acute and chronic rejection
TRANSCRIPT
Acute and Chronic Acute and Chronic RejectionRejection
Jessie S. Wilt, MDJessie S. Wilt, MDAssistant Professor of Clinical MedicineAssistant Professor of Clinical Medicine
Associate Medical DirectorAssociate Medical Director--Lung TransplantationLung TransplantationColumbia UniversityColumbia University
The RThe R---------------- WordWord
Know the difference between acute and Know the difference between acute and chronic rejectionchronic rejectionUnderstand how each is diagnosedUnderstand how each is diagnosedUnderstand treatment optionsUnderstand treatment options

0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5 6 7 8 9years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
.0 .5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5years
Interval % Survival 1 Month 85% 6 Month 67% 1 Year 61% UNOS 1Year 79 % 3 Year 42% UNOS 3 Year 62%
Interval % Survival 1 Month 98% 6 Month 94% 1 Year 93% UNOS 1Year 79 % 3 Year 78% UNOS 3 Year 62%
UNOS 1YR
UNOS 3YR
UNOS 1YR
UNOS 3YR
CPMC
CPMC
ColumbiaColumbia--Presbyterian Medical CenterPresbyterian Medical Center ColumbiaColumbia--Presbyterian Medical CenterPresbyterian Medical CenterKaplanKaplan--Meier Meier -- Patient Patient SurvivalSurvival EstimatesEstimates KaplanKaplan--Meier Meier -- Patient Patient SurvivalSurvival EstimatesEstimatesLung Transplantation Lung Transplantation –– 7/01/1997 to 6/30/2001 Lung Transplantation 7/01/1997 to 6/30/2001 Lung Transplantation –– 7/01/2001 to 12/08/20057/01/2001 to 12/08/2005(n = 92)(n = 92) (n = 136)(n = 136)
PrePre--Program RestructureProgram Restructure Post Program Restructure Post Program Restructure

ADULT LUNG TRANSPLANT RECIPIENTS: Cause Of ADULT LUNG TRANSPLANT RECIPIENTS: Cause Of
DeathDeath (Deaths: January 1992(Deaths: January 1992-- June 2004)June 2004)
CAUSE OF DEATHCAUSE OF DEATH00--30 Days 30 Days (N = 1146)(N = 1146)
31 Days 31 Days -- 1 1 Year Year
(N = 1,717)(N = 1,717)
>1 Year >1 Year -- 3 3 Years Years
(N = 1,428)(N = 1,428)
>3 Years >3 Years -- 5 5 Years Years
(N = 800)(N = 800)
MALIGNANCY, MALIGNANCY, OTHEROTHER 1 (0.1%)1 (0.1%) 44 (2.6%)44 (2.6%) 78 (5.5%)78 (5.5%) 60 (7.5%)60 (7.5%) 70 (8.4%)70 (8.4%)
CMVCMV 00 65 (3.8%)65 (3.8%) 20 (1.4%)20 (1.4%) 4 (0.5%)4 (0.5%) 3 (0.4%)3 (0.4%)
>5 Years >5 Years (N = 829)(N = 829)
BRONCHIOLITISBRONCHIOLITIS 5 (0.4%)5 (0.4%) 82 (4.8%)82 (4.8%) 378 (26.5%)378 (26.5%) 231 (28.9%)231 (28.9%) 225 (27.1%)225 (27.1%)
ACUTE ACUTE REJECTIONREJECTION 63 (5.5%)63 (5.5%) 35 (2.0%)35 (2.0%) 25 (1.8%)25 (1.8%) 4 (0.5%)4 (0.5%) 5 (0.6%)5 (0.6%)
LYMPHOMALYMPHOMA 1 (0.1%)1 (0.1%) 47 (2.7%)47 (2.7%) 32 (2.2%)32 (2.2%) 11 (1.4%)11 (1.4%) 27 (3.3%)27 (3.3%)
INFECTION, NONINFECTION, NON--CMVCMV
245 245 (21.4%)(21.4%) 639 (37.2%)639 (37.2%) 352 (24.6%)352 (24.6%) 162 (20.3%)162 (20.3%) 150 (18.1%)150 (18.1%)
GRAFT FAILUREGRAFT FAILURE 331 331 (28.9%)(28.9%) 307 (17.9%)307 (17.9%) 244 (17.1%)244 (17.1%) 137 (17.1%)137 (17.1%) 127 (15.3%)127 (15.3%)
CARDIOVASCULACARDIOVASCULARR
121 121 (10.6%)(10.6%) 72 (4.2%)72 (4.2%) 50 (3.5%)50 (3.5%) 36 (4.5%)36 (4.5%) 46 (5.5%)46 (5.5%)
TECHNICALTECHNICAL 96 (8.4%)96 (8.4%) 44 (2.6%)44 (2.6%) 11 (0.8%)11 (0.8%) 2 (0.3%)2 (0.3%) 3 (0.4%)3 (0.4%)
OTHEROTHER 283 283 (24.7%)(24.7%) 382 (22.2%)382 (22.2%) 238 (16.7%)238 (16.7%) 153 (19.1%)153 (19.1%) 173 (20.9%)173 (20.9%)

