adult clinical decision rules for trauma - trauma · pdf fileadult clinical decision rules for...
TRANSCRIPT

Adult Clinical Decision
Rules for Trauma William D. Hampton, DO Emergency Physician 26 March 2015
1. Explain statistical sensitivity & specificity and apply that knowledge in the evaluation of clinical decision rules (CDRs).
2. Discuss the various adult trauma clinical decision rules and how they were derived.
3. Compare and contrast the CDRs for head injury, cervical spine injury, and lower extremity injuries in adult trauma patients.
4. Explain the importance of CDRs in triage, selective diagnostic testing, and dispositioning trauma patients.
Learning Objectives
• Faculty/Presenters/Authors/Content Reviewers/Planners disclose no conflict of interest relative to this educational activity.
Disclosure Statement
• To successfully complete this course, participants must attend the entire event and complete/submit the evaluation at the end of the session.
• Society of Trauma Nurses is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's Commission on Accreditation.
Successful Completion

On a busy shift at a local emergency department, you are placed in triage and presented with a variety of patients…
Or you work at a teaching hospital, and are particularly concerned about patient safety come every July…
Or you work as a Nurse Practitioner at a critical access ED, and want to refine your telemedicine trauma referrals…

Or you would simply like to become more comfortable in assessing and caring for critically injured patients…


Statistical Definitions
Definitions Imagine a study evaluating a new test
that screens people for a disease.
http://en.wikipedia.org/wiki/Sensitivity_and_specificity. Accessed last 9/5/2013.
Each person taking the test either has or does not have the disease. The test can be positive (predicting that the person has the disease)
or negative (predicting that the person does not have the disease).
The test results for each subject may or may not match
the subject's actual status.
Definitions True positive Sick people correctly diagnosed as sick
False positive Healthy people incorrectly identified as sick
True negative Healthy people correctly identified as healthy
False negative Sick people incorrectly identified as healthy
http://en.wikipedia.org/wiki/Sensitivity_and_specificity. Accessed last 9/5/2013.
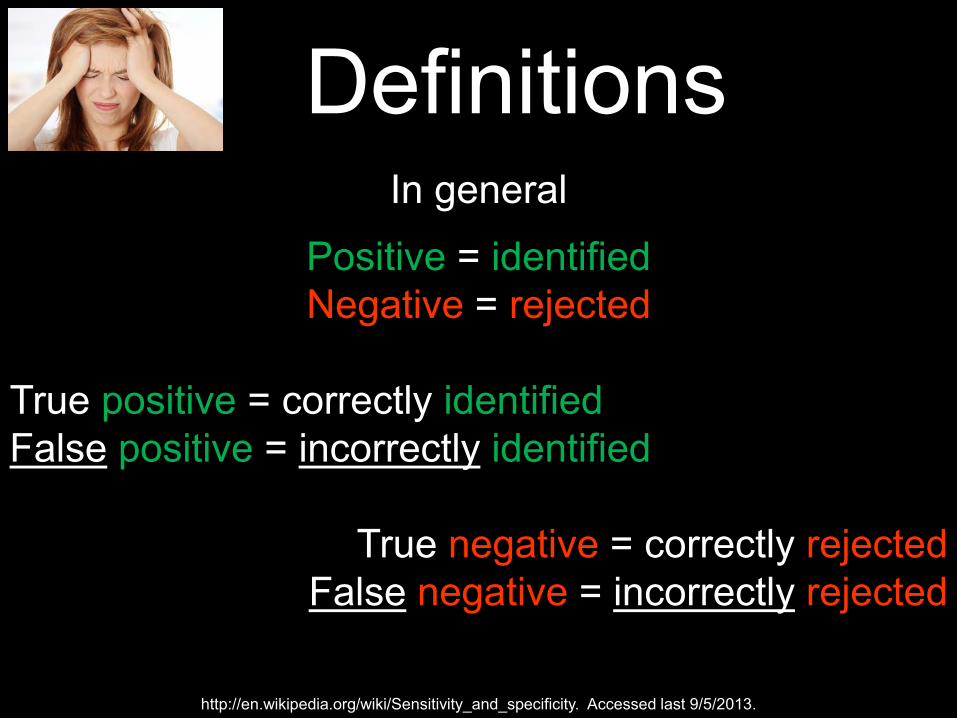
Definitions In general
Positive = identified Negative = rejected
True positive = correctly identified False positive = incorrectly identified
True negative = correctly rejected
False negative = incorrectly rejected
http://en.wikipedia.org/wiki/Sensitivity_and_specificity. Accessed last 9/5/2013.
Sensitivity & Specificity
Snout Spin

Sensitivity
Snout – “Sensitivity rules it out”
Imagine that everyone in the audience came down with URI sx, and someone suggested that it might be Legionnaires’ Dz.
You all have symptoms, but you want to know for certain you don’t have Legionnaire’s!
A highly sensitive test would definitely catch anyone that is positive (for Legionnaires’ Dz). So if they’re not positive, you can be sure that they are negative.
Negative results in a high sensitivity test are used to rule-out the disease.
Specificity
Spin – “Specificity rules it in”
Imagine that everyone in the audience felt well, but you were told that you had been exposed to the SARS Virus.
The CDC is offering treatment to everyone…but it will cost you $10,000. You would like to be certain that you actually have SARS before spending $10,000 on treatment!
A highly specific test would definitively show everyone that is negative for the disease. So if you test positive (for SARS), you can be sure that you are not mistakenly positive!
A positive result from a test with high specificity means a high probability of the presence of disease.
Giddy-up
Case #1 – 65-y/o ♂ fell off ladder CC: 65-y/o ♂ presents to UC
after falling off stepladder 3 hours ago. Lost balance while fixing the roof. Admits “head pain” at site of impact. Denies vomiting, syncope, or other injuries.
PE: Normal vitals. Small bruise noted above left eye. Prefers eyes closed throughout exam.
Case #2 – 24-y/o ♀ slip & fall by pool
CC: 24-y/o ♀ presents after slip and fall on pool deck last night. Friend attributes fall to “the wine.” Admits headache and one episode of vomiting after fall. Denies any other injuries.
PE: Normal vitals. Tender hematoma noted above left ear. Left hemotympanum. GCS is 15.
Cases #1 & 2
Which of these patients needs a CT Head?
65-y/o ♂ 24-y/o ♀ Neither Both
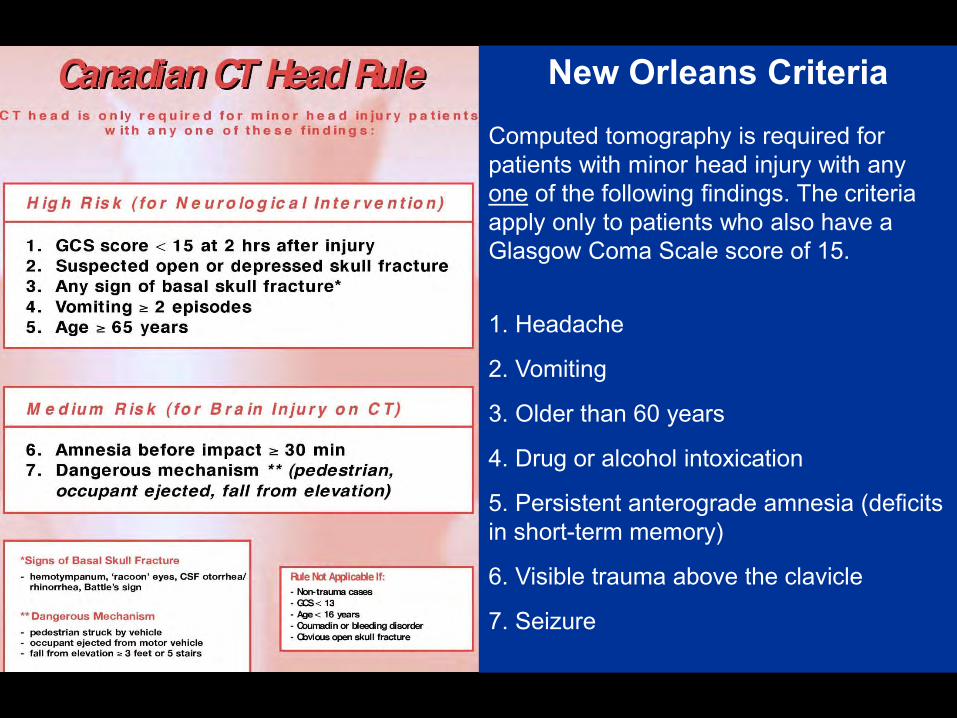
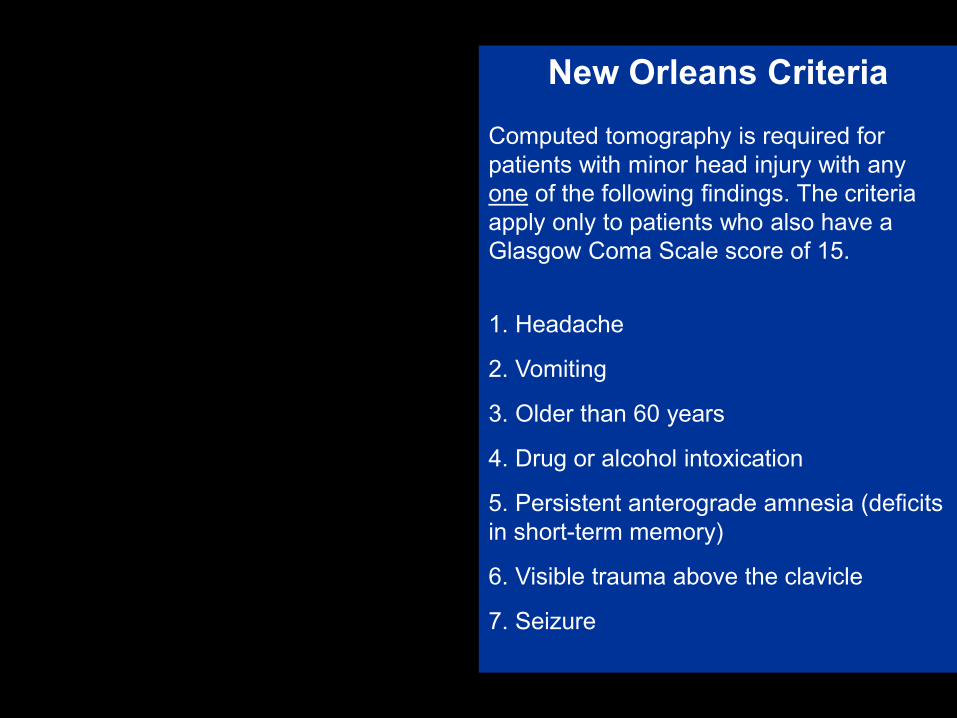
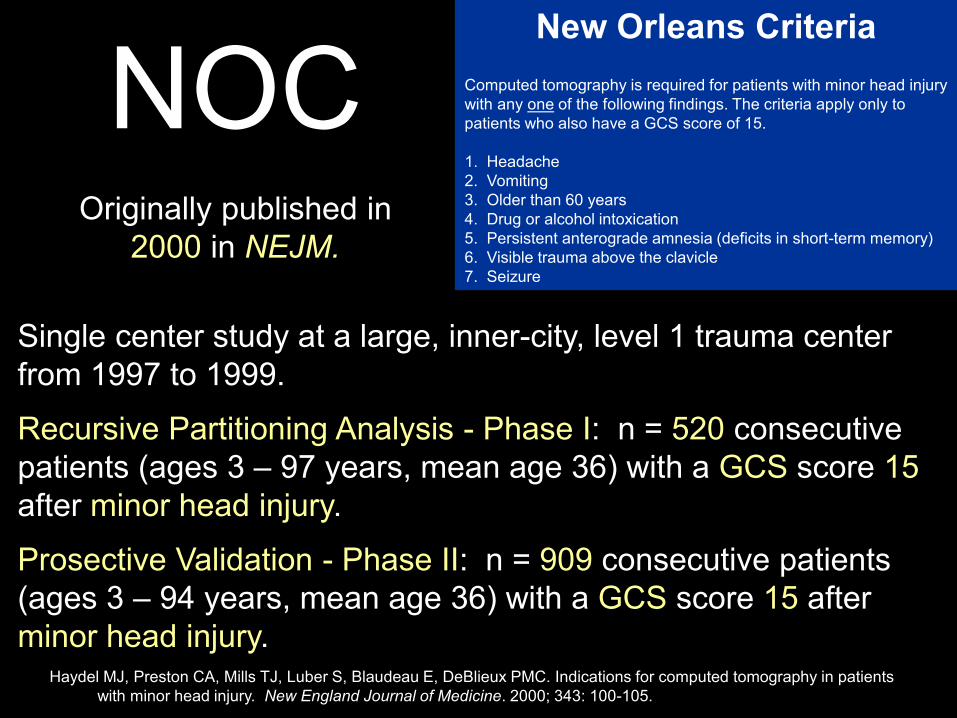
New Orleans Criteria Computed tomography is required for patients with minor head injury with any one of the following findings. The criteria apply only to patients who also have a Glasgow Coma Scale score of 15.
1. Headache
2. Vomiting
3. Older than 60 years
4. Drug or alcohol intoxication
5. Persistent anterograde amnesia (deficits in short-term memory)
6. Visible trauma above the clavicle
7. Seizure
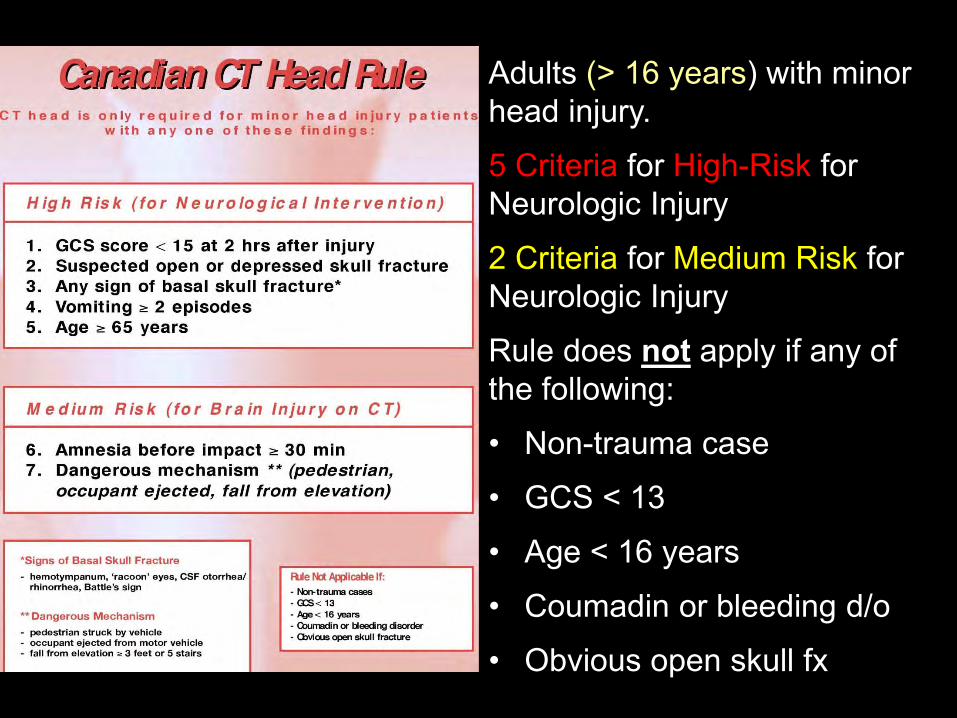
Adults (> 16 years) with minor head injury.
