abnormal psychology psychological disorders treatment and therapy chapters 15 and 16
TRANSCRIPT

ABNORMAL PSYCHOLOGYPSYCHOLOGICAL DISORDERS
TREATMENT AND THERAPYChapters 15 and 16

Abnormal Behavior• The Medical (biological) Model• Other models:
-Behavioral -Psychoanalytic -Cognitive
-Humanistic-existential -Bio-psycho-social
• Criteria of Abnormality– Deviance from social norms– Maladaptive behavior– Personal distress
** Myers: atypical disturbing
maladaptive unjustifiable
In the beginning…• Medical Model –it is useful to think of abnormal behavior as a
disease: i.e. how we refer to mental illness, disorders, and psychopathology. Before this abnormal behavior was based on superstition i.e. possession by devil.
• Diagnosis – involves distinguishing one illness from another• Etiology – refers to the apparent causation and
developmental history of an illness• Prognosis – a forecast about the probable course of an illness
• Thomas Szasz asserts that “strictly speaking, disease or illness can affect only the body; hence there can be no mental illness…” – since abnormal behavior is actually a deviation from SOCIAL norms they are problems in living not actual illnesses.

Psychological Disorders

Rates of Psychological Disorders

Stereotypes and Myths
• Psychological disorders are incurable – yes, some never make it back into society but the majority of people do get better
• Mentally ill people are violent and dangerous – only a modest association has been found between illness and violence. Media?
• Mentally ill people behave in bizarre ways and very differently from normal people – only a small minority of cases

• The Diagnostic System– DSM IV
• (I) CLINICAL SYNDROMES• (II) PERSONALITY DISORDERS• (III) GENERAL MEDICAL CONDITIONS• (IV) PSYCHOSOCIAL STRESSORS• (V) GLOBAL ASSESSMENT OF
FUNCTIONING
DisordersAnxiety Disorder: 2nd most common disorder (Substance abuse is 1st) Afflicts about 1 in 6 Americans…more than 32 million people (U.S.)
Common Characteristics include: FEAR, feeling tense, easily startled, constant worriers. Behavior is self defeating.

Anxiety Disorders
• Types– Panic Disorder– Generalized Anxiety Disorder– Post Traumatic Stress Disorder (PTSD)– Separation Anxiety Disorder– Phobias– Obsessive-Compulsive Disorder
http://www.learner.org/vod/vod_window.html?pid=778

PHOBIAS: Disabled and overwhelmed by fear of specific object or event.
Most common is agoraphobia followed by animals.
Treatments: cognitive, behavioral, biological
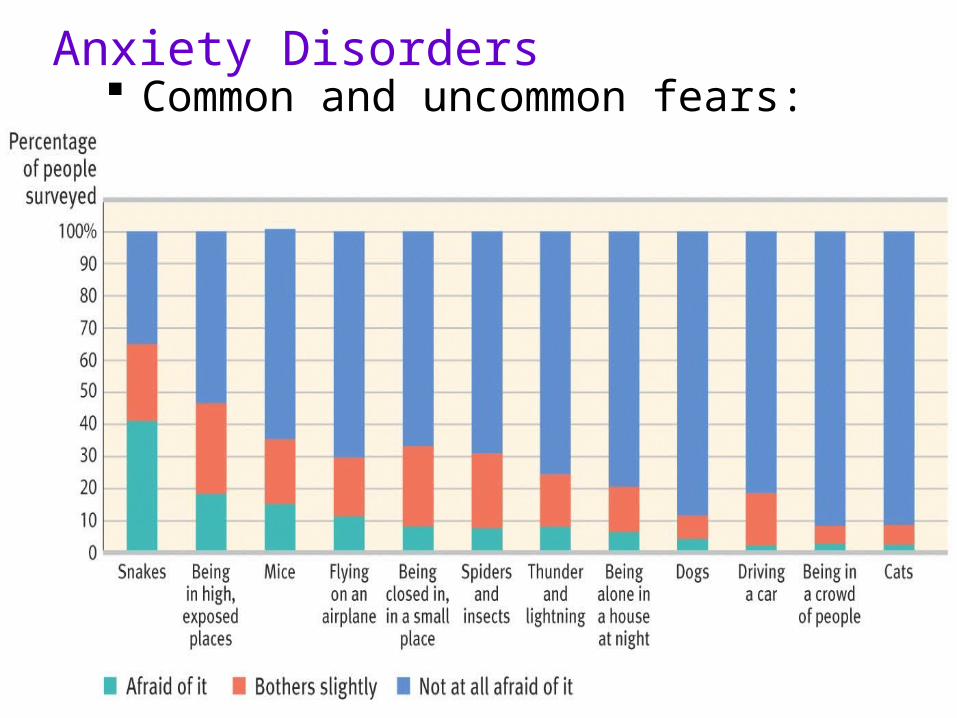
Anxiety Disorders Common and uncommon fears: Phobias
Panic Disorder
Frequent and overwhelming attacks of anxiety; Breathing, Heart rate, Doom

