advanced management of patients with tuberculosis · advanced management of patients with...
TRANSCRIPT

8/22/2014
1
Advanced Management of Patients with Tuberculosis
Little Rock, ArkansasAugust 13‐14, 2014
Extrapulmonary TBLinda Dooley, MDAugust 14, 2014
Linda Dooley, MD has the following disclosures to make:
• No conflict of interests
• No relevant financial relationships with any commercial companies pertaining to this educational activity

8/22/2014
2
Generalizations about Extrapulmonary TB
• Treated the same as pulmonary TB: same meds, DOT
• May be harder to diagnose; AFB culture often negative
• Can be (almost) anywhere
• Some patients have unsuspected pulmonary disease and may be infectious
More generalizations
• Treat longer for 3 types: bone and joint, meningitis, miliary
• More common in immune suppressed patients (HIV, TNF blockers)
• More common in Asian patients
8/22/2014
3
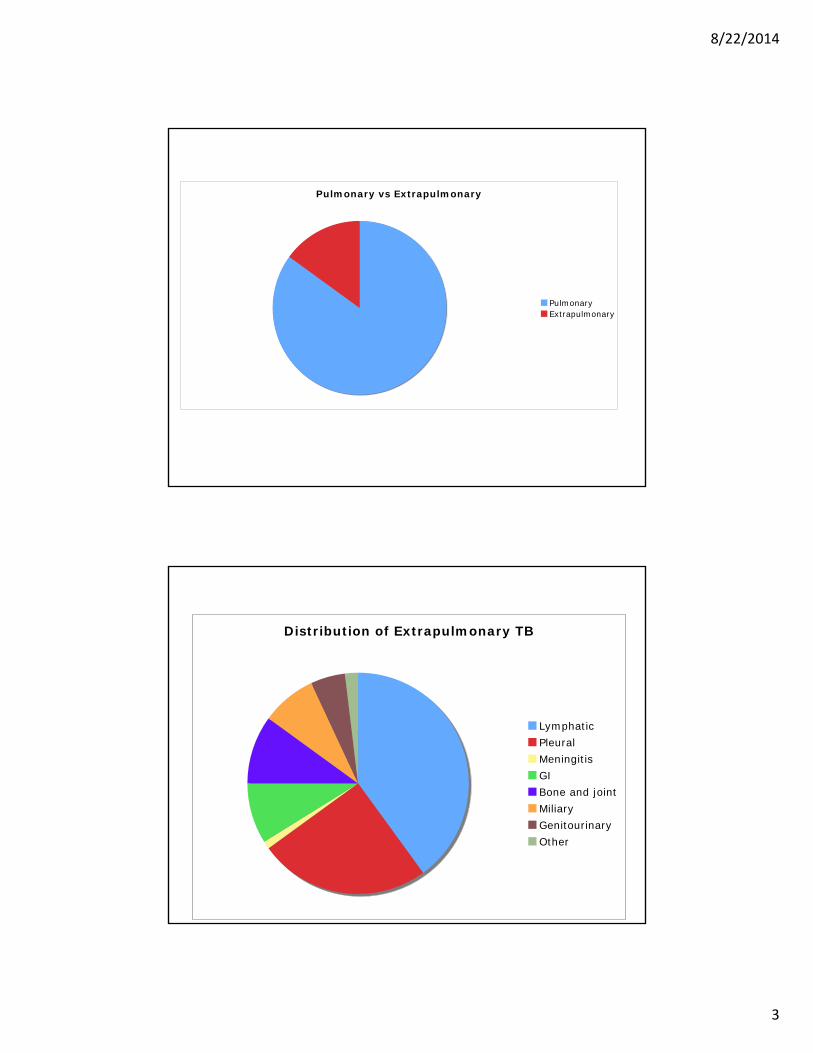
Pulmonary vs Extrapulmonary
PulmonaryExtrapulmonary
Distribution of Extrapulmonary TB
LymphaticPleuralMeningitisGIBone and jointMiliaryGenitourinaryOther

8/22/2014
4
DISTRIBUTION
Patient with extrapulmonary TB may also have pulmonary involvement, even with a normal chest x‐ray
ALWAYS GET SPUTUM FOR AFB EVEN IF THE CHEST X‐RAY IS NORMAL

