abnormal clotting and bleeding - rcp london
TRANSCRIPT

Abnormal Clotting and Bleeding
Simon Lyons
Haematology Consultant
Northumbria

Aim
• To understand the process of taking a bleeding history, requesting appropriate blood tests and interpreting the results
• Reversal of oral anticoagulants– DOAC and VKA
– Understanding the rational to ‘re-anticoagulate’
• Some of the material used today is based on the BMJ learning website for bruising and bleeding module

Case based discussion- Case1
• 29 Young man presents with petechiae
• He is clinically stable
• NEWS NORMAL /Early warning score low
• Has a history of a ‘petechial rash’
• Nose bleed
• Diagnosed with TB on appropriate antimicrobials

Case 1
• What do you think is causing the petechiae?
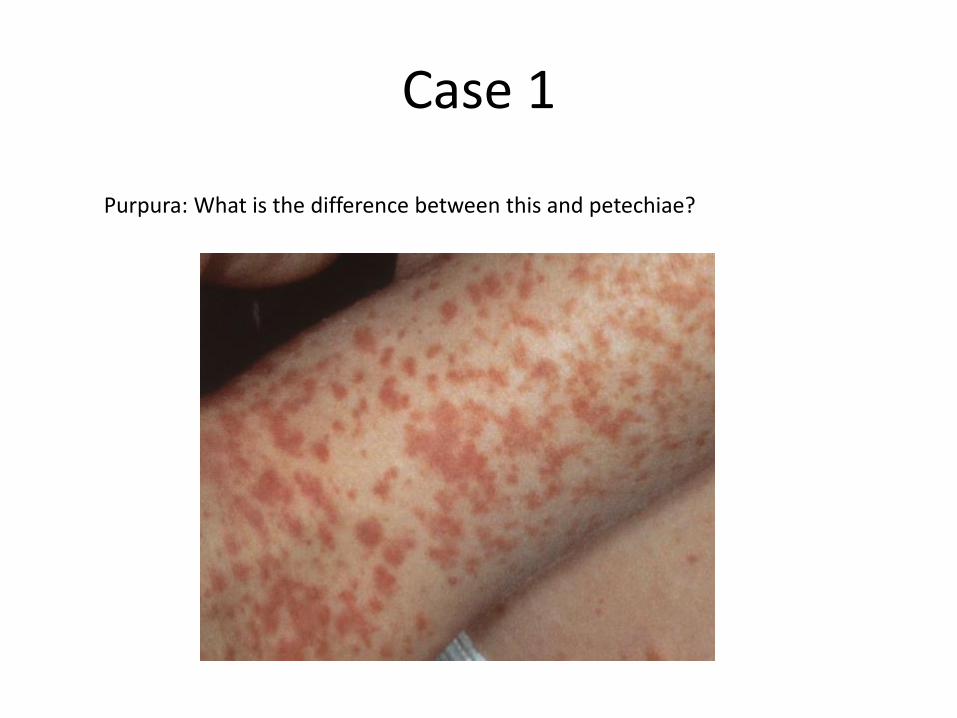
Case 1
Purpura: What is the difference between this and petechiae?

Ecchymoses (Bruises!)

How does the presentation of the ‘bruising’
affect how we think about the diagnosis?
• Petechiae and purpura - both commonly associated with significant thrombocytopenia, ie below 50 x 109/L, or defects of platelet function.
• Ecchymoses are larger (over 1 cm), flat, subcutaneous haemorrhagic lesions, which patients will often refer to as “bruises.” Bruising itself is not necessarily pathological. – However, with a careful clinical history and examination, it should be possible
to differentiate the normal from the abnormal, and therefore direct further investigation appropriately.
• Ecchymoses are common after trauma and injury, but are considered abnormal if their size is out of proportion to the degree of injury. – The location of “spontaneous” bruising is also important to note: ecchymoses
on the lower limbs, a frequent site of innocuous injury, raise less suspicion than those found elsewhere.
• Pathological ecchymoses can be associated with any defect in the haemostatic system, but are also associated with various vascular and collagen disorders.

Haematoma

Haematoma
• A haematoma is a localised collection of blood that has leaked from a damaged blood vessel.
• They can form in organs, spaces, or tissues, and in contrast to ecchymoses, will have three dimensional structure and may be associated with pain, tenderness, or compressive symptoms.
• Defects of secondary haemostasis, such as the inherited or acquired haemophilia's, are associated with the formation of spontaneous or trauma induced haematomas, commonly within muscles.

