abbreviations and terms used in the document - lrv.lt · web viewsam - neo, feasibility study -...
TRANSCRIPT

Preparation of the feasibility study and final project proposals of the projects on the improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals including implementation of energy-sparing technologiesR.3. Feasibility study project
CONFIDENTIAL document.docx
Ministry of Health of the Republic of Lithuania20 September 2010 Version 5.00

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 2 of 281
R.3. Feasibility study
DOCUMENT APPROVAL
Ministry of Health of the Republic of Lithuania
Signature:
First name, surname, position:
Date:
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 3 of 281
R.3. Feasibility study
DOCUMENT VERSIONS
Date Version Description
Prepared (corrected by)
Edited pages
11-05-2010 v1.00 The document which was prepared and submitted for the review of the Contracting Authority
Kestutis Gailius, Linas Dicpetris (ascertained quality)
-
21-06-2010 v2.00 The document which was adjusted according to the comments made by the Contracting Authority on the 21st of May 2010
Kestutis Gailius, Linas Dicpetris (ascertained quality)
Changes in the whole
document
04-08-2010 v3.00 The document which was adjusted according to the comments made by the Contracting Authority on the 30th of June 2010 – 2nd of August 2010
Kestutis Gailius, Linas Dicpetris (ascertained quality)
Changes are
marked in the
document
17-08-2010 v4.00 The document which was adjusted according to the comments made by the Contracting Authority on the 6th of August 2010 – 13th of August 2010
Kestutis Gailius, Linas Dicpetris (ascertained quality)
Changes are
marked in the
document
10-09-2010 V5.00 The document which was adjusted according to the comments made by the Contracting Authority on the 2nd of Septmeber 2010
Kestutis Gailius, Linas Dicpetris (ascertained quality)
Changes are
marked in the
document
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 4 of 281
R.3. Feasibility study
Table of Contents1. ABBREVIATIONS AND TERMS USED IN THE DOCUMENT.............................72. INTRODUCTION....................................................................................123. WORK PERFORMANCE METHODOLOGY...................................................17
3.1 METHODOLOGY OF PERFORMING THE PATIENTS SATISFACTION ANALYSIS...............................173.2 METHODOLOGY OF PERFORMING THE ANALYSIS OF THE SERVICES PROVIDED BY PHCI.............17
3.2.1 Schedule of visits to PHCI.............................................................................................203.3 METHODOLOGY OF PERFORMING THE ANALYSIS OF THE SCOPE OF PHCI ACTIVITY, ITS HUMAN RESOURCES AND THEIR PROSPECTS........................................................................................213.4 METHODOLOGY OF PERFORMING THE ANALYSIS OF THE AVAILABLE MEDICAL EQUIPMENT IN PHCI
223.5 METHODOLOGY OF PERFORMING THE ANALYSIS OF REANIMOBILES FOR THE NEWBORN TRANSPORTATION...............................................................................................................223.6 METHODOLOGY OF PERFORMING THE ANALYSIS OF DIAGNOSING ILLNESSES OR STATES OF PREGNANT WOMEN, DELIVERING WOMEN AND NEWBORNS AND TREATMENT METHODOLOGIES.............233.7 METHODOLOGY OF PERFORMING THE ANALYSIS OF THE QUALIFICATION OF HUMAN RESOURCES. 243.8 METHODOLOGY OF PERFORMING THE ANALYSIS OF THE BUILDINGS AND PREMISES OF PHCI.....24
4. ANALYSIS OF THE PRESENT SITUATION AND ENVIRONMENT...................264.1 REVIEW OF THE DEMOGRAPHIC SITUATION......................................................................26
4.1.1 International migration.................................................................................................274.1.2 Natality.........................................................................................................................274.1.3 Mortality.......................................................................................................................284.1.4 Population and main demographic indicators in the regions........................................284.1.5 Main demographic indicators in the Member States of the European Union................29
4.2 SATISFACTION OF PATIENTS.........................................................................................304.3 ANALYSIS OF THE SERVICES PROVIDED BY PHCI..............................................................34
4.3.1 Comparison of PHCI according to the scope of provided services................................354.3.2 Comparison of PHCI according to the structure of the provided services.....................364.3.3 Structure of all the services provided by PHCI in 2007, 2008 and 2009.......................404.3.4 Conclusions of the analysis of the services provided by PHCI......................................41
4.4 ANALYSIS OF ACTIVITY SCOPE AND HUMAN RESOURCES OF PHCI AND THEIR PROSPECTS.........424.4.1 Comparison of PHCI according to the number of births per employee.........................424.4.2 Comparison of PHCI according to the number of births per obstetrician-gynaecologist
444.4.3 Comparison of the number of staff of PHCI according to age.......................................454.4.4 Comparison of PHCI according to the part of staff on secondary jobs..........................464.4.5 Comparison of PHCI according to the structure of staff in 2010...................................474.4.6 Comparison of PHCI according to the number of births per delivery room...................484.4.7 Comparison of PHCI according to the bed turnover rate..............................................494.4.8 Comparison of PHCI according to the number of bed days per patient........................504.4.9 Comparison of PHCI according to the rate of Caesarean sections from all births in PHCI
514.4.10 Comparison of PHCI according to the rate of births per administrative unit................524.4.11 General comparison of all PHCI of Vilnius and Kaunas according to the rate of births per administrative unit...............................................................................................................534.4.12 Comparison of total rates of perinatal centres in Vilnius and Kaunas..........................53
4.5 DEMAND FOR STAFF..................................................................................................554.6 STAFF FORECASTS.....................................................................................................59
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 5 of 281
R.3. Feasibility study
4.7 LIST OF PHCI RECOMMENDED FOR PARTICIPATION IN THE PROGRAMMES FOR OBTAINING THE SUPPORT FROM THE SWISS GOVERNMENT...............................................................................65
4.7.1 Criteria of selection of PHCI participating in the programme.......................................654.7.2 Priority list of the hospitals participating in the programme........................................704.7.3 Situation of Vilnius perinatal centre..............................................................................73
5. ANALYSIS OF MEDICAL EQUIPMENT.......................................................775.1 ANALYSIS OF MEDICAL EQUIPMENT AVAILABLE AND REQUIRED FOR PHCI..............................77
5.1.1 Medical equipment available for PHCI..........................................................................775.1.2 Needs for PHCI for medical equipment.........................................................................815.1.3 Prices of medical equipment........................................................................................93
6. ANALYSIS OF REANIMOBILES FOR THE NEONATE TRANSPORTATION......1006.1 ANALYSIS OF REANIMOBILES FOR THE NEONATE TRANSPORTATION AVAILABLE FOR PHCI........1006.2 ANALYSIS OF USE OF REANIMOBILES FOR THE NEONATE TRANSPORTATION AVAILABLE AT PHCI
1026.3 NEEDS OF PHCI FOR EXTRA REANIMOBILES OR THEIR RENEWAL.......................................1056.4 ALTERNATIVES FOR THE SATISFACTION OF THE NEEDS FOR REANIMOBILES FOR NEONATE TRANSPORTATION OF PHCI................................................................................................1076.5 RECOMMENDATIONS FOR SATISFACTION OF THE NEEDS OF PHCI FOR REANIMOBILES FOR NEONATE TRANSPORTATION................................................................................................1096.6 NEED FOR INVESTMENTS IN REANIMOBILES FOR THE NEONATE TRANSPORTATION..................110
7. ANALYSIS OF METHODOLOGIES OF DIAGNOSES OF DISEASE OR STATE AND TREATMENT OF PREGNANT WOMEN, DELIVERING WOMEN AND NEONATES....111
7.1 PRESENT STATE OF METHODOLOGIES OF DIAGNOSES OF DISEASE OR STATE AND TREATMENT OF PREGNANT WOMEN, DELIVERING WOMEN AND NEONATES..........................................................1117.2 ALTERNATIVES OF THE APPROVAL OF METHODOLOGIES OF DIAGNOSES OF DISEASE OR STATE AND TREATMENT OF PREGNANT WOMEN, DELIVERING WOMEN AND NEONATES AT THE NATIONAL LEVEL.....1117.3 GUIDELINES FOR THE APPROVAL OF METHODOLOGIES OF DIAGNOSES OF DISEASE OR STATE AND TREATMENT OF PREGNANT WOMEN, DELIVERING WOMEN AND NEONATES AT THE NATIONAL LEVEL.....113
8. ANALYSIS OF THE QUALIFICATION OF HUMAN RESOURCES...................1158.1 ANALYSIS OF THE QUALIFICATION OF THE EMPLOYEES OF PHCI........................................115
8.1.1 Methods of analysis of the qualification of the employees of PHCI.............................1158.2 ANALYSIS OF TRAININGS FOR THE STAFF OF PHCI.........................................................1178.3 NEED FOR TRAININGS OF THE STAFF OF PHCI...............................................................1208.4 NEED FOR INVESTMENTS IN THE ORGANIZATION OF TRAININGS FOR THE STAFF OF PHCI........123
8.4.1 Prices of trainings.......................................................................................................1238.5 ALTERNATIVES OF THE ORGANIZATION OF TRAININGS FOR THE STAFF OF PHCI....................1258.6 RECOMMENDATIONS FOR THE ORGANIZATION OF TRAININGS FOR THE STAFF OF PHCI...........126
8.6.1 Detailed assessment of investments in order to satisfy the needs of PHCI for trainings132
9. ANALYSIS OF BUILDINGS AND PREMISES.............................................1399.1 ANALYSIS OF THE DEMAND FOR MANDATORY REPAIR OF PREMISES OF THE OBSTETRIC AND NEONATAL SUBDIVISIONS...................................................................................................139
9.1.1 Energy-sparing means and their necessity.................................................................1399.1.2 Other measures for repair of the premises of PHCI....................................................1449.1.3 Main indicators of energy audits performed in PHCI during the preparation of the feasibility study........................................................................................................................1459.1.4 List of buildings recommended for renovation...........................................................146
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 6 of 281
R.3. Feasibility study
9.1.5 Essential repair...........................................................................................................1609.2 RATING OF THE LIST OF BUILDINGS RECOMMENDED FOR RENOVATION................................1639.3 FUNDING OF BUILDINGS RECOMMENDED FOR RENOVATION..............................................172
10. INFORMATION SYSTEM ANALYSIS........................................................17510.1 METHODOLOGY OF THE INFORMATION SYSTEM ANALYSIS..............................................17510.2 ASSESSMENT OF THE PRESENT DATA COLLECTION AND ANALYSIS SYSTEMS.......................176
10.2.1 Analysis of the programme used by the obstetric-gynaecologic clinic of KMUC.........17710.2.2 Analysis of the programme used by the neonatal clinic of KMUC...............................17910.2.3 Analysis of the programme used by the obstetric-gynaecologic clinic of VMUH........18210.2.4 Analysis of the programme used by the Swedish hospitals of intensive care of neonates...................................................................................................................................18810.2.5 Analysis of the data collected by the Health Information Centre of the Institute of Hygiene 19410.2.6 Assessment of the present data collection systems and recommendations for their improvement............................................................................................................................199
10.3 NEEDS OF PHCI AND ASSOCIATED INSTITUTIONS AND RECOMMENDATIONS FOR THEIR IMPLEMENTATION..............................................................................................................202
10.3.1 Generalized needs of PHCI and associated institutions for the data accumulation, exchange, analysis and report generation...............................................................................20210.3.2 Minimal set of the data of pregnant women, delivering women and neonates..........20410.3.3 Essence of development of IS and justification of the need.......................................20410.3.4 Recommendations......................................................................................................206
10.4 ANALYSIS OF THE INFORMATION TECHNOLOGY INFRASTRUCTURE OF PHCI.......................20810.5 ASSESSMENT OF SKILLS OF THE STAFF OF PHCI TO WORK WITH INFORMATION SYSTEMS.....20910.6 ALTERNATIVES OF IS IMPLEMENTATION.....................................................................210
10.6.1 Alternative I................................................................................................................21010.6.2 Alternative II...............................................................................................................21410.6.3 Alternative III..............................................................................................................22810.6.4 Optimal alternative of IS PWDWN implementation.....................................................233
10.7 ACTION PLAN FOR THE IMPLEMENTATION OF IS PWDWN............................................23410.7.1 Recommended schedule for the implementation of the development model............23410.7.2 Recommended technical and technological standards..............................................23510.7.3 Information system integration schemes and data exchange models.......................23510.7.4 Description of the information system administration model.....................................24210.7.5 Description of modification of the necessary legal basis............................................246
11. BUDGET OF PROGRAMMES..................................................................24711.1 ACTIVITIES OF PROGRAMMES..................................................................................247
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 7 of 281
R.3. Feasibility study
1. Abbreviations and terms used in the document
Table 1: Abbreviations used in the documentAbbreviation ExplanationAlytus PHCI Public institution Alytus region S.Kudirkos hospitalChristian maternity home
Christian maternity home (branch of public institution Kaunas district hospital)
CR Civil registriesCTG CardiotocogrammeEHH Electronic health historyEHR Electronic health recordeHSCI Electronic health services and collaboration infrastructure
information systemEMR Electronic medical recordErnst & Young, EY Ernst & Young Baltic, UABEU European UnionFMA Fast medical aidIS Information system
IS PWDWN Information system of pregnant women, delivering women and neonates
IT Information technologiesJonava PHCI Public institution Jonava hospitalKaunas 2nd CH Public institution Kaunas 2nd clinical hospitalKedainiai PHCI Public institution Kedainiai hospitalKMUC Kaunas Medical University ClinicKMUC COG Kaunas Medical University Clinic (obstetric services)KMUC NC Kaunas Medical University Clinic (neonatologic services)Kretinga PHCI Public institution Kretinga hospitalKUH Public institution Klaipeda University HospitalKVL Public institution Klaipeda children’s hospitalLazdijai PHCI Public institution Lazdijai hospital
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 8 of 281
R.3. Feasibility study
Abbreviation ExplanationLC Lead Consultants AGMarijampole PHCI Public institution Marijampole hospitalMazeikiai PHCI Public institution Mazeikiai hospitalMHC Ministry of Health of the Republic of LithuaniaP. Mazylio maternity home
P. Mazylio maternity home (branch of public institution Kaunas 2nd clinical hospital)
Panevezys PHCI Public institution Panevezys county hospitalPasvalys PHCI Public institution Pasvalys hospitalPHCI Personal health care institution of LithuaniaRadviliskis PHCI Public institution Radviliskis hospitalRaseiniai PHCI Public institution Raseiniai hospitalRL Republic of LithuaniaRokiskis PHCI Public institution Rokiskis district hospitalSalcininkai PHCI Public institution Salcininkai district hospitalSiauliai PHCI Public institution Siauliai county hospitalSilute PHCI Public institution Silute hospitalSIP State investment programmeSVEIDRA Information system of mandatory health insuranceSvencionys PHCI Public institution Svencionys district hospitalTaurage PHCI Public institution Taurage county hospitalTelsiai PHCI Public institution Telsiai county hospitalTrakai PHCI Public institution Trakai hospitalUkmerge PHCI Public institution Ukmerge hospitalUtena PHCI Public institution Utena county hospitalVCUH COG Vilnius City University Hospital (obstetric services)Vilkaviskis PHCI Public institution Vilkaviskis hospitalVilnius maternity home
Public institution Vilnius maternity home
Visaginas PHCI Public institution Visaginas hospitalVUCL NC Vilnius University Children’s Hospital (neonatologic
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 9 of 281
R.3. Feasibility study
Abbreviation Explanationservices)
VUHSCCF VU hospital Santariskiu Clinic (obstetric services)VUHSC VU hospital Santariskiu ClinicVUHSCSCC VU hospital Santariskiu Clinic (intensive therapy services)WHO World Health Organization
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 10 of 281
R.3. Feasibility study
Table 2: Tems used in the documentTerm ExplanationContract Service purchase contract No S-3 signed between the
Ministry of Health of the Republic of Lithuania and UAB Ernst & Young Baltic on 19 January 2010
Contracting authority
Ministry of Health of the Republic of Lithuania
Framework Agreement
Framework Agreement between the Government of the Republic of Lithuania and the Swiss Confederation Federal Council the Implementation of the Lithuanian-Swiss Cooperation Programme to reduce economic and social disparities within the enlarged European Union (Official Gazette, 2008, No 44-16322)
Main coordinating institution
Ministry of Finance of the Republic of Lithuania
Order Order of the Minister of Health No 117 of 15 March 1999 „ On the approval of the health care procedures for pregnant women, delivering women and neonates“ (published in the Official gazette, 26 March 1999, No. 28, Publ. No.811)
Programme General programme name: „Improvement of health care services for pregnant women, delivering woman and neonates in Lithuania“. The programme consists of a few projects related to the common theme or the same goals. The programme method means that the intermediate institution is given authorizations to make decisions about individual projects.
Project Preparation of the feasibility study and final project proposals of the projects on the improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals including implementation of energy-sparing technologies
Protocol Methodology of diagnostics of disease or state and treatment of pregnant women, delivering women and neonates
Purchase documents
Purchase provisions of the open public procurement tender No 79879
Service provider Ernst & Young Baltic, UAB and Grontmij | Carl Bro, UAB acting on the basis of joint activity
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 11 of 281
R.3. Feasibility study
Term ExplanationTechnical specification
Technical specification of the public procurement provisions of the open public procurement No 79879
Internship Training, qualification improvement, self-education, practice trips (for example, abroad to study), working for another organization or starting to work somewhere in general to obtain competences necessary for a certain activity or position.
CONFIDENTIAL document.docx
Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 12 of 281
R.3. Feasibility study
2. Introduction
On the 19th of January 2010 the Ministry of Health of the Republic of Lithuania (hereinafter – MHC or Contracting authority) and the private limited company Ernst & Young Baltic (hereinafter – EY or Service provider) signed the service purchase contract Nº S-3 (hereinafter – Contract) on implementing the project “Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies“ (hereinafter – Project).
Feasibility study – this document is intended to justify the demand for implementing the Project „Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies“, the approach to its implementation and its financing.
This feasibility study was prepared on the basis of the requirements of the Contract and Technical specification. The feasibility study has the following goals:
► To analyze and describe the scope of stationary health care services provided for pregnant women, delivering women and newborns in Lithuania, dynamics of its alternation in 2007 – 2009 and perspectives considering the strategy of development in the country and in the appropriate sector, demographic situation, necessity for services, demand for users, service availability, quality and satisfaction of patients (according to a representative survey by interviewing at least 1000 inhabitants in the form of a questionnaire), variation in resources compared to the respective results and tendencies in the countries of the European Union;
► To analyze and describe the scope of the activity of the Personal Health Care Institutions/subdivisions providing stationary health care services for pregnant women, delivering women and newborns and their human resources in 2007 - 2009 and forecasts for 2010 – 2015;
► To assess and describe the amount and state of the medical equipment owned by the institutions/subdivisions, to determine a demand for deficient equipment and its amount, to assess the preliminary demand for the financial resources to purchase new equipment;
► To assess and describe the amount and state of the reanimobiles intended for the newborn transportation owned by Kaunas and Vilnius Perinatal centres and district hospitals (Klaipeda University Hospital, Siauliai county hospital and Panevezys county hospital), assess the funding necessary for purchasing these reanimobiles;
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 13 of 281
R.3. Feasibility study
► To perform the analysis of methodologies of diagnostics of a disease or state and treatment of pregnant women, delivering women and newborns, prepare the priority list of necessary new scientific methodologies (clinical standards) and/or recommendations which are necessary to prepare, assess the funding necessary for preparing the methodologies (clinical standards) and/or recommendations above and integrating them into the clinical practice, propose with what approach these methodologies (clinical standards) should be implemented practically;
► Considering the valid legal acts, to asses and describe the possibility for developing and integrating a stand-alone computer information system for the health data about pregnant women, delivering women and newborns or supplement the national electronic health system with functionality intended for collecting, storing, exchanging and assessing the health data about pregnant women, delivering women and newborns;
► To analyze and describe the need for improving the qualification of doctors – obstetricians-gynaecologists, obstetricians, doctors-neonatologists, paediatricians and children’s nurses providing the services for newborns, weaknesses of the staff qualification by indicating the field where it is necessary to improve the qualification and knowledge. To organize the discussion of the analysis with the specialists of the Society of Lithuanian Obstetricians-Gynaecologists, Association of Neonatology and other societies. To prepare and present recommendations for improving or resuming the knowledge, abilities and practical skills necessary for the professional activity of the staff (training organization, possible Internships in foreign countries (firstly in Switzerland), collaborative seminars and consultations with colleagues (including Swiss), participation in conferences), assess the funding necessary for organizing and implementing these activities;
► To assess and describe the present energy efficiency and infrastructure of the buildings and premises of the institutions, which provide and will continue to provide the services for pregnant women, delivering women and newborns, where there are subdivisions of obstetrics and neonatology, prepare proposals for the infrastructure modernization and assess the necessary funding;
► To perform an energy audit of the buildings to be renovated (including the modernization of heating stations, water supply and ventilation/conditioning systems) in the personal health care institutions and prepare recommendations for the necessary works on the basis of the audit conclusions in order to reach maximum (energy) efficiency, calculate the necessary funding;
► To assess the infrastructure of the premises where there are subdivisions of obstetrics and neonatology by firstly paying attention to the presence of medical gas-oxygen and compressed air and vacuum systems or their
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 14 of 281
R.3. Feasibility study
state, electric supply and safety, prepare proposals for the infrastructure modernization, assess necessary funding;
► To present general recommendation for the increase of energy efficiency in every personal health care institution and infrastructure modernization.
Following the Contract provisions, the Service provider has prepared and is presenting the draft feasibility study. When preparing the feasibility study and in order to collect the data necessary for the analysis of personal health care institutions (hereinafter – PHCI), visits to all PHCI were organized and information about their activity was collected. Besides, questionnaires were prepared and sent to the representatives of all PHCI.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 15 of 281
R.3. Feasibility study
The questionnaires prepared and sent to the representatives of PHCI covered the following fields:
► Extent of the services and dynamics of its variation;► Human resources and dynamics of their variation;► Currently available medical equipment and needs for additional
equipment;► Available reanimobiles for the newborn transportation and needs for
additional reanimobiles;► Diagnostic and treatment methodologies currently available;► Currently available information systems and information technology
hardware;► Staff qualification;► Priorities of the activities to be financed;► Present state of the buildings and engineering systems.
Data used for performing the analysis of PHCI:► Data collected while visiting PHCI;► Data collected by using questionnaires (after the representatives of PHCI
filled in the questionnaires prepared by the Service provider);► Other data presented by the representatives of PHCI;► Currently available data at the mandatory health insurance information
system (hereinafter – SVEIDRA) presented by the representatives of the State Patients’ Fund under the Ministry of Health (hereinafter – SPF).
CONFIDENTIALITY OF THE DOCUMENT:The information presented in this feasibility study is intended solely for the persons related to the Project. The information is intended exclusively for the needs of the addressees. The MHC assumes liability for any modification of the data/information in this report and the use of modified results and Ernst & Young assumes no liability for the modification of the results or the use of modified results.
IMPORTANT: The data presented by PHCI, which was not possible to validate in other publicly available information sources or by visiting PHCI, was not audited; therefore, Ernst & Young assumes no liability for the correctness of the data which was not possible to validate in other publicly available information sources or by visiting PHCI.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 16 of 281
R.3. Feasibility study
The actual results of the calculation can differ from the forecasts and assumptions presented in this feasibility study as forecasted events often happen differently than expected and these deviations can be significant.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 17 of 281
R.3. Feasibility study
3. Work performance methodology
3.1 Methodology of performing the patients satisfaction analysis
In order to collect the data necessary for the patient satisfaction analysis, the Computer Assisted Web Interview of the target audience was performed in February-March 2010. The interview was performed by surveying 1048 women who had given birth in 2007 – 2009.
The data collected during the survey was used to perform an assessment research of the services provided by stationary personal health care institutions to pregnant women, delivering women and newborns, the scope of which included:
► Satisfaction of patients with the services provided by the personal health care institutions (PHCI), performance of the staff and conditions: prenatal, perinatal and neonatal;
► Assessment (ratings) of the staff of PHCI;► Criteria of expectations and future choices.
The summary of the patient satisfaction analysis is presented in chapter Nº 4.2.
3.2 Methodology of performing the analysis of the services provided by PHCI
In order to collect the data necessary to perform the analysis of the services provided by PHCI, visits to each PHCI were organised and information about their activity was collected (the schedule of visits is presented in table Nº 3). Besides, questionnaires were prepared and sent to the representatives of all PHCI and the representatives of each PHCI indicated the scope of the provided services therein.
In order to ensure the correctness of the data presented by the representatives of PHCI, the data presented by PHCI was validated by using the data extracted from SVEIDRA and presented by the representatives of NPF.
► Note: When validating the data presented by PHCI and the data extracted from SVEIDRA, it was observed that not all PHCI indicated in the questionnaire the provided services for which NPF does not pay PHCI, i.e., the services for which the patients had paid themselves. Thus, in order to assess the scope of the services provided by each PHCI, not only of the services paid by NPF, when analyzing the scope of the services provided by each PHCI, the data extracted
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 18 of 281
R.3. Feasibility study
from SVEIDRA was used, as it included the scope of the services for which the patients had paid themselves.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 19 of 281
R.3. Feasibility study
The services provided by PHCI were analyzed by the following profiles:► According to the scope of the services provided by each PHCI in 2007,
2008 and 2009;► According to the structure of the services provided by PHCI in 2009;► Structure of the services provided by PHCI in 2007, 2008 and 2009.
A detailed analysis of the services provided by PHCI is presented in chapter Nº 4.3.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 20 of 281
R.3. Feasibility study
3.2.1 Schedule of visits to PHCI Presented below is a schedule of former visits to PHCI.
Table 3. Schedule of visits to PHCIDate Weekday From 8:00
to 9:00From 9:00 to
10:00From 10:00 to
11:00From 11:00
to12:00From 12:00 to
13:00From 13:00 to
14:00From 14:00 to
15:00From 15:00 to
16:00From 16:00 to
17:0004-02-2010
Thursday Public institution Kaunas 2 clinical hospital
08-02-2010
Monday Public institution Jonava hospital
01-03-2010
Monday
02-03-2010
Tuesday Public institution Siauliai county hospital
Public institution Telsiai county hospital
Public institution Mazeikiai hospital
03-03-2010
Wednesday
04-03-2010
Thursday Public institution Kretinga hospital
Public institution Klaipeda University Hospital
Public institution Silute hospital
09-03-2010
Tuesday Public institution Utena county hospital
Public institution Visagino hospital Public institution Svencionys district hospital
18-03-2010
Thursday Public institution Alytus region S.Kudirkos hospital
Public institution Lazdijai hospital Public institution Marijampolės hospital
Public institution Vilkaviskis hospital
19-03-2010
Friday Public institution, clinic of obstetrics and gynaecology of Vilnius city University Hospital
Public institution, Centre branch of Santariskiu Clinic of VU Hospital
Public institution, clinic of neonatology of Vilnius University
Children’s Hospital23-03-2010
Tuesday Public institution Salcininkai district hospital
Public institution Trakai hospital Public institution Vilnius maternity home
24-03-2010
Wednesday
2010.03.25.
Thursday Public institution clinic of obstetrics and gynaecology of Kaunas Medical University Clinic
and clinic of neonatology of Kaunas Medical University Clinic
P. Mazylio maternity home (Public institution, branch of Kaunas 2
clinical hospital)
Christian maternity home (Public institution, branch of Kaunas
county hospital)
26-03-2010
Friday Public institution Ukmerge hospital
Public institution Radviliškio hospital
Public institution Raseiniai hospital Public institution Taurage county hospital
30-03-2010
Tuesday Public institution Kedainiai hospital
Public institution Panevėžio county hospital
Public institution Pasvalys hospital Public institution Rokiskis district hospital
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 21 of 281
R.3. Feasibility study
Note: The experts docent dr. Mindaugas Kliucinskas and dr. Antanas Puzas, the representatives of MHC and UAB Ernst & Young Baltic participated in the visits to each PHCI. The visits to each PHCI listed in the table above were organized in order to assess the correctness of the data presented by PHCI and to see the current situation in each PHCI. The visits to each PHCI in order to analyze its buildings and premises were organized separately and are not presented in this schedule of visits.
3.3 Methodology of performing the analysis of the scope of PHCI activity, its human resources and their prospects
In order to collect the data necessary for performing the analysis of the scope of the activity of each PHCI, its human resources and their perspectives, questionnaires were prepared and sent to the representatives of all PHCI and the representatives of each PHCI presented information about:
► Scope of the activity of PHCI;► Number of confirmed positions;► Number of working persons;► Needs for human resources;► Division of working persons into age groups.
In order to ensure the correctness and comprehensiveness of the data provided by the representatives of PHCI, the representatives of each PHCI were contacted by telephone and during the conversations, by analyzing the data presented by the representatives of PHCI, it was verified if the indicated data was correct and comprehensive.
The scope of the activity of PHCI, human resources and their perspectives were analyzed by the following profiles:
► Comparison of PHCI according to the number of births per employee;► Comparison of the number of staff of PHCI according to age;► Comparison of PHCI according to the percentage of the staff on secondary
jobs;► Comparison of PHCI according to the structure of the staff in 2010;► Comparison of PHCI according to the number of births per one delivery
room;► Comparison of PHCI according to the bed turnover rate;► Comparison of PHCI according to the number of bed-days per one patient;► Comparison of PHCI according to the percentage of Caesarean sections in
all births in PHCI;► Comparison of PHCI according to the percentage of births by
administrative units.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 22 of 281
R.3. Feasibility study
A detailed analysis of the scope of the activity of PHCI, human resources and their perspectives is presented in chapter Nº 4.4.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 23 of 281
R.3. Feasibility study
3.4 Methodology of performing the analysis of the available medical equipment in PHCI
In order to collect the data necessary for performing the analysis of the available medical equipment in PHCI, questionnaires were prepared and sent to the representatives of all PHCI and the representatives of each PHCI indicated the names of the available medical equipment, its models, purpose, available amount, manufacturer, year of manufacturing, state, depreciation, average number of procedures performed with a certain device per month and other data (the data presented by PHCI is presented in Appendix Nº 4 of this document). In order to ensure the correctness and comprehensiveness of the data provided by the representatives of PHCI, the representatives of each PHCI were contacted by telephone and during the conversations, by analyzing the data presented by the representatives of PHCI, it was verified if the indicated data was correct and comprehensive.
The correctness of the data was also ascertained when visiting each PHCI, collecting information about the activity of each PHCI, inspecting the premises of PHCI where PHCI provide the services for pregnant women, delivering women and newborns and available medical equipment (the schedule of visits is presented in table Nº 3).
The analysis of needs for medical equipment in PHCI was performed by the following profiles:
► Comparison of PHCI according to the total demand for medical equipment in each PHCI;
► Comparison of PHCI according to the demand for medical equipment in each PHCI to which PHCI assigned the first-level priority ;
► Comparison of district PHCIs according to their demand for the optimal-package1 medical equipment in each PHCI;
► Expert assessment of PHCI needs.
A detailed analysis of medical equipment of PHCI is presented in chapter Nº 5.
3.5 Methodology of performing the analysis of reanimobiles for the newborn transportation
In order to collect the data necessary for performing the analysis of reanimobiles for the newborn transportation, questionnaires were prepared and sent to the representatives of VUCH, CN, KMUC, KUH, Siauliai and Panevezys PHCI and the representatives of each PHCI presented the information about the available reanimobiles for the newborn transportation:
1 Optimal package is a list of medical equipment made by the experts doc. dr. Mindaugas Kliučinskas and dr. Antanas Pužas, which is necessary for the provision of services of level IIA and where the medical equipment is grouped according to the type of services provided.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 24 of 281
R.3. Feasibility study
► Make of car;► Type, variant, version;► Model;► Year of manufacturing;► Mounted medical equipment;► State of mounted medical equipment;► Number of newborns transported in 2007, 2008, 2009;► Number of kilometres while transporting newborns in 2007, 2008, 2009;► Other information.
The correctness of the information provided about the available reanimobiles for the newborn transportation was validated when visiting each PHCI, collecting information about the activity of each PHCI and inspecting the reanimobiles of PHCI.
After collecting information about reanimobiles for the newborn transportation from each PHCI, the comparative analysis of reanimobiles for the newborn transportation owned by VUCH, CN, KMUC, KUH, Siauliai and Panevezys PHCI was performed. It involved:
► Number of newborns transported by each PHCI in 2007, 2008 and 2009;► Number of kilometres while transporting newborns by each PHCI in the
available reanimobiles for the newborn transportation in 2007, 2008 and 2009.
A detailed analysis of reanimobiles for the newborn transportation is presented in chapter Nº 6.
3.6 Methodology of performing the analysis of diagnosing illnesses or states of pregnant women, delivering women and newborns and treatment methodologies
In order to collect the data necessary for performing the analysis of diagnosing illnesses or states of pregnant women, delivering women and newborns and treatment methodologies, questionnaires were prepared and the representatives of each PHCI indicated:
► Presently available diagnostics of illnesses or states of pregnant women, delivering women and newborns and treatment methodologies;
► Diagnostics of illnesses or states of pregnant women, delivering women and newborns and treatment methodologies which, in the opinion of each PHCI, should be confirmed at the national level.
After collecting from each PHCI the information about diagnosing illnesses or states of pregnant women, delivering woman and newborns and treatment methodologies used by each PHCI which, in the opinion of each PHCI, should be confirmed at the national level, the collected information was summarized
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 25 of 281
R.3. Feasibility study
and the list of diagnostics of illnesses or states of pregnant women, delivering woman and newborns and treatment methodologies which, in the opinion of each PHCI, should be confirmed at the national level was made.
A detailed analysis of diagnosing illnesses or states of pregnant women, delivering women and newborns and treatment methodologies is presented in chapter Nº 7.
3.7 Methodology of performing the analysis of the qualification of human resources
In order to collect the data necessary for performing the analysis of the qualification of human resources in each PHCI, questionnaires were prepared and sent to the representatives of all PHCI and the representatives of each PHCI presented information about:
► Qualification of the persons working in PHCI;► Former trainings and Internships of the persons working in PHCI;► Demand for trainings of the persons working in PHCI.
In order to ensure the correctness and comprehensiveness of the data provided by the representatives of PHCI, the representatives of each PHCI were contacted by telephone and during the conversations, by analyzing the data presented by the representatives of PHCI, it was verified if the indicated data was correct and comprehensive.
The qualification of human resources of PHCI was analyzed by the following profiles:
► Comparison of PHCI by staff qualifications;► Comparison of PHCI by former staff trainings;► Comparison of PHCI by the expressed demand for staff training.
A detailed analysis of the qualification of human resources is presented in chapter Nº 8.
3.8 Methodology of performing the analysis of the buildings and premises of PHCI
In order to collect the data necessary for performing the analysis of the buildings and premises of each PHCI, questionnaires were prepared and sent to the representatives of all PHCI and the representatives of each PHCI presented the data on the buildings and premises where they provide the services for pregnant women, delivering women and newborns (the data presented by PHCI is presented in Appendix Nº 4 to this document).
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 26 of 281
R.3. Feasibility study
In order to ensure the correctness and comprehensiveness of the data provided by the representatives of PHCI, the representatives of each PHCI were contacted by telephone and during the conversations, by analyzing the data presented by the representatives of PHCI, it was verified if the indicated data was correct and comprehensive.
The correctness of the data was also validated when visiting each PHCI, performing a visual inspection, photofixation, cadastre and technical building state review of the premises of each PHCI where PHCI provide services for pregnant women, delivering women and newborns.
The parameters of energy efficiency influencing energy losses in the buildings of PHCI were established by:
► Performing measurements of energy parameters during the heating season, registering the temperatures inside the building premises, outside, heating device and other energy parameters. To perform these measurements, the premises on different floors of the building and different facades of the building were chosen.
► Using the results of measurements performed by other natural or legal persons (in case these measurements are necessary and their reliability causes no doubt).
Infrastructure of PHCI was assessed on the basis of “Methodology of performing the comprehensive audit of using energy, energy resources and cold water in buildings for public use” ratified with the order Nº 4-184 by the Minister of Economy of the Republic of Lithuania on the 29th of April 2008; STR 2.01.09:2005 “Energy utility of buildings. Certification of energy utility“; STR 1.14.01:1999 “Procedure for calculating area and volume of buildings“; STR 2.05.01:2005 ”Thermal technology of enclosures of buildings“.
After performing the analysis of the collected data, the means of improving energy efficiency and infrastructure were established and economic indicators were calculated. This calculation was performed by using the specialized calculation program of the Service provider developed by using long-term practical experience with energy audits. The present and standard needs for thermal energy and economic efficiency of separate means were assessed.
On the basis of assessing the present state of the building constructions and engineering systems and results of the analysis of economic efficiency of separate energy-saving means, the packages of energy-saving means (groups) were formed. In respect of each energy-saving package, possible energy savings and economic efficiency indicators were calculated. The packages of energy-saving means were formed according to the importance of works to be performed in the analyzed building.
A detailed analysis of the buildings and premises of PHCI is presented in chapter Nº 9.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 27 of 281
R.3. Feasibility study
CONFIDENTIAL document.docx

Births Deaths Emigrants Imigrants
Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 28 of 281
R.3. Feasibility study
4. Analysis of the present situation and environment
In this chapter the review of the demographic situation of Lithuania and the Member States of the European Union (hereinafter – EU) and the analysis of the personal health care institutions of Lithuania providing stationary health care services for pregnant women, delivering women and newborns is presented.
4.1 Review of the demographic situationIn this chapter a short review of the demographic situation in Lithuania and the Member States of the EU is presented on the basis of the data of the Department of Statistics under the Government of the Republic of Lithuania.
According to the data of the Department of Statistics, at the beginning of 2010 3 million 329 thousand inhabitants lived in Lithuania; it is 20.9 thousand less than a year ago. The decrease was influenced by negative net migration (more emigrants than immigrants) which made 74.2% of the total decrease and negative natural variation (more people died than were born) – 25.8%.
In the picture below, the statistics of the births, deaths, emigrants and immigrants in 2008 and 2009 is presented.
Picture Nº 1 – The births, deaths, emigrants and immigrants
In the last five years, the population of Lithuania has decreased by 96.3 thousand (2.8 %).
The Council of Statistics of the European Communities (Eurostat) forecasts that the population will decrease by almost 592 thousand inhabitants at the beginning of 2050 compared with the beginning of this year.
CONFIDENTIAL document.docx
Thousand
Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 29 of 281
R.3. Feasibility study
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 30 of 281
R.3. Feasibility study
4.1.1 International migrationIn 2009 22 thousand emigrants declared their departure from Lithuania, which is almost 5 thousand more than in 2008. 6.5 thousand people immigrated, it is 2.8 thousand less than in 2008. The biggest part of international immigrants consisted of the citizens of the Republic of Lithuania (in 2009 – 74.7% of emigrants and 74.3% of immigrants) and one fourth of them consisted of foreigners.
4.1.2 NatalityIn 2009, 36.7 thousand babies were born, it is 1,6 thousand more than in 2008 when 35.1 thousand babies were born or 2.7 thousand more than in 2007. The number of births per 1000 inhabitants increased from 10.5 in 2008 to 11 in 2009. In 2009 the total birth rate (the average number of born-alive children given by a woman during her fertile period of life) was 1.53 (in 2008 – 1.47).
The level of natality in 2009 does not ensure the demographic balance and generation replacement yet. The most favourable demographic situation is when the total birth rate at least ensures simple reproduction of the country’s inhabitants and is about 2.1 – i.e., every woman should give a birth to at least 2 babies.
The Central Intelligence Agency of the United States of America forecasts that the total birth rate of Lithuania will only be 1.24 in 2010.
According to the data of Eurostat, in 2008 Lithuania was in the 15 th place among the states of the EU and overtook such states as Spain, Cyprus or Latvia (see the table below). The total birth rate of Switzerland was 1.48 in 2008.
Table 4. Total birth rate of the countries of the EUNº State 199
9200
0200
1200
2200
3200
4200
5200
6200
7200
81 Ireland 1.91 1.90 1.96 1.98 1.98 1.95 1.88 1.91 2.03 2.102 France 1.79 1.87 1.88 1.86 1.87 1.90 1.92 1.98 1.96 2.003 United
Kingdomn 1.84 1.63 n n 1.77 1.79 1.85 1.90 1.94
4 Sweden 1.50 1.55 1.57 1.65 1.72 1.75 1.77 1.85 1.88 1.915 Denmark 1.74 1.77 1.75 1.72 1.76 1.78 1.80 1.85 1.85 1.896 Finland n 1.73 1.73 1.72 1.76 1.80 1.84 1.84 1.83 1.857 Belgium n 1.62 n n 1.67 1.72 1.76 1.80 1.81 1.828 Netherlands 1.65 1.72 1.71 1.73 1.75 1.73 1.71 1.71 1.72 1.779 Estonia 1.32 1.39 1.34 1.37 1.37 1.47 1.50 1.55 1.64 1.66
10 Luxembourg 1.73 1.78 1.66 1.63 1.62 1.66 1.62 1.64 1.61 1.6111 Slovenia 1.21 1.26 1.21 1.21 1.20 1.25 1.26 1.32 1.38 1.5312 Greece n 1.27 1.25 1.27 1.29 1.31 n 1.38 1.42 1.5113 Czech 1.13 1.14 1.15 1.17 1.18 1.23 1.28 1.33 1.44 1.5014 Bulgaria n 1.27 1.24 1.21 1.23 1.29 1.31 1.38 1.42 1.4815 Lithuania 1.46 1.39 1.30 1.24 1.26 1.26 1.27 1.30 1.35 1.4716 Spain 1.20 1.23 1.24 1.26 1.31 1.33 1.35 1.36 1.40 1.46
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 31 of 281
R.3. Feasibility study
Nº State 1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
17 Cyprus 1.70 1.60 1.60 1.50 1.50 1.49 1.40 n 1.39 1.4618 Latvia 1.18 1.24 1.21 1.23 1.29 1.24 1.31 1.36 1.41 1.4519 Malta 1.72 1.69 1.50 1.46 1.48 1.37 1.37 1.40 1.37 1.4320 Austria 1.34 1.36 1.33 1.40 1.38 1.42 1.41 1.41 1.38 1.4121 Italy 1.23 1.26 1.25 1.27 1.29 1.33 1.32 1.35 1.37 1.4122 Poland 1.37 1.37 1.32 1.25 1.22 1.23 1.24 1.27 1.31 1.3923 Germany n 1.38 n n 1.30 1.40 1.30 1.34 1.37 1.3824 Portugal 1.51 1.56 1.46 1.47 1.44 1.40 1.41 1.36 1.34 1.3725 Hungary n 1.33 1.31 1.31 1.28 1.29 1.32 1.35 1.32 1.3526 Romania 1.30 1.30 1.20 1.30 1.30 1.30 1.30 1.31 1.29 1.3527 Slovakia 1.33 1.29 1.20 1.19 1.20 1.24 1.25 1.24 1.25 1.32
In comparison, in 2009 the highest number of births per 1000 inhabitants was in the counties of Vilnius (12.5) and Klaipeda (11.6), and the lowest – in the counties of Utena (8.6) and Panevezys (9.5).
4.1.3 MortalityIn 2009 42 thousand people died, it is 1.8 thousand less than in 2008. Last year there were 12.6 deaths per 1000 inhabitants and in 2008 – 13.1. Since 1950, the highest level of mortality was in 2007 – 13.5 deaths per1000 inhabitants.
The level of mortality is very different in different counties. In 2009 there were 16 and 13.8 deaths per 1000 inhabitants in the counties of Utena and Panevezys, and 11.6 and 11.8 deaths respectively in the counties of Klaipeda, Telsiai and Vilnius.
4.1.4 Population and main demographic indicators in the regionsAt the beginning of 2010 one fourth of the country’s inhabitants lived in Vilnius county, one fifth – in Kaunas county. The smallest counties were Taurage, Utena, Telsiai and Marijampole. In the last five years, the population has only increased in Vilnius county (0.2%). It has decreased in the other regions, especially in Utena (6.1%), Siauliai (5.3%), Alytus (5.2%), Taurage (5.1%) and Panevezys (4.8%).
In the table below, the population and the main demographic indicators of the counties are presented.
Table 5. Population and main demographic rates in the regions
Total
Population at the beginning of 2010
Per 1000 inhabitants in 2009
Born
Dead
Marriages
DivorcesThousand %
3329.0 100.011.
012.
6 6.2 2.8Alytus county 173.4 5.2 9.6 13.4 5.5 2.8Kaunas county 666.3 20.0 11.0 12.3 5.9 2.8
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 32 of 281
R.3. Feasibility study
Total
Population at the beginning of 2010
Per 1000 inhabitants in 2009
Born
Dead
Marriages
DivorcesThousand %
3329.0 100.011.
012.
6 6.2 2.8Klaipeda county 376.5 11.3 11.6 11.6 6.6 2.8Marijampole county 178.4 5.4 10.6 13.1 5.6 2.9Panevezys county 278,4 8,4 9,5 13,8 5,0 2,8Siauliai county 341,7 10,3 10,2 12,9 5,6 2,8Taurage county 124,8 3,8 9,9 13,5 5,7 2,8Telsiai county 171,1 5,1 10,6 11,8 5,3 2,7Utena county 168,1 5,0 8,6 16,0 5,5 2,8Vilnius county 850,3 25,5 12,5 11,8 7,4 2,8
4.1.5 Main demographic indicators in the Member States of the European Union
According to the preliminary data of Eurostat, at the beginning of 2010 501.3 million people lived in the European Union, i.e., 1.5 million more than a year ago. Last year the population increased in twenty Member States of the European Union and it decreased in the remaining ones – Bulgaria, Germany, Estonia, Latvia, Lithuania, Hungary and Romania.
In 2009 there were more births than deaths per 1000 inhabitants in eighteen Member States of the European Union. It mostly happened in Ireland (10), Cyprus (5.5) France (4.4). There were more deaths than births per 1000 inhabitants in nine Member States of the European Union: Bulgaria – 3.8, Hungary – 3.3, Latvia – 3.4, Germany – 2.3, Lithuania – 1.6, Romania – 1.4, Italy and Portugal – 0.5 in each, Estonia – 0.2. Negative net migration per 1000 inhabitants was only in seven Member states of the European Union: Ireland (-9.9), Lithuania (-4.6), Latvia (-2.1), Germany (-0.7), Poland (-0.4), Romania and Bulgaria (-0.1 in each).
In 2009 there were 10.8 births per 1000 inhabitants in the European Union. The level of natality was higher than the average of the European Union in seventeen Member States of the European Union. The highest number of births per 1000 inhabitants was in Ireland (16.8), France (12.9) and the United Kingdom (12.7), the lowest – in Germany (7.9), Italy, Austria and Portugal (9.2 in each).
In 2009 in Lithuania the number of deaths per 1000 inhabitants (12.6) exceeded the average of the European Union (9.6) 1.3 times but it was lower than in Latvia (13.3) and Hungary (13).
In the European Union men live to be 75.8 years and women – 82 years on the average (data of 2006). In Lithuania the average likely life expectancy of men is even 10 years shorter than the average of the European Union.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 33 of 281
R.3. Feasibility study
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 34 of 281
R.3. Feasibility study
4.2 Satisfaction of patientsIn this chapter there is a brief presentation of the results of the representative survey performed in February-March 2010. The survey was performed on the internet and 1048 women who had given a birth in 2007-2009 were interviewed.
The interview involved the questions about the services provided for women:► Prenatal;► Perinatal;► Neonatal.
CONCLUSIONS OF ASSESSING THE PRENATAL CARE
The results of the interview showed the biggest part of the interviewed delivering women were satisfied with the services provided by PHCI during their pregnancy (mean of assessment is 7.8 out of 10 points). The respondents are more satisfied with the services provided by private PHCI than by public PHCI.
