advancements in molecular breast imaging · ce directed reading 524m radioloic technology, may/june...
TRANSCRIPT

523MRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
CEDirected Reading
This article is a Directed Reading. Your access to Directed Reading quizzes for continuing education credit is determined by your membership status and CE preference.
Breast cancer is the second most deadly type of cancer affecting women, accounting for nearly 1 in 3 cancers in women. An esti-
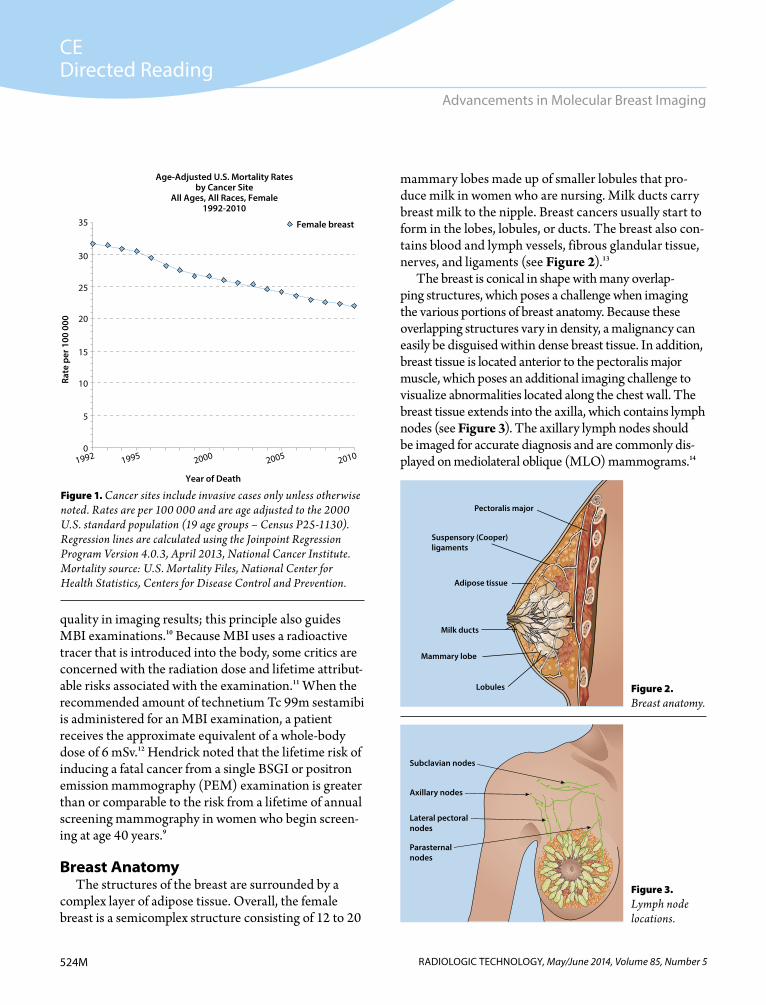
mated 2 830 000 women are living with breast cancer in the United States.1 The mortality rate from breast cancer has decreased, largely because of increased awareness and advancements in medi-cal imaging technology such as molecu-lar breast imaging (MBI) that aid in early detection (see Figure 1).2,3
Although breast cancer is com-mon among women, the disease does not discriminate between the sexes. Approximately 1% of all new breast cancer cases each year occur in men.4 Molecular breast imaging, sometimes referred to as breast-specific gamma imaging (BSGI), is a nuclear medicine procedure—specifically breast scin-tigraphy—that is cost-effective and improves lesion detection, especially in dense breasts. A nuclear medicine tech-nologist or physician injects the patient with technetium Tc 99m sestamibi, a radiopharmaceutical that accumulates
in tumor cells more than in other body cells because of tumor cells’ high meta-bolic activity. Cancer cells are highly metabolic with a higher cytoplasmic mitochondrial density, which causes them to uptake the majority of the trac-ing agent. When the radioactive tracers attach to cells with increased metabolic activity, the results show a highlighted area on the nuclear medicine image.5-8
A mammography unit first was used in the United States in 1969, and although the technology remains the most important tool used for breast cancer detection, the risk of radiation-induced breast cancer from mammogra-phy still is debated.9 As with mammog-raphy and all diagnostic medical imaging examinations that use radiation, physi-cians must weigh the risks of radiation dose with the benefits a test will provide when scheduling an MBI procedure.
In applying the ALARA (as low as reasonably achievable) principle, radio-logic technologists are tasked with keep-ing their patients’ radiation dose as low as possible while maintaining diagnostic
After completing this article, the reader should be able to:Explain breast anatomy and the significance of breast composition. List genetic factors related to breast cancer risk. Discuss traditional breast imaging modalities. Explain practice guidelines, clinical indications, and contraindications for molecular
breast imaging (MBI). Describe the equipment and procedures used for MBI. Discuss the advantages of MBI vs other breast imaging modalities.
Breast cancer is the most common cancer in women, but with early detection, it is a treatable disease. Mammography has long been the medical imaging standard for breast cancer screening, with other breast imaging modalities used as adjunct procedures to support diagnostic interpretation. Molecular breast imaging (MBI) was introduced in the past decade as a promising adjunct to mammography. Using a radiopharmaceutical and a dedicated imaging device, MBI technology helps physicians examine metabolic activity within the breast. This article provides a review of breast anatomy and composition, explores genetic factors related to breast cancer, and examines practice guidelines related to MBI.
Paula R McPeak, MSRS, R.T.(R)(M)
Advancements in Molecular Breast Imaging
CEDirected Reading
524M RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Advancements in Molecular Breast Imaging
quality in imaging results; this principle also guides MBI examinations.10 Because MBI uses a radioactive tracer that is introduced into the body, some critics are concerned with the radiation dose and lifetime attribut-able risks associated with the examination.11 When the recommended amount of technetium Tc 99m sestamibi is administered for an MBI examination, a patient receives the approximate equivalent of a whole-body dose of 6 mSv.12 Hendrick noted that the lifetime risk of inducing a fatal cancer from a single BSGI or positron emission mammography (PEM) examination is greater than or comparable to the risk from a lifetime of annual screening mammography in women who begin screen-ing at age 40 years.9
Breast AnatomyThe structures of the breast are surrounded by a
complex layer of adipose tissue. Overall, the female breast is a semicomplex structure consisting of 12 to 20
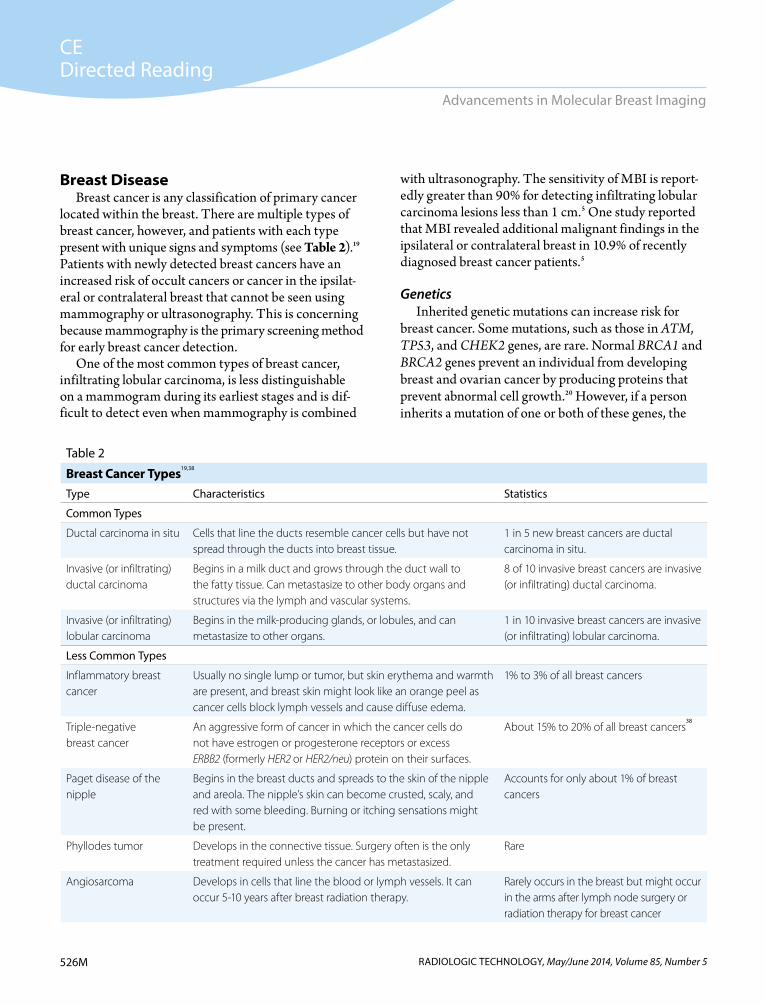
mammary lobes made up of smaller lobules that pro-duce milk in women who are nursing. Milk ducts carry breast milk to the nipple. Breast cancers usually start to form in the lobes, lobules, or ducts. The breast also con-tains blood and lymph vessels, fibrous glandular tissue, nerves, and ligaments (see Figure 2).13
The breast is conical in shape with many overlap-ping structures, which poses a challenge when imaging the various portions of breast anatomy. Because these overlapping structures vary in density, a malignancy can easily be disguised within dense breast tissue. In addition, breast tissue is located anterior to the pectoralis major muscle, which poses an additional imaging challenge to visualize abnormalities located along the chest wall. The breast tissue extends into the axilla, which contains lymph nodes (see Figure 3). The axillary lymph nodes should be imaged for accurate diagnosis and are commonly dis-played on mediolateral oblique (MLO) mammograms.14
Figure 1. Cancer sites include invasive cases only unless otherwise noted. Rates are per 100 000 and are age adjusted to the 2000 U.S. standard population (19 age groups – Census P25-1130). Regression lines are calculated using the Joinpoint Regression Program Version 4.0.3, April 2013, National Cancer Institute. Mortality source: U.S. Mortality Files, National Center for Health Statistics, Centers for Disease Control and Prevention.
