age-related changes in left ventricular twist assessed by two-dimensional speckle-tracking imaging
TRANSCRIPT

ORIGINAL ARTICLES
Age-related Changes in Left Ventricular TwistAssessed by Two-dimensional
Speckle-tracking ImagingMasaaki Takeuchi, MD, Hiromi Nakai, RDCS, Michiko Kokumai, MS,
Tomoko Nishikage, RDCS, Shinichiro Otani, MD, and Roberto M. Lang, MD,
Osaka, Japan, and Chicago, IllinoisThe aim of this study was to determine the normalvalue of left ventricular (LV) twist, and to examinethe effects of aging on LV twist by newly developed2-dimensional ultrasound speckle-tracking imag-ing. We acquired basal and apical LV short-axissecond harmonic images in 118 healthy volun-teers. Using commercially available 2-dimensionalstrain software, time-domain speckle tracking wasperformed, and mean value of LV rotation ob-tained at each plane. LV twist was defined as apicalrotation relative to the base. Adequate data wereobtained in 113 volunteers. During systole, the LVperforms a wringing motion with a counterclock-
doi:10.1016/j.echo.2006.04.011
at the base. The mean value of peak twist was 7.7 �3.5 degrees. Immediately after end systole, rapiduntwisting develops. Different LV twist profiles arenoted according to age. Peak LV twist was signifi-cantly higher, and the rate of LV untwisting signifi-cantly reduced and delayed, with advancing age. LVtwist can be measured noninvasively by 2-dimen-sional ultrasound speckle-tracking imaging. The ob-served reduced and delayed diastolic untwistingwith aging may contribute toward the tendency ofdiastolic dysfunction. This novel method allows thedetailed study of diastolic function in various cardio-vascular diseases. (J Am Soc Echocardiogr 2006;19:
wise rotation at the apex and a clockwise rotation 1077-1084.)
Torsional deformation of the left ventricle (LV) isthe wringing motion, or twist, of the heart impartedby contraction of its obliquely spiraling fibers.1,2
Torsional recoil, or untwisting, is known to predom-inantly occur during isovolumic relaxation.3 Thistorsional recoil, which is associated with the releaseof restoring forces that have accumulated duringsystole, is thought to contribute to diastolic suction,and may represent a sensitive parameter of myocar-dial relaxation.3,4 To date, the evaluation of LVtorsion, rotation, or both has been limited to inva-sive studies using radiopaque markers,5,6 or crude2-dimensional (2D) echocardiographic studies usingpapillary muscle as landmarks7,8 and Doppler tissueimaging.9 Recently, tagged magnetic resonance im-aging (MRI) has shown great promise to assesstorsional deformation,1,3,4 but this equipment is notwidely available, thus, precluding its use in routineclinical practice.
From the Department of Cardiology and Internal Medicine, TaneGeneral Hospital, Osaka, Japan; and Noninvasive Cardiac ImagingLaboratory, Section of Cardiology, Department of Medicine, Uni-versity of Chicago Medical Center (R.M.L.).Reprint requests: Masaaki Takeuchi, MD, Department of Cardiologyand Internal Medicine, Tane General Hospital, 1-2-31 Sakaigawa,Nishi-ku, Osaka, 550-0024 Japan (E-mail: [email protected]).0894-7317/$32.00Copyright 2006 by the American Society of Echocardiography.
The recent development of 2D ultrasound speck-le-tracking imaging has allowed LV twist to beevaluated noninvasively in a variety of patient pop-ulations.10-15 Advancing age is associated with alter-ations in LV diastolic function. The mechanismsunderlying these age-related changes are not fullyunderstood, but probably are caused, in part, bydecreased Calcium uptake by the sarcoplasmic retic-ulum, resulting in prolonged myocardial relax-ation.16 The age-related changes in LV twist have notbeen previously evaluated using 2D speckle-trackingimaging. Accordingly, the aim of this study was2-fold: (1) to establish normal value of LV twist in alarge group of healthy volunteers; and (2) to exam-ine the effect of aging on LV twist.
