acquired macular disorders and related conditions pepaired by: enas abu awwad supervision by : dr....
TRANSCRIPT

Acquired Macular Disorders and Related Conditions
pepaired by: Enas Abu Awwad
Supervision by : Dr. Mohammed Shehadeh
Faculty of Optometry
الوطنية النجاح جامعة
الرحيم الرحمن الله بسم
Age related macular hole
Age related (idiopathic) full_ thickness macular hole (FTMH) affected approximately 3 in 1000 individuals characteristically female.
In the sixth or seventh decade. Presentation:
Is with sever impairment of central vision or as a relatively asymptomatic deterioration . first noticed when the follow eye is closed. The risk of involvement of the follow eye at 5 years is about 10%.
Staging
A macular hole results from the centrifugal displacement of photoreceptors from a central dehiscence of the umbo. The primary events is probably an abnormal vitreofoveolar attachment. with resultant anteroposterior and tangential traction initiating the following sequence.
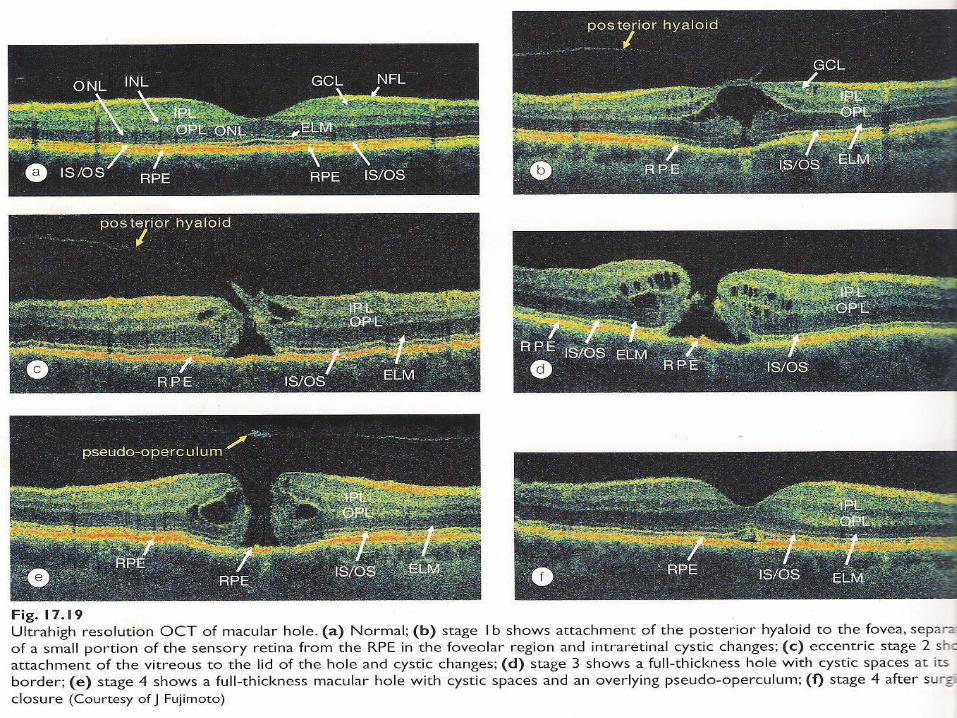
Stage 1a (impending) macular hole is rarely seen clinically and is usually detected in a patient with a FTHM in the other eye. It is characterized by flattening of the umbo, a yellow foveolar spot 100-200µm in diameter and loss of the foveolar reflex.
Stage 1b (occult) macular hole is characterized by a yellow ring with a bridging interface of vitreous cortex that may be associated with mild decrease in visual acuity or metamorphopsia .about 50% of stage 1 hole resolve following spontaneous vitreofoveolar separation.
Stage 2 ( early FTHM) is characterized by a full) thickness defected, less than 300µm in diameter, with or without an overlying prefoveal opacity ( pseudo-operculum) formed by the contracted prefoveal cortical vitreous. Progression from stage 1 to 2 takes between one week and several months.