JHLT 2005, Vol 24; 948JHLT 2005, Vol 24; 948--982982
PERCENTAGE OF ADULT LUNG TRANSPLANT PERCENTAGE OF ADULT LUNG TRANSPLANT RECIPIENTS TREATED FOR REJECTION IN 1ST YEARRECIPIENTS TREATED FOR REJECTION IN 1ST YEARStratified by Type of Induction (Transplants: January 1, 2000 Stratified by Type of Induction (Transplants: January 1, 2000 -- June 30, 2003)June 30, 2003)
0
10
20
30
40
50
60
Overall 18-34 35-49 50-64 65+% tr
eate
d fo
r rej
ectio
n w
ithin
1 y
ear IL2R-antagonist

JHLT 2005, Vol 24; 948JHLT 2005, Vol 24; 948--982982
NUMBER OF REJECTION EPISODES FOR ADULT LUNG NUMBER OF REJECTION EPISODES FOR ADULT LUNG TRANSPLANT RECIPIENTS TREATED FOR REJECTION IN TRANSPLANT RECIPIENTS TREATED FOR REJECTION IN 1ST YEAR1ST YEARStratified by Type of Induction (Transplants: January 1, 2000 Stratified by Type of Induction (Transplants: January 1, 2000 -- June 30, 2003)June 30, 2003)
0
0.5
1
1.5
2
2.5
Overall 18-34 35-49 50-64 65+
Ave
rage
num
ber o
f rej
ectio
n ep
isod
es IL2R-antagonist