5 Criteria for High-Risk for Neurologic Injury
2 Criteria for Medium Risk for Neurologic Injury
Rule does not apply if any of the following:
• Non-trauma case
• GCS < 13
• Age < 16 years
• Coumadin or bleeding d/o
• Obvious open skull fx
New Orleans Criteria Computed tomography is required for patients with minor head injury with any one of the following findings. The criteria apply only to patients who also have a Glasgow Coma Scale score of 15.
1. Headache
2. Vomiting
3. Older than 60 years
4. Drug or alcohol intoxication
5. Persistent anterograde amnesia (deficits in short-term memory)
6. Visible trauma above the clavicle
7. Seizure
CCHR
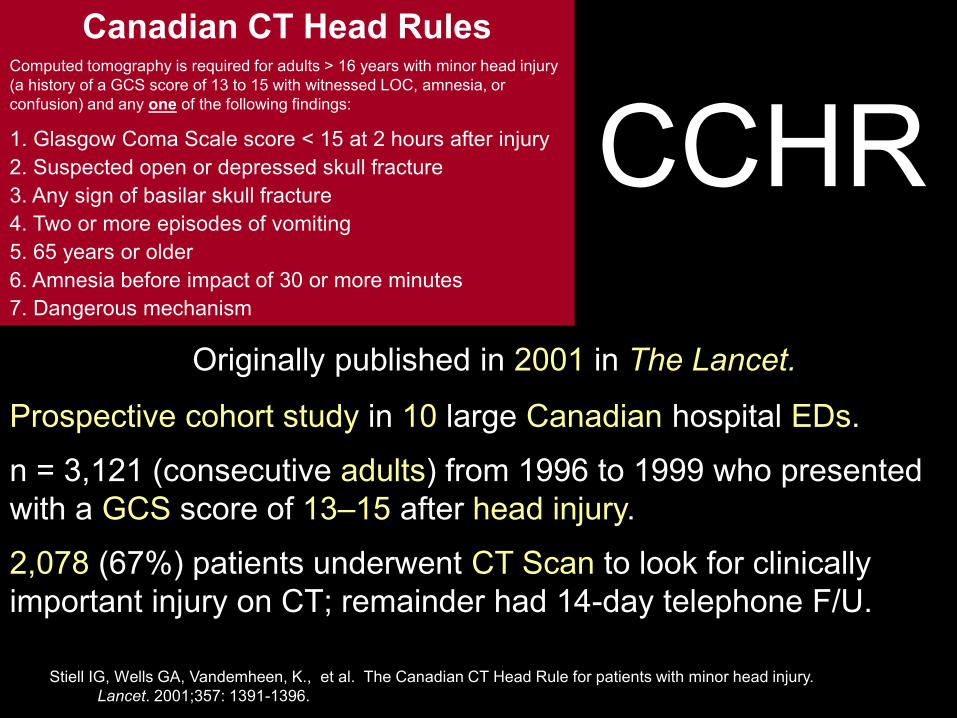
Prospective cohort study in 10 large Canadian hospital EDs.
n = 3,121 (consecutive adults) from 1996 to 1999 who presented with a GCS score of 13–15 after head injury.
2,078 (67%) patients underwent CT Scan to look for clinically important injury on CT; remainder had 14-day telephone F/U.
Originally published in 2001 in The Lancet.
Stiell IG, Wells GA, Vandemheen, K., et al. The Canadian CT Head Rule for patients with minor head injury. Lancet. 2001;357: 1391-1396.
Canadian CT Head Rules
Computed tomography is required for adults > 16 years with minor head injury (a history of a GCS score of 13 to 15 with witnessed LOC, amnesia, or confusion) and any one of the following findings:
1. Glasgow Coma Scale score < 15 at 2 hours after injury
2. Suspected open or depressed skull fracture
3. Any sign of basilar skull fracture
4. Two or more episodes of vomiting
5. 65 years or older
6. Amnesia before impact of 30 or more minutes
7. Dangerous mechanism
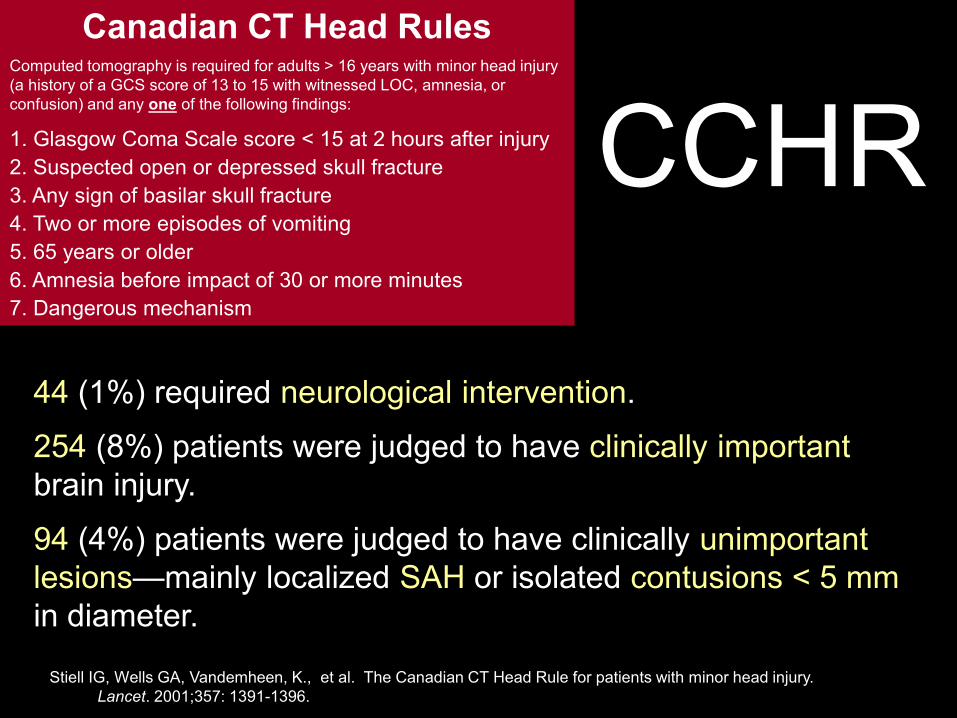
44 (1%) required neurological intervention.
254 (8%) patients were judged to have clinically important brain injury.
94 (4%) patients were judged to have clinically unimportant lesions—mainly localized SAH or isolated contusions < 5 mm in diameter.
Stiell IG, Wells GA, Vandemheen, K., et al. The Canadian CT Head Rule for patients with minor head injury. Lancet. 2001;357: 1391-1396.
CCHR
Canadian CT Head Rules
Computed tomography is required for adults > 16 years with minor head injury (a history of a GCS score of 13 to 15 with witnessed LOC, amnesia, or confusion) and any one of the following findings:
1. Glasgow Coma Scale score < 15 at 2 hours after injury
2. Suspected open or depressed skull fracture
3. Any sign of basilar skull fracture
4. Two or more episodes of vomiting
5. 65 years or older
6. Amnesia before impact of 30 or more minutes
7. Dangerous mechanism
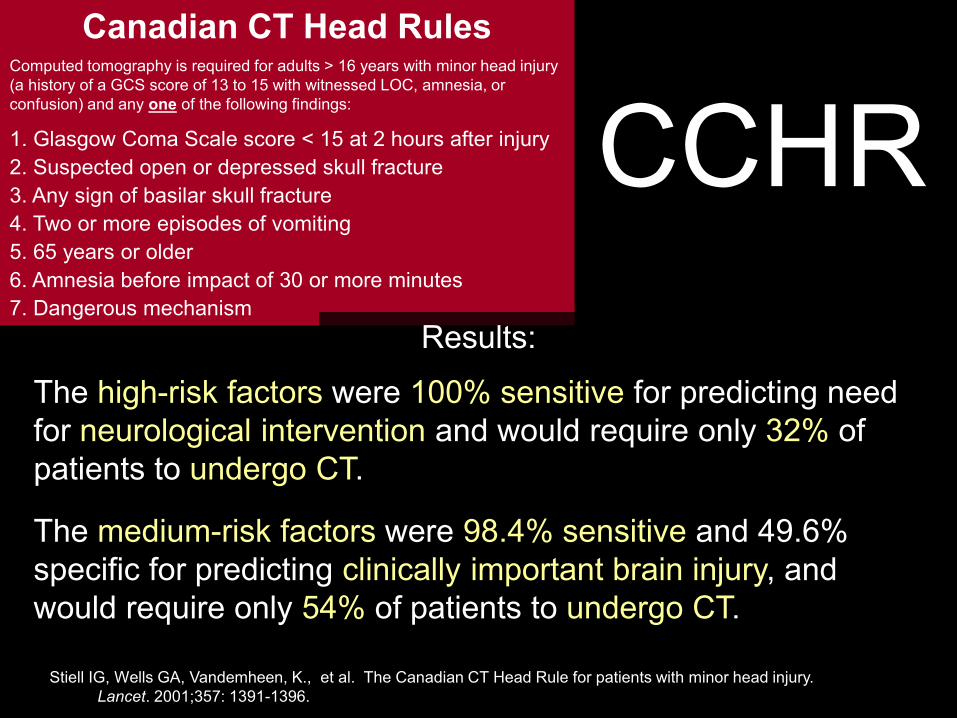
The high-risk factors were 100% sensitive for predicting need for neurological intervention and would require only 32% of patients to undergo CT.
The medium-risk factors were 98.4% sensitive and 49.6% specific for predicting clinically important brain injury, and would require only 54% of patients to undergo CT.
Stiell IG, Wells GA, Vandemheen, K., et al. The Canadian CT Head Rule for patients with minor head injury. Lancet. 2001;357: 1391-1396.
CCHR
Canadian CT Head Rules
Computed tomography is required for adults > 16 years with minor head injury (a history of a GCS score of 13 to 15 with witnessed LOC, amnesia, or confusion) and any one of the following findings:
1. Glasgow Coma Scale score < 15 at 2 hours after injury
2. Suspected open or depressed skull fracture
3. Any sign of basilar skull fracture
4. Two or more episodes of vomiting
5. 65 years or older
6. Amnesia before impact of 30 or more minutes
7. Dangerous mechanism
Results:
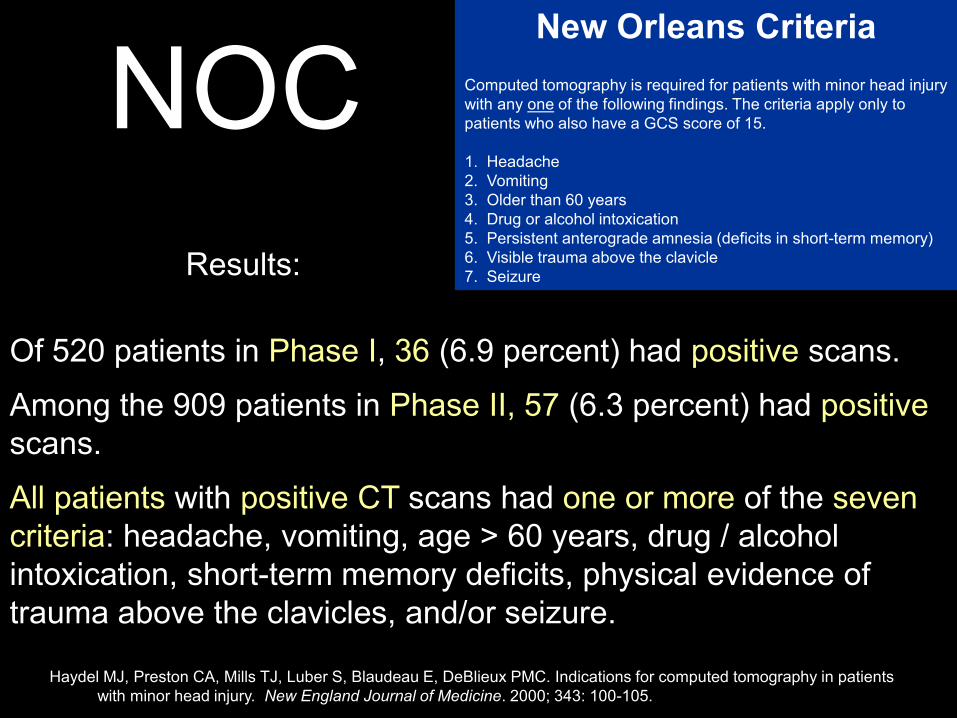
New Orleans Criteria Computed tomography is required for patients with minor head injury with any one of the following findings. The criteria apply only to patients who also have a GCS score of 15. 1. Headache 2. Vomiting 3. Older than 60 years 4. Drug or alcohol intoxication 5. Persistent anterograde amnesia (deficits in short-term memory) 6. Visible trauma above the clavicle 7. Seizure
NOC
Single center study at a large, inner-city, level 1 trauma center from 1997 to 1999.
Recursive Partitioning Analysis - Phase I: n = 520 consecutive patients (ages 3 – 97 years, mean age 36) with a GCS score 15 after minor head injury.
Prosective Validation - Phase II: n = 909 consecutive patients (ages 3 – 94 years, mean age 36) with a GCS score 15 after minor head injury.
Originally published in 2000 in NEJM.