Stage 3 (established FTHM) is characterized by a full-thickness defect more than 400µm in diameter with an attached posterior vitreous face with or without an overlying pseudo-operculum.
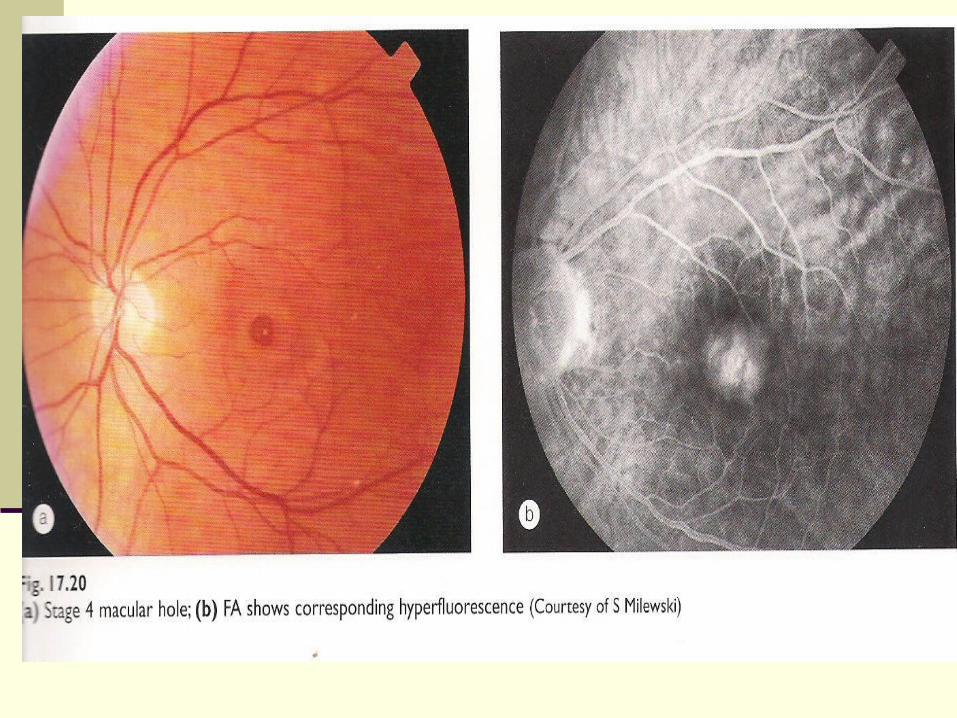
Stage 4 is characterized by a round defect more than 400µm in diameter surrounded by a cuff of subretinal fluid with tiny yellowish deposits within its crater. The posterior vitreous is completely detached, often evidenced by a Weiss ring. Visual acuity is decreased primarily due to the absence of photoreceptors within the central defect, with a resultant absolute central scotoma. In addition, the surrounding cuff of subretinal fluid and secondary retinal elevation cause a surrounding relative scotoma. Vision tends to decline progressively. Stabilizing at 6/60 or worse as the hole reaches its maximal diameter. Some patients may achieve better acuity by employing eccentric fixation.
A FTHM may rarely spontaneously resolve, with improvement of visual acuity, due to spontaneous posterior vitreous detachment and release of vitriol-macular traction.

Diagnostic tests
Watzke-Allen
Laser aiming beam
Optical coherence tomography
Fluorescein angiography

Treatment
Surgical treatment: consists of removal of the cortical vitreous, relief of vitreomacular traction, peeling of the internal limiting membrane (ILM) and gas tamponade followed by strict postoperative face-down positioning.

Central serous retinopathy
Central serous retinopathy (CSR), also known as central serous chorioretinal, is a sporadic disorder of the outer blood-retinal barrier.
Characterized by: A localized detachment of the sensory retina at the
macula secondary to focal RPE defects.
Usually affecting one eye .
IT is usually a self-limited disease typically affecting young or middle-aged men with type A personality (stressed people)

•Risk factors of CSR:
Emotional stress.
Untreated hypertension.
Alcohol use.
Systemic lupus erythematosus .
Organ transplantation .
Gastro-oesophageal reflux
Cushing disease and the administration of steroids, both by inhalation and orally.
Women with CSR tend to be older than affected men, and it is also associated with pregnancy.

Typical CSR: diagnosis Presentation: is with unilateral blurred vision
associated with a relative positive scotoma, micropsia, metamorphopsia and occasionally macropsia. There is also a delay in retinal recovery time after exposure contrast sensitivity. Occasionally the condition is extrafoveal and asymptomatic.

