abnormal psychology third canadian edition prepared by: tracy vaillancourt, ph.d. chapter 11...
TRANSCRIPT
abnormal PSYCHOLOGY
Third Canadian Edition
Prepared by: Tracy Vaillancourt, Ph.D.
Chapter 11Chapter 11Schizophrenia
Schizophrenia
• Psychotic disorder characterized by major disturbances in thought, emotion, and behaviour– disordered thinking in which ideas are not
logically related– faulty perception and attention– flat or inappropriate affect– bizarre disturbances in motor activity
Prevalence and Comorbidity
• Prevalence = 1% of general population – usually appears in late adolescence or early
adulthood– appears earlier for men than for women
• Comorbid Conditions– substance abuse (70%)– depression (40%) – anxiety disorders
Clinical Symptoms
Positive Symptoms
• Excesses or distortions
• Delusions
• Hallucinations
Negative Symptoms
• Behavioural deficits
Positive Symptoms
• Excesses or distortions– Disorganized speech
• problems in organizing ideas and in speaking so that a listener can understand
• loose associations• derailment
• Delusions
• Hallucinations
Negative Symptoms
• Behavioural deficits– Avolition
• lack of energy– Alogia
• poverty of speech, amount of speech, poverty of content of speech etc.
– Anhedonia• lack of interest in recreational activities, relationships with
others and sex– Flat affect– Asociality
• few friends, poor social skills, and little interest in being with others
Other Symptoms
• Catatonia – catatonic immobility– waxy flexibility
• Inappropriate affect
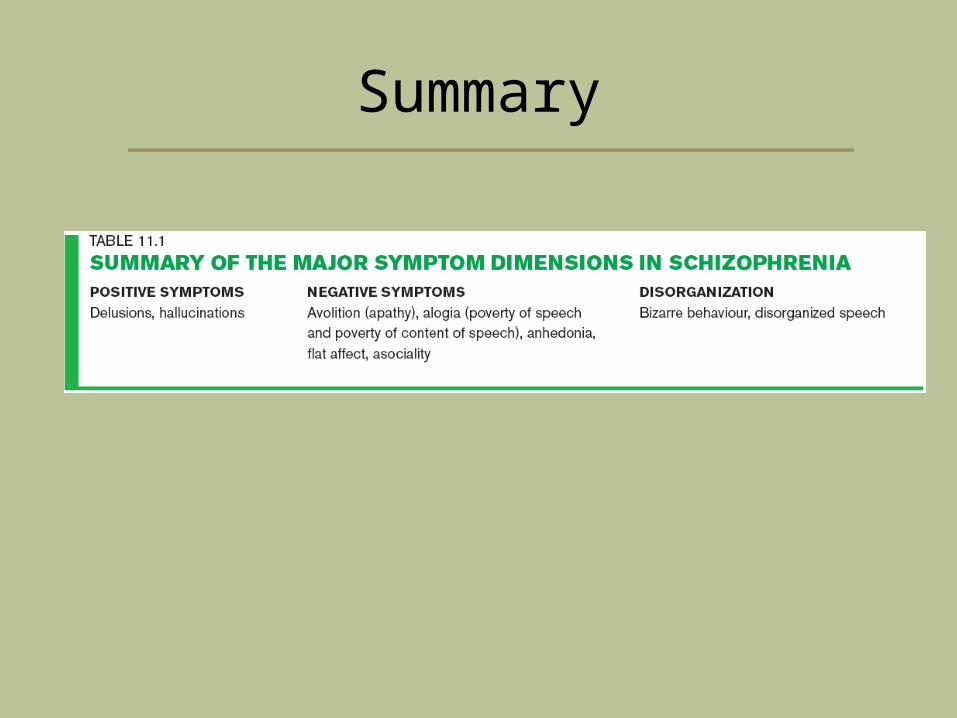
Summary
Early Descriptions of Schizophrenia
• Concept formulated by Emil Kraepelin and Eugen Bleuler
• Kraepelin first presented his notion of dementia praecox– differentiated two groups of endogenous psychoses
• manic-depressive illness • dementia praecox
– dementia paranoides, catatonia, and hebephrenia