Trying to figure this all out requires a good ‘bleeding history’
• Bleeding symptoms are commonly reported.
• In a study of 500 healthy patients who were asked about bleeding problems, 25% of subjects reported epistaxis, 18% easy bruising, 18% prolonged bleeding after a tooth extraction, and 4% gum bleeding.
• 47% of women reported heavy menstrual bleeding.[A]There is also a variation in perception among individuals regarding the significance of bleeding symptoms.
[A] Mauer AC, Khazanov NA, Levenkova N, et al. Impact of sex, age, race, ethnicity and aspirin use on bleeding symptoms in healthy adults.J Thromb Haemost 2011;9(1):100-8

Bleeding History
• A focused clinical history will guide any further investigation by establishing:
– Whether a patient has significant bleeding symptoms
– At what point in the haemostatic process the defect may be located
– Whether this defect is likely to be acquired or inherited.
What is in a good Bleeding History
• History of bleeding symptoms– Mucosal haemorrhages (epistaxis, gum bleeding, haemorrhagic oral
blisters)– Petechiae, suggestive of platelet defects– Swollen joints or soft tissues that could be explained by bleeding;
palpable bruises, suggestive of defects in coagulation factor, especially factor VIII or IX
• Onset• Duration• Intervention required to stop bleeding• Bruising/ecchymoses
– Distribution– Size– Initiating cause
History of Haemostatic Challenges
• Surgical or invasive procedures– Abnormal bleeding during or after these episodes– An absence of significant bleeding following surgical procedures effectively
excludes an inherited bleeding disorder, although many patients will have not experienced sufficient surgical challenges for this to be assessed
– Dental extractions– Prolonged or delayed bleeding– Menorrhagia
• Heavy periods from menarche may be a symptom of inherited bleeding disorders. For example, the overall prevalence of von Willebrand disease among women with chronic heavy menstrual bleeding ranges from 5% to 24%.[B] However, menorrhagia is very difficult to assess, and patient reported severity is extremely subjective
• Menorrhagia that develops later in life is more likely to be secondary to an acquired bleeding defect or physical abnormality, such as uterine fibroids
[B] Committee on Adolescent Health Care; Committee on Gynecologic Practice. Committee Opinion No.580: von Willebrand disease in women.
Obstet Gynecol 2013;122(6):1368-73.

Bleeding History Continued
• History of treatment for iron deficiency anaemia, or requirement for blood transfusion
• Family history of bleeding symptoms– Particularly important if a patient has no personal history
of haemostatic challenges
• Diet/symptoms and risk factors for dietary malabsorption– Various nutritional deficiencies can result in haemorrhagic
symptoms. Consider potential deficiencies of:• Vitamin K, involved in coagulation factor synthesis
• Vitamin C and protein, involved in maintaining connective tissue integrity

Comorbidity is always important to consider
• Comorbidities, in particular liver or renal impairment, and alcohol abuse– Renal impairment can result in platelet
dysfunction secondary to uraemia
– Liver impairment predisposes the bleeding via a number of mechanisms, eg thrombocytopenia as a consequence of portal hypertension and splenomegaly, or clotting factor deficiencies because of reduced synthetic function
• Alcohol is directly bone marrow toxic

Other Medications!
• Prescribed and over the counter medications– May exacerbate an existing bleeding disorder
– Anticoagulants (vitamin K antagonists and novel oral anticoagulants, eg dabigatran, apixaban, rivaroxaban, edoxaban)
– Antiplatelets
• May directly cause bleeding symptoms, for instance by inducing thrombocytopenia or aplastic anaemia
• Look them up!

Case 1 continued
• Your excellent bleeding history demonstrates; – Recent gum bleeding– No previous history of mucosal haemorrhage or swollen joints– Several teeth extracted in childhood with no bleeding complications– Has never had any surgical procedures. – There is no family history of easy bruising or bleeding disorders.
• Despite the unremarkable bleeding history, you remain suspicious of the petechial lesions and order some routine investigations. Admission full blood count shows: – Hb 134 (130-180), WCC 5.2, Plt 2
• Renal function is normal, LFT normal barring AlkP of 278u/l
• What investigations do we need next? • What is the likely diagnosis?
Case 1 continued
• Your excellent bleeding history demonstrates; – Recent gum bleeding– No previous history of mucosal haemorrhage or swollen joints– Several teeth extracted in childhood with no bleeding complications– Has never had any surgical procedures. – There is no family history of easy bruising or bleeding disorders.
• Despite the unremarkable bleeding history, you remain suspicious of the petechial lesions and order some routine investigations. Admission full blood count shows: – Hb 134 (130-180), WCC 5.2, Plt 2
• Renal function is normal, LFT normal barring AlkP of 278u/l
• What investigations do we need next? – Blood Film and Coag Screen, why?

