acute myeloid leukemia: what’s new on the horizon?
TRANSCRIPT

Acute Myeloid Leukemia: What’s New on the Horizon?Final Outcomes Report Jazz Pharmaceuticals Grant

Activity Description: This on-demand activity, featuring renowned faculty Naval Daver, MD from the University of Texas MD Anderson Cancer Center, was recorded during a regional visiting lecture series that reviewed the latest clinical trial data and strategies for integrating novel treatments into precision medicine for Acute Myeloid Leukemia (AML). In addition to the educational content, this activity offered downloadable resources and slides to support clinicians who manage patients with AML and the improvement of the care they provide.
Launch Date: April 22, 2020Expiration Date: April 22, 2021
Credit: 1.0 AMA PRA Category 1 CreditsTM
Sponsor: The University of Texas MD Anderson Cancer CenterEducational Partner: The Academy for Continued Healthcare Learning (ACHL)
Supported by: An educational grant from Jazz Pharmaceuticals, Inc.
Intended Audience: Hematologists, oncologists and other healthcare professionals involved in the care of patients with AML such as pharmacists, oncology nurses, nurse practitioners, physician assistants.
Activity Availability: myCME.com (expired): https://www.mycme.com/courses/acute-myeloid-leukemia-whats-new-on-the-horizon-7046 ACHLcme.org: https://www.achlcme.org/AMLwhatsnewonthehorizon Direct access: https://www.achlcme.org/digital/AMLVPP/index.html
Overview

Activity Screenshots
Naval Daver, MDAssociate ProfessorDepartment of LeukemiaDivision of Cancer MedicineThe University of Texas MD Anderson Cancer Center
70% of learners will discuss the option of
enrolling eligible patients in clinical trials for AML
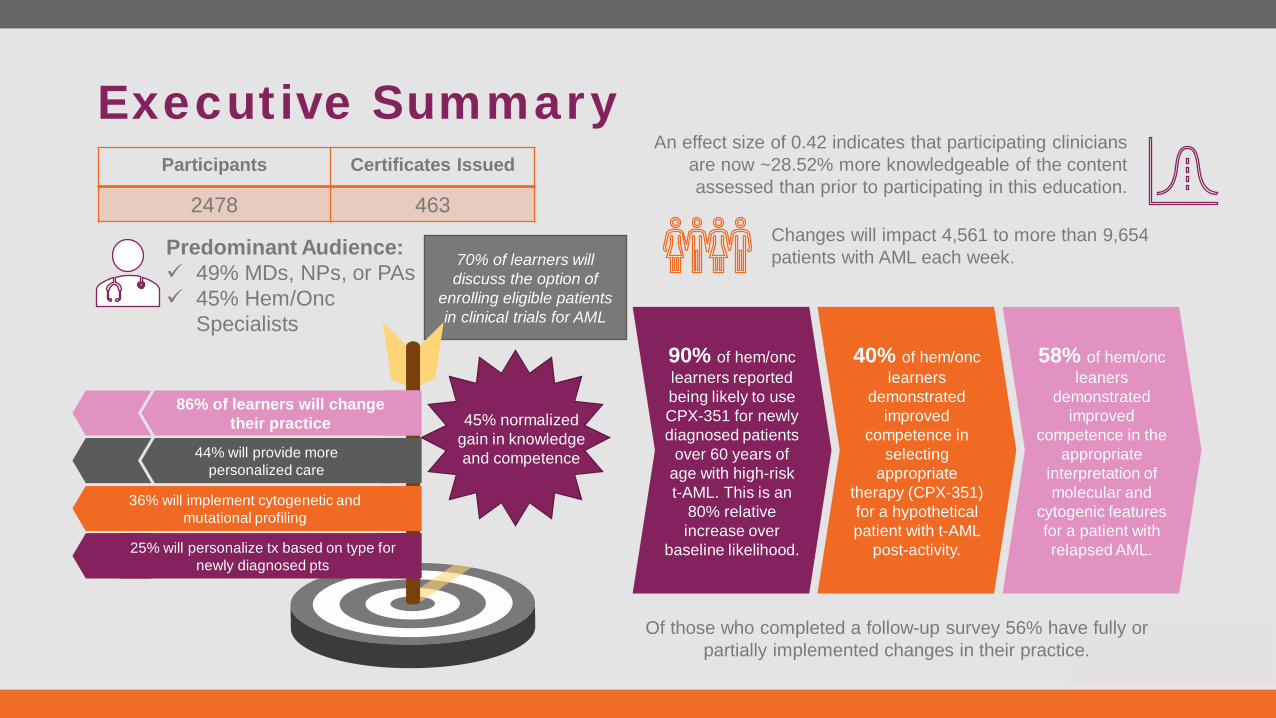
Executive SummaryParticipants Certificates Issued
2478 463
Predominant Audience: 49% MDs, NPs, or PAs 45% Hem/Onc
Specialists
Changes will impact 4,561 to more than 9,654 patients with AML each week.
45% normalized gain in knowledge and competence44% will provide more
personalized care
86% of learners will change their practice
25% will personalize tx based on type for newly diagnosed pts
36% will implement cytogenetic and mutational profiling
Of those who completed a follow-up survey 56% have fully or partially implemented changes in their practice.
58% of hem/onc leaners
demonstrated improved
competence in the appropriate
interpretation of molecular and
cytogenic features for a patient with relapsed AML.
40% of hem/onc learners
demonstrated improved
competence in selecting
appropriate therapy (CPX-351) for a hypothetical patient with t-AML
post-activity.
90% of hem/onc learners reported being likely to use CPX-351 for newly diagnosed patients
over 60 years of age with high-risk t-AML. This is an
80% relative increase over
baseline likelihood.
An effect size of 0.42 indicates that participating clinicians are now ~28.52% more knowledgeable of the content assessed than prior to participating in this education.