During the pregnancy, the patients of public PHCI faced different problems related with the provided services more often than the patients of private PHCI (25%). Two main disadvantages – insufficient gynaecologic care and a perfunctory attitude of the doctor-gynaecologist – was indicated both for private and public PHCI. In the opinion of the respondents, one of the main disadvantages of private clinics and offices is the prices of services, whereas there is often a lack of information about the services provided in the public ones.
During the pregnancy, 77% women had enough information about the observation of the foetus position. The respondents were mostly lacking information about the methods of giving birth and risks during the birth.
CONCLUSIONS OF ASSESSING DELIVERY EXPERIENCE
The results of the survey showed that in 2007-2009 the main criterion when choosing PHCI by the delivering women was their dwelling-place (57%). This factor was especially important for the women who gave a birth in the district centres and other small towns (79%). The delivering women had to go 21 kilometres to PHCI on the average. When choosing PHCI, the recommendations of other women giving birth (32%) and a good reputation of the institution (30%) had a crucial influence for every third mother.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 35 of 281
R.3. Feasibility study
Picture Nº 2 – Choice of PHCI
Most (80%) delivering women were very satisfied with the provided services upon acceptance to PHCI. Every second delivering woman is very satisfied. The women who gave a birth in the district centres and small towns were more satisfied with the acceptance services. The women who were less satisfied wished for more pleasant communication, understanding (55%), and also expedition (19%) and information. Every tenth less-satisfied mother also indicated a lack of professionalism.
During the period of preparation for the birth, delivering women get the most comprehensive information about the foetus position and further preparation for the birth. The women preparing for the birth get the least information about the methods of anaesthesia (both with medicaments and without medicaments) and importance of the contact between a newborn and a mother in the course of two first hours. Lack of information about the methods of anaesthesia is more felt in PHCI of smaller towns and district centres.
Six out of ten (62%) interviewed delivering women gave birth naturally without any anaesthesia with medicaments. This approach is used in smaller towns and district centres much more frequently (84%).
Birth is given by applying epidural anaesthesia in cities and regional centres ten times more frequently (respectively 20% and 2%). This difference is also
CONFIDENTIAL document.docx
Dwelling-place
The recommendations of other women giving birth
The good reputation of the institution
Other
There was no other choice
Pregnancy, health complications
Personal self-determination
Previous experience of maternity home
I was brought in ambulance –not pursued
Pregnant women carried out the doctor's recommendation
Familiar, pre-agreed b doctor and his hospital

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 36 of 281
R.3. Feasibility study
reflected in the possibilities of choosing the methods of anaesthesia given by the institutions – every second delivering woman in PHCI of cities and regional centres was given a possibility to choose epidural anaesthesia (54%) and only every fifth delivering woman had a choice in the institutions of smaller towns (21%).The women tend to assess positively the competence and attentiveness of the staff participating during the birth, but it is to note that the attentiveness of the staff is assessed a little worse than their competence.
Picture Nº 3 – Assessment of competence and attentiveness of the birth staff
The obstetricians and neonatologists got the highest assessment in respect of their competence and attentiveness, the anaesthesiologists and nurses were assessed in these aspects relatively worse. The women giving birth in small towns have a better opinion about their obstetricians, anaesthesiologists and nurses than those giving birth in cities and county centres.
CONFIDENTIAL document.docx
Obstetrician
Doctor obstetrician
Neonatologist
Anaesthesiologist
Nurse
Competence
Attentiveness
Negative assesment
Positive assesment

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 37 of 281
R.3. Feasibility study
Actually, most delivering women were satisfied with the services provided during the birth, but they would like to get more information, explanations about processes taking place, more attention and care.
When assessing the satisfaction with the services provided by PHCI, the mothers were asked to assess the possibility of recommending this institution to their friend/ acquaintance. This rate is generalized by assessing the emotional and rational satisfaction with the institution and its services. A half of the interviewed mothers are very satisfied with PHCI and it is very likely they will recommend it. One third of the interviewed mothers assess the possibility of recommendations a little more reservedly but actually they are more satisfied.
The women giving birth in small towns are more likely to recommend and more satisfied with their PHCI. PHCI mostly lack attentiveness, care, information and professionalism. Professionalism and competence of the staff is indicated as the biggest advantage.
Assessments of the mothers giving birth in cities and smaller towns are different. There is a bigger lack of warmer attention and care in cities, but the competence and professionalism of the staff is praised. On the contrary, in smaller towns there is more joy related with attention and pleasant service, but lack of professionalism is more emphasized.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 38 of 281
R.3. Feasibility study
4.3 Analysis of the services provided by PHCI Depending on the possibilities of provided treatment, scope of work and quality indicators, all health care institutions providing obstetric and neonatologic treatment are divided into three levels2:
► First-level institutions – these are institutions performing the primary care for pregnant women;
► Second A-level institutions – these are institutions providing obstetric and neonatologic treatment of the secondary level, stage A;
► Second B-level institutions – these are institutions providing obstetric and neonatologic treatment of the secondary level, stage A and B;
► Third-level institutions – these are university hospitals providing obstetric and neonatologic treatment of the secondary and third level and performing the functions of perinatal centres.
Within the scope of the project, PHCI providing the services of levels IIA, IIB and/or III were analyzed.
In this chapter, a detailed analysis of the services provided by PHCI is presented.
Note: ► In order to ensure the correctness of the data provided by the
representatives of PHCI, the data presented by PHCI were verified against the data in SVEIDRA provided by the representatives of SPF.
► During the verification of the data provided by the representatives of PHCI it was notices that not all PHCI indicated in the questionnaires the services provided which were not paid by SPF, i.e. the services paid by the patients themselves. Therefore, in order to assess the scope of services provided by each PHCI, and not only of the services paid by SPF, the data contained in SVEIDRA was used for the analysis of the services provided by each PHCI including the scope of the services paid by the patients themselves.
2 Order Nº 117 by the Minister of Health of the Republic of Lithuania of 15 March 1999„ On the approval of the procedure for health care for pregnant women, delivering women and newborns“ (published in the Official Gazette, 26 March 1999, Nº : 28, Publ. Nº: 811)
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 39 of 281R.3. Feasibility study
In the picture below, there is a comparison of PHCI according to the scope of provided services.
4.3.1 Comparison of PHCI according to the scope of provided services
KMUK AGK KMUK NK VMUL AGK VUVL NK0
2000
4000
6000
8000
10000
12000
Comparison of PHCI according to the scope of provided services
200720082009
P.Mažylio gim
dymo...
Krikščio
niškieji
gimd...
Alytaus A
SPĮ
Marijam
polės ASPĮ
Telšių
ASPĮ
Taurag
ės ASPĮ
Utenos A
SPĮ
Trakų ASPĮ
Mažeikių
ASPĮ
Ukmerg
ės ASPĮ
Radviliškio
ASPĮ
Šilutės
ASPĮ
Visagino ASPĮ
Pasvalio
ASPĮ
Kėdainių ASPĮ
Jonavos A
SPĮ
Šalčin
inkų ASPĮ
Kretingos A
SPĮ
Lazdijų ASPĮ
Raseinių ASPĮ
Vilkavišk
io ASPĮ
Rokiškio raj
ono ASPĮ
Švenčio
nių ASPĮ
0
500
1000
1500
2000
2500
3000
3500 Comparison of PHCI according to the scope of provided services
200720082009
VULSKCF KUL Vilniaus gimdymo
namai
Kauno 2-ji KL
Šiaulių ASPĮ Panevėžio ASPĮ
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000Comparison of PHCI according to the scope of provided services
200720082009
Picture Nº 4 – Comparison of PHCI according to the scope of provided services
CONFIDENTIAL document.docx
KMUC COG
KMUC NC VCUH COG
VUCL NC
Tels
iai P
HCI
Chri
stia
n m
ater
nity
ho
me
Alyt
us P
HCI
Mar
ijam
pole
PH
CI
Taur
age
PHCI
Ute
na P
HCI
Trak
ai P
HCI
Maz
eiki
ai P
HCI
Keda
inia
i PH
CI
Visa
gina
s PH
CI
Radv
ilisk
is P
HCI
Silu
te P
HCI
Pasv
alys
PH
CI
Jona
va P
HCI
Ukm
erge
PH
CI
Salc
inin
kai P
HCI
Roki
skis
PH
CI
Kret
inga
PH
CI
Lazd
ijai P
HCI
Rase
inia
i PH
CI
Vilk
avis
kis
PHCI
Sven
cion
ys P
HCI
P. M
azyl
io m
ater
nity
ho
me
Pane
vezy
s PH
CI
Siau
liai
PHCI
Kaun
as
2nd
Viln
ius
mat
erni
ty
hom
e
KVL
VUH
SCCF

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 40 of 281
R.3. Feasibility study
4.3.2 3Comparison of PHCI according to the structure of the provided services
The perinatal centres in Vilnius and Kaunas are different according to the profile of the provided services. In 2009, in the clinic of obstetrics and gynaecology of VUCH, neonatology IIA made 18% of all the provided services, meanwhile the clinic of obstetrics and gynaecology of KMUC did not provide this kind of services at all in 2009.
In 2009, in the clinic of neonatology of KMUC, neonatology IIA made 56% of all the provided services, meanwhile the part of the provided services of neonatology IIA in the clinic of neonatology of VUCH made only 2%. In 2009, the part of the provided services of neonatology IIB in the clinic of neonatology of VUCH made 48% of all the services provided by the clinic of neonatology of VUCH, meanwhile the part of the provided services of neonatology IIB in the clinic of neonatology of KMUC made 18% of all the services provided by the clinic of neonatology of KMUC in 2009.
In the picture below, there is a comparison of the III-level PHCI and/or perinatal centres according to the structure of the provided services. Kaunas perinatal centre and Vilnius perinatal centre performance rates comparison is given in section 4.4.12.
3 Service provided by PHCI is a service provided to a pregnant woman, delivering woman or neonate paid to PHCI by SPF: Obstetrics I, Obstetrics II, Intensive therapy of neonates I, Intensive therapy of neonates II, Neonatology IIA, Neonatology IIB, Neonatology III, Pregnancy pathology I, Pregnancy pathology II, Pregnancy pathology III.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 41 of 281
R.3. Feasibility study
KMUC COG KMUC NC VCUH COG VUCL NC0
500
1,000
1,500
2,000
2,500
3,000
Comparison of PHCI according to the structure of the provided services
Obstetrics IObstetrics IINeonatal intensive care INeonatal intensive care IINeonatology IIANeonatology IIBNeonatology IIIPregnancy pathology IIAPregnancy pathology IIBPregnancy pathology III
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 42 of 281
R.3. Feasibility study
Picture Nº 5 – Comparison of the III-level PHCI and/or perinatal centres according to the structure of the provided services
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 43 of 281
R.3. Feasibility study
In the picture below, there is a comparison of the IIB-level PHCI according to the structure of the provided services.
VUHSCCF
KVL
Vilniu
s mat
ernity
hom
e
Kaunas
2nd C
H
Siaulia
i PHCI
Panev
ezys
PHCI0
500
1,000
1,500
2,000
2,500
3,000
3,500
Comparison of PHCI according to the scope of provided services
Obstetrics IObstetrics IINeonatal intensive care INeonatal intensive care IINeonatology IIANeonatology IIBNeonatology IIIPregnancy pathology IIAPregnancy pathology IIBPregnancy pathology III
Picture Nº 6 – comparison of the IIA- and IIB-level PHCI according to the structure of the provided services
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 44 of 281
R.3. Feasibility study
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 45 of 281
R.3. Feasibility study
In the picture below, there is a comparison of the IIA-level PHCI according to the structure of the provided services.
P.Mažy
lis m
atern
ity...
Christian
mate
rnity
...
Alytus P
HCI
Marija
mpole PHCI
Telsi
ai PHCI
Taura
ge PHCI
Utena P
HCI
Traka
i PHCI
Mazeik
iai PHCI
Ukmer
ge PHCI
Radvil
iskis
PHCI
Silute
PHCI
Visagin
as PHCI
Pasva
lys PHCI
Kedain
iai PHCI
Jonava P
HCI
Salci
ninkai P
HCI
Kretinga
PHCI
Lazdija
i PHCI
Rasein
iai PHCI
Vilkav
iskis
PHCI
Rokiskis
distric
t rajo
...
Sven
cionys
PHCI0
200
400
600
800
1,000
1,200
1,400Comparison of the IIA -level PHCI according to the structure of
the provided services
Ob-stetrics IOb-stetrics IINeona-tology IIA
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 46 of 281
R.3. Feasibility study
Picture Nº 7 – comparison of the IIA -level PHCI according to the structure of the provided services4.3.3 Structure of all the services provided by PHCI in 2007, 2008 and 2009 In 2007 – 2009:
► Obstetrics of level I and II increased by 11% and 15% respectively;► Newborn intensive therapy of level I and II PHCI increased by 27% and 35%, respectively;► Neonatology of level IIA, IIB and III increased by 16%, 2% and 20%, respectively;► Pregnancy pathology of level IIA decreased by 9%;► Pregnancy pathology of level IIB and III increased by 26% and 45%, respectively.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 47 of 281
R.3. Feasibility study
Obst
etrics
I
Obst
etrics
II
Neo
natal
inte
nsive
car
e I
Neo
natal
inte
nsive
car
e II
Neo
natolo
gy II
A
Neo
natolo
gy II
B
Neo
natolo
gy II
I
Pregn
ancy
pat
hology
IIA
Pregn
ancy
pat
hology
IIB
Pregn
ancy
pat
hology
III
0
5,000
10,000
15,000
20,000
25,000
Structure of all the services provided by PHCI in 2007, 2008 and 2009
Picture Nº 8 – Structure of all the services provided by PHCI in 2007, 2008 and 2009
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 48 of 281
R.3. Feasibility study
4.3.4 Conclusions of the analysis of the services provided by PHCI After performing the analysis of the services provided by PHCI, we determined/observed the following:
► In the period of 2007-2009 the scope of the services provided by PHCI increased by 8%. A growth in the number of births may have had the biggest influence on that growth. There is some risk that because of this tendency the representatives of PHCI may have made not completely right decisions related with a demand for the staff, medical equipment and staff training considering their increased load of work and forecasting its growth in the future. In order to avoid these circumstances, needs for the staff, medical equipment and staff training were reviewed by the doctors-experts, docent dr. Mindaugas Kliucinskas and dr. Antanas Puzas. The decisions made by the representatives of PHCI regarding the staff, medical equipment and staff training were adjusted according to the services provided by PHCI, available staff, available medical equipment and other information collected during the visits to PHCI;
► In 2007-2009 a significant growth in the higher-level services is seen (Newborn intensive therapy I – 27%; newborn intensive therapy II – 35%; neonatology IIA – 16%; neonatology III – 20%; pregnancy pathology IIB - 26%; pregnancy pathology III – 45%). This growth could be affected by better diagnostic techniques and equipment, and possibly PHCI seeking to resolve their financial problems by improperly providing a higher level of service. Problems in this area has not been the subject of a feasibility study, so in order to optimize patient treatment, possibly to be addressed PHCI funding issues, which would require additional large-scale analysis;
► The information received when visiting PHCI revealed a tendency of PHCI providing the IIA-level services to provide the services of a higher level than it is indicated in the Order about the possibility to reach a necessary number of births ensuring the succession of the activity of PHCI and payment by NPF for pregnant women care and treatment of newborns;
► The clinic of neonatology of KMUC provided 238% more services than the clinic of neonatology of VUCH provided in total in 2007, 2008 and 2009;
► P. Mazylio maternity home and Christian maternity home are different from the other PHCI providing the IIA-level services by the scope of the provided services: in 2007, 2008 and 2009 they provided 220% and 179% more services respectively than an average PHCI providing the IIA-level services.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 49 of 281
R.3. Feasibility study
4.4 Analysis of activity scope and human resources of PHCI and their prospects
4.4.1 Comparison of PHCI according to the number of births per employee
In the period 2007-2009 the number of births per employee:► Increased in 25 PHCI. This number makes 81% of all PHCI.► Decreased in 5 PHCI. This number makes 16% of all PHCI.► Stayed the same in 1 PHCI. It makes 3% of all PHCI.
The average number of births in the III-level PHCI providing obstetric gynaecologic services per employee was 22 births in the period 2007 – 2009. The average number of births in the IIB-level PHCI providing obstetric gynaecologic services per employee was 26 births in the period 2007 – 2009. The average number of births in the IIA-level PHCI providing obstetric gynaecologic services per employee was 16 births in the period 2007 – 2009.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 50 of 281R.3. Feasibility study
In the picture below, the comparison of PHCI according to the number of births per employee is presented.
KMUC COG VCUH COG0
5
10
15
20
25
30
R.1. Number of births per employee
200720082009
P.Mazylio mate
rnity home
Christian mate
rnity home
Alytus PHCI
Marijam
pole PHCI
Telsiai P
HCI
Taurag
e PHCI
Utena P
HCI
Trakai
PHCI
Mazeikia
i PHCI
Ukmerg
e PHCI
Radviliskis
PHCI
Silute P
HCI
Visaginas P
HCI
Pasvalys
PHCI
Kedainiai P
HCI
Jonava PHCI
Salcininkai
PHCI
Kretinga P
HCI
Lazdijai
PHCI
Raseiniai P
HCI
Vilkavisk
is PHCI
Rokiskis d
istrict P
HCI
Svencionys P
HCI
0
4
8
12
16
20
24
R.1. Number of births per doctor in 2007, 2008 and 2009
200720082009
VUHSCCF KUH
Vilnius maternity h
omeKaunas 2
nd CHSiau
liai PHCI
Panevezys P
HCI
05
1015202530354045
R.1. Number of births per employee
200720082009
Picture No 9 – Number of births per doctor in 2007, 2008 and 2009
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 51 of 281R.3. Feasibility study
4.4.2 Comparison of PHCI according to the number of births per obstetrician-gynaecologistIn the period 2007-2009 the number of births per employee:
► Increased in 25 PHCI. This number makes 81% of all PHCI.► Decreased in 5 PHCI. This number makes 16% of all PHCI.► Stayed the same in 1 PHCI. It makes 3% of all PHCI.
The average number of births in the III-level PHCI providing obstetric gynaecologic services per obstetrician-gynaecologist was 82 births in the period 2007 – 2009. The average number of births in the IIB-level PHCI providing obstetric gynaecologic services per obstetrician-gynaecologist was 143 births in the period 2007 – 2009. The average number of births in the IIA-level PHCI providing obstetric gynaecologic services per obstetrician-gynaecologist was 58 births in the period 2007 – 2009.
KMUC COG VCUH COG0
20
40
60
80
100
120
140
R.2. Comparison of PHCI according to the number of births per obstetrician-gynaecologist
200720082009
P.Mazy
lio maternity
home
Christian mate
rnity home
Alytus P
HCI
Marijam
pole PHCI
Telsia
i PHCI
Taurag
e PHCI
Utena P
HCI
Trakai
PHCI
Mazeikia
i PHCI
Ukmerg
e PHCI
Radviliski
s PHCI
Silute P
HCI
Visagin
as PHCI
Pasvaly
s PHCI
Kedainiai
PHCI
Jonava PHCI
Salcin
inkai PHCI
Kretinga
PHCI
Lazdijai
PHCI
Raseiniai
PHCI
Vilkavis
kis PHCI
Rokiskis
district
PHCI
Svencio
nys PHCI
0
20
40
60
80
100
120
R.2. Comparison of PHCI according to the number of births per obstetrician-gynaecologist
200720082009
VUHSCCF KUH
Vilnius mate
rnity home
Kaunas 2nd CH
Siauliai
PHCI
Panevezys
PHCI
050
100150200250300350400
R.2. Comparison of PHCI according to the number of births per obstetrician-gynaecologist
200720082009
Picture No 10 – Number of births per obstetrician-gynaecologist in 2007, 2008 and 2009
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 52 of 281R.3. Feasibility study
4.4.3 Comparison of the number of staff of PHCI according to ageIn 22 PHCI (67% of all PHCI) most employees were 35 - 45 years old. In four PHCI (12% of all PHCI) most employees were 55 - 60 years old. In the remaining seven PHCI (21% of all PHCI) most employees belonged to several age ranges. These 21% fall in the range from 25 to 60.
KMUC COG KMUC NC VCUH COG VUCL NC0
20
40
60
80
100
120
140
160
180
R.3. Comparison of the number of staff of PHCI according to age
up to 25up to 35up to 45up to 50up to 55up to 60up to 65up to 70up to 100
P.Mazy
lio maternity
home
Alytus P
HCI
Telsiai
PHCI
Utena P
HCI
Mazeikia
i PHCI
Radviliskis
PHCI
Visagin
as PHCI
Kedainiai
PHCI
Salcin
inkai PHCI
Lazdijai
PHCI
Vilkavis
kis PHCI
Svencio
nys PHCI
05
10152025303540
R.3. Comparison of the number of staff of PHCI according to age
up to 25up to 35up to 45up to 50up to 55up to 60up to 65up to 70up to 100
VUHSCCF KUH
Vilnius mater
nity home
Kaunas 2nd CH
Siauliai
PHCI
Panevezys
PHCI
0
10
20
30
40
50
60
R.3. Comparison of the number of staff of PHCI according to age
up to 25up to 35up to 45up to 50up to 55up to 60up to 65up to 70up to 100
Picture No 11 – Number of staff according to the age4
4 Data differing most from the mean was clarified with PHCI representatives by telephone; PHCI representatives confirmed the data correctness.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 53 of 281R.3. Feasibility study
4.4.4 Comparison of PHCI according to the part of staff on secondary jobs According to the presented tables, only 4 per cent of employees of PHCI providing the third level or IIB-level obstetric-gynaecologic services are on secondary jobs. On the average, 26 per cent of employees of PHCI providing the IIA-level obstetric-gynaecologic services are on secondary jobs.
KMUC COG KMUC NC VCUH COG VUCL NC0
1
2
3
4
5
6
7
8
R.4. Comparison of PHCI according to the part of staff on secondary jobs (perc.)
2010
P.Mazylio mate
rnity home
Christian mate
rnity home
Alytus P
HCI
Marijam
pole PHCI
Telsiai
PHCI
Taurag
e PHCI
Utena P
HCI
Trakai
PHCI
Mazeikia
i PHCI
Ukmerg
e PHCI
Radviliskis
PHCI
Silute P
HCI
Visaginas P
HCI
Pasvaly
s PHCI
Kedainiai
PHCI
Jonava PHCI
Salcin
inkai PHCI
Kretinga
PHCI
Lazdijai
PHCI
Raseiniai
PHCI
Vilkavisk
is PHCI
Rokiskis d
istrict
PHCI
Svencio
nys PHCI
0
10
20
30
40
50
60
R.4. Comparison of PHCI according to the part of staff on secondary jobs (perc.)
2010
More than half of doctors arrives from Kaunas
The indicator differs from others because only 146 women give birth at the hospital. It is not expedient to have a large number of personnel holding key positions.
VUHSCCF KUH
Vilnius mate
rnity home
Kaunas 2nd CH
Siauliai
PHCI
Panevezys
PHCI
0
2
4
6
8
10
12
R.4. Comparison of PHCI according to the part of staff on secondary jobs (perc.)
2010
Picture No 12 – Percentage of staff on secondary jobs in 2010
CONFIDENTIAL document.docx
Nearly half of doctors arrives from Vilnius

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 54 of 281R.3. Feasibility study
4.4.5 Comparison of PHCI according to the structure of staff in 2010In six PHCI (18% of all PHCI) children’s nurses make the major part of staff. In seventeen PHCI (52% of all PHCI) obstetricians make the major part of staff. In four PHCI ( 12% of all PHCI) obstetricians-gynaecologists make the major part of staff. In four PHCI (12% of all PHCI) doctors of children’s diseases (paediatricians) make the major part of staff. In two PHCI (6% of all PHCI) specialists of different qualifications make the major part of staff.
KMUC COG KMUC NC VCUH COG VUCL NC0
20
40
60
80
100
120
140
Nurse assistantChildren's nurse (sister med.)ObstetricianThe doctor neonatologistThe doctor obstetrician gynecol-ogistChildren's diseases physician (pediatrician)
P.Mazylio mat..
.
Christian mat..
.
Alytus PHCI
Marijam
pol...
Telsiai P
HCI
Taurag
e ...
Utena P
HCI
Trakai
PHCI
Mazeikia
i ...
Ukmerg
e ...
Radviliskis
...
Silute P
HCI
Visaginas .
..
Pasvalys
...
Kedainiai .
..
Jonava PHCI
Salcininkai
...
Kretinga .
..
Lazdijai
PHCI
Raseiniai .
..
Vilkavisk
is ...
Rokiskis d
istr...
Svencionys..
.
0
5
10
15
20
25
Nurse assistant
Chil-dren's nurse (sister med.)
Obste-trician
The doc-tor neona-tologist
VUHSCCF KUH Vilnius maternity
home
Kaunas 2nd CH
Siauliai PHCI
Panevezys PHCI
0
10
20
30
40
50
60
Nurse assistantChildren's nurse (sister med.)ObstetricianThe doctor neonatologistThe doctor obstetrician gynecol-ogistChildren's diseases physician (pediatrician)
Picture No 13 – Structure of staff of all PHCI in 2010
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 55 of 281R.3. Feasibility study
4.4.6 Comparison of PHCI according to the number of births per delivery roomIn the period 2007-2009 the number of births per delivery room:
► Increased in 24 PHCI. This number makes 77% of all PHCI.► Decreased in 5 PHCI. This number makes 16% of all PHCI.► Stayed the same in 2 PHCI. It makes 7% of all PHCI.
The average number of births in the III-level PHCI providing obstetric gynaecologic services per delivery room was 476 births in the period 2007 – 2009. The average number of births in the IIB-level PHCI providing obstetric gynaecologic services per delivery room was 317 births in the period 2007 – 2009. The average number of births in the IIA-level PHCI providing obstetric gynaecologic services per delivery room was 182 births in the period 2007 – 2009.
KMUC COG VCUH COG0
100
200
300
400
500
600
R.6. Comparison of PHCI according to the number of births per delivery room
200720082009
P.Mazy
lio maternity
home
Christian mate
rnity home
Alytus P
HCI
Marijam
pole PHCI
Telsia
i PHCI
Taurag
e PHCI
Utena P
HCI
Trakai
PHCI
Mazeikia
i PHCI
Ukmerg
e PHCI
Radviliski
s PHCI
Silute P
HCI
Visagin
as PHCI
Pasvaly
s PHCI
Kedainiai
PHCI
Jonava PHCI
Salcin
inkai PHCI
Kretinga
PHCI
Lazdijai
PHCI
Raseiniai
PHCI
Vilkavis
kis PHCI
Rokiskis
district
PHCI
Svencio
nys PHCI
0
100
200
300
400
500
600
R.6. Comparison of PHCI according to the number of births per delivery room
200720082009
VUHSCCF KUH
Vilnius mate
rnity home
Kaunas 2nd CH
Siauliai
PHCI
Panevezys
PHCI
0
100
200
300
400
500
600
R.6. Comparison of PHCI according to the number of births per delivery room
200720082009
Picture No 14 – Number of births per delivery room in 2007, 2008 and 2009
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 56 of 281R.3. Feasibility study
4.4.7 Comparison of PHCI according to the bed turnover rateIn 2009 the bed turnover rate showing the number of patients per bed in the IIA and B-level PHCI was similar and it was 64 and 66, respectively. In the third level PHCI it was 41, i.e., half as low again as in the IIA and B-level PHCI.
KMUC COG KMUC NC VCUH COG VUCL NC0
10
20
30
40
50
60
70
R.7. Comparison of PHCI according to the bed turnover rate
2009
P.Mazy
lio mate...
Christian mate
r...
Alytus P
HCI
Marijam
pole ...
Telsia
i PHCI
Taurag
e PHCI
Utena P
HCI
Trakai
PHCI
Mazeikia
i PHCI
Ukmerg
e PHCI
Radviliski
s ...
Silute P
HCI
Visagin
as PHCI
Pasvaly
s PHCI
Kedainiai
PHCI
Jonava PHCI
Salcin
inkai ...
Kretinga
PHCI
Lazdijai
PHCI
Raseiniai
PHCI
Vilkavis
kis ...
Rokiskis
distri...
Svencio
nys ...
0
20
40
60
80
100
120 R.7. Comparison of PHCI according to the bed turnover rate
VUHSCCF KUH
Vilnius mater
n...
Kaunas 2-n...
Siauliai
PHCI
Panevezys
...
0
20
40
60
80
100
120
R.7. Comparison of PHCI according to the bed turnover rate
2009
Picture No 15 – Bed turnover rate in 2009
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 57 of 281R.3. Feasibility study
4.4.8 Comparison of PHCI according to the number of bed days per patientIn the period 2007-2009 the number of bed days per patient:
► Increased in 14 PHCI. This number makes 42% of all PHCI;► Decreased in 19 PHCI. This number makes 58% of all PHCI.
The average number of bed days in the III-level PHCI providing obstetric gynaecologic services per patient was 7 days in the period 2007 – 2009. The average number of bed days in the IIB-level PHCI providing obstetric gynaecologic services per patient was 4 days in the period 2007 – 2009. The average number of bed days in the IIA-level PHCI providing obstetric gynaecologic services per patient was 4 days in the period 2007 – 2009.
KMUC COG KMUC NC VCUH COG VUCL NC0
2
4
6
8
10
12
14
16
18
R.9. Comparison of PHCI according to the number of bed days per patient
200720082009
P.Mazylio mate
rnity home
Christian mate
rnity home
Alytus P
HCI
Marijam
pole PHCI
Telsiai
PHCI
Taurag
e PHCI
Utena P
HCI
Trakai
PHCI
Mazeikia
i PHCI
Ukmerg
e PHCI
Radviliskis
PHCI
Silute P
HCI
Visaginas P
HCI
Pasvaly
s PHCI
Kedainiai
PHCI
Jonava PHCI
Salcin
inkai PHCI
Kretinga
PHCI
Lazdijai
PHCI
Raseiniai
PHCI
Vilkavisk
is PHCI
Rokiskis d
istrict
PHCI
Svencio
nys PHCI
0123456789
R.9. Comparison of PHCI according to the number of bed days per patient
200720082009
VUHSCCF KUH
Vilnius mate
rnity home
Kaunas 2nd CH
Siauliai
PHCI
Panevezys
PHCI
0
1
2
3
4
5
6
R.9. Comparison of PHCI according to the number of bed days per patient
200720082009
Picture No 16 – Number of bed days per patient in 2007, 2008 and 2009
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 58 of 281R.3. Feasibility study
4.4.9 Comparison of PHCI according to the rate of Caesarean sections from all births in PHCIIn the period 2007 – 2009 the rate of Caesarean sections from all births:
► Increased in 19 PHCI. This number makes 61% of all PHCI.► Decreased in 9 PHCI. This number makes 29% of all PHCI.► Stayed the same in 3 PHCI. This number makes 10% of all PHCI
The increase in the rate of Caesarean sections is largely influenced by the conviction of the society that this termination of pregnancy ensures successful outcome of pregnancy and constant and still increasing fear of doctors related with legal consequences. Meanwhile, a lot of scientific research has proven that Caesarean sections do not have any positive influence on the successful outcome of pregnancy5.The average rate of Caesarean sections in the III-level PHCI providing obstetric gynaecologic services was 28% of all births in the period 2007 – 2009. The average rate of Caesarean sections in the IIB-level PHCI providing obstetric gynaecologic services was 25% of all births in the period 2007 – 2009. The average rate of Caesarean sections in the IIA-level PHCI providing obstetric gynaecologic services was 19% of all births in the period 2007 – 2009.
KMUC COG VCUH COG0%
5%
10%
15%
20%
25%
30%
35%
R.11. Comparison of PHCI according to the rate of Caesarean sections from all births in PHCI
200720082009
P.Mazy
lio m
aternity
home
Christian
mate
rnity home
Alytus P
HCI
Marijam
pole PHCI
Telsia
i PHCI
Taurag
e PHCI
Utena P
HCI
Trakai
PHCI
Mazeikia
i PHCI
Ukmerg
e PHCI
Radvili
skis P
HCI
Silute
PHCI
Visagin
as PHCI
Pasvaly
s PHCI
Kedain
iai PHCI
Jonava PHCI
Salcin
inkai PHCI
Kretinga
PHCI
Lazdijai
PHCI
Raseiniai
PHCI
Vilkavis
kis PHCI
Rokiskis
district
PHCI
Svencio
nys PHCI
0%
5%
10%
15%
20%
25%
30%
35%
R.11. Comparison of PHCI according to the rate of Caesarean sections from all births in PHCI
200720082009
VUHSCCF
KUH
Vilnius m
aternity
home
Kaunas
2nd CH
Siauliai
PHCI
Paneve
zys PHCI
0%
5%
10%
15%
20%
25%
30%
R.11. Comparison of PHCI according to the rate of Caesarean sections from all births in PHCI
200920082009
Picture No 17 – Percentage of Caesarean sections from all births in 2007, 2008 and 20095 Yearly report of the National Health Council „Health care of pregnant women, delivering women and neonates“, R. Nadišauskienė, M. Minkauskienė, E. Markūnienė, A. Armonavičienė, N. Drazdienė, 2005
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 59 of 281R.3. Feasibility study
4.4.10 Comparison of PHCI according to the rate of births per administrative unit In the period 2007-2009 the rate of births per administrative unit (district and/or city):
► Increased in 14 PHCI. This number makes 45% of all PHCI.► Decreased in 15 PHCI. This number makes 48% of all PHCI.► Stayed the same in 2 PHCI. This number makes 7% of all PHCI
The average rate of births in the III-level PHCI providing obstetric gynaecologic services per administrative unit was 63% births in the period 2007 – 2009. The average rate of births in the IIB-level PHCI providing obstetric gynaecologic services per administrative unit was 60% births in the period 2007 – 2009. The average rate of births in the III-level PHCI providing obstetric gynaecologic services per administrative unit was 68% births in the period 2007 – 2009.
KMUC COG VCUH COG0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
R.14. Comparison of PHCI according to the rate of births per administrative unit
200720082009
P.Mazy
lio maternity
home
Christian mate
rnity home
Alytus P
HCI
Marijam
pole PHCI
Telsia
i PHCI
Taurag
e PHCI
Utena P
HCI
Trakai
PHCI
Mazeikia
i PHCI
Ukmerg
e PHCI
Radviliskis
PHCI
Silute P
HCI
Visagin
as PHCI
Pasvaly
s PHCI
Kedainiai
PHCI
Jonava PHCI
Salcin
inkai PHCI
Kretinga
PHCI
Lazdijai
PHCI
Raseiniai
PHCI
Vilkavis
kis PHCI
Rokiskis d
istrict
PHCI
Svencio
nys PHCI
0%20%40%60%80%
100%120%140%160%180%200%
R.14. Comparison of PHCI according to the rate of births per administrative unit
200720082009
VUHSCCF KUH
Vilnius mate
rnity home
Kaunas 2nd CH
Siauliai
PHCI
Panevezys
PHCI
0%
20%
40%
60%
80%
100%
120%
140%
R.14. Comparison of PHCI according to the rate of births per administrative unit
200720082009
Picture No 18 – Percentage of births in PHCI per administrative unit 2007, 2008 and 2009
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 60 of 281
R.3. Feasibility study
4.4.11 General comparison of all PHCI of Vilnius and Kaunas according to the rate of births per administrative unit
The rate of all births in PHCI in the administrative unit of Kaunas in 2007-2009 exceeded the rate of all births in PHCI in the administrative unit of Vilnius in 2007-2009 on the average 1.7 times.
In the picture below, the rate of all births in PHCI of Vilnius and all births of PHCI of Kaunas per administrative unit (district and/or city) in 2007 – 2009 is presented.
All PHCI of Kaunas All PHCI of Vilnius0%
20%
40%
60%
80%
100%
120%
140%
160%
180%
General comparison of all PHCI of Vilnius and all PHCI of Kaunas according to the rate of births per administrative unit
Picture No 19 – General comparison of all PHCI of Vilnius and all PHCI of Kaunas
according to the rate of births per administrative unit
4.4.12 Comparison of total rates of perinatal centres in Vilnius and Kaunas
Currently, Kaunas perinatology centre consists of KMUC COG, where obstetrics services are provided and KMUK NK, where neonatology services are provided. KMUC COG and KMUC NC are located nearby, in the same building. Vilnius perinatology centre consists of VUCH where neonatology services are provided and VCUH COG providing obstetrics services and emergency aid to neonates who are transferred to VCUH when their state is stabilized. VUCH and VCUH are situated in separate districts of Vilnius city.
Comparison of indicators
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 61 of 281
R.3. Feasibility study
In order to objectively compare the services provided by perinatal centres, the indicators of hospitals making perinatal centres were summed up. The rates of Kaunas perinatal centre involve the hospitals KMUC COG and KMUC NC. The rates of Vilnius perinatal centre involve the hospitals VMUH COG and VUCH. In the table below, the indicators of comparison of perinatal centres are presented:
Table 6. The indicators of comparison of perinatal centres
No IndicatorKaunas
perinatal centre
Vilnius perinatal
centre1. Number of births 3,634 3,8282. Number of delivery rooms 7 83. Number of patients 10,156 5,9744. Number of staff 286 262
- Obstetrician 84 63- Neonatologist 26 38- Obstetrician-gynaecologist 55 41- Children’s nurse (nurse) 121 104- Assistant nurse - 16
5. Bed turnover rate 55.8 29.36. Number of bed days per patient 5.21 6.757. Extent of provided services (2009) 11,127 11,341
-Obstetrics I 2,311 2,864-Obstetrics II 2,063 2,520-Neonatal intensive therapy I 245 305-Neonatal intensive therapy II 340 399-Neonatology IIA 2,707 1,860-Neonatology IIB 870 1,371-Neonatology III 683 528-Pregnancy pathology IIA 1,355 1,479-Pregnancy pathology IIB 456 6-Pregnancy pathology III 97 9
While comparing the rates of the perinatal centres, it is apparent that they are mostly very similar. It seems understandable considering the similar number of births. Bigger differences are seen when comparing:
► Number of patients. 59 % more patients came to Kaunas perinatal centre than to Vilnius perinatal centre in 2009. This difference is mostly influenced by the fact that 77% less patients were accepted to VUCH than to KMUC NC. It can be explained by the fact that KMUC NC is located in the same building as KMUC COG and in case a sick neonate is born, he/she is immediately taken. The second reason is that Kaunas perinatal centre serves a bigger part of Lithuania compared to Vilnius perinatal centre (see Appendix No 5 of Order No 117 of the Minister of Health of the Republic of Lithuania on the 15th of March 1999).
► Number of staff. 8% more specialists work at Kaunas perinatal centre than in Vilnius. This difference is mostly influenced by the fact that 33% more specialists work in the field of obstetric in Kaunas than in Vilnius. A bigger
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 62 of 281
R.3. Feasibility study
number of obstetric staff can also be explained by the fact that Kaunas has given more pregnancy pathology services.
► Bed turnover rate. This rate is 48 % higher in Kaunas than in Vilnius. This difference seems understandable considering the fact that this number shows the number of patients per bed. If the number of beds is similar, the number of patients was 59% higher in Kaunas.
4.5 Demand for staffIn this chapter the present situation of staff of PHCI and demand for it in the nearest period is reviewed. Most PHCI indicated that the present number of staff was optimal, but some PHCI took into consideration the increasing scope of services, busyness of staff and lack of employees with specific knowledge (for example, psychologists) and indicated that they had demand for establishment of new positions of employees.
The presently analyzed PHCI have 1,665 positions of this kind:► Obstetricians (about 585);► Children’s nurses (nurses) (about 524);► Obstetricians-gynaecologists (about 344);► Neonatologists (about 173);► Other (operating room nurses, children’s neurologists, ophthalmologists,
doctors’ assistants), (about 39).
KMUC NC, providing the III-level services, has demand for a 0.75 position neonatologist and 32 trained nurses (nurses) whose work would decrease the load of neonatologists working for this PHCI. Presently 31,25 neonatologists work for KMUC NC and they provided 4.1516 neonatal services in 2009 (Neonatology IIA, Neonatology IIB and Neonatology III), meanwhile, 25 neonatologists work for VUCH NC and they provided 1.132 neonatal services in 2009.
According to the data of 2009, one neonatologist of KMUC NC provided 133 neonatal services on the average; meanwhile, according to the data of 2009, one neonatologist of VUCH NC provided 45 neonatal services on the average. In order to evaluate the efficiency indicators more objectively, it is necessary to compare the indictors of perinatology centres presented in section 4.5.1. “Comparison of Vilnius and Kaunas perinatology centres”.
6 Data provided by PHCI
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 63 of 281
R.3. Feasibility study
In the picture below, comparison of PHCI providing the III-level obstetric-gynaecological services according to the demand for staff is provided.
KMUC COG KMUC NC VCUH COG VUCL NC0
50
100
150
200
250
Comparison of PHCI according to the demand for staff
Picture No 20 – Comparison of PHCI according to the demand for staff
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 64 of 281
R.3. Feasibility study
Kaunas 2nd clinical hospital has a demand for one more neonatologist, three nurses and two assistant nurses in 2011. In contrast to Kaunas 2nd clinical hospital, Vilnius maternity home took into account the decreasing scope of provided services and indicated that they needed fewer positions this year: 37 obstetricians (instead of 37.5), two positions less neonatologists and 4.25 positions less nurses.
In the picture below, a comparison of PHCI providing the IIA and IIB-level obstetric-gynaecological services according to the demand for staff is presented.
VUHSCCF
KUH
Vilnius m
atern
ity home
Kaunas
2nd CH
Siaulia
i PHCI
Panev
ezys P
HCI0
20
40
60
80
100
120
140
160Comparison of PHCI according to the demand for staff
Picture No 21 – Comparison of PHCI according to the demand for staff
CONFIDENTIAL document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 65 of 281R.3. Feasibility study
Seven from of 23 analyzed PHCI providing the IIA-level services think that their amount number of staff is optimal and they do not have any demand for extra positions in the nearest future. Meanwhile, 16 other PHCI think that in 2011 they need to have 51 positions more than (see picture below).
In the picture below, a comparison of PHCI providing the IIA-level obstetric-gynaecological services according to the demand for staff is presented.
P.Mazylio maternity...
Alytus PHCI
Telsiai PHCI
Utena PHCI
Mazeikiai PHCI
Radviliskis PHCI
Visaginas PHCI
Kedainiai PHCI
Salcininkai PHCI
Lazdijai PHCI
Vilkaviskis PHCI
Svencionys PHCI
0
10
20
30
40
50
60
70
80 Comparison of PHCI according to the demand for staffMarijampole PHCI indicated a significantly higher demand for personnel in 2010 and 2011 than the current number of personnel at PHCI, whereas the number of births per PHCI employee according to the data of 2007, 2008 and 2009 was 9.08 on average. Also, in 2007, 2008 and 2009 there was no significant growth of this indicator.
Taurage PHCI indicated a significantly higher demand for personnel in 2010 and 2011 than the current number of personnel at PHCI, whereas the number of births per PHCI employee according to the data of 2007, 2008 and 2009 was 15.4 on average. From 2007 to 2009 the number of births per one employee of Taurage PHCI increased by 12%.
Silute PHCI indicated a significantly higher demand for personnel in 2010 and 2011 than the current number of personnel at PHCI, whereas the number of births per PHCI employee according to the data of 2007, 2008 and 2009 was 14,39 on average. From 2007 to 2009 the number of births per one employee of Taurage PHCI decreased by 17 %.
Kretinga PHCI indicated a significantly higher demand for personnel in 2010 and 2011 than the current num-ber of person-nel at PHCI, whereas the number of births per PHCI employee according to the data of 2007, 2008 and 2009 was 10.47 on aver-age. From 2007 to 2009 the number of births per one employee of Kretinga PHCI increased by 31%.
Picture No 22 – Comparison of PHCI according to the demand for staff
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 66 of 281
R.3. Feasibility study
4.6 Staff forecastsConsidering the need for staff until 2011 presented by PHCI and the common tendency of decrease in the Lithuanian population, a possible number of births in each PHCI and the need for staff every year within the period of 2010-2015 was analyzed. While performing assessments, the following presumptions and data sources used:
Data sources► Forecast of the population until 2015 announced by the organization Global
Insight;► Number of births until 2008 announced by the Department of Statistics of
Lithuania;
Presumptions► The number of births in 2008 per 1000 inhabitants is going to stay the same
until 2015;► The distribution of the number of births in PHCI in 2009 (birth percentage) is
not going to change until 2015 and it is going to depend on the common tendency of births in Lithuania;
► The tendency of the number of newborns provided with the neonatal service in neonatal clinics is going to coincide with the tendency of the number of births.
According to the forecast of the number of births by Global Insight and the rate of the number of births per 1000 inhabitants in 2008, a possible tendency of the number of births until 2015 was assessed which showed the number of births will probably decrease along with the decrease in the population.
Table 7. Forecast of the population and number of births in Lithuania Rate 2008 2009 2010p 2011p 2012p 2013p 2014p 2015pPopulation 3,366,692 3,348,619 3,327,008 3,293,838 3,260,884 3,248,501 3,216,669 3,185,272Number of births 34,779 34,592 34,369 34,026 33,686 33,558 33,229 32,905
According to the number of births in 2009, the part of the number of births per each PHCI (distribution) was assessed. When using this rate and the total number of births, a possible number of births per each PHCI until 2015 was assessed.
Table 8. Forecast of the number of births per PHCI
Name of PHCI 2008 20092010p
2011p
2012p
2013p
2014p
2015p
III-level PHCIKMUC COG 3,608 3,634 3,611 3,575 3,539 3,525 3,491 3,457VMUH COG 3,105 3,828 3,803 3,765 3,728 3,714 3,677 3,641IIB-level PHCIVULSKCF 1,530 1,514 1,504 1,489 1,474 1,469 1,454 1,440
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 67 of 281
R.3. Feasibility study
Name of PHCI 2008 20092010p
2011p
2012p
2013p
2014p
2015p
KUH 3,701 3,793 3,769 3,731 3,694 3,680 3,644 3,608Vilnius maternity home 3,434 3,297 3,276 3,243 3,211 3,198 3,167 3,136Kaunas II clinical hospital 1,281 1,493 1,483 1,469 1,454 1,448 1,434 1,420Siauliai PHCI 2,108 2,168 2,154 2,133 2,111 2,103 2,083 2,062Panevezys PHCI 1,436 1,592 1,582 1,566 1,550 1,544 1,529 1,514IIA-level PHCIP.Mazylio maternity home 1,322 1,268 1,260 1,247 1,235 1,230 1,218 1,206Christian maternity home 992 1,021 1,014 1,004 994 990 981 971Alytus PHCI 644 784 779 771 763 761 753 746Marijampole PHCI 555 569 565 560 554 552 547 541Telsiai PHCI 477 429 426 422 418 416 412 408Taurage PHCI 407 443 440 436 431 430 426 421Utena PHCI 192 372 370 366 362 361 357 354Trakai PHCI 638 548 544 539 534 532 526 521Mazeikiai PHCI 559 552 548 543 538 536 530 525Ukmerge PHCI 396 374 372 368 364 363 359 356Radviliskis PHCI 344 356 354 350 347 345 342 339Silute PHCI 339 302 300 297 294 293 290 287Visaginas PHCI 338 328 326 323 319 318 315 312Pasvalys PHCI 332 441 438 434 429 428 424 419Kedainiai PHCI 327 349 347 343 340 339 335 332Jonava PHCI 318 305 303 300 297 296 293 290Salcininkai PHCI 295 253 251 249 246 245 243 241Kretinga PHCI 269 320 318 315 312 310 307 304Lazdijai PHCI 258 282 280 277 275 274 271 268Raseiniai PHCI 257 282 280 277 275 274 271 268Vilkaviskis PHCI 254 313 311 308 305 304 301 298Rokiskis district PHCI 184 145 144 143 141 141 139 138Svencionys PHCI 157 146 145 144 142 142 140 139Other PHCI 4,722 3,091 3,072 3,039 3,010 2,997 2,970 2,943
Considering the tendencies of decrease in the number of births, the need for the neonatal service (the number of newborns needing the neonatal service) will also possibly decrease.
