acute respiratory distress syndrome · short-term clinical benefits ... decrease shunting of blood...
TRANSCRIPT

Acute Respiratory Distress Syndrome

ARDS
Lung complication resulting in dangerously low blood
oxygen
ARDS is often a result of other health complications
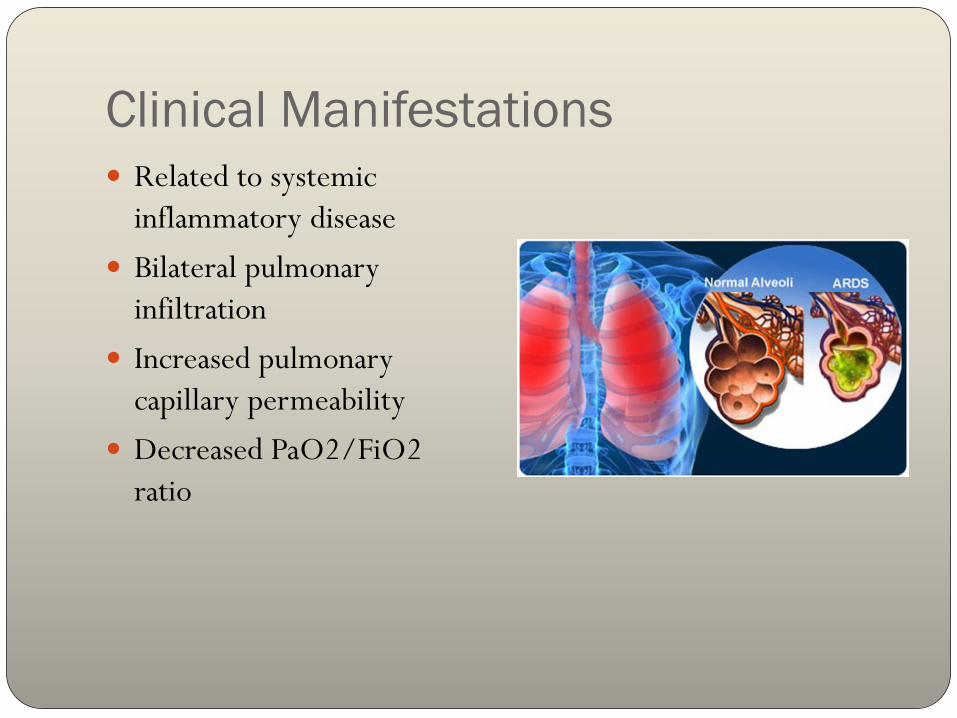
Clinical Manifestations
Related to systemic
inflammatory disease
Bilateral pulmonary
infiltration
Increased pulmonary
capillary permeability
Decreased PaO2/FiO2
ratio

Severity Stages
New classification system
Better predictor of mortality
Three classifications:
Mild PaO2/FiO2 <300 mmHg
Acute lung injury
Moderate <200 mmHg
Severe <100 mmHg
75% of cases are classified moderate or severe

Incidence
9% incidence of ARDS and ALL in the ICU
United States: 64:100,000
Europe: 4.9-13.5:100,000
American Lung Association: 1.5-75 cases/100,000
individuals
25-40% of cases end in death

Increasing Incidence of ARDS cases

Life Expectancy
Dependent of cause of ARDS
Patients with fewer chronic diseases have increased survival
Sepsis induced ARDS has increased risk of mortality
Pulmonary fibrosis is found to be a major factor
1988: 50-70% mortality
2008: 25-40% mortality
Death typically results from MODS from a lack of oxygen
rather than lung failure

Decreasing mortality risk for ARDS patients

Etiology
Direct injury:
Trauma
Aspiration
Inhaling Chemicals
Obstructed airways
Indirect injury
Blood transfusion
Sepsis
Pneumonia

Signs and Symptoms
Depending on the initial trauma specific S/S can occur
Ex. Pneumonia cough
Difficulty breathing
Two-pillow orthopnea: support from pillows to in order to easy
breathing that occurs from the recumbent position
Rapid breathing
Shortness of Breath
Low blood oxygen level

S/S continued Trachea shift: trachea shifts
from its normal position because of fluid accumulation in the pleural space
Jugular distention: jugular veins bulge because of increased central venous pressure
Bruit: “noise” unusual sound blood makes when passing an obstruction Medical professionals will
look for bruit sounds to R/O other diseases

Pathophysiology Early phase: exudative (oozing)
Occur as a result of direct or indirect lung insults Acute inflammatory stage with proinflammatory cytokines, neutrophils,
and overall impaired endothelial cell barrier function
Barrier between the capillaries and the alveoli allow water movement into the alveoli
Most patients will survive this stage
Later phase: fibroproliferative
Alveolar damage
Collagen deposition appears in 3 days; Fibrosis manifests within 3 weeks
Pulmonary fibrosis resulting in 55% of ARDS deaths