Outcomes Reporting Methodology• First-attempt posttest scores are reported throughout:
• Initial answer choices for the posttest provide insight into the learners’ ability to immediately recall and apply the education.
• Pre- and posttest responses have been paired/matched. Non-completer data has been omitted from the analysis to ensure comparison groups are equivalent.
Terminology Defined:• Participant: term used to describe an HCP who reviewed CME front matter and
took action to begin the education.• Hematology/Oncology learner: self-identified physician, nurse practitioner, or
physician assistant specializing in hematology or oncology who consumed the education.
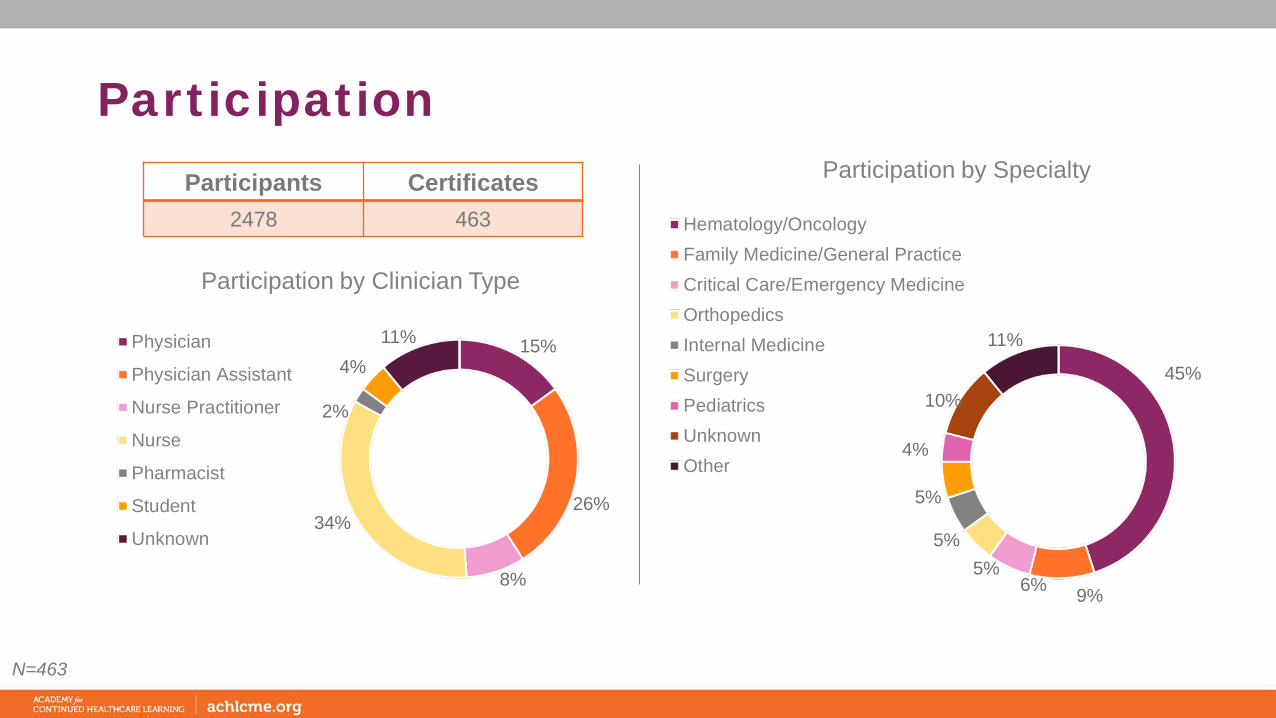
Participation
15%
26%
8%
34%
2%
4%11%
Participation by Clinician Type
Physician
Physician Assistant
Nurse Practitioner
Nurse
Pharmacist
Student
Unknown
Participants Certificates 2478 463
45%
9%6%5%
5%
5%
4%
10%
11%
Participation by Specialty
Hematology/OncologyFamily Medicine/General PracticeCritical Care/Emergency MedicineOrthopedicsInternal MedicineSurgeryPediatricsUnknownOther
N=463
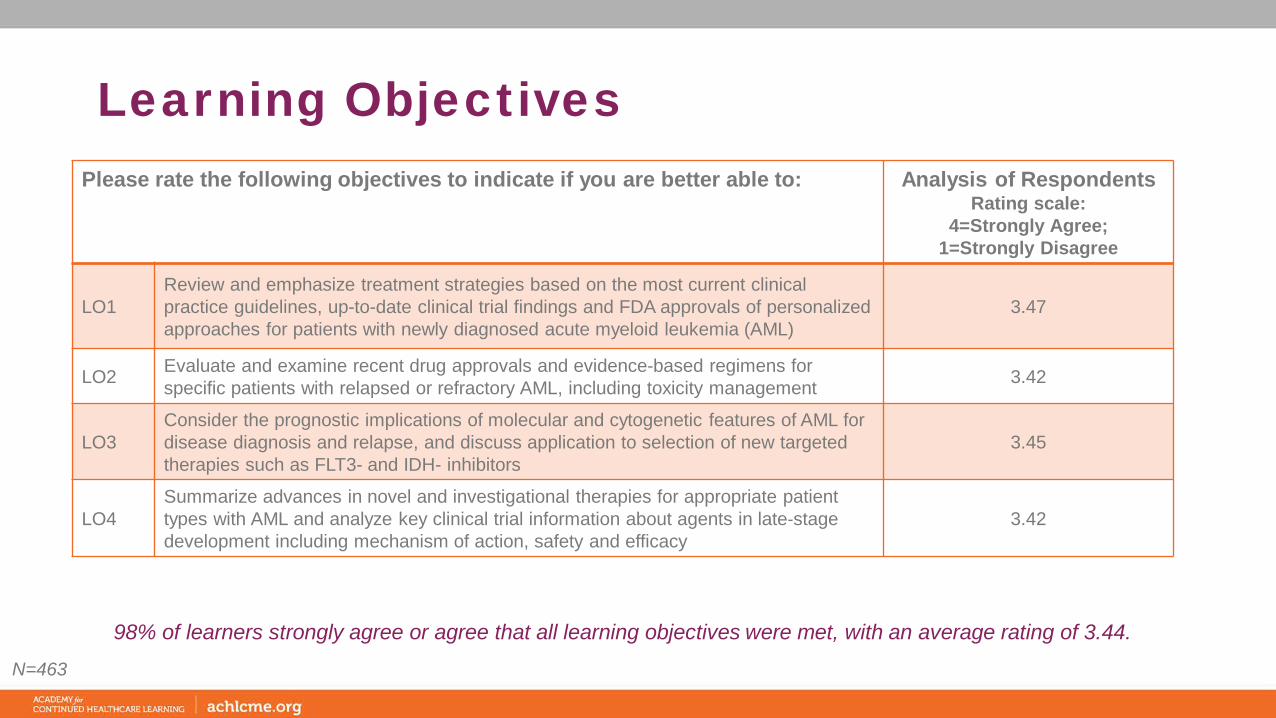
Learning ObjectivesPlease rate the following objectives to indicate if you are better able to: Analysis of Respondents
Rating scale: 4=Strongly Agree;
1=Strongly Disagree
LO1Review and emphasize treatment strategies based on the most current clinical practice guidelines, up-to-date clinical trial findings and FDA approvals of personalized approaches for patients with newly diagnosed acute myeloid leukemia (AML)
3.47
LO2 Evaluate and examine recent drug approvals and evidence-based regimens for specific patients with relapsed or refractory AML, including toxicity management 3.42
LO3Consider the prognostic implications of molecular and cytogenetic features of AML for disease diagnosis and relapse, and discuss application to selection of new targeted therapies such as FLT3- and IDH- inhibitors
3.45
LO4Summarize advances in novel and investigational therapies for appropriate patient types with AML and analyze key clinical trial information about agents in late‐stage development including mechanism of action, safety and efficacy
3.42
N=463
98% of learners strongly agree or agree that all learning objectives were met, with an average rating of 3.44.