Acute Lung RejectionAcute Lung Rejection
A0 A0 No infiltratesNo infiltratesA1A1 Rare perivascular infiltratesRare perivascular infiltratesA2A2 Perivascular infiltrates notable Perivascular infiltrates notable
at at low magnificationlow magnificationA3A3 Infiltrates extend into septaeInfiltrates extend into septaeA4A4 Diffuse infiltrates and alveolar Diffuse infiltrates and alveolar
damagedamage-- With/Without Grade BWith/Without Grade B
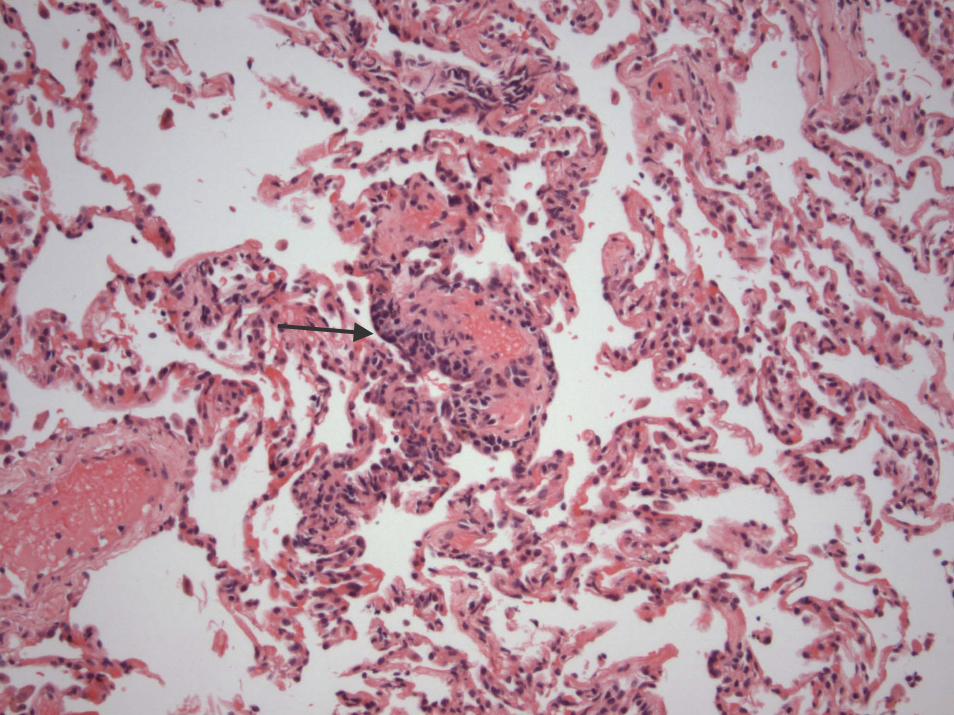
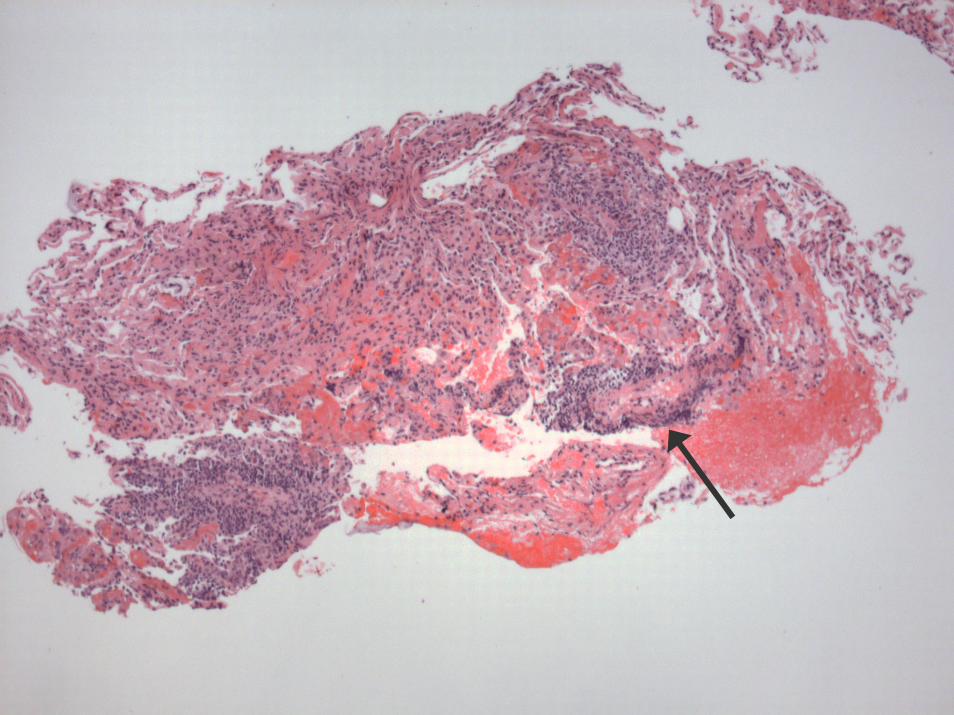
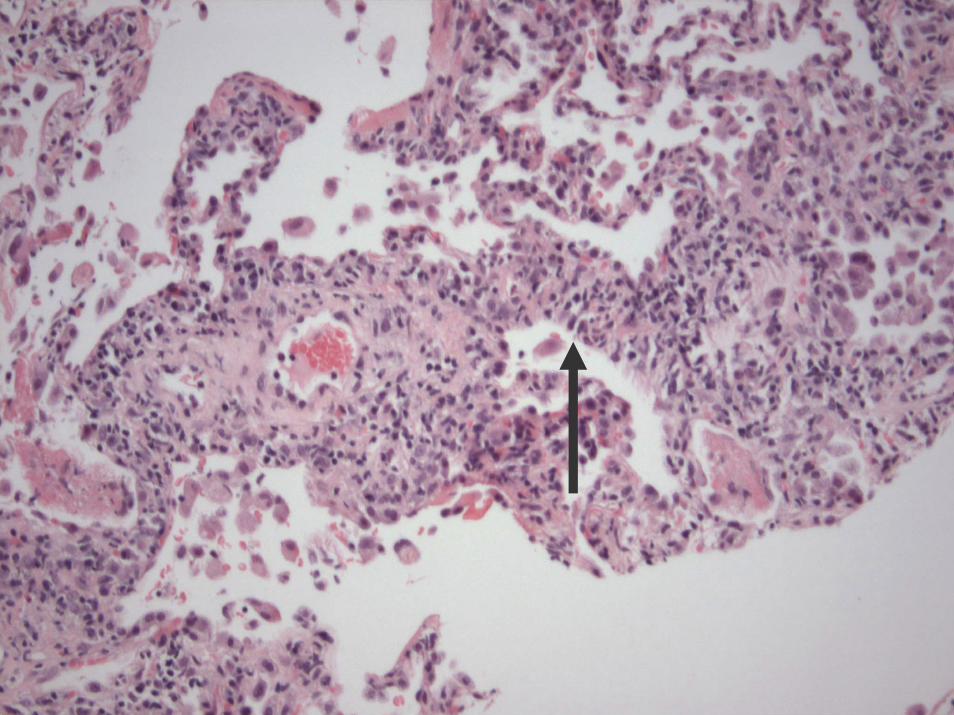

