abg interpretation
TRANSCRIPT
Overview.
Indications of ABG.
Contraindication.
Parameters and reference ranges.
Other useful information from arterial blood gases.
Factors influencing blood gas results.
Primary acid-base disturbances.
Mixed acid–base disorders
Interpretation of ABG.
An arterial blood gas (ABG) test measures the
acidity (pH) and the levels of oxygen and carbon
dioxide in the blood from an artery.
Blood may be collected from one of the following
arteries:
•Radial artery in the wrist
•Femoral artery in the groin
•Brachial artery in the arm
ABGs provide the following information:
•Oxygenation
•Adequacy of ventilation
•Acid-base levels
Respiratory failure - in acute and chronic states.
Any severe illness which may lead to a metabolic
acidosis - for example:
Cardiac failure.
Liver failure.
Renal failure.
Hyperglycaemic states associated with diabetes
mellitus.
Multiorgan failure.

Sepsis.
Burns.
Poisons/toxins.
Ventilated patients.
Sleep studies
An abnormal modified Allen test (Assessment of collateral
circulation).
Local infection or distorted anatomy at the potential
puncture site (eg, from previous surgical interventions,
congenital or acquired malformations, or burns).
The presence of arteriovenous fistulas or vascular grafts.
Known or suspected severe peripheral vascular disease of
the limb involved.

severe coagulopathy.
Anticoagulation therapy with warfarin, heparin and
derivatives, aspirin is not a contraindication for arterial
vascular sampling in most cases.
Use of thrombolytic agents, such as streptokinase or tissue
plasminogen activator.

digital occlusion of
radial and ulnar
artery

clenching of hand
About 30 sec

ulnar artery
occlusion released.

The test is then
repeated, but this
time the radial
artery is released
while the ulnar
artery remains
compressed .
Positive Modified Allen Test (Normal) :
if the hands flushing within 5-15 sec it indicate that the ulnar artery
has good blood flow.
Negative Modified Allen Test (Abnormal):
if the hands does not flushing within 5-15 sec it indicate that the
ulnar circulation is inadequate , in this situation the radial artery
supplying arterial blood to that hand should not be punctured.

Analyte arterial blood gases venous blood gases
pH 7.35 - 7.45 7.32 – 7.43
PaCO2 35-45 mmHg
4.7- 6.0 kPa
41 – 50 mmHg
PaO2 75-100 mmHg
11-13 kPa
25 – 40 mmHg
Base excess
(BE)
−2 to +2 mmol/L
total CO2
(tCO2 )
23-30 mmol/L
100-132 mg/Dl
HCO3 22–26 mEq/L 23 – 27 mmol/L

The venous oxygen is lower than
the arterial oxygen. The PCO2 will
be higher in venous than arterial
blood.
Arterial blood is bright red colour,
but venous blood is dark maroon in
colour.
Arterial blood gases more painful
and have more complication.
Notes :
age and altitude dependent
Kilopascals: to convert pressures to kPa, divide
mmHg by 7.5
mmHg change in PaCO2 above or below 40 mmHg
results in 0.008 unit change in pH in the opposite
direction
change in [HCO3-] of 10 mEq/L will result in a
change in pH of approximately 0.15 pH units in the
same direction
The Base Excess
The metabolic component of the acid–base balance is
reflected in the base excess.
This is a calculated value derived from blood pH and
PaCO2.
It is defined as the amount of acid required to
restore a litre of blood to its normal pH at a PaCO2 of 40
mmHg.
The base excess increases in metabolic alkalosis and
decreases (or becomes more negative) in metabolic
acidosis.
While the base excess may give some idea of the metabolic
nature of a disorder,
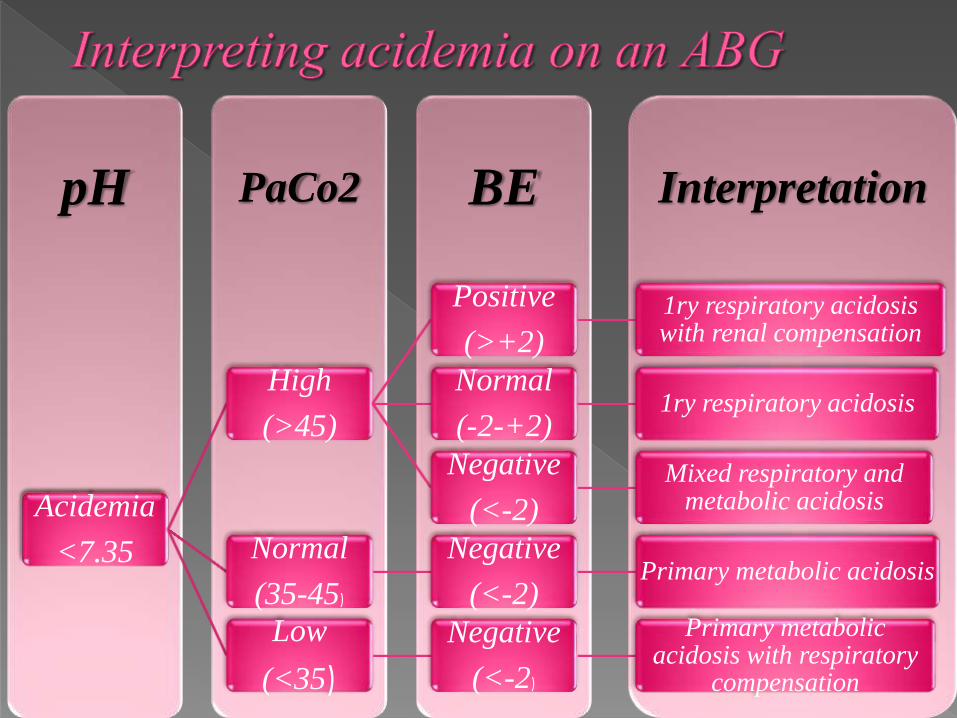
InterpretationBEPaCo2pH
Acidemia
<7.35
High
(>45)
Positive
(>+2)
1ry respiratory acidosis with renal compensation
Normal
(-2-+2)1ry respiratory acidosis
Negative
(<-2)
Mixed respiratory and metabolic acidosis
Normal
(35-45)
Negative
(<-2)Primary metabolic acidosis
Low
(<35)
Negative
(<-2)
Primary metabolic acidosis with respiratory
compensation

InterpretationBEPaCo2pH
Alkalemia>7.35
High
(>45)
Positive
(>+2)
1ry metabolic alkalosis with respiratory compensation
Normal
(35-45)
Positive
(>+2)
Primary metabolic alkalosis
Low
(<35)
Positive
(>+2)
mixed respiratory and metabolic alkalosis
Normal
(-2-+2)
Primary respiratory alkalosis
Negative
(<-2)
Primary respiratory alkalosis with renal
compensation

