access year four annual report - oecd. · pdf filebemonc basic emergency obstetric and newborn...
TRANSCRIPT

Phot
o: Jo
hn H
eale
y/jh
ph.c
om
ACCESS Year Four Annual Report
October 1, 2007 – September 30, 2008 Submitted to: United States Agency for International Development under Cooperative Agreement #GHS-A-00-04-00002-00
Submitted by: Jhpiego in collaboration with Save the Children, Constella Futures, Academy for Educational Development, American College of Nurse-Midwives, IMA World Health
Submitted: October 2008 Revised: December 2008


Table of Contents ABBREVIATIONS AND ACRONYMS ............................................................................................IV
SUMMARY ..............................................................................................................................................VII
MAJOR ACHIEVEMENTS IN YEAR FOUR...................................................................................1 SKILLED BIRTH ATTENDANCE .................................................................................................................1
Core Funds ...............................................................................................................................................1 Field Funds ...............................................................................................................................................3 Regional: AFR/SD and Core Funds .........................................................................................................8 Regional: West Africa Funds ....................................................................................................................9
PREVENTION OF POSTPARTUM HEMORRHAGE .................................................................................10
Core Funds .............................................................................................................................................10 Field Funds .............................................................................................................................................10
NEWBORN CARE ......................................................................................................................................13
Core Funds .............................................................................................................................................13 Field Funds .............................................................................................................................................13
ANTENATAL CARE ...................................................................................................................................17
Core Funds .............................................................................................................................................17 Core Malaria Funds ................................................................................................................................17 Field Funds .............................................................................................................................................18
OTHER ACCESS RESULTS FOR WOMEN’S HEALTH...........................................................................20
ACCESS-FP Funds ................................................................................................................................20 Core FP/RH Funds .................................................................................................................................21 Field Funds .............................................................................................................................................21 Preliminary Work on Pre-eclampsia/Eclampsia......................................................................................23
CHALLENGES AND OPPORTUNITIES .......................................................................................24 Challenges..............................................................................................................................................24 Opportunities...........................................................................................................................................25
ANNEX A: CORE ACTIVITY MATRIX...........................................................................................26
ANNEX B: PROGRAM COVERAGE MATRIX............................................................................35
ANNEX C: SUCCESS STORIES .....................................................................................................40
ANNEX D: ACCESS BUREAU AND COUNTRY FUNDING TABLE (PY1–PY4) ...........43
ANNEX E: HIDN RESULTS PATHWAYS REPORT AND OP INDICATORS...................52

iv ACCESS Year Four Annual Report
Abbreviations and Acronyms ACCESS Access to Clinical, Community, Maternal, Neonatal & Women’s Health Services
AFSOG Afghan Society for Obstetricians and Gynecologists
AHTOP Accelerated Health Officer Training Program
AMTSL active management of the third stage of labor AMA Afghanistan Midwives Association ANC antenatal care
ANM auxiliary nurse-midwife
ART antiretroviral therapy APHIA AIDS, Population and Health Integrated Assistance Program BCC behavior change communication BEmONC basic emergency obstetric and newborn care BP/CR birth preparedness and complication readiness
BPHS basic package of health services
CAC community action cycle CAG community action group CEDPA Centre for Development and Population Activities CCG community core group CCMT community care management and treatment CMT community mobilization team CHEW community health extension worker CHW community health worker CKMC community-based Kangaroo Mother Care CRP community resource person CTO contract technical officer DFID Department for International Development (UK) DHS Demographic Health Survey DOT directly observed therapy DRH Division of Reproductive Health
EmONC emergency obstetric and newborn care ENC essential newborn care
FANC focused antenatal care
FBO faith-based organization
FMOH Federal Ministry of Health
FP family planning
FRONTIERS Frontiers in Reproductive Health Program
GMAP Global Malaria Action Plan

ACCESS Year Four Annual Report v
HC health center
HEW health extension worker
HIDN health, infectious diseases and nutrition HO health officer HP health post HAS health surveillance assistant HSSP Health Services Support Program IEC information, education and communication IMAI integrated management of adult illness IMCI integrated management of childhood illness IP infection prevention IPT intermittent preventive treatment
IR intermediate result
ITN insecticide-treated (bed) net
IUD intrauterine device JICA Japan International Cooperation Agency KMC Kangaroo Mother Care
LAM Lactational Amenorrhea Method
LBW low birth weight
LGA local government area
LRP learning resource package
MAISHA Mothers and Infants, Safe, Healthy and Alive Program
MCH maternal and child health
MCPC managing complications in pregnancy and childbirth
M&E monitoring and evaluation
MIP malaria in pregnancy
MMAM Primary Health Services Development Programme
MNH maternal and newborn health
MOH Ministry of Health
MOHSW Ministry of Health and Social Welfare
MOPH Ministry of Public Health
MSP making pregnancy safer MWRA married women of reproductive age NASCOP National AIDS and STD Control Programme NFHP National Family Health Program NGO nongovernmental organization NMCP National Malaria Control Programme NRHP National Reproductive Health Program

vi ACCESS Year Four Annual Report
PAC postabortion care
PE/E pre-eclampsia/eclampsia
PITC provider-initiated testing and counseling
PMI President’s Malaria Initiative
PMNCH Partnership for Maternal, Newborn and Child Health
PMTCT prevention of mother-to-child transmission of HIV
POPPHI Prevention of Postpartum Hemorrhage Initiative
PPFP postpartum family planning
PPH postpartum hemorrhage
PQI performance and quality improvement
QI quality improvement
QQT quality improvement team
RACHA Reproductive and Child Health Alliance
RBM Roll Back Malaria
RCH reproductive and child health
RHAC Reproductive Health Association of Cambodia
RH reproductive health
RN/M registered nurse-midwife
SBA skilled birth attendance/attendant
SBAI Safe Birth Africa Initiative
SBM/R Standards-Based Management and Recognition SIP syphilis in pregnancy
SNL saving newborn lives
SP sulfadoxine-pyrimethamine
SSC skin-to-skin care
TBA traditional birth attendant
TIMS© Training Information Monitoring System
TOT training of trainers
UNFPA United Nations Population Fund
UNICEF United Nations Children’s Fund
USAID United States Agency for International Development
VIA Visual Inspection of the cervix with Acetic Acid
WHO World Health Organization WRA White Ribbon Alliance

ACCESS Year Four Annual Report vii
Summary The Access to Clinical and Community Maternal, Neonatal and Women’s Health Services (ACCESS) Program seeks to increase use and coverage of maternal, neonatal and women’s health and nutrition interventions. ACCESS is a five-year, $75 million Leader with Associate Awards to Jhpiego in collaboration with Save the Children, Constella Futures, the Academy for Educational Development, American College of Nurse-Midwives and IMA World Health. Since its start in July 2004, ACCESS has received $65.2 million, leaving approximately $9.8 million for FY08 obligations before reaching the Program ceiling. ACCESS has worked in more than 25 countries with large country programs in Bangladesh, Tanzania, Kenya, Nigeria, Malawi, Ethiopia, South Africa and Rwanda. ACCESS has received four associate awards: ACCESS-FP, ACCESS/Afghanistan (Health Services Support Program [HSSP]), ACCESS/Cambodia, and Mothers and Infants, Safe, Healthy and Alive (MAISHA/Tanzania). This report presents ACCESS Program results and activities from 1 October 2007 to 30 September 2008 and is organized by the four results pathways of the United States Agency for International Development’s (USAID) Office of Health, Infectious Diseases and Nutrition (HIDN): skilled birth attendance (SBA), antenatal care (ANC), postpartum hemorrhage (PPH) and newborn care. Important results that do not fit under these pathways are presented under an “other results” category. The final section in this report discusses challenges and programmatic opportunities. Over the past year, through its global program implementation and technical assistance, ACCESS programs made skilled delivery care, including prevention of postpartum hemorrhage services and essential newborn care, available to over eleven million women of reproductive age in eight countries (Afghanistan, Ghana, India, Kenya, Malawi, Nigeria, Rwanda and Tanzania). In Bangladesh, ACCESS-trained counselors promoted essential newborn care at home births: of 38,306 women reached postpartum: 96% of newborns had clean cord care, 85% mothers initiated breastfeeding within one hour of birth, 87% of newborns were dried and wrapped immediately after birth. Beyond the results pathways, ACCESS activities have led to improved coverage for family planning in Nigeria and Kenya, improved post abortion care in Malawi and Haiti, and improved services in PMTCT and ARTs. In Malawi, Afghanistan, South Africa, Nigeria, Ghana, Kenya and Rwanda, ACCESS has improved the quality of care using performance standards at over 330 health facilities. ACCESS has continued collaboration with the World Health Organization (WHO), the Partnership for Maternal, Newborn and Child Health (PMNCH) and the White Ribbon Alliance (WRA). Through our small grant awards for innovative work, faith-based organization (FBO) grants are being implemented by a team representing both Islamic and Christian FBOs and the Ministry of Health (MOH), thereby strengthening working relationships and developing new strategies for sharing knowledge across networks. And with key stakeholders from USAID, UNICEF, Saving Newborn Lives (SNL), USAID cooperating agencies, researchers and field staff, ACCESS sponsored a one-day consultation meeting to discuss community-based skin-to-skin care (SSC) for low birth weight newborns.
viii ACCESS Year Four Annual Report
In the area of malaria, ACCESS contributed to the development of the Roll Back Malaria (RBM) Global Malaria Action Plan (GMAP)—which was finalized in September 2008—through its membership in the Malaria in Pregnancy (MIP) Working Group. When GMAP was officially launched in September at the Millennium Development Goals Summit in New York and in malaria-endemic regions, it was introduced as the global road map for malaria control and elimination around which all stakeholders can coordinate their actions. ACCESS also revised the Malaria Resource Package developed in 2003 to add updated information on MIP and to include an implementation guide. The guide, which outlines seven essential programming components that are needed to put MIP policy into practice at the health facility level, draws on existing country experiences, best practices and lessons learned for practical implementation. The ACCESS Program Web site, which is used to share news and disseminate key tools and resources, had nearly 10,000 new visitors in this year alone, and more than 4,000 people have now completed the seven ACCESS-developed USAID Global Health e-learning courses since their inception. ACCESS has also achieved key results using core funds at the country level. In Kenya and Rwanda, ACCESS contributed to efforts to update the knowledge and skills of service providers in the prevention of postpartum hemorrhage (PPH). From January to September 2008 at health facilities in two ACCESS focus districts in Rwanda where training has been completed, 91% of vaginal births received AMTSL. In India, ACCESS and CEDPA are working together to increase access to and demand for skilled community-based midwives. And in Nigeria, ACCESS continued work with the Mada community in Zamfara State to address financial barriers to health services, including developing ways for women to save and loan money to one another. Using field support funds in multiple countries, ACCESS worked to develop and provide input into national policies on maternal and newborn health (MNH) as well as to scale up capacity building, community outreach and demand generation for MNH interventions:
Over the past year, Kangaroo Mother Care (KMC) has continued to be supported in five country programs—Nigeria, Bangladesh, Malawi, Nepal and Rwanda (using core funds). In Rwanda, KMC was expanded to seven more hospitals.
In Ethiopia, ACCESS initiated the basic emergency obstetric and newborn care (BEmONC) skills strengthening of faculty for pre-service training of health officers and prepared materials for and initiated in-service training of health extension workers (HEWs). ACCESS/Ethiopia increased access to key MNH services by arranging to obtain free misoprostol for HEWs to use to prevent PPH in the third stage of labor, and trained 358 HEWs to improve service delivery at the health post and community levels.
In Cambodia, ACCESS contributed to the revision of national postabortion care (PAC) guidelines, assisted national MNH working groups and updated an integrated postnatal care (PNC) package for midwives for the MOH, which is being field-tested and developed through a partnership of nine international and local organizations.
In Nepal, ACCESS provided technical assistance to the USAID bilateral and Ministry of Health (MOH) to plan an intervention on community-level prevention of eclampsia using high doses of calcium.

ACCESS Year Four Annual Report ix
Afghanistan HSSP finalized national quality assurance standards, which were used to improve the quality of services as documented in baseline and follow-up assessments. HSSP also continued to build the capacity of local nongovernmental organizations (NGOs) implementing the basic package of health services (BPHS). The government of Afghanistan is moving forward to scale up, in a phased manner, the provision of misoprostol at the community level—a direct consequence of the pilot project for community-based prevention of PPH in Afghanistan, where results showed that the use of misoprostol is safe and programmatically effective.
ACCESS/Tanzania held a successful White Ribbon Day event with over 500 participants and assisted Zanzibar to form its own White Ribbon Alliance (WRA). ACCESS continued to scale up focused antenatal care (FANC) training in Tanzania nationally, and was cited for its good work during President Bush’s visit to the country.
President Bush visited Tanzania in February 2008 as part of an effort to observe the current PMI- and PEPFAR-funded initiatives in action. In preparation for this visit, ACCESS developed a press release; identified useful FANC information, education and communication (IEC) materials for display during official site visits; and provided updated program information to USAID for use in preparation of presidential remarks during his visit. The ACCESS FANC program was highlighted by President Bush during a speech he made at Meru District Hospital.
In Malawi, ACCESS continued to increase the quality of reproductive health (RH) services by supporting the Minitry of Health/Reproductive Health Unit to apply the Standards-Based Management and Recognition (SBM-R) quality improvement (QI) approach. At a national stakeholders meeting, RH focal persons from six participating district hospitals presented findings from their internal QI assessments, which measured 14 areas of RH, including prevention and management of PPH. Baseline results from March 2008 were similar across facilities, with a mean score of 34%. By August 2008, all facilities showed improvements, with a mean score of 71%.
A rapid needs assessment sponsored by ACCESS and NMCP in Malawi identified a severe shortage of staff trained on FANC and MIP and shortages of SP and other supplies for IPTp by directly observed therapy (DOT). In response, ACCESS trained 680 ANC service providers from all 28 districts in FANC/MIP and provided basic supplies for IPTp to all 730 health facilities across the country. Supportive supervision visits to 56 facilities revealed that over 80% had the requisite DOT supplies.
In Bangladesh, trained counselors conducted 84,014 pregnancy preparedness home visits, counseling pregnant women on healthy MNH behaviors and steps to take to prepare for birth. The counselors reached 18,999 (50%) recent mothers within 24 hours and 25,800 (67%) within 72 hours and conducted postpartum counseling visits. Among 38,306 women reached: 48% had a birth plan, 76% newborns were attended by a newborn care person, 96% of newborns had clean cord care, 85% mothers initiated breastfeeding within one hour of birth, 87% of newborns were dried and wrapped immediately after birth, and 80% of mothers delayed bathing their newborns for three days.
In Kenya, ACCESS worked to support the Division of Reproductive Health (DRH) to move forward with prevention of mother-to-child transmission of HIV (PMTCT) standards and services. Providers at ACCESS-supported pilot sites in Kenya successfully provided

x ACCESS Year Four Annual Report
integrated ANC/tuberculosis screening services. In addition, Kenya helped develop new policy guidelines on reproductive tract cancer and HIV counseling and testing. ACCESS moved toward integration of FP and STI services with HIV/AIDS services in Kenya with the development of two orientation packages—an FP orientation package and a STI orientation package—for service providers working in comprehensive HIV care centers. Both orientation packages were adopted by the NASCOP and other partners.
In South Africa, ACCESS-supported facilities demonstrated improved quality of antiretroviral therapy (ART) services and technical assistance led to the revision and dissemination of various HIV/AIDS service delivery guidelines.
During this reporting period in Nigeria, 22,092 women delivered with a skilled birth attendant at 18 ACCESS-supported facilities. Of these, 18,471 women received AMTSL (99% of vaginal births). At 16 ACCESS-supported facilities, 10,400 births (42%) were managed using the partograph. In addition, 1,284 women with eclampsia received treatment according to protocol at 17 hospitals reporting. And 18,037 mothers and newborns received postpartum/postnatal care within three days at 34 ACCESS-supported hospitals. With respect to family planning (FP), 26,836 individuals received FP counseling (23,485 females and 901 males at 37 facilities and 2,450 counseled by household counselors) and 1,974 clients at 25 facilities received FP counseling postpartum.
While new country programs, such as Malawi and Ethiopia, began activities during this reporting period, several other existing ACCESS country programs closed, including Haiti, West Africa and ACCESS/Afghanistan (separate from HSSP). ACCESS also received a new associate award in Tanzania—the Mothers and Infants, Safe, Healthy and Alive (MAISHA) Program—to improve clinical and community maternal, neonatal and women’s health services. Under the MAISHA Program, Jhpiego and its partners will collaborate with the Tanzanian MOHSW to deliver critical, evidence-based health interventions on a national scale to reduce maternal and newborn morbidity and mortality, contributing to the achievement of the national targets for Millennium Development Goals (MDGs) Four and Five. The ACCESS/Tanzania program has already successfully implemented this strategy to address malaria in pregnancy (MIP) and syphilis in pregnancy (SIP) using the platform of focused antenatal care (FANC), and will continue to do so under MAISHA. Similarly, ACCESS will assist the Tanzanian MOHSW to strengthen basic emergency obstetric and neonatal care (BEmONC), including the prevention and treatment of PPH, newborn resuscitation, treatment of sepsis, and immediate warming and drying. Finally, the MAISHA program will strengthen the platform of prevention of mother-to-child transmission of HIV/AIDS (PMTCT) established by USAID partners to address gaps in integrating MNH services for HIV-positive women and children. Overall, the MAISHA technical approach will adhere to the principles of integration, national coverage, quality, sustainability, accountability, innovation, gender equity and cost-effectiveness.

ACCESS Year Four Annual Report xi

ACCESS Year Four Annual Report 1
Major Achievements in Year Four SKILLED BIRTH ATTENDANCE Core Funds
In Nigeria, ACCESS continued work with local stakeholders and representatives from Zamfara State to implement a community initiative to address financial barriers to antenatal, obstetric and post-obstetric services. Members of the community were trained as facilitators for the Village Savings and Loan Associations, which now have 120 members. Eight Village Savings and Loan Associations were established—six more than originally planned due to high demand—to help women save money for themselves, for MNH-related and other emergencies, and for helping community members.
Collaborated with global stakeholders to support the international Women Deliver conference in London on 18–20 October 2007, including support to more than 20 participants and panelists. ACCESS and ACCESS-FP facilitated several panel discussions on PPH, SBA, postpartum family planning (PPFP), FBOs and malaria in pregnancy (MIP). WRA representatives presented panel discussions and provided country examples; two representatives from faith-based health networks in Africa presented papers that raised awareness of the role of FBOs in providing health care services.
Major issues to be addressed in the revision of the Managing Complications in Pregnancy and Childbirth Manual have been identified, and ACCESS staff are in the process of re-writing assigned technical sections. Communication with the Making Pregnancy Safer Department of WHO has been on-going to determine a revised timeline given the present delay.
USAID’s Global Health Maternal Survival: Programming Issues e-learning course was completed by more than 250 users since it was uploaded.
Continued to support the Partnership of Maternal, Newborn and Child Health (PMNCH) with a technical advisor who is assisting with implementation of their global activities.
Continued work on the “Guide to Save Mothers and Newborn Lives: A Toolkit for Religious Leaders” to help build the capacity of Christian and Islamic leaders to promote safe motherhood through their sermons and other presentations.
From January to September 2008 at three hospitals and 13 health centers in two ACCESS focus districts in Rwanda where EmONC training has been completed, 91% of vaginal births received AMTSL and 94% of all births were managed using the partograph.
In Rwanda, ACCESS expanded beyond the initial four districts. A new group of national-level trainers was trained. ACCESS and partners assisted the Ministry of Health (MOH) to design a plan for national-level scale up of the MNH strategy. A health facility survey and the qualitative assessment were completed and preliminary reports shared with the MOH and partners. Results informed the development of a draft national community behavior change strategy.
In Rwanda, nine hospitals and their corresponding health centers are benefiting from medical equipment and supplies donated by ACCESS to improve services and safe birth outcomes; increased use of partographs, AMTSL and infection prevention practices have been observed at six district maternity hospitals and 29 health centers; and trainers are ready
2 ACCESS Year Four Annual Report
Newly graduated midwives in Badakshan Province, Afghanistan, take the midwives’ pledge.
to begin on-the-job training of providers at five district hospitals, which is the next step in the strategy to scale up EmONC services in Rwanda.
In Ghana, ACCESS expanded activities—including all modules, BEmONC training, coaching, internal and external assessments, data collection and related training—to the southern part of the Birim North District to include eight new facilities, one of which is a district-level hospital, bringing the total number of facilities covered under the project to 11. Completed SBM-R Modules I, II and III for all 11 facilities. Trained five external assessors to increase sustainability of the quality improvement process and make the Birim North District a national model for the accreditation process.
In Ethiopia, 10 health centers that refer cases to Ambo Hospital Maternity Services were assessed, and EmONC service delivery improved at these health centers with the support of ACCESS and the Ethiopian Society of Obstetricians and Gynecologists (ESOG). Nine of 10 providers were trained in BEmONC (one provider was on leave), and referral linkages between 10 health centers and Ambo Hospital were strengthened.
In Jharkhand, India, where ACCESS and CEDPA trained an additional 19 auxiliary nurse-midwives (ANMs) to competency as SBAs in evidence-based care, and all 37 ACCESS-trained ANMs were provided continued support so that they could provide care in the community and at functional facilities. Among the reporting ANMs, AMTSL was provided at over 94% of deliveries and more than 98% of the newborns delivered by ACCESS-trained ANMs had clean cord care, immediate breastfeeding (within an hour), and immediate drying and wrapping. ACCESS also field-tested and finalized an ANM learning resource package, and continued to strengthen two hospitals and two ANM schools as training centers.
In India, worked with NGO Chetna Vikas to mobilize 223 villages and train more than 3,700 community members, resulting in 100% of these ACCESS-supported villages having a functional emergency transport system for birth preparedness and complications readiness (BP/CR) during pregnancy and childbirth, and 69% using the services provided by the ACCESS-trained ANMs in their area.
In Nepal, developed SBA in-service training site standards (tools), and supported eight training sites with use of the tools to make improvements and monitor the quality of SBA training. Disseminated six project reports on key interventions and results.

ACCESS Year Four Annual Report 3
Field Funds At the request of the national Postabortion Care (PAC) Technical Working Group in
Cambodia, drafted an additional chapter to introduce medical management of incomplete abortion for the national postabortion care (PAC) guidelines, and an accompanying outline for a training module. The national protocol is being used to standardize PAC services in Cambodia.
Provided technical expertise and leadership at the national level in Cambodia as a member of coordination bodies at the MOH, including membership of the Secretariat of the High-Level Midwifery Task Force and the National Neonatal Health sub-working group. ACCESS technical assistance helped the MOH develop a vision statement, terms of reference and a five-year work plan for the Secretariat of the Midwifery Task Force.
In Afghanistan, 139 community midwives graduated from HSSP-supported community midwifery education programs. The midwives were trained in an 18-month competency-based program and have now been deployed to rural and remote areas of Afghanistan.
Afghanistan HSSP continued to build the capacity of NGOs implementing the Basic Package of Health Services (BPHS), training 607 health providers, NGO managers and representatives from the central and provincial MOPH to improve performance in: IP, partnership-defined quality, rational use of drug/management drug supply, gender, general management, behavior change communication (BCC) and human resource management.
Quality assurance standards for 14 areas of the Basic Package of Health Services (BPHS) have been finalized in collaboration with the Afghanistan Ministry of Public Health (MOPH) and the Central Quality Assurance Committee. Baseline assessment results from 38 health facilities in five provinces were presented to the leadership of the MOPH, and HSSP has been asked to expand implementation of the process to all 13 provinces supported by USAID. NGOs are implementing action plans to bridge the performance gaps identified.
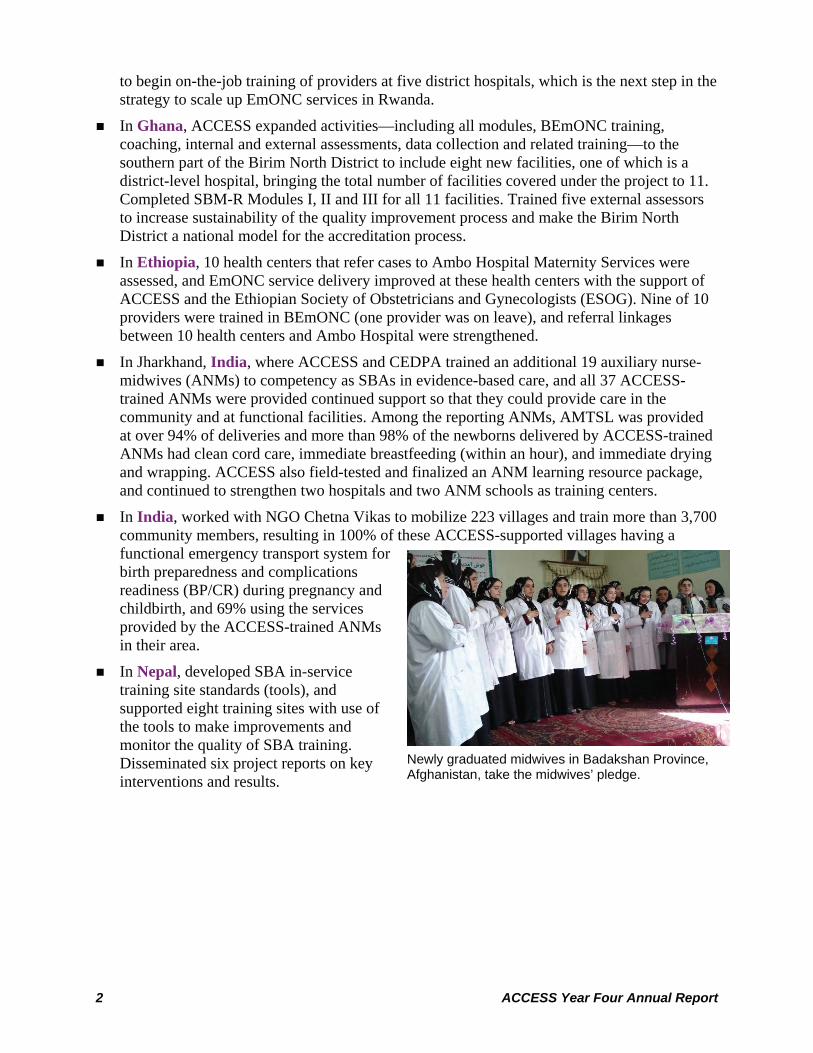
Afghanistan HSSP continues its secretarial and technical support to the National Midwifery Education Accreditation Board (NMEAB) to monitor the quality of the midwifery education programs across the country. Over the last year, 13 midwifery education programs were re-accredited. All HSSP schools that were due for accreditation have also been re-accredited (see Figure 1 below).
4 ACCESS Year Four Annual Report
The winning WRA quilt panel in Afghanistan depicting the story of Bibi Maroon, who died in childbirth.
Figure 1: Assessment Scores for Midwifery Schools
Afghanistan HSSP continued to provide technical support to the Afghanistan Midwives Association (AMA), and has now extended its support to the Afghan Society for Obstetricians and Gynecologists (AFSOG) to strengthen obstetric care. A partnership has been established between the two professional associations, with the AMA providing AFSOG with support in how to run a professional association. Both associations celebrated annual congresses, with the AMA celebrating its Fourth Annual Congress. AFSOG conducted their second congress, attended by 150 participants, with the theme, “Afghan obstetricians, gynecologists and midwives are working together to make women and newborn health better in Afghanistan.” AMA also ran a competition to design a quilt panel for the White Ribbon Alliance’s Mothers’ Memorial Quilt, started in 2007.
Three facilities in Malawi achieved target levels of performance and quality in IP with scores above 80% (88–91%) on IP standards. The facilities were nationally recognized by the MOH.
Developed a Community Mobilization Training Manual for the community MNH package in Malawi and trained 40 more HSAs. The manual targets trainers who train and supervise HSAs on community-level MNH knowledge and skills. Those receiving community mobilization training will be able to support collective analysis, planning and action within villages to combat issues that are more effectively addressed on a community level, such as
Non-binding and binding assessments of HSSP supported midwifery education schools against midwifery education
standards over all compliance by province
83% 83%82%88% 89%91%
95%97%95%92%
97% 98%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Badakhshan Bamyan Hirat Khost Paktiya Takhar
Non-Binding
Binding
Data source: HSSP accreditat ion dbDate: September 2008