Obsessive-Compulsive
Anxiety is reflected in persistent, unwanted and unshakable thoughts or repeated actions. The action does make it go away for a little while, but when it returns you find yourself repeating the same routine over.

OCD
• Common in every life…becomes neurotic when it interferes with adjustment
• Compulsion—symbolic, ritualized behavior
• Obsession—endless preoccupation with some type of urge or thought
• Results from: faulty attempts to resolve guilt, anxiety or insecurity

Anxiety DisordersCommon Obsessions and Compulsions AmongPeople With Obsessive-Compulsive Disorder
Thought or Behavior Percentage*Reporting Symptom
Obsessions (repetitive thoughts)
Concern with dirt, germs, or toxins 40
Something terrible happening (fire, death, illness) 40
Symmetry order, or exactness 24
Excessive hand washing, bathing, tooth brushing, 85or grooming
Compulsions (repetitive behaviors)
Repeating rituals (in/out of a door, 51up/down from a chair)Checking doors, locks, appliances, 46car brake, homework
Why?
•Serve as a diversion from real fears
•Provide person with evidence that she is doing something well, even if it is avoiding cracks on a sidewalk.
•Biological: Anxiety declines in older age and medication has been shown to help.1990 a woman was reported washing her hands 500x a day

Anxiety Disorders: OCD

Anxiety Disorders
• PET Scan of brain of person with Obsessive/ Compulsive disorder
• High metabolic activity (red) in frontal lobe areas involved with directing attention

Posttraumatic Stress Disorder: People who experience an event outside the normal range of human experience often exhibit a range of severely distr-essing symptoms.

PTSD
• Flashbacks, nightmares, guilt, anxiety
• Tied to specific event (War, Natural disaster, accident, rape, etc.)
• Biological…overactive amygdala
• Psychodynamic…incomplete repression
• Medicines, therapy, beta blockers

