acquiredlipidosis of marrow macrophages
TRANSCRIPT

Journal of Clinical Pathology, 1979, 32, 420-428
Acquired lipidosis of marrow macrophagesBirefringent blue crystals and Gaucher-like cells, sea-blue histiocytes, andgrey-green crystals
F. G. J. HAYHOE, R. J. FLEMANS, AND D. C. COWLING'
From the Department ofHaematological Medicine, University ofCambridge, UK
SUMMARY Three varieties of compound lipid inclusions occurring as a secondary phenomenon inmarrow macrophages are detectable and distinguishable by Romanowsky staining, ultravioletfluorescence, and polarised light. Birefringent blue crystals and Gaucher-like cells form one variety,sta-blue granules another, and grey-green crystals a third. All occur chiefly in myeloid leukaemias,either acute or chronic.
Normally, macrophages in the bone marrow maycontain cellular remnants, lipid globules, granulesof iron, and other ingested material, resulting fromphagocytic activity. The appearance of these cellsis well recognised and amply illustrated in haemato-logical atlases.
Inherited disorders of lipid metabolism, usuallyassociated with specific enzyme deficiencies, mayinduce storage of lipids such as sphingolipids inhistiocytes in the reticuloendothelial system. InGaucher's disease, for example, a deficiency offl-glucocerebrosidase leads to accumulation ofglucosyl ceramide, whereas in Niemann Pick diseasedeficiency of sphingomyelinase causes sphingo-myelin (phosphoryl choline ceramide) to accumulate.Other storage diseases with typical clinical syndromesand inheritance are recognised. In most of theseconditions the marrow histiocytes containing thestorage material concerned present a characteristiccytological and cytochemical appearance at bothlight microscope and ultrastructural levels (Stanburyet al., 1972). Among these inherited disorders isprimary sea-blue histiocytosis, a condition in whichthe pathogenesis and the chemistry of the storedmaterial are less clearly established, althoughphospholipid, glycosphingolipids, and ceroid havebeen identified (Sawitsky et al., 1972; Silverstein andEllefson, 1972).
Sea-blue histiocytes occur in the marrow notonly in the primary genetic syndrome but also inother disorders of diverse form and aetiology.
'Present address: Royal Melbourne Hospital, Victoria,AustraliaReceived for publication 31 October 1978
Secondary sea-blue histiocytosis is an example ofwhat has been called acquired lipidosis, in whichinclusions of differing morphology, but probablyall of lipid character, may accumulate in histiocytesin the bone marrow in diseases such as chronicmyeloid leukaemia (CML) (Dosik et al., 1972) anddyserythropoiesis (Lewis and Verwilghen, 1977).Whereas the cytological appearance of sea-bluehistiocytes is now well recognised, the various othercrystalline or discrete inclusion bodies found as asecondary phenomenon in certain blood dyscrasiasare less well known. They include material havinga fibrillary disposition in the cytoplasm so as to givea resemblance to Gaucher cells, first described as asecondary phenomenon in CML by Albrecht (1966),and various kinds of crystals, such as the 'light green'crystals described by Stavem et al. (1977) in bothacute and chronic myeloid leukaemias.During the past few years we have looked specifi-
cally for acquired lipidosis of marrow histiocyteswhen studying bone marrow aspirates and have notedthat some inclusions are strikingly birefringent inpolarised light whereas others are not. The object ofthis paper is to describe and illustrate the distin-guishing features of the three main varieties ofsecondary lipidosis which we have observed duringa survey of some 1000 bone marrow samples, toindicate the conditions in which they may be found,and to make some assessment of their frequency andsignificance.