Alveolar-arterial oxygen gradient :
is a measure of the difference between the alveolar
concentration of oxygen (A) and the arterial
concentration of oxygen(a) .
It is used in diagnosing the source of hypoxemia
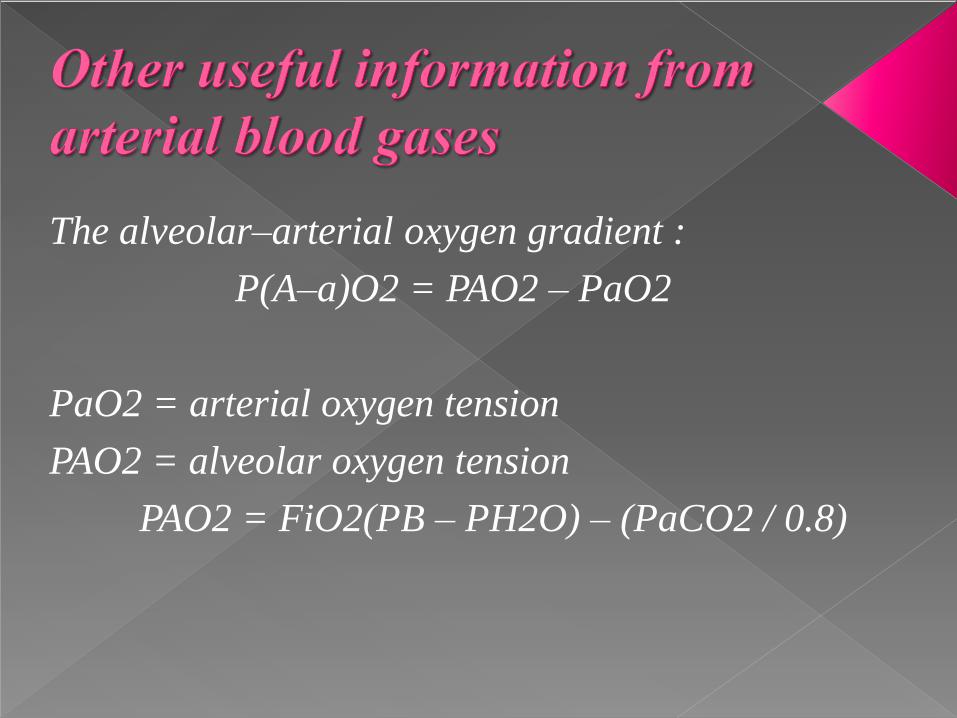
The alveolar–arterial oxygen gradient :
P(A–a)O2 = PAO2 – PaO2
PaO2 = arterial oxygen tension
PAO2 = alveolar oxygen tension
PAO2 = FiO2(PB – PH2O) – (PaCO2 / 0.8)
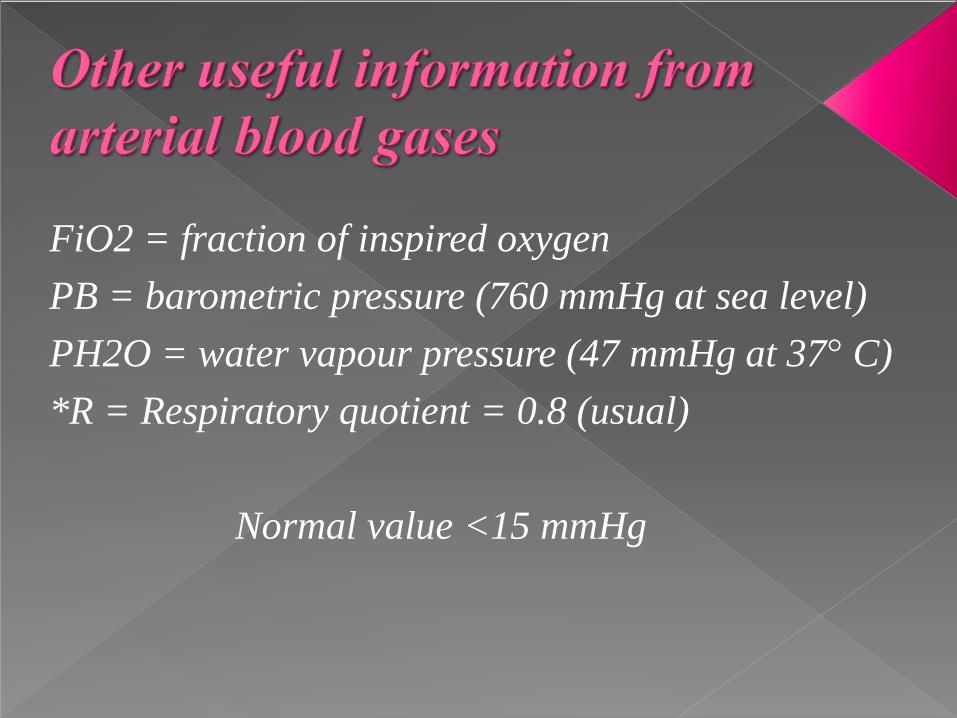
FiO2 = fraction of inspired oxygen
PB = barometric pressure (760 mmHg at sea level)
PH2O = water vapour pressure (47 mmHg at 37° C)
*R = Respiratory quotient = 0.8 (usual)
Normal value <15 mmHg
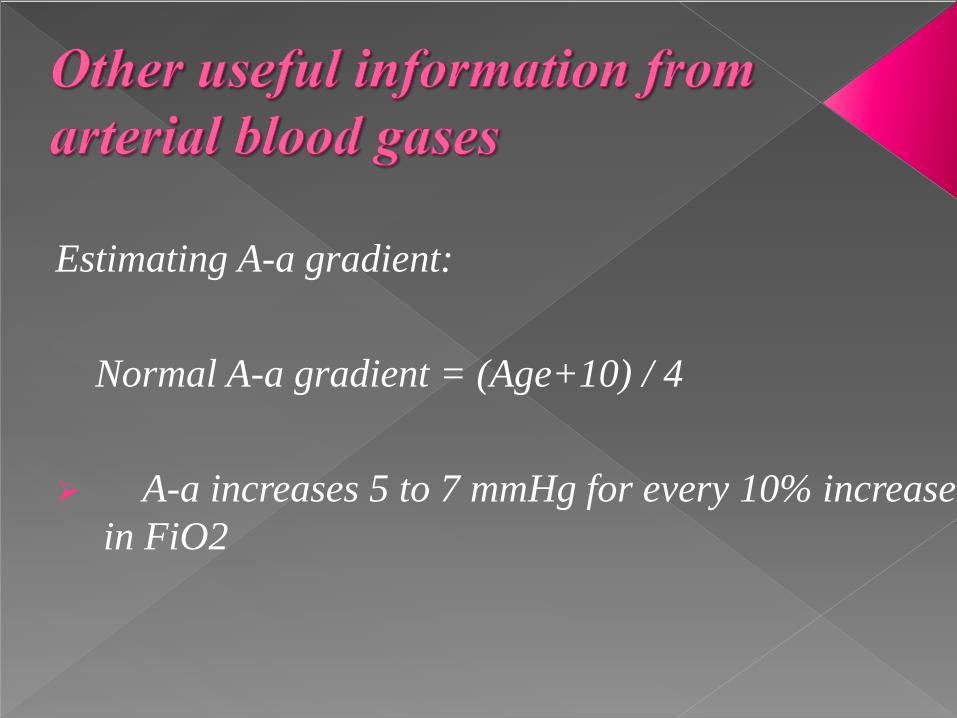
Estimating A-a gradient:
Normal A-a gradient = (Age+10) / 4
A-a increases 5 to 7 mmHg for every 10% increase
in FiO2
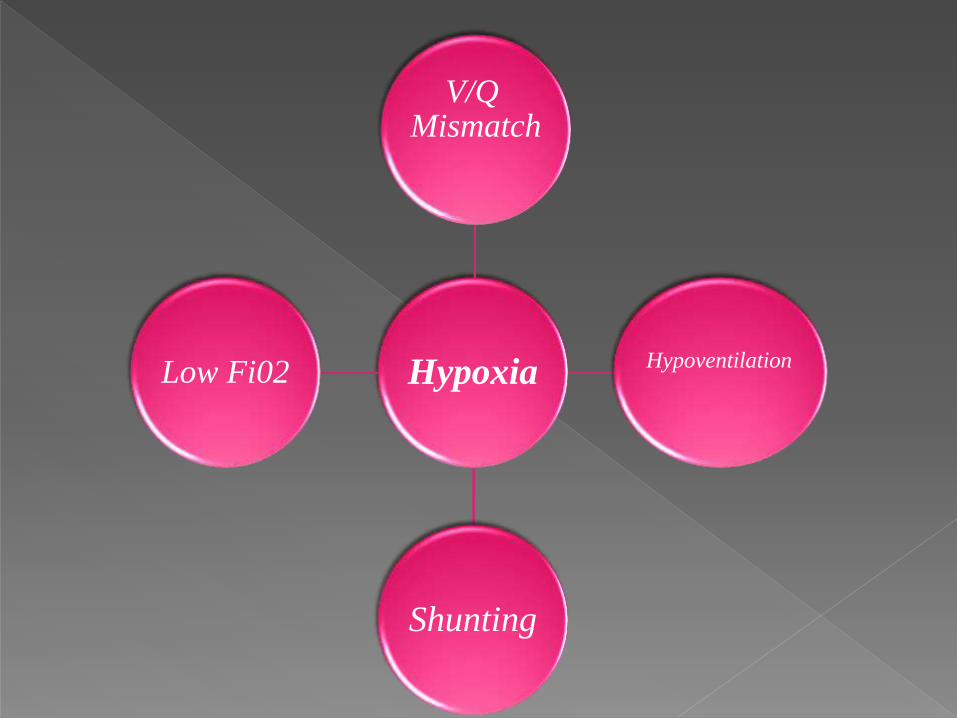
Hypoxia
V/Q Mismatch
Hypoventilation
Shunting
Low Fi02
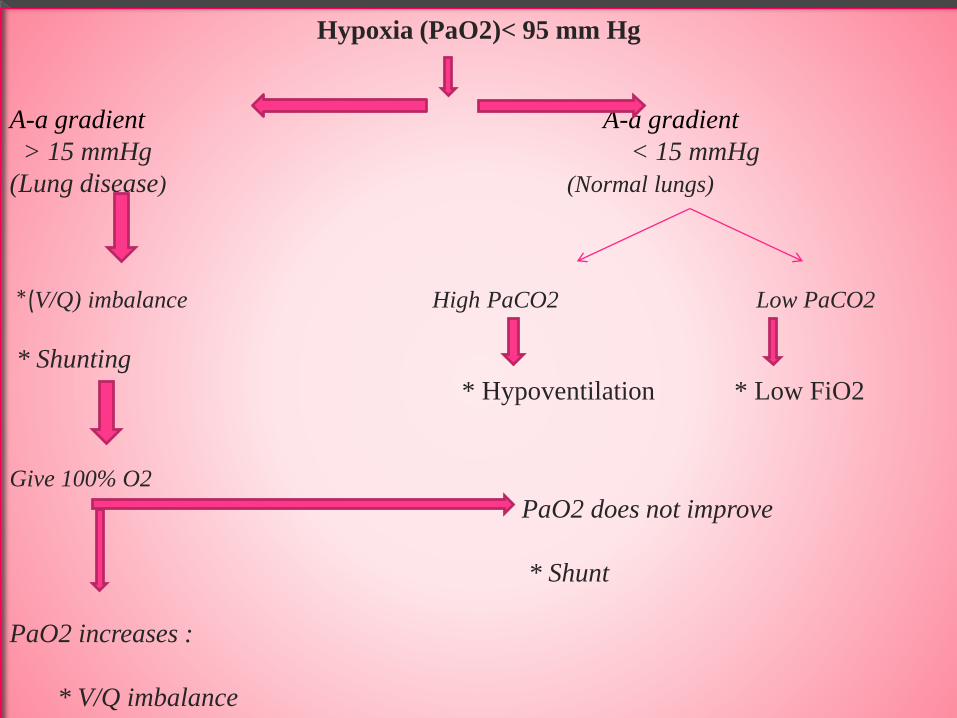
Hypoxia (PaO2)< 95 mm Hg
A-a gradient A-a gradient
> 15 mmHg < 15 mmHg
(Lung disease) (Normal lungs)
*(V/Q) imbalance High PaCO2 Low PaCO2
* Shunting
* Hypoventilation * Low FiO2
Give 100% O2
PaO2 does not improve
* Shunt
PaO2 increases :
* V/Q imbalance

