adult granulosa cell tumor of the ovary: fine-needle-aspiration cytology of 10 cases and review of...
TRANSCRIPT
Adult Granulosa Cell Tumorof the Ovary:Fine-Needle-Aspiration Cytologyof 10 Cases and Review of LiteratureSarfraz Ali, M.D.,1 Paolo Gattuso, M.D.,2 Allison Howard, M.D.,2
Marina B. Mosunjac, M.D.,1 and Momin T. Siddiqui, M.D., F.I.A.C1*
Adult granulosa cell tumor (GCT) of the ovary is mostly diag-nosed in postmenopausal women. They typically secrete estro-gen, which stimulates the endometrium to proliferate andcause abnormal bleeding. This study reviews the cytologic fea-tures of adult GCT of the ovary diagnosed by fine-needleaspiration (FNA). We reviewed slides from ten cases diag-nosed by CT guided FNA from 1995 to 2007 at our institu-tions. Smears were stained with Diff-Quik and Papanicolaoustains. Patient’s history and histologic diagnosis were alsoavailable and reviewed for all cases. The patients ranged inage from 39 to 83 yr. All 10 cases were hypercellular withboth large and small overlapping cell clusters and individualcells. The cytologic features identified included: naked nuclei(10/10 cases), Call-Exner bodies (7/10 cases), blood vesselswith prominent perivascular tumor cell growth (4/10 cases),spindle-shaped hyperchromatic stromal cells within cellularclusters (6/10 cases), mixed inflammation (3/10 cases), tumorcell necrosis (1/10 cases), and prominent metachromaticstroma seen in association with blood vessels (1/10 cases).Moderate to scant delicate cytoplasm was also seen (10/10cases). Small, punctuate cytoplasmic vacuoles were also noted(7/10 cases) and were occasionally prominent (3/10 cases). Ingeneral nuclear to cytoplasmic ratios were high althoughlower than those typically seen in a lymphoma or small-cellcarcinoma. Nuclei were generally centrally located althougheccentrically located nuclei were consistently seen in a minor-ity of cells. Nuclei were monotonous in size showing slightlyconvoluted (occasional rentiform and fetiform nuclei) to polyg-onal outlines. Prominent, central nucleoli were also seen (4/10 cases). Nuclear grooves were also seen (9/10 cases). Noatypical mitotic activity was identified in any of the 10 cases(0/10 cases). In summary, the above cytologic features can
also help in the cytologic diagnosis of adult GCTs. Diagn.Cytopathol. 2008;36:297–302. ' 2008 Wiley-Liss, Inc.
Key Words: fine-needle-aspiration; adult granulosa cell tumor;sex-cord stromal tumor
Granulosa cell tumor (GCT) of the ovary is the most
common malignant sex-cord stromal tumor. As the name
implies, GCT is derived from the granulosa cell, a hormo-
nally active part of the ovarian stroma that is responsible
for estradiol production. GCT is therefore referred to as
an ovarian sex cord-stromal tumor, and it accounts for
70% of the tumors in this category. Although they
account for a large proportion of tumors within this cate-
gory, as a group they comprise only 2–3% of all ovarian
tumors and are therefore rare in every day practice.1–4
GCT can occur at any age but most commonly presents
during the perimenopausal or early postmenopausal pe-
riod, with a median age of diagnosis between 50 and
54 yr in most series.2–7 The estimated incidence of GCT
in the United States is 0.99/100,000.2,8,9
A number of recognized risk factors have been associ-
ated with the development of GCT, although most are not
reproducible and have unknown clinical or biologic sig-
nificance. For instance, menopausal status and parity, use
of fertility drugs or oral contraceptives are not consis-
tently associated with a higher risk.6,8,10,11 Unlike epithe-
lial ovarian cancer, there seems to be no known inherited
predisposition. In particular, inherited germ line mutations
of BRCA1 or BRCA2 have not been associated thus far
with a higher risk of developing GCT.
