aboriginal and torres strait islander health practitioner ... · department of health: aboriginal...
TRANSCRIPT
rsion No.: <no> ; Effective From: <date> Page 1 of 23
Version No.: <no> ; Effective From: <date> Page 1 of 23
[Optional heading here. Change font size to suit]
Version No.: 1.0 Effective From: 1 July 2013 Page 1 of 23
Guideline Document Number # QH-GDL-940:2013
Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
1. Purpose
This Guideline provides recommendations regarding best practice for the clinical governance of Aboriginal and Torres Strait Islander Health Practitioners (Health Practitioners). The purpose of the document is to provide Hospital and Health Services with a standardised and comprehensive clinical governance framework which supports safety and quality in the clinical practice of Aboriginal and Torres Strait Islander Health Practitioners.
2. Scope
This Guideline provides information for all Queensland public health system employees (permanent, temporary and casual) and all organisations and individuals acting as its agents (including Visiting Medical Officers and other partners, contractors, consultants and volunteers).
The guideline is of particular relevance to service managers in the establishment and support of Aboriginal and Torres Strait Islander Health Practitioner roles.
3. Related documents
Forms and templates: Aboriginal and Torres Strait Islander Health Practitioner Practice Plan
4. Review
This Guideline is due for review on: 01/07/2016
Date of Last Review: N/A
Supersedes: N/A
5. Business area contact
Clinician Planning and Leadership
6. Approval and implementation
Policy Custodian: Jan Phillips, Executive Director, Health Systems Innovation Branch
Responsible Executive Team Member: Dr Michael Cleary, Deputy Director-General, Health Service and Clinical Innovation Division
Approving Officer: Dr Michael Cleary, Deputy Director-General, Health Service and Clinical Innovation Division
Approval date: 16 June 2013
Effective from: 1 July 2013
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 2 of 23
7. Table of contents
Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline................. 1
1. Purpose ............................................................................................................................... 1
2. Scope .................................................................................................................................. 1
3. Related documents .............................................................................................................. 1
4. Review ................................................................................................................................. 1
5. Business area contact .......................................................................................................... 1
6. Approval and implementation ............................................................................................... 1
7. Table of contents ................................................................................................................. 2
8. Background .......................................................................................................................... 3
9. Role overview ...................................................................................................................... 3
10. Clinical governance framework ............................................................................................ 4
10.1 Overview ................................................................................................................ 4
10.2 Entrance and commencement ................................................................................ 4
10.2.1 Registration ............................................................................................ 4 10.2.2 Pre-employment screening .................................................................... 5 10.2.3 Defining individual scope of practice ...................................................... 6 10.2.4 Practice plan .......................................................................................... 7 10.2.5 Professional indemnity ........................................................................... 8 10.2.6 Re-entry assessment ............................................................................. 8
10.3 Ongoing monitoring and development .................................................................... 8
10.3.1 Clinical supervision ................................................................................ 8 10.3.2 Professional support .............................................................................. 9 10.3.3 Performance appraisal and development ............................................. 10 10.3.4 Continuing professional development .................................................. 10 10.3.5 Scope of practice review ...................................................................... 11 10.3.6 Delegation ............................................................................................ 11 10.3.7 Referral ................................................................................................ 12 10.3.8 Registration status monitoring .............................................................. 13
11. Definitions of terms used in the guide and supporting documents ...................................... 14
12. References and suggested reading .................................................................................... 15
13. Consultation ....................................................................................................................... 16
Appendix 1. Course information - Clinical ..................................................................................... 18
Appendix 2. Practice plan template ............................................................................................... 20
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 3 of 23
8. Background
The Aboriginal and Torres Strait Islander Health Practitioner role became nationally registered from 1 July 2012 under the National Registration and Accreditation Scheme for health professions. It had been identified that some Aboriginal and Torres Strait Islander primary health care roles across Australia involved a significant clinical component and the performance of a number of high risk clinical activities. On this basis, Health Ministers agreed that national registration was required to provide for the protection of the public by ensuring that only health practitioners who are suitably trained and qualified to practice are registered.
The Aboriginal and Torres Strait Islander Health Practice Board of Australia (National Board) has been established to regulate the profession. With a broad aim of protecting the public and guiding the profession, the National Board establishes registration standards and professional guidelines for Aboriginal and Torres Strait Islander Health Practitioners. The website of the National Board (http://www.ahpra.gov.au/atsi.aspx) includes details about current registration standards
9. Role overview
Aboriginal and Torres Strait Islander Health Practitioners are responsible for delivering safe, high-quality clinical services and patient care. These practitioners operate in accordance with the Primary Clinical Care Manual and applicable legislation and regulations to deliver a range of clinical primary health care services to Aboriginal and Torres Strait Islander people and communities. They may assess and treat health consumers, deliver specific health care programs, maintain health care systems and provide culturally safe and appropriate advice and support in order to contribute to better health outcomes for Aboriginal and Torres Strait Islander people.
To practise as an Aboriginal and Torres Strait Islander Health Practitioner, an individual must hold registration with the National Board. In accordance with the National Board’s registration standards, registrants must be Aboriginal and/or Torres Strait Islander and must hold a Certificate IV in Aboriginal and/or Torres Strait Islander Primary Health Care (Practice) or equivalent qualification. Until 30 June 2015, applicants with other qualifications and experience may be considered for registration under the Grandparenting Provisions Registration Standard.
An Aboriginal and Torres Strait Islander Health Worker is not required to be registered unless it is necessary for employment purposes and to use the title Aboriginal and Torres Strait Islander Health Practitioner, Aboriginal Health Practitioner and/or Torres Strait Islander Health Practitioner. However, a person may independently apply for registration if they wish to do so.
The National Health Training Package outlines the competencies gained through the achievement of the Certificate IV in Aboriginal and/or Torres Strait Islander Primary Health Care (Practice) and provides information about the competency areas in which these practitioners are educated. Appendix 1 includes a list of the clinical skills on which students of the prescribed course are assessed. This information may be useful in determining the individual’s scope of practice (refer section 10.2.3).
In practice, the role of Aboriginal and Torres Strait Islander Health Practitioners will vary across Australia, depending on context, service need, organisational policy and regulatory framework. At service level, an Aboriginal and Torres Strait Islander Health Practitioner’s role will be determined by the services provided, model of care, team skill mix and roles, patient profile, supervision framework, facilities and the individual’s scope of practice.

Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 4 of 23
10. Clinical governance framework
10.1 Overview
Clinical governance refers to the systems for managing, maintaining and improving patient safety and quality of care. The diagram below illustrates the core components of a clinical governance framework for Aboriginal and Torres Strait Islander Health Practitioners.
Strong clinical governance for Aboriginal and Torres Strait Islander Health Practitioners relies on the application of a robust system of verification and endorsement processes upon the entrance and re-entrance of incumbents into these roles. The information obtained through the checking and assessment processes instituted at the outset of employment then provides a platform from which ongoing governance and development mechanisms may effectively operate.