METHODS
Study Participants
In this study, 158 healthy asymptomatic volunteers wererecruited. All study volunteers provided informed consentbefore undergoing a clinical examination to exclude car-diac disease. Exclusion criteria included a history ofhypertension, diabetes, ischemic or valvular heart disease,use of cardiac medication, or a combination of these. Inaddition, a transthoracic echocardiogram was performedto exclude LV hypertrophy, valvular heart disease, and
global or regional wall-motion abnormalities. Forty volun-1077

l short
Journal of the American Society of Echocardiography1078 Takeuchi et al September 2006
teers met at least one exclusion criteria, and were ex-cluded. Thus, the final study group consisted of 118volunteers.
Echocardiography
After completion of the standard echocardiogram, two LVshort-axis planes obtained at the base and the apical levelswere acquired using second harmonic gray scale imagingusing a commercially available ultrasound transducer(M3S probe, Vivid 7, GE Healthcare, Milwaukee, Wis).Care was taken to ensure that the basal short-axis planescontained the mitral valve, and that the apical plane wasacquired distally to the papillary muscles. In each short-axis acquisition, the LV cross section was made as circularas possible. At each plane, 3 consecutive cardiac cycleswere acquired during a breath hold, and digitally stored ina hard disk for offline analysis.
LV Rotation and Rotational Velocity
The time interval between the peak of the R wave on theelectrocardiogram and the aortic valve opening and clo-sure, and time from the R wave to the mitral valve openingand closure, was measured using pulse wave Doppler
Figure 1 Measurement process of left ventricuimaging. A to F, Measuring LV rotation in apica
from the LV outflow and inflow, respectively. From the
basal and apical short-axis data sets, one cardiac cycle wasselected for subsequent analysis. Using commercially avail-able 2D strain software (Echopac PC, version 4.03, GEHealthcare), the endocardial border of each short axis inthe end-systolic frame was manually traced (Figure 1, A).A region of interest (in which the computer software thenautomatically performed speckle tracking) was thendrawn to include the entire myocardium (Figure 1, B). Thesoftware algorithm then automatically segmented the LVshort axis into 6 equidistant segments and selected suit-able speckles for tracking (Figure 1, C ). Once completed,the software algorithm searched these speckles on aframe-by-frame basis using the sum of absolute differencealgorithm. Subsequently, the speckle-tracking algorithmprovided a tracking score, representing the reliability oftracking based on the degree of decorrelation of theblock-matching algorithm. The individual regional track-ing scores were scored with values of 1 (excellent), 2(acceptable), and 3 (poor)13 (Figure 1, D). Segments witha score of 2.5 or greater were excluded from the analysis.Finally, software defined the ventricular centroid for themidmyocardial line on each frame (Figure 1, E), andcalculated the time domain LV rotation and LV rota-
V) rotation by 2-dimensional speckle-tracking-axis view.
lar (L
tional velocity profiles for each segment in both short-

Journal of the American Society of EchocardiographyVolume 19 Number 9 Takeuchi et al 1079
axis planes (Figure 1, F ). The LV rotation profile wasthen smoothed with cubic spline interpolation, fromwhich LV rotational velocity was calculated by differ-entiation. Averaged LV rotation and rotational velocityprofile from 6 segments were used for the calculation ofLV twist and twist velocity. As in previous studies,4,9,13
LV twist and twist velocity were defined as apical LVrotation and rotational velocity relative to the base. Ineach study, we verified that heart rates for the cardiaccycles in which the timing of aortic and mitral valveopening and closure was assessed were the same as thecardiac cycles stored for offline analysis of basal and apicalrotation.
Counterclockwise rotation as viewed from the LV apexwas expressed as a positive value, whereas a clockwiserotation as a negative value. Data points depicting thebasal and apical LV rotation and rotational velocities wereexported to a spreadsheet program (Excel, MicrosoftCorp, Seattle, Wash) to calculate LV twist and twistvelocity. To adjust for intersubject differences in heartrate, the time sequence were normalized to the percent-age of systolic duration (ie, at end systole, t was 100%).End systole was defined as the point of aortic valveclosure. In addition to the twist versus time profiles, peaktwist, peak positive twist velocity, peak negative twistvelocity, and time from the R wave to peak positive(negative) velocity were measured. The degree of untwist-ing, the directional reversal of systolic counterclockwisetwist during diastole, was expressed as percentage ofmaximum systolic twist: untwisting � (Twistmax �Twistt/Twistmax) � 100, where Twistt is twist at time tand Twistmax is maximal systolic twist. Because isovolu-mic relaxation time interval varied from volunteer to volun-teer, the untwisting rate was defined as ([Twistmax �TwistMVO/Twistmax] � 100)/IVRT, where TwistMVO istorsion at mitral valve opening and IVRT is the time ofisovolumic relaxation.