Clinically and morphologically, two types of GCT can
be distinguished, the more frequent Adult type (Adult
Granulosa Cell Tumor, AGCT) and the Juvenile type (Ju-
venile GCT). Juvenile GCT represents only 5% of this tu-
mor type and usually occurs in prepubertal girls and
women younger than 30 years.12 An adnexal mass with or
without endocrine manifestations in a patient usually over
1Department of Pathology, Emory University Hospital, Atlanta, Georgia2Department of Pathology, Rush University Medical Center, Chicago,
Illinois*Correspondence to: Momin T. Siddiqui, M.D., F.I.A.C., Department
of Pathology and Laboratory Medicine, Emory University Hospital, 1364Clifton Road, NE, Atlanta, GA 30322.E-mail: [email protected]
Received 16 August 2007; Accepted 20 November 2007DOI 10.1002/dc.20798Published online in Wiley InterScience (www.interscience.wiley.com).
' 2008 WILEY-LISS, INC. Diagnostic Cytopathology, Vol 36, No 5 297

the age of 50 years is the usual clinical presentation.
AGCTs are hormonally active neoplasms that secrete high
levels of estrogen, which can lead to abnormal uterine
bleeding (Menorrhagia or Metrorrhagia), endometrial
hyperplasia (50–60%) and ultimately adenocarcinoma (5–
10%).5,13 Rarely, AGCTs are androgenic and patients
may present with virilization.14,15
It is clinically very important that a correct and accu-
rate diagnosis of AGCT be established. Fine-needle aspi-
ration (FNA) biopsy is by now an approved and valuable
method in the diagnosis of tumors in many organs. This
method can also be used safely in the diagnosis of ovar-
ian tumors including GCTs. Since individual clinicians
and pathologists encounter such tumors only occasionally,
we felt it worthwhile to document our experience with
the utilization of FNA in the diagnosis of AGCTs. Our
findings are presented in the light of a number of previous
studies on the cytologic features of AGCT.
Materials and Methods
A retrospective review of clinical data of AGCTs was eval-
uated through a search of pathology archives of Emory
University Hospital and Rush University Medical Center.
All cases of AGCTs which were resected, from 1995 to
2007, were reviewed. All cases were primary and proven
histologically. The diagnostic material from CT-guided
FNA on all cases was than retrieved and reviewed for eval-
uating cytological features. The smears from these cases
had been prepared by using both, 95% ethanol-fixed slides
which were stained with Papanicolaou stain, as well as by
air-drying and staining by Diff-Quik techniques.
Results
A total of 10 cases of AGCT were which were diagnosed
by FNA were available and selected for review. All 10
patients had undergone surgical resection and the subse-
quent histological diagnosis was confirmed. The age range
of all the patients was from 39 to 83 years. Two cases
were from the right ovary and eight cases were from the
left ovary.
Salient cytological features were reviewed and are sum-
marized in Table I. All 10 cases were hyper cellular with
both large and small overlapping cell clusters and individ-
ual cells (Fig. 1). Characteristic Call-Exner bodies were
present in most of the cases (Fig. 2). These bodies consist
of small rings of granulosa cells surrounding eosinophilic
fluid and basement membrane material. Blood vessels
with prominent perivascular tumor cell growth and mixed
inflammation were also noted in one third of cases
(Fig. 3). In half of the cases, spindle shaped hyperchro-
matic stromal cells within cellular clusters were present.
Ten percentage of cases showed tumor cell necrosis and
Table I. Cytomorphologic Features of AGCT Which Were Identifiedin the Cases Included in This Study
Cytologic feature of AGCT No. of cases (%)
GeneralHypercellularity 10/10 (100)Call-exner bodies 7/10 (70)Blood vessels 4/10 (40)Spindle-shaped hyperchromatic stromal cells 6/10 (60)Mixed inflammation 3/10 (30)Tumor cell necrosis 1/10 (10)Prominent metachromatic stroma 1/10 (10)Atypical mitotic activity 0/10 (0)High nuclear to cytoplasmic ratio 10/10 (100)
CytoplasmModerate to scant delicate cytoplasm 10/10 (100)Cytoplasmic vacuoles 7/10 (70)
NucleusNaked nuclei 10/10 (100)Nucleoli 4/10 (40)Nuclear grooves 9/10 (90)
Fig. 1. Low power view of fine need aspirate material from an ovarianadult granulosa cell tumor exhibiting hypercellularity with both largeand small overlapping cell clusters and individual dispersed cells (Diff-Quik stain, 3100).
