acute angle-closure glaucoma following neodymium:yag laser posterior capsulotomy
TRANSCRIPT

Acute angle-closure glaucoma following neodymium: YAG laser posterior capsulotomy
Monica Carrillo, MD; Yvonne M. Buys, MD, FRCSC
Posterior capsular opacification following cataract surgery is a relatively common occurrence that is
usually treated with neodymium (Nd):YAG laser capsulotomy. Although this is generally a safe procedure, it is not without risk. The most frequent complications are mild and include transient elevation of the intraocular pressure (lOP) and iritis. 1- 3 Other reported complications include corneal endothelial changes, iris bleeding with small hyphemas, anterior vitreous face rupture, liquefaction of the vitreous, fractures and pitting of intraocular lenses (IOLs), posterior subluxation of IOLs, sustained lOP elevation, aqueous misdirection, iris neovascularization and neovascular glaucoma, central retinal artery occlusion, ciliochoroidal effusions, cystoid macular edema, macular hole formation, retinal detachment, exacerbation of intraocular infection and even endophthalmitis.l-JO
We describe a pseudophakic patient in whom acute angle-closure glaucoma developed secondary to vitreopupillary block 1 day after Nd:Y AG laser capsulotomy.
CASE REPORT
A 60-year-old white woman was referred to the glaucoma service with acute glaucoma in her right eye. Five years earlier she had undergone uneventful bilateral phacoemulsification with implantation of posterior chamber IOLs. The right IOL was a one-piece poly-
From the University Health Network, Toronto Western Hospital and University of Toronto, Toronto, Ont.
Originally received July 23, 2002 Accepted for publication Dec. 2, 2002
Reprint requests to: Dr. Yvonne M. Buys, Toronto Western Hospital, ECW 7-042, 399 Bathurst St., Toronto ON M5T 2S8; fax (416) 603-5682
This article has been peer-reviewed.
Can J Ophtha/mol 2003;38:230-2
methylmethacrylate lens and was reported to be placed in the capsular bag. She subsequently underwent uneventful left Nd:YAG laser capsulotomy. Two days before presentation right Nd: Y AG laser posterior capsulotomy with a total energy of 50 mJ had been performed. Following the procedure the lOP in the right eye was measured as 16 mm Hg, and the patient was sent home using ketorolac tromethamine, instilled three times daily onto the right eye. The following day she experienced pain in her right eye and was found to have an lOP of 70 mm Hg. Treatment with topical therapy gave minimal improvement.
When she presented to the glaucoma service 2 days after the capsulotomy procedure the uncorrected visual acuity in her right eye was 20/100, improving to 20/50 with pinhole. Slit-lamp examination showed slight corneal edema, iris bombe with vitreous in the anterior chamber and posterior displacement of the posterior chamber IOL. The lOP was 45 mm Hg. Gonioscopy confirmed a closed angle.
A diagnosis of vitreopupillary block was made. The patient underwent right Nd: Y AG peripheral laser iridotomy with six laser applications of 5 mJ each. Immediately following the procedure the lOP was 35 mm Hg and the iris bombe had resolved. Central corneal indentation further lowered the lOP to 18 mm Hg, and 1 hour later the lOP was 9 mm Hg. Repeat gonioscopy showed that the angle had opened. Treatment was started with 1% prednisolone acetate, instilled four times daily for 4 days.
When the patient was last seen, 2 months after the iridotomy procedure, her acuity was 20/60 without correction and 20/40 with pinhole. The lOP in the right eye remained stable at 12 mm Hg with no therapy. The vitreous remained in the anterior chamber, the IOL was still posteriorly displaced, and the iridotomy was patent (Fig. 1).
