a tick bite between the first and second tbe · pdf filebetween the first and second tbe...
TRANSCRIPT

hpg/nov 06 Folie 1
A Tick Bite
between
the First and Second TBE Vaccination
Hp. Gnehm, Aarau

hpg/nov 06 Folie 2
Adolescent girl G., 15 years
• Hospital admission July 02 2006
• History: headache the day before admission, on day of hospital admission increasing, piercing, fluctuating.
Fever up to 38,5° C.
Immunizations complete incl. MMR and Hep. B, FSME vaccine doses on May 29 and June 28 2006
Tick bite in endemicity area around June 17 2006
hpg/nov 06 Folie 3
• Personal history:
Twin A born at term, SGA. Twin B, boy, in good health.
At 8 years: recurrent episodes of fever,
clinical presentation and work up negative.
CBC, CRP, ESR normal, IgG, IgA, IgM and IgG-
subclasses normal,
immunization antibodies against T,D,HiB pos.
hpg/nov 06 Folie 4
• Hospital admission on July 02 2006:
38,8° C, well oriented, adequate reactions, weary, neck stiffness, photophobia, GCS 14-15, circulatory and respiratory systems unremarkable, no neurological signs
• CSF: 215 cells/mm3: 26 mono, 189 poly
tot. protein 0.47 g/l, glucose 3.37mmol/l, lactate 2.26 mmol/l

hpg/nov 06 Folie 5
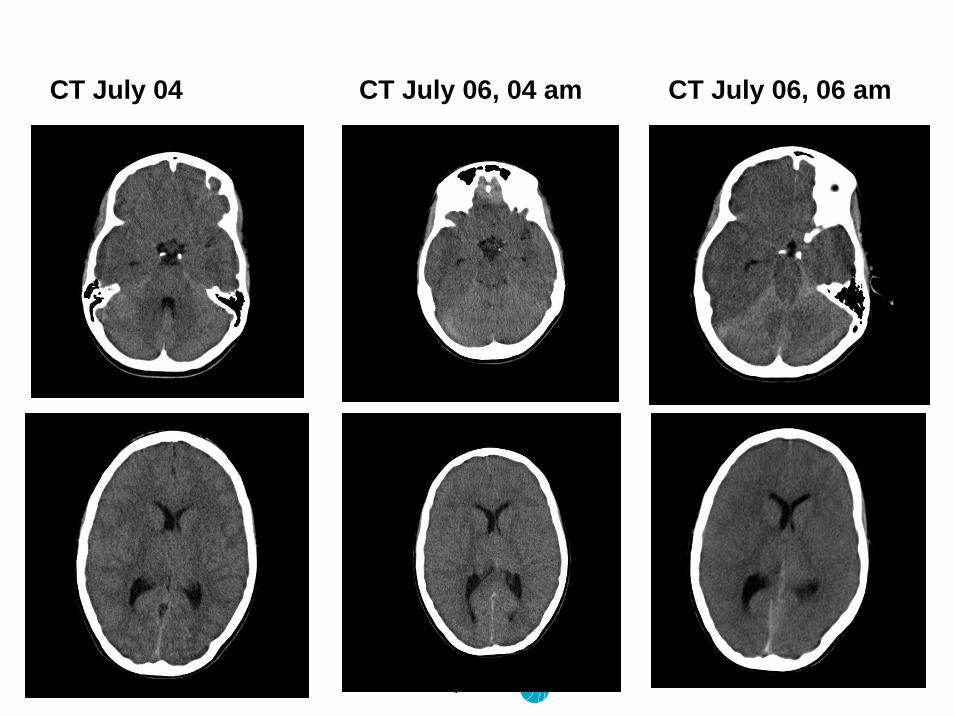
• Course:
Transfer after 2 days to ICU (July 04 2006): drowsiness, coma, generalized convulsions,
CCT: signs of generalized brain edema
2 CCTon July 06: increasing brain edema, loss of differenciation of gray and white matter, whitecerebellum sign
Death July 06 2006

