advanced practice: our experience in palliative rt at romc & the results of a bi-national survey...
TRANSCRIPT

Advanced Practice: Our Experience in
Palliative RT at ROMC & the results of a
bi-national Survey1R Owen, 1M Job, 2C Wright, 3S Whiting,
4THolt1Radiation Therapy Services, ROMC; 2Monash University; 3
Division of Nursing, ROMC; 4Division of Radiation Oncology, ROMC

What have F&C and G&T got in common?

Synopsis
• Background– AP in Aus Context – Identifying a need– Developing AP at
ROMC
• Survey– Why we did the
survey– Results– How it can help
• Future

Background – AP
• Rationale for AP in RT – Increase no. RTs - better career paths,
recognition of roles (Baume, 2002)
– Reform through AP (RORIC 2011)
– Role redesign & EB scope of practice (National Health Workforce Innovation and Reform and Strategic Framework for Action 2011 – 2015)
– Expert inter-professional team -13 recommendations for AP for MRPs
– (Dr Ian Freckleton Report 2012)
– EB National Curriculum Framework for RTs seeking training & recognition as APs (Monash Uni 2014)

Clinical Supervision Framework for AP RT
(07/14) • Collaboration -5 Aus Uni’s• To become an AP
– MPhil/Masters by Research– Concurrent clinical mentoring– A defined pathway for formal
recognition of AP “status” (Monash Uni: Clinical Supevision Framework for Advanced Radiaiton Therapy
Practice 2014)

Our dilemma… No consensus on what an Advanced Practitioner was or how to achieve such a status…

Palliative RT
• Identifying a need:– RT has a significant role in palliation– 14% of all newly diagnosed cancers (Jacob et
al, 2010 Clin Oncol)
– 50 % of all RT treatments are palliative in nature (Nieder et al, 2010 IJROBP)
– Evidence for effectiveness of a single # compared with multiple # (Chow et al, 2007 J Clin Oncol)
– Delay in symptom relief decrease QOL & cause distress

C.2006 - RRPRC
• Creation of a RRPRC by RO• Modelled on successful RRPRC in
UK & Canada– Timely and efficient palliative RT – Reduce patient suffering by wait times,
no visits– Same day consult & treatment– Link to community palliative support– Academic
(Holt & Yau 2010, JMIRO)

Palliative Care
• Palliative Care:– Approach that improves QOL for
patients & families facing terminal illness
– Prevent & relieve suffering– Early identification & assessment– Treatment of pain, & other problems
physical, psychological & spiritual (WHO 2012: Global Atlas of Palliative Care)

