absolute eosinophils count as a marker of mortality in patients with severe sepsis and septic shock...
TRANSCRIPT
Journal of Critical Care (2012) 27, 394–399
Absolute eosinophils count as a marker of mortality inpatients with severe sepsis and septic shock in an intensivecare unit☆,☆☆
Carlos Adolfo Merino MDa,b,⁎, Felipe Tomás Martínez MDb,Felipe Cardemil MDc, José Ramón Rodríguez MDb
aUnidad de Cuidados Intensivos, Hospital Gustavo Fricke. Valparaíso, ChilebEscuela de Medicina, Facultad de Medicina, Universidad de Valparaíso, Valparaíso, ChilecEscuela de Salud Pública, Facultad de Medicina, Universidad de Chile, Santiago, Chile
m
0d
Keywords:Eosinophils;Sepsis;Mortality
AbstractIntroduction: Eosinophils in the circulating blood undergo apoptosis during sepsis syndromes inducedby the action of certain cytokines.Objective: The aim of the study was to evaluate the absolute eosinophils count (EC) as a marker ofmortality in severe sepsis and septic shock.Patients and Method: A prospective cohort study of patients with a diagnosis of sepsis or septic shockadmitted to the intensive care unit (ICU) of the Dr Gustavo Fricke Hospital between January 2008 andDecember 2009 was conducted. Daily EC in all patients was analyzed. Receiver operating characteristiccurve analysis was used to assess the performance of the diagnostic test.Results: We studied a total of 240 patients. The median age was 62 years (interquartile range [IQR],48-72 years), and 67 (27.9%) died. The median EC in patients who died was 43 (IQR, 14-121), whereasin surviving patients, it was 168 (IQR, 98-292) (P b .001). When the EC on the fifth day of hospital staywas assessed, an area under the curve (AUC) of 0.64 (95% confidence interval, 0.55-0.73) wasobserved. Eosinophils count at intensive care unit discharge showed an area under the curve of 0.81(95% confidence interval, 0.76-0.87).Discussion: Eosinophils counts were lower in patients who died of sepsis than in those who sur-vived, but its clinical usefulness seems limited. Their role as an indicator of clinical stability seems tobe important.© 2012 Elsevier Inc. All rights reserved.
☆ Conflicts of interest statement: None to disclose.☆☆ Sources of funding: None.⁎ Corresponding author. Agua Santa 1400, Edificio Riñihue, departa-
ento 1001, Viña del Mar.E-mail address: [email protected] (C.A. Merino).
883-9441/$ – see front matter © 2012 Elsevier Inc. All rights reserved.oi:10.1016/j.jcrc.2011.10.010
1. Introduction
Sepsis and septic shock are high-frequent conditions inintensive care units (ICUs) worldwide. They are responsiblefor about 10% of admissions to these units, and they are

395Absolute EC as a marker of mortality
associated with a significant mortality rate up to 30% [1].This rate has led to the search for tools allowing preciseprognostic evaluation of these patients [2]. Thus, multipleassessment methods have subsequently appeared, such asthe Acute Physiology and Chronic Health Evaluation II(APACHE II) scoring system, and different tests showing aprognostic capacity, such as C-reactive protein (CRP) [3-6];amyloid A protein [7]; interleukins 6 [8], 8 [8], and 10 [3]; atriggering receptor expressed on myeloid cells 1 [9]; andserum procalcitonin levels [4-6]. All these tests have shownan ability, with different degrees of accuracy, to establishdiagnosis and prognosis for each septic episode, but nonehas proven to be the ideal indicator.
Accordingly, some recent studies have appeared concern-ing the value of an old marker of infection used during thefirst decade of the last century as an indicator of sepsis:eosinopenia [10-12]. Eosinophils are cells that normallyaccount for only 1% to 3% of total leukocytes, with a maxi-mum of 350 cells/mm [3,13]. The reduction in the number ofeosinophils is still an unexplained phenomenon, but it may belinked to the action of inflammatory cytokines, such as tumornecrosis factor, and acute phase reactants, such as gluco-corticoids and epinephrine [12]. However, studies report thatalthough correlation with some of these mediators does exist,it is weak. In addition, a reduction in eosinophils CRTH2(Chemoattractant receptor homologous molecule expressedon Th2 lymphocytes) and CCR3 (C-C chemokine receptortype 3) expression during septic shock and a persistence oflow levels of them in nonsurvivors have been observed [14].
