w
Lik
ely
(4)
Ma
jor
(4)
16
16
Extr
em
e r
isk
8
Hig
h R
isk
16/0
9/2
019
18/1
1/2
019
Assu
ran
ce
Acute
Susta
inabili
ty P
rogra
mm
e B
oard
-curr
ently fort
nig
htly
Fin
ance P
erf
orm
ance &
Investm
ent
Com
mitte
e a
nd T
rust B
oard
-month
ly
Hospital M
anagem
ent B
oard
-mo
nth
ly
Perf
orm
ance R
evie
w B
oard
-mo
nth
ly
People
and A
ctivitie
s G
roup (
PA
G)
pro
cess in p
lace -
me
etin
g w
eekly
S
ubm
it m
onth
ly w
ork
forc
e a
nd f
inance d
ata
to N
HS
Im
pro
vem
ent
Cost Im
pro
vem
ent P
rogra
mm
e d
ata
subm
itte
d f
ort
nig
htly to N
HS
Im
pro
vem
ent
Gap
s i
n A
ssu
ran
ce
Agency s
pend/v
acancy r
ate
s
Acti
on
Pla
n
Revie
w o
f M
odel H
ospital data
to e
nsure
its
accura
cy a
nd r
ele
vance in
drivin
g T
rust effic
iency
impro
vem
ents
Update
20/8
/19 fort
nig
htly M
H m
eetin
gs in
tra
in,
with k
ey e
ffic
iency p
rogra
mm
es a
ligned
with le
ads id
entifie
d a
cro
ss t
he T
rust to
test th
e a
ssum
ptio
ns a
nd t
ake forw
ard
recom
mendatio
ns. a
s a
re
sult s
om
e d
ata
cle
ansin
g h
as take
n p
lace, specific
ally
in
pro
cure
ment
and E
SR
F
inance team
to m
odel th
e im
pact of
the p
roposed c
hange t
o t
he f
inance a
rchitectu
re to a
ssess t
he
impro
vem
ent to
the T
rust's
underlyin
g fin
ancia
l deficit.
Tru
st and C
CG
to w
ork
togeth
er
to e
sta
blis
h a
fin
ancia
l m
odel fo
r th
e r
evis
ed F
railt
y p
ath
way; th
is c
ould
th
en b
e u
sed t
o r
oll
out fo
r oth
er
serv
ices that have a
n e
lem
ent
of serv
ice p
rovis
ion o
uts
ide t
he T
rust.
O
bta
inin
g r
ele
vant in
form
atio
n, financia
l and a
ctivity fro
m the T
rust
Confirm
atio
n o
f S
cenario
s
Initia
l A
ssum
ptio
ns D
evelo
pm
ent
and C
onfirm
atio
n w
ith t
he T
rust
Agre
e s
pecia
lty c
ost str
uctu
re f
or
scenario
develo
pm
ent
Pro
duce D
em
and a
nd C
apacity (
Activity)
mo
del
Pro
duce d
eta
iled T
ravel A
naly
sis
P
roduce F
inancia
l and E
conom
ic m
odels
A
lignm
ent
of m
odels
P
repare
and s
hare
dra
ft r
eport
F
inal R
eport
Acti
on
Pla
n D
ue
Date
31/1
2/2
019
31/0
1/2
019
30/0
9/2
019
28/1
0/2
019
Acti
on
Pla
n R
ati
ng
Actio
ns A
lmost
Com
ple
ted
Com
ple
ted
Com
ple
ted
Mo
dera
te
Pro
gre
ss M
ade
La
test
Mo
nth
P
rog
ress
Work
ed w
ith t
he s
yste
m t
o p
rovid
e N
HS
E/I a
n u
pdate
on o
ur
2020/2
1 p
lan. T
he m
odelli
ng s
how
s t
hat th
e T
rust
would
need a
n £
8.5
M C
IP if
it c
ontin
ued t
o c
ontr
act w
ith t
he S
eft
on C
CG
’s o
n a
cost
basis
and a
£3.5
M C
IP if
it w
as o
n a
PbR
contr
act.
TB
206_
19 R
isk
Reg
iste
r D
ec 1
9
Page 142 of 210

Pa
ge
14
of
14
Str
ate
gic
Ob
jecti
ve
SO
3 -
Effic
iently a
nd p
roductively
pro
vid
e c
are
within
agre
ed f
inancia
l lim
its
Lin
k t
o B
AF
Op
en
ed
ID
AD
O/E
xec L
ead
Ris
k L
ead
Tit
le
22/0
7/2
019
2072
Ste
ve S
hanahan
Ste
ve S
hanahan
Fa
ilure
to a
chie
ve 2
019/2
0 f
inancia
l contr
ol to
tal
Descri
pti
on
If the T
rust fa
ils t
o a
chie
ve its
2019/2
0 f
inancia
l contr
ol (a
deficit o
f £8.2
96 m
illio
n)
then t
he T
rust could
be p
ut
into
fin
ancia
l specia
l m
easure
s a
nd it
would
lo
se n
on
-recurr
ent
PS
F (
Pro
vid
er
Susta
inabili
ty F
und)
and F
RF
(F
inancia
l R
ecovery
Fu
nd)
fundin
g o
f up t
o £
18.2
71 m
illio
n.
Th
is r
isk is lin
ked t
o R
isk I
D 1
942 -
era
dic
atin
g t
he T
rust's
deficit b
y 2
023/2
4. T
his
new
ris
k is the s
hort
-term
ris
k a
nd 1
942 is t
he lo
ng
-term
ris
k.
Co
ntr
ols
P
eople
and A
ctivitie
s G
roup (
PA
G)
Hospital M
anagem
ent B
oard
(H
MB
) P
roje
ct M
anagem
ent
Offic
e (
PM
O)
South
port
& F
orm
by C
CG
contr
act sig
ned w
ith m
axim
um
earn
ings o
f £74.9
mill
ion
Gap
s i
n C
on
tro
ls
Sig
ned c
ontr
act
with W
est Lancashire C
CG
outs
tandin
g follo
win
g
outc
om
e o
f arb
itra
tio
n
Late
st S
yste
m R
ecovery
Pla
n (
18.1
0.1
9)
show
s a
£5.0
mill
ion
unm
itig
ate
d r
isk f
or
the T
rust again
st its d
eficit c
ontr
ol to
tal of
£26.5
67m
(befo
re P
SF
and F
RF
)
Ris
k L
evels
L
ikelih
oo
d
Co
ns
eq
ue
nce
Ris
k R
ati
ng
(I
nit
ial)
Ris
k R
ati
ng
(C
urr
en
t)
Ris
k L
evel
(Cu
rren
t)
Ris
k R
ati
ng
(T
arg
et)
R
isk L
evel (T
arg
et)
D
ate
of
La
st
Revie
w
Date
of
Next
Revie
w
Lik
ely
(4)
Ma
jor
(4)
16
16
Extr
em
e r
isk
8
Hig
h R
isk
21/1
0/2
019
18/1
1/2
019
Assu
ran
ce
People
and A
ctivitie
s G
roup (
PA
G)
pro
cess in p
lace -
me
etin
g w
eekly
H
ospital M
anagem
ent B
oard
(H
MB
) m
onth
ly
Fin
ance P
erf
orm
ance &
Investm
ent
Com
mitte
e a
nd T
rust B
oard
- m
onth
ly
Subm
it m
onth
ly w
ork
forc
e a
nd f
inance d
ata
to N
HS
Im
pro
vem
ent
Cost Im
pro
vem
ent P
rogra
mm
e d
ata
subm
itte
d f
ort
nig
htly to N
HS
Im
pro
vem
ent
Acute
Susta
inabili
ty P
rogra
mm
e B
oard
- c
urr
ently fort
nig
htly
Perf
orm
ance R
evie
w B
oard
- m
onth
ly
Gap
s i
n A
ssu
ran
ce
Agency s
pend c
ontin
ues s
ignific
antly in
excess o
f N
HS
Im
pro
vem
ent
agency c
eili
ng
Recru
itm
ent
and r
ete
ntio
n issues r
esultin
g in
hig
h v
acancy r
ate
s
Unid
entifie
d C
ost Im
pro
vem
ent P
lans
Non-r
ecurr
ent
me
asure
s u
sed t
o d
eliv
er
Q1 p
ositio
n n
ot
susta
inable
goin
g in
to f
urt
her
quart
ers
.
Acti
on
Pla
n
Regula
tor
will
require m
onth
ly u
pdate
s o
n d
eliv
ery
of th
e s
yste
m r
ecovery
pla
n.
Fin
ance team
to m
odel th
e im
pact of
the p
roposed c
hange t
o t
he f
inance a
rchitectu
re to a
ssess t
he
impro
vem
ent to
the T
rust's
underlyin
g fin
ancia
l deficit.
Tru
st and C
CG
to w
ork
togeth
er
to e
sta
blis
h a
fin
ancia
l m
odel fo
r th
e r
evis
ed F
railt
y p
ath
way; th
is c
ould
th
en b
e u
sed t
o r
oll
out fo
r oth
er
serv
ices that have a
n e
lem
ent
of serv
ice p
rovis
ion o
uts
ide t
he T
rust.
R
evie
w o
f M
odel H
ospital data
to e
nsure
its
accura
cy a
nd r
ele
vance in
drivin
g T
rust effic
iency
impro
vem
ents
Update
20/8
/19 fort
nig
htly M
H m
eetin
gs in
tra
in,
with k
ey e
ffic
iency p
rogra
mm
es a
ligned
with le
ads id
entifie
d a
cro
ss t
he T
rust to
test th
e a
ssum
ptio
ns a
nd t
ake forw
ard
recom
mendatio
ns. A
s a
re
sult s
om
e d
ata
cle
ansin
g h
as taken p
lace, specific
ally
in
pro
cure
ment
and E
SR
A
Syste
m R
ecovery
Pla
n s
ubm
itte
d o
n 0
2.0
8.1
9 t
o t
he R
egula
tors
. It
was d
iscussed w
ith N
HS
I/N
HS
E o
n
06.0
8.1
9
Acti
on
Pla
n D
ue
Date
31/0
3/2
020
31/0
3/2
019
30/0
9/2
019
31/1
2/2
019
02/0
8/2
019
Acti
on
Pla
n R
ati
ng
Mo
dera
te
Pro
gre
ss M
ade
Com
ple
ted
Com
ple
ted
Actio
ns A
lmost
Com
ple
ted
Com
ple
ted
La
test
Mo
nth
P
rog
ress
Subm
itte
d a
n im
pro
vem
ent pla
n to r
educe the c
urr
ent
deficit g
ap b
y £
1.5
M in Q
3/Q
4.
Page 143 of 210

PUBLIC TRUST BOARD 4 December 2019
Agenda Item TB207/19 Report Title Vision 2020 and the Single
Improvement Plan
Executive Lead Therese Patten, Deputy Chief Executive/Director of Strategy
Lead Officer Donna Lynch, Head of PMO
Action Required
(Definitions below)
To Approve To Note
To Assure X To Receive
For Information
Executive Summary
Vision 2020 describes a number of strategic objectives which have been refined and agreed by the
Trust Board during winter 2019.
The Trust Single Improvement Plan (SIP) is the consolidated plan for all the improvement activities
that are being conducted during the year. The SIP sets out the priorities, actions and timescales that
the Trust needs to deliver to achieve its Vision. The priorities for 2019/20 are:
Quality: September rating - Amber
▪ Recognition and care of the deteriorating patient
▪ Care of the older person
▪ Infection prevention and control
▪ Medicines management
Operations: September rating - Amber
▪ Achievement of quality targets for ED, RTT, cancer and diagnostics
▪ Clinical documentation focus on accuracy, completion and safe storage
Workforce: September rating – Amber
▪ Culture – organisational development, staff engagement and Freedom to Speak Up
▪ Clinical workforce strategy to ensure the right numbers of skilled staff
Finance: September rating – Amber
▪ Deliver our control total
▪ Maximize capacity using transformative efficiency and productivity tools
Strategy: September rating - Amber
▪ Engage with partners to develop opportunities for joint working
▪ Develop an affordable, sustainable acute services model
TB
207_
19 S
ingl
e Im
prov
emen
t Pla
n D
ec 1
9
Page 144 of 210

There are nine risks rated as red with a further six rated as amber, after mitigation is in place.
The executive assurance reports are included in the paper for information purposes.
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
Strategic Objective Principal Risk
x SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
x SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
x SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
x SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
x SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
x SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
Absence of clear direction, engagement and leadership across the system is a risk to the sustainability of the Trust and will lead to declining clinical standards.
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
Caring Statutory Requirement
Effective Annual Business Plan Priority
Responsive Best Practice
Safe Service Change
Well Led
Impact (is there an impact arising from the report on any of the following?)
Compliance Legal
Engagement and Communication Quality & Safety
Equality Risk
Finance Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Board/Committee/Group)
This report will come to Trust Board on a monthly basis.
Page 145 of 210

Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
GUIDE TO ACTIONS REQUIRED (TO BE REMOVED BEFORE ISSUE):
Approve: To formally agree the receipt of a report and its recommendations OR a particular course of action
Receive: To discuss in depth a report, noting its implications for the Board or Trust without needing to formally approve
Note: For the intelligence of the Board without the in-depth discussion as above
Assure: To apprise the Board that controls and assurances are in place
For Information: Literally, to inform the Board
TB
207_
19 S
ingl
e Im
prov
emen
t Pla
n D
ec 1
9
Page 146 of 210

Page 147 of 210

TB
207_
19 S
ingl
e Im
prov
emen
t Pla
n D
ec 1
9
Page 148 of 210

Page 149 of 210

TB
207_
19 S
ingl
e Im
prov
emen
t Pla
n D
ec 1
9
Page 150 of 210

Page 151 of 210

TB
207_
19 S
ingl
e Im
prov
emen
t Pla
n D
ec 1
9
Page 152 of 210

Page 153 of 210

TB
207_
19 S
ingl
e Im
prov
emen
t Pla
n D
ec 1
9
Page 154 of 210

Page 155 of 210

TB
207_
19 S
ingl
e Im
prov
emen
t Pla
n D
ec 1
9
Page 156 of 210

Page 157 of 210

TB
207_
19 S
ingl
e Im
prov
emen
t Pla
n D
ec 1
9
Page 158 of 210

Page 159 of 210

Sin
gle
Im
pro
vem
en
t P
lan
Bo
ard
Up
date
Decem
ber
2019
So
uth
po
rt a
nd
Fo
rmb
y D
istr
ict
Ge
ne
ral H
os
pit
al
Orm
sk
irk
an
d D
istr
ict
Ge
ne
ral H
os
pit
al
No
rth
We
st
Re
gio
na
l S
pin
al
Inju
rie
s C
en
tre
TB
207_
19 S
IP P
rese
ntat
ion
Dec
19
Page 160 of 210

Sin
gle
Im
pro
ve
me
nt
Pla
n -
Ba
ck
gro
un
d
Page 161 of 210

Sin
gle
Im
pro
ve
me
nt
Pla
n –
Pri
ori
tie
s &
T
raje
cto
rie
s
we
have
a d
ream
wha
t is
impo
rtan
tho
w w
e w
ill d
o it
Tru
st V
isio
nP
rio
riti
esSt
rate
gic
Ob
ject
ives
Qu
alit
y P
rio
rity
1 -
Rec
ogn
itio
n an
d ca
re o
f th
e
dete
rio
rati
ng p
atie
nt
Qu
alit
y P
rio
rity
2 -
Car
e o
f th
e o
lder
per
son
Qu
alit
y P
rio
rity
3 -
Infe
ctio
n pr
even
tio
n an
d co
ntro
l
Qu
alit
y P
rio
rity
4 -
Med
icin
es m
anag
emen
t
SO 1
- Im
pro
ve c
linic
al o
utco
mes
and
pat
ien
t
safe
ty t
o e
nsu
re w
e de
liver
hig
h qu
alit
y
serv
ices
Op
erat
ion
s P
rio
rity
1 -
Ach
ieve
men
t o
f qu
alit
y
targ
ets
for
ED, R
TT, c
ance
r an
d di
agno
stic
s
Op
erat
ion
s P
rio
rity
2 -
Clin
ical
do
cum
enta
tio
n fo
cus
on
accu
racy
, co
mpl
etio
n an
d sa
fe s
tora
ge
SO 2
- D
eliv
er s
ervi
ces
that
mee
t N
HS
cons
titu
tio
nal a
nd r
egul
ato
ry s
tand
ards
Fin
ance
Pri
ori
ty 1
- D
eliv
er o
ur c
ont
rol t
ota
l
Fin
ance
Pri
ori
ty 2
- M
axim
ize
capa
city
usi
ng
tran
sfo
rmat
ive
effi
cien
cy a
nd p
rodu
ctiv
ity
too
ls
SO 3
- Ef
fici
entl
y an
d pr
odu
ctiv
ely
pro
vide
care
wit
hin
agre
ed f
inan
cial
lim
its
Wo
rkfo
rce
Pri
ori
ty 1
- C
ultu
re –
org
anis
atio
nal
deve
lopm
ent,
sta
ff e
nga
gem
ent
and
Free
do
m t
o
Spea
k U
p
Wo
rkfo
rce
Pri
ori
ty 2
- C
linic
al w
ork
forc
e st
rate
gy t
o
ensu
re t
he r
ight
num
bers
of
skill
ed s
taff
SO 4
- D
evel
op
a fl
exib
le, r
espo
nsiv
e
wo
rkfo
rce
of
the
righ
t si
ze a
nd w
ith
the
righ
t
skill
s w
ho f
eel v
alue
d a
nd m
oti
vate
d
SO 5
- E
nabl
e al
l sta
ff t
o b
e pa
tien
t-ce
ntr
ed
lead
ers
build
ing
on
an o
pen
and
ho
nest
cult
ure
and
the
deliv
ery
of
the
Trus
t va
lues
Stra
tegy
Pri
ori
ty 1
- E
ngag
e w
ith
part
ners
to
dev
elo
p
opp
ort
unit
ies
for
join
t w
ork
ing
Stra
tegy
Pri
ori
ty 2
- D
evel
op
an a
ffo
rdab
le,
sust
aina
ble
acut
e se
rvic
es m
ode
l
SO 6
- E
ngag
e st
rate
gic
part
ners
to
max
imis
e
the
opp
ort
unit
ies
to d
esig
n an
d de
liver
sust
aina
ble
serv
ices
fo
r th
e po
pula
tio
n o
f
Sout
hpo
rt, F
orm
by a
nd W
est
Lanc
ashi
re
Bec
om
e a
dist
rict
gen
eral
hosp
ital
wit
h sp
ecia
list
skill
s
in t
he c
are
of
old
er p
eopl
e
Be
part
of
an in
tegr
ated
care
sys
tem
del
iver
ing
seam
less
ho
spit
al-t
o-h
om
e
care
tha
t w
ork
s fo
r pa
tien
ts
Inve
st in
our
ho
spit
als,
mak
ing
them
fit
fo
r th
e 21
st
Cen
tury
Cre
ate
a hu
b fo
r ro
utin
e
plan
ned
car
e ru
n fr
om
a
ded
icat
ed h
osp
ital
We
will
bec
om
e an
empl
oye
r o
f ch
oic
e th
at
attr
acts
the
bes
t st
aff
TB
207_
19 S
IP P
rese
ntat
ion
Dec
19
Page 162 of 210

