achievement goal structures & self-regulated learning theory_rime_artino.… · nbme...
TRANSCRIPT
Anthony Artino, PhD Ting Dong, PhD
Kent DeZee, MD, MPH William Gilliland, MD
Donna Waechter, PhD David Cruess, PhD
Steven Durning, MD, PhD
November 7, 2012
Achievement Goal Structures & Self-Regulated Learning: Relationships and Changes in Medical School
Annual Meeting of the

RIME 2011 RIME 2012
Background • Understanding the factors that lead to success in medicine
is challenging • Cognitive factors are typically emphasized
• Fields outside of medical have recently stressed “non-cognitive” factors… – Affect (motivation and emotion) – Behavioral components of self-regulated learning (SRL)
Cognitive Factors
Academic Achievement &
Clinical Performance
Cognitive Factors
Academic Achievement &
Clinical Performance
Affective Factors
SRL Behaviors + +
Learning Environment

RIME 2011 RIME 2012
Theoretical Framework
Learning Environment (perceptions of the learning environment)
Personal Factors
Task Value Beliefs
Self-Efficacy
Beliefs
Achievement Goals
Motivational Beliefs
Achievement Emotions
Outcomes
Academic Achievement
Clinical
Performance
reciprocal linkages
Personal Behaviors
Metacognition
Help-Seeking
Behaviors
Procrastination
Positive Emotions
Negative Emotions
Self-Regulated Learning Strategies
Achievement-Goal Structures
Mastery Goal
Structures
Performance- Approach Goal
Structures
Performance- Avoid Goal Structures
Figure. A social-cognitive model of academic motivation, emotion, and self-regulation (adapted from Pekrun, 2006).

RIME 2011 RIME 2012
Study Objectives
Objective 1: – Assess students’ perceptions of the medical school learning
environment (i.e., the achievement-goal structures)
Objective 2: – Determine how these achievement-goal structures relate to students’
SRL behaviors, academic achievement, and clerkship performance
Objective 3: – Examine differences in achievement-goal structures and students’
SRL behaviors from MS-1 to MS-4

RIME 2011 RIME 2012
Method
• Instructional Context – Uniformed Services University
• Traditional curriculum (2+2)
– Survey administered in Spring (Apr/May) of 2011
• Sample – All students (classes 2011 to 2014) invited to
participate (N = 678) – No exclusion criteria

RIME 2011 RIME 2012
Method
Part 1
Mastery Goal Structures (5 items; α = .83)
• “In preclinical courses at USU, really understanding the material is the main goal.” • “In USU clerkships, really understanding…”
Performance-Approach Goal Structures (3 items; α = .78)
• “In preclinical courses at USU, getting good grades is the main goal.” • “In USU clerkships, getting good grades…”
Performance-Avoid Goal Structures (5 items; α = .88)
• “In preclinical courses at USU, it’s important that you don’t make mistakes in front of everyone.” • “In USU clerkships, it’s important…”
Part 2
Metacognition (8 items; α = .82)
• “In preclinical courses at USU, how often do you set goals for yourself in order to direct your activities?” • “In USU clerkships, how often do you…”
Procrastination (4 items; α = .91)
• “In preclinical courses at USU, how often do you postpone doing course readings until the last minute?” • “In USU clerkships, how often do you…”
Avoidance of Help-Seeking (5 items; α = .84)
• “In preclinical courses at USU, how often do you avoid asking for help, even when the course workload is too hard to manage on your own?” • “In USU clerkships, how often do you…”
Survey (30 items)
5-point response scale: extremely untrue extremely true 5-point response scale: almost never almost all the time

RIME 2011 RIME 2012
Method
all students
clerkship students
(MS-3 to 4)
IM clerkship outcomes
• Achievement/performance outcomes 1. Medical school GPA (cumulative) 2. NBME “shelf” examination in medicine 3. Clinical points
Clerkship clinical grades 4. Exam points
Average of two locally developed exams (MCQs) 5. Dept of Medical Education Cmte (DOMEC) referral
Less than passing clinical grade or NBME shelf exam failure
• Analysis – CFA, Pearson correlations, ANOVAs