Using pulse wave Doppler velocity data of the LVinflow and outflow tract, peak mitral flow velocity of theearly rapid filling (E) wave velocity, peak velocity of thelate filling wave due to atrial contraction (A) wave veloc-ity, deceleration time of the E wave, E/A ratio, isovolumiccontraction time, and isovolumic relaxation time werecalculated.
Statistical Analysis
Data were expressed as mean � SD. Data were analyzedusing analysis of variance to compare the degree ofrotation, twist, and its related variables applying a Bofer-roni correction among 3 groups. When comparing theregional tracking score, the Student t test was used. AP value less than .05 was considered significant.
Interobserver measurement variability was determinedby having a second observer measure LV twist and twistvelocity in 7 randomly selected volunteers. Intraobservervariability was determined by having one observer remea-sure LV twist and twist velocity in 7 volunteers 1 month
apart. Interobserver and intraobserver variabilities werecalculated as correlation coefficients and as the mean andSD of the differences between the two measurements.
RESULTS
Feasibility
Five volunteers who had tracking scores of 2.5 ormore in all 6 segments in the basal short-axis planewere excluded from the study. Thus, the final groupconsisted of 113 volunteers. The average trackingscore for all 6 apical segments was 1.50 � 0.47,which was significantly lower than the averageobtained in the basal plane (1.93 � 0.41, P � .001).The frequency of segments with a score of 2.5 ormore in the basal short-axis planes was 6/113 in theanteroseptal, 31/113 in anterior, 63/113 in lateral,55/113 in posterior, 25/113 in inferior wall, and5/113 in interventricular septum, respectively. Thecorresponding values for the apical short-axis planewas 3/113 in the anteroseptal, 14/113 in anterior,29/113 in lateral, 20/113 in posterior, 11/113 ininferior wall, and 4/113 in interventricular septum,respectively.
Twist and Twist Velocity
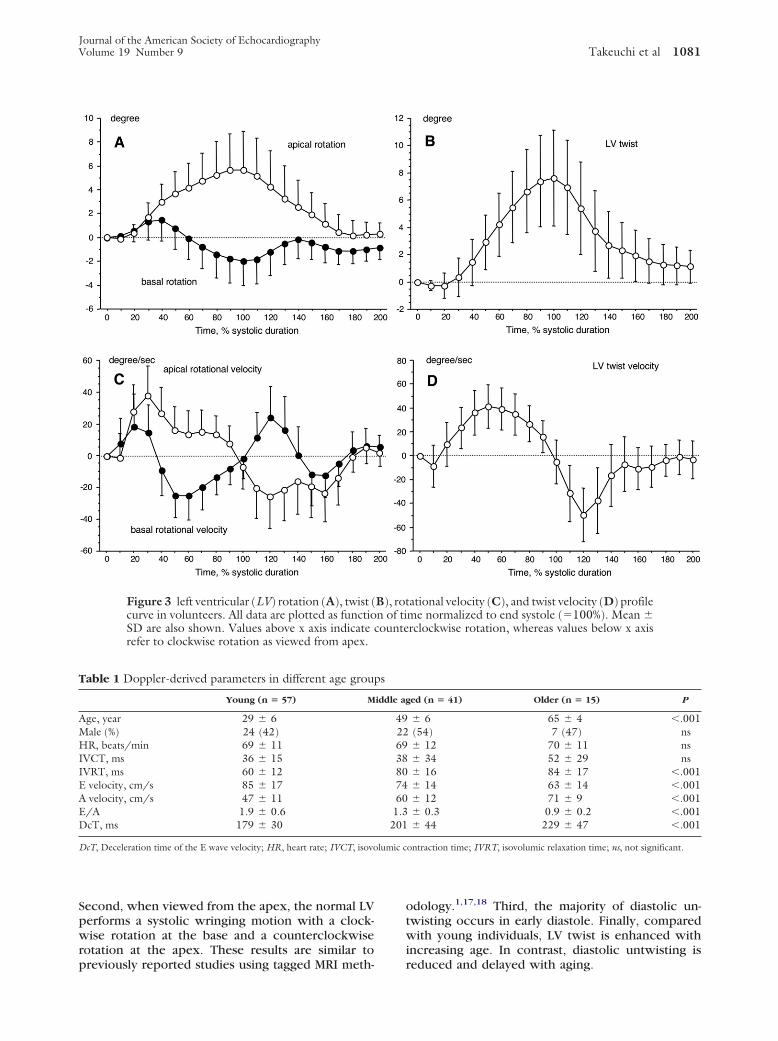
The average frame rate was 75 � 5 frames/s (range:65-86 frames/s). A representative LV rotation androtational velocity versus time profiles obtained inthe base and apical planes is shown in Figure 2. Asseen from the apex, the normal LV performs asystolic wringing motion with an initial minimalcounterclockwise rotation followed by a clockwiserotation at the base and counterclockwise rotationin the LV apex (Figure 3, A) . The systolic rotationattains peak motion at the end of systole in both thebasal and apical planes (maximal apical rotation 5.65 �3.21 degrees; maximal basal rotation �1.97 � 2.08degrees). Thus, peak twist develops near