Table 9. Forecast of the number of newborns who are going to be provided with the neonatal service
Name of PHCI 2008 20092010p
2011p
2012p
2013p 2014p
2015p
III-level PHCIKMUC NC 4,716 4,741 4,710 4,663 4,617 4,599 4,554 4,510VUCH NC 1,111 1,100 1,093 1,082 1,071 1,067 1,057 1,046
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 68 of 281
R.3. Feasibility study
According to the number of births and the number of places of work of the staff in PHCI indicated by PHCI in 2009, the efficiency rate of PHCI „number of births per one place of work” was analyzed and this data was generalized for PHCI providing the service of different levels. According to the table below, PHCI of a certain level works much more efficiently compared with an average PHCI. Therefore the derivative rate of the most efficient working PHCI was assessed: IIA level – mean of five best PHCI, IIB level – mean of three best PHCI, III level – one best PHCI. These best results were used as the good practice which should be reached by all PHCI.
Considering the fact some PHCI working the most efficient according to the rate of the number of births per one place of work have a need for extra places of work, this need for some extra staff seen by PHCI was also assessed when assessing the best (TOP) results.
Table 10. Number of births in PHCI per one place of workLevel of service
Minimal value Assessed mean
Maximal value
Best results
III 24.43 25.02 25.61 25.61- TOP 1IIB 15.80 27.40 40.35 36.08- TOP 3IIA 7.63 17.18 24.31 21.82- TOP 5
In the case of PHCI providing the neonatal service, the rate of „the number of newborns provided with the service per one place of work“ was assessed: 29,77 (KMUC NC) and 10,09 (VUCH NC). The value of the rate of KMUC NC was chosen as the good practice for supplementary reassessment of the rate by adding the need for the extra number of places of work indicated by PHCI – 24,69.
The staff forecast was prepared according to the forecasted number of births and the mean of the best rates of PHCI (number of births per one place of work); in the case of KMUC NC and VUCH NC – according to the number of newborns per one place of work.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 69 of 281
R.3. Feasibility study
Table 11. Staff forecast in PHCI Present
situationNecessary number of staff when assessing efficiency
Forecast
Name of PHCI 2009 2009 2010p 2011p 2012p 2013p 2014p 2015pIII-level PHCIKMUC COG 148.73 142.9 142.0 140.5 139.1 138.6 137.3 135.9KMUC NC 159.25 192.0 190.8 188.9 187.0 186.3 184.4 182.6VMUH COG 149.5 150.5 149.5 148.0 146.6 146.0 144.6 143.1VUCH NC 109.0 44.5 44.3 43.8 43.4 43.2 42.8 42.4III-level sum 566.6 529.9 526.5 521.2 516.1 514.1 509.0 504.1IIB-level PHCIVULSKCF 45.8 42.0 41.7 41.3 40.9 40.7 40.3 39.9KUH 94.0 105.1 104.5 103.4 102.4 102.0 101.0 100.0Vilnius maternity home 94.8 91.4 90.8 89.9 89.0 88.6 87.8 86.9Kaunas II clinical hospital 48.5
41.4 41.1 40.7 40.3 40.1 39.7 39.4
Siauliai PHCI 137.3 60.1 59.7 59.1 58.5 58.3 57.7 57.1Panevezys PHCI 85.5 44.1 43.8 43.4 43.0 42.8 42.4 42.0IIB-level sum 505.8 384.0 381.6 377.8 374.0 372.5 368.9 365.3IIA-level PHCIP.Mazylio maternity 61.0 60.2 59.8 59.2 58.6 58.4 57.8 57.2
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 70 of 281
R.3. Feasibility study
Present situation
Necessary number of staff when assessing efficiency
Forecast
Name of PHCI 2009 2009 2010p 2011p 2012p 2013p 2014p 2015phomeChristian maternity home
42.0 48.5 48.1 47.6 47.2 47.0 46.6 46.1
Alytus PHCI 38.6 37.2 37.0 36.6 36.2 36.1 35.7 35.4Marijampole PHCI 46.5 27.0 26.8 26.6 26.3 26.2 26.0 25.7Telsiai PHCI 27.8 20.4 20.2 20.0 19.8 19.7 19.6 19.4Taurage PHCI 26.5 21.0 20.9 20.7 20.5 20.4 20.2 20.0Utena PHCI 20.8 17.7 17.6 17.4 17.2 17.1 16.9 16.8Trakai PHCI 23.8 26.0 25.8 25.6 25.3 25.2 25.0 24.7Mazeikiai PHCI 36.4 26.2 26.0 25.8 25.5 25.4 25.2 24.9Ukmerge PHCI 22.5 17.8 17.7 17.5 17.3 17.2 17.0 16.9Radviliskis PHCI 17.3 16.9 16.8 16.6 16.5 16.4 16.2 16.1Silute PHCI 20.0 14.3 14.2 14.1 14.0 13.9 13.8 13.6Visaginas PHCI 30.0 15.6 15.5 15.3 15.1 15.1 14.9 14.8Pasvalys PHCI 22.3 20.9 20.8 20.6 20.4 20.3 20.1 19.9Kedainiai PHCI 22.5 16.6 16.5 16.3 16.1 16.1 15.9 15.8Jonava PHCI 21.5 14.5 14.4 14.2 14.1 14.0 13.9 13.8Salcininkai PHCI 15.8 12.0 11.9 11.8 11.7 11.6 11.5 11.4
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 71 of 281
R.3. Feasibility study
Present situation
Necessary number of staff when assessing efficiency
Forecast
Name of PHCI 2009 2009 2010p 2011p 2012p 2013p 2014p 2015pKretinga PHCI 19.0 15.2 15.1 14.9 14.8 14.7 14.6 14.4Lazdijai PHCI 17.8 13.4 13.3 13.1 13.1 13.0 12.9 12.7Raseiniai PHCI 15.0 13.4 13.3 13.1 13.1 13.0 12.9 12.7Vilkaviskis PHCI 16.5 14.9 14.8 14.6 14.5 14.4 14.3 14.1Rokiskis district PHCI 19.0 6.9 6.8 6.8 6.7 6.7 6.6 6.5Svencionys PHCI 10.5 6.9 6.9 6.8 6.7 6.7 6.6 6.6IIA-level sum 592.7 483.2 480.1 475.4 470.6 468.9 464.2 459.6Total: 1,664.93 1,397.2 1,388.1 1,374.4 1,360.6 1,355.5 1,342.1 1,328.9Need (all levels) - -267.7 -276.8 -290.6 -304.3 -309.4 -322.8 -336.0
The results of the staff forecast show the need for staff because of the tendency of decrease in the number of births in 2015 could decrease by 336 places of work.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 72 of 281
R.3. Feasibility study
4.7 List of PHCI recommended for participation in the programmes for obtaining the support from the Swiss Government
4.7.1 Criteria of selection of PHCI participating in the programme When analyzing PHCI, the list of PHCI presented in Appendix Nº3 to the Technical Specification was reviewed in order to assess the service provision by PHCI within the long period (at least 5 years), the level of necessary investments, observance of the requirements of the Order, general condition of the premises and service provision quality. According to these criteria, these PHCI were selected which are recommended to participate in the programmes for obtaining the support from the Swiss Government (the main list) and the list of reserve PHCI was made. The reserve PHCI would obtain the support in case of satisfying the needs of PHCI from the main list for purchasing the mandatory equipment (described in the order).
THE RESERVE LIST
The criteria of assessment of the reserve PHCI and weights of the values assigned to them are described in the table below more particularly. The reserve list includes those PHCI which scored three and more points.Table 12. List of the criteria of assessment of the reserve PHCI Nº Description of criteria Weights of
criteria1. Number of births in case of observing the Order and
not exceeding 6 per cent of the number of Caesarean sections in PHCI providing the IIA-level obstetric service (assessed by subtracting the number of Caesarean sections from the number of births in PHCI and adding 6 per cent to obtained result).In case of observing the Order, the number of births would not exceed 300 in most of the analyzed reserve PHCI.
>=200; < 300 (1 point)< 200 (2 points)
2. Distance to another PHCI of a higher level providing the obstetric and neonatal service.The criterion was prepared considering the fact the period of providing the maternal with the service cannot exceed 1.5 hours since calling the fast medical aid (by assessing the furthest distance). In some PHCI the neonatologist is on duty at home and the operating doctor arrives from his/her home, thus, it is not possible to make any presumptions the service is provided within a shorter period than 1.5 hours.
>=50; < 70 km (1 point)>=30; < 50 km (2 points)< 30 km (3 points)
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 73 of 281
R.3. Feasibility study
Nº Description of criteria Weights of criteria
3. Share of Caesarean sections (percentage).The criterion was prepared following the Order.
> 16; <= 20 (1 point)> 20; <= 25 (2 points)> 25; <= 30 (3 points)
4. Expert assessment of the common situation during the visit (structure of the service provision, equipment, environment, necessity for updating all equipment, necessity for renovating the premises).
Satisfactory (1 point)Bad (2 points)
5. Need for investments in medical equipment per one newborn (Lt).
0 - 1 000 (1 point)1 001 - 2 000 (2points)2 001 - 3 000 (3points)3 001 - (4points)
6. Share of doctors doing secondary work (percentage).This criterion is relevant as it largely shows the number of doctors arriving for duty. Secondary work is often the reason for insufficient qualification.
> 30; <= 50 (1 point)> 50; <= 70 (2 points)> 70 (3 points)
In the table below, the list of the reserve PHCI is presented which would be provided with medical equipment after providing support for the main PHCI or in case of extra financing. The list is made in the order of decreasing priority. In case a few hospitals score the same number of points, this one is written above which had more births in 2009.
Nº Name of PHCI 17 2 3 4 5 6 TotalHospitals providing the obstetric-gynaecologic service
1. Radviliskis PHCI 08 3 0 0 1 0 42. Silute PHCI 1 1 3 0 2 0 73. Raseiniai PHCI 1 1 0 2 2 1 74. Lazdijai PHCI 1 2 0 2 2 0 75. Salcininkai PHCI 1 2 1 1 1 1 76. Rokiskis district PHCI 2 1 0 2 3 1 97. Jonava PHCI 1 2 2 0 2 2 98. Kretinga PHCI 1 3 2 1 1 1 99. Vilkaviskis PHCI 1 3 3 0 3 0 10
7 Number of criterion according to the numeration of criteria presented in the table above8 Zero assessment means that PHCI satisfies the criterion.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 74 of 281
R.3. Feasibility study
10. Svencionys PHCI 2 1 2 2 4 2 13PHCI providing the neonatal service11. KVL PHCI - 3 - - 4 0 7
PHCI providing specialized services12. VUHSCSCC - - - - - - -
Note: The public institution Raseiniai PHCI is listed above the public institution Lazdijai PHCI as it has a bigger part of medical equipment which is older than 3 years.
Note: It is recommended to concentrate the service provision in Klaipeda city which would encourage rational use of the state and support funding. When analyzing the extents of the service provided by KVLV, it is apparent the service which is presently provided by KLVL could be transferred to KUH. It would be irrational to prepare a suitable place for reanimation/intensive care in KLVL according to the number of patients serviced by KLVL (about 10 patients every year) (preparation of a suitable place costs about 200,000 – 300,000 Lt). Therefore it is recommended to include KLVL in the list of the reserve PHCI.
Note: VUHSCSCC was included in the list of reserved hospitals considering the following:► In 2008 – 2009 the hospital was given the support of 2.234.116 € according to
the project „Availability of joint cardiosurgical and anaesthetic help for children and improvement of quality in Vilnius University Hospital Santariskiu Clinic“ (NOR LT042). Beside repair of the premises and training of the employees, funding was also assigned for purchasing medical equipment. On this basis an assumption can be made, the most necessary medical equipment has been purchased by using this funding;
► The hospital provides specialized services for neonates, babies up to one year and children; meanwhile the Programme is intended to improve the total level of the health service provision for the mother and the neonate. On this basis an assumption can be made, a part of asked equipment could be given to the service provision and not only neonates.
In the beginning of the analysis considering major need of investment in medical equipment and maintenance of the facilities and the closeness of Vilnius hospitals, which provide parallel services, an issue of the need of financing of Trakai PHCI was discussed. After detailed analysis has been performed it was decided to include Trakai PHCI into the main list of PHCI due to the following key assumptions, which provide that Trakai PHCI will provide quality services in the future:
1. Irrespective of the fact that Trakai ASPĮ is established only in the distance of 25 km from Vilnius, attention must be paid to the location of other potential hospitals in Vilnius (VUHSCCF, VCUH COG) – these hospitals are in the opposite side of the city compared to Trakai. Considering the actual time which is needed to transport a pregnant woman or a newborn to one
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 75 of 281
R.3. Feasibility study
of the above mentioned hospitals, transport jams in Vilnius should be taken into account. Just for comparison – time needed to drive from a hospital in Kretinga to KUH takes a relatively short time.
2. The actual number of births given in this hospital in 2009 exceeded twice the number settled by the Law, which states that there should be at least 300 births given at the PHCI, it amounted to 544 births.
3. There are no reasons to think that after the newly constructed Vilnius Perinatology Centre starts operating almost 300 births from Trakai hospital will be transferred to Vilnius, and Trakai ASPĮ will stop meeting the requirements established by the Law.
4. According to the results of the patients’ survey carried out in March 2010, patients expressed their most satisfaction with the services provided in the hospital of Trakai.
THE MAIN (NON-RESERVED) LIST
In order to decide in which order those PHCI included in the main (non-reserved) list should be financed, they were written in the order of priority according to pre-defined criteria. These defined criteria assess common rates of the activity of PHCI, attraction, compliance of PHCI with the aims of the Programme. It is recommended to perform all purchase according to the priority list of PHCI made on the basis of these criteria.
Different weights were assigned to the value of each criterion. PHCI were listed in the order of decrease of scored points. In case a few PHCI scored the same number of points, the PHCI with (1) a lower level of the service provision; (2) more births was listed above. In the case of PHCI providing the neonatal service, the PHCI providing more neonatal service was listed above.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 76 of 281
R.3. Feasibility study
In the table below, the criteria are presented according to which the priority list of PHCI was prepared.
Table 13. List of the main criteria for assessing PHCI Nº Description of criteria Weights of criteria1. Level of the service provided by PHCI
One of the aims of this programme is to decrease economic and social differences, therefore it is recommended to pay the biggest attention to regional PHCI providing the IIA-level service. Thus, patients would be given a possibility to get equally qualitative service of a certain level in all Lithuania.
► III level (1 point)► IIB level (2 points)► IIA level ( 3 points)
2. Age of medical equipment, %
It is recommended to update old medical equipment used by PHCI, therefore the extents of available medical equipment were compared which was older than 3 years (i.e., manufactured before 2007). The bigger is the part of such equipment in PHCI, the more priority (more points) it is given.
► < 20 (0 points)► >= 20; < 40 (1 point)► >= 40; < 60 (2
points)► >= 60; < 80 (3
points)► >= 80 (4 points)
3. Number of births per one delivery room in units.
The more births fall per one delivery room, the higher is the load of available equipment and the faster is its depreciation. The priority was given to those PHCI which have more births per one delivery room.
► < 300 (1 point)► >= 300; < 500 (2
points)► >= 500 (3 points)
4. Part of births per one administrative unit, %
In order to use provided equipment in its entirety, i.e., in order to use the investments as efficiently as possible, the priority was given to PHCI accepting more births in the administrative unit assigned to them. This criterion also partially shows the attraction of PHCI.
► < 50 (1 point)► >= 50; < 70 (2
points)► >= 70 (3 points)
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 77 of 281
R.3. Feasibility study
Nº Description of criteria Weights of criteria5. Number of births per one doctor obstetrician-
gynaecologist, %
The more births fall per one doctor obstetrician-gynaecologist, the higher is the workload of the staff of PHCI. In order to facilitate their daily work and decrease a probability of mistakes, their depreciated equipment should be updated. The priority is given to PHCI where more births fall per one doctor obstetrician-gynaecologist.
► < 70 (1 point)► >= 70; < 150 (2
points)► >= 150 (3 points)
6. Number of the neonatal service provided for newborns per one neonatologist, in units
The more neonatal service falls per one neonatologist, the higher is their workload. In order to facilitate their daily work and decrease a probability of mistakes, their depreciated equipment should be updated. The priority is given to PHCI where more births fall per oneneonatologist.
► < 100 (1 point)► >= 100; < 200 (2
points)► >= 200 (3 points)
7. Number of the neonatal service provided for newborns per one intensive care room for newborns, in units
The more neonatal service falls per one intensive care room for newborns, the higher is the equipment load and the faster is its depreciation. The priority is given to PHCI where more neonatal service falls per one room.
► < 1000 (1 point)► >= 1000; < 2000 (2
points)► >= 2000 (3 points)
Note: Criteria 6 and 7 are only applied to KMUC NC and VUCH NC hospitals.
4.7.2 Priority list of the hospitals participating in the programme In the table below, the priority list of the hospitals is provided which provide the stationary health care service for pregnant women, maternal and newborns and are going to provide it in the future and are recommended for participation in the programmes. Those PHCI which only provide the neonatal service are shown separately because of incomparable efficiency rates of their activity.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 78 of 281
R.3. Feasibility study
Table 14. Priority list of the main PHCI
Nº Name of PHCI
Level of the service
provided by hospital
Age of medical equipment
Number of births per one delivery room
(2009)
Part of births per one
administrative unit (2009)
Part of births per one doctor
obstetrician-gynaecologist
(2009)Total sum
level pointsper cent points unit points
per cent points unit points points
1 Trakai PHCI IIA 3 90 4 274 1 143 3 78 2 132 Pasvalys PHCI IIA 3 91 4 221 1 132 3 77 2 133 KMUC COG III 1 100 4 519 3 82 3 72 2 134 P.Mazylio maternity home IIA 3 89 4 423 2 22 1 86 2 125 Christian maternity home IIA 3 61 3 511 3 18 1 107 2 126 Mazeikiai PHCI IIA 3 79 3 184 1 77 3 72 2 127 Ukmerge PHCI IIA 3 100 4 187 1 85 3 58 1 128 Utena PHCI IIA 3 96 4 186 1 93 3 53 1 129 Visaginas PHCI IIA 3 100 4 164 1 107 3 47 1 12
10 Kedainiai PHCI IIA 3 91 4 175 1 52 2 47 1 1111 Panevezys PHCI IIB 2 80 3 265 1 80 3 84 2 1112 Alytus PHCI IIA 3 42 2 196 1 55 2 89 2 1013 Marijampole PHCI IIA 3 65 3 190 1 56 2 62 1 1014 KUL IIB 2 16 0 421 2 115 3 292 3 1015 Vilnius maternity home IIB 2 42 2 366 2 38 1 183 3 1016 VULSKCF IIB 2 48 2 505 3 18 1 98 2 1017 Kaunas II clinical hospital IIB 2 62 3 249 1 26 1 199 3 1018 Taurage PHCI IIA 3 45 2 222 1 48 1 74 2 9
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 79 of 281
R.3. Feasibility study
Nº Name of PHCI
Level of the service
provided by hospital
Age of medical equipment
Number of births per one delivery room
(2009)
Part of births per one
administrative unit (2009)
Part of births per one doctor
obstetrician-gynaecologist
(2009)Total sum
level pointsper cent points unit points
per cent points unit points points
19 VMUH COG III 1 75 3 479 2 44 1 115 2 920 Telsiai PHCI IIA 3 44 2 143 1 39 1 59 1 821 Siauliai PHCI IIB 2 0 0 217 1 72 3 72 2 8
Nº Name of PHCI
Level of the service
provided by hospital
Age of medical equipment
Number of the neonatal service
provided for newborns per
one neonatologist
(2009)
Service provided for
newborns per one intensive
care room (2009)
Total sum
level pointsper cent points unit points unit points points
1 VUCH NC III 1 82 4 139 2 3326 3 10 2 KMUC NC III 1 77 3 357 3 1161 2 9
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 80 of 281
R.3. Feasibility study
4.7.3 Situation of Vilnius perinatal centrePresently Vilnius perinatal centre consists of VMUH COG and VUCH NC. The number of births in VMUH COG in 2009 reached 3,828.
It is planned that the present structure of Vilnius perinatal centre will be changed after building a new block of Santariskiu Clinic of VUH in Santariskiu medical town in which subdivisions services will be provided for pregnant women, delivering women and neonates. VUHSCCF should be moved to mentioned new building. The total obstetric-gynaecological staff of VUHSCCF and its available not depreciated equipment would be transferred to the new block while moving there. It is planned that the number of births accepted in VUHSCCF which reached 1,514 in 2009 will also be accepted in the new department of VUH Santariskiu Clinic.
The end of construction of the new perinatal centre is intended in the fourth quarter of 2011. After its termination, the following should be located there:
► Obstetric-gynaecological consulting room;► Obstetric department;► Department of obstetric pathology;► Department of neonates;► Department of reanimation.
In the future it is intended to change the structure of Vilnius perinatal centre dependently on made strategic decisions considering two possible scenarios.
Table 15. Scenarios of the perinatal centreScenario I Scenario II
Structure of the perinatal centreIn the new department of VUH Santariskiu Clinic neonatal services of the III-level with the III-level reanimation would be provided – neonates born in the clinic would be ensured essential neonatal help and they would be transported to VUCH NC. VMUH COG would lose the status of a perinatal centre and would provide the IIB-level services. The status of VUCH as of a perinatal centre would not be changed.
VMUH COG would lose the status of a perinatal centre and would provide the IIB-level services. The departments of neonate pathology and neonate reanimation and intensive therapy would be fully transferred from VUCH NC to VUH Santariskiu Clinic (including staff and medical equipment). VUCH NC would not provide the neonatal services of the III-level any more.
AdvantagesIn the 2nd part of the protocol created in 25th August 2010 during a joint health sector programes, being funded under the agreement between the
Lithuania’s obstetrics – gynaecologist association and Lithuania’s Neonatologists association prefer the 2nd Vilnius perinatal centre structure
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 81 of 281
R.3. Feasibility study
Scenario I Scenario IIGovernment of the Republic of Lithuania and the Swiss Confederation Federal Council the Implementation of the Lithuanian-Swiss Cooperation Programme to reduce economic and social disparities within the enlarged European Union, implementation oversee committee meeting, the 1st Vilnius perinatal centre structure change scenario is accepted.
change scenario.It is planed that there would be 16 delivery rooms in the new VUHSC building. Considering that medical equipment is provided for 8 delivery rooms, the rest of the rooms could be equipped with medical equipment needed for newborn pathology and newborn reanimation and intensive therapy services. This medical equipment could be reallocated from VUCL NC. Providing neonatal services in VUCL NC and in the new VUHSC building would mean that the services would be duplicated. That means the personnel and medical equipment, needed for neonatal services, would be duplicated too. If neonatal services would be provided in one place the project’s and country’s funding would be used more efficiently.Obstetrics - gynaecology and neonatal services provided in one place is a world’s best practice. This increases the safety of the services because if the newborn is sick, he/ she doesn’t need to be transported to another hospital. Quality neonatal services are provided for the sick newborn in the same place where he/ she was born.
DisadvantagesConsidering that the distance between VUCL NC and the new VUHSC building is small, the idea of transporting the sick newborns with reanimobiles is irrational leading to a faster depreciation of the reanimobiles.
There is no possibility to reallocate the medicine equipment form VUCL NC to the new VUHSC building because there are no rooms dedicated for this equipment. This was confirmed on 26th July 2010 during the meeting with Vilnius perinatal centre representatives.
Extent of obstetric servicesConsidering the fact that about a half of births accepted in the perinatal centre consists of pathological births, the number of births accepted by VMUH COG should decrease from the present 3,828 to about 1,900. Pathological births (other1.900 births) would be accepted in the new obstetric department of VUH
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 82 of 281
R.3. Feasibility study
Scenario I Scenario IISantariskiu Clinic. The number of births planned in this approach in the obstetric department of VUH Santariskiu Clinic could reach about 3.400 (all births of VUHSCCF and pathological births of VMUH COG are taken over).
Extent of neonatal servicesNeonates born in the clinic would be ensured urgent help and they would be transferred to VUCH NC after stabilizing their state.
All neonatal services of the III-level would be ensured in the new obstetric department of VUH Santariskiu Clinic for all neonates of Vilnius and other towns.
Impact on the feasibility studyOn the basis of these assumptions, the need for investments in medical equipment for VMUH COG, VUCH and VUHSCCF was calculated.
In case of coming true scenario II, about 1.86 million investments in purchasing medical equipment would be saved. In Appendix 15, the list of equipment which would not be purchased is presented.The costs of adapting premises for VUCL transferable equipment is not Swiss support or feasibility study object, so the costs are not provided.
Conclusion
Considering the present situation in Vilnius perinatal centre and the long-term and strategic plans of VUHSC, which are known during the preparation of feasibility study, the most important factors which influences the funding given to Vilnius perinatal centre must be stated:
► the 2nd scenario is not real at this time because there are no technical preparation made, there are no funding for it, there are no rooms in the new VUHSC building which would be suitable for VUCL NC to provide it’s services;
► Obstetrics and neonatal buildings being separate, the provision of safe services for sick newborns must be guaranteed. While there are no other options, the safe provision of services for sick newborns must be assured by equipping a newborn reanimation and intensive care department in the new VUHSC building.
Considering the above stated factors and seeking to assure safe provision of services for newborns in Vilnius perinatal centre, the funding for equipping a newborn reanimation and intensive care department must be provided (based on the 1st scenario).
Summary of VUHSCCF funding needs for medical equipment
The situation of VUHSCCF is exceptional compared to other hospitals participating in the Programme. VUHSCCF needs more new medical equipment
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 83 of 281
R.3. Feasibility study
compared to other hospitals because of it’s plans to move to the new VUHSC building and the planned increase in the number of given births. While counting VUHSCCF needs for new medical equipment, the medical equipment owned by VUHSCCF which is not depreciated was taken into account. In the table given below a summarized VUHSCCF need for medical equipment is provided.
Departments
Number of rooms being equipped
Number of medical equipment suitable for reallocating it from VUHSCCF to VUH SC
New medical equipment from optimal package
Additional new medical equipment for VUHSCCF for providing perinatal services
Qty. Sum, Lt Qty. Sum, Lt
Delivery room
8 33 38 1,071,190 8 582,135
Newborn reanimation place in delivery room or in operating room
8 18 33 131,701 0 0
Sick and premature newborns room/ intensive therapy departments
0 20 29 1,641,634 4 413,368
Distant supervision room
0 0 0 0 0 0
Operating room
2 7 4 463,632 0 0
Postoperative intensive observation ward
4 0 0 0 0 0
Other 0 0 0 0 3 241,160Total: 78 104 3,308,15
715 1,236,66
3
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 84 of 281
R.3. Feasibility study
Explanation of table columns:► Column’s “Number of rooms being equipped“ values are counted
considering the predicted birth number (the ratio between rooms equipped and the number of births is explained in chapter 5.1.2 „Needs for PHCI for medical equipment“);
► Column’s “Number of medical equipment suitable for reallocating it from VUHSCCF to VUH SC” values are counted taking into account VUHSCCF medical equipment which is not depreciated (made in 20059 or later);
► Column’s “New medical equipment from optimal package” values are counted by summing the amount of new medical equipment, which is stated in the optimal package list, and the funding needed to buy it;
► Column’s “Additional new medical equipment for VUHSCCF for providing perinatal services” values are counted by summing the amount of new medical equipment, which is needed for providing perinatal services, and the funding needed to buy it.
9 Depreciation term chosen is 2005 because the buy in of medical equipment is planned to start at the end of 2011 and because VUHSCCF‘s number in priority list of the hospitals participating in the programme is 16 th. Based on this an assumption is made that the new medical equipment for VUHSCCF would be bought in 2012.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 85 of 281
R.3. Feasibility study
5. Analysis of medical equipment
5.1 Analysis of medical equipment available and required for PHCI
5.1.1 Medical equipment available for PHCI In order to collect information about medical equipment of PHCI, every PHCI was sent a questionnaire where every PHCI provided information about available medical equipment.
Following the Order No 117„ On the approval of the procedure of health care of pregnant women, delivering women and neonates“ of the Minister of Health of the Republic of Lithuania of 15 March 1999 (published in the Official Gazette on 26 March 1999, No: 28, Publ. No: 811) and the procurement documents, a list of medical equipment was prepared according to which PHCI had to provide information about available medical equipment. The prepared list of medical equipment was classified according to the levels of services provided by PHCI and type of use of medical equipment (for example, medical equipment used in the delivery room).
The list of information requested from PHCI was prepared according to the requirements indicated in the procurement documents and involved:
► Name;► Model;► Purpose;► Manufacturer;► Amount;► Year of manufacturing;► Depreciation of equipment available for PHCI;► Average number of procedures performed per month.
Medical equipment available for every PHCI is presented in Appendix No 4 to this document.
On the basis of the information provided by PHCI about available medical equipment, an analysis of available medical equipment was performed according to:
► Age of medical equipment;► Amount of available and required essential and additional medical
equipment.
Analysis of available medical equipment according to age
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 86 of 281
R.3. Feasibility study
The age of medical equipment available for PHCI was analyzed on the basis of two criteria:
► Amount of medical equipment which is older than 7 years, i.e., was manufactured before 2003;
► Amount of medical equipment which is older than 3 years, i.e., was manufactured before 2007.
The first criterion of the age of medical equipment complies with the present situation of medical equipment available for PHCI. It indicates the amount of available medical equipment which is depreciated in the accounting sense (property which is older than 7 years is considered depreciated in the accounting sense). The second criterion complies with the situation which will happen while purchasing medical equipment at the end of 2012. It indicates the amount of equipment which will be depreciated in 2 years at the time of the purchase.The total amount of medical equipment which is older than 7 years is 1094 units. It makes 47% of all medical equipment available for PHCI. The amount of depreciated equipment distributed according to the level of provided services is equal, respectively:
► The percentage of depreciated equipment in the hospitals providing the IIA-level services makes 64% of all equipment available for the IIA-level hospitals.
► The percentage of depreciated equipment in the hospitals providing the IIB-level services makes 18% of all equipment available for the IIB-level hospitals.
► The percentage of depreciated equipment in the hospitals providing the III-level services makes 59% of all equipment available for the III-level hospitals.
The total amount of medical equipment which is older than 3 years is 1730 units. It makes 74% of all medical equipment available for PHCI. The amount of equipment, which will be depreciated at the time of the procurement, distributed by service levels equals respectively:
► The percentage of medical equipment which will be depreciated in 2 years at the time of the purchase in the hospitals providing the IIA-level services makes 88% of all equipment available for the IIA-level hospitals.
► The percentage of medical equipment which will be depreciated in 2 years at the time of the purchase in the hospitals providing the IIB-level services makes 46% of all equipment available for the IIB-level hospitals.
► The percentage of medical equipment which will be depreciated in 2 years at the time of the purchase in the hospitals providing the III-level services makes 91% of all equipment available for the III-level hospitals.
Detailed quantitative distribution of every kind of medical equipment available for every PHCI according to the age is presented in Appendix No 10.
Analysis of the correlation of available and deficient essential and additional medical equipment
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 87 of 281
R.3. Feasibility study
Another criterion reflecting the present situation of medical equipment available for PHCI is the correlation of available and required essential and additional medical equipment. This correlation indicates the percentage of the need for essential and additional medical equipment expressed by PHCI compared with presently available equipment.
► The average need for available and required essential and additional medical equipment in PHCI providing the IIA-level services is 100%. The average need for required additional medical equipment is 124%.
► The average need for available and required essential and additional medical equipment in PHCI providing the IIB-level services is 98%. The average need for required additional medical equipment is 208%.
► The average need for available and required essential and additional medical equipment in PHCI providing the III-level services is 169%. The average need for required additional medical equipment is 559%.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 88 of 281
R.3. Feasibility study
In the picture below, a detailed correlation of the need for available and required essential and additional equipment of every PHCI is presented.
KMUC COG KMUC NC VCUH COG VUCL NC0
200
400
600
800
1,000
1,200
Required essential equipmentAdditional equipment
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 89 of 281
R.3. Feasibility study
P.Mazylio mater
nity ...
Christian mater
nity ...
Alytus PHCI
Marijampole P
HCITels
iai PHCI
Taurage
PHCI
Utena PHCI
Trakai P
HCI
Mazeikiai
PHCI
Ukmerge PHCI
Radviliskis P
HCISilu
te PHCI
Visaginas P
HCI
Pasvalys P
HCI
Kedainiai PHCI
Jonava PHCI
Salcininkai
PHCI
Kretinga P
HCI
Lazdijai
PHCI
Raseiniai P
HCI
Vilkavisk
is PHCI
Rokiskis d
istrict P
HCI
Svencionys P
HCI
0
50
100
150
200
250
300
350
400
Required essential equipmentAdditional equipment
VUHSCCF KUH
Vilnius mater
nity home
Kaunas 2-nd CH
Siauliai
PHCI
Panevezys
PHCI
0100200300400500600700800
Required essential equipmentAdditional equipment
Picture No 23 – Comparison of PHCI according to the need for available and required essential and additional medical equipment, %
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 90 of 281
R.3. Feasibility study
5.1.2 Needs for PHCI for medical equipmentIn the questionnaire of medical equipment, every PHCI was also asked to present a preliminary amount of required medical equipment in their opinion and the importance of its need. The value of importance „1“ means the need for respective equipment was given the highest priority, value „2“ means the equipment was given an average priority, value “3“ means the equipment was given a low priority and value „4“ means the equipment was given the lowest priority.
After performing the analysis of the data provided by PHCI, the following was established:
► The preliminary required amount of medical equipment essential for every PHCI according to the Order;
► The preliminary amount of medical equipment essential for every PHCI according to the Order to which PHCI gave the highest priority;
► The required amount of medical equipment making the optimal package of medical equipment for county PHCI. The amount of medical equipment making the optimal package of medical equipment for the hospitals providing the IIB and III-level obstetric and neonatal services was not established because of low possibilities to compare the activity of these PHCI on the national level;
► The expert amount of I-priority medical equipment provided for every PHCI.
Optimal package of medical equipment: ► The optimal package of medical equipment is a list of medical equipment
made by the experts, docent dr. Mindaugas and Kliucinskas and dr. Antanas Puzas, which is necessary for the IIA-level service provision and which medical equipment is classified according to the type of provided services.
► Every IIA-level PHCI is provided with packages of medical equipment for the delivery room, ward for ill and premature neonates and operating room according to the number of births. General equipment of an obstetric-gynaecological hospital is provided for the total PHCI.
Justification of medical equipment making the optimal package of medical equipment:
► According to the Order which has been valid since 1999, the equipment necessary for the departments of birth and obstetrics of PHCI providing obstetric services of different levels is approved;
► Within this period (since 1999), certain changes in these needs are observed. When preparing a new list of necessary equipment, the following was considered:► Changed diagnostic peculiarities (criteria based on scientific proofs,
for example, a diagnosis of premature birth);
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 91 of 281
R.3. Feasibility study
► Valid laws (law on the damage to patients’ health; in cases of audits, objective proof describing the state are required);
► Practice noticed during visits to PHCI and available possibilities.► The necessity for equipment is classified into the equipment necessary
for the delivery room and medical equipment essential for the obstetric department;
► The equipment of the delivery room is assessed for every ward of birth-delivery room; meanwhile, the equipment necessary for the obstetric department is assessed according to the scope and sophistication of services provided by PHCI.
Exclusive observations according to the type of medical equipment:► Oxygen source with dispenser:
► Oxygen is supplied centrally to the delivery rooms in all PHCI;► PHCI purchase oxygen according to valid contracts;► Almost all PHCI have dispensers;► It is necessary to renew the oxygen supply systems in certain
hospitals;► Amnioscope:
► It is not necessary to have it in every delivery room;► It is enough to have at least one set in a small hospital and one set
in the delivery room and one set in the obstetric department in the perinatal centres;
► Obstetric forceps:► They are only used in two hospitals of Lithuania (doctors have
experience in their use); in other ones, vacuum extraction is applied in case of indications;
► Most institutions of treatment have metal forceps like instruments necessary for breaking a foetus;
► Obstetric forceps do not break down;► Set for vacuum extraction:
► It is essential for every PHCI providing obstetric services;► This method is quite safe and applied by most specialists;► At least two sets are necessary which have to be always prepared
(sterile scoops);► Electrocardiograph and defibrillator:
► The demand is higher in those PHCI where more pregnant women and delivering women with a high cardiovascular or another extragenital pathology arrive (PHCI providing the IIB and III-level services);
► Microscope used for diagnostics of the foetus water flow and assessment of native smears:
► Perinatal centres which concentrate on women with prematurely breaking foetus water should contain at least one microscope in the departments of birth and obstetrics.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 92 of 281
R.3. Feasibility study
The optimal package of medical equipment in the delivery room of the IIA, B and III-level obstetric hospitals is the same. The need for common equipment in the departments of birth and obstetrics of PHCI providing the IIB and III-level services is established after assessing the exclusive observations above according to the type of medical equipment and after assessing the equipment available for PHCI and the indicated need.
Number of packages (number of delivery rooms) according to the number of births for all PHCI:
► 1 package – up to 400 births;► 2 package - 400 – 800 births;► 3 package - 800 – 1200 births;► 4 package - 1200 – 1600 births;► 5 package - 1600 – 2000 births;► 6 package - 2000 – 2400 births;► 7 package - 2400 – 2800 births;► 8 package – more than 2800 births.
Number of operating rooms according to the number of births for all PHCI:► Up to 1500 births – equipment for 1 (one) s/c operating room and 2 (two)
sets for a postoperative intensive care ward;► Over 1500 births – equipment for 2 (two) s/c operating rooms and 4 (four)
sets for a postoperative intensive care ward.
In the table below, medical equipment making the optimal package of medical equipment is justified.
Table 16. Justification of medical equipment making the optimal package of medical equipment
No Medical equipment and justificationOptimal package of the II-A level obstetric hospital – Delivery room
1. Universal birth bed:► The woman must have a possibility to give birth in a universal
birth bed which can change its position from recumbent to the sitting or semi-recumbent one by creating more physiological conditions for birth through natural paths of birth.
2. Multifunctional monitor for the adult:► A multifunctional monitor for the delivering woman would ensure
a possibility to objectively fix the position of the woman and her foetus once after arriving to the delivery room by writing CTG for 20-30 minutes (it is especially important if auditing is necessary) and continue monitoring in case of an emerging pathology of the foetus and/or delivering woman during the birth. Use of one monitor in a few rooms would decrease its useful life and impair
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 93 of 281
R.3. Feasibility study
No Medical equipment and justificationthe concentration of the staff’s attention in case of a need to continuously register CTG (every physiological birth can suddenly become pathological. It is only possible to say it was physiological after it is over). The Law on the Rights of Patients and Compensation of the Damage to Their Health (see the Law on the Rights of Patients and Compensation of the Damage to Their Health No I-1562 of the Republic of Lithuania of 3 October 1996) passed in Lithuania requires to record the state of the foetus even in case of fully physiological birth after arrival of the delivering woman to the hospital or listening to changes in the rhythm of the foetus’s heart during the birth. This is the only way to justify decisions made in the course of birth in case of a need for auditing.
3. Mobile illumination lamp:► It enables ensuring a focused light source in case of a necessity
to view the paths of birth, suspecting tears or in cases of bleeding;
► Mobility enables not overloading the delivery room with less used devices.
4. Perfusor (volumetric infusion pump - infusometer):► In case of a necessity to administer oxytocin or Mg sulphate
solutions during the birth or early postnatal period, the administration has to be strictly dosed; it is only possible to properly dose dripped solutions with the help to these devices.
5. Set for the view of the paths of birth:► In case of any indications of cutting the perineum or a necessity
to view the paths of birth or suturing cuts and/or tears, it is necessary to have special medical instruments.
6. Heated table for reanimation of the neonate:► Essential device for nursing of an ill neonate.
7. Mobile electric pump:► Essential device for aspiration of the contents of the operative
field and wound.8. Oxygen source with an optic:
► Essential device for long-lasting oxygen therapy.9. Set for reanimation of the neonate:
► Instruments essential for reanimation of the neonate+.9.1. Silicon masks of different sizes;9.2. Sack of Ambu type or T-shaped system (Ayre type);9.3. Laryngoscope with scoops of size No 0 and No 1;9.4. Intubation tubes (inner diameter 2-4 mm);9.5. Intubation tube stylet;9.6. Aspiration catheters (size Fr.5, 6, 8, 10);
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 94 of 281
R.3. Feasibility study
No Medical equipment and justification9.7. Stomach probes (size Fr.5, 8, 10);9.8. Umbilical catheters (size Fr.3,5, 4, 5, 6, 8);9.9. Set of umbilical vessel catheterization;
9.10. Needles of “butterfly” type or (and) intravenous catheters (size 25GA, 21GA, 18GA);
9.11. Three-way cocks;9.12. Set of essential medicaments;9.13. Disposable syringes;9.14. Plaster, gloves, scissors, napkins with 700 spirit.10. Electronic scale:
► Essential device for weighing the neonate.Optimal package of the II-A level obstetric hospital – Common set for
the delivery room and the department of obstetrics1. Portative ultrasound equipment (mobile equipment with an abdominal
and vaginal transducer and possibility to print):► Possibilities of an ultrasound examination during the birth are limited
– in order to specify the state of the foetus, presentation, localization of placenta, state of the uterus, birth of placenta etc. This equipment should be used for all obstetric diagnostics;
► Having a vaginal transducer would obligate to document the state of the cervix uteri when justifying the diagnosis of imminent premature birth (the questions asked while visiting PHCI produced the impression that the diagnosis of this pathology is insufficiently justified in most cases).
2. Cardiotocograph (simple):► Having a cardiotocograph would ensure a possibility to assess the
state of the foetus while women are in hospital – wards of pathology – or decrease the number of hospitalizations in case of arriving because of weekly-felt moves of the foetus (after recording a CTG complying with the norm, it is possible to discharge the woman without hesitaiton). The latter problem occurs at weekends and holidays when the primary health care centre or family clinics do not work.
3. Portative ultrasound stethoscope for heart tones of the foetus:► This is a substitute for a wooden or metal stethoscope which enables
hearing heartbeat of the foetus for the staff and pregnant woman, thus, it makes the future mother and her family to feel well in a psychological sense;
► This device is a few times cheaper than a cardiotocograph.4. Set for vacuum extraction of the foetus (2 units):
► A necessary set of instruments in order to ensure a possibility to quickly complete the birth under certain conditions;
► It is a very safe and fast method if it is suitably applied;► Two sets are necessary as it is essential to sterilize caps, thus, one
set has to always be ready.5. Amnioscope:
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 95 of 281
R.3. Feasibility study
No Medical equipment and justification► Device for assessing the foetus water. ► The examination has a practical value nowadays in case it is not clear
whether the front foetus water bubble is torn or it is necessary to assess the colour of the foetus water and the foetus water involucre is not torn.
6. Perfusor (volumetric infusion pump - infusometer):► In case of a necessity to administer infusotherapy during the birth or
early postnatal period, the administration has to be strictly dosed; it is only possible to properly dose dripped solutions with the help to these devices.
7. Heater of infusion solutions:► According to new recommendations of transfusologists, all solutions
have to reach the body temperature in order not to misbalance the physiological processes of the body; the erythrocyte mass and blood plasma must be kept in low temperature;
► In case of emergencies, it is necessary to unfreeze gradually, otherwise preparations can be spoilt;
► This system can ensure safe and proper preparation of solutions and blood components for transfusions.
Optimal package of the II-A level obstetric hospital – Set for the operating room
1. Operating table:► A tool which is necessary for Caesarean sections, postnatal
complications (suturing deep tears of the paths of birth, opening and treating big bruising);
► The operating table must have a possibility to easily and safely change the position of the patient in order to avoid the vena cava syndrome during the preparation for the operation and at the beginning of the operation before the neonate is born.
2. Operating illuminator:► For qualitative illumination of the operation area.
3. Narcosis device:► In order to ensure safe narcosis of the delivering woman in case of
emergencies of operative treatment.4. Set for a Caesarean section (2 units):
► In order to safely perform necessary interventions.5. Place for reanimation of the neonate – It is necessary to have an
identical place for reanimation of the neonate in the operating room like in the delivery room (see above).
6. Pump for the mother:► For aspiration of the contents of the operation area and wound.
Optimal package of the II-A level obstetric hospital – Set for the postoperative intensive observation ward
1. Functional bed of the delivering woman:► A bed which can change the position of the patient during the
postoperative period by creating possibilities for early nursing of the neonate etc.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 96 of 281
R.3. Feasibility study
No Medical equipment and justification2. Standard monitor of vital functions of the delivering woman:
► It would enable to objectively assess vital functions of the woman during the postoperative period or in case of a serious clinical situation.
Optimal package of the obstetric hospital of the IIA-level–Equipment of the ward for ill and premature neonates
1. Heated reanimation table for the neonate:► Essential device for nursing of an ill neonate.
2. Incubator or heated bed (according to the need of the hospital):► Essential device for care of premature neonates.
3. Oxygen source with instruments of dosage, humidifying and heating:► Essential device for humidifying, heating of the breathing mixture
and long-lasting oxygen therapy.4. Vacuum or electrical pump:
► Essential device for aspiration of the contents of the operative field and wound.
5. System for support of positive pressure in the airway (CPAP) with a set of nasal canulas of different sizes:► Essential device for nursing of the neonate – support of constant
positive pressure in the airway.6. Set for reanimation of the neonate:
► Instruments necessary for reanimation of the neonate.6.1. Silicon masks of different sizes;6.2. Sack of Ambu type or T-shaped system (Ayre type);6.3. Laryngoscope with scoops of size No 0 and No 1;6.4. Intubation tubes (inner diameter 2-4 mm);6.5. Intubation tube stylet;6.6. Aspiration catheters (size Fr.5, 6, 8, 10);6.7. Stomach probes (size Fr.5, 8, 10);6.8. Umbilical catheters (size Fr.3,5, 4, 5, 6, 8);6.9. Set of umbilical vessel catheterization;
6.10. Needles of “butterfly” type or (and) intravenous catheters (size 25GA, 21GA, 18GA);
6.11. Three-way cocks;6.12. Set of essential medicaments;6.13. Disposable syringes;6.14. Plaster, gloves, scissors, napkins with 700 spirit.
7. Monitor for assessment of the state of the neonate:► Essential device for observation of vital functions of the neonate.
8. Syringe infusion pump:► Essential device for dosage of medicaments.
9. Electronic scale:► Essential device for weighing the neonate.
10. Light and heating lamp:► Essential device for therapy and support of temperature of the
neonate.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 97 of 281
R.3. Feasibility study
No Medical equipment and justification11. Phototherapy device:
► Essential device for treating hiperbilirubinemia.