Fig. 1 Clinical governance framework for Aboriginal and Torres Strait Islander Health Practitioners
10.2 Entrance and commencement
Each of the six governance mechanisms identified under Entrance and Commencement in the clinical governance framework presented in section 10.1, is explained below.
10.2.1 Registration
The National Board, in partnership with the Australian Health Practitioner Regulation Agency (AHPRA), is responsible for the registration of Aboriginal and Torres Strait Islander Health Practitioners.
As registration is a mandatory requirement for employment as an Aboriginal and Torres Strait Islander Health Practitioner, Hospital and Health Services should ensure that a registration status check is incorporated in the recruitment and selection process for these positions.
Registration
Pre-employment screening
Defining individual scope of practice
Practice plan
Professional indemnity
Re-entry assessment
Scope of practice review
Delegation
Referral
Registration status monitoring
ENTRANCE AND COMMENCEMENT
ONGOING MONITORING AND DEVELOPMENT
Leadership and accountability
Clinical audit
Legislation
Regulations
Clinical Service Capability Framework
Quality standards
Clinical supervision
Professional support
Performance appraisal and development (PAD)
Continuing professional development (CPD)
Primary Clinical Care Manual - Health management protocols and clinical care guidelines
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 5 of 23
Recruitment and selection processes should include a rigorous pre-employment
screening process whereby a practitioner’s
qualifications, experience and professional standing
are evaluated, verified and documented.
Hospital and Health Services should establish local processes
to ensure that a check of registration status and
conditions is incorporated in the recruitment and selection
process, and the outcome recorded in the Health
Practitioner’s personnel file.
Information about practitioner registration is readily obtained via the online Register of Practitioners on the AHPRA website (http://www.ahpra.gov.au/Registration/Registers-of-Practitioners.aspx). Importantly, in verifying registration, each of the following must be reviewed:
Profession
Registration status
Registration expiry date
Conditions
Undertakings
Reprimands
Restrictions
Notations
Where conditions or notations have been placed upon a Health Practitioner’s registration, these may impact scope of practice and should be monitored via the practice plan (refer sections 10.2.3 and 10.2.4).
Hospital and Health Services should also be aware of ongoing requirements for monitoring registration status (refer section 10.3.8).
10.2.2 Pre-employment screening
As Aboriginal and Torres Strait Islander Health Practitioners are performing clinical functions, working directly with health consumers, it is essential to verify their qualifications and experience as part of a thorough pre-employment screening process.
Hospital and Health Services should establish recruitment and selection processes which provide for the collection, evaluation, verification and recording of information about a Health Practitioner’s education, qualifications, special authorisations, licences, work experience and professional standing.
Applicants for Aboriginal and Torres Strait Islander Health Practitioner positions should be required to submit the following information:
Certificate of qualification/s
Course transcript/s showing units of study
Evidence of current registration (refer 10.2.1)
Completed clinical log book (from training course – refer Appendix 1)
Evidence of licences or special authorisations (e.g. pap smear provider licence)
Details of work history
Professional referees
Other relevant professional information
As well as providing a level of assurance about a practitioner’s training, experience and skills, the information collected and verified at this stage will form the basis for establishing the practitioner’s scope of practice (refer section 10.2.3).

Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 6 of 23
Aboriginal and Torres Strait Islander Health
Practitioners and their supervisors should work together to define a clear
scope of practice and document this in the
practice plan.
10.2.3 Defining individual scope of practice
Scope of practice refers to the activities that an individual is educated, competent and authorised to undertake (ANMC, 2007). A health practitioner’s scope of practice informs their work activities and accountabilities.
As registered health care professionals, Aboriginal and Torres Strait Islander Health Practitioners are recognised as having their own scope of practice. Although they work under direct or indirect clinical supervision, Health Practitioners may initiate and undertake a specified range of clinical activities in the normal practice of their work.
A clearly defined scope of practice has the following potential benefits:
reduces ambiguity and helps to ensure that the Health Practitioner practices safely within their scope
gives the Health Practitioner the awareness and confidence to articulate when an activity is outside scope
helps to identify activities which could reasonably be brought into scope - with or without further training
provides clear information to share with other team members to enhance mutual understanding of roles
An Aboriginal and Torres Strait Islander Health Practitioner’s scope of practice should be defined upon their commencement in a particular role and documented in their practice plan (refer section 10.2.4). The scope of practice should be periodically reviewed and redefined, and the practice plan updated (refer section 10.3.5).
Scope of practice is impacted by many factors. The following should be considered in defining (and re-defining) an Aboriginal and Torres Strait Islander Health Practitioner’s scope of practice:
Individual skills, experience and knowledge (refer section 10.2.2)
Individual training and competencies (refer Appendix 1)
Service models
Context and acuity of service provision
Skills mix in team settings
Supervision arrangements
Patient profile
Facilities
Registration conditions or notations
Legislative, regulatory and policy authorisations
Importantly, in accordance with the Health (Drugs and Poisons) Regulation, 1996, Indigenous Health Workers with Isolated Practice Authorisation who are working in specified isolated locations, have authority to supply and administer medications. Although Aboriginal and Torres Strait Islander Health Practitioners may undertake training and simulated competency assessment in medications as part of their training, they are not authorised to work with medications in Queensland unless they meet the prescribed Isolated Practice requirements.
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 7 of 23
An Aboriginal and Torres Strait Islander Health
Practitioner’s practice plan provides clear boundaries for
their professional practice and should be utilised as the
basis for ongoing clinical supervision, support and
development.
10.2.4 Practice plan
The practice plan is a document which formalises arrangements for the clinical practice and supervision of an Aboriginal and Torres Strait Islander Health Practitioner. The principal purpose of the plan is to support patient safety and high quality care with respect to the clinical practice of the Health Practitioner.
Implementation of the practice plan offers a number of key benefits:
Enhances clarity and transparency in relation to the Health Practitioner’s scope of practice and work activities
Provides a framework for clinical supervision and practice
Provides a mechanism to identify and address areas for ongoing professional learning and development.
Facilitates continuity in the event of changes in nominated clinical supervisor for the Health Practitioner
Supports effective inter-disciplinary practice, where practice plan information is shared with other team members to enhance understanding of role and scope
A practice plan template is included as Appendix 2. This template may be varied in line with local priorities and practices however it is suggested that the practice plan include the following:
Individual scope of practice (refer section 10.2.3)
Practice restrictions or exclusions (e.g. due to notations on registration)
Referral point and process
Practice objectives
Clinical supervision structure and levels of supervision
Any entry or re-entry competency review or assessment requirements
Development requirements/processes/outcomes (e.g. linked to CPD)
Formal agreement, term and review commitments
The following guidelines are recommended for the use of practice plans:
New plan developed every twelve months
Plan is reviewed at least three-monthly in Health Practitioner’s first year in the role, and at least six-monthly thereafter
Plan developed between Health Practitioner and clinical supervisor, with review and input by line manager
Plan linked with the PAD process (refer section 10.3.3)
Copies of plan retained by clinical supervisor, line manager and the Health Practitioner between reviews.