the end ofsystole (7.74 � 3.51 degrees, 97 � 11% of endsystole) (Figure 3, B). During early diastole, a rapiduntwisting motion is observed that is directed op-posite to the systolic rotation. The apical rotationalvelocity shows a systolic counterclockwise rotationfollowed by a diastolic clockwise rotation. The basalrotational velocity has a more complicated profile,including an initial counterclockwise followed by alater clockwise rotation during systole. During diastole,a counterclockwise motion followed by a clockwiserotation was noted (Figure 3, C ). Twist velocity,defined as apical rotational velocities relative to thebase had a net systolic positive velocity (47.7 � 18.5degrees/s) and a diastolic negative velocity (�59.4 �23.4 degrees/s) (Figure 3, D). The time to peakpositive twist velocity was measured in midsystole(52 � 12% of end systole), whereas time to peak
negative twist velocity was measured to occur at
Journal of the American Society of Echocardiography1080 Takeuchi et al September 2006
early diastole (122 � 9% of end systole). No sexdifference was noted in peak twist, untwisting, ortwist velocity.
Effect of Aging on Twist Behavior
To examine the effect of aging on twisting, thehealthy volunteers were divided into 3 groups ac-cording to age (young, �40 years; middle aged,40-60 years; older �60 years). The pulse waveDoppler-derived parameters are shown in Table 1.With aging, the isovolumic relaxation time, deceler-ation time, and peak A wave velocity lengthened andincreased significantly, whereas the peak E wavevelocity and E/A ratio decreased significantly. Theeffect of age on twist and twist velocity is shown inTable 2 and Figure 4. Peak LV twist was significantlygreater in the older group (10.8 � 4.9 degrees)compared with the young (6.7 � 2.9 degrees, P �.001) and middle-aged (8.0 � 3.0 degrees, P � .006)groups. The degree of untwisting during early dias-tole was significantly reduced and delayed in theolder group. Untwisting rates were significantlylower in the middle-aged (0.40 � 0.22%/ms, P �.001) and older (0.41 � 0.19%/ms, P � .03) groupscompared with the young group (0.64 � 0.42%/ms).Although no difference in the peak positive and
Figure 2 Apical and basal left ventricular (LV) roApical (top) and basal (bottom) views. From left toat end systole, rotation, and rotational velocity cucounterclockwise (blue) and clockwise (red) rotadifferent curves from 6 segments (yellow, anterosinferior; and turquoise, septal wall).
peak negative twist velocity were noted among the
3 groups, time to peak negative twist velocity cor-rected by end-systolic time was significantly delayedin the middle-aged group (P � .001).
