acute sinusitis - cecitycecity.com/acp_pier/pdfs/pcd096.pdf · acute sinusitis pier is copyrighted...
TRANSCRIPT

Quality Ratings: The preponderance of data supporting guidance statements are derived from:
level 1 studies, which meet all of the evidence criteria for that study type;
level 2 studies, which meet at least one of the evidence criteria for that study type; or
level 3 studies, which meet none of the evidence criteria for that study type or are derived from expert opinion, commentary, or consensus.
Study types and criteria are defined at http://smartmedicine.acponline.org/criteria.html
Disclaimer: The information included herein should never be used as a substitute for clinical judgement and does not represent an official position of the American College of Physicians. Because all PIER modules are updated regularly, printed web pages or PDFs may rapidly become obsolete.
Therefore, PIER users should compare the module updated date on the offical web site with any printout to ensure that the information is the most
current available.
CME Statement: The American College of Physicians is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide
continuing education for physicians. The American College of Physicians designates this enduring material for a maximum of 1 AMA PRA Category 1
CreditTM. Physicians should claim only credit commensurate with the extent of their participation in the activity. Purpose: This activity has been
developed for internists to facilitate the highest quality professional work in clinical applications, teaching, consultation, or research. Upon completion
of the CME activity, participants should be able to demonstrate an increase in the skills and knowledge required to maintain competence, strengthen
their habits of critical inquiry and balanced judgement, and to contribute to better patient care. Disclosures: Graham Worrall, MD, MSc, MB, BS, FCFP,
current author of this module, has no financial relationships with pharmaceutical companies, biomedical device manufacturers, or health-care related organizations. Deborah Korenstein, MD, FACP, Co-Editor, PIER, has no financial relationships with pharmaceutical companies, biomedical device
manufacturers, or health-care related organizations. Richard B. Lynn, MD, FACP, Co-Editor, PIER, has no financial relationships with pharmaceutical
companies, biomedical device manufacturers, or health-care related organizations.
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Acute Sinusitis View online at http://pier.acponline.org/physicians/diseases/d096/d096.html
Module Updated: 2012-12-03
CME Expiration: 2015-12-03
Author
Graham Worrall, MD, MSc, MB, BS, FCFP
Table of Contents
1. Diagnosis ..........................................................................................................................2
2. Consultation ......................................................................................................................7
3. Hospitalization ...................................................................................................................8
4. Therapy ............................................................................................................................9
5. Patient Counseling ..............................................................................................................14
6. Follow-up ..........................................................................................................................15
References ............................................................................................................................16
Glossary................................................................................................................................20
Tables ...................................................................................................................................21

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 2 of 26
1. Diagnosis Top
Make the diagnosis.
1.1 Obtain pertinent information from history and physical exam.
Recommendations
• Ask about allergies, systemic diseases, trauma, and environmental toxins.
• Ask about similar past episodes of sinusitis.
• Examine for rhinorrhea, pus in the nasal cavity, and local pain.
Evidence
• Atopic disease occurs in about 15% of the U.S. population and may predispose patients to sinusitis
(1).
• Smoking may impair ciliary function and may predispose to sinusitis (2).
• Only one study has directly compared clinical criteria with sinus puncture (3). The investigators
used a four-item risk score that included purulent rhinorrhea with unilateral predominance, local
pain with unilateral predominance, bilateral purulent rhinorrhea, and pus in the nasal cavity. The
risk score had better discrimination than the overall clinical criteria. (See table Sensitivity and
Specificity of a Four-Item Clinical Score for Diagnosing Acute Bacterial Sinusitis.) However, three of
the four items for purulent discharge overlap, and the data do not allow analysis of the effect of
grouping these three as a single item.
• A review of the positive and negative likelihood ratios of clinical symptoms and signs for acute
sinusitis found that most have low likelihood ratios; the best were pain in the teeth (positive
likelihood ratio, 2.5) and purulent nasal secretion (positive likelihood ratio, 5.5) (4).
• Signs and symptoms that have not been adequately assessed in diagnostic performance studies
against sinus puncture or sinus radiography include headache, facial pain and pressure that is
worse when bending forward, olfactory disturbance, fever, halitosis, maxillary toothache, and
cough (5; 6; 7; 8; 9). Most of these symptoms and signs probably are nonspecific or have low
sensitivity despite good specificity (e.g., maxillary toothache), and evidence is lacking.
• An oropharyngeal red streak was noted to be useful diagnostically for acute sinusitis (sensitivity,
70%; specificity, 67%) in a study of 60 patients at a Veterans Affairs urgent care center (54 men;
average age, 51). The generalizability of this finding is unclear and the risk score was more
sensitive and specific (10).
Rationale
• Most cases of sporadic acute sinusitis are due to viral infection; relatively few are due to bacterial
infection.
• Trauma and exposure to noxious agents account for a few cases.
• Other atypical considerations include neoplasms; anatomical abnormalities of the sinuses; genetic
causes, such as cystic fibrosis and the immotile cilia syndrome; endocrine and metabolic disorders,
such as diabetes mellitus; and immunosuppression, including HIV infection, which may lead to
infection with atypical pathogens.
• No good evidence shows that detailed medical review provides useful information in sporadic acute
sinusitis. Personal and family history, however, especially the relation of seasons to recurrent
sinusitis, may lead to suspicion of an underlying disease (e.g., allergy or ciliary dysfunction) that
may increase risk for sinusitis or for a specific form of sinusitis and should be considered in patients
with recurrent or chronic sinusitis. In patients with atopic disease, bacterial infection may
complicate a given episode of allergic rhinitis.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 3 of 26
• The exact signs and symptoms that would maximize diagnostic accuracy in acute bacterial sinusitis
need further study. A risk score compiled from the clinical items listed may be used empirically to
estimate the risk for bacterial sinusitis and to determine the need for treatment.
Comments
• Acute sinusitis is rare in children, who have immature sinuses.
1.2 Perform diagnostic imaging and other specialized studies only rarely in selected patients.
Recommendations
• Avoid sinus radiography, ultrasonography, CT, and MRI in acute sinusitis.
• Consider radiologic studies and sinus puncture only in certain situations: e.g., in patients with
predisposing factors for atypical microbial causes, such as Pseudomonas aeruginosa, or fungal
infection in patients with AIDS or immunocompromised patients.
• In such patients, note that precise bacteriologic diagnosis may be needed to determine optimal
therapy, especially when empirical therapy has failed to achieve a satisfactory response.
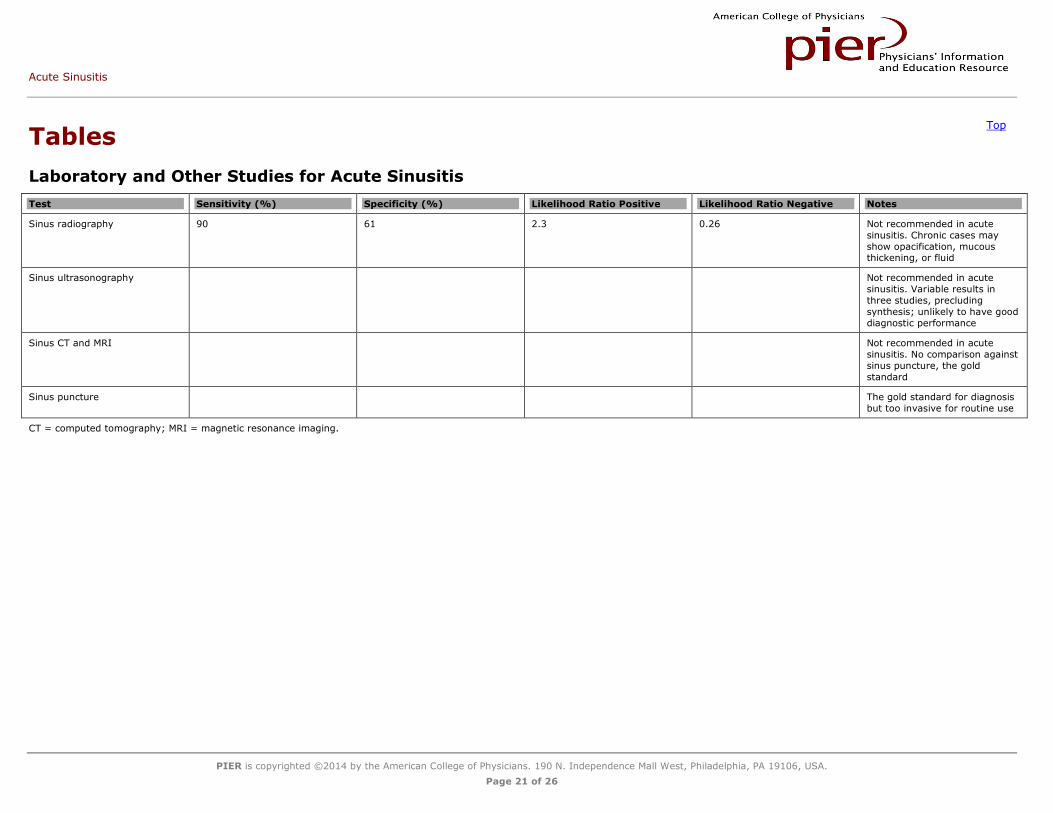
• See table Laboratory and Other Studies for Acute Sinusitis.
Evidence
• Clinical criteria vs. sinus puncture: Only one study has directly compared clinical criteria with sinus
puncture (3). The investigators used a four-item risk score that included purulent rhinorrhea with
unilateral predominance, local pain with unilateral predominance, bilateral purulent rhinorrhea, and
pus in the nasal cavity. The risk score had better discrimination than the overall clinical criteria.