The practice plan is a particularly useful clinical governance tool for Aboriginal and Torres Strait Islander Health Practitioners since these individuals will generally work under the clinical
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 8 of 23
Aboriginal and Torres Strait Islander Health
Practitioners are covered for professional
indemnity, as documented in HR Policy
I3.
Robust pre-employment screening processes will
identify practitioners who are re-entering practice, enabling Hospital and Health Services to undertake an assessment and put appropriate clinical
supervision and support mechanisms in place.
supervision of a health practitioner from another discipline. The plan may assist the clinical supervisor in the process to build understanding about the Health Practitioner role.
To ensure the effectiveness of the practice plan as a governance mechanism, Hospital and Health Services are encouraged to tailor the plan and its use to suit local circumstances and needs.
10.2.5 Professional indemnity
Aboriginal and Torres Strait Islander Health Practitioners are required to hold professional indemnity insurance in accordance with the applicable National Board registration standard. This is an important governance mechanism, ensuring that practitioners are covered in the conduct of their practice.
Health Practitioners employed by the Chief Executive, Department of Health or Hospital and Health Services are included under HR Policy I3, “Indemnity for Queensland Health Employees and Other Persons”. Health practitioners operating within their scope of practice need not secure additional coverage in accordance with the Queensland Health Circular “Professional Indemnity Insurance Standards for Occupational Therapists, Medical Radiation Practitioners and Aboriginal and Torres Strait Islander Health Practitioners” (http://paweb.sth.health.qld.gov.au/qhot/documents/nras_prof_ind_ins_ot_mrp.pdf).
10.2.6 Re-entry assessment
The National Board’s Recency of Practice Registration Standard and related guideline describe particular requirements for Health Practitioners who have not practiced for three or more years (ATSIHPBA, 2013b). In such cases, the National Board may impose conditions upon the practitioner’s registration and require them to undertake further training or assessment.
Health practitioners re-entering practice should be assessed to determine competency and to determine individual scope of practice. Awareness of a practitioner’s lack of recent practice
experience will enable appropriate mechanisms for re-skilling, support and supervised practice to be put in place.
10.3 Ongoing monitoring and development
The clinical governance framework presented in section 10.1 identifies eight mechanisms for governance through Ongoing Monitoring and Development. These are explained below.
10.3.1 Clinical supervision
In order to ensure that Aboriginal and Torres Strait Islander Health Practitioners develop and maintain high standards of professional practice, they should have access to quality clinical supervision.
In addition to their line manager who provides administrative or operational supervision (such as a Senior Health Worker or Health Worker Coordinator), an Aboriginal and Torres Strait Islander Health Practitioner should have an identified clinical supervisor. The clinical supervisor should:
be an experienced nursing, allied health or medical clinician
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 9 of 23
It is important that Aboriginal and Torres Strait Islander Health Practitioners have an
identified clinical supervisor and agreed processes for ongoing
clinical supervision.
Aboriginal and Torres Strait Islander Health
Practitioners may benefit from having
structured professional support mechanisms in
place.
have the clinical and leadership skills to assess and support the development of the Aboriginal and Torres Strait Islander Health Practitioner’s clinical practice
have a strong understanding of how Aboriginal and Torres Strait Islander cultural issues impact on the clinical environment and be able to provide an effective and sensitive response in the management of these relationships
have capacity to observe and provide feedback on the Health Practitioner’s clinical practice
be competent to participate in clinical supervision discussions and to oversee the practice plan (refer section 10.2.4)
The Aboriginal and Torres Strait Islander Health Practitioner and their clinical supervisor should establish and maintain agreed processes for clinical supervision. These will vary depending on the individuals and work context but may include:
Periodic meetings
Practice observation
Clinical practice reflection and discussion
Case reviews
Teleconferencing or videoconferencing
It is important that a Health Practitioner has clarity about the availability and accessibility of clinical supervision and guidance. To this end, the clinical supervisor should clearly communicate:
supervision mechanisms and schedules, including back-up and remote supervision arrangements
their expectations with regard to the Health Practitioner’s clinical practice, including their level of autonomy
expected delegation and referral arrangements
requirements for direct supervision (observed practice) compared to indirect supervision (where the supervisor is accessible but not necessarily present)
It may be necessary for Health Practitioners who are new to the role to receive training on the objectives, principles and expectations of the clinical supervision process, so as to have clarity about the developmental rather than punitive nature of this type of supervision.
10.3.2 Professional support
In addition to the clinical supervision arrangements explained above, Hospital and Health Services should consider establishing other professional support mechanisms for Aboriginal and Torres Strait Islander Health Practitioners. As a new role, professional support may provide the potential for enhanced clinical practice and better understanding, utilisation and application of the role. Professional support mechanisms to be considered include:
Coaching
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 10 of 23
Hospital and Health Services should support
Aboriginal and Torres Strait Islander Health
Practitioners to maintain their registration and to
enhance and update their skills by engaging in CPD.
An Aboriginal and Torres Strait Islander Health
Practitioner’s line manager may conduct the PAD process with input from the clinical
supervisor.
Mentoring
Multi-disciplinary peer support
Aboriginal and Torres Strait Islander Health Practitioner peer support networks
Peer review
Given that Aboriginal and Torres Strait Islander Health Practitioner numbers may be low initially, it may be appropriate to establish state-wide mechanisms or networks for professional support.
10.3.3 Performance appraisal and development
For Aboriginal and Torres Strait Islander Health Practitioners, the Performance Appraisal and Development (PAD) process should be led by the line manager, rather than the clinical supervisor. The line manager is well-placed to appraise the Health Practitioner, and to provide feedback and guidance about their development, progression and career aspirations.
Clinical practice and professional development matters being addressed through the practice plan should be referenced during
the PAD process. Open communication between the two supervisors should enable the clinical supervisor to provide valuable input about the practitioner’s clinical practice and development needs, into the appraisal and development process.
10.3.4 Continuing professional development
Aboriginal and Torres Strait Islander Health Practitioners are required to engage in continuing professional development (CPD) as a condition of registration. This ongoing learning enables Health Practitioners to extend their knowledge and skills and to ensure they stay up-to-date with contemporary practice.
The Registration Standard for CPD stipulates that registrants undertake 60 hours of documented CPD every three years (minimum of 10 hours in any one year) and that 75 per cent of this involve formal learning activities (ATSIHPBA, 2013a). The National Board’s CPD guideline identifies acceptable formal and non-formal CPD activities as follows: Formal learning activities
Tertiary courses
Accredited courses
Conferences, forums and seminars
Undertaking research and presentation of work
Courses leading to a certificate, diploma, degree or higher degree
Online learning (interactive discussion and chat rooms)
In-service education programs
Making presentations
Videoconferencing

Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 11 of 23
Hospital and Health Services should ensure that
Aboriginal and Torres Strait Islander Health Practitioners and their supervisors work
together to periodically review and develop the practitioner’s scope of
practice.
Aboriginal and Torres Strait Islander Health
Practitioners are responsible for the
completion of clinical tasks delegated to them
by their clinical supervisor or other clinicians.