Figure 2. Breast anatomy.
19920
5
10
15
20
25
30
35
1995 2000 2005
Age-Adjusted U.S. Mortality Ratesby Cancer Site
All Ages, All Races, Female1992-2010
Female breast
Year of Death
Rate
per
100
000
2010
©2013 ASRT. All rights reserved.
Pectoralis major
Mammary lobe
Suspensory (Cooper) ligaments
Lobules
Milk ducts
Adipose tissue
©2012 ASRT. All rights reserved.
Subclavian nodes
Axillary nodes
Lateral pectoralnodes
Parasternalnodes
Figure 3. Lymph node locations.

CEDirected Reading
525MRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
McPeak
Breast CompositionThe American College of Radiology (ACR) has pro-
vided terminology to identify breast density by categories and instructs radiologists to include this information when describing a patient’s breast composition in interpre-tive reports.15 Dense breast tissue is an important risk fac-tor for breast cancer because increased density represents a higher proportion of fibroglandular tissue than fatty tissue, and it has not yet been proven whether glandular tissue is more likely to develop cancer or whether it just obscures more tumors on imaging.15 In general, younger women who have not yet reached menopause have denser breasts than women who are older and have reached menopause.16 Mammography’s sensitivity decreases with highly dense tissue. In addition, adipose tissue is radiolu-cent, appearing dark on a mammogram, yet connective and epithelial tissues appear radiologically dense.
Breast cancer also appears radiologically dense on a mammogram, so other methods of imaging could improve detection. MBI yields a high sensitiv-ity for patients with extremely dense breast tissue. Radiopharmaceutical uptake by the mitochondria is not affected by breast tissue density, which makes MBI both highly sensitive and specific for imaging dense
breasts.17 The ACR’s Breast Imaging Reporting and Data System (BI-RADS) categories describe mammog-raphy findings, and BI-RADS classifies the percentage of glandular tissue and fatty tissue in a breast’s composi-tion (see Table 1 and Figure 4).
Table 1
American College of Radiology BI-RADS Categories of Mammographic Breast Density18
BI-RADS Category Characteristics
1 Predominately fat breast tissue. Fibrous and glandular tissue make up 25% of the breast.
2 Scattered densities in the breast tissue. Fibrous and glandular tissue make up 25%-50% of the breast.
3 Heterogeneously dense breast tissue made up of 51%-75% of fibrous and glandular tissue, making it difficult to see small masses on a mammogram.
4 Extremely dense breast tissue made up of 75% fibrous and glandular tissue, which can lead to some missed cancers.
Figure 4. Examples of variation in mammographic density. A. 0%. B. Less than 10%. C. Less than 25%. D. Less than 50%. E. Less than 75%. F. More than 75%. G. A computer-assisted measure. The outer (red) line shows the edge of the breast; the inner (green) line shows the edge of dense tissue. Percent density is calculated by dividing the dense area by the total area and multiplying by 100. Reprinted with permis-sion from Boyd NF, Martin LJ, Bronskill M, Yaffe MJ, Duric N, Minkin S. Breast tissue composition and susceptibility to breast cancer. J Natl Cancer Inst. 2010;102(16):1224-1237.
A
D
B
E
C
F G
CEDirected Reading
526M RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Advancements in Molecular Breast Imaging
Breast DiseaseBreast cancer is any classification of primary cancer
located within the breast. There are multiple types of breast cancer, however, and patients with each type present with unique signs and symptoms (see Table 2).19 Patients with newly detected breast cancers have an increased risk of occult cancers or cancer in the ipsilat-eral or contralateral breast that cannot be seen using mammography or ultrasonography. This is concerning because mammography is the primary screening method for early breast cancer detection.
One of the most common types of breast cancer, infiltrating lobular carcinoma, is less distinguishable on a mammogram during its earliest stages and is dif-ficult to detect even when mammography is combined
with ultrasonography. The sensitivity of MBI is report-edly greater than 90% for detecting infiltrating lobular carcinoma lesions less than 1 cm.5 One study reported that MBI revealed additional malignant findings in the ipsilateral or contralateral breast in 10.9% of recently diagnosed breast cancer patients.5
GeneticsInherited genetic mutations can increase risk for
breast cancer. Some mutations, such as those in ATM, TP53, and CHEK2 genes, are rare. Normal BRCA1 and BRCA2 genes prevent an individual from developing breast and ovarian cancer by producing proteins that prevent abnormal cell growth.20 However, if a person inherits a mutation of one or both of these genes, the
Table 2
Breast Cancer Types19,38
Type Characteristics Statistics
Common Types
Ductal carcinoma in situ Cells that line the ducts resemble cancer cells but have not spread through the ducts into breast tissue.
1 in 5 new breast cancers are ductal carcinoma in situ.
Invasive (or infiltrating) ductal carcinoma
Begins in a milk duct and grows through the duct wall to the fatty tissue. Can metastasize to other body organs and structures via the lymph and vascular systems.
8 of 10 invasive breast cancers are invasive (or infiltrating) ductal carcinoma.
Invasive (or infiltrating) lobular carcinoma
Begins in the milk-producing glands, or lobules, and can metastasize to other organs.
1 in 10 invasive breast cancers are invasive (or infiltrating) lobular carcinoma.
Less Common Types
Inflammatory breast cancer
Usually no single lump or tumor, but skin erythema and warmth are present, and breast skin might look like an orange peel as cancer cells block lymph vessels and cause diffuse edema.
1% to 3% of all breast cancers
Triple-negative breast cancer
An aggressive form of cancer in which the cancer cells do not have estrogen or progesterone receptors or excess ERBB2 (formerly HER2 or HER2/neu) protein on their surfaces.
About 15% to 20% of all breast cancers38
Paget disease of the nipple
Begins in the breast ducts and spreads to the skin of the nipple and areola. The nipple’s skin can become crusted, scaly, and red with some bleeding. Burning or itching sensations might be present.
Accounts for only about 1% of breast cancers
Phyllodes tumor Develops in the connective tissue. Surgery often is the only treatment required unless the cancer has metastasized.
Rare
Angiosarcoma Develops in cells that line the blood or lymph vessels. It can occur 5-10 years after breast radiation therapy.
Rarely occurs in the breast but might occur in the arms after lymph node surgery or radiation therapy for breast cancer

CEDirected Reading
527MRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
McPeak
individual is at an increased risk for both cancers. BRCA1 and BRCA2 gene mutations are linked to breast cancers that usually affect both breasts in younger women.20,21
Each year, approximately 10% of newly diagnosed breast cancers in women aged younger than 50 years occur in women who have a BRCA mutation.21 The American Cancer Society (ACS) reported that a BRCA1 mutation can increase an individual’s risk of breast cancer by as much as 80%, but the average risk ranges from 55% to 65%. A BRCA2 mutation increases breast cancer risk by approximately 45%.20
Understanding risk factors for developing breast can-cer can help patients make decisions about whether to undergo genetic testing and can help physicians advise women on the best course of action for screening and diagnostic examinations. If a close blood relative has had breast cancer, a woman’s risk is doubled, and if 2 first-degree relatives have had breast cancer, the risk is further increased. Nevertheless, 85% of women who develop breast cancer have no family history of the disease.20
Breast Imaging Breast imaging is part of a comprehensive approach
to breast cancer screening and diagnosis. The inten-tion of screening for breast cancer in asymptomatic women is to identify breast cancer before it is clinically apparent. Mammography still is the mainstay of breast cancer screening.22 ACS screening guidelines recom-mend that women have a clinical breast examination every 3 years between the ages of 20 and 39 and annu-ally beginning at age 40.23 The ACS also recommends annual screening mammograms for women aged 40 years and older. Women who have high breast cancer risk based on specific factors such as family history or known BRCA1 or BRCA2 mutations, or women who have not had genetic testing but have known first-degree relatives with BRCA mutations, should have annual mammograms and magnetic resonance (MR) breast imaging.24 Screening mammography and advanced medical imaging of the breast are essential in finding breast cancers while they are smaller and still confined to the breast.20
Although screening and diagnostic mammography are the most important and common imaging proce-dures used for breast evaluation, breast tomosynthesis,
ultrasonography, MR imaging, and scintimammog-raphy all are used in breast imaging for detecting or defining breast cancer and for planning treatment for the disease.
MammographyMammography is the most common screening
modality for breast cancer, and a screening mammo-gram is the only breast imaging examination for which a woman can self-refer.22,23,25 Multiple studies have shown that mammography effectively detects breast cancers and actively contributes to lower mortality rates from the disease. The compression device that f lattens the breast anatomy is one feature that makes mammog-raphy an excellent tool for screening.
