adult bowel care guidelines - southern health nhs … · adult bowel care guidelines 1....
TRANSCRIPT

1 Adult Bowel Care Guidelines Version 1 July 2017
SH CP 205
Adult Bowel Care Guidelines
Version: 1
Summary: This guideline defines statements documenting the standards and expectations
for the clinical assessment and management of adult bowel dysfunction. The
guideline refers to procedures for clinical interventions and their indications.
Keywords: Bowel, constipation, rectal, rectum, DRE, DRF, DRS, stool, digestion, laxative,
enema, suppository, stoma, clinical, neurogenic, dysfunction, diet, fluid,
evacuation, faecal, incontinence, faeces, rectoanal, anal, impaction, irrigation
Target Audience: All SHFT Clinical Staff
Next Review Date: July 2019
Approved &
Ratified by:
Patient Safety Group Date of meeting: 19th June 2017
Date issued: July 2017
Author: Virginia Roberts, Clinical Trainer
Director: Sarah Constantine, Medical Director

2 Adult Bowel Care Guidelines Version 1 July 2017
Version Control
Change Record
Date Author Version Page Reason for Change
Jan 2017
Virginia Roberts 1 All New document Created
Reviewers/contributors
Name Position Version Reviewed & Date
Alison Wileman Continence Service Lead/Advanced Clinical Nurse Specialist – Continence
March 2017
Steve Coopey Head of Clinical Development March 2017
Sharon Guy Clinical Training Team Lead March 2017
Steve Mennear Senior Clinical Pharmacist April 2017
Katherine Steward Integrated Services Matron April 2017
Janet Brember NHS Portsmouth CCG July 2017
Catherine Mclean NHS West Hampshire CCG July 2017
Jason Peett NHS Southeast Hampshire CCG July 2017
Jackie Hunt Infection Control July 2017
Patient safety group committee Patient safety group committee July 2017
3 Adult Bowel Care Guidelines Version 1 July 2017
Quick Reference Guide This guideline defines statements documenting the standards and expectations for the clinical assessment and management of adult bowel dysfunction. The guideline refers to procedures for clinical interventions and their indications. The appendices contain the key documents and evidence supporting practice.

4 Adult Bowel Care Guidelines Version 1 July 2017
Contents
Section Title Page
1. Introduction
5
2. Purpose and Scope
5
3. Who does this guideline apply to?
5
4. Definitions
5
5. Duties and responsibilities
6
6. Bowel Care Statements
7
7. Training requirements
12
8. Monitoring compliance
12
9.
Guideline review 12
10.
Associated trust documents 12
11.
Supporting references 13
Appendix 1
Training needs analysis 14
Appendix 2
Equality Impact Assessment Tool 15
Appendix 3
Competencies 16
Appendix 4
Continence Assessment 20
Appendix 5
Bowel Care Pathway 23
Appendix 6a Appendix 6b
14 Day Food, Stool and Medication Diary Bristol Stool Chart
25 26
Appendix 7
Procedure for Digital Rectal Examination 27
Appendix 8
Procedure for Administration of Enemas and Suppositories 30
Appendix 9
Procedure for Digital Rectal Stimulation 33
Appendix 10
Procedure for Digital Removal of Faeces 35
Appendix 11 Appendix 11a
Trans-Anal Irrigation Suitability Flowchart / Referral form NBD Score
38 40
Appendix 12 Laxative treatment guidelines
41
Appendix 13 Management of lower bowel dysfunction, including DRE and DRF RCN Guidelines (2012)
42
Appendix 14 Guidelines for Management of Neurogenic Bowel dysfunction in individuals with Central Neurological conditions MASCIP (2012)
42

5 Adult Bowel Care Guidelines Version 1 July 2017
Adult Bowel Care Guidelines
1. Introduction
1.1. Bowel care is a fundamental area of patient care that is frequently overlooked yet it is of paramount importance for the quality of life of service users, many of whom may be reluctant to admit to bowel problems or to discuss such issues. (Royal College of Nursing (RCN) 2012) Robert Francis referred to continence as ‘this most basic of needs,’ his report highlighting significant concerns in this area of care (Department of Health, 2010).
1.2. Continence is the ability to voluntarily control emptying the bladder and bowels effectively in a socially acceptable and hygienic way. In the UK half a million people suffer with bowel control problems (Buckley & Lapitan 2009).
1.3. Bowel care may include assessments and interventions of an intimate nature that are to be carried out when there is a specific and adequate clinical indication.
1.4. It is the policy of Southern Health NHS Foundation Trust (SHFT) that bowel care will be carried
out in a safe and consistent manner according to SHFT procedures for bowel care (see Appendices 1 - 11).
1.5. When providing bowel care staff must ensure that they follow standard infection prevention precautions (as outlined in SHCP 19 Standard Precautions Procedure, Infection Prevention and Control Policy: Appendix 5) and practice excellent hand hygiene (as outlined in SHCP12 Hand Hygiene Procedure, Infection Prevention and Control Policy: Appendix 6).
2. Purpose and Scope 2.1. To ensure a high standard of bowel care, including assessment, treatment and
management including rectal interventions. 2.2. To ensure safe, competent practice by all clinicians undertaking bowel care and reduce risk
of complications associated with bowel management. 2.3. To standardise practice across Southern Health Foundation NHS Trust and the wider
healthcare community. 2.4. To ensure that all practice is evidence-based, relevant, appropriate and to minimise harm. 2.5. The guideline will apply to all staff undertaking bowel care for adults. 2.6. In order to carry out invasive bowel care all staff must attend relevant training, achieve
competency, and be working within their job description. 3. Who does this guideline apply to?
3.1. This guideline applies to all Health Care Professionals employed by SHFT required to undertake
bowel care for adults including: healthcare support workers, nurses, doctors and pharmacists.
4. Definitions 4.1 Bowel Care - Activities and interventions provided by health care professionals designed to
maintain bowel function including diet, medication, enema and suppository administration, Digital Rectal Examination, Digital Rectal Stimulation and Digital Removal of Faeces.

6 Adult Bowel Care Guidelines Version 1 July 2017
4.2 Bowel Dysfunction – constipation, faecal incontinence, disordered defaecation. 4.3 Digital Rectal Examination – examination of the rectum by inserting a gloved, lubricated finger
into the rectum. 4.4 Digital Removal of Faeces – removal of stool from the rectum using a gloved, lubricated finger. 4.5 Digital Rectal Stimulation – the insertion of a gloved, lubricated finger through the anus into the
rectum followed by a gentle circular motion of the finger for 20-30 seconds to stimulate reflex evacuation of stool.
4.6 Trans-Anal Irrigation – the facilitation of faecal evacuation from the bowel by introducing water
into the colon via the anus in a quantity sufficient to reach beyond the rectum. 4.7 Neurogenic Bowel Dysfunction – dysfunction of the colon due to loss of normal sensory and
motor control. 4.8 Autonomic Dysreflexia – (AD), also known as Hyperreflexia, is a potentially dangerous
complication of spinal cord injury resulting in acute, uncontrolled hypertension. Acute AD is a reaction of the autonomic nervous system to overstimulation.
5. Duties and responsibilities
5.1. The Quality and Safety Committee 5.2. Southern Health Foundation Trust has a responsibility to provide an effective and appropriate
service to their service users and appropriate training to their staff. The Quality and Safety Committee will monitor compliance with this guideline and provide an audit programme for implementation.
5.3. Clinical leads / Managers / Supervisors
Will ensure that sufficient priority is given to the successful implementation of the policy both
in wards and the community.
Will ensure that all staff attend appropriate training
Monitor compliance with current standards by all clinical staff
Ensure the availability, functioning and maintenance of all appropriate materials plus
equipment and that staff have appropriate training to use them.
Ensure clinical documentation in line with SHFT guideline
Ensuring that any change in practice recommendations are notified to all clinical staff.
Reviewing received audit forms relating to the guideline and feedback to staff.
Ensure all staff participates in audit process for deficits to be identified and action plans to be developed.
5.4. Clinicians / Staff responsibilities
Registered healthcare professionals are accountable for their own practice and will be aware
of their legal and professional responsibilities and work within the code of practice of their
professional body.
Maintaining clinical competency as per competency framework
Attending relevant training provided by the Trust and put it into practice

7 Adult Bowel Care Guidelines Version 1 July 2017
Bringing to the attention of appropriate senior staff any deficiencies in knowledge, ability or
resources that may mediate against safe clinical practice.
Participate in audit programmes related to measuring the quality and safety of physical
assessment and monitoring. This would include addressing any improvements required and
celebration of good practice.
Ensuring they are familiar with relevant policies and procedures in their area of practice.
All staff that carry out bowel care must be trained and assessed as competent prior to
undertaking that skill.
6. Bowel Care Guideline Statements 6.1. Consent
6.1.1. Consent is a service user’s agreement for a health professional to provide care. Before health
care professionals examine, treat or care for any person they must obtain their valid consent. There is a basic assumption that every adult has the capacity to decide whether to consent to, or refuse, proposed medical intervention, unless it is shown that they cannot understand information presented in a clear way. Staff must refer to the Consent for Examination or Treatment Policy (SH CP 16) in relation to this.
6.1.2. Staff need to be mindful that by attending a consultation it may be assumed that a service user is seeking treatment. However, before proceeding with an examination it is vital that the service user’s valid consent is obtained. This means that the service user must have capacity/be competent to make the decision. They must have received sufficient information to take the decision and not be acting under duress.
6.1.3. When service users do not have the ability to consent for themselves the health care professionals should undertake an assessment of mental capacity and make the decision in the service user’s best interests in line with the Mental Capacity Act 2005 and trust policies. This must be documented in the service user’s notes
6.2. Privacy, Dignity and Respect
6.2.1. In all examinations, procedures and interventions the Privacy, Dignity & Respect Policy (SH CP 144) must be followed.
6.2.2. Examinations or procedures involving the rectum and any examinations or interventions involving the removal of clothing to a state of undress which may make a service user feel particularly vulnerable constitute Intimate Procedures. Prior to any such examinations, procedures or interventions service users will be offered a chaperone according to the Chaperone Policy (SH CP 184). The ethnic, religious and cultural background of patients must be taken into account and may have particular significance to intimate procedures.
6.3. Bowel Assessment
6.3.1. Bowel care concerns intimate parts of the body. All interventions relating to assessment and treatment require discretion and sensitivity.
6.3.2. Assessment of bowel continence and function will form part of the holistic patient assessment.
Bowel assessment includes obtaining a history and carrying out relevant clinical examinations. It also includes carrying out and interpreting relevant baseline physiological observations and tests.
6.3.3. A structured approach to assessing bowel dysfunction must be adopted according to evidence
based guidance (NICE, 2007). Bowel assessment is completed as part of the Continence

