a systematic review of the survival fdp_i_implant supported fdp
TRANSCRIPT

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 1/18
A systematic review of the survival andcomplication rates of fixed partialdentures (FPDs) after an observation
period of at least 5 yearsI. Implant-supported FPDs
Bjarni E. PjeturssonKen TanNiklaus P. Lang
Urs Bragger
Matthias Egger Marcel Zwahlen
Authors’ affiliations:Bjarni E. Pjetursson, Niklaus P. Lang, Urs Bragger ,School of Dental Medicine, University of Berne,Berne, SwitzerlandKen Tan, National Dental Center, Singapore,SingaporeMatthias Egger, Marcel Zwahlen, Division ofEpidemiology and Biostatistics, Department ofSocial and Preventive Medicine, University ofBerne, Berne, SwitzerlandMatthias Egger , MRC Health Services ResearchCollaboration, Department of Social Medicine,University of Bristol, Bristol, UK
Correspondence to:Bjarni E. PjeturssonDepartment of Periodontology andFixed ProsthodonticsUniversity of Berne
Freiburgstrasse7CH 3010 BerneSwitzerlandTel.: þ41 31 632 2577Fax: +41 31 632 4915e-mail: [email protected]
Key words: biological complications, complication rates, failures, implant dentistry, long-
itudinal, peri-implantitis, success, survival, systematic review, technical complications
Abstract
Objectives: The objective of this systematic review was to assess the 5- and 10-year survival
of implant supported fixed partial dentures (FPDs) and to describe the incidence of
biological and technical complications.
Methods: An electronic MEDLINE search complemented by manual searching was
conducted to identify prospective and retrospective cohort studies on FPDs with a mean
follow-up time of at least 5 years. Patients had to have been examined clinically at the
follow-up visit. Assessment of the identified studies and data abstraction was performed
independently by two reviewers. Failure and complication rates were analyzed using
random-effects Poisson regression models to obtain summary estimates of 5- and 10-year
survival proportions.
Results: The search provided 3844 titles and 560 abstracts. Full-text analysis was performed
for 176 articles resulting in 21 studies that met the inclusion criteria. Meta-analysis of these
studies indicated an estimated survival of implants in implant-supported FPDs of 95.4%
(95 percent confidence interval (95% CI): 93.9–96.5%) after 5 and 92.8% (95% CI: 90–94.8%)
after 10 years. The survival rate of FPDs supported by implants was 95% (95% CI: 92.2–
96.8%) after 5 and 86.7% (95% CI: 82.8–89.8%) after 10 years of function. Only 61.3% (95%
CI: 55.3–66.8%) of the patients were free of any complications after 5 years. Peri-implantitis
and soft tissue complications occurred in 8.6% (95% CI: 5.1–14.1%) of FPDs after 5 years.
Technical complications included implant fractures, connection-related and suprastructure-
related complications. The cumulative incidence of implant fractures after 5 years was
0.4% (95% CI: 0.1–1.2%). After 5 years, the cumulative incidence of connection-related
complications (screw loosening or fracture) was 7.3% and 14% for suprastructure-related
complications (veneer and framework fracture).Conclusion: Despite a high survival of FPDs, biological and technical complications are
frequent. This, in turn, means that substantial amounts of chair time have to be accepted by
the clinician following the incorporation of implant-supported FPDs. More studies with
follow-up times of 10 and more years are needed as only few studies have described the
long-term outcomes.
In earlier days, oral implants were mainly
used for the treatment of edentulous pa-
tients, and numerous studies have reported
successful outcomes for the rehabilitation
of these patients (e.g., Adell et al. 1981). As
the years passed the indications for implant
therapy were broadened and today, the
majority of patients receiving implants areCopyrightr Blackwell Munksgaard 2004
Date:
Accepted 30 June 2004
To cite this article:
Pjetursson BE, Tan K, Lang NP, Bragger U, Egger M,Zwahlen M. A systematic review of the survival andcomplication rates of fixed partial dentures (FPDs) afteran observation period of at least 5 years. I. Implant-supported FPDs.Clin. Oral Impl. Res. 15, 2004; 625–642doi: 10.1111/j.1600-0501.2004.01117.x
625

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 2/18

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 3/18
Data extraction
Of the included 21 studies, information on
the survival proportions of the reconstruc-
tions and on biological and technical comp-
lications was retrieved. Biological complica-
tions included disturbances in the function
of the implant characterized by a biological
process affecting the supporting tissues.
‘Peri-implantitis’ and ‘soft tissue complica-
tions’ were included in this category.
Technical complications denoted me-
chanical damage of implants, implant
components and/or the suprastructures.
Among these, ‘fractures of the implants,
screws or abutments’, ‘fractures of the
luting cement’ (loss of retention), ‘fractures
or deformations of the framework or ve-
neers’, ‘loss of the screw access hole
restoration’ and ‘screw or abutment loosen-
ing’ were included. From the included
studies the number of events for all of
these categories were abstracted and the
corresponding total exposure time of the
reconstruction was calculated.
Results on implant supported and com-
bined tooth–implant-supported FPDs have
been analyzed separately and have been
reported elsewhere (Lang et al. 2004).
Statistical analysis
By definition, failure and complication rates
are calculated by dividing the number ofevents (failures or complications) in the
numerator by the total exposure time (FPD
time and/or implant time) in the denomi-
nator.
The numerator could usually be ex-
tracted directly from the publication. The
total exposure time was calculated by tak-
ing the sum of:
(1) Exposure time of FPDs/implants that
could be followed for the whole
observation time.
(2) Exposure time up to a failure of the
FPDs/implants that were lost due to
failure during the observation time.
(3) Exposure time up to the end of obser-
vation time for FPDs/implants that
did not complete the observation per-
iod due to reasons such as death,
change of address, refusal to partici-
pate, non-response, chronic illnesses,
missed appointments and work com-
mitments.
For the evaluation of complication-free
FPDs the patient was used as unit of
analysis. For these outcomes total patient
exposure time was calculated by applying
the same procedures as for FPD- or implant
exposure time.
For each study, event rates for FPDs and/
or implants were calculated by dividing the
total number of events by the total FPDs orimplant exposure time in years. For further
analysis, the total number of events was
considered to be Poisson distributed for a
given sum of implant exposure years and
Poisson regression with a logarithmic link
function and total exposure time per study
as an offset variable were used (Kirkwood
& Sterne 2003a, 2003b).
Robust standard errors were calculated
to obtain 95 percent confidence intervals
(95% CI) of the summary estimates of the
event rates. To assess heterogeneity of thestudy-specific event rates, the Spearman
goodness-of-fit statistics and associated P-
value were calculated. If the goodness-of-fit
P-value was below 0.05, indicating hetero-
geneity, random-effects Poisson regression
(with g-distributed random effects) was used
to obtain a summary estimate of the event
rates. Five-year and 10-year survival propor-
tions were calculated via the relationship
between event rate and survival function S,
S(T )¼ exp(ÀT Â event rate), by assuming
constant event rates (Kirkwood & Sterne
2003a, 2003b). The 95% CI for the survival
proportions were calculated by using the
95% confidence limits of the event rates.
Multivariable Poisson regression was used
to investigate formally whether event rates
varied by study design (retrospective versus
prospective cohort studies), year of publica-
tion (1999 or before vs. 2000 or after), or
material (ceramic vs. gold–acrylic as veneer
material). All analyses were performed
using Statas (Stata Corporation, College
Station, TX, USA), version 8.2.
First electronic search
3844 Titles
Independently selected by 2 reviewers640 titles
Agreed by both560 titles
Abstracts obtained
DiscussionAgreed on 151 abstracts
Full text obtained
Total full text articles176
Final number of studies included
21
DiscussionDiscarded
80 titles
Kappa score 0.62
Further handsearching25 studies
67: Mean follow-up time less than 5 years.42: No detailed information on FPDs.
18: No information on the reconstructions.
14: Reporting on totally edentulous patients.
5: Multiple publications on the same
patient cohort
2: Reporting on failures without considering
the entire patient cohort
7: Reporting only on combined tooth-
implant supported FPDs (Lang et al. 2004)
Fig.1 . Search strategy. FPDs, fixed partial dentures.
Pjetursson et al . Systematic review of FPDs
627 | Clin. Oral Impl. Res. 15, 2004 / 625–642
8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 4/18
Results
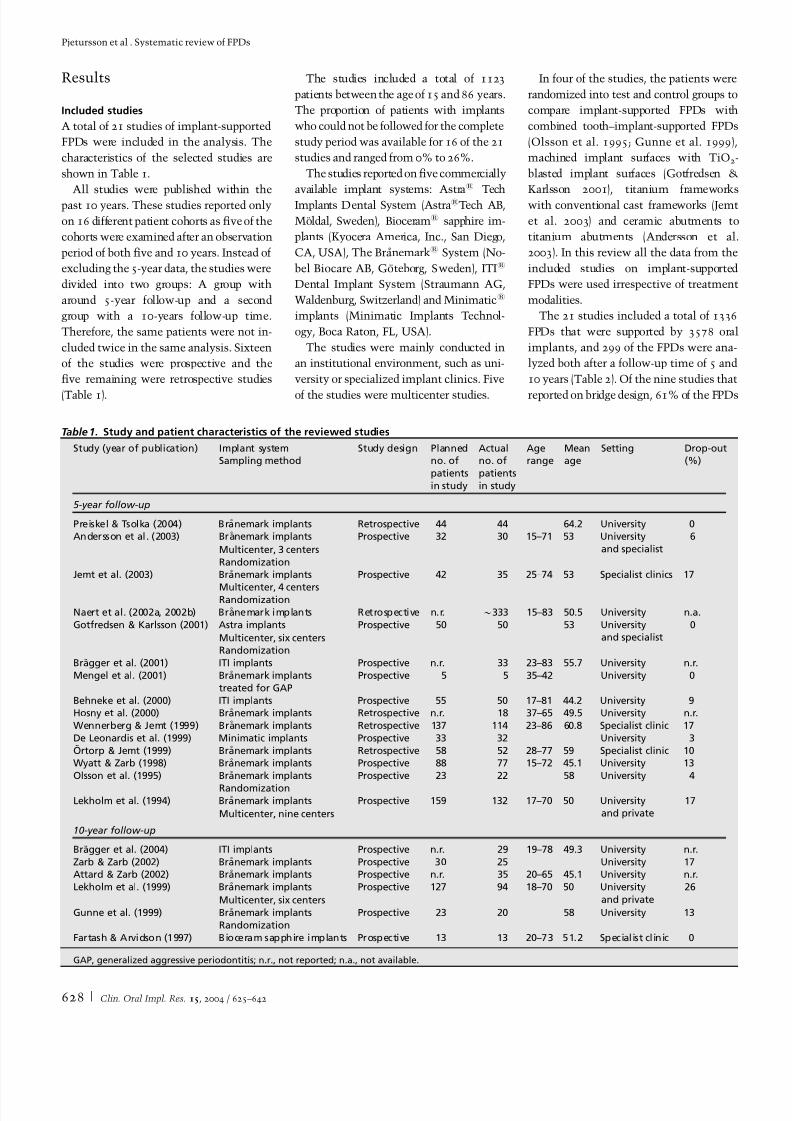
Included studies
A total of 21 studies of implant-supported
FPDs were included in the analysis. The
characteristics of the selected studies are
shown in Table 1.
All studies were published within the
past 10 years. These studies reported only
on 16 different patient cohorts as five of the
cohorts were examined after an observation
period of both five and 10 years. Instead of
excluding the 5-year data, the studies were
divided into two groups: A group with
around 5-year follow-up and a second
group with a 10-years follow-up time.
Therefore, the same patients were not in-
cluded twice in the same analysis. Sixteen
of the studies were prospective and the
five remaining were retrospective studies
(Table 1).
The studies included a total of 1123
patients between the age of 15 and 86 years.
The proportion of patients with implants
who could not be followed for the complete
study period was available for 16 of the 21
studies and ranged from 0% to 26%.
The studies reported on five commercially
available implant systems: Astras Tech
Implants Dental System (AstrasTech AB,
Moldal, Sweden), Biocerams sapphire im-
plants (Kyocera America, Inc., San Diego,
CA, USA), The Branemarks System (No-
bel Biocare AB, Goteborg, Sweden), ITIs
Dental Implant System (Straumann AG,
Waldenburg, Switzerland) and Minimatics
implants (Minimatic Implants Technol-
ogy, Boca Raton, FL, USA).