During a routine screening mammogram, a mam-mographer acquires bilateral images of the patient’s breasts, typically with 2 projections per breast: a cranio-caudal (CC) and an MLO projection. If the patient has signs or symptoms of breast cancer, a diagnostic mam-mogram might be ordered for the affected breast that includes the routine CC and MLO projections, along with additional projections such as coned compression, exaggerated CC, cleavage, and 30° oblique projections as requested by the radiologist.26
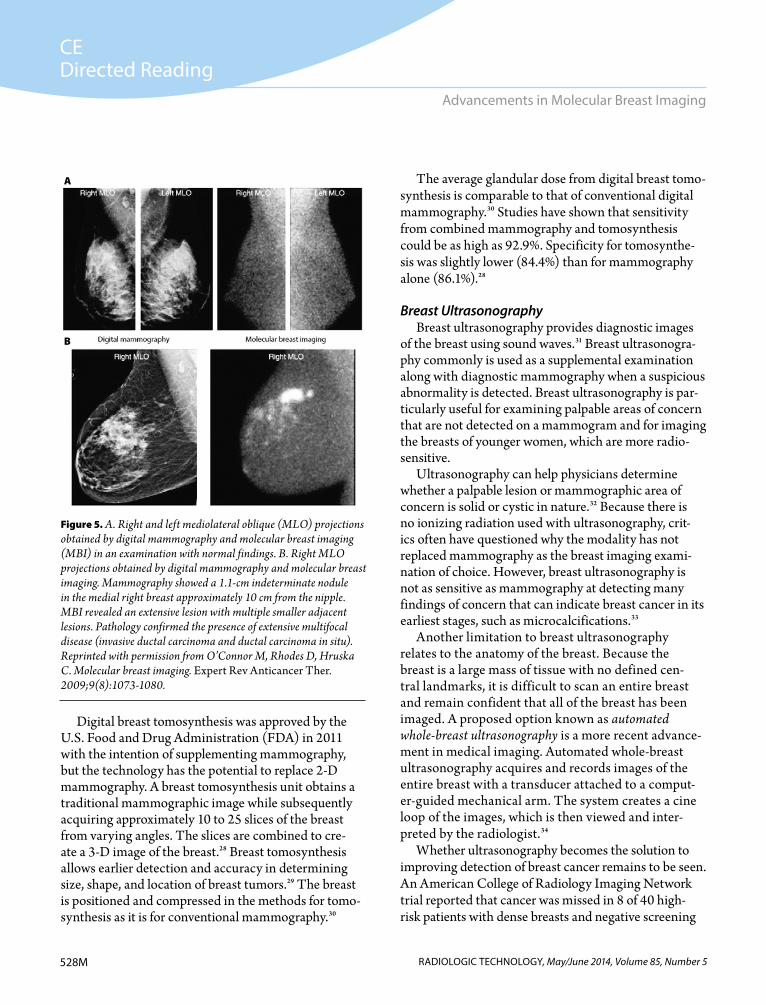
Although statistics repeatedly verify mammog-raphy’s effectiveness in breast cancer detection, the screening and diagnostic method is not 100% accurate. The sensitivity for mammography is reported to be approximately 87% to 97% in women with more fatty tissue in the breast and as low as 30% to 48% in patients with a higher ratio of dense breast tissue.25 Figure 5 demonstrates a comparison between digital mammog-raphy and a molecular breast imaging study. Because mammography has limitations, research to find a better imaging tool for the breast continues.27
Digital Breast TomosynthesisExerting force onto the breast with a compression
paddle during screening or diagnostic mammography helps prevent overlapping of anatomical structures, yet even with appropriate compression, it is impossible to completely eliminate structural superimposition. The ability to display the breast in 3-D can overcome the limitations of structural superimposition in breast imaging.
CEDirected Reading
528M RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Advancements in Molecular Breast Imaging
Digital breast tomosynthesis was approved by the U.S. Food and Drug Administration (FDA) in 2011 with the intention of supplementing mammography, but the technology has the potential to replace 2-D mammography. A breast tomosynthesis unit obtains a traditional mammographic image while subsequently acquiring approximately 10 to 25 slices of the breast from varying angles. The slices are combined to cre-ate a 3-D image of the breast.28 Breast tomosynthesis allows earlier detection and accuracy in determining size, shape, and location of breast tumors.29 The breast is positioned and compressed in the methods for tomo-synthesis as it is for conventional mammography.30
The average glandular dose from digital breast tomo-synthesis is comparable to that of conventional digital mammography.30 Studies have shown that sensitivity from combined mammography and tomosynthesis could be as high as 92.9%. Specificity for tomosynthe-sis was slightly lower (84.4%) than for mammography alone (86.1%).28
Breast UltrasonographyBreast ultrasonography provides diagnostic images
of the breast using sound waves.31 Breast ultrasonogra-phy commonly is used as a supplemental examination along with diagnostic mammography when a suspicious abnormality is detected. Breast ultrasonography is par-ticularly useful for examining palpable areas of concern that are not detected on a mammogram and for imaging the breasts of younger women, which are more radio-sensitive.
Ultrasonography can help physicians determine whether a palpable lesion or mammographic area of concern is solid or cystic in nature.32 Because there is no ionizing radiation used with ultrasonography, crit-ics often have questioned why the modality has not replaced mammography as the breast imaging exami-nation of choice. However, breast ultrasonography is not as sensitive as mammography at detecting many findings of concern that can indicate breast cancer in its earliest stages, such as microcalcifications.33
Another limitation to breast ultrasonography relates to the anatomy of the breast. Because the breast is a large mass of tissue with no defined cen-tral landmarks, it is difficult to scan an entire breast and remain confident that all of the breast has been imaged. A proposed option known as automated whole-breast ultrasonography is a more recent advance-ment in medical imaging. Automated whole-breast ultrasonography acquires and records images of the entire breast with a transducer attached to a comput-er-guided mechanical arm. The system creates a cine loop of the images, which is then viewed and inter-preted by the radiologist.34
Whether ultrasonography becomes the solution to improving detection of breast cancer remains to be seen. An American College of Radiology Imaging Network trial reported that cancer was missed in 8 of 40 high-risk patients with dense breasts and negative screening
Figure 5. A. Right and left mediolateral oblique (MLO) projections obtained by digital mammography and molecular breast imaging (MBI) in an examination with normal findings. B. Right MLO projections obtained by digital mammography and molecular breast imaging. Mammography showed a 1.1-cm indeterminate nodule in the medial right breast approximately 10 cm from the nipple. MBI revealed an extensive lesion with multiple smaller adjacent lesions. Pathology confirmed the presence of extensive multifocal disease (invasive ductal carcinoma and ductal carcinoma in situ). Reprinted with permission from O’Connor M, Rhodes D, Hruska C. Molecular breast imaging. Expert Rev Anticancer Ther. 2009;9(8):1073-1080.
A
B

CEDirected Reading
529MRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
McPeak
mammography findings when mammography and ultrasonography were combined; these results helped to emphasize the need for improved breast imaging technology.12
Breast Magnetic Resonance Imaging Breast MR imaging helps physicians examine struc-
tures of the breast by displaying the breast’s form along with vascular activity. Breast MR imaging displays a particularly high sensitivity (88%-99%) but a reported specificity as low as 37%, which has caused critics to question the modality’s efficacy.35 Breast MR uses high-energy magnetic fields and an enhancing contrast medium to highlight the hydrogen atoms located within breast tissue.36 Because the breast comprises varying tissue densities, MR imaging is effective at displaying cancers that might have been otherwise undetectable on a mammogram.
Breast MR is more expensive than mammography and is not easily justified as a breast screening examina-tion unless a patient fits the specific criteria outlined by the ACS.27 MR is particularly helpful for women who are at high risk for breast cancer, who have heteroge-neously dense breast tissue, and who are undergoing breast cancer treatment planning or staging.37 Breast MR imaging can assist in assessing lumpectomy sites following surgery for breast cancer, evaluating changes in scars, detecting recurrent cancers, or assessing tumor changes after chemotherapy.37
The ACS has not found sufficient evidence to sug-gest that breast MR should replace mammography as a screening tool; however, evidence suggests MR’s usefulness as an adjunct screening tool in select patient populations.38 Limitations to breast MR include cost, insurance coverage, and less accessibility to MR scan-ners than to mammography units.39 Because the equip-ment is large and an expensive investment, it might not be practical for all women’s imaging centers to offer the examination on site.
MBI could emerge as a solution for many limitations of mammography and breast MR imaging. The advan-tages of MBI compared to breast MR include40:
Lower cost. Usefulness in all patient populations in which breast
imaging is indicated. (MR is contraindicated for patients who have a pacemaker, for example.)
Patient comfort. Shorter interpretation times. A higher specificity rating.Studies have suggested that because an MBI
examination acquires fewer images than a breast MR examination, there is less room for error during interpretation of MBI.35 Additional research should be conducted to determine whether MBI should be used as an adjunct to mammography and ultrasonography instead of breast MR.