Notes:► Identical equipment is contained in the IIB and III-level hospitals;► The place for reanimation of the neonate in the operating room is
identical to that one in the delivery room;► Equipment of an ill and premature neonate is different in the IIB and III-
level hospitals (it is assessed and assigned individually according to the extent and needs of services provided by the hospitals);
► Differences of medical equipment making the set from that recommended in the Order:► Secondary A level:
► Equipment of birth in the delivery room:► The set of instruments for breaking operations of the foetus
is not contained as they could only be used in perinatal centres because of possible high traumatism (especially without experience);
► The artificial respiration apparatus is not contained as the narcosis apparatus is included in the set of the operating room instead;
► Obstetric forceps are not contained as these instruments only could be used in perinatal centres because of possible big traumatism (especially without experience);
► The electrocardiograph and the defibrillator are not contained as every PHCI should purchase them independently or in a centralized way in case there are remaining funds in the Programme;
► The microscope is not contained as the microscope is not used in the hospitals providing the IIA-level services and some IIB-level services; its necessity in these PHCI is doubtful as it is known that the foetus water breaking can be suspected by assessing the excretion ph;
► All other medical equipment complies with the Order.► Place for reanimation of the neonate in the delivery room:
► The set of the pleura cavity puncture and drainage is not contained as experience shows that it is not used;
► All other medical equipment complies with the Order.► Equipment of the ward for ill and premature neonates:
► 1-3 incubators did not serve the purpose as this amount is not necessary. A heated reanimation table for the neonate or heated bed is used more often;
► A simpler monitor is included as the multifunctional monitor is not necessary for the services provided;
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 98 of 281
R.3. Feasibility study
► One syringe pump is enough as the volumes are low and an ill neonate is immediately transferred to the hospital of a higher level;
► The portative air compressor is not contained as the system for supporting positive pressure in the airway (CPAP) with the set of nasal cannulas of different sizes is included in the set of the ward for ill and premature neonates;
► The set for lumbal puncture is not included as the hospitals of the IIA-level do not have a need for that. Besides, appropriate competence is necessary for that as the state of the neonate can be harmed in case of performing it without qualification. Such kind of interventions can only be performed in perinatal centres;
► All other medical equipment complies with the Order.
In the table below, the number of the optimal packages of medical equipment considering the number of births in PHCI and place of use of equipment is presented.
Table 17. Number of the optimal packages of medical equipment considering the number of birthsPlace of use of equipment
Number of packages according to the number of births
< 400 400 – 800 1200 – 1600 > 2800Delivery room 1 package 2 packages 4 packages 8 packagesEquipment of the place for reanimation of the neonate in the delivery room
1 package 2 packages 4 packages 8 packages
Operating room 1 package 1 package 2 packages (from 1500 births)
2 packages
Equipment of the ward for ill and premature neonates
1 package 2 packages 4 packages 8 packages
Total set for the department of births and obstetrics
1 package 1 package 1 package 1 package
The required amount of medical equipment making the optimal package of medical equipment was assessed by subtracting the amount of medical equipment available for PHCI manufactured after 2006 from the amount of medical equipment making the optimal package of medical equipment according to the number of births.
CONFIDENTIAL document.docx
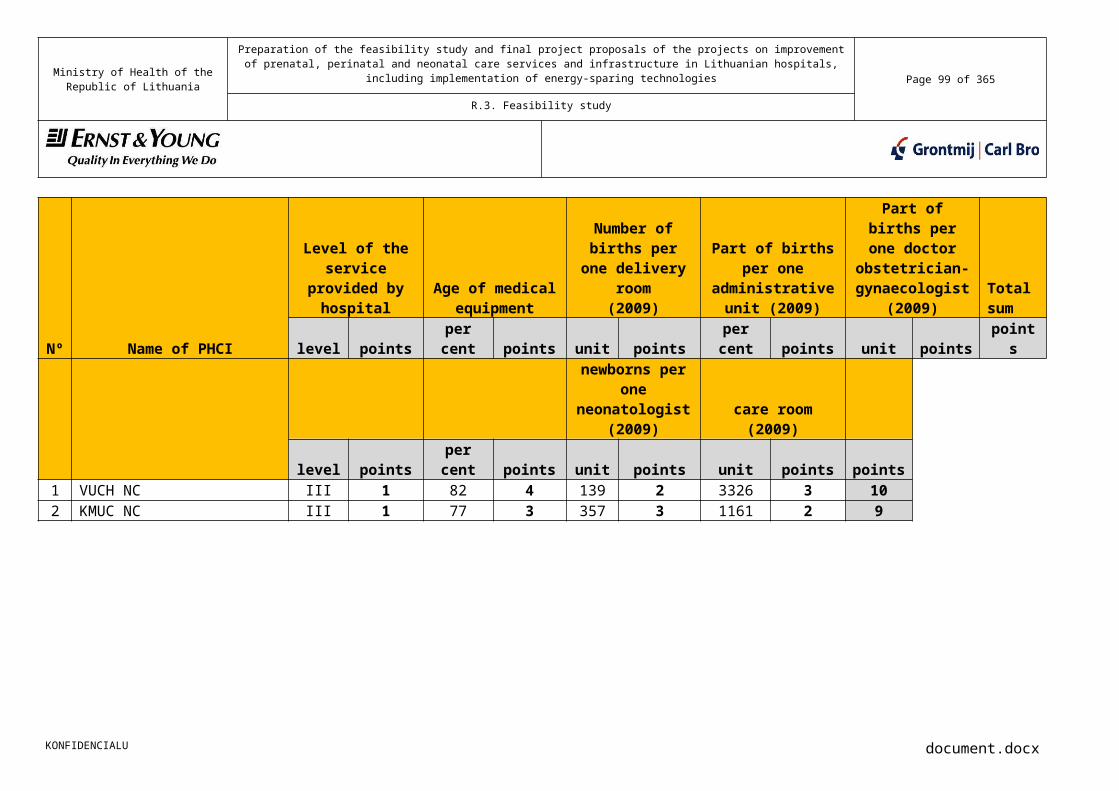
Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 99 of 281
R.3. Feasibility study
For instance, PI Pasvalys hospital had 441 births in 2009; therefore, it is eligible for 2 birth ward packages. A birth ward package consists of one universal birth bed, but since Pasvalys hospital has one new bed, only one extra bed shall be allocated, thus equipping two birth wards in total.
Medical equipment making the optimal package of medical equipment for IIA-level hospitals which is distributed according to the type of provided services is presented in Appendix No 9.
Taking into consideration that level III hospitals have highly qualified specialists with vast experience of work with the advanced medical equipment and knowledge of its advantages, while planning the medical equipment to be allocated to perinatology centres, most consideration was taken of their needs and the number of births and neonates treated. Therefore, for instance, KCUH was allocated 2 encefalographs, whereas VUCH was allocated two monitors for the registration of neonate brain activity.
Expert amount of medical equipment of priority I:The expert amount of medical equipment of priority I was established by the experts, docent dr. Mindaugas Kliucinskas and dr. Antanas Puzas, by reviewing the amount of required medical equipment of priority I expressed by each PHCI. While reviewing the needs of each PHCI, the required amount of medical equipment was:
► Decreased (including total non-assignment);► Increased;► Not changed.
While reviewing the required amount of medical equipment, the following was considered:
► Extent of provided services;► Amount of available non-depreciated medical equipment;► Cases of duplicate medical equipment;► Number of departments of PHCI;► Age of medical equipment at the time of purchase;
In the preparation of Appendix No 13, the amount of equipment allocated as priority I was reduced in Kaunas and Vilnius perinatology centres. The reduced amounts were moved to priority II or III. These changes were made taking into consideration that the Programme budget was exceeded and in order to secure the sufficient funding at least of priority I medical equipment for all the hospitals on the main list.
Expert amount of medical equipment of priority II:
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 100 of 281
R.3. Feasibility study
The expert amount of medical equipment of priority II was established by reviewing the need for medical equipment of priority II presented by each PHCI. The review of the amounts was made based on the same principles as in the case of priority IWhen preparing Appendix No 13, the reduced amounts of the equipment previously grouped as priority I was moved additionally to the list of equipment allocated as priority II. These changes were made taking into consideration that the programme budget was exceeded. The equipment on this list is necessary and, when possible, it is recommended to allocate funding for its purchase.
Expert amount of medical equipment of priority III:
The expert amount of medical equipment of priority III was established by reviewing the amount of required medical equipment of priority III expressed by each PHCI. While reviewing, the same principles were considered as in case of priority I and priority II.
When preparing Appendix No 13, the reduced amounts of the equipment previously grouped as priority I or II was moved additionally to the list of equipment allocated as priority III. These changes were made taking into consideration that the programme budget was exceeded. The equipment on this list is necessary and, when possible, it is recommended to allocate funding for its purchase.
Due to the reasons listed above and the demands of PHCI exceeding the budget for medical equipment, the amounts of medical equipment allocated as a certain priority presented in Annex No 4 and Appendix No 13 may differ. For example:
► Although the amount of medical equipment allocated to PI Pasvalys PHCI is the same in Appendix No 4 and No 13, the priorities and quantities of certain equipment differ. In Annex No 4 experts allocate 2 laringoscopes as priority I to PI Pasvalys PHCI (the priorities of PHCI indicated in Appendix No 4 were not changed), but in Appendix No 13 the number of laringoscopes is separated – one instrument is allocated as priority I and the other as priority III;
► Due to this reason, like in the case of PI Pasvalys PHCI, the demand for 2 encelographs indicated by KCUC NC in Annex No 4 with priority I is divided into priority I and III in Appendix No 13. The same principle applies to the demand for 2 monitors registering brain activity specified by VUCH as priority I.
In picture No 23 below, the amount of required medical equipment is presented in four sections:
► Preliminary required amount of medical equipment necessary according to the Order;
► Preliminary required amount of medical equipment necessary for every PHCI according to the Order which was given the highest priority by PHCI;
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 101 of 281
R.3. Feasibility study
► Preliminary required amount of medical equipment making the optimal package of medical equipment;
► Amount of medical equipment assessed by experts.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 102 of 281
R.3. Feasibility study
KMUC C
OG
KMUC N
C
VCUH CO
GVU
CL NC KVL
VUHSCS
CC0
50100150200250300350400
Preliminary required amount of PHCI medical equipment of priority III, units
Need for necessary equipment, units
Need for necessary equipment given priority I, units
Need for equipment as-sessed by experts which was given priority I, units
P.Mazylio m
aternity..
.
Christian
maternity
...Alyt
us PHCI
Marijampole
PHCITels
iai PHCI
Taurage
PHCI
Utena PHCI
Trakai PH
CI
Mažeikių P
HCI
Ukmerge PHCI
Radvilisk
is PHCI
Silutes PHCI
Visagina
s PHCI
Pasvalys
PHCI
Kedainia
i PHCI
Jonava PHCI
Salcinink
ai PHCI
Kretinga P
HCI
Lazdijai P
HCI
Raseiniai
PHCI
Vilkavisk
is PHCI
Rokiskis
district P
HCI
Svencion
ys ASPĮ
0102030405060708090
Preliminary required amount of PHCI medical equipment of priority IIA, units
Need for necessary equipment, unitsNeed for necessary equipment given priority I, unitsNeed for optimal equipment, units
VUHSCCF KUH
Vilnius m
aternity
home
Kaunas
2nd C
H
Siaulia
i PHCI
Paneve
zys PH
CI0
50100150200250
Preliminary required amount of PHCI medical equipment of priority IIB, units
Need for necessary equipment, units
Need for necessary equipment given priority I, units
Need for equipment assessed by experts which was given priority I, units
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 103 of 281
R.3. Feasibility study
Picture No 24 – Comparison of PHCI according to required medical equipment
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 104 of 281
R.3. Feasibility study
The total amount of required medical equipment consists of:► Preliminary required amount of medical equipment necessary according
to the Order which is common for all PHCI: 2088 units► Preliminary required amount of medical equipment necessary for every
PHCI according to the Order which was given the highest priority by PHCI: 1440 units
► Preliminary required amount of medical equipment making the optimal package of medical equipment: 2274 units
► Amount of medical equipment assessed by experts: 1038 units
5.1.3 Prices of medical equipmentIn order to ascertain present prices of medical equipment, 9 potential suppliers of medical equipment were interviewed. The following suppliers of medical equipment participated in the survey:
► PE ADNEDA;► UAB Spektramed;► UAB Arbor Medical Corporation LT";► UAB ILSANTA;► UAB Hospitex Diagnostics Kaunas;► UAB TRADINTEK;► UAB B.Braun Medical;► UAB Viltechmeda;► UAB EVOMEDA.
Preliminary prices were presented considering:► Extent of purchased medical equipment. In the request, the suppliers
were asked to present the prices in case of purchasing medical equipment:
► Up to 10 units;► Up to 50 units;► Up to 90 units.
► Service level of PHCI where medical equipment would be used. The total list of medical equipment was classified according to the requirements raised for medical equipment of PHCI of a certain level. This classification was performed by the experts, docent dr. Mindaugas Kliucinskas and Dr. Antanas Puzas. The implication is that the monitor of delivering women used in PHCI providing the IIA-level services is different from the monitor of delivering women used in PHCI for the III-level services.
After analyzing the prices of medical equipment presented by the suppliers of medical equipment, the total preliminary list of the prices of medical equipment including VAT was made and the prices were classified according to the purchased amount and service level.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 105 of 281
R.3. Feasibility study
In order to ensure satisfaction of the priority needs of PHCI, while assessing the need for investments in medical equipment, the highest price presented by the suppliers of medical equipment was used.
In the table below, the need for investments in purchasing the required amount of medical equipment is presented in four sections:
► (1) Preliminary need for investments in purchasing the required amount of medical equipment necessary according to the Order;
► (2) Preliminary need for investments in purchasing the required amount of medical equipment necessary for every PHCI according to the Order which was given the highest priority by PHCI;
► (3) Preliminary need for investments in purchasing the required amount of medical equipment making the optimal package of medical equipment. This need also includes the preliminary need for investments in purchasing the required amount of medical equipment necessary for the hospitals providing the IIB and third level obstetric and neonatal services according to the Order;
► (4) Preliminary need for investments in purchasing the required amount of medical equipment of priority I assessed by the experts.
KONFIDENCIALU document.docx
Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 106 of 281
R.3. Feasibility study
Table 18. Required amount of medical equipment and need for investments including VAT
No PHCI
Need for
necessary
equipment, units
Need for necessar
y equipmen
t, Lt
Need for necessar
y equipmen
t given priority I,
units
Need for necessar
y equipmen
t given priority I,
Lt
Need for optimal
equipment, units
Need for optimal
equipment, Lt
Need for equipmen
t assessed
by experts which was
given priority I,
units
Need for equipment assessed
by experts which was
given priority I,
Lt
Need for equipmen
t assessed
by experts which was
given priority II, units
Need for equipmen
t assessed
by experts which
was given priority
II, Lt
Need for equipmen
t assessed
by experts which was
given priority III, units
Need for equipme
nt assessed
by experts which was
given priority III, Lt
III-level PHCI1 KMUC COG 101 4,042,230 91 3,464,342 101 4,042,230 92 3,709,696 70 2,665,999 11 147,1202 KMUC NC 218 9,298,242 192 8,051,533 218 9,298,242 267 7,616,064 59 2,003,927 72 403,8223 VMUH COG 249 6,556,641 117 5,663,214 249 6,556,641 38 1,590,040 50 1,746,510 0 0
4 VUCH NC 374 12,822,695 331 12,511,40
0 374 12,822,695
204 7,553,442 26 382,787 47 751,167
Total III-level PHCI: 942 32,719,809 731 29,690,49
0 942 32,719,809
601 20,469,241 205 6,799,223 130 1,302,109
IIB-level PHCI5 VULHSCCF 202 6,178,215 149 5,398,600 202 6,178,215 91 3,974,083 16 473,234 37 410,3716 KUH 39 2,200,883 36 1,942,883 39 2,200,883 39 2,093,782 11 470,779 20 40,000
7Vilnius maternity home
52 2,187,688 51 2,153,688 52 2,187,688 61 2,271,309 28 379,430 21 55,000
8Kaunas 2nd clinical hospital
78 2,193,585 29 1,593,082 78 2,193,585 26 1,635,322 43 530,714 17 179,328
9 Siauliai PHCI 8 67,696 8 67,696 8 67,696 0 0 1 169,400 4 16,00010 Panevezys
PHCI 65 1,948,025 27 1,138,764 65 1,948,025 34 1,841,842 18 365,168 26 558,55911 KVL 29 825,287 13 520,123 29 825,287 15 442,080 8 111,500 5 178,76012 VUHSCSCC 4 1,242,000 2 1,050,000 4 1,242,000 2 1,050,000 1 32,000 0 0
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 107 of 281
R.3. Feasibility study
No PHCI
Need for
necessary
equipment, units
Need for necessar
y equipmen
t, Lt
Need for necessar
y equipmen
t given priority I,
units
Need for necessar
y equipmen
t given priority I,
Lt
Need for optimal
equipment, units
Need for optimal
equipment, Lt
Need for equipmen
t assessed
by experts which was
given priority I,
units
Need for equipment assessed
by experts which was
given priority I,
Lt
Need for equipmen
t assessed
by experts which was
given priority II, units
Need for equipmen
t assessed
by experts which
was given priority
II, Lt
Need for equipmen
t assessed
by experts which was
given priority III, units
Need for equipme
nt assessed
by experts which was
given priority III, Lt
Total IIB-level PHCI: 477 16,843,379 315 12,294,71
3 477 16,843,379 268 13,308,418 126 2,532,224 130 1,438,019
IIA-level PHCI
13P. Mazylio maternity home
24 416,928.58 12 296,933.7
5 60 1,900,421 14 249,122 15 371,652 8 154,891
14Christian maternity home
34 475,526.73 12 286,550.0
0 46 1,633,969 9 672,150 21 508,069 6 80,816
15 Alytus PHCI 19 444,004 13 230,576 27 1,255,547 12 349,841 10 385,823 12 74,669
16 Marijampole PHCI 31 428,174 5 126,269 34 1,351,517 6 376,269 6 118,834 16 205,382
17 Telsiai PHCI 13 331,364 10 314,564 34 1,329,896 7 435,936 5 54,591 8 329,00018 Taurage PHCI 49 761,146 29 452,701 40 1,373,233 23 972,375 8 147,380 5 53,09119 Utena PHCI 12 302,685 6 165,585 29 1,325,890 6 200,250 4 342,180 14 85,95020 Trakai PHCI 72 979,334 21 407,704 44 1,566,962 10 199,585 4 299,280 18 338,31221 Mazeikiai
PHCI 13 321,423 6 250,500 46 1,549,334 3 126,500 3 38,962 19 203,996
22 Ukmerge PHCI 37 418,596 23 270,701 38 1,420,924 24 957,244 8 163,716 6 41,200
23 Radviliskis PHCI 17 321,982 5 98,091 32 1,370,104 3 404,000 1 5,000 19 435,291
24 Silute PHCI 20 363,918 13 349,727 29 1,267,107 6 161,907 0 0 13 60,97225 Visaginas
PHCI 44 624,911 30 493,011 37 1,437,497 17 559,078 4 42,939 7 50,700
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 108 of 281
R.3. Feasibility study
No PHCI
Need for
necessary
equipment, units
Need for necessar
y equipmen
t, Lt
Need for necessar
y equipmen
t given priority I,
units
Need for necessar
y equipmen
t given priority I,
Lt
Need for optimal
equipment, units
Need for optimal
equipment, Lt
Need for equipmen
t assessed
by experts which was
given priority I,
units
Need for equipment assessed
by experts which was
given priority I,
Lt
Need for equipmen
t assessed
by experts which was
given priority II, units
Need for equipmen
t assessed
by experts which
was given priority
II, Lt
Need for equipmen
t assessed
by experts which was
given priority III, units
Need for equipme
nt assessed
by experts which was
given priority III, Lt
26 Pasvalys PHCI 31 511,328 19 468,285 41 1,527,057 9 431,650 5 357,871 15 181,766
27 Kedainiai PHCI 12 236,750 6 201,350 36 1,374,497 16 679,000 2 25,380 11 105,022
28 Jonava PHCI 79 866,978 47 178,451 38 1,433,634 12 717,932 2 26,000 16 216,94129 Salcininkai
PHCI 8 38,205 3 10,391 37 1,380,624 2 60,591 0 0 12 85,01430 Kretinga PHCI 19 518,560 12 194,550 35 1,433,690 7 263,544 1 250,000 16 104,53031 Lazdijai PHCI 29 448,665 25 406,606 37 1,374,790 16 515,014 0 0 8 77,99732 Raseiniai
PHCI 27 481,217 16 381,304 31 1,403,597 12 218,240 0 0 14 170,736
33 Vilkaviskis PHCI 22 588,474 22 588,474 32 1,362,329 17 449,498 0 0 2 8,000
34 Rokiskis district PHCI 26 362,198 26 362,198 34 1,434,797 20 346,886 0 0 3 10,100
35 Svencionys PHCI 31 518,678 31 518,678 38 1,416,524 20 536,511 0 0 3 10,100
Total IIA-level PHCI: 669 10,761,045 392 7,053,198 855 32,923,94
0 271 9,883,122 99 3,137,675 251 3,084,476Total (without
reserve): 1,777 53,748,071 1,223 45,949,93
1 1,854 66,542,645 1008 38,494,578 417 12,044,62
3 400 4,466,162
Total: 2,088 60,324,233 1,438 50,608,52
3 2,274 82,487,128 1140 43,660,781 430 12,469,12
3 511 5,824,604
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 109 of 281
R.3. Feasibility study
The following alternatives of distribution of medical equipment to PHCI were analyzed and assessed:► (1) The total preliminary need for investments in purchasing the required
amount of medical equipment necessary according to the Order for all PHCI is 60,324,233 million LTL including VAT;
► (2) The total preliminary need for investments in purchasing the required amount of medical equipment necessary for every PHCI according to the Order which was given the highest priority by PHC is 50,608,523 million LTL including VAT;
► (3) The total preliminary need for investments in purchasing the required amount of medical equipment making the optimal package of medical equipment is 82,487,128 million LTL including VAT;
► (4) The total preliminary need for investments in purchasing the required amount of medical equipment assessed by the experts which was given the highest priority by PHCI is 43,660,781 million LTL including VAT.
In order to choose one of the alternatives, the following criteria are recommended to consider:► The need for investments does not exceed the budget of the Programme;► While assessing the need for investments, both the wishes of PHCI were
considered and the needs were assessed in an expert view, considering the extent of provided services, level of the service provision, depreciation of available equipment and other aspects above;
► Within the scope of the Programme, the most important (essential) medical equipment is purchased which is necessary for the service provision.
Alternative (4) satisfies all these criteria as it involves the purchase of the most essential equipment given the first priority by PHCI. The amount of required medical equipment assessed by the experts is presented in Appendix No 13 and involves the total amount asked by PHCI classified according to the levels of provided services. The priorities to equipment were given in order to better plan the necessary budget of the Programme as the budget of equipment necessary to purchase (67,115,358Lt)10 exceeds the budget of the Programme. However, in case of purchasing the equipment of the first priority for lower prices than planned or getting extra funding, it is recommended to purchase the equipment of the second and third priority necessary for PHCI in the main list. The amount of medical equipment assigned to each PHCI according to given priorities is presented in Appendix No 13. To sum up, it is recommended to perform purchases of medical equipment in the following succession:
► Medical equipment of the first necessity (priority I) would be assigned to all PHCI in the main list in the order of decreasing priority;
► In case of remaining assets or emerging extra funding, every PHCI would be assigned medical equipment of the second necessity (priority II) in the order of decreasing priority;
10 During the analysis of medical equipment, it was calculated that the total need of PHCI for essential and specialized medical equipment is 72 million LTL.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 110 of 281
R.3. Feasibility study
► In case of a possibility to assign extra funding for purchasing medical equipment and satisfying the needs of necessity I and II, every PHCI would be assigned medical equipment of the third necessity (priority III) in the order of decreasing priority; In case there are remaining funds after assigning all necessary equipment for PHCI in the main list, it is recommended to assign equipment for PHCI in the reserved list in the order of decreasing priority.
► If the PHCI on the main list are allocated all the required medical equipment and there are spare funds left, it is recommended to allocate the equipment to PHCI on the reserve list at the decreasing priority order.
Note 1: Since it is probable that due to centralized public procurement, medical equipment can be acquired with a lower prices that the present feasibility study estimates, it is recommended to distribute the saved funds for medical equipment after reviewing the demands for medical equipment and assessing the flows of patients. During this assessment, the assumptions made for the calculation of the patients’ flows should be revised and the forecasts should be compared to the factual data of the services provided. For instance, if the actual flows of patients at the newly constructed Vilnius University Obstetrics Clinic are higher than currently forecasted, the demands for medical equipment and the funds allocated should be revised accordingly.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 111 of 281
R.3. Feasibility study
6. Analysis of reanimobiles for the neonate transportation
6.1 Analysis of reanimobiles for the neonate transportation available for PHCI
In the table below, the analysis of reanimobiles for the neonate transportation available for PHCI is presented.
Table 19. The main data of reanimobiles for the neonate transportation available for PHCI
PHCI KMUC COG VUCH KUH Siauliai PHCI
Panevezys PHCI
Make of reanimobile
VW11 Mercedes Benz
VW VW VW
Model Transporter M4
315 Sprinter
Transporter M4
Crafter Crafter
Registration number
ECH 422 CGH 926 DDF 228 EPS 810 EFS 812
Year of manufacturing
2008 2006 2007 2009 2008
Run as at the analysis day (km)
52.587 159.060 80.000 86.875 49.035
Kilometres run in 2009 in transporting neonates (km)
34.526 49.350 35.000 - -
Note: There is no possibility to ascertain the number of kilometres run by Siauliai PHCI and Panevezys PHCI in transporting neonates as these PHCI use common reanimobiles to meet the needs of all PHCI for the neonate transportation.
11 VW - Volkswagen
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 112 of 281
R.3. Feasibility study
In the table below, medical equipment mounted in the reanimobiles for the neonate transportation available for PHCI and the year of its manufacturing/ mounting is presented.
Table 20. Medical equipment mounted in the reanimobiles for the neonate transportation available for PHCI and the year of its manufacturing/ mounting.
PHCI KMUC COG VUCH KUH Siauliai PHCI Panevezys PHCI
Equipment of BASIC level for provision of urgent helpDefibrillator 1995 Not available Not
availableNot available (it is
removed as it is not used, but PHCI
have it)
Brought from the
department, cannot specify
age Medicament optic 1995 2006 2007 2008 1998 Intubation equipment 1995 2006 2008 2008 2000 Neonate heating equipment 1995 2006 2003 2007 2006 Transport incubator 1995 2006 2003 2007 2006
DVP device which can choose the oxygen concentration
1995 2004 2005 2007 2008
Heart and respiration monitor 1995 2005 2006 2007 2008
Pulsoxymeter Not available 2006 2006 2007 2008 Non-invasive blood pressure device Not available 2005 2006 2007 2008 Mucus pump 1995 2006 2003 2008 2008 2 infusion pumps 1995 2006 2007 2008 2008 Oxygen balloons 2002 2005 2002 2002 2002
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 113 of 281
R.3. Feasibility study
6.2 Analysis of use of reanimobiles for the neonate transportation available at PHCI
According to the data of 2007, 2008 and 2009, the average number of neonates transported in the reanimobiles for the neonate transportation available at KMUC NC, VUCH NC and KUH per year was 291.
VUCH NC can be mostly distinguished from the analyzed PHCI as it transported 621 neonates on the average per year according to the data of 2007, 2008 and 2009.
In the picture below, the comparison of the number of the neonate transportation according to PHCI is presented.
KMUC NC VUCL NC KUH Siauliai PHCI Panevezys PHCI0
100
200
300
400
500
600
700
Number of the neonate transportation
Picture No 25 – Number of the neonate transportation
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 114 of 281
R.3. Feasibility study
According to the data of 2007, 2008 and 2009, the average number of kilometres run by the reanimobiles in the neonate transportation available at KMUC NC, VUCH NC and KUH per year wile transporting neonates was 41.630 km.
A reanimobile for the neonate transportation available at VUCH runs from 70 km to 85 km during one transportation on the average; meanwhile, a reanimobile for the neonate transportation available at KMUC runs from 209 km to 276 km during one transportation on the average and a reanimobile for the neonate transportation available for KUH runs from 410 km to 444 km during one transportation on the average.
Considering the arguments above, an assumption can be made that:► A reanimobile available at VUCH performs most transportations in the
locality of Vilnius city;► A reanimobile available at KMUC runs an greater number of kilometres
during one transportation considering the zone serviced by KMUC, so it shows that KMUC mainly carry babies from outside the city of Kaunas;
► A reanimobile available at KUH runs highest average traveled distance per one neonate transportation due to the hospital location (city of Klaipeda is situated near the Lithuanian border) and the distance from perinatal centers in Vilnius and Kaunas cities.
In the picture below, the comparison of the run made in the reanimobiles for the neonate transportation according to PHCI is presented.
KMUC NC VUCL NC KUH Siauliai PHCI Panevezys PHCI0
10,000
20,000
30,000
40,000
50,000
60,000
Comparison of the run passed made in the reanimobiles for the neonate transportation according to PHCI
Picture No 26 – Comparison of the run made in the reanimobiles for the neonate transportation according to PHCI
Note: There is no possibility to ascertain the number of kilometres passed by Siauliai PHCI and Panevezys PHCI in transporting neonates as these PHCI use
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 115 of 281
R.3. Feasibility study
common reanimobiles to meet the needs of all PHCI for the neonate transportation.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 116 of 281
R.3. Feasibility study
The average number of kilometres passed in the reanimobiles for the neonate transportation available for PHCI (readings of the run of the speedometer) is 85.511,4 km until the first quarter.
VUCH NC can be mostly distinguished from all PHCI as the total number of kilometres run by its reanimobile makes 159.060 km, thus, a reanimobile available at VUCH may be more depreciated than reanimobiles available at other PHCI.
In the picture below, the comparison of reanimobiles for the neonate transportation available at PHCI according to the total number of kilometres run (readings of the run of the speedometer) is presented.
10
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
The total number of kilometres passed in the reanimobiles
km
Picture No 27 – Comparison of reanimobiles for the neonate transportation available for PHCI according to the total number of kilometres run
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 117 of 281
R.3. Feasibility study
6.3 Needs of PHCI for extra reanimobiles or their renewal
In the table below, the needs of PHCI for extra reanimobiles for the neonate transportation or their renewal are presented.
Table 21. Recipients of the data provided by PHCI and the data provided No
PHCI Needs/ remarks
1. Public institution Kaunas Medical University Clinic (neonatal services)
Considering the fact KMUC transports 168 neonates and runs about 41.000 kilometres per year on the average and the medical equipment of the presently available reanimobile for the neonate transportation is morally obsolete, during the first year of the Programme implementation, it is necessary to renew the medical equipment of one reanimobile for the neonate transportation available at KMUC.In the last year of the Programme implementation, it is necessary to buy a new reanimobile for the neonate transportation as the presently available reanimobile will be 9 years old in the last year of the Programme implementation (2017) and following the decision of the Government of the Republic of Lithuania No 564 “On the establishment of the minimal value of property, plant and equipment and approval of the minimum and maximum depreciation (amortization) rates of non-current assets in the public sector“ of 10 June 2009, clause 9.2 “Special cars“ of which indicates that the number of years of depreciation of special cars ranges from 4 to 7, the age of the reanimobile available for KMUC NC in 2017 will exceed 7 years, thus the reanimobile available at KMUC NC will be depreciated in 2017.
2. Public institution Vilnius University Children’s hospital (neonatal services)
Considering the fact that VUCH transports about 621 neonates and runs about 48.000 kilometres per year on the average and the reanimobile for the neonate transportation presently available
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 118 of 281
R.3. Feasibility study
No
PHCI Needs/ remarks
at VUCH was manufactured in 2006, the period of its suitable operation is close to expiry, thus, it is necessary to renew the medical equipment of one reanimobile for the neonate transportation available at VUCH.In the last year of the Programme implementation, it is necessary to buy a new reanimobile for the neonate transportation as the presently available reanimobile will be 9 years old in the last year of the Programme implementation (2017) and following the decision of the Government of the Republic of Lithuania No 564 “On the establishment of the minimal value of property, plant and equipment and approval of the minimum and maximum depreciation (amortization) rates of non-current assets in the public sector“ of 10 June 2009, clause 9.2 “Special cars“ of which indicates that the number of years of depreciation of special cars ranges from 4 to 7, the age of the reanimobile available for KMUC NC in 2017 will exceed 7 years, thus the reanimobile available at KMUC NC will be depreciated in 2017.
3. Public institution Klaipeda University hospital
Presently, the reanimobile available for KUH is used not only for the neonate transportation, but for satisfaction of the needs of the total PHCI, thus, the resources necessary for the neonate transportation are not always satisfied in time.Considering the fact that KUH transports about 83 neonates and runs about 36.000 kilometres per year on the average, KUH needs one reanimobile for the neonate transportation; it is necessary to renew a part of medical equipment which would be remounted from that presently mounted in the reanimobile which is used not only for the neonate transportation, but for satisfaction of the needs of the total PHCI.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 119 of 281
R.3. Feasibility study
No
PHCI Needs/ remarks
4. Public institution Siauliai county hospital
Presently, Siauliai PHCI has a new reanimobile for the neonate transportation manufactured in 2009 which is fully completed and fully satisfies the needs of PHCI.
5. Public institution Panevezys county hospital
Presently, Panevezys PHCI has a new reanimobile for the neonate transportation manufactured in 2008 which is fully completed and fully satisfies the needs of PHCI.
6.4 Alternatives for the satisfaction of the needs for reanimobiles for neonate transportation of PHCI
In the table below, the alternatives for the satisfaction of the needs of PHCI for reanimobiles for neonate transportation are presented.
Table 22. Alternatives for the satisfaction of the needs of PHCI for reanimobiles for neonate transportation
Alternative I Alternative IIIn order to ensure that all PHCI have the necessary resources for a few years ahead with which they will be able to perform safe neonate transportation, the following would be bought for all PHCI below:► During the first year of the
programme implementation:► For KUH – a new reanimobile for
the neonate transportation (without medical equipment).
► For VUCH, KMUC and KUH – medical equipment required in reanimobiles for the neonate transportation.
► During the last year of the programme implementation:► For VUCH and KMUC – new
reanimobiles for the neonate transportation (without medical equipment).
In order to ensure that all PHCI have the necessary resources for a few years ahead with which they will be able to perform safe neonate transportations, the following would be bought for all PHCI below: one new reanimobile with fully completed medical equipment in each (during the first year of the programme):
► VUCH;► KMUC;► KUH;► Siauliai PHCI;► Panevezys PHCI.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 120 of 281
R.3. Feasibility study
Alternative I Alternative IINote: Considering the number of neonates transported by Siauliai PHCI and Panevezys PHCI and the number of kilometres run in transporting neonates, investments would not be assigned to these PHCI within the scope of this alternative.
AdvantagesNew reanimobiles would only be bought for those PHCI the available reanimobiles of which are close to the expiry of their suitable operation (or will be close during the last year of the Programme implementation), and other PHCI, the available reanimobiles of which are not close to the expiry of their suitable operation but have a need for renewal of medical equipment, would get renewed medical equipment mounted in the reanimobiles, thus, the necessary resources for safe neonate transportation would be ensured for PHCI.
All PHCI would have at least one new reanimobile for the neonate transportation which would enable to ensure the necessary resources for safe neonate transportation for PHCI for a few years ahead.
Disadvantages and/or risks- A part of purchased reanimobiles
can be not fully used as the number of neonates transported by Siauliai PHCI and Panevezys PHCI per year on the average is low. Siauliai PHCI transports about 18 neonates and Panevezys PHCI respectively transports about 29 neonates per year on the average.
In the table below, the comparison of the alternatives for satisfaction of the needs of PHCI for reanimobiles for the neonate transportation is presented.
Table 23. Comparison of the alternatives for satisfaction of the needs of PHCI for reanimobiles for the neonate transportation is presented
PHCI Alternative I (Lt with VAT)
Alternative II (Lt with VAT)
Year of purchase 2011 2015 Total 2011 2015 Total
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 121 of 281
R.3. Feasibility study
VUCH 0 100.000 100.000
100.000 0 100.000
KMUC 0 100.000 100.000
100.000 0 100.000
KUH 100.000 0 100.000
100.000 0 100.000
Siauliai PHCI 0 0 0 100.000 0 100.000
Panevezys PHCI 0 0 0 100.000 0 100.000
Total (Lt with VAT): 100.000 200.000 300.000
500.000 0 500.000
Note: ► The prices of reanimobiles (without medical equipment) were ascertained after
interviewing suppliers of reanimobiles on the telephone and striking the statistical average of the prices presented by them. UAB Moller Auto (80.000 LTL with VAT), UAB Autojuta (80.000 LTL with VAT), UAB Baltic Auto (80.000 LTL with VAT) and UAB Silberauto (150.000 LTL with VAT) were interviewed.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 122 of 281
R.3. Feasibility study
In the table below, the list of medical equipment required for the reanimobile for the neonate transportation available at every PHCI is presented.
Table 24. List of medical equipment required for the reanimobile for the neonate transportation available at every PHCIPHCI
Required medical equipment Number
VUCH Defibrillator for newborn 2 1KMUC Transport incubator in the reanimobile 1
Transport monitor 13 syringe infusion pumps 3Vacuum or electrical pump 1Artificial inhalation device 2 1System for support of positive pressure in the airway (CPAP) with a set of nasal canulas of different sizes 2
1
KUH Defibrillator for newborn 2 1Siauliai PHCI - -Panevezys PHCI
- -
Note: ► The medical equipment required for the reanimobile for neonate transportation
is included in the list of medical equipment assigned to each PHCI which is presented in Appendix No 13 to this document.
6.5 Recommendations for satisfaction of the needs of PHCI for reanimobiles for neonate transportation
Considering the advantages and disadvantages of alternative I and alternative II, the need for investments and benefit generated, it is recommended to consider the implementation of alternative I and try to ensure that all PHCI will have the necessary resources for safe neonate transportation for a few years ahead; the following would be bought for all PHCI below:► During the first year of the programme implementation:
► For KUH – a new reanimobile for the neonate transportation (without medical equipment).
► For VUCH, KMUC and KUH – medical equipment required in reanimobiles for the neonate transportation.
► During the last year of the programme implementation:► For VUCH and KMUC – new reanimobiles for the neonate transportation
(without medical equipment).
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 123 of 281
R.3. Feasibility study
Note: ► Considering the number of neonates transported by Siauliai PHCI and
Panevezys PHCI and the number of kilometres run in transporting neonates, and the reanimobiles for the neonate transportation presently available, investments would not be assigned to these PHCI;
► KUH has a reanimobile for the neonate transportation which was manufactured in 2007, but the availability of the reanimobile for KUH twenty-four hours a day or in certain urgent (critical) cases is not ensured because of unresolved organizational issues, thus, when making a decision about assigning a reanimobile for the neonate transportation to KUH, we recommend considering this fact and only assign a reanimobile in case it is not possible to resolve the organizational issues related to the availability of the reanimobile twenty-four hours a day.
6.6 Need for investments in reanimobiles for the neonate transportation
In the table below, the need for investments in reanimobiles for the neonate transportation is presented.
Table 25. Need for investments in reanimobiles for neonate transportation is presented.PHCI Field of investment 2011 2015 Total
VUCH Reanimobile 0 100.000 100.000KMUC Reanimobile 0 100.000 100.000KUH Reanimobile 100.000 0 100.000
Total (Lt with VAT): 100.000 200.000 300.000
Note: If the programme is to be implemented within a shorter period, the respective purchases could be planned prior to 2015.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 124 of 281
R.3. Feasibility study
7. Analysis of methodologies of diagnoses of disease or state and treatment of pregnant women, delivering women and neonates
7.1 Present state of methodologies of diagnoses of disease or state and treatment of pregnant women, delivering women and neonates
In 2003–2004 the research of loss-near cases performed in Lithuanian birth hospitals showed it is necessary to prepare and accept national scientific-based methodologies of diagnoses and treatment of serious pregnancy and birth complications and supplement the Lithuanian newborn registration questionnaire with registration of the most important pregnancy and birth complications.12
While performing the analysis of methodologies and protocols currently available at PHCI during the project, visiting PHCI and performing a questionnaire interview, information about methodologies and protocols currently available at PHCI was collected.
After performing the analysis of methodologies and protocols available at PHCI, it was indicated:
► Protocols and methodologies of the same states were given different names in different PHCI
► Protocols and methodologies were created in different PHCI by following different and sometimes old-fashioned literature and different experience;
► Some PHCI assign procedures and their descriptions to protocols and methodologies.
In order to assess the demand for creation of united methodologies, PHCI were asked to list the most relevant methodologies which should be standardized in their opinion. In Appendix No 5 of this document the demand of each PHCI for standardization of methodologies and their approval at the national level is presented.
7.2 Alternatives of the approval of methodologies of diagnoses of disease or state and treatment of pregnant women, delivering women and neonates at the national level
The performed analysis allows thinking that pregnant women, delivering women and neonates could get more qualitative health care services after creating united methodical guidelines which would be followed by all PHCI.
12 Yearly report of the National Health Coucil, „Health care of pregnant women, delivering women and neonates“, R. Nadišauskienė, M. Minkauskienė, E. Markūnienė, A. Armonavičienė, N. Drazdienė, 2005 m.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 125 of 281
R.3. Feasibility study
In the table below, the alternatives of the approval of methodical guidelines of diagnoses of disease or state and treatment of pregnant women, delivering women and neonates at the national level are presented.
Table 26. Alternatives of the approval of methodifcal guidelines at the national level
Alternative I Alternative IIIn order to ensure even service provision to pregnant women, delivering women and neonates, all presently used methodical guidelines have to be reviewed by the Lithuanian Society of Obstetricians and Gynaecologists and Association of Neonatologists, renewed and approved at the national level.
In order to ensure even service provision to pregnant women, delivering women and neonates, all presently used methodical guidelines have to be reviewed and the most relevant/critical ones, mostly influencing the reasons for patients’ death or pathological cases, have to be approved.
AdvantagesIn case of Alternative I, it would be ensured all PHCI are going to use united methodical guidelines approved at the national level.
In case of Alternative II, only critical methodical guidelines would be approved at the national level. It would ensure efficient use of investments.
Disadvantages/risksThe review and preparation of all used methodologies would require more investments than only in case of preparation of critical methodologies (Alternative II). It would be necessary to intend more human resources for preparation of methodologies.
In case of preparing only the most relevant methodologies, risk of not preparing certain less important methodologies, which can influence loss-near cases, could occur.
Demand for investments2.288.000 Lt with VAT (about 130 methodologies)
1.232.000 Lt with VAT (about 70 methodologies)
Demand for investments assessed on the basis of the following assumptions:
► (P.1) The average rate of a specialist’s workday (including costs of accommodation and alimentation) will be 2.200 Lt13 including all taxes;
► (P.2) On the average, 4 specialists will participate in a review of one methodical recommendation;
13 The average rate of a specialist’s workday was assessed on the basis of the price market analysis: the average hourly rate of an expert is up to 250 Lt including all taxes, costs of accommodation and alimentation per one day is about up to 200 Lt with VAT.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 126 of 281
R.3. Feasibility study
► (P.3) The renewal and approval of one methodical recommendation at the national level will last for two workdays on the average.
► (P.4) In case of Alternative I, it is necessary to review about 130 methodical guidelines (see Appendix No 5);
► (P.5) In case of Alternative II, it is necessary to review about 70 methodical guidelines (38 are applied for obstetrics and 32 are applied for neonatology);
► (P.6) Algorithm used for the assessment: rate of a specialist’s workday*; number of specialists participating in the preparation of methodical guidelines*; duration of the preparation and approval of one methodical recommendation at the national level*; number of methodical guidelines.
7.3 Guidelines for the approval of methodologies of diagnoses of disease or state and treatment of pregnant women, delivering women and neonates at the national level
Considering the advantages and disadvantages of Alternative I and Alternative II and the most efficient use of investments, it is recommended to consider implementation of Alternative II and try to ensure the service provision for pregnant women, delivering women and neonates in its extent and prepare the most relevant/critical methodical guidelines. During the meeting of the representatives of the Lithuanian Society of Obstetricians and Gynaecologists and Association of Neonatologists organized by the Ministry of Health Care on the 7th of June 2010, the list of methodical guidelines was reviewed and the decision on their preparation/succession of priorities was made. The priorities of methodical guidelines were set considering the relevance of methodologies, reasons for patients’ death, likelihood of pathology and uncertainties or ambiguities of presently available methodologies. It is expected to prepare methodical guidelines within 5 years by preparing 6-8 methodical guidelines every year. Protocols of the hospitals providing the obstetric and neonatal services of different levels (IIA, IIB, and III) would be prepared along with the methodical guidelines by the same specialists. The priority lists of methodical guidelines are presented in the Appendices No 11 and No 12 to this document.While preparing and approving methodical guidelines and protocols, it is also recommended:► (R.1) During the preparation of methodical guidelines:
To create united descriptions of operations and procedures and the part of a patient’s agreement along with each methodical guideline;
To include representatives from the Lithuanian Society of Obstetricians and Gynaecologists and Association of Neonatologists and Lithuanian Association of Obstetricians and Lithuanian Organizations of Nursing in the process of preparation of methodical guidelines;
To include doctors-specialists of PHCI providing services of different levels in the process of preparation of methodical guidelines;
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 127 of 281
R.3. Feasibility study
To appoint a specialist working in a perinatal centre and having a scientific and pedagogical degree project head of the creation of methodical guidelines;
To include 3-5 specialists in the group of the review/renewal or preparation of methodical guidelines and protocols;
To intend 2-3 workdays for the creation or review/renewal of a methodical guideline;
To pay specialists participating in the preparation/review of methodical guidelines and protocols the payment of the average workday wage multiplied by the coefficient ranging from 1.5 to 3 considering the qualification of a specialist.
► (R.2) Approval of methodical guidelines. In order to ensure all hospitals providing services for pregnant women, delivering women and neonates observe the same methodologies, it is recommended to approve them following the law of the Minister of Health Care „On the approval of the order of health care of pregnant women, delivering women and neonates“ (15 th of March 1999 No117) and by supplementing it with necessary provisions.
► (R.3) Practical implementation of methodical guidelines. In order to ensure the methodical guidelines and protocols approved at the national level are observed, it is recommended to distribute them in the websites of the Lithuanian Society of Obstetricians and Gynaecologists and Association of Neonatologists of the Ministry of Health Care. It is recommended the national audit institution validates the observation of methodical guidelines.
► (R.4) Review/renewal of methodical guidelines. It is proposed to review and renew prepared methodical guidelines and protocols every 4-5 years, if necessary.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 128 of 281
R.3. Feasibility study
8. Analysis of the qualification of human resources
8.1 Analysis of the qualification of the employees of PHCI
8.1.1 Methods of analysis of the qualification of the employees of PHCI When assessing weaknesses of the qualification of the staff, the following sources of information were used:
► Research of the assessment of services provided to pregnant women, delivering women and neonates by stationary personal health care institutions within the scope of the project;
► Need for trainings indicated in the questionnaire of PHCI;► Scientific research by Meile Minkauskiene about cases close to loss;► Scientific research by Janina Ribeliene ”Relations of the satisfaction of
patients with services provided by the birth hospital with the implementation of the initiative of a neonate-friendly hospital of WHO/UNICEF“;
► Information and examples provided by the staff during visits to PHCI.
During the performed research, the satisfaction of patients with provided services, work of the staff and conditions were researched: before the birth, during the birth and after the birth. During the research, conclusions were drawn related to the lack of qualification of the staff:
► Prenatal pregnancy care. Patients indicated two main drawbacks – insufficient gynaecological care and casual attitude of the gynaecologist; they often lack information about provided services.
► Consulting room. Those patients who are less satisfied with services in the consulting room mostly lack pleasant communication, understanding (55%), expedition (19%) and information.
► Birth. Women tend to positively assess the competence and attention of the staff having participated during the birth; however, it is to note that the attention of the staff is assessed a little worse than its competence. Obstetricians and neonatologists got the highest assessments in respect of competence and attention; anaesthesiologists and nurses are assessed relatively worse in these aspects. Most delivering women were satisfied with the services provided during the birth, but they would like to get more information, explanations about occurring processes, more attention and care.
► Postnatal care. The competence of the postnatal care staff is assessed quite positively. Women have the best opinion about the competence of the neonatologist responsible for the care and observation of the neonate. Nurses are assessed relatively worst in this aspect.
