adverse drug reactions of oral cavity
TRANSCRIPT

ADVERSE DRUG REACTIONS OF ORAL CAVITY

ADVERSE DRUG REACTION
An appreciably harmful or unpleasant reaction, resulting from an intervention related to the use of a medicinal product, which predicts hazard from future administration and warrants prevention or specific treatment, or alteration of the dosage regimen, or withdrawal of the product
Edwards and Aronson 2000

ADVERSE DRUG REACTION
“Adverse drug event” includes
(1) harm caused by a drug (commonly
known as adverse drug reaction)
(2) harm caused by appropriate drug use
(usually referred to as a side effect)
(3) medication errors

BURDEN OF ADR
DRUG INDUCED ORAL REACTIONS
Hyposalivation/ hypersalivation Lichenoid reactions/lichen planus Apthous like ulcers Bullous disorders Pigmentation Fibrovascular hyperplasia Keratosis/epithelial hyperplasia Dysesthesia Osteonecrosis of jaw Infection Angioedema Malignancy

HYPOSALIVATION/XEROSTOMIA
Dry mouth is listed as an adverse effect for over 500 medications-Femiano etal 2011
The most frequently reported medication classes are
1. Antidepressants2. Antipsychotics3. Antihistamines4. Muscarinic receptor and a-receptor antagonists5. Antihypertensives (e.g., diuretics, b-blockers,
and angiotensin-converting enzyme [ACE] inhibitors)
6. Bronchodilators7. Skeletal muscle relaxants.

PERSISTENT HYPOSALIVATION CAUSES
SIALADENITIS
DENTAL CARIES
GLOSSO DYNIAGLOSSOPYROSIS

SIALORRHOEA Increased saliva Droling Increased swallowing Drugs responsible-
Alprazolam Xanax AmiodaroneClozapine Digoxin Galantamine Lamotrigine Levodopa Nifedipine

LICHENOID REACTION/ LICHEN PLANUSOral lichen planus (OLP) is a chronic
inflammatory disease that affects the mucus membrane of the oral cavity. It is a T-cell mediated autoimmune disease in which the cytotoxic CD8+ T cells trigger apoptosis of the basal cells of the oral epithelium.
Oral LP presents as white striations or papules often associated with erythema or erosion and ulcers, most commonly in a bilaterally symmetric manner, often on the buccal mucosa, tongue, and gingiva.

PATHOGENESIS OF OLPKeratinocyte antigen expression or unmasking of an antigen
T cells (mostly CD8+, and some CD4+ cells) migrate into the epithelium
Migrated CD8+ cells are activated directly by antigen binding to major histocompatibility complex (MHC)-1 on keratinocyte
Subsequent antigen presentation to CD4+ cells and Interleukin (IL)-12 activates CD4 + T helper cells which activate CD8+ T cells through receptor interaction, interferon γ (INF - γ) and IL-2


Wickham striae

LICHENOID HYPERSENSITIVITY REACTIONS The two classes of medications
historically associated with oral LHRs are
Nonsteroidal anti-inflammatory drugs (NSAIDs) and antihypertensive agents
Sulfonylurea antidiabetic medications (e.g., tolbutamide and glipizide)
Antifungals (e.g., ketoconazole)
Anticonvulsants (e.g.carbamazepine)
Immunomodulatory drugs (e.g. gold salts and penicillamine)
Sulfasalazine Allopurinol, and lithium have
been reported to elicit oral LHRs

Fixed drug eruptions (FDEs) in the oral cavity are lesions that recur at the same site each time the offending medication is taken
The presentation can range from bullous to erosive, hyperpigmented, pruitic, or erythematous lesions
First and second generation antihistamines are known to cause FDE
Fluconazole has caused lesions of the palatal mucosa and oral bullae
Naproxen and oxicams have caused lesions on the lips

APTHOUS LIKE ULCERS
ovoid to round ulcers usually 1 cm or less with a yellowish fibrinous membrane and surrounding erythema

NSAIDs were one of the earliest classes of drugs
associated with the development of aphthous-like
ulcers in the oral cavity
Piroxicam, in particular, was shown to cause such
ulcers
Naproxen,trimethoprim-sulfamethoxazole,
cyclooxygenase-2 inhibitors (e.g., refecoxib), and the
angiotensin receptor blocker losartan have been
implicated in the development of aphthous like
ulcers