8 Adult Bowel Care Guidelines Version 1 July 2017
Assessment of Appendix 4. Assessments are to be documented and recorded in accordance with the Clinical Record Keeping Policy (SH IG 01).
6.3.4. Where the Continence Assessment identifies bowel dysfunction the Bowel Care Pathway is
implemented (see Appendix 5).
6.4. Investigations
6.4.1. Food, Stool and Medication Diary and Fluid Charts
6.4.1.1. A food, stool and medication diary (see Appendix 6) and fluid charts will be completed according to the Bowel Care Pathway.
6.4.1.2. The assessing health care professional will have knowledge of when to refer for specialist dietetic assessment.
6.4.2. Digital Rectal Examination (DRE)
6.4.2.1. DRE is an invasive intimate procedure that can be performed as part of a bowel assessment. DRE can only be performed by a Doctor or Registered Nurse who can demonstrate competence to an appropriate level in accordance with the Nursing and Midwifery Council (NMC) The Code: Professional standards of practice and behaviour (NMC, 2015). Health Care Support Workers (Bands 3 and above) may also carry out this procedure for appropriate named patients where a registered nurse has carried out the initial assessment and providing the care worker has completed the relevant training and demonstrated competence (see Appendix 3).
6.4.2.2. DRE can be performed in the following circumstances:
To establish whether faecal matter is present in the rectum and, if so, to assess the amount
and consistency.
To ascertain anal tone and the ability to initiate a voluntary contraction and to what degree.
To assess anal pathology for the presence of foreign objects.
Prior to administering rectal medication to establish the state of the rectum.
To establish the effects of rectal medication.
To administer suppositories or enema.
To determine a need for digital removal of faeces (DRF) or digital rectal stimulation (DRS)
and evaluating bowel emptiness.
To assess a need for rectal medication and to evaluate its efficacy in certain circumstances.
E.g. in patients who have diminished anorectal sensation.
For digital stimulation to trigger defaecation by stimulating the rectoanal reflex.
To establish anal and rectal sensation.
6.4.2.3. DRE must not be performed when:
No consent has been obtained.
The patient’s doctor has given specific instructions that an invasive bowel procedure should
not take place.
The patient has recently undergone rectal/anal surgery or trauma (seek medical advice).
The patient gains sexual satisfaction from this procedure (open discussion between health
care professional and service user is advised and a chaperone facility made available in
accordance with the Chaperone Policy (SH CP 184)).
The health care professional does not feel competent to perform the procedure (NMC, 2015).

9 Adult Bowel Care Guidelines Version 1 July 2017
6.4.2.4. DRE is performed according to the procedure in Appendix 7.
6.5. Interventions
6.5.1. Medication
6.5.1.1. Medicines Control, Administration and Prescribing Policy (MCAPP) (SH CP 1) applies to the control, preparation, checking, administration and prescribing of medicines in adult bowel care.
6.5.1.2. Medications must only be prepared, checked and administered by the categories of healthcare staff indicated at paragraph 10.2 of the MCAPP (SH CP 1).
6.5.1.3. Medications are to be administered as prescribed. See Laxative Treatment Guidelines for Adults in Appendix 12.
6.5.1.4. Certain medications can be administered at the discretion of nurses and mental health practitioners in accordance with the MCAPP (SH CP 1) (see Appendix C1 of that policy).
6.5.2. Enemas and Suppositories 6.5.2.1. The administration of enemas and suppositories is an invasive intimate intervention and can
only be performed by a Registered Nurse who can demonstrate competence to an appropriate level in accordance with the Nursing and Midwifery Council (NMC) The Code: Professional standards of practice and behaviour (NMC, 2015). Health Care Support Workers (Bands 3 and above) can carry out this procedure for appropriate named patients where a registered nurse has carried out the initial assessment and providing the care worker has completed the relevant training and demonstrated competence. The task can only be delegated in agreement with and in the best interests of the patient.
6.5.2.2. Glycerol suppositories and micro-enemas can be administered at the discretion of nurses in
accordance with the Laxative Treatment Guidelines for Adults (see Appendix 12) and the MCAPP (SH CP 1) (see Appendix D of that policy).
6.5.2.3. Enemas and suppositories are administered according to the procedure in Appendix 8. 6.5.3. Digital Rectal Stimulation (DRS)
6.5.3.1. DRS is an invasive intimate intervention to increase reflex muscular activity in the rectum to
raise rectal pressure and aid stool expulsion. DRS can only be performed by a Registered Nurse who can demonstrate competence to an appropriate level in accordance with the Nursing and Midwifery Council (NMC) The Code: Professional standards of practice and behaviour (NMC, 2015).
6.5.3.2. Health Care Support Workers (Bands 3 and above) can also carry out this procedure for appropriate named patients where a registered nurse has carried out the initial assessment and providing the care worker has completed the relevant training and demonstrated competence (see Appendix 3). The task can only be delegated in agreement with and in the best interests of the patient.
6.5.3.3. DRS can be performed in the following circumstances:
Faecal impaction/loading.
Incomplete defaecation.
Inability to defaecate.
Other bowel emptying techniques have failed.

10 Adult Bowel Care Guidelines Version 1 July 2017
Patients with spinal injury as part of a bowel management programme.
6.5.3.4. DRS must not be performed when:
No consent has been obtained.
The service user’s doctor has given specific instructions that an invasive bowel procedure
should not take place.
The service user has recently undergone rectal/anal surgery or trauma (seek medical
advice).
The service user gains sexual satisfaction from this procedure (open discussion between
health care professional and service user is advised and a chaperone facility made available
in accordance with the Chaperone Policy (SH CP 184)).
The health care professional does not feel competent to perform the procedure (NMC, 2015).
6.5.3.5. DRS is performed according to the procedure in Appendix 9.
6.5.4. Digital Removal of Faeces (DRF)
6.5.4.1. DRF is an invasive intimate intervention for assisted evacuation of the bowel. DRF can only be
performed by a Registered Nurse who can demonstrate competence to an appropriate level in accordance with the Nursing and Midwifery Council (NMC) The Code: Professional standards of practice and behaviour (NMC, 2015). Health Care Support Workers (Bands 3 and above) may also carry out this procedure for appropriate named patients where a registered nurse has carried out the initial assessment and providing the care worker has completed the relevant training and demonstrated competence (see Appendix 3).
6.5.4.2. DRF can be performed in the following circumstances:
Faecal impaction/loading.
Incomplete defaecation.
Inability to defaecate.
Other bowel emptying techniques have failed.
Patients with spinal injury as part of a bowel management programme.
6.5.4.3. DRF must not be performed when:
No consent has been obtained.
The service user’s doctor has given specific instructions that an invasive bowel procedure
should not take place.
The service user has recently undergone rectal/anal surgery or trauma (seek medical
advice).
The service user gains sexual satisfaction from this procedure (open discussion between
health care professional and service user is advised and a chaperone facility made available
in accordance with the Chaperone Policy (SH CP 184)).
The health care professional does not feel competent to perform the procedure (NMC, 2015).
6.5.4.4. DRF is performed according to the procedure in Appendix 10.
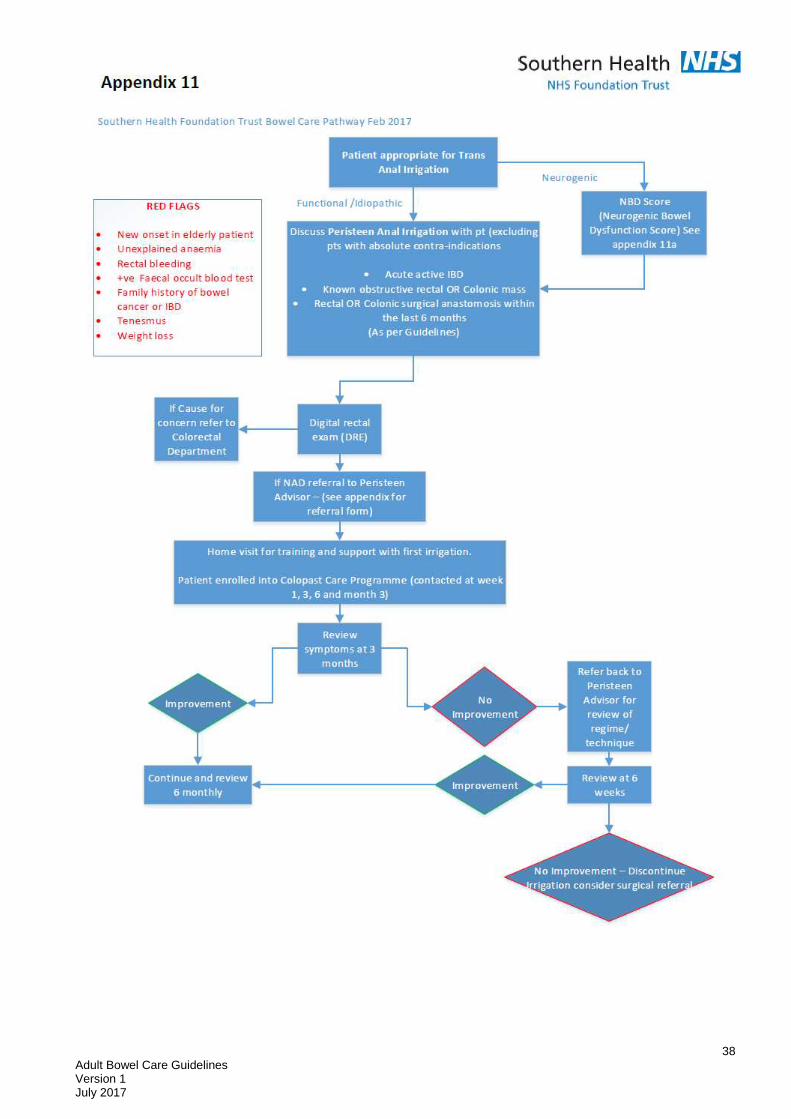
6.5.5. Trans-anal Irrigation 6.5.5.1. Trans-anal Irrigation will only be considered when other less invasive methods of bowel
management have failed to adequately control constipation and/or faecal incontinence and only