Gil et al [15] demonstrated significant differences in meanvalues of eosinophils between patients with infectious andnoninfectious episodes, and counts less than 40 cells/mm3
were strongly related to bacterial etiology. Furthermore, in arecent study, Abidi et al [16] report that eosinopenia consti-tutes a good diagnostic marker in identifying sepsis con-ditions and discriminating their severity. Eosinopenia hasalso been reported as an important prognostic marker in thesepsis syndromes even after adjustments for confoundingfactors such as comorbidities, APACHE II, and SequentialOrgan Failure Assessment (SOFA) scores, and the require-ment of mechanical ventilation is made [17].
The purposes of the present study were to assess theabsolute eosinophils count (EC) as a marker of mortality inpatients with sepsis or septic shock conditions and to eval-uate whether it has any ability to predict mortality.
2. Patients and method
A prospective study of patients with diagnosis of severesepsis or septic shock admitted to the ICU of the Dr GustavoFricke Hospital in Viña del Mar was conducted betweenJanuary 2008 and December 2009. The inclusion criteriainvolved patients with sepsis or septic shock according to thediagnostic criteria established by the American College ofChest Physicians and the Society of Critical Care Medicine
[18,19]. The following exclusion criteria were applied:patients aged younger than 18 years, not meeting severesepsis or septic shock criteria previously established,discharged less than 48 hours after admission to the ICU(because in many cases, they had been done b2 completeblood counts), with unknown sepsis outcome, those withmissing data above or equal to 10% during follow-up, orthose with preexisting disease or treatment that might alterEC such as chronic steroids use or acquired immunodefi-ciency syndrome. All patients were given standard replace-ment doses of corticosteroids (50 mg per 6 hours intravenoushydrocortisone) according to the management guidelines ofthe study center. Because of an earlier unpublished pilotreport in our center, we also considered the hypothesis thatlate changes in EC could be of prognostic significance, andtherefore, we also considered the last 3 ECs observed(48 hours, 24 hours predischarge, and discharge levels) foranalysis. The study protocol was approved by the ethicscommittee at the Dr Gustavo Fricke Hospital.
The main outcome was 30-day mortality. All patientswere followed up daily the entire hospital stay and up to amaximum of 30 days. The following information wascollected: age, sex, septic focus, estimated risk of the septicepisode measured at admission using APACHE II and SOFAscores, and outcome of the septic episode. The EC wasmeasured in each patient by serial complete blood countsduring the entire ICU stay. Admission and daily eosinophilcounts as well as the mean EC obtained during the hospitalstay were registered. The mean EC during hospitalizationwas obtained by dividing daily EC by the total number ofdays in which EC had been registered. This measurementwas performed using a flow cytometer (Coulter STKS;Beckman-Coulter, Brea, CA, USA). We also sought tocompare EC's prognostic capacities with the CRP levelsobserved during the ICU stay because it is also a widely usedinflammatory mediator. All data were stored in a FilemakerPro 9 (Santa Clara, CA, USA) database.
Statistical analysis was carried out using SPSS (IBMCorporation, Armonk, New York, USA) 16.0 and STATA 10(StataCorp, College Station, TX, USA). Quantitative variableswere compared using Student t and Mann-Whitney U testsaccording to sample distribution and variances that were testedby the Kolmogorov-Smirnov and Levene tests, respectively.For qualitative variables, Fisher exact test was used. Receiveroperating characteristic (ROC) curves were used to asses theutility of EC in predictingmortality. If a test with an area underthe curve (AUC) clinically useful was found [20], a cutoffpoint with its respective sensitivity and specificity values wasthen chosen, and likelihood ratios were also calculated. An αless than 5% was considered statistically significant.