Etiology
• Twins: genetic predisposition
• Neural circuits using GABA
• Acquired thru classical & maintained thru operant conditioning
• Cognitive theorists: over-interpret harmless situations as threatening
• High neuroticism & exposure to great stress
Biomedical Therapies
• Psychopharmacology– study of the effects of drugs on mind and
behavior– Anti-anxiety drugs: Zoloft, Buspar, Ativan,
Xanax, Valium, Paxil
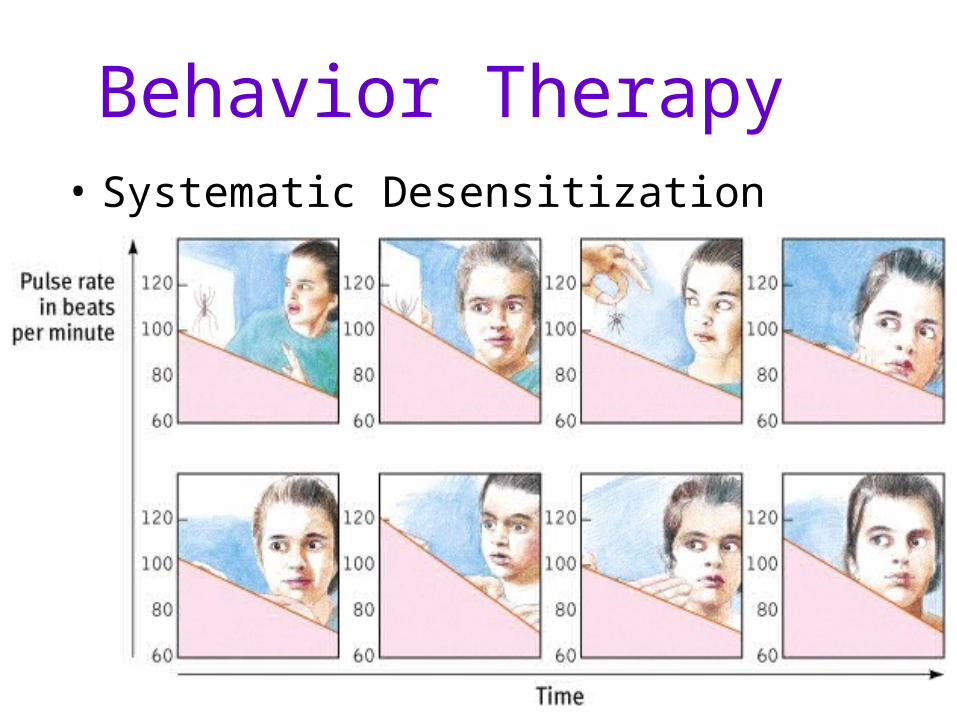
Behavior Therapy• Systematic Desensitization
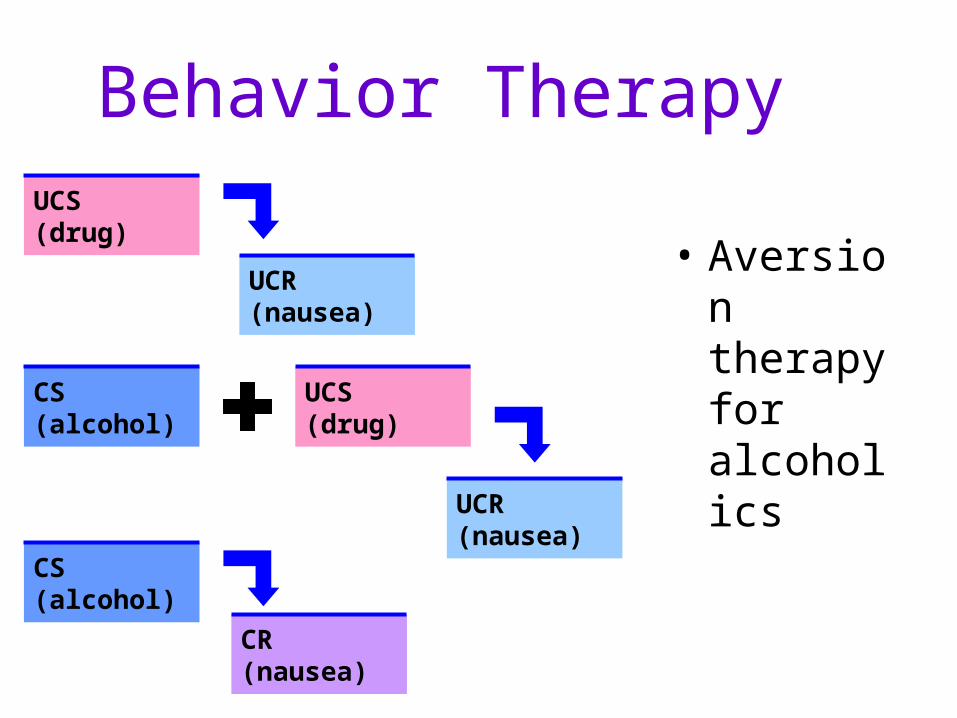
Behavior Therapy
• Aversion therapy for alcoholics
UCS(drug)
UCR(nausea)
UCS(drug)
UCR(nausea)
CS(alcohol)
CS(alcohol)
CR(nausea)