Anion gap :
The anion gap is the difference between primary
measured cations (sodium Na+ and potassium
K+) and the primary measured anions (chloride
Cl- and bicarbonate HCO3-) in serum.
Its used to identify the cause of metabolic
acidosis

Calculation:
With potassium :
= ([Na+] + [K+]) − ([Cl−] + [HCO3−])
Without potassium (daily practice):
= Na+ − (Cl- + HCO3−)
The reference range of the anion gap is 3-11 mEq/L
Delayed processing of the sample may yield a falsely low
PaO2, as the delay allows leucocytes to consume oxygen.
This can be avoided by prompt transport of the sample on
ice.
Air bubbles introduced when performing the arterial
puncture can also cause a falsely high PaO2 and a
falsely low PaCO2.
This can be avoided by gently removing air bubbles within
the specimen immediately after collection without agitating
the sample.
Body temperature can also affect arterial blood gas
tensions.
This is relevant in febrile or hypothermic patients, so
body temperature should be recorded at the time of
collection.
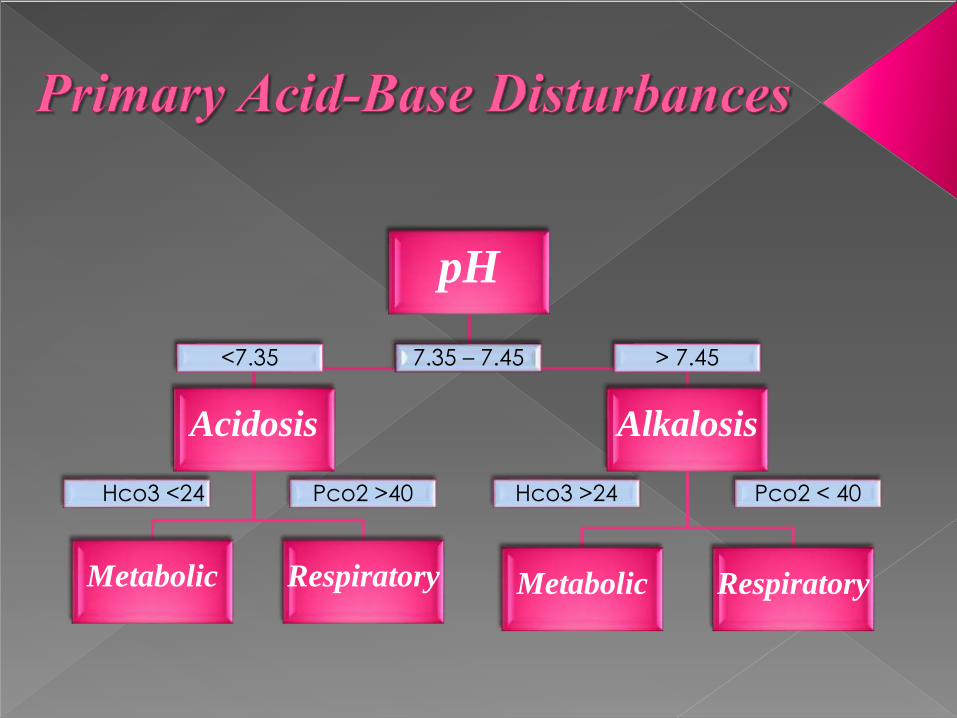
pH
7.35 – 7.45
Acidosis
<7.35
Metabolic
Hco3 <24
Respiratory
Pco2 >40
Alkalosis
> 7.45
Metabolic
Hco3 >24
Respiratory
Pco2 < 40
Metabolic : change in HCO3 and pH in the same
direction .
Respiratory : change in HCO3 and pH in the opposie
direction .
.
One Way To Remember This Relationship Is To Use The
Acronym ROME :
Respiratory Opposite Metabolic Equal
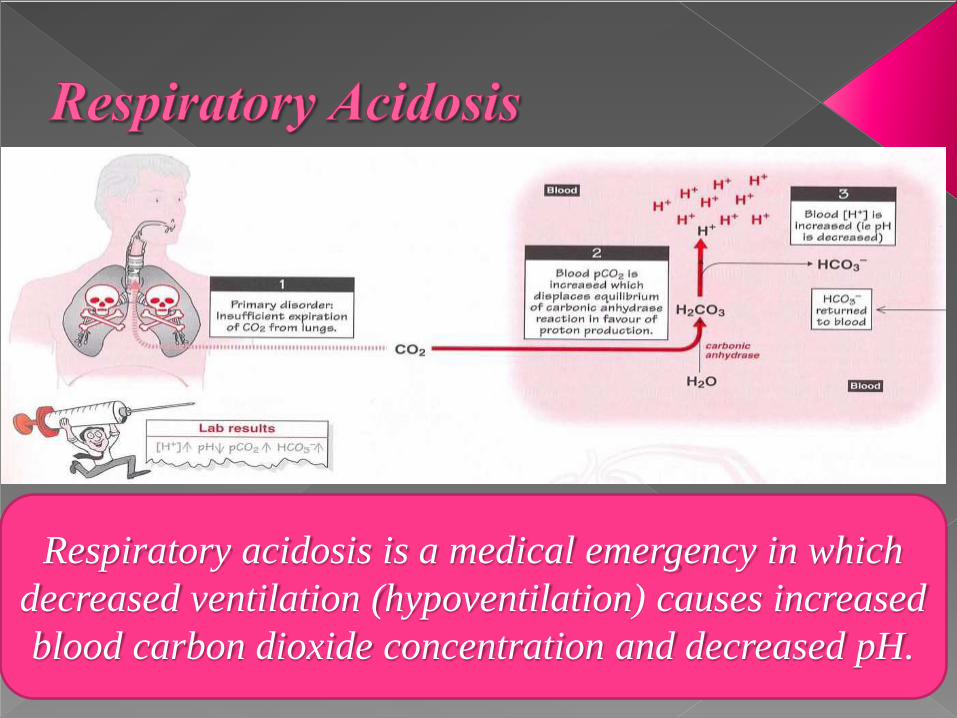
Respiratory acidosis is a medical emergency in which
decreased ventilation (hypoventilation) causes increased
blood carbon dioxide concentration and decreased pH.
Types of Respiratory Acidosis :
acute respiratory acidosis :
the PaCO2 is elevated above the upper limit of the reference range
(over 6.3 kPa or 45 mm Hg) with an accompanying acidemia (pH
<7.36).
chronic respiratory acidosis:
the PaCO2 is elevated above the upper limit of the reference range,
with a normal blood pH (7.35 to 7.45) or near-normal pH secondary to
renal compensation and an elevated serum bicarbonate (HCO3−
>30 mm Hg).
Causes of Respiratory Acidosis :
Respiratory centre depression (↓RR ).
• drugs (anaesthesia, sedative, narcotics )
• Trauma
• Increasing ICP
• Stroke
• Encephalitis
• Central apnea
• Supplemental O2 in chronic Co2 retention (i.e COPD)
Causes of Respiratory Acidosis :
Neuromascular disorders (↓TV ):
• Myasthenia gravis
• Gullain-Barre syndrome
• Poliomyelitis
• Muscular dystrophies
• Myopathies
• Chest wall disease (obesity, kyphoscoliosis )
Causes of Respiratory Acidosis :
Airway obstruction (↓FEV ).
Mechanical hypoventilation (inadequate mechanical
ventilation).
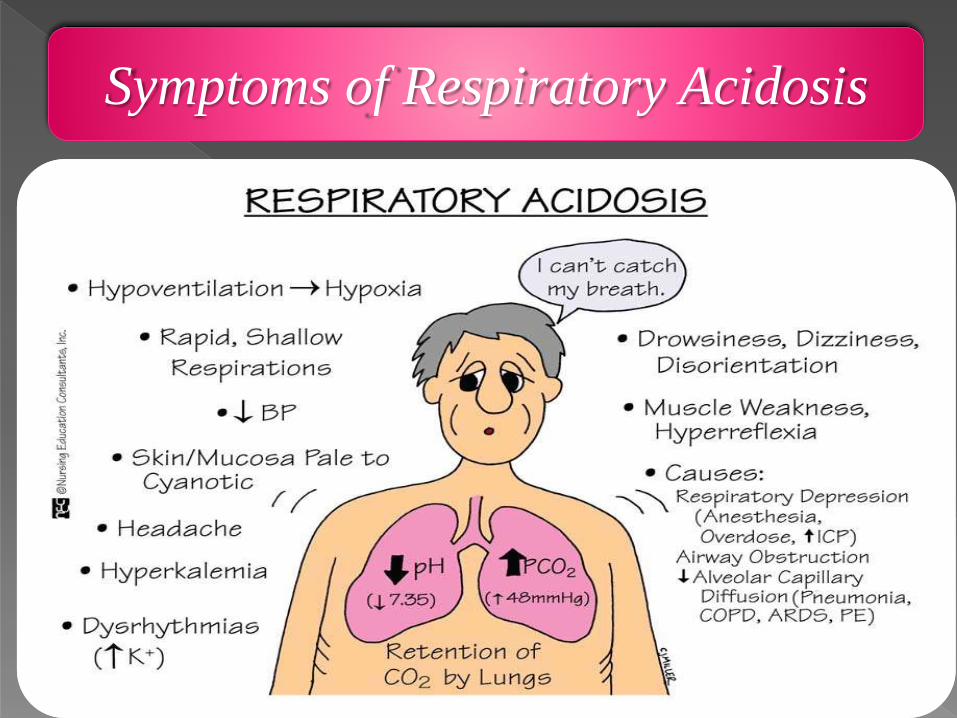
Symptoms of Respiratory Acidosis
Treatment of Respiratory Acidosis
Treatment is aimed at the underlying disease, and
may include:
• Bronchodilator drugs to reverse some types of airway
obstruction
• Noninvasive positive-pressure ventilation (sometimes
called CPAP or BiPAP) or a breathing machine, if
needed