ACCESS Year Four Annual Report 5
President of the United Republic of Tanzania, Jakaya Kikwete, holds a baby at the WRA White Ribbon Day Ceremony.
lack of available transport or local financing schemes to enable the poorest families to take short-term loans for MNH-related emergencies.
In Malawi, assisted the MOH to strengthen BEmONC and PAC pre-service training following a national assessment in 2005, which showed that Malawi has only 2% of the WHO-recommended number of BEmONC facilities. ACCESS trained 12 tutors and 9 preceptors from all 13 nurse-midwifery training institutions in the delivery of BEmONC. Ten tutors and 8 preceptors were also trained in PAC.
The WRA of Tanzania, with support from ACCESS and other key partners, coordinated a successful White Ribbon Day event, with the President of the United Republic of Tanzania and his wife as the guests of honor. The WRA also provided technical assistance to Zanzibar to establish its own chapter of the Alliance, which was launched in March 2008.
ACCESS/Tanzania collaborated with the Ministry of Health and Social Welfare (MOHSW) to establish a Safe Motherhood Working Group, a sub-group of the Reproductive and Child Health Services National Coordination Group, to address MNH issues and the policy and social environments. ACCESS is the Secretariat for this national working group. The Safe Motherhood Working Group, in collaboration with the UN bodies and the MOHSW, organized a successful launch of the ambitious One Plan to cut the number of maternal, newborn and child deaths—alongside an advocacy campaign, Deliver Now for Women and Children in Tanzania—to mobilize communities around this issue. The launch was officiated by the President of United Republic of Tanzania and the Honorable Prime Minister of Norway on 22 April 2008 in Dar es Salaam.
Provided assistance to the Tanzania MOHSW, along with multiple UN agencies, to revise the One Plan, the implementation strategy for the National Road Map Strategic Plan to Accelerate Reduction of Maternal and Newborn Deaths in Tanzania (2006–2010). ACCESS also provided support to the Zanzibar MOHSW in developing their own national road map.
Strengthened the Accelerated Health Officer Training Program (AHOTP) in Ethiopia: upgraded eight of 20 hospitals in the country to serve as training sites; updated BEmONC knowledge and skills of faculty from AHOTP-affiliated universities and providers in the eight selected training hospitals to ensure standardization and quality of MNH training.

6 ACCESS Year Four Annual Report
Bedessa Ethiopian mother and child.
In Ethiopia, strengthened the capacity of Ethiopian Institutions to train health extension workers (HEWs) in the Oromia region: upgraded 12 health centers to serve as training sites; developed HEW safe and clean delivery learning resource package in collaboration with the Federal Ministry of Health, UNICEF, Save the Children US, the Ethiopian Nurse Midwives Association and others; and trained trainers from the health centers.
ACCESS/Ethiopia arranged to obtain free misoprostol for HEWs to use to prevent PPH in the third stage of labor and contributed content on use of misoprostol for the national HEW training manual. Also trained 358 HEWs to improve service delivery at the health post and community levels and, to ensure transfer of skills on the job, provided supportive supervision visits to all health centers (HCs) and health posts (HPs) where the trained HEWs are posted.
In Ethiopia, improved MNH recordkeeping, set up a monitoring and evaluation system that captures MNH outcomes related to pregnancy, delivery and postpartum care (home visits at third trimester and postnatal period). Data collection instruments to link HPs to the community were revised and HEWs were oriented on the revisions.
During this reporting period in Nigeria, 22,092 women delivered with an SBA at 18 ACCESS-supported facilities. Of these, 18,471 women received AMTSL (99% of vaginal births). At 16 ACCESS-supported facilities, 10,400 births (42%) were managed using the partograph.
ACCESS/Nigeria conducted baseline SBM-R EmONC assessments in all its new facilities, provided feedback to facility staff, and provided technical assistance for action plan development with the quality improvement team members in the facilities. ACCESS facilitated follow-up assessments in continuing facilities and held a meeting for the development of FP performance standards to complement the EmONC performance standards. Scores for EmONC standards at six hospitals completing follow-up assessments are provided in Figure 2 below.

ACCESS Year Four Annual Report 7
Trained household counselors in a role play in Nigeria.
Figure 2. EmONC Performance Scores in Nigerian Hospitals
0
10
20
30
40
50
60
70
80
90
100
MMSH GezawaGH
DawakinTofa
KauraNamoda
Zurmi GH KF-WCH
Hospitals
Baseline1st Fo llowup
In Nigeria, ACCESS renovated eight health facilities in Kano and Zamfara States and awarded contracts for additional five selected facilities.
ACCESS/Nigeria trained 85 female household counselors in Kano and Zamfara States who have started conducting household visits, three days per week and three to five visits per day to pregnant women in their communities. They counsel on the importance of ANC and BP/CR, inform about the danger signs during pregnancy, delivery and postpartum/newborn, and describe the importance of breastfeeding and birth spacing using the counseling flip chart developed by ACCESS.
ACCESS/Nigeria increased the capacity of community mobilizers to promote MNH using the community action cycle (CAC) concept. Twenty-one community mobilizers in Kano, Katsina and Zamfara States were trained as trainers, who in turn trained community mobilization teams (CMT) and community core groups (CCG) on how to mobilize communities for MNH in the 10 new local government areas (LGAs) in the three states. The trained CMTs and CCGs created 24 work plans, which are now being implemented.
8 ACCESS Year Four Annual Report
Transporting a pregnant woman, Tanzania.
Regional: AFR/SD and Core Funds Completed revisions to the Best Practices in Essential and Basic Emergency Obstetric and
Newborn Care LRP based on pre-test recommendations. Package is currently being copyedited and formatted.
Planned and held second regional Clinical Training Skills and Curriculum Design courses in April for approximately 20 pre-service midwifery educators from three countries (Ethiopia, Ghana and Tanzania) to build more champions for integrating best practices in BEmONC with midwifery education and practice. Participants assisted in the facilitation of BEmONC Technical Update and Clinical Skills Standardizations in Ethiopia and Ghana, and will participate in upcoming advocacy meetings at the national level.
Integrated the MNH situation analysis with the MOH/Niger 2008 plan with Road Map partners in Niger, and prepared to implement it at the district level.
WHO-AFRO and ACCESS developed the capacity of six country teams to develop, implement and evaluate national road maps in Anglophone countries in eastern and southern Africa1 at a regional workshop in Entebbe, Uganda. Representatives from Malawi, the country most advanced in the operationalization of the Road Map, shared
their experience using a systematic approach to assess and analyze the situation as well as design and plan activities. Ugandan participants shared their successful experiences in community MNH and putting in place a functional MNH monitoring and evaluation system. Each team developed a plan for further operationalization of the Road Map in their own country and identified needs for technical assistance.
The regional Road Map workshop in Entebbe highlighted the need to provide countries with clear guidance on how to operationalize the Road Maps, especially at the district level. ACCESS translated the original WHO-AFRO Road Map guidelines from French to English and revised the draft guidelines with WHO-AFRO and partners at a meeting in Addis Ababa. ACCESS, WHO-AFRO and partners also reviewed the framework for the integration of FP, PMTCT, MIP and nutrition with MNH care during the same meeting.
Assisted the MNH team in Zambia to develop a strong and realistic advocacy plan to support the operationalization of the Road Map at the district level by using critical information—which was generated during a REDUCE-ALIVE workshop in Zambia—to promote MNH as one of the government’s priorities. A few donors also committed to support the implementation of the advocacy plan.
1 Country teams were from Malawi, Zambia, Uganda, Kenya, Namibia and Ethiopia.

ACCESS Year Four Annual Report 9
Regional: West Africa Funds Participated in an assessment visit to Ngaoundere District, Cameroon, along with AWARE-
RH partners, with results showing: At the Protestant Hospital of Ngaoundere District, six staff members were formally
trained in EmONC and had used their new skills to educate other colleagues. The labor ward, antenatal clinic and postnatal clinic were all found to be clean and using appropriate IP practices (e.g., disposal of sharps). Moreover, essential care of the newborn was integrated with routine operations (e.g., protocols for newborn care were posted on the wall and underweight twins were in incubator care).
The Nurse Aide Training School integrated some FANC, partograph, AMTSL, IP and orientation to community mobilization techniques with its curriculum.
Cameroon held a dissemination of best practices workshop during which results from both clinical and social mobilization efforts under ACCESS, as well as other activities on developing referral systems and health mutual schemes, were shared, including:
Utilization of ANC services rose from 45% of pregnant women in 2004 to 63% in 2007 in urban areas, and from 29% to 80% in rural areas of Ngaoundere District.2
Facility-based deliveries in Ngaoundere rose from 16% in 2004 to 47% in 2007. The proportion of cesarean sections was nearly zero in 2004 and rose to 1.6% in 2007. A total of 94 providers were trained in EmONC and five were developed as trainers. For
social mobilization, 22 trainers were trained from 18 health zones, who in turn trained 575 community members. Thus, a core group of EmONC and social mobilization trainers was created as a resource for the country.
2 Data source: Presentation by District Health Team/Adamaoua.

10 ACCESS Year Four Annual Report
PREVENTION OF POSTPARTUM HEMORRHAGE Core Funds
USAID’s Global Health Preventing PPH and Postpartum Care e-learning courses were completed by more than 500 users this reporting period, and more than 800 since inception.
Continued as chair of the Prevention of Postpartum Hemorrhage Initiative (POPPHI) technical working group on training, and participated in the technical working groups on uterotonic drugs and devices, and PPH. With ACCESS support, an AMTSL learning resource package is now available through the POPPHI Web site.
Supported nine technical and advocacy meetings on prevention of PPH in Cambodia attended by 62 stakeholders from USAID, UNICEF, UNFPA, WHO, JICA, GTZ, Save the Children, RACHA and RHAC, as well as the Director and Deputy of the National Reproductive Health Program (NRHP), Pursat, Provincial MCH staff, and national NRHP staff.
ACCESS/Cambodia prepared for PPH project implementation. Specifically, ACCESS/Cambodia drafted a BCC package; developed training materials; conducted an assessment of the referral hospital in Pursat to examine its ability to treat referred PPH cases; and completed a detailed implementation plan in collaboration with the NRHP and RACHA3. The PPH project proposal and accompanying materials were submitted for review to the Cambodian Ethical Review Committee.
Continued support and follow up of small grants to seven local organizations in six African countries (Madagascar, Kenya, Ethiopia, Burkina Faso, Mali and Democratic Republic of the Congo), who are continuing their country-level PPH activities to expand training for AMTSL. As of October 2008, ACCESS has trained 236 health care providers and 47 community leaders, and reached more than 100,000 community members with its PPH subgrants.
In Kenya, the MOH reference manual for the prevention and management of PPH was completed with ACCESS support. This guide for service providers will be used nationwide—primarily through the USAID major funding mechanism, APHIA—to update the knowledge and skills of service providers in the prevention of PPH. Twenty TOTs have been developed to assist in the scale-up of PPH prevention efforts nationwide.
Field Funds
Developed HEW safe and clean delivery learning resource package, oriented trainers to the package, and strengthened clinical sites (seven hospitals and 12 health centers) in Ethiopia to ensure adequate resources to support the learning and training activities of health officers and HEWs, who provide services at the health post and community levels, and will provide misoprostol to prevent PPH.
3 The Cambodian Ethical Review Committee did not approve the distribution of misoprostol; therefore, ACCESS will focus on strengthening AMTSL.
Participant practices bimanual compression of the uterus during PPH training in Kano State, Nigeria.
ACCESS Year Four Annual Report 11
ACCESS-supported facility, Malawi.
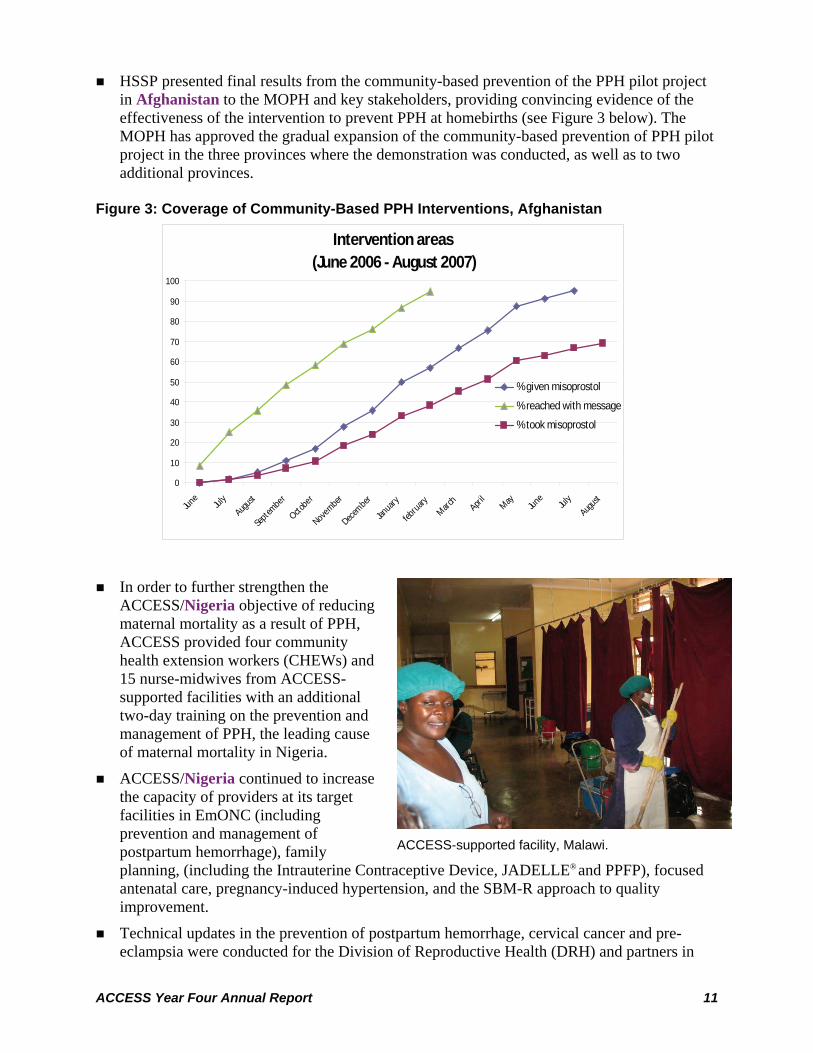
HSSP presented final results from the community-based prevention of the PPH pilot project in Afghanistan to the MOPH and key stakeholders, providing convincing evidence of the effectiveness of the intervention to prevent PPH at homebirths (see Figure 3 below). The MOPH has approved the gradual expansion of the community-based prevention of PPH pilot project in the three provinces where the demonstration was conducted, as well as to two additional provinces.
Figure 3: Coverage of Community-Based PPH Interventions, Afghanistan
Intervention areas (June 2006 - August 2007)
0
10
20
30
40
50
60
70
80
90
100
June
July
August
Septem
ber
Octobe
r
Novem
ber
Decembe
r
Janua
ry
februa
ryMarc
hApri
lMay Jun
eJul
yAugu
st
% given misoprostol
% reached with message
% took misoprostol
In order to further strengthen the ACCESS/Nigeria objective of reducing maternal mortality as a result of PPH, ACCESS provided four community health extension workers (CHEWs) and 15 nurse-midwives from ACCESS-supported facilities with an additional two-day training on the prevention and management of PPH, the leading cause of maternal mortality in Nigeria.
ACCESS/Nigeria continued to increase the capacity of providers at its target facilities in EmONC (including prevention and management of postpartum hemorrhage), family planning, (including the Intrauterine Contraceptive Device, JADELLE® and PPFP), focused antenatal care, pregnancy-induced hypertension, and the SBM-R approach to quality improvement.
Technical updates in the prevention of postpartum hemorrhage, cervical cancer and pre-eclampsia were conducted for the Division of Reproductive Health (DRH) and partners in

12 ACCESS Year Four Annual Report
Kenya to enable them to advocate, formulate, inform and disseminate national policies and guidelines. For example, the DRH managers—using the USAID-funded provincial APHIA programs—have since provided technical assistance to their provincial counterparts.
In Malawi, continued to increase the quality of RH services by supporting the MOH/RHU to apply the SBM-R quality improvement (QI) approach. ACCESS trained 108 members of district-level QI support teams in QI for RH. ACCESS held a national stakeholder’s meeting at which district health management teams and RH focal persons from six participating district hospitals presented findings for their internal QI assessments; baseline results from March 2008 were similar across facilities, with a mean score of 34%. By August 2008, all facilities showed improvements, with a mean score of 71%. Scores for standards related only to normal delivery, including AMTSL, are presented in Figure 4 below.
Figure 4. Results of Normal Labor and Delivery Assessments, Malawi, January–August 2008
10
24
38
2414
19
62
47 48
19
33
60
76
43
76
4352
57
01020304050607080
Machin
ga
Mchinji
Rumphi
Mwanza
Karong
a
Chiradz
ulu
Per
cent
age
(%) Baseline Assessment (Jan
2008)1st Internal Monitoring (April2008)2nd Internal Monitoring (Aug2008)

ACCESS Year Four Annual Report 13
Community meeting, Bangladesh.
NEWBORN CARE Core Funds
Sponsored a one-day consultation meeting with 43 key stakeholders from USAID, UNICEF, SNL, USAID cooperating agencies, researchers and field staff to discuss community-based skin-to-skin care (SSC) for low birth weight newborns. Participants also made recommendations for delivery approaches, such as carrying out SSC in the community as part of a package of essential newborn care interventions (not as a stand-alone intervention), and recommending SSC for all newborns where feasible and acceptable.
Drafted articles on community-based management of neonatal sepsis and Kangaroo Mother Care (KMC) for the MotherNewBorNet newsletter. The first article on community-based management of neonatal sepsis is under final review and will be disseminated in October; the second will be finalized in November 2008.
USAID’s Global Health e-learning courses on Essential Newborn Care and Emergency Obstetric and Newborn Care were completed by more than 800 users this reporting period, and more than 1,100 since inception.
Field-testing in Rwanda, Nepal and Nigeria contributed to the final global facility-based KMC facilitators’ and participants’ manuals.
In Ethiopia, ACCESS adapted KMC training manuals for use, conducted KMC training of trainers for 16 health staff, and introduced KMC services in five hospitals.
In Nepal, ACCESS integrated KMC into postnatal care for low birth weight/premature babies at four hospitals and three primary health centers. Established facility-based KMC services at Mahakali Zonal Hospital and three primary health care centers, and trained 814 female community health volunteers on community KMC.
Based on lessons learned from ACCESS-funded activities in Kanchanpur District, Nepal, ACCESS developed national guidelines for management of LBW infants and KMC, which were endorsed by the MOHP and will be included as part of a community-based integrated neonatal care package to be implemented nationally.
In Rwanda, ACCESS initiated KMC services in seven hospitals, including the University Teaching Hospital in Kigali. Trained 24 service providers in KMC from the eight hospitals.
Field Fund
In Bangladesh, completed a community mobilization scale-up strategy and updated the maternal and newborn health (MNH) and community mobilization (CM) manuals and completed refresher trainings of over 1,160 individuals. The program also developed an MNH orientation manual for village doctors and initiated trainings.3In Bangladesh, CM activities have reached a population of over 500,000 in this reporting period. Of 458 community action groups (CAGs) formed, trained and supported by the project, 403 groups completed action plans to

14 ACCESS Year Four Annual Report
address priority MNH problems. One in every four villages has already established a community-managed emergency transport system. Additionally, one in four has established an emergency finance scheme to assist women and newborns in obtaining timely, appropriate MNH care from difficult-to-reach public service points.
In Bangladesh, developed key training manuals in English and Bangla (for traditional birth attendants and community-based KMC) and held trainings of trainers (TOT): Trainers are training ACCESS counselors to coach mothers to provide KMC to all newborns.
Completed baseline survey data collection and preliminary analysis in Bangladesh and disseminated initial findings to district stakeholders.
Trained counselors in Bangladesh were notified of 38,306 deliveries during the reporting period. They reached 18,999 (50%) of those recent mothers within 24
hours and 25,800 (67%) within 72 hours, and conducted postpartum counseling visits. Among 38,306 women reached postpartum: 48% had a birth plan, 76% newborns were attended by a newborn care person, 96% of newborns had clean cord care, 85% mothers initiated breastfeeding within one hour of birth, 87% of newborns who were delivered at home were dried and wrapped immediately after birth, and 80% of mothers delayed bathing their newborns for three days. (See Figure 5 on the following page for comparisons with last year).
Male community members discussing women’s health, Bangladesh.

ACCESS Year Four Annual Report 15
Figure 5: Practice of Key MNH Behaviors in Sylhet, Bangladesh by Year
31
72
84
7573
5248
76
96
85 87
80
0
25
50
75
100
Birth plan Newborn Care Personat birth
Clean cord cut Breastfeeding within 1hour of birth
Immediate drying &wrapping
Delay bathing for 3days
Indicator
Perc
ent
FY07 FY08
In collaboration with stakeholders, developed Malawi’s national Community Mobilization (CM) Training Manual. The manual targets trainers who train and supervise health surveillance assistants (HSAs), enabling them to train HSAs to empower communities to identify and solve their MNH issues. To date, ACCESS has trained 10 master CM trainers, and 30 district trainers.
Facilitated the integration of targeted community MNH activities into the District Implementation Plans in three ACCESS-focus districts in Malawi (Rumphi, Nkhotakota and Machinga) as part of the national pilot program to mobilize HSAs to provide counseling and referral services to antenatal and postnatal women in the community. Activities included: training of HSAs in the community MNH package; training in monitoring and supervision; organizing drama groups; and mobilizing community-based health care workers to increase access to MNH. Trained HSAs have the knowledge and skills to identify pregnant and postpartum women, provide counseling on MNH care, recognize danger signs, counsel on family planning and refer when appropriate.
Trained HSA, Rumphi, Malawi.

16 ACCESS Year Four Annual Report
PNC role play during a training in Cambodia.
ACCESS/Malawi established KMC as a strategy to decrease neonatal mortality in three focal districts in Malawi. Following a KMC needs assessments in 13 health facilities in the three ACCESS districts, the program facilitated the establishment of KMC units, trained 47 service providers in KMC and ENC, conducted follow-up supervision visits and provided technical assistance to the DHMT to modify and restructure the neonatal ward to include a KMC unit.
In Nigeria, 18,037 mothers and newborns received postpartum/postnatal care within three days at 34 ACCESS-supported hospitals.
To add to the original two facilities offering KMC in Nigeria, ACCESS trained an additional 43 providers in KMC, including obstetricians, pediatricians and nurse-midwives in Kano and Zamfara States to expand the
coverage of facilities offering KMC services.
In Cambodia, ACCESS updated an integrated postnatal care (PNC) package for midwives for the MOH which is being field-tested and developed through a partnership of nine international and local organizations. This activity will result in: an updated national PNC policy, which incorporates key evidenced-based MNH interventions; a substantial group of trained trainers and midwives; extension to community-level workers, a revised supervision and M&E plan; 135 health centers orientated and implementing PNC services according to the new protocols; and a standardized approach to PNC applied by the MOH and all the major NGOs working in this area. In addition, by using this coalition, a jump start on scale-up will have been achieved, with continuing potential for further expansion.
ACCESS contributed to the updating of key RH policy documents in Cambodia, including the community-integrated management of childhood illness (IMCI) curriculum. ACCESS also collaborated with UNICEF and the NRHP on a neonatal situation analysis, helping to formulate recommendations that will serve as the basis for a newborn health action plan for Cambodia.
Afghanistan HSSP provided technical assistance to the MOPH and UNICEF to strengthen clinical training sites for training in obstetric care and care of the newborn. HSSP also launched the first competency-based clinical skills course in Basic Care of the Newborn in Afghanistan and trained 24 National Care of the Newborn trainers, contributing to building the capacity of NGOs implementing the BPHS and improving the quality of service delivery.
Men can practice KMC too (Nigeria).