AJT 2005, 5; 2022AJT 2005, 5; 2022--20302030
Minimal Acute Cellular Minimal Acute Cellular RejectionRejection
Clinical FeaturesClinical Features
AsymptomaticAsymptomatic–– Surveillance transbronchial biopsySurveillance transbronchial biopsy
NonspecificNonspecific–– FeverFever–– MalaiseMalaise–– DyspneaDyspnea–– CoughCough–– SputumSputum

Clinical FindingsClinical Findings
Chest radiographChest radiograph–– ClearClear–– Focal infiltrateFocal infiltrate–– Diffuse hazy opacitiesDiffuse hazy opacities
SpirometrySpirometry–– NormalNormal–– Decline from postDecline from post--operative baselineoperative baseline

Differential DiagnosisDifferential Diagnosis
Acute RejectionAcute RejectionInfectionInfection–– BacterialBacterial–– ViralViral
CMVCMV
–– FungalFungal
Graft dysfunctionGraft dysfunction–– VascularVascular

DiagnosisDiagnosis
Fiberoptic bronchoscopyFiberoptic bronchoscopy–– Bronchoalveolar lavageBronchoalveolar lavage–– Transbronchial biopsyTransbronchial biopsy
1010--12 specimens12 specimensAt least 5 pieces, >100 alveoli, bronchiolesAt least 5 pieces, >100 alveoli, bronchioles
Concomitant diagnosesConcomitant diagnoses–– Concurrent infectionConcurrent infection
CFCFCMVCMV