• Oxygen if the blood oxygen level is low
• Treatment to stop smoking
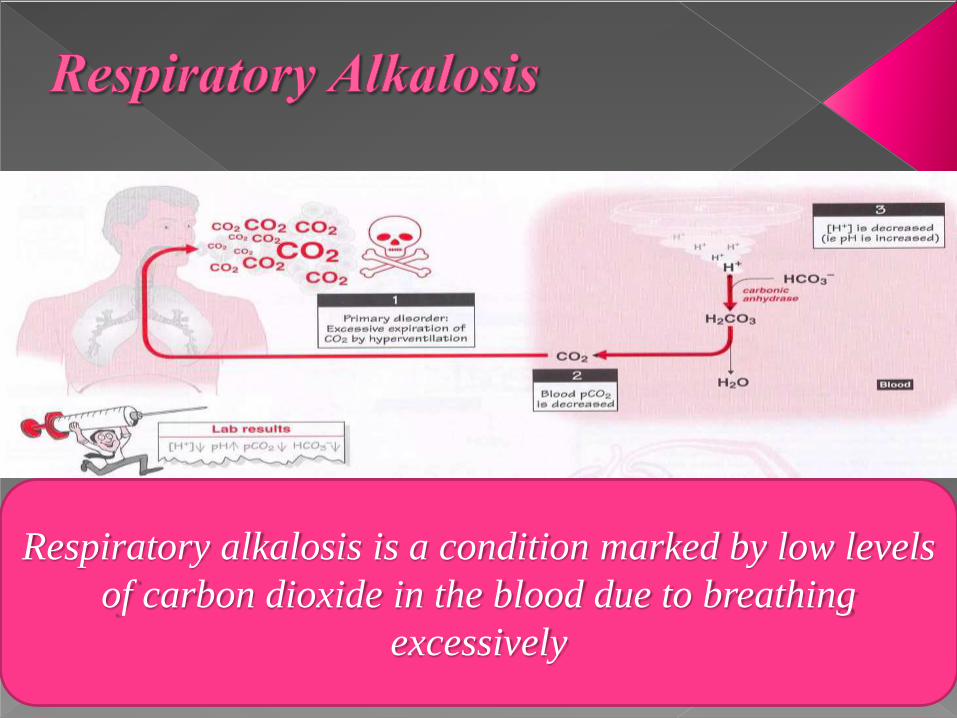
Respiratory alkalosis is a condition marked by low levels
of carbon dioxide in the blood due to breathing
excessively
Types of respiratory alkalosis
Acute respiratory alkalosis:occurs rapidly. For every 10 mmHg drop in PCO2 in arterial
blood, there is a corresponding 2 mEq/L drop in bicarbonate ion due
to acute compensation. During acute respiratory alkalosis, the person
may lose consciousness where the rate of ventilation will resume to
normal.
Chronic respiratory alkalosis:
is a more long-standing condition. For every 10 mmHg drop in
PCO2 in arterial blood, there is a corresponding 5 mEq/L drop in
bicarbonate ion. The drop of 5 mEq/L of bicarbonate ion is a
compensation effect which reduces the alkalosis effect of the drop in
PCO2 in blood. This is termed metabolic compensation.
Causes of Respiratory Alkalosis :
Respiratory centre stimulation :
• CNS disorders
• Hepatic failure
• Gram negative sepsis
• Drugs (theophylline, catecholamine, psychotropic )
• Pregnancy
• Anxiety
• Pain
Mechanical hyperventilation (excessive mechanical
ventilation)
Causes of Respiratory Alkalosis :
Hypoxemia:
• Pulmonary disease (pneumonia, oedema, PE, ILD)
• Sever anaemia
• Heart failure
• High altitude
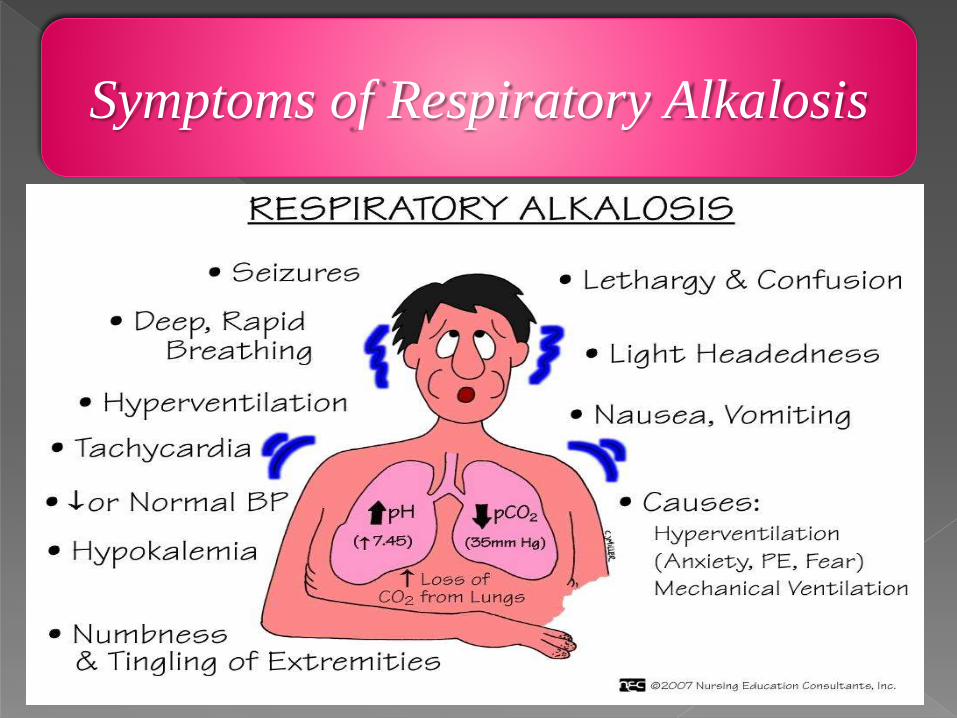
Symptoms of Respiratory Alkalosis
Treatment of Respiratory Alkalosis :
Treatment is aimed at the condition that causes
respiratory alkalosis.
Breathing into a paper bag -- or using a mask that
causes you to re-breathe carbon dioxide -- sometimes
helps reduce symptoms.
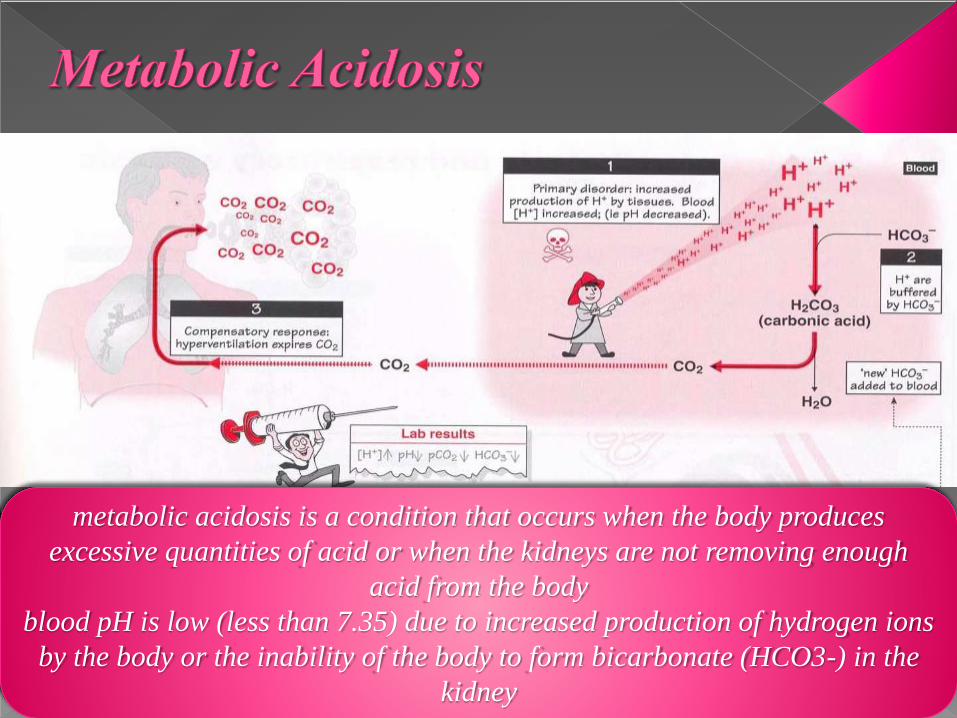
metabolic acidosis is a condition that occurs when the body produces
excessive quantities of acid or when the kidneys are not removing enough
acid from the body
blood pH is low (less than 7.35) due to increased production of hydrogen ions
by the body or the inability of the body to form bicarbonate (HCO3-) in the
kidney
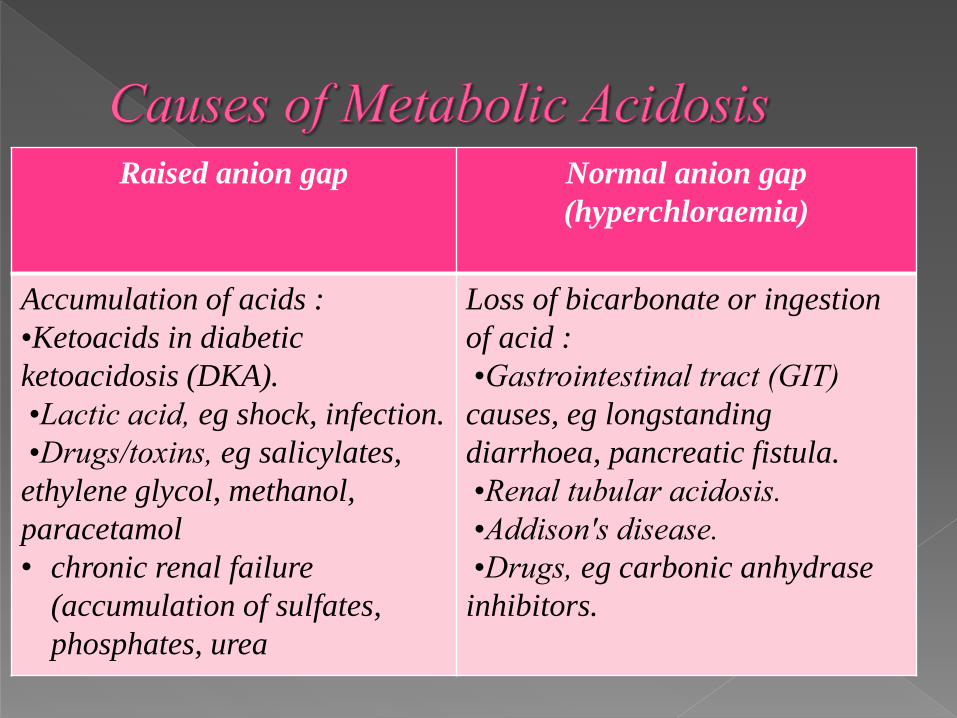
Raised anion gap Normal anion gap
(hyperchloraemia)
Accumulation of acids :
•Ketoacids in diabetic
ketoacidosis (DKA).
•Lactic acid, eg shock, infection.
•Drugs/toxins, eg salicylates,
ethylene glycol, methanol,
paracetamol
• chronic renal failure
(accumulation of sulfates,
phosphates, urea
Loss of bicarbonate or ingestion
of acid :
•Gastrointestinal tract (GIT)
causes, eg longstanding
diarrhoea, pancreatic fistula.
•Renal tubular acidosis.
•Addison's disease.
•Drugs, eg carbonic anhydrase
inhibitors.
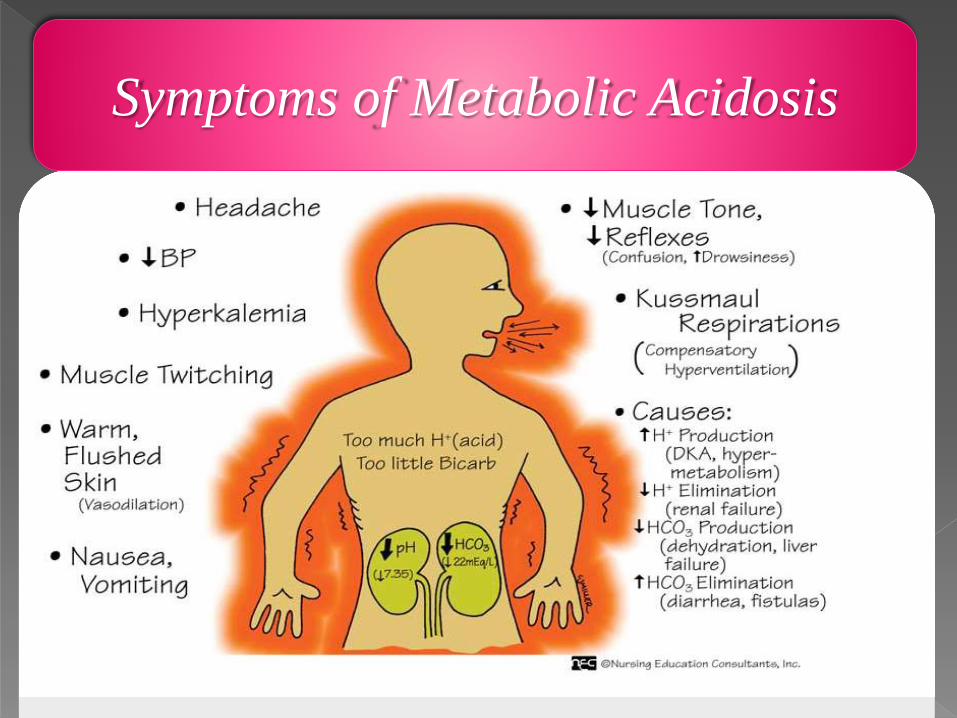
Symptoms of Metabolic Acidosis
Management of Metabolic Acidosis
General measures:
Put the patient in the resuscitation area, or transfer to a high-
dependency area as soon as feasible.
Put the patient on an ECG monitor, SaO2 monitor and BP/HR
monitor.
In patients who are clinically unwell and have deteriorating SaO2
levels or conscious levels, consider intubation and assisted
ventilation, after taking senior A&E/medical/anaesthetic advice.