ACCESS Year Four Annual Report 17
ANTENATAL CARE Core Funds
USAID’s Global Health Antenatal Care and Prevention of Mother-to-Child Transmission of HIV e-learning courses completed by more than 1,500 users this reporting period, and more than 1,800 since inception.
Completed monograph on “Faith-Based Models for Improving Maternal and Newborn Health,” adding to the limited written resources about FBOs and health services.
In Rwanda, expanded the training of providers in FANC from 12 to 24 districts, and held two trainings to update district heads and providers in MIP using the ACCESS-revised LRP consistent with national MIP policies and guidelines. In 25 districts, 58 supervisors and trainers have been trained in FANC and MIP.
Through the FBO Small Grants Program, trained 70 providers in FANC, reached 49 facilities and provided them with supportive supervision to strengthen their ANC service delivery and improve linkages with the community.
Collaborated with the School of Biomedical Engineering at JHU to foster production of innovative products to measure physical effects of PE/E. Analysis of iron-distribution programs also carried out to determine feasibility of antenatal calcium distribution, and literature review resulted in compendium of information and resources for use in advocacy work at global and country levels.
Core Malaria Funds
Completed and published Malaria Action Coalition Final Report (October 2002–September 2007).
Developed two global resources for MIP prevention and control that will directly support countries in efforts to scale up malaria prevention and control: the MIP Implementation Guide and the revised Malaria in Pregnancy Resource Package, both of which are now available online in English and French.
Contributed to the development of a RBM global statement on community distribution of IPTp that will provide guidance to countries in their efforts to scale up MIP prevention and control.
Provided short-term technical assistance in Nigeria to address bottlenecks in implementation of GF activities, which has led to accelerated expansion of GF implementation.
Contributed to the development of the Roll Back Malaria (RBM) Global Malaria Action Plan (GMAP)—the global road map for malaria control and elimination around which all stakeholders can coordinate their actions and achieve the Millennium Development Goals.

18 ACCESS Year Four Annual Report
IMAI training in Kenya includes sessions with expert patient trainers that give the participants realistic case histories and enhance learning.
Field Funds In Rwanda, funds from the President’s Malaria Initiative (PMI) were used to adapt
MIP/FANC manuals for use as training tools for national-level TOT for supervisors.
In Bangladesh, trained counselors conducted 84,014 pregnancy preparedness home visits, counseling pregnant women on healthy MNH behaviors and steps to take to prepare for birth.
ACCESS/Madagascar prepared for dissemination of the summary report of findings of the WHO evaluation, Enquête des Stratégies de Lutte contre le Paludisme Pendant la Grossesse à Madagascar, which identifies the principal barriers to sulfadoxine-pyrimethamine (SP) uptake in the country and makes recommendations to improve IPTp2 coverage nationwide. USAID/Madagascar is reviewing the report before it is disseminated during a half-day stakeholders’ meeting scheduled in November 2008.
A rapid needs assessment sponsored by ACCESS and NMCP in Malawi identified a severe shortage of staff trained on FANC and MIP and shortages of SP and other supplies for IPTp by DOT. In response, ACCESS trained 680 ANC service providers from all 28 districts in FANC/MIP and provided basic supplies for IPTp to all 730 health facilities across the country. Supportive supervision visits to 56 facilities revealed that over 80% had the requisite DOT supplies (i.e., buckets, trays, cups) on site; 11% reported a stock-out in the previous three months; 20% reported having an iron stock-out in the previous three months; and 68% reported having adequate insecticide-treated bead nets (ITNs) for pregnant women.
Supportive supervision visits to the four facilities implementing a pilot program of integrated ANC/tuberculosis screening services in Kenya revealed that screening for tuberculosis was being successfully integrated with ANC services: post-intervention, 91% of 1,069 new ANC clients and 55% of 1,143 ANC revisits were screened for TB.
In Kenya, The rollout of PMTCT-Plus has begun using the integrated management of adult illnesses (IMAI) approach, which was adapted for Kenya with support from ACCESS/Kenya in PY03. Adolescent and pediatric illnesses are included in the Kenya package. Over 200 MCH/ANC/maternity nurses and midwives from 82 high-volume PMTCT sites have been trained to date; of these, 42 sites did not offer ART services before.

ACCESS Year Four Annual Report 19
President Bush at Meru District Hospital: “[PMI] supports treatment for those who are most vulnerable to malaria, especially pregnant women. Here in Tanzania, more than 2,400 health workers have been trained to provide specialized treatment that prevents malaria in expectant mothers.”
In collaboration with the Tanzanian Ministry of Health and Social Welfare (MOHSW), ACCESS continued to scale up clinical training capacity and high-quality service delivery for FANC/MIP/SIP in government and FBO-affiliated health facilities and pre-service education schools:
A total of 760 in-service clinical trainers have been trained since the start of the ACCESS Program in 2004: 679 of the trainers are providers from health facilities in all 21 regions and 81 of the trainers are zonal and regional RCH coordinators from all eight zones. Of these, 319 trainers were trained in this last program year.
This year, ACCESS supported the training of 540 additional providers in FANC/MIP/SIP clinical skills—for a cumulative total of 2,971, for an estimated 49.5% of providers who offer antenatal care in Tanzania. To date, an estimated 32% (1,575) of ANC facilities in the country have been covered.
This year, ACCESS assisted the MOHSW in Tanzania to revise the two-year certificate and three-year diploma nursing and midwifery curricula. To date, ACCESS has integrated FANC/MIP/SIP with the curricula and trained tutors and preceptors at all 51 pre-service nursing and midwifery schools in the country. This year, over 1,600 students graduated from these schools.
At ACCESS’s 30 sentinel facilities in Tanzania, over 33,400 ANC clients were provided services. Of these, 56% received IPT1 and 54% received IPT2, while 64% received TT2 and 77% received ITN vouchers. Positive trends in availability of SP commodities at the sentinel site facilities indicate that SP stock-outs are becoming less of an issue as compared to the beginning of the reporting period. However, 40% of facilities did report at least one SP stock-out.
President Bush visited Tanzania in February 2008 as part of a five-country trip to Africa. Observing the current PMI- and PEPFAR-funded initiatives in action was the focus of his trip. In preparation for this visit, ACCESS developed a press release; identified useful FANC IEC materials for display during official site visits; and provided updated program information to USAID for use in preparation of presidential remarks during his visit. The ACCESS FANC program was highlighted by President Bush during a speech he made at Meru District Hospital.
ACCESS/Tanzania collaborated with T-MARC Company Ltd. to integrate FANC messages with season four of the Mama Ushauri radio serial drama, providing national level exposure to appropriate and correct FANC information through the storylines. ACCESS participated in script development and review to ensure that correct FANC information was incorporated.
Developed and updated several training materials and tools with stakeholders in Tanzania, including the National FANC Advocacy Guides; FANC Learners Guide for Service Providers and Supervisors; Facilitators’ Guide for FANC Trainers; an orientation package for the infection prevention pocket guide; a tool for assessing performance of FANC services at the facility level; and a pre-service quality improvement tool.

20 ACCESS Year Four Annual Report
OTHER ACCESS RESULTS FOR WOMEN’S HEALTH ACCESS supported the National Department of Health (NDOH) in South Africa to
introduce the new national PMTCT guidelines in three provinces. A total of 1,133 health workers (service providers, trainers and M&E coordinators) have been oriented to the new guidelines, which now include implementation of dual therapy (AZT and Nevirapine), replacing the single-dose Nevirapine regimen in the country.
ACCESS/Haiti supported the MOH to improve the quality of PMTCT and FP services at six facilities through facilitative supervision and coaching, which included feedback to service providers to improve their competencies in FP and PMTCT service provision.
ACCESS-FP Funds
Began new field-funded programs in Albania, India and Guinea.
Developed a second e-learning course for USAID's Global Health Learning Center to orient the learner to the rationale and importance of FP during the postpartum period, and to introduce the learner to service delivery, contraceptive method and programmatic considerations unique to FP during the postpartum period.
Revitalized the lactational amenorrhea method (LAM) through the LAM Working Group with the Institute of Reproductive Health at Georgetown University.
Hosted a meeting, “Postpartum Family Planning (PPFP): A review of programmatic approaches through the first year postpartum,” to systematically exchange experiences and lessons learned on PPFP programming; to share pre-tested tools to support PPFP programming and avoid duplication; and to prioritize programmatic topics for research and learning.
Increased PPFP community of practice to include more than 500 members from 66 countries, and served as a key information sharing mechanism for global discussions on topics related to PPFP such as healthy timing and spacing of pregnancy, key messages for PPFP, and PPFP contraceptive technology.
Published the Tanzania DHS secondary analysis of PP data, Uttar Pradesh, India secondary analysis of PP data, LAM technical brief, community-based PPFP and updated programmatic framework.
Promoted PPFP global forums such as the Scaling Up Best Practices Meeting in Bangkok, Thailand; Women Deliver conference in London; Union for African Population Studies Fifth African Population Conference in Arusha, Tanzania; Flexible Fund Meeting; and the Mini-University.
Carried out a postpartum care survey among USAID-supported cooperating agencies and partners to identify, document and share information on the status of postpartum care services they implement and support.
The FRONTIERS Program completed an evaluation of a successful PPFP pilot program implemented by ACCESS-FP in Kenya; final study report is available through the ACCESS Web site.
ACCESS Year Four Annual Report 21
Core FP/RH Funds Translated the postabortion care learning resource package into French and field-tested the
package during a training of 11 providers in Haiti.
Collated feedback from field-tests in Bolivia and Haiti for incorporation into final draft of curriculum; expected date of completion is 30 October 2008.
Field Funds
With HSSP technical support and coordination, Afghanistan’s MOPH finalized and endorsed its first ever comprehensive National Health Communication Strategy for 2008–2010. This document creates a common framework for coordination among all agencies implementing and supporting communication activities in the country. An operational plan will now be developed.
In Kenya, assisted with the development of new policy guidelines on reproductive tract cancer, which include breast and prostate cancers, and HIV testing and counseling. ACCESS also supported the dissemination of the National Standards and Guidelines on Injection Safety and Medical Waste Management to 12 selected hospitals in two provinces. This process also built the capacity of the district trainers who participated in the dissemination.
ACCESS/Kenya initiated community-level training in infection prevention by supporting the orientation of CHEWs and CHWs in 12 communities thus promoting behaviors such as handwashing to minimize infections in the community and reduce visits to the hospitals.
Service delivery data collected in December 2007 from the eight provincial general hospitals where ACCESS/Kenya implemented provider-initiated testing and counseling (PITC) services last year showed that over 100,000 clients were provided with PITC services since completing the training in mid-2007. This year, ACCESS trained 594 service providers in 37 district hospitals across the country in PITC.
Preliminary results of an evaluation of ACCESS/Kenya’s HIV PITC services last year revealed: 1) ACCESS trained 73% of all 402 service providers providing services at provincial general hospitals; 2) number of clients offered HIV counseling increased from 2,861 to 4,662 after initiation of the program; 3) percentage of clients accepting HIV testing increased from 95% to 99%; and 4) 95% of clients offered HIV testing and counseling were satisfied with the service.
In Kenya, worked with the government agency NASCOP and led the ART Technical Working Group’s effort to standardize the multiple clinical mentorship models being used in the country into one unified, nationally accepted model. Through a slow, careful process of consensus building the model was created and the National Mentorship Guidelines and an orientation package were developed.
ACCESS moved toward integration of FP and STI services with HIV/AIDS services in Kenya with the development of two orientation packages—an FP orientation package and a STI orientation package—for service providers working in comprehensive HIV care centers. Both orientation packages were adopted by the NASCOP and other partners. Thirty national trainers were also developed to facilitate the integration of FP and STI services at comprehensive care centers throughout the country.

22 ACCESS Year Four Annual Report
In Nigeria, 11,817 clients received FP counseling and 933 clients received PPFP counseling at 36 ACCESS-supported facilities. ACCESS staff helped to ensure that FP commodities were always available at the facilities.
Five facilities supported by ACCESS/South Africa and the Foundation of Professional Development demonstrated improved performance and quality of ART services using the SBM-R approach to quality improvement. Three facilities assessed during this period improved from a mean score of 37% to 52% out of 165 total standards.
Thirteen new Training Information Management Systems© (TIMS) sites have been established in South Africa during this period: 12 in the KwaZulu-Natal Department of Health and one at the Department of Public Service and Administration. These sites, added to the existing seven sites established in previous years, make a total 20 sites that are monitoring provider training, using the data for reporting, planning and decision making. Furthermore, the Free State Province Department of Health has created an overall strategy to improve monitoring and evaluation with ACCESS assistance, including review of indicators used.
A total of 129 health care providers and program coordinators were trained as trainers on the clinical guidelines for palliative care for adults in South Africa. Participants came from all nine provinces of South Africa and are now cascading the training in their own provinces.
ACCESS/South Africa continued to support two senior technical advisors at the National Department of Health, a service delivery/accreditation expert and a PLWHA coordinator. This support resulted in increased capacity and better collaboration and integration of different HIV/AIDS programs, as well as improvement in the implementation and adherence to the operational plans.
The technical advisor for HIV/AIDS service delivery helped increase capacity to accredit facilities nationally by providing support for accreditation to the provinces and the NDOH Comprehensive Care Management and Treatment (CCMT) Unit to revise policy guidelines, including Step-Down Care Guidelines, PMTCT Guidelines, Adult and Pediatric HAART Guidelines, and Home- and Community-Based Care Guidelines. He assisted the NDOH Human Resource Unit to develop training plans, and helped the TB/HIV cluster with the financial planning of HAART guidelines roll out. He further assisted provinces with conditional grants and CCMT plans.
The PLWHA coordinator helped finalize stigma mitigation indicators, PLHIV synergy strategy/audit, a national database for paralegals; and a support group database. She submitted the Workbook on HIV and AIDS Human Rights for approval and helped develop the Greater Involvement of People with AIDS Implementation Framework and an advocacy toolkit for people living with HIV/AIDS.
Cervical cancer prevention services were established at 12 facilities in the northwest province of South Africa, each of which has a nurse trained in Visual Inspection of the cervix with Acetic Acid (VIA) wash and cryotherapy. To date a total 547 clients have been screened using VIA: 505 women had normal results, 29 had pre-cancerous lesions and were treated with cryotherapy, and 13 women were referred for suspect cancer and other gynecological problems. As a result of this intervention, the National Department of Health is reviewing the National Cervical Cancer Screening Guidelines—which currently focus on Pap smears as the screening modality—to include VIA.

ACCESS Year Four Annual Report 23
Increased access to long-term family planning methods (e.g., IUD, Norplant implants and vasectomy) at two facilities in southern Haiti through “mobile clinics” conducted by two visiting providers.
ACCESS/Haiti purchased and distributed $35,000 worth of equipment and supplies for LAPM/FP to be used in the bilateral project in public institutions.
Preliminary Work on Pre-eclampsia/Eclampsia
Continued worldwide advocacy for prevention and treatment of PE/E, including presentations to groups comprised of USAID and other partners, professional associations and technical working groups in Afghanistan, Bangladesh, Ethiopia, India, Kenya, Nepal, Tanzania and Zambia, and at several global conferences. Also participated in a WHO-sponsored consultation on the state-of-the-art treatments in PE/E in low-resource countries held in Oxford, England.
Provided technical assistance in Nepal to the USAID bilateral and MOH to introduce calcium into ANC and test its acceptability and effect on community-level prevention of eclampsia.
During this reporting period in Nigeria, 1,284 women with eclampsia received treatment according to protocol at 17 hospitals.
Technical updates in the prevention of postpartum hemorrhage, cervical cancer and pre-eclampsia were conducted for the Division of Reproductive Health (DRH) and partners in Kenya to enable them to advocate, formulate, inform and disseminate national policies and guidelines.
Met with USAID and partners in Tanzania to outline need for strategy at community and facility levels for prevention and treatment of PE/E; the USAID mission included this as part of proposed funding for BEmONC throughout the country.
24 ACCESS Year Four Annual Report
Challenges and Opportunities Challenges
Planning for final year in the face of uncertainties: ACCESS currently ends on 26 July 2009. In its last year, ACCESS has received funding and requests to complete activities for ongoing programs in more than eight countries. Staff recognized early in the year that country programs would need a full year of implementation to match the objectives and expectations of the USAID missions and host country governments. Through extended dialogue with the ACCESS CTO, we submitted a letter requesting an extension of the Program through March 2010. This extension has not yet been approved; therefore, ACCESS work planning is currently in flux. In addition, planning for the possibility of losing key staff to the MCHIP Program has created some uncertainties in planning and travel schedules for Program Year Five. We anticipate knowing this information well in advance of Year Five start-up, and will readjust the work plan and level of effort of multiple key staff accordingly.
Delays in implementation of field programs: Several issues have delayed some elements of field implementation. In Afghanistan, a deteriorating security situation prevents travel to program sites; in Kenya, political violence; and in South Africa, the sudden passing of Lunah Ncube, Jhpiego’s Country Director, has created unexpected challenges for program implementation. In addition, Tanzania, Kenya, Ethiopia and South Africa reported delays due to staff attrition and turnover. In many instances, in-country staff who were trained through ACCESS have moved to other districts or other companies and are no longer available as a resource for the Program.
Collaboration with partners on tools and materials: ACCESS is working with other partners to develop or update documents that are of global significance by working in conjunction with several multilateral partners such as WHO and other collaborating agencies. Development of one of these documents—the Managing Complications in Pregnancy and Childbirth (MCPC) Manual—has been delayed because the Department at WHO has limited staff who must balance competing priorities, although they remain committed to this project.
Closing out programs while scaling up others: As ACCESS completes its fourth year, some country programs have closed out. These include Haiti, West Africa Regional Program and Nepal. In Nepal, ACCESS received field support funding for a new set of activities. However, to manage close-out efficiently in Nepal, ACCESS had already cut back staff and minimized program activities. Other countries, like Tanzania, are allocating funds that were discussed last year. As we enter into our final year, ACCESS will carefully plan close out for other countries to ensure a smooth transition.
ACCESS Year Four Annual Report 25
Opportunities Opportunity for advocacy for maternal health in Rwanda: ACCESS has a new Country
Director in Rwanda, Jérémie Zoungrana, who is also a Board Member of the White Ribbon Alliance (WRA). This could be an opportunity to launch the WRA and could be an effective vehicle for advocacy to create political will for drastic changes that will give girls and women access to life-saving care.
Potential for scale up in India: The Government of Jharkhand in India has expressed strong interest in scaling up the ACCESS training approach for Jharkhand. In addition, the Indian Nurses Council is interested in using the learning resource package for the training course, approach and results, which has contributed to discussions about scaling up this project. Similarly, in Rwanda, strong interest in KMC by the government and stakeholders has paved the way to scale up the intervention beyond the original hospital.
Documenting “what works”: As the ACCESS Program ends, we have the opportunity to document what works in several strategic areas and to publish the results. In several ACCESS countries we conducted a baseline and an endline survey, which can generate evidence for these papers.
Integrating MNH and PMTCT: In Malawi, ACCESS has begun to work on an integrated program for MNH and PMTCT in two districts. Demonstrating an increasing trend in the coverage for PMTCT interventions, including infants on ARV, can be powerful evidence for the HIV community to recognize the potential of the MNH platform.

26
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
Ann
ex A
: Cor
e A
ctiv
ity M
atrix
Ta
ble
1: A
CC
ES
S C
ore-
Fund
ed A
ctiv
ities
and
Out
puts
for P
rogr
am Y
ear T
hree
(FY
08) f
rom
Oct
ober
1, 2
007–
Sep
tem
ber 3
0, 2
008
CO
RE
AC
TIVI
TY
MA
JOR
PR
OG
RA
MM
ATI
C O
UTP
UTS
/DEL
IVER
AB
LES
PRO
DU
CED
IR 1
: Glo
bal l
eade
rshi
p fo
r mat
erna
l, ne
onat
al a
nd w
omen
’s h
ealth
AN
D n
utrit
ion
prog
ram
s A
ND
pol
icie
s st
reng
then
ed
1.1
Thro
ugh
glob
al
partn
ersh
ips
prom
ote
way
s an
d m
eans
of
over
com
ing
polic
y an
d pr
ogra
m
barr
iers
to e
nsur
e m
ater
nal,
neon
atal
an
d w
omen
’s
heal
th g
oals
and
in
corp
orat
ion
of
evid
ence
-bas
ed
stra
tegi
es in
co
untry
C
ontin
ued
to s
uppo
rt th
e Pa
rtner
ship
for M
ater
nal,
New
born
, and
Chi
ld H
ealth
(PM
NC
H) t
hrou
gh J
anua
ry 2
008
with
a
tech
nica
l adv
isor
who
is a
ssis
ting
with
the
impl
emen
tatio
n of
thei
r glo
bal a
ctiv
ities
.
C
ontin
ued
as c
hair
of th
e P
reve
ntio
n of
Pos
tpar
tum
Hem
orrh
age
Initi
ativ
e (P
OP
PH
I) te
chni
cal w
orki
ng g
roup
on
train
ing,
an
d pa
rtici
pate
d in
the
tech
nica
l wor
king
gro
ups
on u
tero
toni
c dr
ugs
and
devi
ces,
and
PP
H. W
ith A
CC
ES
S s
uppo
rt, a
n A
MTS
L LR
P is
now
ava
ilabl
e th
roug
h th
e P
OP
PH
I Web
site
.
D
rafte
d ar
ticle
s on
com
mun
ity-b
ased
man
agem
ent o
f neo
nata
l sep
sis
(dis
sem
inat
ion:
Oct
ober
200
8) a
nd K
MC
(fin
aliz
ed:
Nov
embe
r 200
8) fo
r the
Mot
herN
ewB
orN
et n
ewsl
ette
r.
S
pons
ored
a o
ne-d
ay c
onsu
ltatio
n m
eetin
g in
May
200
8 w
ith S
avin
g N
ewbo
rn L
ives
and
US
AID
to d
iscu
ss s
tate
-of-t
he-a
rt co
mm
unity
-bas
ed s
kin-
to-s
kin
care
(SSC
) for
low
birt
h w
eigh
t new
born
s an
d id
entif
y re
com
men
datio
ns fo
r del
iver
y ap
proa
ches
, inc
ludi
ng th
at S
SC
in th
e co
mm
unity
sho
uld
be c
arrie
d ou
t as
part
of a
pac
kage
of e
ssen
tial n
ewbo
rn c
are
inte
rven
tions
(not
as
a st
and-
alon
e in
terv
entio
n), a
nd s
houl
d be
reco
mm
ende
d fo
r all
new
born
s w
here
feas
ible
and
ac
cept
able
.
Fi
eld-
test
ed a
nd fi
naliz
ed g
loba
l fac
ility-
base
d KM
C fa
cilit
ator
s’ a
nd p
artic
ipan
ts’ m
anua
ls (p
rintin
g: D
ecem
ber 2
008)
.
Te
chni
cal m
eetin
g of
Man
agin
g C
ompl
icat
ions
in P
regn
ancy
and
Chi
ldbi
rth (M
CP
C) M
anua
l Rev
isio
n Ta
sk F
orce
took
pl
ace
in G
enev
a on
22–
23 O
ctob
er 2
007,
atte
nded
by
AC
CE
SS
/Jhp
iego
and
WH
O M
akin
g P
regn
ancy
Saf
er (M
PS
) D
epar
tmen
t rep
rese
ntat
ives
. AC
CE
SS
/Jhp
iego
are
now
re-w
ritin
g as
sign
ed te
chni
cal s
ectio
ns a
nd c
omm
unic
atio
n w
ith th
e M
akin
g P
regn
ancy
Saf
er D
epar
tmen
t of W
HO
has
bee
n on
-goi
ng to
det
erm
ine
a re
vise
d tim
elin
e gi
ven
the
pres
ent d
elay
.
C
olla
bora
ted
with
glo
bal s
take
hold
ers
to s
uppo
rt th
e in
tern
atio
nal W
omen
Del
iver
con
fere
nce
in L
ondo
n, 1
8–20
Oct
ober
20
07, i
nclu
ding
sup
port
to m
ore
than
20
parti
cipa
nts
and
pane
lists
. AC
CE
SS
and
AC
CE
SS
-FP
faci
litat
ed s
ever
al p
anel
di
scus
sion
s on
PP
H, S
BA
, pos
tpar
tum
fam
ily p
lann
ing,
FB
Os
and
mal
aria
in p
regn
ancy
(MIP
). W
RA
repr
esen
tativ
es
pres
ente
d pa
nel d
iscu
ssio
ns a
nd p
rovi
ded
coun
try e
xam
ples
; tw
o re
pres
enta
tives
from
faith
-bas
ed h
ealth
net
wor
ks in
A
frica
pre
sent
ed p
aper
s, ra
isin
g aw
aren
ess
of th
e ro
le o
f FB
Os
in p
rovi
ding
hea
lth c
are
serv
ices
.
W
RA
: 1) S
uppo
rted
leve
rage
d by
two
Allia
nces
(Mal
awi a
nd Z
ambi
a) fo
r add
ition
al fu
ndin
g fro
m D
FID
to s
uppo
rt ro
ll-ou
t of
stra
tegi
es; 2
) dev
elop
ed o
r ref
ined
cou
ntry
-spe
cific
M&E
tool
s to
cap
ture
pro
gres
s to
war
d H
IDN
pat
hway
s; a
nd 3
) pro
vide
d te
chni
cal a
ssis
tanc
e (th
roug
h G
eorg
e W
ashi
ngto
n U
nive
rsity
Cap
ston
e P
rogr
am) t
o co
nduc
t a tr
aini
ng o
n da
ta c
olle
ctio
n an
d M
&E
and
car
ry o
ut fo
cus
grou
p di
scus
sion
s an
d ke
y in
form
ant i
nter
view
s in
five
targ
et fa
cilit
ies
in T
anza
nia.