Risk Factors
Old age
Shock
Liver failure
Patients with diabetes have half the risk for developing ARDS
compared to patients without diabetes

Quality of Life Poor muscle function
Pulmonary function returns to normal or near normal at approx. 6 months
Decrease carbon monoxide diffusion capacity
Memory loss: due to brain damage from lack of oxygen
Fatigue
Weakness
Alopecia
Pain from chest tubes
Entrapment Neuropathy
Heterotopic Ossification

Medical Therapy

Diagnosis
Challenging because ARDS has nonspecific characteristics
48% of patients with autopsy-prove ARDS had ARDS diagnosis
in their charts

Rule out other diseases
Left heart failure
Check left heart function
Acute lung injury
Less severe impairment of oxygen; PaO2/FiO2 <300 mmHg

Goals of Treatment
Support breathing
Treat underlying cause
Medications to treat infections, reduce inflammation, and
remove fluid from the lungs.

Health Impact
25-40% of cases are fatal
By 7-10 days a patient has
died or have been weaned
off treatment

Collapsed Lung
Pneumothorax
Air escapes from the lung
and fills the space outside
the lung.
Smokers, COPD, asthma,
cystic fibrosis, tuberculosis

Collapsed Lung
Increased Risk
Smokers
COPD
Asthma
Cystic fibrosis
Tuberculosis
Symptoms
Sharp chest pain
Shortness of breath
Bluish color
Easy fatigue
Rapid heart rate

Treatment
Small pneumothorax
Can go away on its own
Large Pneumothorax
Chest tube
Surgery
Pleurodesis

Surgery
Treat collapsed lung
Stop fluid buildup

Pulmonary Fibrosis
Scarring throughout the lungs

Prevention of ARDS
No drug has proved beneficial in prevention

Corticosteroids
High-dose corticosteroids
Patients with ARDS persisting for at least 7 days had no benefit
in 60 day mortality
Patients treated 14 days after onset had worsened mortality
with corticosteroid therapy
Methylprednisone
No survival advantage shown
short-term clinical benefits included improved oxygenation and
increased ventilator-free and shock-free days
more likely to experience neuromuscular weakness, but the rate
of infectious complications was not increased.

Corticosteroids Summary
may be considered a form of rescue therapy
may improve oxygenation and hemodynamics
does not change mortality
corticosteroids increase mortality in patients who have had
ARDS for >14 d

Statins
Somovstatin
Preadmission use of statins was associated with a reduction in
30-day and 1-year mortality of a cohort of 12,483 critically ill
patients.
Patients under statin treatment developing MODS have a better
outcome than age- and sex-matched MODS patients without
statin therapy.


TNF and IL-1
Small sepsis trials suggest a potential role for antibody to
tumor necrosis factor (TNF) and recombinant interleukin
(IL)-1 receptor antagonist.

Prostacycline
Prostacycline
Inhaled prostacycline also has not been shown to improve
survival.

Nitric Oxide
Inhaled nitric oxide did not change mortality rates in adults
with ARDS.
Improves transient oxygenation

Side Effects
Short-term
Long-term
Muscle wasting and weakness

Mechanical Ventilation

Ventilation
A ventilator doesn’t treat a disease or condition
GOAL: provide breathing support, relieve respiratory
muscles of their work

Ventilation Benefits
Get oxygen into the lungs
Help people breathe easier – relieve respiratory muscles
Provide breathing support


Mask Ventilation

Intubation
Tube is placed in patients mouth and down into the windpipe

High vs. Low Tidal Volume
High Tidal Volume Low Tidal Volume
Over-distend alveoli
Worsen lung injury
Inflammation
Decreased ventilator-
associated lung injury
Increases survival rate
Recommended to use Low Tidal Volume for ARDS

Positive End-Expiratory Pressure
(PEEP)
Airway pressure is maintained above atmospheric pressure at
the end of exhalation
increase volume of gas remaining in the lungs at the end of
expiration
Decrease shunting of blood through lungs and improve gas
exchange
Purpose: Prevent lungs from collapsing

Prone Positioning
Supine: weight of heart and abdominal
organs on lungs contribute to low
compliancy
Prone: improves oxygenation but does
not improve survival
Higher incidence of complications (i.e.
pressure sores and obstruction of the
endotracheal tube)

Weaning from Mechanical Ventilation
Those who wean successfully have less morbidity and
mortality
Spontaneous breathing trials (SBTs)
Progressive decreases in the level of pressure support during
pressure support ventilation

Extracorporeal Membrane Oxygenation
(ECMO)
Blood circulates
outside of body with
help of a machine
Provides oxygenation
and takes out CO2
For severely/non-functional lungs