3. Results
A total of 255 patients were enrolled into the study; 11 ofthese patients were excluded because they did not meet the
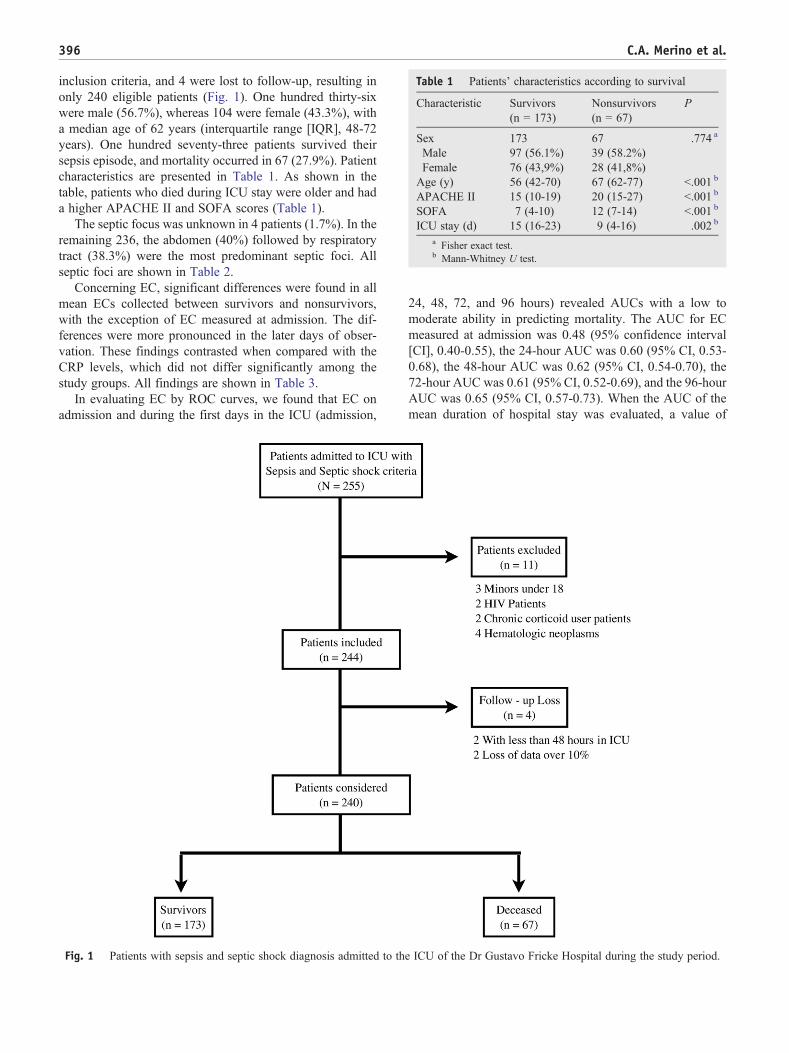
Table 1 Patients' characteristics according to survival
Characteristic Survivors(n = 173)
Nonsurvivors(n = 67)
P
Sex 173 67 .774 a
Male 97 (56.1%) 39 (58.2%)Female 76 (43,9%) 28 (41,8%)Age (y) 56 (42-70) 67 (62-77) b.001 b
APACHE II 15 (10-19) 20 (15-27) b.001 b
SOFA 7 (4-10) 12 (7-14) b.001 b
ICU stay (d) 15 (16-23) 9 (4-16) .002 b
a Fisher exact test.b Mann-Whitney U test.
396 C.A. Merino et al.
inclusion criteria, and 4 were lost to follow-up, resulting inonly 240 eligible patients (Fig. 1). One hundred thirty-sixwere male (56.7%), whereas 104 were female (43.3%), witha median age of 62 years (interquartile range [IQR], 48-72years). One hundred seventy-three patients survived theirsepsis episode, and mortality occurred in 67 (27.9%). Patientcharacteristics are presented in Table 1. As shown in thetable, patients who died during ICU stay were older and hada higher APACHE II and SOFA scores (Table 1).
The septic focus was unknown in 4 patients (1.7%). In theremaining 236, the abdomen (40%) followed by respiratorytract (38.3%) were the most predominant septic foci. Allseptic foci are shown in Table 2.