Pro
gre
ss
to
da
te –
No
ve
mb
er
20
19
Key
Blu
e
Act
ivit
y co
mp
lete
d
Re
dSi
gnif
ican
tly
del
ayed
an
d/o
r o
f h
igh
risk
- n
ot
exp
ecte
d t
o r
eco
ver
Gre
en
P
rogr
essi
ng
on
sch
edu
le
Am
be
rSl
igh
tly
del
ayed
an
d /
or
of
low
ris
k -
can
be
reco
vere
d
Page 163 of 210

Pro
gre
ss
to
da
te –
Ris
ks
No
ve
mb
er
20
19
TB
207_
19 S
IP P
rese
ntat
ion
Dec
19
Page 164 of 210

QU
ALI
TY &
SA
FETY
RA
GR
atin
g
Key
Ach
ieve
me
nts
/Pro
gre
ss
QU
ALI
TY S
TAN
DA
RD
S
Dra
ft C
QC
Insp
ecti
on
Rep
ort
rec
eive
d, f
act
ua
l acc
ura
cy c
om
ple
te a
nd
su
bm
itte
d t
o C
QC
on
tim
e w
ith
in o
ffic
e h
ou
rs. E
xpec
ted
pu
blic
ati
on
da
te N
ove
mb
er /
Dec
emb
er 2
01
9. A
rev
iew
is
curr
entl
y b
ein
g u
nd
erta
ken
to
inco
rpo
rate
an
y in
com
ple
te a
ctio
ns
an
d k
ey t
hem
es f
rom
th
e d
raft
insp
ecti
on
rep
ort
into
th
e q
ua
lity
imp
rove
men
t p
lan
.
The
Med
icin
es D
evel
op
men
t P
lan
co
nti
nu
es t
o b
e m
on
ito
red
an
d u
pd
ate
d o
n a
wee
kly
ba
sis.
Tw
o n
ew a
dd
itio
ns
to t
he
imp
rove
men
t p
lan
incl
ud
e a
6 m
on
th p
lan
an
d a
ssu
ran
ce t
rack
er.
Wa
rd c
hec
klis
ts n
ow
in p
lace
, wee
kly
au
dit
s co
mm
ence
d 2
1 O
cto
ber
an
d o
utc
om
es a
re t
o b
e fe
d in
to t
he
tra
cker
to
pro
vid
e a
ssu
ran
ce a
ga
inst
co
mp
lian
ce a
nd
iden
tify
an
y g
ap
s.
The
fun
din
g a
pp
lica
tio
n o
f £
70
0,0
00
fo
r EP
MA
ha
s b
een
ap
pro
ved
by
NH
SE/I
(M
eds
an
d P
ha
rma
cy Im
pro
vem
ent)
.
SON
AA
S -
The
ass
essm
ent
pro
gra
mm
e co
nti
nu
es t
o b
e ro
lled
ou
t a
cro
ss t
he
Tru
st. 5
wa
rds
ha
ve b
een
ass
esse
d, 2
ra
ted
bro
nze
an
d 3
silv
er in
th
e fi
rst
ass
essm
ent.
Th
e fi
rst
rea
sses
smen
t o
f th
e b
ron
ze w
ard
s to
ok
pla
ce w
/c 2
8 O
cto
ber
an
d o
ne
wa
rd im
pro
ved
th
eir
ove
rall
rati
ng
fro
m B
ron
ze t
o S
ilver
. A
rev
iew
of
the
SON
AA
S p
roce
ss is
ta
kin
g p
lace
w/c
5 N
ove
mb
er t
o
ensu
re t
he
pro
cess
is d
eliv
erin
g m
easu
rab
le im
pro
vem
ents
fo
r p
ati
ents
. Th
is w
ill a
ssis
t in
info
rmin
g t
he
fin
al v
ersi
on
of
the
SOP
, cu
rren
tly
in d
raft
fo
rm.
Spin
al C
entr
e re
furb
ish
men
ts a
nd
dee
p c
lea
nin
g
-P
ati
ent
roo
m a
nd
ba
thro
om
ref
urb
ish
men
t n
eari
ng
co
mp
leti
on
-
Do
mes
tic
ho
urs
incr
ease
d t
o c
orr
esp
on
d w
ith
na
tio
na
l gu
idel
ines
-P
HE
Ass
ura
nce
vis
it o
f n
ati
on
al e
xper
ts s
ched
ule
d f
or
12
No
vem
ber
20
19
to
pro
vid
e a
dvi
ce a
nd
ver
ify
ad
equ
acy
of
pro
cess
es u
nd
erta
ken.
Old
er P
eop
le’s
Pro
gra
mm
e -
The
tra
inin
g p
rog
ram
me
for
Ca
re o
f O
lder
Peo
ple
ha
s co
nti
nu
ed t
o b
e d
eliv
ered
wit
h e
xcel
len
t fe
edb
ack
. 17
0 p
eop
le a
re b
oo
ked
to
un
der
take
th
e p
rog
ram
me
by
the
end
of
20
19
.-T
he
firs
t m
emb
er o
f th
e D
emen
tia
an
d D
elir
ium
Tea
m in
po
st 0
4.1
1.1
9 a
nd
th
e A
dm
ira
l Nu
rse
du
e in
po
st 1
6.1
2.1
9
SAFE
STA
FFIN
G
Ove
rall
fill
rate
fo
r Se
pte
mb
er 2
01
9 w
as
91
.83
%(a
ga
inst
th
e n
ati
on
al a
vera
ge
of
90
%),
an
incr
ease
on
pre
vio
us
mo
nth
.Th
e Tr
ust
co
nti
nu
es t
o p
roa
ctiv
ely
sou
rce
nu
rse
ag
enci
es t
ha
t a
re
wit
hin
th
e fr
am
ewo
rk t
o s
up
ple
men
t N
HSp
an
d T
ier
3 a
gen
cies
to
su
pp
ort
wit
hd
raw
ing
of
hig
h c
ost
off
fra
mew
ork
ag
enci
es.
This
incl
ud
es b
lock
bo
oki
ng
op
po
rtu
nit
ies
tosu
pp
ort
co
nti
nu
ity
of
care
to
ou
r p
ati
ent
gro
up
s a
nd
fu
rth
er r
efle
ctiv
e o
f th
e w
inte
r co
nti
ng
enci
es f
or
the
tru
st.
QU
ALI
TY&
SA
FETY
GO
VER
NA
NC
E
Co
mp
lain
ts p
roce
ss m
ap
pin
g r
evie
w a
nd
inci
den
t p
roce
ss m
ap
pin
g e
xerc
ise
com
ple
ted
wit
h s
ub
seq
uen
t a
ctio
ns
dev
elo
ped
, a f
urt
he
r co
mp
lain
ts r
evie
w in
corp
ora
tin
g p
ati
ent
exp
erie
nce
le
d b
y th
e D
epu
ty D
irec
tor
of
Nu
rsin
g h
as
com
men
ced
in N
ove
mb
er 2
01
9, a
ny
ad
dit
ion
al
act
ion
s w
ill b
e b
uilt
into
th
e In
teg
rate
d G
ove
rna
nce
Imp
rove
men
t P
lan
. N
um
ber
s o
f co
mp
lain
ts
an
d c
on
cern
s a
re d
ecre
asi
ng
, th
e re
spo
nse
s w
ith
in 4
0 d
ays
is im
pro
vin
g –
this
wa
s 3
5.7
6%
Ap
ril 2
01
9 -
Oct
ob
er 2
01
9 c
om
pa
red
to
23
.08
% i
n A
pri
l 20
18
-O
cto
ber
20
18
6
Page 165 of 210

7
Key
Ris
ks/I
ssu
es
Mit
igat
ing
Act
ion
sR
AG
Inab
ility
to
rel
ease
clin
ical
sta
ff t
o p
arti
cip
ate
in M
ou
th C
are
Mat
ters
pro
ject
s Se
cure
d 3
ad
dit
ion
al p
lace
s fo
r M
ou
th C
are
Mat
ters
pro
gram
me
in L
on
do
n 1
5th
N
ove
mb
er 2
01
9A
Win
ter
pre
ssu
res
-C
lear
imp
act
acce
ss a
nd
flo
w o
n Q
ual
ity
& S
afet
y W
inte
r p
ress
ure
s -
Cle
ar im
pac
t ac
cess
an
d f
low
on
Qu
alit
y &
Saf
ety
Par
tici
pat
e in
th
e d
evel
op
men
t o
f th
e sy
stem
win
ter
pla
n
R
Key
Ach
ieve
me
nts
/Pro
gre
ss in
Mo
nth
–Q
ual
ity
& S
afet
y
CQ
C In
spec
tio
n c
om
ple
ted
, aw
ait
ing
fin
al r
epo
rt
Wo
rk r
ela
tin
g t
o t
he
4 q
ua
lity
pri
ori
ties
co
nti
nu
es t
o m
ove
fo
rwa
rd
TB
207_
19 S
IP P
rese
ntat
ion
Dec
19
Page 166 of 210

1.1
Op
era
tio
nal
Pe
rfo
rman
ce (
Exe
cLe
ad: S
teve
Ch
rist
ian
)R
AG
Rat
ing
Pro
gre
ss
8
Can
cer
62
Day
Per
form
ance
fo
r Se
pte
mb
er 2
01
9 w
as 8
2%
an
incr
ease
on
th
e A
ugu
st p
osi
tio
n o
f 7
5.3
% a
nd
th
e b
est
per
form
ance
sin
ce O
cto
ber
20
18
. Th
ere
are
just
fiv
e tr
ust
s n
atio
nal
ly t
hat
are
del
iver
ing
an im
pro
vem
ent
in c
ance
r p
erfo
rman
ce, w
ith
in t
he
regi
on
we
are
the
on
ly s
ervi
ce s
ho
win
g im
pro
vem
ents
in
per
form
ance
.
18
We
ek
RTT
Pe
rfo
rman
ceSe
pte
mb
er 1
8-w
eek
RTT
per
form
ance
was
93
.4%
P
red
icti
on
s fo
r O
cto
ber
sh
ow
per
form
ance
will
rem
ain
aro
un
d 9
3%
an
d c
on
tin
ue
to b
e ab
ove
th
e 9
2%
th
resh
old
.Th
ere
are
curr
entl
y 7
pat
ien
ts w
aiti
ng
ove
r 4
0 w
eeks
, a s
ligh
t in
crea
se ,
ho
wev
er t
he
nu
mb
er o
f 3
0+
wee
k w
aite
rs h
as d
rop
ped
fro
m 9
9 t
o 8
8 o
ver
the
pas
t 4
wee
ks, t
hes
e lo
ng
wai
ters
are
la
rgel
y d
ue
to t
he
con
tin
uin
g ch
alle
nge
s in
Co
mm
un
ity
Pae
dia
tric
s an
d G
ynae
colo
gy.
The
Gyn
aeco
logy
po
siti
on
is p
red
icte
d t
o r
eco
ver
fro
m J
anu
ary
20
20
as
the
Tru
st a
hs
rece
ntl
y ap
po
inte
d 4
co
nsu
ltan
ts
The
Co
mm
un
ity
Pae
dia
tric
s p
erfo
rman
ce w
ill c
on
tin
ue
to b
e co
mp
rom
ised
un
til w
e ca
n a
pp
oin
t in
to t
he
vaca
nt
com
mu
nit
y P
aed
iatr
icia
n p
ost
Dia
gno
stic
sP
erfo
rman
ce f
or
Oct
ob
er a
gain
st t
he
6 w
eek
wai
t ta
rget
was
2.1
6%
an
imp
rove
men
t o
f 0
.5%
ove
r th
e Se
pte
mb
er p
osi
tio
n a
nd
in li
ne
wit
h t
raje
cto
ry s
et w
ith
NH
S I /
CC
GN
on
-ob
stet
ric
Ult
raso
un
d a
nd
Cys
tosc
op
y re
mai
n t
he
area
s o
f m
ost
co
nce
rn, w
ith
34
an
d 1
3 w
aite
rs o
ver
6 w
eeks
, all
oth
er m
od
alit
ies
hav
e si
ngl
e fi
gure
wai
ters
.En
do
sco
py
reco
rded
th
e m
ost
nu
mb
er o
f sc
op
es in
a m
on
th (
on
rec
ord
) in
Oct
ob
er a
t 6
53
wit
h z
ero
ses
sio
ns
can
celle
d d
ue
to n
o n
urs
es.
Len
gth
of
Stay
Len
gth
of
stay
fo
r fu
ll em
erge
ncy
ad
mis
sio
ns,
wh
ich
do
es n
ot
incl
ud
e p
atie
nts
bei
ng
adm
itte
d t
o a
sses
smen
t w
ard
s, w
as r
eco
rde
d a
t 6
.3 d
ays
in O
cto
ber
an
imp
rove
men
t fr
om
th
e Se
pte
mb
er p
osi
tio
n, w
ith
pat
ien
ts o
n a
sses
smen
t w
ard
s st
ayin
g an
ave
rage
of
8 h
ou
rs, w
hic
h is
th
e sa
me
as S
epte
mb
er.
Ther
e w
ere
18
5 s
tran
ded
pat
ien
ts in
Oct
ob
er 2
01
9, a
n in
crea
se f
rom
th
e p
revi
ou
s m
on
th.
Sup
er S
tran
ded
pat
ien
ts a
lso
incr
ease
d t
o 7
0Th
e ke
y in
-mo
nth
pro
gres
s is
th
e re
intr
od
uct
ion
of
the
sen
ior
lead
su
pp
ort
ing
R2
G a
nd
th
e in
tro
du
ctio
n o
f a
Bo
ard
Ro
un
d S
OP
A&
E 4
Ho
ur
Pe
rfo
rman
ceTh
e Tr
ust
s re
po
rted
4 h
ou
r A
&E
per
form
ance
in O
cto
ber
was
84
.6%
a 4
% d
ecre
ase
fro
m t
he
Sep
tem
ber
po
siti
on
of
88
.6%
Th
is is
du
e to
a s
ign
ific
ant
dec
reas
e in
So
uth
po
rt p
erfo
rman
ce w
hic
h h
as d
rop
ped
fro
m 7
7.6
% in
Sep
tem
ber
to
70
% in
Sep
tem
ber
20
19
.Th
e So
uth
po
rt it
sit
e is
exp
erie
nci
ng
sign
ific
ant
dem
and
pre
ssu
res
wit
h a
tten
dan
ces
and
ad
mis
sio
ns
up
by
17
% a
gain
st t
he
sam
eti
me
per
iod
of
last
yea
r.
Win
ter
pla
nn
ing
The
Tru
st h
as in
tro
du
ced
a w
eekl
y W
inte
r O
per
atio
nal
Gro
up
to
su
pp
ort
imp
lem
enta
tio
n o
f th
e h
osp
ital
win
ter
sch
emes
. Th
e sc
hem
es in
clu
de
the
op
enin
g o
f a
16
bed
ded
po
st o
per
ativ
e O
rth
op
aed
ic w
ard
to
su
pp
ort
ap
pro
pri
ate
tran
sfer
of
pat
ien
ts s
till
un
der
acu
te c
are
that
can
rec
eive
th
eir
reh
abili
tati
on
at
Orm
skir
k. T
his
in e
ffec
t w
ill r
elea
se 1
6b
eds
at S
ou
thp
ort
as
this
cu
rren
t co
ho
rt o
f p
atie
nts
rem
ain
on
th
e So
uth
po
rt s
ite
un
til f
it f
or
dis
char
ge.
The
Tru
st B
oar
d h
as s
ign
ed o
ff t
he
bu
sin
ess
case
wit
h r
ecru
itm
ent
and
est
ates
wo
rk c
om
men
ced
wit
h a
tar
get
dat
e o
f o
pen
ing
in t
he
firs
t w
eek
of
Jan
uar
y.
The
atre
Uti
lizat
ion
O
rmsk
irk
imp
rove
d in
mo
nth
to
73
% f
or
Oct
ob
er b
y 1
% a
gain
st t
he
pre
vio
us
mo
nth
. H
ow
ever
So
uth
po
rt u
tiliz
atio
n r
eco
rded
a d
eclin
e in
per
form
ance
du
e to
hig
h n
um
ber
s o
f ca
nce
llati
on
s (1
5.6
6%
mai
nly
att
rib
ute
d t
o p
atie
nt
flo
w is
sues
(i.e
. no
bed
s av
aila
ble
)
Page 167 of 210