Nuclear Medicine Breast Imaging TechniquesWith breast cancer awareness on the rise and statis-
tics proving that early detection can improve survival, many technological advances are aimed at improving breast imaging sensitivity. Nuclear medicine technology helps physicians evaluate both anatomy and function when accumulation of an injected radioactive tracer highlights areas within the body that have high vascu-larity or metabolic activity.6,39,41
ScintimammographyScintimammography is the term that commonly
describes a nuclear medicine examination of the breast. Scintimammography was first introduced in the early 1990s and uses a general large field of view nuclear medicine -camera and technetium Tc 99m methoxyisobutylisonitrile (Tc 99m MIBI). The tech-nologist acquires images with the patient in the prone, breast-pendant position. The use of the large field of view camera makes detector positioning challeng-ing and compromises spatial resolution because the pendant breasts are 4 to 6 cm from the surface of the collimator.5
Although the specificity for primary breast lesions in scintimammography is high (86%-89%), sensitivity for detecting lesions less than 1 cm is low. Large field of view -cameras have a 35% to 65% sensitivity rate when imaging cancers less than or equal to 1 cm.7 Research in nuclear medicine imaging of the breast began to focus on early detection and developing a camera with higher resolution that could display minute breast lesions. As a result, the use of conventional -cameras decreased.5 As technology has developed, 3 specific nuclear medi-cine techniques related to scintimammography have emerged.5

CEDirected Reading
530M RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Advancements in Molecular Breast Imaging
Positron Emission MammographyPositron emission mammography (PEM) uses f lu-
deoxyglucose F 18. The technologist acquires images of patients for a 10-minute period 1 hour after injection of the radiopharmaceutical. Positioning of the patient and breast for PEM is similar to mammography, and slight compression is used. PEM has shown a high sensitivity rate (90%) and the ability to display breast lesions that are not visible on mammograms or ultrasonograms.42 PEM images are acquired in the same projections as screening and diagnostic mammograms, which improves the radiologist’s ability to correlate findings on mammograms and PEM images.41
A study comparing MR imaging of the breast with PEM concluded that MR imaging had better lesion-level sensitivity, but PEM had greater specificity at the breast and lesion levels. Fourteen women in the study (3.6%) had tumors that were not visible on MR scans but could be seen on PEM images.42
Breast-Specific Gamma ImagingBreast-specific gamma imaging (BSGI) often also is
included with the general term MBI. The interchange-able terms can be confusing, however, because of dif-ferences in technology. Both use small field of view -cameras specially designed for breast imaging, but BSGI uses a sodium-iodide scintillation detector, and MBI uses cadmium-zinc-telluride digital detectors.43 The first BSGI camera became commercially available in 2004,32 and more than 250 000 patients have had a BSGI procedure worldwide as of 2011, according to Dilon Technologies Inc (March 2014).
Many health care providers have recognized the important contribution that scintigraphy can make in breast imaging and have continued to introduce a form of scintimammography into the health care setting over the past 10 years with the common goal of early breast cancer detection. The term breast-specific gamma imag-ing has been questioned because use of the word gamma tends to intimidate or alarm the public. More recently, companies have begun to use molecular breast imaging as a more palatable term.44
Molecular Breast ImagingMBI uses a breast-optimized small field of view
-camera with technetium Tc 99m MIBI. Image
acquisition can begin about 5 to 10 minutes after injection.45 The technologist acquires images with the patient in a seated position with the breast slightly com-pressed, and the specially designed camera allows the technologist to maneuver the detector into positioning options to acquire images of the maximum amount of breast tissue.5 The small field of view -camera improves signal-to-noise ratio and spatial resolution. The introduction of small field of view cameras for molecular imaging of the breast has greatly improved lesion localization and detection of small occult breast cancers.35 The MBI camera can be equipped with a 15° slanted collimator that allows imaging of lesions close to the chest wall.23
MBI produces high-contrast images of lesions as small as less than 1 cm. The sensitivity rate of imag-ing lesions less than or equal to 0.7 cm was reported at 88.5% in one study.5,46 The high-resolution cameras have high photon sensitivity and are offered in different sized detectors for different sized breasts.
The MBI detector makes it possible to minimize the object-to-image distance by allowing the patient’s breast to rest virtually on the detector. The detector is small and portable, making it easy for small imaging centers to add MBI without adding a separate nuclear medicine department. The detector’s range of motion allows the technologist to image the breast with angles similar to mammography so that image comparison is more accurate for diagnosis and localization.6 This range of motion also allows for precise imaging of the axilla.
Practice Guidelines and Clinical Indications
The Society of Nuclear Medicine and Molecular Imaging (SNMMI) is the professional organization that provides guidance on the application of nuclear medicine studies. This professional organization com-prises physicians, technologists, and scientists who are dedicated to continuing research and developing com-petencies related to the field of nuclear medicine.5,6,47 Guidelines for breast scintigraphy with breast-specific -cameras have been developed to ensure quality examinations to facilitate diagnostic interpretation. The guidelines are to educate and offer general practice suggestions and can be altered by the overseeing practi-tioner if warranted.47 The current guidelines developed

CEDirected Reading
531MRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
McPeak
by the SNMMI were adopted in 2010 and cover clinical indications, qualifications of personnel, an explanation of the procedure, documentation policies, equipment specifications, quality control policies, and radiation safety practices.47
The SNMMI clinical guidelines, along with ACR appropriateness criteria, are intended to help breast imag-ing practitioners and referring physicians when they are selecting patients for MBI procedures. For example, the ACR rates BSGI appropriateness low and relative radia-tion risk level high for BSGI with Tc 99m MIBI (ie, MBI) for screening, even in high-risk women.48 When a breast cancer has been identified, MBI can be used to assess whether the disease is multicentric, multifocal, confined to one or both breasts, or extended to more than one quadrant and whether the cancer has metastasized to the lymph nodes (ie, initial staging).47
MBI also can assist in evaluating the response of a breast tumor to neoadjuvant chemotherapy and is a noninvasive monitoring method.49 In addition, MBI is helpful for detecting suspected recurrence of breast cancer, as a follow-up examination when the initial mammogram was limited, or if a previous malignancy was not found on a mammogram. Patients who have tested positive for the BRCA1 or BRCA2 gene mutation also are good candidates for MBI.47
An MBI study conducted on patients with known malignancies showed radiotracer uptake in additional areas of concern for 18 of 82 patients. Seventeen of the 18 patients underwent additional biopsies in which 9 areas of concern were found and excision was deter-mined necessary. Of the 9 areas identified, 6 were diag-nosed as cancer. This study showed that MBI is effec-tive in detecting new occult cancers that could alter the course of a patient’s treatment.17
Patients who have had a lumpectomy for a prior breast cancer are monitored closely with surveillance mammograms because of concerns about recurrence near the lumpectomy site. A research study involving 513 women with breast-conserving surgery following a breast cancer diagnosis reported that 42 of the 513 women developed recurrence in close proximity to their lumpectomy site. Because women with a prior history of breast cancer have a higher incidence of recurrence and scar tissue that makes imaging more difficult, MBI is valuable in the early detection of recurrence.47,50
Often a patient has an indeterminate abnormality within a breast, such as nipple discharge, palpable abnormalities not visible with mammography or sonog-raphy, multiple masses, or unexplained architectural distortion.47 When these conditions occur, it is the phy-sician’s responsibility to determine the cause.
Even if a mammographic finding is normal, nipple discharge indicates further testing. Underlying breast cancer has been reported in 5% to 12% of patients who presented with nipple discharge.51 Not all forms of nipple discharge are a concern. The color, presence of blood, ductal location, and whether the discharge is from one or both breasts can indicate malignancy but are not final determining factors. Nipple discharge can be caused by hormones, bacteria, a small benign mass in the breast, or by breast cancer. If mammogram findings are negative and nipple discharge is present, ductogra-phy usually is indicated.52 If a ductography examination is unsuccessful, an MBI study is indicated to evaluate the nipple discharge.47
When a physician discovers a new palpable lesion that cannot be seen on mammograms or ultrasonograms, MBI might be warranted to evaluate the abnormality. MBI could be beneficial in evaluating multiple areas of concern, such as masses or clusters of microcalcifica-tions, and to aid in biopsy targeting. If an area of concern is seen on only one mammographic projection, ultra-sonography or spot imaging can help in evaluation, but MBI could be used to assess the metabolic activity of the lesion. When axillary lymph node metastases are present but the primary tumor location is unknown, MBI can be useful in evaluating the breast for occult disease.
MBI is recommended in patients who have extremely dense breasts and patients with augmented breasts. Approximately two-thirds of premenopausal women in their 40s have extremely dense breast tissue. Although digital mammography has greatly improved the qual-ity of mammograms when imaging dense breast tissue, some radiologists believe that mammography is ineffec-tive for imaging extremely dense breasts.43 Because MBI overcomes the limitations presented by dense breast tis-sue, this technology can be a useful adjunct for younger patients and all women with dense breasts.25,40
The number of breast implant procedures performed in 2005 was reported to be 364 610, and more than half of the implants were placed in women aged younger
CEDirected Reading
532M RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Advancements in Molecular Breast Imaging
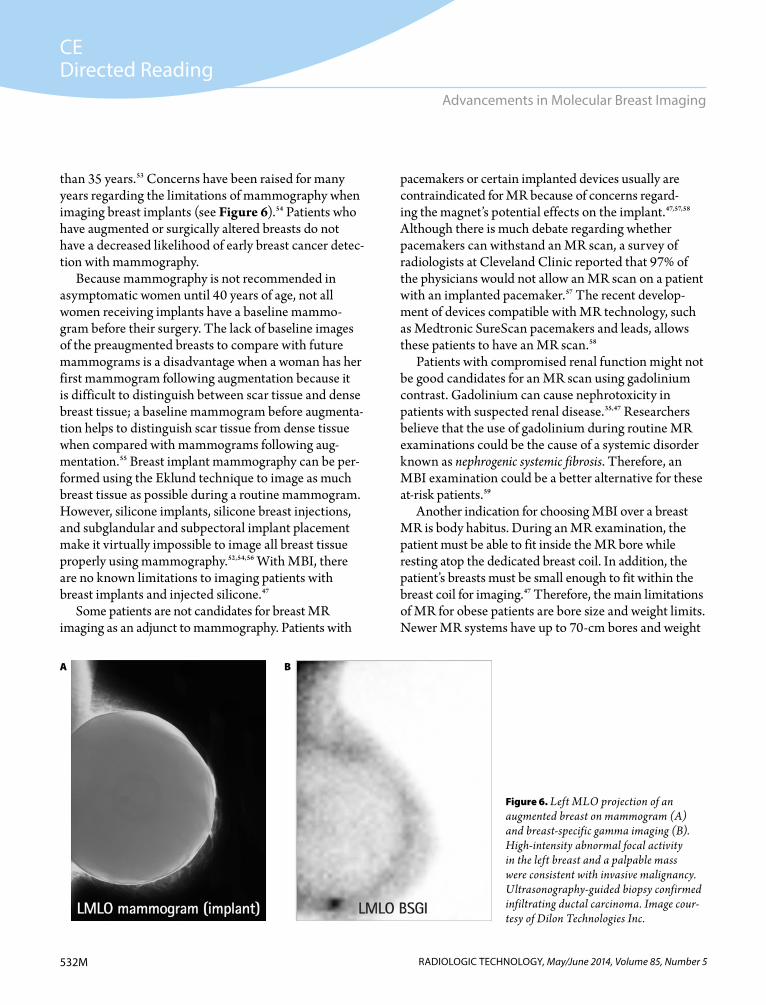
than 35 years.53 Concerns have been raised for many years regarding the limitations of mammography when imaging breast implants (see Figure 6).54 Patients who have augmented or surgically altered breasts do not have a decreased likelihood of early breast cancer detec-tion with mammography.