The Results
• Always consider a repeat FBC if the result is unexpected
• A blood film in ITP should have no other abnormalities than the low platelet count– There should be no red cell fragments
• Coagulation screen to rule out: – DIC– MAHA, this should be accompanied by anaemia,
raised bili, red cell fragmentation• Think about TTP, HUS, aHUS, HELLP

Coag Testing
• Often inappropriately requested, first question to ask is ‘why am I checking a coagulation profile?’.
• A coagulation screen is often requested inappropriately, particularly to assess bleeding risk before interventional procedure– There is no evidence to suggest that pre interventions PT and APTT in the
absence of a bleeding history of high risk factors predicts risk of bleeding • British Committee for Standards in Haematology (BCSH), a coagulation screen is
only required prior to an invasive procedure if the patient [C]:– Has a positive personal or family bleeding history– Is taking an anticoagulant treatment– Has a clear clinical indication that increases the bleeding risk, for example liver
disease.• Historically, the coagulation cascade has been divided into intrinsic, extrinsic, and a
final common pathway. This division does not truly reflect how blood clots in vivo, however it is a useful framework that can be used to interpret the results of in vitro clotting tests.
• A coagulation screen should consist of PT and APTT as a minimum, but ideally should also measure the fibrinogen level.
[C] Chee YL, Crawford JC, Watson HG, Greaves M. Guidelines on the assessment of bleeding risk prior to surgery or invasive procedures.British Committee for Standards in Haematology. Br J Haematol 2008;140(5):496-504
Coag Testing
• Historically, the coagulation cascade has been divided into intrinsic, extrinsic, and a final common pathway. This division does not truly reflect how blood clots in vivo, however it is a useful framework that can be used to interpret the results of in vitro clotting tests.
• A coagulation screen should consist of PT and APTT as a minimum, but ideally should also measure the fibrinogen level.
[C] Chee YL, Crawford JC, Watson HG, Greaves M. Guidelines on the assessment of bleeding risk prior to surgery or invasive procedures.British Committee for Standards in Haematology. Br J Haematol 2008;140(5):496-504

What are we testing with a coag test?
Intrinsic pathway: assesses factors XII, XI, IX, and VIIIExtrinsic pathway: assesses factor VIICommon pathway: assesses factors X, V, II (prothrombin), and fibrinogen


How to approach abnormal coag results.
• The results should be interpreted in the context of the history, symptoms and signs, also consider– Is the result unexpected?– Could the sample have been taken incorrectly– Is the patient on anticoagulation?
• It seems obvious that a patient's clotting results will be abnormal if they are taking an anticoagulant, but the nature of the abnormality will depend on the type of anticoagulant being used.

Abnormal Test resultsPT APTT Fibrinogen Platelets Condition
N N N Factor VII deficiencyEarly VKA therapyLupus anticoagulants (rarely)(Mild factor II,V, X deficiency)
N N N Factor VIII, IX, XI deficiencyFactor XII or contact factor (HMWK or prekallikrein) deficiencyLupus anticoagulants(Mild factor II,V, X deficiency)
N N Vitamin K deficiencyOral anticoagulants (VKAs and DOACS)Unfractionated heparinExcess LMWH (rarely affects coagulation times in therapeutic range)Factor V, X, II deficiencyCombined factor V & VIII deficiency
N/ Liver diseaseMassive transfusionDIC
N/ N Hypo/dysfibrinogenaemia

Normal coagulation screen
• Suggestive bleeding history with normal basic coagulation screen:
• Mild factor deficiency
• Von Willebrand disease
• Platelet function disorder
• FXIII deficiency
• Alpha-2-antiplasmin deficiency

What about newer anticoagulants?