Ideal Conditions & a Plan!
• Willing RO + RRPRC (c.2006) + keen RTs– Pts with complex needs– Comprise a hefty workload, 30-40%
• Began developing an AP role - 2012 • Defined scope of practice• Clinical Mentorship from RO• Collaborated with Monash; post – graduate
study
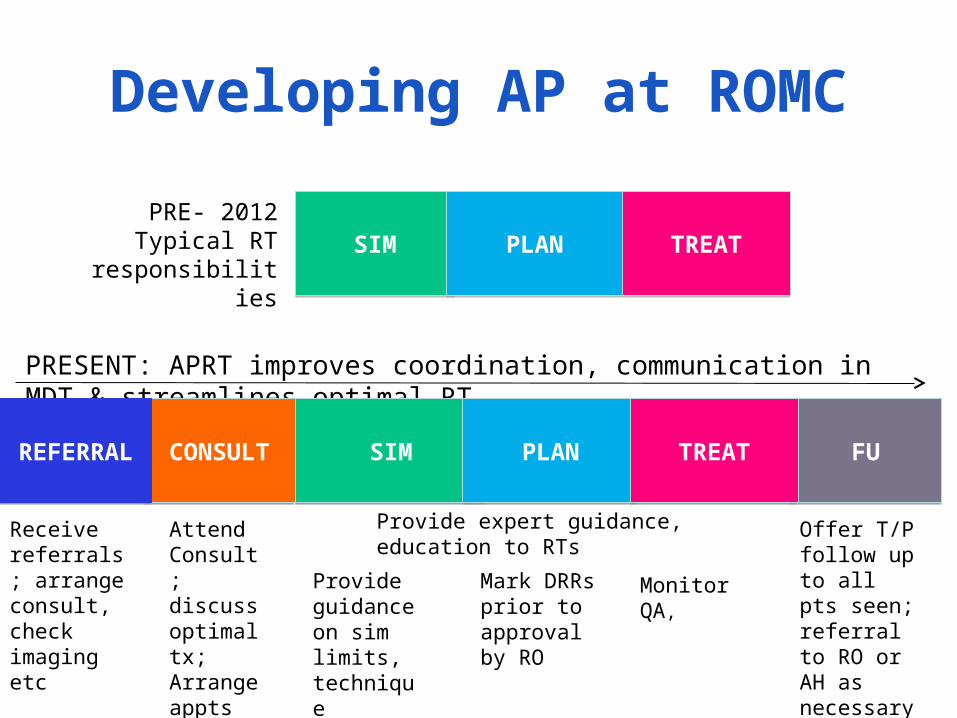
Developing AP at ROMC
SIMSIM PLANPLAN TREATTREATPRE- 2012Typical RT
responsibilities
PRESENT: APRT improves coordination, communication in MDT & streamlines optimal RT
CONSULTCONSULT
Attend Consult; discuss optimal tx;Arrange appts
REFERRAL
REFERRAL
Receive referrals; arrange consult, check imaging etc
FUFU
Offer T/P follow up to all pts seen; referral to RO or AH as necessary; point of contact
SIMSIM PLANPLAN TREATTREAT
Provide expert guidance, education to RTs
Provide guidance on sim limits, technique
Mark DRRs prior to approval by RO
Monitor QA,

Survey
• To determine if there were other RRPRC operating in Aus and NZ and the extent to which RTs might be specialising in palliative RT.– Use this information to assist in
developing our AP role– Validate the need for formal education

Purpose of Survey
• Are there other Rapid Response Clinics?• Are RTs already working in these clinics?• What types of tasks are RTs performing?• Is there a further need for APRTs in Pall RT and
what tasks do you think they would perform?• What level of education and experience do you
think is required to become an AP?• Whether or not RO’s would be willing to provide
clinical mentorship?

Methodology
• Exploratory Study• On-line questionnaire • Following HREC approval
distributed to all RTs and ROs across Australia and NZ– AIR members, Heads of Department,
RANZCR Newsletter• 25 questions

Results
• Distributed electronically between Nov 13 - Feb 14
• Total of 260 responses (~10%RR)• 256 useable• 83.3% Surveys complete
• Out of 221 RTs - 87% Aus, 13% NZ

Demographics - Role

Geography - RTs

Metro or Regional?

Departmental setting

Years of Experience

Entry Level Qualifications

Post Graduate Study
• 51(23%) - 34 studied< 5 yrs ago• 77% no post-graduate study• Types of courses varied
– Monash AP short courses– UK City University – AP modules– AP – Bracytherapy– Masters, MPhil, Grad Cert Pub Health, Dip
Management, post-grad MRI, MPub Health, M Management, M Training and Development

Type of Course

No. identifying as APRTs
• 14 (~ 7% of RT respondents)– 2 Palliative care– 2 Breast localisation and simulation– 2 Pelvic imaging– Radiation Engineering– Remainder non-specific
• Other (23 additional comments)– Palliative Care Specialist– UK trained Palliative Care RT

Rapid Response Clinics
• 2 RTs who identified themselves as APs Palliative care– 1 Rapid Response Clinic– Other trained in the UK
• 4 Rapid Response Clinics – QLD, VIC, Waikato Province, ACT• RR Team were identified to be:
– RO, RT, Nurse, Social Worker, Palliative Care Specialist, OT