hpg/nov 06 Folie 6
week 22 23 24 25 26 27
FSMEvaccine
1st dose 2nd dose
tick bite hospital
Time table: G. , girl 15 years old
hpg/nov 06 Folie 7
CT July 04 CT July 06, 04 am CT July 06, 06 am

hpg/nov 06 Folie 8
• CSF: HSV PCR neg., enterovirus PCR neg., bacterial cultures negative
Borreliosis and FSME IgM and IgG neg.
• Serum: WBC and diff., ESR, CRP normal,
FSME ELISA titer within 4 days: IgM from 41 VE to 62 VE (Virotech-Einh.)
IgG from 28 VE to 34 VE
all other serologies negative

hpg/nov 06 Folie 9
• Brain autopsy:
Inspection: massive brain edema, signs of herniation
Histology: severe lymphocytic meningoencephalitis
(no signs of ADEM)
Cortex Brain stem

hpg/nov 06 Folie 10
Further investigations:Klin. Institut für Virologie, Universität Wien:
FSME Virus July 2 July 6
Neutralizing ab 1 : 20 1 : 320
ELISA IgGVIE units
2660 220‘000
ELISA IgM VIE units
„grenzwertig“ > 1000
hpg/nov 06 Folie 11
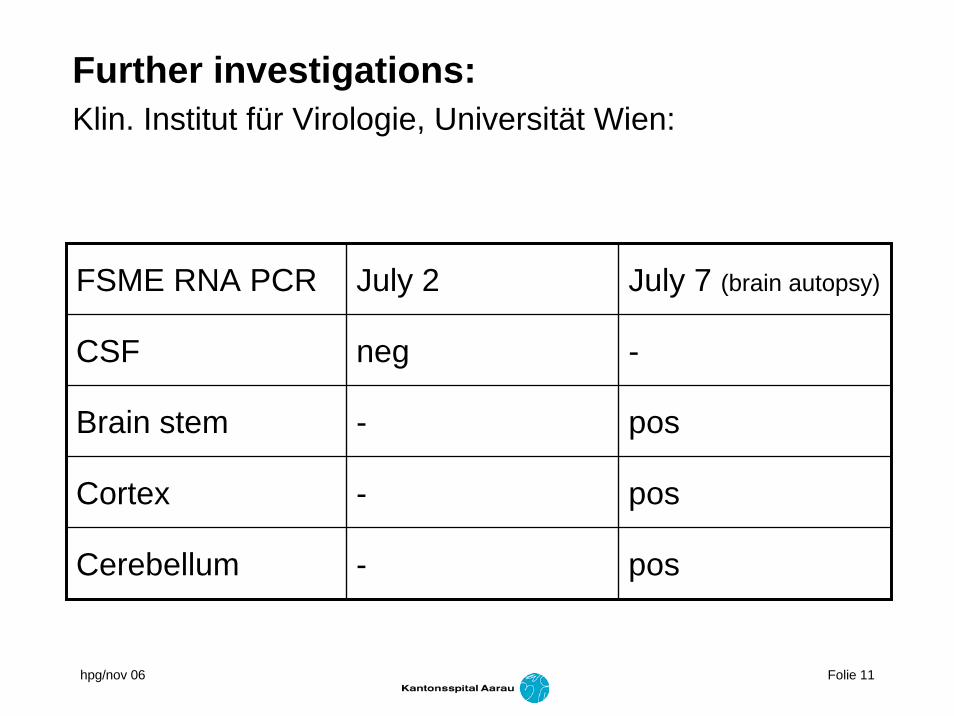
Further investigations:Klin. Institut für Virologie, Universität Wien:
FSME RNA PCR July 2 July 7 (brain autopsy)
CSF neg -
Brain stem - pos
Cortex - pos
Cerebellum - pos
hpg/nov 06 Folie 12
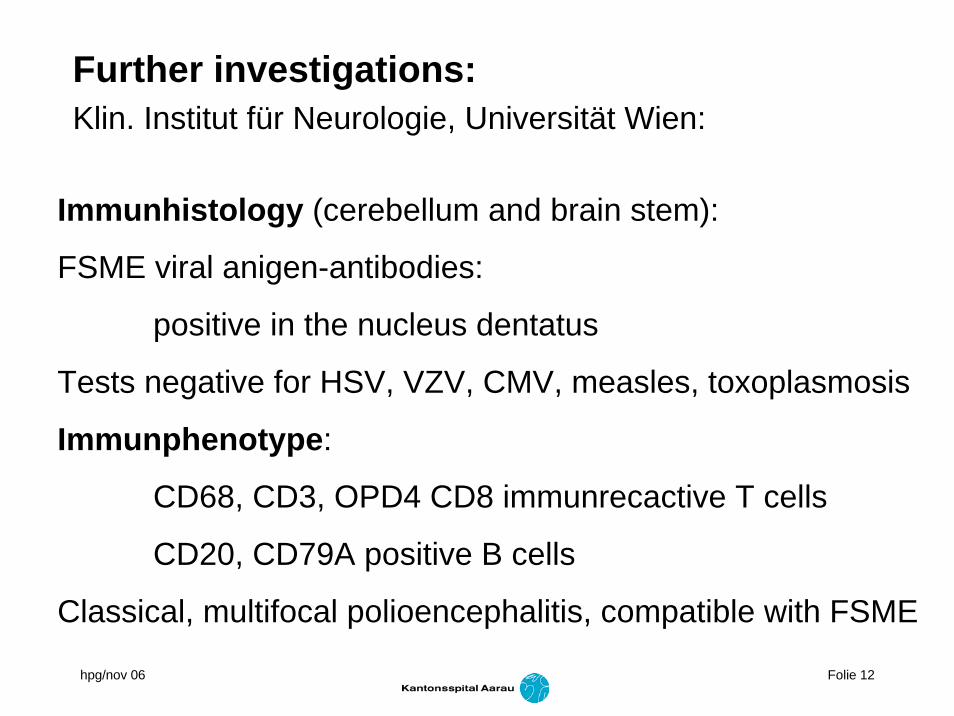
Further investigations:Klin. Institut für Neurologie, Universität Wien:
Immunhistology (cerebellum and brain stem):
FSME viral anigen-antibodies:
positive in the nucleus dentatus
Tests negative for HSV, VZV, CMV, measles, toxoplasmosis
Immunphenotype:
CD68, CD3, OPD4 CD8 immunrecactive T cells