Coag Results
• Newer (NOAC/DOAC) anticoagulants do not routinely need to be monitored but most centres can offer coagulation assay based levels for patients who are bleeding (more information later!)
• Additional questions to ask- Is there an existing medical condition or systemic disease that may account for the abnormal result?
• Liver disease- Most coagulation factors (fibrinogen, II, V, VII, IX, X, and XI) are synthesised by the liver, so it is not unusual for patients with hepatic impairment to have a clotting profile abnormality, potentially in both PT and APTT.– Vitamin K deficiency will cause a similar picture as there is consequent
deficiency in the vitamin K dependant clotting factors (II, VII, IX, and X).
• DIC should be considered in systemically unwell patients, particularly those with severe sepsis. It is a consumptive coagulopathy that results in deficiency of all clotting factors. The PT and APTT will be deranged and fibrinogen is low. It will be associated with a thrombocytopenia and features of a MAHA.
Coag Results
• If after asking these questions it still isn't clear why a coagulation abnormality exists, further investigations may be required.
• Mixing studies: “50:50 mix”– This test is designed to determine whether a clotting abnormality is secondary
to a coagulation factor deficiency or coagulation factor inhibitor. The patient’s plasma is mixed with an equal volume of “normal” plasma and the PT and APTT tests are repeated, the principle being that if the abnormality is due to a factor deficiency, it should be corrected by adding normal plasma replete with clotting factors. If an inhibitor is present it will not be overcome by adding normal plasma, and the abnormality will not correct.
• If results are suggestive of a factor deficiency, specific factor assays may be required.
• Acquired antibodies to clotting factors are rare, but can cause potentially life threatening bleeding. Most commonly the autoantibodies are directed against FVIII (ie acquired haemophilia A), and will cause bleeding symptoms and an elevated APTT that does not correct on mixing.
Case 1 Continued
• This patient has a PT 15.2 seconds (range 12.5 to 15.3) and APTT 35.1 seconds (range 24.6 to 34.9)
• The thrombocytopenia is confirmed by the peripheral blood film: there are no platelet clumps and no other significant abnormalities. Lymphocytes are 0.81 x 109/L (range 1.5 to 4.0 x 109/L), but otherwise the white cell differential is normal. C-reactive protein is 46 mg/L (range 0.3 mg/L to 5.0 mg/L).
• You review the previous blood tests available for the patient. He had a full blood count two months previously which was normal.
• From your history, examination, and basic investigation, what are the two most likely differential diagnoses?
Case 1 Continued
• This patient has a PT 15.2 seconds (range 12.5 to 15.3) and APTT 35.1 seconds (range 24.6 to 34.9)
• The thrombocytopenia is confirmed by the peripheral blood film: there are no platelet clumps and no other significant abnormalities. Lymphocytes are 0.81 x 109/L (range 1.5 to 4.0 x 109/L), but otherwise the white cell differential is normal. C-reactive protein is 46 mg/L (range 0.3 mg/L to 5.0 mg/L).
• You review the previous blood tests available for the patient. He had a full blood count two months previously which was normal.
• From your history, examination, and basic investigation, what are the two most likely differential diagnoses?– Idiopathic ITP– Drug induced ITP
• Thinking of the TB and low lymphocytes what other test is vital?