27
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
RE
AC
TIVI
TY
MA
JOR
PR
OG
RA
MM
ATI
C O
UTP
UTS
/DEL
IVER
AB
LES
PRO
DU
CED
1.2
Par
tner
with
faith
-ba
sed
heal
th c
are
netw
orks
to
expa
nd e
mer
genc
y m
ater
nal a
nd
new
born
car
e in
terv
entio
ns
O
rgan
ized
a p
anel
on
impr
ovin
g m
ater
nal a
nd n
ewbo
rn c
are
thro
ugh
faith
-bas
ed o
rgan
izat
ions
at W
omen
Del
iver
co
nfer
ence
and
ena
bled
two
repr
esen
tativ
es fr
om fa
ith-b
ased
hea
lth n
etw
orks
in A
frica
to p
artic
ipat
e an
d pr
esen
t pap
ers
at th
e W
omen
Del
iver
con
fere
nce,
rais
ing
awar
enes
s of
the
role
FBO
s pl
ay in
pro
vidi
ng h
ealth
car
e se
rvic
es to
wom
en a
nd
child
ren.
D
evel
oped
tool
kits
for r
elig
ious
lead
ers—
one
for C
hris
tian
lead
ers
and
one
for I
slam
ic le
ader
s—to
hel
p bu
ild th
eir c
apac
ity
for p
rom
otin
g sa
fe m
othe
rhoo
d in
thei
r com
mun
ities
and
with
in th
eir c
onst
ituen
cies
. Dra
fts a
re in
fina
l rev
iew
.
P
rese
nted
on
“Rol
e of
Fai
th-B
ased
Org
aniz
atio
ns in
Impr
ovin
g M
ater
nal a
nd N
ewbo
rn H
ealth
” at U
NFP
A O
ffice
s to
the
staf
f in
the
UN
sys
tem
, as
wel
l as
at th
e A
sia
Foru
m fo
r Chr
istia
n Le
ader
s.
C
ompl
eted
FBO
brie
f on
heal
th n
etw
orks
and
com
mun
ity h
ealth
pro
gram
s fo
cuse
d on
beh
avio
r cha
nge.
C
ompl
eted
mon
ogra
ph o
n “F
aith
-Bas
ed M
odel
s fo
r Im
prov
ing
Mat
erna
l and
New
born
Hea
lth,”
addi
ng to
the
limite
d w
ritte
n re
sour
ces
abou
t FB
Os
and
heal
th s
ervi
ces.
D
isse
min
ated
AC
CE
SS
reso
urce
s to
17
faith
-bas
ed h
ealth
net
wor
ks in
Afri
ca a
nd A
sia.
Th
roug
h th
e FB
O S
mal
l Gra
nts
Prog
ram
, tra
ined
70
prov
ider
s in
FA
NC
, rea
ched
49
faci
litie
s an
d pr
ovid
ed th
em w
ith
supp
ortiv
e su
perv
isio
n to
stre
ngth
en th
eir A
NC
ser
vice
del
iver
y an
d im
prov
e lin
kage
s w
ith th
e co
mm
unity
.
1.3
Dis
sem
inat
e A
CC
ES
S P
rogr
am
mat
eria
ls a
nd
reso
urce
s to
st
akeh
olde
rs
wor
ldw
ide
to
adva
nce
know
ledg
e of
pr
ogra
mm
ing
in
mat
erna
l and
ne
wbo
rn h
ealth
9,
000
AC
CES
S m
ater
ials
dis
sem
inat
ed: W
omen
Del
iver
con
fere
nce;
PR
IDE
Pro
ject
(Pak
ista
n); n
atio
nal R
H/C
H m
eetin
g (M
ozam
biqu
e; s
uppo
rted
by J
hpie
go’s
For
te S
aude
pro
ject
); A
PH
A; I
CM
Wor
ld c
onfe
renc
e.
M
ater
ials
com
plet
ed: T
hree
e-le
arni
ng c
ours
e te
chni
cal b
riefs
(on
PP
H, P
MTC
T an
d P
PC
); se
cond
FP
e-le
arni
ng c
ours
e;
FBO
hea
lth n
etw
orks
brie
f and
mon
ogra
ph o
n FB
O M
odel
s fo
r Im
prov
ing
MN
H; M
AC
fina
l rep
ort a
nd re
vise
d M
alar
ia
Res
ourc
e P
acka
ge; f
our A
CC
ES
S P
rogr
am re
sults
brie
fs; a
nd fo
ur A
CC
ES
S c
ount
ry b
riefs
(Nig
eria
, Ken
ya, B
angl
ades
h an
d A
fgha
nist
an).
Tr
aini
ng p
acka
ge a
nd im
plem
ente
r’s g
uide
on
com
mun
ity-b
ased
use
of m
isop
rost
ol a
re in
the
final
sta
ges
of e
ditin
g an
d pr
oduc
tion.
M
ore
than
3,1
00 p
eopl
e co
mpl
eted
the
seve
n e-
lear
ning
cou
rses
on
AN
C, P
ostp
artu
m C
are,
EN
C, P
MTC
T, M
ater
nal
Dis
abilit
y an
d P
reve
ntin
g P
PH
dev
elop
ed b
y A
CC
ES
S th
is y
ear.
A n
ew e
-lear
ning
cou
rse,
AC
CE
SS
-FP
: Pos
tpar
tum
Fa
mily
Pla
nnin
g e-
lear
ning
cou
rse
will
be a
vaila
ble
soon
.
A
CC
ES
S W
eb s
ite: 1
0,00
0 ne
w v
isito
rs a
nd n
early
250
dow
nloa
ds o
f maj
or p
ublic
atio
ns in
this
repo
rting
per
iod.
In A
pril,
th
e fir
st (o
f fou
r) “A
CC
ES
S U
pdat
e” w
as s
ent v
ia e
mai
l to
AC
CE
SS
sta
ff an
d m
ore
than
150
col
leag
ues
at U
SA
ID
Mis
sion
s, c
olla
bora
ting
orga
niza
tions
, and
HID
N a
nd A
CC
ES
S-F
P o
ffice
s.
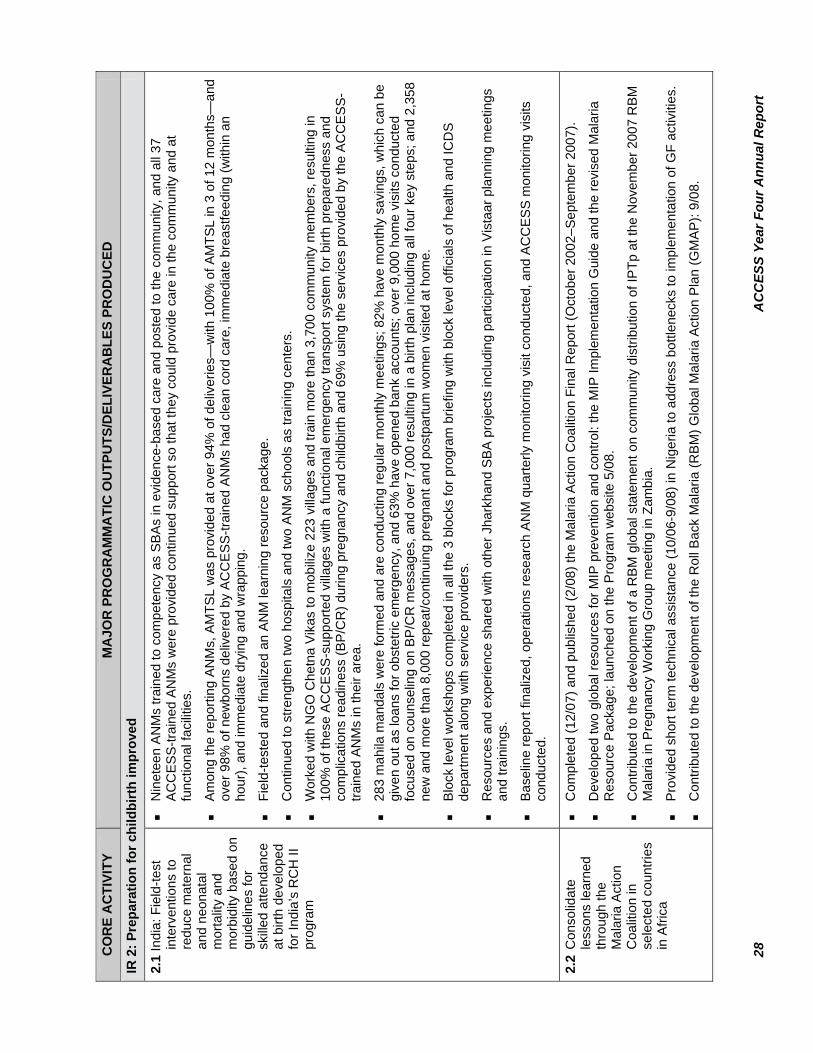
28
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
RE
AC
TIVI
TY
MA
JOR
PR
OG
RA
MM
ATI
C O
UTP
UTS
/DEL
IVER
AB
LES
PRO
DU
CED
IR 2
: Pre
para
tion
for c
hild
birt
h im
prov
ed
2.1
Indi
a: F
ield
-test
in
terv
entio
ns to
re
duce
mat
erna
l an
d ne
onat
al
mor
talit
y an
d m
orbi
dity
bas
ed o
n gu
idel
ines
for
skille
d at
tend
ance
at
birt
h de
velo
ped
for I
ndia
’s R
CH
II
prog
ram
N
inet
een
AN
Ms
train
ed to
com
pete
ncy
as S
BA
s in
evi
denc
e-ba
sed
care
and
pos
ted
to th
e co
mm
unity
, and
all
37
AC
CE
SS
-trai
ned
AN
Ms
wer
e pr
ovid
ed c
ontin
ued
supp
ort s
o th
at th
ey c
ould
pro
vide
car
e in
the
com
mun
ity a
nd a
t fu
nctio
nal f
acilit
ies.
A
mon
g th
e re
porti
ng A
NM
s, A
MTS
L w
as p
rovi
ded
at o
ver 9
4% o
f del
iver
ies—
with
100
% o
f AM
TSL
in 3
of 1
2 m
onth
s—an
d ov
er 9
8% o
f new
born
s de
liver
ed b
y A
CC
ES
S-tr
aine
d A
NM
s ha
d cl
ean
cord
car
e, im
med
iate
bre
astfe
edin
g (w
ithin
an
hour
), an
d im
med
iate
dry
ing
and
wra
ppin
g.
Fi
eld-
test
ed a
nd fi
naliz
ed a
n A
NM
lear
ning
reso
urce
pac
kage
.
C
ontin
ued
to s
treng
then
two
hosp
itals
and
two
AN
M s
choo
ls a
s tra
inin
g ce
nter
s.
W
orke
d w
ith N
GO
Che
tna
Vik
as to
mob
ilize
223
villa
ges
and
train
mor
e th
an 3
,700
com
mun
ity m
embe
rs, r
esul
ting
in
100%
of t
hese
AC
CE
SS
-sup
porte
d vi
llage
s w
ith a
func
tiona
l em
erge
ncy
trans
port
syst
em fo
r birt
h pr
epar
edne
ss a
nd
com
plic
atio
ns re
adin
ess
(BP
/CR
) dur
ing
preg
nanc
y an
d ch
ildbi
rth a
nd 6
9% u
sing
the
serv
ices
pro
vide
d by
the
AC
CE
SS
-tra
ined
AN
Ms
in th
eir a
rea.
28
3 m
ahila
man
dals
wer
e fo
rmed
and
are
con
duct
ing
regu
lar m
onth
ly m
eetin
gs; 8
2% h
ave
mon
thly
sav
ings
, whi
ch c
an b
e gi
ven
out a
s lo
ans
for o
bste
tric
emer
genc
y, a
nd 6
3% h
ave
open
ed b
ank
acco
unts
; ove
r 9,0
00 h
ome
visi
ts c
ondu
cted
fo
cuse
d on
cou
nsel
ing
on B
P/C
R m
essa
ges,
and
ove
r 7,0
00 re
sulti
ng in
a b
irth
plan
incl
udin
g al
l fou
r key
ste
ps; a
nd 2
,358
ne
w a
nd m
ore
than
8,0
00 re
peat
/con
tinui
ng p
regn
ant a
nd p
ostp
artu
m w
omen
vis
ited
at h
ome.
B
lock
leve
l wor
ksho
ps c
ompl
eted
in a
ll th
e 3
bloc
ks fo
r pro
gram
brie
fing
with
blo
ck le
vel o
ffici
als
of h
ealth
and
ICD
S
depa
rtmen
t alo
ng w
ith s
ervi
ce p
rovi
ders
.
R
esou
rces
and
exp
erie
nce
shar
ed w
ith o
ther
Jha
rkha
nd S
BA
pro
ject
s in
clud
ing
parti
cipa
tion
in V
ista
ar p
lann
ing
mee
tings
an
d tra
inin
gs.
B
asel
ine
repo
rt fin
aliz
ed, o
pera
tions
rese
arch
AN
M q
uarte
rly m
onito
ring
visi
t con
duct
ed, a
nd A
CC
ES
S m
onito
ring
visi
ts
cond
ucte
d.
2.2
Con
solid
ate
less
ons
lear
ned
thro
ugh
the
Mal
aria
Act
ion
Coa
litio
n in
se
lect
ed c
ount
ries
in A
frica
C
ompl
eted
(12/
07) a
nd p
ublis
hed
(2/0
8) th
e M
alar
ia A
ctio
n C
oalit
ion
Fina
l Rep
ort (
Oct
ober
200
2–S
epte
mbe
r 200
7).
D
evel
oped
two
glob
al re
sour
ces
for M
IP p
reve
ntio
n an
d co
ntro
l: th
e M
IP Im
plem
enta
tion
Gui
de a
nd th
e re
vise
d M
alar
ia
Res
ourc
e P
acka
ge; l
aunc
hed
on th
e P
rogr
am w
ebsi
te 5
/08.
C
ontri
bute
d to
the
deve
lopm
ent o
f a R
BM
glo
bal s
tate
men
t on
com
mun
ity d
istri
butio
n of
IPTp
at t
he N
ovem
ber 2
007
RB
M
Mal
aria
in P
regn
ancy
Wor
king
Gro
up m
eetin
g in
Zam
bia.
P
rovi
ded
shor
t ter
m te
chni
cal a
ssis
tanc
e (1
0/06
-9/0
8) in
Nig
eria
to a
ddre
ss b
ottle
neck
s to
impl
emen
tatio
n of
GF
activ
ities
.
C
ontri
bute
d to
the
deve
lopm
ent o
f the
Rol
l Bac
k M
alar
ia (R
BM
) Glo
bal M
alar
ia A
ctio
n P
lan
(GM
AP
): 9/
08.

29
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
RE
AC
TIVI
TY
MA
JOR
PR
OG
RA
MM
ATI
C O
UTP
UTS
/DEL
IVER
AB
LES
PRO
DU
CED
IR 3
: Saf
e de
liver
y, p
ostp
artu
m c
are
and
new
born
hea
lth
3.1
Con
tribu
te to
the
know
ledg
e an
d ex
pans
ion
of
prev
entio
n of
PP
H
in A
CC
ES
S
coun
tries
Cam
bodi
a
Sup
porte
d 9
tech
nica
l and
adv
ocac
y m
eetin
gs o
n pr
even
tion
of P
PH
in C
ambo
dia
atte
nded
by
62 s
take
hold
ers
repr
esen
ting
US
AID
, UN
ICEF
, UN
FPA
, WH
O, J
ICA
, GTZ
, Sav
e th
e C
hild
ren,
RA
CH
A a
nd R
HA
C, a
s w
ell a
s th
e D
irect
or
and
Dep
uty
Dire
ctor
of t
he N
RH
P, P
ursa
t Pro
vinc
ial M
CH
sta
ff, a
nd n
atio
nal N
RH
P s
taff.
P
repa
red
for P
PH
pro
ject
impl
emen
tatio
n: d
rafte
d a
BC
C p
acka
ge; d
evel
oped
trai
ning
mat
eria
ls; c
ondu
cted
an
asse
ssm
ent o
f the
refe
rral
hos
pita
l in
Purs
at to
exa
min
e its
abi
lity
to tr
eat r
efer
red
PP
H c
ases
; and
com
plet
ed a
det
aile
d im
plem
enta
tion
plan
in c
olla
bora
tion
with
the
NR
HP
and
RAC
HA
. The
PP
H p
roje
ct p
ropo
sal a
nd a
ccom
pany
ing
mat
eria
ls
wer
e su
bmitt
ed fo
r rev
iew
to th
e C
ambo
dian
Eth
ical
Rev
iew
Com
mitt
ee.
Ken
ya
C
ompl
eted
MO
H re
fere
nce
man
ual f
or th
e pr
even
tion
and
man
agem
ent o
f PP
H.
Tw
enty
TO
Ts h
ave
been
dev
elop
ed a
nd p
rovi
ded
supp
ortiv
e su
perv
isio
n to
ass
ist i
n th
e sc
ale-
up o
f PP
H p
reve
ntio
n ef
forts
nat
ionw
ide.
PPH
Sm
all G
rant
s
As
of O
ctob
er 2
008,
AC
CES
S h
as tr
aine
d 23
6 he
alth
car
e pr
ovid
ers
and
47 c
omm
unity
lead
ers,
and
reac
hed
mor
e th
an
100,
000
com
mun
ity m
embe
rs w
ith it
s P
PH
sub
gran
ts.
3.2
Build
stra
tegi
c op
portu
nitie
s to
im
prov
e sa
fe
deliv
ery
in A
frica
Rw
anda
Expa
nded
bey
ond
the
initi
al 4
dis
trict
s an
d, w
ith o
ther
impl
emen
ting
partn
ers,
ass
iste
d th
e M
inis
try o
f Hea
lth (M
OH
) to
desi
gn
a pl
an fo
r nat
iona
l-lev
el s
cale
-up
of M
NH
. In
a co
llabo
rativ
e ef
fort,
a n
ew g
roup
of n
atio
nal-l
evel
trai
ners
was
trai
ned.
H
elpe
d to
est
ablis
h a
KM
C C
ente
r of E
xcel
lenc
e at
Muh
ima
Dis
trict
Hos
pita
l. In
itiat
ed K
MC
ser
vice
s in
8 h
ospi
tals
, in
clud
ing
the
univ
ersi
ty te
achi
ng h
ospi
tal i
n K
igal
i. Tr
aine
d 24
ser
vice
pro
vide
rs in
KM
C fr
om th
e 8
hosp
itals
.
E
xpan
ded
the
train
ing
of p
rovi
ders
in F
ANC
from
12
to 2
4 di
stric
ts, a
nd h
eld
two
train
ings
to u
pdat
e di
stric
t hea
ds a
nd
prov
ider
s in
MIP
usi
ng th
e A
CC
ES
S-re
vise
d LR
P c
onsi
sten
t with
nat
iona
l MIP
pol
icie
s an
d gu
idel
ines
. In
25 d
istri
cts,
58
supe
rvis
ors
and
train
ers
have
bee
n tra
ined
in F
AN
C/M
IP.
In
trodu
ced
SBM
-R in
5 d
istri
ct h
ospi
tals
.
N
ine
hosp
itals
and
thei
r cor
resp
ondi
ng h
ealth
cen
ters
are
ben
efiti
ng fr
om m
edic
al e
quip
men
t and
sup
plie
s do
nate
d by
A
CC
ES
S.
H
ealth
Fac
ility
Ass
essm
ent a
nd Q
ualit
ativ
e A
sses
smen
t wer
e co
mpl
eted
, and
pre
limin
ary
repo
rts w
ere
final
ized
and
su
bmitt
ed fo
r dis
sem
inat
ion
to M
OH
and
par
tner
s. T
he re
sults
of t
he a
sses
smen
t inf
orm
ed th
e de
velo
pmen
t of a
dra
ft na
tiona
l-lev
el c
omm
unity
beh
avio
r cha
nge
stra
tegy
.

30
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
RE
AC
TIVI
TY
MA
JOR
PR
OG
RA
MM
ATI
C O
UTP
UTS
/DEL
IVER
AB
LES
PRO
DU
CED
3.2
CO
NT.
Thro
ugh
RC
LS (R
elig
ious
Lea
der N
etw
ork
to F
ight
Aga
inst
AID
S) a
nd in
col
labo
ratio
n w
ith IM
A, d
rafte
d M
NH
mes
sage
s fo
r rel
igio
us le
ader
s to
use
dur
ing
serm
ons
rela
ted
to b
oth
the
Kor
an a
nd B
ible
.
Tr
aine
d co
re g
roup
of 2
5 na
tiona
l-lev
el tr
aine
rs fr
om 9
hos
pita
ls.
Tr
aini
ng o
f Nya
mag
abe
Dis
trict
HC
s st
aff t
hrou
gh c
ost s
hare
with
Tw
ubak
ane.
In
crea
sed
EmO
NC
and
FAN
C c
apac
ity fo
r 28
HC
s pr
ovid
ers
in N
yam
agab
e D
istri
ct.
Tr
aini
ng o
f Em
ON
C p
rovi
ders
from
15
hosp
itals
to re
plac
e tu
rned
ove
r sta
ff.
In
3 o
f the
4 a
sses
sed
dist
ricts
, 15
of 2
1 ta
rget
faci
litie
s ar
e pr
ovid
ing
AM
TSL.
H
Cs
Em
ON
C ta
sks
defin
ed a
s a
basi
s fo
r tra
inin
g m
anua
l ada
ptat
ion.
Fu
nctio
nal K
MC
Uni
t ser
ving
as
a tra
inin
g ce
nter
for K
MC
sca
ling
up a
ctiv
ities
. Mor
e th
an 3
11 lo
w b
irth
wei
ght b
abie
s ad
mitt
ed th
is re
porti
ng p
erio
d.
Gha
na
C
ompl
eted
SBM
-R m
odul
es I,
II a
nd II
I of a
ll fa
cilit
ies,
whi
ch h
as re
sulte
d in
the
abilit
y of
key
per
sonn
el in
Biri
m h
ealth
di
stric
t to
train
and
tran
sfer
upd
ates
, qua
lity
assu
ranc
e an
d qu
ality
impr
ovem
ent.
O
f the
se fa
cilit
ies,
82%
reac
hed
the
targ
et 8
5% o
f the
sta
ndar
ds b
y th
e cl
ose
of th
e pr
ojec
t.
Tr
aine
d 39
peo
ple
on S
BM
-R M
odul
es.
Tr
aine
d 5
exte
rnal
ass
esso
rs to
incr
ease
sus
tain
abili
ty o
f the
pro
cess
and
mak
e B
irim
Nor
th a
nat
iona
l mod
el fo
r the
ac
cred
itatio
n pr
oces
s.
R
ecei
ved
natio
nal a
ttent
ion
and
visi
ts fr
om th
e D
irect
or G
ener
al a
nd U
SA
ID M
issi
on s
taff
for a
chie
vem
ents
in s
ervi
ces
stat
istic
s.
Tr
aine
d 14
mid
wiv
es in
sou
ther
n B
irim
Nor
th D
istri
ct in
BE
mO
NC
.
C
ompl
eted
Hea
lth M
anag
emen
t Inf
orm
atio
n S
yste
ms
wor
ksho
ps fo
r par
ticip
ants
from
all
11 fa
cilit
ies.

31
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
RE
AC
TIVI
TY
MA
JOR
PR
OG
RA
MM
ATI
C O
UTP
UTS
/DEL
IVER
AB
LES
PRO
DU
CED
3.3
Impl
emen
t loc
al
finan
cing
m
echa
nism
s to
in
crea
se e
quity
of
heal
th s
ervi
ces
to
the
mos
t vu
lner
able
in
Nig
eria
A
CC
ES
S s
taff
supp
orte
d M
ada
com
mun
ity m
embe
rs a
nd s
take
hold
ers
in Z
amfa
ra s
tate
to d
evel
op p
lans
to o
verc
ome
finan
cial
bar
riers
to a
nten
atal
, obs
tetri
c an
d po
st-o
bste
tric
serv
ices
. Pla
ns in
clud
e tra
inin
g of
two
fem
ale
faci
litat
ors
to
orga
nize
and
sup
port
a pi
lot M
othe
rs’ C
lub,
whi
ch w
ill pr
ovid
e its
mem
bers
with
a m
eans
to s
ave
and
use
thos
e sa
ving
s to
m
ake
loan
s to
one
ano
ther
. Thi
s gr
oup
will
als
o di
scus
s an
d re
info
rce
posi
tive
RH
and
MN
H p
ract
ices
with
in th
e gr
oup
and
in th
e la
rger
com
mun
ity.
E
stab
lishe
d 8
Mot
hers
’ Clu
bs in
the
Mad
a co
mm
unity
.
Tr
aine
d 2
mem
bers
of t
he c
omm
unity
trai
ned
as fa
cilit
ator
s fo
r the
Mot
hers
’ Clu
bs.
12
0 w
omen
join
ed a
s m
embe
rs o
f the
Mot
hers
’ Clu
bs.
C
ompl
eted
initi
al M
&E
repo
rt on
the
esta
blis
hmen
t of t
he M
othe
rs’ C
lubs
in M
ada.