CD20, CD79A positive B cells
Classical, multifocal polioencephalitis, compatible with FSME
hpg/nov 06 Folie 13
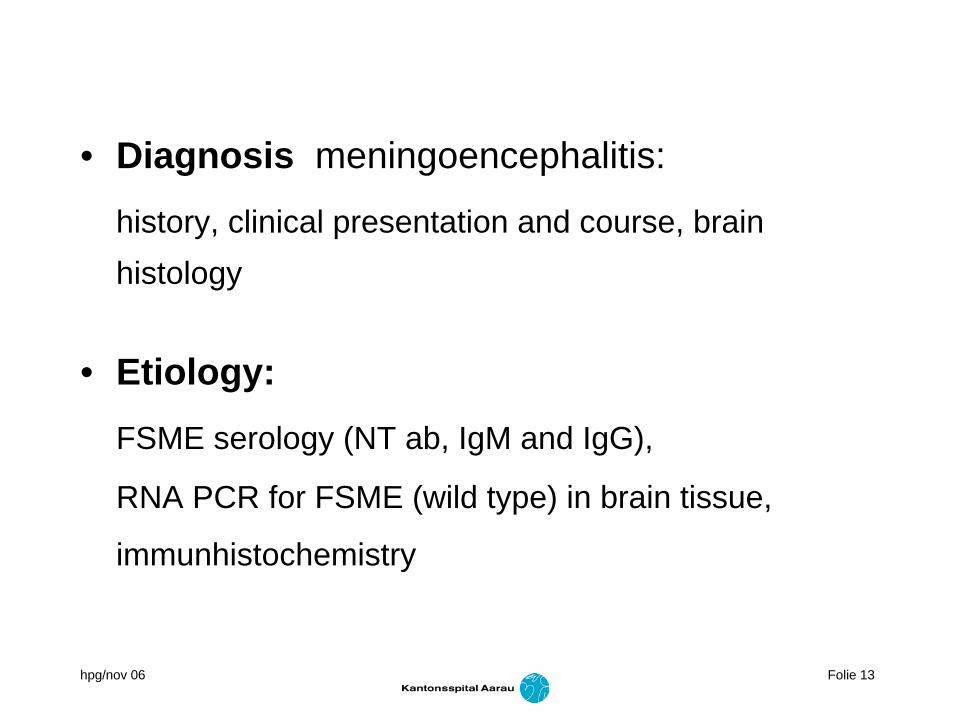
• Diagnosis meningoencephalitis:
history, clinical presentation and course, brainhistology
• Etiology:FSME serology (NT ab, IgM and IgG),
RNA PCR for FSME (wild type) in brain tissue,
immunhistochemistry
hpg/nov 06 Folie 14
Summary of Prof. Stephan Aberle, Wien:
„Die klinischen Angaben, die Histo, die serologischen Befunde und das PCR Ergebnis sprechen für eine gesicherte Infektion mit FSME bei der Patientin … Die vorliegende Sequenzanalyse spricht für Infektion mit WT Virus.“
hpg/nov 06 Folie 15
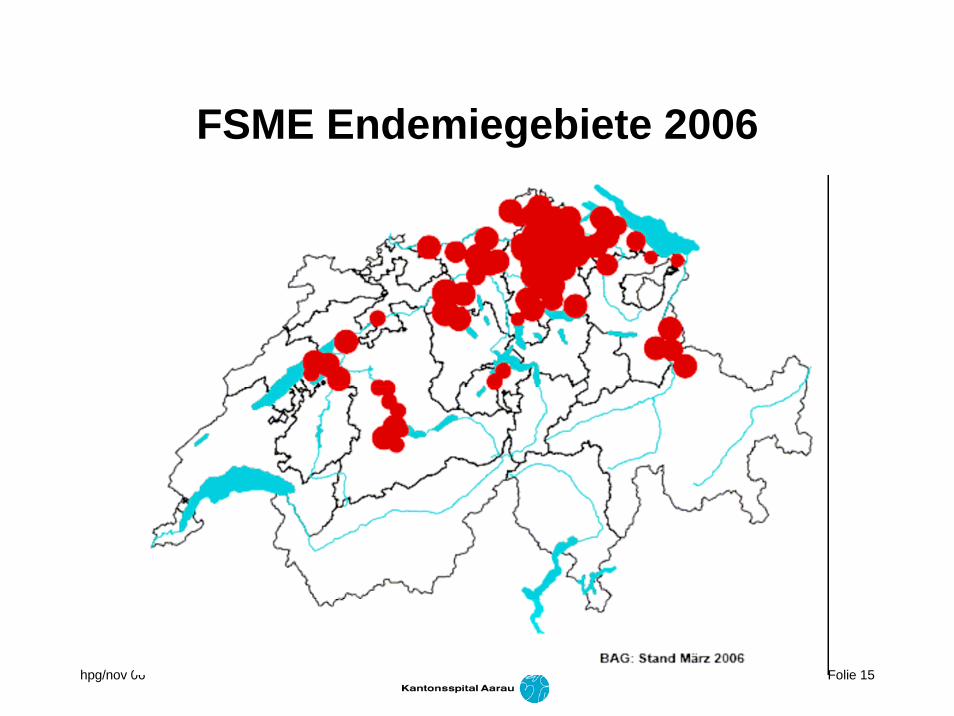
FSME Endemiegebiete 2006