11 Adult Bowel Care Guidelines Version 1 July 2017
following DRE examination by a medical practitioner. The flowchart of Appendix 11 provides guidance for the referral of trans-anal irrigation.
6.5.5.2. Trans-anal irrigation will be carried out for the first time under the direction of a medical practitioner or a Registered Nurse who can demonstrate competence in trans-anal irrigation to an appropriate level in accordance with the Nursing and Midwifery Council (NMC) The Code: Professional standards of practice and behaviour (NMC, 2015).
6.5.5.3. Subsequent to the first administration of trans-anal irrigation, the procedure is suitable for
patient self-administration at the discretion of the medical practitioner.
6.5.5.4. Indications for trans-anal irrigation include:
Neurogenic bowel dysfunction: e.g. spinal cord injury, spina bifida, multiple sclerosis.
Chronic constipation, including both evacuation difficulties and slow transit constipation.
Chronic faecal incontinence.
6.5.5.5. Trans-anal irrigation may be indicated in the following circumstances with close supervision and
monitoring by a medical practitioner or competent Registered Nurse:
Spinal cord injury at or above T6, monitor for autonomic dysreflexia, until it is clear that the
technique is well tolerated and does not provoke autonomic dysreflexia.
Unstable metabolic conditions (frail, known renal disease or liver disease).
Inability to perform the procedure independently or comply with the protocol in the absence
of close involvement of carers (e.g. due to physical disability, cognitive impairment, major
mental/emotional disorder).
Anorectal conditions that could cause pain or bleeding during the procedure (e.g. third
degree haemorrhoids, anal fissure).
6.5.5.6. The following circumstances are contra-indicated except when specifically directed by a medical
practitioner:
Pregnant or planning pregnancy.
Active perianal sepsis.
Diarrhoea. (New onset and no clinical explanation)
Anal fissure.
Large haemorrhoids that bleed easily.
Faecal impaction (clear, if possible before starting irrigation: digital rectal examination if
unsure).
Past pelvic radiotherapy which has caused bowel symptoms.
Known severe diverticular disease.
Use of rectal medications for other diseases.
Congestive cardiac failure.
Anal surgery within the past 6 months.
Children under 3 years old.
6.5.5.7. The following circumstances are contra-indicated and trans-anal irrigation will not be used:
Acute active inflammatory Bowel disease.
Known obstructing rectal or colonic mass.
Severe cognitive impairments.

12 Adult Bowel Care Guidelines Version 1 July 2017
Rectal or colonic surgical anastomosis ( surgical connection of two intestinal structures)
within the last six months
6.6. Neurogenic Bowel Dysfunction
6.6.1. All staff involved in the management of neurogenic bowel dysfunction must demonstrate
competence in the management of autonomic symptoms and acute autonomic dysreflexia. 7. Training requirements 7.1. All practitioners required to undertake bowel care will attend face-to-face foundation training in
bowel care and must demonstrate competence in bowel care assessment and interventions (see Appendix 1). Competency assessment will be undertaken by a competent Registered Nurse, who has been deemed competent at level 4 or above.
7.2. All practitioners will have a working knowledge of relevant current legislation, national
guidelines, organisational policies and procedures. 7.3. All practitioners will have a working knowledge of working within their sphere of competence
and acknowledge when to seek advice. 7.4. All staff must practise their skills regularly to maintain competence. They must refresh their
knowledge and skills at least every three years. (Bowel care competencies Appendix 3) 7.5. Staff (practitioners and assessors) must maintain their competence through clinical practice and
personal study. 7.6. It is possible that unregistered practitioners (bands 3 and 4) will be involved in carrying out
aspects of bowel care. In these cases, the relevant bowel care interventions are delegated by registered practitioners. A registered professional should only delegate bowel care tasks to a person who has had the appropriate training and whom they deem competent to perform the task. The registered healthcare professional will also ensure that the person they have delegated the task to fully understands the nature of the delegated task in relation to what is expected of them. The health care support worker must know their limitations and identify when to seek advice from an appropriate professional.
8. Monitoring compliance
Element to be monitored
Lead Tool Frequency Reporting arrangements
Clinical competency in bowel care
Line manager
Bowel Care Competencies
Annual Appraisal
9. Guideline review
9.1. Guideline should be reviewed in two years
10. Associated trust documents
10.1. This guideline should be read in conjunction with, and with reference to, the following trust documents:

13 Adult Bowel Care Guidelines Version 1 July 2017
10.2. SHFT Care planning Policy SC HP 82
10.3. SHFT Clinical Record Keeping Policy SH IG 01
10.4. SHFT Medicines Control, Administration and Prescribing Policy SH CP 01
10.5. SHFT Chaperone Policy SH CP 184
10.6. SHFT Mental Capacity Act Policy and Guidance SH CP 39
10.7. SHFT Consent for Examination or Treatment Policy SH CP 16
10.8. SHFT Privacy, Dignity & Respect Policy SH CP 144
10.9. SHFT Infection Control Policy SH CP 10
10.10. SHFT Risk Management Strategy and Policy SH NCP 25
11. Supporting references
National Institute for Health and Care Excellence (2007) Faecal incontinence: the management of faecal incontinence in adults – clinical guideline CG49, London: NICE.
Royal College of Nursing (2012) Management of lower bowel dysfunction, including DRE and DRF, London: RCN.
Royal Marsden NHS Foundation Trust (2015) The Royal Marsden Manual of Clinical Nursing Procedures – Ninth Edition, London.
Multidisciplinary Association of Spinal Cord Injured Professionals (2012) Guidelines for Management of Neurogenic Bowel Dysfunction in Individuals with Central Neurological Conditions.
Nursing and Midwifery Council (2015) The Code: Professional standards of practice and behaviour, London, NMC.
Norton, C. (2009) Guidelines for the use of Rectal Irrigation, Kings College, London.
14 Adult Bowel Care Guidelines Version 1 July 2017
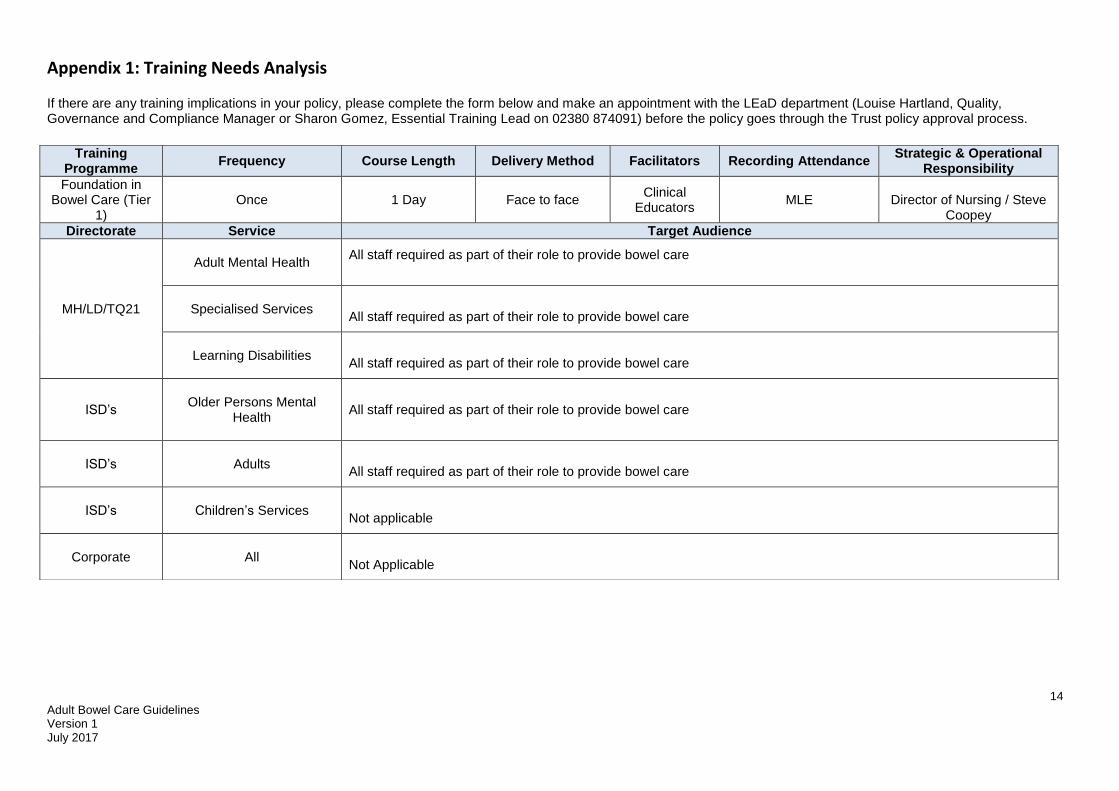
Appendix 1: Training Needs Analysis
If there are any training implications in your policy, please complete the form below and make an appointment with the LEaD department (Louise Hartland, Quality, Governance and Compliance Manager or Sharon Gomez, Essential Training Lead on 02380 874091) before the policy goes through the Trust policy approval process.
Training Programme
Frequency Course Length Delivery Method Facilitators Recording Attendance Strategic & Operational
Responsibility
Foundation in Bowel Care (Tier
1) Once 1 Day Face to face
Clinical Educators
MLE
Director of Nursing / Steve Coopey
Directorate Service Target Audience
MH/LD/TQ21
Adult Mental Health
All staff required as part of their role to provide bowel care
Specialised Services
All staff required as part of their role to provide bowel care
Learning Disabilities
All staff required as part of their role to provide bowel care
ISD’s
Older Persons Mental
Health
All staff required as part of their role to provide bowel care
ISD’s
Adults
All staff required as part of their role to provide bowel care
ISD’s
Children’s Services
Not applicable
Corporate
All
Not Applicable