Fig. 2. The tumor cells showed characteristic Call-Exner body formation(Diff-Quik stain, 3400).
ALI ET AL.
298 Diagnostic Cytopathology, Vol 36, No 5
Diagnostic Cytopathology DOI 10.1002/dc
prominent metachromatic stroma seen in association with
blood vessels. No atypical mitotic activity was identified
in any of the 10 cases. In general nuclear to cytoplasmic
ratios were high although lower than typically seen in a
lymphoma or small cell carcinoma. The cells had moder-
ate to scant delicate cytoplasm in all cases. Small, punctu-
ate cytoplasmic vacuoles were also noted and were occa-
sionally prominent in some of the cases (Fig. 4). Nuclei
which were denuded of cytoplasm (naked nuclei) were
also seen (Fig. 5). The nuclei were generally centrally
located although eccentrically located nuclei were consis-
tently seen in a minority of cells. The nuclei were monot-
onous in size and showed slightly convoluted (occasion-
ally rentiform and fetiform nuclei) to polygonal outlines,
sometimes appearing to ‘‘square off’’ especially those
with eccentric locations (Fig. 6). Prominent central nucle-
oli were also occasionally found. Nuclear grooves were
also seen in 90% of cases and ranged in prominence. In
addition subjective scoring was assigned to the presence
of nuclear grooves and is summarized in Table II.
Discussion
Ovarian cancer accounts for about 3% of all cancers
among women and ranks second among gynecologic can-
cers, following cancer of the uterine corpus.16 In recent
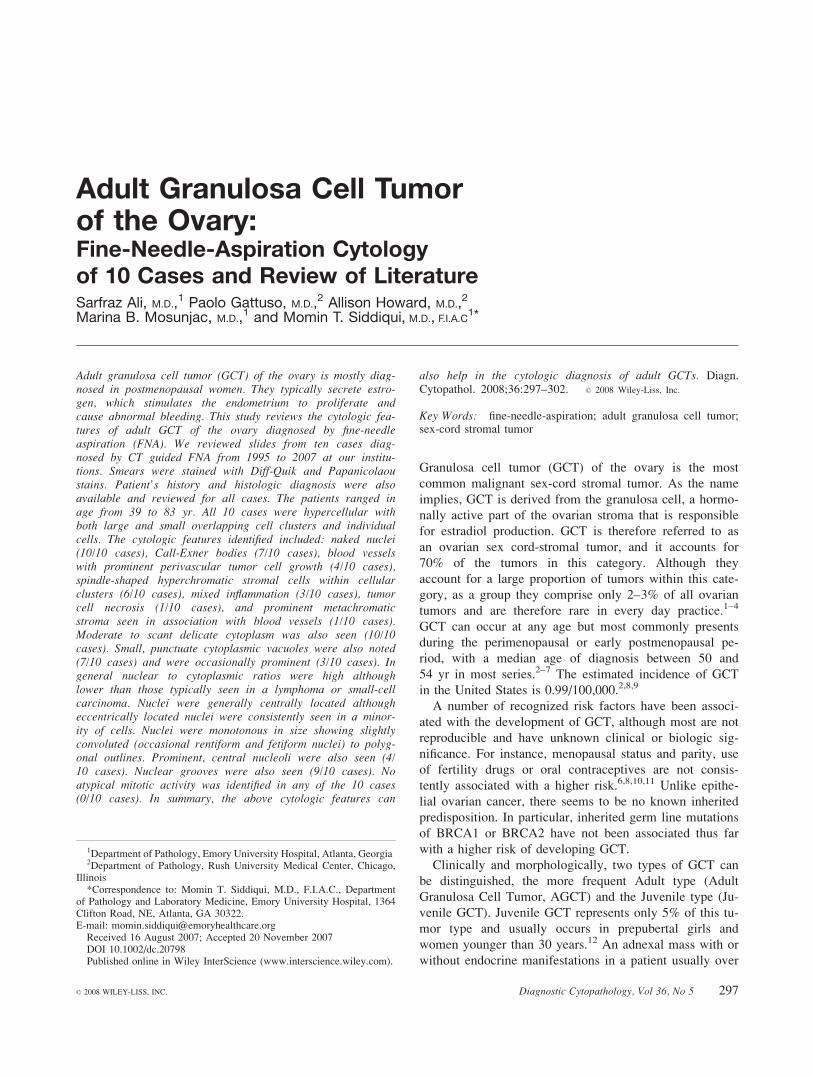
Fig. 3. A blood vessel with prominent tumor cell growth is identifiedhere. The background also shows naked nuclei as well as scattered lym-phocytes (Diff-Quik stain, 3200).