Material and nmehods
The marrow aspirates reviewed came mostly frompatients under our care over the last five years but
420
on January 28, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.5.420 on 1 M
ay 1979. Dow
nloaded from

Acquired lipidosis of marrow macrophages
included about 100 specimens referred to us fromelsewhere. During this period approximately 1000aspirates were studied, including 367 original diag-nostic aspirates from patients with haematologicalmalignancies, aplastic anaemia, or idiopathic throm-bocytopenic purpura, conditions in which acquiredlipidosis of histiocytes has previously been recorded.Aspirates were all smeared directly without use ofanticoagulants. They were stained by Romanowskymethods-either Leishman or May-Grunwald-Giemsa stain (Hopkins and Williams, Revectorbrand).The inclusions in histiocytes were classed according
to their morphology as seen in Romanowsky stains,but all histiocytes showing visible inclusions andmany without were also observed under polarisedlight for the existence of birefringence. Theseobservations were made with a Zeiss photomicro-scope fitted with polarising filters. Examples of eachtype of inclusion recognised by these methods werealso observed under ultraviolet (UV) light using aZeiss fluorescence microscope and transilluminationfor autofluorescence.
Further examples were stained by cytochemicalmethods standard in this laboratory-peroxidase,Sudan black, periodic acid Schiff (PAS), acid andalkaline phosphatase, and a range of non-specificesterases (Hayhoe and Flemans, 1969; Hayhoe andCawley, 1972; Higgy et al., 1977).
Electron microscopy (EM) was carried out onglutaraldehyde-fixed material by standard methods(Cawley and Hayhoe, 1973).
Results
The inclusion material observed in histiocytes wasof three types separable by Romanowsky stains,polarised light, UV autofluorescence, and EM(Table 1).
BIREFRINGENT BLUE CRYSTALS AND
GAUCHER-LIKE CELLS
The typical appearance of these inclusions inRomanowsky preparations is illustrated in Figures
1-5. The crystals stain a blue-grey colour in Roman-owsky preparations and in any individual cell maybe few in number or may occupy the bulk of thecytoplasm. They are more readily seen as the cellbreaks up. They are generally lanceolate and 6-12,uin length, often arranged in bundles (Fig. 1). Whenthe cell is disrupted the crystals lie free on the slide(Fig. 2), and when they are numerous, isolatedcrystals may be seen some distance from a disruptedcell. The crystals are birefringent, and Fig. 3 illus-trates the same cell as in Fig. 2 using polarised lightand showing the birefringence. They are frequentlynot obvious in a Romanowsky-stained preparation,and this is illustrated in the large, binucleated,phagocytic histiocyte in Fig. 4, which also shows thefaint striations of the cytoplasm which may givea pseudo-Gaucher cell appearance. This same cellwith polarised light contained many birefringent
j
./
Fig. 1 Blue crystals (type 1) in a histiocyte showingslightfragmentation from apatient with a typical chronicmyeloid leukaemia.
Table 1 Cytologicalfindings distinguishing inclusions in histiocytes
Type ofinclusion and size Cytochemistry Birefringence Autofluorescence EM
Blue-grey crystal Peroxidase, PAS, Sudan black, Consistently present Absent Microtubular structure inlanceolate 612,4 long and phosphatases usually negative. crystal-shaped structure
Esterases may be positiveSea-blue bodies Peroxidase, PAS, phosphatases, Absent Present Usually structureless osmiophilic1-3 jA diameter esterases variable. Sudan black inclusions. Occasionally finger-
may be positive print patternGrey-green crystal cigar- Peroxidase, PAS, Sudan black, Absent Absent Crystal-shaped withshaped 8-20 long phosphatases, and esterases homogeneous ultrastructure
usually negative
421
on January 28, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.5.420 on 1 M
ay 1979. Dow
nloaded from

422
.
akin. "*
ni-8
._eE_ ..*w@ ..
; :J !! .<S,,: :: !.. aKtEf .: S* stiASE:' :iz' ' i. : :::Bi''l. '0 'S.-4p. -. ; m . . i
f}' w9?=X3e7A'g.s£p:
-_
_!
l*:' _e;. _F5':=A':F': : L.:.S', :. ... jj.,.an,.
.. :::er. .::.
*.;_ .
stF
F. G. J. Hayhoe, R. J. Flemans, and D. C. Cowling
coarser and less densely packed than those of a trueGaucher's disease histiocyte, as illustrated inFigure 6.