Haydel MJ, Preston CA, Mills TJ, Luber S, Blaudeau E, DeBlieux PMC. Indications for computed tomography in patients with minor head injury. New England Journal of Medicine. 2000; 343: 100-105.
NOC
Of 520 patients in Phase I, 36 (6.9 percent) had positive scans.
Among the 909 patients in Phase II, 57 (6.3 percent) had positive scans.
All patients with positive CT scans had one or more of the seven criteria: headache, vomiting, age > 60 years, drug / alcohol intoxication, short-term memory deficits, physical evidence of trauma above the clavicles, and/or seizure.
Results:
Haydel MJ, Preston CA, Mills TJ, Luber S, Blaudeau E, DeBlieux PMC. Indications for computed tomography in patients with minor head injury. New England Journal of Medicine. 2000; 343: 100-105.
New Orleans Criteria Computed tomography is required for patients with minor head injury with any one of the following findings. The criteria apply only to patients who also have a GCS score of 15. 1. Headache 2. Vomiting 3. Older than 60 years 4. Drug or alcohol intoxication 5. Persistent anterograde amnesia (deficits in short-term memory) 6. Visible trauma above the clavicle 7. Seizure
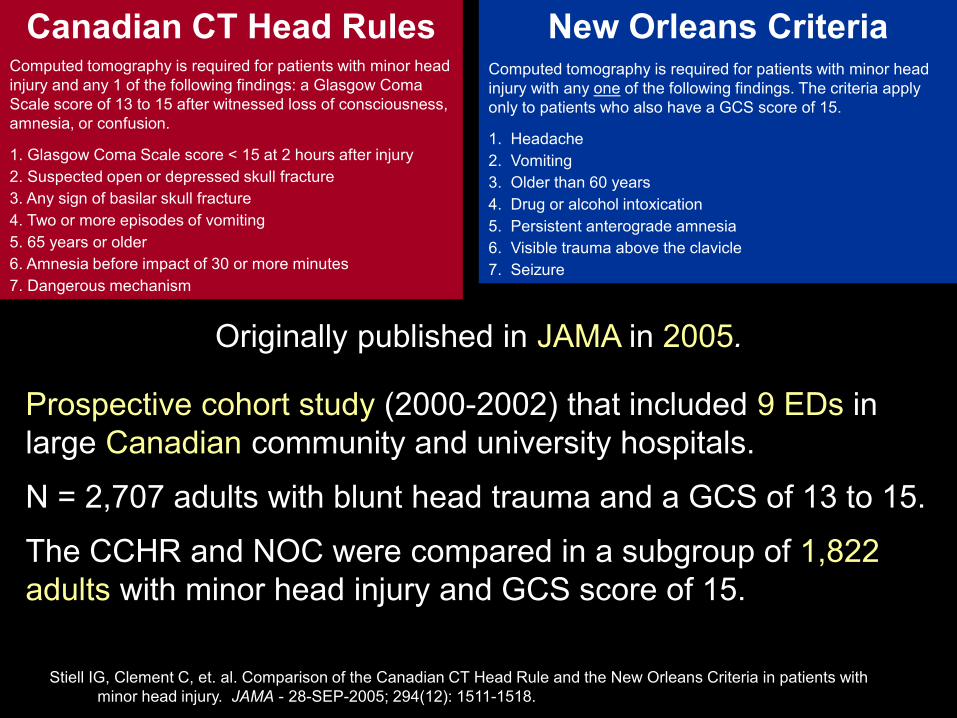
Prospective cohort study (2000-2002) that included 9 EDs in large Canadian community and university hospitals.
N = 2,707 adults with blunt head trauma and a GCS of 13 to 15.
The CCHR and NOC were compared in a subgroup of 1,822 adults with minor head injury and GCS score of 15.
Stiell IG, Clement C, et. al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in patients with minor head injury. JAMA - 28-SEP-2005; 294(12): 1511-1518.
New Orleans Criteria
Computed tomography is required for patients with minor head injury with any one of the following findings. The criteria apply only to patients who also have a GCS score of 15.
1. Headache
2. Vomiting
3. Older than 60 years
4. Drug or alcohol intoxication
5. Persistent anterograde amnesia
6. Visible trauma above the clavicle
7. Seizure
Canadian CT Head Rules
Computed tomography is required for patients with minor head injury and any 1 of the following findings: a Glasgow Coma Scale score of 13 to 15 after witnessed loss of consciousness, amnesia, or confusion.
1. Glasgow Coma Scale score < 15 at 2 hours after injury
2. Suspected open or depressed skull fracture
3. Any sign of basilar skull fracture
4. Two or more episodes of vomiting
5. 65 years or older
6. Amnesia before impact of 30 or more minutes
7. Dangerous mechanism
Originally published in JAMA in 2005.
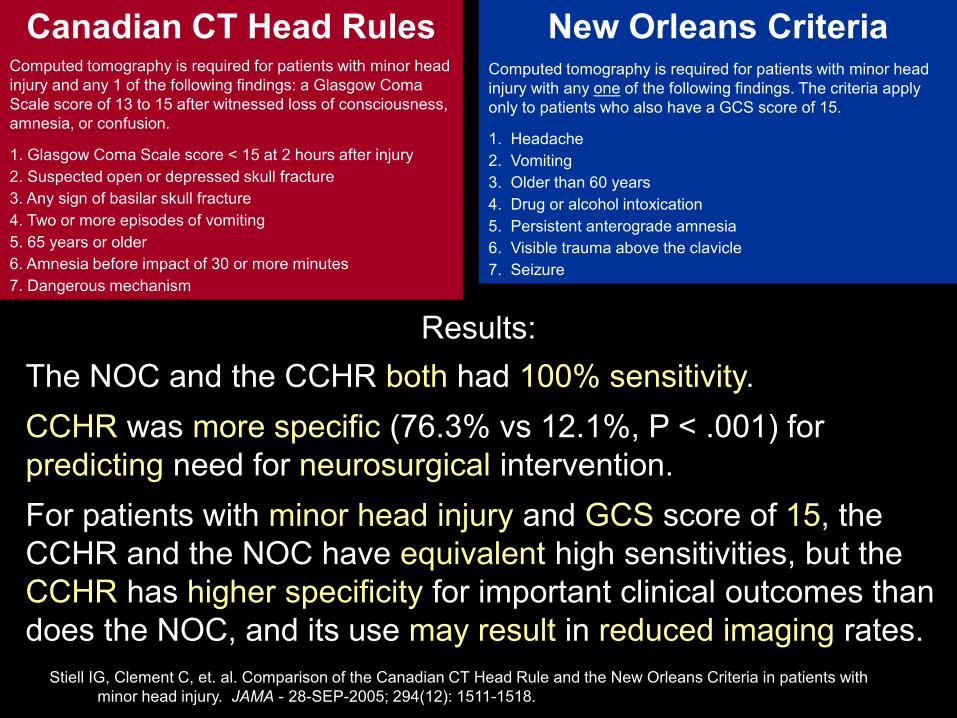
The NOC and the CCHR both had 100% sensitivity.
CCHR was more specific (76.3% vs 12.1%, P < .001) for predicting need for neurosurgical intervention.
For patients with minor head injury and GCS score of 15, the CCHR and the NOC have equivalent high sensitivities, but the CCHR has higher specificity for important clinical outcomes than does the NOC, and its use may result in reduced imaging rates.
Stiell IG, Clement C, et. al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in patients with minor head injury. JAMA - 28-SEP-2005; 294(12): 1511-1518.
New Orleans Criteria
Computed tomography is required for patients with minor head injury with any one of the following findings. The criteria apply only to patients who also have a GCS score of 15.
1. Headache
2. Vomiting
3. Older than 60 years
4. Drug or alcohol intoxication
5. Persistent anterograde amnesia
6. Visible trauma above the clavicle
7. Seizure
Canadian CT Head Rules
Computed tomography is required for patients with minor head injury and any 1 of the following findings: a Glasgow Coma Scale score of 13 to 15 after witnessed loss of consciousness, amnesia, or confusion.
1. Glasgow Coma Scale score < 15 at 2 hours after injury
2. Suspected open or depressed skull fracture
3. Any sign of basilar skull fracture
4. Two or more episodes of vomiting
5. 65 years or older
6. Amnesia before impact of 30 or more minutes
7. Dangerous mechanism
Results:
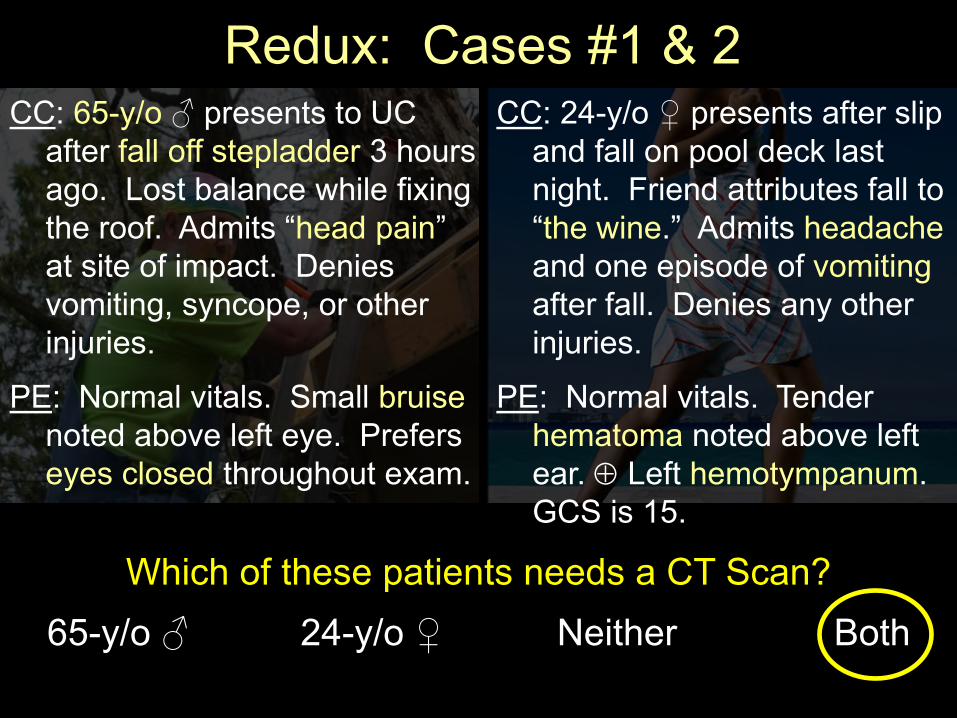
Redux: Cases #1 & 2 CC: 65-y/o ♂ presents to UC
after fall off stepladder 3 hours ago. Lost balance while fixing the roof. Admits “head pain” at site of impact. Denies vomiting, syncope, or other injuries.
PE: Normal vitals. Small bruise noted above left eye. Prefers eyes closed throughout exam.
Which of these patients needs a CT Scan?
65-y/o ♂ 24-y/o ♀ Neither Both
CC: 24-y/o ♀ presents after slip and fall on pool deck last night. Friend attributes fall to “the wine.” Admits headache and one episode of vomiting after fall. Denies any other injuries.
PE: Normal vitals. Tender hematoma noted above left ear. Left hemotympanum. GCS is 15.
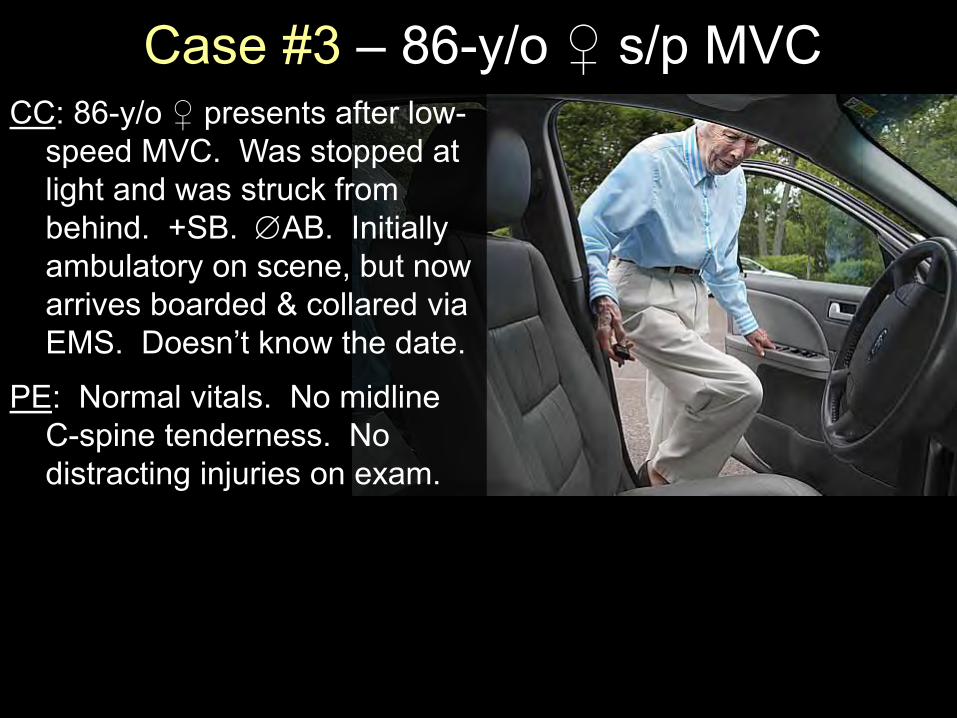
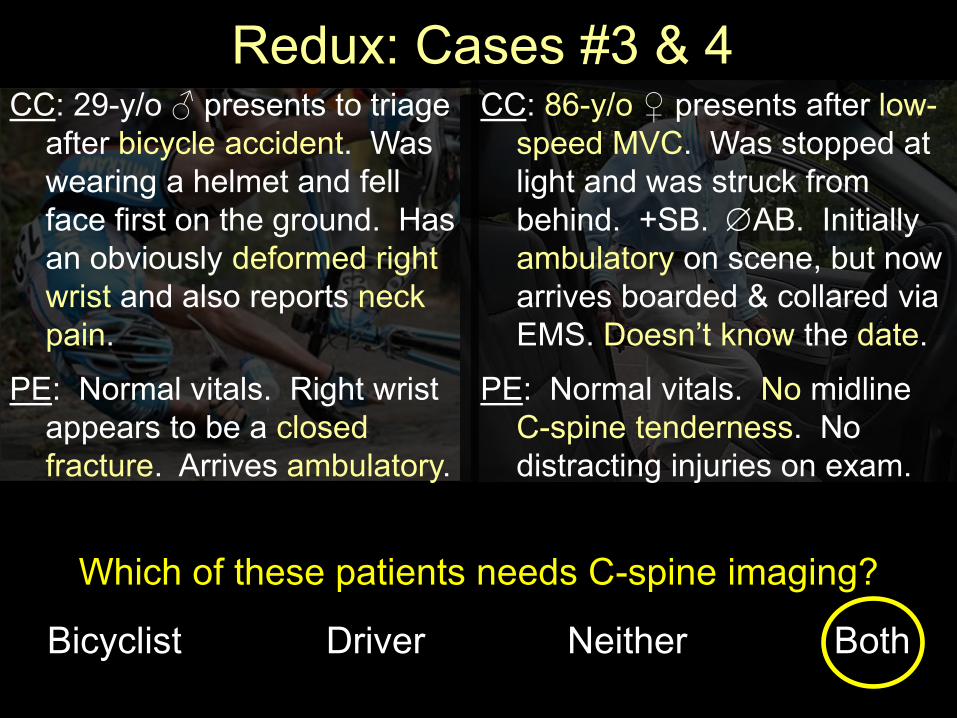
Case #3 – 86-y/o ♀ s/p MVC CC: 86-y/o ♀ presents after low-
speed MVC. Was stopped at light and was struck from behind. +SB. AB. Initially ambulatory on scene, but now arrives boarded & collared via EMS. Doesn’t know the date.