After being asked what is required for the assessment of provided services to be better, the respondents answered that they needed more attention,
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 129 of 281
R.3. Feasibility study
communication and support from the staff of PHCI. The same things are accentuated in the articles by Dr. Meile Minkauskiene: „Knowing that the pregnancy is developing normally and that the emerging questions will be answered is more important. Thus, conversations with the pregnant woman about all issues she is interested in, provision of information about how to live, eat, do sports, make love and prepare for successful birth are becoming a more and more important part of visits taking more and more time.“
Picture No 28 – Results of the survey of the drawbacks of the provided services (opinion of patients)
During the research, it was also noticed that delivering women had a lack of information about postnatal care including natural nursing: 39% respondents answered they were not provided any information about the advantages of nursing at all or it was not comprehensive. It is noted in the recommendations of WHO „Health for everybody in the XXI century“ the encouragement and support of nursing of babies is very important for healthy beginning of a person’s life.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 130 of 281
R.3. Feasibility study
Information about nursing advantages for the neonate and mother
Information about your personal hygiene after giv-ing birth
Information about vaccinations and tests performed for your neonate
Advertising material about bottle-feeding, diapers, neonate insurance
Information about correct nursing
Information about breast careInformation about the indications of sufficient feed-ing of a neonate (peculiarities of bowel movement,
frequency; frequency of urination, etc.)Information about neonate reflexes
Information about the sleeping peculiarities of a neonate
Information about mutual help groups "Mother to mother" and contact information
31
29
29
28
27
26
19
18
14
9
31
38
37
31
35
32
28
26
23
11
18
19
20
20
22
25
23
27
27
18
6
4
9
5
6
6
9
9
9
8
15
9
5
15
9
10
21
20
28
54
Very detailed Detail Not enough detail Incomplete Information has not been provided
Picture No 29 – Results of the survey of information provided for patients
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 131 of 281
R.3. Feasibility study
8.2 Analysis of trainings for the staff of PHCI On the average, 47% of the employees of PHCI providing obstetric-gynaecological services of the III-level have participated in Internships in Lithuania at least once in the last two years14. Meanwhile, the average percentage of employees of PHCI providing services of the same level who have participated in Internships abroad made 12% of all employees.
On the average, 44% of the employees of PHCI providing obstetric-gynaecological services of the III-level have participated in trainings at least once in the last two years.
In the picture below, the comparison of PHCI providing the III-level services according to the staff trainings is presented.
KMUC COG KMUC NC VCUH COG VUCL NC0
20
40
60
80
100
120
140
160
180
200
Comparison of PHCI providing the III-level services according to the staff trainings
14Training is refreshment of knowledge, improvement of qualification, self-education, practice when leaving somewhere (for example, abroad for studies), working for another organization or overall starting to work somewhere in order to obtain competences necessary for a certain activity or position.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 132 of 281
R.3. Feasibility study
Picture No 30 – Comparison of PHCI providing the III-level services according to the staff trainings
On the average, 40% of the employees of PHCI providing obstetric-gynaecological services of the IIA and IIB-level have participated in Internships in Lithuania at least once in the last two years15. Meanwhile, the average percentage of employees of PHCI providing services of the same level who have participated in Internships abroad made 3% of all employees.
On the average, 60% of the employees of PHCI providing obstetric-gynaecological services of the III-level have participated at trainings at least once in the last two years.
In the picture below, the comparison of PHCI providing the IIA and IIB-level services according to the staff trainings is presented.
VUHSCCF KUH
Vilnius maternity h
ome
Kaunas 2-nd CH
Siauliai P
HCI
Panevezys P
HCI
0102030405060708090
100Comparison of PHCI providing the IIA and IIB-level services according to the staff trainings
15Training is refreshment of knowledge, improvement of qualification, self-education, practice when leaving somewhere (for example, abroad for studies), working for another organization or overall starting to work somewhere in order to obtain competences necessary for a certain activity or position.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 133 of 281
R.3. Feasibility study
Picture No 31 – Comparison of PHCI providing the IIA and IIB-level services according to the staff trainings
KONFIDENCIALU document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 134 of 281R.3. Feasibility study
On the average, 32% of the employees of PHCI providing obstetric-gynaecological services of the IIA and IIB-level have participated in Internships in Lithuania at least once in the last two years 16. Meanwhile, the average percentage of employees of PHCI providing services of the same level who have participated in Internships abroad made 2% of all employees.
On the average, 49% of the employees of PHCI providing obstetric-gynaecological services of the III-level have participated at trainings at least once in the last two years.
In the picture below, the comparison of PHCI providing the IIA-level services according to the staff trainings is presented.
P.Mazylio maternity home
Alytus PHCI
Telsiai PHCI
Utena PHCI
Mazeikiai PHCI
Radviliskis PHCI
Visaginas PHCI
Kedainiai PHCI
Salcininkai PHCI
Lazdijai PHCI
Vilkaviskis PHCI
Svencionys PHCI
01020304050607080
1
32
12
34
8
25
0
24
1 0 0 010
0
19
0
1119
0 010
1
18
2 0 05
0 0 0 1 3 0 1 0 0 0 1 0 0 0 0 0 0 0 0
72
0 0
56
9 712
0
2010
1623
31
14
0
40
0
26
15
1 0
16
0
Comparison of PHCI providing the IIA-level services according to the staff trainings
Number of employees who participated in an internship in Lithuania at least once during the last two years
Picture No 32 – Comparison of PHCI providing the IIA-level services according to the staff trainings16Training is refreshment of knowledge, improvement of qualification, self-education, practice when leaving somewhere (for example, abroad for studies), working for another organization or overall starting to work somewhere in order to obtain competences necessary for a certain activity or position.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 135 of 281
R.3. Feasibility study
8.3 Need for trainings of the staff of PHCI In the picture below, the comparison of PHCI providing the III-level services according to the need for the staff trainings is presented.
KMUC COG KMUC NC VCUH COG VUCL NC0
20
40
60
80
100
120
140
160
Comparison of PHCI providing the III-level services according to the need for the staff trainings
Picture No 33 – Comparison of PHCI providing the III-level services according to the need for the staff trainings
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 136 of 281
R.3. Feasibility study
In the picture below, the comparison of PHCI providing the IIA and IIB-level services according to the need for the staff trainings is presented.
VUHSCCF KUH
Vilnius mate
rnity home
Kaunas 2-nd CH
Siauliai
PHCI
Panevezys
PHCI0
20
40
60
80
100
120
Comparison of PHCI providing the IIA and IIB-level services according to the need for the staff trainings
Picture No 34 – Comparison of PHCI providing the IIA and IIB-level services according to the need for the staff trainings
KONFIDENCIALU document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 137 of 281R.3. Feasibility study
In the picture below, the comparison of PHCI providing the IIA-level services according to the need for the staff trainings is presented.
P.Mazylio maternity home
Alytus PHCI
Telsiai PHCI
Utena PHCI
Mazeikiai PHCI
Radviliskis PHCI
Visaginas PHCI
Kedainiai PHCI
Salcininkai PHCI
Lazdijai PHCI
Vilkaviskis PHCI
Svencionys PHCI
0
10
20
30
40
50
60
Comparison of PHCI providing the IIA-level services according to the need for the staff trainings
KONFIDENCIALU document.docx

Ministry of Health of the Republic of LithuaniaPreparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in
Lithuanian hospitals, including implementation of energy-sparing technologies Page 138 of 281R.3. Feasibility study
Picture No 35 – Comparison of PHCI providing the IIA-level services according to the need for the staff trainings
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 139 of 281
R.3. Feasibility study
Presently in Lithuania the staff of PHCI is mostly trained according to international training programmes existing in Lithuania, for example, BLSO, ALSO, STABLE. Trainings are delivered by certified trainers (having passed examinations) who often have international experience. Participants of trainings have to take examinations testing the level of the knowledge assimilation. However, it was established during the visits to PHCI that there is a lack of funding for PHCI to constantly refresh the knowledge and skills of the staff.
8.4 Need for investments in the organization of trainings for the staff of PHCI
8.4.1 Prices of trainingsDuring the project, potential service providers were interviewed on the telephone. In the table below, the prices of trainings indicated by the training service providers according to the training programmes are presented. The prices are indicated excluding VAT.
Table 27. Prices of trainings according to the training programmes
No
Training programme
Price per person for one training programme indicated by the training service provider
Statistical mean of indicated training
prices per person for
one training
programme
UAB“Kriziu tyrimo centras
”
Public institution
“Nacionalinis
medicinos mokymų centras”
KMU, faculty
of post-
diploma
studies
UAB “Zmogaus studiju centras”
UAB “Person premier
“
1. Reanimation of neonates
1,950 - - - - 1,950
2. Modern specialized obstetric help
2,250 2,400 - - - 2,325
3. Stabilization of the state of neonates and preparation for transportation
2,450 2,400 2,120 - - 2,323
4. Conflict management and communication with patients
- - - 630 500 565
5. Modern primary obstetric help17
1,950 - - - - 1,950
17 These trainings would involve the topics of normal pregnancy, normal birth and the postnatal period including aspects of natural feeding (nursing), thus, it is recommended to choose trainings with wider topics and not exclude a possibility to announce an international public procurement and obtain the training services of foreign experts.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 140 of 281
R.3. Feasibility study
The need of investments in conferences was assessed according to the assumptions made on the basis of the experience of medical experts and norms set in the laws of the Republic of Lithuania18:► Registration fee of the conference – about 2.100 LTL with VAT (i.e., about 500
EUR without VAT);► Travel costs – about 1.000 LTL with VAT;► The conference would last for 3 days on the average with of a possibility to
visit 1-2 hospitals during the conference (subject to an agreement in advance);
► Accommodation costs (hotel and catering) – about 800 LTL with VAT per day (i.e., about 230 EUR per day with VAT).
According to the assumptions above, the price of one conference per person would make: about 5.500 LTL with VAT.
The need for investments in Internships abroad was assessed according to the assumptions made on the basis of experience of medical experts and norms set in the laws of the Republic of Lithuania:► Travel costs – about 1.000 LTL with VAT;► The Internship would last for 2 weeks (14 days) on the average;► Accommodation costs (hotel and catering) – about 800 LTL with VAT per day
(i.e., about 230 EUR per day with VAT).
According to the assumptions above, the price of one Internship per person would make: about 12,200 LTL with VAT.
The need for investments in Internships in Lithuania was assessed according to the assumptions made on the basis of the experience of medical experts and analysis of the price market:► The Internship would last for 2 weeks (14 days) on the average);► Accommodation costs (hotel and catering) – about 300 LTL with VAT per day.
According to the assumptions above, the price of one Internship per person would make: about 4,200 LTL with VAT.
18 Order No 116 of the Minister of Finance of the Republic of Lithuania of 21 November 1996 (edition of the Order No 1K-123 of the Minister of Finance of the Republic of Lithuania of 1 April 2008)
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 141 of 281
R.3. Feasibility study
8.5 Alternatives of the organization of trainings for the staff of PHCI
In the table below, the alternatives of the organization of trainings for the staff of PHCI providing obstetric-gynaecological services are presented.
Table 28. Alternatives of the organization of trainings for the staff of PHCIAlternative I Alternative II
In order to ensure that the staff of PHCI has suitable qualification to provide quality services to pregnant women, delivering women and neonates and follow the principle „train the trainer“, trainings for the staff of PHCI would be organized not for the total staff of one PHCI but for a certain part of the staff of PHCI. In case of this alternative, the trained staff of PHCI would get more and various trainings and knowledge , thus, they would be able to share them later with the staff of PHCI who did not participate in the trainings.
In order to ensure that the staff of PHCI has suitable competence to provide quality services to pregnant women, delivering women and neonates, trainings for the staff of PHCI would be organized for a much bigger part of the staff of every PHCI than in alternative I, but they would only include certain trainings on the highest priority topics established according to the conclusions drawn from the survey of patients, in the need expressed by PHCI, scientific researches and proposal of associations:► Trainings of reanimation of
neonates;► Natural feeding (nursing);► Conflict management and
communication with patients.Note: If there is lack of funds for the training of employees of all PHCI on the highest priority topics within the scope of this alternative, the needs of PHCI providing services of a lower level would be satisfied first.
AdvantagesIn this alternative, the trained staff of PHCI would get more and various trainings and knowledge, thus, they would be able to later share them with the staff of PHCI who did not participate in the trainings.
In alternative II, it would be ensured that the staff of PHCI would get the most important and concentrated theoretical and practical knowledge.
Disadvantages
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 142 of 281
R.3. Feasibility study
Alternative I Alternative II
In alternative I, a risk can emerge not all “trainers” will have sufficient skills to train the staff of PHCI who did not participate in the trainings.
In alternative II, the trained staff would only get certain trainings of the highest priorities, thus, universal improvement of qualification would not be ensured.
InvestmentsIn this alternative, the assumptions must be made what part of specialists should be trained. These assumptions are described in the following chapter. Considering the collected data about the prices of available trainings, the total need for investments would make 4,251.000 LTL.
The following number of specialists should be trained:► Trainings of reanimation of neonates
- 1351;► Natural feeding (nursing) - 1080;► Conflict management and
communication with patients - 1669.
Considering the collected data about the prices of available trainings, the total need for investments would make 6,877.540 LTL.
8.6 Recommendations for the organization of trainings for the staff of PHCI
In order to choose the alternative which would mostly comply with the needs of specialists, a meeting with representatives of the Lithuanian Community of Obstetricians-Gynaecologists and Neonatal Association (hereinafter – Associations) was organized on 14t June 2010. During this meeting, methods/measures for the improvement of professional qualification were analyzed:
► Trainings:► Internships, exchanges of specialists;► Conferences (in Lithuania, abroad);► Purchase and/or subscription of books, magazines and other publications.
During the meeting, the participants agreed with the proposed measures of trainings except the development of electronic training environment for trainings in a distant way and organization of a conference in Lithuania because of an insufficiently efficient training method. We would also like to note that after realizing means of information technologies for certain trainings which do not require practical experiments, a risk emerges that those PHCI where staff is older and does not have suitable knowledge for work with information technologies or
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 143 of 281
R.3. Feasibility study
where there are not enough computerized workstations will not be able to use the means of information technologies for trainings.The representatives of the associations supported the organization of Internships from PHCI providing obstetric-gynaecological services of a lower level to PHCI providing obstetric-gynaecological services of a higher level would enable the staff of PHCI to practically familiarize themselves with the methods of work used by PHCI providing obstetric-gynaecological services of a higher level and more complicated cases of illnesses/treatment. Meanwhile, Internships at foreign PHCI with good practice should be organized for specialists of perinatal centres, which would ensure a possibility to practically familiarize themselves with the methods of work used by foreign PHCI with good practice and more complicated cases of illnesses/treatment. A need for 4 Internships was expressed – two for Vilnius and Kaunas perinatal centres each.In order to improve the professional qualification, trips to conferences on the issues which are the most essential for the staff of PHC should be organized. According to the expert assessment, trips to conferences where papers on the following topics are read would be the most useful:
► Healthy neonate, his/her care;► Care, nursing, feeding of a premature neonate;► Intensive therapy of neonates;► Care and birth physiology of a pregnant woman;► Peculiarities of multifoetus pregnancy;► Foetus surgery in cases of (monofoetus and multifoetus) pregnancy.
Considering the fact that libraries presently have enough necessary literature, the purchase and/or subscription of books, magazines and other publications was not approved.During the meeting, the list of trainings compliant with the needs of the staff of PHCI was presented and discussed (see table below).
Table 29. Description of trainings for the staff of PHCI No
Name Description
1. Reanimation of neonates
These trainings are intended for obtaining and strengthening practical skills necessary when providing urgent medical help to neonates. Duration of trainings: about 2 days. Purpose of trainings: to learn to practically provide urgent medical help to neonates.Tasks of trainings:
► To obtain and improve an ability of fast assessment of the state of the neonate;
► To obtain and improve practical skills for reanimation of the neonate;
► To learn to recognize dangerous states of
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 144 of 281
R.3. Feasibility study
No
Name Description
neonates (respiration insufficiency, heart insufficiency, shock etc.);
► To learn to practically provide help, stabilize the state of the neonate after reanimation.
Training for all obstetric and neonatal services, providing specialist.
2. Modern primary obstetric help
These trainings are intended for obtaining and improving practical skills.Duration of trainings: about 3 days. Purpose of trainings: to learn the main skills for assessment of the state and care of the pregnant woman, foetus and delivering woman in case of normal pregnancy, birth, postnatal period; to provide efficient help in cases of the most frequent situations dangerous to the woman and foetus’s life when working in a team with medical specialists of other fields. Tasks of trainings:
► To learn to assess risk in the perinatal period;► To obtain and improve the skills for care of
pregnant women, delivering in case of normal pregnancy, birth, postnatal period;
► To learn to assess the state of the neonate (health neonate);
► To learn the principles of natural feeding (nursing) and means for its encouragement among patients;
► To familiarize with acute states emerging during the pregnancy and birth and possible complications;
► To learn to practically provide efficient help in cases of the most frequent situations dangerous to the woman and foetus’s life.
Training for all obstetric and neonatal services, providing specialist.
3. Stabilization of the state of neonates and preparation for transportation
These trainings are intended for obtaining and improving practical skills necessary to diagnose and provide help in cases of acute states of neonates during the primary period in the hospital. During these trainings, it should be taught to diagnose the main syndromes of respiration, blood circulation, consciousness disorders and provide help in the main cases of respiration, blood circulation and consciousness disorders, stabilize the state of the neonate after
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 145 of 281
R.3. Feasibility study
No
Name Description
reanimation and organize transportation.Duration of trainings: about 2 days.Purpose of trainings: to learn to provide specialized medical help in cases of situations dangerous to the neonate’s life in time and efficiently.Tasks of trainings:
► To obtain the skills for using protocols of care when assessing the state of the neonate;
► To learn to stabilize the state of the neonate after reanimation;
► To obtain and improve practical skills for stabilizing the state of the neonate after reanimation and organizing transportation;
► To learn to stabilize the state of the neonate following these criteria of assessment: sugar, temperature, airway, blood pressure, laboratory examinations and emotional support;
► To encourage professional responsibility when working in a team.
Training for children's nurses, doctors, neonatologists and pediatric physicians (paediatricians), and, as needed, providing obstetric services professionals.
4. Modern specialized obstetric help
These trainings are intended for obtaining practical skills necessary in cases of acute obstetric states.Duration of trainings: about 2 days. Purpose of trainings: to teach the main practical help provision skills and efficient work in a team with medical specialists of other fields providing help for pregnant women and delivering women, in cases of acute obstetric states.Tasks of trainings:
► To learn to assess risk in the perinatal period;► To familiarize oneself with acute states emerging
during the pregnancy and birth and possible complications;
► To improve help provision in cases of acute obstetric states;
► To learn to practically provide efficient help in case of bleeding during the pregnancy, premature birth, pathology of the birth activity, wrong presentation, foetus hypoxy, multifoetus pregnancy, shoulder dystocia, bleeding during the
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 146 of 281
R.3. Feasibility study
No
Name Description
postnatal period.Training for doctors and midwives and obstetricians and gynecologists, as needed, providing specialist neonatal services.
5. Conflict management and communication with patients
During these trainings, it should be taught to apply means for conflict and stress management, understand patients, speak in a “language of values”, obtain the skills of efficient communication and constructive solution of problems.Duration of trainings: about 2 days.Purpose of trainings: to be able to protect oneself from a harmful impact of stress while providing urgent obstetric help and help the delivering woman sensitively and with qualification.Tasks of trainings:
► To learn to recognize stressors mostly occurring at work;
► To learn to recognize the own reactions and dominating behaviour during the stress;
► To learn to apply efficient methods of stress reduction;
► To learn to recognize cases of a psychological crisis among colleagues, patients and their family members and practically apply the basics of crisis intervention in cases of psychological crises;
► To learn to apply efficient principles of conflict resolution at work;
► To obtain practical skills how to tell somebody painful news in case of loss ethically and by causing as little pain as possible.
Training for all obstetric and neonatal services, providing specialist.
6. Natural feeding (nursing)
During these trainings, the principles of natural feeding (nursing) and means for its encouragement among patients should be taught. Duration of trainings: about 1 day.Training for all obstetric and neonatal services, providing specialist.
7. Trainings for the staff of a neonate-favourable
During these trainings, measures of the programme about nursing and its support should be taught to implement which are indicated in the Order No V-613 of the Minister of Health of the Republic of Lithuania „On
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 147 of 281
R.3. Feasibility study
No
Name Description
hospital the approval of the temporary rules of assessment of stationary personal health care institutions following the requirements for a neonate-friendly hospital “ (edition in force) of 27 August 2004.Duration of trainings: about 2 days.Training for all obstetric and neonatal services, providing specialist.
8. Use of new medical equipment
During these trainings, it should be taught to use specialized medical equipment obtained and implemented within the scope of the Project.Duration of trainings: it would depend on the particularity of medical equipment.Training for all obstetric and neonatal services, providing specialist.
During the meeting, the participants consented to the proposed trainings except trainings for the staff of a neonate-favourable hospital, as the participants think PHCI themselves should assign funding to these trainings. The representatives of the associations confirmed a big need for improvement of the skills of communication between the staff of PHCI and patients by organizing trainings oriented towards clinical processes for the staff of PHCI and psychological trainings which could improve the skills of communication between the staff and patients (for example, conflict and stress management, empathy and emotional intellect).After consulting with possible suppliers of medical equipment after the meeting, it was ascertained that a short training on the use of medical equipment is usually included in the price of medical equipment, thus, it was decided not to fund separate trainings within the scope of the Programme.The representatives of the associations also consented to the training principle „train the trainer” which enables performing trainings for the biggest part of specialists providing services for pregnant women, delivering women and neonates. During the meeting, the participants agreed that the biggest effect could be reached in this approach.In order to ensure refreshment of knowledge and continuation of trainings, the representatives of the associations consented to the idea to obligate the heads of PHCI providing obstetric and neonatal services to ensure staff trainings every 3-5 years in the updated order of the Minister of Health regulating perinatal care in Lithuania. It should be controlled by prolonging the licence of activity of PHCI and the licence of speciality activity of the staff.
Considering the decisions made during the meeting and advantages and disadvantages of alternative I and alternative II and need for investments, it is recommended:
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 148 of 281
R.3. Feasibility study
► (R.1) To consider the implementation of alternative I by organizing trainings based on the principle “train the trainer”;
► (R.2) To organize trainings according to the programmes existing in Lithuania and/or by inviting foreign specialists on the following topics:
► Neonatal resuscitation;► Modern primary obstetric assistance (including natural feeding (nursing));► Stabilization of the state of neonates and preparation for transportation;► Modern specialized obstetric assistance;► Conflict management and communication with patients.
► (R.3) To organize Internships for the staff of PHCI providing obstetric-gynaecological services of the IIA or IIB-level to PHCI providing obstetric-gynaecological services of a higher level.
► (R.4) To organize Internships for the staff of perinatal centres to foreign PHCI of good practice. Cooperate with foreign partners (eg, Swiss universities and hospitals). To plan participation in conferences, too.
► (R.5) Participants of trainings should be examined after completing the training course in order to get the biggest benefit.
► (R.6) Purchases of training services could be performed locally and internationally in order to attract the best specialists to train according to the recommended programmes compliant with the needs of PHCI.
► (R.7) To update the Order of the Minister of Health Care and obligate the heads of PHCI providing obstetric and neonatal services to ensure that staff trainings are organized every 3-5 years. It should be controlled by prolonging the licence of activity of PHCI and the licence of the specific professional activity of the staff.
► (R.8) In case of a possibility, to link Programme trainings to prepared guidelines and protocols considering training topic.
8.6.1 Detailed assessment of investments in order to satisfy the needs of PHCI for trainings
While defining the assumptions for assessment of investments in the improvement of qualification of PHCI, the following principles of the Programme were followed:► The Programme has to decrease the separation between the city and
periphery PHCI;► While planning investments in the improvement of qualification of the staff,
special attention should be paid to trainings of obstetricians and children’s nurses.
After supporting the assumption that the most efficient method of training would be based on the principle “train the trainer” with interested parties (representatives of the Ministry of Health, associations, other experts), a part of staff was defined which could be trained in each PHCI. Trained specialists should undertake to present to their colleagues the material learned after returning to
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 149 of 281
R.3. Feasibility study
their PHCI and demonstrate the practical skills learned (as much as possible with the available means).
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 150 of 281
R.3. Feasibility study
Table 30. Part of specialists recommended to trainLevel of services
provided by PHCI
Part of obstetricians and nurses recommended to
trainPart of other specialists recommended to train
IIA 60% 30%IIB 50% 25%III 40% 20%
The need for trainings was reassessed according to the mean of trainings of PHCI providing services of the same level for those PHCI (Kaunas 2nd clinical hospital, Taurage and Mazeikiai PHCI) which expressed a big need for trainings compared with other PHCI but did not indicate trainings as the activity of immediate necessity, i.e., first priority during the interview.
Not all PHCI expressed the need for trainings on conflict management and communication with patients during the survey; however, after analyzing the main expectations of patients and things which should be improved according to their proposals, it was decided to organize these trainings with the support of the associations. It is recommended to train at least 50-60% of all specialists who communicate with patients and can have a big influence on their satisfaction with provided services.
Following these assumptions, the number of necessary trainings and other means for improvement of qualification according to positions was assessed by separately distinguishing reserve PHCI (see table below).
Table 31. Part of specialists recommended to train according to their positionsNo Position Number of
specialistsPart of specialists
with improved qualification*, %
All PHCI
Excluding reserved
PHCI
All PHCI
1 Children’s nurse (nurse) 513 488 95.13
2 Obstetrician 598 514 85.953 Neonatologist 154 143 92.864 Obstetrician-
gynaecologist377 312 82.76
5 Doctor of children’s diseases (paediatrician)
124 70 56.45
Total 1,766 1,527 86.47
A detailed list with the number of trainings and other means for the improvement of qualification according to positions and each PHCI is presented in the table below. Reserve PHCI not subject to funding within the scope of this Programme are marked grey in the list.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 151 of 281
R.3. Feasibility study
*Remark: shows the percentage of personnel of the main PHCIs who will participate in the trainings compared to personnel of all PHCIs who could participate in the trainings.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 152 of 281
R.3. Feasibility study
Table 32. Need for investments in the improvement of qualification of the staff of PHCI
No PHCI
Structure of staff
Neonatal resuscitatio
n
Modern specialize
d obstetric assistanc
e
Modern primary obstetric assistanc
e
Stabilization of the state of
neonates and
preparation for
transportation
Conflict manageme
nt and communication with patients
Internship
abroad
Internship in
LithuaniaConferen
ces
Number of people who will improve
their qualificat
ion
1 2 3 4 5 6 7 8 9IIA, IIB and III and/or perinatal centres 1 KMUC COG Children’s nurse (nurse) 0 0 0 0 0 0 0 0 0 0 Obstetrician 84 34 10 28 0 50 0 0 3 125 Neonatologist 0 0 0 0 0 0 0 0 0 0 Obstetrician-gynaecologist 55 8 8 0 0 33 1 0 3 53
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
2 KMUC NC Children’s nurse (nurse) 121 48 0 48 48 73 0 0 3 220 Obstetrician 0 0 0 0 0 0 0 0 0 0 Neonatologist 26 5 0 5 5 16 1 0 3 35 Obstetrician-gynaecologist 0 0 0 0 0 0 0 0 0 0
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
3 VMUH COG Children’s nurse (nurse) 33 13 13 12 0 20 0 0 0 58 Obstetrician 63 24 22 24 0 38 0 0 3 111 Neonatologist 14 3 3 2 0 8 0 0 0 16 Obstetrician-gynaecologist 41 8 9 9 11 25 1 0 3 66
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
4 VUCH NC Children’s nurse (nurse) 71 28 0 28 28 43 0 0 3 130 Obstetrician 0 0 0 0 0 0 0 0 0 0 Neonatologist 24 5 0 5 5 14 1 0 3 33 Obstetrician-gynaecologist 0 0 0 0 0 0 0 0 0 0
Doctor of children’s diseases (paediatrician)
12 2 0 2 2 7 0 0 0 13
IIA, IIB 5 VUHSCCF Children’s nurse (nurse) 8 4 0 4 0 5 0 0 0 13 Obstetrician 15 8 8 8 0 9 0 1 0 34 Neonatologist 7 2 0 2 2 4 0 0 0 10 Obstetrician-gynaecologist 16 4 0 0 4 10 0 1 0 19
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
6 KUH Children’s nurse (nurse) 23 6 8 8 5 14 0 1 0 42 Obstetrician 47 0 23 0 20 28 0 2 0 73 Neonatologist 10 3 1 1 3 6 0 1 0 15 Obstetrician-gynaecologist 14 0 4 0 0 8 0 1 0 13
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
7 Vilnius maternity home Children’s nurse (nurse) 26 5 0 7 2 16 0 1 0 31 Obstetrician 37 4 8 10 4 22 0 2 0 50 Neonatologist 8 1 0 2 2 5 0 0 0 10 Obstetrician-gynaecologist 18 1 1 5 1 11 0 1 0 20
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
8 Kaunas 2nd clinical hospital Children’s nurse (nurse) 10 2 2 2 2 6 0 1 0 15 Obstetrician 22 5 5 5 5 13 0 1 0 34 Neonatologist 6 0 0 0 0 4 0 0 0 4 Obstetrician-gynaecologist 8 2 2 2 2 5 0 0 0 13
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
9 Siauliai PHCI Children’s nurse (nurse) 39 20 0 0 20 23 0 2 0 65 Obstetrician 57 19 19 19 19 34 0 3 0 113 Neonatologist 9 2 0 0 2 5 0 0 0 9 Obstetrician-gynaecologist 24 5 5 5 5 14 0 1 0 35
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
10
Panevezys PHCI
Children’s nurse (nurse) 29 7 7 0 0 17 0 1 0 32 Obstetrician 30 5 15 0 0 18 0 2 0 40 Neonatologist 6 2 2 0 0 4 0 0 0 8 Obstetrician-gynaecologist 19 5 5 0 0 11 0 1 0 22
Doctor of children’s diseases (paediatrician)
10 0 0 0 0 6 0 1 0 7
KONFIDENCIALU document.docx
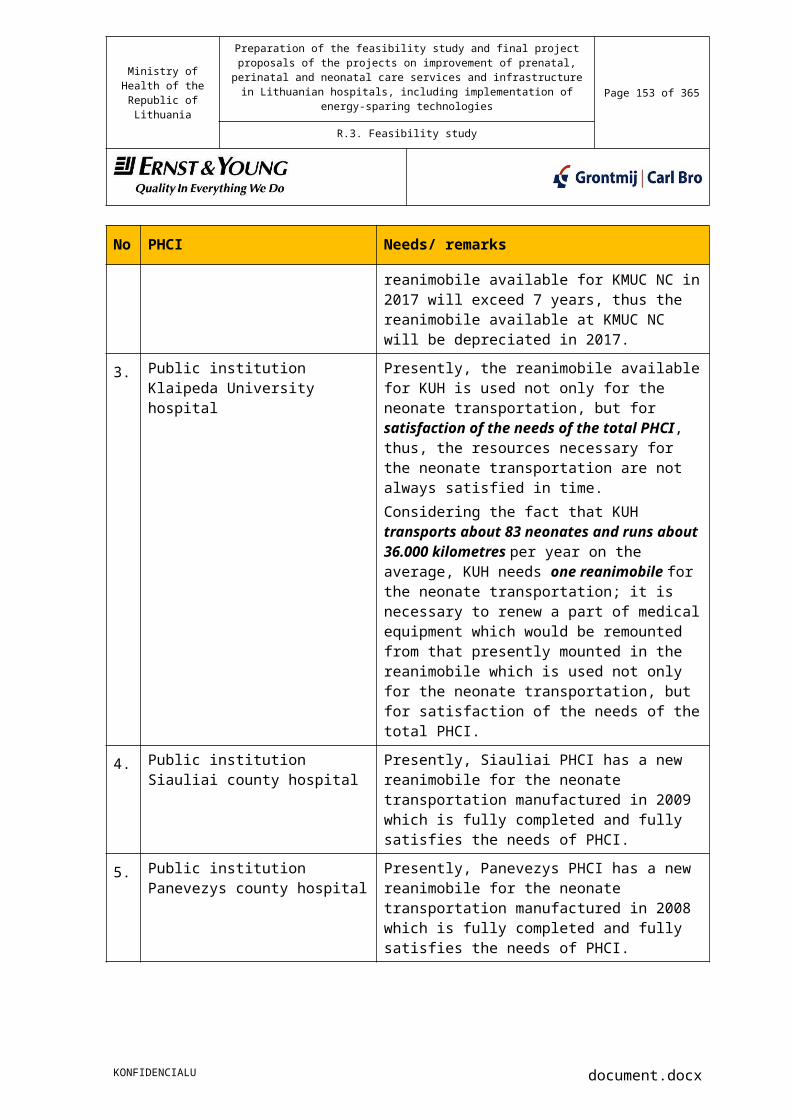
Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 153 of 281
R.3. Feasibility study
No PHCI
Structure of staff
Neonatal resuscitatio
n
Modern specialize
d obstetric assistanc
e
Modern primary obstetric assistanc
e
Stabilization of the state of
neonates and
preparation for
transportation
Conflict manageme
nt and communication with patients
Internship
abroad
Internship in
LithuaniaConferen
ces
Number of people who will improve
their qualificat
ion
1 2 3 4 5 6 7 8 9IIA 11 P.Mazylio maternity home
Children’s nurse (nurse) 26 4 0 4 2 16 0 1 0 27 Obstetrician 18 3 3 11 1 11 0 1 0 30 Neonatologist 4 1 0 0 0 2 0 0 0 3 Obstetrician-gynaecologist 18 2 1 1 1 11 0 1 0 17
Doctor of children’s diseases (paediatrician)
7 1 0 0 0 4 0 0 0 5
12 Christian maternity home
Children’s nurse (nurse) 13 6 0 6 0 8 0 1 0 21 Obstetrician 15 9 9 9 0 9 0 1 0 37 Neonatologist 4 1 0 1 0 2 0 0 0 4 Obstetrician-gynaecologist 13 2 2 2 1 8 0 1 0 16
Doctor of children’s diseases (paediatrician)
3 1 0 1 0 2 0 0 0 4
13 Alytus PHCI
Children’s nurse (nurse) 5 0 0 0 0 3 0 0 0 3 Obstetrician 22 0 6 6 0 13 0 1 0 26 Neonatologist 3 0 0 0 0 2 0 0 0 2 Obstetrician-gynaecologist 8 0 0 0 0 5 0 0 0 5
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
14 Marijampole PHCI
Children’s nurse (nurse) 27 4 2 14 5 16 0 1 0 42 Obstetrician 12 7 7 7 7 7 0 1 0 36 Neonatologist 2 1 1 1 1 1 0 0 0 5 Obstetrician-gynaecologist 8 2 2 2 2 5 0 0 0 13
Doctor of children’s diseases (paediatrician)
11 1 0 1 1 7 0 1 0 11
15 Telsiai PHCI
Children’s nurse (nurse) 6 1 0 1 1 4 0 0 0 7 Obstetrician 15 6 3 0 4 9 0 1 0 23 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 8 2 2 1 2 5 0 0 0 12
Doctor of children’s diseases (paediatrician)
1 0 0 0 0 1 0 0 0 1
16 Taurage PHCI
Children’s nurse (nurse) 8 3 0 3 1 5 0 0 0 12 Obstetrician 14 5 5 2 4 8 0 1 0 25 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 7 1 1 0 1 4 0 0 0 7
Doctor of children’s diseases (paediatrician)
1 0 0 0 0 1 0 0 0 1
17 Utena PHCI 0
Children’s nurse (nurse) 4 2 0 2 0 2 0 0 0 6 Obstetrician 7 4 0 0 0 4 0 0 0 8 Neonatologist 2 1 0 1 1 1 0 0 0 4 Obstetrician-gynaecologist 7 2 2 0 2 4 0 0 0 10
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
18 Trakai PHCI
Children’s nurse (nurse) 6 0 0 0 0 4 0 0 0 4 Obstetrician 10 5 5 5 5 6 0 1 0 27 Neonatologist 5 0 0 0 3 3 0 0 0 6 Obstetrician-gynaecologist 12 3 0 0 3 7 0 1 0 14
Doctor of children’s diseases (paediatrician)
9 0 0 3 3 5 0 0 0 11
19 Mazeikiai PHCI
Children’s nurse (nurse) 2 1 1 1 1 1 0 0 0 5 Obstetrician 15 4 4 4 4 9 0 1 0 26 Neonatologist 3 0 0 0 0 2 0 0 0 2 Obstetrician-gynaecologist 7 1 1 1 1 4 0 0 0 8
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
20 Ukmerge PHCI
Children’s nurse (nurse) 6 1 0 0 2 4 0 0 0 7 Obstetrician 8 2 2 3 2 5 0 0 0 14 Neonatologist 2 1 0 1 1 1 0 0 0 4 Obstetrician-gynaecologist 5 0 0 1 1 3 0 0 0 5
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 154 of 281
R.3. Feasibility study
No PHCI
Structure of staff
Neonatal resuscitatio
n
Modern specialize
d obstetric assistanc
e
Modern primary obstetric assistanc
e
Stabilization of the state of
neonates and
preparation for
transportation
Conflict manageme
nt and communication with patients
Internship
abroad
Internship in
LithuaniaConferen
ces
Number of people who will improve
their qualificat
ion
1 2 3 4 5 6 7 8 921 Radviliskis PHCI
Children’s nurse (nurse) 2 1 1 1 1 1 0 0 0 5 Obstetrician 9 5 5 5 5 5 0 0 0 25 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 7 2 2 2 2 4 0 0 0 12
Doctor of children’s diseases (paediatrician)
1 0 0 0 0 1 0 0 0 1
22 Silute PHCI
Children’s nurse (nurse) 4 0 0 0 0 2 0 0 0 2 Obstetrician 10 8 6 6 0 6 0 1 0 27 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 5 2 2 1 2 3 0 0 0 10
Doctor of children’s diseases (paediatrician)
3 1 0 1 0 2 0 0 0 4
23 Visaginas PHCI
Children’s nurse (nurse) 14 5 0 0 4 8 0 1 0 18 Obstetrician 6 4 4 0 0 4 0 0 0 12 Neonatologist 3 1 0 0 1 2 0 0 0 4 Obstetrician-gynaecologist 7 2 2 0 0 4 0 0 0 8
Doctor of children’s diseases (paediatrician)
7 2 0 0 0 4 0 0 0 6
24 Pasvalys PHCI
Children’s nurse (nurse) 6 3 0 3 0 4 0 0 0 10 Obstetrician 6 4 0 4 0 4 0 0 0 12 Neonatologist 2 1 0 1 0 1 0 0 0 3 Obstetrician-gynaecologist 8 2 2 2 0 5 0 0 0 11
Doctor of children’s diseases (paediatrician)
9 2 0 0 0 5 0 0 0 7
25 Kedainiai PHCI
Children’s nurse (nurse) 5 1 1 1 1 3 0 0 0 7 Obstetrician 11 4 4 4 4 7 0 1 0 24 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 9 0 0 0 0 5 0 0 0 5
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
26 Jonava PHCI
Children’s nurse (nurse) 5 3 0 3 3 3 0 0 0 12 Obstetrician 12 5 5 5 5 7 0 1 0 28 Neonatologist 2 1 0 1 2 1 0 0 0 5 Obstetrician-gynaecologist 9 3 0 0 3 5 0 0 0 11
Doctor of children’s diseases (paediatrician)
12 4 0 0 4 7 0 1 0 16
27 Salcininkai PHCI
Children’s nurse (nurse) 4 1 0 1 0 2 0 0 0 4 Obstetrician 4 0 1 0 0 2 0 0 0 3 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 7 0 0 0 0 4 0 0 0 4
Doctor of children’s diseases (paediatrician)
0 0 0 0 0 0 0 0 0 0
28 Kretinga PHCI
Children’s nurse (nurse) 3 2 2 2 0 2 0 0 0 8 Obstetrician 8 4 4 3 0 5 0 0 0 16 Neonatologist 1 0 0 0 2 1 0 0 0 3 Obstetrician-gynaecologist 5 2 1 0 2 3 0 0 0 8
Doctor of children’s diseases (paediatrician)
11 3 0 0 3 7 0 1 0 14
29 Lazdijai PHCI
Children’s nurse (nurse) 3 2 2 2 2 2 0 0 0 10 Obstetrician 8 5 5 5 5 5 0 0 0 25 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 5 2 2 2 2 3 0 0 0 11
Doctor of children’s diseases (paediatrician)
3 1 1 1 1 2 0 0 0 6
30 Raseiniai PHCI
Children’s nurse (nurse) 4 1 0 1 0 2 0 0 0 4 Obstetrician 7 4 0 4 0 4 0 0 0 12 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 6 1 0 1 0 4 0 0 0 6
Doctor of children’s diseases (paediatrician)
8 2 0 2 2 5 0 0 0 11
31 Vilkaviskis PHCI
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 155 of 281
R.3. Feasibility study
No PHCI
Structure of staff
Neonatal resuscitatio
n
Modern specialize
d obstetric assistanc
e
Modern primary obstetric assistanc
e
Stabilization of the state of
neonates and
preparation for
transportation
Conflict manageme
nt and communication with patients
Internship
abroad
Internship in
LithuaniaConferen
ces
Number of people who will improve
their qualificat
ion
1 2 3 4 5 6 7 8 9 Children’s nurse (nurse) 0 0 0 0 0 0 0 0 0 0 Obstetrician 9 5 6 0 6 5 0 0 0 22 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 10 1 1 0 1 6 0 1 0 10
Doctor of children’s diseases (paediatrician)
4 1 0 1 1 2 0 0 0 5
32 Rokiskis district PHCI
Children’s nurse (nurse) 0 0 0 0 0 0 0 0 0 0 Obstetrician 10 6 6 0 6 6 0 1 0 25 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 8 2 2 0 2 5 0 0 0 11
Doctor of children’s diseases (paediatrician)
5 2 2 0 2 3 0 0 0 9
33 Svencionys PHCI
Children’s nurse (nurse) 0 0 0 0 0 0 0 0 0 0 Obstetrician 7 4 4 4 4 4 0 0 0 20 Neonatologist 1 0 0 0 0 1 0 0 0 1 Obstetrician-gynaecologist 3 1 1 1 1 2 0 0 0 6
Doctor of children’s diseases (paediatrician)
7 1 1 1 1 4 0 0 0 8
Unit price, Lt with VAT 2,360 2,813 2,360 2,811 684 12,200 4,200 5,500
Price of all trainings, Lt with VAT
1,177,391
Lt883,361
Lt965,036
Lt955,682 Lt 727,092 Lt 48,800
Lt197,400
Lt132,000
Lt
Price of all trainings (excluding reserved PHCI)
969,755 Lt 708,939 Lt
832,904 Lt
758,924 Lt 627,912 Lt 48,800 Lt
172,200 Lt
132,000 Lt
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 156 of 281
R.3. Feasibility study
According to the assumptions described in the chapter above, the total need for investments in the improvement of qualification of the staff of PHCI according to the training programmes in the case of alternative I was assessed.
Table 33. Total need for investments in the improvement of qualificationNo Means Supposed need
for investments, LTL with VAT
Share in the budget structure for qualification improvement
1 Trainings: Neonatal resuscitation
969,755 23%
2 Trainings: Modern specialized obstetric assistance
832,904 20%
3 Trainings: Stabilization of the state of neonates and preparation for transportation
758,924 18%
4 Trainings: Modern specialized obstetric assistance
708,939 17%
5 Trainings: Conflict management and communication with patients
627,912 14%
6 Internships to hospitals of a higher level (IIA, IIB to III)
172,200 3%
7 Conferences 132,000 3%8 Internships abroad (for hospitals
of the III level)48,800 1%
Sum (excluding reserved PHCI)
4,251,433 100%
The total budget for the improvement and organization of professional qualification would be 4,251,433 LTL with VAT.
Assessments of the need for investments were performed by assuming that the expenses of accommodation, nutrition and travel of participants of trainings will be covered by PHCI.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 157 of 281
R.3. Feasibility study
9. Analysis of buildings and premises
9.1 Analysis of the demand for mandatory repair of premises of the obstetric and neonatal subdivisions
9.1.1 Energy-sparing means and their necessityDuring the The feasibility study preparation of energy audits for 14 hospitals:
1. PHCI Trakai hospital;2. PHCI Ukmerge hospital;3. PHCI Telsiai country hospital;4. PHCI Panevezys country hospital;5. PHCI Mazeikiai hospital;6. PHCI Kedainiai hospital;7. Christian maternity home;8. PHCI Kaunas 2-nd clinical hospital;9. PHCI Kretinga hospital;10.PHCI Vilkaviskis hospital;11.PHCI Jonava hospital;12.PHCI Raseiniai hospital;13.PHCI Radviliskis hospital;14.PHCI Svencionys hospital.
After performing energy audits of the buildings requiring renovation (including modernization of heating stations, water supply and ventilation/conditioning systems) in those PHCI where an energy audit was not performed or performed before 2004, identified measures and their demand are briefly presented in the table below. Audit reports of PHCI are presented in Appendix 7.
Table 34. Energy-sparing measures and their necessityNo
Energy-sparing measures
Works to be performed to implement the measures
Necessity of measure
1. Wall thermal insulation
1. Wall cleaning and covering with coat against microorganisms; 2. Earthworks (digging/ filling) when insulating the socle of the building;3. Wall thermal insulation with heat insulation materials;
The wall thermal insulation is proposed for those hospitals which normal heat transmission coefficient of external walls U= 0.5–1.5 W/(m²∙K). According to STR 2.05.01:2005 „Thermal technology of building enclosures“, the normal heat transmission coefficient of external walls U in public buildings has to be 0.25 W/(m²∙K). The heat
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 158 of 281
R.3. Feasibility study
No
Energy-sparing measures
Works to be performed to implement the measures
Necessity of measure
4. External finishing (structural plaster, ventilated façade etc.);5. Building base dismantlement and installation of a new one after thermal insulation the socle of the building;6. Façade scaffold, construction waste removal and other minor works.
transmission coefficient of the walls of most hospitals does not comply with the presently valid norms. As the walls leak and get cold, their operating condition does not ensure the sanitary-hygienic requirements applicable to premises. During the heating season, big losses of heat related to walls are suffered. The condition of non-insulated walls is very bad in the aesthetic aspect. After thermal insulation of the walls, a double benefit is derived: it causes lower losses of heat and a longer period until mandatory repair.
2. Roof thermal insulation
Superposed roof1. Cleaning of the present roof covering, „bubble“ fixing;2. Roof thermal insulation when forming slopes;3. Hydraulic insulating two-layer covering installation;4. Thermal insulation material ventilation chimney installation;5. Parapet raise (if necessary);6. Covering parapet, ventilation shaft, climbing hole and other roof elements with tin;7. Rainwater trough installation;8. Active lightning protection installation.
The roof thermal insulation is proposed for those hospitals which normal heat transmission coefficient of roofs U = 0.4–1.0 W/(m²∙K). According to STR 2.05.01:2005 „Thermal technology of building enclosures“, the normal heat transmission coefficient of roofs U in public buildings has to be 0.20 W/(m²∙K). After thermal insulation of the roof, heat is spared, penetration of humidity to the premises is prevented, thermal resistance of enclosures gets better, losses of heat are fewer and the aesthetic view is better.