TreatmentTreatment
Oral corticosteroidsOral corticosteroids–– Boost with taperBoost with taper
Intravenous methylprednisoloneIntravenous methylprednisolone–– 1010--15 mg/kg/day (50015 mg/kg/day (500--1000 mg/day)1000 mg/day)
Augmentation of immunosuppressionAugmentation of immunosuppression–– Change calcineurin inhibitorChange calcineurin inhibitor–– Add mycophenolateAdd mycophenolate
Lympholytic therapyLympholytic therapy
LARGOLARGO
Lung Allograft Gene Expression Lung Allograft Gene Expression Observational StudyObservational Study14 centers U.S., Canada, Europe14 centers U.S., Canada, EuropeEnrolled > 600 patientsEnrolled > 600 patients
CARGOCARGOAlloMapAlloMapTMTM
–– NPV 98NPV 98--99%99%

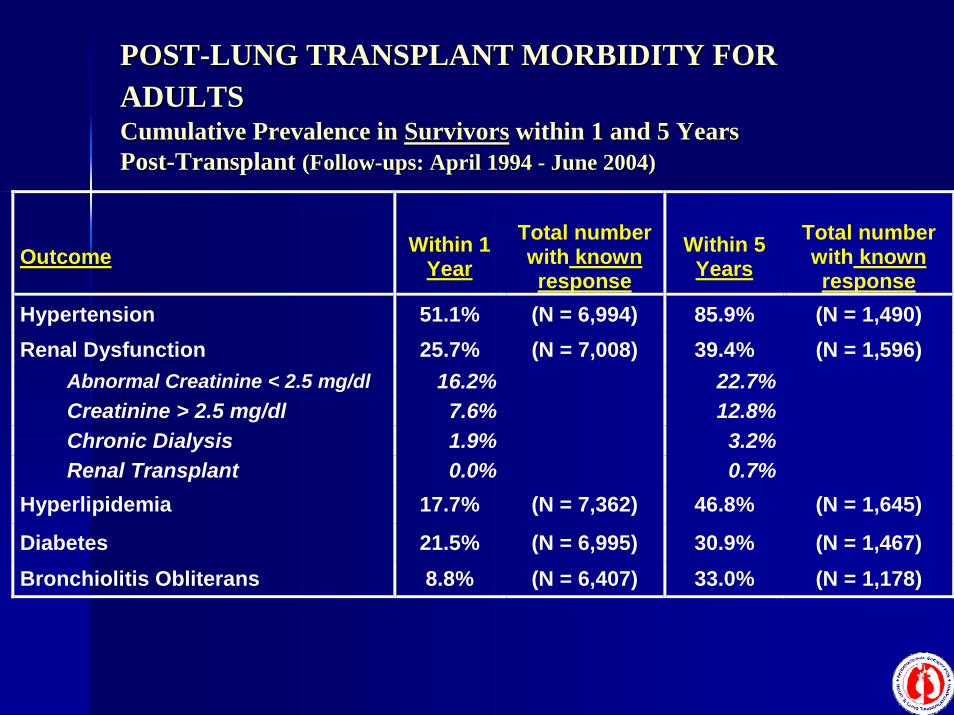
POSTPOST--LUNG TRANSPLANT MORBIDITY FOR LUNG TRANSPLANT MORBIDITY FOR ADULTSADULTSCumulative Prevalence in Cumulative Prevalence in SurvivorsSurvivors within 1 and 5 Years within 1 and 5 Years PostPost--Transplant Transplant (Follow(Follow--ups: April 1994 ups: April 1994 -- June 2004)June 2004)
Outcome Within 1 Year
Total number with known response
Within 5 Years
Total number with known response
Hypertension 51.1% (N = 6,994) 85.9% (N = 1,490) Renal Dysfunction 25.7% (N = 7,008) 39.4% (N = 1,596) Abnormal Creatinine < 2.5 mg/dl 16.2% 22.7% Creatinine > 2.5 mg/dl 7.6% 12.8% Chronic Dialysis 1.9% 3.2% Renal Transplant 0.0% 0.7% Hyperlipidemia 17.7% (N = 7,362) 46.8% (N = 1,645)
Diabetes 21.5% (N = 6,995) 30.9% (N = 1,467) Bronchiolitis Obliterans 8.8% (N = 6,407) 33.0% (N = 1,178)