9
Ke
yR
isks
Mit
igat
ing
Act
ion
sR
AG
Ach
ievi
ng
Co
nst
itu
tio
na
l St
and
ard
s
The
key
issu
es b
ein
g:
•W
ork
forc
e –
gap
s in
acu
te m
edic
ine
ph
ysic
ian
s, r
adio
logi
sts,
an
aest
het
ics
and
ger
iatr
icia
ns
are
clea
rly
imp
acti
ng
on
cu
rren
t p
erfo
rman
ce a
nd
bei
ng
able
to
su
stai
n a
co
nsi
sten
t le
vel o
f p
erfo
rman
ce (
acro
ss 4
ho
ur
stan
dar
d, d
iagn
ost
ic
and
can
cer
in p
arti
cula
r)
•Th
e So
uth
po
rt &
Orm
skir
k sy
stem
bei
ng
able
to
imp
lem
ent
win
ter
sch
emes
an
d d
eliv
er a
gain
st t
he
assu
mp
tio
ns
the
CC
G h
ave
sign
ed o
ff.
The
assu
mp
tio
ns
form
ed t
he
bas
is in
th
e sy
stem
bei
ng
able
to
mit
igat
e th
e ga
p id
enti
fied
by
Ven
n p
arti
cula
rly
wit
hin
th
e o
ut
of
ho
spit
al p
rovi
sio
n (
40
b
eds)
.
The
intr
od
uct
ion
of
the
“Wo
rkfo
rce
Imp
rove
men
t G
rou
p”
mu
st f
ocu
s o
n t
he
tim
ely
recr
uit
men
t o
f th
e cr
itic
al
po
sts
that
co
nti
nu
e to
pro
vid
e ch
alle
nge
s to
mai
nta
in a
n e
ffec
tive
an
d r
elia
ble
ser
vice
off
er.
The
Tru
st h
as r
efer
ence
d p
revi
ou
sly
the
con
cern
s th
at t
he
sch
emes
pu
t fo
rwar
d b
y th
e sy
stem
will
no
t ad
dre
ss t
he
gap
iden
tifi
ed b
y V
enn
du
e to
th
e as
sum
pti
on
s b
ein
g am
bit
iou
s gi
ven
tim
esca
les
set
wit
hin
th
e im
ple
men
tati
on
pla
ns.
Th
e sy
stem
has
set
up
a w
eekl
y U
EC S
yste
m L
ead
ers
mee
tin
g w
hic
h is
ch
aire
d b
y th
e U
EC P
rogr
amm
e D
irec
tor
and
th
is m
eeti
ng
no
w m
on
ito
rs p
rogr
ess
of
each
win
ter
sch
emes
rep
ort
ing
thro
ugh
to
th
e SM
B.
R
TB
207_
19 S
IP P
rese
ntat
ion
Dec
19
Page 168 of 210

20
19
/20
FIN
AN
CIA
L P
LAN
(1
)R
AG
Rat
ing
Key
Ach
ieve
me
nts
/Pro
gre
ssFI
NA
NC
IAL
CO
NTR
OLS
-co
nti
nu
e to
co
ntr
ol s
pen
d a
nd
del
iver
CIP
Cu
rre
nt
pe
rfo
rman
ceTh
e m
on
th 7
YTD
po
siti
on
bef
ore
Pro
vid
er S
ust
ain
abili
ty F
un
din
g (P
SF)
and
Fin
anci
al R
eco
very
Fu
nd
(FR
F) is
a d
efic
it o
f £
16
.32
8 m
illio
n w
hic
h is
£8
69
,000
wo
rse
than
pla
n.
The
in-m
on
th p
osi
tio
n b
efo
re P
SF/F
RF
is a
def
icit
of
£2
.37
2 m
illio
n,
£0
.86
1 m
illio
n w
ors
e th
an p
lan
.
The
Tru
st’s
fo
reca
st o
utt
urn
, bas
ed o
n m
on
th 6
per
form
ance
an
d s
har
ed w
ith
NH
SI/E
on
1 N
ove
mb
er 2
01
9, i
s £
3.6
mill
ion
ove
rsp
en
d a
gain
st t
he
def
icit
pla
n.
Mo
nth
7 e
xpen
dit
ure
is
hig
her
th
an t
he
traj
ecto
ry a
llow
ed t
o a
chie
ve t
his
fo
reca
st o
utt
urn
.Th
e 2
01
9/2
0 C
IP p
rogr
amm
e is
£1
,35
0,0
00 b
ehin
d p
lan
at
mo
nth
7; t
he
fore
cast
ou
ttu
rn is
£4
.3 m
illio
n a
gain
st t
he
£6
.3 m
illio
np
lan
leav
ing
an u
nid
enti
fied
gap
of
£2
.0 m
illio
n.
If m
ater
ial c
ash
red
uci
ng
CIP
sch
emes
can
no
t b
e tr
ansa
cted
du
rin
g th
e re
mai
nd
er o
f th
e ye
ar t
hen
an
y p
ress
ure
on
th
e ex
pen
dit
ure
run
rat
e w
ill n
ot
be
mit
igat
ed.
Tru
st a
ctiv
ity
and
inco
me
per
form
ance
at
mo
nth
7 Y
TD is
as
follo
ws:
•El
ecti
ve –
acti
vity
is 3
.9%
bel
ow
pla
n;
£4
35
,00
0 lo
ss o
f in
com
e.•
A&
E –
acti
vity
5.5
% a
bo
ve p
lan
; £
35
3,0
00
of
add
itio
nal
inco
me.
•N
on
Ele
ctiv
e –
acti
vity
is 2
.4%
bel
ow
pla
n;
£2
,56
7,0
00
add
itio
nal
inco
me
du
e to
cas
e m
ix•
Ou
tpat
ien
ts –
acti
vity
is 3
.94
% a
bo
ve p
lan
; £6
27
,00
0 o
f ad
dit
ion
al in
com
e
No
t al
l of
the
abo
ve a
ctiv
ity
per
form
ance
is p
ayab
le in
20
19
/20
du
e to
:•
On
ly a
pro
po
rtio
n o
f th
e n
on
-ele
ctiv
e va
lue
is p
ayab
le d
ue
to t
he
app
licat
ion
of
the
“ble
nd
ed t
arif
f” a
dju
stm
ent.
•Se
fto
n C
CG
’s c
on
trac
t ap
plie
s th
e “b
len
ded
tar
iff”
to
all
po
ints
of
del
iver
y.
The
Tru
st’s
to
tal i
nco
me
pla
n is
on
sch
edu
le t
o b
e ac
hie
ved
.
Un
der
lyin
g ex
pen
dit
ure
lev
els
in m
on
th 7
hav
e ri
sen
mai
nly
du
e to
ad
dit
ion
al s
taff
hav
ing
bee
n e
mp
loye
d c
om
par
ed t
o p
revi
ou
s m
on
ths.
Th
e Tr
ust
sp
ent
abo
ve £
2.0
mill
ion
in O
cto
ber
on
b
ank
and
age
ncy
sta
ff w
hic
heq
uat
es t
o a
n a
nn
ual
sp
end
of
£2
4 m
illio
n o
n p
rem
ium
rat
e st
aff.
Mo
nth
7 Y
TD a
gen
cy s
pen
d is
£6
.97
8 m
illio
n (
8.4
5%
of
the
pay
bill
); M
edic
al s
taff
£3
.71
7 m
illio
n;
Nu
rsin
g £
2.6
19
mill
ion
.Th
e Tr
ust
bre
ach
ed t
he
NH
SI a
gen
cy t
arge
t ca
p o
f £
4.8
91
mill
ion
in
Sep
tem
ber
.M
on
thly
age
ncy
sp
end
has
incr
ease
d a
gain
in O
cto
ber
to
£1
,10
9,0
00
(9.3
% o
f th
e p
ay b
ill);
Med
ical
sta
ff £
51
1,0
00;
Nu
rsin
g £
45
8,0
00.
Tota
l Ban
k sp
end
is c
on
sist
ent
wit
h p
revi
ou
s m
on
ths;
Oct
ob
er is
£9
44
,000
(7.9
% o
f th
e to
tal p
ay b
ill)
bri
ngi
ng
YTD
sp
end
to
£6
.53
3 m
illio
n (
7.9
% o
f th
e to
tal p
ay b
ill).
Ke
y ac
tio
ns
Wee
kly
mee
tin
gs n
ow
est
ablis
hed
wit
h t
he
Exec
uti
ve t
eam
fo
r C
IP a
nd
th
e w
ider
fin
anci
al r
eco
very
pla
n w
ith
a f
ocu
s o
n t
he
op
era
tio
nal
det
ail b
ehin
d b
oth
of
thes
e ar
eas
(del
iver
y o
f £
1.5
m
illio
n r
eco
very
pla
n s
chem
es r
equ
ired
wef
No
vem
ber
20
19
bu
t th
is w
ou
ld s
till
resu
lt in
th
e Tr
ust
£3
.6 m
illio
n a
way
fro
m t
he
year
en
d p
lan
).El
emen
ts o
f th
e fi
nan
cial
rec
ove
ry p
lan
in
clu
de;
Red
uct
ion
in h
igh
co
st t
emp
ora
ry s
pen
d (
this
will
co
ver
ban
k, a
gen
cy, i
nte
rim
sta
ff a
nd
wai
tin
g lis
t in
itia
tive
s);
Pla
n o
f ac
tio
n o
n h
ow
th
e w
ork
on
fra
gile
ser
vice
s w
ill b
e d
eliv
ered
alo
ng
wit
h u
nfu
nd
ed/u
nd
er f
un
ded
ser
vice
s; M
ake
bes
t u
seo
fN
HSI
su
pp
ort
on
off
er s
uch
as
the
Mo
del
Ho
spit
al.
Co
st Im
pro
vem
en
t P
rogr
amm
eTr
ust
ori
gin
al C
IP p
lan
of
£6
.3 m
illio
n (
excl
ud
ing
£3
72
,000
of
FYE
of
20
18
/19
sch
emes
) w
as t
o b
e d
eliv
ered
by
£4
.5 m
illio
n e
xpen
dit
ure
red
uct
ion
s an
d a
dd
itio
nal
inco
me
of
£1
.8 m
illio
n f
rom
B
PT.
Fo
llow
ing
con
trac
t ag
reem
ent
wit
h o
ur
mai
n c
om
mis
sio
ner
th
e Tr
ust
nee
ds
to d
eliv
er £
6.3
mill
ion
of
exp
end
itu
re r
edu
ctio
ns.
Pro
gre
ss r
e p
lan
A
t m
on
th 7
, th
e Tr
ust
had
tra
nsa
cted
£2
.86
3 m
illio
n o
f C
IPs.
Th
e Tr
ust
is f
ore
cast
ing
del
iver
y o
f £
4.3
mill
ion
, ga
p o
f £
2.0
mill
ion
.
10
Page 169 of 210

20
19
/20
FIN
AN
CIA
L P
LAN
(2
)R
AG
Rat
ing
Key
Ach
ieve
me
nts
/Pro
gre
ss
CA
PIT
AL
PLA
N –
del
iver
pla
nn
ed in
vest
men
t p
rog
ram
me
focu
sin
g o
n IT
, med
ica
l eq
uip
men
t a
nd
imp
rove
men
ts t
o w
ard
en
viro
nm
ents
The
pla
n f
or
20
19
/20
is a
gro
ss c
apit
al s
pen
d t
ota
l of
£5
.1 m
illio
n (
this
exc
lud
es I
FRIC
12
ad
dit
ion
s an
d d
on
ated
ass
ets
of
£1
.3m
illio
n,
£1
.2 m
illio
n o
f w
hic
h is
fo
r th
e G
E R
adio
logy
eq
uip
men
t re
pla
cem
ent
pro
gram
me
). T
her
e co
nti
nu
es t
o b
e si
gnif
ican
t in
vest
men
t in
IT w
ith
£1
.7 m
illio
n in
vest
ed in
20
19
/20
, w
hic
h in
clu
des
pro
ject
s d
esig
ned
to
imp
rove
pat
ien
t fl
ow
an
d p
atie
nt
reco
rds,
alo
ng
wit
h w
ork
on
IT in
fras
tru
ctu
re a
nd
sec
uri
ty. T
he
rolli
ng
pro
gram
me
of
rep
laci
ng
and
up
dat
ing
Med
ical
Eq
uip
men
t co
nti
nu
es w
ith
inve
stm
ent
of
£1
.0 m
illio
n in
2
01
9/2
0.T
he
Esta
tes
cap
ital
pla
n in
clu
des
a 6
Fac
et S
urv
ey t
o h
elp
ste
er f
utu
re in
vest
men
t an
d s
up
po
rt s
trat
egic
inte
nt.
Oth
er e
stat
es
imp
rove
men
t sc
hem
es a
re d
esig
ned
to
imp
rove
ex
isti
ng
pro
per
ties
an
d e
nab
le s
ervi
ce d
eliv
ery
targ
ets
to b
e ac
hie
ved
, in
crea
sin
g p
atie
nt
safe
ty a
nd
imp
rovi
ng
pat
ien
t ex
per
ien
ce.
Tota
l pla
nn
ed s
pen
d f
or
Esta
tes
and
Fac
iliti
es in
20
19
/20
is
£1
.7 m
illio
n.
Pro
gre
ss r
e p
lan
Act
ual
sp
end
YTD
is £
2.0
98
mill
ion
(p
lan
ned
sp
end
yea
r to
dat
e o
f £
4.0
27
mill
ion
) w
ith
a f
urt
her
£1
.13
7 m
illio
n c
om
mit
ted
exp
end
itu
re.
Co
mp
arin
g th
is a
gain
st t
he
ann
ual
pla
n, £
5,1
03
,000
excl
ud
ing
do
nat
ed a
nd
GE
rad
iolo
gy a
sset
s, t
hen
th
e Tr
ust
has
sp
ent/
com
mit
ted
63
.4%
of
the
pla
n a
t th
e en
d o
f O
cto
ber
20
19
.
The
Sou
thp
ort
war
du
pgr
ade
pro
ject
has
star
ted
and
the
firs
t5
war
ds
will
be
com
ple
ted
bef
ore
Ch
rist
mas
.Th
e6
thw
ard
isp
lan
ned
for
com
ple
tio
nb
efo
reth
een
do
fth
efi
nan
cial
year
.
Wo
rkis
pro
gres
sin
gw
ellw
ith
inth
eSp
inal
Un
ito
nth
eIs
ola
tio
nw
ork
san
dth
ew
ork
req
uir
edas
are
sult
of
the
Kle
bsi
ella
ou
tbre
akw
ith
com
ple
tio
nex
pec
ted
inth
eve
ryn
ear
futu
re.
IM&
Tco
nti
nge
ncy
sch
eme
at£4
50
,000
was
ori
gin
ally
inte
nd
edfo
rth
ed
ata
cen
tre,
ho
wev
er,
this
loo
ked
un
likel
yto
be
imp
lem
en
ted
in2
01
9/2
0an
da
re-u
tilis
atio
no
fth
ese
mo
nie
sto
oth
erIT
pro
ject
sis
refl
ecte
din
the
revi
sed
pla
n.
On
a p
osi
tive
no
te t
he
Tru
st h
as b
een
su
cces
sfu
l in
bid
din
g fo
r eP
MA
(Ele
ctro
nic
Pre
scri
bin
g an
d M
edic
ines
Ad
min
istr
atio
n)
and
has
bee
n a
war
ded
£7
00
,00
0 in
20
19
/20
.
The
Bo
ard
ap
pro
ved
a r
evis
ed c
apit
al p
lan
on
6th
No
vem
ber
20
19
an
d a
uth
ori
sati
on
was
giv
en t
o p
roce
ed w
ith
th
e w
inte
r p
lan
at
£3
50
,00
0. H
ow
ever
, co
sts
are
no
w c
lear
er a
nd
an
a
req
ues
t to
incr
ease
th
e sc
hem
e va
lue
to £
49
5,0
00
will
be
dis
cuss
ed a
t Fi
nan
ce, P
erfo
rman
ce &
Inve
stm
ent
Co
mm
itte
e o
n 2
5th
No
vem
ber
20
19
.
TRA
NSF
OR
MA
TIO
N -
dri
ve d
eliv
ery
of
pro
gra
mm
es in
clu
din
g G
IRFT
, M
od
el H
osp
ita
l, th
eatr
e a
nd
ou
tpa
tien
t ef
fici
ency
GIR
FT–
incr
ease
in p
rod
uct
ivit
y; c
on
sist
ent
qu
alit
y; b
ette
r p
ati
ent
exp
erie
nce
; red
uce
d c
ost
of
join
ts
Mo
de
l Ho
spit
alFo
cus
wit
h t
he
NH
SI M
od
el H
osp
ital
tea
m•
Pro
cure
men
t•
Med
ical
Jo
b P
lan
nin
g -
app
rop
riat
e m
edic
al jo
b p
lan
s; r
edu
ctio
n in
WLI
’s
•N
urs
ing
–e-
Ro
ster
ing
and
revi
ew o
f C
linic
al N
urs
e Sp
ecia
lists
•H
R -
imp
rove
men
t in
“ti
me
to r
ecru
it”;
imp
rove
d r
eten
tio
n r
ates
; red
uci
ng
relia
nce
on
age
ncy
•Fa
cilit
ies
Man
agem
ent
car
par
kin
g te
nd
er a
nd
cat
erin
g; p
ort
erin
gca
pac
ity
and
dem
and
an
alys
is;
cate
rin
g ef
fici
ency
•
Med
icin
es M
anag
emen
t
The
atre
Eff
icie
ncy
–p
rod
uct
ivit
y im
pro
vem
ent;
red
uce
late
sta
rts
and
can
cella
tio
ns;
imp
rove
pat
ien
t ex
per
ien
ce
Ou
tpat
ien
t Ef
fici
en
cy –
red
uce
DN
A r
ates
; red
uce
wai
tin
g ti
mes
; o
pp
ort
un
ity
to r
edu
ce n
um
ber
of
clin
ics
11
TB
207_
19 S
IP P
rese
ntat
ion
Dec
19
Page 170 of 210