What specific tasks?
• Common responses (27 free text):– Liaise with: patient, RO, other hospitals for transfer of
inpatients, admin to streamline patient bookings, patients family, RT staff
– Assess imaging and pathology– Attend consultation– With guidance from RO supervises simulation, planning– Voluming and marking of ref images– Patient review and assessment in palliative clinic, pre-
treatment and assists nursing with follow up– Consults with RO and nursing for allied health referrals

How experienced does an RT need to be…?
ROs RTs

What training is required?
RO’s: Clinical Mentorship RO 30% (8); Masters & Clinical Mentorship 26% (7)

What training is required?
“More than basic training with clinical mentorship too, Degree is irrelevant, this requires an apprenticeship (clinical mentorship)”
“It is not so much the qualification but the quality of the candidate and what they are expecting to be able to do additionally as an advanced practitioner”

Do we need AP in Palliative RT?
• Overall– 48 % yes, 52 % No; 78 full text (133/256
responses)
• Radiation Oncologists – 30% Yes; 70% No (20/33 responses)
“…palliation such a large component of our practice we respond very quickly already… if linked to particular staff may make more difficult to manage…”
“all RTs spend time doing and become experienced in palliative RT - its 50+% of their workload”

Flip side
“Palliative patients often have complex needs, both physical and psychological. Many of our patients travel significant distances for treatment. An APRT would be a great asset in supporting these patients”

Do we need AP – Palliative RT?
• Chief RTs:• Equally divided (54% Yes; 46 % No)
“Will better recognize the vital role a
compassionate RT to contribute in rapid treatment planning and delivery; separate from the current management protocol.”

Do we need AP – Palliative RT?
• RTs (102 responses: 52% Yes, 48% No)
• 61 free text; few different themes– Workload– Is it really an “advanced role”– Education– Regional or metro

Workload
“In centres that treat high numbers of palliative patients, I think having an advanced practice RT in this area would assist in the effectiveness and efficiency of service delivery. Additionally, it would relieve some of the burden on the ROs”
“Not enough palliative workload to support this role”
“Large percentage of workload. Often overlooked or seen as not as important due to lack of complexity in planning/ treatment. However it is very important to always deliver high quality care. Also could improve efficiency due to urgency of these cases”

Is it an advanced Role?“Palliative treatments are generally simple and straight
forward. I don't think advanced practice will enable someone to better plan and deliver these treatments as the approach is simple.”
“I think there IS a need because the patient's requirements in
the palliative situation is as specialised as other segments of radiotherapy. (brachy, TBI, paediatric etc)”
“I wouldn't know what an advanced practitioner for palliative therapy would do. Maybe replace a registrar in emergency situations? If this is so our current system works quite well. I believe this should be something all RT staff have the ability to do.”

Education
“I believe advanced practitioner roles require a certain high standard of education. I am unaware/unsure if there is appropriate training available. Having seen advanced practitioner roles in place in the UK, I don't feel comfortable with the knowledge of the position holders with respect to their responsibilities. I think this subject on AP's needs to be approached with caution”

Setting
“As a regional centre it would be nice to improve our times for sim to treatment…”
“We currently only have one RO in our centre… not always available”