Cognitive Therapy
• The Cognitive Revolution
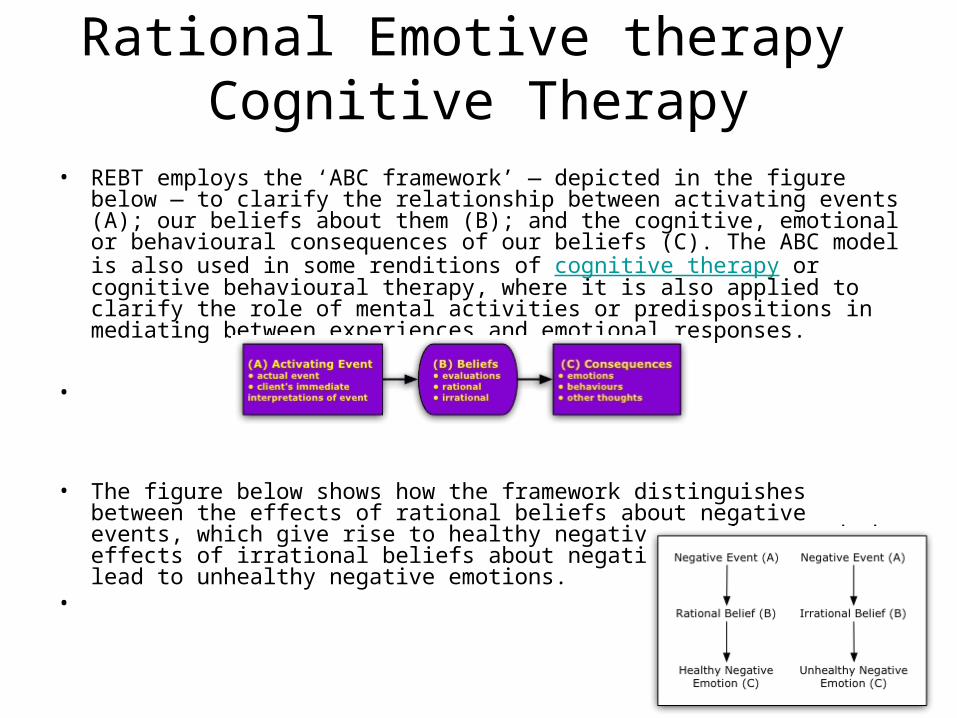
Rational Emotive therapy Cognitive Therapy
• REBT employs the ‘ABC framework’ — depicted in the figure below — to clarify the relationship between activating events (A); our beliefs about them (B); and the cognitive, emotional or behavioural consequences of our beliefs (C). The ABC model is also used in some renditions of cognitive therapy or cognitive behavioural therapy, where it is also applied to clarify the role of mental activities or predispositions in mediating between experiences and emotional responses.
•
• The figure below shows how the framework distinguishes between the effects of rational beliefs about negative events, which give rise to healthy negative emotions, and the effects of irrational beliefs about negative events, which lead to unhealthy negative emotions.
•

Rational Emotive Therapy (cont)The main purpose of REBT is to help clients to replace absolutist philosophies, full of ‘musts’ and ‘shoulds’, with more flexible ones; part of this includes learning to accept that all human beings (including themselves) are fallible and learning to increase their tolerance for frustration while aiming to achieve their goals.
Three primary insights:– While external events are of undoubted influence, psychological
disturbance is largely a matter of personal choice in the sense that individuals consciously or unconsciously select both rational beliefs and irrational beliefs at (B) when negative events occur at (A)
– Past history and present life conditions strongly affect the person, but they do not, in and of themselves, disturb the person; rather, it is the individual’s responses which disturb them, and it is again a matter of individual choice whether to maintain the philosophies at (B) which cause disturbance.
– Modifying the philosophies at (B) requires persistence and hard work, but it can be done.

Beck’s Cognitive therapy--
• Aaron Beck developed a treatment for anxiety and depression based on cognitive theory. Patients tune into their internal dialogue in order to change maladaptive thinking patterns. Beck developed specific procedures to help challenge a client's assumptions and beliefs. Patients learn how to change their thinking.