Non-formal and incidental learning activities
Reflecting on experience in day-to-day activities
Reading books, journals, etc
Secondment and/or contact with other health professionals
Quality assurance activities, such as accreditation
Participation in committees
Information sharing at meetings
Discussion with colleagues
Internet research Aboriginal and Torres Strait Islander Health Practitioners should be supported to ensure they fulfil their CPD requirements for ongoing registration.
10.3.5 Scope of practice review
Following initial definition of the Aboriginal and Torres Strait Islander Health Practitioner’s scope of practice (refer section 10.2.3), scope should be the subject of ongoing discussion and review between the practitioner and their clinical supervisor. The practice plan and clinical supervision arrangements provide the vehicle for ongoing assessment and redefinition of scope of practice.
Other team members should be made aware of key changes to the Aboriginal and Torres Strait Islander Health Practitioner’s scope of practice as these may impact team roles, delegation and other service delivery.
10.3.6 Delegation
Aboriginal and Torres Strait Islander Health Practitioners may be required to take responsibility for clinical tasks that have been delegated to them by other clinicians, where these tasks are within their scope of practice. Hospital and Health Services should ensure that delegation is guided by clear and formal processes to ensure patient safety and quality of care.
In delegating to an Aboriginal and Torres Strait Islander Health Practitioner, a clinician should ensure that the task is:
Within the clinician’s own scope of practice
Within the Aboriginal and Torres Strait Islander Health Practitioner’s scope of practice
Lawful
Appropriate in the context of the patient’s care
Consistent with the standards of the Aboriginal and Torres Strait Islander health practice profession
With consideration to the patient’s cultural needs
Consistent with Hospital and Health Service policy (ANMC,
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 12 of 23
It is important that Aboriginal and Torres Strait Islander Health Practitioners have a clear understanding of their responsibilities in
making and receiving client referrals, with particular consideration to client
cultural needs.
2007)
In delegating a task, the delegating clinician shares accountability for its completion, and therefore may be expected to undertake an assessment to determine that the activity is within the Aboriginal and Torres Strait Islander Health Practitioner’s scope of practice, and to provide instruction, training and clinically-focussed supervision where required to ensure safe completion of the delegated task (Queensland Health, 2013).
In accepting a delegated activity, an Aboriginal and Torres Strait Islander Health Practitioner:
Acknowledges that they accept the delegated task
Agrees that the task is within their scope of practice
Agrees not to further delegate the delegated task
Acknowledges their degree of accountability for performing the task
10.3.7 Referral
Aboriginal and Torres Strait Islander Health Practitioners may work in multidisciplinary teams where high quality service delivery requires team members to have good communication, a good understanding of each other’s skills and responsibilities, and respect for the diversity and value of all members’ contributions. Teamwork of this nature also provides the basis for timely, appropriate and effective referrals.
Aboriginal and Torres Strait Islander Health Practitioners may need to refer patients to other health professionals, or they may receive patient referrals to provide some aspect of their care. In
receiving referrals, Aboriginal and Torres Strait Islander Health Practitioners take responsibility for the referred aspect of patient care and must ensure that the required clinical activities are within their scope of practice.
As with delegation processes, Hospital and Health Services should ensure that referral processes are clear and formal. Specific referral arrangements and expectations, tailored to the local staffing and service model, should be discussed with the clinical supervisor and recorded in the Aboriginal and Torres Strait Islander Health Practitioner’s practice plan (refer section 10.2.4).
In making referrals, the referring health practitioner should ensure that the referral is:
Based upon clinical assessment of patient need
With consideration to the patient’s cultural needs
Within the authority of the referring health practitioner
Within the scope of practice of the health practitioner receiving the referral
Consistent with Hospital and Health Service policy
Supported by appropriate and sufficient communication and information about the patient and their treatment to enable continuing care (ANMC, 2007)
In accepting a referral, the health practitioner:
Acknowledges that they accept the referral
Agrees that the task is within their scope of practice
Acknowledges their degree of accountability for performing the task

Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 13 of 23
Hospital and Health Services should establish local processes to ensure
that the registration status of each Aboriginal and Torres Strait Islander
Health Practitioner is verified annually.
Understands requirements to provide communication and information to the referring health professional.
10.3.8 Registration status monitoring
The ongoing monitoring of health practitioners’ registration status is as important as the initial pre-employment check. Hospital and Health Services should ensure that mechanisms are in place to verify that Aboriginal and Torres Strait Islander Health Practitioners maintain their registration and to be made aware of altered conditions or notations (refer section 10.2.1).
The National Board operates a standardised annual registration cycle ending on 30 November, thus registration status checks should be in place to ensure evidence of ongoing registration from 1 December annually.
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 14 of 23
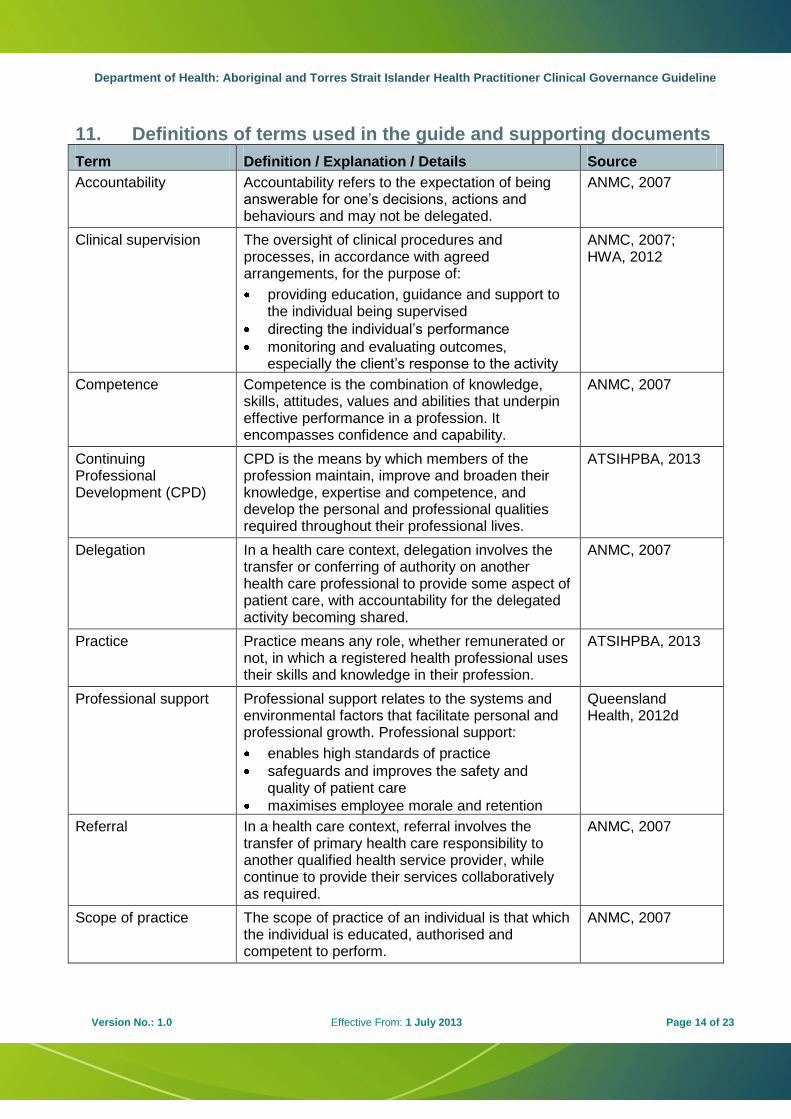
11. Definitions of terms used in the guide and supporting documents
Term Definition / Explanation / Details Source
Accountability Accountability refers to the expectation of being answerable for one’s decisions, actions and behaviours and may not be delegated.