.. :::...: ....:
:: ::: :.::..
.>::,, 6.,tR,j.':44sstu.oSjw. .La#f°sX.,}: .:_ : . . f_ . :.:. ::t ! ::
.. :.;: ::.''. :':.'.;-: !'.... j, .g ........
st { !°I
.. : ::i E: t:
.i.?: ,: , ;.::. ,,. ..:.YL'a*r.: x:z .:: 19] _N1 }:|11: ,= rN - . ...
:>.e'': 'J a _ !..E5 _ 5*:! ... :E:. .. ::.:X
::._::... * := q#BUgm'. . . ! ..i=.i.*.. _: ;1~~
Fig. 2 Blue crystals (type 1) showingfragmentation ofa histiocytefrom the samepatient as in Fig. 1.
Fig. 4 A pseudo-Gaucher cell containing phagocytosedcell debrisfrom a patient with aplastic anaemia.
Fig. 3 The samefield as in Fig. 2 under polarised lightshowing birefringent crystals.
crystals (Fig. 5). The appearance differs from that ofa true Gaucher cell in that the cell is generallysmaller, does not, with a Romanowsky stain, havea typical crumpled tissue-paper type of cytoplasmicstriation, and under polarised light the crystals are
Fig. 5 The samefield as in Fig. 4 showing many rathercoarse birefringent crystals.
... ......::-%:j'..n..
on January 28, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.5.420 on 1 M
ay 1979. Dow
nloaded from
Acquired lipidosis of marrow macrophages
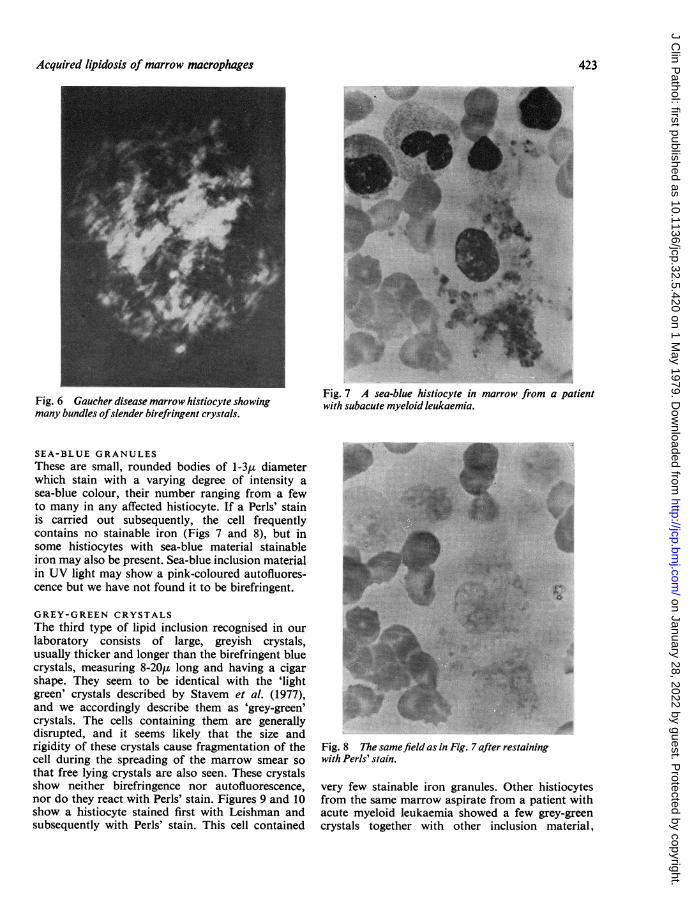
Fig. 6 Gaucher disease marrow histiocyte showingmany bundles ofslender birefringent crystals.