(See table Sensitivity and Specificity of a Four-Item Clinical Score for Diagnosing Acute Bacterial
Sinusitis.)
• Clinical features vs. radiography: Three studies evaluated concordance between clinical exam
features and sinus radiography. One used the overall clinical impression (11); another used a
clinical score comprising purulent nasal secretions on exam, history of URI in the 2 prior weeks,
and sinus pain on tenderness (12); and the third used a clinical score comprising maxillary
toothache, abnormal transillumination, poor response to decongestants, purulent secretions on
exam, and colored nasal discharge on history (8). The latter study also used data for the overall
clinical impression. Synthesis of the data from these three studies suggests that a set of clinical
criteria is moderately accurate, but the data are difficult to interpret because the reference test,
sinus radiography, is not the gold standard for diagnosis of bacterial sinusitis. Acute viral sinusitis
probably causes the same radiographic changes as acute bacterial sinusitis.
• Ultrasonography vs. sinus aspiration: Five studies compared the diagnostic performance of
ultrasonography with sinus aspiration (13; 14; 15; 16; 17). Diagnostic performance varied
substantially; it was the poorest in the study in which ultrasonography was performed and
interpreted by untrained primary care physicians (16).
• Ultrasonography vs. radiography: Three studies compared the diagnostic performance of
ultrasonography with sinus radiography (18; 19; 20), but their results were not conclusive.
• CT vs. radiography: One study compared CT with sinus radiography in 29 patients (18). Sinus CT is
more sensitive than radiography, but diagnosis was confirmed by clinical criteria, not sinus
puncture.
• Another study found sinus x-rays to be less sensitive than sinus CT scans for demonstrating
radiographic changes consistent with acute sinusitis (21).
• A decision analysis found that regardless of the prevalence of bacterial sinusitis in the patient
population (or the individual's likelihood of bacterial sinusitis), sinus radiography is never optimal in
the routine management of uncomplicated sinusitis (22).

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 4 of 26
• Several studies using CT or MRI reported sinus mucosal abnormalities in 15% to 49% of patients
with no symptoms of sinusitis (23; 24; 25; 26; 27; 28). The clinical importance of these chance
findings is uncertain.
• Signs and symptoms that have not been adequately assessed in diagnostic performance studies
compared with sinus puncture or sinus radiography include headache, facial pain and pressure that
is worse when bending forward, olfactory disturbance, fever, halitosis, maxillary toothache, and
cough (5; 6; 7; 8; 9). Most of these symptoms and signs are probably nonspecific or not very
sensitive, and evidence is lacking.
• One small pediatric study found a significant improvement in patients on antibiotics who were
diagnosed clinically (i.e., no diagnostic tests were used) (29).
Rationale
• Cost-effectiveness considerations in plain radiography also pertain to sinus ultrasonography.
Ultrasonography is rarely used in the United States to diagnose sinusitis.
• Radiographs and CT scans have high false-positive rates in acute sinusitis.
• Evidence on the role of CT in diagnosis of acute bacterial sinusitis is very limited. No studies have
compared CT with sinus puncture.
• Despite fairly good diagnostic performance, at a cost of approximately $100, sinus radiography is
not cost-effective compared with symptomatic treatment or use of clinical criteria to guide
antibiotic therapy.
• Even if ultrasonography is less costly than radiography, no strong evidence supports its use by
primary care physicians to diagnose acute bacterial sinusitis.
• Given the current evidence, CT and MRI have no role in diagnosis of acute sinusitis, except when
history and physical exam findings indicate extrasinus local spread or intracranial complications.
• Asymptomatic patients with abnormalities on imaging studies do not require treatment.
• Sinus puncture and culture of aspirate is the gold standard for diagnosis of acute bacterial sinusitis
in the research setting. However, it should not be performed routinely because it is painful and
requires expertise.
Comments
• The occipitomental view (Waters view) is the standard radiographic view for visualizing the
paranasal sinuses, especially the maxillary sinuses; however, a series of three or four radiographs
is often ordered. A common criterion for positive radiography is sinus fluid or opacity. Some studies
also consider mucous membrane thickening, which increases the sensitivity of radiography but
decreases its specificity.
1.3 Consider atypical presentations of acute sinusitis and confounding diagnoses.
Recommendations
• Distinguish between acute sinusitis and chronic sinusitis.
Chronic sinusitis is defined clinically by the presence of sinus signs and symptoms for more than 12 weeks
The diagnosis of subacute sinusitis is reserved for patients with symptoms for 4 to 12 weeks
Acute exacerbations may complicate chronic sinusitis
• In children aged 1 to 5 years, consider the diagnosis of acute sinusitis when upper respiratory tract
signs and symptoms, including daytime and nighttime cough and rhinorrhea independent of color,
persist for more than 10 to 14 days or if symptoms worsen after 5 to 7 days.
• See table Differential Diagnosis of Sinusitis.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 5 of 26
Evidence
• Acute sinusitis must be distinguished from chronic sinusitis because the conditions differ in
histopathology, prognosis, and management potential (30; 31).
• In an observational cohort study of 1307 children aged 1 to 5 years, 121 had persistent respiratory
symptoms meeting criteria for a diagnosis of sinusitis (9.3% [CI, 7.7% to 10.9%]). Patients who
presented with cold and cough symptoms were significantly more likely to meet criteria for sinusitis
than those who came for any other reason (17.3% vs. 4.2%, respectively; P<0.001). If the
proportion of children with otitis media is excluded, 5% of children aged 1 to 5 years who are seen
in primary care pediatrics might be expected to receive antibiotics exclusively for a diagnosis of
sinusitis. At 24 to 48 hours and at 10 to 14 days after the clinic visit, the investigators noted a
trend toward more rapid improvement among those children who were treated with antibiotics
(32).
Rationale
• Acute sinusitis and chronic sinusitis differ in histopathology, prognosis, and management.
• Because chronic sinusitis responds poorly to conventional antibiotic therapy, establishing the exact
duration of symptoms is important.
• Many predisposing factors may further hinder cure, such as severe allergy or structural changes
arising from chronic sinusitis itself or from previous surgery for symptoms.
• Most viral upper respiratory tract infections in children aged 1 to 5 years will show clinical
improvement after 7 to 10 days.
Comments
• In some patients, sinusitis recurs frequently, and it may be difficult to determine whether
recurrence is relapse of previous infection or a de novo episode.
1.4 Look for the rare complications of acute bacterial sinusitis.
Recommendations
• Examine for local extensions of the infection:
Osteitis of the sinus bones
Periorbital cellulitis
Orbital cellulitis
• Examine for metastatic spread to the central nervous system:
Meningitis
Brain abscess
Infection of the intracranial venous sinuses, particularly the cavernous sinus
• Note that patients with ophthalmic or neurologic symptoms or signs should undergo more detailed
clinical neurologic exam.
• Abnormalities may need to be examined further by using appropriate diagnostic imaging, such as
CT.
Evidence
• Brain abscess accounts for about 1 in 10,000 hospital admissions. The proportion of cases of brain
abscess attributable to bacterial sinusitis varies from 0.5% in China to 15% to 25% in Northern
Europe (33).
• Physicians see about 3 million cases of acute sinusitis each year (34), and there are about 5000
brain abscess-related hospital discharges annually (35). From these figures, it can be inferred that
approximately 1000 cases of brain abscesses per year are sinusitis-related, translating to an attack
rate of 1 in 3000 among patients seen for acute sinusitis.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 6 of 26
Rationale
• Serious complications of acute bacterial sinusitis are rare.
• Local complications of sinusitis are usually clinically evident. For example, orbital cellulitis is
diagnosed on the basis of orbital swelling, redness of the conjunctiva, and limitation of extraocular
movements.
• Periorbital and orbital cellulitis are seen mainly in children.
Comments
• The low complication rate does not justify routine use of special diagnostic tests to rule out this
complication.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 7 of 26
2. Consultation Top
Consider specialty consultation in selected patients with presumed sinusitis. Consider consultation for patients in whom sinusitis has a complicated course or is recurrent.
2.1 Reserve consultation for complicated cases or patients whose symptoms
fail to respond to initial therapy.
Recommendations
• Consult an otolaryngologist only when the diagnosis is unclear.
• Consult an ophthalmologist, neurosurgeon, infectious disease expert, or neurologist as needed
when serious complications such as periorbital cellulitis or venous sinus thrombosis are suspected.
• See information on complications.
Evidence
• There is no evidence that involvement of consultant experts (e.g., otolaryngologists) improves
diagnostic accuracy or clinical outcomes of uncomplicated sinusitis.
Rationale
• Consultation results in increased cost without added diagnostic or clinical benefits in patients with
uncomplicated sinusitis.
2.2 Consider consultation in patients with presumed acute sinusitis who do
not respond to initial treatment, who have recurrent sinus infections, or who
have complications.
Recommendations
• Consult an otolaryngologist when sinusitis becomes chronic, an anatomical abnormality is
suspected, or an abscess or meningeal spread of infection is suspected.
• Consult an ophthalmologist when orbital cellulitis is present.
• Consult an allergist when underlying atopic disease may be present.
Evidence
• There is no evidence that expert consultation improves outcomes in patients with uncomplicated
acute sinusitis.
Rationale
• Specialist expertise may be required to treat underlying conditions or severe complications.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 8 of 26
3. Hospitalization Top
Hospitalize patients for serious complications of acute bacterial sinusitis.
3.1 Hospitalize for local extensions of the infection, such as orbital involvement or metastatic spread to the central nervous system.
Recommendations
• Hospitalize for:
Local extension of the infection (osteitis of the sinus bones, orbital cellulitis).
Metastatic spread to the central nervous system (meningitis, brain abscess).