15 Adult Bowel Care Guidelines Version 1 July 2017
Appendix 2: Equality Impact Assessment The Equality Analysis is a written record that demonstrates that you have shown due regard to the need to eliminate unlawful discrimination, advance equality of opportunity and foster good relations with respect to the characteristics protected by the Equality Act 2010. Stage 1: Screening
Date of assessment: 2/04/17
Name of person completing the assessment: Steve Coopey
Job title: Head of Clinical Development
Responsible department: LEaD
Intended equality outcomes: Service users are able to access this service as identified solely by clinical need and therefore this guidance does not discriminate against service users
Who was involved in the consultation of this document?
Alison Wileman
Please describe the positive and any potential negative impact of the policy on service users or staff. In the case of negative impact, please indicate any measures planned to mitigate against this by completing stage 2. Supporting Information can be found be following the link: www.legislation.gov.uk/ukpga/2010/15/contents
Protected Characteristic Positive impact Negative impact
Age x
Disability x
Gender reassignment x
Marriage & civil partnership x
Pregnancy & maternity x
Race x
Religion x
Sex x
Sexual orientation x
Stage 2: Full impact assessment
What is the impact? Mitigating actions Monitoring of actions

16 Adult Bowel Care Guidelines Version 1 July 2017
Appendix 3: Competencies Bowel Care: Digital Rectal Examination, Digital Removal of Faeces and Digital Rectal Stimulation Clinical Competencies
Name:
Role:
Base:
Date initial training completed:
Competency Statement:
The participant demonstrates clinical knowledge and skill in digital rectal examination and removal of faeces without assistance and/or direct supervision (level 3 - see level descriptors). Assessment in practice must be by a Registered Nurse who can demonstrate competence at level 4 or above.
Performance Criteria Assessment Method Level achieved
Date Assessor/self assessed
The Participant will be able to:
1. Demonstrate the knowledge and skill in digital rectal examination (DRE)
a) Demonstrate an awareness of professional accountability and guidelines (e.g. RCN)
Questioning
b) Discuss the rationale for DRE Questioning
c) Demonstrate an understanding of the relevant anatomy and physiology of the gastro-intestinal tract
Questioning
d) Discuss the care of a patient with altered bowel function
Questioning
e) Identify when it would be appropriate to carry out DRE
Questioning
f) Identify when it would be necessary to stop procedure and what action to take
Questioning
g) Discuss the use of appropriate medication e.g. Laxatives,
suppositories , enemas
Questioning
h) Demonstrate knowledge of appropriate use of equipment
Observation
i) Demonstrate preparation of the patient and gain informed consent
Observation
j) Demonstrate the correct procedure to perform DRE
Observation
k) Demonstrate safe disposal of equipment and waste
Observation

17 Adult Bowel Care Guidelines Version 1 July 2017
Performance Criteria Assessment Method Level achieved
Date Assessor/self assessed
l) Complete documentation and any recommendations for treatment / follow up
Observation
m) Recognise symptoms of autonomic dysreflexia in the paralysed patient and take appropriate action
Observation/Questioning
2. Demonstrate the knowledge and skill in digital removal of faeces (DRF)
a) Demonstrate an awareness of professional accountability and guidelines (e.g. RCN)
Questioning
b) Identify the indications for digital removal of faeces
Questioning
c) Demonstrate an understanding of the relevant anatomy and physiology of the gastro-intestinal tract
Questioning
d) Discuss the care of a patient with altered bowel function
Questioning
e) Identify the conditions which contraindicate digital removal of faeces
Questioning
f) Discuss the potential side effects of procedure including stimulation of vagus nerve
Questioning
g) Identify when it would be necessary to stop procedure and what action to take
Questioning
h) Discuss the use of appropriate medication e.g. Laxatives,
suppositories , enema
Questioning
i) Demonstrate preparation of the patient and gain informed consent
Observation
k) Demonstrate the correct procedure to perform digital removal of faeces
Observation
l) Demonstrate safe disposal of equipment and waste
Observation
m) Complete documentation and any recommendations for treatment / follow up
Observation
n) Recognise symptoms of autonomic dysreflexia in the paralysed patient and take appropriate action
Questioning/questioning

18 Adult Bowel Care Guidelines Version 1 July 2017
Performance Criteria Assessment Method Level achieved
Date Assessor/self assessed
The Participant will be able to:
3. Demonstrate the knowledge and skill in digital rectal Stimulation (DRS)
a) Demonstrate an awareness of professional accountability and guidelines (e.g. RCN)
Questioning
b) Discuss the rationale for DRS Questioning
c) Demonstrate an understanding of the relevant anatomy and physiology of the gastro-intestinal tract
Questioning
d) Discuss the care of a patient with altered bowel function
Questioning
e) Identify when it would be appropriate to carry out DRS
Questioning
f) Identify when it would be necessary to stop procedure and what action to take
Questioning
g) Discuss the use of appropriate medication e.g. Laxatives, suppositories , enemas
Questioning
h) Demonstrate knowledge of appropriate use of equipment
Observation
i) Demonstrate preparation of the patient and gain informed consent
Observation
j) Demonstrate the correct procedure to perform DRS
Observation
k) Demonstrate safe disposal of equipment and waste
Observation
l) Complete documentation and any recommendations for treatment / follow up
Observation
m) Recognise symptoms of autonomic dysreflexia in the paralysed patient and take appropriate action
Observation/Questioning
Source: RCN guidelines for the management of lower bowel dysfunction, including DRE and DRF 2012, Guidelines for Management of Neurogenic Bowel Dysfunction in Individuals with Central Neurological Conditions 2012, Southern Health NHS Foundation Trust Bowel Care Guidelines Version 1, 2017.

19 Adult Bowel Care Guidelines Version 1 July 2017
Date all elements of Competency Tool completed to level 3________
Name __________________ Signature _________________Status ___________ Date _______
I confirm that I have assessed the above named individual and can verify that he/she demonstrates competency in Bowel care
including digital rectal examination, digital removal of faeces and digital rectal stimulation
Assessor_______________ Signature _____________________ Status ___________ Date _______
Review
Dates:
Competent
Yes / No
Signature Assessor
signature
Comments

20 Adult Bowel Care Guidelines Version 1 July 2017
APPENDIX 4
CONTINENCE ASSESSMENT (Level 1) Patient Name (Capitals): ....................................................................
Tel No: ................................................................................................
Date: .................................... Time (24hr clock): …............................
Title: Mr Mrs Ms NHS No:
Full address: Post Code:
Telephone no:
Date of birth:
GP/Practice:
Medications (in capitals):
Relevant Medical History (include dates):
Number of pregnancies
Back Problems? Parkinson’s?
Difficult deliveries?
Constipation? Multiple Sclerosis?
Hysterectomy?
Dementia? Spinal Injury?
Pelvic surgery?
Depression? Psychiatric History?
Cystoscopy?
Diabetes? Weight History?
Prostatectomy?
Learning Disability? Other
Previous Investigations
External Vaginal Assessment [Look for: prolapse, sore skin, vaginal atrophic changes]:
Rectal Examination:
Allergies:
Presenting problem and duration:
14 day food and stool diary YES/NO
3 day fluid balance chart: YES/NO
If ‘no’ give reason:
Urine Analysis If Leucocytes/Nitrates/Blood present (ie symptoms of UTI), refer to Medical Practitioner (or appropriate Health Care Professional), resume assessment following treatment.
Patient Weight:

21 Adult Bowel Care Guidelines Version 1 July 2017
How many drinks in 24 hours?
If fluid intake is low, advise 6-8 mugs. If caffeine content is high, advise on decaffeinated drinks. Resume assessment when patient has improved fluid intake
Type of drinks
Bowel habit: Daily...... Alternate Days…… Less Often...... Faecal Incontinence…….
If constipated, treat/refer to medical Practitioner, (Or appropriate Health Care Professional) resume assessment following treatment. If recent abnormal changes and altered bowel habit, refer to doctor immediately.
Consistency of faeces – Bristol Stool Form Scale
Type:
Colour of faeces If patient has any signs of undiagnosed bleeding or black tarry stool and is not taking ferrous sulphate, stop assessment and refer to doctor immediately
Complete fibre score chart. Score: Use the Fibre Score Chart to establish fibre levels. If scores 12 or less, give and explain fibre advice sheet. Consider fibre
SYMPTOM PROFILE
Patient Symptoms – tick relevant points
If any box ticked
Do you leak when you laugh/cough/sneeze/exercise? Do you only ever leak a small amount? Do you know when you have leaked? Do you leak without feeling the need to empty your bladder? Does leaking only wet your underwear (not outer clothes)? Do you feel a strong sudden urge to pass urine and have to go quickly? Do you feel an uncontrollable urge to pass urine prior to leaking? Do you feel that you pass urine frequently? Do you get up at night at least twice to pass urine? Do you leak moderate to large amounts of urine before you reach the toilet?
Follow urinary care pathway
Do you find it hard to start to pass urine? Do you have to strain to pass urine?
Refer to Continence Team/Medical Practitioner for further assessment.

