a variety of disease manifestations focal distribution ......
TRANSCRIPT
Leishmaniasis• a variety of disease manifestations• focal distribution throughout world,
especially tropics and subtropics• new world: southern Texas to northern
Argentina• old world: Asia, Africa, middle east,
Mediterranean• transmitted by sand flies
• new world: Lutzomyia• old world: Phlebotomus
• 350 million at risk• 12 million infected• 1.5-2 million clinical
cases/year


Some Leishmania Species Infecting HumansNew World Cutaneous,Mucocutaneous, and
Diffuse Leishmaniasis
Old World Cutaneous,Recidivans, and
Diffuse LeishmaniasisVisceral
LeishmaniasisMexicana Complex
L. mexicanaL. amazonensis
Braziliensis ComplexL. braziliensisL. panamensisL. guyanensis
L. tropica
L. major
L. aethiopica
L. infantum*
L. donovani
L. infantum*
L. chagasi**
*Both dermotrophic and viscerotrophic strains exist.**L. chagasi (Americas) may be the same as L. infantum (Mediteranean)
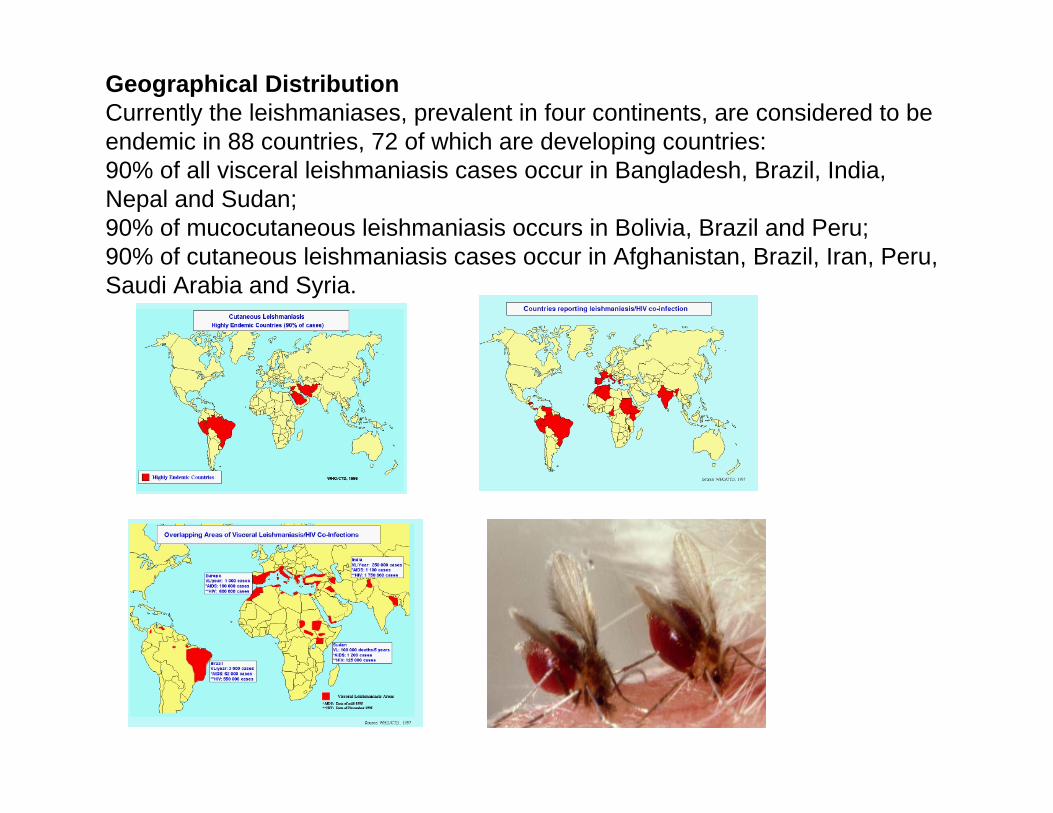
Geographical DistributionCurrently the leishmaniases, prevalent in four continents, are considered to be endemic in 88 countries, 72 of which are developing countries:90% of all visceral leishmaniasis cases occur in Bangladesh, Brazil, India, Nepal and Sudan;90% of mucocutaneous leishmaniasis occurs in Bolivia, Brazil and Peru;90% of cutaneous leishmaniasis cases occur in Afghanistan, Brazil, Iran, Peru, Saudi Arabia and Syria.