8/22/2014
5
Pleural Tuberculosis
• 2nd most common form of extra‐pulmonary TB (15‐20%)
• In most of the world, TB is the most common cause of pleural effusions
• Higher incidence in HIV+ patients
• Commonly a manifestation of primary TB
• May progress from an exudative effusion to an empyema or bronchopleural fistula

8/22/2014
6
TB Empyema
Diagnosis
• Thoracentesis with pleural biopsy
• 30% yield for MTB from pleural fluid
• Exudative fluid with lymphocyte predominance, protein more than 4 g/l ; glucose varies
• Pleural biopsy and culture may double yield of + culture

8/22/2014
7
Tuberculous pleural effusions often resolve without treatment but high risk for later pulmonary disease: treat as case anyway
Treatment
•Same as pulmonary TB
•6 months adequate if no drug resistance or immune problems
•Drop PZA at 2 months and leave EMB in regimen if cultures negative

8/22/2014
8
Surgical/ Specialist Involvement
• For initial diagnosis: thoracentesis and pleural biopsy
• More rarely for repeat thoracentesis if pleural fluid re‐accumulates
• For chest tube placement and possible decortication if empyema develops
Lymphatic TB

8/22/2014
9
• Most common form of extra-pulmonary TB (30-40%)• Most common sites are cervical (scrofula) or mediastinal but can affect any node
Diagnosis and Treatment
• Fine needle aspirate or open biopsy
• Culture for AFB
• Don’t forget CXR and sputum
• More common in women, Asian population, immune suppression (HIV, TNF blockers)
• Treat like pulmonary TB
• Immune reconstitution may occur even with HIV negative patients

8/22/2014
10
Surgical/Specialist Involvement
• ENT if cervical; site determines who does biopsy
• Initial diagnosis by fine needle aspirate or biopsy
• Repeat I&D if swelling worsens
• Site of disease determines need for surgical involvement: immune reconstitution can cause obstruction
TB Meningitis
• 300‐400 cases annually in US
• 1% of TB disease
• Even with effective treatment, case fatality high: 15‐40%
• Early diagnosis both difficult and critical
8/22/2014
11
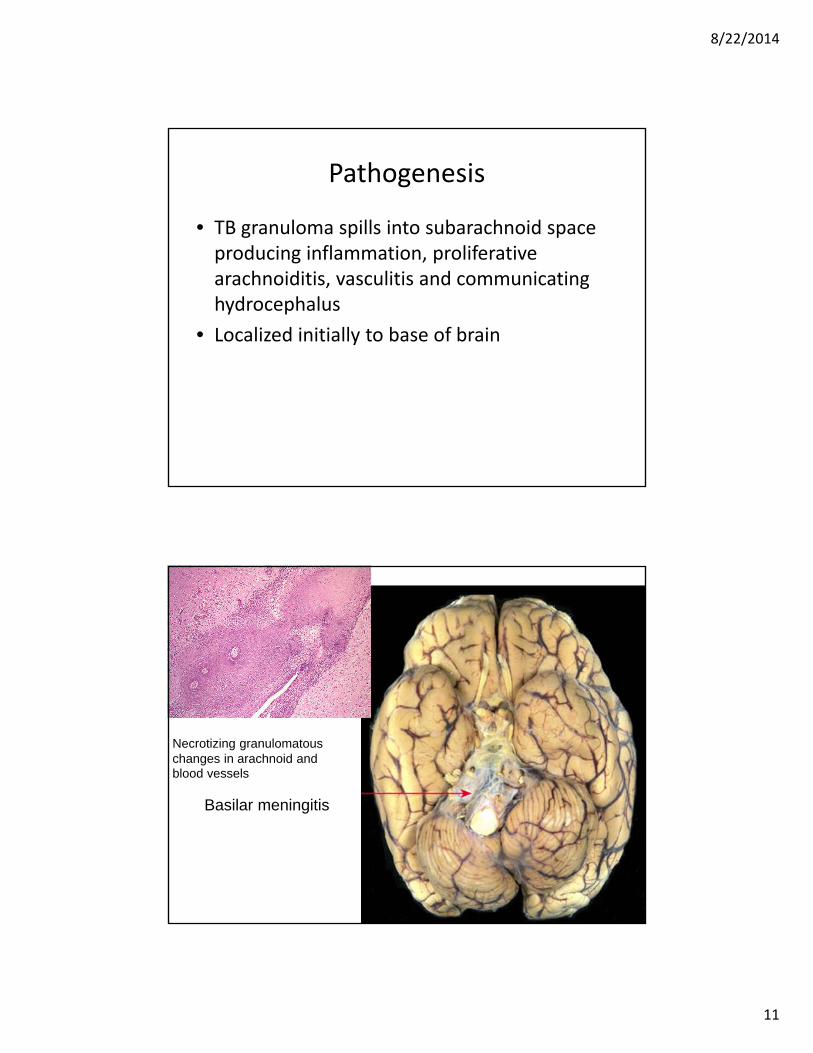
Pathogenesis
• TB granuloma spills into subarachnoid space producing inflammation, proliferative arachnoiditis, vasculitis and communicating hydrocephalus
• Localized initially to base of brain
Necrotizing granulomatous changes in arachnoid and blood vessels
Basilar meningitis