Concerning EC, significant differences were found in allmean ECs collected between survivors and nonsurvivors,with the exception of EC measured at admission. The dif-ferences were more pronounced in the later days of obser-vation. These findings contrasted when compared with theCRP levels, which did not differ significantly among thestudy groups. All findings are shown in Table 3.
In evaluating EC by ROC curves, we found that EC onadmission and during the first days in the ICU (admission,
Fig. 1 Patients with sepsis and septic shock diagnosis admitted to th
24, 48, 72, and 96 hours) revealed AUCs with a low tomoderate ability in predicting mortality. The AUC for ECmeasured at admission was 0.48 (95% confidence interval[CI], 0.40-0.55), the 24-hour AUC was 0.60 (95% CI, 0.53-0.68), the 48-hour AUC was 0.62 (95% CI, 0.54-0.70), the72-hour AUC was 0.61 (95% CI, 0.52-0.69), and the 96-hourAUC was 0.65 (95% CI, 0.57-0.73). When the AUC of themean duration of hospital stay was evaluated, a value of
e ICU of the Dr Gustavo Fricke Hospital during the study period.
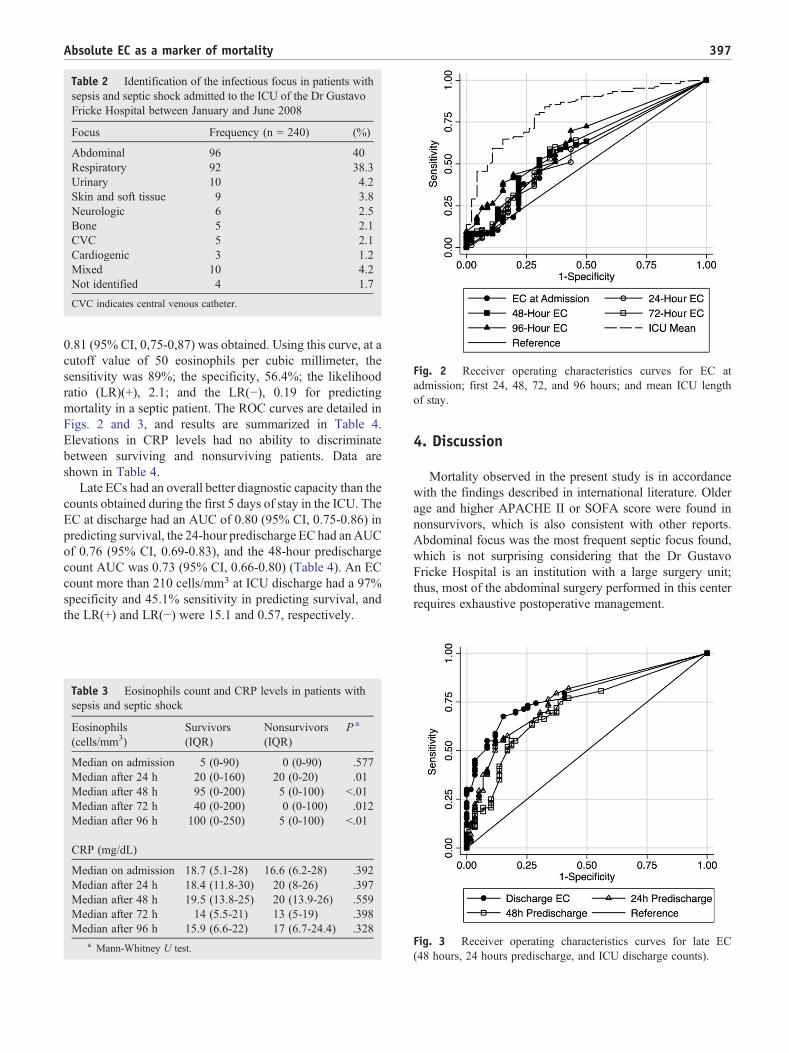
Table 2 Identification of the infectious focus in patients withsepsis and septic shock admitted to the ICU of the Dr GustavoFricke Hospital between January and June 2008
Focus Frequency (n = 240) (%)
Abdominal 96 40Respiratory 92 38.3Urinary 10 4.2Skin and soft tissue 9 3.8Neurologic 6 2.5Bone 5 2.1CVC 5 2.1Cardiogenic 3 1.2Mixed 10 4.2Not identified 4 1.7
CVC indicates central venous catheter.