The studies were mainly conducted in
an institutional environment, such as uni-
versity or specialized implant clinics. Five
of the studies were multicenter studies.
In four of the studies, the patients were
randomized into test and control groups to
compare implant-supported FPDs with
combined tooth–implant-supported FPDs
(Olsson et al. 1995; Gunne et al. 1999),
machined implant surfaces with TiO2
-
blasted implant surfaces (Gotfredsen &
Karlsson 2001), titanium frameworks
with conventional cast frameworks (Jemt
et al. 2003) and ceramic abutments to
titanium abutments (Andersson et al.
2003). In this review all the data from the
included studies on implant-supported
FPDs were used irrespective of treatment
modalities.
The 21 studies included a total of 1336
FPDs that were supported by 3578 oral
implants, and 299 of the FPDs were ana-
lyzed both after a follow-up time of 5 and
10 years (Table 2). Of the nine studies that
reported on bridge design, 61% of the FPDs
Table1. Study and patient characteristics of the reviewed studies
Study (year of publication) Implant systemSampling method
Study design Plannedno. of
patients
in study
Actualno. of
patients
in study
Agerange
Meanage
Setting Drop-out(%)
5-year follow-up
Preiskel & Tsolka (2004) Branemark implants Retrospective 44 44 64.2 University 0Andersson et al. (2003) Branemark implants Prospective 32 30 15–71 53 University
and specialist
6
Multicenter, 3 centers
RandomizationJemt et al. (2003) Branemark implants Prospective 42 35 25–74 53 Specialist clinics 17
Multicenter, 4 centersRandomization
Naert et al. (2002a, 2002b) Branemark implants Retrospective n.r. $333 15–83 50.5 University n.a.
Gotfredsen & Karlsson (2001) Astra implants Prospective 50 50 53 Universityand specialist
0
Multicenter, six centersRandomization
Bragger et al. (2001) ITI implants Prospective n.r. 33 23–83 55.7 University n.r.
Mengel et al. (2001) Branemark implants
treated for GAP
Prospective 5 5 35–42 University 0
Behneke et al. (2000) ITI implants Prospective 55 50 17–81 44.2 University 9Hosny et al. (2000) Branemark implants Retrospective n.r. 18 37–65 49.5 University n.r.
Wennerberg & Jemt (1999) Branemark implants Retrospective 137 114 23–86 60.8 Specialist clinic 17
De Leonardis et al. (1999) Minimatic implants Prospective 33 32 University 3
Ortorp & Jemt (1999) Branemark implants Retrospective 58 52 28–77 59 Specialist clinic 10Wyatt & Zarb (1998) Branemark implants Prospective 88 77 15–72 45.1 University 13
Olsson et al. (1995) Branemark implants Prospective 23 22 58 University 4
RandomizationLekholm et al. (1994) Branemark implants Prospective 159 132 17–70 50 University
and private17
Multicenter, nine centers
10-year follow-up
Bragger et al. (2004) ITI implants Prospective n.r. 29 19–78 49.3 University n.r.
Zarb & Zarb (2002) Branemark implants Prospective 30 25 University 17Attard & Zarb (2002) Branemark implants Prospective n.r. 35 20–65 45.1 University n.r.
Lekholm et al. (1999) Branemark implants Prospective 127 94 18–70 50 University
and private
26
Multicenter, six centers
Gunne et al. (1999) Branemark implants Prospective 23 20 58 University 13
Randomization
Fartash & Arvidson (1997) Bioceram sapphire implants Prospective 13 13 20–73 51.2 Specialist clinic 0
GAP, generalized aggressive periodontitis; n.r., not reported; n.a., not available.
Pjetursson et al . Systematic review of FPDs
628 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 5/18
were metal ceramic, while the remainder
were of gold–acrylic design. Only 10% of
the FPDs were cemented, and 90% were
screw retained.
Thirteen studies reported on patient co-
horts in which all the patients were fol-
lowed for the same observation period: With
a follow-up time of 5 years (Lekholm et al.
1994; Olsson et al 1995; De Leonardis et al.
1999; Ortorp & Jemt 1999; Bragger et al.
2001; Gotfredsen & Karlsson 2001; Mengel
et al. 2001; Jemt et al. 2003; Andersson
et al. 2003) and 10 years (Fartash & Arvid-
son 1997; Gunne et al. 1999; Lekholm
et al. 1999; Wennerberg & Jemt 1999).
The other eight studies represented stu-
dies with variable individual observation
periods ranging from 0 to 16 years (Table 2).
Survival
Implant survival
All of the 21 studies reported on the survi-
val of the implants (Table 3). The reports
were separated into two groups. The first
consisted of the 15 studies with a mean
follow-up time of about 5 years (range
5–7.1 years) (Table 2). Of the originally 3549
implants placed, 181 implants were known
to be lost. Forty-nine percent (89/181) of
those implants were lost before loading and
51% (92/181) were lost during function.
The estimated study-specific 5-year survi-
val proportion varied between 86.3% and
99% (Table 3).
The estimated failure rate per 100 im-
plant years ranged from 0.2 to 2.94 (Fig. 2),
and the summary estimate, derived from
random-effects Poisson regression, was
0.94 failures per 100 implant years (95%
CI: 0.7–1.26) (Table 3).
The summary estimate for the survival
proportion after 5 years for implants sup-
porting FPDs was 95.4% (95% CI: 93.9–
96.5%) (Table 3).
Implant loss prior to functional loading
was detected in 2.5% of all implants
placed. For failures after loading, the esti-
mated annual failure rate was 0.51 (95%
CI: 0.39–0.67) for studies with 5 years of
follow-up, and 0.43 (95% CI: 0.32–0.6) for
the studies with 10 years of follow-up (no
significant difference).
The 10 prospective studies and the five
retrospective studies were also analyzed
separately. For the prospective studies,
based on 1576 implants, the summary
estimate of the survival proportion was
95.6% (95% CI: 93.3–97.2%) and for the
retrospective studies, based on 1973 im-
plants, the summary estimate of the survi-
val proportion was 95% (95% CI: 93–
96.4%). Formally investigating the differ-
ence in event rates in a Poisson regression
analysis confirmed the absence of a study
design effect (P¼0.64).
Comparing the event rates from studies
published between 2000 and 2004 with
those from studies published between
1994 and 1999 revealed a 48% lower
(95% CI: 17–67%) implant failure rate in
more recent studies (P¼0.006).
Table2. Information on implants and FPDs in the reviewed studies
Study(year of publication)
Total no.of implants
Total no.of FPDs
Metal/ ceramic
Gold/ resin
Cemented Screwretained
Follow-up range
Meanfollow-up
5-year follow-up
Preiskel & Tsolka (2004) 286 78 78 0 78n 78n 1–12 6.6
Andersson et al. (2003) 105 36 36 0 19 17 5 5
Jemt et al. (2003) 170 63 63 0 0 63 5 5
Naert et al.
(2002a, 2002b)
1022 409 340 69 n.r. n.r. 0–16 5.5
Gotfredsen & Karlsson
(2001)
133 52 n.r. n.r. n.r. n.r. 5 5
Bragger et al. (2001)w 84 40 40 0 30 10 5 5
Mengel et al. (2001) 36 7 n.r. n.r. n.r. n.r. 5 5
Behneke et al. (2000) 114 68 n.r. n.r. 13 55 5–8.3 5.4
Hosny et al. (2000) 49 18 16 2 0 18 1.3–14 6.5Wennerberg & Jemt
(1999)
422 133 31 99 0 133 5 5
De Loenardis et al.
(1999)
100 33 n.r. n.r. n.r. n.r. 5 5
Ortorp & Jemt (1999) 194 68 57 11 n.r. n.r. 5 5
Wyatt & Zrb (1998)w 230 97 15 82 0 97 1–12 5.4
Olsson et al. (1995)w 46 23 0 23 0 23 5 5
Lekholm et al. (1994)w 558 197 11 152 0 163 5 5
Total 3549 1322 687 438 62 579 5.3
10-year follow-up
Bragger et al. (2004) 69 33 33 0 25 8 8–12 10
Zarb & Zarb (2002) 94 34 n.r. n.r. 0 34 7–16 12
Attard & Zarb (2002) 105 46 n.r. n.r. 0 46 10–15 12.5Lekholm et al. (1999) 461 163 11 152 0 163 10 10
Gunne et al. (1999) 46 23 0 23 0 23 10 10
Fartash & Arvidson
(1997)
29 14 7 7 n.r. n.r. 10 10
Total 804 313 51 182 25 274 10.6
nFPDs were both cemented and screw retained.
wPatients included in 10-year follow-up studies were already analyzed in 5-year follow-up reports.
FPDs, fixed partial dentures; n.r., not reported.
Pjetursson et al . Systematic review of FPDs
629 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 6/18
The second group consisted of six studies
with a mean follow-up time of 10.6 years
(range 10–12.5 years) (Table 2). Of the
original 804 implants placed, 55 implants
were known to be lost. The study-specific
estimated 10-year survival proportion var-
ied between 85.5% and 98.6%, and the
summary estimate of the survival propor-
tion after 10 years for implants supporting
FPDs was 92.8% (95% CI: 90–94.8%)(Table 3).
FPD survival
FPD survival was defined as the FPD
remaining in situ with or without modifi-
cation for the observation period. Seven-
teen studies provided data on survival of
the FPDs (Table 4). The reports were di-
vided into two groups: The first group with
a total of 1289 FPDs and a mean follow-up
time of 5.3 years and the second group with
Table3. Annual failure rates and survival of implants
Study(year of publication)
Totalno. of
implants
Mean follow-uptime
No. offailure
Total implantexposure time
Estimatedfailure rate
(per 100
implant years)
Estimatedsurvival after
5 years (%)
Estimatedsurvival after
10 years (%)
5-year follow-up
Preiskel & Tsolka (2004) 286 6.6 9 1898 0.47 97.7
Andersson et al. (2003) 105 5 3 487 0.61 97
Jemt et al. (2003) 170 7.1 4 1162 0.34 98.3Naert et al. (2002a, 2002b) 1022 5.5 58 5121 1.13 94.5Gotfredsen & Karlsson (2001) 133 5 3 604 0.5 97.5
Bragger et al. (2001) 84 5 1 418 0.24 98.8
Mengel et al. (2001) 36 5 2 160 1.25 93.9
Behneke et al. (2000) 114 5.4 5 625 0.8 96.1Hosny et al. (2000) 49 6.5 2 312 0.64 96.8
Wennerberg & Jemt (1999) 422 5 25 1812 0.14 93.3
De Loenardis et al. (1999) 100 5 1 498 0.2 99Ortorp & Jemt (1999) 194 5 12 903 1.33 93.6
Wyatt & Zarb (1998) 230 5.4 14 1180 1.19 94.2
Olsson et al. (1995) 46 5 6 204 2.94 86.3
Lekholm et al. (1994) 558 5 36 2365 1.52 92.7
Total 3549 181 17,749
Summary estimate (95% CI)n 0.94
(0.7–1.26)
95.4
(93.9–96.5)
10-year follow-up
Bragger et al. (2004) 69 10 1 685 0.15 98.6
Attard & Zarb (2002) 105 12.5 6 1254 0.48 95.3
Zarb & Zarb (2002) 94 12 7 953 0.73 92.9Lekholm et al. (1999) 461 10 34 3753 0.91 91.3
Gunne et al. (1999) 46 10 6 382 1.57 85.5Fartash & Arvidson (1997) 29 10 1 286 0.35 96.6
Total 804 55 7313
Summary estimate (95% CI)w 0.75
(0.54–1.05)
92.8
(90–94.8)
nBased on random-effects Poisson regression, test for heterogeneity, P ¼0.0007.
wBased on standard Poisson regression, test for heterogeneity, P ¼0.081.
FPDs, fixed partial dentures; CI, confidence interval.
Lekholm et al.
Olsson et al.
Wyatt & Zarb
Örtrop & Jemt
De Loenardis et al.
Wennerberg & JemtHosny et al.
Behneke et al.
Mengel et al.Braegger et al.
Gotfredsen & Karlsson
Naert I et al.Preiskel & Tsolka
Jemt et al.
Andersson et al.
S
t u d y
0 1 2 3 4 5 6 7 8
Event Rate per 100 Years
Implant Failure Rate
Summary Estimate
0.94 (95% CI: 0.70-1.26)
Fig.2 . Annual failure rates (per 100 implants). CI, confidence interval.
