after the binge: using the mindful-based strategies to ... strategies to treat binge eating...
TRANSCRIPT

After the Binge: Using the Mindful-based Strategies to Treat Binge Eating Disorders
Nancy Romanick, RD, MBA, MAPC, LAC

Objectives
1. Identify the barriers and goals of evidence-based treatment for Binge Eating Disorder and include these in effective treatment planning with clients with BED
2. Identify and implement an effective treatment protocol for clients with BED that include DBT and mindful-based therapy to address the emotional regulation function of BED
3. Use the Mindful Eating Cycle (Am I Hungry? Mindful Eating for Binge Eating Program) to help their clients explore decision-making, including awareness of hunger and satiety, non-restrictive food selection, and mindful enjoyment of food.

BED Newly recognized in DSM5
• Affects 3 million US Adults
• Most common Eating disorder
• More than twice as prevalent as BN/AN combined
• 1.6% women and .8% men
• Median onset 21 years old
• < 50% of adults with BED are obese, 19% are normal weight, 36% are overweight

Diagnostic Criteria - DSM5 A. An episode of binge eating is characterized by:
• Eating an amount of food, in a discrete period of time, that is definitely larger than what most would eat in a similar period of time under similar circumstances
• A sense of lack of control over eating during the episode
• A feeling that one cannot stop eating or control what or how much one is eating

Diagnostic Criteria - DSM5
B. The binge eating episodes are associated with three or more of the following:
– Eating much more rapidly than normal
– Eating until feeling uncomfortably full
– Eating large amounts of food when not feeling physically hungry
– Eating alone because of being embarrassed by how much one is eating
– Feeling disgusted with oneself, depressed or very guilty after overeating

Diagnostic Criteria - DSM5
C. Marked distress regarding binge eating
D. The binge eating occurs on average at least once a week for three months
E. The binge eating is not associated with the recurrent use of inappropriate compensatory behaviors (purging) and does not occur exclusively during the course of anorexia or bulimia
Severity (BE episodes per week):
Mild 1-3, Moderate 4-7, Severe 8-13, Extreme 14 or more

The Challenge of BEDMisunderstood Disorder Co-Morbid Psychiatric Disturbances
Shame and Secrecy Obesity is the focus
Dieting is Problematic Low self-directedness and Perfectionism

Barriers to effective treatment
• Misunderstood disorder
• 30% of individuals seeking professional treatment for weight management have binge eating disorder.
• Often giving the wrong “prescription” of dietary restraint leading to further feelings of failure

Barriers to effective treatment
• Those with binge eating differ from others seeking weight loss in that they tend to have co-morbid psychiatric disturbances:
–Mood, anxiety, impulsivity, substance use, ADHD and eating pathology.
–Half are depressed or have been depressed.
~ Shapiro 2007, Dingemans 2002, Grilo 2001

Co-occurring Disorders
• High correlation with obesity
• Medical problems: medical problems, PCOS, Diabetes, Cardiovascular disease, gallbladder
• Depression
• Anxiety
• Substance use
• Bipolar disorder and ADHD

Shame and Secrecy
• Binge Eating Disorder goes largely untreated because people who have it don’t readily disclose the behaviors done in private
• Many with BED eat normally around others, or may exhibit restrictive eating and yo-yo dieting.

Focus on Obesity
• Paradoxically, providers who encourage weight management strategies may be unknowingly triggering the symptoms
• Focusing on the obesity, unfortunately perpetuates the shame cycle
• (Sadly, clients don’t understand what they are asking for isn’t working, they just think they are failing treatment over and over again)
• Not all people with BED are obese. It depends on the compensatory behaviors such as excessive exercise or dietary restraint following a binge episode

Barriers to effective treatment
• Dieting is problematic– Creates feelings of deprivation that leads to
cravings, impulsivity and counter regulation, aggravating binge eating
– Hawks et al 2008
– Creates feelings of shame; more likely to drop out of treatment
– Creates impaired sensitivity to hunger and satiety clues

Barriers to effective treatment
• Dieting is problematic (cont)
IT’S NOT ABOUT THE FOOD– Binge eating must be the treatment priority
– Abstinence from binge eating is a predictor of successful maintenance and weight loss, which suggests treatment of the eating disorder is the priority over weight loss
~Dingeman 2002, Grilo 2011