Fig. 2 Receiver operating characteristics curves for EC atadmission; first 24, 48, 72, and 96 hours; and mean ICU lengthof stay.
397Absolute EC as a marker of mortality
0.81 (95% CI, 0,75-0,87) was obtained. Using this curve, at acutoff value of 50 eosinophils per cubic millimeter, thesensitivity was 89%; the specificity, 56.4%; the likelihoodratio (LR)(+), 2.1; and the LR(−), 0.19 for predictingmortality in a septic patient. The ROC curves are detailed inFigs. 2 and 3, and results are summarized in Table 4.Elevations in CRP levels had no ability to discriminatebetween surviving and nonsurviving patients. Data areshown in Table 4.
Late ECs had an overall better diagnostic capacity than thecounts obtained during the first 5 days of stay in the ICU. TheEC at discharge had an AUC of 0.80 (95% CI, 0.75-0.86) inpredicting survival, the 24-hour predischarge EC had anAUCof 0.76 (95% CI, 0.69-0.83), and the 48-hour predischargecount AUC was 0.73 (95% CI, 0.66-0.80) (Table 4). An ECcount more than 210 cells/mm3 at ICU discharge had a 97%specificity and 45.1% sensitivity in predicting survival, andthe LR(+) and LR(−) were 15.1 and 0.57, respectively.
Table 3 Eosinophils count and CRP levels in patients withsepsis and septic shock
Eosinophils(cells/mm3)
Survivors(IQR)
Nonsurvivors(IQR)
P a
Median on admission 5 (0-90) 0 (0-90) .577Median after 24 h 20 (0-160) 20 (0-20) .01Median after 48 h 95 (0-200) 5 (0-100) b.01Median after 72 h 40 (0-200) 0 (0-100) .012Median after 96 h 100 (0-250) 5 (0-100) b.01
CRP (mg/dL)
Median on admission 18.7 (5.1-28) 16.6 (6.2-28) .392Median after 24 h 18.4 (11.8-30) 20 (8-26) .397Median after 48 h 19.5 (13.8-25) 20 (13.9-26) .559Median after 72 h 14 (5.5-21) 13 (5-19) .398Median after 96 h 15.9 (6.6-22) 17 (6.7-24.4) .328
a Mann-Whitney U test.
4. Discussion
Mortality observed in the present study is in accordancewith the findings described in international literature. Olderage and higher APACHE II or SOFA score were found innonsurvivors, which is also consistent with other reports.Abdominal focus was the most frequent septic focus found,which is not surprising considering that the Dr GustavoFricke Hospital is an institution with a large surgery unit;thus, most of the abdominal surgery performed in this centerrequires exhaustive postoperative management.
Fig. 3 Receiver operating characteristics curves for late EC(48 hours, 24 hours predischarge, and ICU discharge counts).

Table 4 Eosinophil count, CRP, and ROC curves
Test AUC (95% CI)
Early ECAdmission 0.52 (0.45-0.60)24 h 0.60 (0.53-0.68)48 h 0.62 (0.54-0.70)72 h 0.61 (0.53-0.69)96 h 0.65 (0.67-0.73)Late EC48 h predischarge 0.73 (0.66-0.80)24 h predischarge 0.76 (0.69-0.83)ICU discharge 0.81 (0.75-0.86)Mean hospitalization 0.81 (0.75-0.87)CRPAdmission 0.54 (0.45-0.62)24 h 0.54 (0.45-0.62)48 h 0.47 (0.38-0.56)72 h 0.54 (0.45-0.64)96 h 0.46 (0.37-0.54)