The Cochrane Library http://onlinelibrary.wiley.com.erl.lib.byu.edu/doi/10.1002/14651858.CD00
3844.pub4/full
Primary outcome
Mortality
Secondary Outcomes Development of multiple organ failure
Duration of mechanical ventilation
Stay in ICU
Long term health related quality of life
Long-term cognitive complications

Hemolung RAS
CO2 removal and less invasive
Similar to dialysis
Uses less blood flow
Smaller catheter
One component system
Active mixing
Battery operated (patient
can move around)

Hemolung RAS
2012
Successful pilot studies
Arterial pCO2 levels reduced by 28% within 24 hours
lessened dyspnea
improved clinical status
effective and stable CO2 removal on the order of 50% of
metabolic production
No unexpected adverse events
All patients were able to avoid intubation

Approved in Canada and Europe
Undergoing large clinical trials

Medical Nutrition Therapy

Medical Nutrition Therapy
MNT GOALS
Hemodynamically stable through fluid administration
Meet nutritional requirements
Facilitate weaning from mechanical ventilation and oxygen
support
Maintain lean body mass
Improve resistance to infection
Restore respiratory muscle and strength

Medical Nutrition Therapy
Fluid administration: Conservative
administration of fluids after resuscitation
Energy Needs: • Calculate with indirect calorimetry (IC)
• Obese individuals : 11-14 kcal/kg or
60%-70% of target value
• Why: High caloric intake increases
levels of CO2.

Medical Nutrition Therapy
Carbohydrate:
Been shown that concentrations of Carbohydrates not as
important as calories provided
Protein:
1.5-2.0 g/kg
For Obese: 2.0-2.5 g/kg
Fat:
Give enough to provide the right amount of calories

Medical Nutrition Therapy
What to monitor and watch closely
CO2
Phosphate
Vitamin A
Vitamin C
Vitamin E
Meet requirements for Essential Fatty Acids
Medical Nutrition Therapy
Enteral Nutrition
Helps maintain GALT
Less likely to overfeed
Reduces ICU and hospital mortality
Parental Nutrition
More likely to overfeed
Used for patients with: Shock, Nonfunctional Gut, and
Peritonitis

Medical Nutrition Therapy Supplementing with arginine, glutamine, omega-3 fatty acids,
and antioxidants?
Improved Oxygenation, Reduced
number of neutrophils, decreased
length of stay, decreased requirement
for mechanical ventilation
No effect on Mortality
Pulmonary Rehabilitation Programs Small portions
Give favorite foods

Medical Nutrition Therapy
Supplementation of Omega 3 over required amounts not
effective.
Do not use RQ for substrate mix
Consider BMI

Case Study: DH
Anthropometrics
Age: 65
Male
Married – lives with wife (62)
4 children not living in the area
Retired manager of local grocery
chain
Height: 5’ 4”
Weight: 122 lbs
BMI: 20.9
UBW: 135 lbs
IBW: 130 lbs
8 lbs under
Case Study: DH
Biochemical Clinical
Hemoglobin – 13.2 (14-17)
Hematocrit – 39 (40-54)
ABG pH – 7.2 (7.35-7.45)
ABG pCO2 – 65 (35-45)
ABG CO2 content – 35 (25-30)
ABG pO2 – 56 (>80)
ABG HCO3- – 38 (24-28)
Extremities: cyanosis, 1+ pitting
edema
R femoral bruit present
Pale skin
Harsh inspiratory breath sounds
noted over right chest – absent
sounds on left
Use accessory muscles at rest

Case Study – DH
Dietary History
General appetite: decreased over
past several weeks
Usual diet:
B: Egg, hot cereal, bread or
muffin, hot tea (with milk and
sugar)
L: soup, sandwich, hot tea (with
milk and sugar)
D: small amount of meat, rice,
2-3 kinds of vegetables, hot tea
(with milk and sugar)
Diagnosed with emphysema more
than 10 years ago
Tobacco use: 2 PPD for 50 years
Alcohol use: 1-2 drinks 1-2
x/week

PES Statement
Inadequate caloric intake related to increased needs from
history of COPD and Acute Respiratory Distress Syndrome as
evidenced by decrease appetite and weight loss.

Oxepa®
Abbott Nutrition product for
modulating Inflammation in Sepsis,
ALI, and ARDS
Benefits:
Improves oxygenation
Decrease time on ventilator
Decreases length of stay in ICU
For sole-source nutrition

Sample Diet Oxepa – 25 kcal/kg for 24 hrs
55kg (122lbs) – 1375 kcals
Protein needs: minimum 82.5 g (1.5-2.0g/kg)
Amount Calories
(kcal)
% in total
Calories
CHO 97 g 388 27
Protein 57.3 g 250.8 18
Fat 86 g 774 55
Fluid 917 ml 0 0
Total
Calories/24
hours
1412