Overall Evaluation
N=463
Please evaluate the following criteria: Analysis of RespondentsRating scale: 4=Excellent; 1=Poor
Quality of the educational content 3.56
The presenters’ ability to effectively convey the subject matter 3.55
83% confirm this
education will increase their competence
77% attest the content was relevant to their practice
67% discuss the option of enrolling eligible patients in clinical
trials for AML
72% report this activity will improve their patient outcomes
77% report education
received from this activity will
increase their performance
Self-reported attestations:

Objectivity & Balance
Activity was perceived as objective, balanced, and non-biased.
95%
5%
This activity was free of commercial bias:
Yes No
60%
38%
2%0%
10%
20%
30%
40%
50%
60%
70%
Excellent Good Fair Poor
Rating of objectivity & balance
N=463

Clinical Confidence: Tx Selection
Interestingly, baseline confidence in the selection of therapy for newly diagnosed AML patients was lower in hem/onc learners. Nonetheless, both groups of learners reported an increase in confidence after their participation.
How confident are you in selecting appropriate therapy for a patient with newly diagnosed treatment-related AML based on patient and disease characteristics?
A. Very confidentB. Somewhat confidentC. Not at all confident
15%
42%
20%
43%54%
80%
42%
3%0%
20%
40%
60%
80%
100%
Pre
Post
Follo
w-u
p
Pre
Post
Follo
w-u
p
Pre
Post
Follo
w-u
p
Very Somewhat Not at all
Hem/Onc (n=211)
Follow-up n=10
18%
34%
67%
41%
55%
33%41%
11%
0%
20%
40%
60%
80%
100%
Pre
Post
Follo
w-u
p
Pre
Post
Follo
w-u
p
Pre
Post
Follo
w-u
p
Very Somewhat Not at all
Other HCPs (n=261)
Follow-up n=6

Clinical Frequency: Tx Selection
Prior to their participation in the activity, 50-55% of learners reported not at all likely to use CPX-351 for a newly diagnosed patient over 60 years old with t-AML; however, marked improvements were observed post-activity. Both learner types reported being more likely to use CPX-351 in this clinical scenario after their participation, with 41% of hem/onc learners reporting being “very” likely to
use CPX-351 in this situation.
How likely are you to select CPX-351 (Liposomal Cytarabine and Daunorubicin) vs. standard-of-care cytarabine plus daunorubicin chemotherapy for a newly diagnosed patient over 60 years of age with high-risk therapy-related AML (t-AML)?
A. Very likely B. Somewhat likely C. Not at all likely
10%
41%
20%
40%49%
60%50%
10%20%
0%
20%
40%
60%
80%
100%
Pre
Post
Follo
w-u
p
Pre
Post
Follo
w-u
p
Pre
Post
Follo
w-u
p
Very Somewhat Not at all
Hem/Oncs (n=211)
Follow-up n=10
13%30%
50%32%
52% 50% 55%
18%
0%
20%
40%
60%
80%
100%
Pre
Post
Follo
w-u
p
Pre
Post
Follo
w-u
p
Pre
Post
Follo
w-u
p
Very Somewhat Not at all
Other HCPs (n=261)
Follow-up n=6

Cohen’s d Effect Size = 0.42
An effect size of 0.42 indicates that participating clinicians are now ~28.52% more knowledgeable of the content assessed than prior to
participating in this education.
Pretest
32%Mean
0.30Standard Deviation
472Sample Size
This Effect Size calculation uses pre- and post-test question responses from all paired pre and posttest takers. First-attempt posttest scores were used to calculate the posttest mean and standard deviation.
Cohen (1988): .2 = small, .5 = medium, .8 = largeWolf (1986): .25 = educationally significant, .50 = clinically significant
Cohen’s d effect size accounts for variances in learner populations and is more sensitive to the size of the learner population.As such, ACHL considers effect size to be a more robust measure of educational effectiveness than normalized gains.
46%Mean
0.37Standard Deviation
472Sample Size
First-attempt Posttest

Pretest vs. Posttest Summary
Participants demonstrated improved knowledge and competence across all three domains, however continued
education and reinforcement is necessary to maintain these gains and application to clinical practice.
Topic % Change*
1 Selection of Therapy 35%
2 Application of Testing 27%
3 Treatment of Relapsed AML 73%
Overview of Correct Responses (Aggregate Learners)
*Relative percent change between pre-assessment score and 1st attempt post-assessment score.
45% Normalized
Gain
34%37%
26%
46% 47% 45%
0%
20%
40%
60%
80%
0 1 2 3 4
Pre 1st Attempt Post

