action levels: what are they, how do they work and where do they fit into “free-from”
DESCRIPTION
ACTION LEVELS: WHAT ARE THEY, HOW DO THEY WORK AND WHERE DO THEY FIT INTO “FREE-FROM”. FDIN FreeFrom Grocery and Foodservice Summit, Daventry 18-19 September 2013. René Crevel. Outline. Background: setting the scene Some definitions Establishment of Reference Doses and Action Levels - PowerPoint PPT PresentationTRANSCRIPT

ACTION LEVELS: WHAT ARE THEY, HOW DO THEY WORK AND WHERE DO THEY FIT INTO “FREE-FROM”FDIN FreeFrom Grocery and Foodservice Summit, Daventry 18-19 September 2013René Crevel

OUTLINE
• Background: setting the scene • Some definitions
• Establishment of Reference Doses and Action Levels
• VITAL 1.0 and VITAL 2.0• ILSI Thresholds to Action Levels
• Free-From and Action Levels• Conclusions

WHY WE NEED ACTION LEVELS
• Food allergy is a food safety risk that needs to be managed
• When used as ingredients, legislation requires allergens to be declared
BUT
• Allergens can also be present inadvertently• How do we manage that risk and protect
allergic consumers effectively?

SOME DEFINITIONS
Action level: concentration of allergen in a food below which the risk of a reaction is deemed insignificant.
Reference Dose: amount of allergen which is used to calculate the action level i.e. the dose at which the risk is deemed insignificant.
Threshold (biological): a dose level below which no (allergic) reactions occur

5
RISK
Fundamental principle of toxicology:
“The dose makes the poison” (Paracelsus, 15th Century)
Implication: the key parameter is risk not hazard
Risk» the likelihood that, under particular conditions of exposure,
an intrinsic hazard will represent a threat to human health.
»Risk = f (hazard, exposure)with a consideration of the nature of the effects

REFERENCE DOSES, ACTION LEVELS AND RISK

MANAGING FOOD ALLERGENS AS A FOOD SAFETY ISSUE
8
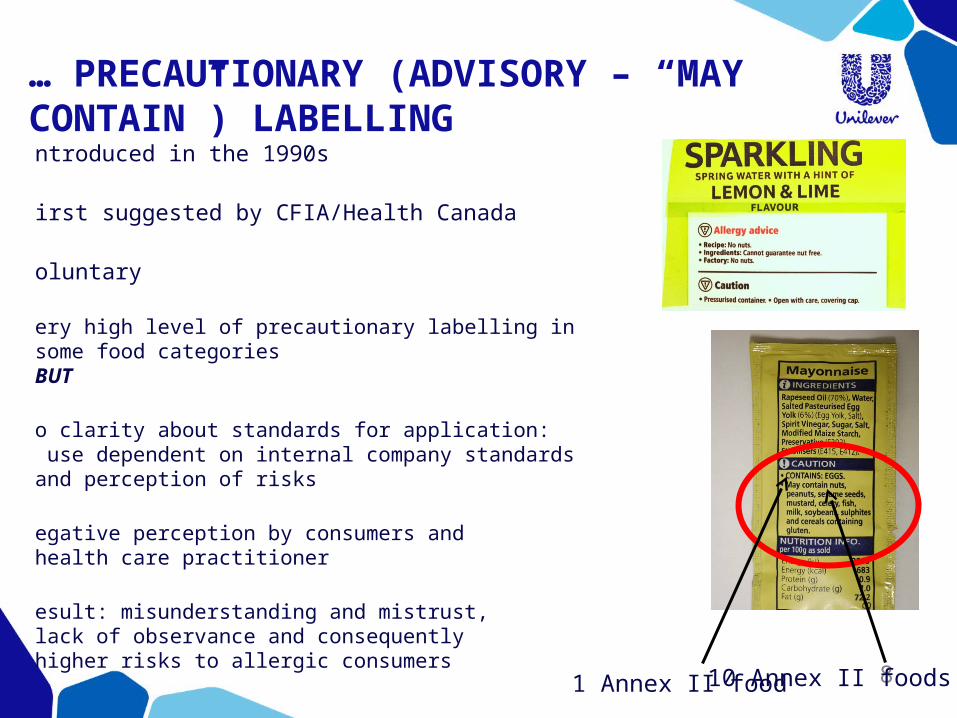
…… PRECAUTIONARY (ADVISORY – “MAY CONTAIN”) LABELLING •Introduced in the 1990s
•First suggested by CFIA/Health Canada
•Voluntary
•Very high level of precautionary labelling in some food categoriesBUT
•No clarity about standards for application: use dependent on internal company standards and perception of risks
•Negative perception by consumers and health care practitioner
•Result: misunderstanding and mistrust, lack of observance and consequently higher risks to allergic consumers 1 Annex II food10 Annex II foods