8/22/2014
12
Diagnosis
• Presentation may mimic bacterial meningitis: acute, rapidly progressive
• May be a slowly progressive dementia over months with personality change, social withdrawal or memory deficits
• Lumbar puncture: AFB stain and culture, PCR, NAAT, low CSF glucose, high protein, lymphocyte predominance
• Negative results do NOT exclude the diagnosis
CSF examination• Serial examination of the CSF by AFB stain and culture is the best diagnostic approach
• Use last fluid obtained; higher yield for larger volume CSF (10‐15cc)
• Typically elevated protein, low glucose, and lymphocyte predominance
• Early CSF may be relatively acellular or PMN predominant
• Smears and cultures may yield positive results days to weeks after therapy has been initiated or may be negative

8/22/2014
13
Nov
CT and MRI helpful in diagnosis
Multiple tuberculomas along enhanced dural reflections
Basilar enhancement and hydrocephalus

8/22/2014
14
Treatment
• Treat if meningitis suspected
• Early treatment essential
Treatment
• 12 months for drug sensitive disease
• 18 months if no PZA
• Extend to 18‐24 months for severe illness, slow clinical response, or immune suppression
• No guidelines for length of treatment for MDR or XDR TB: expert consult essential

8/22/2014
15
CSF Penetration of TB Meds
GOOD FAIR POOR
Isoniazid * Rifampin * Streptomycin *
Pyrazimamide Ethambutol Capreomycin *
Ethionamide Quinolones * Amikacin *
Cycloserine Kanamycin *
Linezolid *
* Can Be Given IV
Steroids
• Adjunctive corticosteroids may be beneficial and are recommended for all children and adults being treated for TB meningitis
• Doses– Children: 2‐4 mg/kg prednisone tapered over 4 weeks
– Adults: 60 mg/d prednisone tapered over 6 weeks or .4 mg/kg/day dexamethasone IV tapered to .1 mg/kg/day
– May need longer slower taper

8/22/2014
16
Surgery
• Hydrocephalus may require urgent shunting.
• Serial LP and steroid therapy may suffice for Stage I pts awaiting response to antibiotics.
• Shunting should not be delayed in patients with stupor, coma or progressive neurologic signs.
Nov 2009
Surgical/Specialist Involvement
• ER doc, radiologist or hospital doc for initial LP for diagnosis
• Neurosurgeon for shunt placement if needed later: surgery need can be
urgent

8/22/2014
17
Case: HIV+ man with abnormal MRI
• MRI done after fall • Extensive work-up all negative except +QFT• Empiric Rx for TB meningitis tried without
reporting and drug induced hepatitis• DOT begun: pt. able to tolerate TB Rx without
PZA

8/22/2014
18
Case: 20 yo Pakistani woman with severe headache and
swollen neck nodes
• Fine needle aspirate: granulomatous tissue
• Normal CXR
• Consultant recommended LN biopsy for better chance MTB and sensitivities
• Pt declined: did not have $8000 required down payment
• Abnormal CT head; no LP done
• Observed induced sputum collection done by NCM had positive NAAT
• Drug sensitive MTB from sputum
• One month later also grew TB from neck aspirate
• Headache resolved on TB therapy