20
19
/20
FIN
AN
CIA
L P
LAN
(3
)R
AG
Rat
ing
Key
Ach
ieve
men
ts/P
rogr
ess
12
Key
Ris
ks/I
ssu
esM
itig
atin
g A
ctio
ns
RA
G
Un
der
lyin
g e
xpen
dit
ure
leve
ls w
ill n
ot
red
uce
to
pre
Q4
20
18
/19
leve
ls,
wh
ich
is
the
ba
sis
of
the
exp
end
itu
re p
lan
.
Nu
rse
esta
blis
hm
ent
bu
sin
ess
case
fu
nd
ing
wa
s a
lloca
ted
in m
on
th 1
an
d w
ill e
na
ble
a
mo
re m
ean
ing
ful a
na
lysi
s ca
n t
ake
pla
ce o
f n
urs
e o
vers
pen
ds
an
d m
itig
ati
ng
act
ion
s
to b
rin
g b
ack
into
ba
lan
ce.
An
aly
sis
of
oth
er o
vers
pen
din
g a
rea
s (m
ain
ly m
edic
al s
taff
) th
at
are
co
ntr
ibu
tin
g a
nd
reco
nci
liati
on
to
det
erm
ine
wh
ere
curr
ent
bu
sin
ess
case
s w
ill r
eso
lve
the
issu
e.
R
Inco
me
pla
n h
as
bee
n r
evis
ed d
ow
n f
ollo
win
g c
on
tra
ct d
iscu
ssio
ns.
Ther
e is
a r
isk
tha
t th
e B
PT
an
d r
epa
tria
tio
n o
f a
ctiv
ity
will
no
t b
e a
chie
ved
.
Dev
elo
pm
ent
of
Tru
st F
ina
nci
al R
eco
very
pla
n (
pa
rt o
f o
vera
ll Sy
stem
Rec
ove
ry P
lan
).
6 k
ey a
rea
s o
f fo
cus
are
:➢
Esta
blis
hm
ent
con
tro
ls
➢M
edic
al b
an
k (P
atc
hw
ork
)➢
Dig
ita
lisa
tio
n o
f o
utp
ati
ents
➢R
epa
tria
tio
n
➢U
nfu
nd
ed s
ervi
ces
➢Fr
ag
ile s
ervi
ces
Each
are
a h
as
an
exe
cuti
ve le
ad
an
d t
he
Tru
st C
EO r
evie
ws
pro
gre
ss o
n t
hes
e p
roje
cts
on
a w
eekl
y b
asi
s.O
cto
ber
20
19
-p
erfo
rma
nce
is b
elo
w p
lan
an
d f
ore
cast
to
be
£2
mill
ion
aw
ay
at
yea
r-en
d. S
chem
es id
enti
fied
ab
ove
will
no
t m
itig
ate
th
e sh
ort
fall
on
oth
er s
chem
es.
A
New
CIP
ta
rget
fo
r ex
pen
dit
ure
red
uct
ion
of
£6
.3 m
illio
nR
Page 171 of 210

WO
RK
FOR
CE
AM
BER
Key
Ach
ieve
men
ts/P
rogr
ess
(1
)W
OR
KFO
RC
E EF
FIC
IEN
CY
•C
hes
hir
e &
Mer
seys
ide
colla
bo
rati
on
on
nu
rsin
g a
nd
mid
wif
ery
ag
ency
ca
ll o
ff c
on
tra
ct a
nd
ra
te c
ard
–Tr
ust
en
ga
ged
wit
h im
ple
me
nta
tio
n f
rom
1 N
ove
mb
er f
ollo
win
g C
art
er a
t Sc
ale
sig
n o
ff.
•Ti
er 2
ag
ency
ca
sca
de
imp
lem
ente
d w
ith
fu
rth
er e
nh
an
cem
ents
for
nu
rsin
g w
ith
a 3
% o
ff f
ram
ewo
rk im
pro
vem
ent
ach
ieve
d in
Sep
tem
ber
an
d m
on
th t
o d
ate
Oct
ob
er t
rack
ing
at
a
13
% im
pro
vem
ent.
•A
lloca
tio
n w
ard
sh
ift
mo
del
ling
in p
rog
ress
to
ass
ess
are
as
an
d p
att
ern
s w
her
e h
igh
er d
ema
nd
s w
ill s
up
po
rt r
edu
ctio
n in
off
fra
mew
ork
nu
rsin
g u
tilis
ati
on
. •
Sup
po
rtin
g A
tten
da
nce
Po
licy
(sic
knes
s a
bse
nce
) la
un
ched
fro
m 2
8th
Jan
ua
ry 2
01
8 w
ith
gu
ida
nce
, tra
inin
g a
nd
su
pp
ort
to
en
sure
a s
ust
ain
ed r
edu
ctio
n in
sic
knes
s a
bse
nce
ra
tes.
Th
e P
olic
y is
un
der
go
ing
a 6
mo
nth
rev
iew
wit
h t
he
firs
t a
nd
sec
on
d r
evie
w s
essi
on
s co
mp
lete
d.
YTD
Sic
knes
s a
bse
nce
ra
tes
ha
ve c
on
sist
entl
y d
ecre
ase
d s
ince
Dec
emb
er 2
01
8 a
nd
co
nti
nu
e to
do
so
in S
epte
mb
er 2
01
9.
Th
e Y
TD r
olli
ng
sic
knes
s a
bse
nce
ra
te h
as
red
uce
d b
y 0
.53
% s
ince
Dec
emb
er 2
01
8 t
o 5
.35
% in
Sep
tem
ber
20
19
. M
on
thly
sic
knes
s a
bse
nce
ra
te
for
Sep
tem
ber
20
19
wa
s a
red
uct
ion
to
4.3
2%
th
e lo
wes
t m
on
thly
sic
knes
s a
bse
nce
ra
te s
ince
20
14
. Th
e Tr
ust
will
co
nti
nu
e to
mo
nit
or
leve
ls c
lose
ly a
nd
co
nti
nu
e th
e fo
cuse
d w
ork
a
rou
nd
imp
rovi
ng
an
d s
up
po
rt s
taff
’s a
tten
da
nce
to
wo
rk.
•P
DR
co
mp
lian
ce d
ecre
ase
d in
mo
nth
to
69
.58
% f
or
Sep
tem
ber
20
19
.All
CB
U’s
ha
ve p
rese
nte
d t
hei
r re
vise
d P
DR
imp
rove
men
ta
t P
erfo
rma
nce
Rev
iew
Bo
ard
s. F
urt
her
su
pp
ort
m
eeti
ng
s p
lan
ned
to
loo
k a
t te
am
ob
ject
ives
.•
Eng
ag
emen
t w
ith
alt
ern
ati
ve m
edic
al b
an
k p
rovi
der
co
mm
ence
d –
Oct
ob
er 2
01
9•
Esta
blis
hm
ent
of
Emp
loye
e R
ela
tio
ns
rep
ort
to
be
pre
sen
ted
at
Wo
rkfo
rce
Co
mm
itte
e o
n a
mo
nth
ly b
asi
s.•
Sco
pin
g e
xerc
ise
un
der
wa
y to
imp
lem
ent
an
Em
plo
yee
Rel
ati
on
s el
ectr
on
ic s
yste
m t
his
will
pro
vid
e a
n a
rtif
icia
l in
telli
gen
ce e
lem
ent
to t
he
pro
cess
an
d a
lso
su
pp
ort
th
e re
com
men
da
tio
ns
follo
win
g t
he
Ba
ron
ess
Did
o H
ard
ing
Rep
ort
•W
ork
forc
eEf
fici
enci
es Im
pro
vem
ent
pro
gra
mm
e sc
op
ed a
nd
go
vern
an
ce a
rra
ng
emen
ts p
rop
ose
d v
ia P
MO
.•
Dev
elo
pm
ent
of
ag
ency
ra
te a
pp
rova
l pro
cess
giv
ing
mo
re a
cco
un
tab
ility
to
div
isio
ns
an
d c
linic
al d
irec
tors
; to
be
fin
alis
ed a
nd
imp
lem
ente
d in
No
vem
ber
.•
Enh
an
cem
ent
to n
urs
e ro
ster
ing
da
shb
oa
rd in
pro
gre
ss w
ith
en
ha
nce
d s
up
po
rt b
ein
g p
rovi
ded
to
ch
eck
an
d c
ha
llen
ge
pro
cess
es.
CLI
NIC
AL
WO
RK
FOR
CE
PLA
N
•Th
e C
linic
al W
ork
forc
e P
lan
–to
be
revi
ewed
fo
llow
ing
cu
rren
t cy
cle
of
bu
sin
ess
pla
nn
ing
.
REC
RU
ITM
ENT
AN
D R
ETEN
TIO
N
•R
edu
ctio
n in
Tim
e to
Hir
e p
rog
ram
me
rep
ort
ing
to
Mo
del
Ho
spit
al a
nd
Wo
rkfo
rce
Imp
rove
men
t G
rou
p•
QI p
rio
rity
fo
r Tr
ust
•Fo
cuss
ed p
iece
s o
f re
cru
itm
ent
bei
ng
un
der
take
n t
o f
ill m
edic
al v
aca
nci
es. E
spec
ially
ha
rd t
o f
ill a
rea
s su
ch a
s R
ad
iolo
gy
an
d O
bst
etri
cs a
nd
Gyn
aec
olo
gy.
•
Sco
pin
g o
f in
tern
ati
on
al r
ecru
itm
ent
op
tio
ns
for
nu
rses
. •
Co
nti
nu
ed r
ecru
itm
ent
to f
ully
est
ab
lish
th
e Tr
ust
rec
ruit
men
t te
am
. •
Wo
rkin
g t
o s
up
po
rt C
BU
s re
cru
itm
ent,
alo
ng
sid
e co
rpo
rate
nu
rse
lea
der
s.
13
TB
207_
19 S
IP P
rese
ntat
ion
Dec
19
Page 172 of 210

WO
RK
FOR
CE
AM
BER
Key
Ach
ieve
men
ts/P
rogr
ess
(2
)LE
AR
NIN
G A
ND
DEV
ELO
PM
ENT
•C
BU
’s c
on
tin
ue
to w
ork
wit
h H
R t
o s
et t
raje
cto
ries
to
incr
ease
ma
nd
ato
ry t
rain
ing
ra
tes
to s
tret
ch t
arg
et o
f 9
5%
. Iss
ue
hig
hlig
hte
d in
rel
ati
on
to
res
usc
ita
tio
n c
om
plia
nce
wh
ich
is
bei
ng
tre
ate
d a
s a
pri
ori
ty b
y th
e o
rga
nis
ati
on
to
ad
dre
ss t
he
issu
e a
nd
incr
ease
co
mp
lian
ce.
•C
BU
’s c
on
tin
ue
to w
ork
wit
h H
R t
o s
et t
raje
cto
ries
to
incr
ease
ap
pra
isa
l ra
tes
to 8
5%
. PD
R c
om
plia
nce
co
nti
nu
es t
o b
e ch
alle
ng
e fo
r th
e o
rga
nis
ati
on
an
d is
cu
rren
tly
on
a d
ow
nw
ard
tr
aje
cto
ry. I
ssu
e d
ue
to b
e a
dd
ress
ed in
Wo
rkfo
rce
Imp
rove
men
t G
rou
p t
o d
iscu
ss w
ith
key
sta
keh
old
ers
ho
w t
o m
ove
fo
rwa
rd w
ith
incr
easi
ng
co
mp
lian
ce. I
n a
dd
itio
n t
o c
om
plia
nce
b
ein
g c
ha
llen
ged
, qu
alit
y o
f a
pp
rais
als
is a
n is
sue
for
the
org
an
isa
tio
n a
nd
th
e O
D t
eam
is c
urr
entl
y ca
rryi
ng
ou
t a
myt
h b
ust
erin
ord
er t
o t
ry t
o in
crea
se c
om
plia
nce
an
d a
dd
ress
th
e is
sue
aro
un
d q
ua
lity.
•
Lea
der
ship
Str
ate
gy
ap
pro
ved
at
Bo
ard
Sep
t 2
01
9
•Sh
ad
ow
Bo
ard
Pro
gra
mm
e co
mm
ence
d in
Sep
t 2
01
9. t
he
pro
gra
mm
e h
as
bee
n w
ell a
tten
ded
, rec
eive
d a
nd
is c
on
tin
uin
g
•Tr
ium
vira
te D
evel
op
men
t P
rog
ram
me
du
e to
co
mm
ence
13
th/1
4th
No
v –
focu
ssed
co
nve
rsa
tio
ns
for
9 x
tri
um
vira
te le
ad
s (A
DO
/AM
D/H
oN
) &
3 x
Exe
c Le
ad
s•
‘Fo
un
da
tio
ns
of
Lea
der
ship
Pro
gra
mm
e’ –
co-d
esig
n w
ith
Asp
ire
for
lau
nch
in F
eb 2
02
0 –
to e
sta
blis
h t
he
‘So
uth
po
rt &
Orm
skir
k W
ay’
of
lea
der
ship
fo
r a
ll st
aff
(2
02
0)
•N
ew C
on
sult
an
ts/S
AS
Do
cto
rs p
rog
ram
me
(20
20
) -
sco
pin
g e
xerc
ise
com
ple
ted
, sp
ecif
ica
tio
n d
ocu
men
t w
ith
Med
ica
l Dir
ecto
r•
Ap
pre
nti
cesh
ip L
evy
–sc
op
ing
exe
rcis
e to
ga
in f
eed
ba
ck o
n t
he
Tru
st’s
pro
po
sal t
o s
pen
d 2
5%
of
ap
pre
nti
cesh
ip le
vy w
ith
pa
rtn
ero
rga
nis
ati
on
s (P
ap
er t
o H
MB
No
v 2
01
9)
•Le
ad
ing
Hea
lth
y W
ork
pla
ces
–b
esp
oke
tra
inin
g d
ay
un
der
dev
elo
pm
ent
wit
h a
fo
cus
on
su
pp
ort
ing
att
end
an
ce t
o b
e p
ilote
d in
Q4
•
Cu
sto
mer
Ser
vice
tra
inin
g u
nd
er c
on
sid
era
tio
n f
or
roll
ou
t st
art
ing
Q4
HEA
LTH
AN
D W
ELLB
EIN
G
•H
ealt
h &
Wel
lbei
ng
Str
ate
gy
ap
pro
ved
at
Wo
rkfo
rce
Co
mm
itte
e Se
pte
mb
er.
•R
evie
wed
an
d u
pd
ate
d t
he
Hea
lth
an
d W
ellb
ein
g (
sick
nes
s a
bse
nce
) act
ion
pla
n f
or
NH
SI p
roje
ct•
To le
ad
on
th
is y
ear’
s F
lu c
am
pa
ign
–2
01
9/2
020
CQ
UIN
N is
fo
r 8
0%
of
fro
ntl
ine
hea
lth
care
wo
rker
s to
be
vacc
ina
ted
. Th
e Tr
ust
rea
ched
th
e 8
0%
ta
rget
on
th
e w
eek
com
men
cin
g
11
/11
/20
19 a
hea
d o
f th
e ca
mp
aig
n s
ched
ule
•
Pro
vid
e ‘m
enta
l hea
lth
fir
st a
id’ t
o s
taff
, ‘M
enta
l Hea
lth
Fir
st A
id T
rain
ing
’ co
nsi
der
ati
on
giv
en o
n h
ow
to
pro
mo
te t
he
role
inlin
e w
ith
th
e H
ealt
h &
Wel
lbei
ng
ag
end
a.
•Tr
ust
Att
end
an
ce a
t N
HSi
Hea
lth
an
d W
ellb
ein
g S
um
mit
–7
thN
ove
mb
er 2
01
9 –
sha
re le
arn
ing
an
d e
xper
ien
ces
wit
h o
ther
pro
vid
ers
on
Hea
lth
& W
ellb
ein
g im
pro
vem
ent
pro
gra
mm
e
14
Page 173 of 210