SEA-BLUE GRANULESThese are small, rounded bodies of 1-3,u diameterwhich stain with a varying degree of intensity asea-blue colour, their number ranging from a fewto many in any affected histiocyte. If a Perls' stainis carried out subsequently, the cell frequentlycontains no stainable iron (Figs 7 and 8), but insome histiocytes with sea-blue material stainableiron may also be present. Sea-blue inclusion materialin UV light may show a pink-coloured autofluores-cence but we have not found it to be birefringent.
GREY-GREEN CRYSTALSThe third type of lipid inclusion recognised in ourlaboratory consists of large, greyish crystals,usually thicker and longer than the birefringent bluecrystals, measuring 8-20g long and having a cigarshape. They seem to be identical with the 'lightgreen' crystals described by Stavem et al. (1977),and we accordingly describe them as 'grey-green'crystals. The cells containing them are generallydisrupted, and it seems likely that the size andrigidity of these crystals cause fragmentation of thecell during the spreading of the marrow smear sothat free lying crystals are also seen. These crystalsshow neither birefringence nor autofluorescence,nor do they react with Perls' stain. Figures 9 and 10show a histiocyte stained first with Leishman andsubsequently with Perls' stain. This cell contained
Fig. 7 A sea-blue histiocyte in marrow from a patientwith subacute myeloid leukaemia.
Fig. 8 The samefield as in Fig. 7 after restainingwith Perls' stain.
very few stainable iron granules. Other histiocytesfrom the same marrow aspirate from a patient withacute myeloid leukaemia showed a few grey-greencrystals together with other inclusion material,
423
MA
on January 28, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.5.420 on 1 M
ay 1979. Dow
nloaded from

F. G. J. Hayhoe, R. J. Flemans, and D. C. Cowling
*.4l..
'A& I
Fig. 9 Grey crystals in a macrophage.
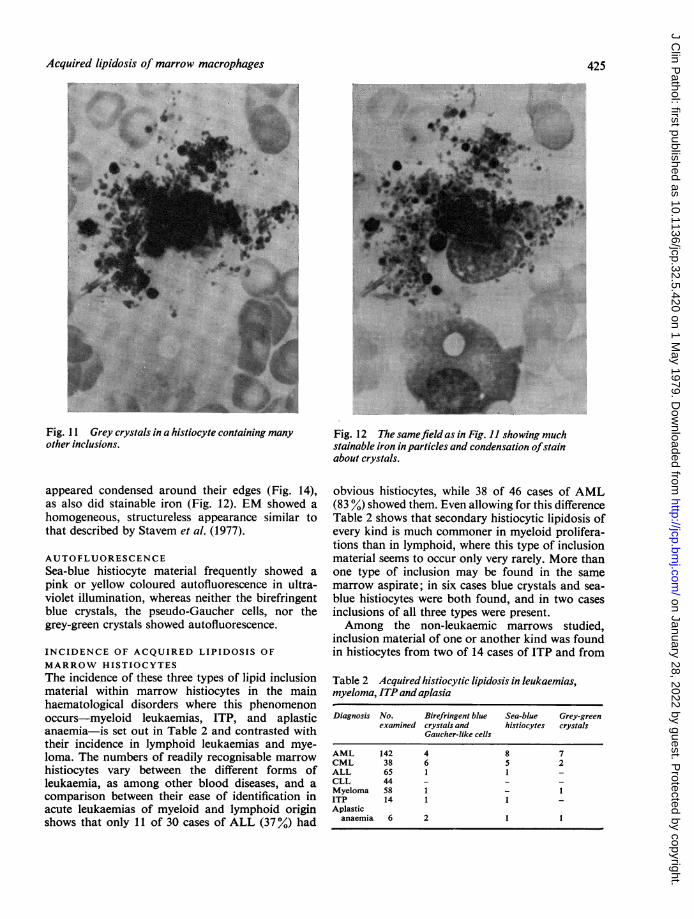
which, when stained by Perls' reaction, was shown tobe stainable iron (Figs 11 and 12).