• Low self-directedness
– Self-directedness is the ability to regulate and adapt behavior to reach one’s goals
–May explain need to seeking weight loss methods
~Latzer 2003, Dalle-Grave 2012
• Perfectionism triggers binge eating
~Sherry & Hall 2009
Barriers to effective treatment

• Low interpersonal esteem, interpersonal discrepancies, depressive affect
• Over-valuation of weight and shape
~ Apfeldorfer 2001, Latzer 2003, Sherry & Hall 2009, Dalle-Grave 2012
Barriers to effective treatment

• Cessation of binge eating
• Improvement in eating-related psychopathology
• Reduction in psychiatric co-morbidity
• Improvement in physical health and relationship with the body.
Goals for Treatment of BED

• Treatment follows function
• The key to determine effective treatment is based largely on the function of the binge eating.
• The Why? Behind the Eating disorder will guide finding a replacement for the need it is replacing.
Cessation of the Binge Eating
• Treatment follows function (Cont)
• Binge eating may be a valuable tool in helping someone protect themselves from harm, rejection, failure, power or other threatening situations. This is supported by a strong belief system.
• An unconscious decision occurs when faced with the choice to do it differently.
Cessation of the Binge Eating

• OF COURSE!• The behavior is reasonable and
understandable given the needs and life circumstances.
• “I’ve never met anyone who didn’t have a great reason for having an eating disorder.”
~Kari Anderson DBH, LPC
Cessation of the Binge Eating

• Abstinence from binge eating is a predictor of successful maintenance and weight loss, which suggests treatment of the eating disorder is the priority over weight loss.
~Dingemans 2002, Grilo 2011
• Significantly greater BMI reduction (3.5 - 4.3%) compared to those who continue to binge eat.
Cessation of the Binge Eating

• Eating-Related Psychopathology
– Perfectionism
– Intolerance to ambiguity
– Unable to trust themselves
– Inability to accept self, weight and shape
– Inability to recognize the underlying beliefs
Goals for Treatment of BED

• Where to start-
– Help the client identify the many faces protecting the function of the eating disorder.
– Calm and reassure by developing the voice of self compassion, “of course” to create a safe environment for change.
– Start with validating the need for the eating disorder thus far.
Goals for Treatment of BED
“Some individuals respond to emotions by eating. Food and the eating process serve to comfort, distract or “distance” oneself from emotions…[this] interferes with the body’s natural physical cues of hunger, fullness, appetite and satiety…the result is disconnection from internal cues.”
~Moving Away From Diets Kratina, King, and Hayes
Goals for Treatment of BED

• Problems with emotions
– Difficulty recognizing, labeling and self-regulating emotions
– Predominant emotions before a binge: anger, loneliness, disgust, exhaustion, shame
– Lack of coping skills
– Difficulty listening to their body and providing self-care
Goals for Treatment of BED

Dissociation and Distraction
Bingeing becomes a Trance-like state:
– To escape emotions which are intolerable and seen as pathological
– To escape thinking about the long-term consequences of actions or to procrastinate unpleasant activities
– To escape one’s critical thoughts and feelings of inferiority
~Shafran 2001, Leahy 2002, LaMella 2010
Goals for Treatment of BED

• Traditional CBT is the most widely researched method of treatment with BN and BED.
• CBT has been shown to eliminate binge eating in 50% participating in treatment. ~ Wilfley, Wilson & Agras 2010
• Traditional CBT alone doesn’t address the internal blocks and motivational factors necessary to change behavior long term
Evidenced Based Treatment of BED

• Dialectical Behavior Therapy– Considered a form of CBT
– Dialectics (acceptance and change)
– Seemingly opposite stances can both be true at the same time. Therefore one can be deemed completely acceptable and at the same time need to change.
– Key to dialectics is the balancing act between validation and pushing for behavior change
– Moving out of black and white, extreme thinking, into a both/and approach (middle path)
Linehan, 1983, Telch 2001
Evidenced Based Treatment of BED

• Dialectical Behavior Therapy (cont)
– Considered a mood regulation model for the treatment of binge eating
Linehan, 1983, Telch 2001
– Mindfulness is taught to counteract dissociation
– Rapid response of binge abstinence, continues throughout treatment an a one year follow up with DBT
– Safer and Joyce 2011
Evidenced Based Treatment of BED