Infection or thrombosis of the intracranial venous sinuses, particularly the cavernous sinus.
Evidence
• Brain abscess accounts for about 1 in 10,000 hospital admissions. The proportion of cases of brain
abscess attributable to bacterial sinusitis varies from 0.5% in China to 15% to 25% in Northern
Europe (33).
• Physicians see about 3 million cases of acute sinusitis each year (34), and there are about 5000
brain abscess-related hospital discharges annually (35). From these figures, it can be inferred that
approximately 1000 cases of brain abscesses per year are sinusitis-related, translating to an attack
rate of 1 in 3000 among patients seen for acute sinusitis.
Rationale
• These complications require long courses of parenteral antibiotics and close observation.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 9 of 26
4. Therapy Top
Choose drug therapy on the basis of the probability of bacterial sinusitis and consider non-drug therapy.
4.1 Consider nasal sprays or sinus irrigation.
Recommendations
• Consider nasal sprays or sinus irrigation to increase mucosal moisture and remove inflammatory
debris and bacteria.
Evidence
• No well-designed, randomized studies have addressed the efficacy of sinus irrigation, nasal sprays,
or other nondrug therapies, but these therapies are often prescribed. Their effectiveness is
unknown.
Rationale
• These agents may relieve symptoms, and the cost is low compared with drug therapy. Because
high-quality data are lacking, sprays and irrigation cannot be strongly recommended or
discouraged.
4.2 Start nonantibiotic therapy for symptoms as an initial strategy in patients
with a low probability of bacterial sinusitis.
Recommendations
• Institute symptomatic therapy:
Mucolytic agents to reduce viscosity of nasal secretions
Decongestants to reduce mucosal inflammation and improve ostial drainage by vasoconstriction
Antihistamines and intranasal steroids to inhibit inflammatory pathways
• Note that patients with only one of the following have a low probability (less than 25%) of bacterial
sinusitis:
URI for more than 7 days
Facial pain
Purulent discharge
Evidence
• Several classes of medications are commonly used to try to restore normal sinus environment and
function in acute sinusitis (36; 37).
• Eleven randomized studies have addressed the use of various ancillary drug therapies, including a
proteolytic enzyme (bromelain), α-adrenergic agonists (xylometazoline and oxymetazoline), a
mucolytic agent (bromhexine), intranasal corticosteroids (budesonide and flunisolide), and an
antihistamine (loratadine) (38; 39; 40; 41; 42; 43; 44; 45; 46; 47; 48). In most patients, these
agents were used in conjunction with antibiotics, and studies did not exclude patients with chronic
sinusitis. Efficacy varied, but generally favorable trends were reported. One randomized, controlled
trial found no benefit for nasal budesonide or oral amoxicillin use in acute sinusitis but suggested,
in secondary analyses, that budesonide is beneficial in patients with less severe symptoms and
detrimental when more severe symptoms are present (48).
• A decision analysis suggested that when the prevalence of acute bacterial sinusitis in a cohort of
patients is less than 25%, empirical symptomatic treatment is the most effective approach
compared with clinical decision rules or radiography to decide on the use of antibiotics or using
antibiotics initially (22).
Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 10 of 26
Rationale
• The cost of extensive use of nonantibiotic drug therapy should be considered.
• No good evidence exists on symptomatic therapy with nonantibiotic drugs in patients with acute
sinusitis.
Comments
• The diversity of agents and study limitations preclude meaningful data synthesis. More data are
needed to establish the efficacy of specific agents and ancillary measures.
• Common adverse effects from the use of ancillary or symptomatic treatments have not been well
studied. Avoid overmedication with antihistamines and other decongestants.
• Of note, a Cochrane review of intranasal steroids in acute sinusitis found four well-designed
randomized, controlled trials with 1943 participants that supported, despite limited current
evidence, their use as monotherapy or as an adjuvant therapy to antibiotics (49).
4.3 Consider antibiotic therapy in patients with a high probability of bacterial sinusitis at presentation, with acute worsening, and those in whom
symptomatic therapy fails after 10 days.
Recommendations
• Treat with antibiotics for bacterial sinusitis in patients:
With symptoms of rhinosinusitis for 10 days or more with no improvement
Who present initially with severe symptoms of fever of 39 °C (102 °F) or above, and either facial pain or purulent nasal discharge for 3 to 4 days
Who experience worsening fever, headache, or nasal discharge after an improving URI
• When using antibiotics, use amoxicillin or amoxicillin/clavulanate as a first-line agent.
• For penicillin-allergic patients or patients with persistent symptoms, consider alternative antibiotics
such as doxycycline or trimethoprim-sulfamethoxazole in adults and doxycycline in older children.
• Avoid empiric use of antibiotics as part of initial management of patients with a low likelihood of
bacterial sinusitis.
• Always consider patient expectations and discuss overall management.
• Consider delaying prescription for antibiotics to reduce overuse.
• See table Drug Treatment for Sinusitis.
• See table Cost-Effective Treatment, Based on Disease Likelihood.
Evidence
• A 2012 clinical practice guideline from the Infectious Diseases Society of America recommends
limiting antibiotics to patients with likely bacterial sinusitis. They also recommend beginning with
amoxicillin-clavulanate when treating bacterial sinusitis, but that recommendation is weak and
based on weak evidence (50).
• Randomized studies have compared antibiotics with placebo for treatment of acute sinusitis (51;
52; 53; 54; 55; 56; 57; 58). Different antibiotic agents were used in these studies, but their
results did not differ significantly.
• Overall, meta-analysis of six of the studies (59) showed that antibiotics were significantly more
effective than placebo, reducing treatment failures by almost half (from 31% to 16%); however,
symptoms improved or were cured in 68% of patients given placebo.
• Another meta-analysis that looked at individual patient data included nine primary care trials and
2547 adults. There were limited data suggesting that antibiotics were beneficial; 15 patients (CI,
Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 11 of 26
NNT[benefit] 7 to NNT[harm] 190) would have to be given antibiotics before an additional patient
was cured. The most significant clinical predictor was purulent discharge in the pharynx; the NNT
was 8 patients with this sign (CI, NNT[benefit] 4 to NNT[harm] 47) before 1 additional patient was
cured (60).
• The highest spontaneous cure rate (85% at 10 days) was seen in one trial that enrolled patients on
the basis of sinusitis-like symptoms without further diagnostic documentation. The trial showed no
benefit of antibiotics, although statistical analysis could not completely exclude a moderate benefit
(56).
• A decision analysis suggests that initial empirical antibiotic therapy is the most cost-effective
strategy for management of acute sinusitis when the expected prevalence of bacterial sinusitis is
greater than 83% (22). In primary care, where the prevalence of acute bacterial sinusitis is low,
the results will be the same whether antibiotics are immediately prescribed or a ‘wait and see’
strategy is used (61).
• Although antibiotic resistance must be considered, no good data confirm that response to antibiotic
treatment depends on in-vitro susceptibility of microbial isolates. On the contrary, convincing
evidence from randomized, controlled trials indicates that the efficacy of amoxicillin in alleviating
clinical symptoms and producing clinical cures is similar to that of broader-spectrum antibiotics.
Folate inhibitors, such as trimethoprim-sulfamethoxazole, have rates of clinical cure and failures
similar to those of newer, more expensive antibiotics (22). However, pneumococcal resistance
rates for trimethoprim-sulfamethoxazole are as high as 18% to 20% (62). Cure rates are also
similar with doxycycline (63).
• Studies done since the 1970s have shown the predominant isolates from acute bacterial sinusitis to
be S. pneumoniae and H. influenzae; however, with recent vaccinations, there appears to be a
relative increase in H. influenzae (29). Studies done in the 1990s have shown some contribution of
M. catarrhalis, especially in children and young adults. Most isolates of M. catarrhalis and about one
third of those of H. influenzae produce β-lactamases and are resistant to penicillin and amoxicillin.
See 3; 36; 64; 65; 66; 67; 68; 69; 70 and 71 for the evolution of bacteriology over time.
• Most studies of the microbial flora of infected sinuses have focused on aspirates from the maxillary
sinuses (15; 16).
• Data comparing microbial flora from infected maxillary and frontal sinuses in individual patients
correlated well but are limited (72).
• Evidence for comparison of amoxicillin with newer, more expensive antibiotics comes from 13
randomized trials including 1553 patients (53; 69; 73; 74; 75; 76; 77; 78; 79; 80; 81; 82; 83). A
meta-analysis synthesized this data (59). Agents being compared were diverse and included
amoxicillin-clavulanic acid, cefuroxime, cefixime, azithromycin, clarithromycin, roxithromycin,
cefaclor, cefpodoxime, and minocycline. The combined failure rate among patients treated with
amoxicillin was low (11% [CI, 8% to 14%]), and the further decrease in clinical failure with broad-
spectrum antibiotics was not significant (risk ratio, 0.86 [CI, 0.62 to 1.19]). Treating 100 patients
with amoxicillin would lead to only 0.85 more failures (CI, 3.1 more to 1.4 fewer failures). Similar
results were obtained when the analysis focused on clinical cures with risk ratios very close to 1.0.
Several studies in the meta-analysis were done at a time when pneumococcal antibiotic resistance
was significantly less common, and caution may be needed in applying the results to the current
setting.
• Although nine randomized studies have compared folate inhibitors with newer, more expensive
antibiotics, the cumulative evidence (summarized in the same meta-analysis) is sparse (total of
410 patients) and the overall quality of the trials is low. The risk ratio for clinical cures and clinical
failures is nevertheless also close to 1.0 (59).

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 12 of 26
• One small study (n = 56) in children under age 10 found that patients who received high-dose
amoxicillin (90 mg/kg) plus potassium clavulanate improved at a much greater rate than those
receiving placebo (50% vs. 14%) (29).
