adverse host tissue responses in...
TRANSCRIPT

ADVERSE HOST TISSUE RESPONSES IN LOOSENING
OF DENTAL IMPLANTS
PROTEOLYTIC ENZYMES AND PERI-IMPLANT TISSUE DESTRUCTION
JIAN MA
Department of Medicine/ Invärtes medicin, Helsinki University Central Hospital Department of Anatomy, University of Helsinki
ORTON Orthopaedic Hospital of the Invalid Foundation, Helsinki
ACADEMIC DISSERTATION
To be presented, with the assent of the faculty of Medicine of the University of Helsinki, for defense in the small Lecture Hall, Haartman Institute,
Haartmaninkatu 3, Helsinki, on March 19th, at 12 noon.
HELSINKI 2004
Supervised by:
Professor Yrjö T. Konttinen, MD, PhD Department of Medicine/ Invärtes medicin Helsinki University Central Hospital, Department of Anatomy, University of Helsinki, and ORTON Orthopaedic Hospital of the Invalid Foundation
Helsinki, Finland
Professor Seppo Santavirta, MD, PhD Department of Orthopaedics and Traumatology Helsinki University Central Hospital Helsinki, Finland
Reviewed by:
Professor Panos N. Papapanou, DDS, PhD Division of Periodontics Columbia University School of Dental and Oral Surgery New York, NY USA
Docent Juha Nevalainen MD, PhD Medical Devices Centre The National Agency for Medicines Helsinki, Finland
Opponent:
Docent Ilmo Leivo, MD, PhD Department of Pathology Haartman Institute University of Helsinki
Helsinki, Finland
ISBN 952-91-6889-6 (paper) ISBN 952-10-1704-X (PDF) http://ethesis.helsinki.fi University Press Helsinki 2004

To WenWen and my parents

CONTENTS
1. LIST OF ORIGINAL PUBLICATIONS 7
2. ABBREVIATIONS 8
3. ABSTRACT 9
4. INTRODUCTION 11
5. REVIEW OF THE LITERATURE 12 1. OSSEOINTEGRATION 12 2. END-STAGE LOSS OF TOOTH/TEETH 12 2.1 Congenital anodontia 12 2.2 Trauma 13 2.3 Cancer 13 2.4 Root caries and periodontitis 13 3. DENTAL IMPLANT CATEGORIES 13
3.1 Implant categories and their indications for use 13 3.2 Clinical implant categories 14 4. DENTAL IMPLANT SUCCESS ANALYSIS 15
4.1 Implant success criteria 15 4.2 Cumulative success rates 15 5. FAILURE OF DENTAL IMPLANTS 17
5.1 Failure types 17 5.1.1 Early stage failure 17
5.1.2 Late stage failure 17 5.1.2.1 Mechanical late stage failure 17 5.1.2.2 Biological late stage failure (loosening) 18
5.2 Cumulative failure rates 18 6. THE CONCEPT OF LOOSENING 18 7. WHY DO DENTAL IMPLANTS LOOSEN/ FAIL 19 7.1 Dentist-related risk factors 19 7.1.1 Preoperative factors 19 7.1.2 Peroperative factors 19 7.1.3 Postoperative factors 19 7.2 Implant material-related risk factors 20 7.2.1 Dental implant material characteristics 20 7.2.2 Implant surface 22 7.2.3 Interface tissue 22 7.3 Host-related risk factors 22 7.3.1 Local risk factors 23 7.3.1.1 Biomechanical occlusal loading 23 7.3.1.2 Peri-implantitis and clinical indices 25
7.3.1.3 Cigarette smoking 26 7.3.1.3 Para-functional habits, bruxism 26
7.3.2 Systemic factors 27 7.3.2.1 Diabetes mellitus 27 7.3.3.2 Osteoporosis 27 7.3.3.3 Medication and irradiation therapy 28 8. ADVERSE HOST TISSUE RESPONSES DURING LOOSENING 29 8.1 Host responses and their types 29 8.2 Extracellular matrix 29 8.2.1 Collagen 30 8.2.2 Fibronectin and integrins 30 8.2.3 Bone 31 8.3 Proteolytic enzymes 32 8.3.1 Proteinases and their characteristics 32 8.3.1.1 Matrix metalloproteinase 32 8.3.1.2 Activation 32 8.3.1.3 Inhibition 33 8.3.2 Collagen degradation 33
8.3.2.1 Intracellular route 33 8.3.2.2 Extracellular route 34 8.3.1.2.1 The intra-helical cleavage site 34 8.3.1.2.2 The extra-helical cleavage site 35 8.3.1.2.3 Intra- and extra-helical cleavage sites 35 8.3.3 Features of collagen degradation 35 8.3.3.1 Collagen degradation in gingival tissue 35 8.3.3.2 Bone collagen degradation 37 8.4 Fibronectin and neutrophil elastase 37 8.5 Cytokines in bone resorption 38
6. AIMS OF THE STUDY 42
7. MATERIALS AND METHODS 43 7.1 Patients and samples 43 7.2 Immunofluorometric assay 43 7.3 Modified pro-urokinase gelatinase-B activity assay 44 7.4 Quantitative immunoblot technique 45 7.5 Immunohistochemical avidin-biotin-peroxidase complex (ABC) staining 45 7.6 Microscopic morphometric evaluation 46 7.7 Statistical methods 46
8. RESULTS 47 8.1 Collagenase levels differed between different peri-implant vertical bone loss groups 47 8.2 Gingival indices did not differ between different peri-implant vertical
bone loss groups 47 8.3 Gelatinase-B levels in PISF correlated with peri-implant vertical bone loss 47 8.4 Gelatinase-B levels in PISF differed between different gingival index groups 47 8.5 Cellular fibronectin staining was higher in gingival tissue 48 8.6 Distribution of integrin receptors for cellular fibronectin in gingival tissue 48 8.7 Increased staining of collagenase-cleaved collagen fragments (cCOL1-3/4C) in untreated chronic periodontitis 48 8.8 Increased expression of osteoclast stimulating cytokines in gingival tissue in chronic periodontitis and implantitis 49
9. DISCUSSION 509.1 Collagenase-2, -3 and gelatinase-B involved in implant bone loss 50 9.2 Gingival index and peri-implant bone loss 52 9.3 Gingival index and gelatinase-B 53 9.4 Collagenase cleaved type I collagen fragment and chronic periodontitis 54 9.5 Cellular fibronectin in chronic periodontitis and loosening 55 9.6 Osteoclast stimulating cytokine network in loosening and periodontitis 56
10. SUMMARY AND CONCLUSIONS 59
11. ACKNOWLEDGMENTS 60
12. REFERENCES 62
7
1. LIST OF ORIGINAL PUBLICATIONS
This thesis is based on the following original publications, which will be referred to in the text by their Roman numerals.
I Ma J, Kitti U, Teronen O, Sorsa T, Husa V, Laine P, Ränk H, Salo T, Lindqvist C, Konttinen YT. Collagenases in different categories of peri-implant vertical bone loss. J Dent Res 2000; 79:1870-1873.
II Ma J, Kitti U, Hanemaaijer R, Teronen O, Sorsa T, Natah S, Tensing E.K., Konttinen Y.T. Gelatinase-B is associated with peri-implant bone loss. Clin Oral Implants Res 2003; 14:709-713.
III Ma J, Sorsa T, Könönen M, Santavirta S, Virtanen I, Konttinen YT. Cellular fibronectin in failing dental implants. Int J Oral Maxillofac Implants 2002; 17:363-368.
IV Ma J, Sorsa T, Billinghurst CR, Poole RA, Kitti U, Santavirta S, Konttinen YT. Direct evidence of collagenolysis in chronic periodontitis. J Periodontal Res2003; 38:564-567.
V Konttinen YT, Ma J, Lappalainen R, Laine P, Kitti U, Santavirta S, Teronen O. Immunohistochemical evaluation of inflammatory mediators in failing implants. Int J Periodontics Restorative Dent. In press.
The original publications are reprinted with the permission of the copyright holders.
8
2. ABBREVIATIONS
ABC avidin-biotin-peroxidase complex
BSA bovine serum albumin
CE Certificate European
CMT chemically modified tetracycline
cFN cellular fibronectin
COL1-3/4C collagenase-cleaved type I collagen 3/4 carboxy-terminal neoepitope
CP chronic periodontitis
DAB 3,3'-diaminobenzidine tetrahydrochloride
EGF epidermal growth factor
FDA Food and Drug Administration
mGI modified Gingival Index
IL interleukin
MMP matrix metalloproteinase
MoAb monoclonal antibody
NIH National Institutes of Health
PBS phosphate buffered saline
PDGF platelet-derived growth factor
PISF peri-implant sulcus fluid
PoAb ployclonal antibody
RANKL receptor activator of nuclear factor kappa B ligand
TBS TRIS buffered saline
TGF transforming growth factor
TIMP tissue inhibitor of metalloproteinases
TNF tumor necrosis factor
9
3. ABSTRACT
Dental implants have been remarkably improved in the past half century: Cumulative success rates at 10 years are satisfactory, about 88% for maxillary and 93% for mandibular implants. Loosening of dental implants is, however, a major complication to be faced, with many risk factors affecting loosening. No matter what these risk factors are, they affect the pathological biological cascades in peri-implant support tissues. This study focused on proteinases and cytokines able to mediate extracellular matrix destruction in peri-implant support tissues during loosening.
Collagenase-2 (a time-resolved immunofluorometric assay), collagenase-3 (a quantitative immunoblot) and gelatinase-B (a modified urokinase assay) were measured in peri-implant sulcus fluid (PISF). The gingival index did not correlate with the degrees of peri-implant vertical bone loss (0.6 ± 0.1 in patients with < 1mm loss, 0.6 ± 0.5 in patients with 1 to 3 mm loss, and 1.2 ± 0.3 in patients with > 3 mm loss, p > 0.05, Kruskall-Wallis test). Collagenase-2 (2021 ± 1038, p < 0.05) and collagenase-3 (16 ± 4, p < 0.05) in PISF were higher in the group with > 3 mm bone loss than in the other two groups with either 1 to 3 mm loss (1265 ± 508 and 12 ± 2) or bone loss < 1 mm (861 ± 164 and 10 ± 1) (Kruskall-Wallis test).
Total gelatinase-B (r = 0.55, p = 0.02) and activated gelatinase-B levels (r = 0.52, p =0.003) in PISF correlated with the peri-implant vertical bone loss (Spearman's rank correlation test). Total (1375[1633]) and activated gelatinase-B (458 [979]) levels in the high-loss group (> 3 mm) were higher than in the 1 to 3 mm (250[533]; 166[200]) and < 1 mm groups (183[480]; 133[225]). Activated gelatinase-B level (225[267]) in the GI > 0.5 group was increased compared to GI = 0 (50[125]) and 0.5 groups (216[375]) (Rank sum test).
Immunohistochemical staining was used to detect cellular fibronectin (cFN) in gingival tissue. cFN was found in epithelial basement membrane, connective tissue papillae, walls of blood vessels, and fibroblasts in lamina propria. Computerized image analysis was applied for quantitation of cFN. cFN staining in the loosened implant group (33 ± 5% positive staining, p < 0.05) was high, but low in the periodontitis group (6 ± 1%, p < 0.05) compared to that in normal controls (12 ± 1%).
Collagenase-cleaved collagen type I 3/4 carboxy-terminal neoepitope (COL1-3/4C) antibody was used to detect gingival COL1-3/4C. Moderate staining was visible in connective tissue bordering the sulcular and junctional epithelium, surrounding some of the fibroblasts, and in some areas infiltrated by inflammatory mononuclear cells. COL1-3/4C staining in chronic periodontitis was more intense and extensive (6.3 ± 1.2%) than that of controls (1.6 ± 0.7%, unpaired student t-test, p < 0.01).
Interleukin-1 (IL-1 ), tumor necrosis factor (TNF- ), IL-6, platelet-derived growth factor (PDGF-A), and transforming growth factor- (TGF- ) were studied as

10
potential components of an osteoclast-stimulating cytokine network by immunohistochemical staining. Many of the macrophage-like cells in perivascular infiltrates in chronic periodontitis and peri-implantitis contained IL-1 , TNF- , IL-6, PDGF-A, and TGF- . In addition, all foreign body giant cells, found only in peri-implantitis tissues, contained these cytokines. Basal cells of epithelium and fibroblast-like cells contained IL-1 , TNF- , IL-6, PDGF-A, and TGF- . The cytokine-staining-intensity in epithelium was most conspicuous in chronic periodontitis, followed by peri-implantitis, and healthy controls, ranked in that order. All cells containing cytokines were included in the morphometric calculations. The percentage of TNF- ,IL-1 , and IL-6 immunoreactive cells was relatively high in peri-implantitis and chronic periodontitis (p < 0.05).
It can thus be concluded that collagenase-2 and -3 and gelatinase-B are associated with peri-implant bone loss. Host collagenases produced by the sulcular and junctional epithelium, fibroblasts, and monocytes/macrophages are able to cleave across the triple helical collagen fibrils in gingival tissue in chronic periodontitis. The low expression of cellular fibronectin synthesis in chronic periodontitis could be due to its degradation by human neutrophil elastase. The fact that cFN expression was relatively high in peri-implantitis suggests that the processes associated with loosening of natural teeth and dental implants differ. The osteoclast-activity cytokines produced in the supporting soft tissues probably stimulate osteoclasts, leading to the alveolar bone loss in a paracrine manner. Therefore, these proteinases and cytokines may conduct extracellular matrix destruction in peri-implant support tissues during loosening of dental implants. Monitoring the progression of loosening will be helpful in its prevention and treatment.
11
4. INTRODUCTION Introduction of the concept of osseointegration in the 1950’s remarkably improved dental implants. They can serve to replace teeth missing or lost for various reasons such as congenital anodontia, traumatic loss of teeth, cancer, root caries, and chronic periodontitis (Gassner et al., 2000; Gurlek et al., 1998; McMillan et al., 1998). They are very useful in the restoration of tooth function and aesthetics (Adell et al., 1985).
Many clinical dental implant systems have been developed. Dental implants can be used as the sole form of therapy or can function together with other dental treatment methods (Callan et al., 2000). When good-quality dental implants and techniques are used, implants show similar cumulative success rates at 10 years after implantation. The 10-year cumulative success rates are about 88% for maxillary and 93% for mandibular implants (O'Roark, 1997), but some implants are lost as a result of primary failure or by loosening, a mode of failure resulting from implant movement or migration in the bone (Franz, 1997). Unfortunately, these patients, who are mostly about 60 years old, are still quite young in terms of current human longevity (Pihakari et al., 1999). As a result of failure or loosening of the implants and the longevity of the patients, some patients would later need to be re-implanted. But often the possibilities for revision operations are limited, due to general and local circumstances (Oikarinen et al., 1995). The high and increasing number of dental implantations performed (Kronstrom et al., 2002) is evidence that loosening of dental implants is a common complication affecting thousands of patients annually worldwide.
Many important risk factors contribute to this loosening, such as non-ideal implantation techniques, oral bacterial pathogens (el Askary et al., 1999; Leonhardt etal., 1999), bio-mechanical overload (Tonetti and Schmid, 1994), and use of non-completely biocompatible implants (Gross, 1988). Biocompatibility refers to the tissue friendliness of the implant or compatibility of a material (Franz, 1997). Most CE-labeled and FDA-approved dental implants are nowadays very biocompatible in the human body and provide good success rates. Not only are such mainstream dental implants used, but also low quality implants, still widely used worldwide, initiate adverse host tissue responses and contribute to premature failure and loosening (Santavirta et al., 1999). The most prominent pathological feature of the loosening of dental implants is a progressive loss of peri-implant support tissues (Schwartz et al., 1997; Esposito et al., 1998b), to which many proteinases as well as osteoclast-mediated bone resorption are related in the process called peri-implantitis (Ingman etal., 1994; Teronen et al., 1997; van der Zee et al., 1997; Klinger et al., 1998).
The focus of this thesis is on the relationship between the extracellular matrix providing peri-implant tissue support and the tissue-destructive proteinases and osteoclast active cytokines. It is important to understand adverse host responses induced by non-ideal and non-compatible implant materials, because this may help to improve diagnosis, prevention, and treatment of implant loosening to the benefit of thousands of implant patients in the future.
12
5. REVIEW OF THE LITERATURE
1. OSSEOINTEGRATIONThe dream of using dental implants can be traced back to ancient times. A tooth-shaped iron implant has been reported in a 2000-year-old human skull (Crubezy et al., 1998). Shells and ivory have been tried as dental implants in the past. Unfortunately, there were no great breakthroughs in implant materials and implantation methods until 1952.
That year Professor Per-Ingvar Brånemark found that a titanium implant bonds to living bone. He called the phenomenon osseointegration, which means that the titanium implant is structurally integrated into living bone with a very high degree of predictability without inflammation in soft and interface tissues or fixture rejection (Brånemark et al., 1977). After that finding, most innovations have dealt with implant-coating materials, and implants having hydroxyapatite, ceramic, and endopore surfaces were introduced (Lacefield, 1988; Albert and Bergeron, 1998). Diamond-coated implants developed in Finland are undergoing pre-clinical research (Aspenberg et al., 1996; Santavirta et al., 1999; Santavirta, 2003). The concept of osseointegration has thus significantly broadened from its original sense to its definition as a direct structural and functional connection between living alveolar bone and the dental implant as a load-carrier (Stanford and Keller, 1991).
Currently, about 70% of Norwegian residents are aware of dental implants (Berge, 2000), and 51% of the Swedes would like to have dental implants (Palmqvist et al., 1991). On the other hand, in European countries 20% of dentists offer implant services (Millennium Research Group, 2002). Dental implants are quite expensive compared to some other conventional dental treatments: One dental implant costs about $1,250 in the USA (Davidoff, 2002). Implant cost-effectiveness should still be improved (Lewis, 1998). Nowadays, 4.8% of people in Sweden and 2.5% of people in Denmark who are from 45 to 69 years old have dental implants (Kronstrom et al., 2002). Therefore, the discovery of osseointegration was such a milestone in dental implantology. Below a short description is provided of those conditions which can be treated with dental implants.
2. END-STAGE LOSS OF TOOTH/TEETH2.1 Congenital anodontia. Congenital anodontia is a genetic disease characterized by partial or complete absence of the primary or permanent teeth. Hereditary anodontia may occur in the whole maxilla and mandibula or in both. It is referred to as complete anodontia. In non-hereditary anodontia, one usually loses one tooth or several teeth (Yanagida and Mori, 1990). This is called partial anodontia or hypodontia, a subdivision of anodontia. Implants can be applied to support prostheses in both cases in children and adults (McMillan et al., 1998).
13
2.2 Trauma. Traumatic loss of a tooth or teeth usually involves the central incisors. This occurs usually in sports, such as skiing, boxing or motor sports (Borgogna et al.,1984; Gassner et al., 2000; Levine et al., 2001). A car accident is also a common cause (Huelke and Sherman, 1973). Trauma victims are usually young with high quality alveolar bone, and an implant prosthesis is the best way to restore the missing tooth or teeth (Sclaroff et al., 2000). It has been calculated that about 5.6% of dental implants in Finland are performed in patients younger than 20 years old (Pihakari etal., 1999). For some traumatic root fractures, immediate implantation is useful, means that the implant is placed immediately after the tooth has been lost, without any delay (Hernandez and Balshi, 1998; Touati and Guez, 2002). Implants are also helpful in war-injured patients (Motamedi et al., 1999).
2.3 Cancer. Nearly 30,000 new head and neck cancer cases were detected in the USA in 1991, with surgical operations probably the first-choice treatment in most of those cases (Caplan and Weintraub, 1993). Damage to mandibular or maxillary bone can often not be avoided, so facial reconstructions and occlusal restorations are required, with dental implants often the best mode of treatment (Gurlek et al., 1998; Ueda et al., 1999; Kovacs et al., 2000).
2.4 Root caries and periodontitis. Nowadays people are living longer than ever before (Guyer et al., 2000). It has been estimated that in the USA over 40% of people over 65 years old are edentulous (Caplan and Weintraub, 1993). A similar survey showed that in the UK 37.6% of those more than 70 years old are edentulous (Douglass et al., 1993). About 0.05% of the Finns become edentulous every year (Takala et al., 1994). Edentulousness has several causes: 70% of the cases are explained by root caries and a further 20% by periodontal diseases (Takala et al., 1994). One similar study has shown that in the USA, 22.5% of the population suffers from root caries (Winn et al., 1996). In Europe, about 20% to 30% of the population suffers from periodontal diseases (Reich, 2001). Utilization of dental implants, which significantly improve mastication and speech, improves the condition of both edentulous and root caries patients (Mangano and Bartolucci, 2001).
To summarize, dental implants efficiently restore both the function and the aesthetics of the teeth in many conditions associated with missing or lost teeth, when used as the only modality of treatment or together with other conventional dental techniques (Searson and Meredith, 1997). Because dental implants must meet different types of demands, multiple kinds of dental implant systems have been designed.
3. DENTAL IMPLANT CATEGORIES 3.1 Implant categories and their indications for use. Dental implants are classified into four groups according to the method used for their fixation to host structures. These categories are endosseous, ramus frame, subperiosteal, and transosteal implants. Endosseous implants are further divided into root (cylindrical) and blade (plate) implants (Dental implants, NIH Consensus Statement, 1988) (Table 1). Endosseous
14
implants form the most widely used implant group. The quantity and quality of alveolar bone is the most important determinant for the outcome of dental implants including their success rates (life in service).
Table 1: Dental implant types and indications for their use
Implant type Alveolar bone Maxilla Mandibular Partially edentulous
Completely edentulous
Endosseous adequate bone (width and height)
Ramus frame enough anterior bone
Subperiosteal, complete, unilateral, circumferential
adequate bone (width and height)
Transosteal, staple, single pin, multiple pin
adequate anterior bone
means that implantation can be performed at this site.
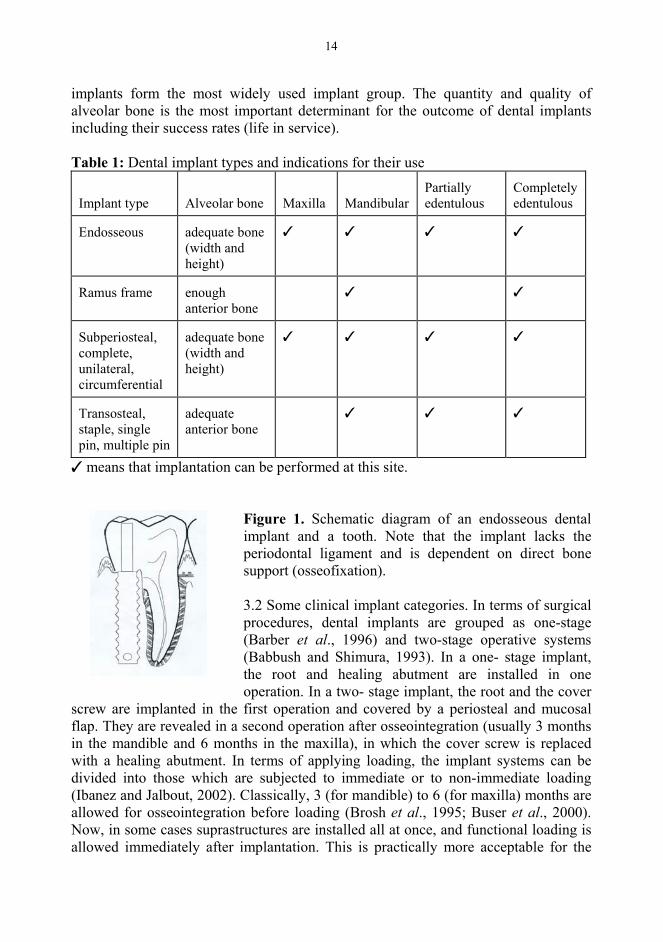
Figure 1. Schematic diagram of an endosseous dental implant and a tooth. Note that the implant lacks the periodontal ligament and is dependent on direct bone support (osseofixation).
3.2 Some clinical implant categories. In terms of surgical procedures, dental implants are grouped as one-stage (Barber et al., 1996) and two-stage operative systems (Babbush and Shimura, 1993). In a one- stage implant, the root and healing abutment are installed in one operation. In a two- stage implant, the root and the cover
screw are implanted in the first operation and covered by a periosteal and mucosal flap. They are revealed in a second operation after osseointegration (usually 3 months in the mandible and 6 months in the maxilla), in which the cover screw is replaced with a healing abutment. In terms of applying loading, the implant systems can be divided into those which are subjected to immediate or to non-immediate loading (Ibanez and Jalbout, 2002). Classically, 3 (for mandible) to 6 (for maxilla) months are allowed for osseointegration before loading (Brosh et al., 1995; Buser et al., 2000). Now, in some cases suprastructures are installed all at once, and functional loading is allowed immediately after implantation. This is practically more acceptable for the
15
patients than a 3-6 month long waiting period (Ericsson and Nilner, 2002). All theses implant technologies are widely used in clinics and affect implant success rates (Callan et al., 2000).
4. DENTAL IMPLANT SUCCESS ANALYSIS4.1 Implant success criteria. Criteria are required for the definition of implant success vs loosening or failure. This is important in evaluation of scientific implant biomaterials and comparison of clinical investigation of multiple implant systems. In 1978, the first success criteria were suggested by the US National Institutes of Health. They includes “1) bone loss no greater than one-third of the vertical height of the implant; 2) good occlusal balance and vertical dimension; 3) gingival inflammation amenable to treatment; 4) mobility of less than 1 mm in any direction; 5) absence of symptoms and infection; 6) absence of damage to adjacent teeth; 7) absence of parathesia or anesthesia or violation of the mandibular canal, maxillary sinus or floor of the nasal passage; 8) healthy collagenous tissue without polymorphonuclear infiltration; 9) provision of functional service for five years in 75% of the cases” (Dental Implants, NIH Consensus Statement, 1978). Unfortunately, the criteria could not be met by many dental implants at that time.
In 1986, modified criteria were suggested by Albrektsson and co-authors: “1) implants are clinically immobile; 2) a radiograph not demonstrating any evidence of peri-implant radiolucency; 3) vertical bone loss less than 0.2 mm annually following the implant’s first year of service; 4) individual implant performance to be characterized by an absence of persistent and irreversible signs and symptoms such as pain, infections, neuropathies, paresthesia, or violation of the mandibular canal; 5) success rate of 85% at the end of a five-year observation period and 80% at the end of a ten-year period to be the minimum criterion for success” (Albrektsson et al., 1986). These are practical and easy to use in assessment of dental implants.
More recently, criteria for implants were approved by The American Academy of Periodontology in 2000 (Iacono, 2000). These include: “1) absence of persistent signs/symptoms such as pain, infection, neuropathies, parathesias, and violation of vital structures; 2) implant immobility; 3) no continuous peri-implant radiolucency; 4) negligible progressive bone loss (less than 0.2 mm annually) after physiologic remodeling during the first year of function; 5) patient/dentist satisfaction with the implant-supported restoration” (Iacono, 2000). These are clear and concise criteria.
4.2 Cumulative success rates. Implant cumulative success rates are usually evaluated in years categorized as less than 5 years (short run), from 5 to 10 years (intermediate run), and greater than 10 years (long run) (Smith and Zarb, 1989). Cumulative success rates of dental implants are affected by many factors. These include implant location in the upper or lower jaw and its position in the dental arch, implant type, diameter and length, prosthetic construction, and whether they are used for single tooth replacement or in an edentulous month (O'Roark, 1991). Cumulative success rates of