Pjetursson et al . Systematic review of FPDs
630 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 7/18
a total of 219 FPDs and a mean follow-up
time of 10 years.
In the former group, 63 out 1289 FPDs
were lost and the study-specific estimated
5-year survival varied between 82.2% and
100% (Table 4). The estimated failure rate
per 100 FPD years ranged from 0 to 3.92
(Fig. 3) and the summary estimate, derived
from a random-effects analysis, was 1.03
(95% CI: 0.65–1.62) (Table 3) translating
into a survival proportion after 5 years for
implant-supported FPDs of 95% (95% CI:
92.2–96.8%).
The studies in the 5-year observationgroup were also divided according to the
veneer material utilized: A group of seven
studies with a total of 712 FPDs with
ceramic as veneer material and a group of
four studies with a total of 450 FPDs with
acrylic veneers. The group with metal
ceramic FPDs showed a significantly
higher (P¼0.014) summary estimate of
the survival proportion after 5 years of
96.6% (95% CI: 95.9–97.3%), compared
with a survival of 90.4% (95% CI: 79.8–
95.6%) for the gold–acrylic FPDs.
In the 10-year observation group, 27 out
of 219 FPDs were lost. The study-specific
survival after 10 years varied between
81.1% and 93.9% (Table 4). The summary
estimate of the survival proportion after 10
years for implant-supported FPDs was
86.7% (95% CI: 82.8–89.8%).
Success
Success was defined as an FPD being free of
all complications over the entire observa-
tion period.
Table4. Annual failure rate and survival of FPDs
Study (year of publication) Total no.of FPDs
Meanfollow-up
time
No. offailure
Total FPDsexposure
time
Estimatedfailure rate
(per 100
FPD years)
Estimatedsurvival after
5 years (%)
Estimatedsurvival after
10 years (%)
5-year follow-up
Preiskel & Tsolka (2004) 78 6.6 2 519 0.39 98.1
Andersson et al. (2003) 36 5 1 164 0.61 97
Jemt et al. (2003) 63 5 3 295 1.02 95Naert et al. (2002a, 2002b) 409 5.5 15 2049 0.73 96.4
Gotfredsen & Karlsson (2001) 52 5 2 236 0.85 95.9
Bragger et al. (2001) 40 5 1 198 0.51 97.5Mengel et al. (2001) 7 5 0 33 0 100
Behneke et al. (2000) 68 5.4 1 372 0.27 98.7
Hosny et al. (2000) 18 6.5 0 117 0 100
Ortorp & Jemt (1999) 68 5 3 323 0.93 95.5Wennerberg & Jemt (1999) 133 5 2 608 0.33 98.4
Wyatt & Zarb (1998) 97 5.4 16 498 3.21 85.2
Olsson et al. (1995) 23 5 4 102 3.92 82.2
Lekholm et al. (1994) 197 5 13 889 1.46 92.9
Total 1289 63 6403
Summary estimate (95% CI)n 1.03 (0.65–1.62) 95 (92.2–96.8)
10-year follow-up
Bragger et al. (2004) 33 10 2 320 0.63 93.9Lekholm et al. (1999) 163 10 21 1378 1.52 85.9Gunne et al. (1999) 23 10 4 191 2.09 81.1
Total 219 27 1889
Summary estimate (95% CI)w 1.43 (1.08–1.89) 86.7 (82.8–89.8)
nBased on random-effects Poisson regression, test for heterogeneity P o0.0001.
wBased on standard Poisson regression, test for heterogeneity P ¼0.035.
FPDs, fixed partial dentures; CI, confidence interval.
Lekholm et al.
Olsson et al.
Wyatt & Zarb
Wennerberg & Jemt
Örtrop & Jemt
Hosny et al.
Behneke et al.
Mengel et al.
Brägger et al.
Gotfredsen & Karlsson
Naert et al.Preiskel & Tsolka
Jemt et al.
Andersson et al.
S t u d y
0 1 2 3 4 5 6 7 8
Event Rate per 100 Years
FPD Failure Rate
Summary Estimate1.03 (95% CI: 0.65-1.62)
Fig.3 . Annual failure rates (per 100 fixed partial dentures [FPDs]). CI, confidence interval.
Pjetursson et al . Systematic review of FPDs
631 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 8/18
Only three (Ortorp & Jemt 1999;
Wennerberg & Jemt 1999; Jemt et al.
2003) out of 21 studies reported how
many patients were free of complications.
For one study (Bragger et al. 2001) this
information could be extracted from the
orginal database.
These four studies included 266 patients
with a mean follow-up time of 5 years, and
122 patients had some kind of complica-
tions over the observation period (in total
253 complications). The summary esti-
mate of the proportion of success after 5
years was 61.3% (95% CI: 55.3–66.8%)
(Table 5). In other words, 38.7% of the
patients had minor or major complications
in the first 5 years after implantation.
Biological complications
Peri-implant mucosal lesions were reported
in various ways by the different authors.
Nine studies provided information on soft
tissue complications and peri-implantitis.
One study (Gotfredsen & Karlsson 2001)
compared implants with TiO2
-blasted and
-machined surfaces and reported a higher
proportion of implants with signs of in-
flammation (pain, redness swelling and
bleeding) at baseline for the TiO2
group
(5% vs. 0%). After 1 year, similar cumu-
lative complication rates were observed
(12% and 9%, respectively). After 5 years,
finally, similar incidences were described
for both groups.
Bragger et al. (2001) defined peri-implan-
titis as probing pocket depth (PPD)
!5 mm and bleeding on probing (BOP)
with 10% of the patients (five patients) or
9.6% of the implants being affected.
Behneke et al. (2000) reported that 4% of
the patients had peri-implantitis at pros-
thesis placement. In addition, 9% of the
patients were diagnosed as having peri-im-
plantitis during the first year. During the
second year and thereafter the annual fre-
quency of peri-implantitis was 2–5%.
Other studies (Lekholm et al. 1994;
Wennerberg & Jemt 1999) reported on
‘soft tissue complications’, defined as fis-
tula, gingivitis or hyperplasia.
One study (Wyatt & Zarb 1998) reported
that 13% of the FPDs (13 out of 97) had at
least one soft tissue complication (infection
and/or inflammation) over the observation
period.
In a random-effects Poisson-model ana-
lysis, the pooled cumulative rate of bio-
logical complications after 5 years for
patients treated with implant-supported
FPDs was 8.6% (95% CI: 5.1–14.1%)
(Table 6).
Technical complications
The most common technical complication
was the fracture of a veneer (acryl, ceramic
and composite). After 5 years, 13.2% (95%
CI: 8.3–20.6%) of the FPDs had fractures
of veneers (Table 7).
Table5 . Any complications in treated patients
Study (year of publication) Total no.of patients
Meanfollow-up
time
No. ofcomplications
Total patientexposure time
Estimatedcomplication rate
(per 100 patient years)
Estimatedsuccess after
5 years (%)
5-year follow-up
Jemt et al. (2003) 42 5 22 195 11.28 56.9
Bragger et al. (2001) 33 5 7 163 4.29 80.7
Ortorp & Jemt (1999) 58 5 30 281 10.68 58.6
Wennerberg & Jemt (1999) 133 5 63 608 10.36 59.6
Total 266 122 1247
Summary estimate (95% CI)n 9.78 (8.07–11.86) 61.3 (55.3–66.8)
nBased on standard Poisson regression, test for heterogeneity P ¼0.12.
CI, confidence interval.
Table6 . Biological complications
Study (year of publication) Total no.
of FPDs
Mean
follow-up
time
No. of
complications
Total FPDs
exposure
time
Estimated failure
rate (per 100
FPD years)
Estimated cumulative
complication rate
after 5 years (%)
5-year follow-up
Jemt et al. (2003) 63 5 3 295 1.02 5
Gotfredsen & Karlsson (2001)n 52 5 9 236 3.81 17.4Bragger et al. (2001) 40 5 4 198 2.02 9.6
Behneke et al. (2000)n 68 5.4 12 372 3.22 14.9
De Leonardis et al. (1999) 33 6.5 1 235 0.42 2.1
Ortorp & Jemt (1999) 68 5 1 323 0.31 1.5
Wennerberg & Jemt (1999) 133 5 15 608 2.48 11.6Wyatt & Zarb (1998) 97 5.4 13 498 2.61 12.2
Lekholm et al. (1994) 197 5 3 889 0.34 1.7
Total 751 61 3654
Summary estimate (95% CI)w 1.79 (1.05–3.03) 8.6 (5.1–14.1)
nIncidence of biological complications calculated by adding the incidence after 1 year to half of the events that occurred after that first, assuming that half of
the complications belonged to new patients and the other 50% of the patients that had already experienced a biological complications after 1 year.
wBased on random-effects Poisson regression, test for heterogeneity P o0.0001.
FPDs, fixed partial dentures; CI, confidence interval.
Pjetursson et al . Systematic review of FPDs
632 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 9/18
The second most common technical
complication, loss of the screw access
hole restoration, was reported only in one
study (Ortorp & Jemt 1999). This occurred
in 8.2% of the anchors.
The third most common technical com-
plication, abutment or occlusal screw loos-
ening, and its cumulative incidence after
5 years of follow-up was 5.8% (95% CI:
3.8–8.7%) (Table 7).
Fracture of abutments and occlusal
screws occurred in 1.5% (95% CI: 0.8–
2.8%) (Table 7) of the abutments after a
follow-up time of 5 years and 2.5% (95%
CI: 1.6–4.7%) after 10 years.
Fracture of implants were a rare compli-
cation with a cumulative incidence of
0.4% (95% CI: 0.1–1.2%) (Table 7) after
a follow-up time of 5 years and 1.8% (95%
CI: 1.2–2.6%) after 10 years.
Two studies, both Bragger et al. (2001,2004), reported on fractures of the luting
cement (loss of retention). They reported a
cumulative incidence of 2.9% after 5 years
and 16% after 10 years.
Discussion
This systematic review is part of a series of
systematic reviews addressing the survival
and complication rates of fixed partial den-
tures of different design.Systematic reviews have been used in
medicine for the last two decades to sum-
marize the cumulative information on the
optimal treatment for clinically important
questions. This research method has
slowly found its way into dental research.
Systematic reviews have mainly been used
to analyze RCTs (Egger et al. 2001).
For this systematic review, no RCTs
were available comparing conventional
fixed prosthodontics to implant-supported
fixed prosthodontics. In the absence of
RCTs, a lower level of evidence, prospec-
tive and retrospective cohort studies were
included in this systematic review in order
to summarize the available information
about survival and complication rates of
implant-supported fixed partial dentures
after a period of at least 5 years.
The results of longitudinal cohort studies
with a mean follow-up time of at least 5
years regarding survival and success of
FPDs and their biological and technical
complications were reviewed systemati- T a b l e 7 .
T e c h n i c a l c o m p l i c a t i o n s
S t u d y
( y e a r o f p u b l i c a t i o n )
M e a n
f o l l o w - u p
t i m e
T o t a l n o . o f
i m p l a n t a t i o n s
T o t a l
i m p l a n t a t i o n
e x p o s u r e
t i m e
E s t i m a t e d
r a t e o f
i m p l a n t f r a c t u r e
( p e r 1 0 0 i m p l a n t
y e a r s )
E s t i m a t e d r a t e
o f a b u t m e n t o r
s c r e w f r a c t u r e ( p e r
1 0 0 i m p l a n t y e a r s )
E s t i m a t e d r a t e o f
l o o s e a b u t m
e n t s
o r s c r e w s ( p
e r 1 0 0
i m p l a n t y e a
r s )
T o t a l
n o . o f
F P D s
T o t a l F P D
e x p o s u r e
t i m e
E s t i m a t e d r a t e
o f v e n e e r f r a c
t u r e
( p e r 1 0 0 F P D y e a r s )
E s t i m a t e d r a t e o f
m e t a l f r a m e w o r k
f r a c t u r e ( p e r
1 0 0 F P D y e a r s )
5 y e a r f o l l o w - u p
P r e i s k e l & T s o l k a ( 2 0 0 4 )
6 . 6
2 8 5
1 8 9 8
0
0 . 0 5
0 . 4 2
7 8
5 1 9
0 . 1 9
n . r .
A n d e r s s o n e t a l . ( 2 0 0 3 )
5
1 0 3
4 8 7
n . r .