ANMC, 2007
Clinical supervision The oversight of clinical procedures and processes, in accordance with agreed arrangements, for the purpose of:
providing education, guidance and support to the individual being supervised
directing the individual’s performance
monitoring and evaluating outcomes, especially the client’s response to the activity
ANMC, 2007; HWA, 2012
Competence Competence is the combination of knowledge, skills, attitudes, values and abilities that underpin effective performance in a profession. It encompasses confidence and capability.
ANMC, 2007
Continuing Professional Development (CPD)
CPD is the means by which members of the profession maintain, improve and broaden their knowledge, expertise and competence, and develop the personal and professional qualities required throughout their professional lives.
ATSIHPBA, 2013
Delegation In a health care context, delegation involves the transfer or conferring of authority on another health care professional to provide some aspect of patient care, with accountability for the delegated activity becoming shared.
ANMC, 2007
Practice Practice means any role, whether remunerated or not, in which a registered health professional uses their skills and knowledge in their profession.
ATSIHPBA, 2013
Professional support Professional support relates to the systems and environmental factors that facilitate personal and professional growth. Professional support:
enables high standards of practice
safeguards and improves the safety and quality of patient care
maximises employee morale and retention
Queensland Health, 2012d
Referral In a health care context, referral involves the transfer of primary health care responsibility to another qualified health service provider, while continue to provide their services collaboratively as required.
ANMC, 2007
Scope of practice The scope of practice of an individual is that which the individual is educated, authorised and competent to perform.
ANMC, 2007
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 15 of 23
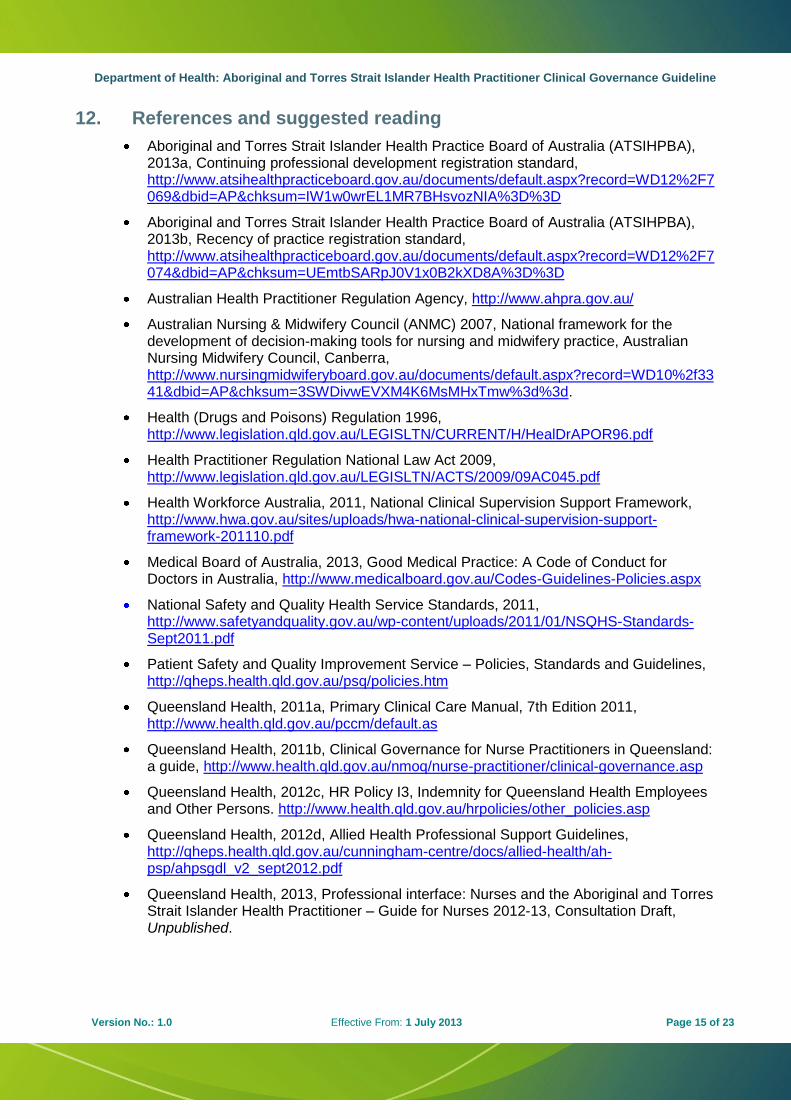
12. References and suggested reading
Aboriginal and Torres Strait Islander Health Practice Board of Australia (ATSIHPBA), 2013a, Continuing professional development registration standard, http://www.atsihealthpracticeboard.gov.au/documents/default.aspx?record=WD12%2F7069&dbid=AP&chksum=IW1w0wrEL1MR7BHsvozNIA%3D%3D
Aboriginal and Torres Strait Islander Health Practice Board of Australia (ATSIHPBA), 2013b, Recency of practice registration standard, http://www.atsihealthpracticeboard.gov.au/documents/default.aspx?record=WD12%2F7074&dbid=AP&chksum=UEmtbSARpJ0V1x0B2kXD8A%3D%3D
Australian Health Practitioner Regulation Agency, http://www.ahpra.gov.au/
Australian Nursing & Midwifery Council (ANMC) 2007, National framework for the development of decision-making tools for nursing and midwifery practice, Australian Nursing Midwifery Council, Canberra, http://www.nursingmidwiferyboard.gov.au/documents/default.aspx?record=WD10%2f3341&dbid=AP&chksum=3SWDivwEVXM4K6MsMHxTmw%3d%3d.
Health (Drugs and Poisons) Regulation 1996, http://www.legislation.qld.gov.au/LEGISLTN/CURRENT/H/HealDrAPOR96.pdf
Health Practitioner Regulation National Law Act 2009, http://www.legislation.qld.gov.au/LEGISLTN/ACTS/2009/09AC045.pdf
Health Workforce Australia, 2011, National Clinical Supervision Support Framework, http://www.hwa.gov.au/sites/uploads/hwa-national-clinical-supervision-support-framework-201110.pdf
Medical Board of Australia, 2013, Good Medical Practice: A Code of Conduct for Doctors in Australia, http://www.medicalboard.gov.au/Codes-Guidelines-Policies.aspx
National Safety and Quality Health Service Standards, 2011, http://www.safetyandquality.gov.au/wp-content/uploads/2011/01/NSQHS-Standards-Sept2011.pdf
Patient Safety and Quality Improvement Service – Policies, Standards and Guidelines, http://qheps.health.qld.gov.au/psq/policies.htm
Queensland Health, 2011a, Primary Clinical Care Manual, 7th Edition 2011, http://www.health.qld.gov.au/pccm/default.as
Queensland Health, 2011b, Clinical Governance for Nurse Practitioners in Queensland: a guide, http://www.health.qld.gov.au/nmoq/nurse-practitioner/clinical-governance.asp
Queensland Health, 2012c, HR Policy I3, Indemnity for Queensland Health Employees and Other Persons. http://www.health.qld.gov.au/hrpolicies/other_policies.asp
Queensland Health, 2012d, Allied Health Professional Support Guidelines, http://qheps.health.qld.gov.au/cunningham-centre/docs/allied-health/ah-psp/ahpsgdl_v2_sept2012.pdf
Queensland Health, 2013, Professional interface: Nurses and the Aboriginal and Torres Strait Islander Health Practitioner – Guide for Nurses 2012-13, Consultation Draft, Unpublished.