22 Adult Bowel Care Guidelines Version 1 July 2017
Does your urine flow ‘stop and start’? Do you feel that it takes a long time to pass urine? Do you feel the need to pass urine once you have voided? Do you feel as if your bladder is not completely empty? Do you feel that your stream is weaker and slower than it used to be?
Do you have difficulty with physical access to a toilet? Do you have difficulty getting on/off the toilet/wiping bottom?
Refer to Occupational Therapist. Resume treatment following assessment
Do you experience pain on passing faeces? Prior
During
After
Do you feel strong/sudden urge to pass a stool/have bowels open?
Refer to Medical Practitioner (or appropriate Health care Professional, resume assessment following treatment.
Do you have the urge to have bowels open? Do you soil yourself before reaching the toilet? Do you have difficulty passing faeces? Do you feel your bowel motions are not frequent/regular enough? Do you only pass small amounts of faeces? Do your bowels still feel full after going to the toilet?
Follow bowel care pathway
Patient unable to answer above questions Patient appears confused Patient has cognitive impairment
Refer to Medical Practitioner for further assessment Resume assessment following consultation.
Signature …………………………………………………………………………………………….. Date …………………………………………………
Assessor print name: …………………………………………………………… Designation (e.g. RN) …………………………………………
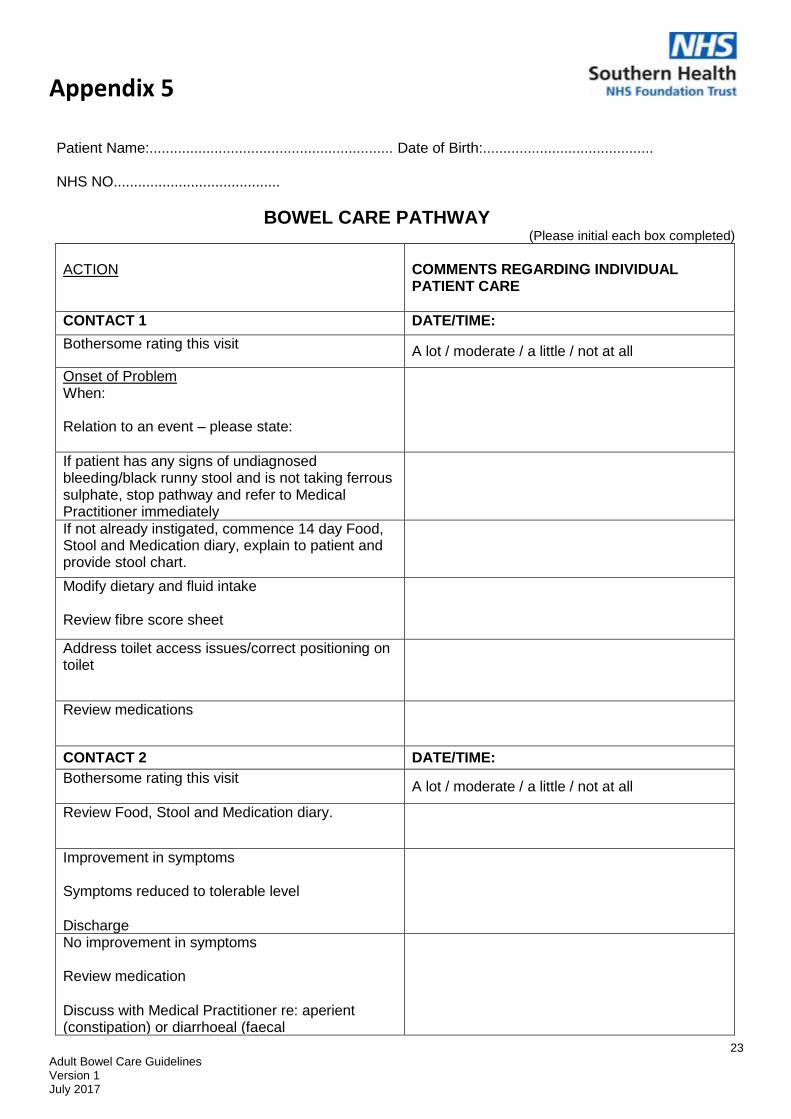
Appendix 5
23 Adult Bowel Care Guidelines Version 1 July 2017
Patient Name:............................................................ Date of Birth:..........................................
NHS NO.........................................
BOWEL CARE PATHWAY (Please initial each box completed)
ACTION
COMMENTS REGARDING INDIVIDUAL PATIENT CARE
CONTACT 1 DATE/TIME:
Bothersome rating this visit A lot / moderate / a little / not at all
Onset of Problem When:
Relation to an event – please state:
If patient has any signs of undiagnosed bleeding/black runny stool and is not taking ferrous sulphate, stop pathway and refer to Medical Practitioner immediately
If not already instigated, commence 14 day Food, Stool and Medication diary, explain to patient and provide stool chart.
Modify dietary and fluid intake
Review fibre score sheet
Address toilet access issues/correct positioning on toilet
Review medications
CONTACT 2 DATE/TIME:
Bothersome rating this visit A lot / moderate / a little / not at all
Review Food, Stool and Medication diary.
Improvement in symptoms
Symptoms reduced to tolerable level
Discharge
No improvement in symptoms
Review medication
Discuss with Medical Practitioner re: aperient (constipation) or diarrhoeal (faecal incontinence) medication

24 Adult Bowel Care Guidelines Version 1 July 2017
Patient Name........................................................ Date of Birth.............................................
NHS NO..............................................
BOWEL CARE PATHWAY cont...... (Please initial each box completed)
Consider Long Term Management
provision of continence products (faecal
incontinence)
need for rectal intervention (constipation)
CONTACT 3
DATE/TIME:
Bothersome rating this visit A lot / moderate / a little / not at all
Review Food, Stool and Medication diary.
Symptoms resolved/reduced to tolerable level.
Discharge
Variance: This patient is unable to commence on a Care Pathway because:
Inform referring medical practitioner if pathway incomplete at any visit
TO BE COMPLETED BY ALL STAFF USING THE PATHWAY
Sign to confirm that you have met all standards or recorded variances
FULL NAME
DESIGNATION
INITIALS
SIGN
DATE
Discharge Date:
Signature:

25 Adult Bowel Care Guidelines Version 1 July 2017
Appendix 6A
14 Day Food, Stool and Medication Diary
Patient’s Name: ………………………………………………… DOB: ………………… NHS No: ……………………..……… Address
………………………………………………………………………………………………………………………………………
DATE FOOD AND DRINK
(Please record everything you eat and drink e.g. Lunch: meat, boiled potatoes, peas, carrots, gravy, apple and yoghurt + 150mls water – please do not write
‘normal diet’)
STOOL TYPE, FAECAL INCONTINENCE/SOILING IF APPROPRIATE AND
TIME OCCURRED (See Bristol Stool Chart)
BOWEL MEDICATION
Name, amount and times

26 Adult Bowel Care Guidelines Version 1 July 2017
APPENDIX 6B
By Cabot Health, Bristol Stool Chart
[CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons

27 Adult Bowel Care Guidelines Version 1 July 2017
Appendix 7 Procedure for Digital Rectal Examination in Adults
Action Rationale
Confirm patient’s identity and Obtain careful history from patient prior to examination, including establishing whether patient has any known allergies. Identify patient by surname, first name and date of birth using open questions checking against NHS number.
To avoid error in patient identification. To assess symptoms, and reduce the risk of allergic reaction.
Ensure Patient is introduced to staff involved in the procedure
Helps reduce anxiety by improving communication.
Explain each step of the procedure to the patient, including potential risks and complications, and also the benefits.
To ensure patient is informed and understands the procedure. Patient information can help to reduce anxiety.
Obtain valid and informed consent and document in patient’s health records. If necessary refer to the Mental Capacity Act 2005, and consider if the examination is in patient’s best interest. Follow the SHFT consent for examination or treatment policy.
To ensure patient is happy for the procedure to take place.
Clarify if the patient requires a formal chaperone. Follow SHFT Chaperone policy.
It is the patient’s choice to have a chaperone if required. Refer to Chaperone policy.
Decontaminate hands as per Southern Health Hand Hygiene Procedure, and apply gloves and apron (single use non sterile disposable)
To reduce the risk of infection, and to protect clothing or uniform from contamination and potential transfer of micro-organisms. Protect hands from contamination with organic matter.
Ensure a bedpan/commode or toilet is readily available.
DRE can stimulate the need for a bowel movement. (need up to date reference) To facilitate easy access for defecation ensuring privacy and dignity.
Perform physical observations required according to whether it is an acute intervention or regular ongoing intervention and observe for signs of Autonomic Dysreflexia in spinal cord injured patients. If at any time the heart rate drops, rhythm changes or signs of Autonomic Dysreflexia STOP the procedure
To provide a baseline measurement to assess any changes in the pulse/blood pressure during or after the procedure (RCN 2012) Spinal cord injured patients have frequently been observed for changes in blood pressure without signs and symptoms of Autonomic dysreflexia. Monitoring blood pressure as part of an ongoing