Get large-bore IV access (a central venous line may be needed) and
rehydrate aggressively. Use colloids if necessary.
Management of Metabolic Acidosis
Consider catheterisation to monitor urine output and obtain urine for
analysis.
If there is any possibility of drug or toxin ingestion, give initial
therapies such as activated charcoal/chelating agents/emetics,
dependent on the specific compound ingested and latest local
guidelines for poisoning.
Liaise with local or national toxicology/poisoning services if there has
been ingestion of a potentially dangerous substance.
Obtain specialist input (usually the on-call general medical team
initially) as soon as possible.
Management of Metabolic Acidosis
Correction of acidosis
Treatment of the underlying cause is the aim. Use of bicarbonate
infusions is not recommended, as it can lead to a fatal outcome. It
should be used only where advised in cases of poisoning.
Specific therapy for the underlying cause
This is the most important and efficient way to correct the acidosis
and improve the patient's outlook. Toxicological/general
medicine/renal medicine expertise should be engaged to offer specific
therapy for the identified underlying problem.
Complications of Metabolic Acidosis
The major problem is suppression of myocardial contractility and
unresponsiveness to catecholamines caused by the acidaemic state.
This may lead to a vicious cycle of hypoperfusion,
worsening lactic acidosis and further cardiac suppression, causing
multi-organ failure. If pH is <7.1-7.2 then cardiac arrhythmias are
likely.
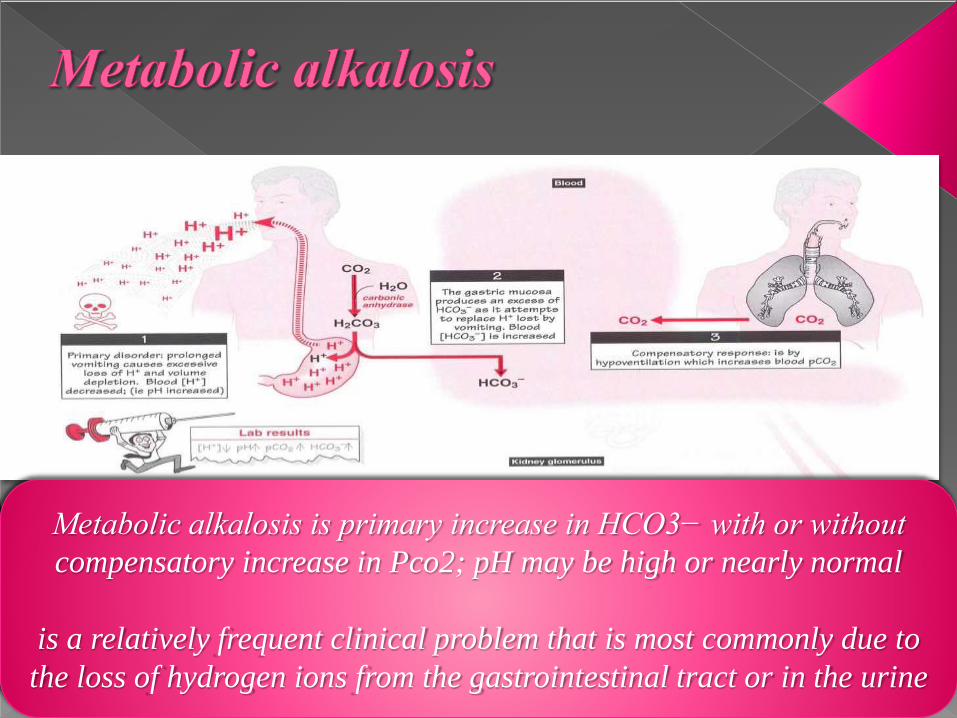
Metabolic alkalosis is primary increase in HCO3− with or without
compensatory increase in Pco2; pH may be high or nearly normal
is a relatively frequent clinical problem that is most commonly due to
the loss of hydrogen ions from the gastrointestinal tract or in the urine
most common causes:
* Vomiting.
* diuretics .
* mineralocorticoid excess.
To differentiate between these conditions, it is usually
helpful to measure the urinary chloride concentration
In causes of metabolic alkalosis associated with a
reduction in the ECV, there will be a stimulus for avid
Na and Cl reabsorption to replenish extracellular
volume. In these setting urinary Cl should be expected
to be very low, < 25 meq/L.
If the urinary Cl is low, indicating a hypovolemic
state, then administration of NaCl and water to
replenish the extracellular volume should stop the
stimulus for aldosterone production and in turn should
lead to appropriate excretion of excess HCO3- and
improvement of hypokalemia. Thus, leading to
correction of the metabolic alkalosis. Such causes of
metabolic alkalosis are said to be saline responsive
In contrast, states of mineralocorticoid excess are
associated with an expanded volume and sometimes
hypertension. The urinary Cl will be high (> 40
meq/L).
In these patients, administration of saline would
further expand the extracellular volume and worsen
