abnormal pupil reactions
TRANSCRIPT

Abnormal Pupil Reactions
Hatlan Alhatlan
211525898

Pupil ?

Function of The Pupil
• The pupil serves an important function to the eye , as it controls the amount of the light that enters the eye , and it does so by the help of the Iris:
• Sphincter muscle(constrictor) Dilator muscle
(Circular) (Radial)

Physiology of The Pupil
• Knowing the physiology is must :
• The parasympathetic pathway :controls the constrictor pupillaemuscle , serves as the pupillary light reflux :
• Also as near , orbicularisand trigeminal
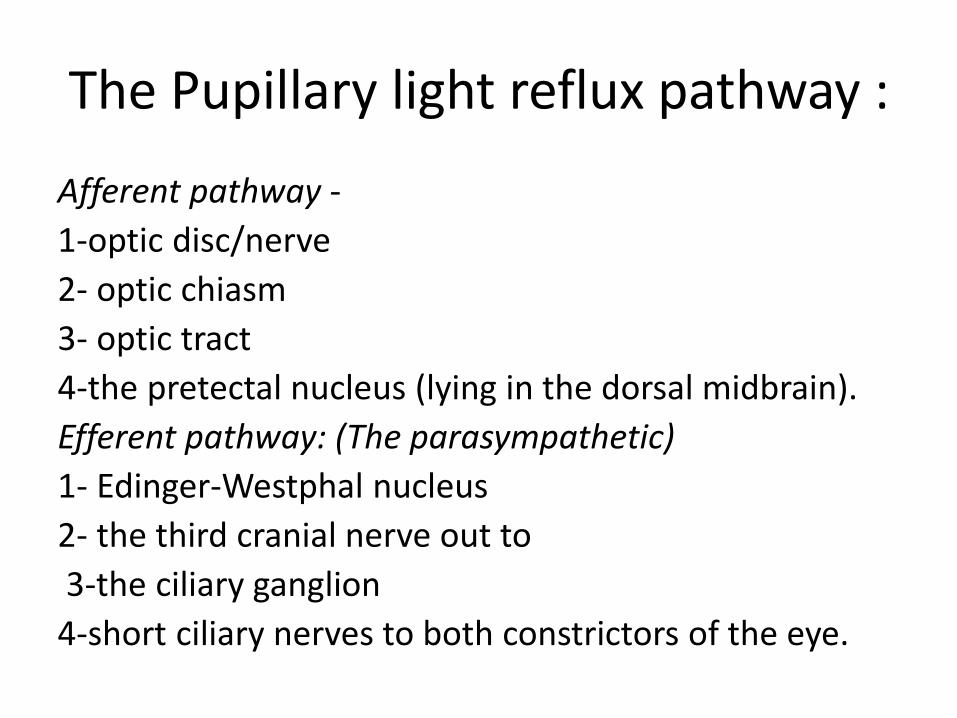
The Pupillary light reflux pathway :
Afferent pathway -
1-optic disc/nerve
2- optic chiasm
3- optic tract
4-the pretectal nucleus (lying in the dorsal midbrain).
Efferent pathway: (The parasympathetic)
1- Edinger-Westphal nucleus
2- the third cranial nerve out to
3-the ciliary ganglion
4-short ciliary nerves to both constrictors of the eye.