9
THE DILEMMA: PRECAUTIONARY LABELLING AND RISK
0
Proportion of products affected (%)
Observance ofprecautionary labelling (%)
Risk Profile
0.1 1 10 100
50
50
25
75
100
75
100
Reference dose
..we believe that we should set a gluten threshold level for “gluten free” labeling that best assists most individuals with celiac disease in adhering life-long to a “gluten-free” diet without causing adverse health consequences. … ..moving to a definition of “gluten-free” that adopts a criterion that is much lower than < 20 ppm gluten could have an adverse impact on the health of Americans with celiac disease.(US FDA)

10
SO, PRECAUTIONARY (ADVISORY) LABELLING…
• … on its own is not a definitive answer• needs standards to ensure consistent application• needs to communicate clearly the risk message
to allergic consumers• needs to be used sparingly if it is to retain
credibility and effectiveness
• Current implementation doesn’t do this
11
LEGISLATORS ARE AWARE OF THE ISSUE…
REGULATION 1169/2011. Chapter V. Article 36
“3. The Commission shall adopt implementing acts on the application of the requirements referred to in paragraph 2 of this Article to the following voluntary food information:
(a) information on the possible and unintentional presence in food of substances or products causing allergies or intolerances;”

NEW ALLERGEN INFORMATION REQUIREMENTS (REG 1169/2011)
Precautionary labelling remains voluntary (Article 36)» However mandatory requirements are introduced (e.g. name of allergenic food)
»Specific rules apply:
“2. Food information provided on a voluntary basis shall meet the following requirements:
(a) it shall not mislead the consumer, as referred to in Article 7;
(b) it shall not be ambiguous or confusing for the consumer; and
(c) it shall, where appropriate, be based on the relevant scientific data.”

So we really do need thresholds for food
allergens, but how do we establish them?

FOOD ALLERGENS: DOSE IS CRITICAL
INCREASING DOSE
Pollen-Food syndrome: Lip tingling,Itch
Rash, hivesNausea, vomiting, shortness of breath
Cardio-respiratory symptoms, severe angioedema, anaphylaxis
Probability of severe effect

15
FOOD ALLERGENS: CHALLENGE DOSE AND DISTRIBUTION OF POPULATION RESPONSES
ED10 (mg) ED05 (mg)
DoseLower 95%
CIDose
Lower 95% CI
17.6 9.2 5.8 2.7
LOAEL: 0.5mg
ED10

16
CHARACTERISING THE HAZARD: APPROACHES

17
VOLUNTARY INCIDENTAL TRACE ALLERGEN LABELLING (VITAL) Originally launched in Australia in 2007 as a voluntary approach by industry to limit use of precautionary labelling
Action levels derived from US-FDA Threshold Working Group report (2006) using a safety assessment approach
Generated great interest across the world : NL, USA, etc
Last Updated on:
19-May-08 Milk* Egg* Soy*^ Fish* Peanuts* Tree nuts* Sesame Seed* Crustacea* Gluten#
Action level 1 (ppm) <5 <2 <10 <20 <2 <2 <2 <2 <20
Action level 2 (ppm) 5 - 50 2 - 20 10 - 100 20 - 200 2 - 20 2 - 20 2 - 20 2 - 20 20 - 100
Action level 3 (ppm) >50 >20 >100 >200 >20 >20 >20 >20 >100
Notes:
* mg/kg (ppm) of total protein
# Gluten includes all gluten type proteins as defined in the Food Standards Code
^ The Action Level for soy is highly conservative
Allergen Protein Level
VITAL GRID
© Australian Food and Grocery Council 2007. All rights reserved
Green: no precautionary labelling neededYellow: precautionary labellingRed: label as ingredient

VOLUNTARY INCIDENTAL TRACE ALLERGEN LABELLING (VITAL) V2.0• Comprehensive review of VITAL
• Base the VITAL grid (action levels) on assessment and evaluation by recognised and independent international external experts
• Allergen Bureau invited Prof Steve Taylor (FARRP, University of Nebraska) to form and chair a Scientific Expert Panel to review the VITAL grid
SEAC 18

