aca reinsurance & high risk pool march 2014
TRANSCRIPT

© 2014 DST Systems, Inc. All rights reserved. © 2014 DST Systems, Inc. All rights reserved.
March 19, 2014
ACA Transitional Reinsurance: Identifying and Assessing High Cost Patients

© 2014 DST Systems, Inc. All rights reserved.
The enclosed materials are highly sensitive, proprietary and confidential. Please use every effort to safeguard the confidentiality of these materials. Please do not copy, distribute, use, share or otherwise provide access to these materials to any person inside or outside DST Systems, Inc. without prior written approval.
This proprietary, confidential presentation is for general informational purposes only and does not constitute an agreement. By making this presentation available to you, we are not granting any express or implied rights or licenses under any intellectual property right.
If we permit your printing, copying or transmitting of content in this presentation, it is under a non-exclusive, non-transferable, limited license, and you must include or refer to the copyright notice contained in this document. You may not create derivative works of this presentation or its content without our prior written permission. Any reference in this presentation to another entity or its products or services is provided for convenience only and does not constitute an offer to sell, or the solicitation of an offer to buy, any products or services offered by such entity, nor does such reference constitute our endorsement, referral, or recommendation.
Our trademarks and service marks and those of third parties used in this presentation are the property of their respective owners.
2
DISCLAIMER

© 2014 DST Systems, Inc. All rights reserved.
DST
▪ Trusted global provider of technology-based service solutions since 1969 that help our clients grow their business & provide exceptional customer experiences
▪ NYSE Listing: “DST”
▪ 2013 Revenue: $2.66 Billion
▪ Worldwide Associates: 11,500+
▪ Locations: 14 worldwide offices
DST
HS ▪ Solutions to health payers and
providers since 1976
▪ Servicing Commercial, Medicaid, Marketplace, MA/MAPD, & Duals health benefit plans
▪ Core systems used to support 22+ M members / 270 M claims
▪ 41+ M medical claims processed annually in BPO
▪ 25+ M pharmacy members supported
DSTHS At A Glance

© 2014 DST Systems, Inc. All rights reserved. 4
Richard Popper Director, Medicaid & Duals Strategy, DST Health Solutions Group Director, Insurance Programs, CCIIO-CMS 2010-13
Center for Consumer Information & Insurance Oversight
Managed team that implemented & administered:
$5 billion Early Retiree Reinsurance Program
Pre-Existing Condition Insurance Plan
CO-OP Loan Program
Executive Director, Maryland Health Insurance Plan 2002-10 Implemented & administered fastest growing state high risk pool in U.S, with 10% of national HRP enrollment
Assistant Director, California Managed Risk Medical Insurance Plan 2000-02 Responsible for MRMIP & AIM programs for high risk uninsured

© 2014 DST Systems, Inc. All rights reserved.
No medical underwriting
No pre-existing condition exclusion riders or waiting periods
Few benefit limits and standardized OOP limits
Reduced member cost sharing for those with limited income
Low initial enrollment penalty
Many “qualifying events” that allow enrollment “churn”:
Newly eligible for APTC
Had website enrollment problems
employer coverage not affordable
“Exceptional circumstances as the exchange may provide.”
5
Marketplace a significantly different product
© 2014 DST Systems, Inc. All rights reserved. 6
Overall structure of transitional reinsurance program Congress included transitional reinsurance program in ACA to improve affordability
Subsidize plan costs of high-risk enrollees to improve premium stability
$10 billion available in 2014, $6 billion in 2015, & $4 billion in 2016
Reinsurance funds generated from assessment of state licensed insurance companies, services or organizations:
$63 & $ 0.11 per capita contribution for 2014; $44 per capita projected for 2015
Reinsurance funds are available for non-grandfathered individual market plans to offset any substantial individual member costs:
2014: HHS will pay 80% of plan per member costs between $45,000 “attachment point” and $250,000 reinsurance cap ($164,000 max per member)
2015: Estimated 50% of plan per member costs between $70,000 attachment point and $250,000 reinsurance cap ($90,000 max per member).