Because mammography is not recommended in asymptomatic women until 40 years of age, not all women receiving implants have a baseline mammo-gram before their surgery. The lack of baseline images of the preaugmented breasts to compare with future mammograms is a disadvantage when a woman has her first mammogram following augmentation because it is difficult to distinguish between scar tissue and dense breast tissue; a baseline mammogram before augmenta-tion helps to distinguish scar tissue from dense tissue when compared with mammograms following aug-mentation.55 Breast implant mammography can be per-formed using the Eklund technique to image as much breast tissue as possible during a routine mammogram. However, silicone implants, silicone breast injections, and subglandular and subpectoral implant placement make it virtually impossible to image all breast tissue properly using mammography.52,54,56 With MBI, there are no known limitations to imaging patients with breast implants and injected silicone.47
Some patients are not candidates for breast MR imaging as an adjunct to mammography. Patients with
pacemakers or certain implanted devices usually are contraindicated for MR because of concerns regard-ing the magnet’s potential effects on the implant.47,57,58 Although there is much debate regarding whether pacemakers can withstand an MR scan, a survey of radiologists at Cleveland Clinic reported that 97% of the physicians would not allow an MR scan on a patient with an implanted pacemaker.57 The recent develop-ment of devices compatible with MR technology, such as Medtronic SureScan pacemakers and leads, allows these patients to have an MR scan.58
Patients with compromised renal function might not be good candidates for an MR scan using gadolinium contrast. Gadolinium can cause nephrotoxicity in patients with suspected renal disease.35,47 Researchers believe that the use of gadolinium during routine MR examinations could be the cause of a systemic disorder known as nephrogenic systemic fibrosis. Therefore, an MBI examination could be a better alternative for these at-risk patients.59
Another indication for choosing MBI over a breast MR is body habitus. During an MR examination, the patient must be able to fit inside the MR bore while resting atop the dedicated breast coil. In addition, the patient’s breasts must be small enough to fit within the breast coil for imaging.47 Therefore, the main limitations of MR for obese patients are bore size and weight limits. Newer MR systems have up to 70-cm bores and weight
Figure 6. Left MLO projection of an augmented breast on mammogram (A) and breast-specific gamma imaging (B). High-intensity abnormal focal activity in the left breast and a palpable mass were consistent with invasive malignancy. Ultrasonography-guided biopsy confirmed infiltrating ductal carcinoma. Image cour-tesy of Dilon Technologies Inc.
A B

CEDirected Reading
533MRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
McPeak
limits between 400 lb and 550 lb.60 MR image quality is somewhat affected by obesity; increased body habitus can cause noise, and the necessity for a large field of view decreases resolution. Patient contact with the bore can degrade MR images, and open bore systems usually have a lower field strength, which also degrades image quality and requires longer examination times.61
MBI might be a better option for patients who have claustrophobia and might be unwilling or unable to undergo an MR scan without sedation. Using seda-tion does not guarantee a successful MR scan free of motion in patients with claustrophobia. Premedication for sedation requires that a patient make transporta-tion arrangements and sign the informed consent form before being medicated. Further, staff at a facility per-forming an MR scan with sedation must be qualified to handle a patient who has taken these medications. Because MBI is a shorter procedure requiring no seda-tion, it is a more appropriate choice for these patients.
When a patient presents with breast cancer requiring chemotherapy, research has suggested that the chemo-therapy be started before surgery or as neoadjuvant therapy. Following neoadjuvant chemotherapy with medical imaging allows physicians to determine tumor shrinkage or growth and whether the chosen chemo-therapy regimen is optimal for a particular patient. MBI can be used to monitor tumor response to neoadjuvant chemotherapy. In a study by Mitchell et al, the authors showed that MBI images acquired 3 to 5 weeks after neoadjuvant chemotherapy were accurate in predicting the presence or absence of residual disease after patients had completed the chemotherapy regimen.62
Finally, sometimes an MBI examination could be used to set a patient’s mind at ease by providing infor-mation to accurately describe a significant finding.47
Clinical ContraindicationsMBI is considered a safe examination for virtually
the entire patient population. There is a rare incidence of allergic reaction including anaphylactic events, angioedema, and generalized hives with itching for some patients following the administration of techne-tium Tc 99m MIBI.63 In clinical breast imaging trials involving 673 women, 19.2% reported alterations in taste and 1.6% reported headache. No anaphylaxis,
chest pain, or ST segment changes on electrocardiogra-phy were reported among study participants (see Table 3).63 Another study performed in Europe over a 2-year period reported allergic reactions in fewer than 0.025% of cases.64
The SNMMI Procedure Guidelines for the Use of Radiopharmaceuticals 4.0 state that “female patients who are postmenarcheal and premenopausal should be asked about pregnancy, lactation, and breast feeding” before receiving radiopharmaceuticals. In addition, the guidelines recommend that pregnancy testing be performed before using any radiopharmaceutical that could expose an embryo or fetus to 50 mSv of radiation or more.65 If possible, women who are pregnant should refrain from nuclear medicine scans, including MBI.66
Examination Procedure Patient Preparation
Other than providing a medical history to include possibility of pregnancy and current lactation practices, patients require no specific preparation or premedica-tion for the MBI examination. For best results, how-ever, women undergoing an MBI should schedule the examination for a time between the 2nd and the 14th day preceding the onset of menstruation.5,67 Women who are lactating might be asked to postpone their MBI examination until 3 months after lactation cessation.5 In addition, if a patient has had a recent cyst aspira-tion or biopsy performed within the breast, the MBI
Table 3
Selected Adverse Events in Women Who Received Technetium Tc 99m Sestamibi63
Adverse Effect ona: N 673 (%)
Special senses 132 (19.6)
Taste alteration 129 (19.2)
General body effects 21 (3.1)
Head (headache) 11 (1.6)
Cardiovascular system 9 (1.3)
Digestive system 8 (1.2)
Smell (parosmia, or distorted odor perception) 8 (1.2)
Gastrointestinal system (nausea) 4 (0.6)a Events reported in more than 0.5% of women who received the
radiopharmaceutical as part of a clinical study.
CEDirected Reading
534M RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Advancements in Molecular Breast Imaging
examination should be scheduled within 3 days of the surgical procedure to avoid false-positive results at the site.47
ExaminationThe MBI examination typically takes place in a
designated nuclear medicine suite. The nuclear medi-cine technologist introduces an intravenous line in the patient’s arm on the contralateral side of the breast to be imaged and administers the radiopharmaceuti-cal.6,44,47 Imaging can begin approximately 5 to 10 minutes after injection. The patient is seated, and the technologist places the breast onto the detector’s sup-portive device. The breast compression used for MBI is minimal, about one-third that used in conventional mammography, which might alleviate some anxiety associated with mammography.45
An upper paddle on the MBI unit lightly supports the superior breast tissue and minimizes radiation scat-ter from the injected pharmaceutical. The technolo-gist acquires a craniocaudal and mediolateral oblique projection of each breast, each with a scan time of 10 minutes, for a total time of 40 minutes.45
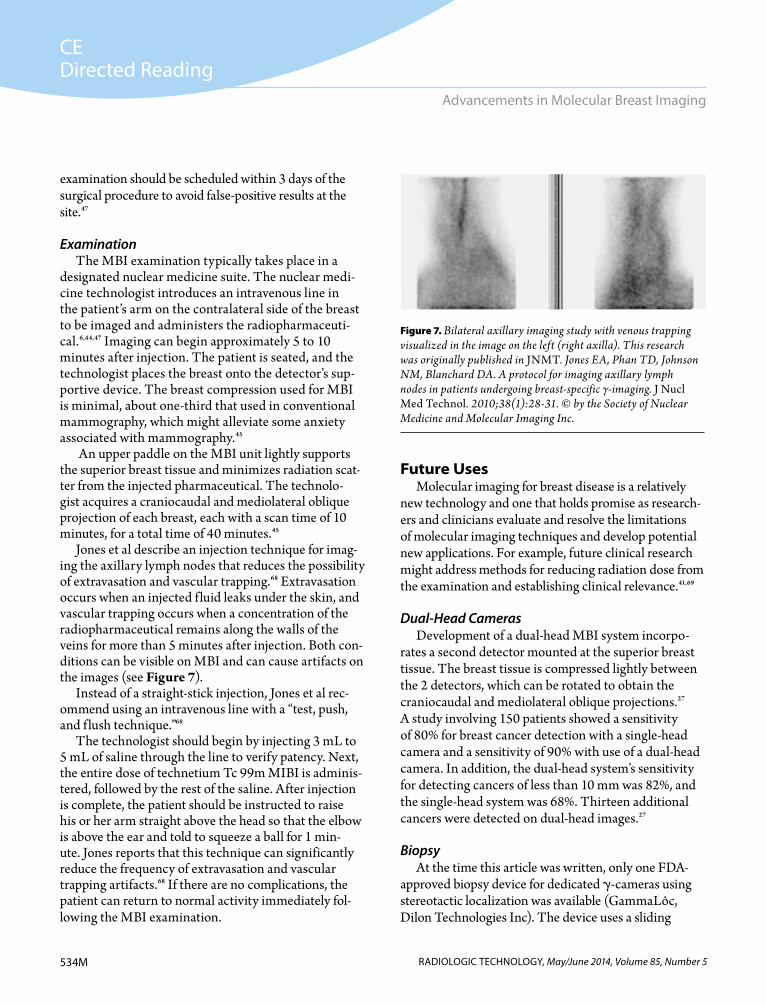
Jones et al describe an injection technique for imag-ing the axillary lymph nodes that reduces the possibility of extravasation and vascular trapping.68 Extravasation occurs when an injected f luid leaks under the skin, and vascular trapping occurs when a concentration of the radiopharmaceutical remains along the walls of the veins for more than 5 minutes after injection. Both con-ditions can be visible on MBI and can cause artifacts on the images (see Figure 7).