• Dialectical Behavior Therapy (cont)– Basic CBT eliminated binge eating and purging in about
50% participants…but when mindfulness training and acceptance-related procedures have been adapted and introduced to eating disorder treatment we have seen the elimination of bingeing sustained over time.
– ~ Safer & Joyce 2011, Anderson & May 2013
Evidenced Based Treatment of BED

Mindfulness
The ability to be aware of your thoughts, emotions, physical sensations, and actions in the present moment without judging or criticizing yourself or your experience.
~ Jon Kabat-Zinn
• Mindfulness-based approaches provide individuals with a heightened ability to simply observe feelings and experiences and disengage automatic reactivity.
• It cultivates a wiser and more balanced relationship with their selves, their eating, and their bodies.

32
AM I HUNGRY- ME-BE
• Key treatment components:
– Why do I eat? Eating Cycles (Mindful, Binge, Restrictive, Overeating)
– Pendulum Swing (Finding the Middle Path)
– Dichotomous thinking
– Body Wisdom – Hunger fullness awareness
– It’s not about the food – meeting your true need
– Internal dialogue – Self care voice (Validation and Change)
From Eat What You Love,
Love What You Eat for
Binge Eating
By Michelle May, MD and
Kari Anderson DBH LPC

33
AM I HUNGRY- ME-BE
• Key treatment components:
– Reducing triggers (TFAR)
– Mindfulness Based Stress Reduction techniques
– Awareness Journals
– My Goodbye!
– Emotions and Needs
– Balancing eating and nourishment- Eat What you love!
– Fearless eating
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC

Mindful Eating Cycle
34

From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
35
Mindful Eating Cycle

Instinctive Eating Cycle
36

37
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Instinctive Eating Cycle

38
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Instinctive Eating Cycle

39
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Instinctive Eating Cycle

40
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Instinctive Eating Cycle

41
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Instinctive Eating Cycle

42
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Instinctive Eating Cycle

Binge Eating Cycle
43

44
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
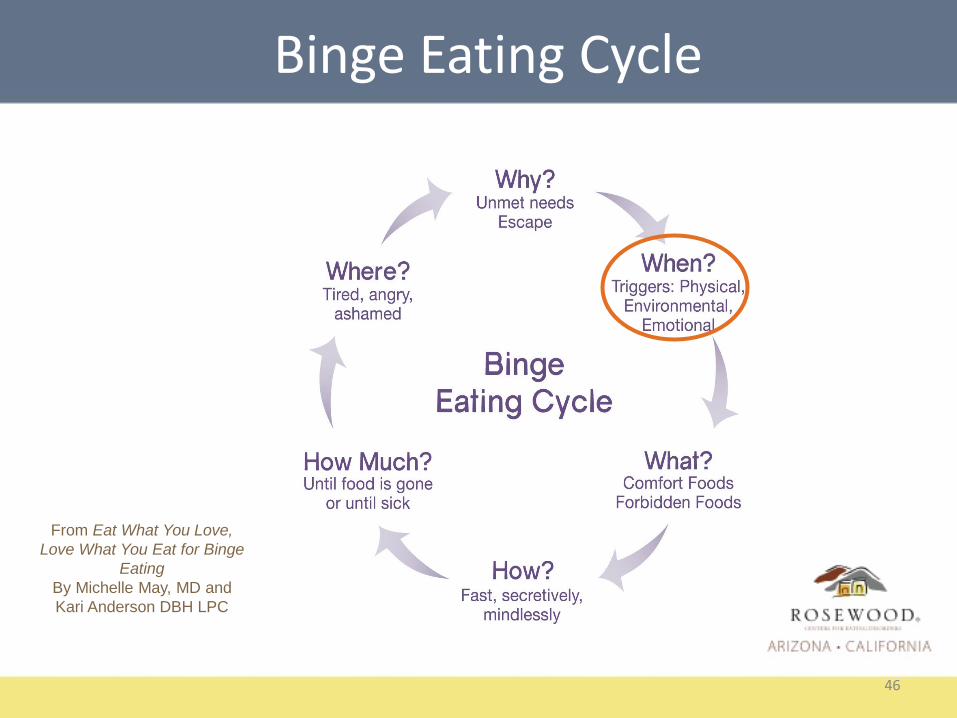
Binge Eating Cycle