What is, isn’t and would be useful for a trained AP to do?
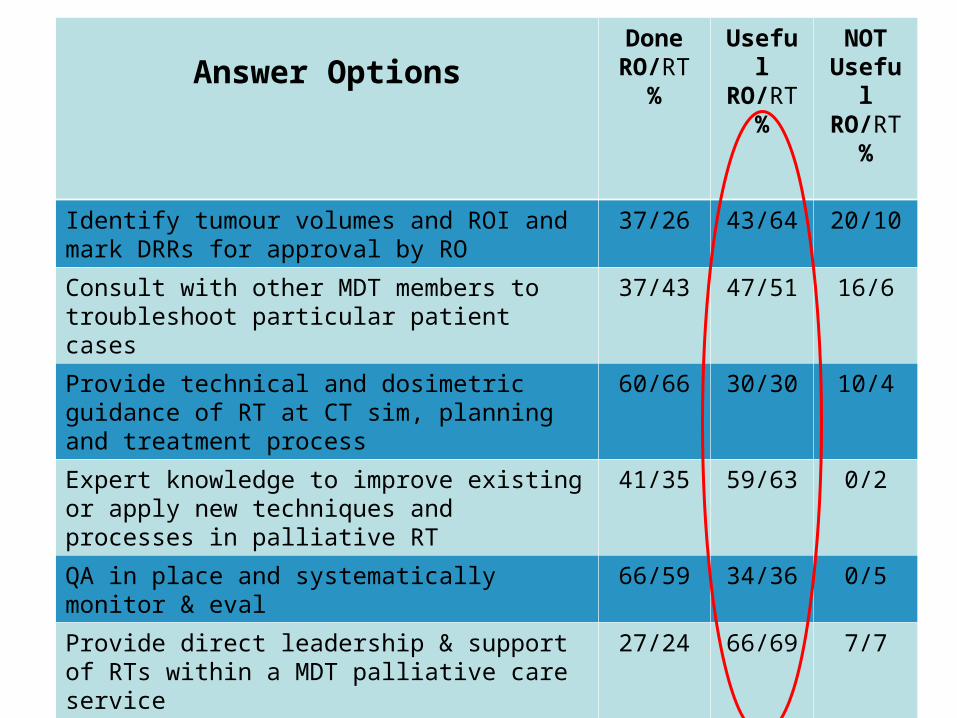
Answer OptionsDone RO/RT
%
Useful
RO/RT%
NOT Usefu
l RO/RT
%
Identify tumour volumes and ROI and mark DRRs for approval by RO
37/26 43/64 20/10
Consult with other MDT members to troubleshoot particular patient cases
37/43 47/51 16/6
Provide technical and dosimetric guidance of RT at CT sim, planning and treatment process
60/66 30/30 10/4
Expert knowledge to improve existing or apply new techniques and processes in palliative RT
41/35 59/63 0/2
QA in place and systematically monitor & eval
66/59 34/36 0/5
Provide direct leadership & support of RTs within a MDT palliative care service
27/24 66/69 7/7
External participation and leadership in professional orgs, commune support & academia
36/11 50/73 14/16
Educate RTs & others about palliative RT 32/14 62/83 4/3
Actively engaged in research & report results
24/13 72/81 6/6
Engage in CPD 55/63 41/37 4/0

RO Mentorship
• Would the RO be willing to provide mentorship for an RT who is training to become and AP
• Yes (67 %)• No (15 %)• Maybe (18 %)

Free Text Comments
• 15• Similar themes emerging
– Registrars & Nursing overlap & RO Domain!
– RO buy in– Already do this stuff (not AP)– Patient focused & appealing– Makes clinic run smoother – continue to
evolve as RT takes on more

Free Text Comments
“I see a challenge with Advanced Practice in palliative care in our centre because these are roles that are often the scope of Oncology Registrars who use this group of patients for learning with the Oncologist”
“Having RT to follow patient from referral to treatment, with expertise in palliative RT has been a great asset for our department, from staff and patient point of view. Being able to quantify or measure this benefit would be the hard part”
“We have nurse practitioners for patient education. We involve pall care specialists. Most of our RT's can already plan and Rx a simple field”

Discussion
• Disappointing response rate…• Few RRPRC in Aus and NZ• Few Specialist Palliative RTs• Respondents (collectively) equally
divided re need• ROs – majority non believers!• Conflicting notions on what AP means
– Education– Many RTs identifying as APs already

Vision – what we need!
• Our experience to date has been positive– Patients– Challenges with staff acceptance
• Need National Consensus on AP• Need a clear pathway to reach and
become “registered” as an AP• Need evidence to convince
– Demonstrate the benefits of AP– Currently evaluating the AP role at ROMC

Acknowledgements
Funding• Medical Radiation
Technologists Board of Queensland
• Allied Health Professional Office of Queensland
Collaboration• Monash University• AIR
InvestigatorsMary JobDr Tanya HoltCaroline WrightSally Whiting

Thank You!