32
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
RE
AC
TIVI
TY
MA
JOR
PR
OG
RA
MM
ATI
C O
UTP
UTS
/DEL
IVER
AB
LES
PRO
DU
CED
IR 4
: Man
agem
ent o
f obs
tetr
ic c
ompl
icat
ions
and
sic
k ne
wbo
rns
impr
oved
4.1
Incr
ease
acc
ess
to
skille
d at
tend
ance
at
birt
h th
roug
h st
reng
then
ing
of
pre-
serv
ice
mid
wife
ry
educ
atio
n of
fron
t-lin
e pr
ovid
ers
in
four
cou
ntrie
s (E
thio
pia,
Gha
na,
Mal
awi a
nd
Tanz
ania
)
In
tegr
ated
the
MN
H s
ituat
ion
anal
ysis
into
the
MO
H/N
iger
200
8 pl
an w
ith R
oad
Map
par
tner
s in
Nig
er.
C
olla
bora
ted
with
WH
O-A
FRO
to p
lan
and
faci
litat
e th
e E
nteb
be re
gion
al R
oad
Map
wor
ksho
p to
ass
ist c
ount
ry te
ams
in
oper
atio
naliz
ing
the
natio
nal R
oad
Map
doc
umen
t. S
ix c
ount
ry te
ams
from
eas
tern
and
sou
ther
n A
frica
par
ticip
ated
in th
e w
orks
hop,
dev
elop
ing
real
istic
pla
ns fo
r ope
ratio
naliz
atio
n an
d id
entif
ying
thei
r nee
d fo
r tec
hnic
al a
ssis
tanc
e.
R
egio
nal A
FR/S
D a
ctiv
ities
incl
uded
upg
radi
ng p
re-s
ervi
ce tr
aini
ng in
four
cou
ntrie
s (E
thio
pia,
Gha
na, M
alaw
i and
Ta
nzan
ia),
and
parti
cipa
nts
from
six
cou
ntrie
s (E
thio
pia,
Ken
ya, M
alaw
i, N
amib
ia, U
gand
a, a
nd Z
ambi
a) s
hare
d th
eir
expe
rienc
es d
evel
opin
g an
d op
erat
iona
lizin
g th
eir n
atio
nal R
oad
Map
doc
umen
t at a
regi
onal
wor
ksho
p pl
anne
d an
d co
nduc
ted
by A
CC
ES
S a
nd W
HO
-AFR
O in
Apr
il 20
08.
P
lann
ed a
nd h
eld
seco
nd re
gion
al C
linic
al T
rain
ing
Ski
lls a
nd C
urric
ulum
Des
ign
cour
se fo
r app
roxi
mat
ely
20 p
re-s
ervi
ce
mid
wife
ry e
duca
tors
from
3 c
ount
ries
(Eth
iopi
a, G
hana
, and
Tan
zani
a) in
ord
er to
bui
ld m
ore
cham
pion
s fo
r im
plem
entin
g be
st p
ract
ices
in b
asic
em
erge
ncy
obst
etric
and
new
born
car
e (B
Em
ON
C) i
nto
mid
wife
ry e
duca
tion
and
prac
tice.
P
artic
ipan
ts a
ssis
ted
in th
e fa
cilit
atio
n of
BE
mO
NC
Tec
hnic
al U
pdat
e an
d C
linic
al S
kills
Sta
ndar
diza
tions
in E
thio
pia
and
Gha
na, a
nd w
ill p
artic
ipat
e in
upc
omin
g ad
voca
cy m
eetin
gs a
t the
nat
iona
l lev
el.
C
ompl
eted
revi
sion
s to
BE
mO
NC
LR
P b
ased
on
pre-
test
reco
mm
enda
tions
; pac
kage
is in
fina
l pro
duct
ion.
Th
e M
OH
in M
adag
asca
r, w
ith a
dvoc
acy
and
supp
ort f
rom
AC
CE
SS, r
epea
ted
the
Roa
d M
ap F
orum
hel
d in
Sep
tem
ber
2007
in A
ntan
anar
ivo.
4.2
Assi
st th
e E
thio
pian
Soc
iety
of
Obs
tetri
cian
s an
d G
ynec
olog
ists
(E
SO
G) t
o bu
ild
capa
city
of s
kille
d pr
ovid
ers
in E
MN
C
10
hea
lth c
ente
rs re
ferr
ing
to A
mbo
Hos
pita
l Mat
erni
ty S
ervi
ces
wer
e as
sess
ed, a
nd E
mO
NC
ser
vice
del
iver
y im
prov
ed a
t th
ese
heal
th c
ente
rs w
ith A
CC
ES
S a
nd E
thio
pian
Soc
iety
of O
bste
trici
ans
and
Gyn
ecol
ogis
ts (E
SO
G) s
uppo
rt. N
ine
of 1
0 pr
ovid
ers
wer
e tra
ined
in B
EmO
NC
(one
pro
vide
r was
on
leav
e), a
nd re
ferr
al li
nkag
es b
etw
een
10 h
ealth
cen
ters
and
A
mbo
Hos
pita
l wer
e st
reng
then
ed.
4.3
Con
tinue
ex
pans
ion
of
Kan
garo
o M
othe
r C
are
serv
ices
for
impr
oved
m
anag
emen
t of
low
birt
h w
eigh
t ba
bies
Fi
eld-
test
ed a
nd fi
naliz
ed g
loba
l fac
ility
-bas
ed K
MC
faci
litat
ors’
and
par
ticip
ants
’ man
uals
(prin
ting:
Dec
embe
r 200
8).
H
eld
cons
ulta
tion
mee
ting
on c
omm
unity
KM
C w
ith 4
3 ke
y st
akeh
olde
rs fr
om U
SA
ID, U
NIC
EF, S
NL,
US
AID
coo
pera
ting
agen
cies
, res
earc
hers
and
fiel
d st
aff.
A re
port
of th
e m
eetin
g ha
s be
en d
isse
min
ated
to m
eetin
g pa
rtici
pant
s an
d st
aff o
f in
tere
sted
org
aniz
atio
ns th
at w
ere
not p
rese
nt a
t the
mee
ting.
E
thio
pia:
Ada
pted
KM
C tr
aini
ng m
anua
l for
use
, con
duct
ed K
MC
TO
T fo
r 16
heal
th s
taff,
and
intro
duce
d K
MC
ser
vice
s in
5
hosp
itals
.
N
epal
: Int
egra
ted
KM
C in
to p
ostn
atal
car
e fo
r LBW
/pre
mat
ure
babi
es a
t fou
r hos
pita
ls a
nd 3
prim
ary
heal
th c
ente
rs;
esta
blis
hed
faci
lity-
base
d K
MC
ser
vice
s at
Mah
akal
i Zon
al H
ospi
tal a
nd 3
prim
ary
heal
th c
are
cent
ers;
and
trai
ned
814

33
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
RE
AC
TIVI
TY
MA
JOR
PR
OG
RA
MM
ATI
C O
UTP
UTS
/DEL
IVER
AB
LES
PRO
DU
CED
4.3
CO
NT.
fe
mal
e co
mm
unity
hea
lth v
olun
teer
s on
com
mun
ity K
MC
. Nat
iona
l gui
delin
es fo
r man
agem
ent o
f LB
W in
fant
s an
d K
MC
w
ere
deve
lope
d an
d en
dors
ed b
y th
e M
OP
H a
nd w
ill b
e in
clud
ed a
s pa
rt of
a c
omm
unity
-bas
ed in
tegr
ated
neo
nata
l car
e pa
ckag
e to
be
impl
emen
ted
natio
nally
. Com
plet
ed fi
nal r
epor
t on
the
com
mun
ity-b
ased
man
agem
ent o
f LB
W b
abie
s.
R
wan
da: I
nitia
ted
KM
C s
ervi
ces
in 7
hos
pita
ls, i
nclu
ding
the
univ
ersi
ty te
achi
ng h
ospi
tal i
n K
igal
i. Tr
aine
d 24
ser
vice
pr
ovid
ers
in K
MC
from
the
8 ho
spita
ls.
B
angl
ades
h: T
rain
ed a
ll 28
6 A
CC
ES
S c
ouns
elor
s on
how
to c
oach
mot
hers
to p
rovi
de K
MC
.
4.4
Pre
vent
ion
of
pre-
ecla
mps
ia/
ecla
mps
ia
P
rovi
ded
tech
nica
l ass
ista
nce
in N
epal
to th
e U
SA
ID b
ilate
ral a
nd M
OH
to in
trodu
ce c
alci
um in
to A
NC
and
test
its
acce
ptab
ility
and
effe
ct o
n co
mm
unity
-leve
l pre
vent
ion
of e
clam
psia
.
M
et w
ith U
SAI
D a
nd p
artn
ers
in T
anza
nia
to o
utlin
e ne
ed fo
r stra
tegy
at c
omm
unity
and
faci
lity
leve
ls fo
r pre
vent
ion
and
treat
men
t of p
re-e
clam
psia
/ecl
amps
ia; U
SA
ID m
issi
on in
clud
ed th
is a
s pa
rt of
pro
pose
d fu
ndin
g fo
r bas
ic e
mer
genc
y ob
stet
ric a
nd n
ewbo
rn c
are
thro
ugho
ut th
e co
untry
.
Te
leco
nfer
ence
with
par
tner
s fro
m U
SAI
D a
nd P
ATH
rega
rdin
g pr
even
tion
and
treat
men
t of p
re-e
clam
psia
/ ecl
amps
ia,
incl
udin
g di
scus
sion
of n
ext s
teps
to ra
ise
this
as
a so
lvab
le is
sue
in m
any
coun
tries
.
M
eetin
gs w
ith U
SA
ID, M
OH
and
oth
er p
artn
ers
in E
thio
pia,
Ken
ya a
nd S
outh
Afri
ca to
dis
cuss
impo
rtanc
e of
stra
tegy
to
decr
ease
mat
erna
l and
new
born
mor
talit
y du
e to
pre
-ecl
amps
ia/e
clam
psia
.

34
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
RE
AC
TIVI
TY
MA
JOR
PR
OG
RA
MM
ATI
C O
UTP
UTS
/DEL
IVER
AB
LES
PRO
DU
CED
IR 5
: Pre
vent
ion
and
trea
tmen
t of p
riorit
y he
alth
pro
blem
s of
non
-pre
gnan
t wom
en o
f rep
rodu
ctiv
e he
alth
age
(Tar
gets
of O
ppor
tuni
ty)
5.1
Fiel
d-te
st a
nd
final
ize
the
revi
sed
post
-abo
rtion
car
e cu
rric
ulum
Tr
ansl
ated
PA
C L
RP
into
Fre
nch
and
field
-test
ed th
e pa
ckag
e du
ring
a tra
inin
g of
11
prov
ider
s in
Hai
ti.
C
olla
ted
feed
back
from
fiel
d-te
sts
in B
oliv
ia a
nd H
aiti
for i
ncor
pora
tion
into
fina
l dra
ft of
cur
ricul
um; e
xpec
ted
date
of
com
plet
ion
is 3
0 O
ctob
er 2
008.

A
nnex
B: P
rogr
am C
over
age
Mat
rix
35
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
Ann
ex B
: Pro
gram
Cov
erag
e M
atrix
A
CC
ESS
clin
ical
(e.g
., ca
paci
ty b
uild
ing
and
serv
ice
deliv
ery)
and
com
mun
ity-b
ased
(e.g
., de
man
d ge
nera
tion)
inte
rven
tions
ove
r the
pa
st y
ear h
ave
reac
hed
wom
en a
nd fa
mili
es in
Afg
hani
stan
, Ban
glad
esh,
Eth
iopi
a, G
hana
, Ind
ia, K
enya
, Mal
awi,
Nig
eria
, Sou
th
Afr
ica,
and
Tan
zani
a. T
able
1 b
elow
pre
sent
s inf
orm
atio
n on
the
type
s of i
nter
vent
ions
bei
ng im
plem
ente
d in
eac
h co
untry
and
the
asso
ciat
ed p
oten
tial p
opul
atio
n co
vera
ge (t
hose
livi
ng in
the
inte
rven
tion
targ
et c
omm
uniti
es a
nd/o
r fac
ility
cat
chm
ent a
reas
). It
is im
porta
nt to
not
e th
at th
is m
atrix
doe
s not
alw
ays c
aptu
re n
atio
nal-l
evel
pol
icy
wor
k. In
add
ition
, AC
CES
S co
untry
pro
gram
s are
at
diff
eren
t sta
ges o
f im
plem
enta
tion—
som
e be
gan
in 2
004
whi
le o
ther
s beg
an in
200
7—th
us, c
over
age
may
be
vast
ly d
iffer
ent.
Fina
lly, A
CC
ESS
is a
glo
bal,
core
-fun
ded
prog
ram
that
use
s its
cor
e fu
nds p
rimar
ily fo
r tec
hnic
al le
ader
ship
and
glo
bal l
earn
ing.
C
ore-
fund
ed c
ount
ry-le
vel i
nter
vent
ions
tend
to b
e re
lativ
ely
smal
l in
geog
raph
ic sc
ope
and
serv
e to
dem
onst
rate
tran
sfer
of r
esea
rch
to p
ract
ice
of e
vide
nce-
base
d ap
proa
ches
in M
NH
. The
se re
sults
are
then
use
d to
info
rm n
atio
nal a
nd g
loba
l pol
icy
and
prog
ram
min
g.
Fiel
d su
ppor
t-fun
ded
prog
ram
s, on
the
othe
r han
d, te
nd to
hav
e la
rger
geo
grap
hic
scop
e an
d fu
ndin
g fo
r sca
le-u
p.
Tabl
e 1:
AC
CES
S Pr
ogra
m C
over
age
CO
UN
TRY
INTE
RVE
NTI
ON
#
OF
CO
MM
UN
ITIE
S #
OF
FAC
ILIT
IES
# O
F D
ISTR
ICTS
/ D
EPA
RTM
ENTS
% O
F D
ISTR
ICTS
/ D
EPA
RTM
ENTS
# O
F R
EGIO
NS/
PR
OVI
NC
ES
TOTA
L PO
PULA
TIO
N
(IN T
AR
GET
A
REA
S)
# O
F W
OM
EN O
F R
EPR
OD
UC
TIVE
A
GE
(15–
49)
AFG
HA
NIS
TAN
P
PG
ski
lled
birth
at
tend
ant
inte
rven
tion
N/A
38
1 B
PH
S h
ealth
fa
cilit
ies1
119
out o
f 329
di
stric
ts
36%
13
out
of 3
2 pr
ovin
ces2
7,05
0,71
6 1,
410,
143
BA
NG
LAD
ESH
P
rena
tal/p
ostn
atal
co
mm
unity
ou
treac
h vi
sits
and
re
ferra
l
7 su
b-di
stric
ts
(upa
zilla
s)
N/A
1
out o
f 64
dist
ricts
1.
6%
N/A
1,
443,
841
287,
324
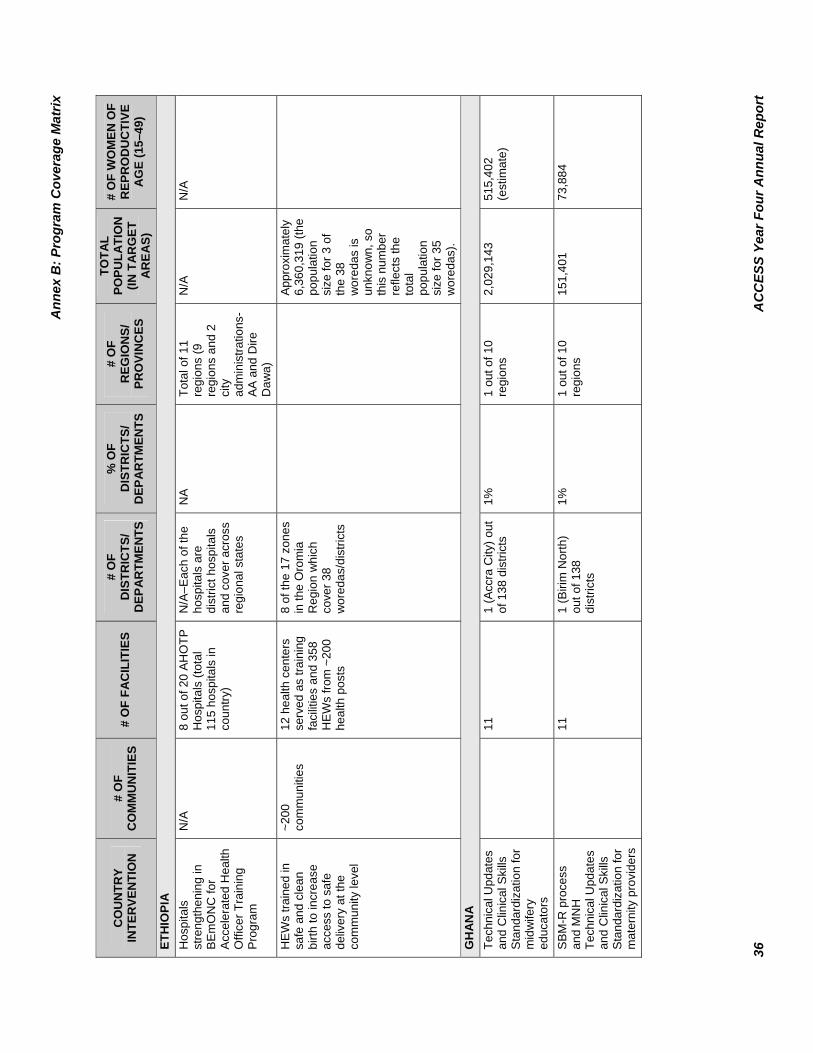
A
nnex
B: P
rogr
am C
over
age
Mat
rix
36
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
UN
TRY
INTE
RVE
NTI
ON
#
OF
CO
MM
UN
ITIE
S #
OF
FAC
ILIT
IES
# O
F D
ISTR
ICTS
/ D
EPA
RTM
ENTS
% O
F D
ISTR
ICTS
/ D
EPA
RTM
ENTS
# O
F R
EGIO
NS/
PR
OVI
NC
ES
TOTA
L PO
PULA
TIO
N
(IN T
AR
GET
A
REA
S)
# O
F W
OM
EN O
F R
EPR
OD
UC
TIVE
A
GE
(15–
49)
ETH
IOPI
A
Hos
pita
ls
stre
ngth
enin
g in
B
Em
ON
C fo
r Ac
cele
rate
d H
ealth
O
ffice
r Tra
inin
g P
rogr
am
N/A
8
out o
f 20
AH
OTP
H
ospi
tals
(tot
al
115
hosp
itals
in
coun
try)
N/A
–Eac
h of
the
hosp
itals
are
di
stric
t hos
pita
ls
and
cove
r acr
oss
regi
onal
sta
tes
NA
To
tal o
f 11
regi
ons
(9
regi
ons
and
2 ci
ty
adm
inis
tratio
ns-
AA a
nd D
ire
Daw
a)
N/A
N
/A
HE
Ws
train
ed in
sa
fe a
nd c
lean
bi
rth to
incr
ease
ac
cess
to s
afe
deliv
ery
at th
e co
mm
unity
leve
l
~200
co
mm
uniti
es
12 h
ealth
cen
ters
se
rved
as
train
ing
faci
litie
s an
d 35
8 H
EW
s fro
m ~
200
heal
th p
osts
8 of
the
17 z
ones
in
the
Oro
mia
R
egio
n w
hich
co
ver 3
8 w
ored
as/d
istri
cts
Appr
oxim
atel
y 6,
360,
319
(the
popu
latio
n si
ze fo
r 3 o
f th
e 38
w
ored
as is
un
know
n, s
o th
is n
umbe
r re
flect
s th
e to
tal
popu
latio
n si
ze fo
r 35
wor
edas
).
GH
AN
A
Tech
nica
l Upd
ates
an
d C
linic
al S
kills
S
tand
ardi
zatio
n fo
r m
idw
ifery
ed
ucat
ors
11
1
(Acc
ra C
ity) o
ut
of 1
38 d
istri
cts
1%
1 ou
t of 1
0 re
gion
s 2,
029,
143
515,
402
(est
imat
e)
SB
M-R
pro
cess
an
d M
NH
Te
chni
cal U
pdat
es
and
Clin
ical
Ski
lls
Sta
ndar
diza
tion
for
mat
erni
ty p
rovi
ders
11
1
(Biri
m N
orth
) ou
t of 1
38
dist
ricts
1%
1 ou
t of 1
0 re
gion
s 15
1,40
1 73
,884
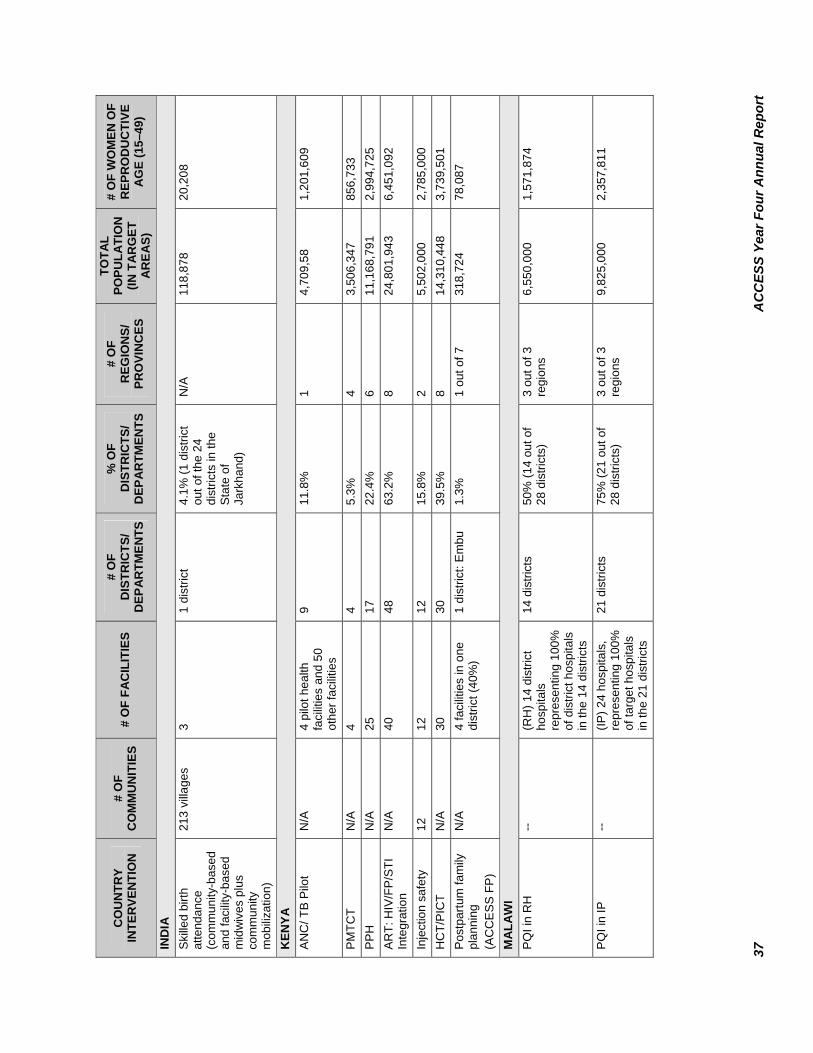
37
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
UN
TRY
INTE
RVE
NTI
ON
#
OF
CO
MM
UN
ITIE
S #
OF
FAC
ILIT
IES
# O
F D
ISTR
ICTS
/ D
EPA
RTM
ENTS
% O
F D
ISTR
ICTS
/ D
EPA
RTM
ENTS
# O
F R
EGIO
NS/
PR
OVI
NC
ES
TOTA
L PO
PULA
TIO
N
(IN T
AR
GET
A
REA
S)
# O
F W
OM
EN O
F R
EPR
OD
UC
TIVE
A
GE
(15–
49)
IND
IA
Skille
d bi
rth
atte
ndan
ce
(com
mun
ity-b
ased
an
d fa
cilit
y-ba
sed
mid
wiv
es p
lus
com
mun
ity
mob
iliza
tion)
213
villa
ges
3 1
dist
rict
4.1%
(1 d
istri
ct
out o
f the
24
dist
ricts
in th
e S
tate
of
Jark
hand
)
N/A
11
8,87
8 20
,208
KEN
YA
AN
C/ T
B P
ilot
N/A
4
pilo
t hea
lth
faci
litie
s an
d 50
ot
her f
acili
ties
9 11
.8%
1
4,70
9,58
1,
201,
609
PM
TCT
N/A
4
4
5.
3%
4
3,50
6,34
7 85
6,73
3 PP
H
N/A
25
17
22
.4%
6
11,1
68,7
91
2,99
4,72
5 A
RT:
HIV
/FP/
STI
Inte
grat
ion
N/A
40
48
63
.2%
8
24,8
01,9
43
6,45
1,09
2
Inje
ctio
n sa
fety
12
12
12
15
.8%
2
5,50
2,00
0 2,
785,
000
HC
T/P
ICT
N/A
30
30
39
.5%
8
14,3
10,4
48
3,73
9,50
1 P
ostp
artu
m fa
mily
pl
anni
ng
(AC
CE
SS
FP
)
N/A
4
faci
litie
s in
one
di
stric
t (40
%)
1 di
stric
t: E
mbu
1.
3%
1 ou
t of 7
31
8,72
4 78
,087
MA
LAW
I P
QI i
n R
H
-- (R
H) 1
4 di
stric
t ho
spita
ls
repr
esen
ting
100%
of
dis
trict
hos
pita
ls
in th
e 14
dis
trict
s
14 d
istri
cts
50%
(14
out o
f 28
dis
trict
s)
3 ou
t of 3
re
gion
s 6,
550,
000
1,57
1,87
4
PQ
I in
IP
--
(IP) 2
4 ho
spita
ls,
repr
esen
ting
100%
of
targ
et h
ospi
tals
in
the
21 d
istri
cts
21 d
istri
cts
75%
(21
out o
f 28
dis
trict
s)
3 ou
t of 3
re
gion
s 9,
825,
000
2,35
7,81
1

A
nnex
B: P
rogr
am C
over
age
Mat
rix
38
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
UN
TRY
INTE
RVE
NTI
ON
#
OF
CO
MM
UN
ITIE
S #
OF
FAC
ILIT
IES
# O
F D
ISTR
ICTS
/ D
EPA
RTM
ENTS
% O
F D
ISTR
ICTS
/ D
EPA
RTM
ENTS
# O
F R
EGIO
NS/
PR
OVI
NC
ES
TOTA
L PO
PULA
TIO
N
(IN T
AR
GET
A
REA
S)
# O
F W
OM
EN O
F R
EPR
OD
UC
TIVE
A
GE
(15–
49)
FAN
C/M
IP
-- 73
0 he
alth
fa
cilit
ies
repr
esen
ting
100%
of
hea
lth fa
cilit
ies
coun
tryw
ide
28 d
istri
cts
100%
3
out o
f 3
regi
ons
13,1
00,0
00
3,14
3,74
9
Pre-
serv
ice
and
in-
serv
ice
--
13 R
N/M
trai
ning
in
stitu
tions
re
pres
entin
g 10
0%
of R
N/M
trai
ning
in
stitu
tions
8 di
stric
ts
29%
(8 o
ut o
f 28
dist
ricts
) 3
out o
f 3
regi
ons
3,79
9,00
0 91
1,68
7
KM
C
--
11 h
ealth
faci
litie
s re
pres
entin
g 10
0%
of ta
rget
hea
lth
faci
litie
s in
3
dist
ricts
3 di
stric
ts
11%
(3 o
ut o
f 28
dist
ricts
) 3
out o
f 3
regi
ons
341,
000
81,8
33
Com
mun
ity M
NH
an
d co
mm
unity
m
obili
zatio
n
816
villa
ges
9 he
alth
cen
ters
re
pres
entin
g 10
0%
of ta
rget
hea
lth
cent
ers
in th
e 5
targ
et a
reas
3 di
stric
ts
11%
(3 o
ut o
f 28
dist
ricts
) 3
out o
f 3
regi
ons
336,
358
80,7
19
NIG
ERIA
Em
erge
ncy
obst
etric
and
ne
wbo
rn c
are
as
an e
ntry
poi
nt to
po
stpa
rtum
fam
ily
plan
ning
and
co
mm
unity
m
obili
zatio
n
71
37: 1
4 ge
nera
l ho
spita
ls; 1
co
mpr
ehen
sive
he
alth
cen
ter a
nd
22 p
rimar
y he
alth
ca
re c
ente
rs
18 L
GA
s (d
istri
cts)
out
of
774
(6 L
GA
s in
ea
ch o
f 3 S
tate
s in
clud
ing
Kan
o,
Zam
fara
and
K
atsi
na)
2.3%
1
out o
f 6
4,20
2,77
5 97
5,04
4 (e
stim
ate)