5-fluorouracil CisplatinMethotrexate Hydroxyurea,
Stomatotoxic drugs


BULLOUS DISORDERSThe development of simultaneous oral and
cutaneous pemphigus vulgaris has been noted with the use of thiol radicale containing drugs, such as penicillamine and NSAIDs

Erythema multiforme (EM), major or minor, can affect both the skin and mucous membranes
EM of the skin and oral mucous membranes has been reported with the administration of infliximab and adalimumab
EM due to intake of diclofenac sodium

SJS and TEN almost always involve the mucous membranes of the mouth, eye, and genitalia, sometimes extensively


pigmentationMetabolites of such medications as the
tetracyclines, minocyclines, antimalarial drugs and phenazine dyes (e.g., clofazimine) may be deposited in the oral mucosa
Drug metabolites chelate with
Iron and melanin
pigmentation

Tetracycline stains
Zidovudine pigmentation

Drugs implicated in pigmentationTetracycline, minocycline
Imatinab
Zidovudine
Oral contraceptives
Chemotherapy agents
Antimalarials

Fibrovascular hyperplasiaCalcium channel blockers, in particular,
nifedipine and amlodipine, are antihypertensive agents that induce hyperplasia of the gingival tissue
Decreased cellular folic acid
Decreased activity of MMP
Failure to activate collagenase
Suggested mechanism

Gingival enlargement
Nifidipine induced Cyclosporin induced
Phenytoin induced

Dysesthesia
Oral dysesthesias,such as sensitivity, burning, dysgeusia, and other altered sensations without clinical signs, may be caused by medications
Salivary gland dysfunction
Low production of saliva
No solution for binding of chemoreceptors on taste buds over the tongue

Drugs causing Dysesthesia
Macrolides-such as clarithromycin (17%); antimycotics,-such as terbinafine (9%)
Fluoroquinolones (8%), Protein kinase inhibitors, ACE-inhibitors, Statins, Proton pump inhibitors
STOMATITIS WITH BMS