30%34% 33%
43%
30%
21%
7%2%
0.00
0.50
1.00
1.50
2.00
2.50
3.00
0%
10%
20%
30%
40%
50%
60%
Pre Post Pre Post Pre Post Pre Post
A B C D
Confidence & LIkelihood ScoresPe
rcen
t of P
re/P
ost R
espo
nses
Other HCPs (n=261)
Confidence Selecting Tx for Newly Dx Likelihood of Selecting CPX-351
48%
38% 35%
49%
12% 12%5%
1%0.00
0.50
1.00
1.50
2.00
2.50
3.00
0%
10%
20%
30%
40%
50%
60%
Pre Post Pre Post Pre Post Pre Post
A B C D
Confidence & Likelihood Scores
Perc
ent o
f Pre
/Pos
t Res
pons
es
Hem/Oncs (n=211)
Confidence Selecting Tx for Newly Dx Likelihood of Selecting CPX-351
Clinical Competence: Selection of Tx for t-AML
The percentage of learners selecting the most appropriate therapy for this hypothetical patient with t-AML increased 40% and 30% postactivity, in
hem/onc and other learner types, respectively. This increased competence correlates with the likelihood to use CPX-351 as reported on slide 11. Further,
both learner types reported increased confidence in selecting therapy for newly diagnosed patients, irrespective of gains in competency. Most learners
accurately recognized that gemtuzumab ozogamicin and enasidenib would not be options without molecular testing. However, approximately one-third of
learners (34-38%) selected the less intensive induction regimen of venetoclax+LDAC postactivity despite the absence of patient and clinical
features that might require that approach. These data suggest that learners may not be familiar with the indications for newer AML therapies.
1. A 62-year-old man was diagnosed with stage II gastric cancer, received surgical treatment followed by chemotherapy with 5-FU and radiation therapy 4 years prior and has remained disease-free since that time. He works as a plumber and has no other comorbidities. He is admitted from the clinic for fatigue, shortness of breath and abnormal blood counts. His peripheral smear showed white blood cell (WBC) count of 12.6x109/L, hemoglobin 8.5 and thrombocyte count of 21x109/L. Bone marrow test showed 86% blast count. He was diagnosed with t-AML, mutational studies were sent and will take 12 days to come back. Which of the following would be the best treatment for this patient?
A. Venetoclax + low dose cytarabine (LDAC)B. CPX-351 C. Gemtuzumab ozogamicin as a single agentD. Enasidenib as a single agent
34%
24%
41%
57%
19%15%
6% 4%
0.00
0.50
1.00
1.50
2.00
2.50
3.00
0%
10%
20%
30%
40%
50%
60%
Pre Post Pre Post Pre Post Pre Post
A B C D
Confidence Score
Perc
ent o
f Pre
/Pos
t Res
pons
es
Hem/Oncs (n=211)
Confidence Selecting Tx for Newly Dx
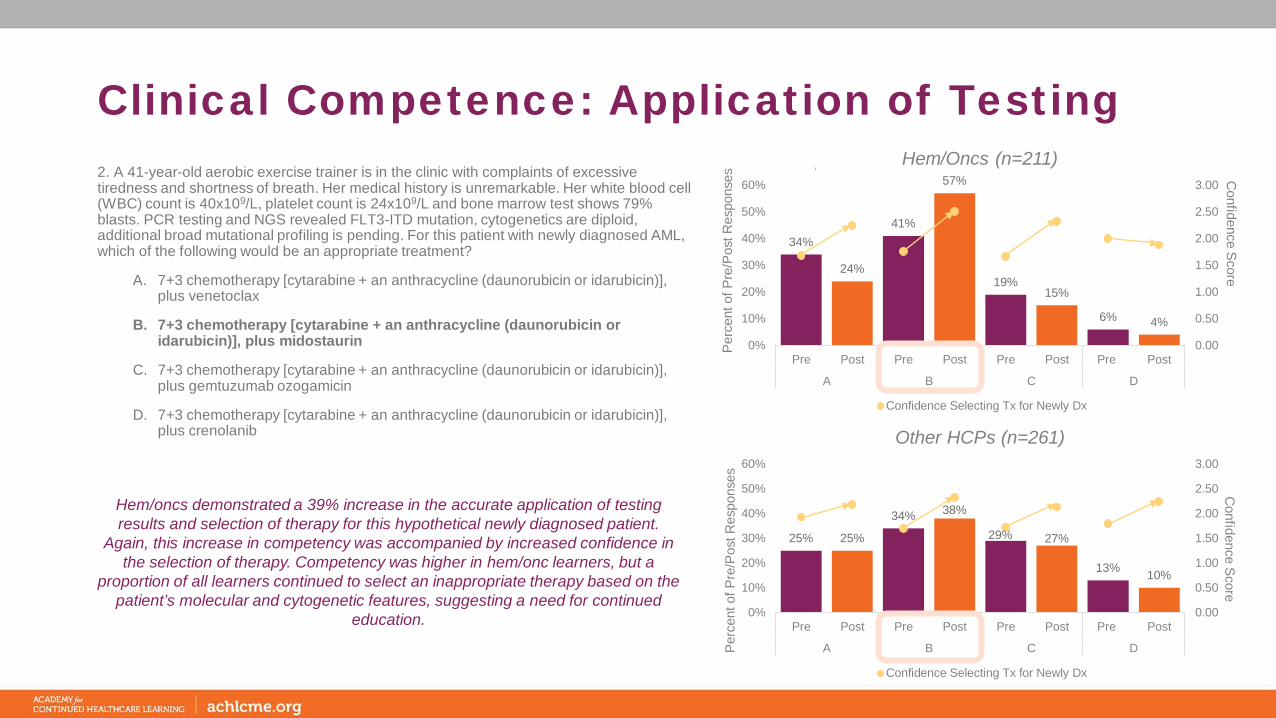
Clinical Competence: Application of Testing
Hem/oncs demonstrated a 39% increase in the accurate application of testing results and selection of therapy for this hypothetical newly diagnosed patient.
Again, this increase in competency was accompanied by increased confidence in the selection of therapy. Competency was higher in hem/onc learners, but a
proportion of all learners continued to select an inappropriate therapy based on the patient’s molecular and cytogenetic features, suggesting a need for continued
education.
2. A 41-year-old aerobic exercise trainer is in the clinic with complaints of excessive tiredness and shortness of breath. Her medical history is unremarkable. Her white blood cell (WBC) count is 40x109/L, platelet count is 24x109/L and bone marrow test shows 79% blasts. PCR testing and NGS revealed FLT3-ITD mutation, cytogenetics are diploid, additional broad mutational profiling is pending. For this patient with newly diagnosed AML, which of the following would be an appropriate treatment?
A. 7+3 chemotherapy [cytarabine + an anthracycline (daunorubicin or idarubicin)], plus venetoclax
B. 7+3 chemotherapy [cytarabine + an anthracycline (daunorubicin or idarubicin)], plus midostaurin
C. 7+3 chemotherapy [cytarabine + an anthracycline (daunorubicin or idarubicin)], plus gemtuzumab ozogamicin
D. 7+3 chemotherapy [cytarabine + an anthracycline (daunorubicin or idarubicin)], plus crenolanib
25% 25%
34% 38%
29% 27%
13% 10%
0.00
0.50
1.00
1.50
2.00
2.50
3.00
0%
10%
20%
30%
40%
50%
60%
Pre Post Pre Post Pre Post Pre Post
A B C D
Confidence Score
Perc
ent o
f Pre
/Pos
t Res
pons
es
Other HCPs (n=261)
Confidence Selecting Tx for Newly Dx