The Sympathetic Pathway
• The sympathetic pathway controls the dilator papillae muscle :
• For withdrawal , emotional fear and vestibular reflex.
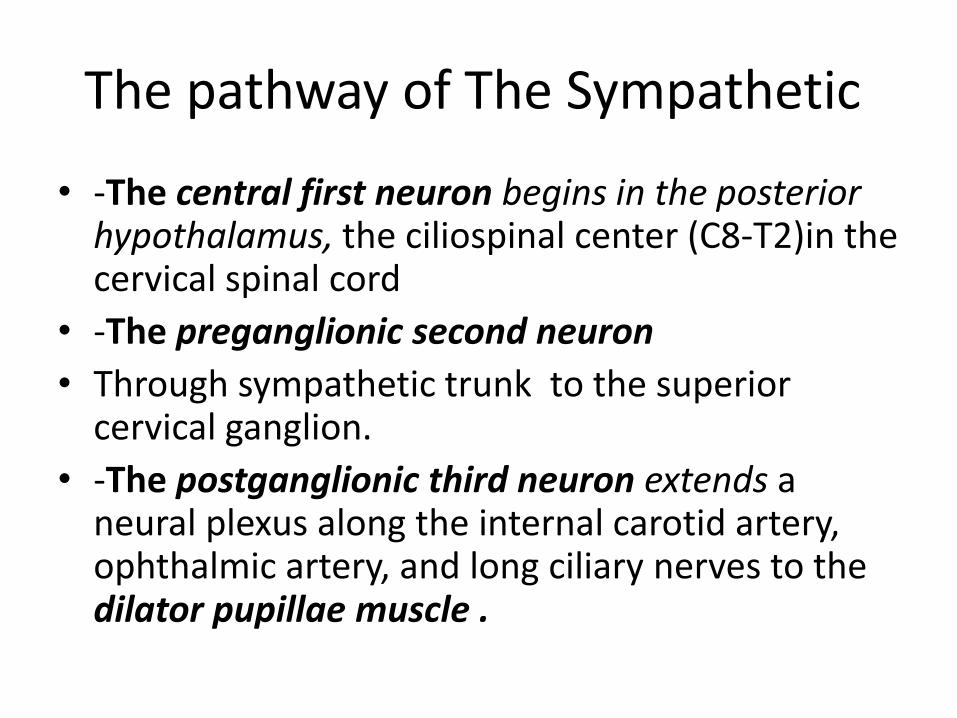
The pathway of The Sympathetic
• -The central first neuron begins in the posterior hypothalamus, the ciliospinal center (C8-T2)in the cervical spinal cord
• -The preganglionic second neuron
• Through sympathetic trunk to the superior cervical ganglion.
• -The postganglionic third neuron extends a neural plexus along the internal carotid artery, ophthalmic artery, and long ciliary nerves to the dilator pupillae muscle .

Let’s Start to evaluate the Pupil
• General examination of the patient
• Provide helpful clues as to what is going on, particularly where there is an underlying neurological cause.
• Telltale neck scar and associated ptosis in patients with Horner's syndrome or a neurosurgical scar in patients with a 3rd nerve palsy.

Pupil Examination
• Important terminologies :
• Examination consists of four steps :
AnisocoriaIsocoria
Unequal pupils size (efferent or unilateral)
Equal pupils size (afferent or
bilateral)

1-Pupil Observation
• Start by a general observation, noting
1. The shape
2. The size of the pupil in ambient bright light. Size is measured in millimetres and the normal pupil ranges from 1-8 mm.
3. The symmetry.
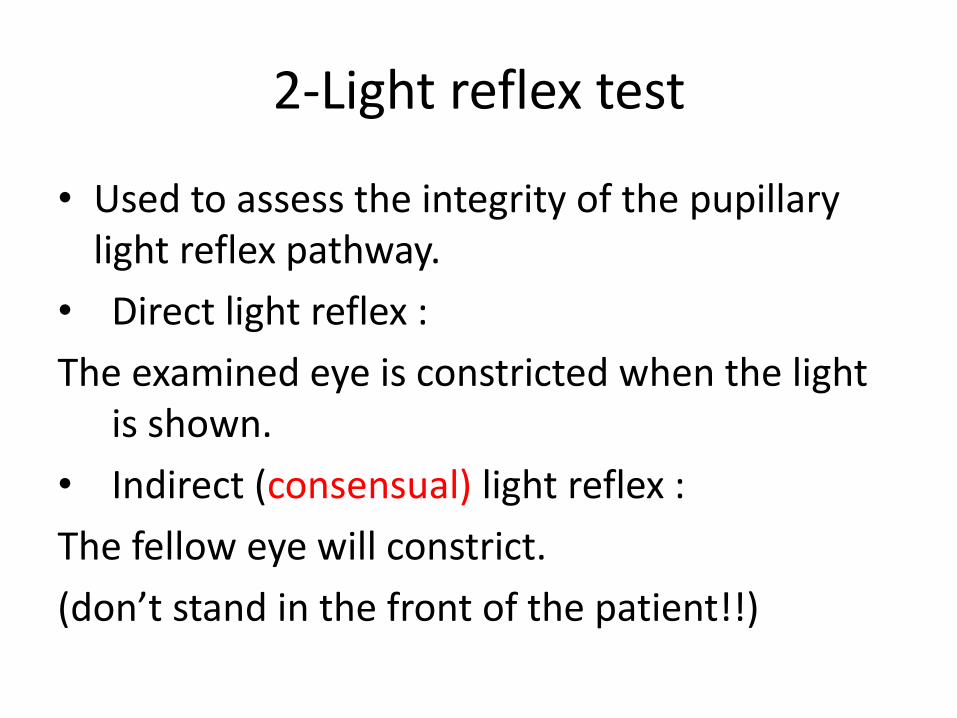
2-Light reflex test
• Used to assess the integrity of the pupillarylight reflex pathway.
• Direct light reflex :
The examined eye is constricted when the light is shown.
• Indirect (consensual) light reflex :
The fellow eye will constrict.
(don’t stand in the front of the patient!!)