PE: Normal vitals. No midline C-spine tenderness. No distracting injuries on exam.
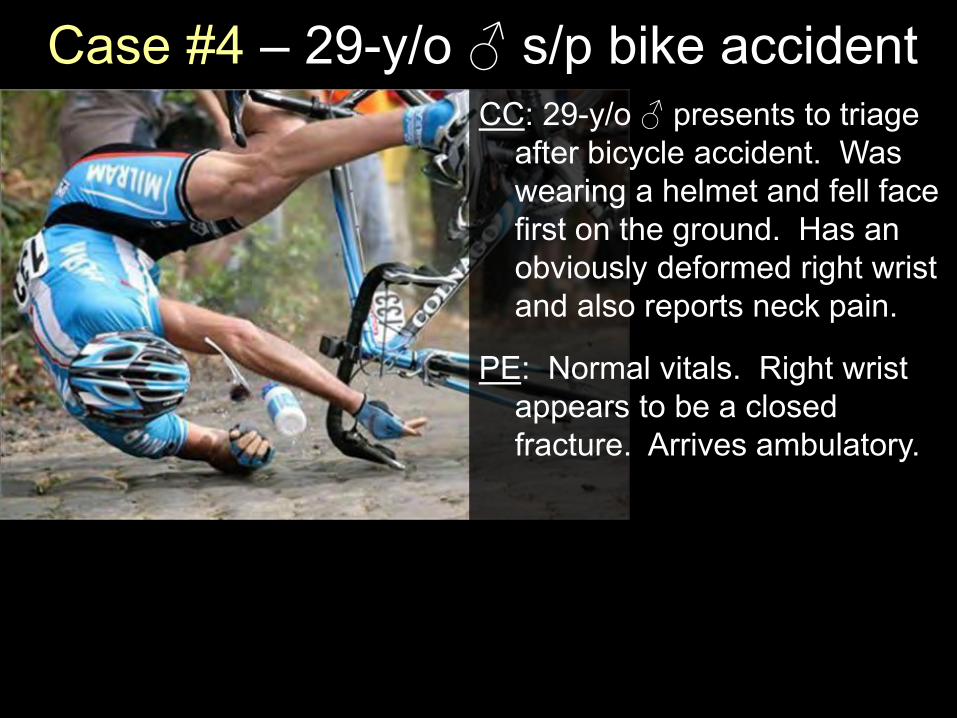
Case #4 – 29-y/o ♂ s/p bike accident CC: 29-y/o ♂ presents to triage
after bicycle accident. Was wearing a helmet and fell face first on the ground. Has an obviously deformed right wrist and also reports neck pain.
PE: Normal vitals. Right wrist appears to be a closed fracture. Arrives ambulatory.

Cases #3 & 4
Which of these patients needs C-spine imaging?
Bicyclist Driver Neither Both
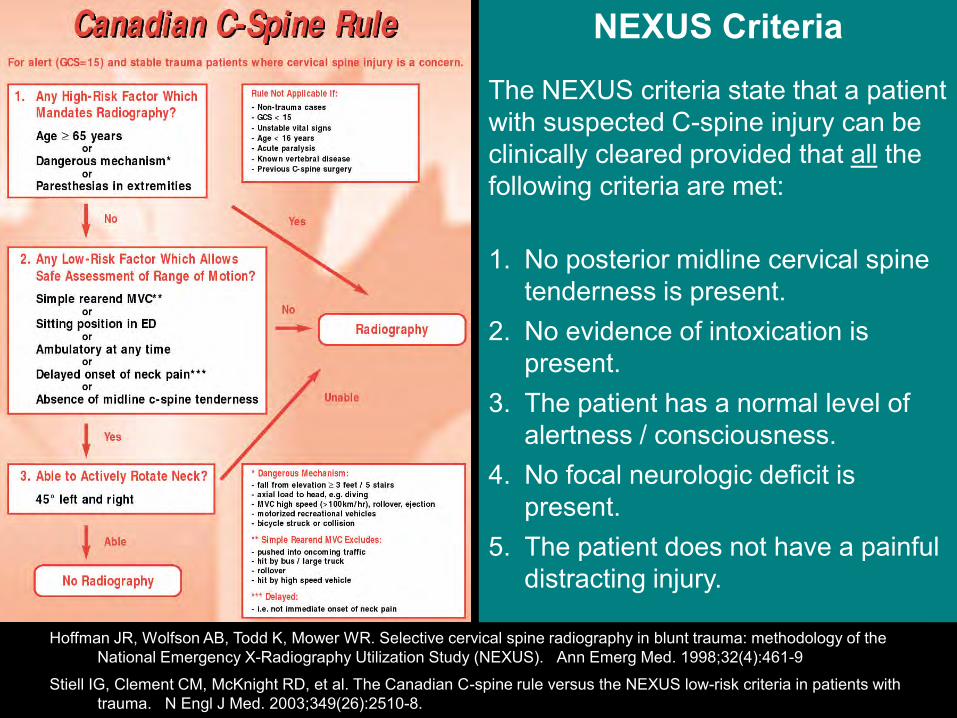
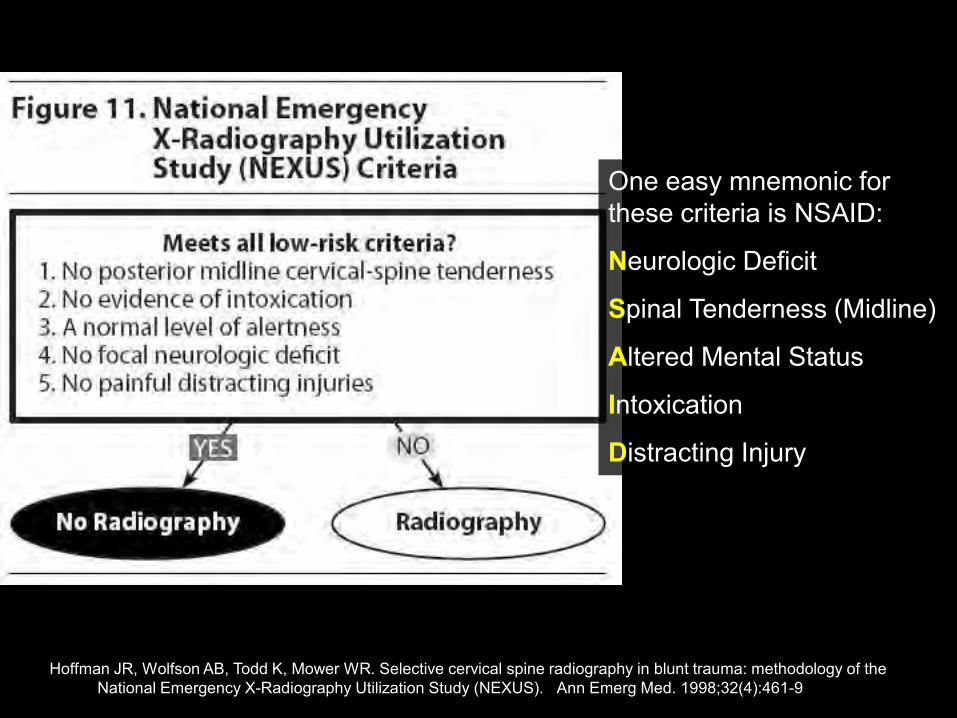
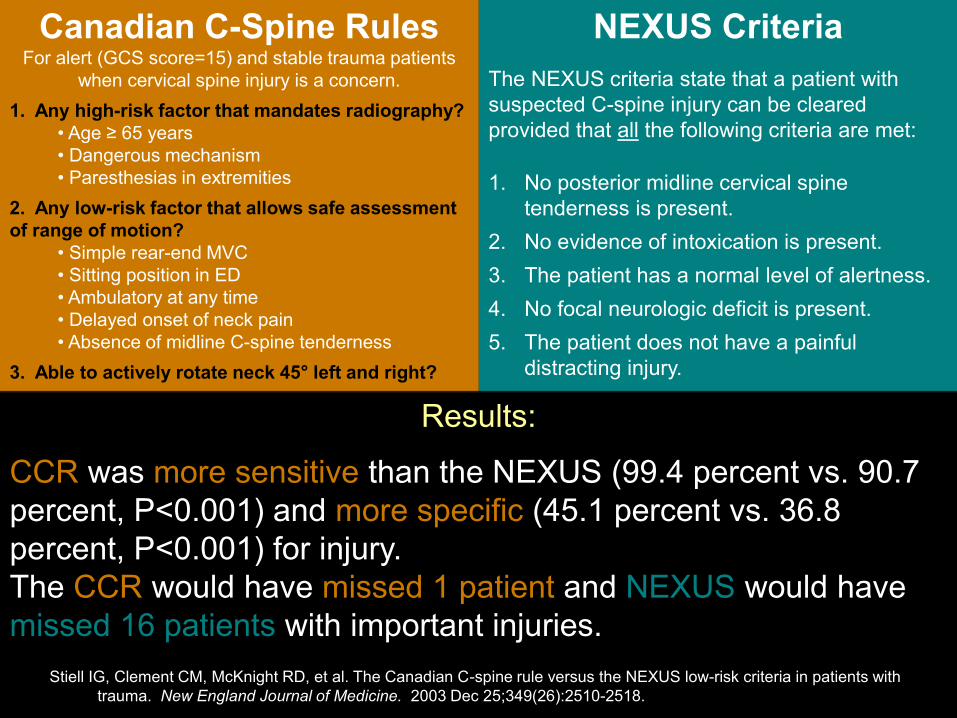
NEXUS Criteria
The NEXUS criteria state that a patient with suspected C-spine injury can be clinically cleared provided that all the following criteria are met:
1. No posterior midline cervical spine tenderness is present.
2. No evidence of intoxication is present.
3. The patient has a normal level of alertness / consciousness.
4. No focal neurologic deficit is present.
5. The patient does not have a painful distracting injury.
Hoffman JR, Wolfson AB, Todd K, Mower WR. Selective cervical spine radiography in blunt trauma: methodology of the National Emergency X-Radiography Utilization Study (NEXUS). Ann Emerg Med. 1998;32(4):461-9
Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med. 2003;349(26):2510-8.
Hoffman JR, Wolfson AB, Todd K, Mower WR. Selective cervical spine radiography in blunt trauma: methodology of the National Emergency X-Radiography Utilization Study (NEXUS). Ann Emerg Med. 1998;32(4):461-9
One easy mnemonic for these criteria is NSAID:
Neurologic Deficit
Spinal Tenderness (Midline)
Altered Mental Status
Intoxication
Distracting Injury
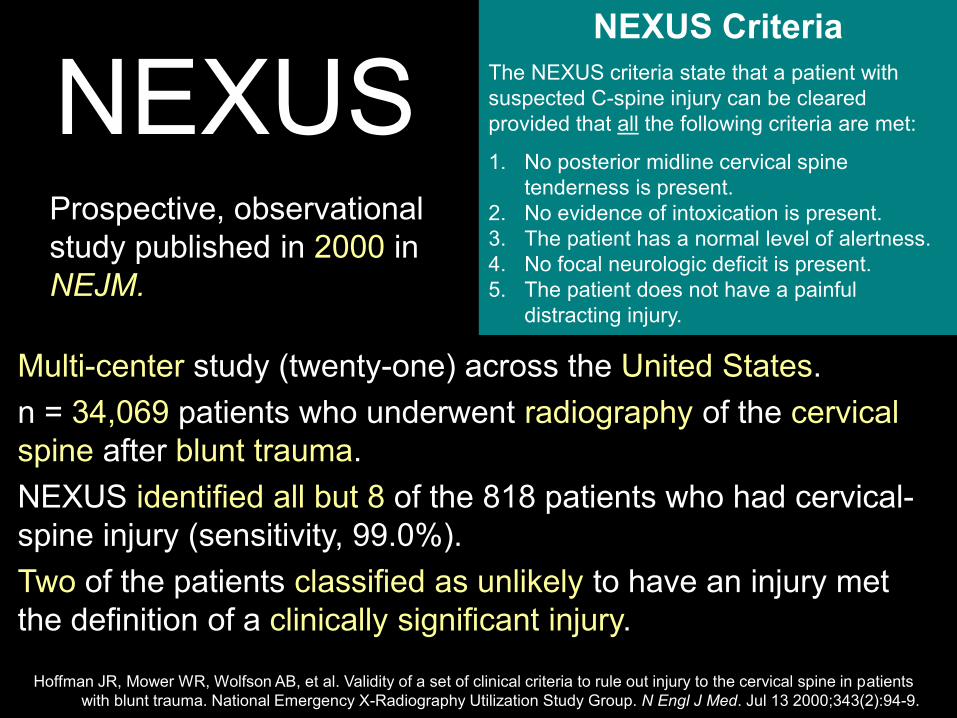
NEXUS
Multi-center study (twenty-one) across the United States.
n = 34,069 patients who underwent radiography of the cervical spine after blunt trauma.
NEXUS identified all but 8 of the 818 patients who had cervical-spine injury (sensitivity, 99.0%).
Two of the patients classified as unlikely to have an injury met the definition of a clinically significant injury.
Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Study Group. N Engl J Med. Jul 13 2000;343(2):94-9.
NEXUS Criteria
The NEXUS criteria state that a patient with suspected C-spine injury can be cleared provided that all the following criteria are met:
1. No posterior midline cervical spine tenderness is present.
2. No evidence of intoxication is present. 3. The patient has a normal level of alertness. 4. No focal neurologic deficit is present. 5. The patient does not have a painful
distracting injury.
Prospective, observational study published in 2000 in NEJM.
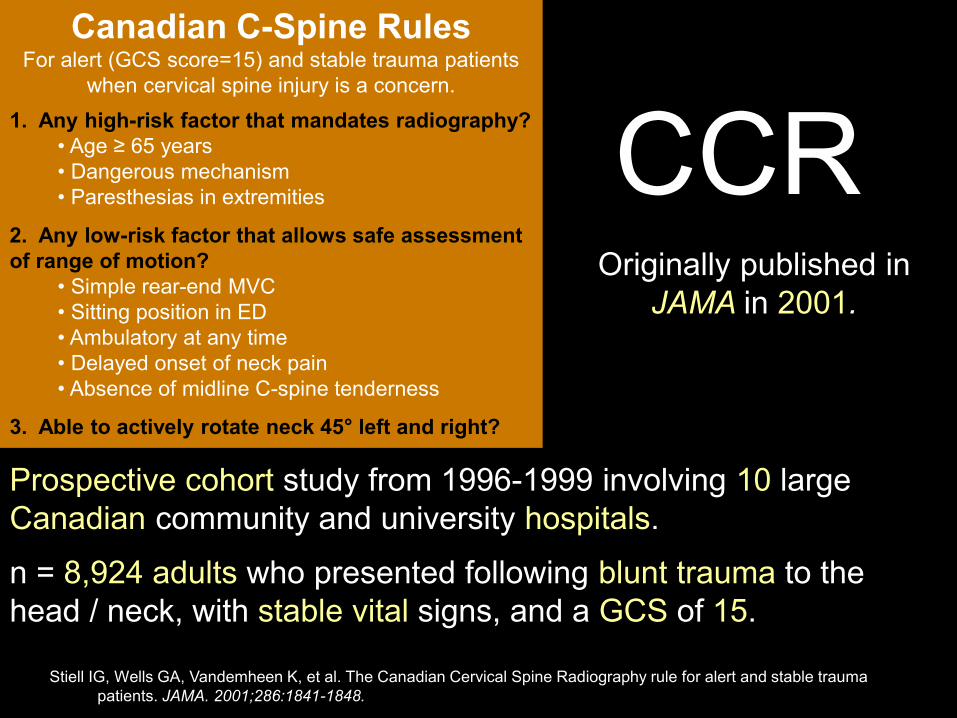
CCR
Prospective cohort study from 1996-1999 involving 10 large Canadian community and university hospitals.
n = 8,924 adults who presented following blunt trauma to the head / neck, with stable vital signs, and a GCS of 15.
Originally published in JAMA in 2001.
Stiell IG, Wells GA, Vandemheen K, et al. The Canadian Cervical Spine Radiography rule for alert and stable trauma patients. JAMA. 2001;286:1841-1848.
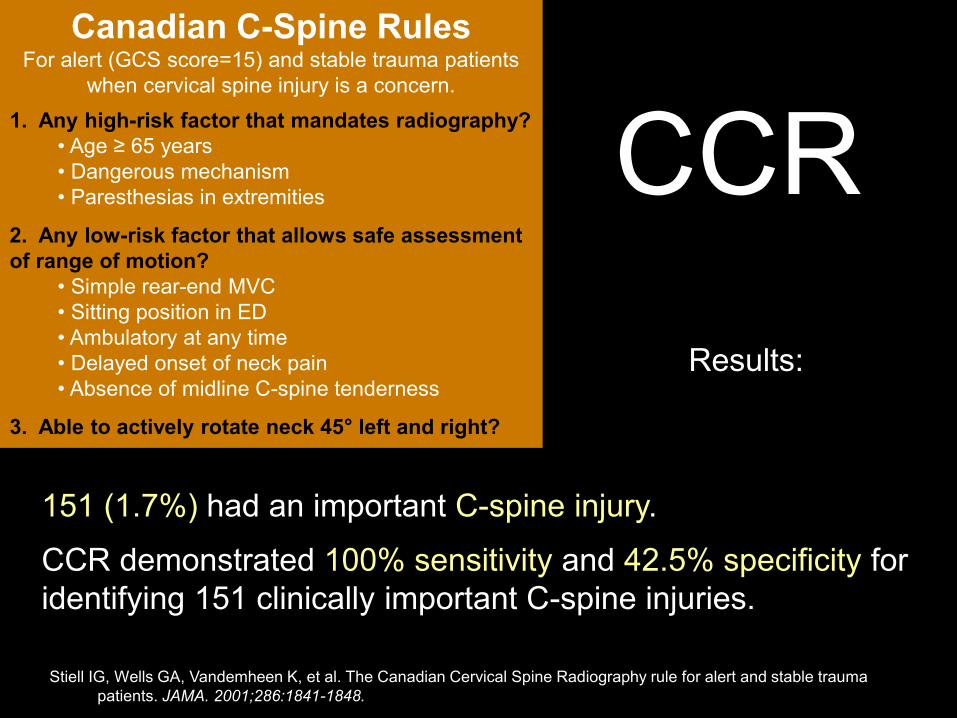
Canadian C-Spine Rules For alert (GCS score=15) and stable trauma patients
when cervical spine injury is a concern.
1. Any high-risk factor that mandates radiography?
• Age ≥ 65 years • Dangerous mechanism • Paresthesias in extremities
2. Any low-risk factor that allows safe assessment
of range of motion?
• Simple rear-end MVC • Sitting position in ED • Ambulatory at any time • Delayed onset of neck pain • Absence of midline C-spine tenderness
3. Able to actively rotate neck 45° left and right?
CCR
151 (1.7%) had an important C-spine injury.
CCR demonstrated 100% sensitivity and 42.5% specificity for identifying 151 clinically important C-spine injuries.
Results:
Stiell IG, Wells GA, Vandemheen K, et al. The Canadian Cervical Spine Radiography rule for alert and stable trauma patients. JAMA. 2001;286:1841-1848.
Canadian C-Spine Rules For alert (GCS score=15) and stable trauma patients
when cervical spine injury is a concern.
1. Any high-risk factor that mandates radiography?
• Age ≥ 65 years • Dangerous mechanism • Paresthesias in extremities
2. Any low-risk factor that allows safe assessment
of range of motion?
• Simple rear-end MVC • Sitting position in ED • Ambulatory at any time • Delayed onset of neck pain • Absence of midline C-spine tenderness
3. Able to actively rotate neck 45° left and right?
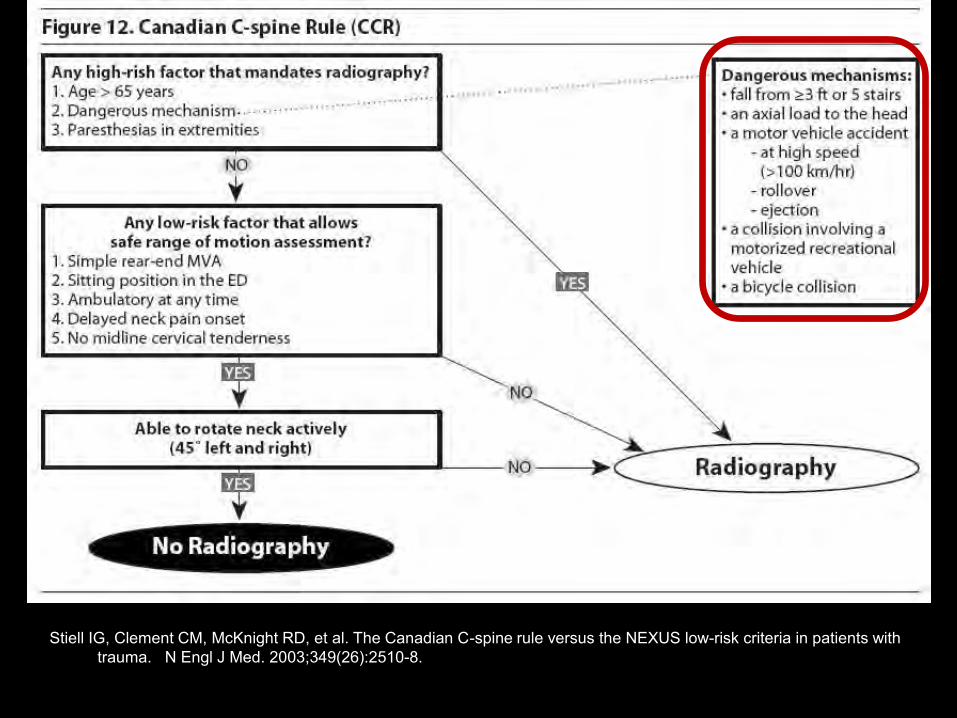
Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med. 2003;349(26):2510-8.
Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med. 2003;349(26):2510-8.

Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. New England Journal of Medicine. 2003 Dec 25;349(26):2510-2518.
Canadian C-Spine Rules For alert (GCS score=15) and stable trauma patients
when cervical spine injury is a concern.
1. Any high-risk factor that mandates radiography?
• Age ≥ 65 years • Dangerous mechanism • Paresthesias in extremities
2. Any low-risk factor that allows safe assessment
of range of motion?
• Simple rear-end MVC • Sitting position in ED • Ambulatory at any time • Delayed onset of neck pain • Absence of midline C-spine tenderness
3. Able to actively rotate neck 45° left and right?
NEXUS Criteria
The NEXUS criteria state that a patient with suspected C-spine injury can be cleared provided that all the following criteria are met:
1. No posterior midline cervical spine tenderness is present.
2. No evidence of intoxication is present.
3. The patient has a normal level of alertness.
4. No focal neurologic deficit is present.
5. The patient does not have a painful distracting injury.
Originally published in NEJM in 2003.
Prospective cohort study in 9 Canadian Emergency Departments.
N = 8,283 patients, 169 (2.0%) of which had clinically important cervical-spine injuries.
Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. New England Journal of Medicine. 2003 Dec 25;349(26):2510-2518.
Canadian C-Spine Rules For alert (GCS score=15) and stable trauma patients
when cervical spine injury is a concern.
1. Any high-risk factor that mandates radiography?
• Age ≥ 65 years • Dangerous mechanism • Paresthesias in extremities
2. Any low-risk factor that allows safe assessment
of range of motion?
• Simple rear-end MVC • Sitting position in ED • Ambulatory at any time • Delayed onset of neck pain • Absence of midline C-spine tenderness
3. Able to actively rotate neck 45° left and right?
NEXUS Criteria
The NEXUS criteria state that a patient with suspected C-spine injury can be cleared provided that all the following criteria are met:
1. No posterior midline cervical spine tenderness is present.
2. No evidence of intoxication is present.
3. The patient has a normal level of alertness.
4. No focal neurologic deficit is present.
5. The patient does not have a painful distracting injury.
Results:
CCR was more sensitive than the NEXUS (99.4 percent vs. 90.7 percent, P<0.001) and more specific (45.1 percent vs. 36.8 percent, P<0.001) for injury. The CCR would have missed 1 patient and NEXUS would have missed 16 patients with important injuries.
Redux: Cases #3 & 4
Which of these patients needs C-spine imaging?
Bicyclist Driver Neither Both
CC: 86-y/o ♀ presents after low-speed MVC. Was stopped at light and was struck from behind. +SB. AB. Initially ambulatory on scene, but now arrives boarded & collared via EMS. Doesn’t know the date.
PE: Normal vitals. No midline C-spine tenderness. No distracting injuries on exam.
CC: 29-y/o ♂ presents to triage after bicycle accident. Was wearing a helmet and fell face first on the ground. Has an obviously deformed right wrist and also reports neck pain.
PE: Normal vitals. Right wrist appears to be a closed fracture. Arrives ambulatory.

Gestalt Psychology term meaning "unified whole"
Refers to theories of visual perception
Developed by German psychologists in the 1920s

More statistical definitions…
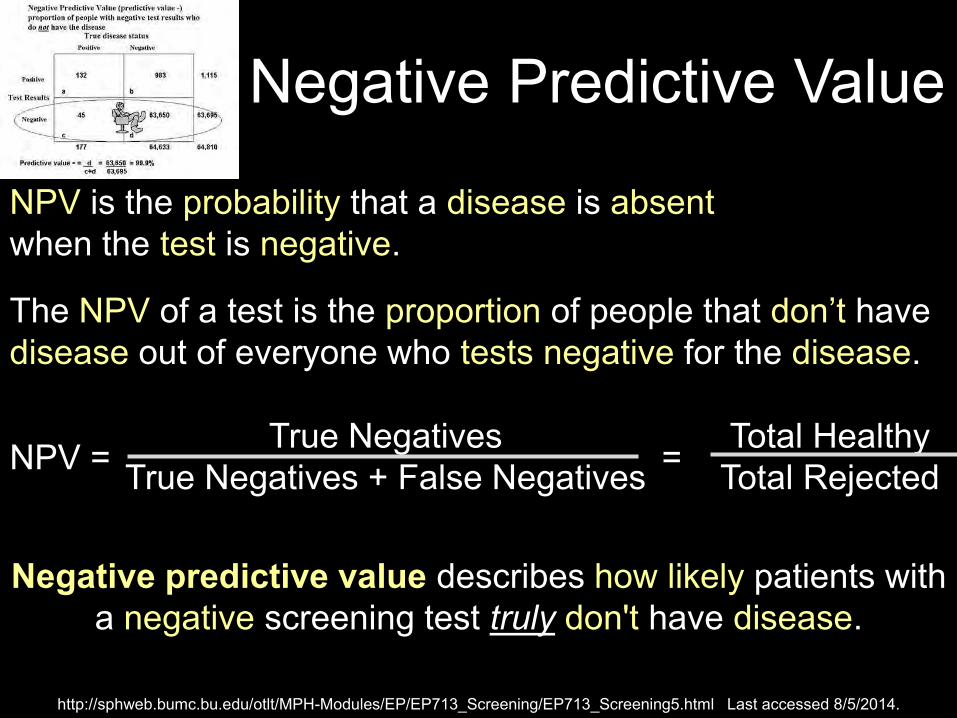
Negative Predictive Value
Negative predictive value describes how likely patients with a negative screening test truly don't have disease.