Clinical Spectrum of LeishmaniasisCutaneous Leishmaniasis (CL)
most common form, relatively benign self-healing skin lesions (aka, localized or simple CL)
Mucocutaneous Leishmaniasis (MCL)simple skin lesions that metastasize, especially to nose and mouth region
Visceral Leishmaniasis (VL)generalized infection of the reticuloendothelial system, high mortality
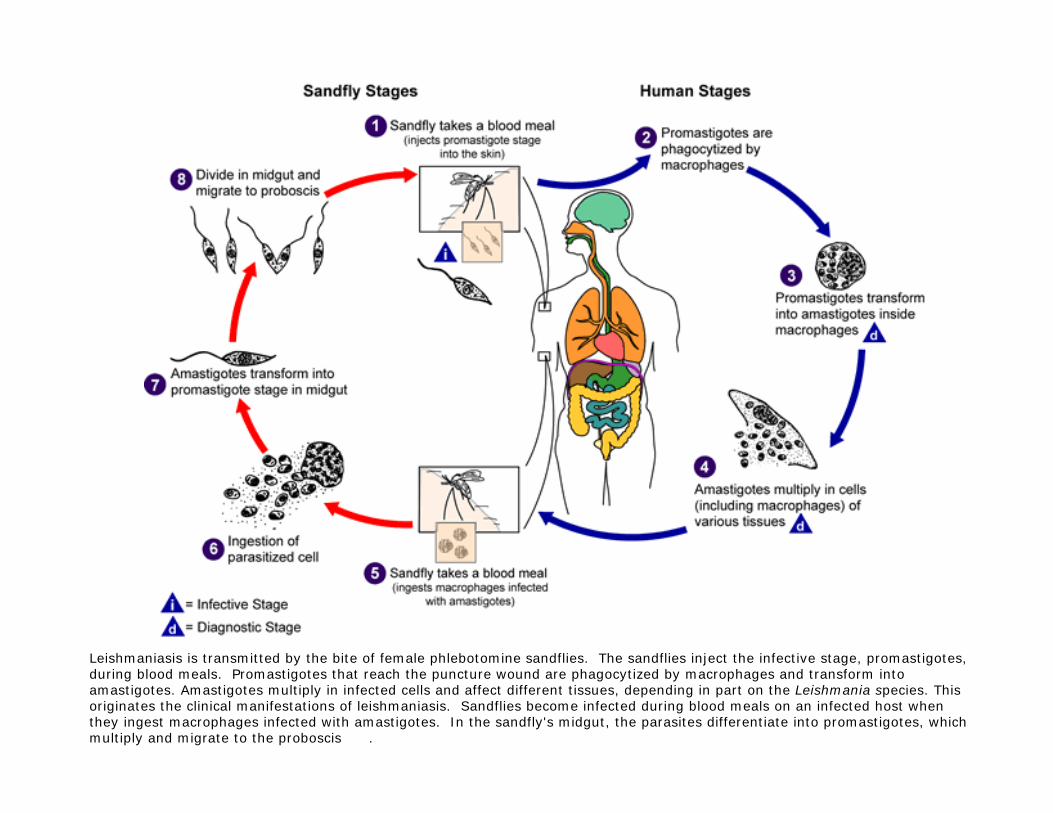
Leishmaniasis is transmitted by the bite of female phlebotomine sandflies. The sandflies inject the infective stage, promastigotes, during blood meals. Promastigotes that reach the puncture wound are phagocytized by macrophages and transform into amastigotes. Amastigotes multiply in infected cells and affect different tissues, depending in part on the Leishmania species. This originates the clinical manifestations of leishmaniasis. Sandflies become infected during blood meals on an infected host when they ingest macrophages infected with amastigotes. In the sandfly's midgut, the parasites differentiate into promastigotes, which multiply and migrate to the proboscis .