26%20%
31%
16%
33%
52%
10% 11%
0%
10%
20%
30%
40%
50%
60%
Pre Post Pre Post Pre Post Pre Post
A B C D
Perc
ent o
f Pre
/Pos
t Res
pons
es
Hem/Oncs (n=211)
Clinical Competence: Tx for Relapsed AML
There were marked increases in the appropriate interpretation of the molecular and cytogenetic features reported for this patient with relapsed AML. Despite
these gains, approximately half of hem/onc learners and more than half of other learners continued to select inappropriate therapies based on the presence of a FLT3-ITD mutation. Education should continue to focus on the interpretation and application of testing results in the selection of therapy for diverse AML patients.
3. A 76-year-old man with AML received 3+7 induction followed by HiDAC x 2 cycles, but his symptoms did not improve. His current white blood cell (WBC) count was 37x109/L, platelets 42x109/L and bone marrow evaluation showed 78% blasts. PCR and NGS testing revealed FLT3-ITD mutation. Which treatment would be appropriate for this patient?
A. CPX-351B. MidostaurinC. GilteritinibD. Ivosidenib
37%
30%35%
17%20%
40%
8%13%
0%
10%
20%
30%
40%
50%
60%
Pre Post Pre Post Pre Post Pre Post
A B C D
Perc
ent o
f Pre
/Pos
t Res
pons
es
Other HCPs (n=261)
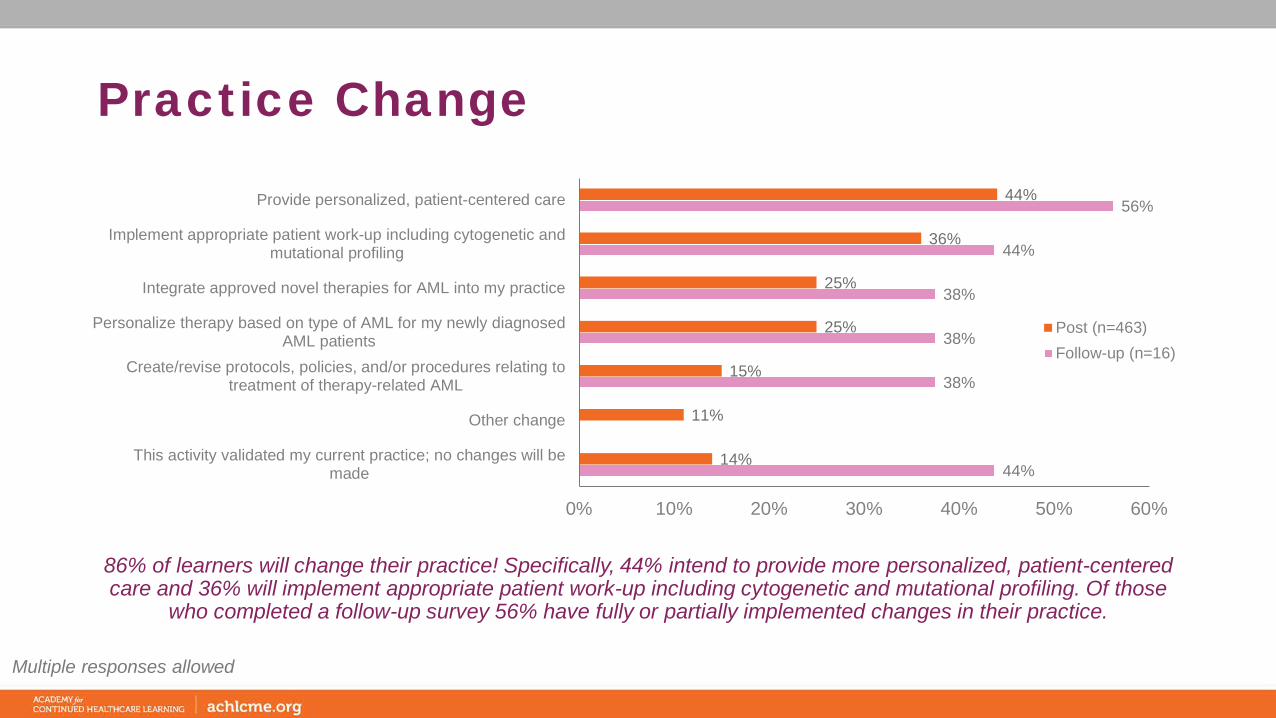
Practice Change
86% of learners will change their practice! Specifically, 44% intend to provide more personalized, patient-centered care and 36% will implement appropriate patient work-up including cytogenetic and mutational profiling. Of those
who completed a follow-up survey 56% have fully or partially implemented changes in their practice.
44%
38%
38%
38%
44%
56%
14%
11%
15%
25%
25%
36%
44%
0% 10% 20% 30% 40% 50% 60%
This activity validated my current practice; no changes will bemade
Other change
Create/revise protocols, policies, and/or procedures relating totreatment of therapy-related AML
Personalize therapy based on type of AML for my newly diagnosedAML patients
Integrate approved novel therapies for AML into my practice
Implement appropriate patient work-up including cytogenetic andmutational profiling
Provide personalized, patient-centered care
Post (n=463)Follow-up (n=16)
Multiple responses allowed