Measurement Variability
The interobserver variability was r � 0.99 for twist(4.13 � 3.51 vs 4.45 � 3.99 degrees) and r � 0.98for twist velocity (1.1 � 33.7 vs 0.9 � 37.8 degrees/s).The limits of agreement analysis revealed that thebias was �0.32 � 0.81 degrees for twist and 0.16 �8.39 degrees/s for twist velocity. Intraobsever vari-ability showed r � 0.98 for twist (4.13 � 3.51 vs4.15 � 3.55 degrees) and r � 0.98 for twist velocity(1.1 � 33.7 vs 0.9 � 33.8 degrees/s). The limits ofagreement analysis showed that the bias was �0.02 �0.77 degrees for twist and 0.18 � 7.52 degrees/s fortwist velocity.
DISCUSSION
The major findings in this study were as follows.First, 2D speckle tracking is feasible in parasternalshort-axis planes, resulting in reliable LV twist andtwist velocity measurements in the majority of indi-
and LV rotational velocity in representative case.2-dimensional (2D) color-coded rotation imagering one cardiac cycle. In 2D color-coded view,otation and rotational velocity curve contains 6
red, anterior; green, lateral; pink, posterior; blue,
tationright,rve du
tion. Reptal;
viduals. This methodology is highly reproducible.
lumic c
Journal of the American Society of EchocardiographyVolume 19 Number 9 Takeuchi et al 1081
Second, when viewed from the apex, the normal LVperforms a systolic wringing motion with a clock-wise rotation at the base and a counterclockwiserotation at the apex. These results are similar to
Figure 3 left ventricular (LV) rotation (A), twist (curve in volunteers. All data are plotted as functioSD are also shown. Values above x axis indicaterefer to clockwise rotation as viewed from apex.
Table 1 Doppler-derived parameters in different age grou
Young (n � 57) M
Age, year 29 � 6Male (%) 24 (42)HR, beats/min 69 � 11IVCT, ms 36 � 15IVRT, ms 60 � 12E velocity, cm/s 85 � 17A velocity, cm/s 47 � 11E/A 1.9 � 0.6DcT, ms 179 � 30
DcT, Deceleration time of the E wave velocity; HR, heart rate; IVCT, isovo
previously reported studies using tagged MRI meth-
odology.1,17,18 Third, the majority of diastolic un-twisting occurs in early diastole. Finally, comparedwith young individuals, LV twist is enhanced withincreasing age. In contrast, diastolic untwisting is
ational velocity (C), and twist velocity (D) profileme normalized to end systole (�100%). Mean �rclockwise rotation, whereas values below x axis
ed (n � 41) Older (n � 15) P
� 6 65 � 4 �.001(54) 7 (47) ns� 12 70 � 11 ns� 34 52 � 29 ns� 16 84 � 17 �.001� 14 63 � 14 �.001� 12 71 � 9 �.001� 0.3 0.9 � 0.2 �.001� 44 229 � 47 �.001
ontraction time; IVRT, isovolumic relaxation time; ns, not significant.
B), rotn of ticounte
ps
iddle ag
492269388074601.3201
reduced and delayed with aging.

systole (
Journal of the American Society of Echocardiography1082 Takeuchi et al September 2006
Systolic Twist
Systolic twist, defined as the wringing motion of theheart as the apex rotates with respect to the basearound the LV long axis, minimizes the transmuralgradients of fiber strain and oxygen demand.19,20
The orientation of the myofibers varies across the LVwall: subepicardial fibers follow the path of a left-handed helix around the cavity, fibers in the midwallare circumferentially oriented, whereas subendocar-dial fibers follow a right-handed helical path. In thenormal LV, because of the specific helical myofiberpattern, LV twisting generated by the subepicardialfibers is partly counteracted by the subendocardialmyofibers. Transmural differences in shortening arecompensated for by this LV twisting, which reducessubendocardial fiber shortening and amplifies sub-epicardial fiber shortening. Decreased systolic twist,which should result in increased gradients of fiberstrain and oxygen consumption, has been reportedin dilated cardiomyopathy21 and myocardial infarc-tion,18,20 possibly contributing to myocardial dys-function.