Sandfly Vector
Human Host Animal Reservoir
MacrophagePromastigote Amastigote
Skin

1) metacyclic promastigotes
2) phagocytosis by macrophage amastigote
3) replication within macrophage
4) release and phagocytosis of amastigotes

The symptoms and pathology associated with leishmaniasisresult from the amastigotes killing the host's cells.
There are many different "diseases" caused by Leishmania. In some diseases the amastigotes do not spread beyond the site of the vector's bite. This results in a "cutaneousleishmaniasis" (oriental sore, Jericho boil, Aleppo boil, or Dehli boil) that often heals spontaneously.
In other instances the amastigotes may spread to the visceral organs (liver, spleen), resulting in "visceral leishmaniasis" (kala-azar or Dum-Dum fever) or to the mucous membranes of the mouth and nose, resulting in "mucocutaneousleishmaniasis" (espundia or uta). Left untreated, these latter diseases result in high rates of mortality.

CUTANEOUS LEISHMANIASIS:
Old World Cutaneous Leishmaniasis (CL)
L. majorcauses a moist, cutaneous, ulcerlike lesion at the site of the bite; it starts as a papule that runs an acute course (1-3 weeks) with early ulceration and a surrounding zone of inflammation, that usually heals in two months to a year leaving a depressed unpigmented scar, and lasting immunity.
It is transmitted by Phlebotomus spp. from gerbil, dogs or rodents to human or human-to-human. It is generally found in sparsely populated rural areas.
New World Cutaneous Leishmaniasis
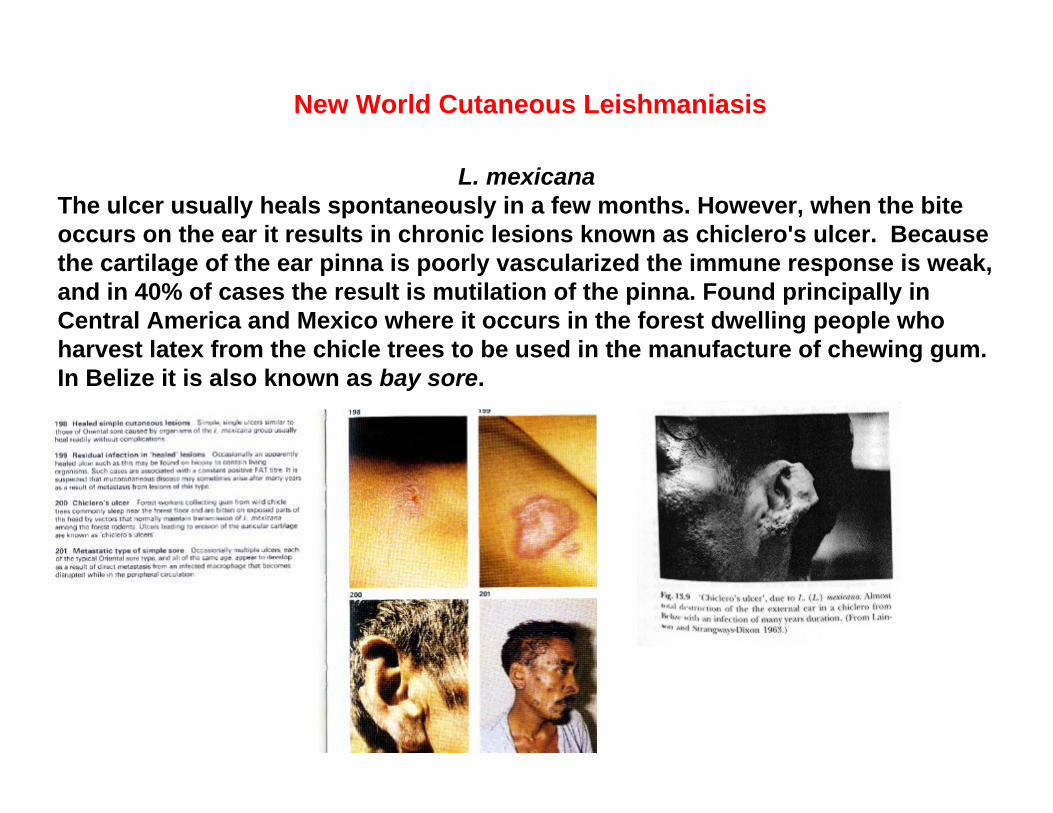
L. mexicanaThe ulcer usually heals spontaneously in a few months. However, when the bite occurs on the ear it results in chronic lesions known as chiclero's ulcer. Because the cartilage of the ear pinna is poorly vascularized the immune response is weak, and in 40% of cases the result is mutilation of the pinna. Found principally in Central America and Mexico where it occurs in the forest dwelling people who harvest latex from the chicle trees to be used in the manufacture of chewing gum. In Belize it is also known as bay sore.