NPV = True Negatives
True Negatives + False Negatives =
Total Healthy Total Rejected
NPV is the probability that a disease is absent when the test is negative.
The NPV of a test is the proportion of people that don’t have disease out of everyone who tests negative for the disease.
http://sphweb.bumc.bu.edu/otlt/MPH-Modules/EP/EP713_Screening/EP713_Screening5.html Last accessed 8/5/2014.
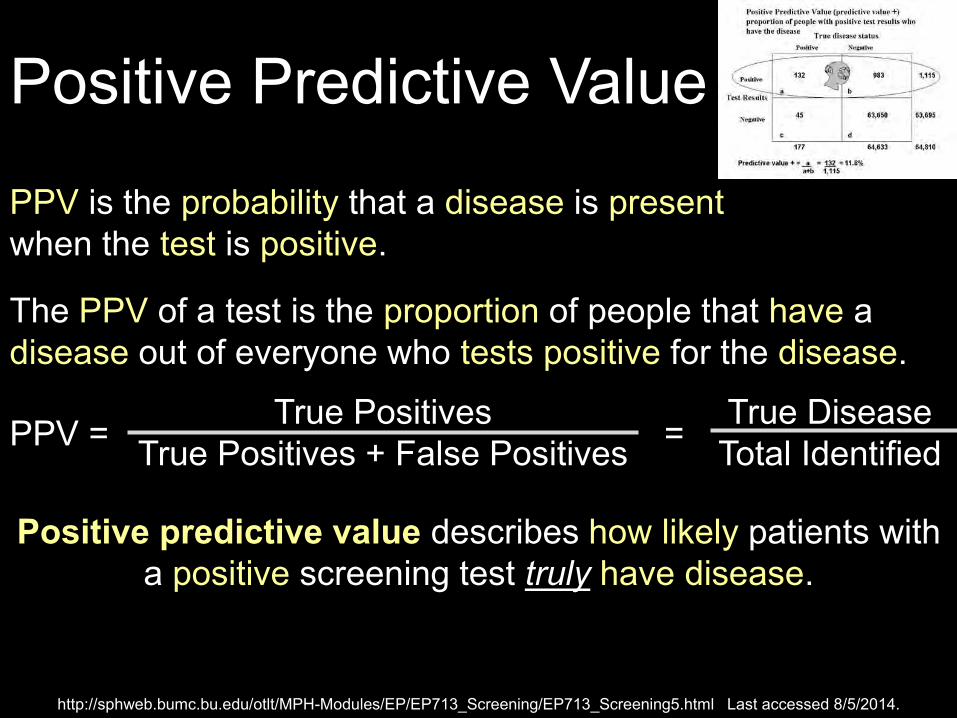
Positive Predictive Value
Positive predictive value describes how likely patients with a positive screening test truly have disease.
PPV = True Positives
True Positives + False Positives =
True Disease Total Identified
PPV is the probability that a disease is present when the test is positive.
The PPV of a test is the proportion of people that have a disease out of everyone who tests positive for the disease.
http://sphweb.bumc.bu.edu/otlt/MPH-Modules/EP/EP713_Screening/EP713_Screening5.html Last accessed 8/5/2014.
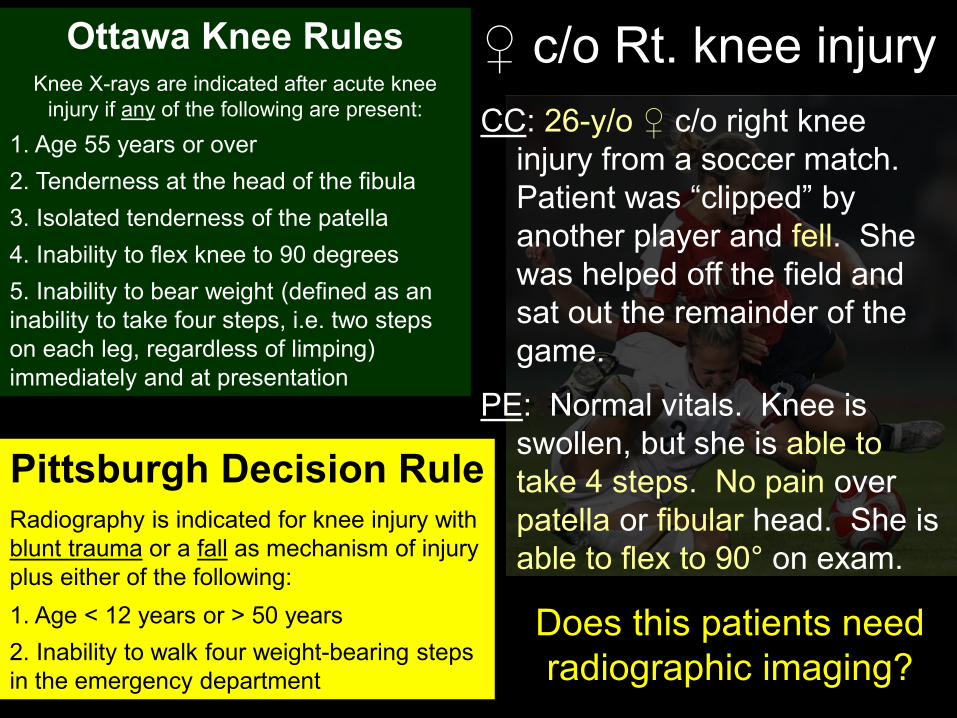
Case #5 – 26-y/o ♀ c/o Rt knee injury
CC: 26-y/o ♀ c/o right knee injury from a soccer match. Patient was “clipped” by another player and fell. She was helped off the field and sat out the remainder of the game.
PE: Normal vitals. Knee is swollen, but she is able to take 4 steps. No pain over patella or fibular head. She is able to flex to 90° on exam.
Does this patient need radiographic imaging?
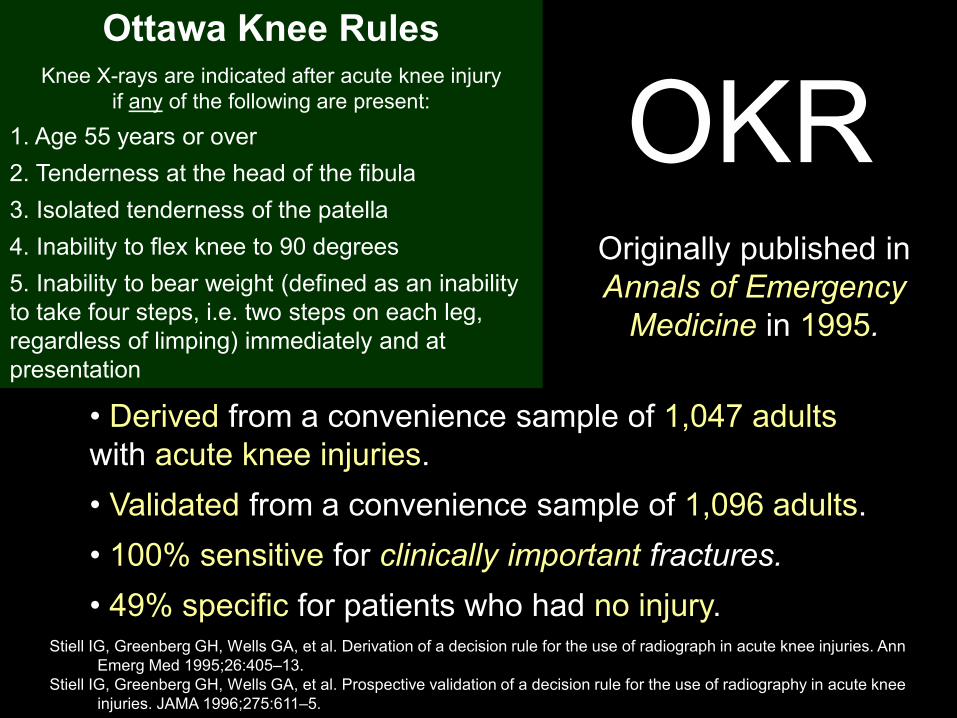
OKR
• Derived from a convenience sample of 1,047 adults with acute knee injuries.
• Validated from a convenience sample of 1,096 adults.
• 100% sensitive for clinically important fractures.
• 49% specific for patients who had no injury.
Originally published in Annals of Emergency
Medicine in 1995.
Stiell IG, Greenberg GH, Wells GA, et al. Derivation of a decision rule for the use of radiograph in acute knee injuries. Ann Emerg Med 1995;26:405–13.
Stiell IG, Greenberg GH, Wells GA, et al. Prospective validation of a decision rule for the use of radiography in acute knee injuries. JAMA 1996;275:611–5.
Ottawa Knee Rules
Knee X-rays are indicated after acute knee injury if any of the following are present:
1. Age 55 years or over
2. Tenderness at the head of the fibula
3. Isolated tenderness of the patella
4. Inability to flex knee to 90 degrees
5. Inability to bear weight (defined as an inability to take four steps, i.e. two steps on each leg, regardless of limping) immediately and at presentation
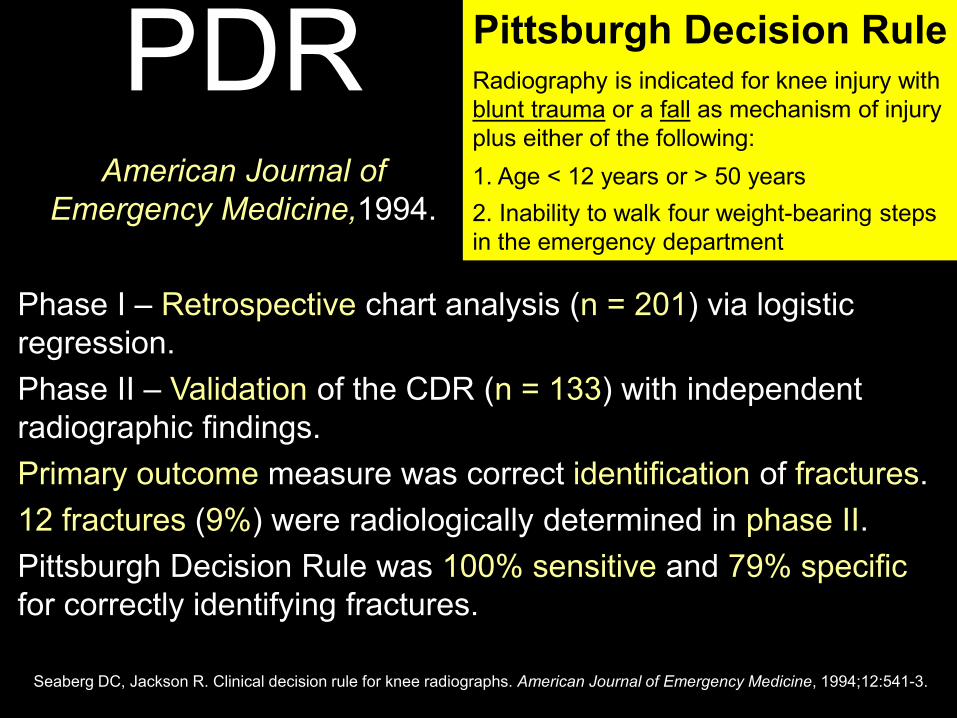
PDR
Phase I – Retrospective chart analysis (n = 201) via logistic regression.
Phase II – Validation of the CDR (n = 133) with independent radiographic findings.
Primary outcome measure was correct identification of fractures.
12 fractures (9%) were radiologically determined in phase II.
Pittsburgh Decision Rule was 100% sensitive and 79% specific for correctly identifying fractures.
Seaberg DC, Jackson R. Clinical decision rule for knee radiographs. American Journal of Emergency Medicine, 1994;12:541-3.
Pittsburgh Decision Rule
Radiography is indicated for knee injury with blunt trauma or a fall as mechanism of injury plus either of the following:
1. Age < 12 years or > 50 years
2. Inability to walk four weight-bearing steps in the emergency department
American Journal of
Emergency Medicine,1994.
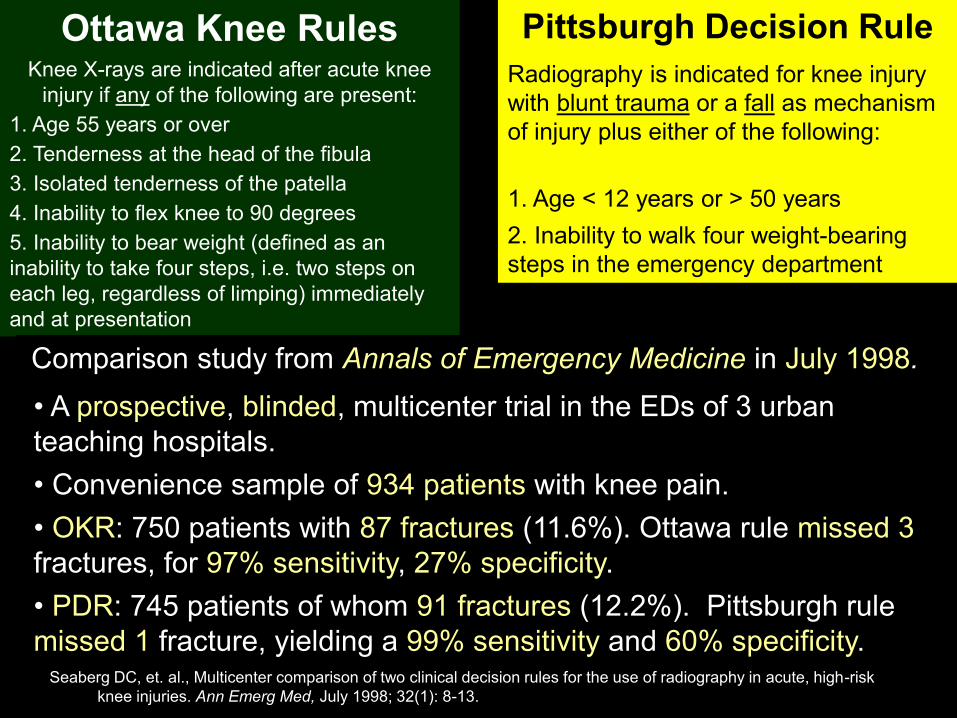
• A prospective, blinded, multicenter trial in the EDs of 3 urban teaching hospitals.
• Convenience sample of 934 patients with knee pain.
• OKR: 750 patients with 87 fractures (11.6%). Ottawa rule missed 3 fractures, for 97% sensitivity, 27% specificity.