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 16 of 23
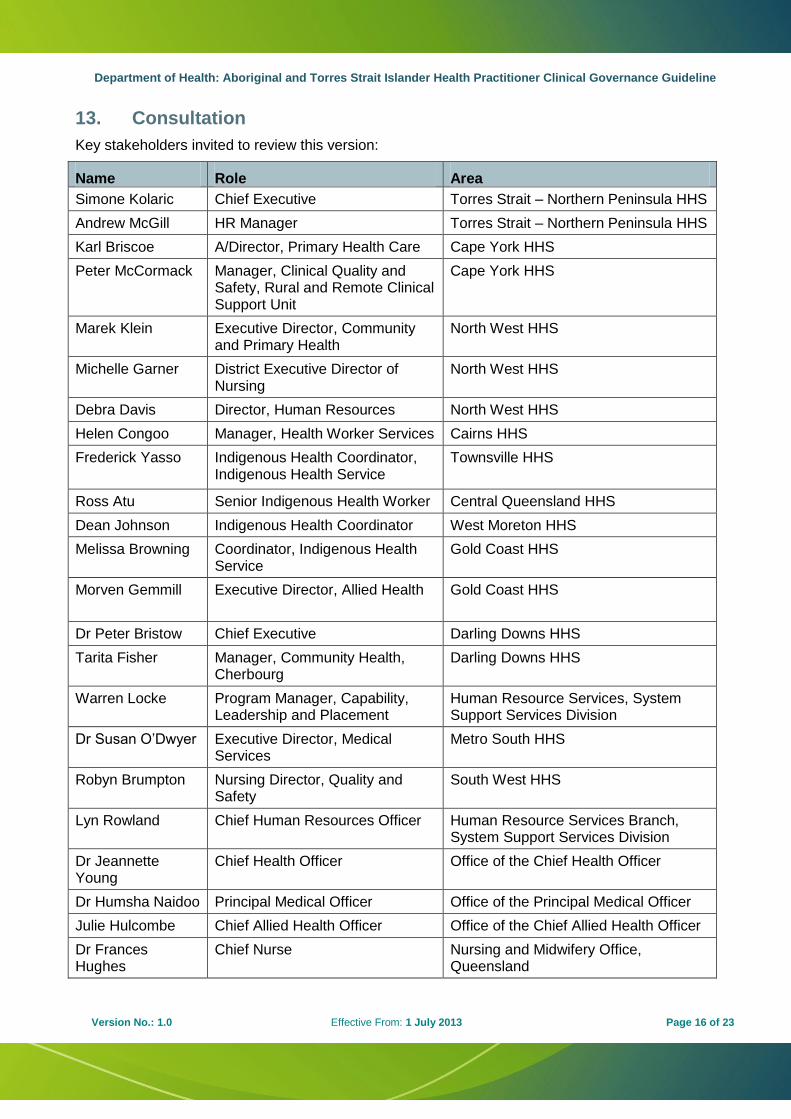
13. Consultation
Key stakeholders invited to review this version:
Name Role Area
Simone Kolaric Chief Executive Torres Strait – Northern Peninsula HHS
Andrew McGill HR Manager Torres Strait – Northern Peninsula HHS
Karl Briscoe A/Director, Primary Health Care Cape York HHS
Peter McCormack Manager, Clinical Quality and Safety, Rural and Remote Clinical Support Unit
Cape York HHS
Marek Klein Executive Director, Community and Primary Health
North West HHS
Michelle Garner District Executive Director of Nursing
North West HHS
Debra Davis Director, Human Resources North West HHS
Helen Congoo Manager, Health Worker Services Cairns HHS
Frederick Yasso Indigenous Health Coordinator, Indigenous Health Service
Townsville HHS
Ross Atu Senior Indigenous Health Worker Central Queensland HHS
Dean Johnson Indigenous Health Coordinator West Moreton HHS
Melissa Browning Coordinator, Indigenous Health Service
Gold Coast HHS
Morven Gemmill Executive Director, Allied Health Gold Coast HHS
Dr Peter Bristow Chief Executive Darling Downs HHS
Tarita Fisher Manager, Community Health, Cherbourg
Darling Downs HHS
Warren Locke Program Manager, Capability, Leadership and Placement
Human Resource Services, System Support Services Division
Dr Susan O’Dwyer Executive Director, Medical Services
Metro South HHS
Robyn Brumpton Nursing Director, Quality and Safety
South West HHS
Lyn Rowland Chief Human Resources Officer Human Resource Services Branch, System Support Services Division
Dr Jeannette Young
Chief Health Officer Office of the Chief Health Officer
Dr Humsha Naidoo Principal Medical Officer Office of the Principal Medical Officer
Julie Hulcombe Chief Allied Health Officer Office of the Chief Allied Health Officer
Dr Frances Hughes
Chief Nurse Nursing and Midwifery Office, Queensland
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 17 of 23
Name Role Area
Nola Simpson Manager, Regulatory Instruments Unit
Policy and Planning Branch, System Policy and Performance Division
Elizabeth Robertson
Nursing Director, Patient Safety Unit
Health Systems Innovation Branch, Health Service and Clinical Innovation Division
Colleen Jen Senior Director Policy and Planning Branch, Systems Policy and Performance Division
Michael Zanco Executive Director Clinical Access and Redesign Unit, Health Systems Innovation Branch, Health Service and Clinical Innovation Division
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 18 of 23
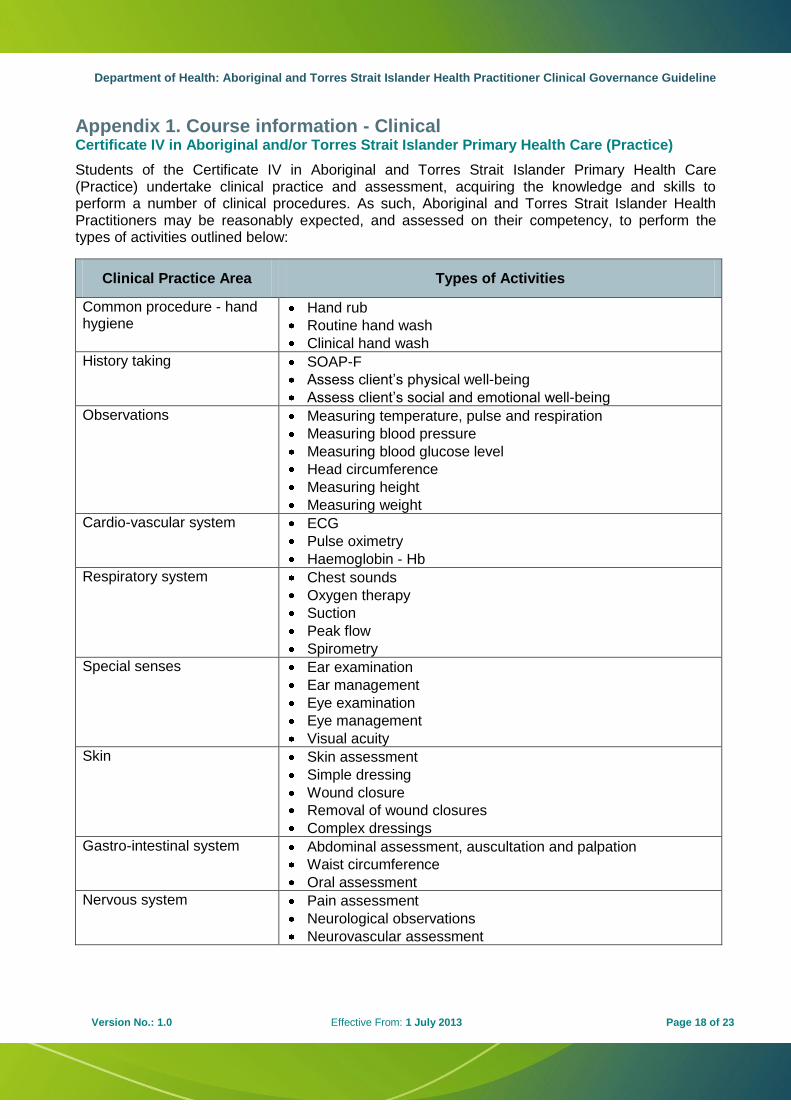