Although LV diastolic function is altered, LV sys-tolic function is usually preserved with aging. Inter-estingly, in our study, compared with young volun-teers, increased systolic twist was noted in oldervolunteers, an observation that is in agreement witha previous tagged MRI study.16 Increased systolictwist has also been described in patients with LVhypertrophy secondary to aortic stenosis17,22,23 andin patients with hypertrophic cardiomyopathy.24 Itis likely that in these patients, impaired subendocar-dial function caused by underperfusion of the sub-endocardium in aortic stenosis and hypertrophiccardiomyopathy leads to a reduction of fiber con-traction in this region of the myocardium resultingin an increase in LV twist per amount of ejection.25
In a similar manner, the subendocardial fibrosisnoted with aging may result in increased twist.Although the mechanism for these observation is
Table 2 Left ventricular twist and twist velocity-derived pa
Young (n � 57)
Peak twist, degree 6.7 � 2.9Twist at AVC, degree 6.5 � 2.9Twist at MVO, degree 4.3 � 3.4Untwisting at 110% ES, % 14.6 � 13.7Untwisting at 120% ES, % 44.6 � 32.0Untwisting at 130% ES, % 70.0 � 33.3Untwisting rate, %/ms 0.64 � 0.42PPTV, degree/s 45.0 � 16.6PNTV, degree/s �58.6 � 24.7Time to PPTV, % 53.5 � 9.8Time to PNTV, % 119.5 � 5.4
AVC, Aortic valve closure; ES, end systole; MVO, mitral valve opening;significant. Time to PPTV and PNTV were expressed as percentage of end
still not precisely understood, our results suggest
that increased systolic twist is not a specific findingassociated with LV hypertrophy, but that a similarmechanism may operate with aging.
Diastolic Untwisting
Studies in normal hearts indicate that torsional re-coil, or untwisting, predominantly occurs duringisovolumic relaxation.3,4 This recoil mechanism is amajor determinant of myocardial compliance and LVsuction that in turn modulates diastolic filling prop-erties.3,4 With aging, reduced and delayed diastolicuntwisting was noted, and this might be associatedwith decreased myocardial compliance. Althoughcontroversy exists regarding the observed reductionin untwisting with aging,16,26 a similar mechanismhas been observed in patients with aortic steno-sis.17,22,23 Our results indicate that increased systolictwist with reduced untwisting occurs in the agingheart, highlighting the need for age-matched controlsubjects in studies of diastolic function. Comparedwith the young group, time to peak negative twistvelocity was significantly prolonged in the middle-aged group, but not in the older group in this study.This could be a result of the small number ofvolunteers in the older group. As expected, Dopplerechocardiography showed significant differences inboth E and A transmural flow velocities among the 3age groups. The reduction in early diastolic fillingoccurring with aging is thought to be partly a resultof the presence of a partially rotated LV that impairsblood flow into the LV during early diastole. Because2D speckle-tracking imaging allows measurementsof untwisting rates during the diastolic isovolumicperiod (before blood flow or wall motion begins),measurement of untwisting and untwisting ratesshould constitute novel markers for the assessmentof LV relaxation.
Limitations
In this study, there was no gold standard for measuring
ers in different age groups
le aged (n � 41) Older (n � 15) P
8.0 � 3.0 10.8 � 4.9 �.0017.9 � 3.1 10.7 � 4.8 �.0015.6 � 2.7 7.3 � 4.2 �.0017.2 � 9.9 5.8 � 8.5 �.001
24.5 � 20.0 19.8 � 15.5 �.00144.9 � 25.9 40.9 � 17.0 �.0010.40 � 0.22 0.41 � 0.19 �.00247.9 � 16.4 57.2 � 27.2 �.157.4 � 21.9 �50.0 � 14.8 ns50.1 � 13.7 50.0 � 14.8 ns25.9 � 11.6 122.6 � 7.5 �.005
peak negative twist velocity; PPTV, peak positive twist velocity; ns, notend systole � 100%)
ramet
Midd
�
1
PNTV,
LV twist and twist velocity. However, a previous study

Journal of the American Society of EchocardiographyVolume 19 Number 9 Takeuchi et al 1083
has recently validated the accuracy of speckle-trackingimaging versus tagged MRI.10,11,13,15 The exact loca-tion of the basal and apical plane may vary frompatient to patient and may induce some measuringerror. The resolution of the 2D image may be aproblem in some individuals and border recognitionmay be another limiting factor for assessing LVrotation. The 2D speckle-tracking analysis cannoteliminate the errors introduced by through-planemotion, particularly in the basal plane. With anytomographic method, the same point may not beseen during systolic contraction and diastolic relax-ation. The relatively higher tracking score in the
Figure 4 Mean � SD of left ventricular (LV) twisolder volunteers.