Instead of a straight-stick injection, Jones et al rec-ommend using an intravenous line with a “test, push, and f lush technique.”68
The technologist should begin by injecting 3 mL to 5 mL of saline through the line to verify patency. Next, the entire dose of technetium Tc 99m MIBI is adminis-tered, followed by the rest of the saline. After injection is complete, the patient should be instructed to raise his or her arm straight above the head so that the elbow is above the ear and told to squeeze a ball for 1 min-ute. Jones reports that this technique can significantly reduce the frequency of extravasation and vascular trapping artifacts.68 If there are no complications, the patient can return to normal activity immediately fol-lowing the MBI examination.
Future UsesMolecular imaging for breast disease is a relatively
new technology and one that holds promise as research-ers and clinicians evaluate and resolve the limitations of molecular imaging techniques and develop potential new applications. For example, future clinical research might address methods for reducing radiation dose from the examination and establishing clinical relevance.41,69
Dual-Head CamerasDevelopment of a dual-head MBI system incorpo-
rates a second detector mounted at the superior breast tissue. The breast tissue is compressed lightly between the 2 detectors, which can be rotated to obtain the craniocaudal and mediolateral oblique projections.27 A study involving 150 patients showed a sensitivity of 80% for breast cancer detection with a single-head camera and a sensitivity of 90% with use of a dual-head camera. In addition, the dual-head system’s sensitivity for detecting cancers of less than 10 mm was 82%, and the single-head system was 68%. Thirteen additional cancers were detected on dual-head images.27
BiopsyAt the time this article was written, only one FDA-
approved biopsy device for dedicated -cameras using stereotactic localization was available (GammaLôc, Dilon Technologies Inc). The device uses a sliding
Figure 7. Bilateral axillary imaging study with venous trapping visualized in the image on the left (right axilla). This research was originally published in JNMT. Jones EA, Phan TD, Johnson NM, Blanchard DA. A protocol for imaging axillary lymph nodes in patients undergoing breast-specific γ-imaging. J Nucl Med Technol. 2010;38(1):28-31. © by the Society of Nuclear Medicine and Molecular Imaging Inc.

CEDirected Reading
535MRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
McPeak
slant-hole collimator to obtain 2 separate gamma images that facilitate localization. The patient sits upright in the imaging position, and the physician inserts a needle into the lesion through a grid-support and needle posi-tioning block, which is also the compression paddle.69
This biopsy device makes it possible to sample a sus-picious area displayed on a patient’s MBI examination without having to use mammography or ultrasonog-raphy correlation to locate the suspicious lesion. The procedure takes about 90 minutes.69 A research study conducted on 25 patients undergoing the new biopsy procedure yielded 6 malignancies and 16 high-risk lesions. Of the 6 malignancies detected, all were con-firmed as ductal carcinoma in situ.70,71
Breast Density and Mammography Reporting ActBecause mammography is less effective in women
with dense breasts—the sensitivity of the examina-tion decreases from an average of 66% to 85% to as low as 30%—it is important that women with dense breasts be aware that their mammogram could result in a false-positive result.17,34 The Breast Density and Mammography Reporting Act of 2013, also known as HR 3404, is a federal bill that would mandate how a mammography report is dictated and delivered to a patient with dense breast tissue.
Under the bill, radiologists would be required to include “information regarding the patient’s breast density and language communicating that individuals with more dense breasts may benefit from supplemen-tal screening tests.”72 The bill had not been passed at the time this article was written, but many states were diligently working on the bill, and several states have already enacted their own mandatory breast density legislation (see Figure 8). The Breast Density and Mammography Reporting Act could be a driving force for the advancement of MBI technology. Both mam-mography and ultrasonography have limitations when it comes to dense breast tissue. When patients are more informed of the composition of their breasts, they might choose to request an additional study such as an MBI, which is not limited by dense breast tissue.12
ConclusionMBI has shown promising results for evaluation
of breast disease in several patient populations, but
researchers must continue to investigate the modal-ity’s limitations and potential in larger populations. The technology’s efficacy in imaging dense breasts is particularly important for the early detection of breast cancer and decreased mortality and morbidity from the disease.
Paula R McPeak, MSRS, R.T.(R)(M), is an instructor of radiography and mammography for the Riverside School of Health Careers in Newport News, Virginia.
Reprint requests may be mailed to the American Society of Radiologic Technologists, Communications Department, at 15000 Central Ave SE, Albuquerque, NM 87123-3909, or e-mailed to [email protected].
© 2014 American Society of Radiologic Technologists
References1. SEER stat fact sheets: breast cancer. National Cancer
Institute Web site. http://seer.cancer.gov/statfacts/html /breast.html. Accessed January 13, 2014.
2. DeSantis C, Siegel R, Bandi P, Jemal A. Breast cancer statistics, 2011. CA Cancer J Clin. 2011;61(6):408-418. doi:10.3322/caac.20134.
Enacted law
Endorsed bill
No action
Insurance coverage bill
Working on bill
Figure 8. Legislative efforts by state for mandatory breast density notification. Used with permission from Are You Dense Advocacy Inc, 2013.
Used by permission © Are You Dense Advocacy, Inc., 2013, All Rights Reserved.
CEDirected Reading
536M RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Advancements in Molecular Breast Imaging
3. SEER fast stats. National Cancer Institute Web site. http://seer.cancer.gov/faststats/selections.php?%20-%20Output. Accessed January 13, 2014.
4. Ottini L, Palli D, Rizzo S, Federico M, Bazan V, Russo A. Male breast cancer. Crit Rev Oncol Hematol. 2010;73(2): 141-155. doi:10.1016/j.critrevonc.2009.04.003.
5. Jones EA, Phan TD, Blanchard DA, Miley A. Breast specific γ-imaging: molecular imaging of the breast using 99m Tc-sestamibi and a small-field-of-view γ-camera. J Nucl Med Technol. 2009;37(4):201-205. doi:10.2967/jnmt.109.063537.
6. Scintimammography. RadiologyInfo.org Web site. http://www.radiologyinfo.org/en/info.cfm?pg=scintimammo. Reviewed March 7, 2012. Accessed April 18, 2013.
7. Brem RF, Floerke AC, Rapelyea JA, Teal C, Kelly T, Mathur V. Breast-specific gamma imaging as an adjunct imaging modality for the diagnosis of breast cancer. Radiology. 2008;247(3):651-657. doi:10.1148/radiol.2473061678.
8. Zhou M, Johnson N, Gruner S, et al. Clinical utility of breast-specific gamma imaging for evaluating disease extent in the newly diagnosed breast cancer patient. Am J Surg. 2009:197(2):159-163. doi:10.1016/j.amjsurg .2008.10.002.
9. Hendrick RE. Radiation doses and cancer risks from breast imaging studies. Radiology. 2010;257(1):246-253. doi:10.1148/radiol.10100570.
10. Bevelacqua JJ. Practical and effective ALARA. Health Phys. 2010;98(suppl 2):S39-S47.
11. Conners A, Maxwell R, Tortorelli C, et al. Gamma camera breast imaging lexicon. AJR Am J Roentgenol. 2012;199(6):W767-W774. doi:10.2214/AJR.11.8298.
12. Weigert JM, Bertrand ML, Lanzkowsky L, Stern LH, Kieper DA. Results of a multicenter patient registry to determine the clinical impact of breast-specific gamma imaging, a molecular breast imaging technique. AJR Am J Roentgenol. 2012;198(1):W69-W75. doi:10.2214/AJR.10.6105.
13. Breast anatomy. Nationalbreastcancer.org Web site. http://www.nationalbreastcancer.org/breast-anatomy. Accessed April 10, 2013.
14. Görkem SB, O’Connell AM. Abnormal axillary lymph nodes on negative mammograms: causes other than breast cancer. Diagn Interv Radiol. 2012; 18(5): 473-479. doi:10.4261/1305 -3825.DIR.5491-11.2.