© 2014 DST Systems, Inc. All rights reserved. 7
Structure of transitional reinsurance program Allocation of covered cost for individual as expenses rise
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
$0 $24,000 $48,000 $72,000 $96,000 $120,000 $144,000 $168,000 $192,000 $216,000 $240,000 $264,000
Share of Plan Covered Costs
An Individual Member's Covered Costs
Member OOP Costs Plan Costs
HHS TransitionalReinsurance

© 2014 DST Systems, Inc. All rights reserved.
Since initial Covered California enrollment is:
Lower than expected
Contains adverse selection from long term uninsured, and
Made up of approximately 20,000 high risk individuals from California Managed Risk Medical Insurance Plan, and Federal Pre-Existing Condition Insurance Plan.
8
High cost composition of initial Covered California enrollment
High risk individuals will make up disproportionate share of plan membership

© 2014 DST Systems, Inc. All rights reserved. 9
Plan cost exposure & average PMPY costs of high risk enrollees
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
$- $10,000 $20,000 $30,000 $40,000 $50,000 $60,000
HHSTransitionalReinsurance
Member OOP Costs
PlanCosts
High Risk Pool average $12,471
Calif Duals average $13,625
Fed PCIP average $32,108
© 2014 DST Systems, Inc. All rights reserved. 10
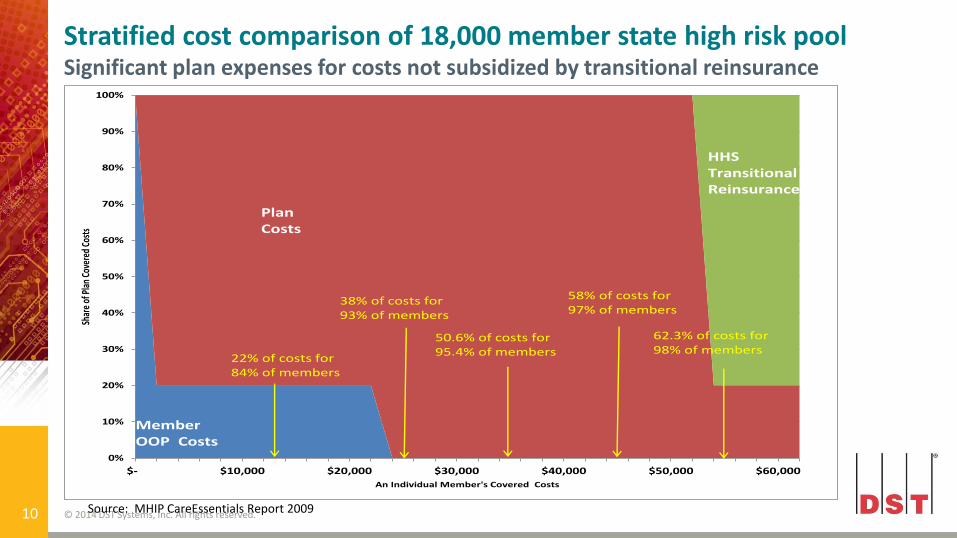
Stratified cost comparison of 18,000 member state high risk pool Significant plan expenses for costs not subsidized by transitional reinsurance
Source: MHIP CareEssentials Report 2009
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
$- $10,000 $20,000 $30,000 $40,000 $50,000 $60,000
Shar
e of
Pla
n Co
vere
d Co
sts
An Individual Member's Covered Costs
HHSTransitionalReinsurance
Member OOP Costs
PlanCosts
22% of costs for 84% of members
38% of costs for 93% of members
50.6% of costs for 95.4% of members
58% of costs for 97% of members
62.3% of costs for 98% of members

© 2014 DST Systems, Inc. All rights reserved.
For large state high risk pool, with income subsidies and benefits comparable to Covered California plans, and 215% MLR:
Only 31% of 2009 net plan costs would have been eligible for 80% subsidy under HHS Transitional Reinsurance
Reinsurance subsidies would have been provided for 3% of members with qualifying catastrophic plan costs over $45,000.
63% of 2009 net plan costs would not have been subsidized by HHS Transitional Reinsurance
39% of 2009 net plan costs were for members who incurred PM costs between $10,000 to $45,000, ineligible for HHS Reinsurance in 2014
20% of net plan costs would be in “100% plan cost phase.”
11
Significant portion of plan costs not covered under HHS transitional reinsurance

© 2014 DST Systems, Inc. All rights reserved. 12
Stratified 2011 costs of 20,000 member Federal Pre-Existing Condition Insurance Plan (PCIP)
Source: Federal PCIP Claims Incurred 2011, paid thru 1/2012
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
$- $10,000 $20,000 $30,000 $40,000 $50,000 $60,000
Shar
e of
Pla
n Co
vere
d Co
sts
An Individual Member's Covered Costs
HHSTransitionalReinsurance
Member OOP Costs
PlanCosts
6% of costs for 47% of members
15% of costs for 87% of members
20% of costs for 90% of members
25% of costs for 91% of members
29% of costs for 93% of members