COMMENTS
The most frequently reported complication fol-
230 Pupillary block following capsulotomy-Carrillo et al
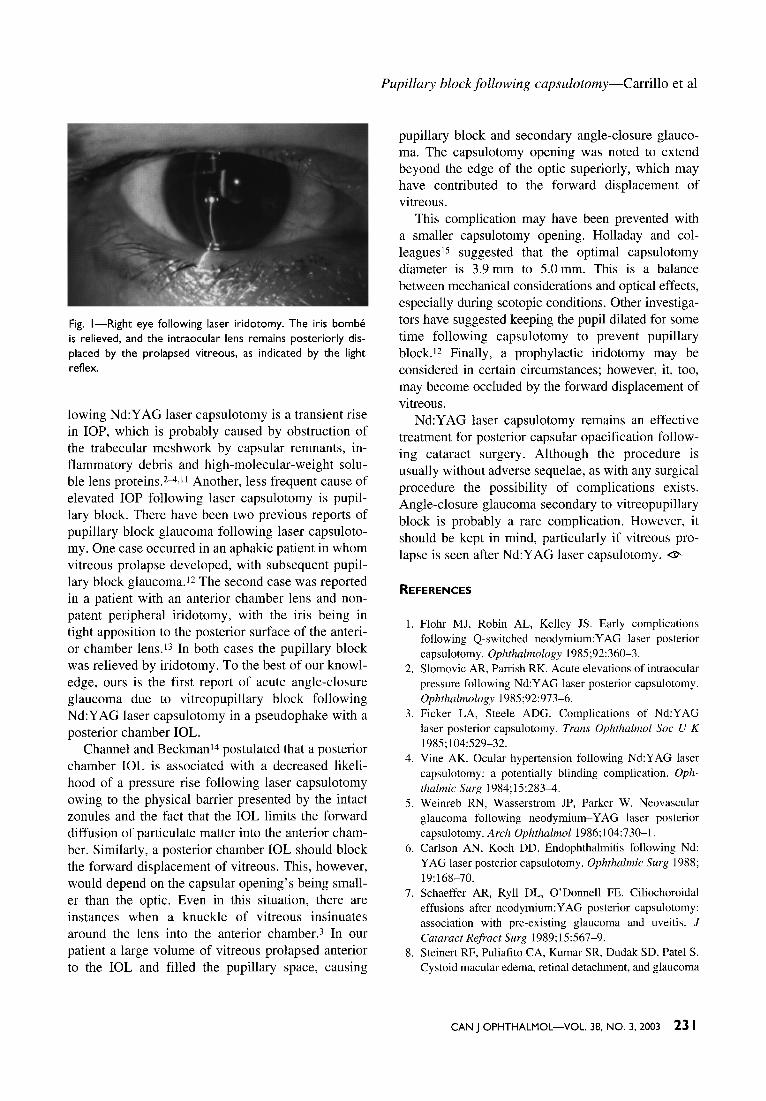
Fig. 1-Right eye following laser iridotomy. The iris bombe is relieved, and the intraocular lens remains posteriorly displaced by the prolapsed vitreous, as indicated by the light reflex.
lowing Nd: Y AG laser capsulotomy is a transient rise in lOP, which is probably caused by obstruction of the trabecular meshwork by capsular remnants, inflammatory debris and high-molecular-weight soluble lens proteins.2-4,11 Another, less frequent cause of elevated lOP following laser capsulotomy is pupillary block. There have been two previous reports of pupillary block glaucoma following laser capsulotomy. One case occurred in an aphakic patient in whom vitreous prolapse developed, with subsequent pupillary block glaucoma. 12 The second case was reported in a patient with an anterior chamber lens and nonpatent peripheral iridotomy, with the iris being in tight apposition to the posterior surface of the anterior chamber lens.I3 In both cases the pupillary block was relieved by iridotomy. To the best of our knowledge, ours is the first report of acute angle-closure glaucoma due to vitreopupillary block following Nd:YAG laser capsulotomy in a pseudophake with a posterior chamber IOL.
Channel and Beckmani4 postulated that a posterior chamber IOL is associated with a decreased likelihood of a pressure rise following laser capsulotomy owing to the physical barrier presented by the intact zonules and the fact that the IOL limits the forward diffusion of particulate matter into the anterior chamber. Similarly, a posterior chamber IOL should block the forward displacement of vitreous. This, however, would depend on the capsular opening's being smaller than the optic. Even in this situation, there are instances when a knuckle of vitreous insinuates around the lens into the anterior chamber. 3 In our patient a large volume of vitreous prolapsed anterior to the IOL and filled the pupillary space, causing
Pupillary block following capsulotomy-Carrillo et al
pupillary block and secondary angle-closure glaucoma. The capsulotomy opening was noted to extend beyond the edge of the optic superiorly, which may have contributed to the forward displacement of vitreous.