Appendix 1. Course information - Clinical Certificate IV in Aboriginal and/or Torres Strait Islander Primary Health Care (Practice)
Students of the Certificate IV in Aboriginal and Torres Strait Islander Primary Health Care (Practice) undertake clinical practice and assessment, acquiring the knowledge and skills to perform a number of clinical procedures. As such, Aboriginal and Torres Strait Islander Health Practitioners may be reasonably expected, and assessed on their competency, to perform the types of activities outlined below:
Clinical Practice Area Types of Activities
Common procedure - hand hygiene
Hand rub
Routine hand wash
Clinical hand wash
History taking SOAP-F
Assess client’s physical well-being
Assess client’s social and emotional well-being
Observations Measuring temperature, pulse and respiration
Measuring blood pressure
Measuring blood glucose level
Head circumference
Measuring height
Measuring weight
Cardio-vascular system ECG
Pulse oximetry
Haemoglobin - Hb
Respiratory system Chest sounds
Oxygen therapy
Suction
Peak flow
Spirometry
Special senses Ear examination
Ear management
Eye examination
Eye management
Visual acuity
Skin Skin assessment
Simple dressing
Wound closure
Removal of wound closures
Complex dressings
Gastro-intestinal system
Abdominal assessment, auscultation and palpation
Waist circumference
Oral assessment
Nervous system
Pain assessment
Neurological observations
Neurovascular assessment
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 19 of 23
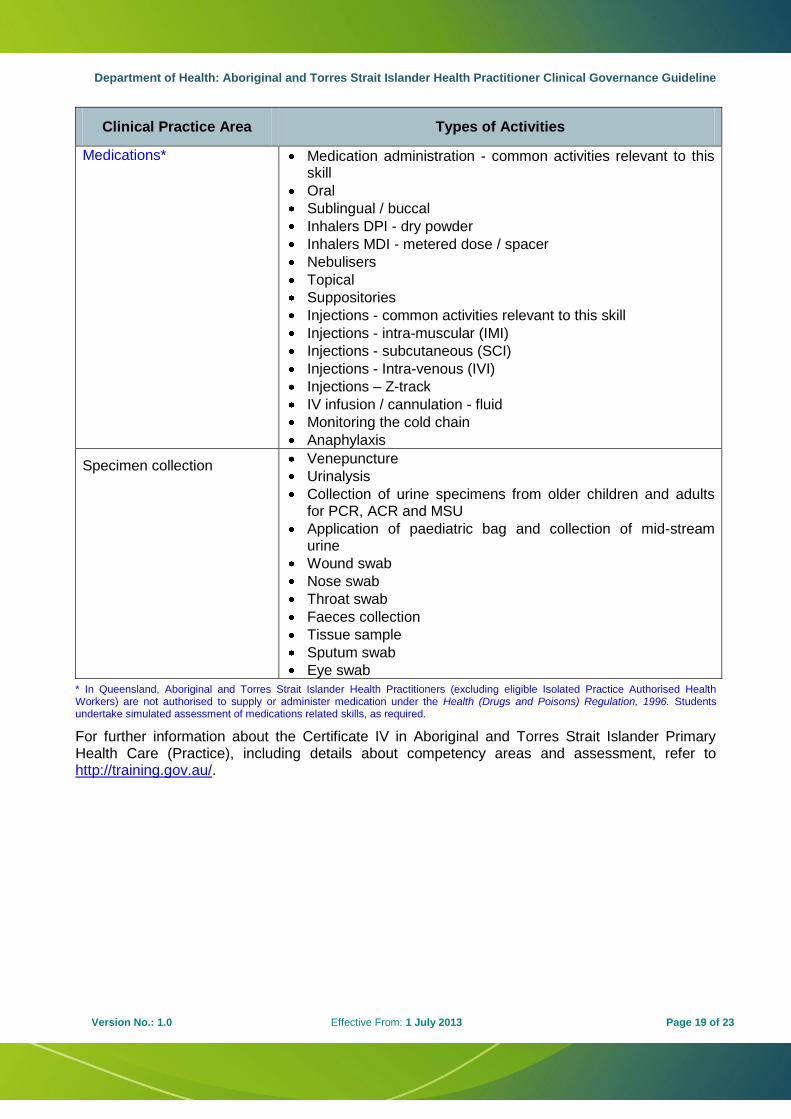
Clinical Practice Area Types of Activities
Medications* Medication administration - common activities relevant to this skill
Oral
Sublingual / buccal
Inhalers DPI - dry powder
Inhalers MDI - metered dose / spacer
Nebulisers
Topical
Suppositories
Injections - common activities relevant to this skill
Injections - intra-muscular (IMI)
Injections - subcutaneous (SCI)
Injections - Intra-venous (IVI)
Injections – Z-track
IV infusion / cannulation - fluid
Monitoring the cold chain
Anaphylaxis
Specimen collection Venepuncture
Urinalysis
Collection of urine specimens from older children and adults for PCR, ACR and MSU
Application of paediatric bag and collection of mid-stream urine
Wound swab
Nose swab
Throat swab
Faeces collection
Tissue sample
Sputum swab
Eye swab
* In Queensland, Aboriginal and Torres Strait Islander Health Practitioners (excluding eligible Isolated Practice Authorised Health Workers) are not authorised to supply or administer medication under the Health (Drugs and Poisons) Regulation, 1996. Students undertake simulated assessment of medications related skills, as required.