• PDR: 745 patients of whom 91 fractures (12.2%). Pittsburgh rule missed 1 fracture, yielding a 99% sensitivity and 60% specificity.
Seaberg DC, et. al., Multicenter comparison of two clinical decision rules for the use of radiography in acute, high-risk knee injuries. Ann Emerg Med, July 1998; 32(1): 8-13.
Ottawa Knee Rules
Knee X-rays are indicated after acute knee injury if any of the following are present:
1. Age 55 years or over
2. Tenderness at the head of the fibula
3. Isolated tenderness of the patella
4. Inability to flex knee to 90 degrees
5. Inability to bear weight (defined as an inability to take four steps, i.e. two steps on each leg, regardless of limping) immediately and at presentation
Pittsburgh Decision Rule
Radiography is indicated for knee injury with blunt trauma or a fall as mechanism of injury plus either of the following:
1. Age < 12 years or > 50 years
2. Inability to walk four weight-bearing steps in the emergency department
Comparison study from Annals of Emergency Medicine in July 1998.
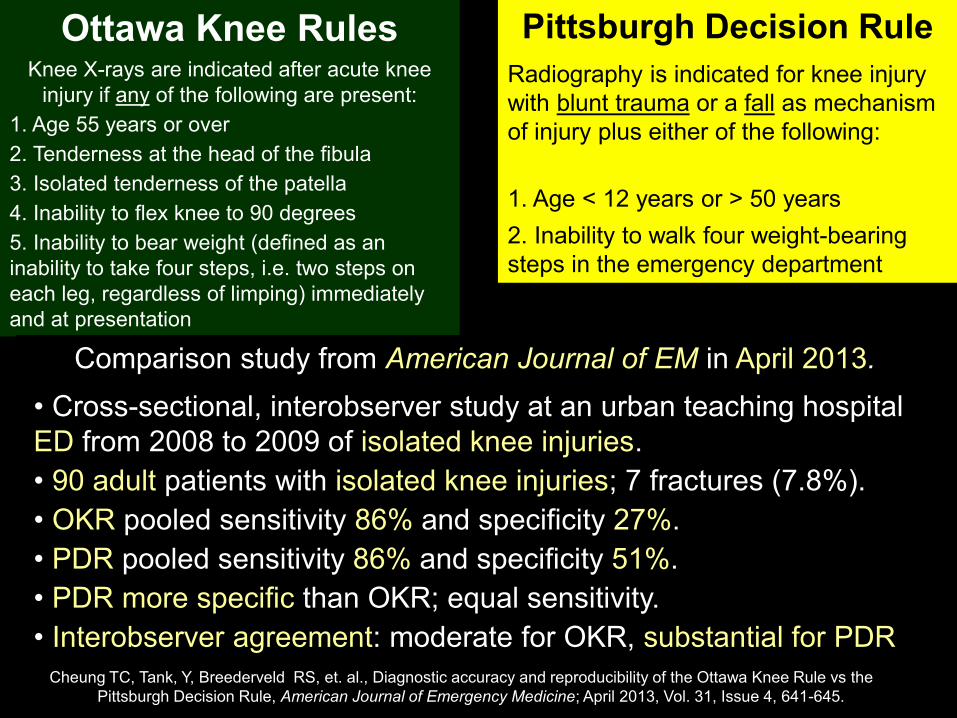
• Cross-sectional, interobserver study at an urban teaching hospital ED from 2008 to 2009 of isolated knee injuries.
• 90 adult patients with isolated knee injuries; 7 fractures (7.8%).
• OKR pooled sensitivity 86% and specificity 27%.
• PDR pooled sensitivity 86% and specificity 51%.
• PDR more specific than OKR; equal sensitivity.
• Interobserver agreement: moderate for OKR, substantial for PDR Cheung TC, Tank, Y, Breederveld RS, et. al., Diagnostic accuracy and reproducibility of the Ottawa Knee Rule vs the
Pittsburgh Decision Rule, American Journal of Emergency Medicine; April 2013, Vol. 31, Issue 4, 641-645.
Ottawa Knee Rules
Knee X-rays are indicated after acute knee injury if any of the following are present:
1. Age 55 years or over
2. Tenderness at the head of the fibula
3. Isolated tenderness of the patella
4. Inability to flex knee to 90 degrees
5. Inability to bear weight (defined as an inability to take four steps, i.e. two steps on each leg, regardless of limping) immediately and at presentation
Pittsburgh Decision Rule
Radiography is indicated for knee injury with blunt trauma or a fall as mechanism of injury plus either of the following:
1. Age < 12 years or > 50 years
2. Inability to walk four weight-bearing steps in the emergency department
Comparison study from American Journal of EM in April 2013.
No X-rays needed.
Cases #10 – 26-y/o ♀ c/o Rt. knee injury
Does this patients need radiographic imaging?
CC: 26-y/o ♀ c/o right knee injury from a soccer match. Patient was “clipped” by another player and fell. She was helped off the field and sat out the remainder of the game.
PE: Normal vitals. Knee is swollen, but she is able to take 4 steps. No pain over patella or fibular head. She is able to flex to 90° on exam.
Pittsburgh Decision Rule
Radiography is indicated for knee injury with blunt trauma or a fall as mechanism of injury plus either of the following:
1. Age < 12 years or > 50 years
2. Inability to walk four weight-bearing steps in the emergency department
Ottawa Knee Rules
Knee X-rays are indicated after acute knee injury if any of the following are present:
1. Age 55 years or over
2. Tenderness at the head of the fibula
3. Isolated tenderness of the patella
4. Inability to flex knee to 90 degrees
5. Inability to bear weight (defined as an inability to take four steps, i.e. two steps on each leg, regardless of limping) immediately and at presentation
Case #6 – 28-y/o ♂ c/o Lt. ankle injury
CC: 28-y/o ♂ presents for a left ankle injury. “Rolled” his ankle while playing basketball. He was briefly weight-bearing initially, but has been non-weight bearing for the last hour.
PE: Normal vitals. Left ankle is swollen with bruising. Bony tenderness along lateral malleolus. Arrives via wheelchair.
Does this patients need radiographic imaging?
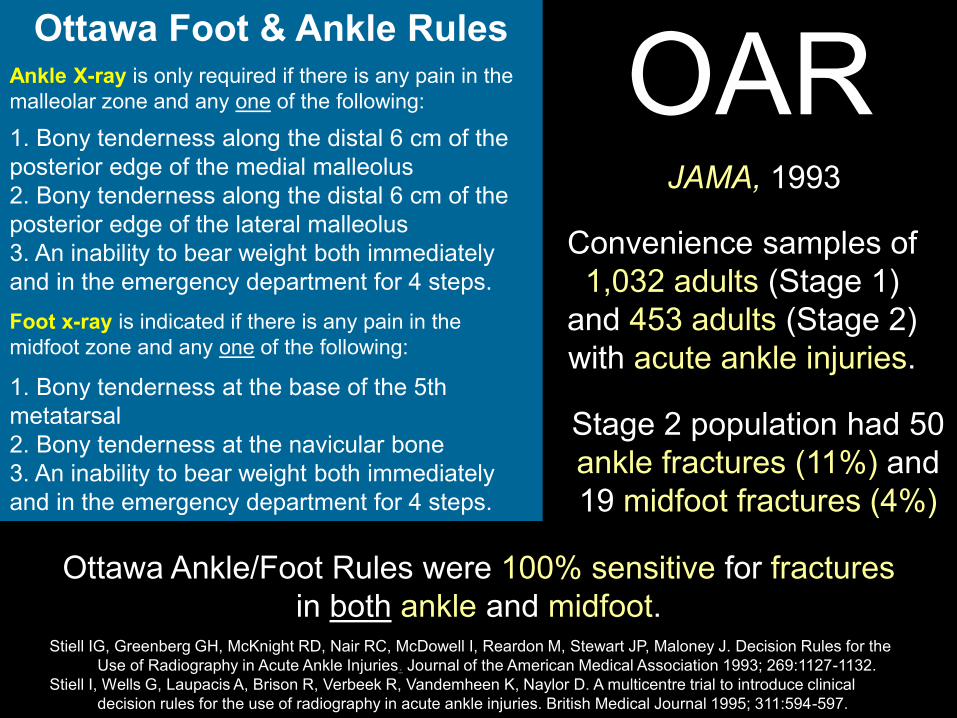
OAR Convenience samples of
1,032 adults (Stage 1) and 453 adults (Stage 2) with acute ankle injuries.
JAMA, 1993
Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Reardon M, Stewart JP, Maloney J. Decision Rules for the Use of Radiography in Acute Ankle Injuries. Journal of the American Medical Association 1993; 269:1127-1132.
Stiell I, Wells G, Laupacis A, Brison R, Verbeek R, Vandemheen K, Naylor D. A multicentre trial to introduce clinical decision rules for the use of radiography in acute ankle injuries. British Medical Journal 1995; 311:594-597.
Ottawa Foot & Ankle Rules
Ankle X-ray is only required if there is any pain in the malleolar zone and any one of the following:
1. Bony tenderness along the distal 6 cm of the posterior edge of the medial malleolus 2. Bony tenderness along the distal 6 cm of the posterior edge of the lateral malleolus 3. An inability to bear weight both immediately and in the emergency department for 4 steps.
Foot x-ray is indicated if there is any pain in the midfoot zone and any one of the following:
1. Bony tenderness at the base of the 5th metatarsal 2. Bony tenderness at the navicular bone 3. An inability to bear weight both immediately and in the emergency department for 4 steps.
Stage 2 population had 50 ankle fractures (11%) and 19 midfoot fractures (4%)
Ottawa Ankle/Foot Rules were 100% sensitive for fractures in both ankle and midfoot.
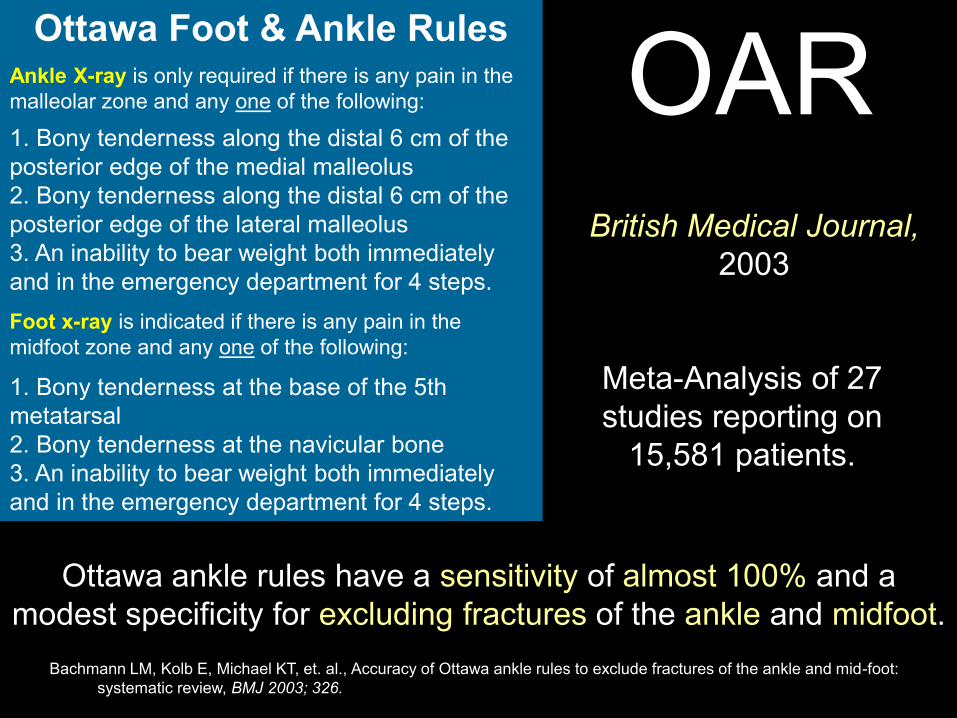
OAR
Meta-Analysis of 27 studies reporting on
15,581 patients.
British Medical Journal,
2003
Bachmann LM, Kolb E, Michael KT, et. al., Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review, BMJ 2003; 326.
Ottawa ankle rules have a sensitivity of almost 100% and a modest specificity for excluding fractures of the ankle and midfoot.
Ottawa Foot & Ankle Rules
Ankle X-ray is only required if there is any pain in the malleolar zone and any one of the following:
1. Bony tenderness along the distal 6 cm of the posterior edge of the medial malleolus 2. Bony tenderness along the distal 6 cm of the posterior edge of the lateral malleolus 3. An inability to bear weight both immediately and in the emergency department for 4 steps.
Foot x-ray is indicated if there is any pain in the midfoot zone and any one of the following:
1. Bony tenderness at the base of the 5th metatarsal 2. Bony tenderness at the navicular bone 3. An inability to bear weight both immediately and in the emergency department for 4 steps.
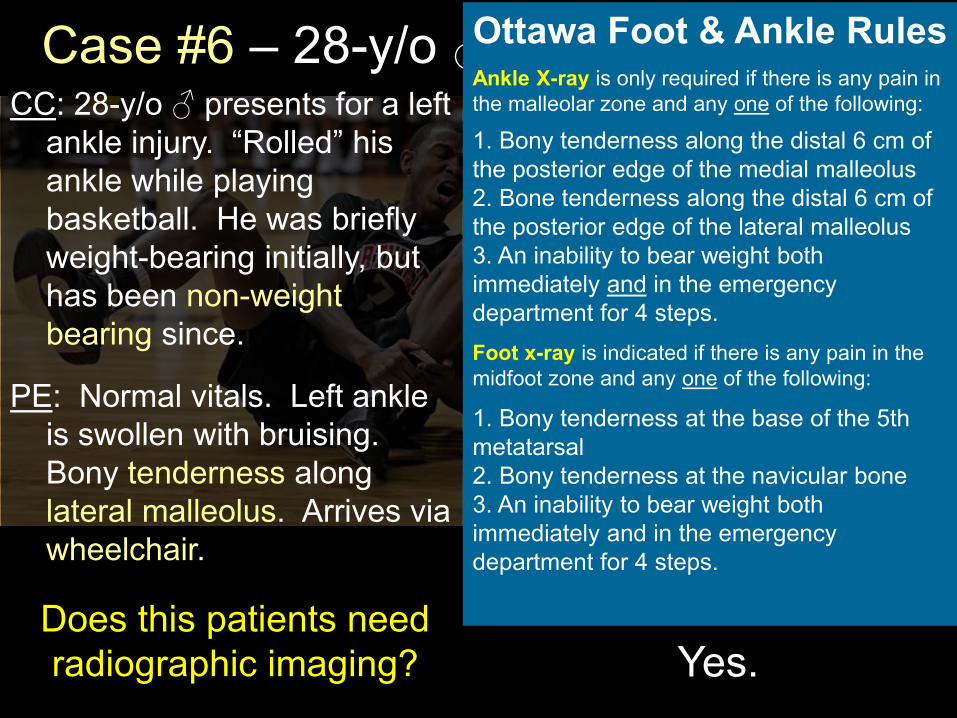
Case #6 – 28-y/o ♂ c/o Lt. ankle injury CC: 28-y/o ♂ presents for a left
ankle injury. “Rolled” his ankle while playing basketball. He was briefly weight-bearing initially, but has been non-weight bearing since.