Replacement for unmet needs
Escape from awareness of self-critical thoughts and negative emotional states
Cycle drivers for binge eating
45
46
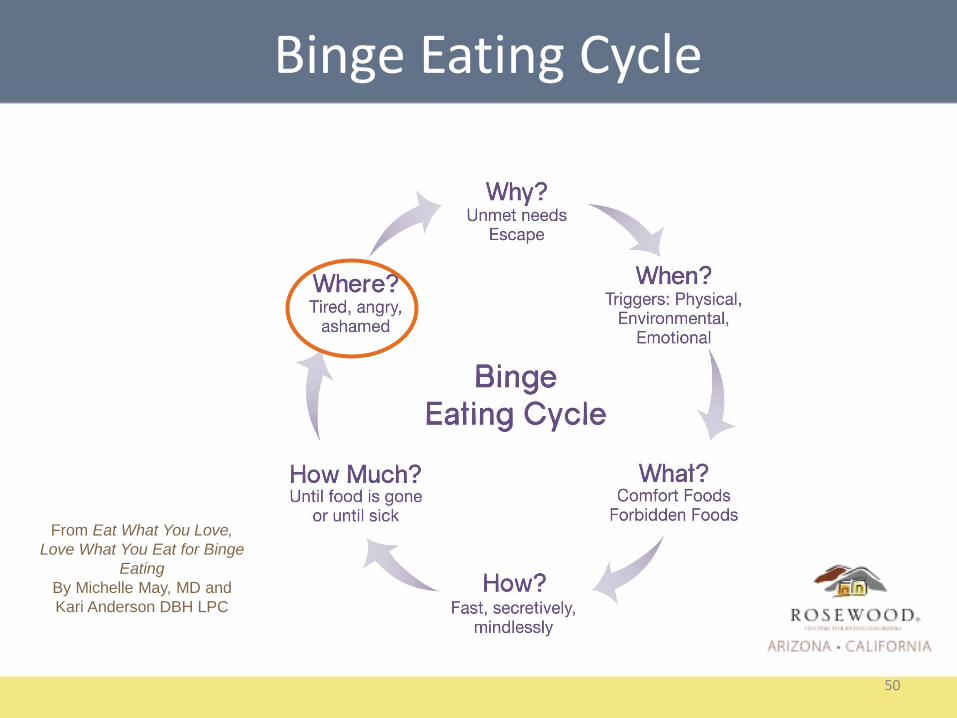
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Binge Eating Cycle

47
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Binge Eating Cycle

48
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Binge Eating Cycle

49
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Binge Eating Cycle
50
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Binge Eating Cycle

51

Restrictive Eating Cycle
52
Restrictive Eating Cycle

53
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Restrictive Eating Cycle

54
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Restrictive Eating Cycle

55
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Restrictive Eating Cycle
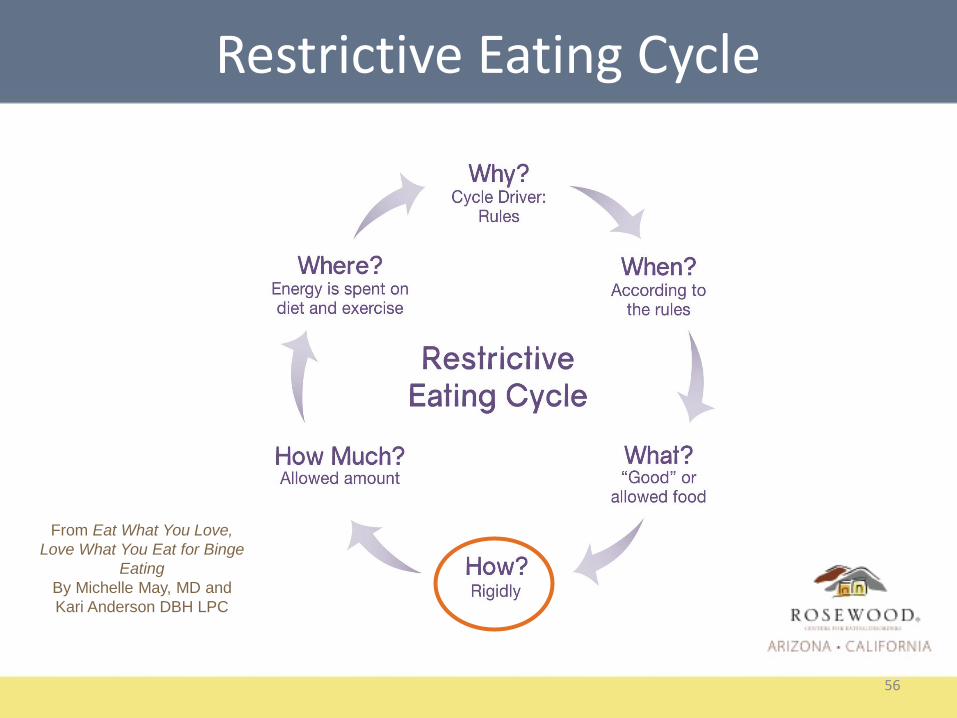
56
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Restrictive Eating Cycle