0 . 2 1
n . r .
3 6
1 6 4
0 . 6 1
0
J e m t e t a l . ( 2 0 0 3 )
5 – 7 . 1
n
1 6 9
1 1 6 2
0 . 0 9
0 . 1 7
0 . 7 7
6 3
2 9 5
3 . 3 9
0 . 3 4
G o t f r e d s e n & K a r l s s o n
( 2 0 0 1 )
5 . 5
1 3 3
6 0 4
0
0 . 3 3
2 . 8 1
5 2
2 3 6
0 . 8 5
0
B r a ¨ g g e r e t a l . ( 2 0 0 1 )
5
8 4
4 1 8
0 . 2 4
0
1 . 6 7
4 0
1 9 8
2 . 0 2
0
B e h n e k e e t a l . ( 2 0 0 0 )
5 . 4
1 1 4
6 2 5
0
0
2 . 0 8
6 8
3 7 2
1 . 8 8
n . r .
H o s n y e t a l . ( 2 0 0 0 )
6 . 5
4 9
3 1 2
0
0
n . r .
1 8
1 1 7
n . r .
0
O ¨ r t o r p & J e m t ( 1 9 9 9 )
5
1 9 4
9 0 3
0
0 . 1 1
0 . 2 2
6 8
3 2 3
5 . 5 7
0
W e n n e r b e r g & J e m t
( 1 9 9 9 )
5
4 2 2
1 8 1 2
0
0 . 8 8
1 . 2 1
1 3 3
6 0 8
2 . 9 6
0 . 1 6
W y a t t & Z a r b ( 1 9 9 8 )
5 . 4
2 3 0
1 1 8 0
0
0 . 8 5
0 . 8 5
9 7
4 9 8
4 . 6 2
0 . 4
L e k h o l m e t a l . ( 1 9 9 4 ) w
5
5 5 8
2 3 4 6
0 . 2 1
0 . 3 8
1 . 1 5
1 9 7
8 8 9
5 . 5 1
n . r .
S u m m a r y e s t i m a t e e v e n t
r a t e s ( 9 5 %
C I )
0 . 0 7 z
( 0 . 0 2 – 0 . 2 3 )
0 . 3
y
( 0 . 1 6 – 0 . 5 7 )
1 . 1 9 y
( 0 . 7 7 – 1 . 8 2 )
2 . 8 4 y
( 1 . 7 4 – 4 . 6 2 )
0 . 1 6 z
( 0 . 0 7 – 0 . 3 6 )
C u m u l a t i v e 5 y e a r
c o m p l i c a t i o n r a t e s
( 9 5 %
C I )
0 . 4 % z
( 0 . 1 – 1 . 2 )
1 . 5 % y
( 0 . 8 – 2 . 8 )
5 . 8 % y
( 3 . 8
– 8 . 7 )
1 3 . 2 % y
( 8 . 3 – 2 0 . 6 )
0 . 8 % z
( 0 . 4 – 1 . 8 )
n M e a n f o l l o w - u p t i m e w a s 7 . 1 y e a r s f o r
t h e i m p l a n t s a n d 5 y e a r s f o r t h e F P D s .
w I n f o r m a t i o n w a s g i v e n o n n u m b e r o f p
a t i e n t s w i t h c o m p l i c a t i o n s .
z B a s e d o n s t a n d a r d P o i s s o n r e g r e s s i o n .
y B a s e d o n r a n d o m - e f f e c t s P o i s s o n r e g r e s s i o n .
F P D s , fi x e d p a r t i a l d e n t u r e s ; C I , c o n fi d e n c e i n t e r v a l ; n . r . , n o t r e p o r t e d .
Pjetursson et al . Systematic review of FPDs
633 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 10/18
cally. Survival was defined as FPD remain-
ing in situ with or without modifications.
Success was defined as the FPDs remaining
in situ free of all complications over the
entire observation period.
When multiple publications with differ-
ent follow-up times on the same cohort
were available, only the publication with
the longest follow-up time is generally
included in a systematic review. For five
out of six studies with a mean follow-up
time of 10 years or more, a 5-year report
was also available. Instead of excluding the
5-year data, the studies were divided into
two groups: A group with about 5 years of
follow-up and a second group with about
10 years of follow-up.
Even with follow-up periods of at least
5 years, some clinicians may argue that
this is still too short to obtain reliable
information on survival and complicationrates. Due to the fact that use of dental
implants for rehabilitation of partially
edentulous patients is relatively new, a
mean follow-up period of at least 5 years
was a necessary compromise. However, it
is acknowledged that information on long-
term survival is still scarce, and the results
of the present review should not be extra-
polated to follow-up times measured in
decades. The present review demonstrated
that the existing longitudinal studies did
not include many patients with a prolongedfollow-up time.
The search of the present review aimed
to identify longitudinal cohort studies re-
porting on FPDs. When titles and abstracts
did not provide sufficient information on
study duration and whether or not infor-
mation on the suprastructure was provided,
a full-text analysis of the articles was
carried out. The majority of longitudinal
implant studies did not address the recon-
structions at all. Nor did they distinguish
between different types of reconstructions.
Therefore, a substantial portion of the pub-
lished literature could not be included in
this systematic review. Moreover, only
English-language publications were in-
cluded. This could be problematic for two
reasons: (a) the precision of summary esti-
mates is reduced if a substantial number of
additional studies published in other lan-
guages exist; (b) bias may be introduced if
the results of studies published in English
differ systematically from those published
in other languages. However, a recent em-
pirical study found little effect of the in-
clusion/exclusion of trials published in
language other than English on combined
effect estimates in meta-analyses of RCTs.
(Egger et al. 2003). The search strategy
performed for this review identified indeed
a few studies reporting in other languages.
It is impossible to judge whether or not the
patient cohorts excluded from the present
review might have differed in terms of
survival, event rates and success.
Instead of performing a formal quality
assessment of the included studies and sen-
sitivity analysis, this review used stringent
inclusion criteria. For example, only studies
with a clinical follow-up examination were
included to avoid the potential inaccuracies
in event description in studies that based
their analysis on patient self-reports.
The studies were mainly conducted in
an institutional environment, such as uni-versity or specialized implant clinics. Five
of the studies were multicenter studies.
Therefore, the long term outcomes ob-
served here cannot be generalized to dental
service provided in private practice.
The cumulative failure rates of implant-
supporting FPDs were 5% after 5 years,
and 7.2% after 10 years, respectively. Ap-
proximately 2.5% or half of the lost im-
plants were lost prior to functional loading.
This result is in agreement with the result
from a previous systematic review (Ber-glundh et al. 2002). Clearly, a limitation
of the present review is that the assump-
tion of a constant annual event rate is not
fully met when considering the first and
the subsequent years after implantation.
Nevertheless, the results of the present
analysis should be robust as only informa-
tion of studies with a mean follow-up of 5
years or more were included.
The lower event rates in more recently
published studies are compatible with the
hypothesis of a learning curve over the
years, although a later year of publication
does not necessarily translate to later years
of implantation.
Regarding the different implant systems,
the majority of the studies reported on the
experience with the Branemark Nobel Bio-
care System that showed results below the
average of the entire review. The other
three implant systems, Astras Tech Sys-
tem, ITIs Dental Implant System and
Minimatic implants all yielded results
above the average.
The cumulative failure rate of the im-
plant supported FPDs was 4.8% after 5
years and 13.3% after 10 years. This in-
crease in the failure proportion over the
second five-year period might be explained
by the different FPD design (gold–acrylic)
in the older studies and, to some extent,
also by increased experience of the clinical
research teams.
To evaluate the influence of different
FPD designs on the failure rate the results
from studies reporting on metal ceramic
FPDs were compared with those from stu-
dies reporting on gold–acrylic FPDs. There
was a significant difference with the former
showing a cumulative failure rate of 3.4%
and the latter one 9.6% over a 5-year
period. The high failure rate of the FPDs
with a gold framework and acrylic veneers
is thought to be due to high numbers of
veneer fractures and esthetic complica-tions.
Only three studies (Ortorp & Jemt 1999;
Wennerberg & Jemt 1999; Jemt et al. 2003)
reported on success, i.e., number of pa-
tients without any complications at all
during the observation period. There is
definitely a lack of detailed, standardized
information on complications. The sum-
mary estimate of the cumulative complica-
tion rate after an observation period of
5 years was 38.7%. The complications
may be minor, such as screw or abutmentloosening, loss of access hole restorations,
loss of retention or minor acryl/ceramic
chipping, or they may be major, such
as implant fractures, fractures of the
metal framework or veneer material that
require replacement of the entire recon-
struction.
The cumulative incidence of peri-im-
plantitis and soft tissue complication was
8.6% after a follow up time of 5 years. For
the biologic complications the results must
be interpreted with caution, because of
different criteria for soft tissue complica-
tions being used in various studies.
Literature-based systematic reviews of
prognosis and survival outcomes are ham-
pered by a variety of problems (Altman
2001). The present systematic review re-
vealed several shortcomings in the previous
clinical studies. Hence, it appears appro-
priate to make the following recommenda-
tions: Long-term cohort studies on dental
implants should be prospective, have com-
plete follow-up information preferentially
Pjetursson et al . Systematic review of FPDs
634 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 11/18
with similar length of follow-up for all
patients. This means that data on well-
defined time periods should be reported
for the entire cohort, especially for the
different years after implantation. Due to
various definitions of implant success
authors should report data on implant sur-
vival in combination with incidence of
complications. The events of implant loss
should be grouped into losses that occur
prior to loading and those that take place
during function. Survival and success (free
of all complications) of the suprastructures
should be reported. Well-defined criteria
should be used for the assessment of the
biological and technical complications.
Data from clinical and radiographic assess-
ments should be described as frequency
distributions. Collaborative efforts to con-
duct a pooled individual patient data ana-
lysis of the patients and implants in thevarious studies would allow to develop and
use common definitions of complications
and to obtain a clearer picture on true long-
term survival.
Clinical assessments should include
PPD, clinical attachment level (CAL) and
BOP. Biological complications defined
by (1) the threshold level of PPD, (2)
the presence/absence of BOP/suppura-
tion assessed at any examination interval
and (3) crestal bone loss over time must
be described for implants and neighbor-ing teeth.
Technical complications should be di-
vided into (1) major: such as, implant
fracture, loss of suprastructures, (2) med-
ium: such as, abutment or abutment frac-
ture, veneer or framework fractures,
esthetic and phonetic complications and
(3) minor: such as abutment and screw
loosening, loss of retention, loss of screw
hole sealing, veneer chipping (may be po-
lished) and occlusal adjustments. The type
and number of events of technical compli-
cations per time interval as well as time/
cost required should also be reported.
In conclusion, it may be stated that
despite the high survival of implant-sup-
ported FPDs (95% after 5 years and 86.7%
after 10 years), biological and technical
complications were frequent (38.7% after
5 years). This, in turn, means that sub-
stantial amounts of chair time have to be
accepted by the patient, dental service and
society at large following the incorporation
of implant supporting FPDs.
Acknowledgements: This study has
been supported by the Clinical
Research Foundation (CRF) for the
promotion of Oral Health, University of
Berne, Switzerland. B. E. P. was an ITI
Scholar for the year 2002/2003 (ITI
Foundation grant).
Conflicts of interest : None declared.
Resume
L’objectif de cette revue systematique a ete de revoir
la survie implantaire apres cinq et dix ans de proth-
eses partielles fixees sur implants et de decrire l’in-
cidence des complications biologiques et techniques.
Une recherche Medline completee par une recherche
manuelle ont identifie des etudes prospectives et
retrospectives sur ces protheses avec un temps
moyen de suivi d’au moins cinq annees. Les patients
avaient du subir un examen clinique lors de ce suivi.
Les etudes et les releves des donneesont ete effectues
de maniere independante par deux personnes. Lestaux de complications et d’echecs ont ete analyses en
utilisantles modeles deregression Poisson aveceffets
hasard pour obtenir des estimations des proportions
de survie de cinq a dix ans. La recherche a apporte 3
844 titres et 560 resumes. L’analysedes manuscripts
complets a ete effectuee pour 176 articles resultant
en 21 etudes qui atteignaient les criteres d’inclusion.