cutaneous leishmaniasis, is usually localized to the site in which the sandfly bite occurs. The amastigotes multiply in the reticuloendothelialsystem of the skin. The incubation period spans from a period of day up to several months. If kept clean the sores will heal spontaneously within 2 months to 1 year. However, these sores often are the sites of secondary infections and can result in permanent disfiguration.
Once the infection has been cleared the host is immune to reinfection. In some regions, residents inoculate their children in a site normally not visible to protect the child from getting disfiguring scars later in life.
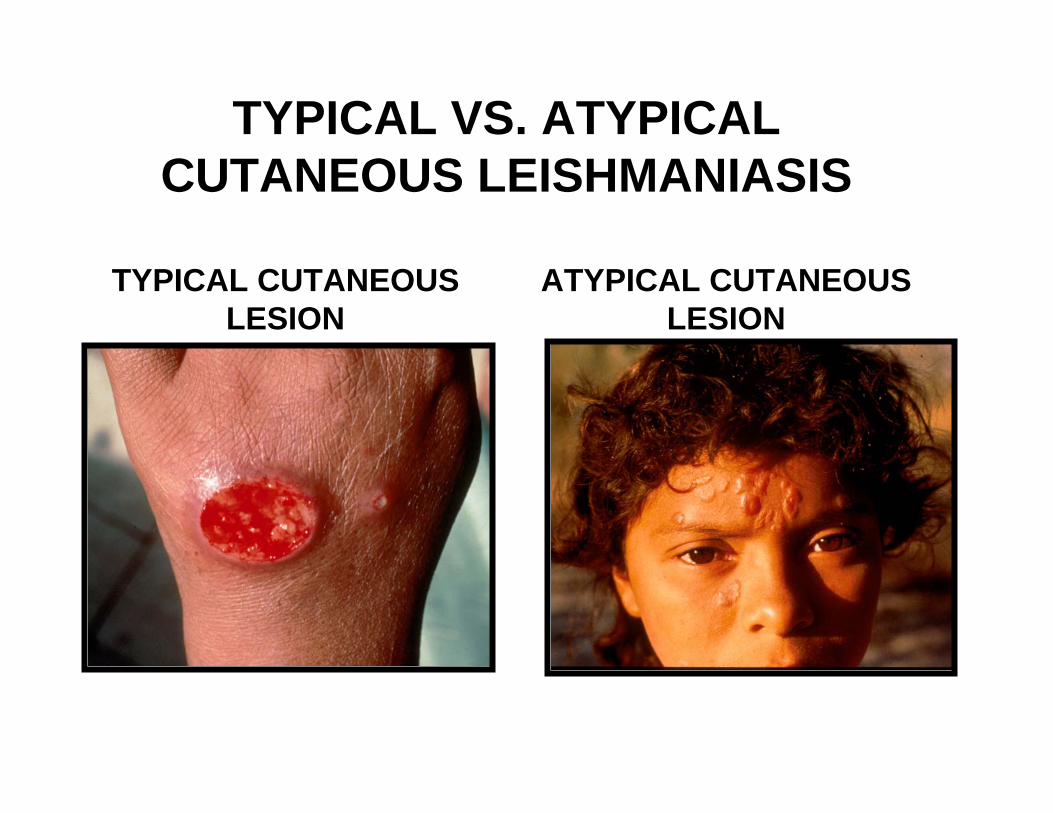
TYPICAL VS. ATYPICALCUTANEOUS LEISHMANIASIS
TYPICAL CUTANEOUSLESION
ATYPICAL CUTANEOUSLESION

L. braziliensisInoculation of promastigotes by the bite of a sandfly results in a small, red, skin papule that is itchy and ulcerates in 1-4 weeks like cutaneousleishmaniasis; this ulcer usually heals spontaneously within 6-15 months.
However, there is metastatic spread of the promastigotes from the site of the bite via the lymphatics. Disease is called espundia; the metastatic lesion involves the nasal and buccal mucosa causing destruction and malformations of the cartilage and soft tissues. The ulcerations can involve the nose, pharynx, palate and lips. Invasion of the larynx may result in a loss of speech. In Brazil 1/3 of the espundia cases are in children. May take many years for it to spread from the initial site of bite. Death may occur from secondary infections or respiratory complications.
Muco-cutaneous leishmaniasis