Fig. 4. Small, punctuate cytoplasmic vacuoles were also noted and wereoccasionally prominently present in some cells (Diff-Quik stain, 3400).
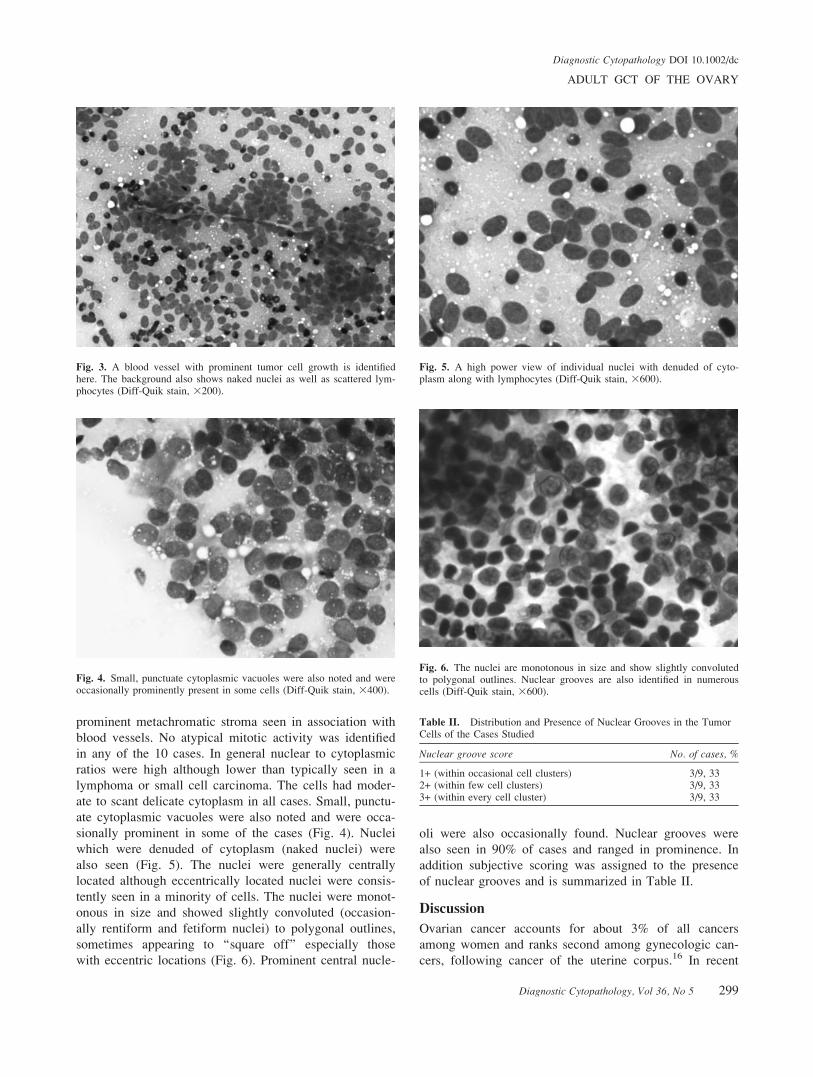
Fig. 5. A high power view of individual nuclei with denuded of cyto-plasm along with lymphocytes (Diff-Quik stain, 3600).
Fig. 6. The nuclei are monotonous in size and show slightly convolutedto polygonal outlines. Nuclear grooves are also identified in numerouscells (Diff-Quik stain, 3600).