CYTOCHEMICAL AND ELECTRON MICROSCOPICFINDINGSNormal marrow histiocytes show variable cyto-chemical findings; they may show diffuse PASstaining and may contain some granules of PAS-positive material. They may contain granules stainingwith Sudan black. They are usually strongly positivefor acid and alkaline phosphatase. Of the esterasestains, the oc-naphthyl butyrate esterase methodusually gives a strong reaction, whereas the ox-naphthyl AS-D-chloroacetate esterase is usuallynegative or only weakly positive. When interpretingcytochemical reactions in and around the inclusionmaterial of histiocytic lipidosis the backgroundreactivity of the histiocyte cytoplasm must be takeninto account. Apart from occasional staining of sea-blue material by Sudan black B all other cytochemi-cal reactions seemed probably negative in theinclusion material, although, when the reaction waspositive in the histiocyte cytoplasm, some condensa-tion or localisation of reaction product at the surfaceof the inclusions was commonly noted.Thus the blue crystals and Gaucher-like inclusion
Fig. 10 The samefield as in Fig. 9 stained with Perls'stain.
material did not give any positive cytochemicalreactions although the /i-naphthyl butyrate reactionwas positive elsewhere in the histiocyte cytoplasmwith some apparent concentration of reactionproduct at the surface of the crystals. Under EMthese crystals contain numerous microtubules withan arrangement similar to that seen in Gaucher'sdisease (Fig. 13).
Sea-blue histiocytes gave variable Sudan blackstaining of inclusions, some staining strongly, othersnot staining. Other cytochemical methods gavegenerally negative results although PAS, acid andalkaline phosphatase, and cx-naphthyl butyratereactions, which give variable to strong cytoplasmicstaining in the histiocytes, also gave a suggestionof occasional concentration of reaction product atthe granule surface.EM showed the presence of rounded osmiophilic
inclusions, sometimes in groups in vacuoles. In twomarrows studied we were unable to find the 'finger-print' pattern inclusions described by Parker et al.(1976) resembling the appearance seen in Niemann-Pick disease.
Grey-green inclusions were apparently themselvesunstained by the cytochemical methods althoughthe strongly positive ax-naphthyl butyrate stain
424
on January 28, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.5.420 on 1 M
ay 1979. Dow
nloaded from
Acquired lipidosis of marrow macrophages
Fig. 1 1 Grey crystals in a histiocyte containing many Fig. 12 The samefield as in Fig. 1I showing muchother inclusions. stainable iron in particles and condensation ofstain
about crystals.
appeared condensed around their edges (Fig. 14),as also did stainable iron (Fig. 12). EM showed ahomogeneous, structureless appearance similar tothat described by Stavem et al. (1977).
AUTOFLUORESCENCESea-blue histiocyte material frequently showed apink or yellow coloured autofluorescence in ultra-violet illumination, whereas neither the birefringentblue crystals, the pseudo-Gaucher cells, nor thegrey-green crystals showed autofluorescence.
INCIDENCE OF ACQUIRED LIPIDOSIS OF
MARROW HISTIOCYTESThe incidence of these three types of lipid inclusionmaterial within marrow histiocytes in the mainhaematological disorders where this phenomenonoccurs-myeloid leukaemias, ITP, and aplasticanaemia-is set out in Table 2 and contrasted withtheir incidence in lymphoid leukaemias and mye-loma. The numbers of readily recognisable marrowhistiocytes vary between the different forms ofleukaemia, as among other blood diseases, and acomparison between their ease of identification inacute leukaemias of myeloid and lymphoid originshows that only 11 of 30 cases of ALL (37%) had
obvious histiocytes, while 38 of 46 cases of AML(83 %) showed them. Even allowing for this differenceTable 2 shows that secondary histiocytic lipidosis ofevery kind is much commoner in myeloid prolifera-tions than in lymphoid, where this type of inclusionmaterial seems to occur only very rarely. More thanone type of inclusion may be found in the samemarrow aspirate; in six cases blue crystals and sea-blue histiocytes were both found, and in two casesinclusions of all three types were present.Among the non-leukaemic marrows studied,
inclusion material of one or another kind was foundin histiocytes from two of 14 cases of ITP and from
Table 2 Acquired histiocytic lipidosis in leukaemias,myeloma, ITP and aplasia
Diagnosis No. Birefringent blue Sea-blue Grey-greenexamined crystals and histiocytes crystals
Gaucher-like cells
AML 142 4 8 7CML 38 6 5 2ALL 65 1 1 -CLL 44 - -
Myeloma 58 1 - 1ITP 14 1 1 -Aplasticanaemia 6 2 1 1
425
on January 28, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.5.420 on 1 M
ay 1979. Dow
nloaded from

F. G. J. Hayhoe, R. J. Flemans, and D. C. Cowling
Fig. 13 EMphotograph ofbundles ofmicrotubules in a blue crystal which wouldbe birefringent.