VA is usually reduced to 6/9-6/12 and often correctable to 6/6 with a weak ’plus’ lens. The elevation of the sensory retina gives rise to an acquired hypermetropia with disparity between the subjective refraction of the eye.
Signs:. A round or oval detachment of the sensory retina is
present at the macula.
. The subretinal fluid may be clear or turbid and small precipitates may be present on the posterior surface of the sensory detachment. Occasionally, an abnormal focus in the RPE can be detected, through which fluid has leaked from the choriocapillaris into the subretinal space.

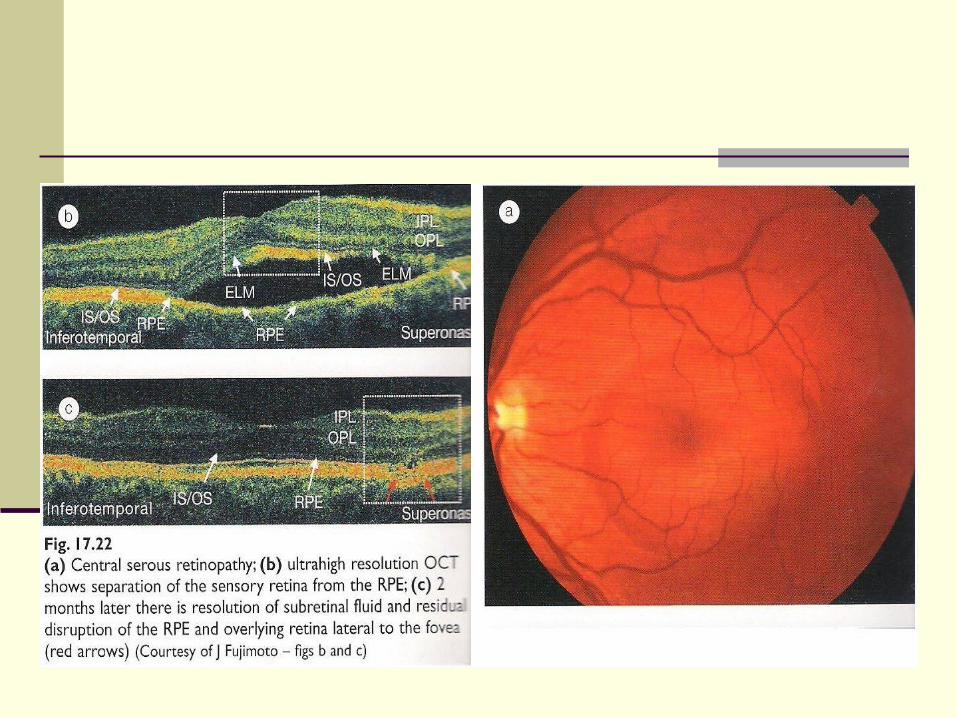
Optical Coherence Tomography: show an elevation of full-thickness sensory retinal layer from the highly reflective RPE layer, separated by an optically empty zone. Sometimes a defect in the RPE may be demonstrated.
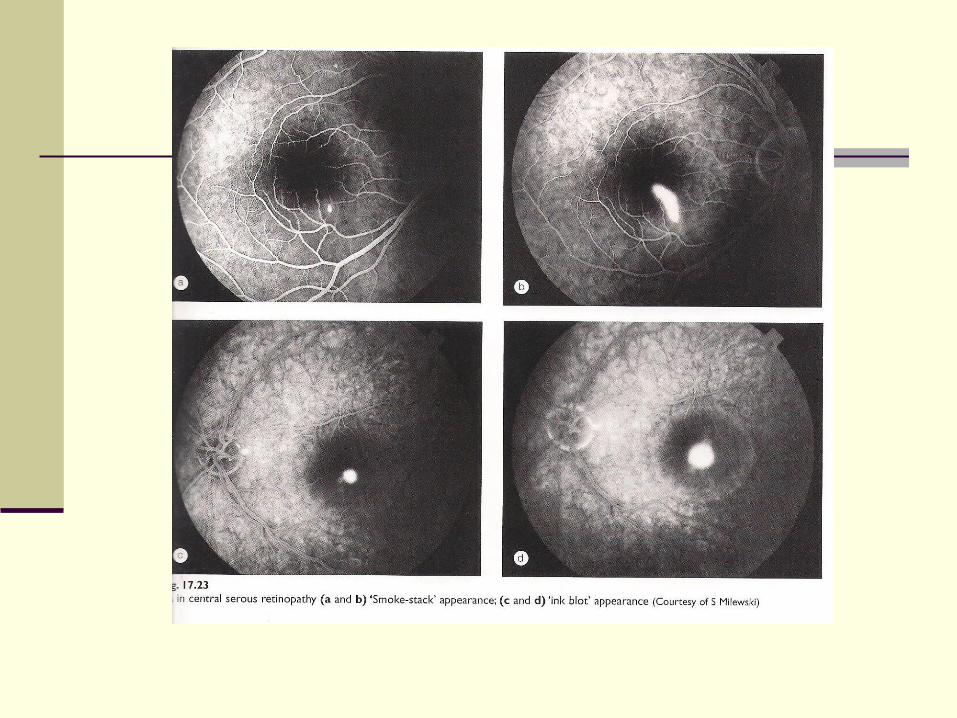
FA show one of the following patterns:
A. smoke-stack appearance is the most common .
B. Ink-blot appearance is less common.