RIME 2011 RIME 2012
Results
• 304 students (45%) completed the survey – 180 preclinical students (53%) – 124 clinical students (37%)
• 223 men (73%) and 81 women
• Study participants vs. non-participants – MCAT scores and medical school GPA did not differ
between the two groups: F(2, 633) = .72, P = .49
RIME 2011 RIME 2012
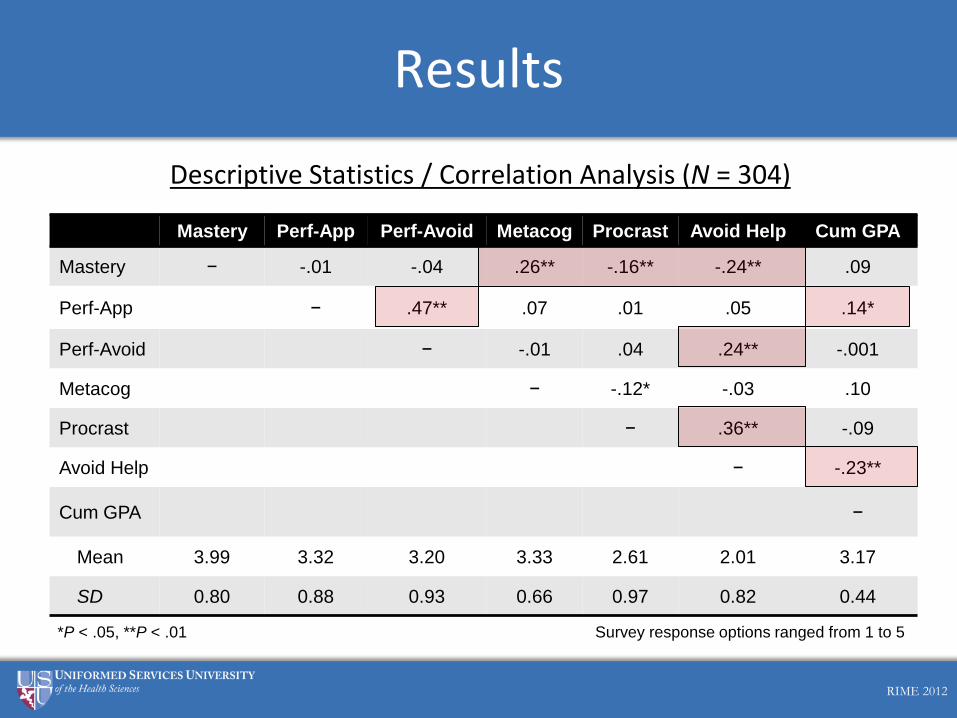
Descriptive Statistics / Correlation Analysis (N = 304)
Results
Mastery Perf-App Perf-Avoid Metacog Procrast Avoid Help Cum GPA
Mastery − -.01 -.04 .26** -.16** -.24** .09
Perf-App − .47** .07 .01 .05 .14*
Perf-Avoid − -.01 .04 .24** -.001
Metacog − -.12* -.03 .10
Procrast − .36** -.09
Avoid Help − -.23**
Cum GPA −
Mean 3.99 3.32 3.20 3.33 2.61 2.01 3.17
SD 0.80 0.88 0.93 0.66 0.97 0.82 0.44
*P < .05, **P < .01 Survey response options ranged from 1 to 5

RIME 2011 RIME 2012
Correlation Analysis (Clerkship Students, n = 126)
Results
Mastery Perf-App Perf-Avoid Metacog Procrast Avoid Help
NBME -.05 -.16 -.04 .01 -.01 -.15
Exam Points -.02 -.20* -.11 -.01 -.06 -.22*
Clinical Points .03 -.12 -.20* .11 -.21* -.34**
DOMEC -.19* .04 .11 -.04 .11 .20*
Note. DOMEC coded 1 = referred to committee; 0 = not referred to committee *P < .05, **P < .01

RIME 2011 RIME 2012
Results
Achievement-Goal Structures: Changes Across Medical School (N = 304)
2
2.5
3
3.5
4
4.5
5
MS-1 MS-2 MS-3 MS-4
Sel
f-Effi
cacy
Res
pons
e O
ptio
ns
Mastery Goal Structures
Performance- Avoid Goal Structures d = 0.24
d = 0.21
d = 0.46 d = 0.29 d = 0.34

RIME 2011 RIME 2012
Discussion
• Perceptions of mastery goal structures are associated with adaptive SRL behaviors
• Perceptions of performance-avoid goal structures are associated with maladaptive behavior
Perform-Avoid
Structures
Help Avoidance
+
Mastery Structures
Metacognition +
Procrastination
Help Avoidance
-
-

RIME 2011 RIME 2012
Discussion
• Maladaptive behaviors are associated with lower academic achievement and poorer clinical performance
Help Avoidance
CumulativeGPA
-
IM Exam Points
IM Clinical Points
DOMEC Referral
-
-
+
Procrastination -

RIME 2011 RIME 2012
Discussion
• Students’ perceptions of the learning environment (achievement-goal structures) appear to change from MS-1 to MS-4 – Mastery goal structures decline in MS-2,
and then recover to MS-1 levels in clinical years – Performance-avoid goal structures steadily rise from MS-1
to MS-3
• Why? – Educational context – Nature of content and skills being taught/learned – Other factors?
Mastery Structures
MS-1
MS-2
MS-1
MS-2
Perform-Avoid
Structures
MS-3

RIME 2011 RIME 2012
Limitations
• Data not longitudinal – Differences observed across medical school should
not be over-interpreted
• Self-reported SRL behaviors – Assessing behaviors can be problematic
• Limited generalizibility – Medical students at one institution

RIME 2011 RIME 2012
Learning Environment
Implications
• Provides conceptual framework for understanding factors that may influence SRL in medical school
• Findings may help medical educators appreciate…
Classroom
Environment
Clinical Settings
Teacher Behaviors
SRL Behaviors
Academic Achievement
Clinical Performance
Anthony Artino, PhD [email protected]
Ting Dong, PhD Kent DeZee, MD, MPH William Gilliland, MD Donna Waechter, PhD
David Cruess, PhD
Questions?
Annual Meeting of the

RIME 2011 RIME 2012
Next Steps
• Measure beliefs, emotions, and behaviors longitudinally across UME/GME
• “Zoom in” on what students think, feel, and do during specific learning activities – Validate self-regulated learning micro-analytic
technique