La meta-analyse de ces etudes a indique une estima-
tion de survie de ces implants dans les groupes
combines implants-dents de 95,4% (intervalle de
confidencede 95% : 93,9 a 96,5%) apres cinqannees
et de 92,8% (90,0 a 94,8%) apres dix annees. Le taux
de survie des protheses sur implants etaient de
95,0% (92,2 a 96,8%) apres cinq annees et de 86,7
% (82,8 a 89,8%) apres dix annees. Seul 61,3% (55,3
a 66,8%) des patients n’avaient eu aucune complica-
tion apres cinq annees. La paroımplantite et les
complications des tissus mous arrivaient dans 8,6%
(5,1 a 14,1%) des cas apres cinq annees. Les compli-
cations techniques comprenaient les fractures des
implants, des complications de connexion ou bien
relies a la superstructure. L’incidence cumulative des
fractures d’implants apres cinqans etait de 0,4% (0,1
a 1,2%). Apres cinq annees, l’incidence cumulative
des complications en relation avec la connexion (vis
lache ou fracturee) etait de 7,3% et 14% des super-
structures avaient des complications (fracture de la
masse ou des veneer). Malgre la survie importante
des protheses fixees, des complications tant techni-
ques que biologiques sont frequentes. Ceci signifie
que des quantites importantes de temps au fauteuil
doivent etre acceptees par le clinicien apres l’inser-
tion d’un implant supportant une prothese fixee.
Davantage d’etudes avec un temps de recul de dix
ans ou plus sont necessaires car seul quelques etudes
ont decrits la situation a si long terme.
Zusammenfassung
Ziel: Ziel dieser systematischen Ubersicht war ei-
nerseits die Bestimmung der Uberlebenszeit von
implantat-getragenem festsitzendem Zahnersatz
(FPDs) nach 5 und 10 Jahren und andererseits die
Haufigkeit von biologischen und technischen Kom-
plikationen zu beschreiben.
Methoden: Man fuhrte eine manuell erganzte elek-
tronische Medline-Suche durch, um prospektive und
retrospektive Kohortenstudien uber FPDs mit einer
durchschnittlichen Beobachtungszeit von mindes-
tens 5 Jahren zu identifiziernen. Die Patienten
mussten bei den Nachkontrollen auch klinisch un-
tersucht worden sein. Die Aufnahme der ausgewahl-ten Studien und die Abstraktion der Daten wurde
von zwei Personen unabhangig voneinander durch-
gefuhrt. Mit Hilfe eines Possion Regressionsmodells
analysierte man die Misserfolgs- und Komplika-
tionsraten und erhielt so zusammenfassende Schatz-
werte fur die uberlebenswahrscheinlichkeit nach 5
und 10 Jahren.
Resultate: Die Suche lieferte 3844 Titel und 560
Abstracts. Die Analyse des gesamten Textes erfolgte
bei 176 Artikeln, von denen aus 21 Studien, die
Einschlusskriterien erfullten. Die Meta-Analyse
dieser Studien ergab eine geschatzte Uberlebensrate
der Implantate in gemischt zahn-implantat-getra-
genen FPDs von 95.4% (95 Prozent Zuverlassigkeit-
sintervall (95% CI): 93.9–96.5%) nach 5 Jahren und92.8% (95% CI: 90–94.8%) nach 10 Jahren. Die
Uberlebensrate der FPDs, die nur von Implantaten
getragen werden betrug 95% (95% CI: 92.2–96.8%)
nach 5 Jahren und 86.7% (95% CI: 82.8–89.8%)
nach 10 Jahren in Funktion. Nach 5 Jahren hatten
nur gerade 61.3% (95% CI: 55.3–66.8%) der
Patienten noch nie irgendwelche Komplikationen.
Nach 5 Jahren waren Periimplantitis und Weichge-
webskomplikationen bei den FPDs in 8.6% der
Falle einmal aufgetreten (95% CI: 5.1–14.1%).
Die technischen Komplikationen berucksichtigten
Implantatfrakturen sowie Probleme bei der Sekun-
darteilverbindung und den Suprastrukturen. Das
kumulative Eintreffen einer Implantatfraktur nach
5 Jahren betrug 0.4% (95% CI: 0.1–1.2%). Ebenfallsnach 5 Jahren gab es kumulativ bei 7.3% der Sekun-
darteilverbindungen Probleme (geloste oder fraktur-
ierte Schrauben) und bei 14% der Suprastrukturen
Komplikationen (Porzellan- oder Gerustfrakturen).
Zusammenfassung: Trotz einer hohen Uberlebens-
rate von FPDs sind biologische und technische
Komplikationen haufig. Dies wiederum bedeutet,
dass der Kliniker nach der Eingliederung von
implantat-getragenen FPDs mit beachtlicher Ar-
beitszeit fur Reparaturarbeiten rechnen muss. Es
sind vor allem Langzeitstudien von 10 und mehr
Jahren notig, weil bisher nur wenige Arbeiten die
Langfristfolgen beschreiben.
Resumen
Objetivos: El objetivo de esta revision sistematica
fue valorar la supervivencia de dentaduras parciales
fijas soportadas por implantes (FPDs) y describir la
incidencia de complicaciones biologicas y tecnicas.
Metodos: Se llevo a cabo una busqueda electronica
por Medline complementada con una busqueda
manual para identificar estudios cohorte prospecti-
vos y retrospectivos acerca de FPDs con un tiempo
de seguimiento medio de al menos 5 anos. Los
pacientes tenıan que haber sido examinados clınica-
mente en la visita de seguimiento. La valoracion de
Pjetursson et al . Systematic review of FPDs
635 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 12/18
los estudios encontrados y de la abstraccion de datos
se llevo a cabo independientemente por dos revi-
sores. Los ındices de fracaso y complicacion se
analizaron usando modelos de regresion de efectos
aleatorios de Poisson para obtener estimaciones de
los sumarios de las proporciones de supervivencia a
los 5 y 10 anos.
Resultados: Los resultados proporcionaron 3844 tı-
tulos y 560 resumenes. Se llevo a cabo analisis de
todo el texto para 176 artıculos resultando en 21estudios que coincidieron con los criterios de inclu-
sion. Un meta analisis de estos estudios indicaron
una supervivencia estimada de los implantes en
FPDs soportados por dientes e implantes combina-
dos del 95.4% (Intervalos de confianza del 95 por
ciento (95% DI): 93.9–96.5) tras 5 anos y 86.7%
(95% CI: 82.8–89.8%) tras 10 anos en funcion. Solo
el 61.3% (95% CI: 55.3–66.8%) de los pacientes
estuvieron libres de complicaciones tras 5 anos.
Periimplantitis y complicaciones de los tejidos blan-
dos ocurrieron en el 8.6% (95% CI 5.1–14.1%) de
los FPDs tras 5 anos Las complicaciones tecnicas
incluyeron fracturas de implantes, complicaciones
relacionadas con la conexion de la supraestructura.
La incidencia acumulada de fracturas de implantes alos 5 anos fue del 0.4% (95% CI: 0.1–1.2%). Tras 5
anos la incidencia acumulada de complicaciones
relacionadas con la conexion (aflojamiento o fractura
de tornillos) fue del 7.3% y del 14% para las
complicaciones relacionadas con las supraestruc-
turas (fracturas de las coronas o de las estructuras).
Conclusion: A pesar de una alta tasa de superviven-
cia de los FPDs, las complicaciones biologicas y
tecnicas son frecuentes. Esto, en cambio, significa
que se debe aceptar por parte de los clınicos que se
produciran una cantidades significativas de tiempo
de sillon tras la incorporacion de FPDs implantoso-
portados. Se necesitan mas estudios de seguimiento
de 10 o mas anos ya que solo unos pocos estudioshan descrito los resultados a largo plazo.
References
Adell, R., Lekholm, U., Rockler, B. & Branemark,
P.I. (1981) A 15-year study of osseointegrated
implants in the treatment of the edentulous
jaw. International Journal of Oral Surgery 10:
387–416.
Albrektsson, T., Zarb, G., Worthington, P. & Eriks-
son, A.R. (1986) The long-term efficacy of cur-
rently used dental implants. A review and
proposed criteria of success. International Journal
of Oral & Maxillofacial Implants 1: 11–25.
Altman, D.G. (2001) Systematic reviews of evalua-
tions of prognostic variables. British Medical
Journal 323: 224–8.
Andersson, B., Glauser, R., Maglione, M. & Taylor,
A. (2003) Ceramic implant abutments for short-
span FPDs: a prospective 5-year multicenter
study. International Journal of Prosthodontics 16:
640–646.
Attard, N. & Zarb, G.A. (2002) Implant prostho-
dontic management of posterior partial edentu-
lism: long-term follow-up of a prospective study.
Journal of the Canadian Dental Association 68:
118–124.
Behneke, A., Behneke, N. & d’Hoedt, B. (2000) The
longitudinal clinical effevtiveness of ITI solid
screw implants in partially edentulous patients:
a 5year follow-up report. International Journal of
Oral & Maxillofacial Implants 15: 633–645.
Berglundh, T., Persson, L. & Klinge, B. (2002) A
systematic review of the incidence of biological
and technical complications in implant dentistry
reported in prospective longitudinal studies of at
least 5 years. Journal of Clinical Periodontology
29 (Suppl. 3): 197–212.
Bragger, U., Aeschlimann, S., Burgin, W., Ham-
merle, C.H.F. & Lang, N.P. (2001) Biological
and technical complications and failures with
fixed partial dentures (FPD) on implants and teeth
after four to five years of function. Clinical Oral
Implants Research 12: 26–34.
Bragger, U., Karoussis, I. , Person, R., Pjetursson,
B.E., Salvi, G. & Lang, N.P. (2004) Technical and
biological complications and failures with single
crowns and fixed partial dentures on implant of
the ITIs Dental Implant System: a 10-year pro-
spective cohort syudy. Clinical Oral Implants
Research in press.
Buser, D., Mericske-Stern, R., Bernard, J.P., Beh-
neke, A., Behneke, N., Hirt, H.P., Belser, U.C. &
Lang, N.P. (1997) Long-term evaluation of non-
submerged ITI implants. Part 1: 8-year life table
analysis of a multi-center study with 2359
implants. Clinical Oral Implants Research 8:
161–172.
Buser, D., Weber, H.P. & Lang, N.P. (1990) Tissue
integration of non-submerged implants. 1-year
results of a prospective study with 100 ITI hol-
low-cylinder and hollow-screw implants. Clinical
Oral Implants Research 1: 33–40.
Cochran, D. (1996) Implant therapy I. Annals of
Periodontology 1: 707–790.
De Leonardis, D.D., Gark, A.K. & Pecora, G.E.
(1999) Osseointegration of rough acid-etched tita-
nium implants: 5-year follow-up of 100 mini-
matic implants. International Journal of Oral &
Maxillofacial Implants 14: 384–391.
Egger, M., Juni, P., Bartlett, C., Holenstein, F.
& Sterne, J. (2003) How important are compre-
hensive literature searches and the assessment of
trial quality in systematic reviews? Empirical
study (7 (1)). Health Technology Assessment 7:
1–76.
Egger, M., Smith, G.D. & Altman, D.G. (2001)
Systematic Reviews in Health Care: Meta-ana-
lysis in Context. London: BMJ Publishing Group.
Esposito, M., Hirsch, J., Lekholm, U. & Thomsen,
P. (1998) Biological factors contributing to failures
of osseointegrated implants I. Success criteria and
epidemiology. European Journal of Oral Sciences
106: 527–551.
Fartash, B. & Arvidson, K. (1997) Long-term eva-
luation of single crystal sapphire implants as
abutments in fixed prosthodontics. Clinical Oral
Implant Research 8: 58–67.
Fiorellini, J., Martuscelli, G. & Weber, H.P. (1998)
Longitudinal studies of implant systems. Perio-
dontology 2000 17: 125–131.
Fritz, M. (1996) Implant therapy II. Annals of
Periodontology 1: 796–815.
Gotfredsen, K. & Karlsson, U. (2001) A Prospective
5-year study of fixed partialprostheses supported
by implants with machined and TiO2-blasted
surface. Journal of Prosthodontics 10: 2–7.
Gunne, J., Astrand, P., Lindh, T., Borg, K. &
Olsson, M. (1999) Tooth–implant and implant
supported fixed partial dentures: a 10-year report.
International Journal of Prosthodontics 12:
216–221.
Hosny, M., Duyck, J., van Steenberghe, D. & Naert,
I. (2000) Within-subject comparison between con-
nected and nonconnected tooth-to-implant fixed
partial prostheses: up to 14-year follow-up study.