ICG early phase shows dilated choroidal vessels at the posterior pole. The mid stage show multiple areas of hyperfluorescence due to choroidal hyperpermeability, suggesting a more generalized RPE or choroidal vascular disturbance.

Course
Short. Most common, spontaneous absorption of Subretinal fluid occurs within 3-6 months with return to normal or near-normal visual acuity.
Prolonged. In some patients CSR last longer than 6 months but
spontaneously resolves within 12 months. Even if visual acuity return to normal, some degree of subjective visual impairment such as micropsia may persist, but seldom causes any significant disability.
Chronic. In a minority of cases, particularly those older than 50 years, the condition lasts longer than 12 months and is characterized by progressive RPE changes.

Management:
Most cases don’t required treatment.
Argon laser photocoagulation
PDT
Careful follow-up is required as 2-5% of treated eyes subsequently develop CNV.
Cystoid Macular Oedema
CMO is the result of accumulation of fluid in the outer plexiform and inner unclear layers of the retina with the formation of fluid-filled cyst-like changes.
In the short term CMO is usually innocuous; however, long-standing cases usually lead to coalescence of the microcystic spaces into large cavities and subsequent lamellar hole formation at the fovea with irreversible damage to central vision.
CMO is a common and non-specific condition that may occur with any type of macular Oedema.
Diagnosis:
Presentation varies with the cause. Visual acuity may already be impaired by pre-existing disease such as branch vein occlusion. In cases without pre-existing disease the patient complains of impairment of central vision associated with a positive central scotoma.
Signs Slit-lamp biomicroscopy shows loss of the foveal
depression, thickening of the retina and multiple Cystoid areas in the sensory retina (figs 17.25b).
In early cases Cystoid changes may be difficult to discern and the main finding is a yellow spot at the foveola.
OCT shows a collection of hyporeflective spaces within the retina, with overall macular thickening and loss of the foveal depression. OCT is as effective at detecting CMO as FA and produces highly reproducible measurements so that serial examination may be used to assess response to treatment and lamellar hole formation. However, unlike FA it can also be used in eyes with opaque media and is useful in detecting vitreoretinal traction.
FA: The arteriovenous phase shows small hyperfluorescent spot
due to early leakage. The late phase shows a “ flower-petal’ pattern of
hyperfluorescence caused by accumulation of dye within microcystic spaces in the outer plexiform layer of the retina, with its radial arrangement of fibres about the centre of the foveola (Henle layer).