16
dental implants have been tabulated according to life in service, mandibular or maxillary location, and use as a single replacement or in an edentulous month (Table 2).
Table 2: Cumulative success rates for dental implants
General Mandible Maxilla Single1 Edentulous
5 years 95.4%2 98.2%3 97.3%3 98.3%4 93.9%5
5-10 years 92.2%2 93%6 88%6 97.4%7 88.3%8
> 10 years 87%9 91%10 81%10 89%11 no reported 1Single = Single implant prostheses; 2Brocard et al., 2000; 3Buser et al., 1997; 4Buser et al., 2002; 5Higuchi et al., 1995; 6O'Roark, 1997; 7Priest, 1999; 8Zarb and Schmitt, 1991; 9Keller et al., 1999; 10Adell et al., 1985; 11Walther et al., 1996.
It can be concluded that, due to their high success rates, dental implants constitute a remarkable improvement in modern dentistry. At the end of 10 years in service, a similar cumulative success rate has been found for different dental implants in a 3000-implant study; Rates were 88% for maxillary and 93% for mandibular implants, which covered a 25-year observation period (O'Roark, 1997). It has been calculated that in Finland about 52 to 55% of a total of 17,785 dental implants have been performed in patients whose mean age is 49.5 years (range, 40 to 59) (Pihakari et al., 1999). Thus, many patients will be about 60 years or older when their implants fail more than 10 years after implantation. Among these failure patients, some require revision operations. In other patients, general and local contra-indications may restrict the possibilities for re-implantation (Oikarinen et al., 1995). It would therefore be beneficial if dental implants would last for a lifetime.
A huge number of dental implantations have been performed worldwide. The Brånemark osseointegration implant system has been used more than 600,000 times during the last 30 years (Clapp et al., 1996). In the USA alone, it has been estimated that more than 300,000 dental implants are performed annually (Parker and Miller, 1989; Klinger et al., 1998). According to a recent report, those actually implanted in the USA in 2000 numbered 910,000 (Annual Industry Report, 2000). The number of patients who suffer from failures would therefore be high, although implant failure rates are quite low. The main symptom of loosening is a gradually increasing mobility associated with pain, especially when masticating (Buchs et al., 1996).
Unfortunately, there are no reliable surveys reporting how many dental implants will be required in the future. The revenue of the European dental implant market by 2006 has been predicted to reach $269.8 million (Millennium Research Group, 2002). The compound annual growth rate of the Japanese dental implant market from 2002 to 2006 has been estimated to be 9.4% (The Japanese market for dental implants, 2002).
17
Because of the growing demand for dental implants, their failure is becoming one of the most challenging dental complications of our times (Duyck and Naert, 1998; Esposito et al., 1998; el Askary et al., 1999).
The first nine implantations performed by a novice dentist have been reported to fail (Lambert et al., 1997). Failure rates even as high as 38.5% for some dentists were reported a decade ago (Owall et al., 1992). However, with improvements in dental implantation skills and equipment, it is possible to diminish the failure rates in the future.
5. FAILURE OF DENTAL IMPLANTS5.1 Failure types. Failure is a condition or instance of not functioning or not functioning adequately (Koenisberger, 1998). In 1978, the NIH recommended the following criteria for removal of a dental implant: “1) chronic pain; 2) significant movement; 3) infection; 4) significant progressive loss of supportive bone; 5) intolerable dysthesia (anesthesia or parasthesia); 6) oro-antral or oro-nasal fistulae; 7) bone fracture; 8) psychological or other significant medical problems; 9) uncorrectable implant breakdown; 10) possible irreversible damage to adjacent teeth; 11) cosmetic problems” (Dental Implants, NIH Consensus Statement, 1978). Generally, early- and late-stage failures can be distinguished in terms of osseointegration.
5.1.1 Early-stage failure. Early-stage failure refers to a failure to establish osseointegration before loading; the failure rate was about 3.6% in a 16,935-implant study (Esposito et al., 1998a), in which the main reasons were suggested to be surgical trauma leading to impaired wound healing, premature loading, and infection (Esposito et al., 1998).
5.1.2 Late-stage failure. Late-stage failure is defined as a failure to maintain the achieved osseointegration after loading (Esposito et al., 1998). From the point of view of loading time and mechanism, late-stage failure can further be divided into mechanical and biological late-stage failure.
5.1.2.1 Mechanical late-stage failure. Mechanical late-stage failure rates are high within the first 4 months (120 days), that is, during the early post-implantation period (Tonetti, 1998). They comprise implant fractures, abutment screw fracture, and mechanical retention problems of over-denture (Goodacre et al., 1999). Implant fractures usually involve the framework, veneering material, and opposing prosthesis. The mechanical failure rate has been calculated to be about 1.4% (Brocard et al.,2000). The two-stage external hex screw-type implants have been reported to fail at a rate of about 8.7% (Schwarz, 2000). Mechanical complications have shown a tendency to decline (Eckert et al., 2000).
18
5.1.2.2 Biological late-stage failure (loosening). The main reasons for loosening are chronic infection (implant plaque) and overload, together with host characteristics which result in adverse tissue responses (Esposito et al., 1998; Santavirta et al., 1999). Loosening is a result of marginal infection and bio-mechanical overload or a combination of these two factors (Tonetti and Schmid, 1994). Some of the late-stage loosening is caused by metal fatigue fractures (Hoyer et al., 2001).
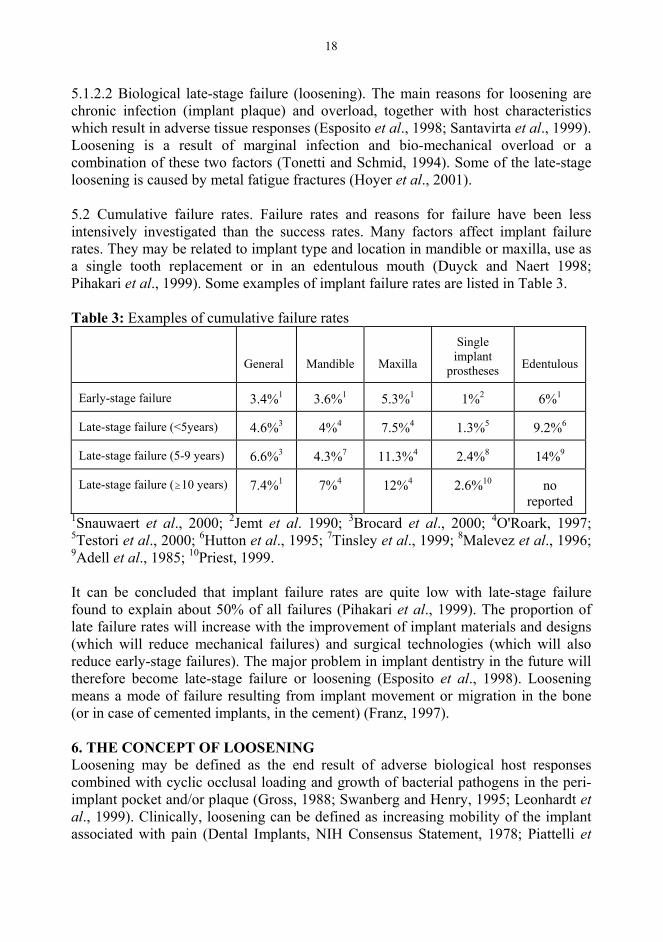
5.2 Cumulative failure rates. Failure rates and reasons for failure have been less intensively investigated than the success rates. Many factors affect implant failure rates. They may be related to implant type and location in mandible or maxilla, use as a single tooth replacement or in an edentulous mouth (Duyck and Naert 1998; Pihakari et al., 1999). Some examples of implant failure rates are listed in Table 3.
Table 3: Examples of cumulative failure rates
General Mandible Maxilla
Single implant
prostheses Edentulous
Early-stage failure 3.4%1 3.6%1 5.3%1 1%2 6%1
Late-stage failure (<5years) 4.6%3 4%4 7.5%4 1.3%5 9.2%6
Late-stage failure (5-9 years) 6.6%3 4.3%7 11.3%4 2.4%8 14%9
Late-stage failure ( 10 years) 7.4%1 7%4 12%4 2.6%10 no reported
1Snauwaert et al., 2000; 2Jemt et al. 1990; 3Brocard et al., 2000; 4O'Roark, 1997; 5Testori et al., 2000; 6Hutton et al., 1995; 7Tinsley et al., 1999; 8Malevez et al., 1996; 9Adell et al., 1985; 10Priest, 1999.
It can be concluded that implant failure rates are quite low with late-stage failure found to explain about 50% of all failures (Pihakari et al., 1999). The proportion of late failure rates will increase with the improvement of implant materials and designs (which will reduce mechanical failures) and surgical technologies (which will also reduce early-stage failures). The major problem in implant dentistry in the future will therefore become late-stage failure or loosening (Esposito et al., 1998). Loosening means a mode of failure resulting from implant movement or migration in the bone (or in case of cemented implants, in the cement) (Franz, 1997).
6. THE CONCEPT OF LOOSENINGLoosening may be defined as the end result of adverse biological host responses combined with cyclic occlusal loading and growth of bacterial pathogens in the peri-implant pocket and/or plaque (Gross, 1988; Swanberg and Henry, 1995; Leonhardt et al., 1999). Clinically, loosening can be defined as increasing mobility of the implant associated with pain (Dental Implants, NIH Consensus Statement, 1978; Piattelli et
19
al., 1998a). Radiologically, loosening is characterized by loss of peri-implant crestal bone (Engquist et al., 1988).
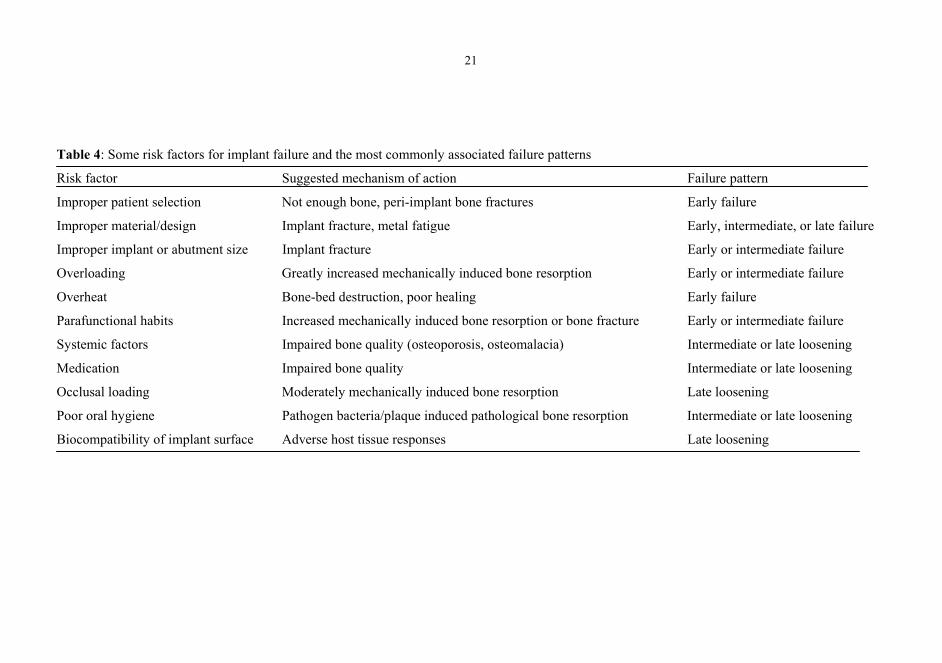
7. WHY DO DENTAL IMPLANTS LOOSEN/ FAIL?This is a very complicated question, which needs to be clarified in the future. Of the many risk factors found to affect the failure process directly or indirectly (Duyck and Naert, 1998; Esposito et al., 1998; el Askary et al., 1999), some are listed in Table 4, and their associations with various loosening patterns. These risk factors can be grouped into three categories, namely dentist-, implant-, and host-related risk factors.
7.1 Dentist-related risk factors7.1.1 Preoperative factors. Clinical radiographic techniques are routinely used before implant dentistry is planned (Verhoeven and Cune, 2000). Radiographs are used to check the quantity and quality of the implant bone beds and their relation to surrounding structures such as the mandibular canal and maxillary sinus (Dula et al.,2001). Methods used include periapical X-rays, the panoramic X-ray, computed tomography, and magnetic resonance imaging (Butterfield et al., 1997). It has been reported that intraoral X-rays are associated with an approximately 14% magnification (Lazzerini et al., 1996), and panoramic images have been increased approximately 25% in size (Reddy et al., 1994). X-ray magnifications may thus lead to mistakes in planning and in performance of dental implantations, making special methods necessary to correct for eventual magnification which will enable recording of exact anatomical measurements.
7.1.2 Peroperative factors. Overheat which is produced by friction from high torque equipment damages the implant bone bed and contributes to early-stage failure of implants (Piattelli et al., 1998b). About 3.6% of implant failures have been estimated to be related to surgical trauma (Esposito et al., 1998). Secondly, a nonideal position for the dental implant may subject it to non-axial loading during mastication. This increases risk for implant fractures and peri-implant bone fractures, which usually occurs in the posterior region that is subjected to a high load, in particular if the patient has comparatively low bone density in this region (Kerstein, 2001). Hollow implants lead to increased implant fracture rates if the implant is too small in diameter. This usually happens with the use of two-stage external hex screw-type implant systems (Piattelli et al., 1998c). Selection of too-short implants may also increase the failure rate.
7.1.3 Postoperative factors. Improper design and guidance of the crown contribute to failure. Too high a cusp or too high an occlusal alignment can increase occlusal loading to an unacceptable level (Reitz, 1994; Gittelson, 2002). The crown can also contribute to too-wide contact between the counter tooth and the implant, which leads to high occlusal load of the implant in bone. Occlusal forces contribute to implant fractures and peri-implant bone fractures. Crown width, cusp height, guidance, and occlusal alignment can all be used to control occlusal forces (Weinberg et al., 1988).
20
Currently, a T-scan occlusal analysis system provides one option to assess occlusal forces (Chapman and Kirsch, 1990). The T-Scan system is a computerized dental device which can quantitatively analyze occlusal contacts (position, strength, and frequency of occlusal contacts).
Ideally, occlusal loading should be distributed to peri-implant bone though the long axis of the implant. The more the lateral loading and non-axial forces can be reduced, the better (Kaukinen et al., 1996; Reitz, 1994). If this does not succeed, occlusal loading will be focused on the abutment neck area of the peri-implant bone. This has been confirmed by use of finite element analysis for biomechanical modeling (O'Mahony et al., 2000). Excessive loading leads to multiple complications, which can lead to loosening of the implant or to implant abutment fractures. In terms of implant bone bed, it may lead to bone microfractures and marginal or periapical bone loss (Piattelli et al., 1998b). Therefore, improper implant restoration may lead to implant failure, but peri-implant bone loss can be associated even with properly fixed implants, which will be discussed in biological occlusal loading (7.3.1.1).
In short, any improper decision increases the risk of failure. As a result of the development of clinical implantology in the past half century, these kinds of failures are relatively few now and will become even less frequent in the future (Albrektsson, 2001). From the viewpoint of prevention, however, clinical dentists should pay close attention to all steps during implant treatments.
7.2 Implant material-related risk factors7.2.1 Dental implant material characteristics. The ideal dental implant material should be “1) biocompatible (Santavirta et al., 1991; Edgerton and Levine, 1993), 2) of appropriate rigidity for prosthetic function, 3) intimately adaptable to both bone and gingiva surrounding the implant, 4) functionally able to dissipate forces resulting from occlusal load on the prostheses supported by the implant to the underlying bone, 5) resistant to the large and diverse peri-implant microbial load” (LeGeros and Craig, 1993).
In fact, none of the dental implants meets all these characteristics. Biocompatibility, one of the most important factors, means the ability of the implant to elicit an appropriate host response in its specific application (Edgerton and Levine, 1993). Use of bioincompatible implant materials leads to implant failure initiated by adverse host tissue responses (Santavirta et al., 1999). Multiple coating technologies have been developed to improve implant biocompatibility at the host-implant interfaces (Aspenberg et al., 1996). These coatings comprise titanium oxide (TiO2) coating, ceramic coating, or diamond coating (Aspenberg et al., 1996; Santavirta, 2003). Biodegradable ceramic coating may have the best future prospects.
Most dental implant materials presently used in clinics are quite biocompatible in human tissues in their specific dental application. They are usually made of titanium,
21
Table 4: Some risk factors for implant failure and the most commonly associated failure patterns
Risk factor Suggested mechanism of action Failure pattern
Improper patient selection Not enough bone, peri-implant bone fractures Early failure
Improper material/design Implant fracture, metal fatigue Early, intermediate, or late failure
Improper implant or abutment size Implant fracture Early or intermediate failure
Overloading Greatly increased mechanically induced bone resorption Early or intermediate failure
Overheat Bone-bed destruction, poor healing Early failure
Parafunctional habits Increased mechanically induced bone resorption or bone fracture Early or intermediate failure
Systemic factors Impaired bone quality (osteoporosis, osteomalacia) Intermediate or late loosening
Medication Impaired bone quality Intermediate or late loosening
Occlusal loading Moderately mechanically induced bone resorption Late loosening
Poor oral hygiene Pathogen bacteria/plaque induced pathological bone resorption Intermediate or late loosening
Biocompatibility of implant surface Adverse host tissue responses Late loosening
22
titanium-aluminum-vanadium (Ti-6Al-4V), cobalt-chromium-molybdenum and more rarely of other alloys (Lacefield, 1988). Their use is evidence-based and supported by their good success rates (Adell et al., 1981).
7.2.2. Implant surface. The dental implant surface can be separated into the collar area and non-collar area. Smooth surfaces are favored for collar areas to reduce bacteria adhesion and to reduce subsequent peri-implantitis. In contrast, a smooth surface reduces the degree of osseointegration of the non-collar (root) area (Wiskott et al., 1999), whereas rough or porous implant surfaces improve osseointegration (Lumbikanonda et al., 2001). Rough surfaces also enhance osteoblast adhesion (Noth et al., 1999). Unfortunately, these requirements are in conflict with each other at the transition of the root to collar area. This conflict cannot yet be completely solved, which means that the risk for failure of dental implants will rise.
3) Interface tissue. There are three kinds of connections between dental implants and host bone (Craig and LeGeros, 1999). 1) The direct bone and implant connection, which is called osseointegration (Brånemark et al., 1977), 2) Fibro-osseous integration, which is mediated by an intervening fibrous tissue layer approximately 100 micrometers thick (Weiss, 1986; Ko et al., 1992; Piattelli et al., 1998a), 3) Periodontal connective tissue-like attachment which is found, it seems, very rarely, and refers to the periodontal ligament-like organization of peri-implant collagen fibers (Takata et al., 1993; Choi, 2000) or to cementum formation on endosseous dental implants in some cases (Guarnieri et al., 2002).
Fibro-osseous integration, indicating the presence of a thin fibrous interface tissue, is the most frequently seen mode of attachment among these three different types of connections. Interface tissue is a result of implant wound healing, with multiple components of the extracellular matrix identified in this fibrous interface tissue (Table 3). Type I and III collagens in the interface tissue reflect the stability of the implant capsule (von Recum et al., 1993). Cellular fibronectin has been found and probably plays a role in the direct attachment of the fibrous interface to the implant surface (Bagambisa et al., 1994).
In summary, dental implant materials have been remarkably improved in the past half century to meet all kinds of demands. However, research and development are needed to develop even more biocompatible and functional materials to prevent implant failures and to prolong implant life in service.
7.3 Host-related factors. Dental implants are located in the oral cavity, peri-implant soft tissues, and host bone, which means that microbes and host-related factors affect the outcome. Host-related factors can be divided into local and systemic risk (prognostic) factors. As we studied proteolytic enzymes as markers and mediators of biological late-stage loosening, they are in the main issue of this review of host-related factors of significance for implant success.
23
7.3.1. Local risk factors7.3.1.1 Biomechanical occlusal loading. Even well-performed and optimally occlusally restored dental implants tend to lead to peri-implant bone loss. In order to review this in more detail, dental implants will be compared with natural teeth.
Three functional hypotheses aim to explain how periodontal ligament tissue supports the tooth during high occlusal force. 1) Periodontal ligament tissue is a tensional support tissue (Mühlemann, 1967). Collagens, in particular the interstitial collagens type I and III, provide tensile strength in the human body and are the main collagens in the periodontal ligament (Persikov and Brodsky, 2002). About 10% of the collagen in the periodontal ligament is remodeled every day, which makes this site the most rapidly remodeling of all tissues in the human body (Laurent, 1987). This indicates that collagen in the periodontal ligament ages very rapidly under high occlusal loading, and means that the structural integrity of the periodontal collagen is compromised but maintained by high remodeling. 2) Periodontal ligament tissue forms a viscoelastic system, and the impact load of occlusal forces is balanced by a viscoelastic cushion effect. When squeezed under loading, the periodontal ligament slowly releases fluid into the tissues and blood and lymphatic vascular system, thus absorbing the energy of the impact (Picton and Wills, 1978). 3) The periodontal ligament is part of a stomatognathic complex, which is a stress feedback pathway (Lund, 1991). Masticatory muscles are controlled by sensory input which activates negative feedback to avoid excessive loading of one or several teeth (Linden and Millar, 1988). These three periodontal ligament functions can together effectively control even high occlusal load, which could not safely be distributed to the alveolar bone socket of the teeth. Tooth movements correlate with occlusal forces, although there occurs only a little tooth displacement even under a high load (Figure 2A).
Clearly, the interface tissue between the dental implant and its bone bed can hardly distribute the tension to peri-implant support tissue as effectively as does the periodontal ligament. The eventual function of the interface tissue as a viscoelastic shock-absorbing cushion has not been studied. Dental implants lack the stress receptors located in the tensional periodontal ligament tissue in natural teeth, and their stomatognathic sensor system is less sensitive than that of healthy teeth (Klineberg and Murray, 1999; Jacobs and van Steenberghe, 1991; Jacobs and van Steenberghe, 1993). Therefore, due to non-optimal load protection and force-absorbing and -distributing systems, a dental implant is subjected to implant micromotion ranging from 50 to 150 micrometers (Szmukler-Moncler et al., 1998). Implant micromotions are defined as recoverable displacements of the implant that occur during a finite period of loading. Horizontal movement of the maxillary central incisor ranges between 0 and 200 m (Mühlemann, 1967), so the maximal micromotion of a dental implant is less than that of a natural tooth. It has been concluded that occlusal loading strains the hard peri-implant bone, because implants lack the protective periodontal ligament system. The relationship of displacement and implant loading continues to
24
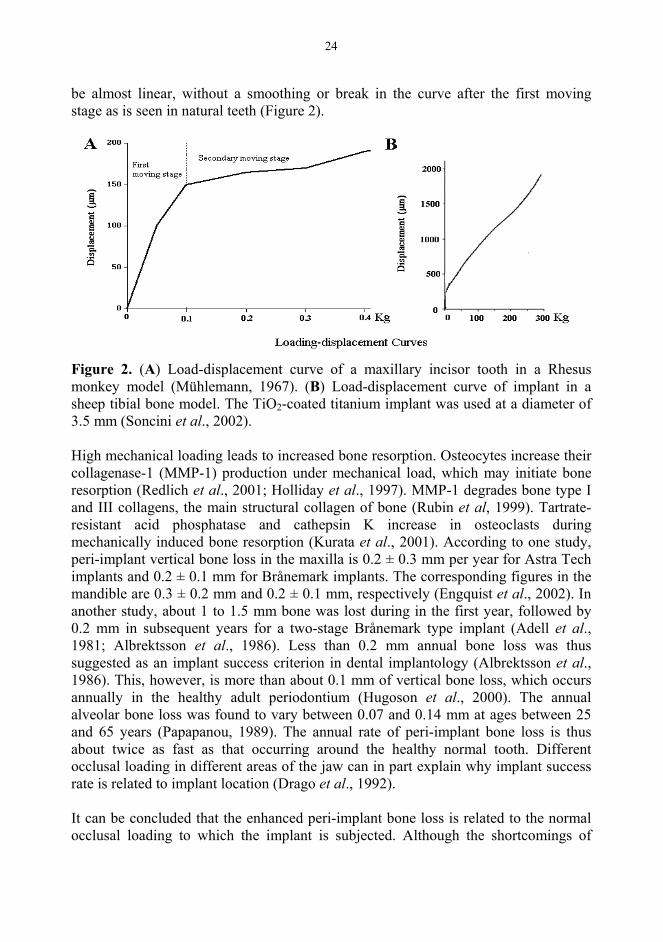
be almost linear, without a smoothing or break in the curve after the first moving stage as is seen in natural teeth (Figure 2).
Figure 2. (A) Load-displacement curve of a maxillary incisor tooth in a Rhesus monkey model (Mühlemann, 1967). (B) Load-displacement curve of implant in a sheep tibial bone model. The TiO2-coated titanium implant was used at a diameter of 3.5 mm (Soncini et al., 2002).
High mechanical loading leads to increased bone resorption. Osteocytes increase their collagenase-1 (MMP-1) production under mechanical load, which may initiate bone resorption (Redlich et al., 2001; Holliday et al., 1997). MMP-1 degrades bone type I and III collagens, the main structural collagen of bone (Rubin et al, 1999). Tartrate-resistant acid phosphatase and cathepsin K increase in osteoclasts during mechanically induced bone resorption (Kurata et al., 2001). According to one study, peri-implant vertical bone loss in the maxilla is 0.2 ± 0.3 mm per year for Astra Tech implants and 0.2 ± 0.1 mm for Brånemark implants. The corresponding figures in the mandible are 0.3 ± 0.2 mm and 0.2 ± 0.1 mm, respectively (Engquist et al., 2002). In another study, about 1 to 1.5 mm bone was lost during in the first year, followed by 0.2 mm in subsequent years for a two-stage Brånemark type implant (Adell et al., 1981; Albrektsson et al., 1986). Less than 0.2 mm annual bone loss was thus suggested as an implant success criterion in dental implantology (Albrektsson et al., 1986). This, however, is more than about 0.1 mm of vertical bone loss, which occurs annually in the healthy adult periodontium (Hugoson et al., 2000). The annual alveolar bone loss was found to vary between 0.07 and 0.14 mm at ages between 25 and 65 years (Papapanou, 1989). The annual rate of peri-implant bone loss is thus about twice as fast as that occurring around the healthy normal tooth. Different occlusal loading in different areas of the jaw can in part explain why implant success rate is related to implant location (Drago et al., 1992).
It can be concluded that the enhanced peri-implant bone loss is related to the normal occlusal loading to which the implant is subjected. Although the shortcomings of
25
dental implants in comparison to natural teeth may never be overcome, dental implants are still a good choice compared to some other conventional prosthetic treatments.
7.3.1.2 Peri-implantitis and clinical indices. Poor oral hygiene and a rough implant surface contribute to the formation of bacterial plaque (Figure 3). To improve implant longevity, a rough implant surface which increases plaque formation at the collar area should be avoided (Grossner-Schreiber et al., 2001). Micro-gaps between various implant components favor bacterial adhesion and colonization. They are usually located in the implant-transmucosal abutment interface, transmucosal abutment-prosthesis interface, and implant-prosthesis interface (O'Mahony et al., 2000a). Oral hygiene and professional implant maintenance are strongly recommended (Springstead et al., 1993).
More than 300 bacterial microorganisms have been discovered in the infected implant plaque. Porphyromonas gingivalis, Bacteroides forsythus, Fusobacterium nucleatum,Campylobacter gracilis, Streptococcus intermedius, and Peptostreptococcus microsare clearly related to peri-implantitis (Kalykakis et al., 1998; Leonhardt et al., 1999). Bacteria produce bacterial collagenases, which have been shown to cleave gingival collagen (Mailman, 1979; Harrington, 1996). Even more importantly, bacterial components may stimulate the peri-implant host cells to produce collagenases and osteoclast-activating cytokines. Osteoclasts resorb peri-implant bone and lead to vertical peri-implant bone loss.
Dental plaque with its bacteria is probably the main pathogenetic factor in chronic periodontitis and peri-implantitis (Watts, 1996). Pathogenic bacteria can induce resident host cells to produce or release proteinases or to both, which contributes to periodontal tissue destruction (Teronen et al., 1997). Pathogenic bacteria can increase proteinase levels by several mechanisms. Bacteria may be chemotactic, leading to leukocyte accumulation (Miller et al., 1975). Upon phagocytosis, polymorphonuclear leukocytes release MMPs and other hydrolytic enzymes (Ding et al., 1997). Bacterial membrane components can induce polymorphonuclear leukocytes to produce MMPs (Ding et al., 1996). Bacterial proteinases can convert proMMPs into their active counterparts, which may be a rate-limiting step during tissue degradation (Okamoto etal., 1997; Sorsa et al., 1992).
Chronic periodontitis is an inflammatory process characterized by increased pocket probing depth, bleeding on probing, and increasing tooth mobility (O'Reilly and Claffey, 1996). Many clinical indices have been introduced in order to grade the degree of inflammation in periodontitis. These include plaque index (Silness and Loë, 1964), periodontal index (Russell, 1967), periodontal disease index (Ramfjord, 1967), and gingival index (Löe, 1967).
26
Peri-implant gingival mucosa around dental implants is composed of keratinized oral epithelium covering a connective tissue matrix. Its molecular composition, including collagen, cells, and vascular structures, is almost identical to that of healthy tooth gingival mucosa. However, the thickness of the entire gingival soft tissue and of the keratin layer in peri-implant mucosa was found to be 34% and 50% thinner, respectively, than in healthy mucosa (Lindhe and Berglundh, 1998). As a result of these circumstances, all kinds of products from the oral cavity and peri-implant pocket easily penetrate the peri-implant mucosa. This may be the reason for the presence of very high numbers of inflammatory cells around loosened dental implants (Liljenberget al., 1996).
Peri-implantitis is also an inflammatory process which shares some of its features with chronic periodontitis (Meffert, 1996). Some of the periodontal indices have been modified to be applied in peri-implantitis in order to quantify the degree of inflammation (Mombelli et al., 1987). Modified gingival index and bleeding on probing, suggested as diagnostic markers of peri-implantitis, are also good markers for clinical follow-up of implant treatments (Mombelli et al., 1987; Luterbacher et al.,2000).
7.3.1.3 Cigarette smoking. In the USA in 1997, about 924 million packs of cigarettes were consumed by 12- to 17-year-old youth alone. Each day in the USA, the number of smokers of this age equals approximately 3.76 million (DiFranza and Librett, 1999). In Finland in 2000, nearly 0.34 million workers were subjected to environmental tobacco smoke at work, representing 16% of the employed population. Although smoking indoors is forbidden by Finnish law, 0.6 million Finns (1% of the population) were surprisingly found to suffer from indirect smoking at home (Kauppinen and Virtanen, 2002).
Nicotine, a major component of tobacco, inhibits collagen production by gingival fibroblasts and enhances collagen breakdown (Tipton et al., 1995). Nicotine is cytotoxic to periodontal ligament cells and inhibits their growth (Alpar et al., 1998; James et al., 1999). It prevents differentiation of osteoblast-like cells to osteoblasts (Nociti et al., 2002) and reduces alveolar bone quality (Yuhara et al., 1999). Serum nicotine levels correlate with severity of periodontal attachment loss (Gonzalez et al., 1996). In a series of 12,329 periodontitis-affected patients in the USA, smoking was identified as a risk factor in more than 50% (Tomar and Asma, 2000; Wallace, 2000). Smoking has also been linked to the loosening of dental implants (Schwartz-Arad et al., 2002).
7.3.1.4 Para-functional habits, bruxism. Para-functional habits and bruxism are very common occlusal diseases. Heavy occlusal forces constitute a risk factor for loosening of dental implants. Metal fatigue and implant fractures occur more frequently in these patients than in controls. More than 77% of all implant fractures have been reported to occur in patients who have signs and a history of chronic bruxism (Rangert, 1994).
27
Para-functional habits are related to increased peri-implant bone loss (Engel et al., 2001). Attention should be paid to para-functional habits when decisions on dental implantation are made (Misch, 2002).
7.3.2 Systemic factors. Systemic factors affect both the quality and quantity of bone, which constitute important prognostic factors for dental implant survival. These systemic factors comprise poorly controlled diabetes, osteoporosis, osteomalacia, irradiation, and medications (Roberts et al, 1992).
7.3.2.1 Diabetes mellitus. Diabetes mellitus, a common disease, was in the USA in 1998 the fifth most common disease leading to death (Guyer et al., 2000). The incidence rate of diabetes mellitus in Finland during 1989-1994 was 0.402/1000 annually, which is high compared to the average normal rate (0.032/1000) (Patterson et al., 2001). About 10% of all Canadians are currently found to suffer from diabetes, which is a risk factor for periodontal diseases (Matthews et al., 2002).
Diabetic lesions involve bone, gingival, and vascular tissues (Johnson, 1992). This disease is thought to suppress collagen synthesis (Schneir et al., 1979; Spanheimer etal., 1988), and it increases the expression of MMPs. The levels of MMP-8 and MMM-9 activities in saliva correlate with clinical periodontal findings such as gingival bleeding and pocket depth (Collin et al., 2000). MMP-8 and MMP-9 act cooperatively in degradation of type I collagen in gingival and bone tissues. These conclusions have been confirmed in a rat model (Golub et al., 1978). Although most studies of diabetic lesions have been focused on periodontitis, diabetes mellitus has also been considered a risk factor and occasionally even a contraindication for performing dental implantations. Recently, it has been reported that dental implants in diabetes are successful, at least in the short term (Olson et al., 2000).
7.3.3.2 Osteoporosis. Osteoporosis is a very common disease, with the number of elderly people affected only in Europe, Japan, and the USA being 75 million (South-Paul, 2001). Two million cases of bone fractures have been annually found in the USA to be associated with osteoporosis (Riggs et al., 1988).
The main pathological features of osteoporosis are low bone mass and a microarchitectural deterioration of bone leading to fragility, and thence to an increased fracture risk. The multiple pathogenic factors related to osteoporosis comprise genetic predisposition and subtle alterations in systemic and local hormones, together with environmental influences (Lazner et al., 1999). Currently research interest is focused on the role of cathepsin K in the degradation of bone matrix in osteoporosis (Lazner et al., 1999).
Both the maxilla and mandible can be affected by osteoporosis, which has been considered a risk factor for implant failures and periodontal diseases. The local bone quality of the implantation bed is a more sensitive prognostic factor in this respect
28
than that of peripheral bone in general in osteoporosis patients (Becker et al., 2000). Implants in osteoporosis have been successful in the short term, but long-term results have not been reported (Eder and Watzek, 1999).
7.3.3.3 Medication and irradiation therapy. Some medications widely used in clinics cause bone loss. In particular, glucocorticosteroids cause iatrogenic osteoporosis by increasing bone resorption via stimulation of osteoclastogenesis (Canalis and Delany, 2002).
Other drugs with deleterious effects on bone include chemotherapeutic agents such as doxorubicin and methotrexate, which inhibit osteoblasts and diminish bone formation (Friedlaender et al., 1984). Implants are often used in cancer-surgery patients. In oral cancer patients, however, tumor resection is usually combined with irradiation, which locally impairs bone quality and impairs the prognosis of dental implants in the long-term. In one study, irradiation had no effect on implant success rate in the short term (Jisander et al., 1997), whereas another study found implant survival to be lower (Visch et al., 2002).
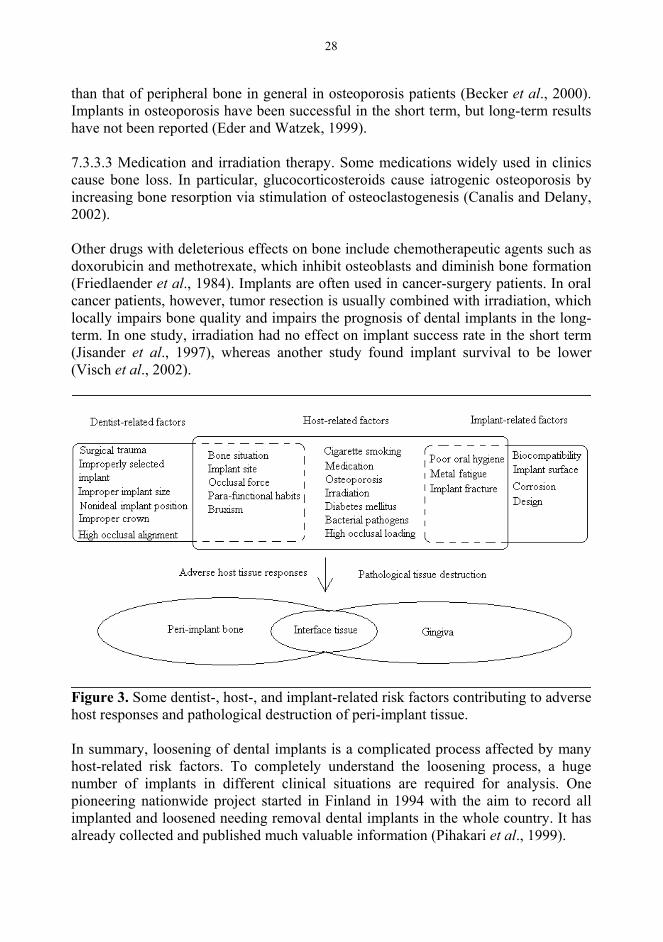
Figure 3. Some dentist-, host-, and implant-related risk factors contributing to adverse host responses and pathological destruction of peri-implant tissue.
In summary, loosening of dental implants is a complicated process affected by many host-related risk factors. To completely understand the loosening process, a huge number of implants in different clinical situations are required for analysis. One pioneering nationwide project started in Finland in 1994 with the aim to record all implanted and loosened needing removal dental implants in the whole country. It has already collected and published much valuable information (Pihakari et al., 1999).