VISCERAL LEISHMANIASISL. donovani causes the classic type found in India. This is a metastatic disease. Rarely is a lesion seen at the site of bite and parasites are only occasionally seen in blood, but are present in the spleen and lymph nodes. The incubation period is 1-4 months. Disease is characterized by fever, anemia, splenomgegaly, wasting, imbalance of serum proteins and hyperpigmentation of the skin. The death rate is very high if left untreated. L. infantum causes the Mediterranean form of kala azar and has dogs, jackals and foxes as reservoirs. Humans are accidental hosts.


L. donovani group
This visceral disease has a new and old world form: particularly Brazil, and Mediterranean Europe, North Africa, East Africa, India and China.
The amastigote forms are found within the reticulo-endothelial cells of the viscera, ie the spleen, lymph nodes, liver and intestine.
The incubation time of 10 days-a year. The symptoms are a slow developing low grade fever, and general malaise, a progressive wasting of the patient with anaemia. Other classic symptoms as the disease progresses is the protrusion of the abdomen, hepatospenomegaly. If untreated death will occur within 2-3 years of contracting the infection.
In acute forms-the disease can run its course within 6- 12 months. Clinical signs include edema, particularly of the face, bleeding mucus membranes, breathing difficulties and diarrhea.

The epidemiology is extremely diverse: 20 Leishmaniaspecies are pathogenic for humans, and 30 sandfly species are proven vectors.
Old World: Phlebotomous spp.New World: Lutzomyia spp
There are two main epidemiological entities:
Zoonotic, where animal reservoir hosts are involved in the transmission cycle
Urban endemic: mostly human-human

Diagnosis of CL, MCL, DCL• suspected because of:
• geographical presence of parasite• history of sandfly bite• + skin lesion:
• chronic, painless, ‘clean’ ulcer• nasopharyngeal lesions• nodular lesions
• demonstration of parasite
• delayed hypersensitivity skin test
• serology?
• amastigotes (scrapings, biopsy, aspirates)
• in vitro culture (promastigotes)
• inoculate into hamsters

make incision in active part of lesion

A, B: Leishmania tropica amastigotes from an impression smear of a biopsy specimen from a skin lesion. In A, an intact macrophage is practically filled with amastigotes (arrows), several of which have a clearly visible nucleus and kinetoplast; in B, amastigotes are being freed from a rupturing macrophage. Patient had traveled to Egypt, Africa, and the Middle East.C: Three Leishmania amastigotes, each with a clearly visible nucleus and kinetoplast

VL Diagnosis• suspected because of:
• geographical presence of parasite• history of sandfly bite• prolonged fever, splenomegaly,
hepatomegaly, anemia, etc.• amastigotes in bone marrow
aspirates• in vitro culture of aspirates• serological tests
• direct agglutination• ELISA dipstick (39 kDa Ag)
Treatment
• Kala azar is treated today essentially as it was in 1940. The major drug is Sodium stibogluconate or Pentastam, a derivative of antimony, which was developed in 1930! Severe reactions including death occur in 10% of those treated. The recommended one month treatment costs around $150. Drug resistance has also developed. Up to 70% of infected patients in India have drug-resistant parasites.
• Amphotericin is used with or after an antimony compound for visceral leishmaniasis unresponsive to the antimonial alone.
• Pentamidine isotionate has been used in antimony-resistant visceral leishmaniasis, but although the initial response is often good, the relapse rate is high and it is associated with serious side-effects.
• Recently a new drug was developed, miltefosine. This is a membrane signaling pathway inhibitor. This can be taken orally and is very effective against visceral leishmaniasis. Clinical trials have a 95% cure rate!
• Pentamidine is also used for New World cutaneous leishmaniasis, but it usually heals spontaneously.
• There is no treatment for muco-cutaneous leishmaniasis.
Control and Epidemiology
• depends on local transmission
• avoid sandfly bites• bed nets• insecticides• destruction of dog
reservoir• ‘tropica vaccine’
• historical inoculation in covered areas
• risk of recidiva or VL
New World Dermal• zoonosis (arboreal
mammals = reservoir)• lowland forest• occupational
Old World Dermal• urban = dog reservoir• rural = rodent reservoir
Visceral• India (Ld): human-fly-
human• Africa (Ld): rodent
reservoir• others: dogs (with lesions)
are usual reservoir