PE: Normal vitals. Left ankle is swollen with bruising. Bony tenderness along lateral malleolus. Arrives via wheelchair.
Yes. Does this patients need radiographic imaging?
Ottawa Foot & Ankle Rules
Ankle X-ray is only required if there is any pain in the malleolar zone and any one of the following:
1. Bony tenderness along the distal 6 cm of the posterior edge of the medial malleolus 2. Bone tenderness along the distal 6 cm of the posterior edge of the lateral malleolus 3. An inability to bear weight both immediately and in the emergency department for 4 steps.
Foot x-ray is indicated if there is any pain in the midfoot zone and any one of the following:
1. Bony tenderness at the base of the 5th metatarsal 2. Bony tenderness at the navicular bone 3. An inability to bear weight both immediately and in the emergency department for 4 steps.

Summary – Adult & Pediatric CDRs
Canadian CT Head Rules
Computed tomography is required for adults > 16 years with minor head injury (a history of a GCS score of 13 to 15 with witnessed LOC, amnesia, or confusion) and any one of the following findings:
1. Glasgow Coma Scale score < 15 at 2 hours after injury
2. Suspected open or depressed skull fracture
3. Any sign of basilar skull fracture
4. Two or more episodes of vomiting
5. 65 years or older
6. Amnesia before impact of 30 or more minutes
7. Dangerous mechanism
New Orleans Criteria
Computed tomography is required for patients with minor head injury with any one of the following findings. The criteria apply only to patients who also have a GCS score of 15.
1. Headache
2. Vomiting
3. Older than 60 years
4. Drug or alcohol intoxication
5. Persistent anterograde amnesia
6. Visible trauma above the clavicle
7. Seizure
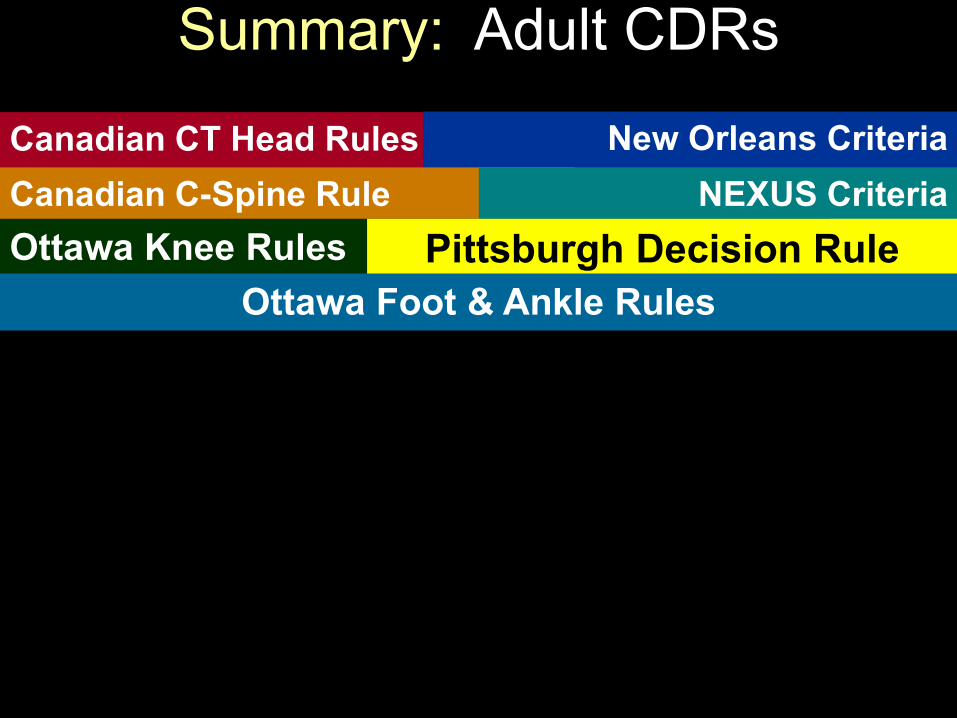
Summary: Adult CDRs
Canadian C-Spine Rule For alert (GCS score=15) and stable trauma patients when
cervical spine injury is a concern.
1. Any high-risk factor that mandates radiography?
• Age ≥ 65 years • Dangerous mechanism • Paresthesias in extremities
2. Any low-risk factor that allows safe assessment of
range of motion?
• Simple rear-end MVC • Sitting position in ED • Ambulatory at any time • Delayed onset of neck pain • Absence of midline C-spine tenderness
3. Able to actively rotate neck 45° left and right?
NEXUS Criteria
The NEXUS criteria state that a patient with suspected C-spine injury can be cleared provided that all the following criteria are met:
1. No posterior midline cervical spine tenderness is present.
2. No evidence of intoxication is present.
3. The patient has a normal level of alertness.
4. No focal neurologic deficit is present.
5. The patient does not have a painful distracting injury.
Ottawa Knee Rules
Knee X-rays are indicated after acute knee injury if any of the following are present:
1. Age 55 years or over
2. Tenderness at the head of the fibula
3. Isolated tenderness of the patella
4. Inability to flex knee to 90 degrees
5. Inability to bear weight (defined as an inability to take four steps, i.e. two steps on each leg, regardless of limping) immediately and at presentation.
Pittsburgh Decision Rule Radiography is indicated for knee injury with blunt trauma or a fall as mechanism of injury plus either of the following:
1. Age < 12 years or > 50 years
2. Inability to walk four weight-bearing steps in the emergency department
Ottawa Foot & Ankle Rules
Ankle X-ray is only required if there is any pain in the malleolar zone and any one of the following:
1. Bony tenderness along the distal 6 cm of the posterior edge of the medial malleolus 2. Bony tenderness along the distal 6 cm of the posterior edge of the lateral malleolus 3. An inability to bear weight both immediately and in the emergency department for 4 steps.
Foot x-ray is indicated if there is any pain in the midfoot zone and any one of the following:
1. Bony tenderness at the base of the 5th metatarsal 2. Bony tenderness at the navicular bone 3. An inability to bear weight both immediately and in the emergency department for 4 steps.

How am I supposed to remember all
this $#!+?
www.mdcalc.com
www.mdcalc.com
Adult Trauma Clinical Decision Rules:
Let’s play the quiz!
1. In evaluating a screening test’s ability to “rule out” a disease, what statistical characteristic is desirable?
A. High specificity
B. High sensitivity
C. Low specificity
D. Low sensitivity
B. High Sensitivity
(Snout “Sensitivity Rules it Out”)
Quiz – Adult Trauma CDRs
2. In evaluating a test’s ability to confirm or “rule in” a given disease, what statistical characteristic is desirable?
A. High specificity
B. Low specificity
C. High sensitivity
D. Low sensitivity
A. High specificity
(Spin “Specificity Rules it In”)
Quiz – Adult Trauma CDRs
3. The Canadian CT Head Rule (CCHR) and the New Orleans Criteria (NOC) are used to determine which group of patients does not need a CT Head?
A. Adults with a complaint of headache
B. Adults with severe head injuries
C. Children with a complaint of headache
D. Children with severe head injuries
E. Adults with minor head injuries
E. Adults with minor head injuries
Quiz – Adult Trauma CDRs
4. The Canadian C-Spine Rule (CCR) and the Nexus Criteria (NEXUS) are useful to determine no C-spine imaging in which group of patients?
A. Adults with non-traumatic neck pain
B. Children with suspected C-spine injury
C. Adults with paresthesias of hands or feet
D. Children with croup
E. Adults with suspected C-spine injury
E. Adults with suspected C-spine injury
Quiz – Adult Trauma CDRs
5. A test with a high negative predictive value (NPV) can be best be characterized by which of the following?
A. NPV is the probability that a disease is absent when the test is negative.
B. NPV describes how likely patients with a negative screening test truly don't have disease.
C. The NPV of a test is the proportion of people that don’t have disease out of everyone who tests negative for the disease.
D. None of the above
E. All of the above
E. All of the above
Quiz – Adult Trauma CDRs
6. A test with a high positive predictive value (PPV) can be best be characterized by which of the following?
A. PPV is the probability that a disease is present when the test is positive.
B. PPV describes how likely patients with a positive screening test truly have the disease.
C. The PPV of a test is the proportion of people that have disease out of everyone who tests positive for the disease.
D. None of the above
E. All of the above
E. All of the above
Quiz – Adult Trauma CDRs
7. The Ottawa Knee Rules (OKR), Pittsburg Decision Rules (PDR), and the Ottawa Foot & Ankle Rules (OAR) are used to determine the need for what in the injured patient?
A. X-rays
B. CT scans
C. EKG
D. Ultrasound for DVT
E. Splinting and/or crutches
A. X-rays
Quiz – Adult Trauma CDRs
8. In today’s lecture, what was the important take-home point in the discussion of Gestalt?
A. Gestalt is a psychology term meaning unified whole.
B. Gestalt refers to theories of visual perception.
C. It was described by psychologists in the 1920s.
D. Relying exclusively on Clinical Decision Rules is a “best practice” strategy.
E. If your clinical intuition tells you to more aggressively work-up or treat your patient, go with your instinct.
E. If your clinical intuition tells you to more aggressively work-up or treat your patient, go with your instinct.
Quiz – Adult Trauma CDRs
References
Kline JA, Courtney DM, Kabrhel C, Moore CL, Smithline HA, Plewa MC, Richman PB, O'Neil BJ, Nordenholz K. Prospective multicenter evaluation of the pulmonary embolism rule-out criteria. Journal of Thrombosis and Haemostasis. 2008 May;6(5):772-780.
Kuppermann N, Holmes JF, Dayan PS, et. al.; Pediatric Emergency Care Applied Research Network (PECARN). Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009 Oct 3;374(9696):1160-70.
McKay R , Shepherd J, The use of the clinical scoring system by Alvarado in the decision to perform computed tomography for acute appendicitis in the ED. Am J Emerg Med. 01-JUN-2007; 25(5): 489-493.
Meltzer AC, Brigitte MB, et. al., “Poor Sensitivity of a Modified Alvarado Score in Adults with Suspected Appendicitis,”. Annals of Emergency Medicine. August 2013; 62(2): 126-131.
Osmond MH, Klassen TP, Wells GA, et. al., CATCH: a clinical decision rule for the use of computed tomography in children with minor head injury. CMAJ, March 9, 2010 vol. 182 no. 4, 341-348 .
Perry JJ, Stiell IG, Sivilotti MLA, “High risk clinical characteristics for subarachnoid haemorrhage in patients with acute headache: prospective cohort study,” 2010, BMJ, 341: c5204: 1-8.
Perry JJ, Stiell IG, Sivilotti MLA, “Sensitivity of computed tomography performed within six hours of onset of headache for diagnosis of subarachnoid haemorrhage: prospective cohort study,” BMJ. 2011; 343: d4277: 1-10.
Quinn J, McDermott D, Stiell I, Kohn M, Wells G. Prospective validation of the San Francisco Syncope Rule to predict patients with serious outcomes. Ann Emerg Med. 2006;47(5):448–454.
Reed MJ, Newby DE, Coull AJ, Prescott RJ, Jacques KG, Gray AJ. The ROSE (Risk Stratification of Syncope in the Emergency Department) study. J Am Coll Cardiol. 2010;55(8):713–721.
Seaberg DC, Jackson R. Clinical decision rule for knee radiographs. American Journal of Emergency Medicine, 1994;12:541-3.
Stiell IG, Wells GA, Vandemheen K. et al. The Canadian CT Head Rule for patients with minor head injury. Lancet. 2001;3571391-1396.
Stiell IG, Greenberg GH, Wells GA, et al. Derivation of a decision rule for the use of radiograph in acute knee injuries. Ann Emerg Med 1995;26:405–13.
Stiell IG, Greenberg GH, Wells GA, et al. Prospective validation of a decision rule for the use of radiography in acute knee injuries. JAMA 1996;275:611–5.
Stiell IG, Wells GA, Hoag RH, et al. Implementation of the Ottawa knee rule for the use of radiography in acute knee injuries. JAMA 1997;278:2075–9.
Alvarado, A. “A practical score for the early diagnosis of acute appendicitis,” Annals of EM,1996:15:557-564.
Body R, et. al., “Do risk factors for chronic coronary heart disease help diagnose acute myocardial infarction in the Emergency Department?” Resuscitation, 2008; 79(1): 41-45.
Colivicchi F, Ammirati F, Melina D, et al.; OESIL (Osservatorio Epidemiologico sulla Sincope nel Lazio) Study Investigators. Development and prospective validation of a risk stratification system for patients with syncope in the emergency department: the OESIL risk score. Eur Heart J. 2003;24(9):811–891.
Dunning J, Daly JP, Lomas JP, et al. Derivation of the children's head injury algorithm for the prediction of important clinical events decision rule for head injury in children. Arch Dis Child 2006;91(11):885-91.
Gravel J, Hedrei P, Grimard G, Gouin S, Prospective Validation and Head-to-Head Comparison of 3 Ankle Rules in a Pediatric Population, Annals of Emergency medicine, Vol. 54, No. 4, October 2009, 534-540.
Haydel, MJ, Preston, CA, Mills, TJ, Luber, S, Blaudeau E, DeBlieux, PMC, Indications for computed tomography in patients with minor head injury. New England Journal of Medicine. 2000; 343: 100-105.
Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Study Group. N Engl J Med. Jul 13 2000;343(2):94-9.
Kline JA, Mitchell AM, Kabrhel C, Richman PB, Courtney DM. Clinical criteria to prevent unnecessary diagnostic testing in emergency department patients with suspected pulmonary embolism. Journal of Thrombosis and Haemostasis. 2004;2:1247-1255.
D. O.