CONFIDENTIAL document.docx
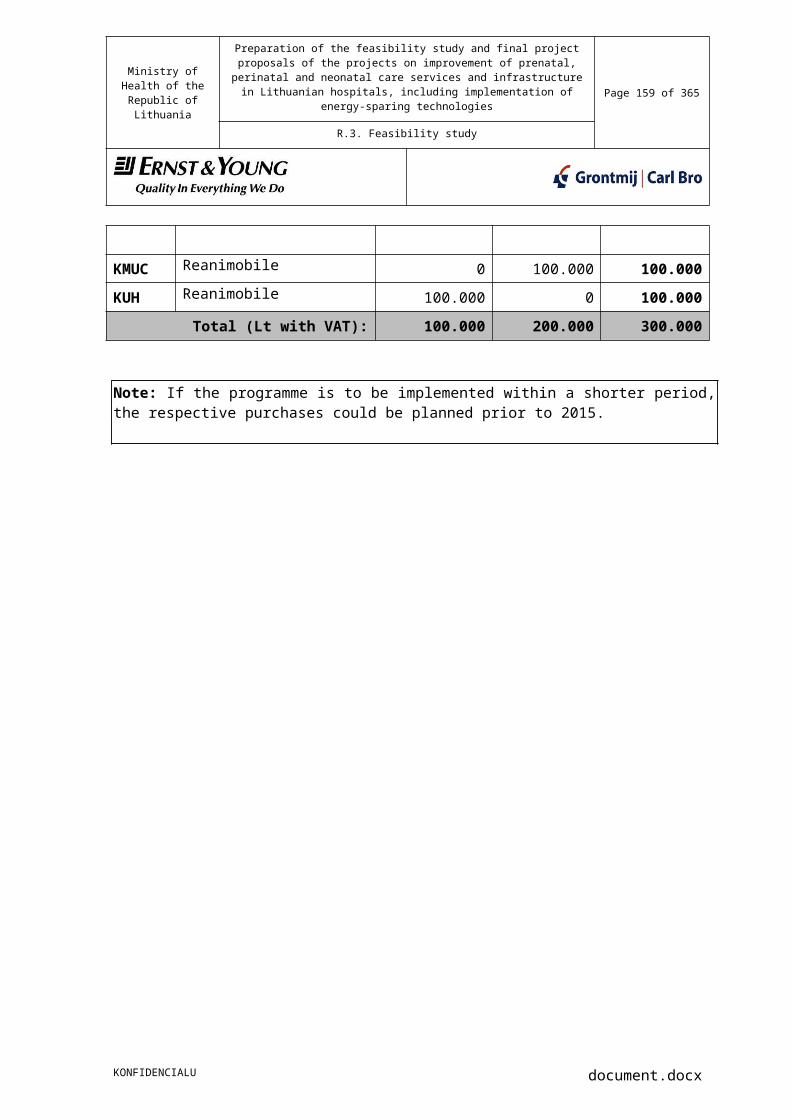
Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 159 of 281
R.3. Feasibility study
No
Energy-sparing measures
Works to be performed to implement the measures
Necessity of measure
Pitch roof1. Dismantlement of the old roof covering;2. Rafter repair or changing (if necessary);3. Covering of wooden roof elements with antiseptic and flame retardants;4. Anti-condensation film installation;3. Thermal insulation of the loft span or roof pitch between rafters with heat insulation material;4. Diffusive film installation;5. Roof covering installation on installed purlins;6. Rain canalization system installation;7. Active lightning protection installation.
3. Window changing
1. Dismantlement of old windows and removal for utilization;2. Mounting of new windows;3. Patching, polishing and painting window opening edges;4. Changing internal window sills (if necessary).
It is proposed to change windows for those hospitals where normal heat transmission coefficient of windows U = 2.0-3.5 W/(m²∙K). According to STR 2.05.01:2005 „Thermal technology of building enclosures“, the normal heat transmission coefficient of windows U in public buildings has to be 1.6 W/(m²∙K). After replacing windows with new ones, thermal and sound insulation of this enclosure gets better. Microventilation installed in new windows compensates
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 160 of 281
R.3. Feasibility study
No
Energy-sparing measures
Works to be performed to implement the measures
Necessity of measure
lack of air which used to penetrate through unsealed windows and caused big losses of heat during the heating season.
4. Door changing 1. Dismantlement of old doors and removal for utilization;2. Mounting of new doors;3. Patching, polishing and painting door opening edges.
External doors are changed for those hospitals where normal heat transmission coefficient of roofs U = 2.0-3.5 W/(m²∙K). According to STR 2.05.01:2005 „Thermal technology of building enclosures“, the normal heat transmission coefficient of doors U in public buildings has to be 1.6 W/(m²∙K).
5. Heating system modernization
1. Dismantlement of old heating equipment, piping and removal for utilization;2. Mounting of new trunk, stand and distribution piping when insulating (if necessary);3. Mounting of control and closing armature;4. Heat equipment mounting;5. Restoration of damaged finishing.
Heating systems are changed for those hospitals which have old cast iron or steel heating equipment without a control possibility. As it is always colder in the corner and northern premises of buildings, it is difficult to ensure the requirements defined in the hygienic norms and rules of the Republic of Lithuania HN 42:2004 "Microclimate of residential and public buildings" and reach a comfortable temperature in the premises during the cold months of the year. Thus, after installing new heating equipment with thermoregulators (according to clause 9.5 of HN 47-1995), it is possible to distribute thermal energy inside the building more efficiently. It is recommended to insulate trunk and stand piping mounted in colder premises (for example, in cellars or lofts).
6. Heating station modernization
1. Dismantlement of old heating station
Heating stations are changed for those hospitals where
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 161 of 281
R.3. Feasibility study
No
Energy-sparing measures
Works to be performed to implement the measures
Necessity of measure
equipment and removal for utilization;2. Installation of a new heating station;3. Heating station connection to trunk networks.
heating stations are old, regulated manually and of elevator type. Old heating stations are reconstructed according to the Rules of heat supply network and heating station installation No 4-80 approved by the Minister of Economics on the 24th of February 2005. After modernizing the heating station, it is possible to automate the mode of the heating stations depending on the changes in the external temperature. It will be easier to operate and maintain the mounted new equipment in the heating station. Heat suppliers will be able to regulate heat supply with computers from their workstation.According to clause 9.2 of the hygienic norms and rules HN 47-1995, maternity institutions are attributed to the first category of heat supply (with autonomous heat supply); therefore, this requirement has to be considered while reconstructing the heating station.
7. Ventilation system modernization
1. Dismantlement of old ventilation aggregates, air intakes and removal for utilization;2. Measurement of new air intakes with necessary regulative and closing armature;3. Installation of new ventilation aggregate.
The ventilation system is modernized for those hospitals where the present ventilation system does not comply with the hygienic norms and rules of the Republic of Lithuania HN 47-1995 „Medical institutions. Hygienic norms and rules“. According to clause 9.9 of these rules, medical institutions have to contain natural and mechanical supply exhaustive
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 162 of 281
R.3. Feasibility study
No
Energy-sparing measures
Works to be performed to implement the measures
Necessity of measure
ventilation. According to clauses 9.14 and 9.15, conditioned air has to be supplied to operating rooms, delivery rooms, wards for neonates, premature and traumatized babies and it has to be additionally cleaned with bacteriocidic filters. It is necessary to apply 2 or 3 stage cleaning of supplied air. After installing new recuperative ventilation equipment which has efficiency of up to 90 per cent, it would be possible to spare much thermal energy.
8. Power supply system modernization
1. Dismantlement of illuminators, old insulation cables and removal for utilization;2. Power cabinet repair;3. Mounting of new cables and illuminators with energy-sparing lamps.
The power supply system is modernized for those hospitals which do not comply with clauses 7.1-7.10 of the hygienic norms and rules HN 47-1995 and do not meet the requirements of „Rules of special premise and technologic process electrical equipment installation“. Consumption of power is mostly reduced after changing old illuminators with heating lamps to new ones with energy-sparing lamps having the same irradiance.
9. Medical gas-oxygen and compressed air vacuum system installation
Dismantlement of old systems (if any). Mounting of new systems with connection sockets (outlets), gas distribution shield mounting, equipment (vacuum compressor, station) mounting.
The minimal supply requirements for reanimation-intensive therapy wards and operating rooms according to the orders of the Minister of Health NoV-827 „On the approval of the description of the conditions and procedure of the reanimation and intensive care service provision to children and adults“ of 27-10-2005 and No 101 „On the approval of the Lithuanian medical norm MN 4:2001
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 163 of 281
R.3. Feasibility study
No
Energy-sparing measures
Works to be performed to implement the measures
Necessity of measure
“Technical regulations of medical device safety” and the medical norm MN 100:2001 “Technical regulations of active implanted medical device safety” of 08-04-2001.
Note: ► The reconstruction of external enclosures of the building (thermal insulation of
external walls, roofs and changing of windows and external entrance doors) is a measures which spares energy and improves the condition of the building, restores the technical condition of the building and its value, prolongs the duration of the building and improves its aesthetic view.
9.1.2 Other measures for repair of the premises of PHCI Upon assessment of the facilities of the premises where obstetric and neonatal subdivisions are located and considering the potentially funded activities, the summarized measures are presented in the table below.
Table 35. Other measures for repair of the premises of PHCI No
Measures of repair
Works to be performed to implement the measures
Necessity of measure
1. Ram installation for disabled people
Installation of a ram with an appropriate slope: basement installation and concreting works, rail installation.
Ram installation following STR 2.03.01:2001 „Structures and territories. Requirements to meet the needs of disabled people”.
2. Repair of internal premises
Suspended ceiling installation, floor, ceiling, wall finishing.
Internal finishing of premises is made following the requirements of part 8 of HN 47-1995 „Medical institutions”.
CONFIDENTIAL document.docx
Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 164 of 281
R.3. Feasibility study
9.1.3 Main indicators of energy audits performed in PHCI during the preparation of the feasibility study In the table below, the main indicators of energy audits performed in PHCI during the preparation of the feasibility study are presented.
Table 36. Main rates of energy audits performed in PHCI during the preparation of the feasibility study
No Name of hospitalActual consumption per standard year after recalculation kWh/m2 per year
Heat consumption after renovation kWh/m2 per year
Percentage of heat consumption
1 Public institution Trakai hospital 146 105 28,08%2 Public institution Ukmerge hospital 284 196 30,99%3 Public institution Telsiai county hospital 235 177 24,68%4 Public institution Panevezys county hospital 225 160 28,89%5 Public institution Mazeikiai hospital 160 110 31,25%6 Public institution Kedainiai hospital 667 473 29,09%
7Christian maternity home (branch of public institution Kaunas county hospital) 236 175 25,85%
8 Public institution Kaunas 2nd clinical hospital 240 165 31,25% Mean (priority PHCI): 274 195 28,82%
1 Public institution Kretinga hospital 397 346 12,85%2 Public institution Vilkaviskis hospital 208 150 27,88%3 Public institution Jonava hospital 128 96 25,00%4 Public institution Raseiniai hospital 160 130 18,75%5 Public institution Radviliskis hospital 203 145 28,57%6 Public institution Svencionys hospital 442 314 28,96%
Mean (reserve PHCI): 256 197 23,21%
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 165 of 281
R.3. Feasibility study
9.1.4 List of buildings recommended for renovationIn the tables below in this chapter, the priority and reserve lists of buildings recommended for renovation including the measures intended to implement in hospitals, amounts of investments and savings are presented.
Based on the experience of an analogical energy efficiency programme, such as the national projects proposed to be financed from the funds of the European Union according to the measures „Renovation of public buildings at the national level“, the duration of separate projects should not exceed 36 months from the date of signing the funding contract. Procurement procedures would be performed within 6 months, design works – within 6 months and contracting works – within 22 months. The project administration activity would involve the total project performance period, i.e., from signing the funding contract to transferring the object.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 166 of 281
R.3. Feasibility study
Table 37. List of buildings recommended for renovation with amounts of measures intended to implement in hospitals, investments and savings
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
1 Public institution Trakai hospital 146 1,502,727.27 Lt 1,818,300.00 Lt
AThermal insulation of external walls (with the socle part) 98 1,400.00 m2 350.00 404,958.68 Lt 490,000.00 Lt
B Roof thermal insulation 48 1,582.00 m2 350.00 457,603.31 Lt 553,700.00 Lt
C Heating system changing 27 1,582.00 m2 200.00 261,487.60 Lt 316,400.00 Lt
D Electrical system changing 18 1,582.00 m2 100.00 130,743.80 Lt 158,200.00 Lt
E Ventilation system renovation 0 1.00 unit 300,000.00 247,933.88 Lt 300,000.00 Lt
2 Public institution Ukmerge hospital 277 1,399,033.06 Lt 1,692,830.00 Lt
AThermal insulation of external walls (with the socle part) 212 2,654 m2 420 921,223.14 Lt 1,114,680.00 Lt
B Roof thermal insulation 80 1,600 m2 350 462,809.92 Lt 560,000.00 Lt
C Window and door 4.95 33 m2 550 15,000.00 Lt 18,150.00 Lt
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 167 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
changing
3Public institution Telsiai county hospital 349 2,979,512.40 Lt 3,605,210.00 Lt
A Window and door changing 46 461 m2 550 209,545.45 Lt 253,550.00 Lt
B Wall and socle thermal insulation 266 4,424 m2 450 1,645,289.26 Lt 1,990,800.00 Lt
C Heating system renovation 58 6,054.3 m2 200 1,000,710.74 Lt 1,210,860.00 Lt
D Ventilation system renovation 0 1 unit 150,000 123,966.94 Lt 150,000.00 Lt
4Public institution Panevezys county hospital 337 1,718,099.17 Lt 2,078,900.00 Lt
AThermal insulation of external walls (with the socle part) 241 2,676 m2 400 884,628.10 Lt 1,070,400.00 Lt
B Roof thermal insulation 113 1,616 m2 500 667,768.60 Lt 808,000.00 Lt
C Window and glass block changing 19 127 m2 500 52,479.34 Lt 63,500.00 Lt
D Changing of 0 220 m 140 25,454.55 Lt 30,800.00 Lt
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 168 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
internal water supply trunk piping during thermal insulation
EExtension of the ventilation system with freezing aggregates 0 4,248 m2 25 87,768.60 Lt 106,200.00 Lt
5 Public institution Mazeikiai hospital 215 1,831,636.36 Lt 2,216,280.00 Lt
AThermal insulation of external walls (with the socle part) 189 2,100 m2 350 607,438.02 Lt 735,000.00 Lt
B Thermal insulation system renovation 176 3,770 m2 200 623,140.50 Lt 754,000.00 Lt
C Ventilation system renovation 35.34 1 unit 477,280 394,446.28 Lt 477,280.00 Lt
D Medical gas installation 0 1 unit 250,000 206,611.57 Lt 250,000.00 Lt
6 Public institution Kaunas Medical University Clinic (obstetric and
217 3,612,241.32 Lt 4,370,812.00 Lt
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 169 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
neonatal services)
A Heating system reconstruction 121 10,923.40 m2 180.00 1,624,968.60 Lt 1,966,212.00 Lt
BRecuperative ventilation system reconstruction 30 5,462.00 m2 200.00 902,809.92 Lt 1,092,400.00 Lt
C Heating station reconstruction 107 1.00 unit 80,000.00 66,115.70 Lt 80,000.00 Lt
DInternal power supply system modernization 7 5,462.00 m2 100.00 451,404.96 Lt 546,200.00 Lt
EChanging of trunk heating piping from boiler room to heating station 22 800.00 m2 170.00 112,396.69 Lt 136,000.00 Lt
FCompressed air and oxygen supply system 0 1,00 unit 550,000.00 454,545.45 Lt 550,000.00 Lt
7Public institution Klaipeda University hospital 709 7,432,917.36 Lt 8,993,830.00 Lt
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 170 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
AThermal insulation of external walls (with the base part) 412 3,849 m2 350 1,113,347.11 Lt 1,347,150.00 Lt
B Roof thermal insulation 105 3,850 m2 400 1,272,727.27 Lt 1,540,000.00 Lt
C Heating system reconstruction 112 11,221.00 m2 180.00 1,669,239.67 Lt 2,019,780.00 Lt
D Ventilation system reconstruction 0 11,221.00 m2 200.00 1,854,710.74 Lt 2,244,200.00 Lt
E Heating station reconstruction 70 1.00 unit 80,000.00 66,115.70 Lt 80,000.00 Lt
FInternal power supply system modernization 3 11,221.00 m2 100.00 927,355.37 Lt 1,122,100.00 Lt
G Window changing 177.7 1,105.00 m2 300.00 273,966.94 Lt 331,500.00 LtH Door changing 6.2 26.00 m2 350,00 7,520.66 Lt 9,100.00 Lt
ICompressed air and oxygen supply system 0 1.00 unit 300,000.00 247,933.88 Lt 300,000.00 Lt
8 Christian maternity home (Branch of public institution
44 706,314.05 Lt 854,640.00 Lt
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 171 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
Kaunas county hospital)
A Roof thermal insulation 28 467
m2
400 154,380.17 Lt 186,800.00 LtB Heating system
reconstruction 7 1,203.00m2
180.00 178,958.68 Lt 216,540.00 LtC Ventilation system
reconstruction 0 1,203.00m2
200.00 198,842.98 Lt 240,600.00 LtD Heating station
reconstruction 10 1,00 unit 60,000.00 49,586.78 Lt 60,000.00 Lt
EInternal power supply system modernization 1 1,203.00
m2
100.00 99.421,49 Lt 120,300.00 LtF Window changing 2 11.00 m2 300.00 2,727.27 Lt 3,300.00 LtG Door changing 1 6.00 m2 350.00 1,735.54 Lt 2,100.00 Lt
HCompressed air and oxygen supply system 0 1.00 unit 25,000.00 20,661.16 Lt 25,000.00 Lt
9 Public institution Kedainiai hospital 234 1,076,933.88 Lt 1,303,090.00 Lt
AThermal insulation of external walls (with the socle part) 142 1,185
m2
460 450,495.87 Lt 545,100.00 Lt
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 172 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
B Roof thermal insulation 37 467
m2
350 135,082.64 Lt 163,450.00 LtC Heating system
reconstruction 32 1,203.00m2
180.00 178,958.68 Lt 216,540.00 LtD External heat
network renovation 48 540.00m2
700.00 312,396.69 Lt 378,000.00 Lt
10
Vilnius City University Hospital (obstetric services) 0 330,578.51 Lt 400,000.00 Lt
A Ventilation system reconstruction 0 1 unit 400,000.00 330,578.51 Lt 400,000.00 Lt
11
Public institution Vilnius city University hospital (obstetric services) 0 445,123.97 Lt 538,600.00 Lt
A Ventilation system renovation 0 1 unit 300,000.00 247,933.88 Lt 300,000.00 Lt
B Compressed air supply equipment 0 1 unit 78,650.00 65,000.00 Lt 78,650.00 Lt
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 173 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
C Vacuum supply equipment 0 1 unit 66,550.00 55,000.00 Lt 66,550.00 Lt
D
Compressed air, vacuum and oxygen supply systems with gas provision shields 0 1 unit 93,400.00 77,190.08 Lt 93,400.00 Lt
12Public institution Vilnius maternity home 67 3,236,363.64 Lt 3,916,000.00 Lt
A Heating system reconstruction 67 7,580 m² 200 1,252,892.56 Lt 1,516,000.00 Lt
B Ventilation system renovation 0 4 unit 600,000.00 1,983,471.07 Lt 2,400,000.00 Lt
13Public institution Kaunas 2nd clinical hospital 796 7,167,293.22 Lt 8,672,424.80 Lt
AThermal insulation of external walls (with the socle part) 650 10,000.00 m² 350.00 2,892,561.98 Lt 3,500,000.00 Lt
B Thermal insulation of the span adjoining the
20 200.00 m² 350.00 57,851.24 Lt 70,000.00 Lt
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 174 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
outsideC Heating system
reconstruction 178 10,604.00 m² 200.00 1,752,727.27 Lt 2,120,800.00 LtD Ventilation system
reconstruction 0 13,552.84 m² 150.00 1,680,104.13 Lt 2,032,926.00 Lt
EInternal power supply system modernization 3 13,552.84 m² 70.00 784,048.60 Lt 948,698.80 Lt
14
P. Mazylio maternity home (Branch of public institution Kaunas 2nd clinical hospital) 0 157,024.79 Lt 190,000.00 Lt
AMechanical (forced traction system) renovation 0 1 unit 190,000.00 157,024.79 Lt 190,000.00 Lt
15Public institution Marijampole hospital 50 1,549,153.72 Lt 1,874,476.00 Lt
A Ventilation system reconstruction 0 2.00 unit 600,000.00 991,735.54 Lt 1,200,000.00 Lt
B Heating system 50 914.92 m² 200.00 151,226.45 Lt 182,984.00 Lt
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 175 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
reconstruction
CInternal power supply system modernization 2 914.92 m² 100.00 75,613.22 Lt 91,492.00 Lt
D
Compressed air, vacuum and oxygen supply systems with gas provision shields 0 1.00 unit 400,000.00 330,578.51 Lt 400,000.00 Lt
16 Pasvalys PHCI5 0 99,173.55 Lt 120,000.00 Lt
AVacuum station and the supply system installation 0 1.00 unit 120,000.00 99,173.55 Lt 120,000.00 Lt
17 Public institution VU hospital Santariskiu clinic (obstetric services)3
- - - - - -
18 Public institution Siauliai county hospital1
- - - - - -
18 Public institution Alytus region
- - - - - -
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 176 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after recalculation per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
S.Kudirkos hospital1
20 Public institution Taurage county hospital2
- - - - - -
21 Public institution Utena county hospital5
- - - - - -
22 Public institution Visaginas hospital5
- - - - - -
Total 35,244,126.28 42,645,392.80
Explanations of the table:1 - EA performed, and municipality has applied to the Ministry of Economy;2 - EA audit performed at the expense of the municipality. The application to the Ministry of Economy is being prepared;3 - It is intended to move the hospital to other premises;4 - New ventilation systems are being implemented;5 Measures implemented from the structural funds of the European Union.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 177 of 281
R.3. Feasibility study
-Table 38. Reserve list of buildings recommended for renovation with amounts of measures intended to implement in hospitals, investments and savings
No Name of hospital
Saving MWh/year after reassessment per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
1Public institution Kretinga hospital 156 1,522,394.21 1,842,097.00
ARoof (span) thermal insulation 112 1,400.00 m2 350.00 404,958.68 490,000.00
BHeating system reconstruction 48 3,052.00 m2 200.00 504,462.81 610,400.00
C Internal power supply system modernization 11 1.00 unit 302,147.00 249,708,26 302,147.00
DVentilation system reconstruction 0,6 1.00 unit 406,000.00 335,537.19 406,000.00
ECompressed air and oxygen supply system 0 457.00 m² 150.00 56,652.89 68,550.00
2Public institution Vilkaviskis hospital 129 1,300,322.31 1,573,390.00
A
Thermal insulation of external walls (with the socle part) 88 1,665.00 m2 430.00 591,694.21 715,950.00
BHeating system reconstruction 18 1,203.00 m2 180.00 178,958.68 216,540.00
CVentilation system reconstruction 0 1,203.00 m2 200.00 198,842.98 240,600.00
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 178 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after reassessment per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
DHeating station reconstruction 26 1.00 unit 60,000.00 49,586.78 60,000.0
EInternal power supply system modernization 7 1,203.00 m2 100.00 99,421.49 120,300.00
GCompressed air and oxygen supply system 0 1.00 250,000.00 206,611.57 250,000.00
3Public institution Jonava hospital 48 1,078,181.82 1.304,600.00
A Base wall thermal insulation 16 180.00 m2 500.00 74,380.17 90,000.00B Roof thermal insulation 13 670.00 m2 350.00 193,801.65 234,500.00
CHeating station reconstruction 10 1,514.00 unit 60.00 75,074.38 90,840.00
DHeating system reconstruction 12 1,514.00 unit 200.00 250,247.93 302,800.00
FInternal power supply system modernization 1 1,514.00 unit 100.00 125,123.97 151,400.00
G External door changing 2 12.20 m2 1,300.00 13,107.44 15,860.00
HVentilation system reconstruction 0 1,514.00 unit 300.00 375,371.90 454,200.00
4Public institution Silute hospital 343 1.473,489.50 1,782,922.30
A Window changing 53 260.63 m2 700.00 150,777.69 182,441.00B External door changing 2.1 19.84 m2 1,200.00 19,678.31 23,810.76C External wall thermal 124 1,966.98 m2 280.00 455,168.09 550,753.39
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 179 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after reassessment per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
insulation
EUpper span thermal insulation 66 1,036.43 m2 250.00 214,138.14 259,107.15
FInstallation of warmed floors on the ground 56 818.20 m2 150.00 101,429.75 122,730.00
G
Heating and hot water supply system modernization 43 3,395.40 m2 200.00 561,223.14 679,080.00
5Public institution Raseiniai hospital 86 m2 2,030,314.05 2,456,680.00
A Base wall thermal insulation 45 500.00 m2 500.00 206,611.57 250,000.00
BHeating system reconstruction 46 4,363.36 m2 200.00 721,216.53 872,672.00
CVentilation system reconstruction 0 4,363.36 m2 300.00 1,081,824.79 1,309,008.00
D Oxygen supply system 0 1.00 unit 50,000.00 41,322.31 50,000.00
6Public institution Rokiskis district hospital 74 367,253.72 444,377.00
AHeating system reconstruction 67 564.59 m2 200.00 93,320.66 112,918.00
BInternal power supply system modernization 7 564.59 m2 100.00 46,660.33 56,459.00
C Ventilation system installation (for delivery
0 1.00 unit 240,000.00 198,347.11 240,000.00
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 180 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after reassessment per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
rooms)
DOxygen supply system repair 0 1.00 unit 60,000.00 49,586.78 60,000.00
7Public institution Radviliskis hospital 373 2,366,595.04 2,863,580.00
A Wall thermal insulation 305 4,350.00 m2 350 1,258,264.46 1,522,500.00
BOutside heating network renovation 61 150.00 m 700 86,776.86 105,000.00
C Heating system renovation 31 6,355.40 m2 200 1,050,479.34 1,271,080.00
8Public institution Svencionys hospital 276.00 m2 1.277,326.45 1,545,565.00
A
Thermal insulation of external walls (with the base part) 190.00 2,000.00 m2 350.00 578,512.40 700,000.00
B Roof thermal insulation 72.00 720.00 m2 350.00 208,264.46 252,000.00
CWindow and balcony door changing 34.30 361.00 m2 500.00 149,173.55 180,500.00
D External door yard 2.13 24.10 m2 650.00 12,946.28 15,665.00
EHeating system reconstruction 1.41 2,162.00 unit 200.00 357,355.37 432,400.00
9Public institution Klaipeda hospital 10.00 484,917.36 586,750.00
B Roof thermal insulation 10.00 605.00 m2 350.00 175,000.00 211,750.00E Ventilation system 0 1.00 unit 400,000.00 330,578.51 400,000.00
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 181 of 281
R.3. Feasibility study
No Name of hospital
Saving MWh/year after reassessment per standard year
Amount of unit
Measure
Unit price, LTL with VAT
Increase of energy efficiency, LTL without VAT
Increase of energy efficiency, LTL with VAT
modernization
10
Public institution VU hospital Santariskiu clinic (intensive therapy services) 7.00 363,636.36 440,000.00
AInternal power supply system modernization 7.00 550.00 m2 100.00 45,454.55 55,000.00
BVentilation system modernization 0 1.00 unit 400,000.00 330,578.51 400,000.00
11
Public institution Salcininkai hospital1 - - - - - 0.00
12
Public institution Lazdijai hospital2 - - - - - 0.00
Total 12,264,430.83 14,839,961.30
Explanations of the table:1 - EA performed, and municipality has applied to the Ministry of Economy;2 - EA audit performed at the expense of the municipality. The application to the Ministry of Economy is being prepared;
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 182 of 281
R.3. Feasibility study
9.1.5 Essential repairIn the table below, the areas of premises (premises where the services provided for pregnant women, neonates (eg, maternity ward, showers) and / or where medical equipment will be mounted) and other facility improving measures. PHCI according to the need for funding could also update the restrooms.
Table 39. Areas of premises (where medical equipment will be mounted) proposed to repair and other facility-improving measuresNo Name of hospital Amount of
unitMeasure
Unit price, LTL with VAT
Repair, LTL without VAT
Repair, LTL with VAT
1 Public institution Ukmerge hospital 0.00 0.00
2Public institution Telsiai county hospital 140,495.87 170,000.00
A Repair of premises 170.00 m² 1,000.00 14,.495.87 170,000.00
3Public institution Panevezys county hospital 25,454.55 30,800.00
AChanging of internal water supply trunk piping when thermal insulation 220.00 m 140.00 25,454.55 30,800.00
4 Public institution Mazeikiai hospital 161,157.02 195,000.00A Fire protection system 1.00 unit 150,000.00 123,966.94 150,000.00B Ram installation 1.00 unit 37,190.08 45,000.00
5
Public institution Kaunas Medical University Clinic (obstetric and neonatal services) 1,430,198.35 1,730,540.00
AReconstruction of internal water supply and sewage systems 5462.00 m² 170.00 767,388.43 928,540.00
B Repair of premises 802.00 m² 1,000.00 662,809.92 802,000.00
6Public institution Klaipeda University hospital 1,127,008.26 1,363,680.00
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 183 of 281
R.3. Feasibility study
No Name of hospital Amount of unit
Measure
Unit price, LTL with VAT
Repair, LTL without VAT
Repair, LTL with VAT
AReconstruction of internal water supply and sewage systems 11,221.00 m² 80.00 741,884.30 897,680.00
B Repair of premises 466.00 m² 1,000.00 385,123.97 466,000.007 Public institution Kedainiai hospital 0.00 0.00
8
Public institution Vilnius city University hospital (obstetric services) 57,851.24 70,000.00
A Split mending and façade painting 1.00 Unit 70,000.00 57,851.24 70,000.00
9
Public institution Vilnius University Children’s hospital (neonatal services) 0.00 0.00
10Public institution Vilnius maternity home 313,223.14 379,000.00
AChanging doors of the premises of the obstetric block 122.00 m² 1,500.00 151,239.67 183,000.00
BChanging cold, hot, circulation and fire protection water supply trunk piping 980.00 m 200.00 161,983.47 196,000.00
11Public institution Kaunas 2nd clinical hospital 745,773.14 902,385.50
AReconstruction of internal water supply and sewage systems 1,930.37 m² 150.00 239,302.07 289,555.50
B Repair of premises 612.83 m² 1,000.00 506,471.07 612,830.00
12
P. Mazylio maternity home (Branch of public institution Kaunas 2nd clinical hospital) 33,057.85 40,000.00
A Repair of water supply inlet (with 1.00 unit 40,000.00 33,057.85 40,000.00
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 184 of 281
R.3. Feasibility study
No Name of hospital Amount of unit
Measure
Unit price, LTL with VAT
Repair, LTL without VAT
Repair, LTL with VAT
accounting and filters)
13Public institution Marijampole hospital 75,613.22 91,492.00
AReconstruction of internal water supply and sewage systems 914.92 m² 100.00 75,613.22 91,492.00
14 Public institution Trakai hospital 165,289.26 200,000,00A Repair of premises 200.00 m² 1,000.00 165,289.26 200,000,0015 Public institution Pasvalys hospital 0.00 0.00
16Public institution VU hospital Santariskiu clinic (obstetric services) 0.00 0.00
17Public institution Siauliai county hospital 0.00 0.00
18Public institution Alytus region S.Kudirkos hospital 0.00 0.00
19Public institution Taurage county hospital 0.00 0.00
20Public institution Utena county hospital 0.00 0.00
21 Public institution Visaginas hospital 0.00 0.00Total for priority PHCI: 4,275,121.90 5,172,897.50
1 Public institution Kretinga hospital 171,074.38 207,000.00A Repair of premises 207.00 m² 1,000.00 171,074.38 207,000.002 Public institution Vilkaviskis hospital 831,826.45 1,006,510.00A Reconstruction of internal water supply
and sewage systems1,203.00 170.00 169,016.53 204,510.00
B Repair of premises 802.00 1,000.00 662,809.92 802,000.00
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 185 of 281
R.3. Feasibility study
No Name of hospital Amount of unit
Measure
Unit price, LTL with VAT
Repair, LTL without VAT
Repair, LTL with VAT
3 Public institution Jonava hospital 1,464,090.91 1,771,550.00A Reconstruction of internal water supply
and sewage systems1,514.00 unit 170.00 212,710.74 257,380.00
B Repair of premises 1,514.17 unit 1,000.00 1,251,380.17 1,514,170.004 Public institution Silute hospital 0.00 0.005 Public institution Raseiniai hospital 152,892.56 185,000.00A Repair of premises 185 m² 1,000.00 15,.892.56 185,000.006 Public institution Rokiskis district
hospital 156,905.54 189,855.70
A Reconstruction of internal water supply and sewage systems
564.59 230.00 107,318.76 129,855.70
B Repair of premises 60 1,000.00 49,586.78 60,000.007 Public institution Radviliskis hospital - - - 0.00 0.008 Public institution Svencionys hospital - - - 0.00 0.009 Public institution Klaipeda children’s
hospital- - - 0.00 0.00
10 Public institution VU hospital Santariskiu clinic (intensive therapy services)
- - - 0.00 0.00
11 Public institution Salcininkai hospital - - - 0.00 0.0012 Public institution Lazdijai hospital - - - 0.00 0.00
Total for reserve PHCI: 1,397,731.98 1,691,255.70Total for priority and reserve PHCI: 5,672,853.88 6,864,153.20
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 186 of 281
R.3. Feasibility study
9.2 Rating of the list of buildings recommended for renovationConsidering the demands of PHCI and the extent of energy-sparing, a list of buildings recommended for renovation was made; it is presented in the tables below by applying different rating criteria. The most optimal funded rating according to the amount of investments in sparing thermal energy 1 MWh/year is presented in tables 39, 40, 41 of the priority list and table 42 of the reserve list. This value is also used for rating as it shows how efficiently the monetary expression is used for decrease of losses of thermal energy.
Criteria of rating of the priority and reserve lists of buildings recommended for renovation:
► From the lowest amount of investments in sparing thermal energy 1 MWh/year after recalculation for a standard year;► From the highest to the lowest expected energy efficiency.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 187 of 281
R.3. Feasibility study
Table 40. Priority list of buildings recommended for renovation by rating from the lowest sum of investments to savethermal energy 1 MWh/year after recalculation for a standard year
No Name of hospitalSparing MWh/year after reassessment for a standard year
Investments for increase of energy efficiency, LTL without VAT
Investments for increase of energy efficiency, LTL with VAT
Investments per 1 MWh/year for sparing 1LTL/MWh/year
1. Public institution Kedainiai hospital 234 1,076,933.88 1,303,090.00 5,568.76
2. Public institution Ukmerge hospital 277 1,399,033.06 1,692,830.00 6,111.30
3. Public institution Panevezys county hospital 337 1,718,099.17 2,078,900.00 6,168.84
4. Public institution Mazeikiai hospital 215 1,831,636.36 2,216,280.00 10,308.28
5. Public institution Telsiai county hospital 349 2,979,512.40 3,605,210.00 10,330.11
6. Public institution Kaunas 2nd clinical hospital 796 7,167,293.22 8,672,424.80 10,895.01
7. Public institution Trakai hospital 146 1,502,727.27 1,818,300.00 12,454.11
8. Public institution Klaipeda University hospital 709 7,432,917.36 8,993,830.00 12,685.23
9. Christian maternity home (Branch of public institution Kaunas county hospital) 44 706,314.05 854,640.00 19,423.64
10. Public institution Kaunas 217 3,612,241.32 4,370,812.00 20,141.99
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 188 of 281
R.3. Feasibility study
No Name of hospitalSparing MWh/year after reassessment for a standard year
Investments for increase of energy efficiency, LTL without VAT
Investments for increase of energy efficiency, LTL with VAT
Investments per 1 MWh/year for sparing 1LTL/MWh/year
Medical University Clinic (obstetric and neonatal services)
11. Public institution Marijampole hospital 50 1,549,153.72 1,874,476.00 37,489.52
12. Public institution Vilnius maternity home 67 3,236,363.64 3,916,000.00 58,447.76
13. Public institution Vilnius University Children’s hospital (neonatal services)4 0 445,123.97 538,600.00 0.00
14. Public institution Vilnius city University hospital (obstetric services)4 0 330,578.51 400,000.00 0.00
15. P. Mazylio maternity home (Branch of public institution Kaunas 2nd clinical hospital)4 0 157,024.79 190,000.00 0.00
16. Public institution Pasvalys hospital5 0 99,173.55 120,000.00 0.00
17. Public institution VU hospital Santariskiu clinic (obstetric services)3 0 0.00 0.00 0.00
18. Public institution Siauliai 0 0.00 0.00 0.00
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 189 of 281
R.3. Feasibility study
No Name of hospitalSparing MWh/year after reassessment for a standard year
Investments for increase of energy efficiency, LTL without VAT
Investments for increase of energy efficiency, LTL with VAT
Investments per 1 MWh/year for sparing 1LTL/MWh/year
county hospital119. Public institution Alytus
region S.Kudirkos hospital1 0 0.00 0.00 0.00
20. Public institution Taurage county hospital2 0 0.00 0.00 0.00
21. Public institution Utena county hospital5 0 0.00 0.00 0.00
22. Public institution Visaginas hospital5 0 0.00 0.00 0.00
Total 3,441.00 35,244,126.28 42,645,392.80 12,393.31
Explanations of the table:1 - EA performed, and municipality has applied to the Ministry of Economy;2 - EA audit performed at the expense of the municipality. The application for the Ministry of Economy is being prepared;3 - It is intended to move the hospital to other premises;4 - New ventilation systems are being implemented;5 - Measures implemented from the structural funds of the European Union.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 190 of 281
R.3. Feasibility study
Table 41. Priority list of buildings recommended for renovation by rating from the highest to the lowest expected energy efficiency
No Name of hospitalSparing MWh/year after reassessment for a standard year
Investments for increase of energy efficiency, LTL without VAT
Investments for increase of energy efficiency, LTL with VAT
1. Public institution Kaunas 2nd clinical hospital 796 7.167.293,22 8.672.424,802. Public institution Klaipeda University hospital 709 7.432.917,36 8.993.830,003. Public institution Telsiai county hospital 349.00 2,979,512.40 3,605,210004. Public institution Panevezys county hospital 337.00 1,718,099.17 2,078,900.005. Public institution Ukmerge hospital 277.00 1,399,033.06 1,692,830.006. Public institution Kedainiai hospital 234.00 1,076,933.88 1,303,090.007. Public institution Kaunas Medical University Clinic (obstetric and
neonatal services) 217.00 3,612,241.32 4,370,812.008. Public institution Mazeikiai hospital 215.00 1,831,636.36 2,216,280.009. Public institution Trakai hospital 146.00 1,502,727.27 1,818,300.0010.
Public institution Vilnius maternity home 67.00 3,236,363.64 3,916,000.0011.
Public institution Marijampole hospital 50.00 1,549,153.72 1,874,476.0012. Christian maternity home (Branch of public institution Kaunas
county hospital) 44.00 706,314.05 854,640.0013. Public institution Vilnius University Children’s hospital (neonatal
services)4 0.00 445,123.97 538,600.00
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 191 of 281
R.3. Feasibility study
No Name of hospitalSparing MWh/year after reassessment for a standard year
Investments for increase of energy efficiency, LTL without VAT
Investments for increase of energy efficiency, LTL with VAT
14. Public institution Vilnius city University hospital (obstetric services)4 0.00 330,578.51 400,000.00
15. P. Mazylio maternity home (Branch of public institution Kaunas 2nd clinical hospital)4 0.00 157,024.79 190,000.00
16.Public institution Pasvalys hospital5 0.00 99,173.55 120,000.00
17. Public institution VU hospital Santariskiu clinic (obstetric services)3 0.00 0.00 0.00
18.Public institution Siauliai county hospital1 0.00 0.00 0.00
19.Public institution Alytus region S.Kudirkos hospital1 0.00 0.00 0.00
20.Public institution Taurage county hospital2 0.00 0.00 0.00
21.Public institution Utena county hospital5 0.00 0.00 0.00
22.Public institution Visaginas hospital5 0.00 0.00 0.00
Total: 3,441.00 35,244,126.28 42,645,392.80
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 192 of 281
R.3. Feasibility study
Explanations of the table:1 - EA performed, and municipality has applied to the Ministry of Economy;2 - EA audit performed at the expense of the municipality. The application for the Ministry of Economy is being prepared;3 - It is intended to move the hospital to other premises;4 - New ventilation systems are being implemented;5 - Measures implemented from the structural funds of the European Union.
Table 42. Reserve list of buildings recommended for renovation by rating from the lowest sum of investments to savethermal energy 1 MWh/year after reassessment for a standard year
No Name of hospital
Sparing MWh/year after reassessment for a standard year
Investments for increase of energy efficiency, LTL without VAT
Investments for increase of energy efficiency, LTL with VAT
Investments per 1 MWh/year for sparing 1LTL/MWh/year
23. Public institution Silute hospital 343.00 1,473,489.50 1,782,922.30 5,198.02
24. Public institution Svencionys hospital 276.00 1,277,326.45 1,545,565.00 5,599.87
25. Public institution Rokiskis district hospital 74.00 367,253.72 444,377.00 6,005.09
26. Public institution Radviliskis hospital 373.00 2,366,595.04 2,863,580.00 7,677.16
27. Public institution Kretinga hospital 156.00 1,522,394.21 1,842,097.00 11,808.31
28. Public institution Vilkaviskis hospital 129.00 1,300,322.31 1,573,390.00 12,198.05
29. Public institution Jonava hospital 48.00 1,078,181.82 1,304,600.00 27,179.17
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 193 of 281
R.3. Feasibility study
No Name of hospital
Sparing MWh/year after reassessment for a standard year
Investments for increase of energy efficiency, LTL without VAT
Investments for increase of energy efficiency, LTL with VAT
Investments per 1 MWh/year for sparing 1LTL/MWh/year
30. Public institution Raseiniai hospital 86.00 2,030,314.05 2,456,680.00 28,566.05
31. Public institution Klaipeda children’s hospital 10.00 484,917.36 586,750.00 58,675.00
32. Public institution VU hospital Santariskiu clinic (intensive therapy services) 7.00 363,636.36 440,000.00 62,857.14
33. Public institution Salcininkai hospital1 0.00 0.00 0.00 0.00
34. Public institution Lazdijai hospital2 0.00 0.00 0.00 0.00
Total 1.502.00 12,264,430.83 14,839,961.30 9,880.22
Explanations of the table:1 - EA performed, and municipality has applied to the Ministry of Economy;2 - EA audit performed at the expense of the municipality. The application for the Ministry of Economy is being prepared;
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 194 of 281
R.3. Feasibility study
Table 43. Reserve list of buildings recommended for renovation by rating from the highest to the lowest expected energy efficiency
No Name of hospital
Sparing MWh/year
after reassessment for a standard
year
Investments for increase of
energy efficiency, LTL
without VAT
Investments for increase of
energy efficiency, LTL
with VAT
1. Public institution Radviliskis hospital 373 2,366,595.04 2,863,580.00
2. Public institution Silute hospital 343 1,473,489.50 1,782,922.30
3. Public institution Svencionys hospital 276 1,277,326.45 1,545,565.00
4. Public institution Kretinga hospital 156 1,522,394.21 1,842,097.00
5. Public institution Vilkaviskis hospital 129 1,300,322.31 1,573,390.00
6. Public institution Raseiniai hospital 86 2,030,314.05 2,456,680.00
7. Public institution Rokiskis district hospital 74 367,253.72 444,377.00
8. Public institution Jonava hospital 48 1,078,181.82 1,304,600.00
9. Public institution Klaipeda children’s hospital 10 484,917.36 586,750.00
10. Public institution VU hospital Santariskiu clinic (intensive therapy services) 7 363,636.36 440,000.00
11. Public institution Salcininkai hospital1 0 0.00 0.00
12. Public institution Lazdijai hospital2 0 0.00 0.00
Total: 1502 12,264,430.83 14.839.961,30
Explanations of the table:1 - EA performed, and municipality has applied to the Ministry of Economy;2 - EA audit performed at the expense of the municipality. The application for the
Ministry of Economy is being prepared;
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 195 of 281
R.3. Feasibility study
9.3 Funding of buildings recommended for renovationPresent situation:
The demand for the funds for the measures intended in the priority list does not exceed the funds provided for in the programme; therefore, we recommend full funding of the activities provided for in the priority list (100 per cent).
Table 44. Possibilities of the programme budget and funding of the priority and the reserve list
MeasuresIntended costs for the project
activities, LTL with VAT
Improvement of thermal insulation in buildings 15,356,300Heating, hot water supply system and heating station modernization
11,284,900
Ventilation and conditioning system modernization/ implementation
11,133,600
Power supply system modernization 2,987,000Medical gas, oxygen, vacuum and compressed air supply system modernization
2,244,000
Note. The need for funding for the execution of separate Project activities is calculated according to the currency rate 1 CHF = 2.2 LTL.
It is recommended to use the reserve taking into consideration the following two alternatives: ► Alternative I. Implement better measures, for example, install geothermal
heating systems in PHCI with old boiler houses, old heat distribution system and high heat consumption. Since geothermal heating is the low-temperature heating system method, it is not suitable for the heating equipment (radiator) systems. Upon installation of geothermal heating, all the indoor heating distribution system should be changed by installing collectors and floor heating. For the installation of floor heating, floor finishing has to be performed. Installation of floor heating requires twice as much investment as the heating device (radiator) system installation. Although the geothermal heating system requires rather substantial funding, in respect of energy efficiency it could pay off within 15-25 years, as the expenses would only consist of low electricity costs.
► Alternative II. Implement measures for reserve PHCI. This alternative is further divided into 2 variants presented in this section below.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 196 of 281
R.3. Feasibility study
Alternative 1:
According to the first chosen rating criterion (from the lowest amount of investments to save thermal energy of 1 MWh/year after recalculation for a standard year), the support would be sufficient for 2 hospitals.
Table 45. Distribution of the demand for funding and programme funds of the reserve list according to the lowest sum of investments to savethermal energy 1 MWh/year after reassessment for a standard year.
No Name of hospital
Sparing MWh/year
after reassessment for a standard
year
Investments for increase of energy
efficiency, LTL without VAT
Investments for increase of energy efficiency, LTL with
VAT
Investments per 1 MWh/year for
sparing 1LTL/MWh/year
1 Public institution Silute hospital 343.00 1,473,489.50 1,782,922.30 5,198.022 Public institution Svencionys hospital 276.00 1,277,326.45 1,545,565.00 5,599.87
Total: 3,328,487.30 -
3Public institution Rokiskis district hospital 74.00 367,253.72 444,377.00 6,005.09
4 Public institution Radviliskis hospital 373.00 2,366,595.04 2,863,580.00 7,677.165 Public institution Kretinga hospital 156.00 1,522,394.21 1,842,097.00 11,808.316 Public institution Vilkaviskis hospital 129.00 1,300,322.31 1,573,390.00 12,198.057 Public institution Jonava hospital 48.00 1,078,181.82 1,304,60.00 27,179.178 Public institution Raseiniai hospital 86.00 2,030,314.05 2,456,680.00 28,566.05
9Public institution Klaipeda children’s hospital 10.00 484,917.36 586,750.00 0.00
10
Public institution VU hospital Santariskiu clinic (intensive therapy services) 7.00 363,636.36 440,000.00 0.00
11 Public institution Salcininkai hospital1 0.00 0.00 0.00 0.00
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 197 of 281
R.3. Feasibility study
12 Public institution Lazdijai hospital2 0.00 0.00 0.00 0.00Total: 1,502.00 12,264,430.83 14,839,961.30 -
Alternative 2:According to the second chosen rating criterion (from the highest to the lowest expected energy efficiency), the support would be sufficient for 1 hospital.
Table 46. Distribution of the demand for funding and programme funds of the reserve list according to the highest expected energy efficiency.