Indirect Light Reflex Test

3- Swinging Flashlight Test
• Also known as (Marcus gunn test).
• Used to compare between direct and consensual light reflex.
• It’s preformed by equal exposure of light to each eye.
• Normally both pupils should be of the same size and constricted.
• Abnormally if the pupil dilate if light is shown.

• That’s caused by withdrawal reflex of the fellow eye.
• Called as RAPD (relative afferent pupillarydefect).

Near Reflex
• Used to test accommodation.
• Preformed by asking the patient to fixed at distant the to bring it to a near object (arm’s length).
• Normally the pupil will have a brisk constriction.
• Near-light dissociation =significant better pupillary near reflex than light reflex.
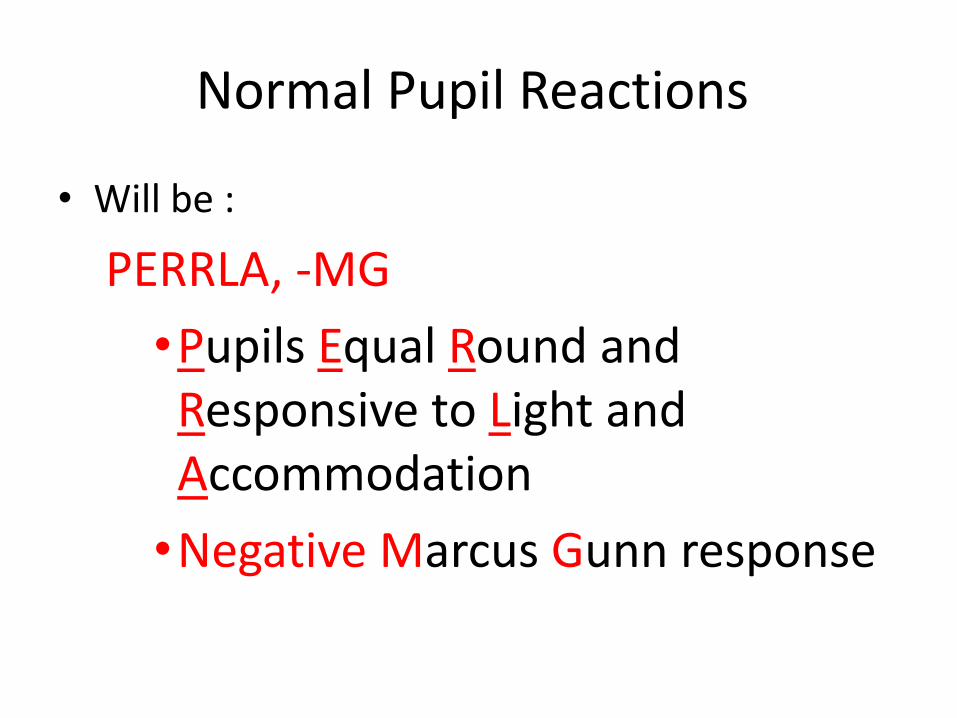
Normal Pupil Reactions
• Will be :
PERRLA, -MG
•Pupils Equal Round and Responsive to Light and Accommodation
•Negative Marcus Gunn response