Table II. Distribution and Presence of Nuclear Grooves in the TumorCells of the Cases Studied
Nuclear groove score No. of cases, %
1+ (within occasional cell clusters) 3/9, 332+ (within few cell clusters) 3/9, 333+ (within every cell cluster) 3/9, 33
ADULT GCT OF THE OVARY
Diagnostic Cytopathology, Vol 36, No 5 299
Diagnostic Cytopathology DOI 10.1002/dc

years, incidence of ovarian cancer has declined by 0.7%.
However, *22,000 new cases of ovarian cancer will still
be diagnosed in the United States in 2007.16 These malig-
nancies will also account for more than 14,000 deaths in
the United States this year.16
GCTs are relatively rare functional neoplasms of the
ovary. These tumors are regarded as malignancies,
although of a low-grade type. Most GCTs (70–90%) are
pathologic Stage I disease at diagnosis.5,8,17–19 Although
patients with AGCT present with early-stage disease,
relapses tend to occur in a more indolent fashion, often
many years after the original diagnosis.20,21 Patients with
GCT require long-term clinical follow-up because of the
known, yet unpredictable, recurring or metastasizing
behavior many years after a disease-free interval even in
those with Stage I or Stage II tumor at diagnosis.22,23
It is also important to know that AGCT are usually
diagnosed during child bearing years, however the age
range is broad since they sometimes occur before puberty
or even after menopause.1 A majority of these tumors are
associated with hyperestrinism, which leads to excessive
estrogen production, leading to isosexual precocious pu-
berty in children and to metrorrhagia in adults, including
women in the postmenopausal age group.10 However,
some of the cases are hormonally inactive at the clinical
level, and very rarely androgenic.14,15
The concept of prognosis for AGCT is also of interest.
A number of clinical, pathologic, and molecular prognos-
tic factors have been proposed for AGCT, although the
reproducibility of many factors has been difficult to estab-
lish. More than 75% of GCTs are diagnosed as Interna-
tional Federation of Gynecology and Obstetrics (FIGO)
stage I and only 6% are stage IV.17 Stage of Granulosa
tumor is clearly the most important prognostic factor.6,8,18
The reported 5-year survival rate for patients with stage I
disease ranges from 75 to 95%.5,18 This contrasts with the
55–75% 5-year survival rate for patients with stage II
tumors and the 22–50% survival rate for stage III/IV can-
cers,7,8,19 demonstrating the potential for late relapse and
death in patients with advanced disease. Although AGCT
has been considered to be of low-grade malignancy, 10–
50% of the patients develop recurrences presenting as late
as 20 to 30 years after initial diagnosis.21 A number of
pathologic and molecular factors have also been evaluated
for their prognostic significance. Fujimoto et al., evaluated
several histopathologic variables including stage, p53 sta-
tus, histologic pattern with or without Call-Exner bodies,
mitotic index (MI), and lymphovascular space invasion.19
In this report, only MI and lymphovascular space invasion
were independent prognostic factors. In particular,
patients who experienced a relapse had a significantly
higher MI (median, five mitoses/10 HPF) than those with-
out recurrence (median, 1.5 mitoses/10 HPF; P < 0.001).
Furthermore, the disease-free survival rate at 80 months
for patients with tumors containing fewer than four mito-
ses/10 HPF was 90%, compared with 25% for patients
whose tumors demonstrated four or more mitoses/10 HPF
(P < 0.0005). Other studies however, have not found a
convincing association between MI and prognosis.18,24
Morphologically, different growth patterns can be
observed in AGCT: microfollicular (most frequent), mac-
rofollicular, trabecular, insular, solid-tubular, gyriform,
and diffuse (sarcomatoid). FNA cytology is a well estab-
lished technique for the diagnosis of various neoplastic
and non-neoplastic ovarian masses.25,26 Angstrom et al.,
has reported an accuracy rate of over 90% in benign and
malignant ovarian neoplasms diagnosed by FNA cytol-
ogy.25 In addition, Sevin et al., has reported a sensitivity
of greater than 90% in diagnosing malignant ovarian neo-
plasms by FNA.26 It was the purpose of this study to
review the cytologic features of AGCT which had been
diagnosed by FNA.