Pjetursson et al . Systematic review of FPDs
636 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 13/18
International Journal of Prosthodontics 13:
340–346.
Jemt, T., Bergendal, B., Arvidson, K., Bergendal, T.,
Karlsson, L.D., Linden, B., Rundcrantz, T. &
Wendelhag, I. (2003) Implant-supported welded
titanium frameworks in the edentulous maxilla:
a 5-year prospective multicenter study. Interna-
tional Journal of Prosthodontics 16: 415–421.
Karoussis, I.K., Bragger, U., Salvi, G.E., Burgin, W.
& Lang, N.P. (2003) Effect of implant design onsurvival and success rates of titanium oral im-
plants: a 10-year prospective cohort study of the
ITI Dental Implant System. Clinical Oral Im-
plants Research 15: 8–17.
Kirkwood, B.R. & Sterne, J.A.C. (2003a) Poisson
regression. In: Essential Medical Statistics,
249–262. Oxford: Blackwell Science Ltd.
Kirkwood, B.R. & Sterne, J.A.C. (2003b) Survival
analysis: displaying and comparing survival pat-
terns. In: Essential Medical Statistics, 272–286.
Oxford: Blackwell Science Ltd.
Lang, N.P., Pjetursson, B.E., Tan, K., Bragger, U.,
Egger, M. & Zwahlen, M. (2004) A systematic
review of the survival and complication rates of
fixed partial dentures (FPDs) after an observationperiod of at least 5 years II. Combined tooth–
implant supported FPDs. Clinical Oral Implants
Research doi:10.1111/j.1600-0501.2004.01118.x
Lekholm, U., Gunne, J., Henry, P., Higuchi, K.,
Linden, U., Bergstrom, C. & van Steenberghe, D.
(1999) Survival of the Branemark implant in
partially edentulous jaws: a 10-year prospective
multicenter study. International Journal of Oral
& Maxillofacial Implants 4: 639–645.
Lekholm, U., van Steenberghe, D., Herrmann, I.,
Bolender, C., Folmer, T., Gunne, J., Henry, P.,
Higuchi, K., Laney, W.R. & Linden, U. (1994)
Osseointegrated implants in the treatment of
partially edentulous jaws: a prosopective 10-year
multicenter study. International Journal of Oral
& Maxillofacial Implants 9: 627–635.Mengel, R., Schroder, T. & Flores-de-Jacoby, L.
(2001) Osseointergrated implants in patients trea-
ted for generalized chronic periodontitis and gen-
eralized aggressive periodontitis: 3- and 5-year
results of a prospective long-term study. Journal
of Periodontology 72: 977–989.
Naert, I., Koutsikakis, G., Duyck, J., Quirynen, M.,
Jacobs, R. & van Steenberghe, D. (2002a) Biologic
outcome of implant-supported restorations in the
treatment of partial edentulism. Part I: a long-
itudinal clinical evaluation. Clinical Oral Im-
plants Research 13: 381–389.
Naert, I., Koutsikakis, G., Quirynen, M., Duyck, J.,
van Steenberghe, D. & Jacobs, R. (2002b) Biologic
outcome of implant-supported restorations in thetreatment of partial edentulism. Part 2: a long-
itudinal radiographic evaluation. Clinical Oral
Implants Research 13: 390–395.
Olsson, M., Gunne, J., Astrand, P. & Borg, K. (1995)
Bridges supported by free-standing implants ver-
sus bridges supported by tooth and implant. A
five-year prospective study. Clinical Oral Im-
plants Research 6: 114–121.
Ortorp, A. & Jemt, T. (1999) Clinical experiences of
implant-supported prostheses with laser-welded
titanium frameworks in the partially edentulous
jaw: a 5-year follow-up study. Clinical Implant
Dentistry and Related Research 1:84–91.
Preiskel, H.W. & Tsolka, P. (2004) Cement- and
screw-retained implant-supported prostheses: up
to 10 years of follow-up of a new design. Interna-tional Journal of Oral & Maxillofacial Implants
19: 87–91.
van Steenberghe, D., Quirynen, M. & Naert, I.
(1999) Survival and success rates with oral en-
dosseous implants. In: Lang, N.P., Karring, T. &
Lindhe, J., eds. Proceedings of the 3rd European
Workshop on Periodontology , pp. 246–254. Ber-
lin: Quintessence.
Wennerberg, A. & Jemt, T. (1999) Complications in
partially edentulous implant patients: a 5-year
retrospective follow-up study of 133 patients sup-
plied with unilateral maxillary prosteses. Clinical
Implant Dentistry and Related Research 1: 49–56.
Wyatt, C.C.L. & Zarb, G.A. (1998) Treatment out-
comes of patients with implant-supported fixedpartial prostheses. International Journal of Oral
& Maxillofacial Implants 13: 204–211.
Zarb, J.P. & Zarb, G.A. (2002) Implant prosthodontic
management of anterior partial edentulism: long-
term follow-up of a prospective study. Journal of
the Canadian Dental Association 68: 92–96.
List of excluded full-text articles and the reason for exclusion
Adell, R. (1985) Tissue integrated prostheses in
clinical dentistry. International Dental Journal 35:
259–265.
Exclusion criteria: reporting on technique.
Ahren, S. & Kahnberg, K.-E. (2001) The adaptation
of implant-supported superstructures to the alveolar
crest: a follow-up of 49 cases. Implant Dentistry 10:
172–177.
Exclusioncriteria: no information on the reconstruc-
tions.
Albrektsson, T. (1988) A multicenter report on
osseointergrated oral implants. Journal of Prosthetic
Dentistry 60: 75–84.
Exclusion criteria: totally edentulous patients.
Albrektsson, T., Dahl, E., Enbom, I., Engevall, S.,
Engquist, B., Eriksson, A.R., Feldmann, G., Frei-
berg, N., Glantz, P.O., Kjellman, O., Kristersson,L., Kvint, S., Kondell, P.O., Palmquist, J., Werndahl,
L. & Astrand, P. (1988) Osseointegraded oral im-
plant: a Swedish multicenter study of 8139 conse-
cutively inserted Nobelpharma implants. Journal of
Periodontology 59: 287–297.
Exclusion criteria: mean follow-up time less than
5 years.
Arlin, M.L. (2002) Analysis of 435 Screw-Vent
dental implants placed in 161 patients: software
enhancement of clinical evaluation. Implant Den-
tistry 11: 58–66.
Exclusioncriteria: no information on the reconstruc-
tions.
Babbush, C.A. & Green, A.H. (1977) Implant den-
tistry: a long-term survey & comparative study with
fixed bridgework. Journal of Oral Implantology 7:
89–105.Exclusion criteria: mean follow-up time less than
5 years.
Babbush, C.A. & Shimura, M. (1993) Five-year
statistical and clinical observations with the IMZ
two-stage osteointergrated implant system. Interna-
tional Journal of Oral & Maxillofacial Implants 8:
245–253.
Exclusion criteria: mean follow-up time less than
5 years.
Bahat, O. (2000) Branemark system implants in the
posterior maxilla: clinical study of 660 implants
followed for 5 to 12 years. International Journal of
Oral & Maxillofacial Implants 15: 646–653.
Exclusion criteria: no information on the reconstruc-
tions.
Balshi, T.J. & Wolfinger, G.J. (1999) Dental im-
plants in the diabetic patient: a retrospective study.
Implant Dentistry 8: 355–359.
Exclusion criteria: no information on the reconstruc-
tions.
Bass, S.L. & Triplett, R.G. (1991) The effects of
preoperative resorption and jaw anatomy on implant
success: a report of 303 cases. Clinical Oral Im-
plants Research 2: 193–198.
Exclusion criteria: mean follow-up time less than
5 years.
Becker, W., Dahlin, C., Lekholm, U., Bergstrom,
C., van Steenberghe, D., Higuchi, B.E. & Becker, E.
(1999) Five-year evaluation of implants placed
at extraction and with dehiscences and fenestra-tion defects augmented with ePTFE membranes:
results from a prospective multicenter study.
Clinical I mplant Dentistry and Related Research
1: 27–32.
Exclusion criteria: no information on the reconstruc-
tions.
Bergendal, B. & Palmqvist, S. (1999) Laser-welded
titanium frameworks for implant supported fixed
prostheses: a 5-year report. International Journal of
Oral & Maxillofacial Implants 14: 69–71.
Exclusion criteria: totally edentulous patients.
Block, M.S., Gardinger, D., Kent, J.N., Misiek, D.J.,
Finger, I.M. & Guerra, L. (1996) Hydroxy-
apatite-coated cylindrical implants in the post-
erior mandible: 10-year observations. International
Journal of Oral & Maxillofacial Implants 11:
626–633.
Exclusion criteria: no detailed information on FPDs.
Block, M.S. & Kent, J.N. (1992) Prospective review
of integral implants. Dental Clinics of North Amer-
ica 36: 27–38.
Exclusion criteria: mean follow-up time less than
5 years.
Block, M.S. & Kent, J.N. (1994) Long-term follow-
up on hydroxylapatite-coated cylindrical dental im-
plants: a comparison between developmental and
Pjetursson et al . Systematic review of FPDs
637 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 14/18
recent periods. Journal of Oral and Maxillofacial
Surgery 52: 937–943.
Exclusion criteria: no detailed information on FPDs.
Bosker, H & van Dijk, L. (1989) The transmandi-
bular implant: a 12-year follow-up study. Journal of
Oral and Maxillofacial Surgery 47: 442–450.
Exclusion criteria: totally edentulous patients.
Brocard, D., Barthet, P., Baysse, E., Duffort, J.F., Eller,
P., Justumus, P., Marin, P., Oscaby, F., Simonet, T.,
Benque, E. & Brunel, G.A. (2000) A multicenter
report on 1,022 consecutively placed ITI implants: a
7-year longitudinal study. International Journal of
Oral & Maxillofacial Implants 15: 691–700.
Exclusion criteria: mean follow-up time less than
5 years.
Brose, M.O., Avers, R.J., Rieger, M.R. & Duck-
worth J.E. (1989) Submerged aluminia dental root
implants in humans: five-year evaluation. The Jour-
nal of Prosthetic Dentistry 61: 594–601.
Exclusion criteria: no detailed information on FPDs.
Buchmann, R., Khoury, F., Faust, C. & Lange, D.E.
(1999) Peri-implant conditions in periodontally com-promised patients following maxillary sinus augmen-
tation. Clinical Oral Implants Research 10: 103–110.
Exclusion criteria: no detailed information on FPDs.
Buchs, A.U., Hahn, J. & Vassos, D.M. (1995)
Interim clinical study report: a thereaded, hydroxyl-
apatite-coated implant – five-year post-restoration
safety and efficacy. Journal of Oral Implantology
11: 266–274.
Exclusion criteria: mean follow-up time less than
5 years.
Buchs, A.U., Hahn, J. & Vassos, D.M. (1995)
Efficacy of threaded hydroxyapatite-coted implants
placed in the anterior maxilla. Implant Dentistry 4:
272–275.Exclusion criteria: mean follow-up time less than
5 years.
Buser, D., Mericske-Stern, R., Dula, K. & Lang,
N.P. (1999) Clinical experience with one-stage non-
submerged implants. Advances in Dental Research
13: 153–161.
Exclusion criteria: no detailed information on FPDs.
Buser, D., Mericske-Stern, R., Bernard, J.P., Beh-
neke, A., Behneke N., Hirt, H.P., Belser, U.C. &
Lang, N.P. (1997) Long-term evaluation of non-
submerged ITI implants. Part 1: 8-year life table
analysis of a multi-center study with 2359 implants.
Clinical Oral Implants Research 8: 161–172.
Exclusion criteria: mean follow-up time less than
5 years.
Campelo, L.D., Camara, J.R. (2002) Flapless im-
plant surgery: a 10-year clinical retrospective analy-
sis. International Journal of Oral & Maxillofacial
Implants 17: 271–276.
Exclusioncriteria: no information on the reconstruc-
tions.
Carlson, B., Gunnar, E. & Carlsson, E. (1994)
Prosthodontic complications in osseointergrated
dental implant treatment. International Journal of
Oral & Maxillofacial Implants 9: 90–94.
Exclusion criteria: follow-up time less than 5 years.
Cavicchia, F., & Bravi, F. (1994) Free-standing vs
tooth-connected-implant-supported fixed partial re-
storation: a comparative retrospective clinical study
of the prosthetic results. International Journal of
Oral & Maxillofacial Implants 9: 711–718.