39
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
CO
UN
TRY
INTE
RVE
NTI
ON
#
OF
CO
MM
UN
ITIE
S #
OF
FAC
ILIT
IES
# O
F D
ISTR
ICTS
/ D
EPA
RTM
ENTS
% O
F D
ISTR
ICTS
/ D
EPA
RTM
ENTS
# O
F R
EGIO
NS/
PR
OVI
NC
ES
TOTA
L PO
PULA
TIO
N
(IN T
AR
GET
A
REA
S)
# O
F W
OM
EN O
F R
EPR
OD
UC
TIVE
A
GE
(15–
49)
SOU
TH A
FRIC
A
Impl
emen
tatio
n of
A
ntire
trovi
ral
Ser
vice
Sta
ndar
d-ba
sed
Man
agem
ent
N/A
5
2
dist
ricts
4%
of t
he 5
3 di
stric
ts
coun
tryw
ide
2 ou
t of 9
1,
068,
771
287,
878
Cer
vica
l scr
eeni
ng
serv
ice
prov
isio
n us
ing
VIA
and
Cry
othe
rapy
N/A
12
1
dist
rict
2% o
f the
53
dist
ricts
co
untry
wid
e
1 ou
t of 9
63
2179
17
0,68
8
TAN
ZAN
IA
FAN
C/M
IP s
ervi
ce
deliv
ery
scal
e-up
N
A
1,57
5 (3
2% o
f all
faci
litie
s)
133
out o
f 133
(m
ainl
and)
10
0%
21 o
ut o
f 21
(100
%)
39,4
00,0
00
7,88
0,00
0
Tech
nica
l Upd
ates
an
d C
linic
al S
kills
S
tand
ardi
zatio
n fo
r M
idw
ifery
E
duca
tors
NA
1 (c
linic
al tr
aini
ng
faci
lity)
1
(Mor
ogor
o) o
ut
of 1
30
1%
1 ou
t of 2
1 N
A
1,75
3,36
2 3,
507,
462
Not
e: D
ata
sour
ces
for p
opul
atio
n fig
ures
incl
ude
natio
nal c
ensu
s da
ta; U
S C
ensu
s B
urea
u, In
tern
atio
nal D
atab
ase,
http
://w
ww
.cen
sus.
gov/
ipc/
ww
w/id
bpyr
.htm
l; W
orld
Gaz
ette
er a
t ww
w.w
orld
-gaz
ette
er.c
om);
http
://po
pula
tion.
wn.
com
http
://w
ww
.odc
i.gov
/cia
/pub
licat
ions
/fact
book
/inde
x.ht
ml (
Mad
agas
car)
; Ken
ya 1
999
Pop
ulat
ion
and
Hou
sing
Cen
sus
Vol
ume
VII:
Ana
lytic
al R
epor
t on
Pop
ulat
ion
Pro
ject
ions
, 200
2 (K
enya
). N
iger
ia: P
opul
atio
n C
omm
issi
on re
port.
Mal
awi:
Sou
rces
: P
opul
atio
n R
efer
ence
Bur
eau,
200
7 W
orld
Pop
ulat
ion
Dat
ashe
et. P
opul
atio
n R
efer
ence
Bur
eau,
Fam
ily P
lann
ing
Wor
ldw
ide
2008
Dat
a S
heet
. Afg
hani
stan
and
Ta
nzan
ia: W
omen
of r
epro
duct
ive
age
estim
ated
at 2
0% o
f the
tota
l pop
ulat
ion.

40 ACCESS Year Four Annual Report
Annex C: Success Stories Bangladesh: Respect for TBA Increased after Training Rasheda Begum, an experienced traditional birth attendant (TBA), has been delivering babies for more than 10 years. After the death of her mother-in-law, who taught her these traditional skills, the community began turning to Rasheda as the most trusted and dependable TBA in the area. Nevertheless, Rasheda confessed to knowing nothing about safe and clean delivery, handwashing, newborn stimulation, immediate breastfeeding, or community-based Kangaroo Mother Care (CKMC) practices at the time. Having now received TBA training from the ACCESS Program, she is feeling much more confident about her ability to help mothers and newborns. Since her training, Rasheda attended a delivery in which a baby stopped breathing. She was happy to see the impact of her training when she gave the newborn extra stimulation and the baby began breathing again. When, in a separate case, a placenta was taking longer than usual to expel, Rasheda gave the newborn to the mother and asked her to begin breastfeeding. Within minutes, the placenta came out smoothly. Rasheda also applied her new CKMC knowledge when confronted with a comparatively small newborn who was shivering after drying and wrapping. She put the newborn in CKMC position with the mother where it fell asleep quickly, and was warmed and well protected from risk. Ethiopia: Community Mobilization for Pregnancy-Related Complications Mobilizing communities to inform, address and solicit support for maternal and neonatal health emergencies is a major activity of the ACCESS HEW Training Program in Ethiopia. Tekaye Seifu, a HEW who completed training in the first round, was able to implement some of the CM skills she was exposed to during the training in Urgesa Kebele, a remote village near Bedelle in southern Ethiopia. Within a couple of months, Tekaye was able to organize a group of 80 women to meet once a week and to each contribute the equivalent of five US cents during each meeting. Recently, one member of the group suffered from pregnancy-related complications, and the collection was used to help fund her transportation to Bedelle Health Center for treatment. Women withdrawing funds for maternal or neonatal emergencies are not required to replenish what they use. Tekaye is proud of her success in mobilizing the women to have access to treatment for complications, and anticipates continuing the group meetings to assist more women in her village.
TBAs at a training.

ACCESS Year Four Annual Report 41
Malama Hajara and her new born baby (first delivery at Dawanau PHC).
Nigeria: Success of a Community Action Cycle The objective of the community action cycle is to increase awareness of and strengthen access to EmONC services. After receiving proper training, the community mobilization team (CMT) members returned to their respective communities to begin the process of identifying groups and committees that will participate in the CM process. A broad spectrum of community members including women, men and adolescents were selected in Dawanau community and environs to form the community core group (CCG) and committees. During the exploration process, the communities and core group discussed the state of maternal
and newborn care and consensus was reached that the lack of skill birth attendants at Dawanau PHC is the root cause of high home delivery rates. To address this problem, the community requested the services of volunteer nurse-midwives from within and outside the community to establish delivery services at Dawanau PHC. In addition, the CCG and community partitioned a space at the PHC to serve as a labor room. It was laudable that three nurse-midwives volunteered to help provide delivery services at the health facility and resumed work there in November 2007. By the end of the quarter, nine deliveries had been recorded at Dawanau PHC. During the quarter, nurse-midwives were trained to provide long-acting methods of FP. Hajiya Ramatu Usman, a nurse-midwife working at Zurmi General Hospital and mother of five children, was a participants. She was so impressed by the long-term contraceptive potential of JADELLE® that she accepted the method herself and had it inserted during the training. She indicated that she would like to use it for four years. During the SBM-R training which followed, she expressed complete satisfaction with the method, “As the nurse-midwife-in-charge of the Maternity Unit in Zurmi General Hospital and after my training in IUD and JADELLE insertion/removal, I now see an average of six FP clients a day coming for different methods. I use the knowledge that I got during the ACCESS training to train my subordinates in the hospital. I am glad that I went through the training done by ACCESS, which has made me to be more confident to provide services to my clients. May the
Hajiya Ramotu Usman.

42 ACCESS Year Four Annual Report
Almighty God continue to guide the ACCESS staff. I am ready to give my full support and will come to help whenever I am invited. My husband is also very happy with the JADELLE and wants my other two co-wives, who have 12 children between them, to also use the method.” Tanzania: Pre-service Education BEmONC for Nursing and Midwifery Schools in Tanzania Deodata Kihuwe is a midwifery tutor who attended a clinical standardization course on BEmONC, one of the activities in the Pre-service Education Initiative for Africa Region supported by WHO-AFRO/ACCESS/Jhpiego and the MOHSW. Conducted in September 2007, the course helped midwifery tutors and preceptors improve their clinical skills. In April 2008, Deodata participated in the Effective Teaching Skills course to improve her teaching skills, ability to communicate her BEmONC knowledge, and demonstrate the related skills. When Deodata went back to her school (Bagamoyo Nursing and Midwifery Certificate School) after the course, she gave feedback to the students, administrators and staff in the Department of Maternal Health at Bagamoyo District Hospital. Deodata explained the content of the course as well as the learning and teaching processes. Maro, the assistant medical officer-in-charge of the Maternal and Newborn Unit, was excited and said, “Providers in the labor ward will now be getting additional support. Deodata, you went through critical topics like removal of retained placenta and resuscitation of newborn. You will provide updates to other service providers.” Maro even phoned Jhpiego’s office on the following day to express his appreciation and said, “I am very happy to see that our hospital maternal and newborn care providers will be supported. Deodata will be of great help in the labor ward, especially on my absence! BEmNOC topics that Deodata went through are similar to what I was taught in LSS. Thanks to Jhpiego!” Ghana: SBM-R Success Leads to Improved Performance Holy Horniel Maternity Home is a private facility located in the Birim North District, Ghana. The midwife in charge is also the owner. The primary assessment tool for the project was a standardized basic emergency obstetric and neonatal care assessment tool (adapted using Ghana’s National Reproductive Health Standards and Protocols). The tool grouped standards under two areas: labor and delivery care and other infrastructure. During a baseline assessment in January 2008 (after the midwife, Contance Asante, had completed SBM-R Module I), the facility scored 57% on labor and delivery care and 60% on other infrastructure. After the midwife had completed SBM-R Module II, a second assessment of the facility revealed tremendous improvements in labor and delivery care (97%) and other infrastructure (100%). On a recent visit to donate an advanced childbirth simulator, further improvements beyond the required standards were observed and the midwife said, “We are most grateful to Jhpiego and its representatives. Our performance has improved so much and we promise to put this model to very good use and continue to improve on the standards attained.” During the SBM-R Module III workshop, Parent to the District, Mr. Kyeremeh (also the Deputy Director of Nursing Services at the regional level) was so impressed with the concept and the achievements that he stated, “I am going to apply SBM-R to all my activities at home!”

ACCESS Year Four Annual Report 43
ANNEX D: ACCESS Bureau and Country Funding Table (PY1–PY4)
ACCESS COUNTRY PROGRAM YEAR FUNDING OBLIGATED (*ANTICIPATED) KEY ACTIVITIES
1 $0 2 $0 3 (new) $120,000 – Core Build capacity of skilled
providers in EMNC through Ethiopian Society of Obstetricians and Gynecologists
Training health officers Training community
health extension workers
Collaboration with AFR/SD pre-service initiative
4 (new) $1,792,476 – Field Training health officers in BEmONC
Training community health extension workers
ETHIOPIA
$105,000 – Core Build capacity of skilled providers in EMNC through Ethiopian Society of Obstetricians and Gynecologists
Collaboration with AFR/SD pre-service initiative ($174,991, core, for 3 countries)
1 $0 2 $0 3 (new) $180,000 – Core Expand EmONC
training Collaboration with AFR/
SD preservice initiative 4 $114,000– Core Expand EmONC training
GHANA
Core Collaboration with AFR/SD preservice initiative ($174,991, core, for 3 countries)

44 ACCESS Year Four Annual Report
ACCESS COUNTRY PROGRAM YEAR FUNDING OBLIGATED (*ANTICIPATED) KEY ACTIVITIES
1 $0 2 (new) $100,000 – Field Expansion of PAC 3 $30,000 (Field carry
forward) Expansion of PAC and
FP
GUINEA
4 $100,000 - Field Revise pre-service module for school of medicine
Train medical faculty and update in clinical skills and instructional design
1 $0 Institutionalizing best practices for FP [activities began in PY 1 and will be reported in 1st annual report even though we never got an approved workplan]
2 (new) $1,120,000 – Field Institutionalizing best practices for FP
Training for voluntary counseling and testing (VCT) counselors and antiretroviral therapy (ART) within PMTCT programs
3 $1,700.000 – Field (est.) $125,000 – Core
Strengthen counseling and testing services for HIV in clinical setting
4 $3,132,740 – Field (anticipated)
Strengthen counseling and testing services for HIV in clinical setting
Scaling up ART services
KENYA
$64,000 – Core Expanding AMTSL service delivery
1 $0 2 $0 3 (new) $50,000 – Field Quality and
sustainability of focused antenatal care (FANC), intermittent preventive therapy (IPT) services
MADAGASCAR
4 $600,000-Field (FY08 PMI)
Scale up FANC and quality improvements

ACCESS Year Four Annual Report 45
ACCESS COUNTRY PROGRAM YEAR FUNDING OBLIGATED (*ANTICIPATED) KEY ACTIVITIES
1 $0 2 $0 3 $ 215,000 – Core Expand EmONC
training Collaboration with
AFR/SD pre-service initiative
MALAWI
4 (new) $2,690,000 – Field Expansion of PAC, FP and Emergency Obstetric and Newborn Care (EmONC) in eight districts
FANC/IPT Community-based
maternal and newborn care
Kangaroo Mother Care (KMC)
1 $0 2 (new) $1,000,000 – Field
(multi-year) Emergency obstetric
care and obstetric fistula
3 $2,000,000 – Field Improvement of EmONC services
Community mobilization regarding access to skilled providers
Policy work on deployment of skilled providers
$125,000 – Core Conduct study on local financing mechanisms to increase equity of health services in Nigeria
4 $2,323,000 – Field Improvement of EmONC services
Community mobilization regarding access to skilled providers
Policy work on deployment of skilled providers
NIGERIA
$130,000 – Core Apply lessons learned on local financing mechanisms to increase equity of health services in Nigeria

46 ACCESS Year Four Annual Report
ACCESS COUNTRY PROGRAM YEAR FUNDING OBLIGATED (*ANTICIPATED) KEY ACTIVITIES
1 $0 2 $0 3 (new) $650,000 – Core Implementation of Safe
Birth Africa Initiative 4 (new) $782,000 – Core Implementation of Safe
Birth Africa Initiative
RWANDA
$350,000 – Field/PMI Expand FANC/MIP 1 $0 2 $0 3 (new) $600,000 – Field Dissemination of clinical
guidelines around HIV/ AIDS prevention and treatment
SOUTH AFRICA
4 $1,245,000 – Field Dissemination of clinical guidelines and quality improvement around HIV/AIDS prevention and treatment
1 (new) $950,000 – Field Integrated ANC and PMTCT
Pre-service training in focused ANC
Dissemination of IP guidelines
Support to WRA 2 $1,625,000 – Field Integrated ANC and
PMTCT Preservice training in
focused ANC Dissemination of IP
guidelines Support to WRA Support to CEEMI
(Malaria Center) 3 $1,962,000 – Field Scale up FANC and MIP
Strengthen nutrition in in-service and pre-service training
$80,000 – Core Collaboration with AFR/SD pre-service initiative ($250,000, core, for 3 countries)
4 $3,973,000 – Field Scale up FANC and MIP
TANZANIA
Core Collaboration with AFR/SD pre-service initiative ($174,991, core, for 3 countries)

ACCESS Year Four Annual Report 47
ACCESS COUNTRY PROGRAM YEAR FUNDING OBLIGATED (*ANTICIPATED) KEY ACTIVITIES
1 $0 2 $0 3 (new) $50,000 - Field (pay back) Enhance the Social
Mobilization effort to fight HIV/AIDS
ZAMBIA
4 $0 1 $920,000 – MAC Core
$770,000 – MAC Field Field support from
Kenya, Madagascar, REDSO ESA, Rwanda and WARP
Coordination with MAC core funding
2 $900,000 – MAC Core $685,000 – MAC Field
Field support from Kenya, Madagascar, REDSO and Mali
3 $440,000 – MAC Core ($200,000 new + $240,000 estimated carry forward)
Personnel support in field and HQ to consolidate lessons learned
MALARIA ACTION COALITION
4 $100,000 – MAC Core Personnel support in field and HQ to consolidate lessons learned
1 $0 2 (new) $3,000,000 - Field Support to the Afghan
Midwives Association (AMA)
Assist in the development of a new maternal and newborn health strategy
Establish demonstration project for the prevention of postpartum hemorrhage (PPH) for home births
Feasibility study for a maternity waiting home in Badakhshan Province
3 (new) Carry forward – Field $8,500,000 – Associate Award/HSSP (multi-year)
Support to AMA Continuation of PPH
study Activities to support
new program on improving quality of care in 13 provinces and training community midwives
AFGHANISTAN AFGHANISTAN (CONT.)
4 $4,391,056 – Associate Award/HSSP
Expansion and scale up of PPH prevention
Activities to support new program on improving quality of care in 13 provinces

48 ACCESS Year Four Annual Report
ACCESS COUNTRY PROGRAM YEAR FUNDING OBLIGATED (*ANTICIPATED) KEY ACTIVITIES
and training community midwives
$112,624 – Field Support to AMA 1 $0 2 (new) $2,600,000 – Field
(multi-year) Support a community
based initiative in Sylhet to improve access to evidence-based maternal and newborn health interventions
3 $3,061,000 – Field Community mobilization and behavior change for maternal and newborn health
Policy work and advocacy for strengthening services
BANGLADESH
4 $0 1 $0 2 $95,000 – Core/ANE Policy support for
maternal and newborn health
Strengthen midwifery skills and increasing access to skilled providers
3 (new) $600,000 – Associate Award (1.8 million multi-year funding)
Policy support for maternal and newborn health
Strengthen midwifery skills and increasing access to skilled providers
Expansion of evidence-based maternal and new born interventions
$200,000 – Core PPH prevention 4 $1,100,000 – AA (over
three years) Policy support for
maternal and newborn health
Strengthen midwifery skills and increasing access to skilled providers
Expansion of evidence-based maternal and new born interventions
CAMBODIA
$120,317 – Core (includes carry forward)
PPH prevention

ACCESS Year Four Annual Report 49
ACCESS COUNTRY PROGRAM YEAR FUNDING OBLIGATED (*ANTICIPATED) KEY ACTIVITIES
1 $0 2 (new) Core Improving auxiliary nurse
midwives (ANMs) skills to provide services and increasing demand in the community
3 $500,000 – Core $50,000 – Field
Improving ANM skills to provide services and increasing demand in the community
INDIA
4 $496,000 – Core Improving ANM skills to provide services and increasing demand in the community
1 (new) $200,000 – Field Development of human resource strategy for skilled birth attendants (SBAs) and community-based maternal and newborn care
2 $2,450,000 – Field (multi-year)
Develop SBA learning resource package
Develop and test a community strategy for the identification and management of low birth weight (LBW) infants
Assist with national guidelines for LBW in the National Neonatal Health strategy
Policy work on the enabling environment of SBAs in rural communities.
CEDPA (adolescent health)
3 $1,000,000 – Field (carry forward)
Curriculum development and training for skilled providers
Guidelines development for LBW infants
Community management of LBW infants
$160,000 – Core KMC
NEPAL
4 Carry forward TBD – Field TBD – Core
Continue expansion of KMC

50 ACCESS Year Four Annual Report
ACCESS COUNTRY PROGRAM YEAR FUNDING OBLIGATED (*ANTICIPATED) KEY ACTIVITIES
1 (new) $1,500,000 – Field Increased accessibility and use of PMTCT
Strengthened reproductive health— postabortion care (PAC), infection prevention and family planning (FP)
Assess cervical cancer prevention
2 $695,000 – Field Increase accessibility and use of PMTCT services
Strengthen RH – PAC, FP, IP
Assess Cervical Cancer Prevention activities
3 $450,000 – Field Strengthen PMTCT training and services
Strengthen RH – PAC, FP, IP
HAITI
4 $130,000- Core FP/RH Field-test PAC module Revise curriculum
1 $0 2 $0 3 $127,000 Kenya
USAID/EAST AFRICA
4 $0 (carry forward) 1 (new) $200,000 Angola, Ethiopia,
Ghana, Mozambique, Nigeria, Mali, Senegal, Tanzania
2 $400,000 Zambia, Niger, Senegal, Burkina Faso, Mauritania, Ghana*, Ethiopia*, Malawi*, Tanzania*
3 $400,000 Ghana, Tanzania, Ethiopia, Malawi
AFR/SD BUREAU
4 $400,000 Ghana, Tanzania, Ethiopia

ACCESS Year Four Annual Report 51
ACCESS COUNTRY PROGRAM YEAR FUNDING OBLIGATED (*ANTICIPATED) KEY ACTIVITIES
1 $430,000 Nepal, Bangladesh, Cambodia, Afghanistan, India, Indonesia, Philippines, Pakistan, West Timor
2 $0 ($373,150 carry forward)
Nepal, Bangladesh, Cambodia, Afghanistan, India, Indonesia, Philippines, Pakistan, West Timor
3 $0 ($208,932 carry forward)
ANE BUREAU
4 $0 ($34,722 carry forward)
1 (new) $50,000 Guatemala, Peru, Bolivia, DR, Paraguay
2 $75,000 (received as GH/HIDN core)
Bolivia, DR, Guatemala, Peru
3 *$0 ($17,271 carry forward)
LAC BUREAU
4 $0 1 (new) $300,000 Mauritania, Cameroon 2 $300,000 Cameroon, one new
country TBD 3 $300,000 Cameroon, Mauritania,
Togo, Niger
USAID/WEST AFRICA
4 $0 (carry forward) Cameroon, Mauritania, Togo, Niger

52
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
AN
NEX
E: H
IDN
RES
ULT
S PA
THW
AYS
REP
OR
T A
ND
O
P IN
DIC
ATO
RS
MA
TER
NA
L H
EALT
H P
ATH
WA
YS
Ski
lled
Car
e at
Del
iver
y M
ater
nal m
orta
lity
ratio
s ref
lect
the
wid
est d
ispa
rity
in h
uman
dev
elop
men
t ind
icat
ors b
etw
een
deve
lope
d an
d de
velo
ping
cou
ntrie
s and
bet
wee
n th
e ric
h an
d th
e po
or w
ithin
cou
ntrie
s. Ea
ch y
ear m
ore
than
500
,000
wom
en d
ie d
ue to
com
plic
atio
ns o
f pre
gnan
cy a
nd c
hild
birth
. Ano
ther
15
to 2
0 m
illio
n w
omen
suff
er d
irect
and
long
-term
dis
abili
ties t
hat a
re e
asily
pre
vent
ed if
safe
del
iver
y ca
re is
pro
vide
d to
the
maj
ority
of c
hild
bear
ing
and
refe
rral
to sp
ecia
lized
leve
l of c
are
to a
smal
l per
cent
age
who
dev
elop
com
plic
atio
ns. T
he m
ajor
dire
ct c
ause
s of m
ater
nal m
orta
lity
are:
hem
orrh
age,
hy
perte
nsiv
e di
sord
ers,
infe
ctio
n, a
borti
on, o
bstru
cted
labo
r and
ane
mia
. Man
y of
thes
e co
mpl
icat
ions
can
be
prev
ente
d or
app
ropr
iate
ly m
anag
ed if
a
skill
ed b
irth
atte
ndan
t (SB
A) i
s con
duct
ing
the
deliv
ery
at a
faci
lity
or a
t hom
e. S
kille
d bi
rth a
ttend
ant (
SBA
) is d
efin
ed a
s a h
ealth
pro
vide
r with
m
edic
al tr
aini
ng su
ch a
s a d
octo
r, m
idw
ife o
r nur
se. T
hese
skill
ed in
divi
dual
s req
uire
the
man
date
, com
mod
ities
, dru
gs a
nd e
quip
men
t to
prov
ide
skill
ed c
are.
USA
ID is
supp
ortin
g po
lices
, stra
tegi
es a
nd p
rogr
ams t
hat p
rom
ote
safe
del
iver
y by
skill
ed b
irth
atte
ndan
ts, a
s wel
l as i
mm
edia
te
post
partu
m c
are.
Bec
ause
of t
he st
agna
nt o
r inc
reas
ing
mat
erna
l mor
ality
ratio
s in
Afr
ica,
USA
ID w
ill fo
cus i
ts a
ctiv
ities
to a
ddre
ss th
is p
robl
em
parti
cula
rly in
Afr
ican
cou
ntrie
s. 1.
Re
sear
ch to
ana
lyze
glo
bal d
ata
to g
uide
pro
gram
min
g; to
ass
ess n
ew in
terv
entio
ns a
nd d
ocum
ent e
ffec
tiven
ess a
nd c
ost e
ffec
tiven
ess o
f sel
ecte
d st
rate
gies
; to
addr
ess r
emai
ning
cha
lleng
es, i
nclu
ding
hum
an re
sour
ces c
onst
rain
ts, f
inan
cial
bar
riers
and
equ
ity g
aps t
o se
rvic
e ut
iliza
tion
and
in
parti
cula
r SB
A u
se b
y th
e m
argi
naliz
ed a
nd u
nder
serv
ed w
omen
.