15. Boyd NF, Martin LJ, Bronskill M, Yaffe MJ, Duric N, Minkin S. Breast tissue composition and susceptibility to breast can-cer. J Natl Cancer Inst. 2010;102(16):1224-1237. doi:10.1093 /jnci/djq239.
16. Mavi A, Cermik TF, Urhan M, et al. The effect of age, meno-pausal state, and breast density on 18F-FDG uptake in normal
glandular breast tissue. J Nucl Med. 2010;51(3):347-352. doi:10.2967/jnumed.109.068718.
17. Killelea BK, Gillego A, Kirstein LJ, et al. George Peters award: how does breast-specific gamma imaging affect the management of patients with newly diagnosed breast cancer? Am J Surg. 2009;198(4):470-474. doi:10.1016/j.amj surg.2009.06.016.
18. Mammogram reports—BI-RADS. American Cancer Society Web site. http://www.cancer.org/treatment/understanding yourdiagnosis/examsandtestdescriptions/mammogramsan dotherbreastimagingprocedures/mammograms-and -other-breast-imaging-procedures-mammo-report. Revised February 7, 2013. Accessed January 13, 2014.
19. Types of breast cancers. American Cancer Society Web site. http://www.cancer.org/cancer/breastcancer/detailedguide /breast-cancer-breast-cancer-types. Reviewed September 11, 2013. Accessed January 13, 2014.
20. Breast cancer risk factors you cannot change. American Cancer Society Web site. http://www.cancer.org/cancer/br eastcancer/moreinformation/breastcancerearlydetection/br east-cancer-early-detection-risk-factors-you-cannot-change. Reviewed September 14, 2013. Accessed January 7, 2014.
21. Kwon JS, Gutierrez-Barrera AM, Young D, et al. Expanding the criteria for BRCA mutation testing in breast cancer survi-vors. J Clin Oncol. 2010;28(27):4214-4220. doi:10.1200/JCO .2010.28.0719.
22. Watson L. Appropriate use of breast imaging modalities. Radiol Technol. 2012;84(4):371M-390M.
23. Smith RA, Cokkinides V, Brawley OW. Cancer screening in the United States, 2009: a review of current American Cancer Society guidelines and issues in cancer screening. CA: Cancer J Clin. 2009;59(1):27-41. doi:10.3322/caac.20008.
24. Breast cancer: early detection. American Cancer Society recommendations for early breast cancer detection in women without breast symptoms. American Cancer Society Web site. http://www.cancer.org/cancer/breastcancer/moreinfo rmation/breastcancerearlydetection/breast-cancer-early-de tection-acs-recs. Revised January 28, 2014. Accessed January 30, 2014.
25. Zhou M, Johnson N, Blanchard D, Bryn S, Nelson J. Real-world application of breast-specific gamma imaging, initial experience at a community breast center and its potential impact on clinical care. Am J Surg. 2008;195(5):631-635. doi:10.1016/j.amjsurg.2008.01.006.
26. Frank ED, Long BW, Smith BJ. Merrill’s Atlas of Radiographic Positioning and Procedures. Vol 3. 12th ed. St Louis, MO: Mosby; 2011:386.
27. Hruska CB, Phillips SW, Whaley DH, Rhodes DJ, O’Connor MK. Molecular breast imaging: use of a dual-head dedi-cated gamma camera to detect small breast tumors. AJR

CEDirected Reading
537MRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
McPeak
Am J Roentgenol. 2008;191(6):1805-1815. doi:10.2214/AJR .07.3693.
28. Teertstra HJ, Loo CE, van den Bosch MA, et al. Breast tomosynthesis in clinical practice: initial results. Eur Radiol. 2010;20(1):16-24. doi:10.1007/s00330-009-1523-2.
29. Breast tomosynthesis (3D mammography). Massachusetts General Hospital Web site. http://www.massgeneral.org /imaging/services/3D_mammography_tomosynthesis.aspx. Accessed January 7, 2014.
30. Reynolds A. Breast density and digital breast tomosynthesis. Radiol Technol. 2013;85(1):63M-82M.
31. Ultrasound—breast. RadiologyInfo.org Web site. http://www.radiologyinfo.org/en/info.cfm?pg=breastus. Accessed April 18, 2013.
32. Athanasiou A, Tardivon A, Ollivier L, Thibault F, El Khoury C, Neuenschwander S. How to optimize breast ultrasound. Eur J Radio . 2009;69(1):6-13. doi:10.1016/j.e jrad.2008.07.034.
33. Sehgal CM, Weinstein SP, Arger PH, Conant EF. A review of breast ultrasound. J Mammary Gland Biol Neoplasia. 2006;11(2):113-123.
34. Kelly KM, Dean J, Comulada WS, Lee SJ. Breast cancer detection using automated whole breast ultrasound and mammography in radiographically dense breasts. Eur Radiol. 2010;20(3):734-742. doi:10.1007/s00330-009-1588-y.
35. Brem RF, Petrovich I, Rapelyea JA, Young H, Teal C, Kelly T. Breast-specific gamma imaging with 99m Tc-sestamibi and magnetic resonance imaging in the diagnosis of breast cancer: a comparative study. Breast J. 2007;13(5):465-469.
36. Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57(2):75-89.
37. Magnetic resonance imaging (MRI)—breast. RadiologyInfo .org Web site. www.radiologyinfo.org/en/info.cfm?pg =breastmr. Accessed April 18, 2013.
38. Triple negative breast cancer. Susan G Komen Web site. http://ww5.komen.org/uploadedFiles/Content_Binaries /KOMEED079100.pdf. Accessed February 3, 2014.
39. Mankoff DA. Molecular imaging as a tool for translating breast cancer science. Breast Cancer Res. 2008;10(suppl 1):S3. doi:10.1186/bcr2126.
40. Brem RF, Shahan C, Rapelyea JA, et al. Detection of occult foci of breast cancer using breast-specific gamma imaging in women with one mammographic or clinically suspicious breast lesion. Acad Radiol. 2010;17(6):735-743. doi:10.1016/j .acra.2010.01.017.
41. Fowler AM. A molecular approach to breast imaging. J Nucl Med. 2014;55(2):177-180. doi:10.2967/jnumed.113.126102.
42. Berg WA, Madsen KS, Shilling K, et al. Breast cancer: com-parative effectiveness of positron emission mammography
and MR imaging in presurgical planning for the ipsilateral breast. Radiology. 2011;258(1):59-72. doi:10.1148/radiol .10100454.
43. Kaplan DA. Beyond the mammogram: molecular breast imaging emerges. Diagnostic Imaging Web site. http://www .diagnosticimaging.com/display/article/113619/1830269. Published March 24, 2001. Accessed June 18, 2013.
44. Molecular breast imaging. Dilon Diagnostics Web site. http://www.dilon.com/diagnostic-products/molecular -breast-imaging. Accessed March 1, 2013.
45. O’Connor M, Rhodes D, Hruska C. Molecular breast imag-ing. Expert Rev Anticancer Ther. 2009;9(8):1073-1080. doi:10.1586/era.09.75.
46. Tadwalkar RV, Rapelyea JA, Torrente J, et al. Breast-specific gamma imaging as an adjunct modality for the diagnosis of invasive breast cancer with correlation to tumour size and grade. Br J Radiol. 2012;85(1014):e212-e216. doi:10.1259 /bjr/34392802.
47. Goldsmith SJ, Parson W, Guiberteau MJ, Stern LH et al. SNM practice guideline for scintigraphy with breast-specific γ-cameras 1.0. J Nucl Med Technol. 2010;38(4)219-224. doi:10.2967/jnmt.110.082271.
48. American College of Radiology. ACR appropriateness criteria. Breast cancer screening. http://www.acr.org /~/media/ACR/Documents/AppCriteria/Diagnostic /BreastCancerScreening.pdf. Published 2012. Accessed January 29, 2014.
49. Wagenaar DJ, Boughey JC, Hruska CB, et al. Molecular breast imaging for neoadjuvant chemotherapy assessment. Poster presented at: The World Molecular Imaging Congress; September 10, 2010; Kyoto, Japan. http://www.wmis .org/abstracts/2010/forSystemUse/papers/P1008B.html. Accessed January 7, 2014.
50. Pinsky RW, Rebner M, Pierce LJ, et al. Recurrent cancer after breast-conserving surgery with radiation therapy for ductal carcinoma in situ: mammographic features, method of detection, and stage of recurrence. AJR Am J Roentgenol. 2007;189(1):140-144. doi:10.2214/AJR.06.1281.
51. Richards T, Hunt A, Courtney S, Umeh H. Nipple discharge: a sign of breast cancer? Ann R Coll Surg Engl. 2007;89(2):124-126. doi:10.1308/003588407X155491.
52. Kruger G, Singh G. Breast ductography. Radiopaedia.org. http://radiopaedia.org/articles/breast-ductography-1. Accessed January 9, 2014.
53. Smathers RL, Boone JM, Lee LJ, Berns EA, Miller RA, Wright AM. Radiation dose reduction for augmentation mammography. AJR Am J Roentgenol. 2007;188(5):1414-1421. doi:10.2214/AJR.06.0998.
54. Deapen D. Breast implants and breast cancer: a review of inci-dence, detection, mortality, and survival. Plast Reconstr Surg.
CEDirected Reading
538M RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Advancements in Molecular Breast Imaging
2007;120(7 suppl 1):70S-80S. doi:http://dx.doi.org/10.1136 /bmj.f2399.