VITAL SCIENTIFIC EXPERT PANEL:MODUS OPERANDI
SEAC 19

DATA SELECTION CRITERIA
C
riteria for inclusion:» Published studies or unpublished clinical data
» Allergy confirmed by history or other factors
» Double Blind Placebo Controlled Food Challenge (DBPCFC)
» Description of NOAEL and/or LOAEL (or can determine from dosing regime)
» Data on individual patients
» Objective symptoms @ doses or history and subjective symptoms at the last dose
C
riteria for exclusion» High starting doses and significant numbers of first-dose reactors
SEAC 20

ALLERGENS ANALYSED BY VITAL SCIENTIFIC EXPERT PANEL
21
Celeriac/celeryFish
LupineSesame seedShrimp
SoybeanWheatCashewMustard
PeanutMilkEggHazelnut
Assembled and evaluated clinical data on almost all priority allergenic foods on the EU list
No data at all:Molluscs

ALLERGEN THRESHOLD STUDIES
SEAC 22
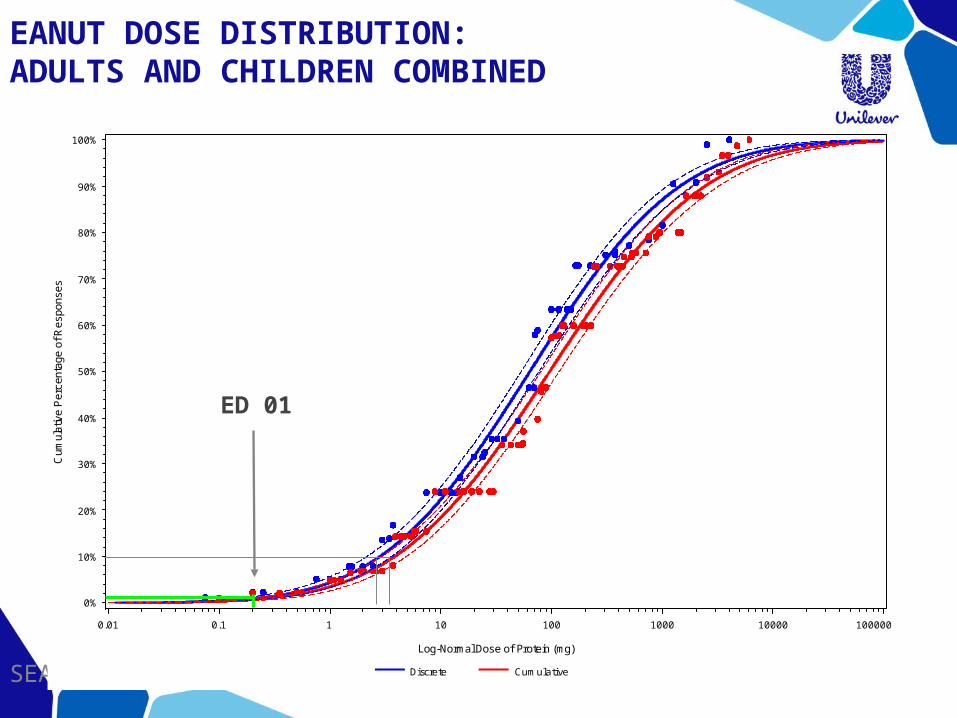
PEANUT DOSE DISTRIBUTION: ADULTS AND CHILDREN COMBINED
SEAC 23
Cum
ulat
ive
Per
cent
age
of R
espo
nses
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Log-Normal Dose of Protein (mg)
0.01 0.1 1 10 100 1000 10000 100000
Discrete Cumulative
ED 01

24
VITAL SCIENTIFIC EXPERT PANEL RECOMMENDATIONS AND PROPOSED ACTION LEVELS.
AllergenNo of data
points
Reference dose (mg Protein)
VITAL 2.0 action level
for 5 g Serving
Size: (ppm)
VITAL 1.0 Level(ppm)
50 g Serving Size: Action Level (ppm)
250 g Serving Size: Action Level (ppm)
Peanut 750 0.20 40 [2] 4.0 0.80Milk 351 0.10 20 [5] 2.0 0.40Egg 206 0.03 6 [2] 0.6 0.12
Hazelnut 202 0.10 20[2 – tree
nuts]2.0 0.40
Soy 80 1.00 200 [10] 20.0 4.00Wheat 40 1.00 200 [20 – gluten] 20.0 4.00Cashew 31 2.00 400 40.0 8.00Mustard 33 0.05 10 1.0 0.20Lupin 24 4.00 800 80.0 16.00Sesame 21 0.20 40 [2] 4.0 0.80
Shrimp 48 10.00 2000 [2 –
crustacea]200.0 40.00
Celery 39 Insufficient dataFish 19 Insufficient data