Patient Care Impact
41%
40%
13%
3% 3%
Number of patients with AML seen per week:
0
1-5
6-10
11-20
>20
Changes will impact 4,561 to more than 9,654 patients with AML each week. This assumes data in chart above is representative of all engaged learners (2,478), who indicated they would change their practice as a result of their
participation in this activity (86%).
N=463
18%
20%
19%
17%
Insurance/Reimbursement
Issues Lack of Staff Time
Lack of Resources
Do Not Have anImplementation Strategy
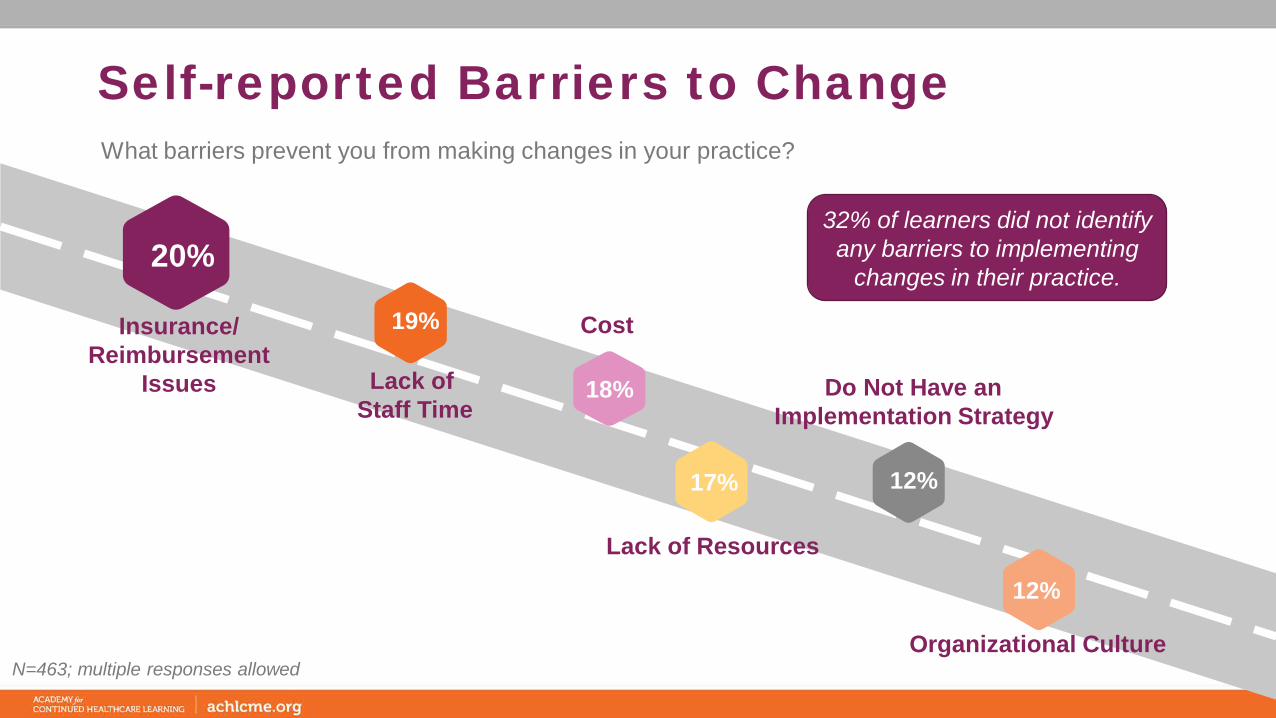
Self-reported Barriers to Change
Cost
12%
12%
Organizational Culture
What barriers prevent you from making changes in your practice?
N=463; multiple responses allowed
32% of learners did not identify any barriers to implementing
changes in their practice.