Diagnosis Keys
• Determine which pupil is abnormal.
• Search for associated signs.
Disorders of the pupil may result from:
• Ocular disease.
• Disorders of the controlling neurological pathway.
• Pharmacological action.
Anisocoria
• This is physiological in about 20% of people.
• How to assess it :
• An affected Large Pupil has poor constriction in a well lit room.
• An affected small pupil has poor dilatation in well lit room.
The abnormally reacting pupil
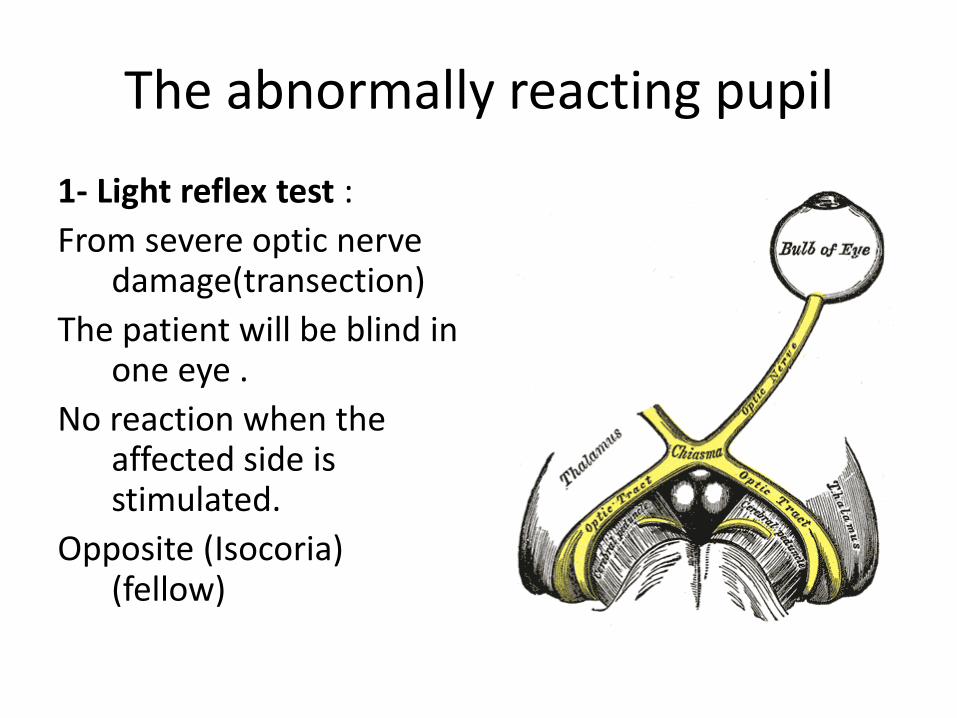
1- Light reflex test :
From severe optic nerve damage(transection)
The patient will be blind in one eye .
No reaction when the affected side is stimulated.
Opposite (Isocoria) (fellow)

The abnormally Reacting Pupil
2- Swinging flashlight test:when the pupil exhibits an RAPD, it is described as a Marcus Gunn pupil. It suggests:
• Optic nerve disease, central retinal artery or vein, A mild RAPD may also occur in amblyopia .
The abnormally Reacting Pupil
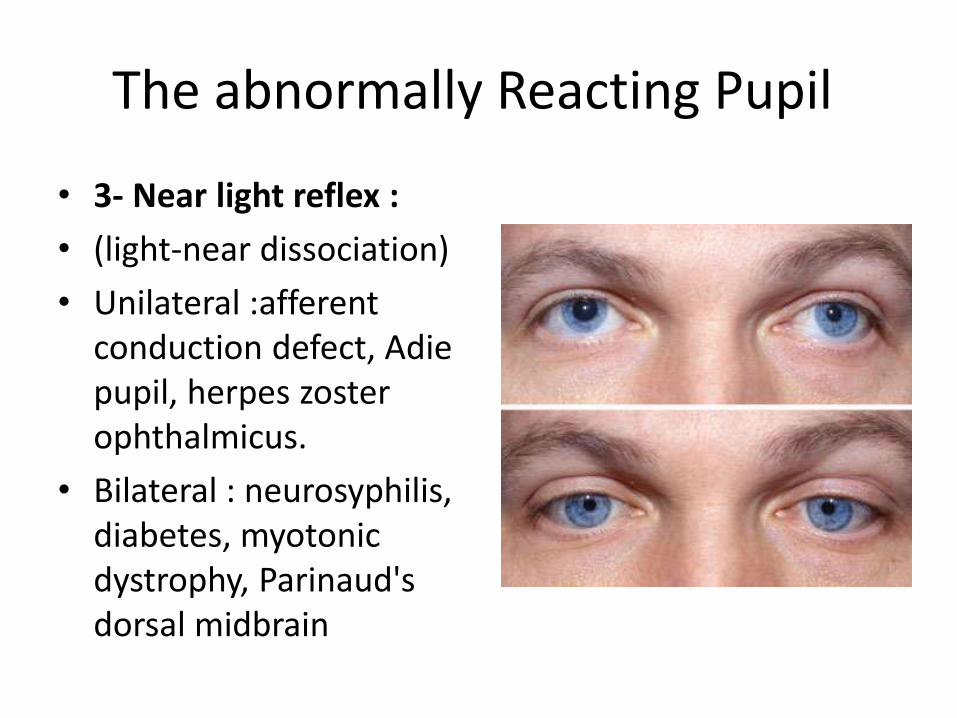
• 3- Near light reflex :
• (light-near dissociation)
• Unilateral :afferent conduction defect, Adie pupil, herpes zoster ophthalmicus.
• Bilateral : neurosyphilis, diabetes, myotonicdystrophy, Parinaud'sdorsal midbrain

Diseases affecting the pupils
• Congenital : 1. Aniridia : bilateral
absence pupil. (Glaucoma)
2. Coloboma : partial absence of pupil.
3. Leukocoria : White pupil (retinoblastoma or congenital cataract)

Diseases affecting the pupils
• Acquired :
1. Pseudoexfoliation
syndrome :grey-white
fibrogranular extracellular matrix material deposited on the anterior lens.
2. Sphincter tear: due to trauma
3. Synechiae : post. between iris +lens or ant. Between iris and cornea.