15
WO
RK
FOR
CE
AM
BER
Key
Ach
ieve
men
ts/P
rogr
ess
(3
)O
D, C
ULT
UR
E A
ND
STA
FF E
NG
AG
EMEN
T
•So
Pro
ud
Big
Co
nve
rsa
tio
ns
con
tin
ue
acr
oss
th
e o
rga
nis
ati
on
–d
ata
ga
ther
ing
fo
r b
eha
vio
urs
th
at
un
der
pin
ou
r SC
OP
E va
lues
, fo
cus
gro
up
to
be
hel
d N
ov/
Dec
20
19
•St
aff
En
ga
gem
ent
Stra
teg
y a
pp
rove
d a
t B
oa
rd S
ept
20
19
•In
-ho
use
co
ach
ing
ser
vice
lau
nch
ed O
ct 2
01
9. P
urc
ha
se o
f o
nlin
e co
ach
ing
mo
du
les
for
all
sta
ff t
o a
cces
s fo
r a
12
mo
nth
per
iod
(2
02
0)
•St
aff
FFT
–in
crea
se in
co
mp
leti
on
s fr
om
2.1
% (
Q1
) to
13
.7%
(Q2
) -
CB
U in
fog
rap
hic
s ci
rcu
late
d e
arl
y N
ov
20
19
•St
aff
Su
rvey
lau
nch
ed O
ct 2
01
9 –
incr
ease
in c
om
mu
nic
ati
on
s vi
a e
-co
mm
s a
nd
so
cia
l med
ia.
Cu
rren
t re
spo
nse
ra
te 3
1%
. C
losi
ng
Da
te 2
9th
No
vem
ber
•Ta
len
t M
an
ag
emen
t Se
lf-D
iag
no
stic
To
ol –
curr
entl
y o
ut
for
con
sult
ati
on
–o
nlin
e re
po
rt e
xpec
ted
Dec
20
19
•C
on
tin
ued
bes
po
ke O
D In
terv
enti
on
s to
su
pp
ort
th
e ro
ll o
ut
of
SON
AA
S &
tea
m d
evel
op
men
ts f
or
spec
ific
ho
t sp
ot
are
as
•C
orp
ora
te In
du
ctio
n r
evie
w t
ake
n p
lace
, rep
ort
to
be
tab
led
at
HM
B in
No
vem
ber
20
19
.•
Bo
ard
Vis
ibili
ty i
nit
iati
ves
on
go
ing
–w
ill b
e re
view
ed w
hen
new
Ch
ief
Exec
uti
ve c
om
men
ces
in p
ost
. •
Mo
nth
ly V
alu
ing
Ou
r P
eop
le G
rou
p m
eeti
ng
s to
del
iver
Wo
rkfo
rce
& O
D P
lan
•SO
Pro
ud
Co
nve
rsa
tio
ns
–fo
cuss
ed c
on
vers
ati
on
s o
n t
he
beh
avi
ou
rs t
o u
nd
erp
in o
ur
SCO
PE
Va
lues
–N
ov
& D
ec 2
01
9
•R
elo
cati
on
of
HR
co
nsu
lta
tio
n h
as
con
clu
ded
. Fu
rth
er c
ab
ling
, net
wo
rkin
g a
nd
infr
ast
ruct
ure
wo
rk h
as
beg
an
to
be
un
der
take
n i
n o
rder
to
su
pp
ort
th
e a
dd
itio
na
l wo
rkst
ati
on
s,
con
tra
cto
rs h
ave
bee
n s
ou
rced
an
d h
ave
beg
an
to
un
der
take
th
is p
iece
of
wo
rk.
•W
ork
forc
eEf
fici
enci
es Im
pro
vem
ent
pro
gra
mm
e sc
op
ed a
nd
go
vern
an
ce a
rra
ng
emen
ts p
rop
ose
d v
ia P
MO
.•
Ag
reem
ent
ob
tain
ed t
o im
ple
men
t re
visi
on
s to
sa
lary
sa
crif
ice
veh
icle
s sc
hem
es t
o a
dd
ress
issu
es a
nd
ga
in im
pro
vem
ents
an
d e
ffic
ien
cies
•R
ost
erin
g p
olic
y d
evel
op
men
t –
att
ain
ed f
ina
l sig
n o
ff a
t p
olic
y ra
tifi
cati
on
gro
up
. •
Rev
iew
of
form
at
an
d b
eha
vio
ura
l co
ntr
act
of
the
Wo
rkfo
rce
Co
mm
itte
e
HR
IMP
RO
VEM
ENT
PR
IOR
ITIE
S
•W
ork
forc
e Im
pro
vem
ent
Gro
up
-h
eld
mo
nth
ly–
dri
ver
dia
gra
ms
& a
ctio
n p
lan
s in
pla
ce –
rep
ort
s in
to H
osp
ita
l Im
pro
vem
ent
Bo
ard
•C
ore
ma
nd
ato
ry t
rain
ing
rem
ain
s a
bo
ve t
he
Tru
st t
arg
et a
t 8
8.3
4%
(31
/10
/19
)•
Co
nti
nu
ed r
edu
ctio
n o
f Y
TD s
ickn
ess
ab
sen
ce r
ate
–0
.53
% r
edu
ctio
n s
ince
Dec
emb
er 2
01
8•
Sup
po
rtin
g A
tten
da
nce
Po
licy
Rev
iew
•Em
plo
yee
Rel
ati
on
s P
olic
y re
view
•In
crea
se P
DR
co
mp
lian
ce•
Incr
ease
sta
ff s
urv
ey r
esp
on
se r
ate
•R
edu
ce T
ime
to H
ire
•In
crea
se f
lu v
acc
ina
tio
n r
ate
fo
r cl
inic
al s
taff
•A
pp
oin
tmen
t o
f ke
y en
ab
ler
role
s fo
r H
R T
ran
sfo
rma
tio
na
l Ch
an
ge
as
per
th
e B
usi
nes
s C
ase
•R
e-es
tab
lish
men
t St
aff
Net
wo
rk M
eeti
ng
s•
Pri
ori
ty r
ecru
itm
ent
to r
ole
s th
at
sup
po
rt t
he
win
ter
pla
n TB
207_
19 S
IP P
rese
ntat
ion
Dec
19
Page 174 of 210

16
Key
Ris
ks/I
ssu
es
Mit
igat
ing
Act
ion
sR
AG
Sick
ne
ss A
bse
nce
rate
re
du
ctio
nN
ew p
olic
y, H
ealt
h a
nd
Wel
lbei
ng
init
iati
ves,
ear
ly s
up
po
rt t
o “
Ho
t Sp
ot”
are
as,
Trai
nin
g fo
r al
l man
ager
s o
n r
ole
an
d r
esp
on
sib
ility
of
dea
ling
wit
h s
ickn
ess
abse
nce
. P
olic
y u
nd
er r
evie
w a
t 6
mo
nth
s p
ost
imp
lem
enta
tio
n.
Rev
iew
dis
cuss
ion
s to
ok
pla
ce
wit
h a
ll ke
y st
akeh
old
ers
on
06
/09
/19
an
d 0
1/1
1/1
9. H
ealt
hy
deb
ate
and
dis
cuss
ion
to
ok
pla
ce w
ith
th
ose
wh
o a
tten
ded
on
th
e 0
1/1
1/1
9 t
her
efo
re m
ovi
ng
the
revi
ew
forw
ard
. Fin
al f
urt
her
dat
e to
co
ncl
ud
e th
e re
view
is t
o b
e ar
ran
ged
.
A
De
velo
pm
en
t o
f ad
min
an
d c
leri
cal s
taff
ban
kEn
gage
men
t w
ith
NH
SP t
o p
rovi
de
sup
po
rt t
o d
evel
op
men
t o
f ad
min
an
d c
leri
cal b
ank.
P
roje
cto
ngo
ing.
A
CB
U’s
fai
ling
to m
ee
t tr
aje
cto
rie
s o
f im
pro
vem
en
t fo
r ap
pra
isal
sP
DR
co
mp
lian
ce c
on
tin
ues
to
be
chal
len
ge f
or
the
org
anis
atio
n a
nd
is c
urr
entl
y o
n a
d
ow
nw
ard
tra
ject
ory
. Iss
ue
du
e to
be
add
ress
ed in
WIG
to
dis
cuss
wit
h k
ey
stak
eho
lder
s h
ow
to
mo
ve f
orw
ard
wit
h in
crea
sin
g co
mp
lian
ce. I
n a
dd
itio
n t
o
com
plia
nce
bei
ng
chal
len
ge,
qu
alit
y o
f ap
pra
isal
s is
an
issu
e fo
r th
e o
rgan
isat
ion
an
d
the
OD
tea
m is
cu
rren
tly
carr
yin
g o
ut
a m
yth
bu
ster
in o
rder
to
try
to
incr
ease
co
mp
lian
ce a
nd
ad
dre
ss t
he
issu
e ar
ou
nd
qu
alit
y. T
eam
ob
ject
ives
als
o b
ein
g co
nsi
der
ed.
A
Lack
of
recr
uit
ing
man
age
r o
wn
ers
hip
in
ke
y re
spo
nsi
bili
tie
s to
imp
rove
Tim
e t
o
Hir
eR
ecru
itm
ent
web
site
to
be
dev
elo
ped
. E
scal
atio
n p
roce
ss a
nd
dee
p d
ive
into
b
reac
hes
of
KP
I tar
gets
req
uir
ed.
Mee
tin
gs b
ein
g se
t u
p w
ith
CB
U’s
to
un
der
stan
d
role
s an
d r
esp
on
sib
iliti
es w
ith
in t
he
pro
cess
. Tra
inin
g se
ssio
ns
for
Rec
ruit
ing
Man
ager
s se
t u
p in
No
vem
ber
/ D
ecem
ber
to
ro
ll o
ut
and
to
ou
tlin
e re
spo
nsi
ble
an
d
acco
un
tab
ility
th
rou
gho
ut
the
recr
uit
men
t jo
urn
ey.
A
Cap
acit
y o
f th
eH
R B
usi
ne
ss S
erv
ice
s Te
am -
The
re a
rea
sign
ific
ant
nu
mb
er
or
Org
anis
atio
nal
Ch
ange
pie
ces
of
wo
rk t
o c
om
e o
ut
of
the
CIP
an
d M
od
el h
osp
ital
w
ork
wh
ich
will
cau
se a
sig
nif
ican
t am
ou
nt
of
pre
ssu
re o
n t
he
op
era
tio
nal
HR
b
usi
ne
ss s
erv
ice
s te
am.
The
re is
als
o n
ow
un
pla
nn
ed
ab
sen
ce in
th
e t
eam
an
d
som
e n
ew
ap
po
intm
en
ts o
f te
am m
em
be
rs w
ho
are
no
t as
exp
eri
en
ced
as
som
e
colle
agu
es.
Tem
po
rary
fun
din
g se
cure
d f
rom
E&
F to
su
pp
ort
th
e vo
lum
e o
f su
pp
ort
an
d w
ork
b
ein
g u
nd
erta
ken
in t
hat
CB
U.
R
QI T
rain
ing
Pro
gram
me
–to
de
velo
p a
tra
inin
g ac
tio
n p
lan
fo
llow
ing
the
en
d o
f th
e N
HSi
‘In
tro
du
ctio
nto
QI’
N
HSI
dis
cuss
ed w
ith
Hea
d o
f P
MO
–p
aper
pre
sen
ted
to
HM
B n
o f
urt
her
act
ion
agr
eed
R
WO
RK
FOR
CE
(4)
AM
BER
Page 175 of 210

AC
UTE
SU
STA
INA
BIL
ITY
RA
GR
atin
g
17
Key
Ach
ieve
me
nts
/Pro
gres
s in
Mo
nth
CM
HC
P M
id Y
ear
rev
iew
was
su
cces
sfu
l wit
h t
he
full
£4
97
kre
qu
este
d in
May
bei
ng
rele
ased
to
th
e p
rogr
amm
e (p
revi
ou
sly
they
had
rel
ease
d in
pri
nci
ple
th
e fi
rst
£4
00
k)D
raft
Ou
tlin
e P
CB
C d
eliv
ered
on
31
stO
cto
ber
Join
t C
om
mit
tee
hel
dth
eir
inau
gura
l mee
tin
g o
n t
he
7th
No
vem
ber
to
rev
iew
th
e d
raft
ou
tlin
e P
CB
CA
rev
iew
gro
up
mad
e u
p o
f C
CG
, NH
SE, C
MH
CP
an
d T
rust
co
lleag
ues
met
on
th
e 8
thN
ove
mb
er
Key
Ris
ks/I
ssu
es
Mit
igat
ing
Act
ion
sR
AG
The
lack
of
avai
lab
le c
apit
alto
en
able
del
iver
y o
f an
y o
f th
e em
ergi
ng
scen
ario
s w
ill im
pac
t o
n t
he
syst
em
s ab
ility
to
co
nsu
lt w
ith
th
e p
ub
licTh
e la
ck o
f cu
rren
t an
d p
roje
cte
d c
linic
al w
ork
forc
e to
en
able
d
eliv
ery
of
any
of
the
clin
ical
mo
del
s to
be
real
ised
Exp
lori
ng
alte
rnat
ive
del
iver
y sc
en
ario
s an
d o
ngo
ing
dis
cuss
ion
s w
ith
N
HSE
I an
d C
MH
CP
Exp
lori
ng
alte
rnat
ive
wo
rkfo
rce
mo
del
s to
en
able
del
iver
y in
clu
din
g o
pp
ort
un
itie
s ar
ou
nd
sin
gle
serv
ice
mo
del
s an
d o
ngo
ing
dis
cuss
ion
s w
ith
NH
SEI a
nd
CM
HC
P
R
Key
Ach
ieve
men
ts/P
rogr
ess
SER
VIC
E C
HA
NG
E P
RO
PO
SAL
The
dra
ft o
utl
ine
PC
BC
was
del
iver
ed o
n t
he
31
stO
cto
ber
20
19
set
tin
g o
ut
the
fou
nd
atio
n o
f a
full
bu
sin
ess
case
des
crib
ing
wh
ere
we
are
, wh
ere
we
wan
t to
be
and
ho
w w
e w
ill g
et t
her
e. T
he
new
mo
del
s o
f ca
re h
ave
bee
n p
rese
nte
d in
th
e d
raft
ou
tlin
e P
CB
C a
lon
gsid
e 5
em
ergi
ng
de
liver
y sc
enar
ios
ran
gin
g fr
om
a b
ran
d n
ew h
osp
ital
bu
ild t
hro
ugh
to
op
tim
isin
g th
e ex
isti
ng
two
sit
es w
ith
as
littl
e ca
pit
al a
s p
oss
ible
. Alt
ho
ugh
th
ed
raft
ou
tlin
e P
CB
C d
escr
ibes
th
e st
and
ard
s o
f cl
inic
al c
are
ou
r p
op
ula
tio
ns
sho
uld
exp
ect
tor
rece
ive
th
rou
gh t
he
care
mo
del
s, t
he
del
iver
y sc
en
ario
s d
o n
ot
yet
iden
tify
a f
inan
cial
or
wo
rkfo
rce
sust
ain
able
so
luti
on
. Fo
llow
ing
revi
ew w
ith
th
e Tr
ust
Bo
ard
, Jo
int
Co
mm
itte
e, S
efto
n T
ran
sfo
rmat
ion
Bo
ard
an
d a
rev
iew
gro
up
co
nsi
stin
g o
f N
HSE
I an
d C
MH
CP
co
lleag
ues
th
e ac
ute
su
stai
nab
ility
pro
gram
me
is b
ein
g re
fres
hed
alig
nin
g n
ew p
rio
riti
es t
o a
del
iver
y p
lan
.
CLI
NIC
AL
SCEN
AR
IOS
All
5 c
linic
ally
led
mo
del
s o
f ca
re h
ave
un
der
gon
e th
e fi
nal
sta
ge o
f th
e ch
eck
and
ch
alle
nge
pro
cess
-th
ese
mo
del
s o
f ca
re o
f st
ill d
raft
an
d w
ill u
nd
ergo
fu
rth
er d
evel
op
men
t in
th
e n
ext
stag
e as
par
t o
f a
wid
er e
nga
gem
ent
app
roac
h w
ith
pat
ien
ts a
nd
th
e p
ub
lic p
ost
pu
rdah
an
d C
hri
stm
as (e
xpec
ted
to
sta
rt
in J
anu
ary
20
20
)
ESTA
TES
SO
LUTI
ON
S
Sch
edu
les
of
acco
mm
od
atio
n a
nd
ind
icat
ive
cap
ital
cost
s fo
r th
e in
itia
l em
ergi
ng
sce
nar
ios
hav
e b
een
pro
du
ced
. Fu
rth
er w
ork
is r
equ
ired
to
val
idat
e th
e fi
nd
ings
an
d a
lign
wit
h n
ew s
cen
ario
s to
be
dev
elo
ped
FIN
AN
CE
SOLU
TIO
NS
The
Seft
on
Tra
nsf
orm
atio
n F
inan
ce D
irec
tors
Gro
up
co
nti
nu
e to
hav
e o
vers
igh
t o
f th
e ac
tivi
ty a
nd
fin
anci
al m
od
ellin
g an
d h
ave
set
the
sco
pe
for
the
nex
t p
has
e o
f w
ork
TB
207_
19 S
IP P
rese
ntat
ion
Dec
19
Page 176 of 210


PUBLIC TRUST BOARD 4 December 2019
Agenda Item TB209/19 Report
Title
Charity Name Change
Executive Lead Steve Shanahan, Director of Finance
Lead Officer Mark Wilson, Assistant Director of Finance
Action Required
(Definitions below)
To Approve To Note
To Assure To Receive
For Information
Executive Summary
This paper requests the renaming of the Charity from “Southport and Ormskirk Hospital NHS Trust Charitable Fund” to “Southport and Ormskirk Hospitals Charity”. A Board resolution is required so that a formal application to the Charity Commission can be made to change the name. R e c o m m e n d a t i o n s :
The Board is asked to approve the change of name for the charity.
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
Strategic Objective Principal Risk
SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
TB
209_
19 C
harit
y N
ame
Cha
nge
Dec
19
Page 177 of 210

SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
If the system does not have an agreed acute services strategy it may lead to non-alignment of partner organisations plans resulting in the inability to develop and deliver sustainable services
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
Caring Statutory Requirement
Effective Annual Business Plan Priority
Responsive Best Practice
Safe Service Change
Well Led
Impact (is there an impact arising from the report on any of the following?)
Compliance Legal
Engagement and Communication Quality & Safety
Equality Risk
Finance Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Committee)
An on line submission to the Charity Commission will be made and the Board resolution attached.
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
Page 178 of 210

Charity name change
1 Introduction 1.1 As part of the charity re-launch strategy a minor amendment is required to the charity name.
1.2 To formalise this, the Charity Commission require a Board resolution authorising the name
change.
2 Name change
2.1 The name change is from “Southport & Ormskirk Hospital NHS Trust Charitable Fund” to “Southport and Ormskirk Hospitals Charity”.
2.2 The Board should note that the marketing materials have already been prepared under the new proposed name.
2.3 Logo is shown below:
3 Recommendation
3.1 It is recommended that the Board approve the change of name of the charity.
TB
209_
19 C
harit
y N
ame
Cha
nge
Dec
19
Page 179 of 210


PUBLIC TRUST BOARD 4 December 2019
Agenda Item TB209/19 Report
Title
Charity Investment Policy
Executive Lead Steve Shanahan, Director of Finance
Lead Officer Mark Wilson, Assistant Director of Finance
Action Required
(Definitions below)
To Approve To Note
To Assure To Receive
For Information
Executive Summary
The majority of the charity’s monies are invested in a portfolio of shares and gilts. The Investment policy provides a framework for this investment together with ethical constraints. A number of changes to the existing policy are contained in this report and the final policy for approval is shown in appendix 1. R e c o m m e n d a t i o n s :
It is recommended that the Trust Board acting as the Corporate Trustee approve the charity’s
investment policy.
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
Strategic Objective Principal Risk
SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
TB
209_
19 C
harit
y In
vest
men
t Pol
icy
Dec
19
Page 180 of 210

SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
If the system does not have an agreed acute services strategy it may lead to non-alignment of partner organisations plans resulting in the inability to develop and deliver sustainable services
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
Caring Statutory Requirement
Effective Annual Business Plan Priority
Responsive Best Practice
Safe Service Change
Well Led
Impact (is there an impact arising from the report on any of the following?)
Compliance Legal
Engagement and Communication Quality & Safety
Equality Risk
Finance Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Committee)
Policy to be sent to Investment advisors.
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
Page 181 of 210

Charity Investment Policy
1 Introduction 1.1 The purpose of the investment policy is to ensure that the charitable fund portfolio is effectively
managed by providing a framework to the Investment advisors that sets out the allocation to each asset class within the constraints set by the charity.
1.2 This policy covers the framework allocation and the ethical constraints.
2 Policy changes
2.1 UK and overseas equity should be combined rather than listed separately with a limited risk of 75%.
2.2 Upper limit on alternatives (now that it encompasses a wider range of assets) should be lifted to 15%.
2.3 Include a comment on capacity for loss in our investment policy statements – see below.
2.4 ‘The Charity has a moderate ability to bear investment losses which means that in extreme circumstances falls in the value of the portfolio of up to 35% would not have a material impact on the overall financial ability to carry out its function. Under the current structure and based on historic data, the investment manager estimates this strategy has the potential to fall up to 23% peak to trough in an investment cycle.’
2.5 On ethical investments include the point that the charity will not invest in no win no fee medical claims companies.
3 Charitable Fund Committee
3.1 The above changes have been agreed by the Charity Committee and appendix 1 sets out the final investment policy.
3.2 The Investment advisors also provided a comparison with other charities in terms of risk
appetite which has been shared with the Committee members. 4 Risk appetite 4.1 Based on other charities, this investment policy in general is slightly on the cautious side of the
‘average’ charity, with a marginally lower equity content. 4.2 The reason for this is due to the ongoing potential that the portfolio may need to help meet
short term requirements when there are cash flow issues and investments need to be liquidated.
4.3 With the charity relaunch and the prospect of a significant increase in donations, then a further
review in 6 months may be required to re-assess risk appetite. 5 Conclusion 5.1 The final investment policy satisfies the charity’s objectives and has been through the
appropriate review and governance. 6 Recommendation 6.1 It is recommended that the Trust Board acting as the Corporate Trustee approve the charity’s
investment policy.
TB
209_
19 C
harit
y In
vest
men
t Pol
icy
Dec
19
Page 182 of 210

Appendix 1 – Charity Investment policy
Introduction The purpose of the investment policy is to ensure that the charitable fund portfolio is effectively managed by providing a framework to the Investment advisors that sets out the allocation to each asset class within the constraints set by the charity. Allocation
Asset Class Allocation Tactical Variance
Total range
UK Sovereign Debt 30% +/-10% 20% to 40%
Cash 0% +15% 0% to 15%
Equity Investments 65% +/-10% 55% to 75%
Alternative Assets (hedge, commercial property, commodities)
5% +/- 10% 0% to 15%
In terms of the risk profile and time horizon a medium risk strategy should be adopted with an indefinite time horizon. Ethical constraints The following ethical investment constraints have been set by the Trustees, which means that investments in those companies involved wholly or substantially in the following are excluded:
1. Tobacco. 2. Armaments. 3. Alcohol. 4. Betting/gaming. 5. Payday loans. 6. No win no fee medical claims companies.
Wholly or substantially is defined as more than two thirds of the business. Equity constraint No individual direct equity holding should account for more than 10% of the equity exposure of the fund. Portfolio transfers Transfers of cash into and out of the portfolio should be managed between the Charity and the Investment advisors to ensure there is sufficient notice period to make informed decisions. Where the Trust foresees that it will require funds to be liquidated from the portfolio, the Charity should inform the Investment advisors with details of the value to be liquidated and the required liquidation date.
Page 183 of 210

Surplus funds in the charity’s bank account over and above the current requirements should be transferred to the Investment advisors. The Assistant Director of Finance has delegated authority to transfer monies into the portfolio and to request transfers out. Reserves The value of the portfolio must always be greater than the charity’s reserve target. The reserve is made up of the unrestricted funds (general). Targets Income generation from the portfolio is from dividends on equity shares and UK sovereign debt. The target income generation is reviewed annually and currently stands at 3.5% of the average annual portfolio value. Capacity for loss The Charity has a moderate ability to bear investment losses which means that in extreme circumstances falls in the value of the portfolio of up to 35% would not have a material impact on the overall financial ability to carry out its function. Under the current structure and based on historic data, the investment manager estimates this strategy has the potential to fall up to 23% peak to trough in an investment cycle. Monitoring The Investment advisors will report each quarter to the Charitable Fund Committee. The report will include the following:
1. Full details of the portfolio. 2. Comparison of returns against an appropriate industry benchmark. 3. Income generation for the quarter. 4. A table showing the actual allocation percentages by asset class.
Review An annual performance review will take place at the end of each financial year. This in turn will feed into the investment policy review where the allocation of the portfolio can be considered together with the income generation target.
TB
209_
19 C
harit
y In
vest
men
t Pol
icy
Dec
19
Page 184 of 210


PUBLIC TRUST BOARD 4 December 2019
Agenda Item TB210/19a Report Title Learning lessons to improve
Our People Practices
Executive Lead Jane Royds, Director of HR and OD
Lead Officer Laura Hilton, Head of HR
Action Required
(Definitions below)
To Approve To Note
✓ To Assure ✓ To Receive
For Information
Executive Summary
The Committee’s highlight report for September 2019 is set out below:
Alert N/A Advise There are a number of recommendations in the attached paper that need to be agreed in order to strengthen the Trusts compliance with investigation findings and recommendations. Further timescales were requested following presentation of this paper, at board in October 2019 in relation to the implementation of the Employee Relations Tracker system (Empactis). The timescales have been set out in the revised paper. Full implementation of the Employee Relations Tracker system (Empactis) is expected by May 2020. Assure
The board can take assurance that many of the recommendations set out by Baroness Harding are
already in place at S&O.
Recommendation: This paper is to assure the Board.
Strategic Objective(s) and Principal Risks(s)
(The content provides evidence for the following Trust’s strategic objectives for 2019/20)
Strategic Objective Principal Risk
SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
✓ SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in question.
TB
210_
19a
Lear
ning
Les
sons
to Im
prov
e ou
r P
eopl
e P
ract
ices
Rep
ort
- U
pd...
Page 185 of 210

✓ SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
✓ SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
✓ SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
If the system does not have an agreed acute services strategy it may lead to non-alignment of partner organisations plans resulting in the inability to develop and deliver sustainable services
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
✓ Caring ✓ Statutory Requirement
✓ Effective Annual Business Plan Priority
Responsive ✓ Best Practice
✓ Safe Service Change
✓ Well Led
Impact (is there an impact arising from the report on any of the following?)
✓ Compliance Legal
✓ Engagement and Communication Quality & Safety
Equality Risk
Finance ✓ Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Board/Committee/Group)
A further update paper to be provided to Workforce Committee in October 2019.
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee ✓ Workforce Committee
GUIDE TO ACTIONS REQUIRED (TO BE REMOVED BEFORE ISSUE):
Approve: To formally agree the receipt of a report and its recommendations OR a particular course of action
Receive: To discuss in depth a report, noting its implications for the Board or Trust without needing to formally approve
Note: For the intelligence of the Board without the in-depth discussion as above
Assure: To apprise the Board that controls and assurances are in place
For Information: Literally, to inform the Board
Page 186 of 210

Learning lessons to improve our people practices 1. Introduction
This paper is to advise the Trust Board about the content of a letter sent to Provider chief executives and chairs on the 24th May 2019 from Baroness Dido Harding, Chair, NHS England and NHS Improvement about why Trusts need to learn lessons to improve our people practices. The letter shares the outcomes of an important piece of work recently undertaken in response to a very tragic event that occurred at a London NHS trust three years ago. This paper will provide details of the case of Amin Abdullah who was the subject of an investigation and disciplinary procedure in late 2015 and includes additional guidance relating to the management and oversight of local investigation and disciplinary procedures. 2. Background In the case of Amin Abdullah the protracted procedure culminated in Amin’s summary dismissal on the grounds of gross misconduct. Tragically, in February 2016 just prior to an arranged appeal hearing, Amin took his own life. This triggered the commissioning of an independent inquiry undertaken by Verita Consulting, the findings of which were reported to the board of the employing Trust and to NHS Improvement in August 2018. The report concluded that, in addition to serious procedural errors having been made, throughout the investigation and disciplinary process Amin was treated very poorly, to the extent that his mental health was severely impacted. Verita’s recommendations were accepted by the Trust, in full, and have largely been implemented. Subsequently, NHS Improvement established a ‘task and finish’ advisory group to consider to what extent the failings identified in Amin’s case are either unique to that Trust or more widespread across the NHS, and what learning can be applied. Comprising of multi-professional stakeholders and subject matter experts representing both the NHS and external bodies, together with an advocate for Amin’s partner, the Group conducted an independent analysis of both the Verita findings and several historical disciplinary cases, the outcomes of which had attracted criticism in Employment Tribunal proceedings and judgements. HR directors of provider organisations were advised of the Group’s activity and invited to share details of any local experiences and/or examples of measures being taken to improve the management of employment issues. The analysis highlighted several key themes associated with the Verita inquiry which were also common to other historical cases considered. Principal among these were: poor framing of concerns and allegations; inconsistency in the fair and effective application of local policies and procedures; lack of adherence to best practice guidance; variation in the quality of investigations; shortcomings in the management of conflicts of interest; insufficient consideration and support of the health and wellbeing of individuals; and an over-reliance on the immediate application of formal procedures, rather than consideration of alternative responses to concerns. This paper aims to outline where S&O’s current processes and procedures are against the 7 areas of focus set out in Baroness Harding’s guidance and the Business HR team’s commitment to further improve and strengthen our people practice in relation to the management of employee relations cases. 3. Guidance relating to the management and oversight of local investigation and disciplinary
procedures 3.1. Adhering to best practice The Trusts key disciplinary and grievance policies are in the process of being significantly reviewed to ensure that they maintain keeping in line with current best practice as advised in the Arbitration Conciliation Advisory Service (ACAS) Code of practice on disciplinary and grievance procedures. The Trusts Managing High Professional Standards policy applicable to the management of our medical workforce has also recently been reviewed.
TB
210_
19a
Lear
ning
Les
sons
to Im
prov
e ou
r P
eopl
e P
ract
ices
Rep
ort
- U
pd...
Page 187 of 210
The recommendation of Baroness Harding suggests that procedures should also follow the principles of the NMCs best practice guidance on local investigations (when published). The Business HR team in partnership with staff side will ensure review of this once published and make any amendments to our process if required. All formal employee relations cases have an assigned HR representative to advise and support the management of procedures. Through this the Business HR team ensure that independence and objectivity is applied throughout the process and action is taken to prevent any perceived conflicts of interest. This is supported by our policies and procedures and also applicable to the HR representative assigned to the differing steps of the process. Where required advisors to disciplinary and appeal panels may also be assigned as subject matters experts to ensure objectivity. All employee relations policies and procedures ‘owned’ by the Business HR team have recently been reviewed or are currently going through review and will be reviewed in accordance with the recommendations following this independent investigation. 3.2. Applying rigorous decision making Trust processes can be considered to be in line with the application of just culture principles. Policies have been drafted to ensure that preliminary investigative work is undertaken before any process progresses to a formal procedure. Within the Trusts revised disciplinary policy the usage of the NHS Incident Decision tree (Just Culture Guide) is proposed to be used on the outset of any employee relations case to guide and inform the appropriate next steps, for example when considering the suspension of an employee where a serious allegation has come to light. If following a preliminary investigation the senior manager in possession of the allegation recommends suspension, the Business HR team ensure that this is escalated to the respective Director of the Trust, Deputy Director, Assistant Director of Operations, Head of Nursing or equivalent. By adopting this practice ensures plurality and informed decisions are made on the outset. The Trust has significantly invested into their mediation service within the last 3 years and now has 27 trained mediators available throughout the Organisation. Where mediation is deemed appropriate, this is an enabler for cases to be managed at a local and informal stage of the process.
3.3. Ensuring people are trained and competent to carry out their role The appointment of investigating officers is decided in collaboration of the case manager/commissioning manager (revised policy) and the assigned HR representative. When appointing investigating officers this will be dependent on the seniority, neutrality and experience of the individual. As all employee relations cases will be assigned a HR representative, it is their role to guide, advise and coach that investigating officer as the process progresses. To support the competence of investigating officers, hearing and appeal boards, the Trust has guides and training established which are available on the Trusts intranet. The Business HR team will also review those guides and training programmes to ensure consistency with the revised policies. 3.4. Assigning sufficient resources Within the Business HR team monthly case reviews are held as a team which allows capacity and demand oversight and appropriate delegation to ensure the timeliness of investigations internal to the Business HR team. Any concerns regarding resource will be escalated to the appropriate senior member of the management team to ensure resolution. Additionally the Trust has invested in the development and resourced a bank of investigating officers to ensure that the Trust has access to independent investigating officers should resourcing be of concern.
Page 188 of 210

The Business HR team have scoped out and requested as part of the HR Business Case Investment in an Employee Relations Tracker system (Empactis) which is recommended by NHSI and will automate some of the processes associated with ER cases and ensure timely responses/reminders in line with the policy timescales. The system will enable timescales in relation to cases to be reported on easily and the identification of any hotspots areas in order to ensure effective and timely interventions. A HR Business Partner – Project Lead has been appointed to lead on the roll out of the implementation of this system and will commence in post on 9th December 2019. Timescales in relation to this policy are as follows:
• Detailed Project Initial Document and Project Plan to be drafted December 2019
• ESR Data cleanse to commence December 2019 – January 2020
• Procurement and Information Governance process to commence December 2019
• Contract and Information Governance sign off by mid-January 2020
• Project to initiate February 2020
• Phase 1 will focus on Case Management and include Disciplinary, Grievance, MHPS, Dignity at Work case types.
o This phase will include ESR interfacing. o The 1st Case Type to go-live as a full workflow for manager use will be Disciplinary. o Other case types will initially be tracked using the platform i.e. not as a workflow and
so will continue to be managed by HR; workflow for the remaining case types will introduced in a staged way during 2020.
• The Trust would like to be live by 31st May 2020 with Case Management. 3.5. Decisions relating to the implementation of suspensions / exclusions When a suspension is likely, the Business HR team ensure that the decision to suspend is escalated to the Director of the Trust, Deputy Director, Assistant Director of Operations, Head of Nursing or equivalent. The revised policy will ensure that the escalation of a decision to suspend ensures preliminary investigative work has been undertaken, that decisions to suspend are informed, safe and alternatives to suspensions are considered. 3.6. Safeguarding people health and wellbeing On the outset of an employee relations case the individual is reminded of the support services available to them through the Trusts health and wellbeing service and employee assistance provider. The individual is advised that a self-referral to those services can be made or alternatively a management referral will be made on their behalf. In some circumstances a case manager/commissioning manager may automatically refer an individual to support services dependent on the nature of the allegations or individuals circumstances. Once an employee relations case has been commissioned a terms of reference will be drafted by the case manager/commissioning manager that includes timeframes for the completion of the investigatory process and also when the individual will be informed of the outcome of the process. This timeframe will be shared with the individual by the investigating officer through the course of their investigation. The case manager/commissioning manager is responsible for keeping the individual informed on the progress of the investigation and any delays to the originally anticipated timeframe of completion. 3.7. Board level oversight Going forward the board will receive data relating to employee relations cases via a dashboard presented at Workforce Committee held on a monthly basis. This group is chaired via the Director of HR and OD and the minutes and papers of that group are shared with the Board via the Corporate Governance structure. The board will also receive data relating to employee relations cases directly via the CBU Performance Review meetings chaired by the Chief Executive Officer.
TB
210_
19a
Lear
ning
Les
sons
to Im
prov
e ou
r P
eopl
e P
ract
ices
Rep
ort
- U
pd...
Page 189 of 210

Detailed discussions relating to employee relations cases are shared during the monthly one to one meetings held between the Head of HR and HR Business Partners. 4. Recommendations It is recommended that the board can take assurance that many of the recommendations set out by Baroness Harding are already in place at S&O. There are however areas that can be strengthened and the Business HR team will commit to improve those in the coming months, and will provide an assurance at regular intervals. . Actions to be taken:
• Review the contents of the NMCs ‘best practice guidance on local investigations’ when published, making any necessary amendments to process where needed.
• The team will develop a suspension pro-forma in order to record the process of escalation and informed decisions when the need to suspend arises. Whilst this can be evidenced at present this will ensure consistency and a central record of this information. Once developed a recommendation for this suspension pro-forma to be added as an appendices within the disciplinary policy to encourage its usage.
• The Business HR team to ensure evidence that a preliminary investigation has been undertaken prior to commencement of a formal process. Currently this can be difficult to evidence the separation of a preliminary and formal process.
• The Business HR team to will refresh a local training programme for investigations of employee relation cases.
• Continue to develop and review toolkits and guides to ensure they are fit for purpose.
• Add to terms of reference templates that the requirement for the commissioning manager to ensure wellbeing support is offered at regular intervals and a communication plan is established on the outset of an employee relations process.
• Develop and establish a governance framework in relation to the reporting of cases.
• Business Case funding will implement an employee relations case management system to ensure timeliness of case management. This system has shown much improvement when implemented in other Trusts.
• Investment in Employee Relations Tracker system – to automate some of the process and ensure timely responses in line with the policy timescales.
This paper is to assure the Board that an action plan is in place.
Page 190 of 210