Exclusion criteria: mean follow-up time less than
5 years.
Chanavaz, M. (1996) Sinus grafting related to im-
plantology. Statistical analysis of 15 years of surgical
experience (1979–1994). Journal of Oral Implantol-
ogy 22: 119–130.
Exclusion criteria: no information on the reconstruc-
tions.
Chapman, R.J. & Grippo, W. (1996) The locking
taper attachment for implant abutments: use and
reliability. Implant Dentistry 5: 257–261.
Exclusion criteria: no detailed information on FPDs.
Cosci, F. & Cosci, B. (1997) A 7-year retrospective
study of 423 immediate implants. Compendium of
Continuing Education Dentistry 18: 940–942,
944, 946 passim.
Exclusion criteria: Mean follow-up time less than
5 years.
Cummings, J. & Arbree, N.S. (1995) Prosthodontictreatment of patients receiving implants by predoc-
toral students: five-year follow-up with the IMZ
system. The Journal of Prosthetic Dentistry 74:
56–59.
Exclusion criteria: mean follow-up time less than
5 years.
De Bruyn, H., Collaert, B., Linden, U., Johansson,
C., Albrektsson, T. (1999) Clinical outcome of
Screw Vent implants. Clinical Oral Implants
Research 10: 139–148.
Exclusion criteria: no detailed information on FPDs.
Denissen, H.W., Kalk, W., Veldhuis A.A.H. & van
den Hooff, A. (1989) Eleven-year study of hydro-
xyapatite implants. The Journal of Prosthetic Den-
tistry 61: 706–712.
Exclusion criteria: includes only single crowns and
overdentures.
Deporter, D.A., Todescan, R., Watson, P.A., Phor-
oah, M., Pillar, R.M. & Tomlinson, G. (2001) A
prospective human clinical trial of Endopore dental
implants in restoring the partially edentulous max-
illa using fixed prostheses. International Journal of
Oral & Maxillofacial Implants 16: 527–536.
Exclusion criteria: mean follow-up time less than
5 years.
Eckert, S.E., Meraw, S.J., Cal, E. & Ow, R.K. (2000)
Analysis of incidence and associated factors with
fractured implants: a retrospective study. Interna-
tional Journal of Oral & Maxillofacial Implants 15:662–667.
Exclusion criteria: no detailed information on FPDs.
Eckert, S.E. & Wollan, P.C. (1998) Retrospective
review of 1170 implants placed in partially edentu-
lous jaws. The Journal of Prosthetic Dentistry 79:
415–421.
Exclusion criteria: mean follow-up time less than
5 years.
Ellegaard, B., Baelum,V. & Karring T. (1997) Im-
plant therapy in periodontally compromised pa-
tients. Clinical Oral Implants Research 8: 180–188.
Exclusion criteria: mean follow-up time less than
5 years.
Elsubeihi, E.S. & Zarb, G.A. (2002) Implant
prosthodontics in medically challenged patients:
the University of Toronto experience. Journal of
the Canadian Dental Association 68: 103–108.
Exclusion criteria: no detailed information on FPDs.
Engel, E., Gomez-Roman, G. & Axmann-Krcmar
D. (2001) Effect of occlusal wear on bone loss and
periotest value of dental implants. International
Journal of Prosthodontics 14: 444–450.
Exclusion criteria: no detailed information on FPDs.
Ericsson, I., Lekholm, U., Branemark, P.I., Lindhe,
J., Glantz, P.O. & Nyman, S. (1986) A clinical
evaluation of fixed bridge restorations supported by
combination of teeth and osseointegrated titanium
implants. Journal of Clinical Periodontology 13:
307–312.
Exclusion criteria: mean follow-up time less than
5 years.
Evian, C.I. (1996) A comparison of hydroxyapatite-
coated micro-vent and pure titanium Swede-Vent
implants. International Journal of Oral & Maxillo-
facial Implants 11: 639–644.
Exclusion criteria: mean follow-up time less than
5 years.
Fettig, R.H. & Kay, J.F. (1994) A seven-year clinical
evaluation of soft-tissue effects of hydroxylapatite
coated vs. uncoated subperiosteal implants. Journal
of Oral Implantology 20: 42–48.
Exclusion criteria: totally edentulous patients.
Friberg, B., Nilsson, H., Olsson, M. & Palmquist, C.
(1997) Mk II: the self-tapping Branemark implant: 5-
year result of a prospective 3-center study. Clinical
Oral Implants Research 8: 279–285.
Exclusion criteria: totally edentulous patients.
Fugazzotto, P.A., Gulbranson, H.J., Wheeler, S.L. &
Lindsay, J.A. (1993) The use of IMZ osseointegrated
implants in partially and completely edentulous
patients: success and failure rates of 2,023 implantcylinders up to 60þ months in function. Interna-
tional Journal of Oral & Maxillofacial Implants 8:
617–620.
Exclusion criteria: mean follow-up time less than
5 years.
Fugazzotto, P.A., Kirsch, A., Ackermann, K.L. &
Neuendorff, G. (1999) Implant/tooth-connected re-
storations utilizing screw-fixed attachments: a sur-
vey of 3,096 sites in function for 3 to 14 years.
International Journal of Oral & Maxillofacial Im-
plants 14: 819–823.
Exclusion criteria: no detailed information on FPDs.
Fugazzotto, P.A., Wheeler, S.L. & Lindsay, J.A.
(1993) Success and failure rates of cylinder implantsin Type IV bone. Journal of Periodontology 64:
1085–1087.
Exclusion criteria: mean follow-up time less than
5 years.
Garlini, G., Bianchi, C., Chierichetti, V., Sigurta,
D., Maiorana, C. & Santoro, F. (2003) Retrospective
clinical study of osseotite implants: zero-to 5-year
results. International Journal of Oral & Maxillofa-
cial Implants 18: 589–593.
Exclusion criteria: mean follow-up time less than 5
years.
Golec, T.S. & Krauser, J.T. (1992) Long-term retro-
spective studies on hydroxyapatite-coated endosteal
Pjetursson et al . Systematic review of FPDs
638 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 15/18
and subperiosteal implants. Dental Clinics of North
America 36: 39–65.
Exclusion criteria: mean follow-up time less than
5 years.
Gomez-Roman, G., Kruppenbacher, M., Weber,
P.A. & Schulte, W. (2001) Immediate postextrac-
tion implant placement with root-analod stepped
implants: surgical procedure and statistical outcome
after 6 years.International Journal of Oral & Max-
illofacial Implants. 16: 503–513.
Exclusion criteria: mean follow-up time less than
5 years.
Goto, M., Jin-Nouchi, S., Ihara, K. & Katsuki, T.
(2002) Longitudinal follow-up of osseointegrated
implants in patients with resected jaws. Interna-
tional Journal of Oral & Maxillofacial Implants 17:
225–230.
Exclusioncriteria: no information on the reconstruc-
tions.
Gunne, J., Astrand, P., Borg, K. & Olsson, M. (1992)
Implants in partially edentulous patients. A long-
itudinal study of bridges supported by both implants
and natural teeth. Clinical Oral Implants Research3: 49–56.
Exclusion criteria: mean follow-up time less than
5 years.
Gunne, J., Jemt, T. & Linden, B. (1994) Implant
treatment in partially edentulous patients: a report
on protheses after 3 years. International Journal of
Prosthodontics 7: 143–148.
Exclusion criteria: mean follow-up time less than
5 years.
Guttenberg, S.A. (1993) Longitudinal report on
hydroxyapatite-coated implants and advanced surgical
techniques in a private practice. Compendium of
Continuing Education Dentistry 15 (Suppl.): 549–553.
Exclusion criteria: mean follow-up time less than
5 years.
Haas, R., Haimbock, W., Mailath, G. & Watzek, G.
(1996) The relationship of smoking on peri-implant
tissue: a retrospective study. The Journal of Pros-
thetic Dentistry 76: 592–596.
Exclusion criteria: no detailed information on FPDs.
Haas, R., Mensdorff-Pouilly, N., Mailath, G. &
Watzek, G. (1996) Survival of 1,920 IMZ implants
followed for up to 100 months. International Jour-
nal of Oral & Maxillofacial Implants 11: 581–588.
Exclusion criteria: mean follow-up time less than
5 years.
Hahn, J. & Vassos, D.M. (1997) Long-term efficacy
of hydroxyapatite-coated cylindrical implants. Im-
plant Dentistry 6: 111–115.
Exclusion criteria: mean follow-up time less than
5 years.
Haraldson, T. & Zarb, G. (1988) A 10-year follow-
up study of the masticatory system after treatment
with osseointergrated implant bridges. Scandina-
vian Journal of Dental Research 96: 243–252.
Exclusion criteria: totally edentulous patients.
Hardt, C.R.E., Grondahl, K., Lekholm, U. & Wenn-
stron, J.L. (2002) Outcome of implant therapy in
relation to experienced loss of periodontal bone
support: a retrospective 5-year study. Clinical Oral
Implants Research 13: 488–494.
Exclusion criteria: no information on the reconstruc-
tions.
Hellden, L., Ericson, G., Elliot, A., Fornell, J.,
Holmgren, K., Nilner, K. & Olsson, C.O. (2003) A
prospective 5-year multisenter study of the cresco
implantology concept. International Journal of
Prosthodontics16: 554–562.Exclusion criteria: no detailed information on FPDs.
Heller, A.L. & Heller, R.L. (1996) Clinical evalua-
tions of a porous-surfaced endosseous implant sys-
tem. Journal of Oral Implantology 22: 240–246.
Exclusion criteria: mean follow-up time less than
5 years.
Henry, P.J., Tollman, D.E. & Bolender, C. (1993)
The applicability of osseointegrated implants in the
treatment of partially edentulous patients: three-
year results of a prospective multicenter study.
Quintessence International 24: 123–129.
Exclusion criteria: mean follow-up time less than
5 years.
Herrmann, I., Lekholm, U. & Holm, S. (2003)
Statistical outcome of random versus selected with-
drawal of dental implants. International Journal of
Prosthodontics 16: 25–30.
Exclusion criteria: multiple publications on the
same patient cohorts.
Herrmann, I., Lekholm, U., Holm, S. & Karlsson, S.
(1999) Impact of implant interdependency when
evaluating success rates: a statistical analysis
of multicenter results. International Journal of
Prosthodontics 12: 160–166.
Exclusion criteria: multiple publications on the
same patient cohort.
Higuchi, K.W., Folmer, T. & Kultje, C. (1995)Implant survival rates in partially edentulous pa-
tients: a 3-year prospective multicenter study. Jour-
nal of Oral and Maxillofacial Surgery 53: 264–268.
Exclusion criteria: mean follow-up time less than
5 years.
Hultin, M., Fischer, J., Gustafsson, A., Kallus, T. &
Klinge, B. (2000) Factors affecting late fixture loss
and marginal bone loss around teeth and dental
implants. Clinical Implant Dentistry and Related
Research 2: 203–208.
Exclusion criteria: no information on the reconstruc-
tions.
Hultin M., Gustafsson, A. & Klinge, B. (2000)
Long-term evaluation of osseointegrated dental im-plants in the treatmentof partly edentulous patients.
Journal of Periodontology 27: 128–133.
Exclusion criteria: multiple publications on the
same patient cohort.
Hurska, A., Borelli, A., Bordanaro, A.C., Marzaduri,
E. & Hruska, K.L. (2002) Immediate loading im-
plants: a clinical report of 1301 implants. Journal of
Oral Implantology 28: 200–209.
Exclusion criteria: no detailed information on FPDs.
Hurzeler, M.B., Kirsch, A., Ackermann, K.L. &
Quinones, C.R. (1996) Reconstruction of the se-
verely resorbed maxilla with dental implants in the
augmented maxillary sinus: a 5-year clinical inves-
tigation. International Journal of Oral & Maxillo-
facial Implants 11: 466–475.
Exclusion criteria: mean follow-up lessthan 5 years.
Ivanoff, C.J., Grondahl, K., Bergstrom, C., Lekholm
U. & Branemark P.I. (2000) Influence of bicortical
or monocortical anchorage on maxillary implant
stability: a 15-year retrospective study of Branemark
implants. International Journal of Oral & Maxillo-
facial Implants 15: 103–110.
Exclusion criteria: totally edentulous patients.