This complication may have been prevented with a smaller capsulotomy opening. Holladay and colleagues15 suggested that the optimal capsulotomy diameter is 3.9 mm to 5.0 mm. This is a balance between mechanical considerations and optical effects, especially during scotopic conditions. Other investigators have suggested keeping the pupil dilated for some time following capsulotomy to prevent pupillary block.I2 Finally, a prophylactic iridotomy may be considered in certain circumstances; however, it, too, may become occluded by the forward displacement of vitreous.
Nd:YAG laser capsulotomy remains an effective treatment for posterior capsular opacification following cataract surgery. Although the procedure is usually without adverse sequelae, as with any surgical procedure the possibility of complications exists. Angle-closure glaucoma secondary to vitreopupillary block is probably a rare complication. However, it should be kept in mind, particularly if vitreous prolapse is seen after Nd:YAG laser capsulotomy. ~
REFERENCES
1. Flohr MJ, Robin AL, Kelley JS. Early complications following Q-switched neodymium: Y AG laser posterior capsulotomy. Ophthalmology 1985;92:360-3.
2. Slomovic AR, Parrish RK. Acute elevations of intraocular pressure following Nd:YAG laser posterior capsulotomy. Ophthalmology 1985;92:973-6.
3. Ficker LA, Steele ADG. Complications of Nd:YAG laser posterior capsulotomy. Trans Ophthalmol Soc UK 1985; I 04:529-32.
4. Vine AK. Ocular hypertension following Nd:YAG laser capsulotomy: a potentially blinding complication. Ophthalmic Surg 1984; 15:283-4.
5. Weinreb RN, Wasserstrom JP, Parker W. Neovascular glaucoma following neodymium-YAG laser posterior capsulotomy. Arch Ophthalmoll986;104:730-1.
6. Carlson AN, Koch DD. Endophthalmitis following Nd: YAG laser posterior capsulotomy. Ophthalmic Surg 1988; 19:168-70.
7. Schaeffer AR, Ryll DL, O'Donnell FE. Ciliochoroidal effusions after neodymium:YAG posterior capsulotomy: association with pre-existing glaucoma and uveitis. J Cataract Refract Surg 1989;15:567-9.
8. Steinert RF, Puliafito CA, Kumar SR, Dudak SD, Patel S. Cystoid macular edema, retinal detachment, and glaucoma
CAN J OPHTHALMOL-VOL. 38, NO.3, 2003 231
Pupillary block following capsulotomy-Carrillo et al
after Nd:YAG laser posterior capsulotomy. Am J Ophthalmol!99I;II2:373-80.
9. Mastropasqua L, Ciancaglini M, Carpineto P, Lobefalo L, Gallenga PE. Aqueous misdirection syndrome: a complication of neodymium:YAG posterior capsulotomy. J Cataract Refract Surg 1994;20:563-5.
10. Find! 0, Drexler W, Menapace R, Georgopoulos M, Rainer G, Hitzenberger CK, eta!. Changes in intraocular lens position after neodymium:YAG capsulotomy. J Cataract Refract Surg 1999;25:659-62.
II. Parker WT, Clorfeine GS, Stocklin RD. Marked intraocular pressure rise following Nd:YAG laser capsulotomy. Ophthalmic Surg 1984;15:103-4.
12. Ruderman JM, Mitchell PG, Kraff M. Pupillary block
following Nd: Y AG laser capsulotomy. Ophthalmic Surg 1983;14:418-9.
13. Gstalder RJ. Pupillary block with anterior chamber lens following Nd:YAG laser capsulotomy. Ophthalmic Surg 1986;17:249-50.
14. Channel MM, Beckman M. Intraocular pressure changes after neodymium YAG laser posterior capsulotomy. Arch Ophthalmol 1984; 102: 1024-6.
15. Holladay JT, Bishop JE, Lewis JW. The optimal size of a posterior capsulotomy. JAm Intraocul Implant Soc 1985; 11:18-20.
Key words: glaucoma, laser capsulotomy, complication, cataract
IN THE NEXT ISSUE • DANS LE PROCHAIN NUMERO
Outcomes of primary scleral buckling for
stage 4 retinopathy of prematurity
Presbyopia complicating preexisting strabismus
Trichotillomania
232 CAN J OPHTHALMOL-VOL. 38, NO. 3, 2003