Appendix 1
TB
210_
19a
Lear
ning
Les
sons
to Im
prov
e ou
r P
eopl
e P
ract
ices
Rep
ort
- U
pd...
Page 191 of 210


PUBLIC TRUST BOARD 4 November 2019
Agenda Item TB210/19b Report Title Workforce Disability Equality
Standard Report
Executive Lead Jane Royds: Director of Human Resources and OD
Lead Officer Bob Davies: Equality Lead
Action Required
(Definitions below)
To Approve To Note
To Assure ✓ To Receive
For Information
Executive Summary
The Committee’s highlight report for August 2019 is set out below:
Alert
• 30.48% of the workforce have not disclosed if they do or do not have a disability. The Trust
needs to promote to staff the purpose of self-reporting and self-reporting process on ESR.
Advise
• The WDES report highlights that staff with a disability have poorer experiences in areas such
as bullying and harassment and attending work when ill.
• Paper has been reformatted as per action following October’s Board meeting. New formatted
report was accepted at Workforce Committee in November 2019.
Assure
• The WDES action plan will be monitored and updated. Updates will be provided to the various
Trust groups / committees and the report and updates are also a requirement of the equality
section of the quality contract with the CCG’s.
Recommendation
The Workforce Committee is asked to receive the report.
Strategic Objective Principal Risk
✓ SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial resources the sustainability of services will be in
TB
210_
19b
FS
Wor
kfor
ce D
isab
ility
Equ
ality
Sta
ndar
d In
form
atio
n R
epor
t Apr
il 19
- M
ar 2
0
Page 192 of 210

question.
✓ SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
✓ SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
If the system does not have an agreed acute services strategy it may lead to non-alignment of partner organisations plans resulting in the inability to develop and deliver sustainable services
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
✓ Caring ✓ Statutory Requirement
✓ Effective Annual Business Plan Priority
✓ Responsive ✓ Best Practice
✓ Safe Service Change
✓ Well Led
Impact (is there an impact arising from the report on any of the following?)
Compliance ✓ Legal
✓ Engagement and Communication Quality & Safety
✓ Equality Risk
Finance ✓ Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Committee)
The Trust has compiled a WDES report and action plan that will be monitored at various Trust committees and groups i.e. Workforce Committee Valuing Our People Group, reporting is also a requirement in the CCG equality section of the quality contract, the Trust will set up a disability staff network to obtain the views of staff with a disability or long-term medical condition, the WDES action plan highlights areas for development i.e. Reporting a disability on ESR, Recruitment, Staff Bandings, Bullying and Harassment
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
Page 193 of 210

1
Southport and Ormskirk Hospital NHS Trust Workforce Disability Equality Standard Information Report April 2019 – March 2020
1. Executive Summary This paper provides a general overview of the Workforce Disability Equality Standard (WDES) and the metrics against the nine indicators within the Workforce Disability Equality Standard (WDES). It also provides analysis of the metrics and outlines actions (Appendix 1 WDES Action Plan) to address the gaps between the experience of Disabled and Non-disabled staff.
2. Introduction The Workforce Disability Equality Standard (WDES) is mandated by the NHS Standard Contract and will apply to all NHS Trusts and Foundation Trusts from April 2019. The WDES is a data-based standard that uses a series of measures (Metrics) to improve the experiences of Disabled staff in the NHS. The WDES comprises ten Metrics. All of the Metrics draw from existing data sources (recruitment dataset, ESR, NHS Staff Survey, HR data) with the exception of one; Metric 9b asks for narrative evidence of actions taken, to be written into the WDES annual report The Metrics have been developed to capture information relating to the experience of Disabled staff in the NHS. Research has shown that Disabled staff have poorer experiences in areas such as bullying and harassment and attending work when feeling ill, when compared to non-disabled staff. The ten Metrics have been informed by research by Middlesex and Bedford Universities, conducted on behalf of NHS England, and by Disability Rights UK on behalf of NHS Employers. The annual collection of the WDES Metrics will allow NHS Trusts and Foundation Trusts to better understand and improve the employment experiences of Disabled staff in the NHS. The WDES Metrics have been designed to be as simple and straightforward as possible. The development of the WDES owes a great deal to the consultation and engagement with NHS key stakeholders, including Disabled staff, trade unions and senior leaders.
3. WDES Highlights The information below provides highlights from the WDES report for 2018-19, the information also provides the Trust figures compared to the average for combined acute and community hospital. Please note this is the first year the WDES report have been compiled so there are no comparisons available. Q/ Do you have any physical or mental health conditions, disabilities or illnesses that have lasted or are expected to last for 12 months or more? (NHS staff survey 2018) Southport Ormskirk Hospital NHS Trust response is 19.8% other Trusts average is 17.1%, therefore SOHT is 2.7% above the national average response. The 2018-19 Trust ESR figures for staff highlighting they have a disability is 2.55% although19.8% of staff highlighted they have a disability in the NHS staff survey 2018. The Trust are in the process of promoting to staff the process they should follow to register having a disability on ESR, staff are also informed in a letter after supporting attendance meetings that they can record their disability on ESR or there manager can support them with updating ESR. The Trust is also looking at introducing a Reasonable Adjustment / Disability Passport for staff with a disability.
TB
210_
19b
Wor
kfor
ce D
isab
ility
Equ
ality
Sta
ndar
d R
epor
t
Page 194 of 210

2
The Trust is aiming to set up a Disability staff network group which will look at why 30.48% of Trust staff have not disclosed if they do or don’t have a disability. Metric 2/ Relative likelihood of Disabled staff compared to non-disabled staff being appointed from shortlisting 432 disabled staff were shortlisted and 16 were hired this is a success rate of 3.70% compared to 2515 non-disabled staff shortlisted and 150 who were successful which is a 5.96% success rate. Metric 3/ Relative likelihood of disabled staff compared to non-disabled staff entering the formal capability process For the purposes of Year 1 WDES report, capability is defined as capability on the grounds of performance, not ill health. The figures highlight that no disabled or non-disabled staff entered the formal capability process on the grounds of performance in 2018-19. Metric 4/ Percentage of Disabled staff compared to non-disabled staff experiencing harassment, bullying or abuse from:
i/ Patients/service users, their relatives or other members of the public in the last 12 months Disabled staff = 37.3% Non-disabled 26.7% Difference = 10.6% ii/ Managers Disabled staff = 24.4% Non-disabled 11.5% Difference = 12.9% iii/ Other colleagues Disabled staff = 30.8% Non-disabled 15.9% Difference = 14.9% Metric 5,6,7/ Staff with a disability highlighted in metric 5, 6, 7 of the report a score / response that is worse than staff without a disability, the responses highlight that appropriate actions need to be complied to address the issues raised. Metric 8/ Has your employer made adequate adjustment(s) to enable you to carry out your work?(NHS staff survey) The Trust response rate is 77% other Trusts average is 72%, SOHT is 5% above the national average response.
4. Staff Profile As of March 2019 Southport and Ormskirk Hospital NHS Trust employed 2986 people of which 2.55% disclosed they have a disability. Disability – Non Disabled Staff Information: 2.55% of the Workforce have disclosed that they consider themselves to have a Disability, 66.97% of staff have told us they don’t consider themselves to have a Disability with the remainder 30.48% either not declaring, preferring not to say and the others unspecified
Disability Headcount Percentage %
No 2000
66.97% of staff don’t consider themselves to have
a disability
Not Declared 127
30.48% not disclosed
Prefer Not To Answer 1
Unspecified 782
Yes 76
2.55% of staff consider themselves to have a
disability
Grand Total 2986 100%
5. Workforce Metrics Three workforce Metrics, compares the data for both Disabled and non-disabled staff.
Page 195 of 210

3
Note: Definitions for these categories are based on Electronic Staff Record occupation codes with the exception of medical and dental staff, which are based upon grade codes. Workforce Disability Equality Standard Indicators: For each of workforce indicators, the standard compares the metrics for disabled and non-disabled staff were the figures don’t equate to 100% this is due to the information not stated / not given Workforce Metrics
For the following three workforce Metrics, compare the data for both Disabled and non-disabled staff.
Metric:
Data for reporting year
Non – Clinical
1
Percentage of staff in AfC pay bands or medical and dental subgroups and very senior managers (including Executive Board members) compared with the percentage of staff in the overall workforce. Organisations should undertake this calculation separately for non-clinical and for clinical staff. Cluster 1 (Bands 1 - 4) Cluster 2 (Band 5 - 7) Cluster 3 (Bands 8a - 8b) Cluster 4 (Bands 8c - 9 & VSM Cluster 5 (Medical & Dental Staff, Consultants) Cluster 6 (Medical & Dental Staff, Non-Consultants career grade) Cluster 7 (Medical & Dental Staff, Medical and dental trainee grades) Note: Definitions are based on Electronic Staff Record occupation codes with the exception of Medical and Dental staff, which are based upon grade codes.
2018-19
Cluster Cluster 1 Cluster 2 Cluster 3 Cluster 4
Disabled
4% 4% 0% 0%
Non-Disabled
58% 67% 69% 89%
Clinical
2018-19
Cluster Cluster 1 Cluster 2 Cluster 3 Cluster 4
Disabled
2% 2% 3% 0%
Non-Disabled
70% 71% 64% 86%
Cluster 5: Med & Dental Consultant
2018-19
Disabled
0%
Non-Disabled
58%
Cluster 6: Med & Dental Consultant Non –Consultant
Career Grade
2018-19
Disabled
2%
Non-Disabled
64%
Cluster 7: Medical & Dental Trainee Grades
2018-19 2017-18
Disabled
1%
Non-Disabled
94%
Metric 2:
TB
210_
19b
Wor
kfor
ce D
isab
ility
Equ
ality
Sta
ndar
d R
epor
t
Page 196 of 210

4
2 Relative likelihood of Disabled staff compared to non-disabled staff being appointed from shortlisting across all posts. Note: i) This refers to both external and internal posts. ii) If your organisation implements a guaranteed interview scheme, the data may not be comparable with organisations that do not operate such a scheme. This information will be collected on the WDES online reporting form to ensure comparability between
organisations.
Recruitment: The information below highlights the ratio of Disabled and Non-Disabled staff being appointed from short listing; please note this refers to both internal and external posts 2018-19
Head Count Ratio
WDES Category
Shortlisted Hired Shortlisted Ratio
Disabled 432 16 0.96 0.04
Non-Disabled
2515 150 0.94 0.06
NULL 31 8 0.79 0.21
Not Stated / Not Given
49 1 0.98 0.02
Relative likelihood of Disabled staff compared to non-disabled staff being appointed from shortlisting across all posts: 1.6, A figure below 1:00 indicates that Disabled staff are more likely than Non-Disabled staff to be appointed from shortlisting
Metric 3:
3
Relative likelihood of Disabled staff compared to non-disabled staff entering the formal capability process, as measured by entry into the formal capability procedure. Note: i) This Metric will be based on data from a two-year rolling average of the current year and the previous year. ii) This Metric is voluntary in year one.
Relative likelihood of Disabled staff compared to non-disabled staff entering the formal capability process 2018-19
WDES Category
Head Count
Disabled 0
Non-Disabled 0
Not Stated 1
Total 1
Figure for disabled and none disabled staff is the same 0%
National NHS Staff Survey Metrics For each of the following four Staff Survey Metrics, compare the responses for both Disabled and non-disabled staff
Metric 4:
4 a/ Percentage of Disabled staff compared to non-disabled staff experiencing harassment, bullying or abuse from:
i/ Patients/service users, their relatives or other members of the public in the last 12 months
i/ Patients/service users, their relatives or other members of the public: Disabled Non-Disabled : 37.3 % 26.7%
Page 197 of 210

5
ii/ Managers iii/ Other colleagues b/ Percentage of Disabled staff compared to non-disabled staff saying that the last time they experienced harassment, bullying or abuse at work, they or a colleague reported it.
ii/ Managers: Disabled Non-Disabled 24.4% 11.5%
iii/ Other colleagues: Disabled Non-Disabled 30.8% 15.9 %
b/ % of Disabled staff compared to non-disabled staff saying that the last time they experienced harassment, bullying or abuse at work, they or a colleague reported it. Disabled Non-Disabled 52.8% 46.5%
Metric 5: Q14
5 Percentage of Disabled staff compared to non-disabled staff believing that the Trust provides equal opportunities for career progression or promotion.
Disabled Non-Disabled 78.5% 80.9 %
Metric 6: Q11
6 Percentage of Disabled staff compared to non-disabled staff saying that they have felt pressure from their manager to come to work, despite not feeling well enough to perform their duties
Disabled Non-Disabled 31.8% 19.7%
Metric 7: Q5
7 Percentage of Disabled staff compared to non – disabled staff saying that they are satisfied with the extent to which their organisation values their work
Disabled Non-Disabled 26.9% 37.8%
The following NHS Staff Survey Metric only includes the responses of Disabled staff
Metric 8: Q28b
8 Percentage of Disabled staff saying that their employer has made adequate adjustment(s) to enable them to carry out their work.
Disabled 76.2%
NHS Staff Survey and the engagement of Disabled staff For part a) of the following Metric, compare the staff engagement scores for Disabled, non-disabled staff and the overall Trust’s score For part b) add evidence to the Trust’s WDES Annual Report
Metric 9:
9 a) The staff engagement score for Disabled staff, compared to non-disabled staff and the overall engagement score for the organisation. b) Has your Trust taken action to facilitate the voices of Disabled staff in your organisation to be heard? (Yes) or (No) Note: For your Trust’s response to b) If yes, please provide at least one practical example of current action being taken in the relevant section of your WDES annual report. If no, please include what action is planned to address this gap in your WDES annual report. Examples are listed in the WDES technical guidance.
Disabled Non-Disabled 6.2 6.6 Yes: Staff & Family Friends Test NHS Staff Survey Big Brew / Conversation Setting Up of a Disability Staff Network So Proud Pulse Check
TB
210_
19b
Wor
kfor
ce D
isab
ility
Equ
ality
Sta
ndar
d R
epor
t
Page 198 of 210

6
Board Representation Metric For this Metric, compare the difference for Disabled and non-disabled staff
Metric 10:
10
Percentage difference between the organisation’s Board voting membership and its organisation’s overall workforce, disaggregated:
• Trust board headcount
• Executive and Non-executive
• Workforce
• Please note were figures don’t equate to 100% this is due to staff responses unknown or null response
Non-Disabled Disabled
Trust board members – Headcount:
14 0
of which: Voting Board Members 11 0
:Non-Voting Board Members 3 0
Trust Board Members
of which: Exec Board Members 11 0
:Non Exec Board Members 3 0
Workforce
Overall workforce % by disability 67% 2%
Differences
Total Board –overall workforce 33% -2%
Voting membership –Overall workforce
33% -2%
Executive-Overall Workforce 33% -2%
5. Trust Actions taken to be compliant with the WDES
• WDES Reporting template completed and sent to NHS England
• WDES Report completed and will be uploaded onto the Trust website
• WDES Action plan completed and to be reviewed and updates to be provided at each Valuing Our Peoples Assurance Group and Workforce Committee meeting
6. Recommendations
• WDES paper to be presented to the appropriate Trust Valuing Our Peoples Assurance Group and Workforce Committee meeting
The Valuing Our Peoples Assurance Group and Workforce Committee meeting to:
• Note that the NHS Workforce Disability Equality Standard (WDES) came into effect on the 1st April 2019 and will be completed by the Trust on an annual basis.
• Note that the Trust will put in place WDES action plan and agree that the performance against the plan will be reported through the various Trustwide Valuing Our Peoples Assurance Group and Workforce Committee meeting
• An annual report will be complied for submission to the NHS England Co-ordinator, Commissioner outlining progress on the Workforce Disability Equality Standards.
• Workforce Disability Equality Standard report will be published on the Trust website
• A copy of the WDES Indicators has been sent to NHS England Appendix 1: Workforce Disability Equality Standard (WDES) Action Plan
WDES ACTION PLAN 2019-20 Final.doc
Appendix 2: WDES Technical guidance
Page 199 of 210

7
wdes-technical-guidance-v1.pdf
TB
210_
19b
Wor
kfor
ce D
isab
ility
Equ
ality
Sta
ndar
d R
epor
t
Page 200 of 210