28 Adult Bowel Care Guidelines Version 1 July 2017
intervention is thought to be of little benefit. The Practitioner should observe for signs of potential shock/Autonomic Dysreflexia (Coggrave et al 2009)
Assist the patient to lie on the left side, with knees drawn to the abdomen, and buttocks near the edge of the bed.
To promote the stability of the patient and to allow ease of digital rectal examination by following the natural anatomy of the colon. (RCN 2012)
Place a disposable protective pad underneath the patient’s hips and buttocks and cover area to be. exposed
To reduce potential infection risk caused by soiled linen. To promote dignity of the patient and avoid embarrassment if faecal staining occurs during or after the procedure.
Inform the patient that you are about to begin the procedure and that you will be examining the outer and internal area.
To ensure the patient is aware the examination is about to begin.
Observe the perianal area prior to procedure for evidence of skin soreness, excoriation, swelling, haemorrhoids, lesions, such as skin tags, rectal prolapse, fistulas, foreign bodies, faecal matter, mucus, blood or infestation.
To assess for abnormalities such as bleeding, discharge or prolapse, all of which should be reported to medical staff before examination is undertaken. (RCN 2012) Swelling may be indicative of possible mass or abscess.
Palpate the perianal area by starting at the 12 o’clock position moving clockwise to 6 o’clock and then returning to 12 o’clock and moving to 6 o’clock anticlockwise.
To assess for any irregularities, indurations, tenderness or abscess formation.
Lubricate gloved finger with lubricant gel. To prevent trauma to rectal mucosa and minimize discomfort as lubrication reduces friction. To ease finger into anus/rectum.
Prior to insertion, encourage the patient to breathe out or talk and place gloved finger on the anus for a few seconds. On insertion, assess anal sphincter control.
To prevent the anal sphincter from spasm on insertion. Gently placing a finger on the anus initiates the anal reflex, causing the anus to contract and then relax (RCN 2012) If there is resistance on insertion, this indicates good internal sphincter tone, it is only during defecation that the sphincter should relax. (RCN 2012).
With the finger inserted in the anus, sweep clockwise, then anticlockwise. Note any irregularities.
Palpating around the anus at 360 degrees allows to establish any tenderness or swelling in the rectum (steggall 2008)
Assess for faecal matter in the rectum. Note consistency, amount and type using the Bristol stool chart.
To assess if rectum is loaded, for constipation and/or the need for further intervention.
Observe the patient throughout the procedure:
To note signs of distress, pain, bleeding and general discomfort.

29 Adult Bowel Care Guidelines Version 1 July 2017
STOP • If anal area is bleeding • If the patient asks you to • If patient is showing signs of
Autonomic Dysreflexia
Or Autonomic Dysreflexia (Refer to section/page in policy not written yet)
When procedure is completed, clean residual lubricating gel from the perianal area.
To promote comfort and prevent skin excoriation.
Make the patient comfortable and offer toilet, commode, bedpan or other equipment as appropriate and assist as required.
Examination may have stimulated the anorectal reflex and the urge to defecate.
Dispose of all equipment and PPE as per SHFT Handling and Disposal of waste policy, remove gloves and apron and decontaminate hands as per the SHFT Hand Hygiene Procedure.
To prevent cross infection and environmental contamination and to ensure staff and patient safety.
Document procedure in the patient’s health records including the reason for DRE, the outcome and review date to assess the need for repeat DRE.
To comply with NMC Code and SHFT guidelines on documentation. To monitor effects and improve communication and enhance delivery of care.
If any abnormality is found ensure an appropriate referral is made in line with SHFT policy
To promote continuity of care and patient safety.
References Higgins, D. (2006) How to administer an enema. Nursing Times, 102(20), 24-25 Kyle, G (2007) Bowel care part 4. Administering an enema. Nursing Times; 103(45), 26-27. Kyle, G (2009) Should a suppository be inserted with the blunt end or the pointed end first, or does it not matter? Nursing times, 105(2), 16. Royal College of Nursing (2012) Management of Lower Bowel Dysfunction including DRE &DRF – guidance for nurses. Steggall, M.J (2008) digital rectal examination. Nursing standard, 22(47), 46-48. Cggrave et al (2009) Guidelines for Management of Neurogenic Bowel Dysfunction after Spinal Cord injury.

30 Adult Bowel Care Guidelines Version 1 July 2017
Appendix 8 Procedure for Administering Suppositories and Enemas
Action Rationale
Obtain careful history from patient prior to examination, including establishing whether patient has any known allergies.
To assess symptoms, and reduce the risk of allergic reaction.
Establish indications for use and eliminate any contra-indications or allergies prior to proceeding.
To ensure appropriateness, suitability and safety of administration.
Ensure Patient is introduced to staff involved in the procedure
Helps reduce anxiety by improving communication.
Explain each step of the procedure to the patient, including potential risks and complications, and also the benefits.
To ensure patient is informed and understands the procedure. Patient information can help to reduce anxiety.
Obtain valid and informed consent and document in patient’s health records. If necessary refer to the Mental Capacity Act 2005, and consider if the examination is in patient’s best interest. Follow the SHFT consent for examination or treatment policy.
To ensure patient is happy for the procedure to take place.
Identify patient by surname, first name and date of birth using open questions checking against NHS number.
To ensure correct identification of the patient.
Establish that the patient has no known allergies.
To reduce the risk of allergic reactions.
Clarify if the patient requires a formal chaperone. Follow SHFT Chaperone policy.
It is the patient’s choice to have a chaperone if required. Refer to Chaperone policy.
Check Suppository/Enema to be administered against Medicines Administration chart or, if at nurses discretion according to policy, document the administration appropriately.
To protect patient from harm and ensure effective record keeping.
Ensure Medicines Administration chart specifies:
Patients full name
Patients date of birth
Prescriber’s signature and date prescribed
Name of suppository/Enema to be administered
Dose to be administered
Route of administration
Patients allergy status
To maintain patient safety.
Read manufacturer’s instructions for use. To ensure the enema or suppository is

31 Adult Bowel Care Guidelines Version 1 July 2017
prepared and administered in accordance with manufacturer’s instructions.
Allow patient to empty bladder first if required. To reduce the feeling of discomfort during the procedure (Higgins 2006).
Ensure a bedpan, commode or toilet is readily available.
In case the patient feels the need to expel the enema or suppository before the procedure is completed.
Decontaminate hands as per Southern Health Hand Hygiene Procedure, and apply gloves and apron (single use non sterile disposable)
To reduce the risk of infection, and to protect clothing or uniform from contamination and potential transfer of micro-organisms. Protect hands from contamination with organic matter.
Administration of Enemas: Prepare the enema by warming to body temperature in accordance with manufacturer’s instructions.
Warming the enema solution to body temperature may be beneficial as heat is an effective stimulant to the intestinal mucosa. Cold solutions should be avoided as they may cause cramping. (Higgins 2006) If water is used to warm the enema, care must be taken not to overwarm.
Assist the patient to lie on the left side, with knees drawn to the abdomen, and buttocks near the edge of the bed.
To allow ease of passage and flow of fluid into rectum. The anatomical structure of the sigmoid colon assists enema distribution and retention
Place some lubricating gel on nozzle of enema
To prevent trauma to the anal and rectal mucosa, reducing surface friction (Higgins 2006)
Expel excessive air from enema prior to administration
Excessive air may cause abdominal discomfort or pain (kyle 2007)
Inform the patient that you are about to commence the procedure, slowly introduce the nozzle to the depth recommended by the manufacturer
To ensure the nozzle is in the rectum
Introduce the fluid slowly as recommended by the manufacturer
To promote comfort (will find a better answer when completed my research.
Once instilled, slowly withdraw the nozzle To avoid reflex emptying of the rectum
Ask the patient to retain the enema for 10-15 minutes before evacuating the bowel
To enhance the evacuant effect
Administration of suppository: Open the packet/suppository and lubricate the suppository with lubricating gel or water according to the manufacturer’s instructions
Lubrication reduces surface friction, avoiding anal mucosa trauma. Aids ease of suppository insertion.
Insert the suppository into the rectum, ensuring that it is placed against the bowel wall.
Suppositories need body heat in order to dissolve and become effective. If they are placed in faecal matter they will remain intact and be ineffective. (Kyle 2009) There is inconclusive evidence regarding whether suppositories should be inserted blunt

32 Adult Bowel Care Guidelines Version 1 July 2017
end first (Higgins 2007). Please refer to individual manufacturer’s instructions for use.
Observe the patient throughout the procedure: STOP
If anal area is bleeding
If the patient asks you to
If patient is showing signs of Autonomic Dysreflexia
To note signs of distress, pain, bleeding and general discomfort. Or Autonomic Dysreflexia (Refer to section/page in policy not written yet)
When completed procedure, clean residual lubricating gel from the perineal area.
To prevent skin excoriation and promote comfort.
Ensure patient is comfortable and ask them to retain the suppository for 20 minutes, or until they are no longer able to do so.
To allow the suppository to melt and release the active ingredients.
Ensure patient has access to commode/bedpan/toilet
In case rapid bowel evacuation following procedure.
Dispose of all equipment and PPE as per SHFT Handling and Disposal of waste policy, remove gloves and apron and decontaminate hands as per the SHFT Hand Hygiene Procedure.
To prevent cross infection and environmental contamination and to ensure staff and patient safety.
Document the procedure carried out, and the outcome of the procedure in the patient’s health records
To comply with NMC Code and SHFT guidelines on documentation. To monitor effects and improve communication and enhance delivery of care.
If any abnormality is found ensure an appropriate referral is made in line with local policy
To promote continuity of care and patient safety.
References Higgins, D. (2006) How to administer an enema. Nursing Times, 102(20), 24-25 Kyle, G (2007) Bowel care part 4. Administering an enema. Nursing Times; 103(45), 26-27. Kyle, G (2009) Should a suppository be inserted with the blunt end or the pointed end first, or does it not matter? Nursing times, 105(2), 16.