53
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
AC
TIVI
TY T
ITLE
EX
PEC
TED
RES
ULT
EN
D
DA
TE
IND
ICA
TOR
ST
ATU
S D
UR
ING
FIS
CA
L YE
AR
(F
Y08
REF
ERS
TO R
ESU
LTS
AC
CO
MPL
ISH
ED D
UR
ING
FY0
8 W
ITH
ALL
R
ESO
UR
CES
); FY
09 T
AR
GET
REF
ERS
TO
RES
ULT
S PL
AN
NED
TO
BE
AC
CO
MPL
ISH
ED D
UR
ING
10/
1/08
–9/3
0/09
W
ILL
ALL
RES
OU
RC
ES
NA
RR
ATI
VE
PAR
AG
RA
PH
FY08
Res
ults
FY
09 T
arge
t A
sses
smen
t of
mat
erni
ty c
are
and
birth
out
com
es
D
irect
cau
ses
of m
ater
nal
mor
talit
y (M
M)
Pe
rinat
al a
nd n
eona
tal
mor
talit
y
MM
glo
bal e
stim
ates
Impa
ct o
f ces
area
n se
ctio
n
Phys
ical
, psy
chol
ogic
al
and
econ
omic
co
nseq
uenc
e of
mor
talit
y an
d m
orbi
dity
Impa
ct o
f FP
on
MM
FY06
FY
06
FY07
FY
07
FY08
/09
FY 0
7
Com
plet
ed
Com
plet
ed
Ong
oing
O
ngoi
ng
Ong
oing
Mat
erna
l mor
talit
y m
easu
rem
ent t
ools
Sam
plin
g at
ser
vice
site
(S
SS
) to
mea
sure
MM
RA
PID
to m
easu
re M
M in
fa
cilit
ies
V
erba
l aut
opsy
FY08
FY
08
FY08
Ong
oing
O
ngoi
ng
Ong
oing
Impl
emen
tatio
n ap
proa
ches
Qua
lity
impr
ovem
ent
colla
bora
tives
Con
tinui
ty a
nd q
ualit
y of
ca
re
Fi
nanc
ing
FY08
FY
09
FY 0
9
Ong
oing
O
ngoi
ng
Ong
oing

54
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
2.
Intr
oduc
tion
and
expa
nsio
n of
pro
ven
inte
rven
tions
incl
udes
tech
nica
l lea
ders
hip,
adv
ocac
y an
d po
licy
dial
ogue
with
MO
H a
nd M
issi
ons t
o en
sure
safe
birt
h pr
omot
ing
use
of p
rove
n in
terv
entio
ns, s
uch
as c
lean
del
iver
y, u
se o
f the
par
togr
aph,
etc
., by
SB
As t
o ad
dres
s the
maj
or d
irect
ca
uses
of m
ater
nal d
eath
. Int
rodu
ctio
n in
cou
ntrie
s whi
ch h
ave
wea
k m
ater
nal h
ealth
serv
ices
will
focu
s on
one
dist
rict (
at le
ast 2
0% o
f po
pula
tion
or fa
cilit
ies)
. Exp
ansi
on is
def
ined
as m
ovin
g be
yond
one
dis
trict
and
cov
erin
g 20
% o
f the
pop
ulat
ion
in a
dis
trict
/sta
te/c
ount
ry. S
BA
is
an
indi
cato
r cap
ture
d by
DH
S. A
ttem
pt w
ill a
lso
be m
ade
to c
aptu
re d
ata
at th
e di
stin
ct/p
rovi
sion
al le
vel w
here
USA
ID p
artn
ers a
re a
ctiv
e.
Als
o se
e th
e pa
thw
ay o
n pr
even
tion
of p
ostp
artu
m h
emor
rhag
e.
A
CTI
VITY
TIT
LE
EXPE
CTE
D
RES
ULT
EN
D
DA
TE
IND
ICA
TOR
ST
ATU
S D
UR
ING
FIS
CA
L YE
AR
(F
Y08
REF
ERS
TO R
ESU
LTS
AC
CO
MPL
ISH
ED D
UR
ING
FY0
8 W
ITH
A
LL R
ESO
UR
CES
); FY
09
TAR
GET
R
EFER
S TO
RES
ULT
S PL
AN
NED
TO
B
E A
CC
OM
PLIS
HED
DU
RIN
G
10/1
/08–
9/30
/09
WIL
L AL
L R
ESO
UR
CES
NA
RR
ATI
VE P
AR
AG
RA
PH
FY08
RES
ULT
S FY
09 T
AR
GET
Te
chni
cal l
eade
rshi
p an
d pa
rtner
ship
to a
dvan
ce
SB
A a
ctiv
ities
at a
co
untry
leve
l
Tool
s di
ssem
inat
ed
& p
artn
ersh
ip w
ith
FBO
s, P
MN
CH
&
WR
A to
initi
ate
coun
try le
vel S
BA
ac
tiviti
es
FY08
co
mpl
eted
C
ompl
eted
P
roje
ct c
lose
-out
D
ocum
ents
sha
red
with
par
tner
s an
d its
us
e ex
pend
ed th
roug
h FB
Os,
WR
A an
d ot
her p
artn
ers.
W
ider
dis
sem
inat
ion
of d
ocum
ents
and
pr
ogra
mm
atic
less
ons
lear
nt w
ill b
e sh
ared
at t
he p
roje
ct c
lose
-out
mee
tings
. In
trodu
ctio
n of
in
terv
entio
ns fo
r ski
lled
birth
atte
ndan
ce th
roug
h E
ssen
tial M
ater
nal a
nd
New
born
Hea
lth (E
MN
H)
SB
A in
trodu
ced
in
7 co
untri
es (a
t le
ast 2
0% in
one
di
stric
t)
FY09
O
n-go
ing
9 (Cor
e: G
hana
, Ind
ia,
Tanz
ania
, Eth
iopi
a)
(Fie
ld: H
aiti,
C
amer
oon,
M
aurit
ania
, Nig
er,
Ethi
opia
, Tog
o)
3 (Gha
na, I
ndia
, E
thio
pia)
AC
CE
SS
had
fiel
d su
ppor
t fun
ds fo
r PA
C
from
the
PR
H O
ffice
thro
ugh
Dec
. 31,
20
07.
Expa
nsio
n of
ski
lled
birth
at
tend
ance
in c
ount
ries
SB
A e
xpan
ded
in 3
co
untri
es th
roug
h pr
e-se
rvic
e tra
inin
g
FY09
O
n-go
ing
4 (Fie
ld: M
alaw
i, Ta
nzan
ia, N
iger
ia,
Afg
hani
stan
)
7 (Fie
ld: M
alaw
i, Ta
nzan
ia,
Eth
iopi
a,
Nig
eria
,Gha
na,
Indi
a,
Afg
hani
stan
)
Mis
sion
fund
s ex
pand
ed a
ctiv
ities
in
Tanz
ania
, Mal
awi,
Nig
eria
, Afg
hani
stan
. A
ctiv
ities
will
expa
nd to
nat
iona
l lev
el in
G
hana
and
sta
te le
vel i
n In
dia
usin
g ot
her
non-
AC
CE
SS
reso
urce
s.
Pre
-ser
vice
trai
ning
pic
ked
up b
y M
issi
on
fund
ing
in M
alaw
i, Ta
nzan
ia, a
nd E
thio
pia.
Saf
e B
irth
Afri
ca In
itiat
ive
(SB
AI)
Focu
s in
1 A
frica
n co
untri
es to
in
crea
se S
BA a
nd
cove
rage
with
pr
oven
inte
rven
tions
FY09
O
n-go
ing
1 (Rw
anda
) 1 (R
wan
da)
Incl
ude
natio
nal-l
evel
sup
porti
ve a
ctiv
ities
fo
r SB
A a
nd fo
cuse
d ac
tiviti
es in
4 d
istri
cts
cont
inui
ng.
Ant
enat
al C
are
Pat
hway

55
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
Whi
le a
nten
atal
car
e (A
NC
) atte
ndan
ce h
as b
een
risin
g sl
owly
thro
ugho
ut th
e w
orld
, it r
emai
ns q
uite
low
in A
sia.
Mos
t pre
gnan
t wom
en in
Asi
a an
d A
fric
a do
not
mak
e th
e re
com
men
ded
min
imal
num
ber o
f ant
enat
al v
isits
(4 v
isits
). Q
ualit
y an
tena
tal c
are
(AN
C) i
mpr
oves
mat
erna
l hea
lth a
nd h
elps
to
pro
mot
e he
alth
y ou
tcom
es fo
r wom
en a
nd n
ewbo
rns.
Ant
enat
al c
are
(AN
C) c
an a
ssis
t in
early
det
ectio
n of
obs
tetri
c co
mpl
icat
ions
and
med
ical
pr
oble
ms e
xace
rbat
ed b
y pr
egna
ncy.
It is
a k
ey e
ntry
poi
nt fo
r pre
gnan
t wom
en to
rece
ive
a br
oad
rang
e of
pre
vent
ive
heal
th se
rvic
es in
clud
ing
nutri
tion
supp
lem
enta
tion;
pre
vent
ion
and
treat
men
t of m
alar
ia, H
IV/A
IDS,
syph
ilis;
and
teta
nus t
oxoi
d im
mun
izat
ion;
and
cou
nsel
ing
abou
t use
of a
sk
illed
birt
h at
tend
ant.
GH
will
exp
and
prog
ram
s to
stre
ngth
en fo
cuse
d an
tena
tal c
are
that
pro
vide
ass
essm
ent a
nd a
ctio
n to
pro
vide
car
e fo
r eac
h w
oman
’s in
divi
dual
situ
atio
n—ta
king
into
con
side
ratio
n th
e ex
istin
g co
untry
spec
ific
prev
alen
ce o
f inf
ectio
ns, s
uch
as m
alar
ia a
nd H
IV/A
IDS
for
mal
aria
in p
regn
ancy
(MIP
) and
pre
vent
ion
of m
ater
nal-t
o-ch
ild-tr
ansm
issi
on o
f HIV
(PM
TCT)
pro
gram
s. 3.
R
esea
rch
to a
sses
s the
eff
ectiv
enes
s of m
icro
nutri
ents
supp
lem
enta
tion
and
nutri
tiona
l app
roac
hes o
n ne
onat
al a
nd m
ater
nal s
urvi
val.
A
CTI
VITY
TIT
LE
EXPE
CTE
D
RES
ULT
EN
D
DA
TE
IND
ICA
TOR
ST
ATU
S D
UR
ING
FIS
CAL
YEA
R (F
Y08
REF
ERS
TO R
ESU
LTS
AC
CO
MPL
ISH
ED D
UR
ING
FY0
8 W
ITH
ALL
RES
OU
RC
ES);
FY 0
9 TA
RG
ET
REF
ERS
TO R
ESU
LTS
PLA
NN
ED T
O B
E A
CC
OM
PLIS
HED
DU
RIN
G 1
0/1/
08–9
/30/
09 W
ILL
ALL
RES
OU
RC
ES
NA
RR
ATI
VE P
AR
AG
RA
PH
FY08
Res
ults
FY
09 T
arge
t N
utrit
iona
l ap
proa
ches
for
neon
atal
/mat
erna
l he
alth
Effe
cts
of lo
w
dose
Vit
A o
n bi
rth
outc
omes
FY08
O
ngoi
ng

56
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
4.
Intro
duct
ion
and
expa
nsio
n w
ill in
clud
e ac
tiviti
es to
incr
ease
focu
sed
ante
nata
l car
e in
Afr
ican
cou
ntrie
s with
hig
h m
alar
ia a
nd H
IV/A
IDS
prev
alen
ce to
pre
vent
HIV
tran
smis
sion
from
mot
hers
to c
hild
. Stre
ngth
enin
g A
NC
will
be
part
of E
ssen
tial M
ater
nal a
nd N
ewbo
rn H
ealth
(E
MN
C) a
ctiv
ities
in m
ost t
arge
ted
coun
tries
.
AC
TIVI
TY T
ITLE
EX
PEC
TED
R
ESU
LT
END
D
ATE
IN
DIC
ATO
R
STA
TUS
DU
RIN
G F
ISC
AL
YEA
R
(FY0
8 R
EFER
S TO
RES
ULT
S A
CC
OM
PLIS
HED
DU
RIN
G F
Y08
WIT
H A
LL
RES
OU
RC
ES);
FY 0
9 TA
RG
ET R
EFER
S TO
R
ESU
LTS
PLA
NN
ED T
O B
E A
CC
OM
PLIS
HED
D
UR
ING
10/
1/08
–9/3
0/09
WIL
L A
LL
RES
OU
RC
ES
NA
RR
ATI
VE P
AR
AG
RA
PH
FY08
RES
ULT
S FY
09 T
AR
GET
P
rom
otio
n of
fo
cuse
d A
NC
with
W
HO
, IC
M, W
RA
an
d FB
Os
Dev
elop
men
t an
d di
ssem
inat
ion
of te
chni
cal
mat
eria
ls a
nd
prom
otio
n of
fo
cuse
d A
NC
at
coun
try le
vel
FY07
On-
goin
g C
ompl
eted
C
ore
fund
ing
supp
orte
d pa
rtner
s to
use
an
d di
ssem
inat
e te
chni
cal m
ater
ials
to
prom
ote
focu
sed
AN
C. M
ost
impl
emen
tatio
n is
cov
ered
by
field
sup
port
see
belo
w. M
alar
ia p
reve
ntio
n du
ring
preg
nanc
y is
a k
ey fo
cus
of A
NC
ac
tiviti
es.
Intro
duct
ion
of
focu
sed
AN
C
with
in E
MN
C
Focu
sed
AN
C
impl
emen
ted
in
3 co
untri
es
FY08
5 (Cor
e: In
dia)
(F
ield
: Rw
anda
, E
thio
pia,
RS
A, K
enya
)
4 (Cor
e: In
dia,
Mal
awi)
(Fie
ld: R
SA
, Ken
ya)
Cor
e O
HA
fund
s su
ppor
t int
egra
tion
of
PM
TCT
in F
AN
C in
Mal
awi.
PM
TCT
field
sup
port
fund
s us
ed in
Ken
ya
for F
Y08
.
Expa
nsio
n of
An
emia
pre
vent
ion
activ
ities
S
ee a
lso
the
nutri
tion
path
way
s
Scal
e up
an
emia
pr
even
tion
activ
ities
in o
ne
coun
try
FY08
4 (Fie
ld: M
alaw
i, N
iger
ia,
Tanz
ania
, Afg
hani
stan
)
5 (Fie
ld: M
alaw
i, N
iger
ia,
Tanz
ania
, Afg
hani
stan
, R
wan
da)
Mis
sion
fund
ing
FAN
C in
clud
ed in
Mal
awi R
H s
tand
ards
Expa
nsio
n of
fo
cuse
d A
NC
in
Tanz
ania
All A
NC
se
rvic
es
upgr
aded
with
M
IP a
nd
PMTC
T na
tion
wid
e
FY09
On-
goin
g O
ngoi
ng
Mis
sion
fund
ing

57
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
Pre
vent
ion
of P
ostp
artu
m H
emor
rhag
e P
athw
ay
Seve
re b
leed
ing
is th
e si
ngle
mos
t im
porta
nt c
ause
of m
ater
nal d
eath
wor
ldw
ide.
Ove
r 30%
of a
ll m
ater
nal d
eath
s are
due
to h
emor
rhag
e in
Asi
a an
d A
fric
a. A
n es
timat
ed 1
4 m
illio
n ca
ses o
f sev
ere
post
partu
m h
emor
rhag
e (P
PH) o
ccur
eve
ry y
ear w
ith a
cas
e fa
talit
y ra
te o
f app
roxi
mat
ely
1%
(140
,000
dea
ths)
. Ute
rine
aton
y ac
coun
ts fo
r 70–
90%
of a
ll PP
H c
ases
; act
ive
man
agem
ent o
f the
third
stag
e of
labo
r (A
MTS
L) is
an
evid
ence
-bas
ed,
feas
ible
, low
-cos
t int
erve
ntio
n th
at c
an p
reve
nt 6
0 pe
rcen
t of u
terin
e at
ony
that
lead
s to
hem
orrh
age
and
mat
erna
l dea
th.
1.
Res
earc
h to
dev
elop
a si
mpl
e sy
ringe
mec
hani
sm to
del
iver
a u
tero
toni
c dr
ug (o
xyto
cin)
in a
pre
-fill
ed d
evic
e (U
nije
ct),
a m
ulti-
coun
try su
rvey
to
dete
rmin
e th
e co
vera
ge o
f AM
TSL
prac
tice,
and
com
paris
on o
f the
rela
tive
impa
ct o
f oxy
toci
n ve
rsus
con
trolle
d co
rd tr
actio
n.
A
CTI
VITY
TIT
LE
EXPE
CTE
D R
ESU
LT
END
D
ATE
IN
DIC
ATO
R
STA
TUS
DU
RIN
G F
ISC
AL
YEA
R (F
Y08
REF
ERS
TO R
ESU
LTS
AC
CO
MPL
ISH
ED
DU
RIN
G F
Y08
WIT
H A
LL R
ESO
UR
CES
); FY
09
TAR
GET
REF
ERS
TO R
ESU
LTS
PLA
NN
ED T
O B
E A
CC
OM
PLIS
HED
D
UR
ING
10/
1/08
-9/3
0/09
WIL
L A
LL
RES
OU
RC
ES
NA
RR
ATI
VE
PAR
AG
RA
PH
FY08
RES
ULT
S FY
09 T
AR
GET
O
xyto
cin
in U
nije
ct d
evel
opm
ent
Oxy
toci
n in
Uni
ject
av
aila
ble
for f
ield
tria
l, pi
lots
, and
co
mm
erci
aliz
atio
n
FY09
O
n-go
ing
Glo
bal s
urve
y of
AM
TSL
prac
tices
C
over
age
of A
MTS
L pr
actic
es a
sses
sed
and
diss
emin
ated
in 1
0 co
untri
es
FY08
C
ompl
eted
8
coun
tries
Feas
ibilit
y of
usi
ng c
omm
unity
m
idw
ives
(mat
rone
s) to
adm
inis
ter
Oxy
toci
n in
Unj
iect
Feas
ibilit
y of
usi
ng
com
mun
ity m
idw
ives
to
adm
inis
ter O
xyto
cin
in
Uni
ject
dem
onst
rate
d in
Se
nega
l
FY09
C
ontin
uing
Com
paris
on o
f rel
ativ
e ef
fect
iven
ess
of th
ree
AM
TSL
com
pone
nts
Rel
ativ
e ef
fect
iven
ess
of
oxyt
ocin
vs.
con
trolle
d co
rd
tract
ion
clar
ified
for f
utur
e pr
ogra
m e
mph
asis
FY 0
9 Pl
anni
ng

58
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
2.
Intro
duct
ion
and
expa
nsio
n w
ill in
clud
e te
chni
cal l
eade
rshi
p in
mob
ilizi
ng M
issi
on su
ppor
t for
pre
vent
ion
of P
PH p
reve
ntio
n pr
ogra
ms;
ass
istin
g M
issi
ons w
ith th
e in
trodu
ctio
n an
d ex
pans
ion
of P
PH in
terv
entio
ns in
a to
tal o
f 29
coun
tries
(exp
ansi
on in
10
coun
tries
by
FY 2
008
(’07
fund
s).
A
CTI
VITY
TI
TLE
EXPE
CTE
D
RES
ULT
EN
D
DA
TE
IND
ICA
TOR
ST
ATU
S D
UR
ING
FIS
CA
L YE
AR
(FY0
8 R
EFER
S TO
RES
ULT
S A
CC
OM
PLIS
HED
D
UR
ING
FY0
8 W
ITH
ALL
RES
OU
RC
ES);
FY 0
9 TA
RG
ET R
EFER
S TO
RES
ULT
S PL
AN
NED
TO
BE
AC
CO
MPL
ISH
ED
DU
RIN
G 1
0/1/
08-9
/30/
09 W
ILL
ALL
R
ESO
UR
CES
NA
RR
ATI
VE P
AR
AG
RA
PH
FY08
Res
ults
FY
09 T
arge
t In
crea
sed
awar
enes
s of
AM
TSL
stan
dard
s in
25
coun
tries
FY06
New
glo
bal p
olic
y fo
r com
mun
ity-
base
d P
PH
FY06
Glo
bal a
nd
coun
try p
olic
ies
for P
PH
in m
id
and
low
-reso
urce
se
tting
s
FY09
Tech
nica
l le
ader
ship
Impr
oved
sys
tem
s fo
r ute
roto
nics
FY
09
On-
goin
g O
n-go
ing
Pro
ject
clo
se-o
ut
Con
tribu
tion
to re
gion
al a
nd n
atio
nal l
evel
m
eetin
gs a
nd P
OP
PH
I wor
king
gro
ups.
W
ider
dis
sem
inat
ion
of d
ocum
ents
and
pr
ogra
mm
atic
less
ons
lear
nt w
ill b
e sh
ared
at
clos
e-ou
t mee
tings
.
Intro
duct
ion
of
PP
H p
reve
ntio
n pr
ogra
ms
into
co
untri
es
PP
H p
rogr
ams
intro
duce
d in
at
leas
t 17
focu
s co
untri
es (a
t lea
st
25%
of f
acilit
ies
in
one
dist
rict)
FY09
O
n-go
ing
10
(Cor
e: G
hana
, Ind
ia,
DR
C, T
anza
nia,
E
thio
pia,
Ken
ya)
(Fie
ld: C
amer
oon,
M
aurit
ania
, N
iger
,Tog
o, E
thio
pia)
4 (Cor
e: G
hana
, In
dia,
Eth
iopi
a)
(Fie
ld, K
enya
)
Pilo
t act
iviti
es in
itiat
ed b
y co
re fu
nds.
M
issi
on fu
nds
thou
gh A
CC
ES
S o
r oth
er
bila
tera
l are
exp
andi
ng P
PH
act
iviti
es.
Gha
na a
nd E
thio
pia
will
con
tinue
to re
ceiv
e co
re p
rese
rvic
e fu
nds.
K
enya
will
intro
duce
PP
H a
t pro
vinc
ial l
evel
th
roug
h A
ssoc
iate
Aw
ard.
Ex
pans
ion
of
PP
H p
reve
ntio
n pr
ogra
ms
in
coun
tries
PP
H p
reve
ntio
n pr
ogra
ms
expa
nded
in 1
0 co
untri
es
(20%
of f
acili
ties
in c
ount
ry)
FY09
O
n-go
ing
4 (Cor
e: R
wan
da)
(Fie
ld: M
alaw
i, N
iger
ia, A
fgha
nist
an)
8 (Cor
e: R
wan
da),
(Fie
ld: A
fgha
nist
an,
Nig
eria
, Eth
iopi
a,
Mal
awi,
Tanz
ania
, In
dia,
Gha
na,)
Act
iviti
es w
ill e
xpan
d to
nat
iona
l lev
el in
Gha
na
and
stat
e le
vel i
n In
dia
usin
g ot
her n
on-
AC
CE
SS
reso
urce
s.