basal plane compared with the apical plane might
account for this limitation. However, previous stud-ies have shown that LV twist increases nonlinearlytoward the apex, thus, limiting the impact ofthrough-plane motion at the base.9,27 Although theframe rate in this study was higher than that de-scribed in previous tagged MRI studies, furtherrefinements aimed to imaging at even higher framerates would be ideal to assess mechanical eventsoccurring during isovolumic relaxation.
Conclusions
The 2D speckle-tracking imaging can be used to
nd twist velocity (B) in young, middle-aged, and
t (A) anoninvasively quantify LV twist with high feasibility.

Journal of the American Society of Echocardiography1084 Takeuchi et al September 2006
Measurements are simple and reproducible. Withaging, LV twist is significantly enhanced and un-twisting significantly reduced and delayed, suggest-ing prolonged myocardial relaxation. This study isthe first to report normal values of LV twist and twistvelocity over a wide range of ages. These valuescould be used as age controls in different studies.This novel method allows the detailed study ofdiastolic function, especially myocardial relaxationin various cardiovascular diseases.
REFERENCES
1. Buchalter MB, Rademakers FE, Weiss JL, Rogers WJ, Weis-feldt ML, Shapiro EP. Rotational deformation of the canineleft ventricle measured by magnetic resonance tagging: effectsof catecholamines, ischemia, and pacing. Cardiovasc Res1994;28:629-35.
2. Buckberg G. Basic science review: the helix and the heart.J Thorac Cardiovasc Surg 2002;124:863-83.
3. Rademakers FE, Buchalter MB, Rogers WJ, Zerhouni EA, We-isfeldt ML, Weiss JL, et al. Dissociation between left ventricularuntwisting and filling: accentuation by catecholamines. Circula-tion 1992;85:1572-81.
4. Dong S, Hees P, Siu C, Weiss J, Shapiro E. MRI assessment ofLV relaxation by untwisting rate: a new isovolumic phasemeasure of tau. Am J Physiol Heart Circ Physiol 2001;281:H2002-9.
5. Ashikaga H, Criscione JC, Omens JH, Covell JW, Ingels NB Jr.Transmural left ventricular mechanics underlying torsionalrecoil during relaxation. Am J Physiol Heart Circ Physiol2004;286:H640-7.
6. Yun KL, Niczyporuk MA, Daughters GT II, Ingels NB Jr,Stinson EB, Alderman EL, et al. Alterations in left ventriculardiastolic twist mechanics during acute human cardiac allograftrejection. Circulation 1991;83:962-73.
7. Mirro MJ, Rogers EW, Weyman AE, Feigenbaum H. Angulardisplacement of the papillary muscles during the cardiac cycle.Circulation 1979;60:327-33.
8. Tischler M, Niggel J. Left ventricular systolic torsion andexercise in normal hearts. J Am Soc Echocardiogr 2003;16:670-4.
9. Notomi Y, Setser R, Shiota T, Martin-Miklovic M, Weaver J,Popovic Z, et al. Assessment of left ventricular torsional defor-mation by Doppler tissue imaging: validation study withtagged magnetic resonance imaging. Circulation 2005;111:1141-7.
10. Amundsen B, Helle-Valle T, Edvardsen T, Torp H, Crosby J,Lyseggen E, et al. Noninvasive myocardial strain measurementby speckle tracking echocardiography. J Am Coll Cardiol2006;47:789-93.