No Name of hospitalSparing MWh/year after reassessment for a standard year
Investments for increase of energy
efficiency, LTL without VAT
Investments for increase of energy efficiency, LTL with
VAT1 Public institution Radviliskis hospital 373.00 2,366,595.04 2,863,580.00
Total: 2,863,580.002 Public institution Silute hospital 343.00 1,473,489.50 1,782,922.303 Public institution Svencionys hospital 276.00 1,277,326.45 1,545,565.004 Public institution Kretinga hospital 156.00 1,522,394.21 1,842,097.005 Public institution Vilkaviskis hospital 129.00 1,300,322.31 1,573,390.006 Public institution Raseiniai hospital 86.00 2,030,314.05 2,456,680.007 Public institution Rokiskis district hospital 74.00 367,253.72 444,377.008 Public institution Jonava hospital 48.00 1,078,181.82 1,304,600.009 Public institution Klaipeda children’s hospital 10.00 484,917.36 586,750.00
10Public institution VU hospital Santariskiu clinic (intensive therapy services) 7.00 363,636.36 440,000.00
11 Public institution Salcininkai hospital1 0.00 0.00 0.00
KONFIDENCIALU document.docx

Ministry of Health of the Republic of Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of
energy-sparing technologies Page 198 of 281
R.3. Feasibility study
12 Public institution Lazdijai hospital2 0.00 0.00 0.00Total: 1,502.00 12,264,430.83 14,839,961.30
Since during the programme implementation there can be doubts as to the going concern of PHCI, it is recommended to select alternative I, based on which better measures would be implemented than planned at the start of preparation of the feasibility study.
KONFIDENCIALU document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 199 of 281
R.3. Feasibility study
10. Information system analysis
10.1 Methodology of the information system analysisIn the picture below, the scheme of the information system analysis methodology is presented including the activities of the information system analysis.
Picture No 36 – Activities of the information system analysis
In the following subdivisions of chapter 10 of this document “Information system analysis“, the descriptions of each performed activity of the information system analysis and results received during their performance are presented.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 200 of 281
R.3. Feasibility study
10.2 Assessment of the present data collection and analysis systems
In the table below, the main recipients of the data submitted by PHCI and the submitted data are presented.
Table 47. Recipients of the data submitted by PHCI and the submitted dataNo
Recipient of data/ document
Submitted data Forms
1. Ministry of Health of the Republic of Lithuania and its subordinate institutions
Statistical data ► ► No 003-1/a - „Medical sheet of pregnancy termination“;
► ► No 010/a - „Record journal of pregnant women, delivering women and neonates“;
► ► No 096/a - „History of birth (partogramme, course of pregnancy, protocol of surgical operation)“;
► ► No 097/a - „History of development of the neonate;
► ► No 025-111/a – Records of the course of pregnancy (Personal history of health)“;
► ► No 075/a - „Journal of observation of pregnant women“;
► No 113/a - „Card of a pregnant woman, delivering woman and neonate“.
► No 103-1/a - „ Birth certificate “;
► No 025/a – “Personal history of health (ambulatory card)“;
► No 003/a - „Medical history of stationary treatment“.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 201 of 281
R.3. Feasibility study
No
Recipient of data/ document
Submitted data Forms
2. State Patients’ Fund under the Ministry of Health of the Republic
Data for performance of payments for provided services
► No 066/a-LK – Statistical card of the discharged person.
3. Health Information Centre of the Institute of Hygiene
Statistical data ► ► No 010-1-1/a - „Card of the neonate“;
► ► No 010-2-1/a - „Car of the stillborn“.
4. Physical entities Certificate approving the fact of birth of the child and other data.
► No 103-1/a - Birth certificate.
Below in this chapter, the assessment of the systems of collection and analysis of the data of PHCI about pregnant women, delivering women and neonates is presented.
After performing interviews in PHCI, it was established that the systems of collection and analysis of the data of PHCI about pregnant women, delivering women and neonates are used by the PHCI listed below:
► Obstetric-gynaecologic clinic of KMUC;► Neonatal clinic of KMUC;► Obstetric-gynaecologic clinic of VMUH.
10.2.1 Analysis of the programme used by the obstetric-gynaecologic clinic of KMUC
In the obstetric-gynaecologic clinic of KMUC, a specialized programme for collection and analysis of the data on pregnant women, delivering women and neonates is used; it was developed by a private company according to a special order of the obstetric-gynaecologic clinic of KMUC.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 202 of 281
R.3. Feasibility study
Table 48. Analysis of the specialized programme for the data collection and analysis used by the obstetric-gynaecologic clinic of KMUC No
Aspect Description
1. Legal environment
The employees of the obstetric-gynaecologic clinic of KMUC use this programme according to the internal procedure approved by docent dr. Mindaugas Kliucinskas, the head of the department of birth of the obstetric-gynaecologic clinic of KMUC.
Note: The role of the specialized programme used by the obstetric-gynaecologic clinic of KMUC for collection of the data about pregnant women, delivering women and neonates, the system manager and administrator are not formalized, its functions, users and managed data are not defined. The documentation of this programme (specification, regulations and other documents) is not prepared, either.
2. Objectives To make preconditions for the collection and analysis of the data on pregnant women, delivering women and neonates.
3. Organizational environment
Programme manager: ► Obstetric-gynaecologic clinic of KMUC.
Programme administrator: ► Obstetric-gynaecologic clinic of KMUC.
Providers of data:► Employees of the obstetric-gynaecological clinic of
KMUC.
Recipients of data: ► Employees of the obstetric-gynaecological clinic of
KMUC.
Note: The organizational environment of the programme is not formally defined.
4. Information structure
The main groups of data accumulated in the programme:► (D.1) Personal data of patients;► (D.2) Data of births;► (D.3) Data of neonates;
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 203 of 281
R.3. Feasibility study
No
Aspect Description
► (D.4) Data of former pregnancies;► (D.5) Data of performed examinations;► (D.6) Clinical data.
Note: The information structure of the programme is not formally defined.
5. Functional structure
The main functional parts of the programme:► (F.1) Functional module of planning operations;► (F.2) Functional module of bed management;► (F.3) Functional module of patient registration and
search;► (F.4) Functional module of report generation;► (F.5) Functional module of registration of births in
another place;► (F.6) Functional module of message generation and
sending;► (F.7) Functional module of programme
administration.
Note: The functional structure of the programme is not formally defined.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 204 of 281
R.3. Feasibility study
Picture No 37 – Screen form of the specialized programme for the data collection and analysis used by the obstetric-gynaecological clinic of KMUC
Note: ► The programme is web based.
10.2.2 Analysis of the programme used by the neonatal clinic of KMUC In the neonatal clinic of KMUC, a specialized programme for collection and analysis of the data on pregnant women, delivering women and neonates is used; it was developed by a private company according to a special order of the neonatal clinic of KMUC.
Table 49. Analysis of the specialized programme for the data collection and analysis used by the neonatal clinic of KMUCNo
Aspect Description
Legal environment
The employees of the neonatal clinic of KMUC use this programme according to the internal procedure approved by the head of the department of reanimation and
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 205 of 281
R.3. Feasibility study
No
Aspect Description
intensive therapy of neonates of KMUC.
Note: The role of the specialized programme used by the neonatal clinic of KMUC for collection of the data about pregnant women, delivering women and neonates, the system manager and administrator are not formalized, its functions, users and managed data are not defined. The documentation of this programme (specification, regulations and other documents) is not prepared, either.
Objectives To make preconditions for the collection and analysis of the data on pregnant women, delivering women and neonates.
Organizational environment
Programme manager: ► Neonatal clinic of KMUC.
Programme administrator: ► Neonatal clinic of KMUC.
Providers of data:► Employees of the neonatal clinic of KMUC.
Recipients of data: ► Employees of the neonatal clinic of KMUC.
Note: The organizational environment of the programme is not formally defined.
Information structure
The main groups of data accumulated in the programme:► (D.1) Personal data of patients;► (D.2) Data of births;► (D.3) Data of neonates;► (D.4) Data of former pregnancies;► (D.5) Data of performed examinations;► (D.6) Clinical data.
Note: The information structure of the programme is not formally defined.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 206 of 281
R.3. Feasibility study
No
Aspect Description
Functional structure
The main functional parts of the programme:► (F.1) Functional module of patient registration and
search;► (F.2) Functional module of data analysis;► (F.3) Functional module of report formation;► (F.4) Functional module of programme
administration.
Note: The functional structure of the programme is not formally defined.
Picture No 38 – Data entering screen form No 1 of the specialized programme for the data collection and analysis used by the neonatal clinic of KMUC
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 207 of 281
R.3. Feasibility study
Picture No 39 – Data entering screen form No 2 of the specialized programme for the data collection and analysis used by the neonatal clinic of KMUC
Note: ► The programme used by the neonatal clinic of KMUC is developed in the
programming language Visual FoxPro.
► In Appendix No 1 to this document, the extent and structure of the data accumulated in the specialized programme for the data collection and analysis used by the neonatal clinic of KMUC is presented.
10.2.3 Analysis of the programme used by the obstetric-gynaecologic clinic of VMUH
In the obstetric-gynaecologic clinic of VMUH, a specialized programme for collection and analysis of the data on pregnant women, delivering women and neonates is used; it was developed by a private company according to a special order of the obstetric-gynaecologic clinic of VMUH.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 208 of 281
R.3. Feasibility study
Table 50. Analysis of the specialized programme for the data collection and analysis used by the obstetric-gynaecologic clinic of VMUHNo
Aspect Description
Legal environment
The employees of the obstetric-gynaecologic clinic of VMUH use this programme according to the internal procedure approved by Grazina Drasutiene, the head of the obstetric-gynaecologic clinic of VMUH.
Note: The role of the specialized programme used by the obstetric-gynaecologic clinic of VMUH for collection of the data about pregnant women, delivering women and neonates, the system manager and administrator are not formalized, its functions, users and managed data are not defined. The documentation of this programme (specification, regulations and other documents) is not prepared, either.
Objectives To make preconditions for the collection and analysis of the data on pregnant women, delivering women and neonates.
Organizational environment
Programme manager: ► Obstetric-gynaecologic clinic of VMUH.
Programme administrator: ► Obstetric-gynaecologic clinic of VMUH.
Providers of data:► Employees of the obstetric-gynaecological clinic of
VMUH.
Recipients of data: ► Employees of the obstetric-gynaecological clinic of
VMUH.
Note: The organizational environment of the programme is not formally defined.
Information structure
The main groups of data accumulated in the programme:► (D.1) Data necessary for the clinic management;► (D.2) Personal data of patients;
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 209 of 281
R.3. Feasibility study
No
Aspect Description
► (D.3) Data of births;► (D.4) Data of neonates;► (D.5) Data of former pregnancies;► (D.6) Data of performed examinations;► (D.7) Clinical data.
Note: The information structure of the programme is not formally defined.
Functional structure
The main functional parts of the programme:► (F.1) Functional module of patient registration and
search;► (F.2) Functional module of data analysis;► (F.3) Functional module of report formation;► (F.4) Functional module of programme
administration.
Note: The functional structure of the programme is not formally defined.
Note: ► The programme used by the obstetric-gynaecological clinic of VMUH was
developed using MS Access.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 210 of 281
R.3. Feasibility study
Picture No 40 – Data entering screen form No 1 of the specialized programme for the data collection and analysis used by the obstetric-gynaecological clinic of VMUH
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 211 of 281
R.3. Feasibility study
Picture No 41 – Data entering screen form No 2 of the specialized programme for the data collection and analysis used by the obstetric-gynaecological clinic of VMUH
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 212 of 281
R.3. Feasibility study
Picture No 42 – Data entering screen form No 3 of the specialized programme for the data collection and analysis used by the obstetric-gynaecological clinic of VMUH
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 213 of 281
R.3. Feasibility study
10.2.4 Analysis of the programme used by the Swedish hospitals of intensive care of neonates
In the Swedish hospitals of intensive care of neonates, a specialized programme for collection and analysis of the data about pregnant women, delivering women and neonates is used; it was developed by a private company MedSciNet AB which also has an established subdivision in Lithuania – UAB MedSciNet Lt.
Table 51. Analysis of the specialized programme for the data collection and analysis used by all the Swedish hospitals of intensive care of neonates No
Aspect Description
1. Legal environment
PNQ is the Registered National Quality Register of Sweden.
2. Objectives This system is aimed at answering the questions: which medical care treatment approaches are applied, how they differ in various regions of the country and in how these differences influence the results of treatment and children’s health in the future.By using this register, the following questions can be answered:
► How does the availability of specialized care influence the results of treatment?
► How does the obstetric care influence the result of treatment in serious cases of premature birth?
► How do the methods of treatment of neonatologists influence the result of treatment in serious cases of premature birth?
► How do the differences between the methods of treatment in different regions of the country influence the results of treatment?
► How do the differences of reasons for hospitalization (indications) influence the duration and tariffs of treatment?
►
3. Organizational environment
Programme manager: ► Umeå landsting (regional authority; health care of
Sweden is organized from local taxes, therefore legal issues are mostly resolved at this level).
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 214 of 281
R.3. Feasibility study
No
Aspect Description
Programme administrator: ► Swedish Community of Neonatologists (makes
decisions related with the contents of accumulated data and programme functionality).
Providers of data:► Employees of all neonatal departments of Swedish
hospitals.
Recipients of data: ► Medical staff working in neonatal departments; ► Pediatricians and other specialists who take over
the treatment after the neonatal period (they get reports for improvement of methods of work and quality).
► Specialists of the Ministry of Health forming the policy of health care.
► Society.
4. Information structure
The main groups of data accumulated in the programme:► Information about the course of pregnancy;► Information about the birth;► Information about the neonate and his/her care.
Note: ► Information accumulated in the programme fully
covers „EURONEOSTAT Perinatal dataset“, information is exported in the format suitable for EURONEOSTAT.
5. Functional structure
The main functional parts of the programme:► (1) Module of data entering:
► (1.1) Woman’s diseases;► (1.2) Pregnancy, complications;► (1.3) Birth;► (1.4) Information about the state of the
neonate and treatment;► (1.5) Movement to another medical institution;► (1.6) Epicrisis formation.
► (2) Module of standard (pre-prepared) reports;
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 215 of 281
R.3. Feasibility study
No
Aspect Description
► (3) Functional module of report generation;► (4) Module of data export;► (5) Measures for data quality assurance (lists of
non-filled-in forms etc.);► (6) Module of administration of the programme and
its users.
Picture No 43 – Screen form of the specialized programme used by all the Swedish hospitals of intensive care of neonates – „Information of the umbilical cord blood
examination“
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 216 of 281
R.3. Feasibility study
Picture No 44 – Screen form of the specialized programme used by all the Swedish
hospitals of intensive care of neonates – „Information of reanimation“
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 217 of 281
R.3. Feasibility study
Picture No 45 – Screen form of the specialized programme used by all the Swedish hospitals of intensive care of neonates – „Eye care protocol“
CONFIDENTIAL document.docx
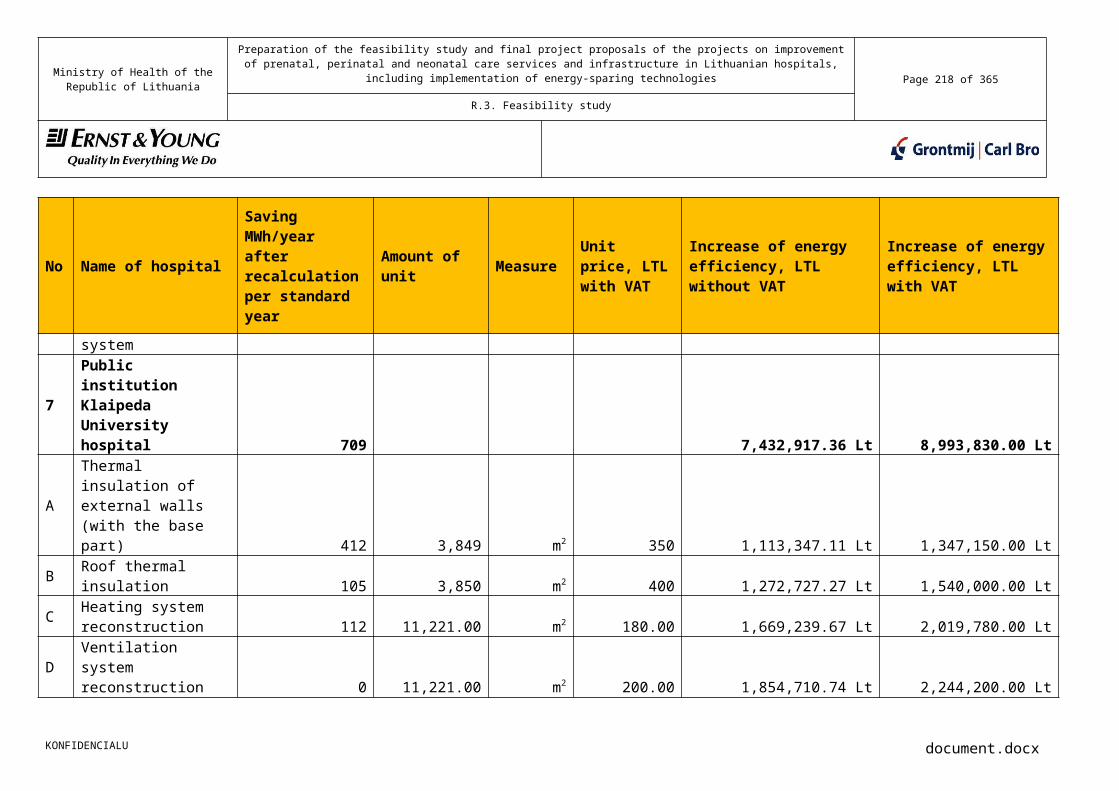
Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 218 of 281
R.3. Feasibility study
Picture No 46 – Screen form of the specialized programme used by all the Swedish hospitals of intensive care of neonates – „Child’s treatment“
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 219 of 281
R.3. Feasibility study
10.2.5 Analysis of the data collected by the Health Information Centre of the Institute of Hygiene
Presently the Health Information Centre of the Institute of Hygiene (hereinafter - HICIH) collects the report forms listed below (hereinafter – Report forms) from all PHCI providing obstetric-gynaecological and neonatal services:
► No 010-1-1/a – “Card of the neonate“;► No 010-2-1/a - ”Card of the stillborn“.
PHCI providing obstetric-gynaecological and neonatal services fill-in paper Report forms and sends the filled-in Report forms to HICIH.
Before sending paper forms to HICIH, some PHCI enter the data of those paper forms to the specialized programme of HICIH functioning in the environment of DOS (Disk Operating System) operating system. Then the entered data is transferred electronically to the database of HICIH.
About 50% of the data of all report forms are entered in the specialized programme of HICIH and transmitted to HICIH in electronically.
After getting paper Report forms, HICIH performs the data quality verification. The data of Report forms which was not transmitted in an electronic form is entered in the database HICIH. In case of getting paper Report forms the data of which was transmitted in an electronic form, HICIH verifies if the information included in paper Report forms corresponds with the electronically transmitted data. In case of any discrepancies between the data in paper Report forms and the electronically transmitted data, the employees of PHCI who filled-in Report forms are contacted and the information submitted in the Report forms and in an electronic form is corrected.
HICIH prepares a summarized statistical publication from the data collected from PHCI.
Note: ► Currently, PHCI administrate the Report forms No. 010-1-1/a – “Card of the
neonate“ and No 010-2-1/a – “Card of the stillborn“ in accordance with the Order No. 515 of 29 November 1999 of the Minister of Health of the Republic of Lithuania “On the procedure for the operating accounting and reporting at health care institutions”.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 220 of 281
R.3. Feasibility study
Picture No 47 – No 010-1-1/a - „Card of the neonate“ – front side
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 221 of 281
R.3. Feasibility study
Picture No 48 – No 010-1-1/a - „Card of the neonate“ – back side
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 222 of 281
R.3. Feasibility study
Picture No 49 – No 010-2-1/a - „Card of the stillborn“ – front side
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 223 of 281
R.3. Feasibility study
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 224 of 281
R.3. Feasibility study
Picture No 50 – No 010-2-1/a - „Card of the stillborn“ – back side
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 225 of 281
R.3. Feasibility study
10.2.6 Assessment of the present data collection systems and recommendations for their improvement
Considering the results of the performed analysis of the present data collection systems, the assessment of the present data collection systems and recommendations for their improvement are presented in the table below.
Table 52. Assessment of the present data collection systems No
Data collection system
Assessment of the data collection system and recommendations for its improvement
1. System used in the obstetric-gynaecological clinic of KMUC
AssessmentThe data collection system used by the obstetric-gynaecological clinic of KMUC is not prepared for accumulation of the data of all pregnant women, delivering women and neonates. This data collection system was developed in the programming language Visual Basic; therefore, this system is difficult to develop and expand. The instruments for the data analysis and report formation realized in the system are very primitive. The system is not formalized and the system documentation is not prepared, either.
Note:► The data accumulated in the system does not involve
all the data which has been indicated by PHCI and associated institutions as necessary to accumulate, exchange, analyze and form reports.
Recommendations for its improvementConsidering the fact, the data collection system used by the obstetric-gynaecological clinic of KMUC is not formalized, the system documentation is not prepared and the system is developed in the programming language Visual Basic (not ensuring portability) the system will be difficult to make compliant with eHSCI IS and difficult to develop and expand, and the instruments for the data collection and analysis realized in the system do not meet the objectives raised for IS PWDWN in order to develop IS PWDWN satisfying the needs of all PHCI and functioning at the national level; we do not recommend
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 226 of 281
R.3. Feasibility study
No
Data collection system
Assessment of the data collection system and recommendations for its improvement
to develop and expand this system or keep as basis for the development of IS PWDWN.
5. System used in the neonatal clinic of KMUC
AssessmentThe data collection system used by the neonatal clinic of KMUC is not prepared for accumulation of the data of all pregnant women, delivering women and neonates. This data collection system was developed in the programming language Visual Basic; therefore, this system is difficult to develop and expand. The instruments for the data analysis and report generation realized in the system are very primitive. The system is not formalized and the system documentation is not prepared, either.
Note:► The data accumulated in the system does not involve
all the data which has been indicated by PHCI and associated institutions as necessary to accumulate, exchange, analyze and form reports.
Recommendations for its improvementConsidering the fact the data collection system used by the neonatal clinic of KMUC is not formalized, the system documentation is not prepared and the system is developed in the programming language Visual Basic difficult to make compliant with eHSCI IS and develop and expand, and the instruments for the data collection and analysis realized in the system do not meet the objectives raised for IS PWDWN in order to develop IS PWDWN satisfying the needs of all PHCI and functioning at the national level; we do not recommend to develop and expand this system or keep as basis for the development of IS PWDWN.
9. System used in the obstetric-gynaecological clinic of VMUH
AssessmentThe data collection system used by the obstetric-gynaecological clinic of VMUH is not prepared for accumulation of the data of all pregnant women,
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 227 of 281
R.3. Feasibility study
No
Data collection system
Assessment of the data collection system and recommendations for its improvement
delivering women and neonates. This data collection system was developed on the basis of the MS Access software package; therefore, this system is difficult to develop and expand. The instruments for the data analysis and report formation realized in the system do not meet the objectives raised for IS PWDWN. The system is not formalized and the system documentation is not prepared, either.
Note:► The data accumulated in the system does not involve
all the data which has been indicated by PHCI and associated institutions as necessary to accumulate, exchange, analyze and form reports.
Recommendations for its improvementConsidering the fact the data collection system used by the obstetric-gynaecological clinic of VMUH is not formalized, the system documentation is not prepared and the system is developed on the basis of the MS Access software package difficult to make compliant with eHSCI IS and develop and expand, and the instruments for the data collection and analysis realized in the system do not meet the objectives raised for IS PWDWN in order to develop IS PWDWN satisfying the needs of all PHCI and functioning at the national level; we do not recommend to develop and expand this system or keep as basis for the development of IS PWDWN.
13. System used by the Swedish hospitals for collection of the data of pregnant women, delivering women and neonates
AssessmentThe data collection system used by the Swedish hospitals is prepared to accumulate all the data about pregnant women, delivering women and neonates used in the Swedish obstetric-gynaecological and neonatal practices. This data collection system is developed on the basis of Microsoft .NET Framework and is suitable for uncomplicated modification, expansion and data exchange with other systems.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 228 of 281
R.3. Feasibility study
No
Data collection system
Assessment of the data collection system and recommendations for its improvement
Note: ► The system used by the Swedish hospitals for
collection of the data of pregnant women, delivering women and neonates is not based on open standards.
► The data accumulated in the system does not involve all the data which has been indicated by PHCI and associated institutions as necessary to accumulate, exchange, analyze and form reports.
Recommendations for its improvementConsidering the fact that the data collection system used by the Swedish hospitals is prepared to accumulate all the data of pregnant women, delivering women and neonates used in the Swedish obstetric-gynaecological and neonatal practices and this data collection system is developed on the basis of Microsoft.NET Framework, suitable for uncomplicated modification, expansion and data exchange with other systems, we recommend to assess the possibility to use the data collection system used by the Swedish hospitals as basis for the development of IS PWDWN.
10.3 Needs of PHCI and associated institutions and recommendations for their implementation
In this chapter, generalized needs of PHCI and associated institutions for the data accumulation, exchange, analysis and report generation and recommendations for their implementation are presented.
10.3.1 Generalized needs of PHCI and associated institutions for the data accumulation, exchange, analysis and report generation
In this chapter, generalized needs of PHCI and associated institutions for the data accumulation, exchange, analysis and report generation are presented.
Table 53. Needs of PHCI and related institutions
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 229 of 281
R.3. Feasibility study
No
Data collection system
Assessment of the data collection system
1. Data collection Representatives of PHCI and associated institutions indicated their need to only accumulate the minimal set of the data about pregnant women, delivering women and neonates which would be necessary for qualitative assessment and improvement of the methods of treatment and which major part presently is filled-in in the forms presented below:► No 010-1-1/a - „Card of the neonate“ (hereinafter –
Card of the neonate);► No 010-2-1/a - „Card of the stillborn“ (hereinafter –
Card of the stillborn).
Notes:► The needs of representatives of PHCI and associated
institutions for the data accumulation, exchange, analysis and report formation were approved by representatives of the Lithuanian Society of Obstetricians and Gynaecologists, the Neonatal Association and the Ministry of Health and recorded in the minutes of the meeting of representatives of the Lithuanian Society of Obstetricians and Gynaecologists, the Neonatal Association and the Ministry of Health on 7 June 2010;
► During the meeting of representatives of the Lithuanian Society of Obstetricians and Gynaecologists, the Neonatal Association and the Ministry of Health on 7 June 2010, a decision was made that the need for collection of additional data about pregnant women, delivering women and neonates would be determined at the stage of the detailed analysis of the information system implementation with the help of the Lithuanian Society of Obstetricians and Gynaecologists and the Neonatal Association.
2. Data exchange Representatives of PHCI and related institutions indicated the need to exchange the data of pregnant women, delivering women and neonates:► After developing eHSCI IS, exchanging the data of
pregnant women, delivering women and neonates should be implemented through the data exchange
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 230 of 281
R.3. Feasibility study
No
Data collection system
Assessment of the data collection system
component of eHSCI IS;► As long as eHSCI IS is not developed, exchanging the
data of pregnant women, delivering women and neonates should be implemented through the instruments of the information system being developed.
3. Data analysis ► Representatives of PHCI and related institutions expressed the need that specialized instruments for the data analysis should be realized in the information system being developed.
4. Report formation ► Representatives of PHCI and related institutions expressed the need that the set of standard reports should be realized in the information system being developed.
10.3.2 Minimal set of the data of pregnant women, delivering women and neonates
Representatives of PHCI and associated institutions indicated their need to only accumulate the minimal set of the data about pregnant women, delivering women and neonates which would be necessary for qualitative assessment and improvement of the methods of treatment and which major part presently is filled-in in the forms presented below:
► No 010-1-1/a - ”Card of the neonate“ ;► No 010-2-1/a – “Card of the stillborn“.
Note:► During the meeting of representatives of the Lithuanian Society of Obstetricians
and Gynaecologists, the Neonatal Association and the Ministry of Health on 7 June 2010, a decision was made that the need for collection of additional data about pregnant women, delivering women and neonates would be determined at the stage of the detailed analysis of the information system implementation with the help of the Lithuanian Society of Obstetricians and Gynaecologists and the Neonatal Association.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 231 of 281
R.3. Feasibility study
10.3.3 Essence of development of IS and justification of the needIn this chapter the essence of development of IS and justification of the need is presented.
Table 54. Measures which could be applied after developing ISNo
Fields of use of IS
Benefit receiver
Direct benefit Risk/danger
1. ► Data transmission to ESI
► Every patient
► Patient’s ESI is filled-in since his/her birth
-
2. ► Data transmission to the civil registry and for receipt of benefit for the born child
► Every patient
► Decrease in administrative burden for parents after the birth of the child
► Civil registries and subdistricts will not be ready to accept data
3. ► Analysis of a long-lasting effect of diagnoses and methodologies of treatment at the national level
► Every patient
► Ministry of Health
► Republic of Lithuania
► Improvement of diagnoses and methods of treatment at the national level
► There is a risk that it will not be executed as long as this function is not assigned to a specific organizational unit
4. ► Self-analysis of the results of work
► Every PHCI► Ministry of
Health
► Improvement of diagnoses and methods of treatment at the level of every PHCI
► There is a risk that it will be only by used by high-maturity PHCI
5. ► Scientific and academic research
► Certain PHCI► Republic of
Lithuania
► Use of accumulated data for scientific research and works
► There is a risk that it will be only by used by PHCI employing experts who participate in the academic
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 232 of 281
R.3. Feasibility study
No
Fields of use of IS
Benefit receiver
Direct benefit Risk/danger
and research field
6. ► Report preparation
► Every PHCI ► Decrease in the administrative burden for PHCI
► Increase in administrative burden during the transitional period due to possible overlapping of activities
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 233 of 281
R.3. Feasibility study
10.3.4 RecommendationsIn this chapter, the recommendations for the data accumulation, exchange, analysis and report formation for PHCI are presented.
Table 55. Recommendations for the data accumulation, exchange, analysis and report formation for PHCINo
Recommendation
1. ► In order to ensure continuity of the medical history of the patient, it is recommended to exchange the health data of pregnant women, delivering women and neonates indicated by PHCI as necessary to exchange with other PHCI and transfer to ESI in order to ensure exchange of the health data about pregnant women, delivering women and neonates between PHCI at the same time.
2. ► In order to ensure continuity of the data administration, it is recommended to provide PHCI with a possibility to use technical instruments with which every PHCI would be able to accumulate, exchange, analyze and generate reports about pregnant women, delivering women and neonates by relieving PHCI of the IT infrastructure administration.
3. ► It is recommended to ensure access to the data indicated by PHCI as necessary for the data accumulation, exchange, analysis and report formation according to the target groups (roles of users).
4. ► It is recommended to automatically generate forms necessary for the recipients of the data (Ministry of Health of the Republic of Lithuania, State Patients’ Fund under the Ministry of Health of the Republic, Health Information Centre of the Institute of Hygiene, natural persons) from the data accumulated by PHCI and transmit them with help of information systems, i.e., at the level system - system by giving up printing paper forms and sending them by regular mail.
5. ► It is recommended to transmit the data necessary for the registration of a child to the civil registries from the data entered by PHCI to the information system under development through the information system of information systems of national institutions (hereinafter – ISISNI) at the level system - system by creating an electronic service „Registration of a
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care
services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies Page 234 of 281
R.3. Feasibility study
No
Recommendation
child“. Thus, it would be possible to eliminate the intermediary link (parents) for communicating the fact about the birth of a child to the civil registries and printing form No 103-1/a - ”Birth Certificate “ on paper and delivering it to the civil registry for the registration of the child.
► Moreover, the civil registries would be able to automatically transmit the data to the subdistricts upon getting the fact of the birth of the child and initiate granting benefits to the parents for the born child.
CONFIDENTIAL document.docx

Lietuvos Respublikos sveikatos apsaugos ministerija
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies 235 lapas iš 281
R.3. Feasibility study
10.4 Analysis of the information technology infrastructure of PHCIIn the table below, the data collected during the information technology infrastructure analysis of PHCI is presented
Table 56. Data collected during the information technology infrastructure analysis of PHCINo Name of hospital Computerized workstations (CW)
Speed of internet
ServersPresent
server load
Separate room for server
storage
Network infrastructure Present throughput
of local networkIII level Available amount
of CWDeficient amount
of CWAvailable amount of
serversType of servers
Routers
Separators
Concentrators
Firewalls
1Public institution Kaunas Medical University Clinic, Clinic of Obstetrics and Gynaecology
19 6Non-
satisfactory
1
Non-satisfactory
Available
- 2 - - Non-
satisfactory2 Public institution Kaunas Medical
University Clinic, Neonatal Clinic
3Public institution Vilnius city University Hospital, Clinic of Obstetrics and Gynaecology
15 30Satisfactory
0-
Non-satisfactory Not
available- 3 - -
Satisfactory
4 Public institution Vilnius University Children’s Hospital, Neonatal Clinic
1 10 Satisfactory 5 Network/ DB/ Mail
Non-satisfactory Available 1 4 - - Satisfactory
IIB level 5 Public institution VU hospital Santariskiu
Clinic Central branch3 50 Satisfactory 0 - Non-
satisfactoryNot
available- - - - Satisfactory
6Public institution Klaipeda University Hospital
1 10Satisfactory
9 Files/ Network/ DB/
Mail/ Applications Satisfactory
Available1 2 - 1
Satisfactory
7 Public institution Vilnius maternity home 18 50 Satisfactory 0 - -Not
available4 - - - -
8 Public institution Kaunas 2nd clinical hospital
- - - - - - - - - - - -9 Public institution Siauliai county hospital 8 - Satisfactory 1 Proxy Satisfactory Available 4 - Satisfactory10
Public institution Panevezys county hospital
4 4 Satisfactory 0 - - Available - 1 - - SatisfactoryIIA level11
P. Mazylio maternity home (branch of Kaunas 2nd clinical hospital)
5 6 Satisfactory 1 Applications Non-satisfactory
Not available
3 1 - - Non-satisfactory
12
Christian maternity home (branch of public institution Kaunas county hospital)
14 3 Non-satisfactory
0 - - Available 2 3 - - Satisfactory13
Public institution Alytus county S.Kudirkos hospital
9 14 Non-satisfactory
3 Files/ AD/ Proxy
Non-satisfactory Available - 4 - - Satisfactory
14 Public institution Marijampole hospital 4 2 Satisfactory 1 DB Satisfactory Not
available- 2 - - Satisfactory
15 Public institution Telsiai county hospital - 4 - - - Non-
satisfactory - - - - - -16 Public institution Taurage county hospital 2 7 Non-
satisfactory3 Network/ DB/
Applications Satisfactory Not available
1 - - - Non-satisfactory
17 Public institution Utena county hospital - 2 - 0 - - - - - - - -18 Public institution Trakai hospital - - Non-
satisfactory0 - Non-
satisfactory - - - - - -19 Public institution Mazeikiai hospital 2 2 Non-
satisfactory1 DB Satisfactory Not
available1 6 - - Non-
satisfactory20 Public institution Ukmerge hospital - 1 Satisfactory - - - - - - - - -21 Public institution Radviliskis hospital 1 2 Satisfactory 1 DB Satisfactory Available 3 - - Satisfactory22 Public institution Silute hospital - - Non-
satisfactory0 - - Available - - - - Non-
satisfactory23 Public institution Visaginas hospital 1 7 Satisfactory 1 Applications Non-
satisfactoryNot
available- 3 - - Satisfactory
CONFIDENTIAL document.docx

Lietuvos Respublikos sveikatos apsaugos ministerija
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including implementation of energy-sparing technologies 236 lapas iš 281
R.3. Feasibility study
24 Public institution Pasvalys hospital - 2 Satisfactory - - - - - - - - -25 Public institution Kedainiai hospital - - - - - - - - - - - -26 Public institution Jonava hospital - - - - - - - - - - - -
27
Public institution Salcininkai district hospital
1 -Satisfactory
4 Files/ Network/ DB/ Applications
Satisfactory -- - - -
-
28 Public institution Kretinga hospital - - - - - - - - - - - -29 Public institution Lazdijai hospital - 3 - - - - - - - - - -30 Public institution Raseiniai hospital - 2 Satisfactory - - - - - - - - -31 Public institution Vilkaviskis hospital - 3 - - - - - - - - - -32 Public institution Rokiskis district hospital - 3 Satisfactory - - - - - - - - -33
Public institution Svencionys district hospital
- - - - - - - - - - - -
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 237 of 281
R.3. Feasibility study
After performing the analysis of the information technologies currently available to PHCI, it was determined that presently most PHCI did not have any information technology infrastructure, thus, it is recommended to consider that and when developing IS PWDWN to raise a requirement that the developed IS PWDWN has to function without big resources of the information technology infrastructure, i.e., a centralized information system with one common database has to be developed where the data of separate PHCI are logically separated and the representatives of PHCI are able to connect to the centralized information system by using a web based browser from their usual computerized workstation.
Presently most computerized workstations of PHCI are fully used for solving other issues not related with ordering of the data of pregnant women, delivering women and neonates, thus, most PHCI which have computerized workstations and a part of those not having any indicated their need for new computerized workstations will have to acquire computerized workstations by themselves in order to use IS PWDWN.
On the basis of information collected during the interview, we can see most PHCI have access to the internet communication which speed satisfies the needs of PHCI, thus, we can make an assumption most PHCI will be able to use PWDWN IS which will be accessible on the internet communication without any extra investments. The other PHCI which do not have access to the internet will have to implement access to the internet communication in order to use PWDWN IS. The expenses for implementation of access to the internet communication are not material in the context of this programme, thus, it is recommended to those PHCI which do not have access to the internet communication to implement it on the own expenses.
10.5 Assessment of skills of the staff of PHCI to work with information systems
After performing the assessment of skills of the staff of PHCI to work with information systems19, it was determined the staff of PHCI has sufficient skills of working with the developed IS PWDWN except the skills related with use of the functionality of the developed IS PWDWN which should be given to the staff of PHCI by organizing trainings of use of the functionality of IS PWDWN. It is recommended to obligate the implementer of IS PWDWN to prepare detailed instructions of use of IS PWDWN, comprehensive material for the trainings and to raise a requirement the Implementer of IS PWDWN that IS PWDWN has to be ergonomic and intuitive.
19 According to the data submitted by PHCI during the interview in March-April 2010 and information collected during visits to PHCI.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 238 of 281
R.3. Feasibility study
10.6Alternatives of IS implementation10.6.1 Alternative I
Below Alternative I is presented:► In order to satisfy the needs of representatives of PHCI and associated
institutions for accumulation, exchange and analysis of the data about pregnant women, delivering women and neonates and report generation, a centralized IS PWDWN is developed; it is common for all PHCI;
► The developed IS PWDWN only involves the minimal set of the data about pregnant women, delivering women and neonates indicated in the chapter No 10.2.2 of this document and functions independently on eHSCI IS as long as eHSCI IS is not developed, but it is developed so that IS PWDWN can function as the applicable solution of eHSCI IS after developing eHSCI IS;
► IS PWDWN is centralized and common for all PHCI, but the data of separate PHCI is fully separated logically, thus, every PHCI can only access its own data. Employees of a certain PHCI can only access depersonalized and generalized data of other PHCI;
► As long as eHSCI IS is not developed, the data exchange with PHCI having their information systems happens directly through IS PWDWN, but it is intended while developing IS PWDWN, the data exchange with PHCI having their information systems happens through the eSPI IS data exchange component after developing eHSCI IS.
In the table below, the advantages and disadvantages of Alternative I are presented.
Table 57. Advantages and disadvantages of Alternative IAdvantages Disadvantages
In case of implementing this alternative, the minimal set of the data about pregnant women, delivering women and neonates is accumulated in IS PWDWN which gives a possibility:► To accumulate, exchange and analyze the
most important data;► To perform Lithuanian (usual) qualitative
assessment of applied methods of treatment and their improvement;
► To discontinue using the presently filled-in forms of the Neonate and Stillborn.
The scope of this alternative would not enable a decrease in the administrative burden for the employees of PHCI and associated institutions by discontinuing the use of the presently filled-in statistical forms (except those of the Neonate and Stillborn).
Although in case of implementing this alternative the information technology solution of much less extent and functionality would be developed, the
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 239 of 281
R.3. Feasibility study
Advantages Disadvantages
duration of implementation of this alternative is shorter than the duration of implementation of the third alternative by 5.5 months that would develop the information technology solution of much bigger extent and functionality.
In order to implement this alternative, it is necessary to invest by 722,000 LTL less than in case of implementing the second alternative and by 1,542,000 LTL less than in case of implementing the third alternative.
In the table below, potential risks of Alternative I are presented.
Table 58. Potential risks of Alternative I No
Potential risks
1. ► Non-assurance of the continuity of eHSCI IS development , i.e., interruption of further development of eHSCI IS.
Note: ► In this case IS PWDWN would be able to function without eHSCI IS, but
the functionality of the data exchange module presented in picture No 52 and described in table No 72 would not be implemented.
2. ► Reluctance of PHCI to use the developed IS PWDWN, as PHCI will not be able to modify the information system themselves; only the manager of the information system will be able to make changes.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 240 of 281
R.3. Feasibility study
In the table below, the assessment of investments and support costs of Alternative I is presented.
Table 59. Detailed assessment of investments and support costs of Alternative IInvestments
Software: Amount
Unit price, LTL with
VAT
Sum, LTL with VAT
System softwareSoftware licences of the database management
1 50,000 50,000
Operating systems of servers for DB pool
1 9,000 9,000
Operating systems of servers 2 3,000 3,000Development of applicable software
Preparation of the specifications of IS PWDWN, project of IS PWDWN and other documentation necessary to develop IS PWDWN
1 50,000 50,000
Development of IS PWDWN20 580,000 580,000Analysis (2 employees, 100 h each)
1 40,000 40,000
Design (2 employees, 150 h each)
1 60,000 60,000
Construction (3 employees, 500 h each)
1 300,000 300,000
Implementation(2 employees, 150 h each)
1 60,000 60,000
Test operation (2 employees, 300 h each)
1 120,000 120,000
Trainings for users of IS PWDWN (100 users from all 35 PHCI)
1 18,000 18,000
Other costs related to the development of IS PWDWN
1 220,000 220,000
Technical maintenance of implementation of IS PWDWN
1 150,000 150,000
20 Note: The costs of development of IS PWDWN which would be integrated with eHSCI IS, information systems of PHCI and other institutions have been assessed according to the stages of implementation of the information system by assuming the average hourly rate of employees of the implementer is 200 LTL with VAT and expert assessment by assessing the duration of works of development of the system in hours.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 241 of 281
R.3. Feasibility study
InvestmentsAdministration of the implementation project of IS PWDWN
1 70,000 70,000
Hardware Amount
Unit price, LTL with
VAT
Sum, LTL with VAT
IT infrastructureServers 2 20,000 40,000Network equipment package 1 50,000 50,000Data storage 1 100,000 100,000
Total need for investments (LTL with VAT) 1,120,000Costs of support
Field Sum, LTL with VAT
Costs of hardware support Note: ► The costs of hardware support have been assessed by
assuming that the period of useful life of hardware is 5 years and without including the costs of computerized workstations support in the costs of hardware support. Computerized workstations would be supported by PHCI at their own expense.
38,000
Costs of software support Note: ► The costs of software support have been assessed by
assuming that the yearly costs of software support make 10%21 of the value of software.
85,000
In the table below, the assessment of the duration of implementation of Alternative I is presented.
Table 60. Assessment of the duration of implementation of Alternative INo Activity Duration
1. Preparation of the documents of the public purchase of the technical maintenance services for implementation of PWDWN IS
3 month
2. Execution of the public purchase of the technical maintenance services for implementation of PWDWN IS
5 month
21 Worldwide IT Benchmark Report 2006: Volume 2: IT Spending & Staffing Analysis: Multi-Year Trends: Pharmaceuticals & Medical Products Analysis
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 242 of 281
R.3. Feasibility study
No Activity Duration
3. Preparation of public tender documentation and project of IS PWDWN and other documentation necessary to develop IS PWDWN
2 months
4. Public procurement of the services of development and implementation of a stand-alone information system (IS PWDWN) which would be integrated with eHSCI IS, information systems of PHCI and other institutions
6 months
5. Development and implementation of a stand-alone information system (IS PWDWN) only involving the minimal set of the data about pregnant women, delivering women and neonates which would be integrated with eHSCI IS, information systems of PHCI and other institutions:
7 months
1.1. Analysis(2 employees, 100 h)
0.5 month
1.2. Design(2 employees, 150 h)
0.5 month
1.3. Construction(3 employees, 500 h)
3 months
1.4. Implementation (2 employees, 150 h)
0.5 month
1.5. Test operation(2 employees, 300)
2 months
6. Trainings for users of IS PWDWN(100 users from all 35 PHCI)
1 month
The total duration of implementation of Alternative I (certain activities of implementation of the alternative can be performed simultaneously; therefore, the sum of the duration of implementation of the activities is not equal to the total duration of implementation of the alternative).
15 months
Note: ► The duration of implementation of the activities of this alternative does not
include the document coordination with Swiss experts that is not purposeful to prognosticate in this stage; therefore the duration of implementation of these activities are preliminary.
10.6.2 Alternative IIBelow Alternative II is presented:
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 243 of 281
R.3. Feasibility study
► In order to satisfy the needs of representatives of PHCI and associated institutions for accumulation, exchange and analysis of the data about pregnant women, delivering women and neonates and report generation and decrease in administrative burden for employees of PHCI and associated institutions, a centralized IS PWDWN is developed; it is common for all PHCI and involves the minimal set of the data about pregnant women, delivering women and neonates and all data in statistical paper forms presently filled-in by employees of PHCI; it would enable to refuse the presently filled-in statistical paper forms;
► In case of implementing this alternative, IS PWDWN would be developed as basis for the development of IS PWDWN by using standard and justificatory solutions of information technologies used for the data collection, analysis and exchange in the foreign obstetric-gynaecological and neonatal practice (for example, on the basis of solutions used in the practice of Sweden or Switzerland;
► The developed IS PWDWN functions independently on eHSCI IS as long as eHSCI IS is not developed, but it is developed so that IS PWDWN can function as the applicable solution of eHSCI IS after developing eHSCI IS;
► IS PWDWN is centralized and common for all PHCI, but the data of separate PHCI is fully separated logically, thus, every PHCI can only access its own data. Employees of a certain PHCI can only access depersonalized and generalized data of other PHCI;
► As long as eHSCI IS is not developed, the data exchange with PHCI having their information systems is made directly through IS PWDWN, but it is intended while developing IS PWDWN that the data exchange with PHCI having their information systems will be made through the eSPI IS data exchange component after developing eHSCI IS.
In the table below, the advantages and disadvantages of Alternative II are presented.
Table 61. Advantages and disadvantages of Alternative IIAdvantages Disadvantages
In case of implementing this alternative, the minimal set of the data about pregnant women, delivering women and neonates and all data in statistical forms presently filled-in by employees of PHCI is accumulated in IS PWDWN which gives a possibility:► To accumulate, exchange and analyze
all data;► To perform qualitative assessment of
applied methods of treatment and their improvement based on the
It is necessary to change habits of employees of PHCI, i.e., change the model of activity by discontinuing the use of presently filled-in statistical paper forms and fill in the same data in the developed IS PWDWN.Filling-in of statistical forms is regulated by the legal acts of the Ministry of Health; therefore, in this case it would also be necessary to change the legal acts regulating filling-in of statistical
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 244 of 281
R.3. Feasibility study
Advantages Disadvantages
experience of the practice of foreign countries;
► To decrease administrative burden for the employees of PHCI and associated institutions by refusing of presently filled-in statistical paper forms and filling in the same data in the developed IS PWDWN.
forms.
Although in case of implementing this alternative the information technology solution of much bigger extent and functionality would be developed, the duration of implementation of this alternative is not longer than the duration of implementation of the first alternative that would develop the information technology solution of much less extent and functionality.