Diseases affecting the pupils
• Neurological :1- Horner’s syndrome :disruption of the sympathetic
nerves supplying the eye.Triad of : • Partial ptosis (upper eyelid
drooping).• Miosis (pupillary constriction).• Enophthalmos .• (Normal pupillary reaction)
• Causes : Many causes : 1. Central : Multiple
sclerosis, spinal cord tumors Syringomyelia.
2. Preganglionic: Pancoast's tumour
3. Postganglionic : internal Carotid dissection

Horner’s syndrome :

2- 3rd cranial nerve palsy :
• Fixed and dilated pupil not reacting to light .
• Many causes at base of skull.
• Ptosis and 4 EOM paralysis , except lateral rectus and superior oblique.

3rd Nerve Palsy
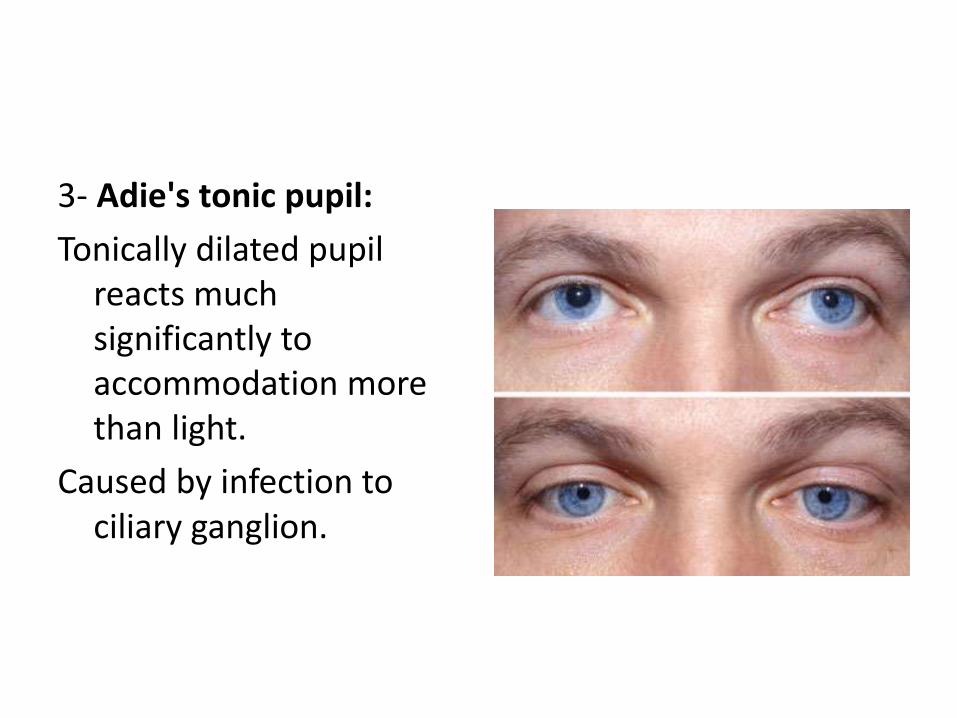
3- Adie's tonic pupil:
Tonically dilated pupil reacts much significantly to accommodation more than light.
Caused by infection to ciliary ganglion.

4-Argyll Robertson pupils: Caused by neurosyphilis.
They are characterized by bilateral (usually asymmetrical) small, irregular pupils showing a light-near dissociation.
Difficult to dilate.

Drugs Affecting Pupil
•Mydriatics (bilateral or unilateral )
• Topical : sympathomimetics(eg, phenylephrine, adrenaline) and antimuscarinics (eg, cyclopentolate, tropicamide, atropine).
• Systemic: sympathomimetics (eg, adrenaline (epinephrine)) and antimuscarinics (eg, atropine).
•Miotics (bilateral or unilateral)
• Topical : muscarinicagonists (eg, pilocarpine).
• Systemic: opiates (eg, morphine and organophosphates).

Remember :
• Take a good history to help exclude an ocular cause for the pupillary changes and to see if a medical condition exists which may contribute to the pupillary problem.
• Determine whether it is the small or the large pupil that is abnormal.
• Search for associated signs that may help make a diagnosis.
Resources :
• http://www.patient.co.uk/
• Lecture notes on ophthalmology 9th edition.

Thanxxxxxxxxxx