55. Shiffman MA. Mammograms in cosmetic breast surgery. In: Mastopexy and Breast Reduction: Principles and Practice. Berlin, Germany: Springer-Verlag; 2009:37-40.
56. Takayanagi, S. Augmentation mammaplasty using implants: a review. Arch Plast Surg. 2012;39(5): 448-451. doi:10.5999/aps.2012.39.5.448.
57. Zikria JF, Machnicki S, Rhim E, Bhatti T, Graham RE. MRI of patients with cardiac pacemakers: a review of the medical literature. AJR Am J Roentgenol. 2011;196(2):390-401. doi:10.2214/AJR.10.4239.
58. Sutton R, Kanal E, Wilkoff BL, et al. Safety of magnetic reso-nance imaging of patients with a new Medtronic EnRhythm MRI SureScan pacing system: clinical study design. Trials. 2008;9(1):68. doi:10.1186/1745-6215-9-68.
59. Issa N, Poggio ED, Fatica RA, Patel R, Ruggieri PM, Heyka RJ. Nephrogenic systemic fibrosis and its association with gadolinium exposure during MRI. Cleve Clin J Med. 2008;75(2):95-111.
60. Robinson ML, Strunk R. Weight and aperture considerations for different imaging modalities. American Roentgen Ray Society Web site. https://www.arrs.org/education/cert/demo2 /requiredReading.cfm?product_code=C0801_00XX&edu _module=1. Accessed February 10, 2014.
61. Miller JC. Factors that limit imaging. Radiology Rounds [newsletter]. 2005;3(7). http://www.mghradrounds.org/index .php?src=gendocs&link=2005_july. Accessed January 9, 2014.
62. Mitchell D, Hruska CB, Boughey JC, et al. 99m Tc-sestamibi using a direct conversion molecular breast imaging system to assess tumor response to neoadjuvant chemotherapy in women with locally advanced breast cancer. Clin Nucl Med. 2013; 38(12):949-956. doi:10.1097/RLU .0000000000000248.
63. Indications and usage for Technetium TC 99M sestamibi. Drugs.com Web site. http://www.drugs.com/pro/techne tium-tc-99m-sestamibi.html. Revised September 2013. Accessed January 10, 2014.
64. Silindir M, Ozer AY. Adverse reactions to radiopharmaceu-ticals (ARRP): particularly to technetium radiopharmaceu-ticals. FABAD Journal Pharmaceutical Sciences. 2008;33:109-117.
65. Callahan RJ, Chilton HM, Ponto JA, Swanson DP, Royal HD, Bruce AD. Procedure guidelines for the use of radiopharma-ceuticals 4.0*. J Nucl Med Technol. 2007;35(4):272-275.
66. James DJ, Cardew P, Warren-Forward HM. Determining the pregnancy status of patients before diagnostic nuclear medicine procedures: the Australian experience. J Nucl Med Technol. 2011;39(3):220-225. doi:10.2967/jnmt.111.088740.
67. Lee A, Chang J, Lim W, et al. Effectiveness of breast‐specific gamma imaging (BSGI) for breast cancer in Korea: A com-parative study. Breast J. 2012;18(5):453-458. doi:10.1111/j .1524-4741.2012.01280.x.
68. Jones E. A protocol for imaging axillary lymph nodes in patients undergoing breast-specific gamma-imaging. J Nucl Med Technol. 2010;38(1):16-19. doi:10.2967/jnmt .109.062711.
69. Hruska CB, O’Connor MK. Nuclear imaging of the breast: translating achievements in instrumentation into clinical use. Med Phys. 2013;40(5):050901. doi:10.1118/1.4802733. Accessed January 10, 2014.
70. Welch B, Lorino C, Chiarella MD, Hodge T. Clinical use of a stereotactic breast-specific gamma imaging system in the localization of breast lesion for biopsy [poster]. Dilon Technologies Inc. Accessed December 2012.
71. Spanu A, Sanna D, Chessa F, Cottu P, Manca A, Madeddu G. Breast scintigraphy with breast-specific γ-camera in the detection of ductal carcinoma in situ: a correlation with mammography and histologic subtype. J Nucl Med. 2012;53(10):1528-1533. doi:10.2967/jnumed.112.103010.
72. H.R. 3404: Breast Density and Mammography Reporting Act of 2013. GovTrack Web site. https://www.govtrack.us /congress/bills/113/hr3404. Updated October 30, 2013. Accessed January 7, 2014.
539MRADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Directed Reading Quiz
continued on next page
Advancements in Molecular Breast Imaging
1. Molecular breast imaging (MBI):1. is cost-effective.2. is a first-line screening modality.3. improves lesion detection in dense breasts.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
2. When the recommended amount of technetium Tc 99m sestamibi is administered for an MBI examination, a patient receives the approximate equivalent of a whole-body dose of ______ mSv.a. 3b. 5c. 6d. 7
3. Breast cancers usually start to form in the breast’s:1. lobes.2. lobules.3. ducts.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
4. Dense breast tissue is an important risk factor forbreast cancer; increased fibroglandular density is associated with an increased cancer risk. a. trueb. false
5. A BRCA2 mutation increases breast cancer risk byapproximately ______ %.a. 30b. 35c. 40d. 45
Read the preceding Directed Reading and choose the answer that is most correct based on the article.
Renewed through July 1, 2019*
To earn continuing education credit: Take this Directed Reading quiz online at asrt.org/drquiz. Or, transfer your responses to the answer sheet on Page 544M and mail to:
Processing Center, 2908 Stewart Creek Blvd., Charlotte, NC 28216.
New and rejoining members are ineligible to take DRs from journal issues published prior to their most recent join date unless they have purchased access to the quiz from the ASRT. To purchase access to other quizzes, go to asrt.org/store.
* Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date. Some quizzes are renewed and the expiration date extended. Check online at asrt.org/drquiz or call Member Services at 800-444-2778.
14803-03 1.0 Category A+ creditsOriginal Expiration Date: Jun. 30, 2016*Approved by MDCB. Check MDCB.org for details.

RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Directed Reading Quiz
continued on next page
540M
6. A diagnostic mammogram might include coned compression views along with which additional projections?
1. exaggerated craniocaudal 2. cleavage 3. 30° oblique
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
7. Limitations to ultrasonography as a breast imaging
tool include:1. inability to differentiate between solid and
cystic lesions.2. poor detection of microcalcifications.3. difficulty ensuring that the entire breast
has been scanned.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
8. Some critics have questioned breast magnetic resonance (MR) imaging’s efficacy because of its: a. high false-positive results.b. low specificity.c. low sensitivity.d. poor resolution.
9. Breast-specific gamma imaging differs from general MBI in:a. positioning.b. detector type.c. camera type.d. radiopharmaceutical administered.
10. In MBI, image acquisition can begin approximately ______ minutes after injection of the radiopharmaceutical. a. 5 to 10 b. 15 to 20 c. 30 to 45 d. 60 to 90
11. With the development of small field of view cameras, MBI has improved:
1. localization of tumors.2. signal-to-noise ratio.3. detection of small occult breast cancers.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
12. The MBI detector’s range of motion allows the technologist to image the breast with angles similar to mammography so that image comparison is more accurate for diagnosis and localization.a. trueb. false
13. Currently, MBI is appropriate for all of the following except:a. assessing whether breast disease is multifocal or
multicentric.b. evaluating tumor response to chemotherapy.c. screening for breast cancer in women who have a
high risk of developing cancer. d. detecting suspected recurrence.
RADIOLOGIC TECHNOLOGY, May/June 2014, Volume 85, Number 5
Directed Reading Quiz
541M
14. According to the article, a molecular breast imaging study may be indicated in patients with nipple discharge: a. only if a mammography finding is abnormal. b. after ductography is unsuccessful.c. when a fine-needle biopsy is unsuccessful.d. if breast MR is contraindicated.
15. Approximately ______ of premenopausal women in their 40s have extremely dense breast tissue.a. one-quarterb. one-thirdc. one-halfd. two-thirds
16. Indications for choosing molecular breast imaging instead of MR imaging of the breast include:
1. the presence of an implanted medical device in the patient.
2. compromised renal function in the patient.3. a patient with small body habitus.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
17. For best results, women undergoing an MBI examination should schedule the examination between the ______ day preceding the onset of menstruation. a. 1st and 5th b. 2nd and 14th c. 3rd and 10th d. 4th and 8th
18. During an MBI examination, the radiopharmaceutical is administered in the ______ side being examined. a. leg of the ipsilateral b. leg of the contralateral c. arm of the ipsilateral d. arm of the contralateral
19. According to Jones et al, which of the following techniques can reduce the possibility of extravasation and vascular trapping in a molecular breast imaging procedure?a. straight-stick injectionb. test, push, flush c. Seldinger techniqued. continuous fluid drip
20. Mammography has a higher false-positive rate in women with dense breasts, yielding a sensitivity rate as low as ______%.a. 10b. 30c. 66d. 85

Grass-roots Advocacy Action Center Read the latest news on the CARE bill
and MARCA. Find contact information for your elected
federal, state and local officials. Contact your legislators and take action.
Check it out at www.asrt.org/takeaction
State Legislative and Regulatory Tracking Tool Access regulatory and legislative reports
by state or other searchable criteria. Search pending and enacted legislation. Keep current on changes affecting your
practice and profession.
Learn more at www.asrt.org/statetracking
New Advocacy Tools
Get Involved and Support Your Profession
New!
New!
©2013 ASRT. All rights reserved.
GR13_Adv_FillerAds.indd 2 12/12/13 4:11 PM