© 2014 DST Systems, Inc. All rights reserved.
For Federal Pre-Existing Condition Insurance Plan
370% MLR and no income subsidies:
74% of 2011 Federal PCIP net plan costs would have been eligible to receive 80% HHS Transitional Reinsurance subsidies
Reinsurance subsidies would have been provided for 8% of members with qualifying catastrophic net plan costs over $45,000.
25% of 2011 net plan costs would not have been subsidized by HHS Transitional Reinsurance
15% of costs would be in “100% plan cost phase”
Issue for Covered California plans:
Will initial plan cost exposure have wide distribution, like state high risk pools, where majority of high costs are not subsidized by HHS reinsurance
Or will plans have more catastrophic cost exposure, like PCIP, with significant amount of costs covered by transitional reinsurance.
13

© 2014 DST Systems, Inc. All rights reserved. 14
Comparison of sample cost exposure below HHS transitional reinsurance
0%
10%
20%
30%
40%
50%
60%
70%
$5,000 $10,000 $15,000 $20,000 $25,000 $30,000 $35,000 $40,000 $45,000
Cumulative Percent of Plan Cost
Individual Member Total Annual Plan Cost
Federal PCIP 2011
State High Risk Pool 2009
$45,000 HHS Transitional Reinsurance
Attachment Point

© 2014 DST Systems, Inc. All rights reserved. 15
Common diagnosis cost drivers below reinsurance attachment point for state high risk pool Diagnosis % of plan costs Average 2009 PMPY cost
HIV/AIDS 11.1% $12,127
Osteoarthritis 4.4% $6,420
Coronary Artery 3.1% $4,511
Leukemia 2% $38,318
Breast Cancer 1.9% $8,907
Colon Cancer 1.9% $31,618
Bipolar Disorder 1.8% $5,074
Crohn’s Disease 1.4% $15,844
Cerebrovascular Disease
1.3% $4,713
MS 1.3% $20,049
Cirrhosis of Liver 1.2% $24,121 Source: MHIP CareEssentials Report 2009

© 2014 DST Systems, Inc. All rights reserved. 16
Common diagnosis cost drivers for Federal Pre-existing Health Insurance Plan
Diagnosis % of plan costs /2
Cancer 19.8%
Maintenance Chemotherapy, radiation 8.8%
Osteoarthritis 6.3%
Spondylosis / disc disorders 6.2%
Coronary Artery & other heart disease 4.7%
High risk behavioral health & substance abuse admissions more prevalent in individual market
Diagnosis % of plan inpatient admissions /1
Psychosis 6%
Vaginal Labor & Delivery 4.6%
Alcohol/Drug Abuse & Rehab 2%
1 – MHIP CareEssentials Report 2009 2 – 2012 & 2013 Federal PCIP reports, cms.gov
© 2014 DST Systems, Inc. All rights reserved. 17
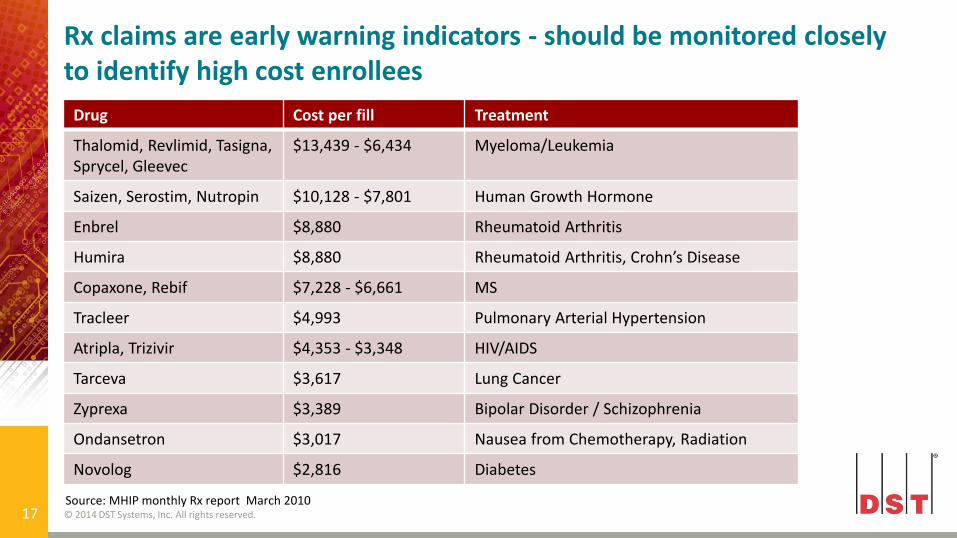
Rx claims are early warning indicators - should be monitored closely to identify high cost enrollees
Drug Cost per fill Treatment
Thalomid, Revlimid, Tasigna, Sprycel, Gleevec
$13,439 - $6,434 Myeloma/Leukemia
Saizen, Serostim, Nutropin $10,128 - $7,801 Human Growth Hormone
Enbrel $8,880 Rheumatoid Arthritis
Humira $8,880 Rheumatoid Arthritis, Crohn’s Disease
Copaxone, Rebif $7,228 - $6,661 MS
Tracleer $4,993 Pulmonary Arterial Hypertension
Atripla, Trizivir $4,353 - $3,348 HIV/AIDS
Tarceva $3,617 Lung Cancer
Zyprexa $3,389 Bipolar Disorder / Schizophrenia
Ondansetron $3,017 Nausea from Chemotherapy, Radiation
Novolog $2,816 Diabetes
Source: MHIP monthly Rx report March 2010