hypertension. It would not correct the alkalosis which
is primarily due to hypokalemia. Such causes of
metabolic alkalosis are said to be saline resistant.
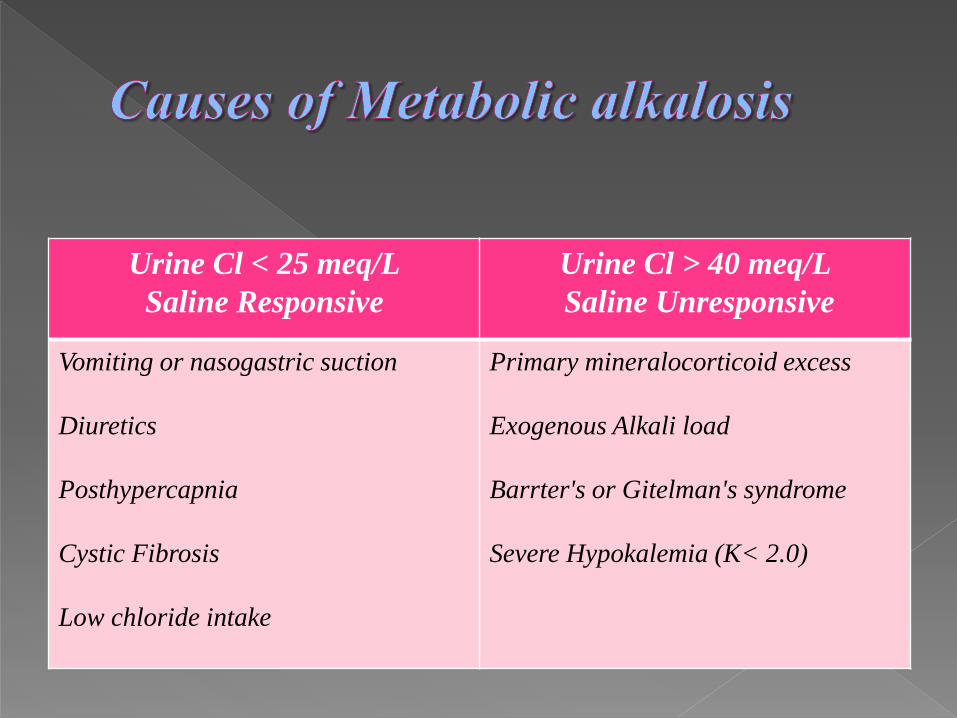
Urine Cl < 25 meq/L
Saline Responsive
Urine Cl > 40 meq/L
Saline Unresponsive
Vomiting or nasogastric suction
Diuretics
Posthypercapnia
Cystic Fibrosis
Low chloride intake
Primary mineralocorticoid excess
Exogenous Alkali load
Barrter's or Gitelman's syndrome
Severe Hypokalemia (K< 2.0)
Causes of saline resistant metabolic alkalosis can
further be distinguished based on whether or not the
patient is hypertensive. Mineralocorticoid excess states
tend to be associated with hypertension while
exogenous alkali load, Barrters and Gitelman's
syndrome are associated with normal blood pressure.
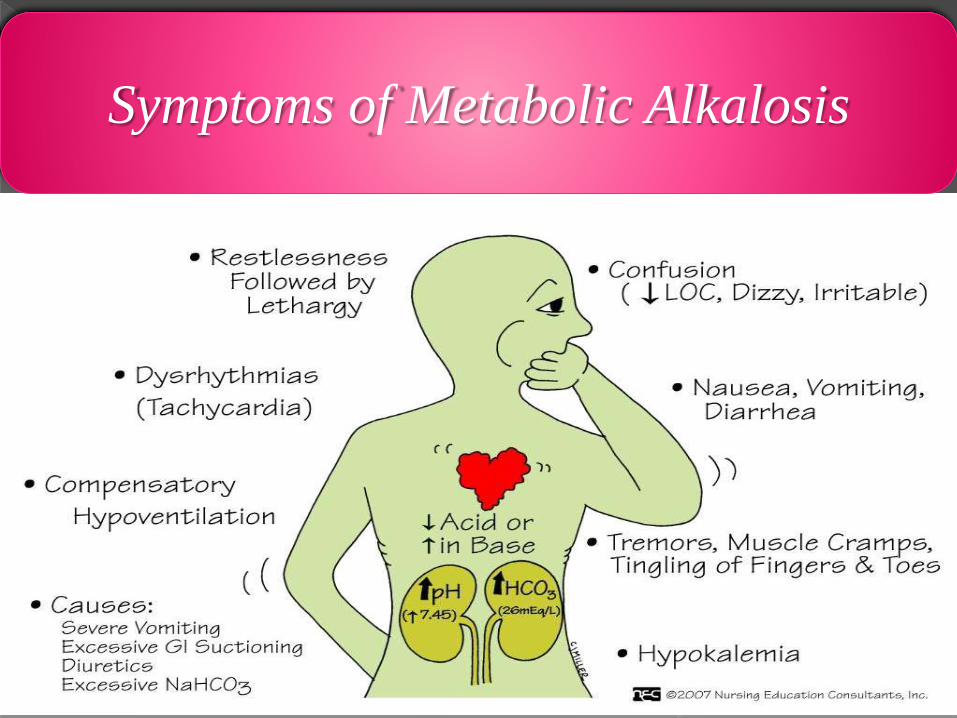
Symptoms of Metabolic Alkalosis
Saline - Responsive metabolic alkalosis:
Re-expand volume with Normal Saline ( Primary Therapy).
Supplement with Potassium to treat hypokalemia (alkalosis
associated with severe hypokalemia will be resistant to volume
resuscitation until K is repleted) .
H+ blockers or PPIs if vomiting/NG suction to prevent further
losses in H+ ions.
Discontinue diuretics.
Acetazolamide if NS contraindicated due to CHF.
(Monitor for hypokalemia).
HCl or NH4Cl in emergency. (HCl can cause
hemolysis, NH4Cl should not be used in liver disease)
Hemodialysis in patients with marked renal failure
Saline – Unresponsive metabolic alkalosis
(Mineraldocorticoid excess).
Surgical removal of mineralocorticoid producing
tumor.
Aldosterone inhibitor.
ACE inhibitor.
Discontinue steroids.
Potassium repletion (only intervention needed to treat
the alkalosis).
When a patient develops an acid-base imbalance, the body
attempts to compensate.
the lungs and the kidneys are the primary buffer response
systems in the body.
The body tries to overcome either a respiratory or
metabolic dysfunction in an attempt to return the pH into
the normal range.
Metabolic compensation occurs over 2-3 days reflecting
altered renal HCO3 production l secretion .
Respiratory compensation through ventilation control of
PaCo2 occurs immediately
A patient can be uncompensated, partially compensated, or
fully compensated
If the pH is between 7.35-7.45, the condition is fully
compensated.
If the pH is outside the range of 7.35-7.45, the condition is
only partially compensated
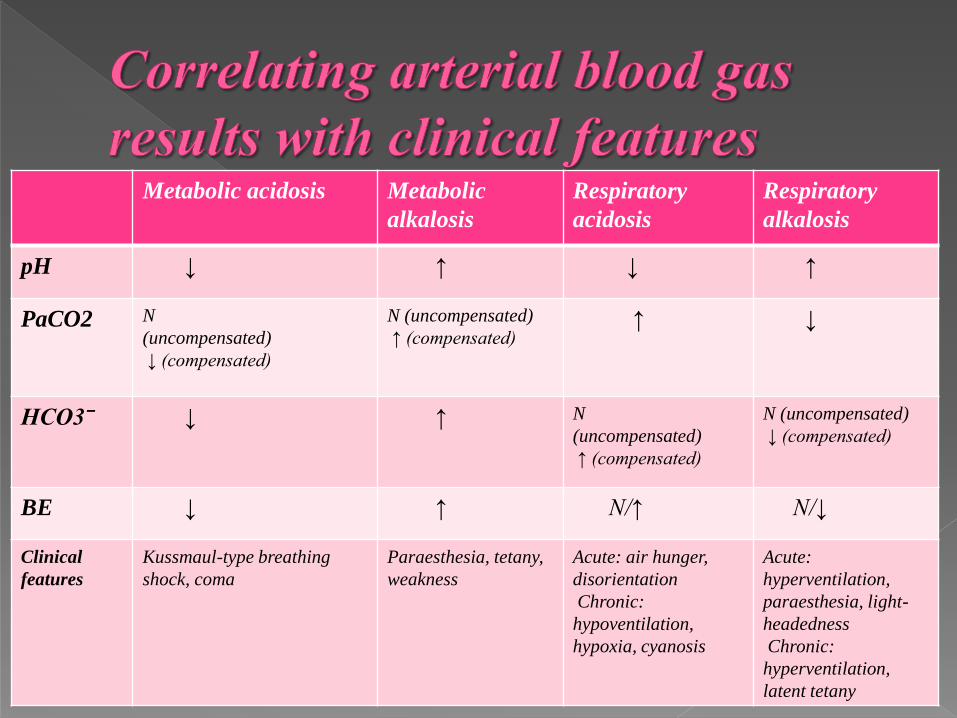
Metabolic acidosis Metabolic
alkalosis
Respiratory
acidosis
Respiratory
alkalosis
pH ↓ ↑ ↓ ↑
PaCO2 N
(uncompensated)
↓ (compensated)
N (uncompensated)
↑ (compensated)↑ ↓
HCO3ˉ ↓ ↑ N
(uncompensated)
↑ (compensated)
N (uncompensated)
↓ (compensated)
BE ↓ ↑ N/↑ N/↓
Clinical
features
Kussmaul-type breathing
shock, coma
Paraesthesia, tetany,
weakness
Acute: air hunger,
disorientation
Chronic:
hypoventilation,
hypoxia, cyanosis
Acute:
hyperventilation,
paraesthesia, light-
headedness
Chronic:
hyperventilation,
latent tetany