In order to implement this alternative, it is necessary to invest by 722,000 LTL more than in case of implementing the first alternative.
In order to implement this alternative, it is necessary to invest by 620.000 LTL less than in case of implementing the third alternative.
In case of implementing this alternative, the information technology solution of similar extent and functionality would be developed as in case of the third alternative that may not satisfy all needs of the representatives of PHCI, but the duration of implementation of this alternative would be shorter by 5.5 months than the duration of implementation of the third alternative.
In the table below, potential risks of Alternative II are presented.
Table 62. Potential risks of Alternative II No
Potential risks
1. ► Non-assurance of the continuity of eHSCI IS development , i.e., interruption of further development of eHSCI IS.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 245 of 281
R.3. Feasibility study
No
Potential risks
Note: ► In this case IS PWDWN would be able to function without eHSCI IS, but
the functionality of the data exchange module presented in picture No 52 and described in table No 72 would not be implemented.
2. ► Reluctance of PHCI to use the developed IS PWDWN, as PHCI will not be able to modify the information system themselves; only the manager of the information system will be able to make changes.
3. ► Reluctance of PHCI to change their habits, i.e., change the model of activity by discontinuing the use of filled-in statistical paper forms and fill in the data presently accumulated in statistical forms in the developed IS PWDWN.
► Note: Filling-in of statistical forms is regulated in the legal acts of the Ministry of Health; therefore, in this case it would also be necessary to change the legal acts regulating filling-in of statistical forms, change of which could be the means to ensure that PHCI discontinues filling in statistical forms and starts filling in the data accumulated in the statistical forms by IS PWDWN instruments.
4. ► The qualitative assessment and improvement of applied methods of treatment based on the experience of foreign practice may not be applicable to the Lithuanian obstetric-gynaecological and neonatal practice.
In the table below, the data is presented which would be accumulated in the case of implementing Alternative II of IS PWDWN.
Table 63. Data which would be accumulated in case of implementing Alternative II of IS PWDWNNo
Purpose Groups of data Forms where relevant data is currently presented
1. For accumulation
Before the birth of the neonate[the data from the first visit to the gynaecologist related to the moment of pregnancy to the moment of birth of the neonate is entered in EMH of the pregnant woman]► Clinical data:
► Data of the course of pregnancy;
► Data of development of the foetus;
► Data of performed examinations;
► Data of performed
► No 003-1/a - „Medical sheet of interruption of pregnancy“.
► No 010/a - „Record journal of pregnant women, delivering women and neonates“.
► No 075/a - „Journal of
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 246 of 281
R.3. Feasibility study
No
Purpose Groups of data Forms where relevant data is currently presented
procedures;► Anamnestic data of
former pregnancies;► Data of illnesses of the
mother.► Statistical data 22 :
► Data of the course of pregnancy;
► Data of development of the foetus;
► Data of performed examinations;
► Data of performed procedures;
► Anamnestic data of former pregnancies;
► Data of illnesses of the mother.
► Data for performing payments for provided services:► Personal data;► Data of provided
services.
observation of pregnant women“.
► No 113/a - „Card of the pregnant women, delivering woman and neonate“.
► No 025-111/a - „Records of the course of pregnancy (Personal history of health)“.
► No 066/a-LK - „Statistical card of the discharged person“.
Immediately after birth of the neonate [the data from the moment of birth of the neonate to 1 month after the moment of birth of the neonate is entered in EMH of the delivering woman and newly opened EMH of the neonate]► Clinical data:
► Data of performed examinations;
► Data of performed procedures;
► Data of birth;► Data of the neonate;► Data of development
of the neonate;► Data of illnesses of the
► No 066/a-LK - „Statistical card of the discharged person“.
► No 010/a - „Record journal of pregnant women, delivering women and neonates“.
► No 010-1-1/a - „Card of the neonate“.
► No 010-2-1/a – „Card of the 22 Statistical data – depersonalized clinical data and other data related with the service provision for pregnant women, delivering women and neonates
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 247 of 281
R.3. Feasibility study
No
Purpose Groups of data Forms where relevant data is currently presented
mother;► Data of illnesses of the
neonate.► Statistical data:
► Personal data;► Data of performed
examinations;► Data of performed
procedures;► Data of birth;► Data of the neonate;► Data of development
of the neonate;► Data of illnesses of the
mother;► Data of illnesses of the
neonate.► Data for performing
payments for provided services:► Personal data;► Data of provided
services.
stillborn“.► No 096/a - „History of birth
(partogramme, course of pregnancy, protocol of surgical operation)“.
► No 075/a - „Journal of observation of pregnant women“.
► No 097/a - „History of development of the neonate“.
► No 113/a - „Card of the pregnant women, delivering woman and neonate“.
► No 103-1/a - „Certificate of birth of the child“.
After birth of the neonate[the data from 1 month after birth of the neonate to 1 year after birth of the neonate is entered in EMH of the baby’s mother and EMH of the baby]► Clinical data:
► Data of performed examinations;
► Data of performed procedures;
► Data of development of the baby;
► Data of illnesses of the baby.
► Statistical data: ► Personal data;► Data of performed
examinations;
► No 066/a-LK - „Statistical card of the discharged person“.
► No 003/a - „Medical history of stationary treatment“.
► No 025/a – „Personal history of health (ambulatory card)“.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 248 of 281
R.3. Feasibility study
No
Purpose Groups of data Forms where relevant data is currently presented
► Data of performed procedures;
► Data of development of the baby;
► Data of illnesses of the baby.
► Data for performing payments for provided services:► Personal data;► Data of provided
services.During the pediatric period[the data from 1 year after birth of the neonate to 18 years after birth of the neonate and later is entered in EMH of the child]► Clinical data:
► Data of performed examinations;
► Data of performed examinations;
► Data of performed procedures;
► Data of development of the child;
► Data of illnesses.► Statistical data:
► Personal data;► Data of performed
examinations;► Data of performed
procedures;► Data of development
of the child;► Data of illnesses of the
child.► Data for performing
payments for provided services:► Personal data;
► No 066/a-LK - „Statistical card of the discharged person“.
► No 003/a - „Medical history of stationary treatment“.
► No 025/a – „Personal history of health (ambulatory card)“.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 249 of 281
R.3. Feasibility study
No
Purpose Groups of data Forms where relevant data is currently presented
► Data of provided services.
Note:► The data accumulated during the „Pediatric period“ is not
included in the extent of the information system of the health data about pregnant women, delivering women and neonates.
28. For provision
► Clinical data: ► Data of the course of
pregnancy;► Data of development
of the foetus;► Data of performed
examinations;► Data of performed
procedures;► Data of birth;► Data of the neonate;► Data of development
of the neonate;► Data of development
of the baby;► Data of development
of the child;► Anamnestic data of
former pregnancies;► Data of illnesses of the
mother;► Data of illnesses of the
neonate;► Data of illnesses of the
baby;► Data of illnesses of the
child.► Statistical data:
► Data of the course of pregnancy;
► Data of development of the foetus;
► Data of performed examinations;
► No 066/a-LK - „Statistical card of the discharged person“.
► ► No 003-1/a - „Medical sheet of interruption of pregnancy“;
► ► No 010/a - „Record journal of pregnant women, delivering women and neonates“;
► ► No 010-1-1/a - „Card of the neonate“;
► ► No 010-2-1/a - „Card of the stillborn“;
► ► No 096/a - „History of birth (partogramme, course of pregnancy, protocol of surgical operation)“;
► ► No 097/a - „History of development of the neonate;
► ► No 025-111/a - Records of the course of pregnancy (Personal history of health)“;
► ► No 075/a - „Journal of observation of pregnant women“;
► No 113/a - „Card of the pregnant women, delivering woman and neonate“.
► No 103-1/a - „Certificate of birth of the child“;
► No 025/a – „Personal history of health
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 250 of 281
R.3. Feasibility study
No
Purpose Groups of data Forms where relevant data is currently presented
► Data of performed procedures;
► Data of birth;► Data of the neonate;► Data of development
of the neonate;► Data of development
of the baby;► Data of development
of the child;► Anamnestic data of
former pregnancies;► Data of illnesses of the
mother;► Data of illnesses of the
neonate;► Data of illnesses of the
baby;► Data of illnesses of the
child.► Data for performing
payments for provided services:► Personal data;► Data of provided
services.
(ambulatory card)“;► No 003/a - „Medical history
of stationary treatment“.
29. For the analysis at the level of PHCI
► Clinical data: ► Data of the course of
pregnancy;► Data of development
of the foetus;► Data of performed
examinations;► Data of performed
procedures;► Data of birth;► Data of the neonate;► Data of development
of the neonate;► Data of development
of the baby;
► ► No 003-1/a - „Medical sheet of interruption of pregnancy“;
► ► No 010/a - „Record journal of pregnant women, delivering women and neonates“;
► ► No 010-1-1/a - „Card of the neonate“;
► ► No 010-2-1/a -„Card of the stillborn“;
► ► No 096/a - „History of birth (partogramme, course of pregnancy, protocol of surgical operation)“;
► ► No 097/a - „History of
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 251 of 281
R.3. Feasibility study
No
Purpose Groups of data Forms where relevant data is currently presented
► Data of development of the child;
► Anamnestic data of former pregnancies;
► Data of illnesses of the mother;
► Data of illnesses of the neonate;
► Data of illnesses of the baby;
► Data of illnesses of the child.
► Statistical data: ► Data of the course of
pregnancy;► Data of development
of the foetus;► Data of performed
examinations;► Data of performed
procedures;► Data of birth;► Data of the neonate;► Data of development
of the neonate;► Data of development
of the baby;► Data of development
of the child;► Anamnestic data of
former pregnancies;► Data of illnesses of the
mother;► Data of illnesses of the
neonate;► Data of illnesses of the
baby;► Data of illnesses of the
child.
development of the neonate;
► ► No 025-111/a - Records of the course of pregnancy (Personal history of health)“;
► ► No 075/a - „Journal of observation of pregnant women“;
► No 113/a - „Card of the pregnant women, delivering woman and neonate“;
► No 103-1/a - „Certificate of birth of the child“;
► No 025/a – „Personal history of health (ambulatory card)“;
► No 003/a - „Medical history of stationary treatment“.
30. For report formation
► Clinical data: ► Data of the course of
► No 066/a-LK - „Statistical card of the discharged
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 252 of 281
R.3. Feasibility study
No
Purpose Groups of data Forms where relevant data is currently presented
pregnancy;► Data of development
of the foetus;► Data of performed
examinations;► Data of performed
procedures;► Data of birth;► Data of the neonate;► Data of development
of the neonate;► Data of development
of the baby;► Data of development
of the child;► Anamnestic data of
former pregnancies;► Data of illnesses of the
mother;► Data of illnesses of the
neonate;► Data of illnesses of the
baby;► Data of illnesses of the
child.► Statistical data:
► Data of the course of pregnancy;
► Data of development of the foetus;
► Data of performed examinations;
► Data of performed procedures;
► Data of birth;► Data of the neonate;► Data of development
of the neonate;► Data of development
of the baby;► Data of development
person“.► ► No 003-1/a - „Medical
sheet of interruption of pregnancy“;
► ► No 010/a - „Record journal of pregnant women, delivering women and neonates“;
► ► No 010-1-1/a - „Card of the neonate“;
► ► No 010-2-1/a - „Card of the stillborn“;
► ► No 096/a - „History of birth (partogramme, course of pregnancy, protocol of surgical operation)“;
► ► No 097/a - „History of development of the neonate;
► ► No 025-111/a - Records of the course of pregnancy (Personal history of health)“;
► ► No 075/a - „Journal of observation of pregnant women“;
► No 113/a - „Card of the pregnant women, delivering woman and neonate“.
► No 103-1/a - „Certificate of birth of the child“;
► No 025/a – „Personal history of health (ambulatory card)“;
► No 003/a - „Medical history of stationary treatment“.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 253 of 281
R.3. Feasibility study
No
Purpose Groups of data Forms where relevant data is currently presented
of the child;► Anamnestic data of
former pregnancies;► Data of illnesses of the
mother;► Data of illnesses of the
neonate;► Data of illnesses of the
baby;► Data of illnesses of the
child.► Data for performing
payments for provided services:► Personal data;► Data of provided
services.
In the table below, the assessment of investments and support costs in case of Alternative II is presented.
Table 64. Detailed assessment of investments and support costs in case of Alternative II
InvestmentsSoftware: Amo
untUnit price, LTL with
VAT
Sum, LTL with VAT
Systematic softwareSoftware licences of the database management
2 50,000 100,000
Operating systems of service stations for DB pool
2 9,000 18,000
Operating systems of service stations 2 3,000 6,000Development of applicable software
Preparation of the specifications of IS PWDWN, project of IS PWDWN and other documentation necessary to develop IS PWDWN
1 340,000 340,000
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 254 of 281
R.3. Feasibility study
InvestmentsPurchase of the licences of standard and proven solutions of information technologies used for the data collection, analysis and exchange in the foreign obstetric-gynaecological and neonatal practice
1 100,000 100,000
Application of standard and proven solutions of information technologies used for the data collection, analysis and exchange in the foreign obstetric-gynaecological and neonatal practice to meet the specific Lithuanian needs 23
1 800,000 800,000
Implementation of the integration with eHSCI IS in order to ensure the data exchange with EMH and registers connected to eHSCI
1 80,000 80,000
Implementation of the integration with HIS in order to ensure IS PWDWN will be able to transmit the data to HIS and get the data from HIS(Implementation of getting the data from one PHCI HIS and its presentation is included in the sum. If other PHCI HIS were not able to use the standard information exchange mechanism developed during the project of development of IS PWDWN, implementation of new integration with PHCI HIS would additionally cost 45.000LTL with VAT ).
1 80,000 80,000
Trainings for users of IS PWDWN (100 users from all 35 PHCI)
1 18,000 18,000
Other costs related to the development of IS PWDWN
1 220,000 220,000
Technical maintenance of implementation of IS PWDWN
1 150,000 150,000
Administration of the implementation project of IS PWDWN
1 70,000 70,000
Hardware Amount
Unit price, LTL with
VAT
Sum, LTL with VAT
23 It is assumed that the adjustment of standard and justificatory solutions of information technologies used for the data collection, analysis and exchange in the foreign obstetric-gynaecological and neonatal practice does not require changing more than 30% of the solution.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 255 of 281
R.3. Feasibility study
InvestmentsIT infrastructure
Service stations 4 20,000 80,000Network equipment package 1 100,000 100,000Data storage 1 100,000 100,000
Total need for investments (Lt with VAT) 2,042,000Costs of support
Field Sum, LTL with VAT
Costs of hardware support Note: ► The costs of hardware support have been assessed by
assuming that the period of useful service of hardware is 5 years and without including the costs of support of computerized workstations in the costs of hardware support of. Computerized workstations would be supported by PHCI at own expense.
56,000
Costs of software support Note: ► The costs of support of software have been assessed by
assuming that the yearly costs of software support make 10%24 of the value of software.
170,000
In the table below, the assessment of the duration of implementation of Alternative II is presented.
Table 65. Assessment of the duration of implementation of Alternative IINo
Activity Duration
1. Preparation of the documents of the public purchase of the technical maintenance services for implementation of PWDWN IS
3 months
2. Execution of the public purchase of the technical maintenance services for implementation of PWDWN IS
5 months
3. Preparation of the public tender documentation and project of IS PWDWN and other documentation necessary to develop IS PWDWN
3 months
24 Worldwide IT Benchmark Report 2006: Volume 2: IT Spending & Staffing Analysis: Multi-Year Trends: Pharmaceuticals & Medical Products Analysis
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 256 of 281
R.3. Feasibility study
No
Activity Duration
4. Public purchase of the licences of standard and proven solutions of information technologies used for the data collection, analysis and exchange in the foreign obstetric-gynaecological and neonatal practice and services of their adaptation according to Lithuanian needs
6 months
5. Adaptation of standard and proven solutions of information technologies used for the data collection, analysis and exchange in the foreign obstetric-gynaecological and neonatal practice to meet the specific needs of Lithuania
4 months
6. Implementation of the integration with eHSCI IS in order to ensure the data exchange with EMH and registers connected to eHSCI
1 month
7. Implementation of the integration with HIS in order to ensure that IS PWDWN will be able to transfer the data to HIS and get the data from HIS
1 month
8. Trainings for the users of IS PWDWN (100 users from all 35 PHCI)
1 month
9. Test operation 2 months
The total duration of implementation of Alternative II (certain activities of implementation of the alternative can be performed simultaneously; therefore, the sum of durations of implementation of the activities is not equal to the total duration of implementation of the alternative).
15 months
Note: ► The duration of implementation of the activities of this alternative does not
include the document coordination with Swiss experts that is not purposeful to prognosticate in this stage; therefore the duration of implementation of these activities are preliminary.
10.6.3 Alternative IIIBelow, Alternative III is presented:
► In order to satisfy the needs of representatives of PHCI and associated institutions for accumulation, exchange and analysis of the data about pregnant women, delivering women and neonates and report formation and decrease in the administrative burden of employees of PHCI and associated institutions, a centralized IS PWDWN is developed; it is common for all PHCI and involves the minimal set of the data about pregnant women, delivering women and neonates and all data in
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 257 of 281
R.3. Feasibility study
statistical paper forms presently filled-in by employees of PHCI; it would give a possibility to discontinue the use of presently filled-in statistical paper forms;
► The developed IS PWDWN functions independently on eHSCI IS as long as eHSCI IS is not developed, but it is developed so that IS PWDWN can function as the applicable solution of eHSCI IS after developing eHSCI IS;
► IS PWDWN is centralized and common for all PHCI, but the data of separate PHCI is fully separated logically, thus, every PHCI can only access its own data. Employees of a certain PHCI can only access depersonalized and generalized data of other PHCI;
► As long as eHSCI IS is not developed, the data exchange with PHCI having their information systems is made directly through IS PWDWN, but it is intended while developing IS PWDWN that the data exchange with PHCI having their information systems should be made through the eSPI IS data exchange component after developing eHSCI IS.
Note: ► In the extent of this alternative, a standard solution for solving issues of
collecting, analyzing, exchanging and assessing the data about pregnant women, delivering women and neonates existing somewhere in the market would not be applied and the total information system solution would be developed „ab initio“, which would allow ensuring all needs of the representatives of PHCI will be considered and the developed solution will fully comply with expectations of the representatives of PHCI.
In the table below, the advantages and disadvantages of Alternative III are presented.
Table 66. Advantages and disadvantages of Alternative IIIAdvantages Disadvantages
In case of implementing this alternative, the minimal set of the data about pregnant women, delivering women and neonates and all data in statistical forms presently filled in in by employees of PHCI is accumulated in IS PWDWN which gives a possibility:► To accumulate, exchange and
analyze all data;► To perform qualitative assessment
of newly created and reviewed present methods of treatment
It is necessary to change habits of employees of PHCI, i.e., change the model of activity by discontinuing the use of the presently filled-in statistical paper forms and fill in the same data in the developed IS PWDWN.Filling-in of statistical forms is regulated in the legal acts of the Ministry of Health; therefore, in this case it would also be necessary to change the legal acts regulating filling-in of statistical forms.In case of implementing this alternative, the information
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 258 of 281
R.3. Feasibility study
Advantages Disadvantages
and protocols and their improvement;
► To decrease administrative burden for the employees of PHCI and associated institutions by discontinuing the use of presently filled-in statistical paper forms and filling-in the same data in the developed IS PWDWN.
technology solution of much bigger extent and functionality would be developed as in case of alternative I, but the duration of implementation of this alternative would be shorter by 5.5 months than the duration of implementation of the first alternative.In case of implementing this alternative, the information technology solution of similar extent and functionality would be developed and it may satisfy all expectations of the representatives of PHCI as it would be developed “ab initio” as in case of alternative II, but the duration of this alternative would be longer by 5.5 months than the duration of implementation of the third alternative.In order to implement this alternative, it is necessary to invest by 1,542,000 LTL more than in case of implementing the first alternative and by 620,000 LTL more than in case of implementing the second alternative.
In the table below, potential risks of Alternative III are presented.
Table 67. Potential risks of Alternative III No
Potential risks
1. ► Non-assurance of continuity of eHSCI IS development, i.e., interruption of further development of eHSCI IS. In this case IS PWDWN would be able to function without eHSCI IS, but the functionality of the data exchange module presented in picture No 52 and described in table No 72 would not be implemented.
2. ► Reluctance of PHCI to use the developed IS PWDWN as PHCI will not be able to modify the information system themselves; only the manager of the information system will be able to make changes.
3. ► Reluctance of PHCI to change their habits, i.e., change the model of activity by discontinuing the use of filled-in statistical paper forms and fill in the data presently accumulated in statistical forms in the
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 259 of 281
R.3. Feasibility study
No
Potential risks
developed IS PWDWN.
Note: ► In case of implementing Alternative III, the data set of the same scope would
be accumulated in IS PWDWN, as in case of implementing Alternative II. The description of the data set accumulated in IS PWDWN in case of implementing Alternative III is presented in the description of Alternative II with more details.
In the table below, the assessment of investments and costs of support in case of Alternative III is presented.
Table 68. Detailed assessment of investments and costs of support in case of Alternative III
InvestmentsSoftware: Amoun
tUnit price, LTL with
VAT
Sum, LTL with VAT
System softwareSoftware licences of the database management
2 50,000 100,000
Operating systems of service stations for DB pool
2 9,000 18,000
Operating systems of service stations 2 3,000 6,000Development of applicable software
Preparation of the specifications of IS PWDWN, project of IS PWDWN and other documentation necessary to develop IS PWDWN
1 340,000 340,000
Development of IS PWDWN25
Analysis (3 employees, 250 h each)
1 150,000 150,000
Design (4 employees, 250 h each)
1 200,000 200,000
25 IS PWDWN would be integrated with eHSCI IS, information systems of PHCI and other institutions (register of residents, national information system of social insurance etc.). The costs of development are assessed according to the stages of implementation of the information system by assuming the average hourly rate of employees of the implementer is 200 LTL with VAT and expert assessment by assessing the duration of the system development works in hours.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 260 of 281
R.3. Feasibility study
InvestmentsConstruction (5 employees, 1100 h each)
1 1,100,000 1,100,000
Implementation (3 employees, 250 h each)
1 150,000 150,000
Test operation (2 employees, 500 h each)
1 200,000 200,000
Trainings for users of IS PWDWN (100 users)
1 18,000 18,000
Other costs related to the development of IS PWDWN
1 300,000 300,000
Technical maintenance of implementation of IS PWDWN
1 200,000 200,000
Administration of the implementation project of IS PWDWN
1 100,000 100,000
Hardware Amount
Unit price, LTL with
VAT
Sum, LTL with VAT
IT infrastructureServers 4 20,000 80,000Network equipment package 1 100,000 100,000Data storage 1 100,000 100,000
Total need for investments (LTL with VAT) 2,862,000Costs of support
Sum, LTL with VAT
Costs of hardware support Note: ► The costs of hardware support have been assessed by
assuming the period of useful life of hardware is 5 years and without including the costs of support of computerized workstations in the costs of hardware support. Computerized workstations would be supported by PHCI at own expense.
56,000
Costs of software support Note: ► The costs of software support have been assessed by
assuming that the yearly costs of software support make 10%26 of the value of software.
244,000
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 261 of 281
R.3. Feasibility study
In the table below, the assessment of the duration of implementation of Alternative III is presented.
Table 69. Assessment of the duration of implementation of Alternative IIINo Activity Duration
1. Preparation of the documents of the public purchase of the technical maintenance services for implementation of PWDWN IS
3 months
2. Execution of the public purchase of the technical maintenance services for implementation of PWDWN IS
5 months
3. Public procurement of the services of the preparation of the specifications of IS PWDWN, technical specification for the implementer, project of IS PWDWN and other documentation necessary to develop IS PWDWN
3 months
4. Public purchase of the services of development and implementation of a stand-alone information system (IS PWDWN) which would be integrated with eHSCI IS, information systems of PHCI and other institutions (the civil register, national information system of social insurance)
6 months
5. Development and implementation of a stand-alone information system (IS PWDWN) which would be integrated with eHSCI IS, information systems of PHCI and other institutions (the civil register, national information system of social insurance:
13.5 months
4.1. Analysis (3 employees, 250 h each) 1.5 months
4.2. Design (4 employees, 250 h each) 1.5 months
4.3. Construction (5 employees, 1100 h each) 6 months
4.4. Implementation (3 employees, 250 h each) 1.5 months
4.5. Test operation (2 employees, 500 each) 3 months
6. Trainings for users of IS PWDWN (100 users from all 35 PHCI) 1 month
The total duration of implementation of Alternative III (certain activities of implementation of the alternative can be performed simultaneously; therefore, the sum of durations of implementation of the activities is not equal to the total duration of implementation of the alternative)
20.5 month
26 Worldwide IT Benchmark Report 2006: Volume 2: IT Spending & Staffing Analysis: Multi-Year Trends: Pharmaceuticals & Medical Products Analysis
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 262 of 281
R.3. Feasibility study
Note: ► The duration of implementation of the activities of this alternative does not
include the document coordination with Swiss experts that is not purposeful to prognosticate in this stage; therefore the duration of implementation of these activities are preliminary.
10.6.4 Optimal alternative of IS PWDWN implementationConsidering the advantages and disadvantages of Alternative I, Alternative II and Alternative III, potential risks, infrastructure available for PHCI, skills of the staff of PHCI to work with information systems, duration of implementations of the alternatives, preliminary need for investments, costs of support and needs of PHCI and the fact that presently none of the PHCI of Lithuania has solutions suitable for exchanging the data about pregnant women, delivering women and neonates, it is recommended to consider implementation of Alternative I:
► In order to satisfy the needs of representatives of PHCI and associated institutions for accumulation, exchange and analysis of the data about pregnant women, delivering women and neonates and report generation, a centralized IS PWDWN is developed; it is common for all PHCI;
► The developed IS PWDWN only involves the minimal set of the data about pregnant women, delivering women and neonates indicated in the chapter No 10.2.2 of this document and functions independently on eHSCI IS as long as eHSCI IS is not developed, but it is developed so that IS PWDWN can function as the applicable solution of eHSCI IS after developing eHSCI IS;
► IS PWDWN is centralized and common for all PHCI, but the data of separate PHCI is fully separated logically, thus, every PHCI can only access its own data. Employees of a certain PHCI can only access depersonalized and generalized data of other PHCI;
► As long as eHSCI IS is not developed, the data exchange with PHCI having their information systems is made directly through IS PWDWN, but it is intended while developing IS PWDWN that the data exchange with PHCI having their information systems should be made through the eSPI IS data exchange component after developing eHSCI IS.
Note: ► The recommended alternative is that one requiring the least investments for
its implementation; it is implemented within the shortest period and complies with the needs of the representatives of the Lithuanian Community of Obstetricians-Gynaecologists and the Neonatal Association. The compliance of the recommended alternative with the needs of the representatives of the Lithuanian Community of Obstetricians-Gynaecologists and the Neonatal Association was approved with the protocol of the meeting of the representatives of the Lithuanian Community of Obstetricians-Gynaecologists and the Neonatal Association and the representatives of the Health Care Ministry and Ernst & Young on the 7th of June 2010;
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 263 of 281
R.3. Feasibility study
► The developed PWDWN IS would be used not only by the employees of the main PHCI, but also by the employees of reserved PHCI.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 264 of 281
R.3. Feasibility study
10.7 Action plan for the implementation of IS PWDWN 10.7.1 Recommended schedule for the implementation of the
development model In the table below, a preliminary schedule for the implementation of the recommended development model is presented.
Table 70. Schedule for the implementation of the recommended development model No Activity Duration
13. Administration and preparation of documents for the public procurement of IS PWDWN implementation technical supervision services
3 months
14. Performance of administration and public procurement of IS PWDWN implementation technical supervision services
5 months
15. Preparation of IS PWDWN public procurement documents, IS PWDWN project and other documents required for the development of IS PWDWN.
6 months
16. Public procurement of the services of development and installation of an independent information system (IS PWDWN), which would be integrated with eHSCI IS, information systems of PHCI and other institutions
7 months
17. Development and installation of IS PWDWN covering only a minimum data package of pregnant women, delivering women and neonates and integrated with eHSCI IS, information systems of PHCI and other institutions:
16.1
Analysis(2 employees, 100 h)
0.5 month
16.2
Design(2 employees, 150 h)
0.5 month
16.3
Construction(3 employees, 500 h)
3 months
16.4
Implementation (2 employees, 150 h)
0.5 month
16.5
Test operation(2 employees, 300)
2 months
17 Trainings for users of IS PWDWN(100 users from all 35 PHCI)
1 month
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 265 of 281
R.3. Feasibility study
No Activity Duration
The total duration of implementation of Alternative I (certain activities of implementation of the alternative can be performed simultaneously; therefore, the sum of durations of implementation of the activities is not equal to the total duration of implementation of the alternative).
15 months
Note: ► The duration of implementation of the activities of this alternative does not
include the document coordination with Swiss experts that is not purposeful to prognosticate in this stage; therefore the duration of implementation of these activities are preliminary.
10.7.2 Recommended technical and technological standardsThe conception of a modern system oriented towards the patient’s needs and service is based on an electronic medical history (EMH). EMH is the basis of the e. health system and a fully functioning EMH system is the most important objective of e. health, and in order to ensure its full functioning, the systems providing the data to the EMH system should use the same technical and technological standards. Meanwhile, technical and technological standards are among the main aspects ensuring interconnection (interoperability) between the systems; therefore, it is recommended to apply the technical and technological standards presented in the table of Appendix No 6 to this document while developing the information system of pregnant women, delivering women and neonates after performing the review of the standards applicable in the field of e. health within the scope of the project executed by the Ministry of Health, during which Ernst & Young had applied the Services of the assessment of the novelty of the solution for the national electronic health system, its suitability for operation and consulting on the issues of the development according to the contract No S-266 of 14 October 2009; this review is presented in Appendix No 2 to this document – „Review of the standards in the field of electronic health“ and considering the recommendations presented to the IS architecture of the e. health service and collaboration infrastructure during the implementation of the project presented in Appendix No 3 to this document - “ IS architecture of the e. health service and collaboration infrastructure.10.7.3 Information system integration schemes and data exchange
modelsExtension of eHSCI IS with the functionality for the collection, storage, exchange and assessment of the health data about pregnant women, delivering women and neonates would enable to avoid the need for extra works of the system integration and possibly emerging risks of incompatibility between the systems.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 266 of 281
R.3. Feasibility study
As the recommended standards and requirements applicable to eHSCI IS, requirements for the applicable systems of eHSCI, requirements for the integration to eHSCI and technical conditions, requirements for infrastructure and safety of eHSCI were formed within the scope of the project executed by the Ministry of Health, during which Ernst & Young had applied the Services of the assessment of the novelty of the solution for the national electronic health system, its suitability for operation and consulting on the issues of the development according to the contract No S-266 of 14 October 2009, in this document we refer to the results obtained during the project above and the documents prepared:
► E.1, E.2, E.3.1 Report on the assessment and recommendations for the present situation, applicable e. health service objectives and e. health standards;
► Е.3.2.R.1 – Requirements and technical conditions for the interconnection between SPĮ IS with eHSCI IS.
Presented below are data groups according to which every PHCI should transmit the data to the recipients of data from the data accumulated in the IS of Pregnant women, delivering women and neonates:
► Ministry of Health of the Republic of Lithuania and its subordinate institutions;
► Health Information Centre of the Institute of Hygiene;► Other institutions;► Natural persons.
Table 71. Data groups which every PHCI should transmit to the recipients of dataNo
Groups of data Forms where the relevant data is presented at present
1. ► Clinical data: ► Data of the course of
pregnancy;► Data of development of the
foetus;► Data of performed
examinations;► Data of performed procedures;► Data of birth;► Data of the neonate;► Data of development of the
neonate;► Data of development of the
baby;► Data of development of the
► ► No 010-1-1/a - „Card of the neonate“;
► ► No 010-2-1/a - „Card of the stillborn“.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 267 of 281
R.3. Feasibility study
No
Groups of data Forms where the relevant data is presented at present
child;► Anamnestic data of former
pregnancies;► Data of illnesses of the
mother;► Data of illnesses of the
neonate;► Data of illnesses of the baby;► Data of illnesses of the child.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 268 of 281
R.3. Feasibility study
Important: ► The data accumulated by every PHCI in the IS of pregnant women, delivering
women and neonates can be stored in the same technical infrastructure but they have to be separated from other PHCI at the logical level.
► Access to all data accumulated by every PHCI in the IS of pregnant women, delivering women and neonates should be granted to the employees of that PHCI only based on the activities they perform .
► Access to certain data accumulated by every PHCI in the IS of pregnant women, delivering women and neonates harmonized with PHCI should be provided to the above recipients of data of PHCI according to the target groups, for example, the recipients of statistical data can only access depersonalized statistical information.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 269 of 281
R.3. Feasibility study
In the picture below, the conceptual architecture of eHSCI IS and depicted applicable system of eHSCI – „Pregnant women, delivering women and neonates IS“ is presented.
Sveikatos priežiūros sektoriaus administruojančios institucijos ir kiti dalyviaiSveikatos priežiūros įstaigos
e. Sveikatos paslaugų ir bedradarbiavimo infrastruktūros informacinė sistema
Portalas
Gyventojai
e. paslaugų teikimo funkcinis komponentas
Duomenų sauga
Autorizavimas§ Prieigos kontrolė§ Informacijos saugos
politikos
Autentikavimas
Duomenų mainų terpė
Gyventojų sritis Sveikatos priežiūros specialistų sritis
Sistemos valdymas
Administravimas
Stebėsena
Auditas
Sveikatos priežiūros specialistai
Viešojo administravimo institucijos
Registrai
Valstybinės ir savivaldybių IS
RegistraiRegistrai
Registrų IS
RegistraiRegistraiRegistrų ISSPĮ IS SPĮ IS SVEIDRA Vaistinės IS
Sveikatos priežiūros specialistas Pacientas
Viešojo administravimo institucijų interoperabilumo sistema (VAIISIS)
§ Procesų ir darbo sekų valdymas
§ Dokumentinių įrašų valdymas
Archyvavimas
Rezervinės kopijos
E. paslaugų kūrimas ir konfigūravimas
§ Talpinimas/ perkėlimas§ Redagavimas§ Pateikimas/ leidyba§ Paieška
Turinio valdymas
Duomenų mainų terpės valdymas
Paslaugų ir procesų gyvavimo ciklo valdymas
§ Apibrėžimas§ Konstravimas§ Publikavimas§ Sustabdymas
Duomenų mainų ir sąveikos komponentų katalogas
e. Sveikatos paslaugų gyventojams katalogas
e. Sveikatos paslaugų specialistams katalogas
SPĮ IS
Taikomieji sprendimaiE. Paslaugos
Informaciniai ištekliai
Terminologijos paslaugos Objektų ID katalogas
Specialistų katalogas
Pacientų katalogas
ESI informacinė sistema
Aktų katalogas Aktų nuorodų katalogas
SPĮ katalogas
Įskaitant dokumentų saugyklą
Įskaitant dokumentų nuorodų saugyklą
Prieiga prie ESI ir jos tvarkymas
e. siuntimai
§ Metaduomenų valdymas
§ Duomenų mainų ir sąveikos komponentų projektavimas ir kūrimas
eSPBI taikomasis sprendimas –
„Nėščiųjų, gimdyvių ir naujagimių IS“
Picture No 51 – Conceptual architecture of eHSCI IS and depicted applicable system of eHSCI – „Pregnant women, delivering women and neonates IS“
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 270 of 281
R.3. Feasibility study
In the picture below, the eHSCI scheme of the data exchange between the information system of pregnant women, delivering women and neonates and the hospital information systems (hereinafter – HIS) in case of having developed and functioning eHSCI IS.
Logical area No. i2
Picture No 52 – Data exchange between IS PWDWN, eHSCI IS and HIS in case of having developed and functioning eHSCI IS
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 271 of 281
R.3. Feasibility study
Table 72. Description of the data exchange between IS PWDWN, eHSCI IS and HIS in case of having developed and functioning eHSCI ISNo
Interface Description
1. Between the IS PWDWN user environment and IS PWDWN
The IS PWDWN user environment functions in the IS PWDWN environment and gives representatives of every hospital a possibility to connect only to the logical area of the own hospital. Note: ► Representatives of hospitals have a possibility to
connect only to the logical area of the own hospital or can see depersonalized and generalized data of all hospitals.
2. Between IS PWDWN, eHSCI IS and HIS
IS PWDWN, eHSCI IS and HIS exchange clinical and administrative data:► Clinical data:
► Clinical data from IS PWDWN is transmitted to EMH functioning in the environment of eHSCI IS through the eHSCI IS data exchange medium;
► Clinical data from EMH functioning in the environment of eHSCI IS is transmitted to IS PWDWN through the eHSCI IS data exchange medium;
► Clinical data from eHSCI IS is transmitted to EMI functioning in the environment of HIS through the eHSCI IS data exchange medium;
► Clinical data from EMI functioning in the environment of HIS is transmitted to EMH functioning in the environment of eHSCI IS through the eHSCI IS data exchange medium.
► Administrative data:► After the neonate is born and registered in IS
PWDWN, IS PWDWN initiates the creation of EMH of the neonate in the environment of eHSCI IS.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 272 of 281
R.3. Feasibility study
In the picture below, the eHSCI scheme of the data exchange between the information system of pregnant women, delivering women and neonates (hereinafter – IS PWDWN) and the hospital information systems (hereinafter – HIS) in case eHSCI IS is not yet developed and functioning .
Picture No 53 – Data exchange between IS PWDWN, eHSCI IS and HIS in case eHSCI IS is not yet developed and functioning
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 273 of 281
R.3. Feasibility study
Table 73. Description of the data exchange between IS PWDWN, eHSCI IS and HIS in case eHSCI IS is not yet developed and functioningNo
Interface Description
1. Between the IS PWDWN user environment and IS PWDWN
The IS PWDWN user environment functions in the IS PWDWN environment and gives representatives of every hospital a possibility to connect only to the logical area of the own hospital. Note: ► Representatives of hospitals have a possibility to
connect only to the logical area of the own hospital or can see depersonalized and generalized data of all hospitals.
2. Between IS PWDWN, eHSCI IS and HIS
IS PWDWN and HIS exchange clinical and administrative data:► Clinical data:
► Clinical data from IS PWDWN is transmitted to EMI functioning in the environment of HIS;
► Clinical data from EMI functioning in the environment of HIS is transmitted to IS PWDWN;
► Administrative data:► After the neonate is born and registered in IS
PWDWN, IS PWDWN initiates the creation of EMI of the neonate in the environment of HIS.
10.7.4 Description of the information system administration model As presently it is not decided yet who will become manager and keeper of IS PWDWN, two alternatives for the choice of the manager and keeper of IS PWDWN, their advantages and disadvantages/risks are presented in the table below.
Table 74. Alternatives for the choice of the manager and keeper of IS PWDWN Alternative I Alternative II
► The Ministry of Health of the Republic of Lithuania or its subordinate institution is manager and keeper of IS PWDWN.
► One of perinatal centres of Lithuania is manager and keeper of IS PWDWN.
Advantages► In case an institution subordinate to
the Ministry of Health, which administrates information systems
► Specialists of the highest qualification would administrate the data from IS PWDWN and they
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 274 of 281
R.3. Feasibility study
Alternative I Alternative IIor has experience in their administration and is intended to get extra assignations for management and keeping of IS PWDWN, was appointed manager and keeper of IS PWDWN, the manager and keeper of IS PWDWN would have enough experience and be more interested in proper administration of IS PWDWN than perinatal centres.
► The Ministry of Health or its subordinate institution would have more political power to force regional PHCI to transmit data to IS PWDWN than perinatal centres.
would have enough competence to properly administrate, analyze the data and assess applicable methods of treatment.
Disadvantages/ risks► Considering the low possibility that
the people not working at perinatal centres will have enough competence to properly administrate, analyze the data and assess applicable methods of treatment, there is a risk that the data of IS PWDWN will not be properly administrated.
► As the maintenance of information systems is not a direct activity of perinatal centres, there is a risk that perinatal centres will not be interested in properly maintain the developed IS PWDWN.
► As the maintenance of IS PWDWN requires extra costs which the perinatal centre should cover from its own budget, there is a risk that the perinatal centre will not allocate funds for the maintenance of IS PWDWN.
► Perinatal centres may not have enough political power to force regional PHCI to provide data to perinatal centres, or the data provided by regional PHCI to perinatal centres may of insufficient quality.
► People working for perinatal centres may not have/spare enough time to administrate, analyze and assess the data of IS PWDWN if these functions are not included in their job descriptions and they are not additionally motivated for that.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 275 of 281
R.3. Feasibility study
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 276 of 281
R.3. Feasibility study
In the table below, the description of the information system administration model is presented.
Table 75. Description of the administration modelNo Field Description
1) Applicable system of eSBI - „IS of pregnant women, delivering women and neonates“
1.1. ► Owner and administrator
► Owner and administrator of the information system:► Alternative I – Ministry of Health or its
subordinate institution;► Alternative II – one of the perinatal centres.
► Functions performed by the manager and administrator of the information system:► Management and keeping of the data of the
information system at the levels of the Ministry of Health and its subordinate institutions and EMH.
1.2. ► Providers of data ► Data will be provided by:► PHCI providing services for pregnant women,
delivering women and neonates.
1.3. ► Recipients of data
► Data from the information system will be received by:► PHCI providing services for pregnant women,
delivering women and neonates;► Physical entities;► Ministry of Health of the Republic of
Lithuania;► Institutions subordinate to the Ministry of
Health of the Republic of Lithuania;► Civil registries.
1.4. ► Information structure
► The data which will be stored in the information system are presented in the chapter of this document „Generalized needs of PHCI for the data accumulation, exchange, analysis and report formation“.
1.5. ► Functional structure
► The main functions of the information system:
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 277 of 281
R.3. Feasibility study
No Field Description
► Accumulation of the data about pregnant women, delivering women and neonates;
► Analysis of the data about pregnant women, delivering women and neonates;
► Transmission of the data about pregnant women, delivering women and neonates to EMH;
► Reading of the data about pregnant women, delivering women and neonates from EMH;
► Management of the data classifiers.
2) Typical regulations of the information systems for which PHCI having their own systems will provide data to the applicable system of eHSCI– „IS of pregnant women, delivering women and neonates”
2.1. ► Owner and administrator
Owner and administrator of the information system:PHCI providing services for pregnant women,
delivering women and neonates;Data of the information system are managed at
the level of PHCI according to the target groups by:
► Neonatologist;► Children’s nurse (nurse);► Obstetrician-gynaecologist;► Obstetrician;► Doctor of children’s diseases (pediatrician);► Assistant nurse;► Administrator of PHCI.
2.2. ► Providers of data Data for the information system will be provided by:► IS of pregnant women, delivering women and
neonates.
2.3. ► Recipients of data
Data from the information system will be received by:► IS of pregnant women, delivering women and
neonates.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 278 of 281
R.3. Feasibility study
2.4. ► Information structure
The data which will be stored in the information system are presented in the chapter of this document „Generalized needs of PHCI for the data accumulation, exchange, analysis and report generation“.
2.5. ► Functional structure
The main functions of the information system:► Entering of the data about pregnant women,
delivering women and neonates;► Accumulation of the data about pregnant
women, delivering women and neonates;► Analysis of the data about pregnant women,
delivering women and neonates;► Transmission of the data about pregnant
women, delivering women and neonates to the IS of pregnant women, delivering women and neonates;
► Reading of the data about pregnant women, delivering women and neonates to the IS of pregnant women, delivering women and neonates;
► Management of the data classifiers.
10.7.5 Description of modification of the necessary legal basis In the table below, the description of the legal basis necessary to modify is presented.
Table 76. Description of the legal basis necessary to modifyNo Legal act Necessary changes
1. ► Regulation of pregnant women, delivering women and neonates IS
► Has to be prepared.
2. ► Order No 515 “On the order of accounting and accountability of the activity of health care institutions” of the Minister of Health Care of the Republic of Lithuania.
► Has to be modified.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 279 of 281
R.3. Feasibility study
11. Budget of programmes
11.1 Activities of programmesWhile assessing different alternatives and possible risks of their implementation in the feasibility study, the need for investments was recommended for the following activities:
► Purchase and installation of medical equipment;► Purchase of reanimobiles with special equipment;► Development of computer database;► Strengthening of abilities of medical staff;► Development of methodologies of obstetric and neonatal diagnosis and
treatment;► Necessary repair not related to the increase in energy efficiency;► Introduction of energy-sparing technologies.
Moreover, at the start of the Programme before assimilating the support and at the end of the Programme it is recommended to perform an assessment of impact on the health care system, which would help to make a better assessment of the achievement of the Programme objectives, define clear performance indicators of objectives for monitoring their current and target values.
Table 77. Budget of the programme „Improvement of health care of pregnant women, delivering women and neonates in Lithuania“ No
Activity Indicative budget of the activity, LTL with VAT (rounded)
1. Purchase and implementation of medical equipment
44,866,800
2. Purchase of reanimobiles with special equipment
300,000
3. Development of computer database 1,120,0004. Strengthening of abilities of medical staff 4,251,0005. Development of guidelines of obstetric and
neonatal diagnosis and treatment1,232,000
6. Necessary repair not related to the increase in energy efficiency
5,173,000
7. Reserve (about 10%) 6,880,800
Note. The need for funds to execute separate activities of the Project is calculated according to the currency rate 1 CHF = 2.2 LTL.
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 280 of 281
R.3. Feasibility study
It is recommended to use the reserve of the programme „Improvement of health care of pregnant women, delivering women and neonates in Lithuania“ in the following cases:
► In order to reduce the risk of increase in the value of investments: as the Programme will be implemented within a few years, the prices of medical equipment to be purchased, works of repair and purchased services can rise;
► When preparing methodologies and organizing the activity of the improvement of the qualification of staff, if necessary, for extra export of activities;
► For extra purchase of essential medical equipment which is provided for in the feasibility study.
► For the purpose of acquisition of apparatus for the mandatory hearing inspection of the newborns pursuant to the order of the Minister of Health, which is currently being prepared
In the end of the Programme Introduction of Energy-Saving Technology to Lithuanian Hospitals, which Provide Services to the Pregnant, Women in Labour and the Newborns we recommend performing energy audits in hospitals , which have been granted support, thus, helping to better assess the achievement of objectives of the Programme.
Table 78. Budget of the programme „Introduction of energy-sparing technologies in Lithuanian hospitals providing services for pregnant women, delivering women and neonates”
MeasuresExpected costs of activities of the
project, LTL, with VAT
Improvement of thermal insulation in buildings 15.356.300Modernization of the heating, hot water supply systems and heat stations 11.284.900
Modernization/ implementation of the ventilation and conditioning systems 11.133.600
Modernization of the power supply systems 2.987.000Modernizations of the medical gas, oxygen, vacuum and compressed air supply systems 1.883.600
Reserve 2.812.200
Note. The need for funding for the execution of separate Project activities is calculated according to the currency rate 1 CHF = 2.2 LTL.
It is recommended to use the reserve of the programme „Introduction of energy-sparing technologies in Lithuanian hospitals providing services for pregnant women, delivering women and neonates“ in the following cases:
CONFIDENTIAL document.docx

Ministry of Health of the Republic of
Lithuania
Preparation of the feasibility study and final project proposals of the projects on improvement of prenatal, perinatal and neonatal care services and infrastructure in Lithuanian hospitals, including
implementation of energy-sparing technologies Page 281 of 281
R.3. Feasibility study
► In order to reduce the risk of increase in the value of investments: as the Programme will be implemented within a few years, the prices of medical equipment to be purchased, works of repair and purchased services can rise;
► For the implementation of better measures in PHCI.
Note:► Funds for the project implementation are preliminary. The exact need for
funding will be clear after performing public procurement of all the project activities.
CONFIDENTIAL document.docx