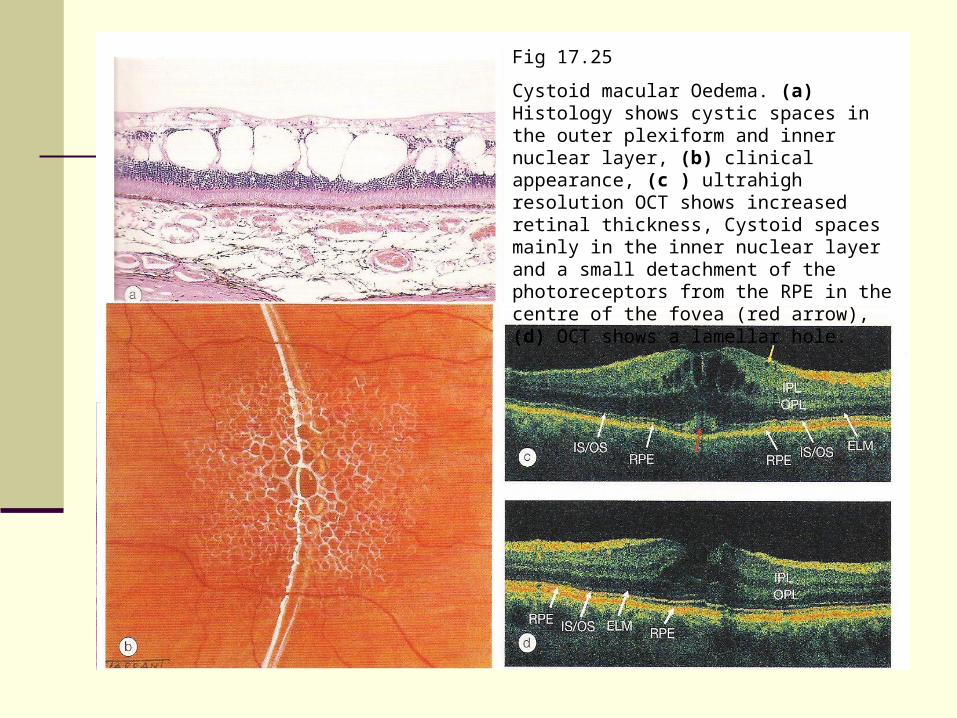
Fig 17.25
Cystoid macular Oedema. (a) Histology shows cystic spaces in the outer plexiform and inner nuclear layer, (b) clinical appearance, (c ) ultrahigh resolution OCT shows increased retinal thickness, Cystoid spaces mainly in the inner nuclear layer and a small detachment of the photoreceptors from the RPE in the centre of the fovea (red arrow), (d) OCT shows a lamellar hole.

Causes and treatment:
Retinal vascular disease: by laser photocoagulation
Intraocular inflammation : NSAIDs or topical steroids
Following cataract surgery : Acetazolmid or diamox
Following other surgical procedures
Drug-induced : involves stopped of medication
Retinal dystrophies
Miscellaneous

Macular epiretinal membrane
Pathogenesis:Macular epiretinal membranes that develop at the
vitreoretinal interface consist of proliferation of retinal glial cells which have gained access to the retinal surface through breaks in the internal limiting membrane.
It has been postulated that these breaks may be created when the posterior vitreous detaches from the macula.

The causes are as follows: idiopathic membrane predominantly affect otherwise healthy
elderly individuals and about 10% of cases.
secondary membranes may be associated with the following condition:
retinal procedures such as detachment surgery, photocoagulation and cryotherapy may either induce or worsen a pre-existing macular epiretinal membrane. Untreated, these membranes usually cause a variable but permanent reduction of vision. Very occasionally, however, the membrane may separate spontaneously from the retina.
Other causes include retinal vascular disease, intraocular inflammation and ocular trauma.

The clinical appearance of epiretinal membranes depends on their density and
any associated distortion of the retinal vasculature. It is convenient to divide the
condition into (a) cellophane maculopathy and (b) macular pucker.