It is possible to have a mixed respiratory and
metabolic disorder that makes interpretation of an
arterial blood gas result difficult.
As a general rule, when a normal pH is accompanied
by an abnormal PaCO2 or HCO3ˉ then a mixed
metabolic-respiratory disorder exists.
Respiratory acidosis and metabolic acidosis :
A patient with acute pulmonary oedema after an
acute myocardial infarct
Respiratory alkalosis and metabolic alkalosis:
A patient with hepatic cirrhosis who is given
diuretics.
Respiratory acidosis and metabolic alkalosis :
A patient with long-standing chronic obstructive
pulmonary disease who is given diuretics for
concomitant heart failure.
Respiratory alkalosis and metabolic acidosis.
A patient with chronic renal failure who begins to
hyperventilate secondary to anxiety

Step 1 : Is The pH normal?
pH
Alkalemia
>7.45
Step 2 : Is the disturbance respiratory or metabolic?
Match The CO2 Or The HCO3 With The pH
ROME :
Respiratory Opposite Metabolic Equal
Step 3 : Is there appropriate compensation for the
primary disturbance?
pH is between 7.35-7.45 fully compensated
pH is outside 7.35-7.45 partially
compensated.
Step 4 : Are The pO2 And The O2 Saturation normal?
pO2 (<80 mmHg)
Hypoxia
SO2 (<95 %)
Hypoxaemic respiratory failure (type I respiratory
failure): PaO2 is less than 60 mm Hg (8 kPa) with a
normal or low PaCO2
Hypercapnic respiratory failure (type II respiratory
failure): PaCO2 is more than 50 mm Hg (6.5 kPa) and
indicates inadequate alveolar ventilation.
Respiratory failure may be acute or chronic:
Acute hypercapnic respiratory failure develops over minutes to hours. The pH is usually therefore less than 7.3.
Chronic respiratory failure develops over several days or longer. There is sufficient time for renal compensation and an increase in bicarbonate so the pH is usually only slightly decreased. Clinical markers of long-standing hypoxaemia include polycythaemia and cor pulmonale.