8/22/2014
19
Pericardial TB

8/22/2014
20
Pericardial TB
• Uncommon and difficult diagnosis
• Presents with acute or insidious onset; nonspecific symptoms
• Ultrasound helpful; acid fast studies may not be positive
• Surgery for progressive tamponnade or recurrent effusions on TB Rx
• Steroids reduce mortality and need for surgery or repeat pericardiocentesis: start at 60 mg/d 1st month and reduce over 11 weeks
Surgical/Specialist Involvement
• Cardiothoracic surgeon essential for initial diagnosis as well as for management of recurrent effusion or tamponnade
• May require urgent management
• Pericardial stripping may be needed

8/22/2014
21
Bone and Joint TB
Skeletal TB
• Spinal TB (Pott’s disease) most common location: 40%
• Next most common: hip (40%) and knee (10%)
• Can be anywhere
• Frequently delayed diagnosis
• X‐ray not helpful in distinguishing other infectious destructive etiology

8/22/2014
22
Diagnosis
• Joint aspiration: WBC may be granulocytes or lymphocytes
• WBC count varies widely
• Protein 4‐6 g/dl; glucose may be low
• Acid fast culture yield high (up to 80%)
• Presence of positive smear much lower (20%)
Treatment
• Standard TB therapy with extended treatment
• 12 months minimum but extend for slow or uncertain response

8/22/2014
23
Surgical/Specialist Involvement• Orthopedist, primary care, or rheumatologist may do initial arthrocentesis for diagnosis
• Surgery may be needed if bone/joint stabilization required or if prosthesis needs to be removed
• With spinal TB, neurosurgery or spine surgeon involvement essential for spine stabilization (external or surgical)
• Effective treatment may preclude need for surgery
Soft Tissue TB

8/22/2014
24
Soft Tissue TB• Often adjacent to bony and may be direct spread from bony structure or may erode into bone: can be difficult to know if bone involved
• If not sure if bone involved, treat like skeletal TB (longer duration)
• I&D of abscess will only be diagnostic if acid fast cultures done
• Surgical involvement for diagnosis and management of large abscesses
Gastrointestinal and Peritoneal TB
• Peritoneal TB 10% extra‐pulmonary
• GI tract: any site possible but more common terminal ileum and cecum then rest of colon
• Often delayed diagnosis
• TB bacilli may be ingested rather than inspired: consider early if patient drank or ate unpasteurized milk products
• Acid fast cultures frequently negative: pathology caseating necrotizing granulomas

8/22/2014
25
Peritoneal TB
Laparoscopic view of peritoneal granulomas
Peritoneal TB: laparoscopic view of spiderweb adhesions

8/22/2014
26
Treatment
• If cultures negative or pending, assume PZA resistance
Esophageal TB Duodenal TB
Consider the age of your patient and possible childhood exposure to M. bovis
84 yo man with normal CXR

8/22/2014
27
Surgical/Specialist Involvement
• Gastroenterologist or general surgery may make initial diagnosis
• Patient may need paricentesis for initial diagnosis or management of recalcitrant ascites
Urogenital TB

8/22/2014
28
Genitourinary TB
• 10‐15% extrapulmonary TB
• Often insidious onset, subtle nonspecific symptoms, delay in diagnosis
• Hematogenous spread from primary site, often years after infection
• Any part of GU tract may be affected
Ureteral abnormalities (multiple “beading” strictures); may be virtually diagnostic of renal TB