hpg/nov 06 Folie 16
FSME S
ticho
rte
imAar
gau
hpg/nov 06 Folie 17
B BAG OFSP UFSP SFOPHFSME___________________________________________________
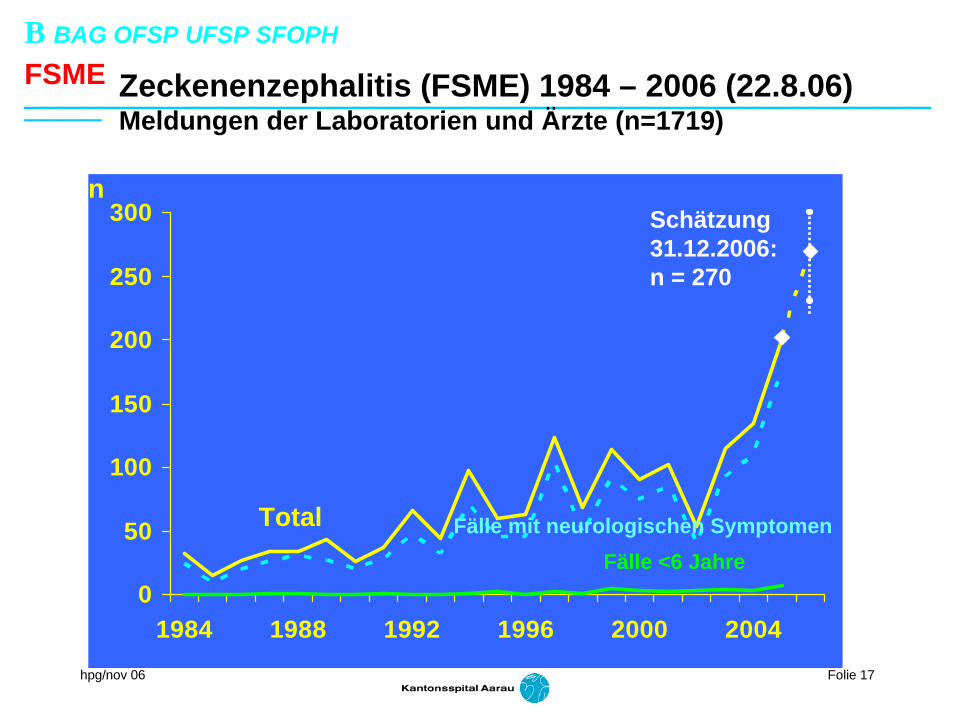
0
50
100
150
200
250
300
1984 1988 1992 1996 2000 2004
n
Fälle mit neurologischen SymptomenTotalFälle <6 Jahre
Schätzung31.12.2006:n = 270
Zeckenenzephalitis (FSME) 1984 – 2006 (22.8.06)Meldungen der Laboratorien und Ärzte (n=1719)

hpg/nov 06 Folie 18
Impfprophylaxe nach Exposition
Frühsommer-Meningoenzephalitis (FSME) PEP– passiv:
nicht für Kinder/Jugendliche < 14 J– aktiv:
nur möglich bei schon Teilimmunisierten, falls:letzte Impfung mindestens 14 Tage zurückliegt &Zeckenstich weniger als 48h zurückliegt
hpg/nov 06 Folie 19
• Pathogenesis:– immune competent adolescent girl
– impact of second FSME immunization?
– second FSME immunization administered later thanrecommended post-exposure immunization (PEP)
– no similar case known (Baxter data file)
FSME Immun 0.5ml 19 mio doses SAE 0.99/100‘000 FSME Immun 0.25ml 5 mio doses SAE 1.19/100‘000