If the pH 7.30 , the PaCo2 is 50 , and the HCO3 is 24 ,
what is likely diagnosis ?
If the pH 7.30 , the PaCo2 is 50 , and the HCO3 is 24 ,
what is likely diagnosis ?
Uncompensated Respiratory Acidosis
If the pH 7.49 , the PaCo2 is 25 , and the HCO3 is 22 ,
what is likely diagnosis ?
If the pH 7.49 , the PaCo2 is 25 , and the HCO3 is 22 ,
what is likely diagnosis ?
Acute Respiratory Alkalosis
If the pH 7.35 , the PaCo2 is 25 , and the HCO3 is 9 ,
what is likely diagnosis ?
If the pH 7.35 , the PaCo2 is 25 , and the HCO3 is 9 ,
what is likely diagnosis ?
Compensated Metabolic Acidosis
If the pH 7.29 , the PaCo2 is 30 , and the HCO3 is 18 ,
what is likely diagnosis ?
If the pH 7.29 , the PaCo2 is 30 , and the HCO3 is 18 ,
what is likely diagnosis ?
Partially Compensated Metabolic Acidosis.
If the pH 7.45 , the PaCo2 is 48 , and the HCO3 is 28 ,
what is likely diagnosis ?
If the pH 7.45 , the PaCo2 is 48 , and the HCO3 is 28 ,
what is likely diagnosis ?
Compensated Metabolic Alkalosis