four of six cases of aplastic anaemia, and in iso-lated cases of hereditary dyserythropoietic anaemia,,8-thalassaemia, hypersplenism, ,B-lipoproteinaemia,and angioimmunoblastic lymphadenopathy. Histio-cytes with these types of inclusion were not foundin any of several hundred marrow samples, mostlywithin normal limits cytologically, from patientswith Hodgkin's disease or other lymphomas, or inmarrows from patients with anaemias secondary todeficiency of haematinic factors or to haemolysis.
Discussion
Earlier observations on acquired lipidosis of marrowhistiocytes have been reviewed by Dosik et al. (1972),who noted particularly the occurrence of Gaucher-like cells and sea-blue histiocytes in chronic myeloidleukaemia. A range of cytological appearancestransitional between normal marrow macrophagesand classical Gaucher cells had been described byKattlove et al. (1969). These cells, and also sea-bluehistiocytes, have been reported to occur occasionallyin small numbers in the marrow from patients withpolycythaemia, rheumatoid arthritis, thrombo-
cytopenic purpura, and hyperlipoproteinaemia(Dosik et al., 1972; Sawitsky et al., 1972). They havealso been observed in thalassaemia and in congenitaldyserythropoietic anaemia. A further type of in-clusion was described by Stavem et al. (1977) aslight green crystals; this was found in six of 11randomly selected marrow aspirates from patientswith acute or chronic myeloid leukaemia.The present study leads us to believe that the
Gaucher-like cells of other writers are one cyto-logical manifestation of the accumulation of bire-fringent crystalline material in marrow macrophages.These inclusions may be invisible with light micro-scopy of Romanowsky-stained slides and revealedonly by polarised light. The composition of theinclusion material is probably the same as in trueGaucher's disease, namely, glucosyl ceramide;certainly the ultrastructure shows a similar patternof parallel bundles of microtubules which probablyaccount for the birefringence noted.
This type of acquired birefringent inclusion inmyeloid leukaemias may arise f; o n increasedbreakdown of granulocytes with overproduction ofglucosyl ceramide, which the marrow macrophages,
426
on January 28, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.5.420 on 1 M
ay 1979. Dow
nloaded from

Acquired lipidosis of marrow macrophages
Fig. 14 Marrow histiocyte containing grey crystals withstrongly positive cytoplasmic stainingfor a-naphthylbutyrate esterase and stain outlining unstained centreofcrystals.
despite increased glucocerebrosidase activity, areunable to metabolise. A similar mechanism has beenpostulated in dyserythropoietic states (Van Dorpeetal., 1973).