• Bleuler broke with Kraepelin on 2 major points:– did not believe in early onset– did not believe in inevitably progress toward dementia
• proposed own term— schizophrenia
Categories of Schizophrenia
• Disorganized schizophrenia • Catatonic schizophrenia • Paranoid schizophrenia
– grandiose delusions– delusional jealousy– ideas of reference
• Undifferentiated schizophrenia– person does not meet the criteria for any of the above types
• Residual schizophrenia – no longer meets full criteria for schizophrenia but still shows
some signs of illness
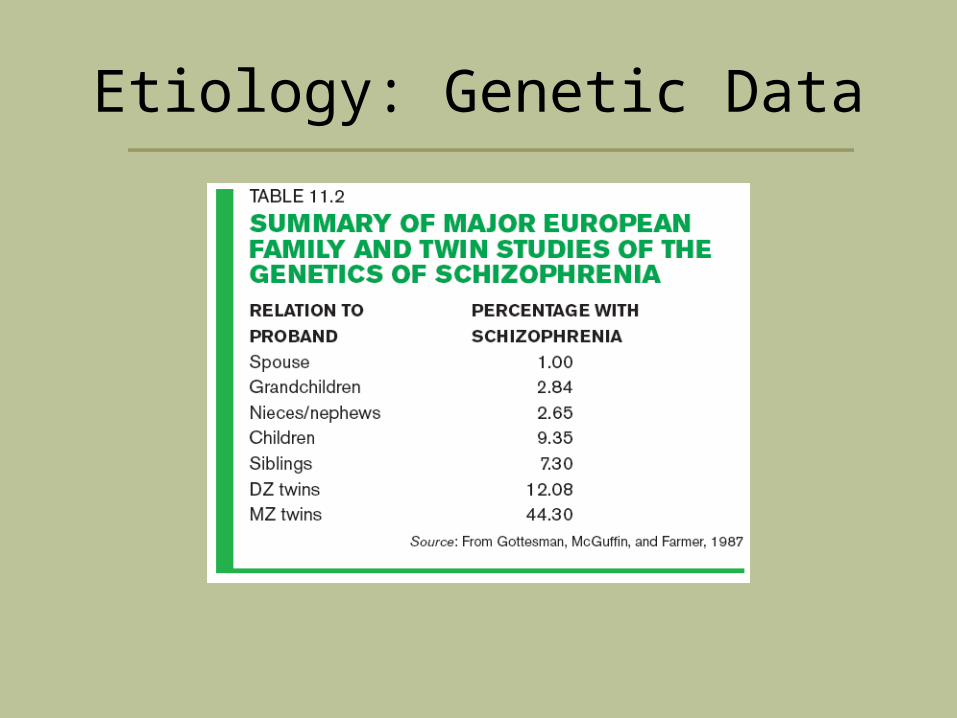
Etiology: Genetic Data
Etiology: Molecular Genetics
• Not likely transmitted by a single gene• Now using “endophenotypic strategy”
– Endophenotypes – characteristics that reflect actions of genes predisposing individual to a disorder, even in the absence of diagnosable pathology (Turetsky et al., 2007,p. 69)
• assumed to be determined by fewer genes than the more complex schizophrenia phenotype
– Some examples: • serotonin type 2A receptor (5—HT2a) gene• dopamine D3 receptor gene• chromosomal regions on chromosomes 6, 8, 13, and 22,• microdeletion on chromosome 22ql1
The Genain Quadruplets
Dopamine Theory
• Schizophrenia thought to be related to > activity of dopamine – drugs effective in treating schizophrenia dopamine
activity– also produce side effects similar to Parkinson’s
disease which is caused in part by dopamine
– other clues provided by amphetamine psychosis• closely resembles paranoid schizophrenia and can
exacerbate symptoms of schizophrenia • amphetamines cause release of norepinephrine
and dopamine– dopamine thought to be the culprit of the symptoms
Brain Structure and Function
• Enlarged Ventricles– enlarged ventricles which implies a loss of subcortical brain cells
• Structural problems – in subcortical temporal-limbic areas, such as hippocampus and
basal ganglia, and prefrontal and temporal cortex