59
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
New
born
Hea
lth P
athw
ay
Each
yea
r, ap
prox
imat
ely
4 m
illio
n ne
wbo
rns d
ie w
ithin
the
first
mon
th o
f life
acc
ount
ing
for o
ver 6
0% o
f inf
ant m
orta
lity
and
alm
ost 4
0% o
f dea
ths
amon
g ch
ildre
n un
der f
ive
year
s of a
ge. M
ost n
eona
tal d
eath
s are
cau
sed
dire
ctly
by
infe
ctio
ns (3
6%) a
nd lo
w b
irth
wei
ght i
s the
mos
t im
porta
nt in
dire
ct
caus
e of
dea
th w
ith 6
0 to
80%
of n
eona
tal d
eath
s occ
urrin
g am
ong
new
born
s tha
t are
bor
n to
o sm
all.
Prio
rity
mus
t be
plac
ed o
n ho
me-
and
com
mun
ity-
base
d ap
proa
ches
bec
ause
a la
rge
maj
ority
of b
irths
occ
ur a
t hom
e an
d ca
n be
pre
vent
ed a
nd m
anag
ed a
t hom
e. A
n ad
ditio
nal c
onsid
erat
ion
in th
e A
frica
n co
ntex
t is t
hat o
ver h
alf a
mill
ion
new
born
s are
infe
cted
by
the
HIV
viru
s ann
ually
thro
ugh
mot
her-t
o-ch
ild- t
rans
miss
ion
(MTC
T). T
he u
ptak
e of
pre
vent
ion
of m
othe
r-to-
child
tran
smiss
ion
of H
IV (P
MTC
T) c
ontin
ues t
o be
lim
ited,
rang
ing
from
1%
to 1
0% in
sub-
Saha
ran
Afr
ica.
The
rela
tivel
y hi
gh a
nten
atal
car
e co
vera
ge in
Afri
ca (o
ver 7
5% fo
r one
visi
t) an
d sk
illed
birt
h at
tend
ance
(45%
) pro
vide
an
exce
llent
pla
tform
for s
calin
g up
PM
TCT
if th
e tw
o pr
ogra
ms a
re b
ette
r lin
ked.
1.
R
esea
rch
to a
sses
s pro
gram
feas
ibili
ty a
nd e
ffec
tiven
ess o
f com
mun
ity b
ased
Ess
entia
l New
born
Car
e (c
lean
del
iver
y an
d co
rd c
are,
war
mth
, ea
rly a
nd e
xclu
sive
bre
astfe
edin
g, a
nd e
arly
reco
gniti
on a
nd re
ferr
al fo
r com
plic
atio
ns);
com
mun
ity b
ased
infe
ctio
n m
anag
emen
t (ho
me-
base
d po
stna
tal c
are,
Chl
orhe
xidi
ne fo
r cor
d ca
re, s
impl
ified
ant
ibio
tic re
gim
en);
new
born
car
e an
d PM
TC
T in
tegr
atio
n; a
nd n
ewbo
rn te
chno
logy
de
velo
pmen
t (G
enta
mic
in in
Uni
ject
, Chl
orhe
xidi
ne, R
esus
cita
tion
devi
ce).
A
CTI
VITY
TIT
LE
EXPE
CTE
D
RES
ULT
EN
D D
ATE
IN
DIC
ATO
R
STA
TUS
DU
RIN
G F
ISC
AL Y
EAR
(FY0
8 R
EFER
S TO
RES
ULT
S A
CC
OM
PLIS
HED
DU
RIN
G F
Y08
WIT
H A
LL R
ESO
UR
CES
); FY
09
TAR
GET
R
EFER
S TO
RES
ULT
S PL
AN
NED
TO
BE
AC
CO
MPL
ISH
ED D
UR
ING
10/
1/08
-9/3
0/09
WIL
L A
LL R
ESO
UR
CES
NA
RR
ATI
VE
PAR
AG
RA
PH
FY08
RES
ULT
S FY
09 T
AR
GET
C
omm
unity
bas
ed E
NC
in
Ban
glad
esh
Pro
gram
fe
asib
ility
of
com
mun
ity b
ased
EN
C
dem
onst
rate
d
FY06
C
ompl
eted
in
2006
Com
mun
ity b
ased
in
fect
ion
prev
entio
n an
d m
anag
emen
t:
Chl
orhe
xidi
ne (J
HU
, B’
desh
)
Mul
ti-ce
nter
sep
sis
(WH
O &
BU
)
Stan
dby-
by
antib
iotic
&
resu
scita
tion
(BU
, Za
mbi
a)
G
enta
mic
in in
Uni
ject
Effe
ctiv
enes
s &
pr
ogra
m fe
asib
ility
dem
onst
rate
d
FY09
C
HX:
C
ontin
uing
S
epsi
s:
plan
ning
Za
mbi
a:
Con
tinui
ng
Gen
ta: p
lann
ing
New
born
tech
nolo
gy
G
enta
mic
in in
U
nije
ct
FY09
G
enta
: sta
rted

60
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
AC
TIVI
TY T
ITLE
EX
PEC
TED
R
ESU
LT
END
DA
TE
IND
ICA
TOR
ST
ATU
S D
UR
ING
FIS
CAL
YEA
R (F
Y08
REF
ERS
TO R
ESU
LTS
AC
CO
MPL
ISH
ED D
UR
ING
FY0
8 W
ITH
ALL
RES
OU
RC
ES);
FY 0
9 TA
RG
ET
REF
ERS
TO R
ESU
LTS
PLA
NN
ED T
O B
E A
CC
OM
PLIS
HED
DU
RIN
G 1
0/1/
08-9
/30/
09 W
ILL
ALL
RES
OU
RC
ES
NA
RR
ATI
VE
PAR
AG
RA
PH
avai
labl
e fo
r fie
ld tr
ial
D
eliv
ery
mec
hani
sm
for C
HX
deve
lope
d
Use
of
resu
scita
tion
devi
ces
eval
uate
d in
In
dia
and
mor
e w
idel
y av
aila
ble
in
Afri
ca
S
epsi
s sc
reen
ing
land
scap
e an
alys
is
FY08
CH
X: s
tarte
d
Res
us:
cont
inui
ng
Sep
sis
scr.
tool
an
alys
is:
com
plet
ed
Met
a-an
alys
is o
f glo
bal
new
born
dat
a (3
0 co
untri
es)
Glo
bal s
tatu
s of
ne
wbo
rn c
are
asse
ssed
FY06
C
ompl
eted

61
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
2.
Intr
oduc
tion
and
expa
nsio
n w
ill in
clud
e te
chni
cal l
eade
rshi
p in
mob
ilizi
ng M
issi
on su
ppor
t for
new
born
hea
lth p
rogr
ams;
ass
istin
g M
issi
ons
with
the
intro
duct
ion
and
expa
nsio
n of
new
born
inte
rven
tions
in a
tota
l of 2
7 co
untri
es (1
8 in
trodu
ctio
n an
d 9
expa
nsio
n) b
y 20
08
A
CTI
VITY
TIT
LE
EXPE
CTE
D R
ESU
LT
END
DA
TE
IND
ICA
TOR
ST
ATU
S D
UR
ING
FIS
CA
L YE
AR
(F
Y08
REF
ERS
TO R
ESU
LTS
AC
CO
MPL
ISH
ED D
UR
ING
FY0
8 W
ITH
ALL
RES
OU
RC
ES);
FY 0
9 TA
RG
ET R
EFER
S TO
RES
ULT
S PL
AN
NED
TO
BE
AC
CO
MPL
ISH
ED
DU
RIN
G 1
0/1/
08–9
/30/
09 W
ILL
ALL
R
ESO
UR
CES
NA
RR
ATI
VE P
AR
AG
RA
PH
FY08
RES
ULT
S FY
09 T
AR
GET
Te
chni
cal
lead
ersh
ip
Tech
nica
l gui
delin
es
and
mat
eria
ls
deve
lope
d
FY09
O
n-go
ing
9 co
untri
es
(Rw
anda
, Nig
eria
, M
alaw
i, C
ambo
dia,
Indi
a,
Afgh
anis
tan,
N
epal
, Eth
iopi
a Ba
ngla
desh
)
Pro
ject
clo
se-o
ut
Wid
er d
isse
min
atio
n of
doc
umen
ts a
nd
prog
ram
mat
ic le
sson
s le
arnt
will
be
shar
ed a
t the
pro
ject
clo
se-o
ut m
eetin
gs
Intro
duct
ion
of
new
born
car
e in
to
coun
tries
EN
C in
trodu
ced
in a
t le
ast 1
2 ne
w c
ount
ries
(at l
east
3 d
istri
cts)
FY09
O
n-go
ing
9 (Cor
e: In
dia,
G
hana
, Ta
nzan
ia,
Eth
iopi
a, K
enya
) (F
ield
:, M
aurit
ania
, To
go, N
iger
, C
amer
oon,
E
thio
pia)
4 (Cor
e: In
dia,
G
hana
, Eth
iopi
a)
(Fie
ld: K
enya
)
Ken
ya: A
t pro
vinc
ial l
evel
thro
ugh
Ass
ocia
te A
war
d in
FY
09.
Expa
nsio
n of
ne
wbo
rn c
are
in
coun
tries
ENC
exp
ande
d in
9
new
cou
ntrie
s (>
3 di
stric
t)
FY09
O
n-go
ing
7 (Cor
e: R
wan
da,
Nep
al)
(Fie
ld: N
iger
ia,
Ban
glad
esh,
A
fgha
nist
an,
Cam
bodi
a,
Mal
awi)
10
(Cor
e: R
wan
da)
(Fie
ld: E
thio
pia,
N
iger
ia,
Ban
glad
esh,
A
fgha
nist
an,
Mal
awi,
Cam
bodi
a,
Tanz
ania
, Ind
ia,
Gha
na)
Cor
e fu
nds
in R
wan
da. A
ctiv
ities
will
ex
pand
to n
atio
nal l
evel
in G
hana
and
st
ate
leve
l in
Indi
a us
ing
othe
r non
-A
CC
ES
S re
sour
ces.
Th
roug
h M
issi
on fu
ndin
g in
Nig
eria
, B
angl
ades
h, A
fgha
nist
an, C
ambo
dia,
an
d M
alaw
i, Ta
nzan
ia a
nd E
thio
pia.

62
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
OP
IND
ICA
TOR
S
MA
TER
NA
L A
ND
CH
ILD
HEA
LTH
08
targ
et, t
o be
ach
ieve
d w
ith a
ll fu
nds,
as
of 9
/30/
08
(as
set i
n N
ovem
ber,
2007
PR
)
08 a
ctua
l, ac
hiev
ed w
ith
all f
unds
, as
of
9/30
/08
(as
repo
rted
in
Dec
embe
r, 20
08 P
R)
Expl
anat
ion:
1,0
00 c
hara
cter
text
bo
x (p
er in
dica
tor)
requ
ired
to
expl
ain
devi
atio
n (1
0%) w
hen
targ
ets
are
not m
et, t
arge
ts a
re
sign
ifica
ntly
exc
eede
d, o
r whe
n dr
oppi
ng a
n in
dica
tor.
Dro
p-do
wn
incl
udes
: a) s
hift
in p
rogr
amm
ing
emph
asis
; b) u
nexp
ecte
d pr
ogra
m
impl
emen
tatio
n de
lays
; c) h
ost
gove
rnm
ent e
nviro
nmen
t; d)
late
ar
rival
of p
rogr
amm
ing
fund
s; e
) dr
oppi
ng in
dica
tor;
or f
) oth
er.
09 ta
rget
, to
be
achi
eved
w
ith a
ll fu
nds,
as
of 9
/30/
09
(as
set i
n D
ecem
ber,
2008
PR
)
2010
ta
rget
, to
be
achi
eved
w
ith a
ll fu
nds,
as
of 9
/30/
10
(as
set i
n D
ecem
ber,
2008
PR
)
DQ
A:
Dat
e D
QA
was
co
mpl
ete
d fo
r thi
s in
dica
tor
Num
ber o
f peo
ple
train
ed in
re
sear
ch w
ith U
SG
assi
stan
ce
3,90
0
Num
ber o
f po
stpa
rtum
/new
born
vis
its
with
in 3
day
s of
birt
h in
U
SG
-ass
iste
d pr
ogra
ms
80,0
00
818
Gha
na, I
ndia
Num
ber o
f ant
enat
al c
are
(AN
C) v
isits
by
skill
ed
prov
ider
s fro
m U
SG
-as
sist
ed fa
cilit
ies
210,
000
5,85
0 In
dia
Num
ber o
f peo
ple
train
ed
in m
ater
nal/
new
born
he
alth
thro
ugh
US
G-
supp
orte
d pr
ogra
ms*
65,0
00
7,27
6 A
ctua
l exc
eeds
targ
et s
ince
AC
CE
SS
-su
ppor
ted
e-le
arni
ng c
ours
es g
rant
ed
mor
e ce
rtific
ates
than
ant
icip
ated
whe
n th
e ta
rget
s w
ere
set a
nd m
ore
mah
ila m
anda
l le
ader
s pa
rtici
pate
d in
trai
ning
s as
par
t of
the
Indi
a ac
tiviti
es th
an a
ntic
ipat
ed
Num
ber o
f del
iver
ies
with
a
skille
d bi
rth a
ttend
ant (
SB
A)
in U
SG
-ass
iste
d pr
ogra
ms
110,
000
12,8
79 G
hana
, R
wan
da, I
ndia
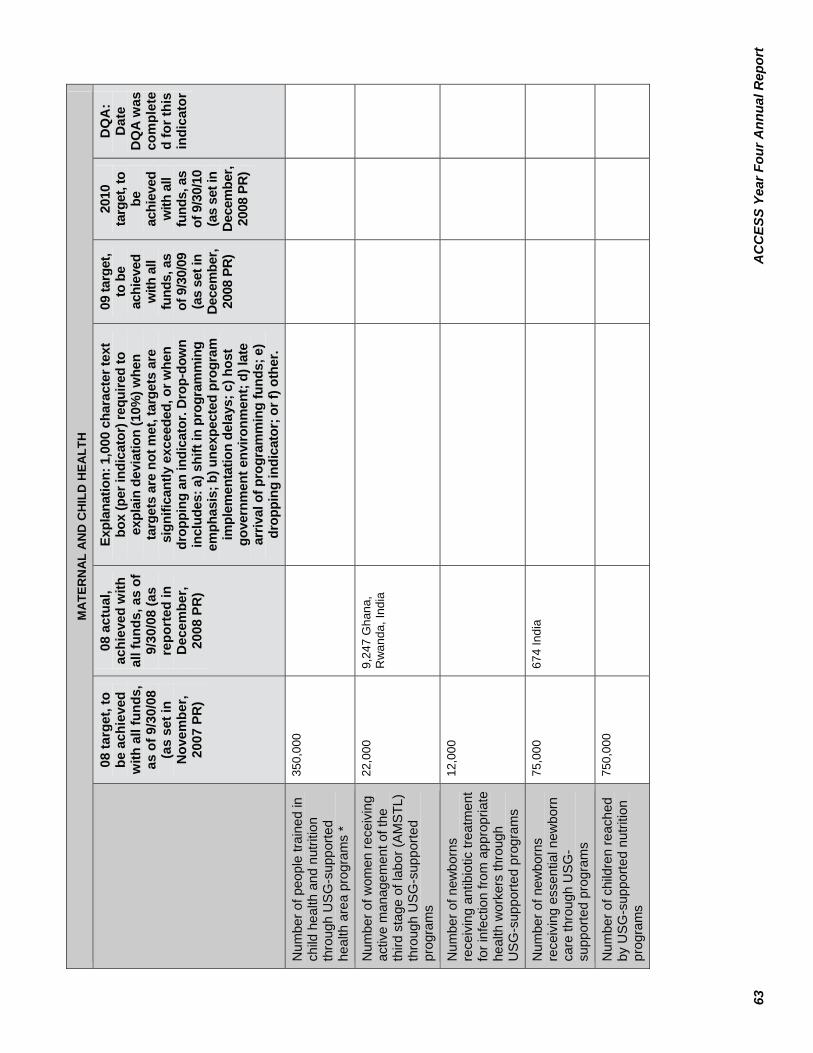
63
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
MA
TER
NA
L A
ND
CH
ILD
HEA
LTH
08
targ
et, t
o be
ach
ieve
d w
ith a
ll fu
nds,
as
of 9
/30/
08
(as
set i
n N
ovem
ber,
2007
PR
)
08 a
ctua
l, ac
hiev
ed w
ith
all f
unds
, as
of
9/30
/08
(as
repo
rted
in
Dec
embe
r, 20
08 P
R)
Expl
anat
ion:
1,0
00 c
hara
cter
text
bo
x (p
er in
dica
tor)
requ
ired
to
expl
ain
devi
atio
n (1
0%) w
hen
targ
ets
are
not m
et, t
arge
ts a
re
sign
ifica
ntly
exc
eede
d, o
r whe
n dr
oppi
ng a
n in
dica
tor.
Dro
p-do
wn
incl
udes
: a) s
hift
in p
rogr
amm
ing
emph
asis
; b) u
nexp
ecte
d pr
ogra
m
impl
emen
tatio
n de
lays
; c) h
ost
gove
rnm
ent e
nviro
nmen
t; d)
late
ar
rival
of p
rogr
amm
ing
fund
s; e
) dr
oppi
ng in
dica
tor;
or f
) oth
er.
09 ta
rget
, to
be
achi
eved
w
ith a
ll fu
nds,
as
of 9
/30/
09
(as
set i
n D
ecem
ber,
2008
PR
)
2010
ta
rget
, to
be
achi
eved
w
ith a
ll fu
nds,
as
of 9
/30/
10
(as
set i
n D
ecem
ber,
2008
PR
)
DQ
A:
Dat
e D
QA
was
co
mpl
ete
d fo
r thi
s in
dica
tor
Num
ber o
f peo
ple
train
ed in
ch
ild h
ealth
and
nut
ritio
n th
roug
h U
SG
-sup
porte
d he
alth
are
a pr
ogra
ms
*
350,
000
Num
ber o
f wom
en re
ceiv
ing
activ
e m
anag
emen
t of t
he
third
sta
ge o
f lab
or (A
MS
TL)
thro
ugh
US
G-s
uppo
rted
prog
ram
s
22,0
00
9,24
7 G
hana
, R
wan
da, I
ndia
Num
ber o
f new
born
s re
ceiv
ing
antib
iotic
trea
tmen
t fo
r inf
ectio
n fro
m a
ppro
pria
te
heal
th w
orke
rs th
roug
h U
SG
-sup
porte
d pr
ogra
ms
12,0
00
Num
ber o
f new
born
s re
ceiv
ing
esse
ntia
l new
born
ca
re th
roug
h U
SG
-su
ppor
ted
prog
ram
s
75,0
00
674
Indi
a
Num
ber o
f chi
ldre
n re
ache
d by
US
G-s
uppo
rted
nutri
tion
prog
ram
s
750,
000

64
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
MA
TER
NA
L A
ND
CH
ILD
HEA
LTH
08
targ
et, t
o be
ach
ieve
d w
ith a
ll fu
nds,
as
of 9
/30/
08
(as
set i
n N
ovem
ber,
2007
PR
)
08 a
ctua
l, ac
hiev
ed w
ith
all f
unds
, as
of
9/30
/08
(as
repo
rted
in
Dec
embe
r, 20
08 P
R)
Expl
anat
ion:
1,0
00 c
hara
cter
text
bo
x (p
er in
dica
tor)
requ
ired
to
expl
ain
devi
atio
n (1
0%) w
hen
targ
ets
are
not m
et, t
arge
ts a
re
sign
ifica
ntly
exc
eede
d, o
r whe
n dr
oppi
ng a
n in
dica
tor.
Dro
p-do
wn
incl
udes
: a) s
hift
in p
rogr
amm
ing
emph
asis
; b) u
nexp
ecte
d pr
ogra
m
impl
emen
tatio
n de
lays
; c) h
ost
gove
rnm
ent e
nviro
nmen
t; d)
late
ar
rival
of p
rogr
amm
ing
fund
s; e
) dr
oppi
ng in
dica
tor;
or f
) oth
er.
09 ta
rget
, to
be
achi
eved
w
ith a
ll fu
nds,
as
of 9
/30/
09
(as
set i
n D
ecem
ber,
2008
PR
)
2010
ta
rget
, to
be
achi
eved
w
ith a
ll fu
nds,
as
of 9
/30/
10
(as
set i
n D
ecem
ber,
2008
PR
)
DQ
A:
Dat
e D
QA
was
co
mpl
ete
d fo
r thi
s in
dica
tor
Num
ber o
f cas
es o
f chi
ld
pneu
mon
ia tr
eate
d w
ith
antib
iotic
s by
trai
ned
faci
lity
or c
omm
unity
hea
lth w
orke
rs
in U
SG
-sup
porte
d pr
ogra
ms
13,0
00
Num
ber o
f chi
ldre
n le
ss th
an
12 m
onth
s of
age
who
re
ceiv
ed D
PT3
from
US
G-
supp
orte
d pr
ogra
ms
(can
no
t dro
p th
is in
dica
tor)*
180,
000
Num
ber o
f chi
ldre
n un
der 5
ye
ars
of a
ge w
ho re
ceiv
ed
vita
min
A fr
om U
SG
-su
ppor
ted
prog
ram
s (c
an
not d
rop
this
indi
cato
r)
620,
000
Lite
rs o
f drin
king
wat
er
disi
nfec
ted
with
US
G-
supp
orte
d po
int-o
f-use
tre
atm
ent p
rodu
cts
360,
000,
000
Num
ber o
f cas
es o
f chi
ld
diar
rhea
trea
ted
in U
SA
ID-
assi
sted
pro
gram
s*
1,00
0,00
0
Num
ber o
f bas
elin
e or
fe
asib
ility
stud
ies
* 1
2 Ba
selin
e st
udie
s w
ere
cond
ucte
d in
R
wan
da a
nd In
dia
durin
g th
is p
erio
d.
0
Num
ber o
f spe
cial
stu
dies
80

65
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
MA
TER
NA
L A
ND
CH
ILD
HEA
LTH
08
targ
et, t
o be
ach
ieve
d w
ith a
ll fu
nds,
as
of 9
/30/
08
(as
set i
n N
ovem
ber,
2007
PR
)
08 a
ctua
l, ac
hiev
ed w
ith
all f
unds
, as
of
9/30
/08
(as
repo
rted
in
Dec
embe
r, 20
08 P
R)
Expl
anat
ion:
1,0
00 c
hara
cter
text
bo
x (p
er in
dica
tor)
requ
ired
to
expl
ain
devi
atio
n (1
0%) w
hen
targ
ets
are
not m
et, t
arge
ts a
re
sign
ifica
ntly
exc
eede
d, o
r whe
n dr
oppi
ng a
n in
dica
tor.
Dro
p-do
wn
incl
udes
: a) s
hift
in p
rogr
amm
ing
emph
asis
; b) u
nexp
ecte
d pr
ogra
m
impl
emen
tatio
n de
lays
; c) h
ost
gove
rnm
ent e
nviro
nmen
t; d)
late
ar
rival
of p
rogr
amm
ing
fund
s; e
) dr
oppi
ng in
dica
tor;
or f
) oth
er.
09 ta
rget
, to
be
achi
eved
w
ith a
ll fu
nds,
as
of 9
/30/
09
(as
set i
n D
ecem
ber,
2008
PR
)
2010
ta
rget
, to
be
achi
eved
w
ith a
ll fu
nds,
as
of 9
/30/
10
(as
set i
n D
ecem
ber,
2008
PR
)
DQ
A:
Dat
e D
QA
was
co
mpl
ete
d fo
r thi
s in
dica
tor
Num
ber o
f inf
orm
atio
n ga
ther
ing
or re
sear
ch a
ctiv
ities
130
Num
ber o
f cou
ntrie
s w
ith
expa
nsio
n of
pos
tpar
tum
he
mor
rhag
e pr
even
tion
inte
rven
tions
(AM
TSL)
*
22
4 In
dia,
Gha
na,
Eth
iopi
a, R
wan
da
Indi
a, G
hana
and
Eth
iopi
a in
trodu
ced
AMTS
L an
d ex
pand
ed in
Gha
na
4 In
dia,
G
hana
, Et
hiop
ia a
nd
Rw
anda
N/A
Num
ber o
f cou
ntrie
s w
ith
intro
duct
ion
and
expa
nsio
n of
cut
ting
edge
nut
ritio
n in
terv
entio
ns (e
.g.,
CTC
and
M
N fo
rtific
atio
n)
49
Num
ber o
f cou
ntrie
s w
ith
intro
duct
ion
and
expa
nsio
n of
new
dia
rrhe
al d
isea
se
prev
entio
n an
d m
anag
emen
t pr
ogra
ms
(PO
U, z
inc
and
OR
T)*
23
Pers
on-d
ays
of te
chni
cal
supp
ort p
rovi
ded
to m
issi
ons
thro
ugh
TDYs
500
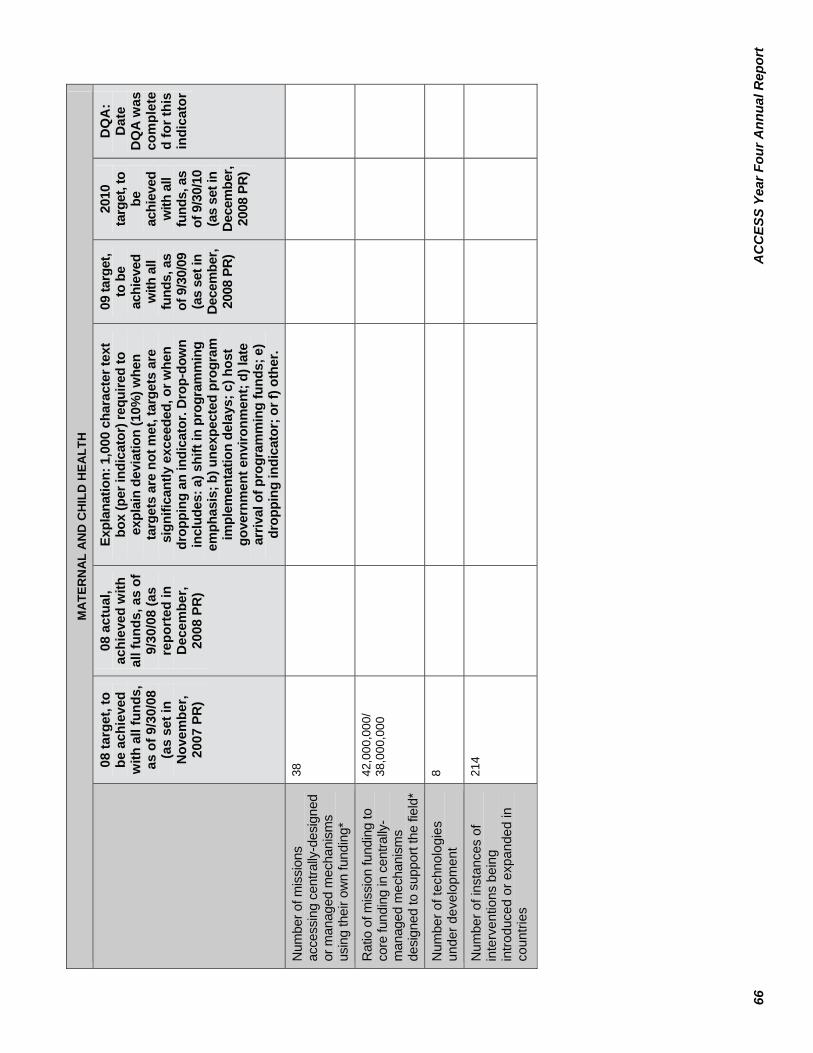
66
AC
CES
S Ye
ar F
our A
nnua
l Rep
ort
MA
TER
NA
L A
ND
CH
ILD
HEA
LTH
08
targ
et, t
o be
ach
ieve
d w
ith a
ll fu
nds,
as
of 9
/30/
08
(as
set i
n N
ovem
ber,
2007
PR
)
08 a
ctua
l, ac
hiev
ed w
ith
all f
unds
, as
of
9/30
/08
(as
repo
rted
in
Dec
embe
r, 20
08 P
R)
Expl
anat
ion:
1,0
00 c
hara
cter
text
bo
x (p
er in
dica
tor)
requ
ired
to
expl
ain
devi
atio
n (1
0%) w
hen
targ
ets
are
not m
et, t
arge
ts a
re
sign
ifica
ntly
exc
eede
d, o
r whe
n dr
oppi
ng a
n in
dica
tor.
Dro
p-do
wn
incl
udes
: a) s
hift
in p
rogr
amm
ing
emph
asis
; b) u
nexp
ecte
d pr
ogra
m
impl
emen
tatio
n de
lays
; c) h
ost
gove
rnm
ent e
nviro
nmen
t; d)
late
ar
rival
of p
rogr
amm
ing
fund
s; e
) dr
oppi
ng in
dica
tor;
or f
) oth
er.
09 ta
rget
, to
be
achi
eved
w
ith a
ll fu
nds,
as
of 9
/30/
09
(as
set i
n D
ecem
ber,
2008
PR
)
2010
ta
rget
, to
be
achi
eved
w
ith a
ll fu
nds,
as
of 9
/30/
10
(as
set i
n D
ecem
ber,
2008
PR
)
DQ
A:
Dat
e D
QA
was
co
mpl
ete
d fo
r thi
s in
dica
tor
Num
ber o
f mis
sion
s ac
cess
ing
cent
rally
-des
igne
d or
man
aged
mec
hani
sms
usin
g th
eir o
wn
fund
ing*
38
Rat
io o
f mis
sion
fund
ing
to
core
fund
ing
in c
entra
lly-
man
aged
mec
hani
sms
desi
gned
to s
uppo
rt th
e fie
ld*
42,0
00,0
00/
38,0
00,0
00
Num
ber o
f tec
hnol
ogie
s un
der d
evel
opm
ent
8
Num
ber o
f ins
tanc
es o
f in
terv
entio
ns b
eing
in
trodu
ced
or e
xpan
ded
in
coun
tries
214