Blue pigment macrophages or sea-blue histiocyteswere first described in the spleen and later in bonemarrow by Moeschlin (1951). The recognition of arather benign genetic syndrome characterised byaccumulation of sea-blue histiocytes in spleen, liver,and bone marrow emerged during the next 20 years,and the condition became known as the sea-bluehistiocyte syndrome. There is agreement that thesea-blue material contains phospholipid and glyco-sphingolipid, but patients may have a raised plasmatriglyceride level, and Jacobsen et al. (1972) recordeda deficiency of lecithin-cholesterol acyl transferasein some hereditary cases. Secondary sea-blue histio-cytosis has been described in the spleen and marrowof a patient with hyperlipidaemia by Parker et al.(1976), who suggested that the sea-blue histiocytemight be regarded as a marker for abnormal lipidmetabolism. Although this suggestion may be correctin a very general sense, the occurrence of these cellsin the marrow in myeloid leukaemias and occasio-ally in dyserythropoietic states probably has asimilar cause to that leading to the accumulation ofbirefringent blue crystals and Gaucher-like cells,namely, failure of the macrophage enzymes-in thiscase chiefly sphingomyelinase-to cope with the
overproduction of sphingomyelin (phosphoryl cho-line ceramide) resulting from increased turnover ofgranulocytes or erythroblasts in the marrow. Theparallel with Niemann-Pick disease is apparent, andindeed sea-blue material shows weak autofluorescencein UV light and ultrastructurally may show character-tic lamellar whorls similar to those described inNiemann-Pick disease (Parker et al., 1976). In thesestructures the osmiophilic material is thought to bephosphoryl choline and unstained material theceramide portion of sphingomyelin. The lamellar or'fingerprint' pattern may not always be shown bysea-blue material, since we did not find it in eitherof two cases examined by electron microscopy in thepresent study.The third type of lipid inclusions, the grey-green
crystals, show no autofluorescence or birefringence.Stavem et al. (1977) found them only in patientswith myeloid leukaemias and not in lymphoidleukaemias. Our experience is similar, although wehave also found them in one patient with aplasticanaemia and in another with myeloma and eosino-philia. The chemical composition of these grey-green crystals is unknown, and they do not show aperiodic structure in the electron microscope.
Cytochemical studies have not generally been veryhelpful in distinguishing these varieties of acquiredlipidosis. Apart from occasional sudanophilia ofsea-blue granules the intrinsic reactions of allinclusion materials appear weak or negative toperoxidase, PAS, Sudan black, B acid and alkalinephosphatase, and non-specific esterases, althougha surface positivity may be seen with all inclusions,especially to the lysosomal enzymes acid phospha-tase and o-naphthyl butyrate esterase, which areusually strongly positive in normal histiocytes.These variable positive reactions of inclusionmaterial may reflect non-specific surface adsorptionof reaction products or a functional localisation ofenzymes to the site of the inclusion because com-ponents of the inclusion material may serve assubstrates for enzyme activity.The presence of birefringence in pathological
material, including conditions associated with lipidstorage, is reviewed by Wolman (1975). The differ-ences between birefringent and non-birefringentdeposits in histiocytes are not thought to be of greatsignificance, since variations in the proportion ofpolar lipids to other cytoplasmic constituents andthe degree of dispersal or concentration may dictatewhether the lipid molecules are arranged in anorderly fashion leading to birefringence or not.Nevertheless, although we have observed variabilityin intensity of birefringence in the blue crystals andGaucher-like cells, it does seem to offer a reasonablyconsistent and easily recognised discriminatory
427
on January 28, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.5.420 on 1 M
ay 1979. Dow
nloaded from

428 F. G. J. Hayhoe, R. J. Flemans, and D. C. Cowling
feature separating these inclusions from the othertwo types.
All three inclusions appear virtually restricted tostates of pathological myelopoiesis, chiefly myeloidleukaemias, dyserythropoietic or aplastic anaemias,and, much less commonly, idiopathic thrombo-cytopenic purpura. In lymphoproliferative states,in the common anaemias, and in normal bonemarrow aspirates, they are sufficiently rare that apositive finding must cast doubt on the diagnosis. Inour own series, only a single case of acute lympho-cytic leukaemia showed inclusions of both bluecrystals and sea-blue material, while the single case ofmyeloma with inclusions also showed a markedreactive eosinophilia from which the material mayhave been derived. Sea-blue histiocytes have beendescribed recently in the marrow and spleen of apatient with lymphocytic lymphoma (Mason et al.,1978), but there were unusual features in this case,and the presence of two diseases could not be ex-cluded.