29
Some of the risk factors overlap with each other and affect the loosening process independently or cooperatively (Figure 3). However, no matter the type of risk factor, they eventually contribute to peri-implant tissue destruction. The main pathological feature of loosening is a progressive loss of peri-implant support tissue as a result of adverse host tissue responses (Tonetti and Schmid, 1994; Duyck and Naert, 1998; Santavirta et al., 1999).
8. ADVERSE HOST RESPONSES DURING LOOSENING8.1 Host responses and their typesResponse is a basic concept in medicine, which means any organic process elicited by a stimulus (Koenisberger, 1998). Generally, host responses are grouped into inflammation, foreign body reactions, immunological and toxicological reactions, and tumorigenesis.
Two kinds of interactions exist between dental implants and their host tissues. Host tissues affect implant materials, which can for example become corroded (Voitik, 1996). On the other hand, implantation and implant materials induce various kinds of tissue reactions such as wound healing, inflammation, foreign-body reactions, and fibrosis (von Recum et al., 1993; Meffert, 1996; Konttinen et al., 2001). What type of tissue response is elicited is determined by the degree of biocompatibility of the implant material. Biocompatibility means the capability of a prosthesis implanted in the body to exist in harmony with tissue without causing deleterious changes such as fibrous capsule formation, wear, and infection (Koenisberger, 1998). The more biocompatible are the implant materials applied, the fewer adverse host tissue responses will follow.
Unfortunately, no completely biocompatible implant material has yet been found. Non-biocompatible materials have been considered to exert adverse effects in loosening of hip implants (Edgerton and Levine, 1993; Santavirta et al., 1999). Development of more biocompatible implants or coating materials is one of the main directions of current research. For example, diamond-coated implants have been developed for joint replacement and dental implantology in Finland (Aspenberg et al.,1996; Santavirta et al., 1999).
Special attention was in this study paid to host tissue responses, which induce a rise in various proteinases and osteoclast-activating cytokines, leading to destruction of extracellular matrix (collagen, cellular fibronectin, and bone) in the peri-implant support tissue. Knowledge of the relationship between implants and host tissue responses may lead to the development of future diagnostic markers. Their use may allow us to monitor the progression of loosening, which will be helpful in its prevention and treatment.
8.2 Extracellular matrix
30
8.2.1 Collagens. Collagens are the most abundant extracellular proteins in man, with 20 different types of collagens identified (Persikov and Brodsky, 2002). Collagens are composed of hundreds of amino acids, and glycine is located at every repeating Gly-X-Y triplet amino acid sequence. These amino acid triplets form a single chain, which is the smallest structural unit of collagen. Three -chains form a triple helical collagen monomer. These collagen monomers align into a nearly three-quarter-overlapping collagen fiber, which is stabilized through intermolecular cross-links. These fibers are then organized into collagen bundles and networks in tissues (Persikov and Brodsky, 2002).
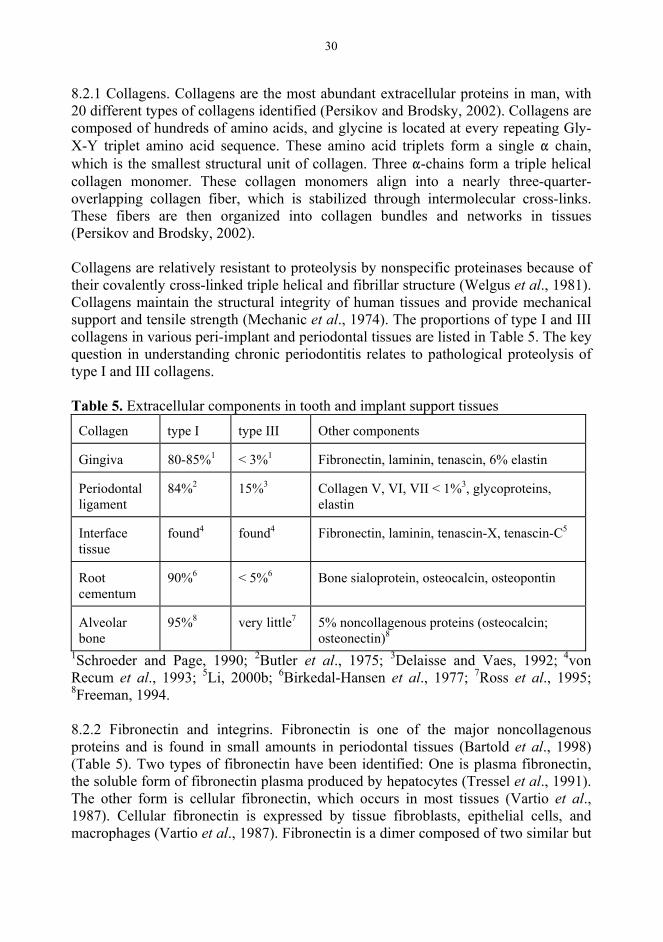
Collagens are relatively resistant to proteolysis by nonspecific proteinases because of their covalently cross-linked triple helical and fibrillar structure (Welgus et al., 1981). Collagens maintain the structural integrity of human tissues and provide mechanical support and tensile strength (Mechanic et al., 1974). The proportions of type I and III collagens in various peri-implant and periodontal tissues are listed in Table 5. The key question in understanding chronic periodontitis relates to pathological proteolysis of type I and III collagens.
Table 5. Extracellular components in tooth and implant support tissues
Collagen type I type III Other components
Gingiva 80-85%1 < 3%1 Fibronectin, laminin, tenascin, 6% elastin
Periodontal ligament
84%2 15%3 Collagen V, VI, VII < 1%3, glycoproteins, elastin
Interface tissue
found4 found4 Fibronectin, laminin, tenascin-X, tenascin-C5
Root cementum
90%6 < 5%6 Bone sialoprotein, osteocalcin, osteopontin
Alveolar bone
95%8 very little7 5% noncollagenous proteins (osteocalcin; osteonectin)8
1Schroeder and Page, 1990; 2Butler et al., 1975; 3Delaisse and Vaes, 1992; 4von Recum et al., 1993; 5Li, 2000b; 6Birkedal-Hansen et al., 1977; 7Ross et al., 1995; 8Freeman, 1994.
8.2.2 Fibronectin and integrins. Fibronectin is one of the major noncollagenous proteins and is found in small amounts in periodontal tissues (Bartold et al., 1998) (Table 5). Two types of fibronectin have been identified: One is plasma fibronectin, the soluble form of fibronectin plasma produced by hepatocytes (Tressel et al., 1991). The other form is cellular fibronectin, which occurs in most tissues (Vartio et al.,1987). Cellular fibronectin is expressed by tissue fibroblasts, epithelial cells, and macrophages (Vartio et al., 1987). Fibronectin is a dimer composed of two similar but

31
not completely identical chains. Cellular fibronectin acts as a bridge-like link between cells and collagen matrix and has been shown to be a substrate for cell adhesion (McDonald and Kelley, 1980; Bartold et al., 1998).
The extracellular matrices mainly affect the cells through cellular receptors known as integrins (Mohri, 1996). Integrins are heterodimeric glycoproteins composed of and
subunits. Thus far, 15 different chains have been identified; the corresponding number for subunits is eight.
8.2.3 Bone Bone is connective tissue, which is composed of calcified extracellular matrix and bone cells (Gartner and Hiatt, 1997). The organic portion is composed of collagen fibers (type I collagen) and ground substance (keratan sulfate, chondroitin sulfate, hyaluronic acid) (Batge et al., 1992). The inorganic portion accounts for about 65% of the dry weight of the bone. Type I collagen fibers are embedded in a complex of calcium and phosphate which forms hydroxyapatite [Ca10(PO4)6(OH)2] (Schroeder and Page, 1990).
Osteoblasts, which originate from periosteum and endosteum, are located on the external surface of bone or of the internal surface of the bone adjacent to the bone marrow. They secrete and deposit collagen type I and non-collagenous proteins around themselves. These kinds of osteoblasts turn into osteocytes when they become embedded in bone (Gartner and Hiatt, 1997). In mature bone, osteocytes occupy lacunae in the solid and mineralized bone matrix and communicate with each other through their cytoplasmic extensions located in bone canaliculi.
Osteoclasts are multinucleated giant cells containing multiple vacuoles and lysosomes (Blair, 1998). The surface of the osteoclast forms a ruffled border containing extensive folds facing the bone surface. Formation of a tight junction and a ruffled border is an indication of osteoclast activation (Teitelbaum, 2000). That region forms a subosteoclastic compartment (Howship’s lacuna), in which pH falls, due to the action of a proton pump (Everts et al., 1992). Hydrogen ions, produced by carbonic anhydrase within the osteoclast, cause acid dissolution of the hydroxyapatite crystals in the subosteoclastic compartment (Blair, 1989; Teitelbaum, 2000). The organic matrix is subsequently subjected to proteolysis via the action of cathepsin K or collagenases or both (Drake et al., 1996; Holliday et al., 1997; Konttinen et al., 2001). This process results in the formation of resorption pits (Everts et al., 2002).
Osteoblasts and osteoclasts are responsible for many physiological processes such as bone development and remodeling. All bones develop via endochondral (such as mandible) and intramembranous (such as maxilla) bone formation (Gartner and Hiatt, 1997). Collagen fibers in immature woven bone are not organized into lamellae. In mature bone, collagen fibers are re-organized into highly structured lamellae. Mechanical loading affects bone remodeling and bone quality according to the law of
32
Wolff (Wolff, 1985). The bone formed can be compact cortical bone or the less dense and metabolically more active trabecular bone. The skull skeleton is important for the protection of the brain, support of the teeth, and implants, and provision of a frame for facial expression.
8.3 Proteolytic enzymes8.3.1 Proteinases and their characteristics Almost all components of the extracellular matrix can be degraded by matrix metalloproteinases (MMPs). The three other major enzyme categories are cysteine, serine, and aspartic proteinases. This classification into four main categories is based on their mechanism of action, which is dependent on the structure of the catalytically active site of the enzyme. The major pathways responsible for the degradation of ECM are MMP-, plasmin-, polymorphonuclear leukocyte-, and serine proteinase-dependent pathways (Birkedal-Hansen et al., 1995). These are pH-dependent, as indicated in Table 6. These are cooperatively or independently involved in almost all physiological and pathological proteolytic processes such as bone and periodontal ligament tissue remodeling, periodontal diseases, oral cancer, loosening of hip implants, and rheumatoid arthritis (Cox et al., 1992; Birkedal-Hansen et al., 1995; Konttinen et al., 1998; Konttinen et al., 2002). Phagocytic (entirely inside of cells) and osteoclastic (in a sealed microenvironment between osteoclast and bone) pathways are important, as well (Birkedal-Hansen et al., 1993).
8.3.1.1 Matrix metalloproteinases. MMPs form a family of neutral endoproteinases with at present over 20 known members (MMP-1 to MMP-28). Their common denominator is that they are able to function at a neutral (body) pH, under which circumstances they can degrade almost all components of the extracellular matrix (Brinckerhoff and Matrisian, 2002). On the basis of their substrate specificity and structure, MMPs are grouped into collagenases, gelatinases, stromelysins, matrilysins, membrane-type MMPs, and various other diverse MMPs, like MMP-20. MMP-20 degrades amelogenin (Llano et al., 1997; Ryu et al., 1999).
8.3.1.2 MMP activation. MMPs are tightly controlled at several levels and most are not present in normal tissues at high levels. They are produced and secreted or released or both by different kinds of activated resident and immigrant host cells. Their cellular sources include epithelia, fibroblasts, macrophages, and polymorphonuclear leukocytes, but some of them are also found in osteoclasts and osteoblasts in bone (Uitto et al., 1998; Lazarus et al., 1968; Birkedal-Hansen et al.,1995). MMPs are secreted as latent proMMPs (zymogens), which need to be activated. Once activated, MMPs initiate tissue destruction if they are able to overcome their endogenous inhibitor shield (Birkedal-Hansen, 1995). Therefore, production or secretion or both, activation, and inhibition represent key points in the regulation of the MMP-driven tissue remodeling and destruction.

33
The cysteine switch has been suggested as the mechanism responsible for the activation of proMMPs. Two cysteine-switch activation cascades have been identified: one is proteolytic and one non-proteolytic. In the former, the propeptide domain in proMMPs, which covers and blocks the enzymatically active catalytic domain, is cleaved. The proteolytic activators comprise plasmin, kallikrein, cathepsin G, bacterial proteinases, and tumor-associated trypsin-2 (TAT-2) (Eeckhout and Vaes G, 1977; Owen et al., 1995; Okamoto et al., 1997; Sorsa et al., 1997). In the latter, the non-proteolytic cysteine switch activation cascade, all activators break the Cys97-Zn++
bond and lead to a conformational change in the MMPs. The nonproteolytic activators comprise organo-mercurials, hypochlorous acid, and oxidants (Sorsa et al., 1989; Saari et al., 1990; Birkedal-Hansen, 1995).
Figure 4. Modified schematic illustration of activation and inhibition of MMPs (Libby and Lee, 2000).
8.3.1.3 MMP inhibition. Activated MMPs can be inhibited by their endogenous inhibitors in vivo,with 2 macroglobulin playing an important role in this respect in serum. Due to its large size, it has no access to interstitial body fluids. In tissues, the tissue inhibitors of metalloproteinases (TIMPs) play a major role (Libby and Lee, 2000); four TIMPs (TIMP-1, -2, -3, -4) have been identified (Brew et al., 2000) (Figure 4). Tetracyclines also inhibit collagenase (Golub et al., 1985; Suomalainen et al., 1992). Chemically modified tetracyclines (CMTs) were developed from tetracyclines in the 1980´s (Golub et al., 1983). They are non-antimicrobial, but they inhibit MMPs, and are promising as medication for the modulation of collagen degradation in various tissue-destructive diseases (Golub et al., 1987; Golub et al., 1998; Ramamurthy et al., 2002).
8.3.2 Collagen degradationCollagen degradation has been a vital research topic in many diseases such as rheumatoid arthritis, loosening of hip implants, periodontitis, and oral cancer (Birkedal-Hansen, 1995). The two collagen degradation routes discovered are the intracellular and extracellular routes (van der Zee et al., 1997). Type I and III collagens are the most common collagens in periodontal and peri-implant tissue (Table 5).
8.3.2.1 Intracellular route. Some of the newly synthesized collagens are degraded within the cell before secretion (Bienkowski et al., 1978). It has been calculated that

34
more than 40% of them are degraded at a higher level of adenosine monophosphate (Baum et al., 1978), and then the content of collagens in tissues changes.
Resident cells such as fibroblasts first phagocytose the mature collagen fibrils surrounding them. This mature collagen fibril degradation then results in lysosomes mediated by acidic cysteine proteinases. This has been nicely demonstrated by electron microscopy (Garant, 1976; van der Zee et al., 1997). The intracellular mature collagen degradation route is the main pathway in a physiological steady state (Everts et al., 1996).
8.3.2.2 Extracellular route. This route has been suggested to play a major role in pathological conditions involving various MMPs (Everts et al., 1996) (Table 6). In addition, cathepsin K and TAT-2 may play a role in this route (Koivunen et al., 1991; Konttinen et al., 2002; Moilanen et al., 2003).
8.3.1.2.1 The intra-helical cleavage site. Collagen degradation sites are divided into intra- and extra-helical. The intra-helical cleavage site, cleaved by fibroblast-type collagenase, was first described in 1962 (Gross and Lapiere, 1962). Fibroblast collagenase, later called MMP-1 or collagenase-1, can initially cleave at a single site between Gly775-Leu/Ile776 of the triple helix of type I, II, and III collagen fibers (Sakai and Gross, 1967). Cleavage at this site results in the generation of a three-quarter (TCA) and a one-quarter-length (TCB) collagen degradation fragment (Gross and Nagai, 1965; Gross et al., 1974). Both of theses collagen fragments spontaneously undergo helix-to-coil transition and are thus denatured into non-helical gelatin derivatives at physiological body temperatures (Welgus et al., 1981). Gelatin is further rapidly degraded by MMP-1 or by gelatinases such as MMP-2 and MMP-9 or by both. Therefore, MMP-1 (and other similar collagenases) act as the rate-limiting enzyme in collagen proteolysis (Lehninger et al., 2000).
In the past several decades, new interstitial collagenases have been identified. Collagenase-2 (MMP-8 or neutrophil collagenase) was discovered in polymorphonuclear neutrophilic leukocytes (Lazarus et al., 1968). It effectively degrades type I collagen (Hasty et al., 1987), and its levels in gingival crevicular fluid correlate with periodontal tissue destruction (Lee et al., 1995). Collagenase-3 (MMP-13) was first discovered in breast cancer (Freije et al., 1994), and later in cartilage and synovial membrane, where it effectively degrades type II collagen (Mitchell et al., 1996; Konttinen et al., 1999). MMP-1 efficiently cleaves type III collagen. MMP-1, MMP-8, and MMP-13 constitute the collagenase sub-group (Krane et al., 1996).
Membrane type-1 MMP (MT1-MMP) has of course collagenase characteristics. MT1-MMP cleaves the Gly775-Leu776 of 1(I), which is the classical collagenase cleavage site. However, MT1-MMP cleaves the Gly781-Ile782 bond of 2(I), whereas classical collagenases cleave the Gly775-Leu776 bond of 2(I) (Ohuchi et al., 1997). MMP-2 (gelatinase-1) is also a collagenase (Aimes and Quigley, 1995; Konttinen et al., 1998);
35
it cleaves triple-helical collagen peptides (Lauer-Fields et al., 2000). Purified human neutrophil elastase can cleave native type I collagen and is, in that sense, a collagenase. But the exact neutrophil elastase cleavage sites were not identified (Kafienah et al., 1998).
The collagenase-cleaved 1/4 fragment diffuses more quickly out of the cartilage than does the larger 3/4 fragment (Vankemmelbeke et al., 1998). The collagen 3/4 fragment has some interesting feedback functions in vivo. The collagen type I 3/4 fragment raises the number of focal adhesions of smooth muscle cells (Carragher et al., 1999). Collagen degradation fragments are chemotactic to periodontal ligament fibroblasts, which initiate the periodontal tissue repair cycle (Terranova and Nishimura, 1996).
8.3.1.2.2 The extra-helical cleavage site. Stromelysin-1 (MMP-3) cleaves collagen at a non-helical site (Wu et al., 1991; Clavel et al., 1992). This kind of cleavage leads to the removal of cross-links and to depolymerization of the collagen fibrils, i.e., to collagen solubilization. MMP-3 is a telo-peptidase (Nakano et al., 1987).
8.3.1.2.3 Intra- and extra-helical cleavage sites. Cathepsin K has both collagenase and telo-peptidase characteristics, and can cleave collagen at multiple intra- and extra-helical sites (Garnero et al., 1998; Kafienah et al., 1998). It is produced by chondrocytes (Konttinen et al., 2002), fibroblasts (Hou et al., 2001), foreign body giant cells (Konttinen et al., 2001), odontoclasts (Domon et al., 1999), and osteoclasts (Bromme et al, 1996). The intra-helical cleavage sites for cathepsin K are Met159-Gly160, Ser162-Gly163 and Arg165-Gly166 of the 1 chain of type I collagen (Nosaka etal., 1999).
Bacterial collagenases, produced by pathogenic bacteria in dental or implant plaque, cleave at multiple intra- and extra-helical sites (Harrington, 1996). However, it seems that the degradation of type I collagen in periodontitis is mainly mediated by mammalian collagenases, not by bacterial enzymes (Sorsa et al., 1999; Romanelli etal., 1999; Soell et al., 2002).
8.3.3 Features of collagen degradation8.3.3.1 Collagen degradation in gingival tissue. Two pathological processes have been hypothesized to affect tissue destruction in chronic periodontitis. The burst tissue destruction concept was first suggested by Socransky et al. (Socransky et al., 1984; Soell et al., 2002). This theory states that chronic periodontitis is not a continuously active disease progressing at a predictable speed, but is characterized by recurrent and random acute episodes. ProMMPs, especially proMMP-1 or proMMP-2, accumulate in the extracellular matrix in periodontal tissue. When these proMMPs are suddenly activated by activators produced as a result of the action of cytokines such as interleukin-1 and epidermal growth factor, a burst of tissue damage ensues (van der Zee et al., 1994; van der Zee et al., 1996). Another study testing this hypothesis

36Table 6: Proteolytic enzymes and some of their characteristic
General characteristics Type I, II and III collagens cleavage characteristics
Group Members Cellular sources Optimal
pH Collagen cleavage site
Intra-helical Extra-helical PathwayIC EC
MMPs Collagenases (MMP-1, 8, 13) Gelatinases (MMP-2, 9) Membrane type MMPs (MT-1, 2, 3, 4-MMP) Stromelysin (MMP-3, 10, 11) Others (MMP-19, 20)
Fibroblasts Keratinocytes Monocytes Macrophages Neutrophils Osteoclasts
6 9 Collagenases (I, II, III)1 MMP-3 (I, III)4
MMP-2 (I)2
MT1-MMP (I, II, III)3
+
Serine PMN elastase Cathepsin G Plasminogen activators Plasmin Plasma kallikrein Mast cell chymases Tryptase Tumor-associated trypsins
Neutrophils 6 10 PMN elastase (I)5 PMN elastase (III)6
Cathepsin G (II)7 +
Aspartic Cathepsin D Breast tumor cells 3.5 5 +
Cysteine Cathepsin B, H, L, N, K, S, W Osteoclasts Foreign body giant cells Fibroblasts Chondrocytes
3 7 Cathepsin K (I, II)8 Cathepsin K (I, II)8, 9 + +
IC = intracellular pathway, EC = Extracellular pathway; I, II, and III refer to the type of collagen cleaved. 1Gross and Lapiere, 1962; 2Aimes and Quigley, 1995; 3Ohuchi et al., 1997; 4Wu et al., 1991; Clavel et al., 1992; 5Kafienah et al., 1998; 6Mainardi et al., 1980; 7Starkey, 1977; 8Garnero et al., 1998; 9Konttinen et al., 2001.