For further information about the Certificate IV in Aboriginal and Torres Strait Islander Primary Health Care (Practice), including details about competency areas and assessment, refer to http://training.gov.au/.
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 20 of 23
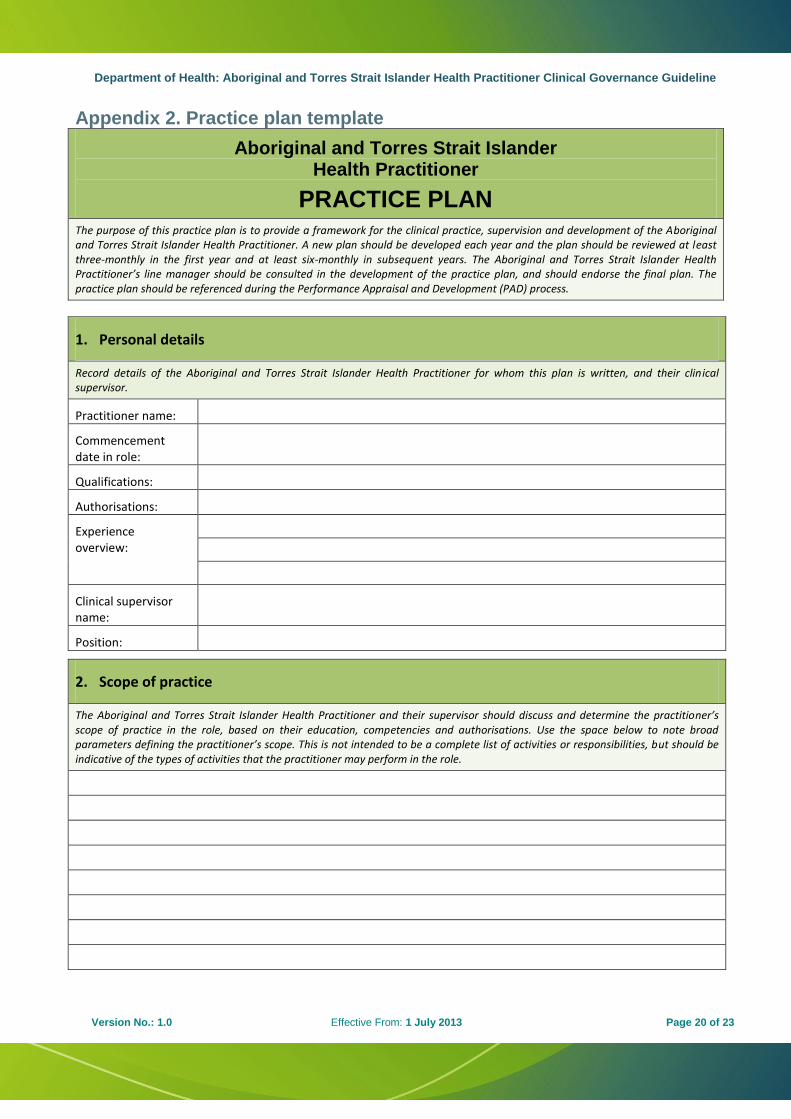
Appendix 2. Practice plan template
Aboriginal and Torres Strait Islander Health Practitioner
PRACTICE PLAN
The purpose of this practice plan is to provide a framework for the clinical practice, supervision and development of the Aboriginal and Torres Strait Islander Health Practitioner. A new plan should be developed each year and the plan should be reviewed at least three-monthly in the first year and at least six-monthly in subsequent years. The Aboriginal and Torres Strait Islander Health Practitioner’s line manager should be consulted in the development of the practice plan, and should endorse the final plan. The practice plan should be referenced during the Performance Appraisal and Development (PAD) process.
1. Personal details
Record details of the Aboriginal and Torres Strait Islander Health Practitioner for whom this plan is written, and their clinical supervisor.
Practitioner name:
Commencement date in role:
Qualifications:
Authorisations:
Experience overview:
Clinical supervisor name:
Position:
2. Scope of practice
The Aboriginal and Torres Strait Islander Health Practitioner and their supervisor should discuss and determine the practitioner’s scope of practice in the role, based on their education, competencies and authorisations. Use the space below to note broad parameters defining the practitioner’s scope. This is not intended to be a complete list of activities or responsibilities, but should be indicative of the types of activities that the practitioner may perform in the role.
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 21 of 23
3. Practice restrictions and exclusions
The Aboriginal and Torres Strait Islander Health Practitioner and their supervisor should discuss and determine any particular practice restrictions or exclusions for the practitioner, that is, activities which are outside their scope of practice and which should not be performed.
4. Practice referrals
The Aboriginal and Torres Strait Islander Health Practitioner and their supervisor should discuss and agree upon an appropriate referral process and referral parameters, considering the scope of practice of the practitioner and the particular clinical setting.
Clinical assessment process for determining need for referral:
Types of clinical tasks likely to be referred:
Practitioners to whom clinical referrals are likely to be made:
Agreed referral process:
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 22 of 23
5. Practice development plan
The Aboriginal and Torres Strait Islander Health Practitioner and their supervisor should discuss clinical practice aspirations and expectations within the practitioner’s scope of practice. Use this section to record agreements about clinical practice objectives and development needs.
Clinical practice objective for the practitioner’s clinical practice for the next 12 months:
Clinical practice development priorities i.e. experience and/or competencies the practitioner needs to develop in order to achieve the practice objective:
Specific plans for achievement of development priorities (e.g. supervised practice, CPD, practice assessment etc.)
6. Clinical supervision arrangements
The Aboriginal and Torres Strait Islander Health Practitioner and their clinical supervisor should discuss and reach agreement about the supervision arrangements that will be in place for the implementation of the practice plan.
Agreed supervision structure that will be in place for the duration of the plan (e.g. Fortnightly meetings, monthly case review, etc). Include expected duration and location of meetings and any resource requirements:
Arrangements for access to clinical supervisor between supervision sessions:
Department of Health: Aboriginal and Torres Strait Islander Health Practitioner Clinical Governance Guideline
Version No.: 1.0 Effective From: 1 July 2013 Page 23 of 23
Clinical supervision arrangements (continued)
Process for practice conflict and/or dispute resolution:
Types of activities for which direct supervision by the clinical supervisor is required (i.e. observed practice):
Types of activities for which indirect supervision is acceptable (i.e. clinical supervisor is accessible but need not observe practice).
7. Agreement
Practice plan start date: End date:
Review date 1:
Review date 2:
Review date 3:
Aboriginal and Torres Strait Islander Health Practitioner name:
Signed: Date:
Clinical supervisor name:
Signed: Date:
Line manager name:
Signed: Date: