adhd child to adult cindy ruttan do 2008 kansas osteopathic conference kansas osteopathic conference...
TRANSCRIPT

ADHD Child to AdultADHD Child to Adult Cindy Ruttan DO 2008Cindy Ruttan DO 2008
Kansas Osteopathic ConferenceKansas Osteopathic Conference
OVPK KS OVPK KS

Key points to coverKey points to cover Symptoms/ HistorySymptoms/ History Who it effects-agesWho it effects-ages Collecting informantsCollecting informants Rule out diagnosisRule out diagnosis Treatment optionsTreatment options
Behavioral Behavioral MedicationsMedications

ADHD is like---ADHD is like---
I stopped to think, and forgot to I stopped to think, and forgot to start again.start again.
I was trying to daydream, but my I was trying to daydream, but my mind kept wanderingmind kept wandering. .

What is ADHD ?What is ADHD ?
Neuro- Behavioral Disorder Neuro- Behavioral Disorder Inattention-( executive functions) Inattention-( executive functions) HyperactivityHyperactivity ImpulsivityImpulsivity
Speculate: Dopamine and NE Speculate: Dopamine and NE dysregulationdysregulation
Affects 7-12% of pediatric group Affects 7-12% of pediatric group pop.pop.
High chance for Co-morbidityHigh chance for Co-morbidity Costly due to ER use, injury and Costly due to ER use, injury and Hospital useHospital use..

ADHD Review HistoryADHD Review History
Core criteria DSM-III: Core criteria DSM-III: 3 separate symptom 3 separate symptom areasareas
DSM-III-R DSM-III-R one long list one long list
DSM-IV DSM-IV two core dimensionstwo core dimensions

ADHD and DSM IV criteriaADHD and DSM IV criteria
Concerned by …may change in Concerned by …may change in future DSM’s.future DSM’s.
1.1. Age of onset- ? 7 yearsAge of onset- ? 7 years
2.2. Age appropriate Symptoms are Age appropriate Symptoms are needed for helping diagnose needed for helping diagnose disorder from Child/ Adol/ disorder from Child/ Adol/ AdultsAdults
3.3. Various inputs needed –they Various inputs needed –they can conflictcan conflict

MOATMOATADHD DiagnosisADHD Diagnosis MMovement excessive ovement excessive (Hyperactive)(Hyperactive)
OOrganization problems rganization problems (difficulty finishing (difficulty finishing tasks)tasks)
AAttention problemsttention problems TTalking impulsivelyalking impulsively
Meet criteria of 6 of 9 symptoms, present prior to age 7yrs and Meet criteria of 6 of 9 symptoms, present prior to age 7yrs and present in 2 or more settings.present in 2 or more settings.
The Psychiatric Interview 2The Psychiatric Interview 2ndnd ed Carlat ed Carlat

Children's ADHDChildren's ADHD Review of past 10 yearsReview of past 10 years
Reviews in Child Adolescent Reviews in Child Adolescent Psychiatry (Williams and Psychiatry (Williams and Wilkins) Pg 9-17. by Wilkins) Pg 9-17. by Dennis Cantwell MDDennis Cantwell MDReprint from the J. of Reprint from the J. of the American Academy of the American Academy of Child and Adolescent Child and Adolescent PsychiatryPsychiatry..

ADHD Natural HxADHD Natural Hx 30% Developmental Delay30% Developmental Delay 40% Continual Display40% Continual Display
Internalizing disordersInternalizing disordersDepression Depression AnxietyAnxiety
30% Developmental Decay30% Developmental DecayExternalizing disordersExternalizing disorders
ODDODDCDCD

ADHD info from 10 year ADHD info from 10 year reviewreview Core symptoms may change over Core symptoms may change over time. Consider the younger one time. Consider the younger one presented the more persistent presented the more persistent diagnosis and the older one is diagnosis and the older one is diagnosis the fewer symptoms diagnosis the fewer symptoms that are present.that are present.
Examples Include:Examples Include: Temper outburstsTemper outbursts Aggressive argumentative Aggressive argumentative behaviorbehavior
Fearless Fearless Sleep disturbanceSleep disturbance

Diagnostic concerns…Diagnostic concerns… Can one diagnosis contribute to all Can one diagnosis contribute to all
symptoms reported?symptoms reported? Can you be observing more than one Can you be observing more than one
disorder?disorder? ADHD –diagnosis of exclusion.ADHD –diagnosis of exclusion.
considerconsider: Hyper behavior and Mania/ : Hyper behavior and Mania/ Hypomania Hypomania Decreased focus/inattention Decreased focus/inattention with Depression with Depression

ADHD Co morbiditiesADHD Co morbidities CDCD
Possible reduction in Substance Abuse Disorder Possible reduction in Substance Abuse Disorder ( Drugs and ETOH) if treated early for ADHD ( Drugs and ETOH) if treated early for ADHD with Stimulantswith Stimulants
ODDODD LDLD Anxiety 20-40%Anxiety 20-40%
OCD increase up to 11%^OCD increase up to 11%^ Tourette’s-rare (usually reverse) / TicTourette’s-rare (usually reverse) / Tic
Tic 10-15%^ Tic 10-15%^ Mood Disorder 5-40% depressionMood Disorder 5-40% depression
Bipolar 10-22%^ Bipolar 10-22%^ Poor interpersonal skills/demoralizedPoor interpersonal skills/demoralized
David Krefetz DO MBA FACN, FAPA David Krefetz DO MBA FACN, FAPA ADHD with Comorbidity in Pediatric Populations:ADHD with Comorbidity in Pediatric Populations: Impllications for Eval and Management ^Impllications for Eval and Management ^

DBD (Disruptive BehaviorDBD (Disruptive Behavior Disorder)Disorder)
refers to the refers to the Comorbidity diagnosis of ODD/CDComorbidity diagnosis of ODD/CD
Worry about aggression and Worry about aggression and delinquencydelinquency
Academic underachievementAcademic underachievementIncreased risk for substance abuseIncreased risk for substance abuseIncreased social maladaptationIncreased social maladaptationNote having both DBD and ADHD Note having both DBD and ADHD
makes the ADHD harder to treat.makes the ADHD harder to treat.NO medications FDA approved NO medications FDA approved
for ODD/ CDfor ODD/ CD

Learning DisordersLearning Disorders
InputInput Process of getting info into the brainProcess of getting info into the brain
IntegrationIntegration Organization and understandingOrganization and understanding
MemoryMemory Storage of info to retrieve laterStorage of info to retrieve later
OutputOutput Communicate from brain to others or put Communicate from brain to others or put
into action in the environmentinto action in the environment
ADHD and LD Booklet for Parents by Larry B Silver MDADHD and LD Booklet for Parents by Larry B Silver MD

Input DisabilityInput Disability
Visual PerceptionVisual Perception Auditory PerceptionAuditory Perception Auditory Lag Auditory Lag (Auditory (Auditory Processing )Processing )
ADHD and LD Booklet for Parents by Larry B Silver MDADHD and LD Booklet for Parents by Larry B Silver MD

Integration DisabilityIntegration Disability
SequencingSequencingAbstractionAbstractionOrganizationOrganizationMemoryMemory
ADHD and LD Booklet for Parents by Larry B Silver MDADHD and LD Booklet for Parents by Larry B Silver MD

Output DisabilityOutput Disability
Language Language MotorMotor
GrossGrossFineFineADHD and LD Booklet for Parents by Larry B Silver MDADHD and LD Booklet for Parents by Larry B Silver MD

DiagnosingDiagnosing ADHDADHD NO lab tests, or psychologic tests NO lab tests, or psychologic tests
that definitely diagnose.that definitely diagnose. Recommend Academic Testing to Recommend Academic Testing to
establish level in school and any establish level in school and any LD’s.LD’s.
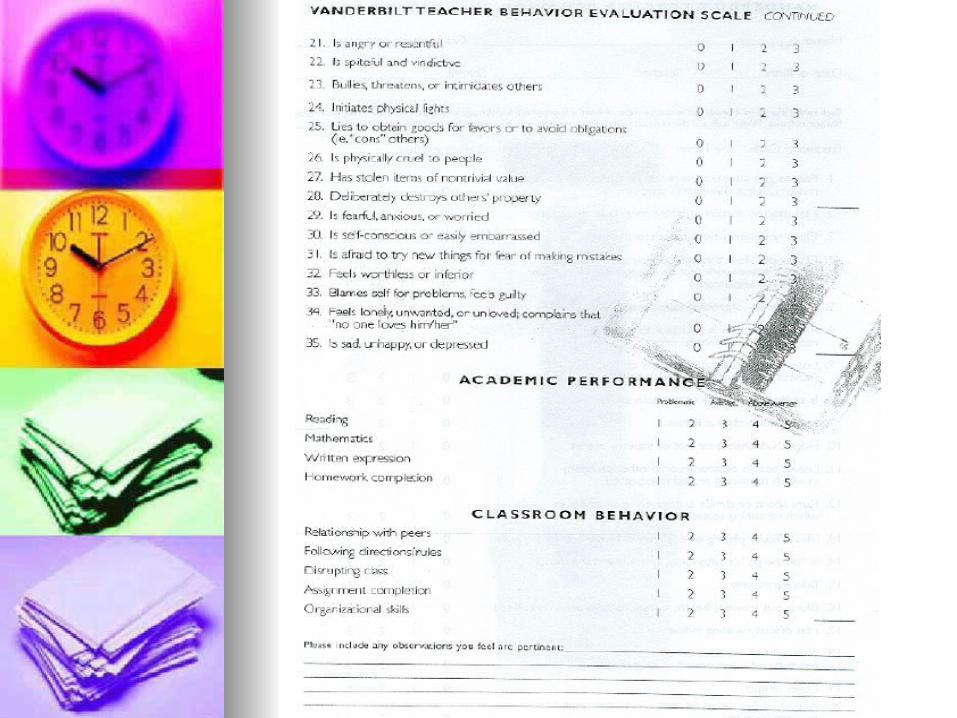
Obtain Conners Forms or Obtain Conners Forms or Vanderbuilt Scales that help with Vanderbuilt Scales that help with defining criteria –or use the DSM IV defining criteria –or use the DSM IV criteria.criteria.
TOVA or CPT may help with TOVA or CPT may help with identification of ADHD symptoms identification of ADHD symptoms and how well the meds are working.and how well the meds are working.

Early Medical interventionEarly Medical interventionwith Medication has shown:with Medication has shown:
For individuals with ADHD in For individuals with ADHD in childhood to decrease the risk for childhood to decrease the risk for subsequent non-nicotine SUD in subsequent non-nicotine SUD in adol and early adulthood. adol and early adulthood.
? (Worked best for those with the milder ? (Worked best for those with the milder form of ADHD)form of ADHD)
A Literature Review Series Vol 1 No. 3A Literature Review Series Vol 1 No. 3

Children with ADHD at risk for Children with ADHD at risk for ETOH problemsETOH problems ADHD is a risk factor for ETOH ADHD is a risk factor for ETOH
problems –parental behaviors and problems –parental behaviors and environmental stress contribute too.environmental stress contribute too. More likely to drink heavy and to have More likely to drink heavy and to have
enough problems to diagnose ETOH enough problems to diagnose ETOH Abuse or Dependency.Abuse or Dependency.
onset average age 15 onset average age 15 Consider a possible subset of ADHD Consider a possible subset of ADHD
disorder with antisocial behavior patternsdisorder with antisocial behavior patterns ETOH and ADHD seem to run in ETOH and ADHD seem to run in
families which thus seem to be under families which thus seem to be under more “stress” situations.more “stress” situations.
Addiction Science Made Easy 4-8-07Addiction Science Made Easy 4-8-07 WWW.NATTC.orgWWW.NATTC.org

Young Adults –college ageYoung Adults –college age
Problems noted:Problems noted: Harder to adjust to adult life, college life with Harder to adjust to adult life, college life with
poorer social skills and less self esteem.poorer social skills and less self esteem. Lower GPA, less financially, inc. school drop outLower GPA, less financially, inc. school drop out Less methodical, inc. procrastination, less self Less methodical, inc. procrastination, less self
control/self disciplinary behaviors control/self disciplinary behaviors
Symptoms look differentSymptoms look different Impulsive and hyper = mental restlessness or Impulsive and hyper = mental restlessness or
subjective feelings of such.subjective feelings of such.

Adult ADHDAdult ADHD
Nature of disorder is disorganized, Nature of disorder is disorganized, forgetful and poor self regulation forgetful and poor self regulation
Majority can not remember to take Majority can not remember to take their medication if on IR or multi their medication if on IR or multi doses needed.doses needed. InconvenienceInconvenience EmbarrassedEmbarrassed Safety and long term effectsSafety and long term effects Different feeling…Different feeling…

Adult ADHDAdult ADHD
Basic same core symptoms as Basic same core symptoms as with Peds ADHDwith Peds ADHD
Review HX of Ed, job and Review HX of Ed, job and familyfamily
Standard rating Standard rating scales/specific for ADULTS scales/specific for ADULTS
Collateral info coping Collateral info coping /stressors/stressors
Rule out other diagnosisRule out other diagnosis Review options for Review options for
Treatment as they match Treatment as they match patient goalspatient goals Meds/ CBTMeds/ CBT


Adult ADHD who had Adult ADHD who had diagnosis as childdiagnosis as child Many loose full diagnostic Many loose full diagnostic
status( functional remission)10% vs status( functional remission)10% vs Persistent ADHD at15% by 25 yrs Persistent ADHD at15% by 25 yrs old.old.
reality is ADHD had remitted only for reality is ADHD had remitted only for a minority.a minority.
Inattentiveness remains when Inattentiveness remains when inattention and Hyperactivity decline.inattention and Hyperactivity decline.
If one put partial remission + Persistant If one put partial remission + Persistant = 65% have symptoms of ADHD.= 65% have symptoms of ADHD.

Functional ImpairmentFunctional Impairment
Lower Socioeconomic Lower Socioeconomic Relationship impairedRelationship impaired Dec. academic accomplishmentsDec. academic accomplishments Employment issuesEmployment issues Driving record badDriving record bad Dating, vol. work, community Dating, vol. work, community
service, socializing with friends service, socializing with friends /family, culture and educational out /family, culture and educational out of school activities limited. of school activities limited.

Adult ADHD cont-Adult ADHD cont-
Common Common Maladaptive Maladaptive Beliefs:Beliefs:
Self mistrustSelf mistrust FailureFailure InadequateInadequate IncompetentIncompetent InstabilityInstability
Common Common Dysfunctional Dysfunctional Coping Behaviors Coping Behaviors seen: seen:
AvoidanceAvoidance Procrastination Procrastination Pseudo efficiency Pseudo efficiency
low priority tasks low priority tasks first then high first then high priority tasks last.priority tasks last.
Busy without Busy without completion of completion of thingsthings

Co morbidity is “The RULE” Co morbidity is “The RULE” with Adult ADHDwith Adult ADHD
Mood Disorders—Mood Disorders—50-60%50-60%
Depression-Depression-recurrentrecurrent
BADBAD
CyclothymiaCyclothymia
DysthymiaDysthymia
DEP NOSDEP NOS
Anxiety DisordersAnxiety Disorders
40-50%40-50%
GADGAD
Anxiety NOSAnxiety NOS

Co morbidity cont-Co morbidity cont-Adult ADHDAdult ADHDVarious % Various % SUDSUD LDLD IEDIED TouretteTourette Antisocial Personality DisorderAntisocial Personality Disorder Borderline Personality DisorderBorderline Personality Disorder Dependent Personality DisorderDependent Personality Disorder

Behavioral Behavioral InterventionsInterventions

Treatment Options Treatment Options withwith or or withoutwithout medications 1 medications 1 PraisePraise reward positive reward positive
behaviors by : behaviors by : verbalize itverbalize it
Speak individual / publicSpeak individual / public Write it Write it Reward itReward it
Physical Activity -participationPhysical Activity -participation Material - for doing good job in classMaterial - for doing good job in class
Dec / Jan 2008 ADDitude Magazine pg 49Dec / Jan 2008 ADDitude Magazine pg 49

Cont: Treatment Options Cont: Treatment Options with or or withoutwithout Medication 2 Medication 2 Follow up with teachers regarding childs Follow up with teachers regarding childs
Positive and Negative attributesPositive and Negative attributes. Keep . Keep open communication.open communication.
Make sure IEP/504 is being used.Make sure IEP/504 is being used. Address LD issues and grade Address LD issues and grade
appropriate level of work in sinkappropriate level of work in sink Do help at home with homework or Do help at home with homework or
working ahead if possible/ tutorworking ahead if possible/ tutor
Dec / Jan 2008 ADDitude Magazine pg 49Dec / Jan 2008 ADDitude Magazine pg 49

Cont: Treatment Options Cont: Treatment Options with or or withoutwithout Medication 3 Medication 3 Encourage routine healthy food and snacks –due Encourage routine healthy food and snacks –due
to side effects form medicationsto side effects form medications Peanut butter / double up on Breakfast drinkPeanut butter / double up on Breakfast drink
Consider type and delivery style of medications Consider type and delivery style of medications including time frame medications given and duration including time frame medications given and duration of actionof action
Keep structured as possible and avoid chaotic Keep structured as possible and avoid chaotic situations-you as a parent stay calm, cool and situations-you as a parent stay calm, cool and collected.collected.
Give yourself time to accomplish the task/ goal Give yourself time to accomplish the task/ goal desired. Keep a Daytimer/ planner if neededdesired. Keep a Daytimer/ planner if needed
Give an exercise break Give an exercise break
Dec / Jan 2008 ADDitude Dec / Jan 2008 ADDitude Magazine pg 49Magazine pg 49

Cont: Treatment Options Cont: Treatment Options with or or withoutwithout Medication 4 Medication 4 Use verbal and non-verbal cues to Use verbal and non-verbal cues to
remind or stay focusedremind or stay focused Keep good sleep hygiene. Insomnia Keep good sleep hygiene. Insomnia
is common with ADD/ ADHD either a is common with ADD/ ADHD either a part of the disorder itself or part of the disorder itself or exacerbated by medicationsexacerbated by medications
Try to avoid arguments and Try to avoid arguments and confrontations leading to poor self confrontations leading to poor self esteemesteem
Dec / Jan 2008 ADDitude Magazine pg 49Dec / Jan 2008 ADDitude Magazine pg 49

Therapy Goal:Therapy Goal:
Sensitize the patient to and Sensitize the patient to and interrupt dysfunctional behaviorsinterrupt dysfunctional behaviors Coping skillsCoping skills Problem focused Problem focused Adaptive thinkingAdaptive thinking Anger managementAnger management Communication skillsCommunication skills

RX TreatmentsRX Treatments

Medication OptionsMedication Options
19 meds are FDA approved19 meds are FDA approved18 are stimulants18 are stimulants
Use Lowest Dose which addresses Use Lowest Dose which addresses symptoms—as one increases dose if symptoms—as one increases dose if no improvement noted than lowest no improvement noted than lowest dose which provided improvement is dose which provided improvement is the best dose.the best dose.
List symptoms from patients concern List symptoms from patients concern then family and compare… may not then family and compare… may not agree.agree.

Medication DiversionMedication Diversion Transfer of meds from one it is prescribed to Transfer of meds from one it is prescribed to
one whom it is not.one whom it is not. Taking more (quantity)Taking more (quantity) misuse for Euphoric desiremisuse for Euphoric desire Combo with other substancesCombo with other substancesStudy of those Diagnosed with ADHD and its Study of those Diagnosed with ADHD and its
misuse:misuse:22% of adol and young adults in study misused 22% of adol and young adults in study misused
in some capacity.in some capacity.ADHD patients Sold it more than the non ADHD patients Sold it more than the non ADHD group. Those who sold had comorbid ADHD group. Those who sold had comorbid diagnosis of SUD and CD.diagnosis of SUD and CD.
IR prep most often divertedIR prep most often diverted
A Literature Review Series Vol 1 No. 3 Pg 19-21A Literature Review Series Vol 1 No. 3 Pg 19-21

MedicationsMedications
StimulantsStimulants Short Short IntermediateIntermediate Long Long Transdermal Transdermal
Stimulant Pro DrugsStimulant Pro Drugs Non StimulantsNon Stimulants
SNRI SNRI Adrenergic AgentsAdrenergic Agents AntidepressantsAntidepressants Dopaminergic AgentsDopaminergic Agents

Stimulants FDA ApprovedStimulants FDA Approved
Adult FDA Approved is in BLUEAdult FDA Approved is in BLUE Amphetamine Amphetamine
AdderallAdderall DexedrineDexedrine DextrostatDextrostat Adderall XR 2004Adderall XR 2004 Dexedrine SpanulesDexedrine Spanules
Not recommended under age 3 yrsNot recommended under age 3 yrs

Stimulants cont-Stimulants cont-FDA approvedFDA approved
MethylphenidateMethylphenidate RitalinRitalin Methylin chewable, Oral solMethylin chewable, Oral sol Metadate ERMetadate ER FocalinFocalin Focalin XR 2005Focalin XR 2005 Methylin ERMethylin ER Ritalin SRRitalin SR Metadate CDMetadate CD Ritalin LA Ritalin LA ConcertaConcerta
Not recommended for children under age 6Not recommended for children under age 6
MethylphendateTransdermal PatchMethylphendateTransdermal Patch
New Stimulant Delivery New Stimulant Delivery
OptionOption

Transdermal Methylphenidate PatchTransdermal Methylphenidate Patch
Daytrana Daytrana FDA approved ages 6-12FDA approved ages 6-12 10,15, 20 and 30 mg10,15, 20 and 30 mg Recommended one patch dailyRecommended one patch daily Start with the 10 mg patch if no improvement in 1 Start with the 10 mg patch if no improvement in 1
week increase-- cont to adjust dose per 1 week week increase-- cont to adjust dose per 1 week intervals.intervals.
Location hip (rotate area/ sides) may cause irritation Location hip (rotate area/ sides) may cause irritation Delivered over 9 hoursDelivered over 9 hours Possibly effects initial height but minimal to not Possibly effects initial height but minimal to not
significant in adulthoodsignificant in adulthood Much the same side effect profile as oral agentsMuch the same side effect profile as oral agents Remove 2 hours prior to effectsRemove 2 hours prior to effects wearing off.wearing off.
Current Psychiatry Vol 5 No.6 / June 2006Current Psychiatry Vol 5 No.6 / June 2006

Stimulant Pro DrugStimulant Pro Drug
Vyvanse - LisdexamfetamineVyvanse - Lisdexamfetamine FDA approvedFDA approved for for ages 6-12ages 6-12
30, 50, and 70 mg capsules30, 50, and 70 mg capsules
Start with 30 mg/day. If needed titrate up with Start with 30 mg/day. If needed titrate up with 20mg every 3-7 days as tolerated to max of 70 20mg every 3-7 days as tolerated to max of 70 mg/daymg/day
1.1. Effect about 12 hoursEffect about 12 hours2.2. Steady state in 2-3 daysSteady state in 2-3 days3.3. Half life 9.5 hoursHalf life 9.5 hours
Current Psychiatry Vol.6 no.6 June 2007Current Psychiatry Vol.6 no.6 June 2007

Vyvanse – Vyvanse – Lisdexamfetamine cont-2Lisdexamfetamine cont-2Blocks NE and Dopamine reuptake in Presyn Blocks NE and Dopamine reuptake in Presyn
neuronneuronNoted improvement 2 hrs after dosing.Noted improvement 2 hrs after dosing.Large change in corrected QTC intervals--? Large change in corrected QTC intervals--?
Need more info about cardiac riskNeed more info about cardiac risk Possibly Less risk for abuse at Possibly Less risk for abuse at
recommended doses—may be misused at recommended doses—may be misused at higher than therapeutic doses.higher than therapeutic doses.
Current Psychiatry Vol.6 no.6 June 2007Current Psychiatry Vol.6 no.6 June 2007

Vyvanse – Vyvanse – Lisdexamfetamine cont-3Lisdexamfetamine cont-3 Caution in Patients:Caution in Patients:
Co morbid eating Co morbid eating Sleep disorderSleep disorder HTN or cardiovascular illnessHTN or cardiovascular illness
Monitor HR and BPMonitor HR and BP
Do not prescribe to patients taking Do not prescribe to patients taking MAOIMAOI or who or who have taken one in 2 have taken one in 2 weeks of the presentation.weeks of the presentation.
Current Psychiatry Vol.6 no.6 June 2007Current Psychiatry Vol.6 no.6 June 2007

Stimulant: side effectsStimulant: side effects
Review Black Box WarningsReview Black Box Warnings regarding CV risks and Sudden regarding CV risks and Sudden Death.Death.
Encourage Food prior to taking Encourage Food prior to taking MedicationsMedications
Understand possibility of PsychosisUnderstand possibility of Psychosis May make Mania or Tics worseMay make Mania or Tics worse Can write for 90 day RXN as of Dec Can write for 90 day RXN as of Dec
0707

Stimulant Black Box WarningsStimulant Black Box Warnings
Pre-existing Cardiac Pre-existing Cardiac abnormality, abnormality, cardiomyopathy, arrythmias, cardiomyopathy, arrythmias, or other disorders which or other disorders which the use of a the use of a sympathomimetic could be sympathomimetic could be dangerous or increase the dangerous or increase the vulnerability of patients vulnerability of patients liveslives.. Murmurs, syncopy history, HTNMurmurs, syncopy history, HTN
Consult Cardiology to be safe.Consult Cardiology to be safe. Current Psychiatry Vol. 5 No. 10 / Oct 2006Current Psychiatry Vol. 5 No. 10 / Oct 2006

STRATTERA = STRATTERA = Atomoxetine 2002Atomoxetine 2002
FDA approved for: FDA approved for: ChildChildAdolAdoladultadult

SNRISNRI – –AtomoxetineAtomoxetine Non Stimulant --FDA Approved Non Stimulant --FDA Approved Full effect 3-7 weeks peak levels 1-2 hrs or Full effect 3-7 weeks peak levels 1-2 hrs or
3-4 for slow metabolizers3-4 for slow metabolizers Shorter sleep latency , improved sleepShorter sleep latency , improved sleep Increased risk of suicidal ideation in Increased risk of suicidal ideation in
children and adolescents (see precautions)children and adolescents (see precautions) Dose by Body Weight.Dose by Body Weight.
Do not exceedDo not exceed 1.4 mg/kg/day or 100 mg 1.4 mg/kg/day or 100 mg whichever is less.whichever is less. Start low go slow (start Start low go slow (start 0.5mg/kg/day for 10 day then 0.8 for 10 days 0.5mg/kg/day for 10 day then 0.8 for 10 days then 1.2 in a individual or BID dose)then 1.2 in a individual or BID dose)
Over 70 kg start at 40 mg dose and increase Over 70 kg start at 40 mg dose and increase after 10 days to 60 mg for 10 days then to 80mg after 10 days to 60 mg for 10 days then to 80mg after 2-4 weeks consider max dose at 100 mg/ after 2-4 weeks consider max dose at 100 mg/ day. day.

Cont:SNRICont:SNRI - -AtomoxetineAtomoxetine
Safety not established under age 6 yearsSafety not established under age 6 years Lower dose if a slow CYP2D6 metabolizer Lower dose if a slow CYP2D6 metabolizer
or go slower to increase after 4 weeks if on or go slower to increase after 4 weeks if on another drug which also uses/ inhibits 2D6another drug which also uses/ inhibits 2D6
Modify dose by 50-25 % theraputic dose if Modify dose by 50-25 % theraputic dose if hepatic issues hepatic issues
Monitor BP,hepatic dysfunction,CV issues Monitor BP,hepatic dysfunction,CV issues always review the Adv. Effects list.always review the Adv. Effects list.
Monitor BPMonitor BP Adults with more Anxiety, emotional Adults with more Anxiety, emotional
dysregulationdysregulation

Cont:SNRICont:SNRI - -AtomoxetineAtomoxetine
Adults start with 40 mg then in 3 Adults start with 40 mg then in 3 days increase to 80 mg either in days increase to 80 mg either in one AM dose or split dose 40 one AM dose or split dose 40 bid. Max is 100mg.bid. Max is 100mg.

Adrenergic OptionsAdrenergic Options Not FDA approved in children Not FDA approved in children or Adolescentsor Adolescents Clonidine Clonidine
Helps with impulsivity, insomnia associated with Helps with impulsivity, insomnia associated with Stimulant meds, hyperarousal, agitation, and tic Stimulant meds, hyperarousal, agitation, and tic disorderdisorder
Oral and transdermal patchOral and transdermal patch
Side affects:Side affects: Sedation daytime if dosed in daytime.Sedation daytime if dosed in daytime. Withdrawl hypertensive episodesWithdrawl hypertensive episodes 5 reported sudden deaths5 reported sudden deaths when used in when used in
combo with stimulantscombo with stimulants

Adrenergic OptionsAdrenergic Options Not FDA approved in children Not FDA approved in children or Adolescentsor Adolescents GuanfacineGuanfacine
Similar to Clonidine in it’s usesSimilar to Clonidine in it’s uses Less sedation and hypotension than Less sedation and hypotension than
ClonidineClonidine Not recommended or use with caution in Not recommended or use with caution in
patients with renal insufficiencypatients with renal insufficiency Refractory ADHD with Tic issues, may Refractory ADHD with Tic issues, may
help with nightmares associated with help with nightmares associated with PTSDPTSD
Always read Adverse Effects, Always read Adverse Effects, contraindications and Precautions in contraindications and Precautions in the package insertsthe package inserts
AntidepressantsAntidepressants: : Not FDA Not FDA approved in children/adolecents for approved in children/adolecents for ADHD treatment nor Adults for ADHDADHD treatment nor Adults for ADHD Buproprion max 450 mg/ day in Buproprion max 450 mg/ day in
Divided dose unless using 300XL for Divided dose unless using 300XL for Once daily dosing.Once daily dosing. 50 % or adult respond50 % or adult respond HA, Dry mouth, nausea, insomniaHA, Dry mouth, nausea, insomnia
Venlafaxine prelim studies suggest Venlafaxine prelim studies suggest efficacy efficacy
TCA’s (Amitriptyline, desipramine, TCA’s (Amitriptyline, desipramine, imipramine,nortriptyline)imipramine,nortriptyline)
MAOI’s open label suggest improved MAOI’s open label suggest improved concentration in children with ADHDconcentration in children with ADHD

Dopaminergic Agents: Dopaminergic Agents: Not FDA Not FDA approved in Adults or children **approved in Adults or children **
Cholinergic Agents:Cholinergic Agents:Not FDA Not FDA approved in Adults or children *approved in Adults or children *
Modafinil** Modafinil** Donepezil* Donepezil*

Herbal and Natural Products:Herbal and Natural Products:Not FDA approved in Adults or Not FDA approved in Adults or children for ADHDchildren for ADHD Ginko BilobaGinko Biloba Omega 3 Fatty AcidsOmega 3 Fatty Acids Vitamins/MineralsVitamins/Minerals
ZincZincIronIron

Treatment Summary Treatment Summary
RX treatment optimal and better RX treatment optimal and better for core symptoms than for core symptoms than Behavioral treatment alone.Behavioral treatment alone.
Combo of RX and Behavioral Combo of RX and Behavioral was superior to either alone.was superior to either alone.

Can meet someone, fall deeply in love,
marry, fight, hate, and divorce,
all in about 35 minutes or less.
Clinical Practice GuidelinesClinical Practice Guidelines CPG’s CPG’s www.pediatrics.org/cgi/content/full/105/5/11www.pediatrics.org/cgi/content/full/105/5/11
5858 www.aacap.org/galleries/practiceParametewww.aacap.org/galleries/practiceParamete
rs/New_ADHD_Parameter.pdfrs/New_ADHD_Parameter.pdf
Valid rating scale:Valid rating scale: VanderbuiltVanderbuilt Conners FormsConners Forms www.massgeneral.org/schoolpsychiatry/screeningtoowww.massgeneral.org/schoolpsychiatry/screeningtoo
ls_table.aspls_table.asp www.med.nyu.edu/psych/assets/adhdscreen18.pdfwww.med.nyu.edu/psych/assets/adhdscreen18.pdf
Vol. 6 No. 4 /April 2007Vol. 6 No. 4 /April 2007

ReferencesReferences The Psychiatric Interview 2The Psychiatric Interview 2ndnd Ed. Carlat Ed. Carlat Dec/Jan2008ADDitude MagazineDec/Jan2008ADDitude Magazine Clinical Handbook of Psychotropic Drugs for Clinical Handbook of Psychotropic Drugs for
children and adolescents 2children and adolescents 2ndnd Ed. Kalyna Ed. Kalyna Bezchlibnyk-Butler and Adil Virani Bezchlibnyk-Butler and Adil Virani
Current Psychiatry Current Psychiatry Vol.5 No. 2 / Feb.2006 Vol.5 No. 2 / Feb.2006
Atomoxetine package insertAtomoxetine package insert New Perspectives on Adult ADHD New Perspectives on Adult ADHD
College Years CME Part 5 of 6College Years CME Part 5 of 6 ADHD : A Disorder with Life time Impact CME part 3 of ADHD : A Disorder with Life time Impact CME part 3 of
66 Advances in ADULT ADHD CME Part 7 of 8Advances in ADULT ADHD CME Part 7 of 8
ADHD Drug Therapy: Long and short of it.ADHD Drug Therapy: Long and short of it.

ReferencesReferences Primary Psychiatry Primary Psychiatry
July 2004: Vol.11 No.7July 2004: Vol.11 No.7 NeuroPsychiatry Reviews NeuroPsychiatry Reviews
Jan 08 Vol.9 No.1 pg.21Jan 08 Vol.9 No.1 pg.21 Psychiatric News Psychiatric News
Feb.1, 08 Vol 43 No.3 pg.23Feb.1, 08 Vol 43 No.3 pg.23