• In a randomized, placebo-controlled trial of 188 children who were diagnosed with sinusitis, 58
received amoxicillin, 48 received amoxicillin-clavulanate, and 55 received placebo. Day 14
improvement rates were 79%, 81%, and 79%, respectively. The rates of adverse events
(amoxicillin, 19%; amoxicillin-clavulanate, 11%; placebo, 10%), relapse (amoxicillin, 12%;
amoxicillin-clavulanate, 13%; placebo, 13%), and recurrence of sinus symptoms (amoxicillin, 9%;
amoxicillin-clavulanate, 13%; placebo, 13%) were similar among treatment groups (57).
• The withdrawal rate in randomized trials averages between 4% and 6% with amoxicillin, folate
inhibitors, or doxycycline (59; 63). A larger proportion of patients, up to 10% to 20% in most
reports, have more minor adverse reactions. Rates of adverse events have been as high as 50% in
a few trials (e.g., see 54); most events were gastrointestinal. In most cases, side effects ceased
once antibiotic treatment was stopped.
• The Sinus and Allergy Health Partnership published an executive summary on antimicrobial
treatment guidelines for acute bacterial rhinosinusitis (84).
• A 2010 French prospective cohort study of 5640 patients with acute sinusitis in primary care found
that most patients got better soon, whether or not antibiotics were prescribed (85).
• A 2009 meta-analysis of 12 randomized, controlled trials comprising 4430 patients found that a 5-
day course of antibiotics was as effective as a 10-day course (86).
Rationale
• Antibiotics may be useful in patients with a high likelihood of definite bacterial sinusitis.
• In situations in which the prevalence of bacterial sinusitis is expected to be 25% to 83%, use of
clinical rules based on signs and symptoms to determine the need for antibiotic treatment in
selected patients is cost effective.
• In most clinical practices, the prevalence of bacterial sinusitis among patients with acute sinusitis
symptoms is probably less than 83% and most often less than 25%.
• A large proportion of H. influenzae isolates possess β-lactamases.
• The data as a whole suggest that if antibiotics are to be used, amoxicillin and doxycycline are
adequate agents. Trimethoprim-sulfamethoxazole is acceptable for β-lactam-allergic adults.
• Data are limited on the optimal duration of antibiotic treatment for acute sinusitis. Traditionally,
long courses (7 to 14 days) have been used in clinical practice. Nevertheless, there is no evidence
that such long courses are needed to treat acute bacterial sinusitis.
• First-generation cephalosporins have minimal efficacy against S. pneumoniae and H. influenzae.
Second-generation cephalosporins, such as cefpodoxime, are considered to be second-line agents
for acute sinusitis.
Comments
• Pneumococcal resistance to macrolides and other agents has increased in past years (62), and
trimethoprim-sulfamethoxazole is not a recommended second-line agent in children (87). However,
it continues to be an acceptable first-line agent in adults (84; 88; 89).
• Newer, broad-spectrum agents are more costly, and substantial concern exists about promoting
the development of widespread resistance among bacteria in the community and in the host (90;
91; 92).
• The evolution of regional bacterial resistance may need to be taken into account, but evidence is
lacking that this would lead to better clinical outcomes.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 13 of 26
• A variety of other recommendations for acute sinusitis exist but without evidence to support clinical
superiority to amoxicillin, folate inhibitors, or doxycycline.
• A 2008 Cochrane meta-analysis of 57 randomized, controlled trials (93) found a slight statistical
difference between antibiotic and placebo, but also high cure rates at 7 to 15 days with either
placebo (80%) or antibiotic (90%). No significant differences were found between antibiotic
regimens. A meta-analysis of 9 trials with patient level data available showed similar results (60).
• Doxycycline has a broader spectrum of activity than amoxicillin; it also covers β-lactamase-
producing strains of H. influenzae and M. catarrhalis. Its use should satisfy concerns about
antimicrobial resistance when prescribing treatment for acute sinusitis.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 14 of 26
5. Patient Counseling Top
Inform the patient about sinusitis.
5.1 Inform the patient about the disease.
Recommendations
• Reassure and inform the patient about the nature of the disease, expected duration of illness, and
details of therapy.
• Inform the patient about the evidence on antibiotic use.
Evidence
• No randomized or other well-designed studies have addressed the effects of patient education on
the course of sinusitis.
Rationale
• Thoughtful explanation may help address the patient's expectations.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 15 of 26
6. Follow-up Top
Tailor follow-up to aspects of a specific patient's illness.
6.1 Consider office follow-up in selected cases of sinusitis, but not routinely.
Recommendations
• Consider follow-up evaluation when symptoms persist or new symptoms develop.
• Note that routine follow-up evaluations are probably not warranted in patients whose symptoms
resolve or improve substantially.
• Consider follow-up in patients whose symptoms persist after 2 to 3 weeks.
• Note that earlier follow-up may be indicated if new, worsening symptoms appear, especially
symptoms suggestive of serious complications.
Evidence
• There is no evidence from randomized or other well-designed trials indicating whether routine
follow-up evaluation improves outcomes in patients with acute uncomplicated sinusitis.
Rationale
• Failure to improve may suggest the presence of complications.
Comments
• Routine office follow-up may increase the cost of management of this generally benign condition
without meaningful clinical gains.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 16 of 26
References Top
1. Spector SL. Overview of comorbid associations of allergic rhinitis. J Allergy Clin Immunol. 1997;99:S773-80. (PMID: 9042070)
2. Mahakit P, Pumhirun P. A preliminary study of nasal mucociliary clearance in smokers, sinusitis and allergic rhinitis patients. Asian Pac J Allergy Immunol. 1995;13:119-21. (PMID: 8703239)
3. Berg O, Carenfelt C. Analysis of symptoms and clinical signs in the maxillary sinus empyema. Acta Otolaryngol. 1988;105:343-9. (PMID: 3389120)
4. Worrall G. Acute sinusitis. Can Fam Physician. 2011;57:565-7. (PMID: 21642737)
5. Hadley JA, Schaefer SD. Clinical evaluation of rhinosinusitis: history and physical examination. Otolaryngol Head Neck Surg. 1997;117:S8-11. (PMID: 9334783)
6. Shapiro GG, Rachelefsky GS. Introduction and definition of sinusitis. J Allergy Clin Immunol. 1992;90:417-8. (PMID: 1527329)
7. Williams JW, Simel DL. Does this patient have sinusitis? Diagnosing acute sinusitis by history and physical examination. JAMA. 1993;270:1242-6. (PMID: 8355389)
8. Williams JW, Roberts L, Distell B, Simel DL. Diagnosing sinusitis by X-ray: is a single Waters view adequate? J Gen Intern Med. 1992;7:481-5. (PMID: 1403202)
9. Williams JW, Simel DL, Roberts L, Samsa GP. Clinical evaluation for sinusitis. Making the diagnosis by history and physical examination. Ann Intern Med. 1992;117:705-10. [Full Text] (PMID: 1416571)
10. Thomas C, Aizin V. Brief report: a red streak in the lateral recess of the oropharynx predicts acute sinusitis. J Gen Intern Med. 2006;21:986-8. (PMID: 16918746)
11. Axelsson A, Runze U. Symptoms and signs of acute maxillary sinusitis. ORL J Otorhinolaryngol Relat Spec. 1976;38:298-308. (PMID: 1034250)
12. Jannert M, Andréasson L, Helin I, Pettersson H. Acute sinusitis in children—symptoms, clinical findings and bacteriology related to initial radiologic appearance. Int J Pediatr Otorhinolaryngol. 1982;4:139-48. (PMID: 6982255)
13. Revonta M. Ultrasound in the diagnosis of maxillary and frontal sinusitis. Acta Otolaryngol Suppl. 1980;370:1-55. (PMID: 6272532)
14. Kuusela T, Kurri J, Sirola R. Ultrasound in the diagnosis of paranasal sinusitis of conscripts: comparison of results of
ultrasonography, roentgen examination, and puncture and irrigation. Ann Med Milit Fenn. 1982;57:138-41.
15. van Buchem L, Peeters M, Beaumont J, Knottnerus JA. Acute maxillary sinusitis in general practice: the relation between clinical picture and objective findings. Eur J Gen Pract. 1995;1:155-60.
16. Laine K, Määttä T, Varonen H, Mäkelä M. Diagnosing acute maxillary sinusitis in primary care: a comparison of ultrasound, clinical examination and radiography. Rhinology. 1998;36:2-6. (PMID: 9569433)
17. Savolainen S, Pietola M, Kiukaanniemi H, Lappalainen E, Salminen M, Mikkonen P. An ultrasound device in the diagnosis of acute maxillary sinusitis. Acta Otolaryngol Suppl. 1997;529:148-52. (PMID: 9288296)
18. Berg O, Carenfelt C. Etiological diagnosis in sinusitis: ultrasonography as clinical complement. Laryngoscope. 1985;95:851-3. (PMID: 3892209)
19. Rohr AS, Spector SL, Siegel SC, Katz RM, Rachelefsky GS. Correlation between A-mode ultrasound and radiography in the diagnosis of maxillary sinusitis. J Allergy Clin Immunol. 1986;78:58-61. (PMID: 3522707)
20. Jensen C, von Sydow C. Radiography and ultrasonography in paranasal sinusitis. Acta Radiol. 1987;28:31-4. (PMID: 2952138)
21. Burke TF, Guertler AT, Timmons JH. Comparison of sinus x-rays with computed tomography scans in acute sinusitis. Acad Emerg Med. 1994;1:235-9. (PMID: 7621202)
22. Evidence Report: Diagnosis and Treatment of Acute Bacterial Sinusitis. Boston: New England Medical Center, Evidence-based Practice Center; 1998. AHCPR contract 290-97-0019.