We are grateful to Mr J. Emmines for the EM pre-parations and to Miss J. Thompson for typing themanuscript.
References
Albrecht, M. (1966). 'Gaucher-Zellen' bei chronischmyeloischer Leukamie. Blut, 13, 169-179.
Cawley, J. C., and Hayhoe, F. G. J. (1973). Ultrastructureof Haemic Cells, p. 3. W. B. Saunders, Philadelphiaand London.
Dosik, H., Rosner, F., and Sawitsky, A. (1972). Acquiredlipidoses: Gaucher-like cells and 'blue cells' in chronicgranulocytic leukemia. Seminars in Haematology, 9,309-316.
Hayhoe, F. G. J., and Cawley, J. C. (1972). Acuteleukaemia; cellular morphology, cytochemistry andfine structure. Clinics in Haematology, 1, 49-94.
Hayhoe, F. G. J., and Flemans, R. J. (1969). An Atlas ofHaematological Cytology, pp. 316-317. Wolfe MedicalBooks, London.
Higgy, K. E., Burns, G. F., and Hayhoe, F. G. J. (1977).Discrimination of B, T and null lymphocytes by
esterase cytochemistry. Scandinavian Journal ofHaematology, 18, 437-448.
Jacobsen, C. D., Gjone, E., and Hovig, T. (1972). Sea-blue histiocytes in familial lecithin: cholesterol acyl-transferase deficiency. Scandinavian Journal ofHaemato-logy, 9, 106-113.
Kattlove, H. E., Williams, J. C., Gaynor, E., Spivack, M.,Bradley, R. M., and Brady, R. 0. (1969). Gaucher cellsin chronic myelocytic leukemia: an acquired abnorma-lity. Blood, 33, 379-390.
Lewis, S. M., and Verwilghen, R. L. (1977). Dyserythro-poiesis, p. 17. Academic Press, London.
Mason, B. A., Bowers, G. R., Guccion, J. G., andSchechter, G. P. (1978). Sea-blue histiocytes in apatient with lymphoma. American Journal ofMedicine,64, 515-518.
Moeschlin, S. (1951). Spleen Puncture, p. 24. Heinemann,London.
Parker, A. C., Bain, A. D., Brydon, W. G., Harkness,R. A., Smith, A. F., Smith, I. I., and Boyd, D. H. A.(1976). Sea-blue histiocytosis associated with hyper-lipidaemia. Journal of Clinical Pathology, 29, 634-638.
Sawitsky, A., Rosner, F., and Chodsky, S. (1972). Thesea-blue histiocyte syndrome, a review: genetic andbiochemical studies. Seminars in Haematology, 9,285-297.
Silverstein, M. N., and Ellefson, R. D. (1972). Thesyndrome of the sea-blue histiocyte. Seminars inHaematology, 9,299-307.
Stanbury, J. B., Wyngaarden, J. B., and Fredrickson,D. S. (1972). The Metabolic Basis of Inherited Disease.3rd Edition. pp. 736, 790. McGraw-Hill, New York.
Stavem, P., Ly, B., and Bj0rneklett, A. (1977). Lightgreen crystals in May-Grunwald and Giemsa-stainedbone marrow macrophages in patients with myeloidleukaemia. Scandinavian Journal of Haematology, 18,67-72.
Van Dorpe, A., Broeckaert-Van Orshoven, A., Desmet,V., and Verwilghen, R. L. (1973). Gaucher-like cellsand congenital dyserythropoietic anaemia, type II(HEMPAS). British Journal of Haematology, 25, 165-170.
Wolman, M. (1975). Polarized light microscopy as atool of diagnostic pathology: a review. Journal ofHistochemistry and Cytochemistry, 23, 21-50.
Requests for reprints to: Professor F. G. J. Hayhoe,Department of Haematological Medicine, University ofCambridge Clinical School, Hills Road, Cambridge CB22QL, UK.
on January 28, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.5.420 on 1 M
ay 1979. Dow
nloaded from