Psychoanalytic Treatment
• Free association• Dream analysis• Hypnosis• Insight therapy– therapist suggests insights to
patient’s problems; goal is to gain insight to underlying issues of problems
• Interpretation of resistance (blocking anxiety laden material from consciousness)/transference (transfer to the analyst the emotions linked to other important relationships)
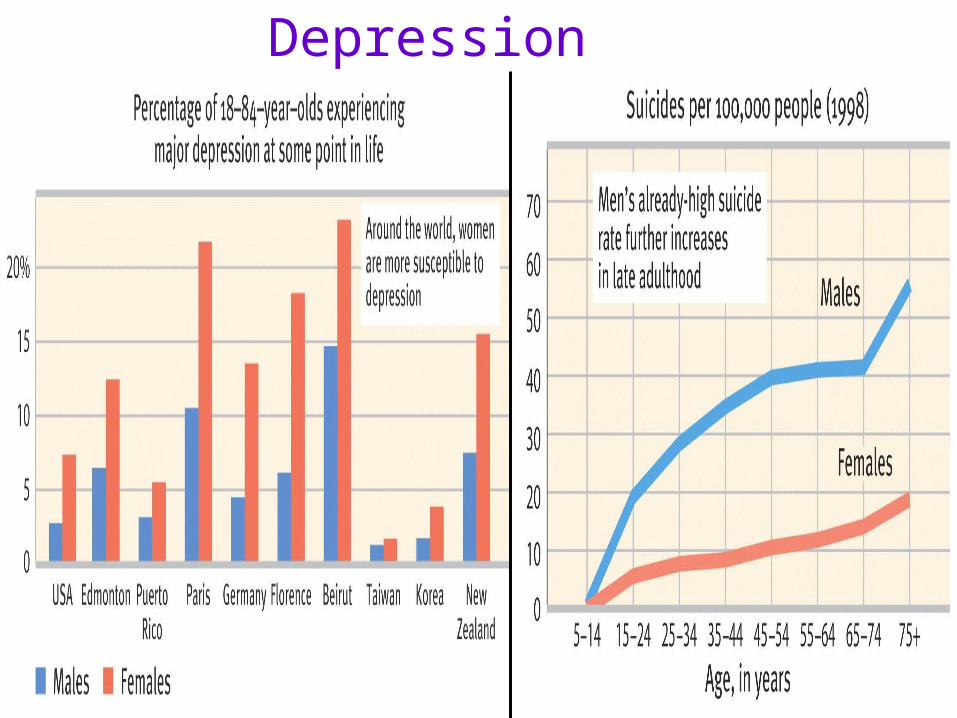
Mood Disorders (Affective Disorders)
Depression is the primary symptom.
Major mood disordersMajor mood disorders: major depression, dysthymic disorder, bipolar disorder, seasonal affective disorder.
Differentiated from normal moods by duration, intensity, lack of cause.
More common in women
Greatest risk: 15-24 and 35-44
Episodes reoccur in half of cases

Mood Disorders
• Major Depression
– Sadness, hopelessness, guilt; emotionally disconnected
• Dysthymic Disorder
– Chronic, but low grade
• Seasonal Affective Disorder (SAD)
– Symptoms appear in fall and winter; phototherapy
• Bipolar Disorder (Manic-Depressive Disorder)
– Major depression and Mania
– Behavioral and cognitive symptoms
– Onset in early 20’s
– Drug therapy…lithium
http://www.learner.org/vod/vod_window.html?pid=786

Etiology
• Twin studies: suggest genetic predisposition• Neural circuits using Serotonin &
Norepinephrine• Cognitive theorists: pessimistic view• Behavioral theorists: inadequate social skills• High stress
The word depression causes confusion.
Bad moods are part of life, clinical depression can kill you.
It affects 1/20 Americans a year.
Signs: don’t feel hopeful or happy about anything, slow motion, nothing tastes good, getting up requires great effort
Mood Disorders-Depression
Mood Disorders-DepressionSocial-cognitive explanation
• Self-defeating beliefs
• Learned helplessness
• Negative thoughts feed negative moods
• Negative moods feed negative thoughts

Mood Disorders-DepressionSocial-cognitive explanation
The vicious Cycle of Depression can be broken at any point!
(negative)
(pessimism)
(hopeless)
(thoughts or actions)

Mood Disorders-Depression
Altering any one component of the chemistry-cognition or mood circuit can alter the others
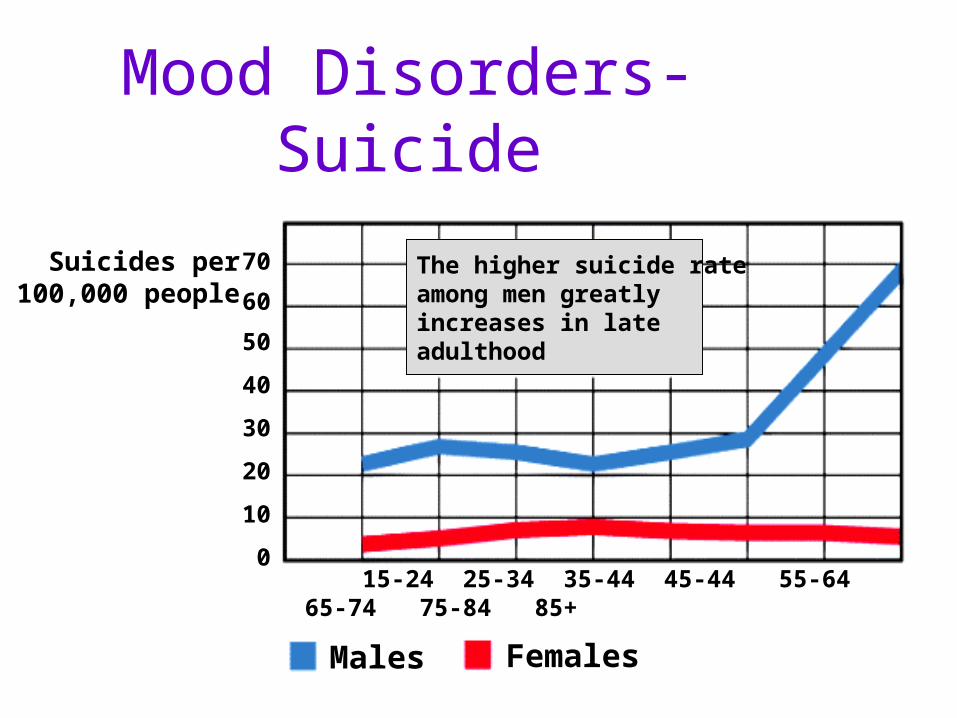
Mood Disorders- Suicide
15-24 25-34 35-44 45-44 55-64 65-74 75-84 85+
Suicides per100,000 people
70
60
50
40
30
20
10
0
Males Females
The higher suicide rateamong men greatly increases in late adulthood