SEAC 25
WHAT DO THESE REFERENCE VALUES MEAN? THE CLINICAL DATA (1)
“Anaphylaxis developed at a cumulative dose of peanut of 0.02g to 11.7g”(i.e. from 5mg to 2750mg of peanut protein)
VITAL 2.0 Reference dose for peanut is at least 25-fold lower than the lowest dose to provoke an anaphylactic reaction

WHAT DO THESE REFERENCE VALUES MEAN? THE CLINICAL DATA (2)
SEAC 26
8 – 37 mg of peanut protein(32 – 148 mg of whole peanut)

WHAT DO THESE REFERENCE DOSES MEAN? THE CLINICAL DATA (3)
27
• 24 patients• Dose escalation: 0.05mg to 2286mg peanut protein • Only small percentage of mild reactions up to 0.4mg peanut protein• 6662 doses delivered, 1023 symptoms recorded, 3% severe, • no severe symptoms below 25mg peanut protein
• 869 children challenged• Starting doses 3 - 5mg protein for cows’ milk, wheat, soy, hen’s egg• 8-10% first dose reactors for milk and hen’s egg• 0.5 - 1% at risk of severe reactions• starting doses were 33 and 166-fold higher than VITAL Reference Doses for milk and egg respectively

CONCLUSIONS OF THE VSEP
28

MOVING FORWARD
•The ILSI-Europe Food Allergy Task Force Expert Group “Thresholds to Action Levels”
•The ILSI “Thresholds to Action Levels” workshop Reading 13-14 September 2012
SEAC 29

CONCLUSIONS ENDORSED BY THE WORKSHOP PARTICIPANTS
• A transparent set of reference doses (as a basis for action levels) would be a desirable outcome, in principle.
• Data from food challenge studies provide the appropriate foundation from which these action levels can be derived
• Sufficient data exist to move forward and better estimate the risk to the allergic population for the allergens specified in the report
• The proposed reference doses, based on the work of the VITAL Scientific Panel, constitute a reasonable first pass to minimise risk to the allergic consumer while maintaining food choices 30

ACTION LEVELS AND “FREE-FROM”
• Action Levels and Reference Doses are critical to the concept of “free-from”, but are they the threshold for “free-from”
• NO, because they have been developed to apply to everyday foods, manufactured using everyday sanitation processes, etc
• WHY? • The Reference Doses are NOT No Effect Levels• “Free-from” are specially prepared for and used by people
who are at the very sensitive end of the spectrum and enhanced procedures need to be used to ensure that the risk remains low
• However they can be used as a benchmark
SEAC 31

ACTION LEVELS AND “FREE-FROM”
November 201132
“FREE FROM” “MAY CONTAIN”“NOT SUITABLE FOR”
“SUITABLE FOR”
No reactions In the vast majority of allergic Individuals
No severe reactions in the vast majority of allergic individuals
No mild reactions in the vast majority of highly sensitive allergic Individuals
PUBLIC HEALTH OUTCOME
ALLERGEN STATUS
Allergen management controls managed, with
unavoidable traces present despite efforts
Allergen analytically absent to a high degree of
confidence, GMPs to ensure absence of specific
allergen
AMOUNT OF ALLERGENIC PROTEIN
Allergen management cross-contact control
well-managed to a low level
MANAGEMENTPARAMETER
Lower limit of analytical detection
Action Level
lower higher
Manufacturing facility “IN CONTROL”

CONCLUDING REMARKS
• The debate about Action Levels has focussed on the numbers• Allergic consumers do not understand them as proposed • They worry that they would make their life more dangerous.
• In fact, Action levels agreed and accepted across industry should improve safety through
• a consistent standard and approach• a common understanding of risk • Clear communication of that risk to allergic consumers, as well as to those who
advise them (allergists, dieticians, etc).
• This is a much better situation than the one we currently have, where the consumer cannot know how the risk posed by allergens has been assessed and mitigated
• Implementation of harmonised Action levels, based on agreed and accepted Reference Doses, will enable food-allergic people to make safe choices with increased confidence.
33

34
THANK YOU FOR YOUR
ATTENTION