Case 1 Continued
• This patient has a PT 15.2 seconds (range 12.5 to 15.3) and APTT 35.1 seconds (range 24.6 to 34.9)
• The thrombocytopenia is confirmed by the peripheral blood film: there are no platelet clumps and no other significant abnormalities. Lymphocytes are 0.81 x 109/L (range 1.5 to 4.0 x 109/L), but otherwise the white cell differential is normal. C-reactive protein is 46 mg/L (range 0.3 mg/L to 5.0 mg/L).
• You review the previous blood tests available for the patient. He had a full blood count two months previously which was normal.
• From your history, examination, and basic investigation, what are the two most likely differential diagnoses?– Idiopathic ITP– Drug induced ITP
• Thinking of the TB and low lymphocytes what other test is vital? – HIV HepC (I always check Hep B also!!)
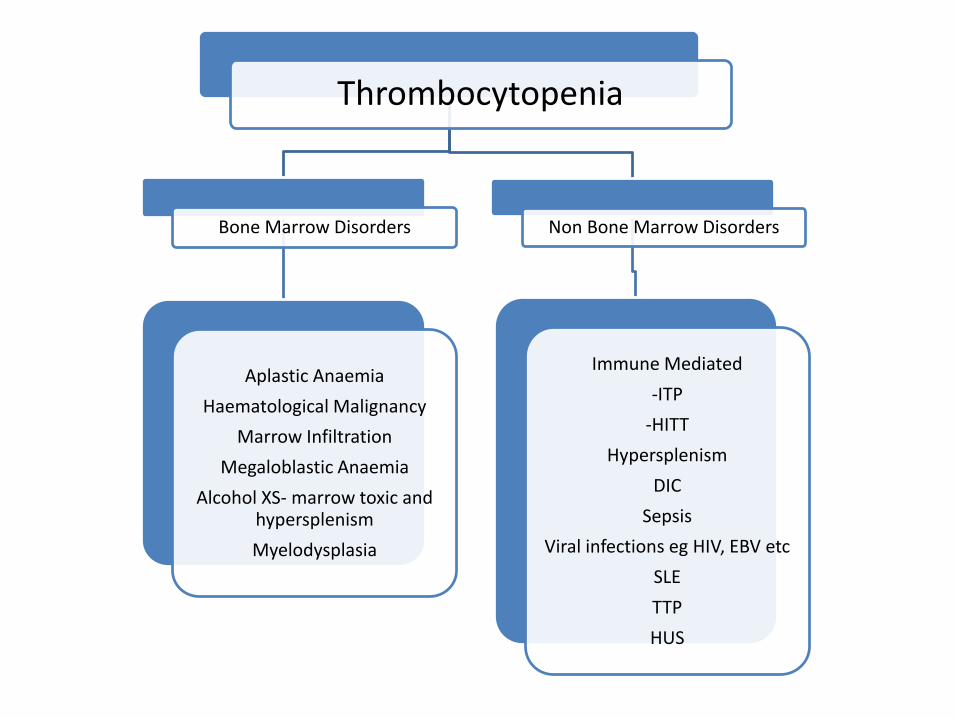
Thrombocytopenia
Bone Marrow Disorders
Aplastic Anaemia
Haematological Malignancy
Marrow Infiltration
Megaloblastic Anaemia
Alcohol XS- marrow toxic and hypersplenism
Myelodysplasia
Non Bone Marrow Disorders
Immune Mediated
-ITP
-HITT
Hypersplenism
DIC
Sepsis
Viral infections eg HIV, EBV etc
SLE
TTP
HUS

Case 2
• Trauma occurs most commonly from a standing height
• 87 year old lady admitted with a fall from standing height
• She is anticoagulated for a PTE in 2012



(Sorry… Just pretending! She’s all
right really!) (she’s a Stunt Granny)

First thoughts on this case?

First thoughts? What on earth is an
87 year-old who had a PE in 2012 still anticoagulated for?!

First thoughts?
Who kept her on anticoagulation?! She walks with a stick and is OBVIOUSLY at risk of falls!

First thoughts?How is reversing her
anticoagulation going to help reduce the risk of her ICH? The horse has bolted!
But I am glad she was not on a DOAC!

First thoughts?
What on earth are we supposed to do with her in the future??

It is worth noting:
0
10
20
30
40
50
60
70
80
90
0 20 40 60 80 100 120
Series1
8% of individuals >80 years of age are anticoagulated