Major problems and challenges for disease control
Technical, managerial, financial and political constraints.
There is no recognized cost-effective control package. Although tools for control have been considerably improved in recent years, they are still far from perfect:
Parasitology: existing tools (spleen, bone marrow [BM], lymph node aspirates) are either invasive methods and difficult to decentralize (spleen, BM) or of low sensitivity (lymph nodes). Treatment of VL cases by first-line drugs (Sb5+) is long expensive (US$ 120-150). Poor compliance often leads to increased unresponsiveness.
Vector control by spraying houses with insecticide is not sustainable. Animal reservoir control through environmental management is expensive and difficult to implement; the efficacy of dog culling is questionable.
Other constraints: lack of well-trained technical personnel, and weak delivery systems. Political and financial commitments are low and the level of implementation is frequently poor. Notification of leishmaniasis is compulsory in only 33 countries. Leishmaniasis is a disease of poverty: patients are the poorest among the poor (India: 88% of patients have a daily income of less than US$ 2), with poor socioeconomic environment and low educational level; they live either in remote rural areas or poor suburbs.

Problems with Control programs
Enzootic foci in wild animals: humans were rarely infected (central Asia)
Rural endemic foci: as humans colonized areas parasite moved into domesticated dogs, and cases in humans became more common (Asia, Russia, China, Mediterranean)
Urban endemic foci: wild animal populations are reduced in importance of life cycle-dogs become reservoirs and frequent transmission to humans (Central Asia, Eastern China)
Endemic / epidemic foci: few reservoirs- transmission principally man-man (India today)
Each of these different types of situation requires different approaches to control
Control of vectors
Protection vs bites
Treatment if infected persons
Elimination of reservoirs
Vaccination

When an infected Phlebotomid sand fly takes a blood meal it infects the vertebrate host with promastigote metacyclic forms. Within a short time the promastigotes are taken up by macrophages, the first line of defense of the immune system. During the process of uptake by the macrophage, the promastigote loses its flagella and transforms into the amastigoteform. Once internalized in a phagosome the macrophage lysosome fuses with the phagosome to from a phagolysosome containing the parasite.
How does the parasite survive this hostile environment?
Leishmania-Macrophage Interactions
• attachment and entry• involves CR3 and surface molecules
on parasite (Lipophosphoglycan)• entry is typical phagocytosis• phagosome fuses with lysosome

SURVIVAL IN THE MACROPHAGE PHAGOLYSOSOME
Respiratory burst products:H2O2, superoxide hydroxyl radicals
Cell Biology of Promastigote Entry into Macrophages
Promastigotes are taken up by phagocytosis and the parasites differentiate into amastigotes inside the phagosome. This is a very hostile environment where cells taken up by the macrophage are normally destroyed by:
• Oxidative burst - Phagocytosis of a foreign body activates an NAD(P)H oxidase in the plasma membrane. This produces the highly reactive superoxide and hydroxyl radicals at the site of engulfment. These radicals react with the pathogen's phospholipid membrane and also with its macromolecules. • Acidification - After fusion of the phagosome with the endosome, the vesicle is acidified by a proton ATPase. The low pH (4.5-5.0) causes denaturation of proteins, which become susceptible to acid hydrolases.
• Digestion - The endosome fuses with primary lysosomes, and acid hydrolases are released which degrade DNA, RNA, proteins and carbohydrates.