PUBLIC TRUST BOARD 4 November 2019
Agenda Item TB210/19c Report Title
Workforce Race Equality Standard Report
Executive Lead Jane Royds: Director of Human Resources and OD
Lead Officer Bob Davies: Equality Lead
Action Required
(Definitions below)
To Approve To Note
To Assure ✓ To Receive
For Information
Executive Summary
The Committee’s highlight report for August 2019 is set out below:
Alert
• To highlight the Trusts compliance to NHS England to complete the Workforce Race Equality
Standard (WRES) report and action plan, the report highlights the comparisons between BME
and white staff across a number of indicators.
Advise
• Ensure that the Trust data for the WRES has been uploaded onto NHS England site and will
be published on the Trust website and sent to the CCG as part of the equality section of the
quality contract.
• Paper has been reformatted as per action following October’s Board meeting. New formatted
report was accepted at Workforce Committee in November 2019.
Assure
• The WRES action plan will be monitored and updated. Updates will be provided to the various
Trust groups / committees and the report and updates are also a requirement of the equality
section of the quality contract with the CCG’s.
Recommendation
The Workforce Committee is asked to receive the report
Strategic Objective Principal Risk
✓ SO1 Improve clinical outcomes and patient safety to ensure we deliver high quality services
If quality is not maintained in line with regulatory standards this will impede clinical outcomes and patient safety.
SO2 Deliver services that meet NHS constitutional and regulatory standards
If the Trust cannot achieve its key performance targets it may lead to loss of services.
SO3 Efficiently and productively provide care within agreed financial limits
If the Trust cannot meet its financial regulatory standards and operate within agreed financial
TB
210_
19c
FS
Wor
kfor
ce R
ace
Equ
ality
Sta
ndar
d In
form
atio
n R
epor
t Apr
il 19
- M
ar 2
0
Page 201 of 210

resources the sustainability of services will be in question.
✓ SO4 Develop a flexible, responsive workforce of the right size and with the right skills who feel valued and motivated
If the Trust does not attract, develop, and retain a resilient and adaptable workforce with the right capabilities and capacity there will be an impact on clinical outcomes and patient experience.
✓ SO5 Enable all staff to be patient-centred leaders building on an open and honest culture and the delivery of the Trust values
If the Trust does not have leadership at all levels patient and staff satisfaction will be impacted
SO6 Engage strategic partners to maximise the opportunities to design and deliver sustainable services for the population of Southport, Formby and West Lancashire
If the system does not have an agreed acute services strategy it may lead to non-alignment of partner organisations plans resulting in the inability to develop and deliver sustainable services
Linked to Regulation & Governance (the report supports …..)
CQC KLOEs
GOVERNANCE
✓ Caring ✓ Statutory Requirement
✓ Effective Annual Business Plan Priority
✓ Responsive ✓ Best Practice
✓ Safe Service Change
✓ Well Led
Impact (is there an impact arising from the report on any of the following?)
Compliance ✓ Legal
✓ Engagement and Communication Quality & Safety
✓ Equality Risk
Finance ✓ Workforce
Equality Impact Assessment
If there is an impact on E&D, an Equality Impact Assessment must accompany the report)
Policy
Service Change
Strategy
Next Steps (List the required Actions and Leads following agreement by Committee)
The Trust has compiled a WDES report and action plan that will be monitored at various Trust committees and groups i.e. Workforce Committee Valuing Our People Group, reporting is also a requirement in the CCG equality section of the quality contract, the Trust will set up a disability staff network to obtain the views of staff with a disability or long-term medical condition, the WDES action plan highlights areas for development i.e. Reporting a disability on ESR, Recruitment, Staff Bandings, Bullying and Harassment
Previously Presented at:
Audit Committee Quality & Safety Committee
Charitable Funds Committee Remuneration & Nominations Committee
Finance, Performance & Investment
Committee Workforce Committee
Page 202 of 210

1
Southport and Ormskirk Hospital NHS Trust Workforce Race Equality Standard Information Report April 2018 – March 2019 1. Executive Summary This paper provides a general overview of the Workforce Race Equality Standard (WRES) and the Trust’s metrics against the nine indicators within the Workforce Race Equality Standard (WRES). It also provides analysis of the metrics and outlines actions (Appendix 1 WRES Action Plan) to address the gaps between the experience of BME and White staff. 2. Introduction The NHS Equality and Diversity Council agreed in July 2014 that action across the NHS needs to be taken to ensure employees from black and ethnic minority (BME) backgrounds have equal access to career opportunities and receive fair treatment in the workplace. The move follows recent reports which have highlighted disparities in the number of BME people in senior leadership positions across the NHS, as well as lower levels of wellbeing amongst the BME population. Following a period of consultation, the NHS Equality and Diversity Council agreed two measures that compliment each other whilst being distinct to improve equality across the NHS and these would be mandatory requirements embedded within the NHS Contract from April 2015. 1. The Workforce Race Equality Standard (WRES) 2. NHS Equality Delivery System 2 (EDS2) There are nine metrics. Four of the metrics are specifically on workforce data and four of the metrics are based on data derived from the national NHS Staff Survey indicators. The latter will highlight any differences between the experience and treatment of White staff and BME staff in the NHS, with a view to closing the gaps highlighted by those metrics. The final metric requires provider organisations to ensure that their Boards are broadly representative of the communities they serve. The CQC will take this into account within the ‘Well Led’ domain. 3. Drivers for WRES implementation The research Snowy White Peaks by Roger Kline (2013) showed:
• Unfair treatment of BME staff adversely affects the care and treatment of patients
• Talent is being wasted through unfairness in the appointment, treatment and development of a large section of the NHS workforce
• Precious staff resources are being wasted through the impact of such treatment on morale and discretionary effort
• Diverse teams and leaderships are more likely to show the innovation and increased organisational effectiveness the NHS needs.
• Organisations whose leadership composition bears little relationship to the communities they serve will be less likely to deliver the patient focussed care that is needed
• Nationally there has been a decrease in the proportion of BME Board members, Senior Managers and Nurse Managers in recent years; there are less BME Leaders and Managers in 2013 than in 2003 (Kline 2015).
• Statistically White staff are 1.74 times more likely to be appointed once shortlisted than BME staff (Kline, 2013);
• BME staff are twice as likely to enter formal disciplinary processes and be disciplined for similar offences than white staff (Archibong et al, 2010);
• Black nurses take 50% longer to be promoted and are less likely to access national training programmes (NHSLA);
• BME staff experiences correlate to the staff survey results on bullying, career progression, promotion and discrimination.
• 2014 Francis found BME Whistle-blowers are treated less favourably than white whistle-
TB
210_
19c
Wor
kfor
ce R
ace
Equ
ality
Sta
ndar
d R
epor
t
Page 203 of 210

2
blowers. 4. Staff Profile As of March 2019 Southport and Ormskirk Hospital NHS Trust employed 2986 people of which Workforce
Ethnicity: The Trust workforce consists of 10.95% from Black Minority and Ethnic groups 82.65% White staff and 6.40% not stated unspecified prefer not to answer. 5. WRES Highlights: The information below provides a comparison for the WRES reports for 2017-18 and 2018-19, the information also provides the Trust figures compared to the average for combined acute and community hospital. BME staff in clinical and non–clinical bands 8a-9 Non Clinical: The 2018-19 WRES report highlights that there has been no increase in non-clinical BME staff in bands 8b to 9 and there are no BME staff in band 8b 8c 9 these figures are the same in the 2017-18 WRES report. Clinical: The WRES report highlights that there has been no increase in clinical BME staff in bands 8b – 8d and there are no BME staff in band 8b, 8c. 8d these figures are the same in the 2017-18 WRES report. Relative likelihood of BME and white staff being appointed from shortlisting across all posts 3.70% of BME staff were hired from those shortlisted compared to 5.96% of white applicants hired from shortlisting in 2018-19. The 2018-19 WRES data highlights that there has been an increase in BME staff being successful at interview and being hired by the Trust. 2018-19 = 3.70% compared to 1.78% in 2017-18 this is an increase of 1.78% Relative likelihood of BME and white staff entering the formal disciplinary process The number of BME staff (1) entering the disciplinary process in 2018-19 is the same as the 2017 -18 WRES figures, the figure for white staff has decreased to 23 in 2018-19 compared to 38 in 2017-18. NHS staff survey responses that are specific to WRES questions: Q1/ The percentage of staff experiencing harassment, bullying or abuse from patients, relatives or the public in last 12 months. In the last 12 months Trust figures for white staff has seen a decrease of 0.1% and a 9.2% increase for BME staff. The Trust figures compared to the average combined acute and community Trusts is 0.2% higher for white staff and 0.4% lower for BME staff. Q2/ Percentage of staff experiencing harassment, bullying or abuse from staff in last 12 months. Experiences of Trust staff experiencing harassment; bullying or abuse from staff in last 12 months has seen a 1.8% increase for white staff and a decrease of 6.5% for BME staff. The Trust figures compared to the average combined acute and community Trusts is 0.7% lower for white staff and 2.1%% lower for BME staff. Q3/ Percentage of Trust staff believing that Trust provides equal opportunities for career progression or promotion. Experiences of white staff have seen an increase of 1.2% and an increase of 5.4% for BME staff. The Trust figures compared to the average combined acute and community Trusts is 6% lower for white staff and 8.2% higher for BME staff.
Page 204 of 210

3
Q4/ In the last 12 months have you personally experienced discrimination at work from any of the following manager/team leader or other colleagues? Experience of white staff has seen a 0.3% increase from 2017 and there has been an increase of 3.5% from 2017 for BME staff The Trust figures compared to the average combined acute and community Trusts is 0.4% higher for white staff and 1% lower for BME staff. 6. Workforce Race Equality Standard Indicators: 6.1 Workforce: For each of these four workforce indicators, the standard compares the metrics for White and BME staff were the figures don’t equate to 100% this is due to the information not stated / not given.
Indicator Data for reporting year
2018-19 2017-18
1
Percentage of staff in each of the AfC Bands 1-9 or Medical and Dental subgroups and VSM (including executive Board members) compared with the percentage of staff in the overall workforce disaggregated by: • • Non-Clinical staff • • Clinical staff - of which • - Non-Medical staff • - Medical and Dental staff Note: Definitions are based on Electronic Staff Record occupation codes with the exception of Medical and Dental staff, which are based upon grade codes.
Non - Clinical
Band Band 1 Band 2 Band 3 Band 4 Band 5 Band 6 Band 7 Band 8a Band 8b Band 8c Band 8d Band 9 2017-18 VSM CQIR IRPM WCOO
BME 7.17% 1.29% 4.0% 0.61% 1.96% 1.96% 3.45% 4.76% 0.00% 0.00%
14.29% 0.00%
16.67% 0.00% 0.00% 0.00%
White 84.75% 93.89% 86.40% 95.09% 90.20% 94.12% 86.21% 90.48% 100% 100%
85.71% 100%
83.33% 100% 100% 100%
BME 7.0% 1.3% 4.3% 0.6% 1.9% 2.2% 3.3% 5.0% 0% 0%
14.3% 0%
33.3% 0% 0% 0%
White 84.7% 93.7% 84.5% 95.8% 90.4% 93.5% 90.0% 95.0% 100% 100% 66.7% 100%
66.7% 100% 100% 100%
Clinical
2018-19 2017-18
Band Band 2 Band 3 Band 4 Band 5 Band 6 Band 7 Band 8a Band 8b Band 8c Band 8d VSM FMWC MT02 WHO3 WHO7
BME 9.68% 2.97% 0.00% 7.10% 5.32% 1.35% 8.62% 0.00% 0.00% 0.00%
0.00% 0.00% 80% 0.00% 16.67%
White 80.24% 91.82% 96.08% 87.33% 90.05% 91.89% 86.21% 91.30% 100% 100%
100% 100% 0.00% 100%
66.67%
BME 9%
3.2% 0%
7.5% 4.8% 2.0% 8.9% 0.00% 0.00% 0.00%
0.00% 0.00%
N/A 0.00%
16.67%
White 80.2% 92.2% 98.1% 87.2% 90.6% 91.2% 85.7% 90.5% 100% 100%
100% 100% N/A
100% 66.67%
Med & Dental Consultant
2018-19 2017-18
TB
210_
19c
Wor
kfor
ce R
ace
Equ
ality
Sta
ndar
d R
epor
t
Page 205 of 210

4
BME 42.06%
White 42.99%
BME 45.9%
White 40.5%
Med & Dental Consultant Non –Consultant Career Grade
2018-19 2017-18
BME 56.38%
White 28.72%
BME 54.2%
White 30.1%
Medical & Dental Trainee Grades
2018-19 2017-18
BME 23.91%
White 66.30%
BME 24.7%
White 65.6%
Board- Ex- Non Exec
BME 18.18%
White 84.62%
BME 33.3%
White 66.67%
2
Relative likelihood of staff being appointed from shortlisting across all posts Note: This refers to both external and internal posts
Recruitment: The information below highlights the ratio of BME and White Staff being appointed from short listing; please note this refers to both internal and external posts 2018-19 & 2017-18 2018-19
Head Count Ratio
WRES Category
Shortlisted Hired Shortlisted Ratio
BME 432 16 0.96 0.04
White 2515 150 0.94 0.06
NULL 31 8 0.79 0.21
Not Stated / Not Given
49 1 0.98 0.02
2017-18
Head Count Ratio
WRES Category
Shortlisted Hired Shortlisted Ratio
BME 393 7 0.98 0.02
White 2289 98 0.96 0.04
NULL 10 2 0.83 0.17
Not Stated / Not Given
47 1.00
3 Relative likelihood of staff entering the formal disciplinary process, as measured by entry into a formal disciplinary investigation Note: This indicator will be based on data from a two year rolling average of the current year and the previous year. For consistency, organisations should use the same methodology as they have always used.
Disciplinary Process: Overall breakdown of cases by ethnic origin categorised in line with WRES requirements as at 31.3.2019 2018-19
WRES Category
Head Count
BME 1
White 23
Not Stated 1
Total 25
2017-18
WRES Category
Head Count
BME 1
White 38
Not Stated 4
Page 206 of 210

5
Total 43
4 Relative likelihood of staff accessing non-mandatory training and CPD
Training: The information below highlights the ratio of BME and White staff accessing training in 2018-19 and 2017-18 2018-19
WRES Category
Head Count Enrolment Headcount
Ratio
BME 244 226 0.93
White 2551 2219 0.87
NULL 12 8 0.67
Not Stated / Not Given
178 160 0.89
2017-18
WRES Category
Head Count Enrolment Headcount
Ratio
BME 242 223 0.92
White 2603 2447 0.94
NULL 12 10 0.83
Not Stated / Not Given
206 191 0.93
6.2 NHS Staff Survey: The 2018 NHS Staff Survey was completed by 1,147 staff this is a response rate of 40% which is average for combined acute and community trusts in England (43%) and compares with a response rate in the Trust in 2017 of (45%) , For each of these four staff survey indicators, the Standard compares the metrics for each survey question response for White and BME staff. Key Findings KF25, KF26, and KF21, split between White and Black and Minority Ethnic (BME) staff, as required for the Workforce Race Equality Standard. Note that for question Q17, the percentage featured is that of “Yes” responses to the question. Key Finding and question numbers are the same in 2018 as 2017. Figures in bold highlight BME figures
Indicator Data for reporting year 2018
Data for previous year 2017
5 15a: Percentage of staff experiencing harassment, bullying or abuse from patients, relatives or the public in last 12 months Experiences of staff experiencing harassment, bullying or abuse from patients, relatives or the public in last 12 months has seen the figures for white staff decrease by 0.1% and a 9.2% increase for BME staff.
White staff 28.4 % BME staff : 29.4% Average (median) for combined Acute and Community Trusts White staff– 28.2% BME staff- 29.8%
White staff: 28.5% BME staff: 20.2%
6 Percentage of staff experiencing harassment, bullying or abuse from staff in last 12 months Experiences of experiencing harassment, bullying or abuse from staff in last 12 months has seen a 1.8% increase for white staff and a decrease of 6.5% for BME staff.
White staff: 25.7% BME staff: 26.5% Average (median) for combined Acute and Community Trusts White staff– 26.4% BME staff- 28.6%
White staff: 23.9% BME staff: 33%
TB
210_
19c
Wor
kfor
ce R
ace
Equ
ality
Sta
ndar
d R
epor
t
Page 207 of 210

6
7 Percentage believing that trust provides equal opportunities for career progression or promotion Experience of white staff has seen an increase of 1.2% for white staff and an increase of 5.4% for BME staff.
White staff: 80.5% BME staff: 80.4% Average (median) for combined Acute and Community Trusts White staff: 86.5% BME staff: 72.3%
White staff:79.3% BME staff: 75%
8 In the last 12 months have you personally experienced discrimination at work from any of the following? b) Manager/team leader or other colleagues Experience of white staff has seen a 0.3% increase from 2017 and there has been a increase of 3.5% from 2017 for BME staff.
White staff: 7% BME staff: 13.6% Average (median) for combined MH/LD and Community Trusts White staff: 6.6% BME staff: 14.6%
White staff: 6.7% BME staff: 10.1%
6.3 Board Representation Indicator: For this indicator, compare the difference for white and BME staff
Indicator Data for reporting year
9 Percentage difference between the organisations’ Board membership and its overall workforce disaggregated:
• By voting membership
of the Board
• By executive
membership of the Board Note: This is an amended version of the previous definition of Indicator 9
The information below provides information on the headcount and percentage difference between the organisations board membership and its overall workforce for BME and White Staff By executive and non-executive board membership = BME: 14.29% White:78.57% Not Stated: 7.14% 2018-19
WRES Category
Head Count
Head count %
Board Head Count
Board Headcount %
BME 258 8.18% 2 14.29%
White 2679 84.97% 11 78.57%
Null 23 0.73% 0 0.00
Not Stated /Not Given
193 6.12% 1 7.14%
2017-18
WRES Category
Head Count
Head count %
Board Head Count
Board Headcount %
BME 242 7.9% 3 30%
White 2603 85.01% 6 60%
Null 12 0.39% 0 0.00
Not Stated /Not Given
206 6.7% 1 10%
7. Trust Actions taken to be compliant with the WRES
Page 208 of 210

7
• WRES Reporting template completed and sent to NHS England
• WRES Report completed and will be uploaded onto the Trust website
• WRES Action plan completed and to be reviewed and updates to be provided at each Valuing Our Peoples Assurance Group and Workforce Committee meeting
8. Recommendations
• WRES paper to be presented to the appropriate Trust Valuing Our Peoples Assurance Group and Workforce Committee meeting
The Valuing Our Peoples Assurance Group and Workforce Committee meeting to:
• Note that the NHS Workforce Race Equality Standard came into effect on the 1st April 2015 and is completed by the Trust on a annual basis.
• Note that the Trust has put in place WRES action plan and agree that the performance against the plan will be reported through the various Trustwide Valuing Our Peoples Assurance Group and Workforce Committee meeting
• An annual report will be compiled for submission to the NHS England Co-ordinator, Commissioner outlining progress on the Workforce Race Equality Standards.
• Workforce Race Equality Standard report will be published on the Trust website
• A copy of the WRES Indicators has been sent to NHS England Appendix 1: Workforce Race Equality Standard (WRES) Action Plan
WRES ACTION PLAN 2019-20 Final.doc
Appendix 2:
wres-technical-guidance-2017 (1).pdf
Appendix 3:
wres-nhs-board-bulletin.pdf
TB
210_
19c
Wor
kfor
ce R
ace
Equ
ality
Sta
ndar
d R
epor
t
Page 209 of 210

8
Page 210 of 210