Question 1What on earth is an
87 year-old who had a PE in 2012 still anticoagulated for?!
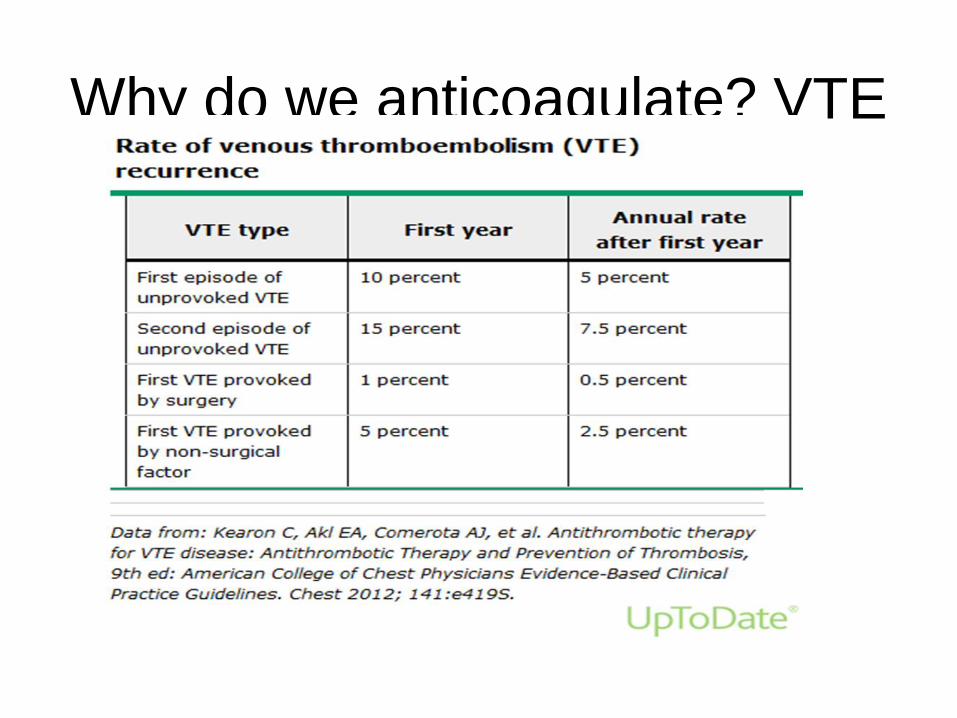
Why do we anticoagulate? VTE
Venous thromboembolic diseases: diagnosis, management and
thrombophilia testing
Clinical guideline [CG144]
• 1.2.4 Offer a VKA beyond 3 months to patients with an
unprovoked PE, taking into account the patient's risk of
VTE recurrence and whether they are at increased risk
of bleeding. Discuss with the patient the benefits and
risks of extending their VKA treatment. [2012]
• 1.2.5 Consider extending the VKA beyond 3 months for
patients with unprovoked proximal DVT if their risk of
VTE recurrence is high and there is no additional risk of
major bleeding. Discuss with the patient the benefits and
risks of extending their VKA treatment. [2012]

Why do we anticoagulate?- AF
• Summary of 4 major studies in AF with warfarin
• 45-82% risk reduction in CVA
• Multiple observational studies and randomized trials report the risk of ICH attributable to anticoagulant therapy with warfarin to be in the range of 0.2 to 0.4 percent per year
• SPAF: Stroke Prevention in Atrial Fibrillation; AFASAK: Copenhagen AFASAK Study; BAATAF: Boston Area Anticoagulation Trial for Atrial Fibrillation; and CAFA: Canadian Atrial Fibrillation Anticoagulation Study
• Connolly SJ, Laupacis AN, Gent M, et al. J Am Coll Cardiol 1991; 18:349.
Question 2
Who kept her on anticoagulation?! She walks with a stick and is OBVIOUSLY at risk of falls!
Not an easy question to definitively answer
• Man-Son-Hing et al. estimated that elderly patients need to
fall 295 times per year for the benefit of stroke reduction to
be outweighed by serious bleeding
• Also- ‘those who are at most risk have most to gain’
– E.g the frequency of CVA increases with age, but older patients are
less likely to be offered anticoagulation despite the clear benefits
• nice.org.uk/guidance/cg180 Atrial fibrillation: management
– 1.4.4 ‘Do not withhold anticoagulation solely because the person is
at risk of having a fall’
Man-Son-Hing, M., Nichol, G., Lau, A., Laupacis, A., 1999. Choosing antithrombotic therapy for elderly patientswith atrial fibrillation who are at risk for falls. Arch. Intern. Med.159 (7), 677–685
Risks for ICH on Anticoagulation• Thrombocytopenia or known coagulation
defect associated with bleeding
• Active bleeding or recent surgery with a concern for ongoing bleeding
• Prior severe bleeding (including ICH) while on an oral anticoagulant
• Suspected aortic dissection
• Malignant hypertension
• Combined use of anticoagulant and antiplatelet agents
Question 3 (part i)How is reversing her
anticoagulation going to help reduce the risk of her ICH? The horse has bolted!