Defense strategies:
a) Detoxification with antioxidant enzymes:
Trypanothione peroxidase is a unique antioxidant enzyme which detoxifies hydrogen peroxide.
Superoxide dismutase - removes the reactive superoxide molecule.
b) Down-regulation - Lipophosphoglycans on the surface of the promastigote interfere with signal transduction pathways, specifically inhibits protein kinase C, which trigger the respiratory burst in response to the parasite.
c) Hydrolytic enzymes:
Leishmania possess surface glycoproteins that are refractory to host lysosomal enzymes and may also destroy them.
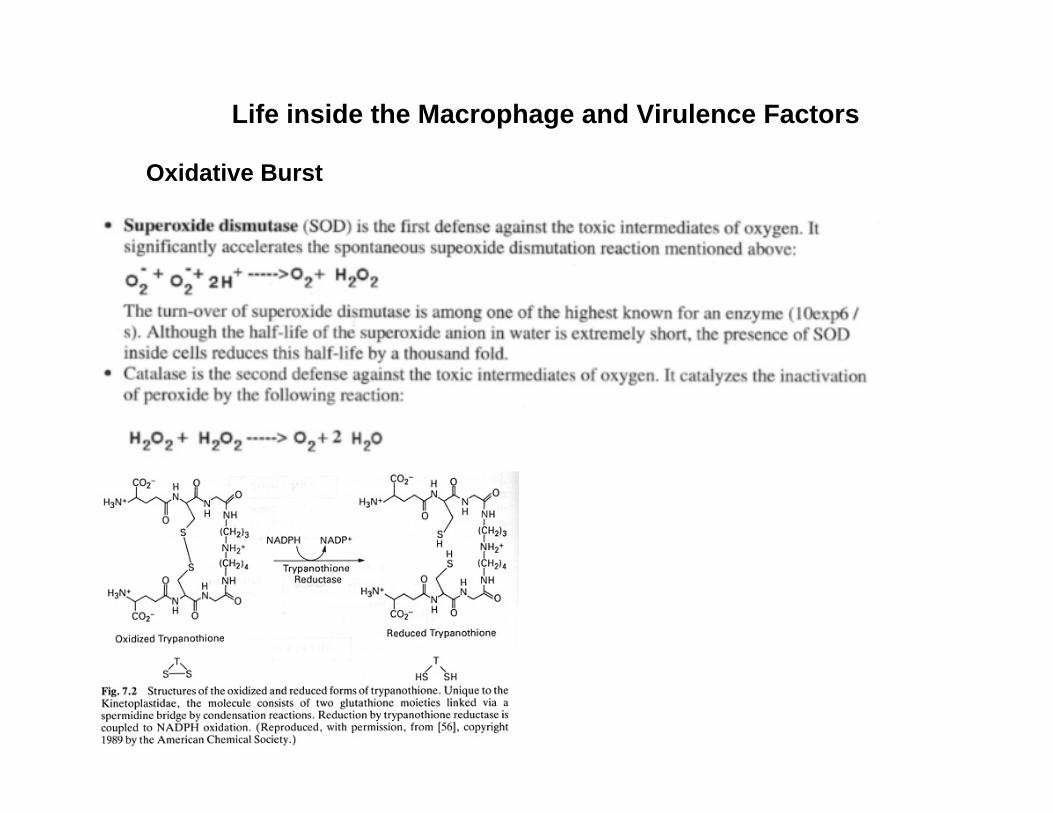
Life inside the Macrophage and Virulence Factors
Oxidative Burst
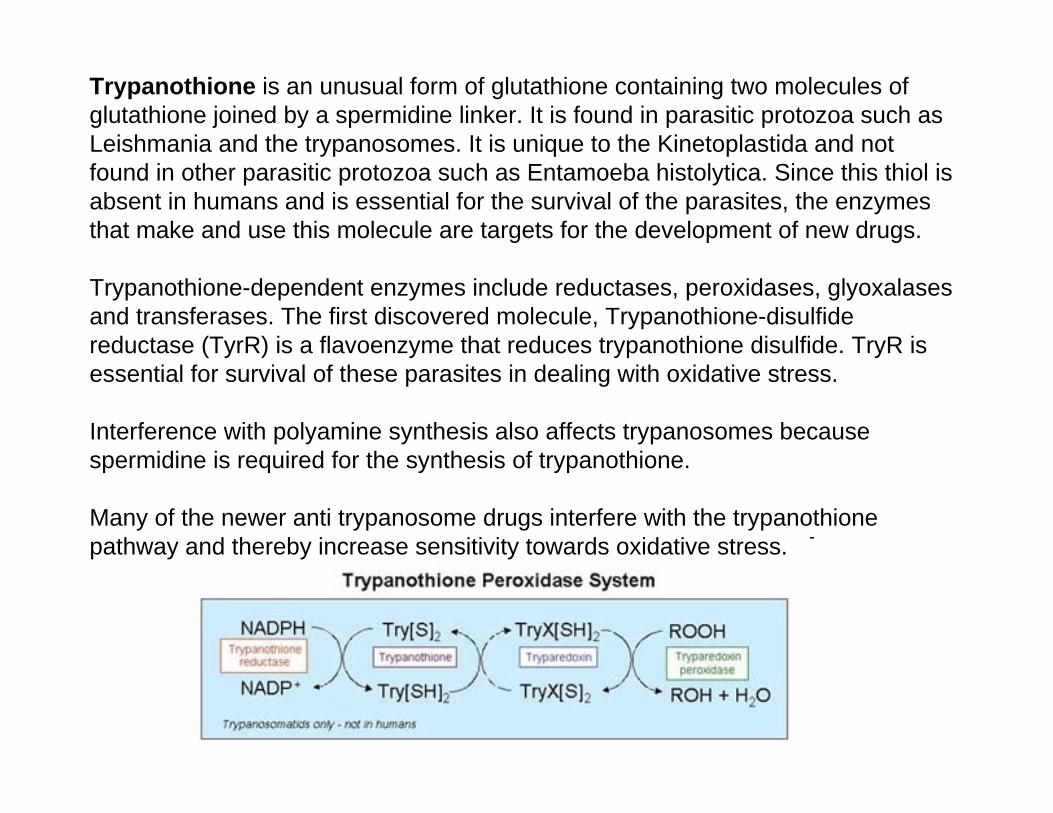
Trypanothione is an unusual form of glutathione containing two molecules of glutathione joined by a spermidine linker. It is found in parasitic protozoa such as Leishmania and the trypanosomes. It is unique to the Kinetoplastida and not found in other parasitic protozoa such as Entamoeba histolytica. Since this thiol is absent in humans and is essential for the survival of the parasites, the enzymes that make and use this molecule are targets for the development of new drugs.
Trypanothione-dependent enzymes include reductases, peroxidases, glyoxalasesand transferases. The first discovered molecule, Trypanothione-disulfide reductase (TyrR) is a flavoenzyme that reduces trypanothione disulfide. TryR is essential for survival of these parasites in dealing with oxidative stress.
Interference with polyamine synthesis also affects trypanosomes because spermidine is required for the synthesis of trypanothione.
Many of the newer anti trypanosome drugs interfere with the trypanothionepathway and thereby increase sensitivity towards oxidative stress.
10 August 2001
Promise of a leishmaniasis vaccine based on sand fly salivary proteins