• Prefrontal cortex– known to play a role in behaviours such as speech, decision-
making, and willed action all of which are disrupted in schizophrenia
• Note. MRI studies have shown reductions in grey matter in the prefrontal cortex
Other Etiologies
• Psychological Stress in life stress the likelihood of a relapse
• Social class and schizophrenia t rates of schizophrenia found in central city areas
inhabited by people in the → socio-economic class• sociogenic hypothesis• social-selection theory
• Family and Schizophrenia – Schizophrenogenic mother
Biological Treatments
• Shock and Psychosurgery– prefrontal lobotomy
• Drug Therapies– Antipsychotic drugs (aka neuroleptics)
• First Generation (Conventional) Antipsychotic Drugs
– primarily target D2 receptors
• Second Generation (Atypical) Antipsychotics– primarily target D3 and D4 receptors
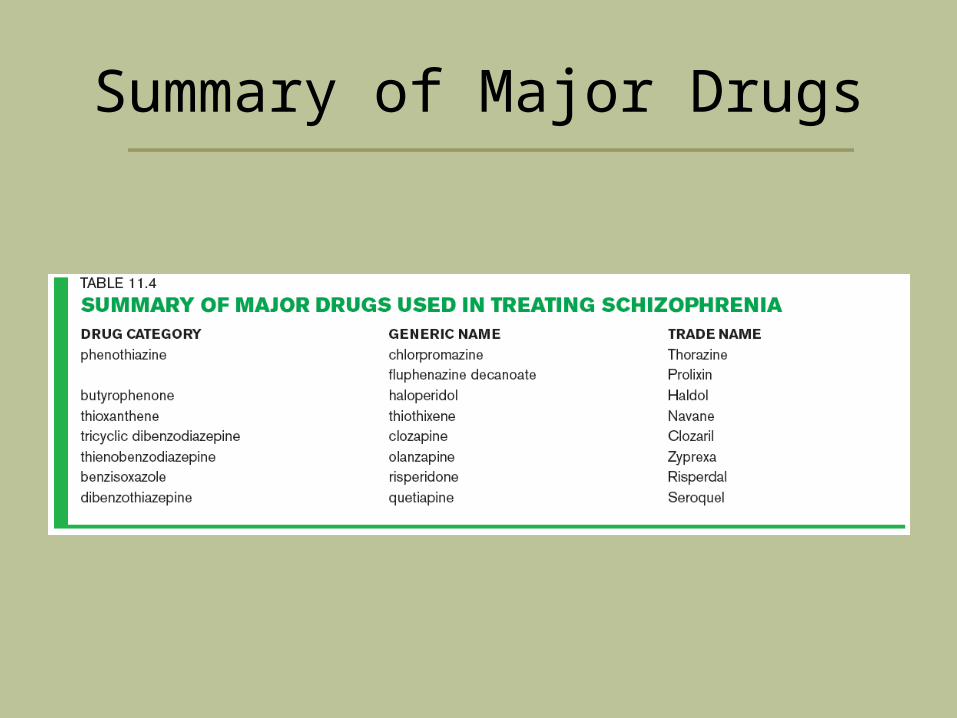
Summary of Major Drugs
Psychological Treatments
• Social Skills Training
• Family Therapy and Reducing Expressed Emotions
• Cognitive-Behavioural Therapy
• Personal Therapy
• Treatment Focus on Basic Cognitive Functions– cognitive enhancement therapy
Other Issues
• Homelessness
• Employment and Housing
• Substance Abuse– Note. Lifetime prevalence rate for substance
abuse among people with schizophrenia is 50%
• Stigmatization
Copyright
Copyright © 2008 John Wiley & Sons Canada, Ltd. All rights reserved. Reproduction or translation of this work beyond that permitted by Access Copyright (The Canadian Copyright Licensing Agency) is unlawful. Requests for further information should be addressed to the Permissions Department, John Wiley & Sons Canada, Ltd. The purchaser may make back-up copies for his or her own use only and not for distribution or resale. The author and the publisher assume no responsibility for errors, omissions, or damages caused by the use of these programs or from the use of the information contained herein.