23. Calhoun KH, Waggenspack GA, Simpson CB, Hokanson JA, Bailey BJ. CT evaluation of the paranasal sinuses in symptomatic and asymptomatic populations. Otolaryngol Head Neck Surg. 1991;104:480-3. (PMID: 1903859)
24. Lloyd GA, Lund VJ, Scadding GK. CT of the paranasal sinuses and functional endoscopic surgery: a critical analysis of 100 symptomatic patients. J Laryngol Otol. 1991;105:181-5. (PMID: 2019802)
25. Gordts F, Clement PA, Destryker A, Desprechins B, Kaufman L. Prevalence of sinusitis signs on MRI in a non-ENT paediatric population. Rhinology. 1997;35:154-7. (PMID: 9532633)
26. Kaliner MA, Osguthorpe JD, Fireman P, Anon J, Georgitis J, Davis ML, et al. Sinusitis: bench to bedside. Current findings, future directions. Otolaryngol Head Neck Surg. 1997;116:S1-20. (PMID: 9212028)

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 17 of 26
27. Axelsson A, Chidekel N. Symptomatology and bacteriology correlated to radiological findings in acute maxillary sinusitis. Acta Otolaryngol. 1972;74:118-22. (PMID: 4403519)
28. Patel K, Chavda SV, Violaris N, Pahor AL. Incidental paranasal sinus inflammatory changes in a British population. J Laryngol Otol. 1996;110:649-51. (PMID: 8759538)
29. Wald ER, Nash D, Eickhoff J. Effectiveness of amoxicillin/clavulanate potassium in the treatment of acute bacterial sinusitis in children. Pediatrics. 2009;124:9-15. (PMID: 19564277)
30. Cotran RS, Robbins SL, Kumar V, Schoen, FJ. In: Cotran RS, Robbins SL, Kumar V, Schoen FJ, eds. Robbins Pathologic Basis of Disease. 5th ed. Philadelphia: WB Saunders; 1995:53-83.
31. Lanza DC, Kennedy DW. Adult rhinosinusitis defined. Otolaryngol Head Neck Surg. 1997;117:S1-7. (PMID: 9334782)
32. Aitken M, Taylor JA. Prevalence of clinical sinusitis in young children followed up by primary care pediatricians. Arch Pediatr Adolesc Med. 1998;152:244-8. (PMID: 9529461)
33. Wispelwey B, Scheld WM. Brain abscess. In: Mandell GL, Douglas RG, Bennett JE, Dolin R, eds. Principles and Practice of Infectious Diseases. 4th ed. New York: Churchill Livingstone; 1995:887-98.
34. National Ambulatory Medical Care Survey. National Center for Health Statistics. (CD-ROM) 1990-1995;Series 13.
35. National Hospital Discharge Survey. National Center for Health Statistics. (CD-ROM) 1993-1995;Series 13.
36. Benninger MS, Anon J, Mabry RL. The medical management of rhinosinusitis. Otolaryngol Head Neck Surg. 1997;117:S41-9. (PMID: 9334787)
37. Infectious rhinosinusitis in adults: classification, etiology and management. International Rhinosinusitis Advisory Board. Ear Nose Throat J. 1997;76:1-22. (PMID: 9509732)
38. Taub SJ. The use of bromelains in sinusitis: a double-blind clinical evaluation. Eye Ear Nose Throat Mon. 1967;46:361-2 passim. (PMID: 5342723)
39. Ryan RE. A double-blind clinical evaluation of bromelains in the treatment of acute sinusitis. Headache. 1967;7:13-7. (PMID: 4859824)
40. Seltzer AP. Adjunctive use of bromelains in sinusitis: a controlled study. Eye Ear Nose Throat Mon. 1967;46:1281-8. (PMID: 4864820)
41. Lewison E. Comparison of the effectiveness of topical and oral nasal decongestants. Eye Ear Nose Throat Mon. 1970;49:16-8. (PMID: 4098115)
42. Harris PG. A comparison of ‘bisolvomycin’ and oxytetracycline in the treatment of acute infective sinusitis. Practitioner. 1971;207:814-7. (PMID: 4947232)
43. Meltzer EO, Orgel HA, Backhaus JW, Busse WW, Druce HM, Metzger WJ, et al. Intranasal flunisolide spray as an adjunct to oral antibiotic therapy for sinusitis. J Allergy Clin Immunol. 1993;92:812-23. (PMID: 8258615)
44. Wiklund L, Stierna P, Berglund R, Westrin KM, Tönnesson M. The efficacy of oxymetazoline administered with a nasal bellows container and combined with oral phenoxymethyl-penicillin in the treatment of acute maxillary sinusitis. Acta Otolaryngol Suppl. 1994;515:57-64. (PMID: 8067245)
45. McCormick DP, John SD, Swischuk LE, Uchida T. A double-blind, placebo-controlled trial of decongestant-antihistamine for the treatment of sinusitis in children. Clin Pediatr (Phila). 1996;35:457-60. (PMID: 8877243)
46. Barlan IB, Erkan E, Bakir M, Berrak S, Basaran MM. Intranasal budesonide spray as an adjunct to oral antibiotic therapy for acute sinusitis in children. Ann Allergy Asthma Immunol. 1997;78:598-601. (PMID: 9207726)
47. Braun JJ, Alabert JP, Michel FB, Quiniou M, Rat C, Cougnard J, et al. Adjunct effect of loratadine in the treatment of acute sinusitis in patients with allergic rhinitis. Allergy. 1997;52:650-5. (PMID: 9226059)
48. Williamson IG, Rumsby K, Benge S, Moore M, Smith PW, Cross M, et al. Antibiotics and topical nasal steroid for treatment of acute maxillary sinusitis: a randomized controlled trial. JAMA. 2007;298:2487-96. (PMID: 18056902)
49. Zalmanovici A, Yaphe J. Steroids for acute sinusitis. Cochrane Database Syst Rev. 2007;(2):CD005149. (PMID: 17443574)
50. Chow AW, Benninger MS, Brook I, Brozek JL, Goldstein EJ, Hicks LA, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54:e72-e112. (PMID: 22438350)
51. Axelsson A, Chidekel N, Grebelius N, Jensen C. Treatment of acute maxillary sinusitis. A comparison of four different methods. Acta Otolaryngol. 1970;70:71-6. (PMID: 4989705)
52. Ganança M, Trabulsi LR. The therapeutic effects of cyclacillin in acute sinusitis: in vitro and in vivo correlations in a placebo-
controlled study. Curr Med Res Opin. 1973;1:362-8. (PMID: 4359033)
Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 18 of 26
53. Wald ER, Chiponis D, Ledesma-Medina J. Comparative effectiveness of amoxicillin and amoxicillin-clavulanate potassium in acute paranasal sinus infections in children: a double-blind, placebo-controlled trial. Pediatrics. 1986;77:795-800. (PMID:
3520469)
54. Lindbaek M, Hjortdahl P, Johnsen UL. Randomised, double blind, placebo controlled trial of penicillin V and amoxycillin in treatment of acute sinus infections in adults. BMJ. 1996;313:325-9. (PMID: 8760738)
55. van Buchem FL, Knottnerus JA, Schrijnemaekers VJ, Peeters MF. Primary-care-based randomised placebo-controlled trial of antibiotic treatment in acute maxillary sinusitis. Lancet. 1997;349:683-7. (PMID: 9078199)
56. Stalman W, van Essen GA, van der Graaf Y, de Melker RA. The end of antibiotic treatment in adults with acute sinusitis-like complaints in general practice? A placebo-controlled double-blind randomized doxycycline trial. Br J Gen Pract. 1997;47:794-9. (PMID: 9463979)
57. Garbutt JM, Goldstein M, Gellman E, Shannon W, Littenberg B. A randomized, placebo-controlled trial of antimicrobial treatment for children with clinically diagnosed acute sinusitis. Pediatrics. 2001;107:619-25. (PMID: 11335733)
58. Merenstein D, Whittaker C, Chadwell T, Wegner B, D’Amico F. Are antibiotics beneficial for patients with sinusitis complaints? A randomized double-blind clinical trial. J Fam Pract. 2005;54:144-51. (PMID: 15689289)
59. de Ferranti SD, Ioannidis JP, Lau J, Anninger WV, Barza M. Are amoxycillin and folate inhibitors as effective as other antibiotics for acute sinusitis? A meta-analysis. BMJ. 1998;317:632-7. (PMID: 9727991)
60. Young J, De Sutter A, Merenstein D, van Essen GA, Kaiser L, Varonen H, et al. Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371:908-14. (PMID: 18342685)
61. de Bock GH, van Erkel AR, Springer MP, Kievit J. Antibiotic prescription for acute sinusitis in otherwise healthy adults. Clinical cure in relation to costs. Scand J Prim Health Care. 2001;19:58-63. (PMID: 11303550)
62. Doern GV, Pfaller MA, Kugler K, Freeman J, Jones RN. Prevalence of antimicrobial resistance among respiratory tract isolates of Streptococcus pneumoniae in North America: 1997 results from the SENTRY antimicrobial surveillance program. Clin Infect Dis. 1998;27:764-70. (PMID: 9798031)
63. de Bock GH, Dekker FW, Stolk J, Springer MP, Kievit J, van Houwelingen JC. Antimicrobial treatment in acute maxillary sinusitis: a meta-analysis. J Clin Epidemiol. 1997;50:881-90. (PMID: 9291872)
64. Urdal K, Berdal P. The microbial flora in 81 cases of maxillary sinusitis. Acta Otolaryngol (Stockh). 1949;37:20-5.
65. Bjorkwall T. Bacteriological examinations in maxillary sinusitis: bacterial flora of the maxillary antrum. Acta Otolaryngol Suppl (Stockh). 1950;83:1-58.