398 C.A. Merino et al.
Significant differences were found in the ECs measured inthe first 96 hours after study inclusion and in the mean ECobtained during the hospitalization stay between survivorsand nonsurvivors. However, when the predictive capacity ofEC was estimated, we found that it was limited during thefirst days of hospitalization with areas under the ROC curvesprogressively increased from 0.52 at admission to 0.65 after96 hours of hospitalization. Of these curves, only delayed-period curves reach statistical and clinical significance, thussuggesting that diagnostic accuracy of the test improveswith increasing hospital time. The importance of this ob-servation is based on the fact that the day 5 AUC was theearlier marker clinically useful found in this study sample,and if we consider that the mean hospital length of stay was9 days for nonsurvivors, it may have some utility as a markerof mortality in patients hospitalized in ICU affected bysepsis or septic shock. That a ROC curve with a promisingAUC of 0.81 (95% CI, 0.75-0.87) was observed when themean eosinophil count during the whole length of ICU staystrongly reinforces the idea that late changes in EC areprobably responsible for the improvement in the predictivecapacity of mortality in our study sample.
These results contrast with the promising AUC of the ECat admission observed by Abidi et al [17] (0.82; 95% CI,0.77-0.88) in a recent report on the prognostic significanceof eosinopenia. Our study design did not exclude patientswho received replacement doses of corticosteroids afteradmission to ICU, this being part of the current behavior inour unit for the management of patients with septicepisodes. We believe that the differences observed couldbe due to the routine use of hydrocortisone at our studycenter because steroids are known inducers of eosinopenia[13,17,21]. It is possible that the use of this interventioncould preclude the use of EC as an early prognostic markerin sepsis. However, because the late prediction of survival
seems to be unaltered, we hypothesize that their role asmarkers of clinical stability is unaffected. That the observedAUC is of similar magnitude than the one observed byAbidi et al further strengthens this interpretation.
Therefore, we believe that the most important results inthis study come from the late EC whose AUC was signi-ficantly better than that observed during the earlier days ofhospitalization. The most useful AUC was seen at ICUdischarge, with a value that is as promising as the oneobserved in the mean EC during the whole ICU stay.Eosinophils counts are widely available, and a value morethan 210 cells/mm3 can be considered among the manycriteria that intensivists use to decide ICU discharge. Thisfinding is highly encouraging because ECs are cheap andwidely available. These characteristics make them an acces-sible test for the intensivist even in low-income countrieswhere advanced mediators of septic activity cannot be usedbecause of high costs.
In this study, CRP levels had no ability to discriminatebetween surviving and nonsurviving patients. Mixed resultshave been reported in the literature regarding CRP'sprognostic capacity in critically ill septic patients, but currentevidence seems to suggest that single CRP values are lessuseful for prognostication than changes in CRP over time[3-7,22-24]. Our results agree with this viewpoint and addthat single EC measurements have more prognosticsignificance than isolated CRP levels.
This study has some limitations that require consideration.We did not use a nonseptic control group, and therefore, ourconclusions only apply to septic patients. Although aprognostic association in this subgroup of patients could befound, we believe that it is unlikely because most changes inEC happen in septic patients [16] because of the maladaptivecytokine storm that is characteristic of the disease patho-physiology. It would also have been interesting to compareEC's performance in predicting mortality with plasma pro-calcitonin, another widely used mediator in septic patients.We were unable to measure it because it was not an availabletest at the study center when our investigation was conducted.
In conclusion, EC is lower in patients who have adverseoutcomes. Patients with persistent eosinopenia are at anincreased risk of dying and, therefore, should be closelymonitored. In the steroid-treated patient, EC has a predictivecapacity that seems to be limited but increases as the hos-pitalization advances. The test seems to be more useful as anindicator of clinical stability than a early prognostic marker.
References
[1] Angus D, Linde-Zwirble W, Lidicker J, et al. Epidemiology of severesepsis in the United States: analysis of incidence, outcome, andassociated costs of care. Crit Care Med 2001;29(7):1303-10.
[2] Rivers E, Mcintyre L, Morro D, et al. Early and innovativeinterventions for severe sepsis and septic shock: taking advantage ofa window of opportunity. CMAJ 2005;173(9):1054-65.

399Absolute EC as a marker of mortality
[3] Heper Y, Akalin H, Mistic R, et al. Evaluation of C-reactive protein,tumor necrosis factor alpha, and interleukin-10 as diagnostic andprognostic parameters in patients with community-acquired sepsis,severe sepsis, and septic shock. Eur J Microbiol Infect Dis 2006;25:481-91.