The cytological features described in the literature are
quiet distinctive, such as monotonous cells, microfollicu-
lar pattern, and nuclear grooves. We found all of these
characteristic features in AGCT cells demonstrated by
FNA in our study. All of the 10 cases exhibit microfollic-
ular cell pattern. The tumor cells were relatively monoto-
nous, with nuclear grooves in almost all cell nuclei (90%)
in our study. Call-Exner bodies have been demonstrated
in 30–60% of cases of AGCT.4,9,24 We observed Call-
Exner bodies in more than two thirds (70%) of our cases.
The distinct nuclear appearance is one of the hallmark
features of ovarian AGCT. AGCT tumor nuclei are typi-
cally uniform and pale and are often grooved (nuclear
grooves) giving them a ‘‘coffee-bean’’ appearance. We
detected nuclear grooves in 9 of the 10 cases studied,
however the number of cells exhibiting this nuclear fea-
ture was variable (Table II). Conflicting data exist about
the presence of nucleoli in AGCTs. Aboud et al., and
others demonstrated in their studies that nucleoli were
absent in AGCT cells.20,27–29 In contrast to these reports,
nucleoli have been observed in AGCT cells in some other
studies.21,30,31 In our study, we were able to detect promi-
nent nucleoli in only 4 of 10 cases.
Nuclear grooves being one of the classic features of
AGCT need to be discussed further since this feature is
not exclusive to this tumor alone. Proliferating Brenner
Tumor and Sex Cord Tumor with Annular Tubules
(SCTAT) are two other primary ovarian tumors that are
characterized by the presence of prominent nuclear
grooves which are indistinguishable on the basis of cytol-
ogy alone. These three ovarian tumors are all composed
of sheets and trabecular structures lined by a pseudostrati-
fied layer of relatively monotonous cells with the so-
called coffee-bean-shaped nuclei. Proliferating Brenner
Tumor and SCTAT have small nucleoli, which can be
helpful in differentiating from AGCT.32,33 Immunohisto-
ALI ET AL.
300 Diagnostic Cytopathology, Vol 36, No 5
Diagnostic Cytopathology DOI 10.1002/dc

chemistry, as demonstrated by some studies, can also be
useful in the differential diagnosis since AGCT is immu-
noreactive for Inhibin and CD99.34,35 The epithelial nests
of Brenner tumor are immunoreactive for cytokeratin and
epithelial membrane antigen, which can help in the diag-
nosis. SCTAT is mainly differentiated on the basis
rosettes, with or without a central acellular core compris-
ing of basement membrane material.33 The rosettes
observed in SCTAT are three dimensional with greater
cellularity than that seen in Call-Exner bodies of AGCT.
In addition, the luminal material in Call-Exner bodies is
less defined than in the rosettes of SCTAT.33
Occasionally, AGCT with a diffuse pattern can be mis-
taken for a poorly differentiated carcinoma. The nuclear
appearance can be very helpful for differentiating the two
entities.36 AGCT nuclei are normally uniform and pale
and are often grooved, whereas the nuclei of undifferenti-
ated carcinomas are often hyperchromatic, without
grooves, and unequal in size and shape.36 Nuclear atypia
and multiple mitotic figures are also less common in
AGCT, as in our study. These two features are frequently
observed in undifferentiated carcinomas.36,37 For difficult
cases, immunohistochemistry staining for epithelial mem-
brane antigen and inhibin may be useful, where AGCT
would be epithelial membrane antigen-negative and
inhibin-positive, whereas carcinoma would exhibit the
reverse pattern.38,39
To conclude, AGCTs may create a diagnostic challenge
in cytologic preparations because of its rarity. We have
studied only a few cases of AGCT by FNA. The most con-
sistent features of AGCTs in cellular aspirates include
cohesion and discohesion, naked nuclei and nuclear
grooves. The findings of admixed hyperchromatic spindle-
shaped stromal cells and blood vessels can also help sup-
port the cytologic diagnosis of adult GCT. We feel that the
cytologic picture of GCTs is fairly characteristic and
includes specifically monotonous cells, nuclear grooves
and Call-Exner bodies. The distinguishing cytologic picture
in FNA preparation should, together with the clinical find-
ings, lead to a correct preoperative diagnosis of adult GCT.