33 Adult Bowel Care Guidelines Version 1 July 2017
Appendix 9 Procedure for Digital Rectal Stimulation in Adults
Action Rationale
Obtain careful history from patient prior to examination, including establishing whether patient has any known allergies.
To assess symptoms, and reduce the risk of allergic reaction.
Ensure Patient is introduced to staff involved in the procedure
Helps reduce anxiety by improving communication.
Explain each step of the procedure to the patient, including potential risks and complications, and also the benefits.
To ensure patient is informed and understands the procedure. Patient information can help to reduce anxiety.
Obtain valid and informed consent and document in patient’s health records. If necessary refer to the Mental Capacity Act 2005, and consider if the examination is in patient’s best interest. Follow the SHFT consent for examination or treatment policy.
To ensure patient is happy for the procedure to take place.
Identify patient by surname, first name and date of birth using open questions checking against NHS number.
To ensure correct identification of the patient.
Clarify if the patient requires a formal chaperone. Follow SHFT Chaperone policy.
It is the patient’s choice to have a chaperone if required. Refer to Chaperone policy.
Ask the patient if they wish to use the toilet prior to undertaking the procedure.
For comfort of the patient.
Ensure the bedpan/commode/toilet is readily available.
To facilitate easy access for defecation ensuring privacy and dignity
Perform physical observations required according to whether an acute intervention or regular ongoing intervention and observe for signs and symptoms of Autonomic Dysreflexia in Spinal cord injured patients. If at any time the heart rate drops, rhythm changes or signs of Autonomic Dysreflexia STOP the procedure
To provide a baseline measurement to assess any changes in the pulse/blood pressure during or after the procedure (RCN 2012). Spinal cord injured patients have frequently been observed for changes in blood pressure without signs and symptoms of Autonomic dysreflexia. Monitoring blood pressure as part of an ongoing intervention is thought to be of little benefit. The Practitioner should observe for signs of potential shock/Autonomic Dysreflexia. (Coggrave et al 2009)
Assist the patient to lie on the left side, with knees drawn to the abdomen, and buttocks near the edge of the bed
To promote the stability of the patient and to allow ease of digital rectal stimulation by following the natural anatomy of the colon. (RCN 2012)

34 Adult Bowel Care Guidelines Version 1 July 2017
Place a disposable protective pad underneath the patient’s hips and buttocks and cover area to be exposed.
To reduce potential infection risk caused by soiled linen. To promote dignity of the patient and avoid embarrassment if faecal staining occurs during or after the procedure.
Place lubricating gel onto gloved finger and anus.
To prevent trauma to the anal and rectal mucosa, reducing surface friction (Higgins 2006)
Inform the patient of imminent procedure To ensure the patient is aware that the procedure is about to begin.
Gently insert single gloved finger into the rectum up to the 2nd joint only. Turn the finger so that the padded area is in contact with the bowel wall throughout. (Coggrave et al 2009)
To prevent trauma to the
Gently rotate in a clockwise direction 6-8 times for approximately 10 seconds, or until relaxation of the sphincter felt.
To minimize discomfort and to stimulate peristalsis and promote movement of the stool into the rectum.
Observe the patient throughout the procedure: STOP
If in discomfort
If perianal area bleeding
If patient asks you to
If there are signs and symptoms of Autonomic Dysreflexia.
To note signs of distress, pain, bleeding and general discomfort or Autonomic Dysreflexia.
Gently remove finger and await reflex evacuation of the stool (Coggrave et al 2009)
To promote comfort of the patient
If reflex activity does not occur, repeat every 5-10 minutes until rectum is empty or activity ceases. Do not repeat more than three times if reflex activity does not occur (Coggrave et al 2009)
Digital removal of faeces may be required if faeces felt in the rectum (Coggrave et al)
When completed procedure, clean the perianal area.
To promote comfort and prevent skin excoriation.
Dispose of all equipment as per Handling and Disposal of waste policy, remove gloves and apron and decontaminate hands as per the SHFT Hand Hygiene Procedure.
To ensure staff and patient safety and to prevent infection.
Document all actions and outcomes in patient’s health records.
To comply with NMC Code and SHFT guidelines on documentation
If any abnormality is found ensure an appropriate referral is made in line with local policy
To promote continuity of care and patient safety.
References Higgins, D. (2006) How to administer an enema. Nursing Times, 102(20), 24-25 Kyle, G (2007) Bowel care part 4. Administering an enema. Nursing Times; 103(45), 26-27. Royal College of Nursing (2012) Management of Lower Bowel Dysfunction including DRE &DRF – guidance for nurses. Coggrave et al (2009) Guidelines for the management of Neurogenic Bowel Dysfunction after Spinal Cord injury.

35 Adult Bowel Care Guidelines Version 1 July 2017
Appendix 10
Procedure for Digital Removal of Faeces Action Rationale
Obtain careful history from patient prior to examination, including establishing whether patient has any known allergies.
To assess symptoms, and reduce the risk of allergic reaction.
Ensure Patient is introduced to staff involved in the procedure
Helps reduce anxiety by improving communication.
Explain each step of the procedure to the patient, including potential risks and complications, and also the benefits.
To ensure patient is informed and understands the procedure. Patient information can help to reduce anxiety.
Obtain valid and informed consent and document in patient’s health records. If necessary refer to the Mental Capacity Act 2005, and consider if the examination is in patient’s best interest. Follow the SHFT consent for examination or treatment policy.
To ensure patient is happy for the procedure to take place.
Identify patient by surname, first name and date of birth using open questions checking against NHS number.
To ensure correct identification of the patient.
Clarify if the patient requires a formal chaperone. Follow SHFT Chaperone policy.
It is the patient’s choice to have a chaperone if required. Refer to Chaperone policy.
Ask the patient if they wish to use the toilet prior to undertaking the procedure.
For comfort of the patient.
Ensure the bedpan/commode/toilet is readily available.
To facilitate easy access for defecation ensuring privacy and dignity
Perform physical observations required according to whether an acute intervention or regular ongoing intervention and observe for signs and symptoms of Autonomic Dysreflexia in Spinal cord injured patients. If at any time the heart rate drops, rhythm changes or signs of Autonomic Dysreflexia STOP the procedure
To provide a baseline measurement to assess any changes in the pulse/blood pressure during or after the procedure (RCN 2012). Spinal cord injured patients have frequently been observed for changes in blood pressure without signs and symptoms of Autonomic dysreflexia. Monitoring blood pressure as part of an ongoing intervention is thought to be of little benefit. The Practitioner should observe for signs of potential shock/Autonomic Dysreflexia. (Coggrave et al 2009)
Decontaminate hands prior to the procedure according to SHFT policy Apply single use apron and single use disposable non-sterile gloves
To reduce the risk of transfer of transient micro organisms on the healthworkers hands and to protect the clothing or uniform from contamination

36 Adult Bowel Care Guidelines Version 1 July 2017
Gather and prepare all required equipment for the procedure ensuring patients dignity
To facilitate easier insertion of the finger and reduce sensation and discomfort for the removal of faecal matter (RCN 2012)
Assist the patient to lie on the left side, with knees drawn to the abdomen, and buttocks near the edge of the bed
To promote the stability of the patient and to allow ease of digital rectal stimulation by following the natural anatomy of the colon. (RCN 2012)
Place a disposable protective pad underneath the patient’s hips and buttocks and cover area to be exposed.
To reduce potential infection risk caused by soiled linen. To promote dignity of the patient and avoid embarrassment if faecal staining occurs during or after the procedure.
Place lubricating gel onto gloved finger and anus.
To prevent trauma to the anal and rectal mucosa, reducing surface friction (Higgins 2006)
Inform the patient of imminent procedure To ensure the patient is aware that the procedure is about to begin.
Prior to insertion of gloved finger into the anus, observe area for evidence of skin excoriation, swelling, haemorrhoids, rectal prolapse
May indicate incontinence or pruritus. Swelling may indicate possible mass or abscess. Any abnormalities such as bleeding, discharge or prolapse should be reported to medical staff before any medical examination is undertaken.(RCN2012)
If Scybala type stool felt (Bristol stool type 1) Remove one lump at a time.
In a solid mass, gently push finger into middle of the mass, split it and remove small pieces at a time.
Avoid using a hooked finger to remove faeces.
A period of rest may allow further faecal matter to descend into the rectum.
Use extra lubrication as required
Place faecal matter into receptacle as it is removed.
To minimize discomfort and reduce risk of trauma Use of a hooked finger may cause damage to the rectal mucosa and anal sphincter(RCN2012) To dispose of appropriately.
Observe the patient throughout the procedure: STOP
If in discomfort
If perianal area bleeding
If patient asks you to
If there are signs and symptoms of Autonomic Dysreflexia.
To note signs of distress, pain, bleeding and general discomfort or Autonomic Dysreflexia.
If faecal matter is too hard to break up, or is more than 4cm wide, stop the procedure and discuss with the multidisciplinary team
To avoid unnecessary pain and damage to the anal sphincter.
When the procedure is complete, cleanse the anal area
To make the patient comfortable, prevent irritation , soreness and skin excoriation.
Dispose of all equipment as per Handling and Disposal of waste policy, remove gloves and apron and decontaminate hands as per the SHFT Hand Hygiene Procedure.
To ensure staff and patient safety and to prevent infection.

37 Adult Bowel Care Guidelines Version 1 July 2017
Document all actions and outcomes in patient’s health records.
To comply with NMC Code and SHFT guidelines on documentation
If any abnormality is found ensure an appropriate referral is made in line with local policy
To promote continuity of care and patient safety.
References Higgins, D. (2006) How to administer an enema. Nursing Times, 102(20), 24-25 Kyle, G (2007) Bowel care part 4. Administering an enema. Nursing Times; 103(45), 26-27. Royal College of Nursing (2012) Management of Lower Bowel Dysfunction including DRE &DRF – guidance for nurses. Coggrave et al (2009) Guidelines for the management of Neurogenic Bowel Dysfunction after Spinal Cord injury.
38 Adult Bowel Care Guidelines Version 1 July 2017
39 Adult Bowel Care Guidelines Version 1 July 2017
Referrer’s Details
Referrer Name: Contact Tel:
Date of Referral: Base:
Patient Information
Name:
DOB:
Address:
Contact Tel:
Consultant:
GP’s Details:
Emergency Contact:
Underlying Diagnosis:
Relevant Medical / Surgical History:
Current Relevant Medication:
Reason For Referral:
Has a Bowel Assessment Form been completed?
Has patient consented to procedure?
Had the patient had a DRE?
---- Please delete as appropriate:
Does the patient suffer from Crohn’s or Colitis? Yes No
Has the patient had bowel surgery in the last six months? Yes No
Has the patient been diagnosed as having a bowel malignancy? Yes No
Has the patient experienced rectal bleeding? Yes No
Previous Bowel Investigations? Yes No
If yes, please give details:
Additional information:
Are there any lone worker issues that should be known? Please state:
Peristeen Advisor Referral Form
Please send to: Marian Shannon, Peristeen Advisor Mobile: 07734964445 Email: [email protected] NHS email: [email protected] Fax: 01733 392022