57
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Restrictive Eating Cycle

58
From Eat What You Love,
Love What You Eat for Binge
Eating
By Michelle May, MD and
Kari Anderson DBH LPC
Restrictive Eating Cycle

Trigger React
Re-Act
Mindlessness
59

Trigger Pause
Respond (Response-Ability)
Mindfulness
60

BED Research Study 2012
• Purpose was to test a 10 week program for BED using evidence based modalities for BED integrating the Mindful Eating Cycle Framework
• Research by Michelle May, MD and Kari Anderson DBH LPC

BED Research Study 2012
• Purpose was to test a 10 week program for BED using evidence based modalities for BED integrating the Mindful Eating Cycle Framework
• Research by Michelle May, MD and Kari Anderson DBH LPC

BED Research Study 2012
Six measures pre and post
• BES : Binge Eating Scale
• MAAS: Mindful Attention Awareness Scale
• STC : Starting the Conversation
• RAPA: Rapid Assessment of Physical Activity
• PHQ -9 Patient Health Questionnaire
• GAD-7 General Anxiety Disorder

Results Summary Study 2012• Participants started at severe binge eating level; BES
decreased to non-bingeing level by 10 weeks
• Decrease depression – moderate to mild
• Decrease anxiety- High mild to low mild
• Improved Mindful Awareness/Attention
• Improved dietary choices
• Slight improvement in physical activity
• Low attrition rate (14%)
• High participant evaluation score (9.6 out of 10)

Role of Eating Cycle Awareness
• Binge Eating = Out of Control
• Restrictive Eating= In Control
• Mindful Eating = In Charge

Autonomous Eating
– More concern for the quality of one’s food
– More energy, sustained healthy eating
Control Eating
– Drains energy and more concerned for quantity of food
Verstuyf, Patrick, Vansteenkiste & Texeira, 2012
Motivation and Eating
66

Intrinsic goals that are autonomous in motivation have distinctly better outcomes in eating regulation than those with extrinsic motivation and controls.
Pelletier and Dion 2007
Better Outcomes
67

Mindfulness-based approaches provide individuals with a heightened ability to simply observe feelings and experiences and disengage automatic reactivity.
Cultivates a wiser and more balanced relationship with their self, their eating, and their body.
Conclusion
68


Contact Information
Nancy Romanick RDN, MBA, LAChttp://www.mybalancedlifecounseling.com/my_Balanced_Life,_LLC/Welcome.html
For information on training www.AmIHungry.com
email information:
References will be provided

Continuing Education Certificate
2-Ways to earn CE’s for Webinars
1. Attending ‘LIVE’ Webinars1) Attend LIVE Webinar presentation. 2) Within a few hours following the LIVE Webinar you will receive an email with an
Evaluation Form and Post-Test attached. 3) Complete both forms and return to [email protected]) Upon receipt of the Post-Test and Evaluation Form, and successful completion of
the post-test (score of 80% or better), a CE Certificate will be sent to you.
2. Attending Recorded Webinars under the TRI Website ‘CE Webinar’ Tab
1) Register at TRI where you will find a list of chosen pre-recorded webinars under the CE Webinar Tab.
2) Here you will be able watch the full video presentation and have access to the Post-test and Evaluation Summary. A CE Certificate is downloadable available upon passing the post test.
How To Contact Us:
Send questions about Continuing Education to:[email protected]
Visit us for more Continuing Education Opportunities:www.RosewoodInstitute.org
Contact us: 1-800-845-2211