© 2014 DST Systems, Inc. All rights reserved. 18
Initial average plan costs for high risk pool members will decrease over time, but often remains above premium
Source: Mercer analysis of high risk pool plans 2009
$13.910
$20.398
$10.065 $9.433
$0.000
$5.000
$10.000
$15.000
$20.000
$25.000
FY08 FY09
Short Term Subscribers Long Term Subscribers
Plan cost comparison among subscribers not subject to preexisting condition exclusion
© 2014 DST Systems, Inc. All rights reserved.
Third Party Payers, such as:
Hospitals and other providers
AIDS Drug Assistance Program
Disease Advocacy Organizations (American Cancer, Hemophilia Societies)
Provider networks
Plan benefit structure and authorization requirements.
19
Monitoring drivers of high cost enrollment

© 2014 DST Systems, Inc. All rights reserved. 20
Recommendations

© 2014 DST Systems, Inc. All rights reserved.
Interface directly with plans claim and Rx systems, to quickly enable care managers to identify patients at high risk for hospitalization or costly complications, and determine proactive interventions
Evaluate gaps in care through review of member’s overall clinical profile
Measure and report HEDIS compliance status
Evaluate performance of providers, including prescribing patterns, medication screenings, diagnosis testing, preventive visits and benchmarking with peer providers
Have predictive modeling to stratify claims diagnosis, often prior to high cost claims, for early interventions and care coordination.
21
Utilize effective data analytics software

© 2014 DST Systems, Inc. All rights reserved.
Receipt of reinsurance and risk adjustment payments dependent on plan establishing a “distributed data collection approach”
Plans must establish an “edge server”
Secure, dedicated, electronic server environments to house medical and pharmacy claims, encounter data, and enrollment information
Issuers directed to make data accessible to HHS to install, update, and operate common software to monitor plan costs
Plans expected to load claims and enrollment data to edge server monthly
Offers plans an opportunity to actively monitor claims expenses and identify high cost member for interventions.
22
HHS Edge Server Month submission a useful opportunity to monitor high cost members

© 2014 DST Systems, Inc. All rights reserved.
All diagnoses – most high risk members suffer from multiple conditions (cancer and depression), and the most acute often masks additional care needs
Medication inventory and adherence
Condition severity
Recent and major surgeries and procedures
Nursing and rehabilitation therapies
High risk factors (weight, tobacco, substance abuse)
Supportive assistance (family, caregivers)
Language, education, cognitive, locomotion capabilities and needs.
23
Utilize effective member assessment tools
© 2014 DST Systems, Inc. All rights reserved.
Complete, record and update health risk assessments
Create patient-centered care plans to monitor and close existing care gaps and engage members
Integrate care for comorbidities, including both medical and behavioral health conditions
Track quality of care issues
Maintain a complete history of all member activity for those enrolled in a care plan
Real-time interface with core claims systems for up to date eligibility, benefits, and claims history
View member profiles, medical claims, and pharmacy data.
24
Utilize effective care management systems
© 2014 DST Systems, Inc. All rights reserved.
Apply medication therapy management and reconciliation
Process utilization management referrals and authorizations
Complete discharge planning surveys
Assist with transitional care plans and schedule necessary appointments and equipment use
Integrate with care analysis software for stratification and identification of members needing outreach and intervention.
25
Effective care management systems, cont’d

© 2014 DST Systems, Inc. All rights reserved. 26
Develop specialized care management teams
Medical staff focus on standard care management and utilization management practices is not enough
Must move beyond pregnancy, diabetes and asthma
Prevalence of significant, multiple chronic disease in initial Covered California population far exceeds standard Medi-Cal and commercial enrollment
Core staff needed to focus on intensive care management
Lower member to case manager ratios necessary during 2014 and 2015
Enrollment of high cost cases will continue after open enrollment ends
Due to significant SEP options for those newly diagnoses with high cost conditions
Don’t neglect young members - 23% of high risk pool enrollee were under age 30, with frequent behavioral health & substance abuse conditions.

© 2014 DST Systems, Inc. All rights reserved.
Questions
Richard Popper Director, Duals & Medicaid Strategy
410.294.8215
Jill Singletary Senior Sales Executive
214.695.8372
www.dsthealthsolutions.com