[4] Claeys R, Vinken S, Spapen H, et al. Plasma procalcitonin and C-reactive protein in acute septic shock: clinical and biological correlates.Crit Care Med 2002;30(4):757-62.
[5] Castelli GP, Pognani C, Meisner M, et al. Procalcitonin and C reactiveprotein during systemic inflammatory response syndrome, sepsis andorgan dysfunction. Crit Care Med 2004;8(4):R234-42.
[6] Castelli GP, Pognani C, Cita M, et al. Procalcitonin, C-reactive protein,white blood cells and SOFA score in ICU: diagnosis and monitoring ofsepsis. Minerva Anestesiol 2006;72(1-2):69-80.
[7] Cicarelli DD, Vieira JE, Benseñor FE. Comparison of C-reactiveprotein and serum amyloid A protein in septic shock patients. MediatorInflamm 2008;2008:1-5.
[8] Renz H, Herzum I. Inflammatory markers in SIRS, sepsis and septicshock. Curr Med Chem 2008;15(6):581-7.
[9] Gibot S, Kolopp-SardaMN, BénéMC, et al. Plasma level of a triggeringreceptor expressed onmyeloid cells-1: its diagnostic accuracy in patientswith suspected sepsis. Ann Intern Med 2004;141:9-15.
[10] Shaaban H, Daniel S, Sison R, et al. Eosinopenia: is it a good marker ofsepsis in comparison to procalcitonin and C-reactive protein levels forpatients admitted to a critical care unit in an urban hospital? J Crit Care2010;25:570-5.
[11] Simon CE. A manual of clinical diagnosis. London: Henry Klimpton;1922.
[12] Bass DA, Gonwa TA, Szejda P, et al. Eosinopenia of acute infection:production of eosinopenia by chemotactic factors of acute inflamma-tion. J Clin Invest 1980;65:1265-71.
[13] Rothenberg ME. Eosinophilia. N Engl J Med 1998;338:1592-600.
[14] Venet F, Lepape A, Debard AL, et al. The Th2 response as monitoredby CRTH2 or CCR3 expression is severely decreased during septicshock. Clin Immunol 2004;113(3):278-84.
[15] Gil H, Magy N, Mauny F, et al. Value of eosinopenia in inflamma-tory disorders: an ‘old’marker revisited. RevMed Interne 2003;24:431-5.
[16] Abidi K, Khoudri I, Belayachi J, et al. Eosinopenia is a reliable markerof sepsis on admission to medical intensive care units. Crit Care 2008;12(2):R59.
[17] Abidi K, Belayachi J, Derras Y, et al. Eosinopenia, an early marker ofincreased mortality in critically ill medical patients. Intensive CareMed 2011;37:1136-42.
[18] Members of the American College of Chest Physicians/Society of CritCare Med Consensus Conference Committee: American College ofChest Physicians/Society of Crit Care Med Consensus Conference:definitions for sepsis and organ failure and guidelines for the use ofinnovative therapies in sepsis. Crit Care Med 1992;20:864-74.
[19] Levy M, Fink M, Marshall J, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med 2003;31(4):1250-6.
[20] Akobeng AK. Understanding diagnostic tests 3: receiver operatingcharacteristics curves. Acta Paediatr 2007;26(3):259-62.
[21] Altman L, Hill J, Hairfield W, et al. Effects of corticosteroids oneosinophil chemotaxis and adherence. J Clin Invest 1981;67(1):28-36.
[22] Póvoa P, Teixeira-Pinto AM, Carneiro AH. The Portuguese Commu-nity-Acquired Sepsis Study Group (SACiUCI): C-reactive protein, anearly marker of community-acquired sepsis resolution: a multi-centerprospective observational study. Crit Care 2011;15(4):R169.
[23] Coelho L, Póvoa P, Almeida E, et al. Usefulness of C-reactive proteinin monitoring the severe community-acquired pneumonia clinicalcourse. Crit Care 2007;11(4):R92.
[24] Vincent JL, Donadello K, Schmit X. Biomarkers in the critically illpatient: C-reactive protein. Crit Care Clin 2011;27(2):241-51.