Features of anticoagulant-associated ICH
• Rapid deterioration with first 24-48 hours, increasing ICH
volume
• Poor outcome associated with:
– ICH volume
– Intraventricular extension of bleeding
• Majority of warfarin-related ICH occurs with INR 2-3.5
• Rapid reversal of anticoagulant effect essential:
– To prevent haematoma expansion
– To facilitate appropriate surgical intervention
Sjoblom et al. Stroke (2001), 32, 2567-2574Management and prognostic features of ICH during anticoagulant therapy: A Swedish Multicenter Study

Question 3 (part ii)
But I am glad she was not on a DOAC!
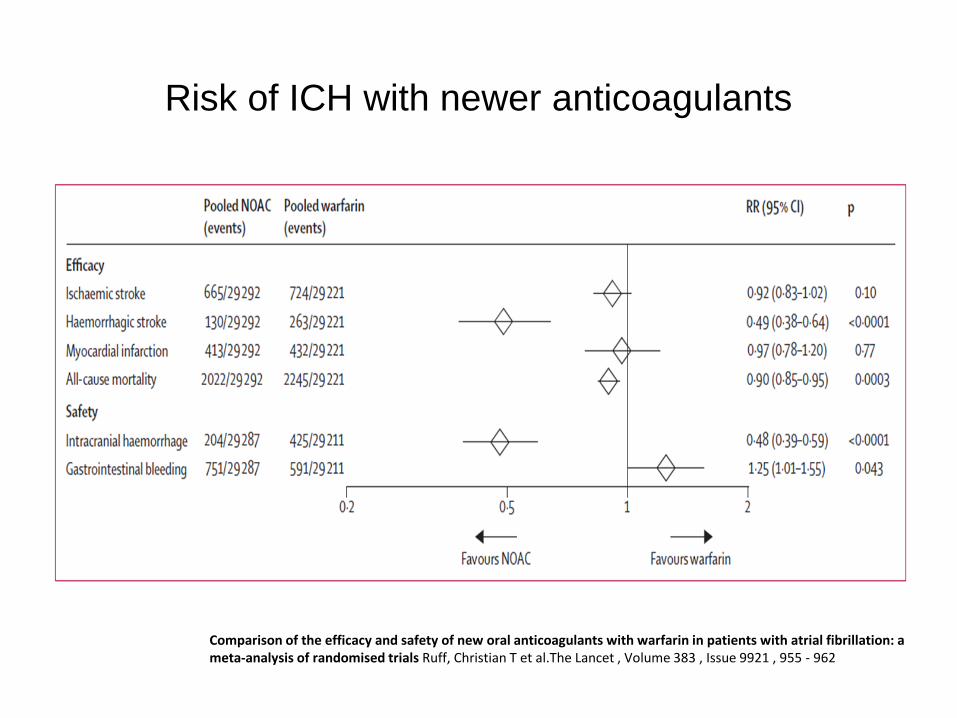
Risk of ICH with newer anticoagulants
Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: ameta-analysis of randomised trials Ruff, Christian T et al.The Lancet , Volume 383 , Issue 9921 , 955 - 962

What can we do?
Warfarin reversal
– Regional guideline
– Vitamin K
– Beriplex (Prothrombin Complex Concentrate)
• Life/limb/sight threatening bleeding
• Always give 5mg IV vitamin K concurrently
• Check INR immediately and at 24 hours

LMWH reversal
• Heparin works by potentiating the action of antithrombin to inhibit Factor Xa and to a lesser extent, thrombin
• Anti-Xa levels can be used to assess drug levels accurately
• Protamine fully reverses UFH, no such guarantee for LMWH (about 60%)
• Protamine – slow IV injection over 10 minutes