37
suggests that, in chronic periodontitis, MMP-2 may be the main proteolytic enzyme responsible for degradation (Kerkvliet et al., 1999). This is compatible with the finding that MMP-2 is also a collagenase (Aimes and Quigley, 1995; Konttinen et al., 1998).
The other main hypothesis is based on continuous tissue destruction (Reynolds, 1996). Its main premise is that the collagen degradation is a result of an imbalance between MMPs and their TIMP inhibitor levels. Total MMP activity levels, especially those of the collagenases, are supposed to exceed levels of the TIMPs (Sorsa et al., 1992; Golub et al., 1997; Romanelli et al., 1999). Some evidence has been published which suggests that high net MMP activity leads to continuous tissue destruction (Ingman etal., 1996; Romanelli et al., 1999).
8.3.3.2 Bone collagen degradation. Both the cysteine proteinase cathepsin K and collagenases are able to hydrolyze type I collagen (Drake et al., 1996; Holliday et al., 1997). However, it is unknown whether they both participate in osteoclastic bone resorption. A recent paper suggests that calvarial osteoclasts are for their activity dependent on both cysteine proteinases and MMPs, but long bone osteoclasts are mainly dependent on cysteine proteinases. It seems, therefore, that bone resorption by cathepsin K or collagenases or both is dependent on type of bone (Everts et al., 1999). MMP-9 has been implicated in the degradation of cathepsin- and collagenase-cleaved and denatured collagen fragments, and it cleans the bottoms of the bone resorption lacunae (Everts et al., 2002).
Both MMP-1 and MMP-9 are expressed by osteoclasts (Holliday et al., 1997; Wucherpfennig et al., 1994). It has been disputed whether it is MMP-1 or MMP-9 which initiates osteoclast-mediated bone resorption. It seems that MMP-1 from osteoblasts is required to initiate bone resorption (Holliday et al., 1997). MMP-9 seems to be involved in the recruitment of osteoclasts to resorption sites (Blavier and Delaisse, 1995). More recently, MMP-9 has been suggested to be involved in bone remodeling (Delaisse et al., 2000).
8.4 Fibronectin and neutrophil elastaseThe extracellular matrix is a complex and dynamic meshwork of proteins. In addition to collagens, glycoproteins provide structural support to cells, but they also have a profound influence on many cellular activities. Increased degradation and/or production of fibronectin is involved in many physiological and pathological disease conditions, such as chronic leg ulcers (Herrick et al., 1997).
In chronic periodontitis, the periodontal pathogen Actinobacillus actinomycetemcomitans adheres to fibronectin (Mintz and Fives-Taylor, 1999). Changes in content of cellular fibronectin are usually caused by its proteolytic degradation rather than by changes in its synthesis. Human neutrophil elastase effectively degrades cellular fibronectin. Neutrophil elastase has been found to be the
38
most important enzyme able to degrade fibronectin to Fn fragments in vivo(McDonald et al., 1982). The three elastase cleavage sites are located in the transglutaminase, gelatin binding, and cell adhesive fibronectin domains (McDonald and Kelley, 1980). Fibronectin has been detected in periodontitis-affected gingival tissue (Haapasalmi et al., 1995). Fibronectin degradation fragments are increased in gingival crevicular fluid, and their concentration decreases after periodontal treatment (Talonpoika et al., 1993). The increased concentration of fibronectin fragments in gingival crevicular fluid has been thought to indicate ongoing inflammation and tissue destruction (Talonpoika et al., 1989).
Cellular fibronectin binds to the implant surface (Bagambisa et al., 1994). Titanium (Ti) elevates cellular fibronectin in fibroblast culture (Chou et al., 1996). The expression of cellular fibronectin is higher in the interface tissue collected from revision operations of totally replaced hips (Li et al., 2000).
8.5 Cytokines in bone resorptionBone is a dynamically remodeling tissue, in which parts of the old deteriorated bone are removed and replaced by new bone, regulated according to the law of Wolff (Blair, 1998). This is important for the maintenance of bone quality. The process is usually precisely regulated, leading to balanced bone resorption and formation (Schwartz et al., 1997). Coupling refers to the fact that under normal conditions bone mass is maintained via coupling of osteoclast-mediated bone resorption to osteoblast-mediated bone formation, which balance each other. This process is regulated by hormones and locally by cytokines (Schwartz et al., 1997; Blair, 1998; Raisz, 1999).
“Cytokine” is a generic term for soluble molecules which mediate interactions between cells. Cytokines are relatively small molecules, usually less than 30 kDa in size. They are proteins or glycoproteins (Schwartz et al., 1997). They regulate their target cells via cell surface-bound cytokine receptors in four different ways: A cytokine can have an autocrine, intracrine, juxtacrine, or paracrine mode of action. “Autocrine” (Figure 5A) refers to the synthesis of a cytokine by one cell that influences the growth and functional activities of the cells producing that cytokine via a specific receptor on its surface (Klinger et al., 1998). “Intracrine” (Figure 5B) refers to the direct action of a cytokine on a cell. Cytokines are produced as cytokine and receptor complexes that are rapidly internalized by the cells and translocated to the nucleus without being degraded. The cytokines contain a nuclear transport sequence that mediates the transport of this cytokine into the nucleus. “Juxtacrine” refers to regulatory actions exerted between cells (from one cell to another cell). There are two kinds of contacts between cells communicating in a juxtacrine manner. One contact is mediated via a membrane-bound cytokine, which interacts with the cytokine receptor on the adjacent cell (Figure 5C). The other mode of juxtacrine action is mediated via a pericellular matrix-associated cytokine, which interacts with receptors on a neighboring cell (Figure 5C). “Paracrine” refers to the fact that cytokines expressed by one type of cell are secreted into body fluids and influence the activities of some
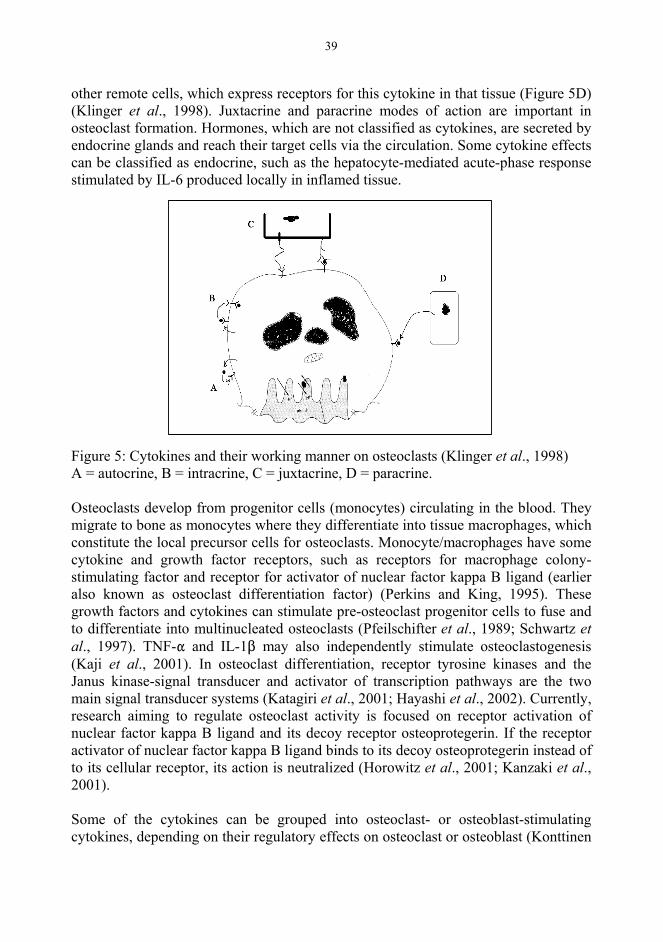
39
other remote cells, which express receptors for this cytokine in that tissue (Figure 5D) (Klinger et al., 1998). Juxtacrine and paracrine modes of action are important in osteoclast formation. Hormones, which are not classified as cytokines, are secreted by endocrine glands and reach their target cells via the circulation. Some cytokine effects can be classified as endocrine, such as the hepatocyte-mediated acute-phase response stimulated by IL-6 produced locally in inflamed tissue.
Figure 5: Cytokines and their working manner on osteoclasts (Klinger et al., 1998) A = autocrine, B = intracrine, C = juxtacrine, D = paracrine.
Osteoclasts develop from progenitor cells (monocytes) circulating in the blood. They migrate to bone as monocytes where they differentiate into tissue macrophages, which constitute the local precursor cells for osteoclasts. Monocyte/macrophages have some cytokine and growth factor receptors, such as receptors for macrophage colony-stimulating factor and receptor for activator of nuclear factor kappa B ligand (earlier also known as osteoclast differentiation factor) (Perkins and King, 1995). These growth factors and cytokines can stimulate pre-osteoclast progenitor cells to fuse and to differentiate into multinucleated osteoclasts (Pfeilschifter et al., 1989; Schwartz etal., 1997). TNF- and IL-1 may also independently stimulate osteoclastogenesis (Kaji et al., 2001). In osteoclast differentiation, receptor tyrosine kinases and the Janus kinase-signal transducer and activator of transcription pathways are the two main signal transducer systems (Katagiri et al., 2001; Hayashi et al., 2002). Currently, research aiming to regulate osteoclast activity is focused on receptor activation of nuclear factor kappa B ligand and its decoy receptor osteoprotegerin. If the receptor activator of nuclear factor kappa B ligand binds to its decoy osteoprotegerin instead of to its cellular receptor, its action is neutralized (Horowitz et al., 2001; Kanzaki et al., 2001).
Some of the cytokines can be grouped into osteoclast- or osteoblast-stimulating cytokines, depending on their regulatory effects on osteoclast or osteoblast (Konttinen

40
et al., 1997). Many osteoclast-stimulating cytokines have been found, although many of them may have an indirect mode of action via the receptor activation of the nuclear factor kappa B system in Table 7 (Wright and Goodman, 2000). Many of them are produced by multiple resident or immigrant cells in peri-implant tissues. Producer cells include fibroblasts, keratinocytes, monocyte/macrophages, foreign body giant cells, osteoclasts and osteoblasts (Koka and Reinhardt 1997; Giudiceandrea et al., 1998; Sandros et al., 2000; Xu et al., 2000). Increased osteoclast numbers and osteoclast activity contribute to pathological bone loss in periodontitis, to loosening of hip implants, and to osteoporosis (Schwartz et al., 1997; Konttinen et al., 1997; Tervahartiala et al., 2001). Peri-implant bone loss has not, however, been studied in this respect to assess whether osteoclast-stimulating cytokines are increased around loosening dental implants.
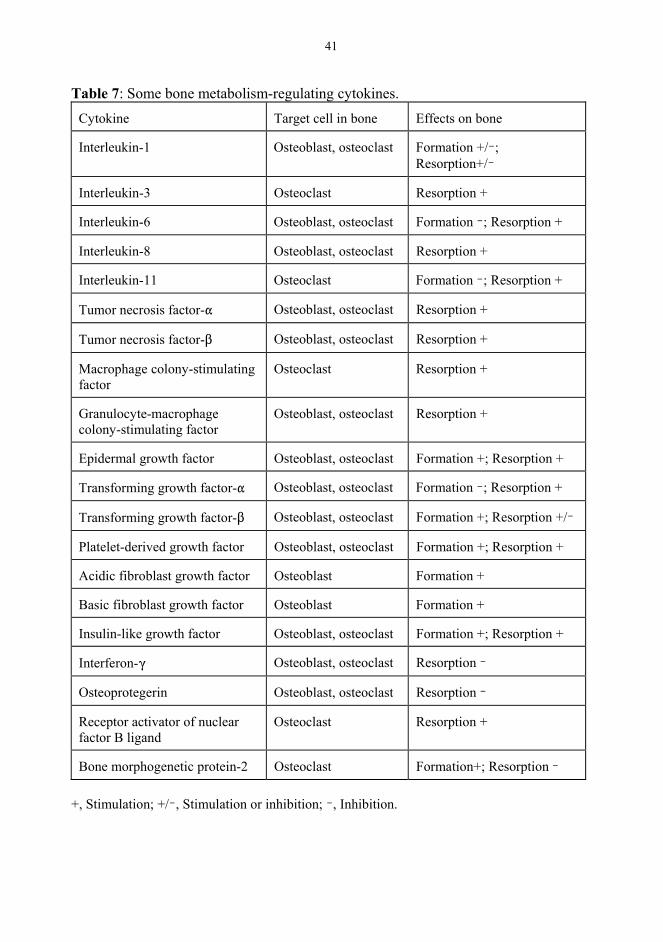
41
Table 7: Some bone metabolism-regulating cytokines.Cytokine Target cell in bone Effects on bone
Interleukin-1 Osteoblast, osteoclast Formation +/ ;Resorption+/
Interleukin-3 Osteoclast Resorption +
Interleukin-6 Osteoblast, osteoclast Formation ; Resorption +
Interleukin-8 Osteoblast, osteoclast Resorption +
Interleukin-11 Osteoclast Formation ; Resorption +
Tumor necrosis factor- Osteoblast, osteoclast Resorption +
Tumor necrosis factor- Osteoblast, osteoclast Resorption +
Macrophage colony-stimulating factor
Osteoclast Resorption +
Granulocyte-macrophage colony-stimulating factor
Osteoblast, osteoclast Resorption +
Epidermal growth factor Osteoblast, osteoclast Formation +; Resorption +
Transforming growth factor- Osteoblast, osteoclast Formation ; Resorption +
Transforming growth factor- Osteoblast, osteoclast Formation +; Resorption +/
Platelet-derived growth factor Osteoblast, osteoclast Formation +; Resorption +
Acidic fibroblast growth factor Osteoblast Formation +
Basic fibroblast growth factor Osteoblast Formation +
Insulin-like growth factor Osteoblast, osteoclast Formation +; Resorption +
Interferon- Osteoblast, osteoclast Resorption
Osteoprotegerin Osteoblast, osteoclast Resorption
Receptor activator of nuclear factor B ligand
Osteoclast Resorption +
Bone morphogenetic protein-2 Osteoclast Formation+; Resorption
+, Stimulation; +/ , Stimulation or inhibition; , Inhibition.
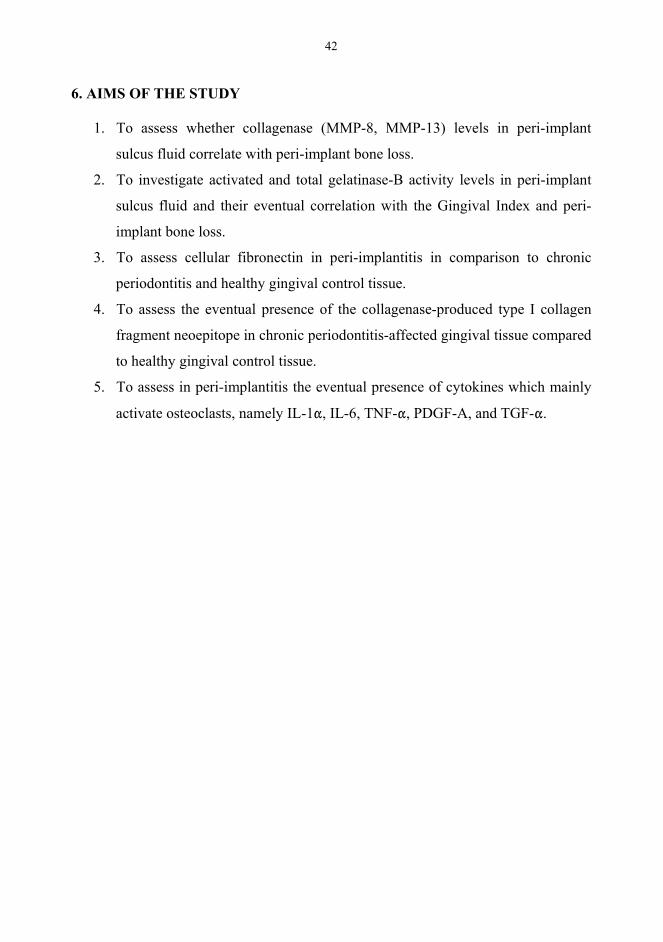
42
6. AIMS OF THE STUDY
1. To assess whether collagenase (MMP-8, MMP-13) levels in peri-implant
sulcus fluid correlate with peri-implant bone loss.
2. To investigate activated and total gelatinase-B activity levels in peri-implant
sulcus fluid and their eventual correlation with the Gingival Index and peri-
implant bone loss.
3. To assess cellular fibronectin in peri-implantitis in comparison to chronic
periodontitis and healthy gingival control tissue.
4. To assess the eventual presence of the collagenase-produced type I collagen
fragment neoepitope in chronic periodontitis-affected gingival tissue compared
to healthy gingival control tissue.
5. To assess in peri-implantitis the eventual presence of cytokines which mainly
activate osteoclasts, namely IL-1 , IL-6, TNF- , PDGF-A, and TGF- .
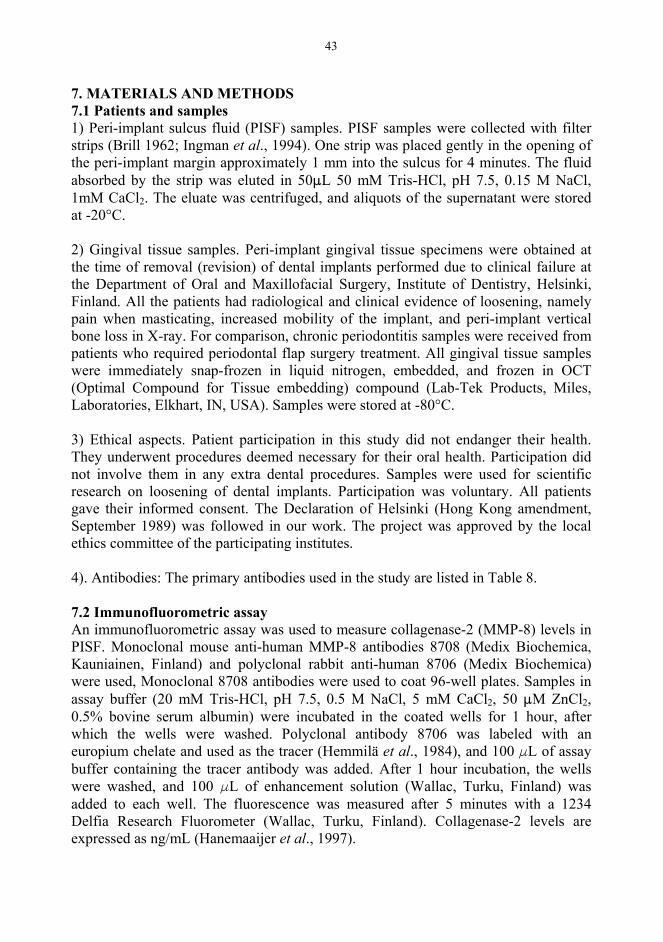
43
7. MATERIALS AND METHODS7.1 Patients and samples1) Peri-implant sulcus fluid (PISF) samples. PISF samples were collected with filter strips (Brill 1962; Ingman et al., 1994). One strip was placed gently in the opening of the peri-implant margin approximately 1 mm into the sulcus for 4 minutes. The fluid absorbed by the strip was eluted in 50 L 50 mM Tris-HCl, pH 7.5, 0.15 M NaCl, 1mM CaCl2. The eluate was centrifuged, and aliquots of the supernatant were stored at -20°C.
2) Gingival tissue samples. Peri-implant gingival tissue specimens were obtained at the time of removal (revision) of dental implants performed due to clinical failure at the Department of Oral and Maxillofacial Surgery, Institute of Dentistry, Helsinki, Finland. All the patients had radiological and clinical evidence of loosening, namely pain when masticating, increased mobility of the implant, and peri-implant vertical bone loss in X-ray. For comparison, chronic periodontitis samples were received from patients who required periodontal flap surgery treatment. All gingival tissue samples were immediately snap-frozen in liquid nitrogen, embedded, and frozen in OCT (Optimal Compound for Tissue embedding) compound (Lab-Tek Products, Miles, Laboratories, Elkhart, IN, USA). Samples were stored at -80°C.
3) Ethical aspects. Patient participation in this study did not endanger their health. They underwent procedures deemed necessary for their oral health. Participation did not involve them in any extra dental procedures. Samples were used for scientific research on loosening of dental implants. Participation was voluntary. All patients gave their informed consent. The Declaration of Helsinki (Hong Kong amendment, September 1989) was followed in our work. The project was approved by the local ethics committee of the participating institutes.
4). Antibodies: The primary antibodies used in the study are listed in Table 8.
7.2 Immunofluorometric assayAn immunofluorometric assay was used to measure collagenase-2 (MMP-8) levels in PISF. Monoclonal mouse anti-human MMP-8 antibodies 8708 (Medix Biochemica, Kauniainen, Finland) and polyclonal rabbit anti-human 8706 (Medix Biochemica) were used, Monoclonal 8708 antibodies were used to coat 96-well plates. Samples in assay buffer (20 mM Tris-HCl, pH 7.5, 0.5 M NaCl, 5 mM CaCl2, 50 M ZnCl2,0.5% bovine serum albumin) were incubated in the coated wells for 1 hour, after which the wells were washed. Polyclonal antibody 8706 was labeled with an europium chelate and used as the tracer (Hemmilä et al., 1984), and 100 L of assay buffer containing the tracer antibody was added. After 1 hour incubation, the wells were washed, and 100 L of enhancement solution (Wallac, Turku, Finland) was added to each well. The fluorescence was measured after 5 minutes with a 1234 Delfia Research Fluorometer (Wallac, Turku, Finland). Collagenase-2 levels are expressed as ng/mL (Hanemaaijer et al., 1997).
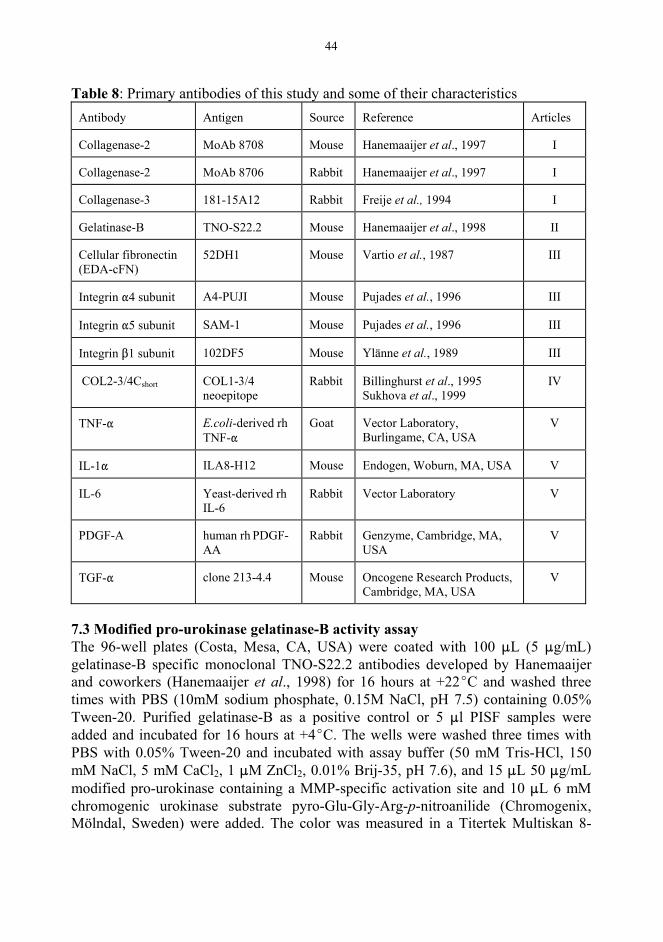
44
Table 8: Primary antibodies of this study and some of their characteristicsAntibody Antigen Source Reference Articles
Collagenase-2 MoAb 8708 Mouse Hanemaaijer et al., 1997 I
Collagenase-2 MoAb 8706 Rabbit Hanemaaijer et al., 1997 I
Collagenase-3 181-15A12 Rabbit Freije et al., 1994 I
Gelatinase-B TNO-S22.2 Mouse Hanemaaijer et al., 1998 II
Cellular fibronectin (EDA-cFN)
52DH1 Mouse Vartio et al., 1987 III
Integrin 4 subunit A4-PUJI Mouse Pujades et al., 1996 III
Integrin 5 subunit SAM-1 Mouse Pujades et al., 1996 III
Integrin 1 subunit 102DF5 Mouse Ylänne et al., 1989 III
COL2-3/4Cshort COL1-3/4 neoepitope
Rabbit Billinghurst et al., 1995 Sukhova et al., 1999
IV
TNF- E.coli-derived rh TNF-
Goat Vector Laboratory, Burlingame, CA, USA
V
IL-1 ILA8-H12 Mouse Endogen, Woburn, MA, USA V
IL-6 Yeast-derived rh IL-6
Rabbit Vector Laboratory V
PDGF-A human rh PDGF-AA
Rabbit Genzyme, Cambridge, MA, USA
V
TGF- clone 213-4.4 Mouse Oncogene Research Products, Cambridge, MA, USA
V
7.3 Modified pro-urokinase gelatinase-B activity assayThe 96-well plates (Costa, Mesa, CA, USA) were coated with 100 L (5 g/mL) gelatinase-B specific monoclonal TNO-S22.2 antibodies developed by Hanemaaijer and coworkers (Hanemaaijer et al., 1998) for 16 hours at +22 C and washed three times with PBS (10mM sodium phosphate, 0.15M NaCl, pH 7.5) containing 0.05% Tween-20. Purified gelatinase-B as a positive control or 5 l PISF samples were added and incubated for 16 hours at +4 C. The wells were washed three times with PBS with 0.05% Tween-20 and incubated with assay buffer (50 mM Tris-HCl, 150 mM NaCl, 5 mM CaCl2, 1 M ZnCl2, 0.01% Brij-35, pH 7.6), and 15 L 50 g/mL modified pro-urokinase containing a MMP-specific activation site and 10 L 6 mM chromogenic urokinase substrate pyro-Glu-Gly-Arg-p-nitroanilide (Chromogenix, Mölndal, Sweden) were added. The color was measured in a Titertek Multiskan 8-

45
channel photometer (Flow Laboratories, Irvine, Scotland). The results are expressed as U/mL (Verheijen et al., 1997; Hanemaaijer et al., 1998).
To measure total gelatinase-B activity, PISF samples were first incubated with 0.5 mM 4-aminophenylmercuric acetate (APMA) (Sigma) for 2 hrs at +37 C to activate progelatinase-B. The assay detects as little as 3.75 x 10-15 mol gelatinase-B in biological fluid samples (Verheijen et al., 1997).
7.4 Quantitative immunoblot techniqueThe diluted PISF samples adjusted to contain 2 g protein were treated with Laemmli´s buffer, pH 6.8, containing 5 mM dithiothreitol, and heated for 5 minutes at +100 C. High- and low-range prestained SDS-PAGE standards (Bio-Rad, Hercules, CA, USA) served as molecular weight markers. Samples were separated on 8 to 10% SDS-polyacrylamide cross-linked gel at 200 V for 45 minutes and electrophoretically transferred to a nitrocellulose membrane (Bio-Rad). Non-specific binding was blocked by incubation with 3% gelatin in 10 mM Tris-HCl, pH 8.0, containing 22 mM NaCl and 0.05% Tween. This membrane was incubated with polyclonal rabbit anti-human MMP-13 IgG overnight at +20 C. The MMP-13 antibody was used at a concentration of 0.5 g/mL. After repeated washings, the membrane was incubated with alkaline phosphatase-labeled anti-rabbit immunoglobulins (Sigma) (1:100) for 1 hour at +20 C. After a 15-minute washing with 10 mM Tris-HCl, pH 8.2, containing 22 mM NaCl and 0.05% Tween washing buffer, the color was developed by addition of nitro blue tetrazolium and 5-bromo-4-chloro-3-indolyl-phosphate diluted with N-N-dimethyl-formide (Sigma) in 100 mM Tris-HCl, pH 9.5, containing 5 mM MgCl2and 100 mM NaCl. The secondary antibody alone did not recognize the band detected with specific antibodies in immunoblotting. Known concentrations of MMP-13 were used in all tests as positive controls and standards for quantitative immunoblots. Immunoblots were quantitated by image densitometer (Model G5-700, Bio-Rad) and the Molecular Analyst Program (Image analysis system version 1.4). Results are expressed as ng per mL (Golub et al., 1998).
7.5 Immunohistochemical avidin-biotin-peroxidase complex (ABC) stainingTwo 6- m cryostat cut gingival sections were mounted on gelatin-formalin-coated glass slides and fixed in cold acetone at +4 C for 5 minutes. After washes with 20mM Tris-HCl, 150 mM NaCl, pH 7.4 (TBS), endogenous peroxidase was inhibited by incubation in 0.4% H2O2 in methanol at room temperature for 30 minutes. The staining was done by use of the Vectastain® Elite ABC mouse Kit (Vector Laboratories, Burlingame, CA, USA). Briefly, serial sections were incubated with normal horse serum (diluted 1:50 in TBS containing 0.1% bovine serum albumin) at room temperature for 20 minutes. After blotting of the excess serum, the sections were treated at room temperature with: 1) primary antibodies diluted in TBS containing 0.1% BSA overnight at +4 C. 2) biotinylated IgG (dilution 1:100, Vector) at +22 C for 30 minutes, and 3) avidin-biotin-peroxidase complex (1:100 in TBS; Vector Labs). The sites of peroxidase binding were revealed by incubation in 3,3'-

46
diaminobenzidine tetrahydrochloride (Sigma) in 0.006% H2O2 at +22 C for 1 to 10 minutes in darkness.
Normal IgG of the same subtype but with irrelevant specificity was used instead of and at the same concentration as the primary antibodies as a negative staining control to confirm the specificity of the immunohistochemical staining results. One synovial membrane sample from a rheumatoid arthritis patient was severed as a positive sample control in each staining. Both the negative staining and positive sample controls confirmed the specificity of immunohistochemical staining results.
One of the sections on each slide was counterstained with Harris hematoxylin for one minute. The sections were dehydrated in a graded ethanol series, cleared in xylene, and mounted in synthetic mounting medium (Diatex, Becker Industrifärg AB, Märsta, Sweden).
7.6 Microscopic morphometric evaluationMicroscopic morphometric evaluation (quantitative assessment) was performed with a low-light charge-screen coupled with a 12-bit PC digital image camera (SensiCam, Kelheim, Germany) mounted on a Leitz Diaplan (Ernst Leitz, Wetzlar, Germany) light microscope linked to a semiautomatic Analysis Pro 3.0 image analysis and processing system (Soft Analysis System GmbH, Münster, Germany). Morphometry was performed under x 400 magnification on tissue sections without counterstaining. The whole section area was analyzed (Xu et al., 2000). After adjustment of illumination and focus, the image was recorded in digitalized form in a computer. After setting the threshold for the optimal signal-to-noise ratio, it was used for the whole sample during the procedure. The results of quantitative assessment are expressed as percentage of positively staining area of the total tissue area (Xu et al., 2000).
7.7 Statistical methodsStatistical calculations were made using BMDP 2.0 for Windows software (Los Angeles, CA, USA). The value for a statistically significant difference was set at 0.05. Shapiro and Wilk´s W test were first used to test the data for normality.
Normally distributed data are expressed as means and standard deviations. Non-normally distributed data are expressed as means and interquartiles (Q3, Q1, and [Q3-Q1]). For analysis of the eventual statistical difference between two groups, the un-paired t-test was used for normally distributed groups, whereas the Mann-Whitney rank sum test was used if at least one of the two groups had a non-normal distribution. For three group comparisons, the Kruskal-Wallis test was used for normally distributed data, whereas one-way analysis of variance (ANOVA) was used for non-normally distributed data. Correlations between two groups were calculated using Spearman’s rank correlation for normally distributed variables and the Pearson rank test for non-normally distributed variables.
47
8. RESULTS
8.1 Collagenase levels differed between different peri-implant vertical bone loss groups (I)Collagenase-2 (n = 6, 2021 ± 1038, p<0.05) and collagenase-3 (16 ± 4, p<0.05) in peri-implant sulcus fluid were higher (Kruskall-Wallis test) in the group which had lost more than 3 mm of bone than in the two other groups with < 1 mm (n = 32, 861 ± 164 and 10 ± 1, respectively) or 1 to 3 mm (n = 11, 1265 ± 508 and 12 ± 2, respectively) of bone loss. A significant linear correlation appeared between site-specific collagenase-2 and collagenase-3 levels (r = 0.692, p < 0.005) (Pearson rank test).
8.2 Gingival indices did not differ between different peri-implant vertical bone loss groups (I) Gingival index results showed no differences among different peri-implant vertical bone loss groups (0.6 ± 0.1 in patients with < 1 mm bone loss, 0.6 ± 0.5 in patients with 1-3 mm bone loss, and 1.2 ± 0.3 in patients with more than 3 mm bone loss, p >0.05, Kruskall-Wallis test).
8.3 Gelatinase-B levels in PISF correlated with peri-implant vertical bone loss (II)Degree of in vivo activated gelatinase-B correlated (r = 0.942, p < 0.0001) with total gelatinase-B (n = 46, Spearman's rank correlation test). Both total gelatinase-B (r = 0.553, p = 0.021) and activated gelatinase-B levels (r = 0.529, p = 0.003) in PISF correlated with peri-implant bone loss (n = 46, Spearman's rank correlation test). Total gelatinase-B (median = 1375, Q3 =2079, Q1 = 445, [Q3 Q1] = 1633) and activated gelatinase-B (median = 458, Q3 = 979, Q1 = 200, [Q3 Q1] = 979) levels were increased in the group with > 3 mm peri-implant bone loss compared to < 1 mm (total gelatinase-B, median = 183, Q3 = 558, Q1 = 78, [Q3-Q1] = 480, p = 0.013; activated gelatinase-B, median = 133, Q3 = 275, Q1 = 50, [Q3 Q1] = 225, p = 0.015) and 1 to 3 mm groups (total gelatinase-B, median = 250, Q3 = 583, Q1 = 50, [Q3 Q1] = 533, p = 0.027); (activated gelatinase-B, median = 166, Q3 = 233, Q1 = 33, [Q3 Q1] = 200, p = 0.035) group (Rank sum test).
8.4 Gelatinase-B levels in PISF differed between gingival index groups (II)Activated gelatinase-B level (median = 225, Q3 = 375, Q1 = 108, [Q3-Q1 = 267]) in the GI > 0.5 group was higher than that in the GI = 0 (median = 50, Q3 = 142, Q1 = 17, [Q3 Q1 = 125], p = 0.012) and GI 0.5 (median = 216, Q3 = 425, Q1 = 50, [Q3
Q1 = 375], p = 0.17) group (Rank sum test). Total gelatinase-B levels in the GI > 0.5 (median = 350, Q3 = 258, Q1 = 42, [Q3 Q1 = 216]) and GI 0.5 (median = 417, Q3 = 1083, Q1 = 171, [Q3-Q1 = 912], p = 0.02) groups were clearly high compared to the GI = 0 (median = 83, Q3 = 258, Q1 = 42, [Q3-Q1 = 217], p = 0,043) group (Rank sum test).
48
8.5 Cellular fibronectin staining was higher in gingival tissue (III)All gingival samples showed immunoreactivity to cellular fibronectin. The staining pattern of cellular fibronectin was similar in peri-implantitis, chronic periodontitis, and in normal healthy controls. The staining intensity of cellular fibronectin in the extracellular matrix varied among different regions of the peri-implant and gingival tissue samples. Cellular fibronectin staining was stronger in the blood vessel wall than in the surrounding perivascular and interstitial matrix. Intense cellular fibronectin staining was also evident in the epithelial basement membrane and in the lamina propria, especially in connective tissue papillae. Oral epithelium did not stain for cellular fibronectin. The staining of other areas in the lamina propria dominated by fibroblasts was less conspicuous. Foreign bodies, probably of implant- or surgical instrument-derived metal, were embedded in the extracellular matrix as small, round particles. Most such particles were surrounded by a cellular fibronectin layer approximately 5 to 10 m thick. Staining controls with monoclonal mouse IgG1 with an irrelevant specificity were negative.
Cellular fibronectin was high in peri-implantitis compared to that in healthy gingival control tissue (n = 10, 33 ± 5% vs 12 ± 1%, p = 0.003). In contrast, cellular fibronectin staining was low in chronic periodontitis compared to that in healthy gingival control tissue (6 ± 1% vs 12 ± 1%; p = 0.006).
8.6 Distribution of integrin receptors for cellular fibronectin in gingival tissue (III)
4 subunit. Keratinocytes were integrin 4 subunit-negative. Some integrin 4subunit positive fibroblasts were visible in the connective tissue stroma. Almost all endothelial cells in postcapillary venules and capillaries were negative or at most weakly positive for the integrin 4 subunit.
5 subunit. The integrin 5 subunit was strongly expressed in the endothelium of postcapillary venules and capillary blood vessels, in particular in the connective tissue papillae. Fibroblasts were only weakly positive. No integrin 5 subunit-positive cells were found in the oral epithelium.
1 subunit. The integrin 1 subunit was strongly expressed in the basal cell layer of the oral epithelium and in some cells of the stratum spinosum, but in no other layers of the oral epithelium. Immunoreactivity almost as strong occurred in vascular endothelial cells, and comparatively weak staining in fibroblasts in the lamina propria. The distributions of integrin subunits binding cellular fibronectin were studied, but no significant differences were found between periodontitis and loosening dental implants.
8.7 Increased staining of collagenase-cleaved collagen fragments (cCOL1-3/4C) in un-treated chronic periodontitis (IV)
49
Moderate cCOL1-3/4C staining appeared in the submucosa below the sulcular and junctional epithelium in chronic periodontitis-affected gingival tissue samples. Similar staining of moderate intensity was observable around some of the fibroblasts embedded in the periodontal connective tissue matrix. In addition, most of the interstitial collagen in areas infiltrated by inflammatory mononuclear cells stained with the COL1-3/4C antibodies. Control samples contained some COL1-3/4C immunoreactivity (1.6 ± 0.7%; n = 10) below the sulcular and junctional epithelium, but the extent of this staining was less than that in chronic periodontitis (6.3 ± 1.2%; n = 10; p 0.005, unpaired student t test). Some pilot studies on collagenase-cleaved collagen neoepitopes were also done on peri-implant tissues still available at that time of the thesis work, but the sample sizes were small and the results were inconsistent. Therefore, these results were not published.
8.8 Increased expression of osteoclast-stimulating cytokines in gingival tissue in chronic periodontitis and implantitis (V)Perivascular mononuclear cell infiltrates in the lamina propria in chronic periodontitis contained mainly macrophages. In peri-implantitis, multinuclear foreign body giant cells were frequently observable. Many of the macrophages in chronic periodontitis and peri-implantitis contained immunoreactive cytokines. All of the foreign body giant cells always contained all of the osteoclast-stimulating cytokines analyzed in the present study. Some of the fibroblast-like cells contained IL-1 and TNF- , but IL-6, PDGF-A, and TGF- also appeared in such cells. Normal healthy gingival control tissue contained only a few cytokine immunoreactive cells.
TNF- , IL-1 , IL-6, PDGF-A, and TGF- positive cells appeared in the basal cell layer of sulcular epithelium, with a few cytokine immunoreactive cells visible in the prickle-cell layer. Staining intensity was most conspicuous in chronic periodontitis, followed by peri-implantitis and normal healthy controls in this ranking order. TNF- ,IL-1 , and IL-6 immunoreactive cells were most numerous in chronic periodontitis and peri-implantitis. PDGF-A and TGF- immunoreactive cells were no more frequent in chronic periodontitis than in healthy gingival control tissues.
50
9. DISCUSSION
Dental implant materials dramatically developed during the past half century after introduction of osseointegration, a remarkable milestone in dentistry (Brånemark et al., 1977). Dental implants meet multiple demands with regard to function and aesthetics, and mechanical failures have decreased as a result of development of implant materials (Adell et al., 1985; Kronström et al., 2002). Osseointegration can be achieved more often than before due to improvement in surgical methods and equipment, but loosening of dental implants has become a major problem in implant dentistry (Duyck and Naert, 1998; Esposito et al., 1998a, b; el Askary et al., 1999). Many risk factors increase the rate of loosening (Esposito et al., 1998a; el Askary etal., 1999): Nonbiocompatible implant materials constitute one important risk factor, because they cause adverse host responses (Edgerton and Levine, 1993; Santavirta etal., 1999). All risk factors affect pathomechanisms responsible for loosening (Figure 3). One of the main features of the process is progressive loss of peri-implant support tissues (Tonetti and Schmid, 1994; Duyck and Naert, 1998). Many proteolytic enzymes are increased around loosening dental implants (Ingman et al., 1994; Teronen et al., 1997; Sorsa et al., 1999) and in chronic periodontitis (Reynolds and Meikle, 1997; Romanelli et al., 1999). We followed and extended the previous work on proteolytic enzymes and also studied osteoclast-stimulating cytokines, because osteoclasts seem to play an important role in peri-implant bone tissue destruction during loosening of dental implants.
9.1 Collagenase-2, -3, and gelatinase-B involved in peri-implant bone lossType I collagen is the dominant organic component in bone tissue (Table 5). Its proteolytic degradation is an important step in pathological bone tissue destruction (Birkedal-Hansen et al., 1993). Cathepsin K cleaves the collagen triple helix at intra- and extra-helical sites (Blair, 1998; Garnero et al., 1998). Collagenases (collagenase-1, 2, 3) cleave triple helical type I collagen fibers at one site only (Gross and Lapiere, 1962). Both cysteine proteinases and MMPs seem to be involved in bone resorption. Cathepsin K and collagenase-3 are expressed by osteoclasts (Bromme et al, 1996; Kusano et al., 1998). Both cathepsin K and MMPs such as proMMP-1 are detectable in the subosteoclastic compartment (Everts et al., 1992; Delaisse et al., 1993; Everts et al., 1998). Recently, cathepsins, not collagenases, have been suggested to be responsible for the resorption of long enchondral bones, such as in loosening of hip implants (Everts et al. 1999; Konttinen et al. 2001). However, both cathepsins and certain collagenases are required for osteoclastic resorption of calvarial/ membranous bone (Everts et al., 1999). Unfortunately, no report exists on the eventual presence of cathepsin K in peri-implant sulcus fluid or gingival crevicular fluid. In contrast to cathepsin K, cathepsin C has been found in chronic periodontitis tissue (Soell et al., 2002).
Collagenase-3 is required for the migration of pre-osteoclasts during the development of the bone marrow cavity in long bones (Blavier et al., 1995). It contributes to the
51
degradation of unmineralized bone matrix on the bone surface, which is assumed to be the first step in bone resorption (Uchida et al., 2001). Increased expression of collagenase-3 has been suggested to be typical for foreign body reactions, which probably contributes to aseptic loosening of total hip implants (Imai et al., 1998). The elevated collagenase-3 activity in gingival crevicular fluid associated with bone loss suggests that it may contribute to bone collagen degradation in chronic periodontitis (Golub et al., 1997). These observations may explain why, in our patients with advanced vertical bone loss, collagenase-3 levels in PISF were high. It remains unclear, however, if and how collagenase-3 or any of the neutral MMPs contributes to bone loss.
The role of collagenase-2 in bone resorption is debatable. It was first found in polymorphonuclear neutrophilic leukocytes (Lazarus et al., 1968), and later was also detected in many other cell types. It has been described in periodontal ligament cells (Salo et al., 1995), articular chondrocytes (Cole et al., 1996), synovial fibroblasts and endothelial cells (Hanemaaijer et al., 1997), odontoblasts, and dental pulp cells (Palosaari et al., 2000). Collagenase-2 is also expressed in chicken and rat osteoclasts, but not in human osteoclasts (Sorsa et al., 1998).
Rats have collagenase-2 and -3, but contrary to earlier belief, they lack collagenase-1 (MMP-1). Such tetracycline analogs, which inhibit MMPs, have been found to reduce bone destruction in a model in which rat osteoclasts digest bovine bone. This implies that collagenase-2 or -3 or both are involved in bone resorption (Greenwald et al., 1998). Collagenase-2 is related to many developmental and metabolic bone diseases, and is required for the normal development of mandibles and hind limbs in rats (Sasano et al., 2002). Collagenase-2 in GCF has been studied in both adult and juvenile periodontitis (Ingman et al., 1993); its activity in GCF is typical for chronic periodontitis, and its activity levels correlate with periodontal bone loss (Sorsa et al., 1988; Lee et al., 1995; Romanelli et al., 1999). Relatively high collagenase-2 levels occur in PISF around loosening implants compared to those in well-fixed implants (Teronen et al., 1997). These observations have now been extended by our demonstration that collagenase-2 levels in PISF correlated with degree of vertical bone loss.
Gelatinases (gelatinase-A and B) form a sub-group of the MMP family. Gelatinase-B/MMP-9, but not gelatinase-A/MMP-2, is expressed by human osteoclasts (Wucherpfennig et al., 1994; Okada et al., 1995). Logically, gelatinase-B has been recently found to be involved in bone remodeling (Delaisse et al., 2000). It is involved with the recruitment of osteoclasts to resorption sites (Blavier and Delaisse, 1995). Gelatinase-B from osteoclasts proteolytically activates transforming growth factor-beta, which is deposited in the bone matrix and plays a regulatory role in bone remodeling (Dallas et al., 2002).
52
Gelatinase-B/MMP-9 degrades cathepsin-produced multiple collagen fragments and collagenase-produced 3/4 and 1/4 collagen fragments, which have been spontaneously denatured to gelatin (Birkedal-Hansen 1995; Kusano et al. 1998). Gelatinase-B is a cooperative enzyme acting in concert with collagenases in collagen degradation. Furthermore, gelatinase-B has been found to remove bone collagen remnants left by osteoclasts in resorption lacunae. This is an obligatory step in the linkage between bone resorption and bone formation (Delaisse et al., 2000; Everts et al., 2002). In other words, gelatinase-B is important for the activation-resorption-formation cycle (ARF cycle) (Lassus et al., 1998). Quite in line with these observations, it has been reported that a specific synthetic gelatinase inhibitor prevents bone resorption (Hill etal., 1994).
Gelatinase-B exists in many immigrant and resident cells. In chronic periodontitis, polymorphonuclear neutrophilic leukocytes, monocyte/macrophages, and keratinocytes produce gelatinase-B (Salo et al., 1991; Westerlund et al., 1996), and is also expressed by odontoclasts, which participate in deciduous root resorption (Linsuwanont et al., 2002). In this work, gelatinase-B levels were associated with the extent of peri-implant bone loss. Future studies should evaluate the true prognostic value of the markers identified and the effect of therapeutic interventions targeting them.
9.2 Gingival index and peri-implant bone lossGingival index, a useful clinical periodontal index used in the diagnosis of gingivitis (Löe, 1967; Ainamo and Bay, 1975), is helpful for evaluation of degree of inflammation in gingival tissue in gingivitis and chronic periodontitis (Löe, 1967; Ainamo and Bay, 1975). Gingival index has been modified to make it suitable for assessment of inflammation around dental implants (Chaves et al., 1993; Mombelli etal., 1987), and both gingival index and the modified gingival index serve to describe and quantitate disease activity (Ciancio et al., 1986). The value of the gingival index may be affected by many factors and changes in terms of time and stages of disease.
Compared to gingival index, peri-implant vertical bone loss is an important measure of disease outcome, which is quite stable. This is a pathological result of all kinds of implant risk factors and mechanisms. It is generally accepted that peri-implant bone loss is related to adverse biological host responses together with cyclic occlusal loading and oral bacterial pathogens (Gross, 1988; Swanberg and Henry, 1995; Leonhardt et al., 1999; Santavirta 1999). Because gingival index reflects gingival inflammation, which is generally caused by bacterial pathogens, a high gingival index may not be related to high peri-implant vertical bone loss. Indeed, it was observed in this study that gingival index did not correlate with peri-implant boss loss.
In contrast, in another study, a high gingival index was positively correlated in many peri-implantitis affected patients with bone vertical resorption (Mombelli et al., 1987; Luterbacher et al., 2000). Gingival index is a useful clinical criterion, but the

53
relationship between gingival index and peri-implant bone loss is not yet clear. Mechanical peri-implant bone loss, not necessarily reflected in gingival index, should not be neglected (Redlich et al., 2001; Engquist et al., 2002), because abnormal mechanical loading may have serious consequences for implant patients. Prevention of peri-implant bone loss is thus a key question in dental implantology, because peri-implant bone is the strongest tissue among all peri-implant support tissues (Albrektsson et al., 1986).
Our current view on mechanical bone loss is that it is induced by multiple bone-destructive proteinases. High mechanical forces induce osteocytes to produce cathepsin K and collagenase-1 (Kurata et al., 2001; Redlich et al., 2001). Both cysteine proteinases and MMPs are required for bone resorption (Everts et al., 1992; Everts et al., 1998). Especially cathepsin K inhibitors have been intensively developed for treatment of diseases associated with bone and cartilage destruction (Votta et al., 1997). Chemically modified tetracyclines are now available, which have been shown to have anti-MMP features (Golub et al., 1987; Golub et al., 1998; Ramamurthy et al., 2002). Such drugs might offer a good choice for implant patients in the future. Dentists are already paying attention to underlying bone loss around those implants also used in patients with a low gingival index.
Collagenase-3/MMP-13, collagenase-2/MMP-8, and gelatinase-B/MMP-9 were well correlated in this study with irreversible peri-implant vertical bone loss. Measurements of collagenase-3 and collagenase-2 or gelatinase-B in PISF could therefore sever as biomarkers to indicate the degree of peri-implant vertical bone loss. These findings offer new insights into the pathomechanisms contributing to loosening of dental implants, although the exact site and mode of action remain unclear.
9.3 Gingival index and gelatinase-BIt is generally assumed that a similar pathological process is shared by chronic periodontitis and loosening of dental implants (Meffert, 1996). The main clinical symptoms are quite similar. These are an enhanced probing pocket depth or implant pocket depth, bleeding on probing, and increasing tooth or implant mobility (Mombelli et al., 1987; O'Reilly and Claffey, 1996). Besides gingival index, many other clinical indices have been established in periodontology, including plaque index (Silness and Löe, 1964), periodontal index (Russell, 1967), and periodontal disease index (Ramfjord, 1967). Some of the periodontal indices have been further modified and introduced to implantology (Mombelli et al., 1987; Luterbacher et al., 2000). They are useful in the evaluation of degree of peri-implantitis in the clinic and in research and are used in clinical trials.
In addition to indices, molecular medicine has dramatically developed in the past three decades. Currently, some new molecular diagnostic markers identified in laboratories are being introduced as clinical chair-side tests (Sorsa et al., 1999; Mancini et al., 1999). Gelatinase B/MMP-9 has not been analyzed in such a clinical
54
setting. In vivo activated gelatinase-B/MMP-9 levels in PISF seem to be reflected in gingival index when it is higher than 0.5. This combination of gingival index and gelatinase-B may help clinical dentists in recognition of patients at risk for peri-implant bone loss.
9.4 Collagenase-cleaved type I collagen fragment and chronic periodontitisIt is widely accepted that degradation of type I collagen during periodontitis progression is mediated through mammalian proteinases, not bacterial enzymes (Sorsa et al., 1992; van der Zee et al., 1997; Sorsa et al., 1999). Pathogenic bacteria have been reported to affect host cells, which are producing proteinases at four levels. Bacterial components are chemotactic and induce host cells to produce chemokines (Miller et al., 1975). Polymorphonuclear leukocytes release MMPs when bacteria are phagocytosed (Ding et al., 1997). Bacterial membrane can induce polymorphonuclear leukocytes to produce MMPs (Ding et al., 1996). The bacterial proteinases activate proMMPs, which is a rate-limiting step (Sorsa et al., 1992; Okamoto et al., 1997). No direct evidence has been available, however, on actual collagenlysis mediated by the classical mammalian collagenases.
Collagenase-cleaved type I collagen neoepitope/COL1-3/4C staining was detected in the matrix associated with the sulcular and junctional epithelium. Collagenase-1 is not found in periodontal pocket epithelium (Woolley and Davies, 1981; Ingman et al., 1996), but collagenase-2 and collagenase-3 have been detected in the pocket epithelium (Uitto et al. 1998; Tervahartiala et al., 2000). Collagenases produced in the pocket epithelium seem to become activated and to be able to cleave across the collagen fibril triple helices. Apparently, they overcome their endogenous proteinase inhibitor (TIMP) shield. This is important for the formation and progression of periodontal pockets as assessed from the microanatomical location of the COL1-3/4C neoepitope.
COL1-3/4C staining was detected in the matrix surrounding some of the fibroblasts. Fibroblasts produce low levels of collagenase-1 (Kubota et al., 1996; Dahan et al.,2001). Collagenase-2 has not been found in gingival fibroblasts, but has been described in periodontal ligament fibroblasts (Salo et al., 1995). Collagenase-3 is expressed by gingival fibroblasts (Uitto et al., 1998; Tervahartiala et al., 2000). These results imply that collagenases produced by some of the interstitial fibroblasts can contribute to local and pericellular collagenolysis.
COL1-3/4C staining was discovered in the interstitial matrix infiltrated by inflammatory cells, and much of the interstitial collagen was destroyed in such inflammatory areas. This is compatible with findings describing collagenases in monocytes/macrophages. Collagenase-1 was found in macrophages in the 1970's (Wahl et al., 1974). Collagenase-2 and -3 mRNA and the corresponding enzyme proteins have been detected in monocyte/macrophage-like cells (Uitto et al., 1998; Tervahartiala et al., 2001). Collagenase-2 among the three collagenases is the most
55
effective collagenase in the cleavage of type I collagen (Hasty et al., 1987). Pro-collagenases which have accumulated in the extracellular matrix can become locally activated and lead to collagen-fibril destruction (van der Zee et al., 1996). Almost 70% of the collagen in gingival tissue is degraded in one inflammation cycle (Bartold et al., 2000). Direct morphological evidence is now reported here for the first time demonstrating that collagenases mediate collagen-fibril breakdown in gingival tissue in chronic periodontitis.
9.5 Cellular fibronectin in chronic periodontitis and looseningResearch on extracellular matrix and proteolytic enzymes has changed our views on periodontitis. One of the serine proteinases is human neutrophil elastase. Elastase activities in gingival crevicular fluid and in the saliva of chronic periodontitis patients are significantly increased compared with activities in healthy controls, but they decrease in GCF after periodontal treatments such as scaling, root planning, and curettage (Ingman et al., 1994). The increased elastase levels in GCF and saliva have been proposed as useful biochemical markers to monitor the course and treatment of chronic periodontitis (Ingman et al., 1994; Uitto et al., 1996).
Every enzyme shows some substrate specificity. Elastase in vivo has been able to degrade fibronectin to fibronectin fragments (McDonald et al., 1992). Cellular fibronectin staining was in our study found in gingival connective tissue. Elastase-positive cells have been also found in gingival tissue (Ingman et al., 1994). It has been tentatively considered to be the main proteolytic enzyme responsible for the degradation of fibronectin in skin wounds (Grinnell and Zhu, 1996; Herrick et al., 1997). It removes fibronectin from human basement membranes, as has been shown by an electron microscopic study (Morris et al., 1993; Bonnefoy and Legrand, 2000). A conclusion which might be drawn from these previous studies and the present study is that the decreased staining of cellular fibronectin may be the result of increased elastase activity. This is supported by previous studies of biochemical markers in GCF, which found high levels of fibronectin fragments in GCF at periodontal disease sites. The level of fragments decreased after periodontal treatment (Lopatin et al., 1989; Talonpoika et al., 1989). These findings, together with the present quantitative morphometric results, suggest that increased human neutrophil elastase activities in GCF and cellular fibronectin fragments may prove useful markers for progressive connective tissue degradation in chronic periodontitis. This relationship between elastase and cellular fibronectin staining probably explains the decreased cellular fibronectin in chronic periodontitis.
Elastase activities were not up-regulated in PISF or saliva, not even in severe peri-implantitis. Overexpression of cellular fibronectin around loosening dental implants would seem to be due to increased local synthesis combined with relatively modest degradation. In fibroblast cell culture, titanium (Ti) can significantly enhance expression of cell fibronectin (Chou et al., 1996). Cellular fibronectin staining was higher in loosening of our dental implants. To evaluate this in some depth, we

56
compared our findings with some studies of aseptic loosening of total hip replacements. Elastase activity is increased in interface tissue extracts and joint fluid (Takagi et al., 1995). Expression of cellular fibronectin is not decreased, but increased in interface tissues (Li et al., 2000). It seems that, in aseptic loosening of totally replaced hips, the stimulators of cellular fibronectin synthesis greatly surpass the influences of proteinase-mediated degradation. The difference between loosening of dental implants and aseptic loosening of totally replaced hips is that there are many more foreign bodies (debris) around loosening hip implants than around the loosening dental implants. The (sub)micron-size particles around the hip arise as a result of cyclic loading (=walking) and friction and abrasion between the gliding surfaces of the head of the femoral stem and the acetabular cup (Campbell et al., 1995). It has been calculated that in a metal-to-(conventional) polyethylene joint composite, more than 100,000 particles of ultra-high molecular weight polyethylene (Wagner and Wagner, 2001) are formed at every step and that normally a patient takes about more than 106 steps per year (Silva et al., 2002). The number of particles has been found to range from 8.5 x 108 to 5.7 x 1011 per gram of dry tissue weight (Vaughn et al., 1999). Changes in extracellular matrix are considered a reflection of cellular history and initiate various cascades (Nathan et al., 1991). Increased expression of cellular fibronectin might be viewed as a result of periprosthetic host responses.
9.6 Osteoclast-stimulating cytokine network in loosening and periodontitisParts of old bone are placed by new bone to maintain bone strength. This is possible due to dynamic bone remodeling cycles (Blair, 1998). The cycle is normally balanced by an essential coupling between bone resorption and formation (Schwartz et al., 1997). Cytokines regulate osteoclast, and osteoblast formation and their functions (Schwartz et al., 1997; Blair, 1998; Raisz, 1999), and can be categorized into osteoclast- and osteoblast-regulating cytokines, although both cells can be affected. Pathological bone resorption is suggested to be driven by an excess of cytokines, which stimulate osteoclasts or inhibit osteoblasts (Oates and Cochran, 1996; Konttinen et al., 1997).
The in vivo working concentrations of cytokines on osteoclasts are not yet known. The fact that osteoclast-stimulating cytokines can be visualized using a staining method has been established in our laboratory (Konttinen et al., 1997; Xu et al. 2000). When TNF- , IL-1 , IL-6, PDGF-A, and TGF- were studied in loosening of dental implants and in chronic periodontitis, TNF- , IL-1 , and IL-6 were increased in loosening of dental implants and in chronic periodontitis. Titanium stimulates release of IL-1 , IL-6, and TNF- from macrophages and fibroblasts (Manlapaz et al., 1996; Wang et al., 1996). Foreign body giant cells were seen in peri-implantitis. If macrophages encounter an implant and/or particles too large to be phagocytosed, they form foreign body giant cells (Mariano and Spector, 1974). These foreign body giant cells seem to have a high capacity to produce osteoclast-stimulating cytokines. All the foreign body giant cells always contained all of the osteoclast-stimulating cytokine analyzed. As to cytokine profile, chronic periodontitis and peri-implantitis were quite
57
similar, but not completely identical. Both are characterized by a progressive loss of bone support tissue.
Overlapping effects may be necessary to guarantee efficient osteolysis (Goldring and Goldring, 1996). TNF- stimulates the production of IL-1 and IL-6. IL-1 has been considered particularly important in osteolysis during loosening. TNF- has already been studied in chronic periodontitis (Lindemann et al., 1988; Tervahartiala et al., 2001). Because cytokine expression in peri-implantitis is limited to IL-1 , TNF- ,and IL-6, peri-implantitis might be particularly amenable to treatment with biological cytokine modulators like IL-1 receptor antagonist, TNF- antibodies, or soluble TNF-receptors (Graves, 1999). In chronic periodontitis and peri-implantitis, it may be possible to manage with a local application to the gingival and peri-implant pockets, perhaps using carriers enabling prolonged and/or controlled local release.
Although some new and interesting findings were made in this thesis study, the limitations of the small sample size should be taken into consideration. Samples were obtained from patients representing regular dental implant surgery patients. Although they are representative, they still represent a small sample population. On the other hand, in the interpretation generally accepted statistical methods were used, and they take the uncertainty caused by the small sample size into consideration. Still, confirmation of these findings by other groups is needed and further research with larger sample size and refined methods will provide valuable information.
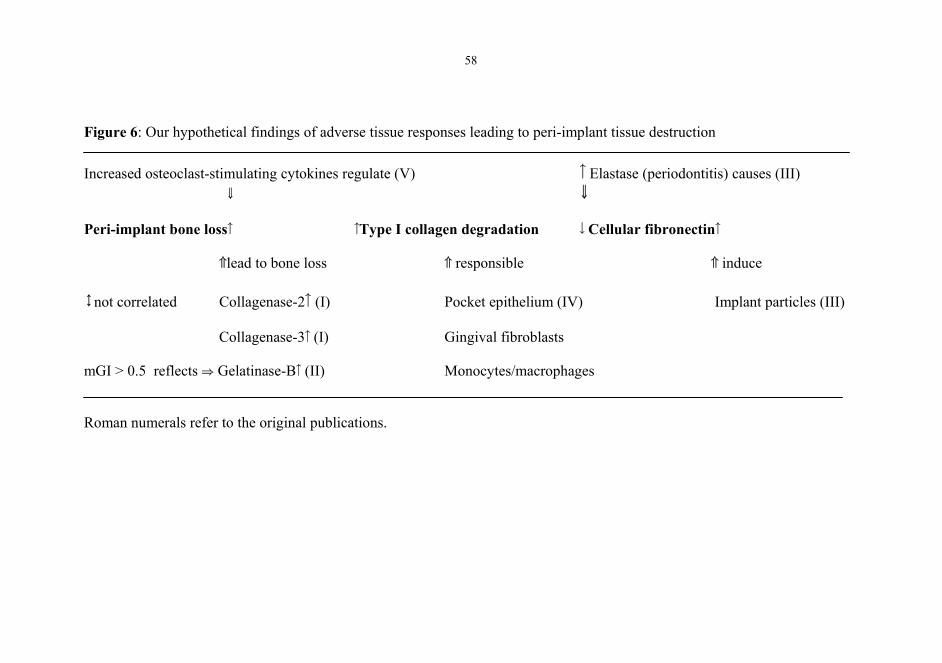
58
Figure 6: Our hypothetical findings of adverse tissue responses leading to peri-implant tissue destruction
Increased osteoclast-stimulating cytokines regulate (V) Elastase (periodontitis) causes (III)
Peri-implant bone loss Type I collagen degradation Cellular fibronectin
lead to bone loss responsible induce
not correlated Collagenase-2 (I) Pocket epithelium (IV) Implant particles (III)
Collagenase-3 (I) Gingival fibroblasts
mGI > 0.5 reflects Gelatinase-B (II) Monocytes/macrophages
Roman numerals refer to the original publications.
59
SUMMARY AND CONCLUSIONS
Loosening of dental implants is an important problem. Bioincompatible implant materials constitute one of the important risk factors which cause an adverse host response in peri-implant tissues. Adverse host responses lead to activation of multiple biological and pathological cascades. The pathological feature is the progressive loss of peri-implant support tissues. Many proteolytic enzymes participate in the process.
Major conclusions: I. Collagenase-3/MMP-13 and collagenase-2/MMP-8 in peri-implant sulcus fluid, produced by adjacent bone osteoclast cells, neutrophils, and mesenchymal cells, reflect irreversible peri-implant vertical bone loss around loosening dental implants. Measurements of collagenase-3 and/or collagenase-2 could serve as markers to indicate the degree of peri-implant vertical bone loss.
II. Gelatinase-B/MMP-9 is associated with peri-implant bone loss. Activation of gelatinase-B/MMP-9, together with elevated modified gingival index (> 0.5), eventually reflect active phases of peri-implantitis. These may prove to be diagnostically useful indicators.
III. In the immunohistochemical expression of cellular fibronectin in loosening of dental implants and chronic periodontitis, distinct quantitative differences exist. These differences suggest that different pathomechanisms are operative in loosening of dental implants and natural teeth. It is necessary to improve the biocompatibility of dental implant materials and to better understand the pathomechanisms of loosening to be able to improve the long-term results for dental implants.
VI. Expression of collagenase-cleaved collagen neoepitopes suggests that the host-cell-derived collagenases are able to cleave across the triple helical collagen fibrils in situ. Collagenases become activated and overcome their endogenous tissue inhibitors at the sulcular and junctional epithelial attachment and monocyte/macrophage-infiltrated areas. Collagenases may contribute to the initiation and progression of periodontal tissue destruction or attachment loss with deepening of periodontal pockets in chronic periodontitis.
V. The osteoclast-activating cytokine network (TNF- , IL-1 , IL-6, PDGF-A, and TGF- ) was activated in both peri-implantitis and chronic periodontitis, but the cytokine profiles differed. During loosening of dental implants, this activation may contribute to peri-implant bone loss and may be an amenable target for local therapies with cytokine modulators.
60
ACKNOWLEDGEMENTS
This study was supported by the Biomaterial and Tissue Engineering Graduate School, the Finnish Center for the Advancement of Technology, the Finska Läkaresällskapet, the Finnish Dental Society Apollonia, the Sigrid Juselius Foundation, the Willhelm and Else Stockmann Foundation, the University of Helsinki, the Academy of Finland, grant for the center of excellence "Biomaterials and Guided Tissue Regeneration", and Clinical EVO Research Grants. I believe that this thesis would not have been possible without their financial assistance. I would like to sincerely express my gratitude to all these agencies.
The work was carried out at the Department of Anatomy, University of Helsinki; the Department of Medicine/ Invärtes medicin, University Central Hospital and ORTON Orthopaedic Hospital, Invalid Foundation.
I would like to thank to Professor Ismo Virtanen, MD, PhD, Chairman of the Department of Anatomy, University of Helsinki. I know that he has been a pioneer and productive researcher and a respected professor during all these years. He is such a kind man that he never shows a “professor-style” to anyone, including me, a foreign student. This does not destroy his prestige as a famous professor in my heart, but only increases my respect for him and his working manner. I want to thank him for having supplied us with the antibodies which made it possible to conduct one of these studies.
I would like to sincerely thank my supervisor Professor Yrjö T. Konttinen, MD, PhD, for his guidance and encouragement of my work. He has really wide knowledge, from clinical medicine to molecular biology, from dental science to internal medicine. He shows a high capability to deal logically with everything. He usually takes a strategically advantageous position in selecting a research topic. He has broad and long-term views in managing the whole group. At the same time, he never feels tired and stops working. He pays attention to details, so many mistakes were avoided due to his work. I would like to thank him for assistance in writing the articles and thesis.
My supervisor Professor Seppo Santavirta, MD, PhD, is a clever, elegant, gentle man. He is usually calm when he listens, and talks in a refined manner when he is discussing. He is a modest and kind man, as well. From all these characteristics, you can clearly realize the kind of firm confidence in his heart which has helped me to overcome all kinds of difficulties and to finish my thesis. I would also like to honestly express my gratitude to him as my supervisor, for his guidance throughout my work during these years.
My sincere thanks go to Professor Timo Sorsa, DDS, PhD, the most important co-author. It was he who introduced me into the area of MMPs. I really appreciate his vast knowledge and skill in periodontal diseases and MMP research. I am truly indebted to him for his advice and suggestions during these years.
61
My sincere thanks are offered to all co-workers on the original publications for their expertise and contribution to the research presented in this thesis. I am indebted to Professor Roeland Hanemaaijer, PhD, of the Gaubius Laboratory, Leiden, the Netherlands, Dr. Ville Husa, DDS, Prof. Mauno Könönen, DDS, PhD, Dr. Pekka Laine, DDS, Prof. Rejo Lappalainen, MSc, PhD, Prof. Christian Lindqvist, DDS, PhD, Dr. Hanne Rönkä, PhD, Prof. Tuula Salo, DDS, PhD, and Docent Olli Teronen, DDS, PhD.
I would like to thank for their constructive criticism and valuable comments on the thesis manuscript the official reviewers, Professor Panos N. Papapanou DDS, PhD, and Docent Juha Nevalainen, MD, PhD.
Dr. Carol Norris, PhD, is acknowledged for author-editing the thesis and her valuable suggestions on academic writing and editing.
I really owe my great gratitude to my wife WenWen Li and my whole family, including my parents Dr. ZongYang Ma and YuYi Zhan, my sister PeiHong Zhan, for their understanding about my leaving during all these years and for their encouragement to prepare this thesis. I thank my other relatives, Dr. ShuYi Ma, Dr. ShaoQi Han, Dr. XiaoYan Han, and Ms XiaoHong Han, for their help and continue support for so many years.
I must warmly acknowledge all TULES (an abbreviation for musculoskeletal disorders in Finnish) research group members and staff at the Department of Anatomy who have helped and given me technical assistance throughout my PhD thesis program. They are Mari Ainola, MSc, Hillevi Boman, BSc, Tong Chen, PhD, Erkki Hänninen, BSc, Ms Paula Hasenson, Mika Hukkanen, PhD, Eija Kaila, BSc, Pipsa Kaipainen, BSc, Kirsti Kari, MSc, Mr Reijo Karppinen, Ms Marjatta Kivekäs, TianFang Li, PhD, Mikko Liljeström, BSc, Zygmunt Mackiewicz, PhD, Mari Määttä, BSc, Sirkku Niissalo, DDS, Outi Rauanheimo, BSc, Nina Santavirta, PhD, Svetlana Solovieva, PhD, Taina Tervahartiala-Saarinen, PhD, and JingWen Xu, PhD.
I would like to thank all the PhD students in the TULES group. I believe that they will be successful in their study and research. They are Ali Ahmed, DDS, Arzu Beklen, DDS, Robert Björkenheim, MB, Uula Kitti, DDS, Lisa Konttinen, MSc, Mikael Laine, DDS, Lauri Lindroos, MD, GuoFeng Ma, MD, Jami Mandelin, MSc, Laura Ojala, MSc, Pauliina Porola, MSc, Pasi Ruuttila, MSc, Eve-Kai Tensing, MD, Eero Waris, MD, and Ville Waris, MD.
Bless you, TULES!
Jian Ma 2004, Helsinki
62
REFERENCES
Adell R (1985). Tissue integrated prostheses in clinical dentistry. Int Dent J 35:259-265. Aimes RT, Quigley JP (1995). Matrix metalloproteinase-2 is an interstitial collagenase. Inhibitor-free
enzyme catalyzes the cleavage of collagen fibrils and soluble native type I collagen generating the specific 3/4- and 1/4-length fragments. J Biol Chem 270:5872-5876.
Ainamo J, Bay I (1975). Problems and proposals for recording gingivitis and plaque. Int Dent J 25:229-235.
Albert FE, Bergeron CA (1998). Endopore: a new generation of implants. J Can Dent Assoc 64:370-373.
Albrektsson T, Zarb G, Worthington P, Eriksson AR (1986). The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants1:11-25.
Albrektsson T (2001). Is surgical skill more important for clinical success than changes in implant hardware? Clin Implant Dent Relat Res 3:174-175.
Annual Industry Report (2000). Implant Dent 9:192-194. Alpar B, Leyhausen G, Sapotnick A, Gunay H, Geurtsen W (1998). Nicotine-induced alterations in
human primary periodontal ligament and gingiva fibroblast cultures. Clin Oral Investig 2:40-46.
Aspenberg P, Anttila A, Konttinen YT, Lappalainen R, Goodman SB, Nordsletten L, et al. (1996). Benign response to particles of diamond and SiC: bone chamber studies of new joint replacement coating materials in rabbits. Biomaterials 17:807-812.
Babbush CA, Shimura M (1993). Five-year statistical and clinical observations with the IMZ two-stage osteointegrated implant system. Int J Oral Maxillofac Implants 8:245-253.
Bagambisa FB, Kappert HF, Schilli W (1994). Cellular and molecular biological events at the implant interface. J Craniomaxillofac Surg 22:12-17.
Barber HD, Seckinger RJ, Silverstein K, Abughazaleh K (1996). Comparison of soft tissue healing and osseointegration of IMZ implants placed in one-stage and two-stage techniques: a pilot study. Implant Dent 5:11-14.
Bartold PM, Walsh LJ, Narayanan AS (2000). Molecular and cell biology of the gingiva. Periodontol 2000 24:28-55.
Batge B, Diebold J, Stein H, Bodo M, Muller PK (1992). Compositional analysis of the collagenous bone matrix. A study on adult normal and osteopenic bone tissue. Eur J Clin Invest 22:805-812.
Baum BJ, Moss J, Breul SD, Crystal RG (1978). Association in normal human fibroblasts of elevated levels of adenosine 3':5'-monophosphate with a selective decrease in collagen production. JBiol Chem 253:3391-3394.
Becker W, Hujoel PP, Becker BE, Willingham H (2000). Osteoporosis and implant failure: an exploratory case-control study. J Periodontol 71:625-631.
Berge TI. (2000) Public awareness, information sources and evaluation of oral implant treatment in Norway. Clin Oral Implants Res 11:401-408.
Bhide VM, Smith L, Overall CM, Birek P, McCulloch CA (2000). Use of a fluorogenic septapeptide matrix metalloproteinase assay to assess responses to periodontal treatment. J Periodontol71:690-700.
Bienkowski RS, Baum BJ, Crystal RG (1978). Fibroblasts degrade newly synthesised collagen within the cell before secretion. Nature 276:413-416.
Billinghurst RC, Dahlberg L, Ionescu M, Reiner A, Bourne R, Rorabeck C, et al. (1997). Enhanced cleavage of type II collagen by collagenases in osteoarthritic articular cartilage. J Clin Invest99:1534-1545.
Birkedal-Hansen H, Butler WT, Taylor RE (1977). Proteins of the periodontium. Characterization of the insoluble collagens of bovine dental cementum. Calcif Tissue Res 23:39-44.
Birkedal-Hansen H, Moore WG, Bodden MK, Windsor LJ, Birkedal-Hansen B, DeCarlo A, et al.(1993). Matrix metalloproteinases: a review. Crit Rev Oral Biol Med 4:197-250.

63
Birkedal-Hansen H (1995). Proteolytic remodeling of extracellular matrix. Curr Opin Cell Biol 7:728-735.
Blair HC, Teitelbaum SL, Ghiselli R, Gluck S (1989). Osteoclastic bone resorption by a polarized vacuolar proton pump. Science 245:855-857.
Blair HC (1998). How the osteoclast degrades bone. Bioessays 20:837-846. Blavier L, Delaisse JM (1995). Matrix metalloproteinases are obligatory for the migration of
preosteoclasts to the developing marrow cavity of primitive long bones. J Cell Sci 108:3649-3659.
Bonnefoy A, Legrand C (2000). Proteolysis of subendothelial adhesive glycoproteins (fibronectin, thrombospondin, and von Willebrand factor) by plasmin, leukocyte cathepsin G, and elastase. Thromb Res 98:323-332.
Borgogna E, Re F, Re G, Torreri S (1984). Maxillofacial injuries in sports: boxing. Minerva Stomatol33:203-207.
Brånemark PI, Hansson BO, Adell R, Breine U, Lindstrom J, Hallen O, et al. (1977). Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl 16:1-132.
Brew K, Dinakarpandian D, Nagase H (2000). Tissue inhibitors of metalloproteinases: evolution, structure and function. Biochim Biophys Acta 1477:267-283.
Brinckerhoff CE, Matrisian LM (2002). Matrix metalloproteinases: a tail of a frog that became a prince. Nat Rev Mol Cell Biol 3:207-214.
Brill N (1962). The gingival pocket fluid. Studies of its occurrence, composition, and effect. Acta Odontol Scand 32: 20.
Brocard D, Barthet P, Baysse E, Duffort JF, Eller P, Justumus P, et al. (2000). A multicenter report on 1,022 consecutively placed ITI implants: a 7-year longitudinal study. Int J Oral Maxillofac Implants 15:691-700.
Bromme D, Okamoto K, Wang BB, Biroc S (1996). Human cathepsin O2, a matrix protein-degrading cysteine protease expressed in osteoclasts. Functional expression of human cathepsin O2 in Spodoptera frugiperda and characterization of the enzyme. J Biol Chem 271:2126-2132.
Brosh T, Persovski Z, Binderman I (1995). Mechanical properties of bone-implant interface: an in vitro comparison of the parameters at placement and at 3 months. Int J Oral Maxillofac Implants10:729-735.
Buchs AU, Hahn J, Vassos DM (1996). Efficacy of threaded hydroxyapatite-coated implants placed in the posterior mandible in support of fixed prostheses. Implant Dent 5:106-110.
Buser D, Mericske-Stern R, Bernard JP, Behneke A, Behneke N, Hirt HP, et al. (1997). Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin Oral Implants Res 8:161-172.
Buser D, von Arx T, ten Bruggenkate C, Weingart D (2000). Basic surgical principles with ITI implants. Clin Oral Implants Res 11 Suppl 1:59-68.
Buser D, Ingimarsson S, Dula K, Lussi A, Hirt HP, Belser UC (2002). Long-term stability of osseointegrated implants in augmented bone: a 5-year prospective study in partially edentulous patients. Int J Periodontics Restorative Dent 22:109-117.
Butler WT, Birkedal-Hansen H, Beegle WF, Taylor RE, Chung E (1975). Proteins of the periodontium. Identification of collagens with the [alpha1(I)]2alpha2 and [alpha1(III)]3 structures in bovine periodontal ligament. J Biol Chem 250:8907-8912.
Butterfield KJ, Dagenais M, Clokie C (1997). Linear tomography's clinical accuracy and validity for presurgical dental implant analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod84:203-209.
Callan DP, Hahn J, Hebel K, Kwong-Hing A, Smiler D, Vassos DM, et al. (2000). Retrospective multicenter study of an anodized, tapered, diminishing thread implant: success rate at exposure. Implant Dent 9:329-336.
Campbell P, Ma S, Yeom B, McKellop H, Schmalzried TP, Amstutz HC (1995). Isolation of predominantly submicron-sized UHMWPE wear particles from periprosthetic tissues. JBiomed Mater Res 29:127-131.
64
Canalis E, Delany AM (2002). Mechanisms of glucocorticoid action in bone. Ann N Y Acad Sci966:73-81.
Caplan DJ, Weintraub JA (1993). The oral health burden in the United States: a summary of recent epidemiologic studies. J Dent Educ 57:853-862.
Carragher NO, Levkau B, Ross R, Raines EW (1999). Degraded collagen fragments promote rapid disassembly of smooth muscle focal adhesions that correlates with cleavage of pp125(FAK), paxillin, and talin. J Cell Biol 147:619-630.
Chapman RJ, Kirsch A (1990). Variations in occlusal forces with a resilient internal implant shock absorber. Int J Oral Maxillofac Implants 5:369-374.
Chaves ES, Wood RC, Jones AA, Newbold DA, Manwell MA, Kornman KS (1993). Relationship of "bleeding on probing" and "gingival index bleeding" as clinical parameters of gingival inflammation. J Clin Periodontol 20:139-143.
Choi BH (2000). Periodontal ligament formation around titanium implants using cultured periodontal ligament cells: a pilot study. Int J Oral Maxillofac Implants 15:193-196.
Chou L, Firth JD, Nathanson D, Uitto VJ, Brunette DM (1996). Effects of titanium on transcriptional and post-transcriptional regulation of fibronectin in human fibroblasts. J Biomed Mater Res31:209-217.
Ciancio SG (1986). Current status of indices of gingivitis. J Clin Periodontol 13:375-8, 381-2. Clapp C, Wheeler JC, Martof AB, Levine PA (1996). Oral squamous cell carcinoma in association with
dental osseointegrated implants. An unusual occurrence. Arch Otolaryngol Head Neck Surg122:1402-1403.
Clavel C, Polette M, Doco M, Binninger I, Birembaut P (1992). Immunolocalization of matrix metallo-proteinases and their tissue inhibitor in human mammary pathology. Bull Cancer 79:261-270.
Cole AA, Chubinskaya S, Schumacher B, Huch K, Szabo G, Yao J, et al. (1996). Chondrocyte matrix metalloproteinase-8. Human articular chondrocytes express neutrophil collagenase. J Biol Chem 271:11023-11026.
Collin HL, Sorsa T, Meurman JH, Niskanen L, Salo T, Ronka H, et al. (2000) Salivary matrix metalloproteinase (MMP-8) levels and gelatinase (MMP-9) activities in patients with type 2 diabetes mellitus. J Periodontal Res 35:259-265.
Cox SW, Eley BM (1992). Cathepsin B/L-, elastase-, tryptase-, trypsin- and dipeptidyl peptidase IV-like activities in gingival crevicular fluid. A comparison of levels before and after basic periodontal treatment of chronic periodontitis patients. J Clin Periodontol 19:333-339.
Craig RG, LeGeros RZ (1999). Early events associated with periodontal connective tissue attachment formation on titanium and hydroxyapatite surfaces. J Biomed Mater Res 47:585-594.
Crubezy E, Murail P, Girard L, Bernadou JP (1998). False teeth of the Roman world. Nature 391:29. Dahan M, Nawrocki B, Elkaim R, Soell M, Bolcato-Bellemin AL, Birembaut P, et al. (2001).
Expression of matrix metalloproteinases in healthy and diseased human gingiva. J Clin Periodontol 28:128-136.
Dallas SL, Rosser JL, Mundy GR, Bonewald LF (2002). Proteolysis of latent transforming growth factor-beta (TGF-beta )-binding protein-1 by osteoclasts. A cellular mechanism for release of TGF-beta from bone matrix. J Biol Chem 277:21352-21360.
Davidoff SR. The dental implant home page. http://www.dental-implants.com/ Delaisse JM, Vaes G. In Biology and Physiology of the Osteoclast. eds. Rifkin BR, Gay CV; CRC
Press, Boca Raton,FL; p289-314, 1992. Delaisse JM, Eeckhout Y, Neff L, Francois-Gillet C, Henriet P, Su Y, et al. (1993). (Pro)collagenase
(matrix metalloproteinase-1) is present in rodent osteoclasts and in the underlying bone-resorbing compartment. J Cell Sci106 :1071-1082.
Delaisse JM, Engsig MT, Everts V, del Carmen Ovejero M, Ferreras M, Lund L, et al. (2000) Proteinases in bone resorption: obvious and less obvious roles. Clin Chim Acta 291:223-234.
Dental Implants: Benefit and Risk. NIH Consens Statement 1978, 1:13-19. http://consensus.nih.gov/cons/003/003_statement.htm Dental implants. NIH Consens Statement online 1988, 7: 1-22.
http://consensus.nih.gov/cons/069/069_statement.htm
65
DiFranza JR, Librett JJ (1999). State and federal revenues from tobacco consumed by minors. Am J Public Health 89:1106-1108.
Ding Y, Uitto VJ, Haapasalo M, Lounatmaa K, Konttinen YT, Salo T, et al. (1996). Membrane components of Treponema denticola trigger proteinase release from human polymorphonuclear leukocytes. J Dent Res 75:1986-1993.
Ding Y, Haapasalo M, Kerosuo E, Lounatmaa K, Kotiranta A, Sorsa T (1997). Release and activation of human neutrophil matrix metallo- and serine proteinases during phagocytosis of Fusobacterium nucleatum, Porphyromonas gingivalis and Treponema denticola. J Clin Periodontol 24:237-248.
Domon S, Shimokawa H, Matsumoto Y, Yamaguchi S, Soma K (1999). In situ hybridization for matrix metalloproteinase-1 and cathepsin K in rat root-resorbing tissue induced by tooth movement. Arch Oral Biol 44:907-915.
Douglass CW, Jette AM, Fox CH, Tennstedt SL, Joshi A, Feldman HA, et al. (1993). Oral health status of the elderly in New England. J Gerontol 48:M39-46.
Drago CJ (1992). Rates of osseointegration of dental implants with regard to anatomical location. JProsthodont 1:29-31.
Drake FH, Dodds RA, James IE, Connor JR, Debouck C, Richardson S, et al. (1996). Cathepsin K, but not cathepsins B, L, or S, is abundantly expressed in human osteoclasts. J Biol Chem271:12511-12516.
Dula K, Mini R, van der Stelt PF, Buser D (2001). The radiographic assessment of implant patients: decision-making criteria. Int J Oral Maxillofac Implants 16:80-89.
Duyck J, Naert I (1998). Failure of oral implants: aetiology, symptoms and influencing factors. Clin Oral Investig 2:102-114.
Eckert SE, Meraw SJ, Cal E, Ow RK (2000). Analysis of incidence and associated factors with fractured implants: a retrospective study. Int J Oral Maxillofac Implants 15:662-667.
Eeckhout Y, Vaes G (1977). Further studies on the activation of procollagenase, the latent precursor of bone collagenase. Effects of lysosomal cathepsin B, plasmin and kallikrein, and spontaneous activation. Biochem J 166:21-31.
Eder A, Watzek G (1999). Treatment of a patient with severe osteoporosis and chronic polyarthritis with fixed implant-supported prosthesis: a case report. Int J Oral Maxillofac Implants 14:587-590.
Edgerton M, Levine MJ (1993). Biocompatibility: its future in prosthodontic research. J Prosthet Dent69:406-415.
el Askary AS, Meffert RM, Griffin T (1999). Why do dental implants fail? Part I. Implant Dent 8:173-185.
Engel E, Gomez-Roman G, Axmann-Krcmar D (2001). Effect of occlusal wear on bone loss and Periotest value of dental implants. Int J Prosthodont 14:444-450.
Engquist B, Bergendal T, Kallus T, Linden U (1988). A retrospective multicenter evaluation of osseointegrated implants supporting overdentures. Int J Oral Maxillofac Implants 3:129-134.
Engquist B, Astrand P, Dahlgren S, Engquist E, Feldmann H, Grondahl K (2002). Marginal bone reaction to oral implants: a prospective comparative study of Astra Tech and Branemark System implants. Clin Oral Implants Res 13:30-37.
Ericsson I, Nilner K (2002). Early functional loading using Branemark dental implants. Int J Periodontics Restorative Dent 22:9-19.
Esposito M, Hirsch JM, Lekholm U, Thomsen P (1998a). Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. Eur J Oral Sci 106:527-551.
Esposito M, Hirsch JM, Lekholm U, Thomsen P. (1998b) Biological factors contributing to failures of osseointegrated oral implants. (II). Etiopathogenesis. Eur J Oral Sci 106:721-764.
Everts V, Delaisse JM, Korper W, Niehof A, Vaes G, Beertsen W (1992). Degradation of collagen in the bone-resorbing compartment underlying the osteoclast involves both cysteine-proteinases and matrix metalloproteinases. J Cell Physiol 150:221-231.
66
Everts V, van der Zee E, Creemers L, Beertsen W (1996). Phagocytosis and intracellular digestion of collagen, its role in turnover and remodelling. Histochem J 28:229-245.
Everts V, Delaisse JM, Korper W, Beertsen W (1998). Cysteine proteinases and matrix metalloproteinases play distinct roles in the subosteoclastic resorption zone. J Bone Miner Res13:1420-1430.
Everts V, Korper W, Jansen DC, Steinfort J, Lammerse I, Heera S, et al. (1999). Functional heterogeneity of osteoclasts: matrix metalloproteinases participate in osteoclastic resorption of calvarial bone but not in resorption of long bone. FASEB J 13:1219-1230.
Everts V, Delaisse JM, Korper W, Jansen DC, Tigchelaar-Gutter W, Saftig P, et al. (2002). The bone lining cell: its role in cleaning Howship's lacunae and initiating bone formation. J Bone Miner Res 17:77-90.
Franz JT. The results of total hip replacement. (http://www.me.utexas.edu/~uer/hips/index.html) Freeman E (1994) Periodontium. in Oral Histology: Development, Structure, and Function. Richard A.
Ten Cate, Publisher: Mosby pp276. Freije JM, Diez-Itza I, Balbin M, Sanchez LM, Blasco R, Tolivia J, et al. (1994). Molecular cloning
and expression of collagenase-3, a novel human matrix metalloproteinase produced by breast carcinomas. J Biol Chem 269:16766-16773.
Friedlaender GE, Tross RB, Doganis AC, Kirkwood JM, Baron R (1984). Effects of chemotherapeutic agents on bone. I. Short-term methotrexate and doxorubicin (adriamycin) treatment in a rat model. J Bone Joint Surg Am 66:602-607.
Garant PR (1976). Collagen resorption by fibroblasts. A theory of fibroblastic maintenance of the periodontal ligament. J Periodontol 47:380-390.
Garnero P, Borel O, Byrjalsen I, Ferreras M, Drake FH, McQueney MS, et al. (1998). The collagenolytic activity of cathepsin K is unique among mammalian proteinases. J Biol Chem273:32347-32352.
Gartner PL, Hiatt JL (1997). Color Textbook of Histology. W.B. Saunders Co, p114-130. Gassner R, Vasquez Garcia J, Leja W, Stainer M (2000). Traumatic dental injuries and Alpine skiing.
Endod Dent Traumatol 16:122-127. Gittelson GL (2002). Vertical dimension of occlusion in implant dentistry: significance and approach.
Implant Dent 11:33-40. Giudiceandrea F, Iacona A, Cervelli G, Grimaldi M, Maggiulli G, Cococcetta N, et al. (1998).
Mechanisms of bone resorption: analysis of proinflammatory cytokines in peritoneal macrophages from titanium implant--an experimental design. J Craniofac Surg 9:254-259.
Goldring SR, Goldring MB (1996). Cytokines and skeletal physiology. Clin Orthop (324):13-23. Golub LM, Schneir M, Ramamurthy NS (1978). Enhanced collagenase activity in diabetic rat gingiva:
in vitro and in vivo evidence. J Dent Res 57:520-525. Golub LM, Lee HM, Lehrer G, Nemiroff A, McNamara TF, Kaplan R, et al. (1983). Minocycline
reduces gingival collagenolytic activity during diabetes. Preliminary observations and a proposed new mechanism of action. J Periodontal Res 18:516-526.
Golub LM, Wolff M, Lee HM, McNamara TF, Ramamurthy NS, Zambon J, et al. (1985). Further evidence that tetracyclines inhibit collagenase activity in human crevicular fluid and from other mammalian sources. J Periodontal Res 20:12-23.
Golub LM, McNamara TF, D'Angelo G, Greenwald RA, Ramamurthy NS (1987). A non-antibacterial chemically-modified tetracycline inhibits mammalian collagenase activity. J Dent Res66:1310-1314.
Golub LM, Lee HM, Greenwald RA, Ryan ME, Sorsa T, Salo T, et al. (1997). A matrix metalloproteinase inhibitor reduces bone-type collagen degradation fragments and specific collagenases in gingival crevicular fluid during adult periodontitis. Inflamm Res 46:310-319.
Golub LM, Lee HM, Ryan ME, Giannobile WV, Payne J, Sorsa T. (1998) Tetracyclines inhibit connective tissue breakdown by multiple non-antimicrobial mechanisms. Adv Dent Res 12:12-26.
Gonzalez YM, De Nardin A, Grossi SG, Machtei EE, Genco RJ, De Nardin E (1996). Serum cotinine levels, smoking, and periodontal attachment loss. J Dent Res 75:796-802.

67
Goodacre CJ, Kan JY, Rungcharassaeng K (1999). Clinical complications of osseointegrated implants. J Prosthet Dent 81:537-552.
Graves DT (1999). The potential role of chemokines and inflammatory cytokines in periodontal disease progression. Clin Infect Dis 28:482-490.
Greenwald RA, Golub LM, Ramamurthy NS, Chowdhury M, Moak SA, Sorsa T (1998). In vitro sensitivity of the three mammalian collagenases to tetracycline inhibition: relationship to bone and cartilage degradation. Bone 22:33-38.
Grinnell F, Zhu M (1996). Fibronectin degradation in chronic wounds depends on the relative levels of elastase, alpha1-proteinase inhibitor, and alpha2-macroglobulin. J Invest Dermatol 106:335-341.
Gross J, Nagai Y (1965). Specific degradation of the collagen molecule by tadpole collagenolytic enzyme. Proc Natl Acad Sci U S A 54:1197-1204.
Gross J, Lapiere CM (1962). Collagenolytic activity in amphibian tissue culture assay. Proc Natl Acad Sci 1197-1204.
Gross J, Harper E, Harris ED, McCroskery PA, Highberger JH, Corbett C, et al. (1974). Animal collagenases: specificity of action, and structures of the substrate cleavage site. Biochem Biophys Res Commun 61:605-612.
Gross UM (1988). Biocompatibility--the interaction of biomaterials and host response. J Dent Educ52:798-803.
Grossner-Schreiber B, Griepentrog M, Haustein I, Muller WD, Lange KP, Briedigkeit H, et al. (2001). Plaque formation on surface modified dental implants. An in vitro study. Clin Oral Implants Res 12:543-551.
Gurlek A, Miller MJ, Jacob RF, Lively JA, Schusterman MA (1998). Functional results of dental restoration with osseointegrated implants after mandible reconstruction. Plast Reconstr Surg101:650-5; discussion 656-9.
Guarnieri R, Giardino L, Crespi R, Romagnoli R (2002). Cementum formation around a titanium implant: a case report. Int J Oral Maxillofac Implants 17:729-32.
Guyer B, Freedman MA, Strobino DM, Sondik EJ (2000). Annual summary of vital statistics: trends in the health of Americans during the 20th century. Pediatrics 106:1307-1317.
Haapasalmi K, Makela M, Oksala O, Heino J, Yamada KM, Uitto VJ, et al. (1995). Expression of epithelial adhesion proteins and integrins in chronic inflammation. Am J Pathol 147:193-206.
Hanemaaijer R, Sorsa T, Konttinen YT, Ding Y, Sutinen M, Visser H, et al. (1997). Matrix metalloproteinase-8 is expressed in rheumatoid synovial fibroblasts and endothelial cells. Regulation by tumor necrosis factor-alpha and doxycycline. J Biol Chem 272:31504-31509.
Hanemaaijer R, Visser H, Konttinen YT, Koolwijk P, Verheijen JH (1998). A novel and simple immunocapture assay for determination of gelatinase-B (MMP-9) activities in biological fluids: saliva from patients with Sjogren's syndrome contain increased latent and active gelatinase-B levels. Matrix Biol 17:657-665.
Harrington DJ (1996). Bacterial collagenases and collagen-degrading enzymes and their potential role in human disease. Infect Immun 64:1885-1891.
Hasty KA, Jeffrey JJ, Hibbs MS, Welgus HG (1987). The collagen substrate specificity of human neutrophil collagenase. J Biol Chem 262:10048-10052.
Hayashi T, Kaneda T, Toyama Y, Kumegawa M, Hakeda Y (2002). Regulation of receptor activator of NF-kappa B ligand-induced osteoclastogenesis by endogenous interferon-beta (INF-beta ) and suppressors of cytokine signaling (SOCS). The possible counteracting role of SOCSs- in IFN-beta-inhibited osteoclast formation. J Biol Chem 277:27880-27886.
Hernandez RE, Balshi TJ (1998). Osseointegration treatment of transverse root fractures in the region of the alveolar crest. J Endod 24:145-147.
Herrick S, Ashcroft G, Ireland G, Horan M, McCollum C, Ferguson M (1997). Up-regulation of elastase in acute wounds of healthy aged humans and chronic venous leg ulcers are associated with matrix degradation. Lab Invest 77:281-288.
Higuchi KW, Folmer T, Kultje C (1995). Implant survival rates in partially edentulous patients: a 3-year prospective multicenter study. J Oral Maxillofac Surg 53:264-268.

68
Hill PA, Murphy G, Docherty AJ, Hembry RM, Millican TA, Reynolds JJ, et al. (1994). The effects of selective inhibitors of matrix metalloproteinases (MMPs) on bone resorption and the identification of MMPs and TIMP-1 in isolated osteoclasts. J Cell Sci 107 ( Pt 11):3055-3064.
Holliday LS, Welgus HG, Fliszar CJ, Veith GM, Jeffrey JJ, Gluck SL (1997). Initiation of osteoclast bone resorption by interstitial collagenase. J Biol Chem 272:22053-22058.
Horowitz MC, Xi Y, Wilson K, Kacena MA. (2001) Control of osteoclastogenesis and bone resorption by members of the TNF family of receptors and ligands. Cytokine Growth Factor Rev 12:9-18.
Hou WS, Li Z, Gordon RE, Chan K, Klein MJ, Levy R, et al. (2001). Cathepsin k is a critical protease in synovial fibroblast-mediated collagen degradation. Am J Pathol 159:2167-2177.
Hoyer SA, Stanford CM, Buranadham S, Fridrich T, Wagner J, Gratton D (2001). Dynamic fatigue properties of the dental implant-abutment interface: joint opening in wide-diameter versus standard-diameter hex-type implants. J Prosthet Dent 85:599-607.
Huelke DF, Sherman HW (1973). Automobile injuries--the forgotten area of public health dentistry. JAm Dent Assoc 86:384-393.
Hugoson A, Laurell L (2000). A prospective longitudinal study on periodontal bone height changes in a Swedish population. J Clin Periodontol 27:665-674.
Hutton JE, Heath MR, Chai JY, Harnett J, Jemt T, Johns RB, et al. (1995). Factors related to success and failure rates at 3-year follow-up in a multicenter study of overdentures supported by Branemark implants. Int J Oral Maxillofac Implants 10:33-42.
Ibanez JC, Jalbout ZN (2002). Immediate loading of osseotite implants: two-year results. Implant Dent11:128-136.
Iacono VJ; Committee on Research, Science and Therapy, the American Academy of Periodontology (2000). Dental implants in periodontal therapy. J Periodontol 71:1934-1942.
Imai S, Konttinen YT, Jumppanen M, Lindy O, Ceponis A, Kemppinen P, et al. (1998). High levels of expression of collagenase-3 (MMP-13) in pathological conditions associated with a foreign-body reaction. J Bone Joint Surg Br 80:701-710.
Ingman T, Sorsa T, Konttinen YT, Liede K, Saari H, Lindy O, et al. (1993). Salivary collagenase, elastase- and trypsin-like proteases as biochemical markers of periodontal tissue destruction in adult and localized juvenile periodontitis. Oral Microbiol Immunol 8:298-305.
Ingman T, Kononen M, Konttinen YT, Siirila HS, Suomalainen K, Sorsa T (1994). Collagenase, gelatinase and elastase activities in sulcular fluid of osseointegrated implants and natural teeth. J Clin Periodontol 21:301-307.
Ingman T, Tervahartiala T, Ding Y, Tschesche H, Haerian A, Kinane DF, et al. (1996). Matrix metalloproteinases and their inhibitors in gingival crevicular fluid and saliva of periodontitis patients. J Clin Periodontol 23:1127-1132.
Ingman T, Tervahartiala T, Ding Y, Tschesche H, Haerian A, Kinane DF, et al. (1996). Matrix metalloproteinases and their inhibitors in gingival crevicular fluid and saliva of periodontitis patients. J Clin Periodontol 23:1127-1132.
Jacobs R, van Steenberghe D (1993). Comparison between implant-supported prostheses and teeth regarding passive threshold level. Int J Oral Maxillofac Implants 8:549-554.
James JA, Sayers NM, Drucker DB, Hull PS (1999). Effects of tobacco products on the attachment and growth of periodontal ligament fibroblasts. J Periodontol 70:518-525.
Jemt T, Lekholm U, Grondahl K (1990). 3-year followup study of early single implant restorations ad modum Branemark. Int J Periodontics Restorative Dent 10:340-349.
Jisander S, Grenthe B, Alberius P. (1997) Dental implant survival in the irradiated jaw: a preliminary report. Int J Oral Maxillofac Implants 12:643-648.
Johnson RB (1992). Morphological characteristics of the depository surface of alveolar bone of diabetic mice. J Periodontal Res 27:40-47.
Kafienah W, Buttle DJ, Burnett D, Hollander AP (1998). Cleavage of native type I collagen by human neutrophil elastase. Biochem J 330 ( Pt 2):897-902.
69
Kaji K, Katogi R, Azuma Y, Naito A, Inoue JI, Kudo A (2001). Tumor necrosis factor alpha-induced osteoclastogenesis requires tumor necrosis factor receptor-associated factor 6. J Bone Miner Res 16:1593-1599.
Kalykakis GK, Mojon P, Nisengard R, Spiekermann H, Zafiropoulos GG (1998). Clinical and microbial findings on osseo-integrated implants; comparisons between partially dentate and edentulous subjects. Eur J Prosthodont Restor Dent 6:155-159.
Kanzaki H, Chiba M, Shimizu Y, Mitani H (2001). Dual regulation of osteoclast differentiation by periodontal ligament cells through RANKL stimulation and OPG inhibition. J Dent Res80:887-891.
Katagiri M, Hakeda Y, Chikazu D, Ogasawara T, Takato T, Kumegawa M, et al. (2001). Mechanism of stimulation of osteoclastic bone resorption through Gas6/Tyro 3, a receptor tyrosine kinase signaling, in mouse osteoclasts. J Biol Chem 276:7376-7382.
Kaukinen JA, Edge MJ, Lang BR (1996). The influence of occlusal design on simulated masticatory forces transferred to implant-retained prostheses and supporting bone. J Prosthet Dent 76:50-55.
Kauppinen TP, Virtanen SV (2002). Exposure to environmental tobacco smoke in Finland in 2000. Scand J Work Environ Health 28 Suppl 2:7-15.
Keller EE, Tolman DE, Eckert SE (1999). Maxillary antral-nasal inlay autogenous bone graft reconstruction of compromised maxilla: a 12-year retrospective study. Int J Oral Maxillofac Implants 14:707-721.
Kerkvliet EH, Docherty AJ, Beertsen W, Everts V (1999). Collagen breakdown in soft connective tissue explants is associated with the level of active gelatinase A (MMP-2) but not with collagenase. Matrix Biol 18:373-380.
Kerstein RB (2001). Current applications of computerized occlusal analysis in dental medicine. Gen Dent 49:521-530.
Klineberg I, Murray G (1999). Osseoperception: sensory function and proprioception. Adv Dent Res13:120-129.
Klinger MM, Rahemtulla F, Prince CW, Lucas LC, Lemons JE (1998). Proteoglycans at the bone-implant interface. Crit Rev Oral Biol Med 9:449-463.
Ko CC, Kohn DH, Hollister SJ (1992). Micromechanics of implant/tissue interfaces. J Oral Implantol18:220-230.
Koenisberger R (1989). Churchill's illustrated medical dictionary. PUBLISHER New York: Churchill Livingstone.
Koivunen E, Ristimaki A, Itkonen O, Osman S, Vuento M, Stenman UH (1991). Tumor-associated trypsin participates in cancer cell-mediated degradation of extracellular matrix. Cancer Res51:2107-2112.
Koka S, Reinhardt RA (1997). Periodontal pathogen-related stimulation indicates unique phenotype of primary cultured human fibroblasts from gingiva and periodontal ligament: implications for oral health disease. J Prosthet Dent 77:191-196.
Konttinen YT, Xu JW, Pätiälä H, Imai S, Waris V, Li TF, et al. (1997). Cytokines in aseptic loosening of total hip replacement. Curr Orthop 11:40-47.
Konttinen YT, Ceponis A, Takagi M, Ainola M, Sorsa T, Sutinen M, et al. (1998). New collagenolytic enzymes/cascade identified at the pannus-hard tissue junction in rheumatoid arthritis: destruction from above. Matrix Biol 17:585-601.
Konttinen YT, Salo T, Hanemaaijer R, Valleala H, Sorsa T, Sutinen M, et al. (1999). Collagenase-3 (MMP-13) and its activators in rheumatoid arthritis: localization in the pannus-hard tissue junction and inhibition by alendronate. Matrix Biol 18:401-412.
Konttinen YT, Takagi M, Mandelin J, Lassus J, Salo J, Ainola M, et al. (2001). Acid attack and cathepsin K in bone resorption around total hip replacement prosthesis. J Bone Miner Res16:1780-1786.
Konttinen YT, Mandelin J, Li TF, Salo J, Lassus J, Liljestrom M, et al. (2002). Acidic cysteine endoproteinase cathepsin K in the degeneration of the superficial articular hyaline cartilage in osteoarthritis. Arthritis Rheum 46:953-960.

70
Kovacs AF (2000). The fate of osseointegrated implants in patients following oral cancer surgery and mandibular reconstruction. Head Neck 22:111-119.
Krane SM, Byrne MH, Lemaitre V, Henriet P, Jeffrey JJ, Witter JP, et al. (1996). Different collagenase gene products have different roles in degradation of type I collagen. J Biol Chem 271:28509-28515.
Kronstrom M, Palmqvist S, Soderfeldt B, Vigild M (2002). Utilization of dental health services among middle-aged people in Sweden and Denmark. Acta Odontol Scand 60:276-280.
Kubota T, Nomura T, Takahashi T, Hara K (1996). Expression of mRNA for matrix metalloproteinases and tissue inhibitors of metalloproteinases in periodontitis-affected human gingival tissue. Arch Oral Biol 41:253-262.
Kurata K, Uemura T, Nemoto A, Tateishi T, Murakami T, Higaki H, et al. (2001). Mechanical strain effect on bone-resorbing activity and messenger RNA expressions of marker enzymes in isolated osteoclast culture. J Bone Miner Res 16:722-730.
Kusano K, Miyaura C, Inada M, Tamura T, Ito A, Nagase H, et al. (1998). Regulation of matrix metalloproteinases (MMP-2, -3, -9, and -13) by interleukin-1 and interleukin-6 in mouse calvaria: association of MMP induction with bone resorption. Endocrinology 139:1338-1345.
Lacefield WR (1988). Hydroxyapatite coatings. Ann N Y Acad Sci 523:72-80. Lambert PM, Morris HF, Ochi S (1997). Positive effect of surgical experience with implants on
second-stage implant survival. J Oral Maxillofac Surg 55:12-18. Lassus J, Salo J, Jiranek WA, Santavirta S, Nevalainen J, Matucci-Cerinic M, et al. (1998).
Macrophage activation results in bone resorption. Clin Orthop (352):7-15. Lauer-Fields JL, Tuzinski KA, Shimokawa K, Nagase H, Fields GB (2000). Hydrolysis of triple-helical
collagen peptide models by matrix metalloproteinases. J Biol Chem 275:13282-13290. Laurent GJ (1987). Dynamic state of collagen: pathways of collagen degradation in vivo and their
possible role in regulation of collagen mass. Am J Physiol 252:C1-9. Lazarus GS, Brown RS, Daniels JR, Fullmer HM (1968). Human granulocyte collagenase.
Science 159:1483-1485. Lazner F, Gowen M, Pavasovic D, Kola I (1999). Osteopetrosis and osteoporosis: two sides of the
same coin. Hum Mol Genet 8:1839-1846. Lazzerini F, Minorati D, Nessi R, Gagliani M, Uslenghi CM (1996). The measurement parameters in
dental radiography: a comparison between traditional and digital technics. Radiol Med 91:364-369.
Lee W, Aitken S, Sodek J, McCulloch CA (1995). Evidence of a direct relationship between neutrophil collagenase activity and periodontal tissue destruction in vivo: role of active enzyme in human periodontitis. J Periodontal Res 30:23-33.
LeGeros RZ, Craig RG (1993). Strategies to affect bone remodeling: osteointegration. J Bone Miner Res Suppl 2:S583-596.
Lehninger AL, Nelson DL, Cox MM (2000). Principles of biochemistry. pp. 427. Leonhardt A, Renvert S, Dahlen G. (1999) Microbial findings at failing implants. Clin Oral Implants
Res 10:339-345. Levine DA, Platt SL, Foltin GL (2001). Scooter injuries in children. Pediatrics 107:E64. Lewis DW. (1998) Optimized therapy for the edentulous predicament: cost-effectiveness
considerations. J Prosthet Dent 79:93-99. Li TF, Xu JW, Santavirta S, Nordsletten L, Michelsson O, Takagi M, et al. (2000a). Distribution of
fibronectins and their integrin receptors in interface tissue from aseptic loosening of hip prostheses. Clin Exp Rheumatol 18:221-225.
Li TF (2000b). Extracellular and pericellular matrix proteins in the synovial membrane-like interface tissue from aseptic loosening of total hip replacement. Doctor thesis. P17-20.
Libby P, Lee RT (2000). Matrix matters. Circulation 102:1874-1876. Liljenberg B, Gualini F, Berglundh T, Tonetti M, Lindhe J (1996). Some characteristics of the ridge
mucosa before and after implant installation.A prospective study in humans. J Clin Periodontol 23:1008-1013.

71
Lindemann RA, Economou JS, Rothermel H (1988). Production of interleukin-1 and tumor necrosis factor by human peripheral monocytes activated by periodontal bacteria and extracted lipopolysaccharides. J Dent Res 67:1131-1135.
Linden RW, Millar BJ (1988). The response characteristics of mechanoreceptors related to their position in the cat canine periodontal ligament. Arch Oral Biol 33:51-56.
Lindhe J, Berglundh T (1998). The interface between the mucosa and the implant. Periodontol 200017:47-54.
Linsuwanont B, Takagi Y, Ohya K, Shimokawa H (2002). Expression of matrix metalloproteinase-9 mRNA and protein during deciduous tooth resorption in bovine odontoclasts. Bone 31:472-478.
Llano E, Pendas AM, Knauper V, Sorsa T, Salo T, Salido E, et al. (1997). Identification and structural and functional characterization of human enamelysin (MMP-20). Biochemistry 36:15101-15108.
Löe H (1967). The Gingival Index, the Plaque Index and the Retention Index Systems. J Periodontol38:Suppl:610-6.
Lopatin DE, Caffesse ER, Bye FL, Caffesse RG (1989). Concentrations of fibronectin in the sera and crevicular fluid in various stages of periodontal disease. J Clin Periodontol 16:359-364.
Lumbikanonda N, Sammons R (2001). Bone cell attachment to dental implants of different surface characteristics. Int J Oral Maxillofac Implants 16:627-636.
Lund JP (1991). Mastication and its control by the brain stem. Crit Rev Oral Biol Med 2:33-64. Luterbacher S, Mayfield L, Bragger U, Lang NP (2000). Diagnostic characteristics of clinical and
microbiological tests for monitoring periodontal and peri-implant mucosal tissue conditions during supportive periodontal therapy (SPT). Clin Oral Implants Res 11:521-529.
Mailman ML (1979). The efficacy of bacterial collagenase for the digestion of gingival tissue collagen. J Dent Res 58:1424.
Mainardi CL, Hasty DL, Seyer JM, Kang AH (1980). Specific cleavage of human type III collagen by human polymorphonuclear leukocyte elastase. J Biol Chem 255:12006-12010.
Malevez C, Hermans M, Daelemans P (1996). Marginal bone levels at Branemark system implants used for single tooth restoration. The influence of implant design and anatomical region. Clin Oral Implants Res 7:162-169.
Mancini S, Romanelli R, Laschinger CA, Overall CM, Sodek J, McCulloch CA (1999). Assessment of a novel screening test for neutrophil collagenase activity in the diagnosis of periodontal diseases. J Periodontol 70:1292-1302.
Mangano C, Bartolucci EG (2001). Single tooth replacement by Morse taper connection implants: a retrospective study of 80 implants. Int J Oral Maxillofac Implants 16:675-680.
Manlapaz M, Malonet WJ, Smith RL (1996). In vitro activation of human fibroblasts by retrieved titanium alloy wear debris. J Orthopaed Res 14:465-472.
Mariano M, Spector WG (1974). The formation and properties of macrophage polykaryons (inflammatory giant cells). J Pathol 113:1-19.
Matthews DC (2002). The relationship between diabetes and periodontal disease. J Can Dent Assoc68:161-164.
McDonald JA, Kelley DG (1980). Degradation of fibronectin by human leukocyte elastase. Release of biologically active fragments. J Biol Chem 255:8848-8858.
McDonald JA, Kelley DG, Broekelmann TJ (1982). Role of fibronectin in collagen deposition: Fab' to the gelatin-binding domain of fibronectin inhibits both fibronectin and collagen organization in fibroblast extracellular matrix. J Cell Biol 92:485-492.
McDonald JA, Kelley DG (1984). Specific binding of fibronectin--antifibronectin immune complexes to procollagen: a new pitfall in immunostaining. J Cell Biol 98:1042-1047.
McMillan AS, Nunn JH, Postlethwaite KR (1998). Implant-supported prosthesis in a child with hereditary mandibular anodontia: the use of ball attachments. Int J Paediatr Dent 8:65-69.
Mechanic GL, Kuboki Y, Shimokawa H, Nakamoto K, Sasaki S, Kawanishi Y (1974). Collagen crosslinks: direct quantitative determination of stable structural crosslinks in bone and dentin collagens. Biochem Biophys Res Commun 60:756-763.
72
Meffert RM (1996). Periodontitis vs. peri-implantitis: the same disease? The same treatment? Crit Rev Oral Biol Med 7:278-291.
Millennium Research Group (2002). European markets for dental implants 2001: executive summary. Implant Dent 11:7-12.
Miller RL, Folke LE, Umana CR (1975). Chemotactic ability of dental plaque upon autologous or heterologous human polymorphonuclear leukocytes. J Periodontol 46:409-414.
Hemmila I, Dakubu S, Mukkala VM, Siitari H, Lovgren T (1984). Europium as a label in time-resolved immunofluorometric assays. Anal Biochem 137:335-343.
Mintz KP, Fives-Taylor PM (1999). Binding of the periodontal pathogen Actinobacillus actinomycetemcomitans to extracellular matrix proteins. Oral Microbiol Immunol 14:109-116.
Misch CE (2002). The effect of bruxism on treatment planning for dental implants. Dent Today 21:76-81.
Mitchell PG, Magna HA, Reeves LM, Lopresti-Morrow LL, Yocum SA, Rosner PJ, et al. (1996). Cloning, expression, and type II collagenolytic activity of matrix metalloproteinase-13 from human osteoarthritic cartilage. J Clin Invest 97:761-768.
Mohri H (1996). Fibronectin and integrins interactions. J Investig Med 44:429-441. Moilanen M, Sorsa T, Stenman M, Nyberg P, Lindy O, Vesterinen J, et al. (2003). Tumor-associated
trypsinogen-2 (trypsinogen-2) activates procollagenases (MMP-1, -8, -13) and stromelysin-1 (MMP-3) and degrades type I collagen. Biochemistry 42:5414-5420.
Mombelli A, van Oosten MA, Schurch E Jr, Land NP (1987). The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol Immunol 2:145-151.
Morris SM, Stone PJ, Snider GL (1993). Electron microscopic study of human lung tissue after in vitro exposure to elastase. J Histochem Cytochem 41:851-866.
Motamedi MH, Hashemi HM, Shams MG, Nejad AN (1999). Rehabilitation of war-injured patients with implants: analysis of 442 implants placed during a 6-year period. J Oral Maxillofac Surg57:907-13; discussion 914-5.
Mühlemann HR (1967). Tooth mobility: a review of clinical aspects and research findings. JPeriodontol 38:Suppl:686-713.
Nakano T, Scott PG (1987). Partial purification and characterization of a neutral proteinase with collagen telopeptidase activity produced by human gingival fibroblasts. Biochem Cell Biol65:286-292.
Nathan C, Sporn M (1991). Cytokine in context. J Cell Biol 113, 981-986. Nociti FH,Jr, Cesar NJ, Carvalho MD, Sallum EA (2002). Bone density around titanium implants may
be influenced by intermittent cigarette smoke inhalation: a histometric study in rats. Int J Oral Maxillofac Implants 17:347-352.
Nosaka AY, Kanaori K, Teno N, Togame H, Inaoka T, Takai M, et al. (1999). Conformational studies on the specific cleavage site of Type I collagen (alpha-1) fragment (157-192) by cathepsins K and L by proton NMR spectroscopy. Bioorg Med Chem 7:375-379.
Noth U, Hendrich C, Merklein F, Altvater T, Rader CP, Schutze N, et al. (1999). Standardized testing of bone implant surfaces with an osteoblast cell culture system. II. Titanium surfaces of different degrees of roughness. Biomed Tech (Berl) 44:6-11.
Oates TW, Cochran DL (1996). Bone cell interactions and regulation by inflammatory mediators. Curr Opin Periodontol 3:34-44.
Ohuchi E, Imai K, Fujii Y, Sato H, Seiki M, Okada Y (1997). Membrane type 1 matrix metalloproteinase digests interstitial collagens and other extracellular matrix macromolecules. J Biol Chem 272:2446-2451.
Oikarinen K, Raustia AM, Hartikainen M (1995). General and local contraindications for endosseal implants--an epidemiological panoramic radiograph study in 65-year-old subjects. Community Dent Oral Epidemiol 23:114-118.
Okada Y, Naka K, Kawamura K, Matsumoto T, Nakanishi I, Fujimoto N, et al. (1995). Localization of matrix metalloproteinase 9 (92-kilodalton gelatinase/type IV collagenase = gelatinase B) in osteoclasts: implications for bone resorption. Lab Invest 72:311-322.
73
Okamoto T, Akaike T, Suga M, Tanase S, Horie H, Miyajima S, et al. (1997). Activation of human matrix metalloproteinases by various bacterial proteinases. J Biol Chem 272:6059-6066.
Olson JW, Shernoff AF, Tarlow JL, Colwell JA, Scheetz JP, Bingham SF (2000). Dental endosseous implant assessments in a type 2 diabetic population: a prospective study. Int J Oral Maxillofac Implants 15:811-818.
O'Mahony A, MacNeill SR, Cobb CM (2000). Design features that may influence bacterial plaque retention: a retrospective analysis of failed implants. Quintessence Int 31:249-256.
O'Roark WL (1991). Improving implant survival rates by using a new method of at risk analysis. Int J Oral Implantol 8:31-57.
O'Reilly PG, Claffey NM (1996). Identifying losing sites at periodontal reevaluation. Curr Opin Periodontol 3:68-77.
O'Roark WL (1997). Survival rate of dental implants: an individual practitioner's anecdotal review of 25 years of experience. J Oral Implantol 23:90-103.
Owall B, Cronstrom R, Rene N (1992). Prosthodontic claims in the Swedish Patient Insurance Scheme. Acta Odontol Scand 50:365-374.
Owen CA, Campbell MA, Sannes PL, Boukedes SS, Campbell EJ (1995). Cell surface-bound elastase and cathepsin G on human neutrophils: a novel, non-oxidative mechanism by which neutrophils focus and preserve catalytic activity of serine proteinases. J Cell Biol 13:775-789.
Palosaari H, Wahlgren J, Larmas M, Ronka H, Sorsa T, Salo T, et al. (2000). The expression of MMP-8 in human odontoblasts and dental pulp cells is down-regulated by TGF-beta1. J Dent Res79:77-84.
Palmqvist S, Soderfeldt B, Arnbjerg D (1991). Subjective need for implant dentistry in a Swedish population aged 45-69 years. Clin Oral Implants Res 2:99-102.
Papapanou PN (1989). Patterns of alveolar bone loss in the assessment of periodontal treatment priorities. Swed Dent J Suppl 66:1-45.
Parker HM, Miller RD (1989). Dental implants and third party carrier coverage. Dent Clin North Am33:905-909.
Patterson CC, Dahlquist G, Soltesz G, Green A, The EURODIAB ACE Study Group. Europe and Diabetes (2001). Is childhood-onset type I diabetes a wealth-related disease? An ecological analysis of European incidence rates. Diabetologia 44 Suppl 3:B9-16.
Perkins SL, Kling SJ (1995). Local concentrations of macrophage colony-stimulating factor mediate osteoclastic differentiation. Am J Physiol 269:E1024-30.
Persikov AV, Brodsky B (2002). Unstable molecules form stable tissues. Proc Natl Acad Sci USA99:1101-1103.
Pfeilschifter J, Chenu C, Bird A, Mundy GR, Roodman GD (1989). Interleukin-1 and tumor necrosis factor stimulate the formation of human osteoclastlike cells in vitro. J Bone Miner Res 4:113-118.
Piattelli A, Scarano A, Piattelli M (1998a). Histologic observations on 230 retrieved dental implants: 8 years' experience (1989-1996). J Periodontol 69:178-184.
Piattelli A, Scarano A, Balleri P, Favero GA (1998b). Clinical and histologic evaluation of an active "implant periapical lesion": a case report. Int J Oral Maxillofac Implants 13:713-716.
Piattelli A, Scarano A, Piattelli M, Vaia E, Matarasso S (1998c). Hollow implants retrieved for fracture: a light and scanning electron microscope analysis of 4 cases. J Periodontol 69:185-189.
Picton DC, Wills DJ (1978). Viscoelastic properties of the periodontal ligament and mucous membrane. J Prosthet Dent 40:263-272.
Pihakari A, Nevalainen J, Hirvonen A, Mäkelä A (2001). The 2000 Dental Implant Yearbook. Publications of the National Agency for Medicines 1/2001.
Priest G (1999). Single-tooth implants and their role in preserving remaining teeth: a 10-year survival study. Int J Oral Maxillofac Implants 14:181-188.
Pujades C, Teixido J, Bazzoni G, Hemler ME (1996). Integrin alpha 4 cysteines 278 and 717 modulate VLA-4 ligand binding and also contribute to alpha 4/180 formation. Biochem J 313:899-908.
Raisz LG (1999). Physiology and pathophysiology of bone remodeling. Clin Chem 45:1353-1358.
74
Ramamurthy NS, Rifkin BR, Greenwald RA, Xu JW, Liu Y, Turner G, et al. (2002). Inhibition of matrix metalloproteinase-mediated periodontal bone loss in rats: a comparison of 6 chemically modified tetracyclines. J Periodontol 73:726-734.
Ramfjord SP (1967). The Periodontal Disease Index (PDI). J Periodontol 38:Suppl:602-10. Rangert B, Krogh PH, Langer B, Van Roekel N (1995). Bending overload and implant fracture: a
retrospective clinical analysis. Int J Oral Maxillofac Implants 10:326-334. Reddy MS, Mayfield-Donahoo T, Vanderven FJ, Jeffcoat MK (1994). A comparison of the diagnostic
advantages of panoramic radiography and computed tomography scanning for placement of root form dental implants. Clin Oral Implants Res 5:229-238.
Redlich M, Reichenberg E, Harari D, Zaks B, Shoshan S, Palmon A (2001). The effect of mechanical force on mRNA levels of collagenase, collagen type I, and tissue inhibitors of metalloproteinases in gingivae of dogs. J Dent Res 80:2080-2084.
Reich E (2001). Trends in caries and periodontal health epidemiology in Europe. Int Dent J 51:392-398.
Reitz JV (1994). Lingualized occlusion in implant dentistry. Quintessence Int 25:177-180. Reynolds JJ (1996). Collagenases and tissue inhibitors of metalloproteinases: a functional balancein
tissue degradation. Oral Dis 2:70-76. Reynolds JJ, Meikle MC (1997). Mechanisms of connective tissue matrix destruction in periodontitis.
Periodontol 2000 14:144-157. Riggs BL, Melton LJ 3rd (1988). Osteoporosis and age-related fracture syndromes. Ciba Found Symp
134:129-142. Roberts WE, Simmons KE, Garetto LP, DeCastro RA (1992). Bone physiology and metabolism in
dental implantology: risk factors for osteoporosis and other metabolic bone diseases. Implant Dent 1:11-21.
Romanelli R, Mancini S, Laschinger C, Overall CM, Sodek J, McCulloch CA (1999). Activation of neutrophil collagenase in periodontitis. Infect Immun 67:2319-2326.
Ross MH, Romrell LJ, Kaye GI (1995). Histology a text and atlas. Third edition. A Williams company. pp150.
Rubin C, Sun YQ, Hadjiargyrou M, McLeod K (1999). Increased expression of matrix metalloproteinase-1 in osteocytes precedes bone resorption as stimulated by disuse: evidence for autoregulation of the cell's mechanical environment? J Orthop Res 17:354-361.
Russell AL (1967). The Periodontal Index. J Periodontol 38:Suppl:585-91. Ryu OH, Fincham AG, Hu CC, Zhang C, Qian Q, Bartlett JD, et al. (1999). Characterization of
recombinant pig enamelysin activity and cleavage of recombinant pig and mouse amelogenins. J Dent Res 78:743-750.
Saari H, Suomalainen K, Lindy O, Konttinen YT, Sorsa T (1990). Activation of latent human neutrophil collagenase by reactive oxygen species and serine proteases. Biochem Biophys Res Commun 171:979-987.
Sakai T, Gross J (1967). Some properties of the products of reaction of tadpole collagenase with collagen. Biochemistry 6:518-528.
Salo T, Lyons JG, Rahemtulla F, Birkedal-Hansen H, Larjava H (1991). Transforming growth factor-beta 1 up-regulates type IV collagenase expression in cultured human keratinocytes. J Biol Chem 266:11436-11441.
Salo T. Kylmäniemi M. Helaakoski T. Virktunen J. Ding Y. Konttinen YT. (1995) MMP-8/neutrophil collagenase mRNA may also be detected in other cells than PMNs. J Dent Res 74(Special issue):1036.
Sandros J, Karlsson C, Lappin DF, Madianos PN, Kinane DF, Papapanou PN (2000). Cytokine responses of oral epithelial cells to Porphyromonas gingivalis infection. J Dent Res 79:1808-1814.
Santavirta S, Nordstrom D, Ylinen P, Konttinen YT, Silvennoinen T, Rokkanen P (1991). Biocompatibility of hydroxyapatite-coated hip prostheses. Arch Orthop Trauma Surg110:288-292.
75
Santavirta S, Takagi M, Gomez-Barrena E, Nevalainen J, Lassus J, Salo J, et al. (1999). Studies of host response to orthopedic implants and biomaterials. J Long Term Eff Med Implants 9:67-76.
Santavirta S (2003). Compatibility of the totally replaced hip---reduction of wear by amorphous diamond coating. Kuopio University Printing Office, Finland, p25.
Sasano Y, Zhu JX, Tsubota M, Takahashi I, Onodera K, Mizoguchi I, et al. (2002). Gene expression of MMP8 and MMP13 during embryonic development of bone and cartilage in the rat mandible and hind limb. J Histochem Cytochem 50:325-332.
Schneir M, Bowersox J, Ramamurthy N, Yavelow J, Murray J, Edlin-Folz E, et al. (1979). Response of rat connective tissues to streptozotocin-diabetes. Tissue-specific effects on collagen metabolism. Biochim Biophys Acta 583:95-102.
Schroeder HE, Page RC. The normal periodontium. In: Schlunger S, Yuodelis R, Page RC, Johnson RH, eds. Periodontal Diseases. Philadephia: Lea & Febiger, 3-52.
Schwartz Z, Goultschin J, Dean DD, Boyan BD (1997). Mechanisms of alveolar bone destruction in periodontitis. Periodontol 2000 14:158-172.
Schwartz-Arad D, Samet N, Samet N, Mamlider A (2002). Smoking and complications of endosseous dental implants. J Periodontol 73:153-157.
Schwarz MS (2000). Mechanical complications of dental implants. Clin Oral Implants Res 11 Suppl 1:156-158.
Sclaroff A, Elluru RG, Gay WD (2000). Dental implantation for restoration of posttraumatic deformities: avulsion injuries. Facial Plast Surg 16:153-167.
Searson L, Meredith N. (1997) The role of implants in restorative dentistry: prosthesis design and aesthetic considerations. Dent Update 24:388-390.
Silness J, Loe H (1966). Periodontal disease in pregnancy. 3. Response to local treatment. Acta Odontol Scand 24:747-759.
Silva M, Shepherd EF, Jackson WO, Dorey FJ, Schmalzried TP (2002). Average patient walking activity approaches 2 million cycles per year: pedometers under-record walking activity. JArthroplasty 17:693-697.
Smith DE, Zarb GA (1989). Criteria for success of osseointegrated endosseous implants. J Prosthet Dent 62:567-572.
Snauwaert K, Duyck J, van Steenberghe D, Quirynen M, Naert I (2000). Time dependent failure rate and marginal bone loss of implant supported prostheses: a 15-year follow-up study. Clin Oral Investig 4:13-20.
Socransky SS, Haffajee AD, Goodson JM, Lindhe J (1984). New concepts of destructive periodontal disease. J Clin Periodontol 11:21-32.
Soell M, Elkaim R, Tenenbaum H (2002). Cathepsin C, matrix metalloproteinases, and their tissue inhibitors in gingiva and gingival crevicular fluid from periodontitis-affected patients. J Dent Res 81:174-178.
Soncini M, Rodriguez Y, Pietrabissa R, Quaglini V, Rizzo S, Zaffe D (2002). Experimental procedure for the evaluation of the mechanical properties of the bone surrounding dental implants. Biomaterials 23:9-17.
Sorsa T, Uitto VJ, Suomalainen K, Vauhkonen M, Lindy S (1988). Comparison of interstitial collagenases from human gingiva, sulcular fluid and polymorphonuclear leukocytes. JPeriodontal Res 23:386-393.
Sorsa T, Suomalainen K, helenius J, Lindy S, Saari H, Konttinen YT, Uitto VJ (1989). Periodontal disease. N Engl J Med 323: 133-135.
Sorsa T, Ingman T, Suomalainen K, Haapasalo M, Konttinen YT, Lindy O, et al. (1992). Identification of proteases from periodontopathogenic bacteria as activators of latent human neutrophil and fibroblast-type interstitial collagenases. Infect Immun 60:4491-4495.
Sorsa T, Salo T, Koivunen E, Tyynela J, Konttinen YT, Bergmann U, et al. (1997). Activation of type IV procollagenases by human tumor-associated trypsin-2. J Biol Chem 272:21067-21074.
Sorsa T, Ramamurthy NS, Vernillo AT, Zhang X, Konttinen YT, Rifkin BR, et al. (1998). Functional sites of chemically modified tetracyclines: inhibition of the oxidative activation of human neutrophil and chicken osteoclast pro-matrix metalloproteinases. J Rheumatol 25:975-982.
76
Sorsa T, Mantyla P, Ronka H, Kallio P, Kallis GB, Lundqvist C, et al. (1999). Scientific basis of a matrix metalloproteinase-8 specific chair-side test for monitoring periodontal and peri-implant health and disease. Ann N Y Acad Sci 878:130-140.
South-Paul JE (2001). Osteoporosis: part I. Evaluation and assessment. Am Fam Physician 63:897-904, 908.
Spanheimer RG, Umpierrez GE, Stumpf V (1988) Decreased collagen production in diabetic rats. Diabetes 37:371-376.
Springstead MC, Thomas MC, Cline NV (1993). Educating a patient with dental implants. Dent Assist62:5-8.
Stanford CM, Keller JC (1991). The concept of osseointegration and bone matrix expression. Crit Rev Oral Biol Med 2:83-101.
Starkey PM (1977). The effect of human neutrophil elastase and cathepsin G on the collagen of cartilage, tendon, and cornea. Acta Biol Med Ger 36:1549-1554.
Sukhova GK, Schonbeck U, Rabkin E, Schoen FJ, Poole AR, Billinghurst RC, et al. (1999). Evidence for increased collagenolysis by interstitial collagenases-1 and -3 in vulnerable human atheromatous plaques. Circulation 99:2503-2509.
Suomalainen K, Sorsa T, Golub LM, Ramamurthy N, Lee HM, Uitto VJ, et al. (1992). Specificity of the anticollagenase action of tetracyclines: relevance to their anti-inflammatory potential. Antimicrob Agents Chemother 36:227-229.
Swanberg DF, Henry MD (1995). Avoiding implant overload. Implant Soc 6:12-14. Szmukler-Moncler S, Salama H, Reingewirtz Y, Dubruille JH (1998). Timing of loading and effect of
micromotion on bone-dental implant interface: review of experimental literature. J Biomed Mater Res 43:192-203.
Takagi M, Konttinen YT, Santavirta S, Kangaspunta P, Sorsa T, Yamakawa M, et al. (1995). Elastase activity, uninhibited by alpha 1-antitrypsin, in the periprosthetic connective matrix around loose total hip prostheses. J Orthop Res 13:296-304.
Takahashi N, Kato T, Kuramitsu HK (1991). Isolation and preliminary characterization of the Porphyromonas gingivalis prtC gene expressing collagenase activity. FEMS Microbiol Lett 68:135-138.
Takala L, Utriainen P, Alanen P (1994). Incidence of edentulousness, reasons for full clearance, and health status of teeth before extractions in rural Finland. Community Dent Oral Epidemiol22:254-257.
Talonpoika JT, Soderling E, Paunio K (1993). Characterization of fibronectin and fibrin(ogen) fragments in gingival crevicular fluid. Scand J Dent Res 101:26-32.
Talonpoika J, Heino J, Larjava H, Hakkinen L, Paunio K (1989). Gingival crevicular fluid fibronectin degradation in periodontal health and disease. Scand J Dent Res 97:415-421.
Takata T, Katauchi K, Akagawa Y, Nikai H (1993). New periodontal ligament formation on a synthetic hydroxyapatite surface. Clin Oral Implants Res 4:130-136.
Teitelbaum SL (2000) Bone resorption by osteoclasts. Science 289:1504-1508. Teronen O, Konttinen YT, Lindqvist C, Salo T, Ingman T, Lauhio A, et al. (1997). Human neutrophil
collagenase MMP-8 in peri-implant sulcus fluid and its inhibition by clodronate. J Dent Res76:1529-1537.
Terranova VP, Nishimura F (1996) Periodontal ligament cells are chemotactic to fibroblast collagenase. J Dent Res 75:993-1001.
Tervahartiala T, Pirila E, Ceponis A, Maisi P, Salo T, Tuter G, et al. (2000). The in vivo expression of the collagenolytic matrix metalloproteinases (MMP-2, -8, -13, and -14) and matrilysin (MMP-7) in adult and localized juvenile periodontitis. J Dent Res 79:1969-1977.
Tervahartiala T, Koski H, Xu JW, Hayrinen-Immonen R, Hietanen J, Sorsa T, et al. (2001). Tumor necrosis factor-alpha and its receptors, p55 and p75, in gingiva of adult periodontitis. J Dent Res 80:1535-1539.
Testori T, Wiseman L, Woolfe S, Porter SS (2001). A prospective multicenter clinical study of the Osseotite implant: four-year interim report. Int J Oral Maxillofac Implants 16:193-200.
The Japanese market for dental implants: executive summary (2002). Implant Dent 11:103-106.
77
Tinsley D, Watson CJ, Ogden AR (1999). A survey of U.K. centres on implant failures. J Oral Rehabil26:14-18.
Tipton DA, Dabbous MK (1995). Effects of nicotine on proliferation and extracellular matrix production of human gingival fibroblasts in vitro. J Periodontol 66:1056-1064.
Tomar SL, Asma S (2000). Smoking-attributable periodontitis in the United States: findings from NHANES III. National Health and Nutrition Examination Survey. J Periodontol 71:743-751.
Tonetti MS, Schmid J (1994). Pathogenesis of implant failures. Periodontol 2000 4:127-138. Tonetti MS (1998). Risk factors for osseodisintegration. Periodontol 2000 17:55-62. Touati B, Guez G (2002) Immediate implantation with provisionalization: from literature to clinical
implications. Pract Proced Aesthet Dent 14:699-707. Tressel T, McCarthy JB, Calaycay J, Lee TD, Legesse K, Shively JE, et al. (1991). Human plasma
fibronectin. Demonstration of structural differences between the A- and B-chains in the III CS region. Biochem J 274:731-738.
Uchida M, Shima M, Chikazu D, Fujieda A, Obara K, Suzuki H, et al. (2001). Transcriptional induction of matrix metalloproteinase-13 (collagenase-3) by 1alpha,25-dihydroxyvitamin D3 in mouse osteoblastic MC3T3-E1 cells. J Bone Miner Res 16:221-230.
Ueda M, Hibino Y, Niimi A (1999). Usefulness of dental implants in maxillofacial reconstruction. JLong Term Eff Med Implants 9:349-366.
Uitto VJ, Nieminen A, Coil J, Hurttia H, Larjava H (1996). Oral fluid elastase as an indicator of periodontal health. J Clin Periodontol 23:30-37.
Uitto VJ, Airola K, Vaalamo M, Johansson N, Putnins EE, Firth JD, et al. (1998). Collagenase-3 (matrix metalloproteinase-13) expression is induced in oral mucosal epithelium during chronic inflammation. Am J Pathol 152:1489-1499.
van der Zee E, Everts V, Hoeben K, Beertsen W (1994). Immunolocalisation of collagenase in rabbit periosteal tissue explants and extraction of the enzyme. The effect of the cytokines IL-1 alpha and EGF. J Cell Sci 107:1047-1053.
van der Zee E, Everts V, Beertsen W (1996). Cytokine-induced endogenous procollagenase stored in the extracellular matrix of soft connective tissue results in a burst of collagen breakdown following its activation. J Periodontal Res 31:483-488.
van der Zee E, Everts V, Beertsen W (1997). Cytokines modulate routes of collagen breakdown. Review with special emphasis on mechanisms of collagen degradation in the periodontium and the burst hypothesis of periodontal disease progression. J Clin Periodontol 24:297-305.
Vankemmelbeke M, Dekeyser PM, Hollander AP, Buttle DJ, Demeester J (1998). Characterization of helical cleavages in type II collagen generated by matrixins. Biochem J 330:633-640.
Vartio T, Laitinen L, Narvanen O, Cutolo M, Thornell LE, Zardi L, et al. (1987). Differential expression of the ED sequence-containing form of cellular fibronectin in embryonic and adult human tissues. J Cell Sci 88:419-430.
Vaughn BK, Dameron TB Jr, Bauer TW, Mochida Y, Akisue T, Eberle RW (1999). Early osteolysis following total hip arthroplasty with use of a Hylamer liner in combination with a modular ceramic femoral head. A case report. J Bone Joint Surg Am 81:1446-1449.
Verheijen JH, Nieuwenbroek NM, Beekman B, Hanemaaijer R, Verspaget HW, Ronday HK, et al.(1997). Modified proenzymes as artificial substrates for proteolytic enzymes: colorimetric assay of bacterial collagenase and matrix metalloproteinase activity using modified pro-urokinase. Biochem J 323:603-609.
Verhoeven JW, Cune MS (2000). Oblique lateral cephalometric radiographs of the mandible in implantology: usefulness and accuracy of the technique in height measurements of mandibular bone in vivo. Clin Oral Implants Res 11:39-43.
Visch LL, van Waas MA, Schmitz PI, Levendag PC (2002). A clinical evaluation of implants in irradiated oral cancer patients. J Dent Res 81:856-859.
Voitik AJ (1996). Corrosion of implantable materials and aging of bone. J Dent Technol 13:24-32. von Recum AF, Opitz H, Wu E (1993). Collagen types I and III at the implant/tissue interface. J
Biomed Mater Res 27:757-761.
78
Votta BJ, Levy MA, Badger A, Bradbeer J, Dodds RA, James IE, et al. (1997). Peptide aldehyde inhibitors of cathepsin K inhibit bone resorption both in vitro and in vivo. J Bone Miner Res12:1396-1406.
Wagner H, Wagner M (2001). Conus hip prosthesis. Acta Chir Orthop Traumatol Cech 68:213-221. Wahl LM, Wahl SM, Mergenhagen SE, Martin GR (1974). Collagenase production by endotoxin-
activated macrophages. Proc Natl Acad Sci U S A 71:3598-3601. Wallace RH (2000). The relationship between cigarette smoking and dental implant failure. Eur J
Prosthodont Restor Dent 8:103-106. Walther W, Klemke J, Worle M, Heners M (1996). Implant-supported single-tooth replacements: risk
of implant and prosthesis failure. J Oral Implantol 22:236-239. Wang JY, Wicklund BH, Gustilo RB, Tsukayama DT (1996). Titanium, chromium and cobalt ions
modulate the release of bone-associated cytokines by human monocytes/macrophages in vitro. Biomaterials 17:2233-2240.
Watts TL (1998). Periodontitis for medical practitioners. BMJ 316:993-996. Weinberg LA (1998). Reduction of implant loading using a modified centric occlusal anatomy. Int J
Prosthodont 11:55-69. Weiss CM (1986). Tissue integration of dental endosseous implants: description and comparative
analysis of the fibro-osseous integration and osseous integration systems. J Oral Implantol12:169-214.
Welgus HG, Jeffrey JJ, Eisen AZ (1981). The collagen substrate specificity of human skin fibroblast collagenase. J Biol Chem 256:9511-9515.
Westerlund U, Ingman T, Lukinmaa PL, Salo T, Kjeldsen L, Borregaard N, et al. (1996). Human neutrophil gelatinase and associated lipocalin in adult and localized juvenile periodontitis. JDent Res 75:1553-1563.
Winn DM, Brunelle JA, Selwitz RH, Kaste LM, Oldakowski RJ, Kingman A, et al. (1996). Coronal and root caries in the dentition of adults in the United States, 1988-1991. J Dent Res 75 Spec No:642-651.
Wiskott HW, Belser UC (1999). Lack of integration of smooth titanium surfaces: a working hypothesis based on strains generated in the surrounding bone. Clin Oral Implants Res 10:429-444.
Wolff JE (1985). Mechanics of the mandible with movable symphysis. Z Morphol Anthropol 76:25-35. Woolley DE, Davies RM (1981). Immunolocalization of collagenase in periodontal disease. J
Periodontal Res 16:292-297. Wright TM, Goodman SB (2000) Implant Wear in Total Joint Replacement: Clinical and Biologic
Issues, Material and Design Considerations: Symposium, Oakbrook, Illinois, American Academy of Orthopaedic Surgeons. p 61-70.
Wu JJ, Lark MW, Chun LE, Eyre DR (1991). Sites of stromelysin cleavage in collagen types II, IX, X, and XI of cartilage. J Biol Chem 266:5625-5628.
Wucherpfennig AL, Li YP, Stetler-Stevenson WG, Rosenberg AE, Stashenko P (1994). Expression of 92 kD type IV collagenase/gelatinase B in human osteoclasts. J Bone Miner Res 9:549-556.
Xu JW, Ma J, Li TF, Waris E, Alberty A, Santavirta S, et al. (2000). Expression of epidermal growth factor and transforming growth factor alpha in interfacial membranes retrieved at revision total hip arthroplasty. Ann Rheum Dis 59:822-827.
Yanagida I, Mori S (1990). Statistical studies on numerical anomalies of teeth in children using orthopantomograms--congenital hypodontia. Osaka Daigaku Shigaku Zasshi 35:580-593.
Ylanne J, Virtanen I (1989). The Mr 140,000 fibronectin receptor complex in normal and virus-transformed human fibroblasts and in fibrosarcoma cells: identical localization and function. Int J Cancer 43:1126-1136.
Yuhara S, Kasagi S, Inoue A, Otsuka E, Hirose S, Hagiwara H (1999). Effects of nicotine on cultured cells suggest that it can influence the formation and resorption of bone. Eur J Pharmacol383:387-393.
Zarb GA, Schmitt A (1991). Osseointegration and the edentulous predicament. The 10-year-old Toronto study. Br Dent J 170:439-444.