66. Van Cauwenberge P, Verschraegen G, Van Renterghem L. Bacteriological findings in sinusitis (1963-1975). Scand J Infect Dis Suppl. 1976;(9):72-7. (PMID: 1070150)
67. Gwaltney JM, Sydnor A, Sande MA. Etiology and antimicrobial treatment of acute sinusitis. Ann Otol Rhinol Laryngol Suppl. 1981;90:68-71. (PMID: 6791566)
68. Jousimies-Somer HR, Savolainen S, Ylikoski JS. Bacteriological findings of acute maxillary sinusitis in young adults. J Clin Microbiol. 1988;26:1919-25. (PMID: 3182986)
69. Wald ER, Reilly JS, Casselbrant M, Ledesma-Medina J, Milmoe GJ, Bluestone CD, et al. Treatment of acute maxillary sinusitis in childhood: a comparative study of amoxicillin and cefaclor. J Pediatr. 1984;104:297-302. (PMID: 6363660)
70. Gwaltney JM, Scheld WM, Sande MA, Sydnor A. The microbial etiology and antimicrobial therapy of adults with acute community-acquired sinusitis: a fifteen-year experience at the University of Virginia and review of other selected studies. J Allergy Clin Immunol. 1992;90:457-61; discussion 462. (PMID: 1527337)
71. Suzuki K, Nishiyama Y, Sugiyama K, Miyamoto N, Baba S. Recent trends in clinical isolates from paranasal sinusitis. Acta Otolaryngol Suppl. 1996;525:51-5. (PMID: 8908270)
72. Antila J, Suonpää J, Lehtonen OP. Bacteriological evaluation of 194 adult patients with acute frontal sinusitis and findings of simultaneous maxillary sinusitis. Acta Otolaryngol Suppl. 1997;529:162-4. (PMID: 9288299)
73. Casiano RR. Azithromycin and amoxicillin in the treatment of acute maxillary sinusitis. Am J Med. 1991;91:27S-30S. (PMID: 1656739)
74. Felstead SJ, Daniel R. Short-course treatment of sinusitis and other upper respiratory tract infections with azithromycin: a comparison with erythromycin and amoxycillin. European Azithromycin Study Group. J Int Med Res. 1991;19:363-72. (PMID: 1660823)
75. Karma P, Pukander J, Penttilä M, Ylikoski J, Savolainen S, Olèc)n L, et al. The comparative efficacy and safety of clarithromycin and amoxycillin in the treatment of outpatients with acute maxillary sinusitis. J Antimicrob Chemother. 1991;27 Suppl A:83-90. (PMID: 1827106)

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 19 of 26
76. Calhoun KH, Hokanson JA. Multicenter comparison of clarithromycin and amoxicillin in the treatment of acute maxillary sinusitis. Arch Fam Med. 1993;2:837-40. (PMID: 8111512)
77. Huck W, Reed BD, Nielsen RW, Ferguson RT, Gray DW, Lund GK, et al. Cefaclor vs amoxicillin in the treatment of acute, recurrent, and chronic sinusitis. Arch Fam Med. 1993;2:497-503. (PMID: 8118565)
78. Edelstein DR, Avner SE, Chow JM, Duerksen RL, Johnson J, Ronis M, et al. Once-a-day therapy for sinusitis: a comparison study of cefixime and amoxicillin. Laryngoscope. 1993;103:33-41. (PMID: 8421417)
79. Matthews BL. Effectiveness and safety of cefixine and amoxicillin in adults with acute bacterial sinusitis. Suprax/Amoxicillin Clinical Study Team. Postgrad Med. 1997:41-49.
80. Rimmer D. Efficacy of cefixime and amoxicillin in adults with acute sinusitis. Suprax/Amoxicillin Clinical Study Team. Postgrad Med. 1997:50-7.
81. von Sydow C, Savolainen S, Söderqvist A. Treatment of acute maxillary sinusitis-comparing cefpodoxime proxetil with amoxicillin. Scand J Infect Dis. 1995;27:229-34. (PMID: 8539546)
82. Brodie DP, Knight S, Cunningham K. Comparative study of cefuroxime axetil and amoxycillin in the treatment of acute sinusitis in general practice. J Int Med Res. 1989;17:547-51. (PMID: 2628131)
83. Mattucci KF, Levin WJ, Habib MA. Acute bacterial sinusitis. Minocycline vs amoxicillin. Arch Otolaryngol Head Neck Surg. 1986;112:73-6. (PMID: 3484423)
84. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Executive summary. Sinus and Allergy Health Partnership. Otolaryngol Head Neck Surg. 2000;123:1-4. (PMID: 10887345)
85. Blin P, Blazejewski S, Lignot S, Lassalle R, Bernard MA, Jayles D, et al. Effectiveness of antibiotics for acute sinusitis in real-life medical practice. Br J Clin Pharmacol. 2010;70:418-28. (PMID: 20716243)
86. Falagas ME, Karageorgopoulos DE, Grammatikos AP, Matthaiou DK. Effectiveness and safety of short vs. long duration of antibiotic therapy for acute bacterial sinusitis: a meta-analysis of randomized trials. Br J Clin Pharmacol. 2009;67:161-71. (PMID: 19154447)
87. Clinical practice guideline: management of sinusitis. Pediatrics. 2001;108:798-808. (PMID: 11533355)
88. Snow V, Mottur-Pilson C, Hickner JM. Principles of appropriate antibiotic use for acute sinusitis in adults. Ann Intern Med. 2001;134:495-7. [Full Text] (PMID: 11255527)
89. Hickner JM, Bartlett JG, Besser RE, Gonzales R, Hoffman JR, Sande MA. Principles of appropriate antibiotic use for acute rhinosinusitis in adults: background. Ann Intern Med. 2001;134:498-505. [Full Text] (PMID: 11255528)
90. Arason VA, Kristinsson KG, Sigurdsson JA, Stefánsdóttir G, Mölstad S, Gudmundsson S. Do antimicrobials increase the carriage rate of penicillin resistant pneumococci in children? Cross sectional prevalence study. BMJ. 1996;313:387-91. (PMID: 8761224)
91. Seppälä H, Klaukka T, Lehtonen R, Nenonen E, Huovinen P. Outpatient use of erythromycin: link to increased erythromycin resistance in group A streptococci. Clin Infect Dis. 1995;21:1378-85. (PMID: 8749619)
92. Nissinen A, Grönroos P, Huovinen P, Herva E, Katila ML, Klaukka T, et al. Development of beta-lactamase-mediated resistance to penicillin in middle-ear isolates of Moraxella catarrhalis in Finnish children, 1978-1993. Clin Infect Dis. 1995;21:1193-6. (PMID: 8589142)
93. Ahovuo-Saloranta A, Borisenko OV, Kovanen N, Varonen H, Rautakorpi UM, Williams JW Jr, Mäkelä M. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev. 2008;(2):CD000243. (PMID: 18425861)

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 20 of 26
Glossary Top
AIDS acquired immunodeficiency syndrome
bid twice daily
CT computed tomography
HIV human immunodeficiency virus
LR+
Positive likelihood ratio
MRI
magnetic resonance imaging
NNT number needed to treat
qd once daily
qid
four times daily
tid three times daily
URI upper respiratory (tract) infection
Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 21 of 26
Tables Top
Laboratory and Other Studies for Acute Sinusitis
Test Sensitivity (%) Specificity (%) Likelihood Ratio Positive Likelihood Ratio Negative Notes
Sinus radiography 90 61 2.3 0.26 Not recommended in acute
sinusitis. Chronic cases may
show opacification, mucous thickening, or fluid
Sinus ultrasonography Not recommended in acute
sinusitis. Variable results in
three studies, precluding
synthesis; unlikely to have good
diagnostic performance
Sinus CT and MRI Not recommended in acute
sinusitis. No comparison against
sinus puncture, the gold
standard
Sinus puncture The gold standard for diagnosis
but too invasive for routine use
CT = computed tomography; MRI = magnetic resonance imaging.
Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 22 of 26
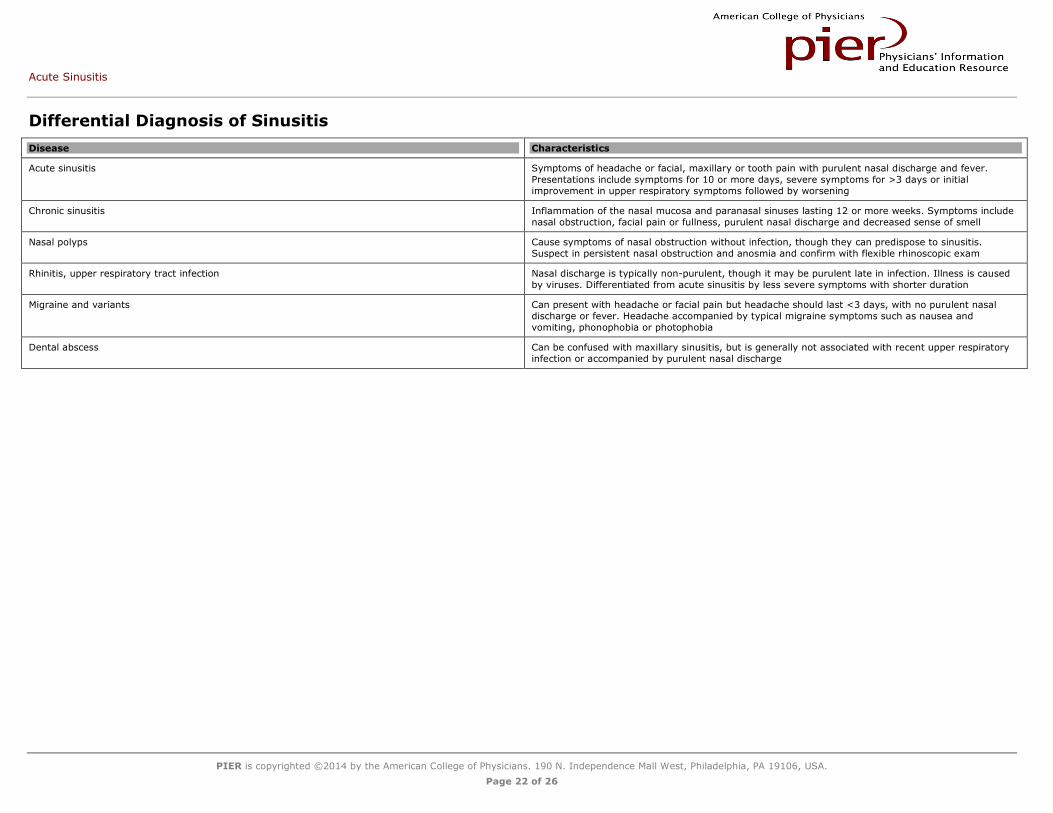
Differential Diagnosis of Sinusitis
Disease Characteristics
Acute sinusitis Symptoms of headache or facial, maxillary or tooth pain with purulent nasal discharge and fever.
Presentations include symptoms for 10 or more days, severe symptoms for >3 days or initial
improvement in upper respiratory symptoms followed by worsening
Chronic sinusitis Inflammation of the nasal mucosa and paranasal sinuses lasting 12 or more weeks. Symptoms include
nasal obstruction, facial pain or fullness, purulent nasal discharge and decreased sense of smell
Nasal polyps Cause symptoms of nasal obstruction without infection, though they can predispose to sinusitis.
Suspect in persistent nasal obstruction and anosmia and confirm with flexible rhinoscopic exam
Rhinitis, upper respiratory tract infection Nasal discharge is typically non-purulent, though it may be purulent late in infection. Illness is caused
by viruses. Differentiated from acute sinusitis by less severe symptoms with shorter duration
Migraine and variants Can present with headache or facial pain but headache should last <3 days, with no purulent nasal
discharge or fever. Headache accompanied by typical migraine symptoms such as nausea and
vomiting, phonophobia or photophobia
Dental abscess Can be confused with maxillary sinusitis, but is generally not associated with recent upper respiratory
infection or accompanied by purulent nasal discharge
Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 23 of 26
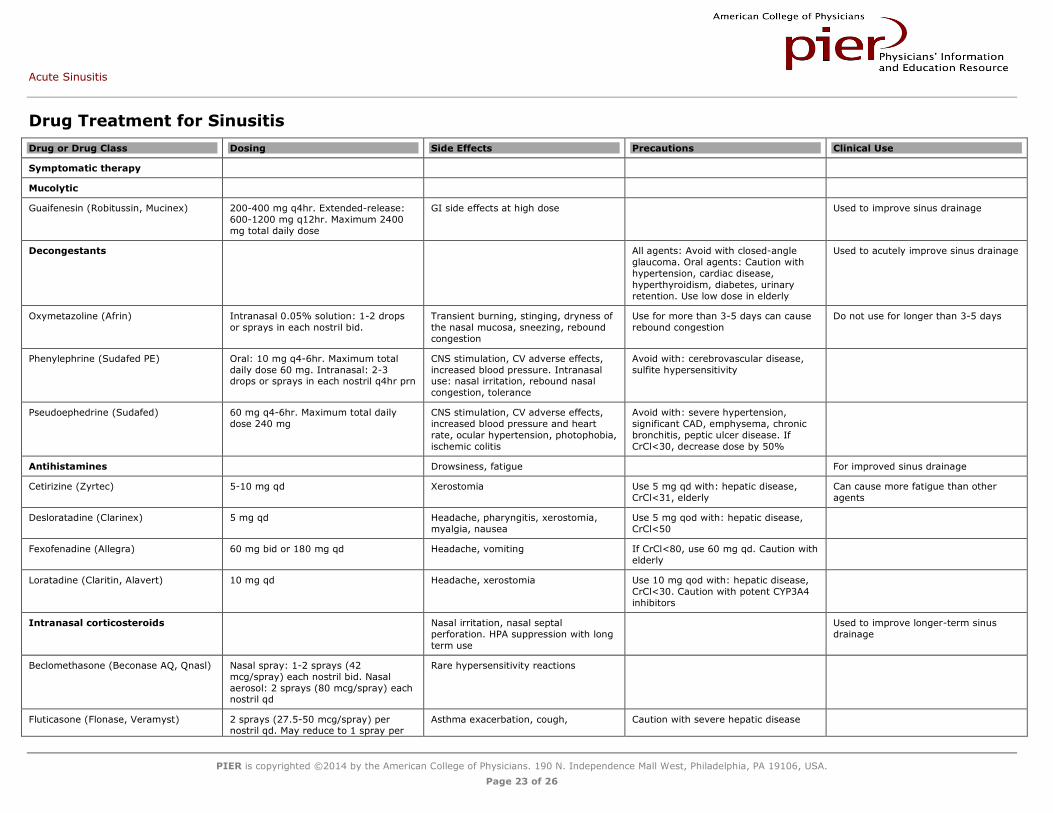
Drug Treatment for Sinusitis
Drug or Drug Class Dosing Side Effects Precautions Clinical Use
Symptomatic therapy
Mucolytic
Guaifenesin (Robitussin, Mucinex) 200-400 mg q4hr. Extended-release:
600-1200 mg q12hr. Maximum 2400
mg total daily dose
GI side effects at high dose Used to improve sinus drainage
Decongestants All agents: Avoid with closed-angle
glaucoma. Oral agents: Caution with
hypertension, cardiac disease,
hyperthyroidism, diabetes, urinary
retention. Use low dose in elderly
Used to acutely improve sinus drainage
Oxymetazoline (Afrin) Intranasal 0.05% solution: 1-2 drops
or sprays in each nostril bid.
Transient burning, stinging, dryness of
the nasal mucosa, sneezing, rebound
congestion
Use for more than 3-5 days can cause
rebound congestion
Do not use for longer than 3-5 days
Phenylephrine (Sudafed PE) Oral: 10 mg q4-6hr. Maximum total
daily dose 60 mg. Intranasal: 2-3 drops or sprays in each nostril q4hr prn
CNS stimulation, CV adverse effects,
increased blood pressure. Intranasal use: nasal irritation, rebound nasal
congestion, tolerance
Avoid with: cerebrovascular disease,
sulfite hypersensitivity
Pseudoephedrine (Sudafed) 60 mg q4-6hr. Maximum total daily
dose 240 mg
CNS stimulation, CV adverse effects,
increased blood pressure and heart
rate, ocular hypertension, photophobia,
ischemic colitis
Avoid with: severe hypertension,
significant CAD, emphysema, chronic
bronchitis, peptic ulcer disease. If
CrCl<30, decrease dose by 50%
Antihistamines Drowsiness, fatigue For improved sinus drainage
Cetirizine (Zyrtec) 5-10 mg qd Xerostomia Use 5 mg qd with: hepatic disease,
CrCl<31, elderly
Can cause more fatigue than other
agents
Desloratadine (Clarinex) 5 mg qd Headache, pharyngitis, xerostomia,
myalgia, nausea
Use 5 mg qod with: hepatic disease,
CrCl<50
Fexofenadine (Allegra) 60 mg bid or 180 mg qd Headache, vomiting If CrCl<80, use 60 mg qd. Caution with
elderly
Loratadine (Claritin, Alavert) 10 mg qd Headache, xerostomia Use 10 mg qod with: hepatic disease,
CrCl<30. Caution with potent CYP3A4
inhibitors
Intranasal corticosteroids Nasal irritation, nasal septal
perforation. HPA suppression with long
term use
Used to improve longer-term sinus
drainage
Beclomethasone (Beconase AQ, Qnasl) Nasal spray: 1-2 sprays (42
mcg/spray) each nostril bid. Nasal
aerosol: 2 sprays (80 mcg/spray) each nostril qd
Rare hypersensitivity reactions
Fluticasone (Flonase, Veramyst) 2 sprays (27.5-50 mcg/spray) per nostril qd. May reduce to 1 spray per
Asthma exacerbation, cough, Caution with severe hepatic disease
Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 24 of 26
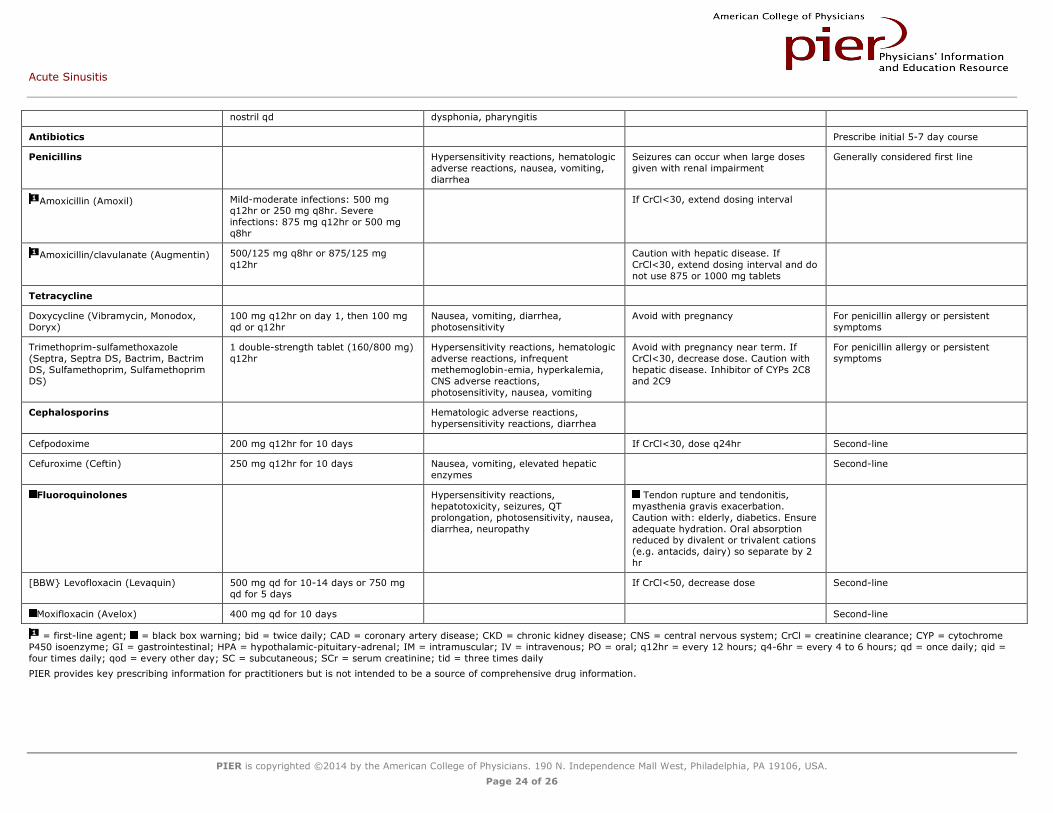
nostril qd dysphonia, pharyngitis
Antibiotics Prescribe initial 5-7 day course
Penicillins Hypersensitivity reactions, hematologic
adverse reactions, nausea, vomiting,
diarrhea
Seizures can occur when large doses
given with renal impairment
Generally considered first line
Amoxicillin (Amoxil) Mild-moderate infections: 500 mg q12hr or 250 mg q8hr. Severe
infections: 875 mg q12hr or 500 mg
q8hr
If CrCl<30, extend dosing interval