40 Adult Bowel Care Guidelines Version 1 July 2017

Key Messages: Lifestyle advice, - fluid intake, fibre and exercise must be
continued throughout laxative therapy Never use two of the same class of drug (i.e. lactulose and
macrogol) Always use a stimulant first line if drug induced
(esp.opioids) – osmotics will just cause bloating Always add in another laxative type (not replace) as often
the synergistic action of bulking, softening and stimulating is much more effective and lowers the side effects of individual agents.
Gradually titrate dose of laxative upwards or downwards. Adjust constipating medication if possible Titrate to maximum tolerated dose before adding/
switching laxatives. Always consider impaction and overflow if patient
reports diarrhoea whilst taking laxatives
Laxative Treatment Guidelines for Adults
Assessment of the patient identifies constipation
(see continence assessment)
Any RED FLAG or signs of obstruction?
RED FLAGS – General
Persistent unexplained change in bowel habit
Palpable mass in the abdomen or pelvis
Persistent rectal bleeding without anal symptoms
Narrowing of stool calibre
Family history of colon cancer, or inflammatory bowel
disease
Unexplained weight loss, iron deficiency anaemia,
fever, or nocturnal symptoms
Severe, persistent constipation that is unresponsive
to treatment
NO
Patient presents with FAECAL IMPACTION?
YES
Consider high dose macrogol compound oral powder 8
sachets daily for max. 3 days
CONSTIPATION - short term or chronic
Bulk Forming Laxative
E.g. Ispaghula husk. Ensure adequate fluid intake
Bulk Forming Laxative unsuitable,
unable to tolerate or ineffective?
add or switch to
Softener / Stimulant
YES
Softener / Stimulant
unsuitable, unable to tolerate or ineffective?
Soft stools (or hard stools after
a few days treatment with macrogol)?
Consider starting or adding an
Oral Stimulant Laxative
YES
CONSTIPATION - short term or chronic
Refer to GP / Specialist
Healthcare Professional
Has response been sufficient or fast enough?
NO
YES
NO
Add suppositories or a micro-enema
Suppositories: Bisacodyl (soft stools); Glycerol (alone or
with Bisacodyl) (hard stools)
Micro Enema: Docusate or Sodium Citrate may be
repeated for hard impacted faeces
Has patient responded to treatment?
NO
Consider Arachis Oil or Sodium Phosphate Enema
Be aware of contraindications (see Laxative Guide)
Has patient responded to treatment?
NO
SEVERE CONSTIPATION
(resistant to at least 2 laxatives tirated appropriately)
Add Osmotic Laxative
Inform patient to stop laxative
and seek advice in the event of diarrhoea
Has patient responded to treatment?
Maintenance Treament
Review regularly and consider slow withdrawal when
stools are soft and easily passed. Aim for 3 bowel
movements per week.
Refer to GP / Specialist Healthcare Professional
NO
CONSTIPATION – drug induced
Commence laxatives on initiation of high dose opiods
DO NOT USE BULK FORMING LAXITIVES
Use softeners for hard stools,
use stimulants for stools not expelled
(Patients taking regular opioids usually start with stimulant
of increasing dose according to effect/tolerability and may
require a softener if stimulant alone is ineffective or stools
become hard. Often both are required).
See Palliative Care Handbook/palliative specialist teams.
YES
YES
Neruological / MS / Stroke / Spinal Injuries etc.
These patients may require a more complicated regime
including rectal stimulation and digital removal of faeces.
Over-use of traditional laxatives (especially osmotics) can
result in faecal incontinence. Seek advice from their
specialist team or the continence service.
Lifestyle advice –
patient leaflet
APPENDIX 12

Bulk Forming Laxatives
Examples Bran, Ispaghula Husk (Fybogel, Isogel, Regulan), Methylcellulose, Sterculia (Normacol
How it Works By absorbing water, expanding and softening the stool. Increased bulk promotes peristaltic action, and decreases transit time, which in turn reduces the amount of water absorbed by the colon
Extra measures Fluid intake must be increased when taking these medications
Side effects May cause abdominal distention and/or flatulence
Contra-indications Not to be used in cases of intestinal obstruction Not to be used in patients with severe slow transit constipation – they add more load to an inefficient bowel and cause more symptoms
Stimulant laxatives (can cause abdominal cramps due to increased intestinal motility. They generally act by stimulating nerves to induce peristalsis, and they also decrease water reabsorption from the colon)
Examples Route Acts within
Extra Measures & Contra-indications
Bisacodyl Oral or rectal (supps or liquid)
10-12 Hours
Oral medication should not be used for long term treatment, which could cause loss of tone on the colon and hypokalaemia (low potassium) Not to be used in cases of intestinal obstruction e.g. faecal impaction
Senna Oral 10-12 hours
May cause the urine to be coloured brown or red Not to be used in cases of intestinal obstruction Not to be used for long term treatment, which could cause loss of tone on the colon and hypokalaemia (low potassium)
Dantron (Danthron) Co-danthramer, Co-danthrusate, Normax
Oral 6-12 Hours
Should be limited to use by terminally ill patients per license and BNF Not to be used in patients with intestinal obstruction Use with caution in people with incontinence as can irritate the skin when leaving the body Can cause red/orange colour to the urine
Docusate Sodium Oral or rectal 24-48 Hours
Has detergent and emulsifying properties which also soften the stool. Not to be used in patients with intestinal obstruction Not to be used long term Can cause abdominal cramps
Glycerol Rectal Suppositories
20 Minutes Lubricate the anorectum Mild irritant effect which stimulates defaecation. There are no significant side-effects or contraindications for their use
Sodium Picosulphate Oral: Picolax Usually Within 3 Hours of first dose
Often used for bowel evacuation prior to investigations or surgery Not to be used for intestinal obstruction or for long term use Side effects include nausea, vomiting and abdominal cramps.
Osmotic Laxatives
Examples Route Acts Within
Extra measures & Contra-indications
Lactulose Oral Approx 48 Hours Accumulative
Broken down to form lactic and acetic acids in the colon, which stimulate peristalsis Osmotic effect which draws water into the stool, leading to softer stools Not to be used in patients with abdominal obstruction Can cause flatulence and abdominal cramps Fluid intake must be increased when taking these medications
Macrogols (e.g. Movicol) Oral 24-48 Hours Causes distention and stimulation of the bowel Less side effects than other medications in this group Reduces the need to strain Safe to use in patients with faecal impaction Can alter the dose according to stool type Fluid intake must be increased when taking these medications
Magnesium salts: Magnesium Hydroxide
Oral Can be within 2 Hours
Rarely used Attract water into the bowel, increasing the volume of the stool, keeping it moist, and also stimulates peristalsis Only for short term use for rapid evacuation of the bowel Not to be used for intestinal obstruction Avoid dehydration, maintain oral fluids
Rectal phosphates Rectal suppositories or enemas
Within 30 minutes
Have a direct osmotic and stimulant effect Only for short term use to produce rapid bowel evacuation Not to be used in patients with abdominal obstruction or acute gastrointestinal conditions Not for use in patients with a neurogenic bowel.
Rectal Sodium citrate: Microlette, Microlax, relaxit Micro-enema
Administered as an enema
Within 30 Minutes
Only for short term use to produce rapid bowel evacuation Not to be used in patients with abdominal obstruction or acute gastrointestinal conditions Care should be taken in patients where sodium salts are contraindicated e.g. Cardiac Failure
Stool Softeners (See also bulk forming laxatives and Docusate Sodium)
Example Route Acts within
Extra measures & Contra-indications
Arachis oil Rectal 12-72 Hours Derived from peanuts – DO NOT GIVE TO PATIENTS WITH NUT ALLERGY Effective in softening the stool in cases of impaction. May increase uptake of and toxicity of drugs, and interfere with absorption of fat-soluble vitamins (Wiesel and bell, 2004) Oral faecal softeners are often viewed as unproved and unsafe, discouraging use (Wiesel and Bell, 2004) Administer before bedtime
There are also a number of newer medicines for constipation, which work differently to the groups above. These don't all necessarily work by their direct effect on the gut. These include Prucalopride, Lubiprostone, and Linaclotide. NB: There are differences in the licenses for these medicines relating to duration of use and criteria for their discontinuation.
Prucalopride: (NICE TA 211) Restricted to use when at least 2 laxatives from different classes have been ineffective at maximum tolerated doses for at least 6 months. Works on the muscle wall of the bowels. It increases the movement of the bowels, making stools easier to pass. It can be helpful for patients for whom constipation remains a problem despite having made changes to lifestyle and diet, and despite having tried several different laxatives.
Lubiprostone: (NICE TA 318) Restricted to use when at least 2 laxatives from different classes have been ineffective at maximum tolerated doses for at least 6 months. Helps to increase secretion of fluid into the bowel. This increases the movement of the bowels, making stools easier to pass. It is helpful for people for whom constipation remains a problem despite recommended changes to lifestyle or diet.
Linaclotide: (NICE CG 61) Consider for people with IBS only if: optimal or maximal tolerated doses of previous laxatives from different classes have not helped; and they have had constipation for at least 12m. Follow-up for people taking linaclotide must take place after 3 months.

43 Adult Bowel Care Guidelines Version 1 July 2017
APPENDIX 13
Management of lower bowel dysfunction, including DRE and DRF RCN Guidelines (2012)
RCN Guidelines.pdf
APPENDIX 14
Guidelines for Management of Neurogenic Bowel dysfunction in individuals with Central Neurological
conditions MASCIP (2012)
MASCIP Guidelines.pdf
Please refer to SHFT website for printable copies