Seasonal Affective Disorder
Winter depression-weight gain, over sleeping, overeating, and craving carbohydrates (deficient exposure to light)
Summer depression-loss of appetite, weight loss, insomnia (heat is the triggering factor)

Bipolar Disorder
Characterized by extreme mood swings, depression to euphoria
Not triggered by identifiable events
a.k.a. manic depression
Mania-inflated self-esteem orGrandiosity. Cannot have mania alone.
“what goes up must come down”
Mania goes through three stages: hypomania, mania, severe mania

Mood Disorders-Bipolar PET scans show that brain energy consumption rises
and falls with emotional switches
Depressed state Manic state Depressed state
May 17 May 18 May 27

Biomedical Therapies
Biomedical Therapies
• Electroconvulsive Therapy (ECT)– therapy for severely depressed patients in which
a brief electric current is sent through the brain of an anesthetized patient
• Psychosurgery– surgery that removes or destroys brain tissue in
an effort to change behavior– lobotomy
• now-rare psychosurgical procedure once used to calm uncontrollably emotional or violent patients

Cognitive Therapy
• A cognitive perspective on psychological disorders
Lost job
Depression
Internal beliefs:I’m worthless. It’s hopeless.
Lost job
Internal beliefs:My boss is a jerk.I deserve something better.
Nodepression

Cognitive Therapy
• Cognitive therapy for depression
Waiting listpatients
Cognitivetraining patients
Cognitive trainingpatients muchless depressed
Pre-therapytest
Post-therapytest
30
25
20
15
10
5
0
Depressionscores

Cognitive behavior therapy
• Combines treating thinking patterns with changing patient’s behavior
• It seeks to make people aware of their negative thinking and to replace it with new ways of thinking, and the practice a more positive approach in everyday settings.

Somatoform Disorders
• SYMPTOMS: bodily symptoms without physical problem
• Conversion Disorder – Hysterical blindness– Hysterical paralysis
• Hypochondria—overly concerned with health/exaggerate minor physical complaints

Conversion Disorder
Emotional difficulties into loss of physiological function.
Unconsciously invent physical symptoms to gain freedom of unbearable conflict.
Common sites for sensory conversions

Etiology
• Histrionic personality traits
• Cognitive theorists: – excessive attention on body sensations– unrealistic standard of good health
• Sick role

Dissociative DisorderA disturbance in conscious awareness, such as identity or memory
Psychogenic Amnesia: sudden loss of memory, may be an attempt to escape from a problem, retain general knowledge
Psychogenic Fugue: combines amnesia with flight- wake up 200 miles away from home have a new identity, marriage, and job, lasts from days to years.