References
1. Kurman RJ. Blaustein’s pathology of the female genital tract. New-
York: Springer-Verlag; 1996. p 783–797.
2. Ohel G, Kaneti H, Schenker JG. Granulosa cell tumors in Israel: A
study of 172 cases. Gynecol Oncol 1983;15:278–286.
3. Evans AT, Gaffey TA, Malkasian GD, Annegers JF. Clinicopatho-
logic review of 118 granulosa and 82 theca cell tumors. ObstetGynecol 1980;55:231–238.
4. Fox H, Langly FA. A clinicopathological study of 92 cases of gran-
ulosa cell tumors of the ovary with special reference to factorsinfluencing prognosis. Cancer 1975;35:231–241.
5. Savage P, Constenla D, Fisher C, et al. Granulosa cell tumors of
the ovary: Demographics, survival and the management of advanceddisease. Clin Oncol (R Coll Radiol) 1998;10:242–245.
6. Miller BE, Barron BA, Wan JY, Delmore JE, Silva EG, Gershenson
DM. Prognostic factors in adult granulosa cell tumors of the ovary.Cancer 1997;79:1951–1955.
7. Piura B, Nemet D, Yanai-Inbar I, Cohen Y, Glezerman M. Granu-
losa cell tumor of the ovary: A study of 18 cases. J Surg Oncol1994;55:71–77.
8. Malmstrom H, Hogberg T, Risberg B, Simonsen E. Granulosa cell
tumors of the ovary: Prognostic factors and outcome. GynecolOncol 1994;52:50–55.
9. Stenwig JT, Hazekamp JT, Beecham JB. Granulosa cell tumors of
the ovary: A clinicopathological study of 118 cases with long-termfollow up. Gynecol Oncol 1979;7:136–152.
10. WillemsenW, Kruitwagen R, Bastiaans B, Hanselaar T, Rolland R. Ovar-ian stimulation and granulosa-cell tumor. Lancet 1993;341: 986–988.
11. The Cancer and Steroid Hormone Study of the Centers for DiseaseControl and the National Institute of Child Health and Human.Development: The reduction in risk of ovarian cancer associatedwith oral-contraceptive use. N Engl J Med 1987;316:650–655.
12. Young RH, Dickersin GR, Scully RE. Juvenile granulosa celltumors of the ovary: A clinicopathologic analysis of 125 cases. AmJ Surg Pathol 1984;8:575–596.
13. Segal R, DePetrillo AD, Thomas G. Clinical review of adult granu-losa cell tumors of the ovary. Gynecol Oncol 1995;56:338–344.
14. Idem. Ovarian tumors with endocrine manifestations. In: DeGrootLJ, editor, Endocrinology. 3rd ed. Philadelphia: W. B. Saunders;1995. vol. 3, p 2113–2127.
15. Nakashima N, Young RH, Scully RE. Androgenic granulosa celltumors of the ovary. A clinicopathologic analysis of 17 cases andreview of the literature. Arch Pathol Lab Med 1984;108:786–791.
16. American Cancer Society. Facts and figures. Atlanta, GA; 2007.
17. Fox H. Pathologic prognostic factors in early stage adult-type gran-ulosa cell tumors of the ovary. Int J Gynaecol Cancer 2003;13:1–4.
18. Lauszus FF, Peterson AC, Greisen J, et al. Granulosa cell tumor ofthe ovary: A population based study of 37 women with stage I dis-ease. Gynecol Oncol 2001;81:456–460.
19. Fujimoto T, Sakuragi N, Okuyama K, et al. Histopathologic prog-nostic factors of adult granulosa cell tumors of the ovary. ActaObstet Gynecol Scand 2001;80:1069–1074.
20. Jeffrey F. Hines MD, Mahmoud A, et al. Recurrent granulosacell tumor of the ovary 37 years after initial diagnosis: A case reportand review of the literature gynecologic oncology 1996;60: 484–488.
21. Ylagan LR, Middleton WD, Dehner LP. Fine needle aspiration cy-tology of recurrent granulosa cell tumor: Case report with differen-tial diagnosis and immunocytochemistry. Diagn Cytopathol 2002;27:38–41.