In 1999 foxhounds at a hunt club in Millbrook, New York, came down with a mysterious illness. They showed bleeding, wasting, hair loss and kidney failure. More than 24 dogs died. Examination of joint fluid from the sick dogs led to the discovery of Leishmania parasites. Since then all of the 12,000 foxhounds in the US have been tested and 12% have antibodies to Leishmania.
The transmission of this disease is a mystery: No sandflies can live further north than New Jersey, the probability is low for sexual transmission or by wounds. , but experts in the Leishmania field do not agree. They theorize that the dogs were bitten by sandflies while touring in the South. Does another vector species exist? The Leishmania species is L. infantum and it is possible that there has been a low level epidemic in people in the US and it was missed.

Unexplained Illness Among Persian Gulf War Veterans in an Air National Guard Unit: Preliminary Report -- August 1990-March 1995
In November 1994, the U.S. Department of Veterans' Affairs (VA), the Department of Defense (DoD), and the Pennsylvania Department of Health requested that CDC investigate a report of unexplained illnesses among members of an Air National Guard (ANG) unit who were veterans of the Persian Gulf War (PGW) (August 1990-June 1991). These veterans had symptoms that included recurrent rash, diarrhea, and fatigue. A three-stage investigation was planned to 1) verify and characterize signs and symptoms in PGW veterans attending the VA medical center; 2) determine whether the prevalence of symptoms was higher among members of Unit A than among members of other units deployed to the PGW and, if so, whether the increased prevalence was associated with PGW deployment; and 3) characterize the illness and identify associated risk factors. This report presents preliminary findings from stages 1 and 2 (stage 3 is in progress).