Topics of Interest
6%
16%
26%
33%
42%
44%
0% 20% 40% 60%
Other
Integrating MRD into clinical practice in AML
Novel therapies in AML
Targeted therapies
Patient education
Management of AML
The broad topic of management of AML was selected with the highest interest for future education (44%). Considerate of the additional topics of interest, the recommendation is for the development of additional education that would continue to address the new and emerging data, the role of testing, implications for
treatment, and treatment selection.
N=463
Other

Activity ImpactSelf-reported changes in knowledge or practice
• Consider new treatments options in patients with AML• Consult with oncologist regarding new/novel treatments• Discuss clinical trials with patients with AML• Discuss importance of implementing immunotherapies as well as
chemotherapies in regimen, if applicable• Address more novel therapies with my team and see which
patients may be appropriate for less intense chemo protocols and/or more targeted therapies.
• Investigate patients’ mutations more closely• Better discuss options with patients and be more informed in
conversations with providers• Better patient care, management of complication• Better understanding of potential side effects and what to monitor for in
patients getting venetoclex• consider venetoclax and gilteritinib.• Discuss treatment options with more knowledge and confidence• Discuss treatment regimen options with other team members• Look more closely at all genetic mutations on bone marrow
analysis• Education on target therapies• Establish better genetic and NGS testing for my site.• Counsel patients more effectively• Further education on the regimens and medications mentioned• I am more aware of new therapies for my AML patients• I will be more informed to speak to patients about their treatment
plans and what options they may have for future treatments.
• Patient education and better management of AML• Pay better attention to the drug classes• Provide adequate work up and discussion with patients• Incorporation of IDH1 and IDH2 in sequencing. Obtaining NGS on
all AML and potentially MDS patients.• Provide better education for my patients• Monitor pts for adverse symptoms r/t these therapies• Provide better education to my patients.• Refer right away. Encourage patients to seek new therapies. Pray for
blastoma treatments• Refer sooner to tertiary center• Counsel patients more knowledgeably• Tailor my anesthetic plan to each individual patient and the treatment
they are receiving. • Endeavor to learn more specifics about the treatments for my pediatric
AML patients.• Treatment in different ages of AML• Try and read pt history thoroughly, Look up drugs more often.• I will be better prepared to teach Pt. about Dx and treatments• Understand what treatments my patient are on. Know what type
of side effects to look for and address with different protocols.• Updated methods for diagnosis of AML• Watching cytogenetics, implementing appropriate care• Improvement of clinical skills and knowledge• Increase knowledge re: cytogenetics in AML.

Implications for the Future• Findings from this activity support continued education focusing on the
selection of therapy• Continued reinforcement of CPX-351 clinical application and recent and
emerging efficacy and safety data• Case-based education with interactivity, decision trees, and learner
feedback to improve competency and application to practice• Expand education to managed care pharmacists, hospital pharmacists,
and payers to inform on the safety and efficacy of recently approved agents
Contact InformationAmanda Kaczerski, MS, CHCPVP, Education DevelopmentAcademy for Continued Healthcare Learning (ACHL)
E: [email protected]: 773-714-0705 ext. 148C: 973-495-4828