Amoxicillin/clavulanate (Augmentin) 500/125 mg q8hr or 875/125 mg
q12hr
Caution with hepatic disease. If
CrCl<30, extend dosing interval and do
not use 875 or 1000 mg tablets
Tetracycline
Doxycycline (Vibramycin, Monodox,
Doryx)
100 mg q12hr on day 1, then 100 mg
qd or q12hr
Nausea, vomiting, diarrhea,
photosensitivity
Avoid with pregnancy For penicillin allergy or persistent
symptoms
Trimethoprim-sulfamethoxazole
(Septra, Septra DS, Bactrim, Bactrim
DS, Sulfamethoprim, Sulfamethoprim
DS)
1 double-strength tablet (160/800 mg)
q12hr
Hypersensitivity reactions, hematologic
adverse reactions, infrequent
methemoglobin-emia, hyperkalemia,
CNS adverse reactions,
photosensitivity, nausea, vomiting
Avoid with pregnancy near term. If
CrCl<30, decrease dose. Caution with
hepatic disease. Inhibitor of CYPs 2C8
and 2C9
For penicillin allergy or persistent
symptoms
Cephalosporins Hematologic adverse reactions,
hypersensitivity reactions, diarrhea
Cefpodoxime 200 mg q12hr for 10 days If CrCl<30, dose q24hr Second-line
Cefuroxime (Ceftin) 250 mg q12hr for 10 days Nausea, vomiting, elevated hepatic
enzymes
Second-line
Fluoroquinolones Hypersensitivity reactions,
hepatotoxicity, seizures, QT
prolongation, photosensitivity, nausea,
diarrhea, neuropathy
Tendon rupture and tendonitis,
myasthenia gravis exacerbation.
Caution with: elderly, diabetics. Ensure
adequate hydration. Oral absorption reduced by divalent or trivalent cations
(e.g. antacids, dairy) so separate by 2
hr
[BBW} Levofloxacin (Levaquin) 500 mg qd for 10-14 days or 750 mg
qd for 5 days
If CrCl<50, decrease dose Second-line
Moxifloxacin (Avelox) 400 mg qd for 10 days Second-line
= first-line agent; = black box warning; bid = twice daily; CAD = coronary artery disease; CKD = chronic kidney disease; CNS = central nervous system; CrCl = creatinine clearance; CYP = cytochrome
P450 isoenzyme; GI = gastrointestinal; HPA = hypothalamic-pituitary-adrenal; IM = intramuscular; IV = intravenous; PO = oral; q12hr = every 12 hours; q4-6hr = every 4 to 6 hours; qd = once daily; qid =
four times daily; qod = every other day; SC = subcutaneous; SCr = serum creatinine; tid = three times daily
PIER provides key prescribing information for practitioners but is not intended to be a source of comprehensive drug information.
Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 25 of 26
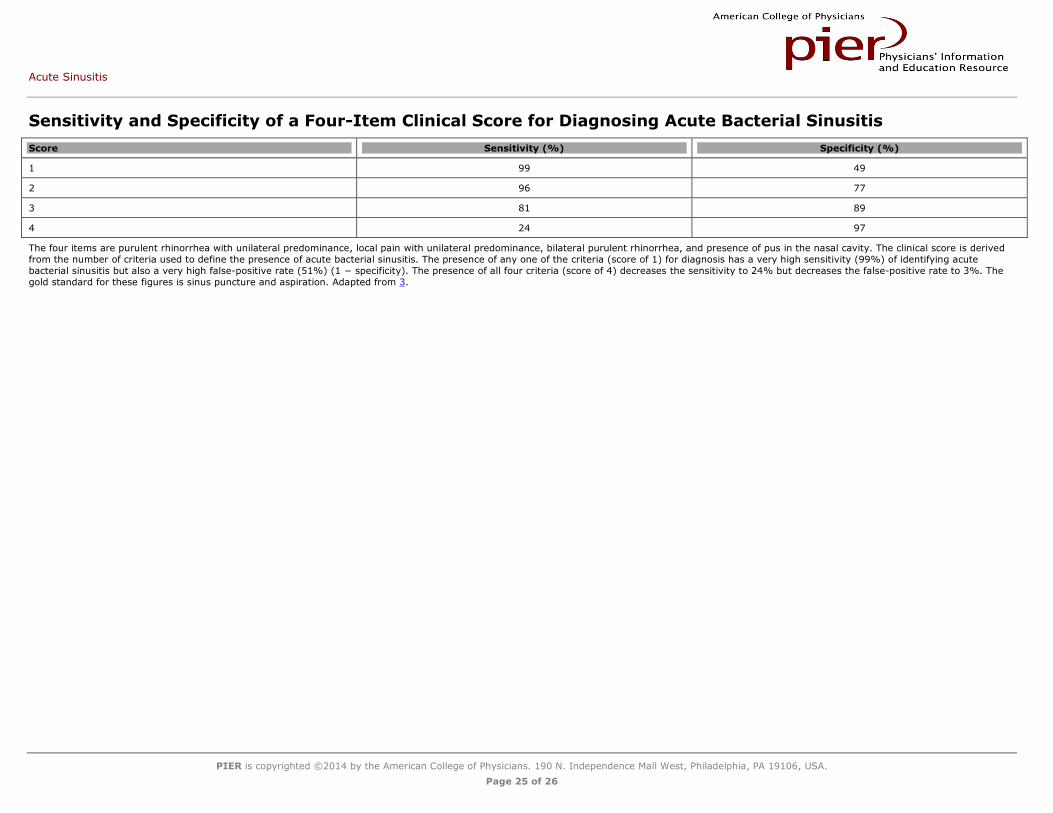
Sensitivity and Specificity of a Four-Item Clinical Score for Diagnosing Acute Bacterial Sinusitis
Score Sensitivity (%) Specificity (%)
1 99 49
2 96 77
3 81 89
4 24 97
The four items are purulent rhinorrhea with unilateral predominance, local pain with unilateral predominance, bilateral purulent rhinorrhea, and presence of pus in the nasal cavity. The clinical score is derived
from the number of criteria used to define the presence of acute bacterial sinusitis. The presence of any one of the criteria (score of 1) for diagnosis has a very high sensitivity (99%) of identifying acute
bacterial sinusitis but also a very high false-positive rate (51%) (1 − specificity). The presence of all four criteria (score of 4) decreases the sensitivity to 24% but decreases the false-positive rate to 3%. The
gold standard for these figures is sinus puncture and aspiration. Adapted from 3.

Acute Sinusitis
PIER is copyrighted ©2014 by the American College of Physicians. 190 N. Independence Mall West, Philadelphia, PA 19106, USA.
Page 26 of 26
Cost-Effective Treatment, Based on Disease Likelihood
Initial Likelihood (%) Management Plan
0-25 Symptomatic treatment
25-83 Apply clinical decision rule to decide on antibiotic use*
>83 Empirical antibiotics†
* For example, use antibiotics if at least two of the following four criteria are present: purulent rhinorrhea with unilateral predominance, local pain with unilateral predominance, bilateral purulent rhinorrhea,
and pus in the nasal cavity. More strict clinical criteria would restrict antibiotic treatment to patients who meet all of the following criteria: symptoms of URI for 7 days or more, facial pain or discomfort, and
purulent discharge in the nose or pharynx. Less strict criteria call for meeting two of those three criteria.
† First-line options include amoxicillin, 500 mg tid, or sulfamethoxazole, 800 mg plus trimethoprim, 160 mg bid for 3 days.
bid = twice daily; tid = three times daily; URI = upper respiratory (tract) infection.