11. Helle-Valle T, Crosby J, Edvardsen T, Lyseggen E, Amund-sen BH, Smith HJ, et al. New noninvasive method for assess-ment of left ventricular rotation: speckle tracking echocardi-ography. Circulation 2005;112:3149-56.
12. Leitman M, Lysyansky P, Sidenko S, Shir V, Peleg E, Binen-
baum M, et al. Two-dimensional strain–a novel software forreal-time quantitative echocardiographic assessment ofmyocardial function. J Am Soc Echocardiogr 2004;17:1021-9.
13. Notomi Y, Lysyansky P, Setser R, Shiota T, Popovic Z,Martin-Miklovic M, et al. Measurement of ventricular torsionby two-dimensional ultrasound speckle tracking imaging.J Am Coll Cardiol 2005;45:2034-41.
14. Reisner SA, Lysyansky P, Agmon Y, Mutlak D, Lessick J,Friedman Z. Global longitudinal strain: a novel index of leftventricular systolic function. J Am Soc Echocardiogr 2004;17:630-3.
15. Suffoletto M, Dohi K, Cannesson M, Saba S, Gorcsan JI.Novel speckle-tacking radial strain from routine black-and-white echocardiographic images to quantify dyssynchrony andpredict response to cardiac resynchronization therapy. Circu-lation 2006;113:960-8.
16. Oxenham HC, Young AA, Cowan BR, Gentles TL, Occle-shaw CJ, Fonseca CG, et al. Age-related changes in myocar-dial relaxation using three-dimensional tagged magnetic res-onance imaging. J Cardiovasc Magn Reson 2003;5:421-30.
17. Nagel E, Stuber M, Burkhard B, Fischer S, Scheidegger M,Boesiger P, et al. Cardiac rotation and relaxation in patientswith aortic valve stenosis. Eur Heart J 2000;21:582-9.
18. Nagel E, Stuber M, Lakatos M, Scheidegger M, Boesiger P,Hess O. Cardiac rotation and relaxation after anterolateralmyocardial infarction. Coron Artery Dis 2000;11:261-7.
19. Taber LA, Yang M, Podszus WW. Mechanics of ventriculartorsion. J Biomech 1996;29:745-52.
20. Tibayan F, Rodriguez F, Langer F, Zasio M, Bailey L, Liang D,et al. Alterations in left ventricular torsion and diastolic recoilafter myocardial infarction with and without chronic ischemicmitral regurgitation. Circulation 2004;110:II109-14.
21. Tibayan F, Lai D, Timek T, Dagum P, Liang D, Daughters G,et al. Alterations in left ventricular torsion in tachycardia-induced dilated cardiomyopathy. J Thorac Cardiovasc Surg2002;124:43-9.
22. Stuber M, Scheidegger M, Fischer S, Nagel E, Steinemann F,Hess O, et al. Alterations in the local myocardial motionpattern in patients suffering from pressure overload due toaortic stenosis. Circulation 1999;100:361-8.
23. Sandstede JJ, Johnson T, Harre K, Beer M, Hofmann S, PabstT, et al. Cardiac systolic rotation and contraction before andafter valve replacement for aortic stenosis: a myocardial tag-ging study using MR imaging. Am J Roentgenol 2002;178:953-8.
24. Young AA, Kramer CM, Ferrari VA, Axel L, Reichek N.Three-dimensional left ventricular deformation in hypertro-phic cardiomyopathy. Circulation 1994;90:854-67.
25. Delhaas T, Kotte J, van der Toorn A, Snoep G, Prinzen FW,Arts T. Increase in left ventricular torsion-to-shortening ratioin children with valvular aortic stenosis. Magn Reson Med2004;51:135-9.
26. Hees PS, Fleg JL, Dong SJ, Shapiro EP. MRI and echocar-diographic assessment of the diastolic dysfunction of normalaging: altered LV pressure decline or load? Am J Physiol HeartCirc Physiol 2004;286:H782-8.
27. Moore CC, Lugo-Olivieri CH, McVeigh ER, Zerhouni EA.Three-dimensional systolic strain patterns in the normal hu-man left ventricle: characterization with tagged MR imaging.
Radiology 2000;214:453-66.