Dissociative Disorder• EXTREMELY RARE• SYMPTOMS: memory loss; disconnection from personal identity;
disconnect events from one another• Psychogenic Amnesia
– Selective forgetting; Usually psychological benefit for forgetting• Psychogenic Fugue
– Complicated type of amnesia– More common in men– Disappear and start new life
• MPD/DID (Multiples…Dissociative Identity Disorder)– Extremely rare– Haunted, confused personality– Childhood abuse– Long-term habit of escaping

Personality Disorders
• Personality Disorders– disorders characterized by inflexible and
enduring behavior patterns that impair social functioning
– usually without anxiety, depression, or delusions
http://www.learner.org/vod/vod_window.html?pid=780

Personality Disorders
• SYMPTOMS: peculiar and unpleasant personality patterns (Off-center)
• Clusters• Antisocial Personality (Psychopaths)
– Conflict with law, Manipulative, impulsive, superficial emotion, no conscience
• Borderline– Intense and unstable relationships, dependent, clingy,
self-destructive; very difficult to treat• Miscellaneous
– Narcissistic, Paranoid, Schizoid, Histrionic

Personality Disorders PET scans illustrate reduced activation in a
murderer’s frontal cortexNormal Murderer

Personality Disorders

And Finally Schizophrenia• Defined as a class of disorders marked by
delusions, hallucinations, disorganized speech, and deterioration of adaptive behavior
• It primarily involves disturbances in perception and thought, with corresponding loss of the ability to function.
• Cognitive processes are severely disrupted.
• Positive symptoms: Hallucinations, disorganized and delusional talk, inappropriate laughter, tears, or rage.
• Negative symptoms: toneless voices, expressionless faces, mute
http://www.learner.org/vod/vod_window.html?pid=788
Schizophrenia
NO two sufferers of schizophrenia suffer the same symptoms. It is the disorder we characterize with “crazy”, “psychotic”, or “insane.”
There are as many people with schizophrenia as there are people in Hawaii! (1 in 100)
Rule of thirds
Statistically, one third of all diagnosed will recover completely, one third will improve over time and one third will not improve.

Etiology of Schizophrenia• Genetic 48% identical 17% fraternal twins• Born to parents with Schizophrenia 46%• Emerge during adolescence or early (15-
24)adulthood and sometimes at 45 it’s either sudden or gradual
• Excess dopamine but new research is not conclusive
• Inability to filter out unimportant stimuli, large brain ventricles, new research with the thalamus is smaller with less metabolic activity
• Neurodevelopment hypothesis – phases of pregnancy during the flu season
• Precipitating stress and unhealthy family dynamics

What’s the cause?
•Levels of dopamine
•4x more likely if someone in family has it
•Prenatal or birth trauma
•Viral infections or lack of nutrition as infants
•2x more likely when born in urban areas
More Specifically



Schizophrenia

Etiology
• Twin & adoption studies
• Dopamine
• Neuro-developmental hypothesis
• Relapse (residual) rates
• Stress

Does Therapy Work?• Meta-analysis
– procedure for statistically combining the results of many different research studies
Poor outcome Good outcome
Averageuntreated
person
Averagepsychotherapy
client
Number ofpersons
80% of untreated people have pooreroutcomes than average treated person

Mental Illness v. Insanity
• Mental illness is a medical decision.
• Insanity is a legal one. To be considered insane a person must be unable to control his/her behavior and be unaware that his behavior is wrong.

Pathology & the Law• Insanity
• Insanity defense
• Involuntary commitment
Culture & Pathology• Relativistic view
• Pan-cultural view

DSM-IV
• Impulse control disorders: impulsive behaviors harm the self or others. Ex. Intermittent explosive disorder, kleptomania, pathological gambling.
• Disorders 1st diagnosed in infancy, childhood, adolescence: appear before adulthood Ex. Mental retardation, learning disorders, and language development

DSM-IV
• Adjustment disorders: extreme emotional reaction to a stressor that occurred w/in the previous month (much greater than most people would experience).
• Personality disorders: long-term disorders with rigid, maladaptive personality traits. Ex. Antisocial personality D, histrionic personality D, narcissistic PD
• Delirium, dementia, amnestic and other cognitive Disorders: diverse group of memory and cognition that is caused by identifiable brain damage. Ex. Alzheimer’s, intellectual impairment (stroke), delirium (change in consciousness) due to overdose

Major Psychological Disorders of Axis 1

Major Psychological Disorders of Axis 1 (continued)

Different dimensions or axes
Each axis reflects a different aspect of a patient’s case: Axis I- used to classify current symptoms Axis II- used to describe developmental and long-
standing personality disorders or maladaptive traits; specific developmental disorders for children such as mental retardation, autism, etc.
Axis III- used to describe physical disorders or general medical conditions that are relevant to treatment
Axis IV- current stress level (based on the past year) Axis V- adaptive functioning: 3 major areas– social
relations, occupational functioning, & use of leisure time