AGEUSIA-LOSS OF TASTE
Amitriptyline Angiotensin II Receptor
Blockers Aspirin Atorvastatin Clopidigral Enalapril Fluoxetine Indomethacin Phenytoin Spironolactone
DYSGEUSIA- TASTE DISTURBANCE
ACE Inhibitors Allopurinol
Alprazolam Aspirin Atorvastatin Baclofen Benztropine Diclofenac Cardizem
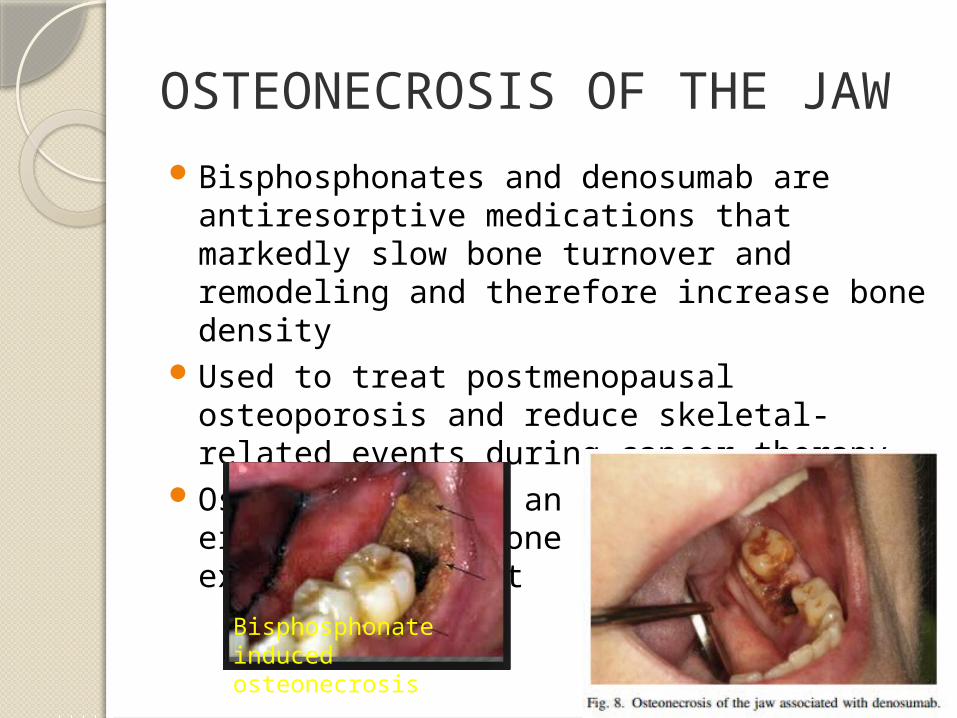
OSTEONECROSIS OF THE JAWBisphosphonates and denosumab are
antiresorptive medications that markedly slow bone turnover and remodeling and therefore increase bone density
Used to treat postmenopausal osteoporosis and reduce skeletal-related events during cancer therapy
Osteonecrosis is an ADE presenting as either exposed bone or a nonhealing extraction socket
Bisphosphonate induced osteonecrosis
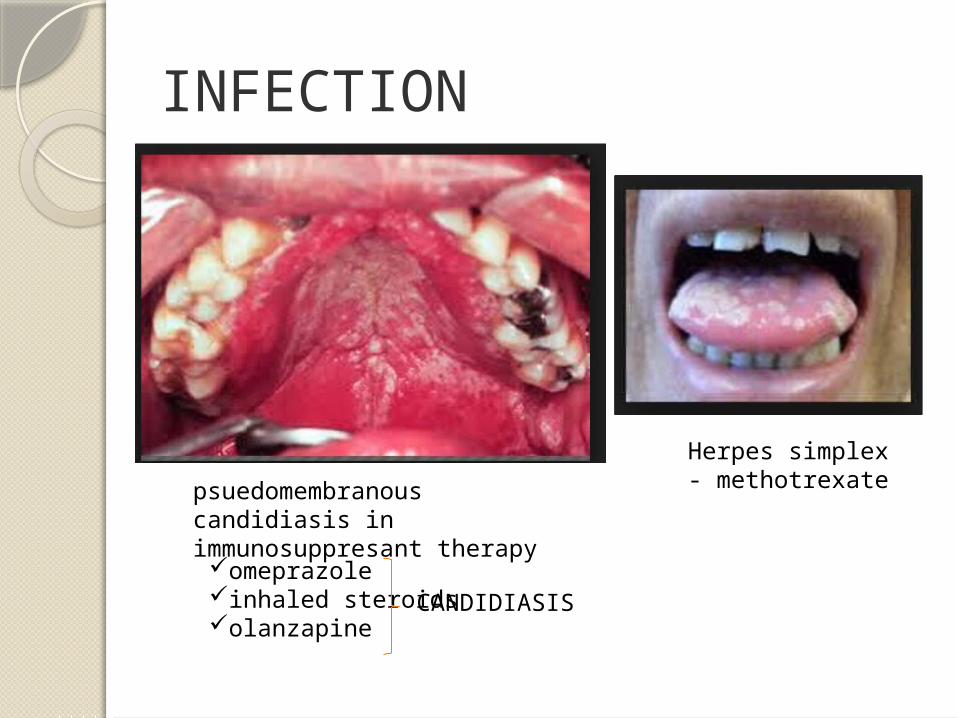
INFECTION
psuedomembranous candidiasis in immunosuppresant therapy
Herpes simplex - methotrexate
omeprazoleinhaled steroidsolanzapine
CANDIDIASIS

BLACK HAIRY TONGUE
Amitriptyline Cephalosporins
Clarithromycin Corticosteroids Prednisone
Clonazepam Lansoprazole Methyldopa Nortriptyline Penicillins
ANGULAR CHELITIS
Atorvastatin Methyldopa Prochlorperazine Simvastatin Sulfasalazine Tetracyclines Vitamin A

AngioedemaAntihypertensive
agents, such as angiotensin receptor blockers
Calcium channel blockers, hydrochlorothiazide
Antiplatelet agents, such as thienopyridine and clopidogrel
Abrupt-onset swelling of the orofacial region and lips can compromise the airway and be life-threatening.

MALIGNANCYA number of chemotherapy and
immunomodulating agents have been shown to increase the risk of lymphoproliferative disorders and neoplasms
Squamous cell carcinoma may develop in patients with oral LP treated with tacrolimus ointment
The issue of drug-induced malignancy is still controversial, and it is difficult to remove confounding factors from studies that show an association

Identification of the underlying pathogenesis of an ADR together with the severity of the reaction will have profound implications on continuation of drug therapy after an ADR
However, because the majority of ADRs is dose-dependent and therefore preventable, individualization of pharmacotherapy may have a major impact on reducing such events
ther umsch 2000