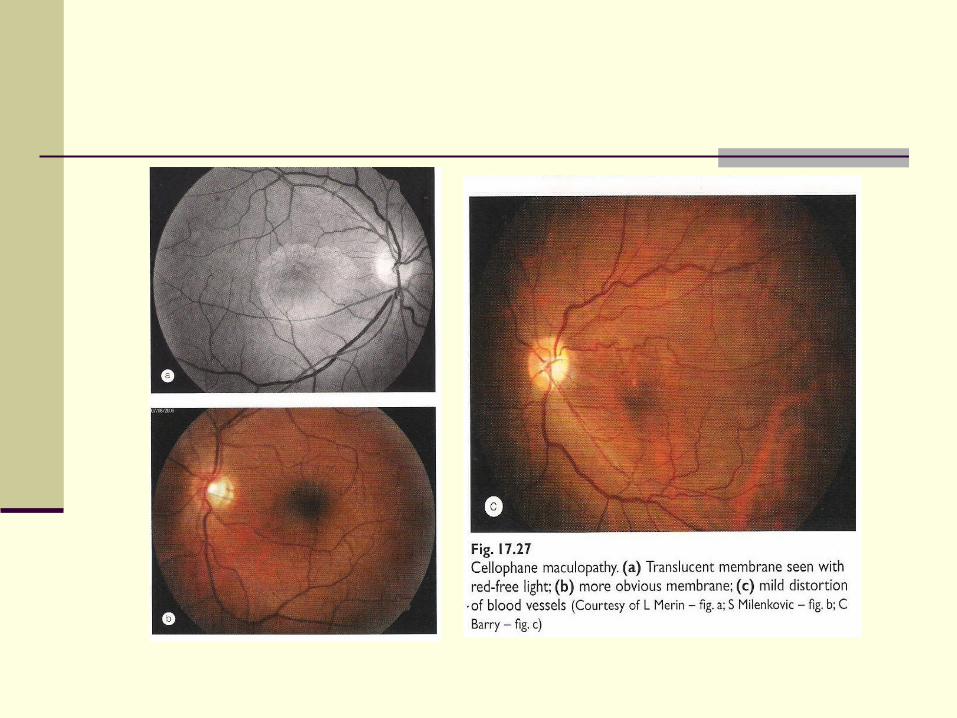
Cellophane maculopathy
Cellophane maculopathy consists of a thin layer of epiretinal cells. It is common and usually secondary to a posterior vitreous detachment.
presentation may be with mild metamorphopsia, although frequently the condition is asymptomatic and is discovered by chance.
signs An irregular light reflex or sheen is present at the macula. The membrane itself is translucent and is best detected using
‘red-free’ light. As it thickens and contracts it becomes more obvious and may
cause mild distortion of blood vessels. Treatment is not appropriate .
Macular pucker
Macular pucker is a more serious condition caused by thickening and contraction of an epiretinal membrane and is much less common than cellophane maculopathy.
Presentation is with metamorphopsia and blurring of central vision.
VA is reduced to 6/12 or worse, depending on severity.
Signs: The macula shows severe distortion of the blood vessels, retinal wrinkling and white striae
which may obscure underlying blood vessels. Associated findings include macular pseudo-holes within the membrane and occasionally
CMO.
FA : highlights the vascular tortuosity and may show hyperfluorescence if leakage is present.
OCT : shows a highly reflective (red) layer on the surface of the retina associated with retinal thickening.
Treatment: by surgical removal of the membrane usually improves or eliminates distortion, and improves visual acuity in about 50% of cases.

Fig.17.28
Macular pucker. a) clinical appearance, (b) FA arterial phase show highlights the vascular tortuosity, ( c) ultrahigh resolution OCT shows a highly reflective membrane at the vitreoretinal interface associated with distortion and increased retinal thickness at the fovea
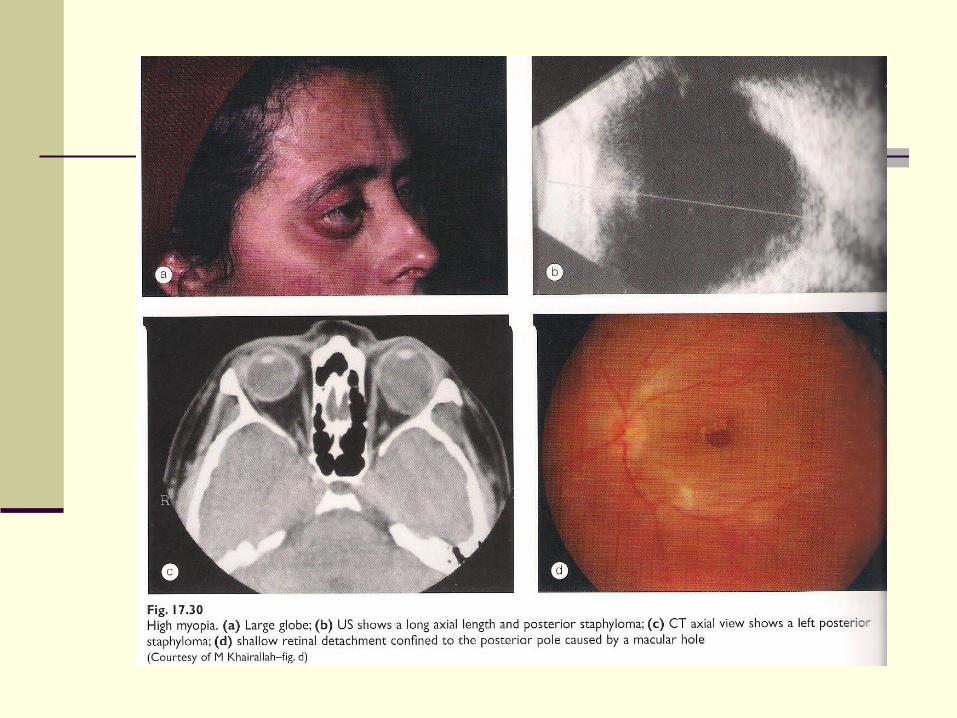
Degenerative myopia
High myopia is defined as an eye with a refractive error >-6D and an axial length of the globe > 26mm.
It affects approximately 0.5% of the general population and 30% of myopic eye.
Pathological or degenerative myopia is characterized by :
progressive and excessive anteroposterior elongation of the globe, which is associated with secondary changes involving the sclera, retina, choroid and optic nerve head.
Maculopathy is the most common cause of visual loss in highly myopic patients.
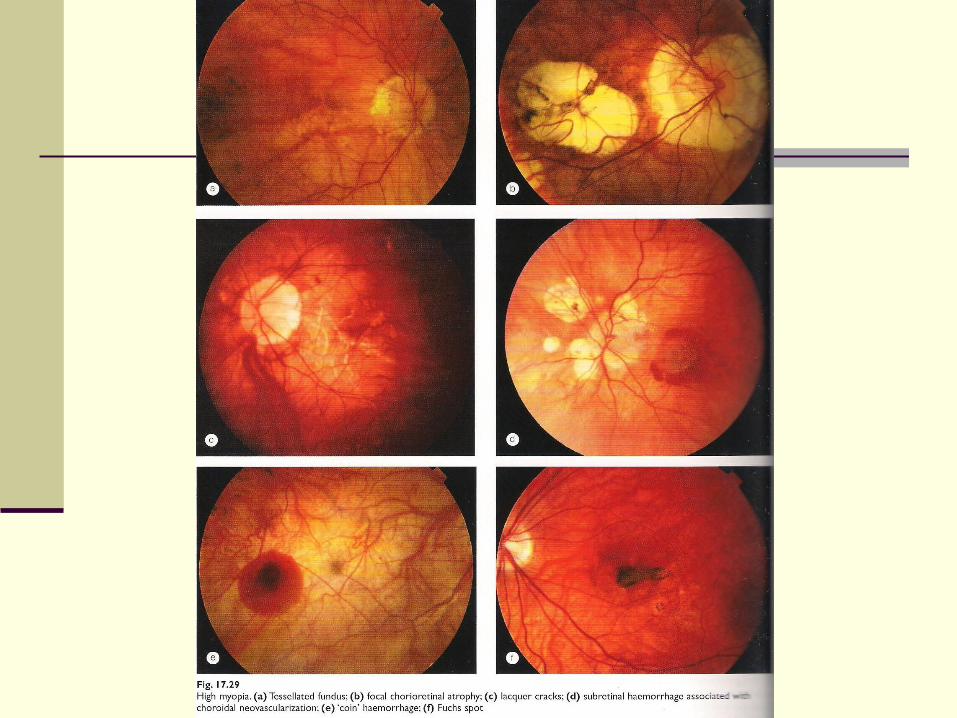
Diagnosis
1. A pale tessellate ( tigroid) appearance due to diffuse attenuation of the RPE with visibility of large choroidal vessels.
2. 3. Focal choroiretinal atrophy characterized by visibility of the larger choroidal
vessels and eventually the sclera.
4. Lacquer cracks consist of ruptures in the RPE-Bruch membrane-choriocapillaris complex characterized by fine, irregular, yellow line, often branching and criss-crossing at the posterior pole.
5. CNV which may develop in association with ‘lacquer cracks’ and areas of patchy atrophy.
6. Subretinal ‘coin’ heamorrhages, which may be intermittent, may develop from lacquer cracks in the absence of CNV.
7. Fuchs spot is a raised, circular, pigmented lesion that may develop after a macular haemorrhage has absorbed.

Complications:
Staphylmas
Focal retinoschisis
Rhegmatogenous retinal detachment
Peripapillary detachment

Associations ocular Cataract, which may be either posterior subcapsular or early onset of nuclear
sclerosis.
Increased prevalence of primary open-angle glaucoma, pigmentary glaucoma and steroid responsiveness.
Retinopathy of prematurity may be associated with the subsequent development of myopia.
Amblyopia is uncommon but may develop when there is a significant difference in myopia between the two eyes.
Systemic Stickler syndrome.
Marfan syndrome.
Ehlers-Danlos syndrome.
Pierre-Robin syndrome