DOAC reversal
• Stop the drug
• Document timing last dose, estimate elimination half life
• Check FBC, coag screen, renal and hepatic function
• Assess bleeding source/control haemorrhage– Can you apply pressure?
– Surgery/radiological/endoscopic intervention?
• Are they on any other drugs such as antiplatelets?
• Dialysis unhelpful for Xa inhibitors (95% protein bound)
• Consider antidote (Dabigatran) or PCC (Xa inhibitors)
Antidotes
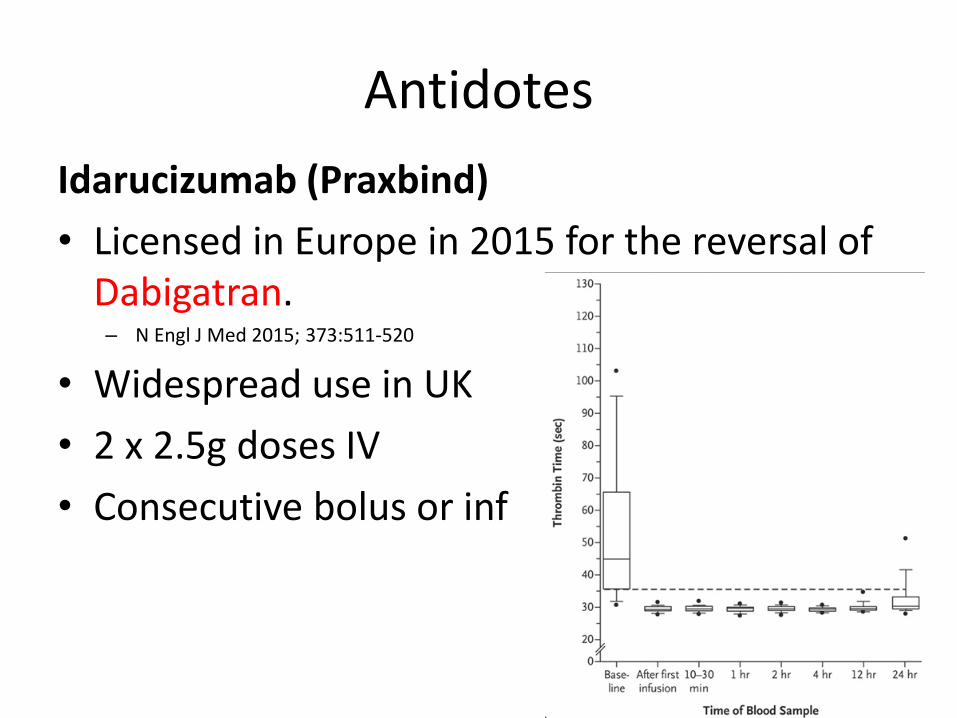
Idarucizumab (Praxbind)
• Licensed in Europe in 2015 for the reversal of Dabigatran.
– N Engl J Med 2015; 373:511-520
• Widespread use in UK
• 2 x 2.5g doses IV
• Consecutive bolus or inf

Antidotes
Andexanet alfa (Andexxa)
• A recombinant modified human factor Xa decoy protein that has been shown to reverse the inhibition of factor Xa (Rivaroxaban and Apixaban) in healthy volunteers.
• N Engl J Med 2016; 375:1131-1141
• FDA approved May 2018
• European approval expected early 2019
Question 4What on earth
are we supposed to do with her in the future??
Is it ever safe to re-anticoagulate?

Question 4• Meta Analysis of all available data suggests
there is not a significant increased risk of recurrent ICH and there is evidence for a reduction in mortality associated with arterial thrombosis risk
• No clear recommendation on re-start
– Individual assessment
– 7-14 days but maybe longer• Murthy et al, Restarting Anticoagulant Therapy After Intracranial Hemorrhage, A Systematic Review and Meta-
Analysis, Stroke. 2017;48:1594-1600
Happy ending, by the way…

Case history 3
• 63 y o man
• 3-4 month history of easy bruising: spontaneous, arms and legs
• Prolonged bleeding from cut to lower lip
• Previous dental extractions/appendicectomy, no problems
• Non-specific pain and swelling of small joints of hands. On 10mg pred
• Previous episode of transverse myelitis
• Hypertension




• Raised PT and APTT: Given oral vitamin K: PT improved, APTT stayed prolonged
• PT 10s, APTT 100s
• DRVVT negative
• FVIII 1%
• FVIII inhibitor 73 BU/ml
• Acquired haemophilia A
Acquired haemophilia A
• Autoantibodies directed specifically against FVIII
• Epidemiology
– Incidence: 1.0 per million per year
– Sex distribution: Equal (overall)
– Median age at onset: 70 years
– Bimodal trend. Young females and elderly males
Acquired haemophilia A
• Idiopathic– 50% of cases
• Malignancy– Any type
• Post-partum• Autoimmune disorders
– Rheumatoid arthritis– SLE– Sjogrens syndrome– IBD
• Medication– Penicillins– Sulphonamides– Anticonvulsants– Alpha IFN
.
Congenital vs Acquired Haemophilia
Congenital
• Haemarthroses
• Muscle bleeds
• Soft tissue bleeds
Acquired
• Large haematomas
• Gross haematuria
• Retropharyngeal and
retroperitoneal haematomas
• Cerebral haemorrhages
• Compartment syndrome
Almost Finished!BOOM!

Thank you