ObliterativeObliterative BronchiolitisBronchiolitis
Narrowing of the small airwaysNarrowing of the small airwaysLittle inflammatory infiltrateLittle inflammatory infiltrateIrreversibleIrreversibleProgressive airflow obstructionProgressive airflow obstruction
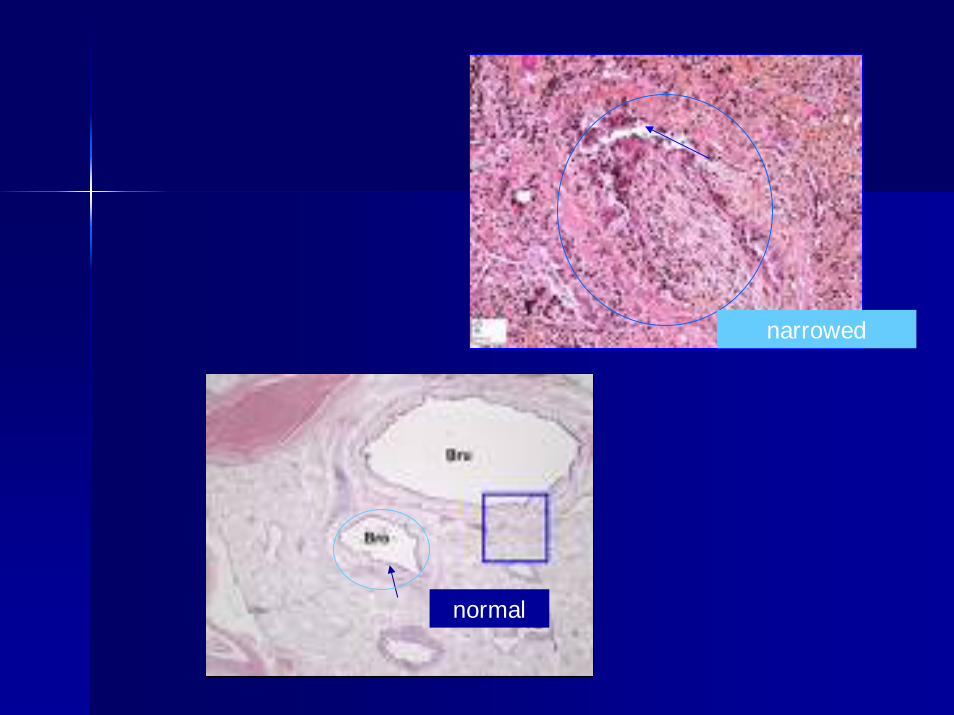
normal
narrowed
Diagnosis of OBDiagnosis of OB
Diagnosis of EXCLUSIONDiagnosis of EXCLUSION–– Exclude infectionsExclude infections–– Exclude airway abnormalitiesExclude airway abnormalities–– Exclude acute rejectionExclude acute rejection
Reduction in Reduction in PFTsPFTs from the from the BESTBEST postpost--transplant baselinetransplant baseline

PFTsPFTs postpost--transplanttransplant
What should your lung function be?What should your lung function be?–– AgeAge–– GenderGender–– HeightHeight–– Donor?Donor?
When are the When are the PFTsPFTs ““the BESTthe BEST””..

BOS BOS –– BronchiolitisBronchiolitisObliteransObliterans SyndromeSyndrome
Once all other diagnoses are excludedOnce all other diagnoses are excludedMany names:Many names:–– BOS, Chronic rejection, Graft failureBOS, Chronic rejection, Graft failure
Clinical DiagnosisClinical Diagnosis–– TransbronchialTransbronchial biopsy cannot detect the biopsy cannot detect the
changeschanges
TreatmentTreatment

Treatment OptionsTreatment Options
Augment immunosuppressive medicationsAugment immunosuppressive medicationsAntiAnti--inflammatory medicationinflammatory medication–– AdvairAdvair–– LipitorLipitor–– AzithromycinAzithromycin
AntiAnti--lymphocyte therapylymphocyte therapy–– PhotopheresisPhotopheresis
ReRe--transplanttransplant

Thank YouThank You