8/22/2014
29
Renal TB
• May have pyuria or hematuria or both
• Acid fast cultures of urine for sterile pyuria
• May need more than 3 specimens of first morning urine collection
• Urine AFB studies not always positive
• NAAT testing may be helpful but negative result does not preclude diagnosis
• Surgery or stenting for obstruction
Prostatic TB
8/22/2014
30
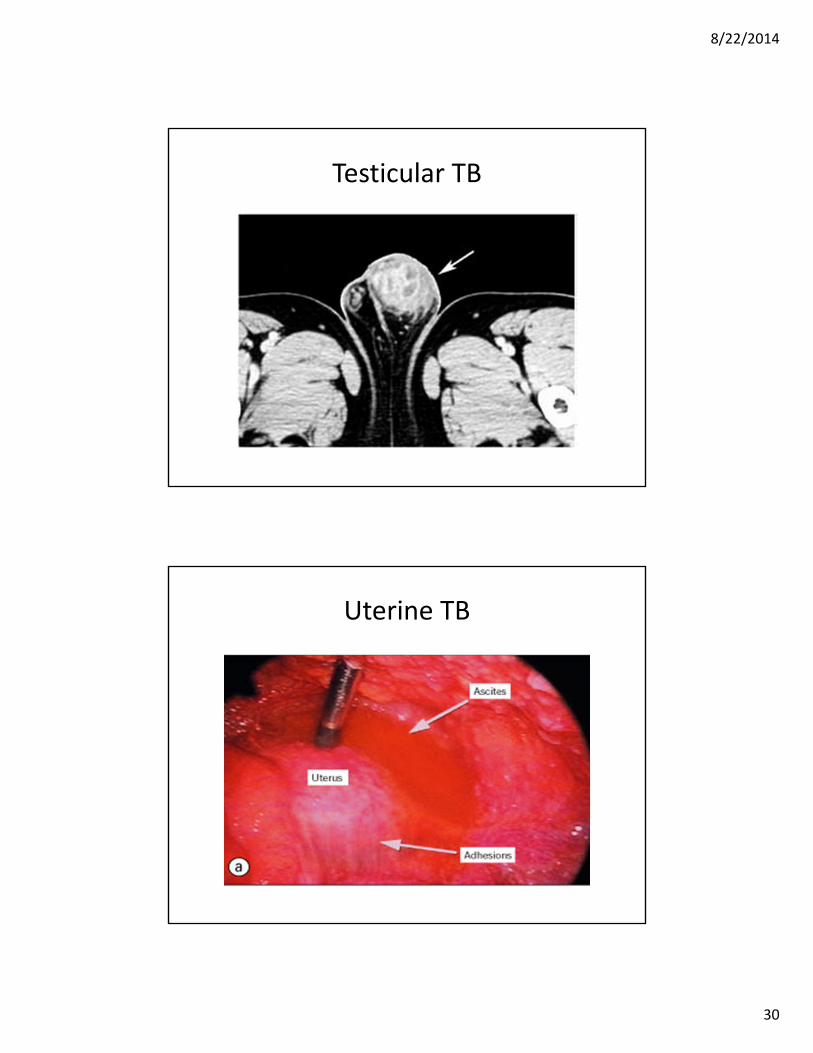
Testicular TB
Uterine TB

8/22/2014
31
Female Genital TB
• With Fallopian tube involvement, unlikely that preservation of fertility possible since usual scarring
• Often diagnosed by pathology after hysterectomy: treat even if involved organ removed
Surgical/Specialist Involvement
• Urology or gynecology involved in initial diagnosis
• Urologist essential if renal obstruction develops for ureteral stent placement and removal
• Obstruction may develop after therapy underway: immune reconstitution

8/22/2014
32
Other TB
Laryngeal TB
Tuberculous Otitis Media

8/22/2014
33
XXXXXXXXXXTB Mastoiditis
Adrenal TB

8/22/2014
34
Adrenal insufficiency and TB
• May have unsuspected adrenal involvement alone or with disseminated TB
• Assessment of adrenal function if slow response or hypokalemia, hyponatremia, hypotension
• Don’t forget adrenal insufficiency possiblity if steroids were stopped after long use
Ocular TB

8/22/2014
35
Ocular TB
• Diagnosis made by ophthalmologist
• Diagnosis of exclusion: patient should be followed by ophthalmology during TB treatment
• No cultures available
• Treat same as pulmonary TB
TB of the Skin

8/22/2014
36
Dermatologic TB
• May be hematogenous or direct spread
• May be injection: accidents in pathology or microbiology lab
• Treatment same as pulmonary TB
What’s left??

8/22/2014
37
TB Everywhere
Miliary or Disseminated TB
• Tiny lesions spread throughout the body
• Distinctive pattern on CXR or CT
8/22/2014
38
Miliary TB• Pulmonary involvement may not be present
• Frequently subacute presentation with fever and weight loss
• More rarely can be a fulminant sepsis‐like presentation with acute onset and rapid deterioration (usually fatal)
• Liver biopsy may be helpful
• Blood cultures may be positive if acid fast studies done
• All AFB may be negative
Treatment of Disseminated TB
• Prolonged treatment needed: 12 months or more
• Cultures may be negative: paucibacillary disease
• Don’t let negative cultures or normal CXR tempt you to shorten therapy

8/22/2014
39
Thank you
Don’t forget to get sputum AFB even if you think only extrapulmonary TB