22. Sasano S, Yamamoto H, Otsuka T, Imura Y, Nishii N, Nitta S. Pulmo-nary multiple metastases of ovarian granulosa cell tumor 15 years afterinitial diagnosis. Jpn J Thorac Cardiovasc Surg 2000;48: 655–658.
23. Williams RJ, Kamel HM, Jilaihawi AN, Prakash D. Metastatic gran-ulosa cell tumor of the diaphragm 15 years after the primary neo-plasm. Eur J Cardiothorac Surg 2001;19:516–518.
24. Bjorkholm E, Silfversward C. Prognostic factors in granulosa celltumors. Gynecol Oncol 1981;11:261–274.
25. Angstrom T, Kjellgren O, Bergman F. The cytological diagnosis ofovarian tumors by means of aspiration biopsy. Acta Cytol 1972;16:336–341.
26. Sevin BU, Greening SE, Nadji M, Averette HE, Nordqvist SRB.Fine needle aspiration cytology in gynecological oncology: Clinicalaspects. Acta Cytol 1979;23:277–281.
27. Aboud E. A review of granulosa cell tumours and thecomas of theovary. Arch Gynecol Obstet 1997;259:161–165.
28. Lal A, Bourtsos EP, Nayar R, DeFrias DV. Cytologic features ofgranulosa cell tumors in fluids and fine needle aspiration specimens.Acta Cytol 2004;48:315–320.
29. Nguyen GK, Redburn J. Aspiration biopsy of granulosa-cell tumorof the ovary: Cytologic findings and differential diagnosis. DiagnCytopathol 1992;8:253–257.
ADULT GCT OF THE OVARY
Diagnostic Cytopathology, Vol 36, No 5 301
Diagnostic Cytopathology DOI 10.1002/dc

30. Martellotto G, Frede S, Ortiz S, Hliba E. Granulosa cell tumors:
Structural and ultra structural analysis. Rev Fac Cien Med Univ
Nac Cordoba 2001;58:117–123.
31. Ali SZ. Metastatic granulosa cell tumor in the liver: Cytopathologic
findings and staining with inhibin. Diagn Cytopathol 1998;19:293–
297.
32. Ordonez NG, MacKay B. Brenner tumor of the ovary: A comparativeimmunohistochemical and ultrastructural study with transitional cellcarcinoma of the bladder. Ultrastruct Pathol 2000;24: 157–167.
33. Ryan LJ, Pambuccian SE, Lai R, Gulbahce HE. Endoscopic ultra-sound-guided fine needle aspiration diagnosis of metastatic sex cordtumor with annular tubule: A case report. Diagn Cytopathol 2006;34:576–579.
34. McCluggage WG, Maxwell P, Sloan JM. Immunohistochemicalstaining of ovarian granulosa cell tumors with monoclonal antibodyagainst inhibin. Hum Pathol 1997;29:1034–1038.
35. Choi YL, Kim HS, Ahn G. Immunoexpression of inhibin a subunit,inhibin/activin beta subunit and CD99 in ovarian tumors. ArchPathol Lab Med 2000;124:563–569.
36. Young RH, Scully RE. Sex cord-stromal, steroid cell, and other
ovarian tumors with endocrine, paraendocrine and paraneo-
plastic manifestations. In: Kurman RJ, editor. Pathology of the
female genital tract. 4th ed. New York: Springer: 1994. p 783–847.
37. Hartman LC, Young RH, Podratz KC. Ovarian sex-cord stromal
tumors. In: Hoskins WJ, Perez CA, Young RC, editors. Principles
and practice of gynecologic oncology, 3rd ed. Baltimore, MD: Lip-
pincott Williams & Wilkins; 2000. p 1075–1091.
38. McCluggage WG. Value of inhibin staining in gynecologic pathol-ogy. Int J Gynecol Pathol 2001;20:79–85.
39. Hildebrant RH, Rouse RV, Longacre TA. Value of inhibin in theidentification of granulosa cell tumors of the ovary. Hum Pathol1997;28:1387–1395.
ALI ET AL.
302 Diagnostic Cytopathology, Vol 36, No 5
Diagnostic Cytopathology DOI 10.1002/dc