Ivanoff, C.-J., Grondahl, K., Sennerby, L., Berg-
strom, C. & Lekholm, U. (1999) Influence of varia-
tions in implant diameters: a 3- to 5-year
retrospective clinical report. International Journal
of Oral & Maxillofacial Implants 14: 173–180.
Exclusion criteria: mean follow-up lessthan 5 years.
Jaffin R.A. & Berman C.L. (1991) The excessive loss
of Branemark fixtures in Type IV bone: a 5-year
analysis. Journal of Periodontology 62: 2–4.
Exclusion criteria: mean follow-up lessthan 5 years.
Jeffcoat, M.K., McGlumphy, E.A., Reddy, M.S.,
Geurs, N.C. & Proskin, H.M. (2003) A comparison
of hydroxyapatite (HA)-coated threaded, HA-coatedcylindric, and titanium threaded endosseous dental
implants. International Journal of Oral & Maxillo-
facial Implants 18: 406–410.
Exclusion criteria: totally edentulous patients.
Jemt, T. & Lekholm, U. (1993) Oral implant treat-
ment in posterior partially edentulous jaws: a 5-year
follow-up report. International Journal of Oral &
Maxillofacial Implants 8: 635–640.
Exclusion criteria: multiple publications on the
same patient cohort.
Jones, J.D., Lupori, J., Van Sickels, J.E. & Gardner,
W. (1999) A 5-year comparison of hydroxyapatite-
coated titanium plasma-spray and titanium plasma-
sprayed cylinder dental implants. Oral Surgery, OralMedicine, Oral Pathology, Oral Radiology, and
Endodontics 87: 649–52.
Exclusion criteria: no information on the reconstruc-
tions.
Kaptein, M.L.A., De Putter, C., De Lange, G.L. &
Blijdorp, P.A. (1999) A clinical evaluation of 76
implant-supported suprastructures in the composite
grafted maxilla. Journal of Oral Rehabilitation 26:
619–623.
Exclusion criteria: mean follow-up time less than
5 years.
Keller, E.E., Tolman, D. & Eckert, S. (1998) En-
dosseous implant and autogenous bone graft recon-
struction of mandibular discontinuity: a 12-year
longitudinal study of 31 patients. International
Journal of Oral & Maxillofacial Implants 13:
767–780.
Exclusion criteria: no detailed information on FPDs.
Keller, E.E., Tolman, D.E. & Eckert, S. (1999)
Surgical–prosthodontic reconstruction of advanced
maxillary bone compromise with autogenous onlay
block bone grafts and osseointegrated endosseous
implants: a 12-year study of 32 consecutive patients.
International Journal of Oral & Maxillofacial Im-
plants 14: 197–209.
Exclusion criteria: no detailed information on FPDs.
Kent, J.N., Block, M.S., Finger, I.M., Guerra, L.,
Larsen, H. & Misiek D.J. (1990) Biointergrated
Pjetursson et al . Systematic review of FPDs
639 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 16/18
hydroxylapatite-coated dental implants: 5-year clin-
ical observations. Journal of the A merican Dental
Association 121: 138–144.
Exclusion criteria: mean follow-up time less than
5 years.
Kucey, B.K.S. (1997) Implant placement in prostho-
dontic practice: a five-year retrospective study. The
Journal of Prosthetic Dentistry 77: 171–176.
Exclusion criteria: mean follow-up time less than
5 years.
Lambrecht, J.T., Filippi,A., Ratzer Kunzel, A. &
Schiel, H.J. (2003) Long-term evaluation of sub-
merged and nonsubmerged ITI solid-screw titanium
implants: a 10-year life table analysis of 468 im-
plants. International Journal of Oral & Maxillo-
facial Implants 18: 826–834.
Exclusion criteria: mean follow-up time less than
5 years.
Lazzara, R, Siddiqui, AA., Binon, P., Feldman, SA.,
Weiner R., Phillips, RM. & Genshor, A. (1996)
Retrospective multicenter analysis of 3i endosseous
dental implants placed over a five-year period. Clin-
ical Oral Implants Research 7: 73–83.Exclusion criteria: mean follow-up time less than
5 years.
Ledermann, P.D., Hassel, T.M. & Hefti, A.F. (1993)
Osseointergrated dental implants as alternative ther-
apy to bridge construction or orthodontics in young
patients: sevenyears of clinical experience. Pediatric
Dentistry 15: 327–333.
Exclusion criteria: mean follow-up time less than
5 years.
Lekholm, U., Sennerby, L., Roos, J. & Becker, W.
(1996) Soft tissue and marginal bone conditions at
osseointegrated implants that have exposed threads:
a 5-year retrospective study. International Journal of
Oral & Maxillofacial Implants 11: 599–604.Exclusion criteria: no detailed information on FPDs.
Leonhardt, A., Grondahl, K., Bergstrom, C. &
Lekhom, U. (2002) Long-term follow-up of osseoin-
tegrated titanium implants using clinical, radio-
graphic and microbiological parameters. Clinical
Oral Implants Research 13: 127–132.
Exclusion criteria: no detailed information on FPDs.
Lindh, T., Dahlgren, S., Gunnarsson, K., Josefsson,
T., Nilson, H., Wilhelmsson, P. & Gunne, J. (2001)
Tooth–implant supported fixed prostheses: a retro-
spective multicenter study. International Journal of
Prosthodontics 14: 321–328.
Exclusion criteria: mean follow-up time less than
5 years.
Lindquist, L.W., Carlsson, G.E. & Jemt T. (1997)
Association between marginal bone loss around
osseointergrated mandibular implants and smoking
habits. A 10-year follow-up study. Journal of Dental
Research 76: 1667–1674.
Exclusion criteria: totally edentulous patients.
Lorenzoni, M., Pertl, C., Polansky, R.A., Jakse, N.
& Wegscheider, W.A. (2002) Evaluation of implants
placed with barrier membranes: a retrospective fol-
low-up study to five years. Clinical Oral Implants
Research 13: 274–280.
Exclusion criteria: mean follow-up time less than
5 years.
Lozada, J.L., James, R.A. & Boskovic, M. (1993) HA-
coated implants: Warranted or not? Compendium of
Continuing Education Dentistry 15: 539–543.
Exclusion criteria: mean follow-up time less than
5 years.
McDermott, N.E., Chuang, S.K., Woo, V.V. &
Dodson, T.B. (2003) Complications of dental im-
plants: identification, frequency, and associated risk
factors.International Journal of Oral & Maxillo-
facial Implants 18: 848–855.
Exclusion criteria: mean follow-up time less than
5 years.
McGlumphy, E.A., Peterson, L.J., Larsen, P.E. &
Jeffcoat, M.K. (2003) Prospective study of 429 hy-
droxyapatite-coated cylindric omniloc implants
placed in 121 patients. International Journal of
Oral & Maxillofacial Implants 18: 82–92.
Exclusion criteria: no detailed information on FPDs.
Meriske-Stern, R., Aerni, D., Buser, D. & Geering,
A.H. (2001) Long-term evaluation of non-submerged
hollow cylinder implants: clinical and radiographic
results. Clinical Oral Implants Research 12:
252–259.Exclusion criteria: no detailed information on FPDs.
Naert, I., Duyck, J., Hosny, M., Jacobs, R., Quir-
ynen M. & van Steenberghe, D. (2001) Evaluation of
factors influencing the marginal bone stability
around implants in the treatment of partial edentu-
lism. Clinical Implant Dentistry and Related Re-
search 3: 30–38.
Exclusion criteria: no detailed information on FPDs.
Naert, I., Quirynen, M., van Steenberghe, M.D. &
Darius, P. (1992) A study of 589 consecutive im-
plants supporting complete fixed prostheses. Part II:
prosthetic aspects. The Journal of Prosthetic Den-
tistry 68: 949–956.
Exclusion criteria: totally edentulous patients.
Naert, I., Quirynen, M., van Steenberghe, D. &
Darius P. (1992) A six-year prosthodontic study of
509 consecutively inserted implants for the treat-
ment of partial edentulism. The Journal of Prosthe-
tic Dentistry 67: 236–245.
Exclusion criteria: mean follow-up time less than
5 years.
Nevins, M. & Langer B. (1993) The successful
application of osseointegrated implants to the poste-
rior jaw: a long-term retrospective study. Interna-
tional Journal of Oral & Maxillofacial Implants 8:
428–432.
Exclusion criteria: mean follow-up time less than
5 years.
Noack, N., Willer, J. & Hoffmann, J. (1999) Long-
term results after placement of dental implants:
longitudinal study of 1, 964 implants over 16 years.
International Journal of Oral & Maxillofacial Im-
plants 14: 748–755.
Exclusion criteria: no detailed information on FPDs.
Nystrom, E., Ahlqvist, J. , Legrell, P.E. & Kahnberg,
K.-E. (2002) Bone graft remodelling and implant
success rate in the treatment of the severely resorbed
maxilla: a 5-year longitudinal study. International
Journal of Oral & Maxillofacial Surgery 31: 158–164.
Exclusion criteria: no detailed information on FPDs.
O’Roark, W.L. (1997) Survival rate of dental im-
plants: an individual practitioner’s anecdotal review
of 25 years of experience. Journal of Oral Implant-
ology 23: 90–103.
Exclusion criteria: no detailed information on FPDs.
Parein, A.M., Ecker, S.E., Wollan, P.C. & Keller
E.E. (1997) Implant reconstruction in the posterior
mandible: a long-term retrospective study. The
Journal of Prosthetic Dentistry 78: 34–42.
Exclusion criteria: mean follow-up time less than
5 years.
Patrick, D., Zosky, J., Lubar, R. & Buchs, A. (1989)
A longitudinal clinical efficacy of Core-Vent dental
implants: a five-year report. Journal of Oral Im-
plantology 15: 95–103.
Exclusion criteria: mean follow-up time less than
5 years.
Piatelli, A., Sacrano, A. & Piatelli M. (1998) Histo-
logical observation on 230 retrieved dentalimplants:
8 years’ experience (1989–1996). Journal of Perio-
dontology 69:178–184.
Exclusion criteria: only reporting on failure.
Polizzi, G., Grunder, U., Goene, R., Hatano, N.,
Henry, P., Jackson, W.J., Kawamura, K., Renouard,
F., Rosenberg, R., Triplett, G., Werbitt, M. &
Linthner, B. (2000) Immediate and delayed Implant
placement into extraction sockets: a 5-year report.
Clinical Implant Dentistry and Related Research 2:
93–99.
Exclusion criteria: no information on the reconstruc-
tions.
Pylant, T., Triplett, G., Key, M.C. & Brunsvold,
M.A. (1992) Retrospective evaluation of endosseous
titanium implants in the partially edentulous pa-
tient. International Journal of Oral & Maxillofacial
Implants 7:195–202.
Exclusion criteria: mean follow-up time less than
5 years.
Quirynen, M., Naert, I., van Steenberghe, D., De-
keyser, C. & Callens, A. (1992) Periodontal aspects
of osseointegrated fixtures supporting a partial
bridge. An up to a 6-years retrospective study.
Journal of Clinical Periodontology 19: 118–126.
Exclusion criteria: mean follow-up time less than
5 years.
Quirynen, M., Peeters, W., Naert, I., Coucke, W.,
van Steenberghe, D. (2001) Peri-implant health
around screw-shaped c.p. titanium machined im-
plants in partially edentulous patients with or with-
out ongoing periodontitis. Clinical Oral Implants
Research 12: 589–594.
Exclusion criteria: no information on the reconstruc-
tions.
Raghoebar, G.M., Timmenga, N.M., Reintsema,
H., Stegenga, A.V. & Vissink, A. (2001) Maxillary
grafting for insertion of endosseous implants: results
after 12-124 months. Clinical Oral Implants Re-
search 12: 279–286.
Exclusion criteria: no detailed information on FPDs.
Rangert, B., Krogh, P.H.J., Langer, B. & van Roekel,
N. (1995) Bending overload and implant fracture: a
retrospective clinical analysis. International Journal
of Oral & Maxillofacial Implants 10: 326–334.
Exclusion criteria: only reporting on failures.
Pjetursson et al . Systematic review of FPDs
640 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 17/18
Renouard, F., Arnoux, J-P. & Sarment, D.P. (1999)
Five-mm-diameter implants without a smooth sur-
face collar: report on 98 consecutive placements.
International Journal of Oral & Maxillofacial Im-
plants 14: 101–107.
Exclusion criteria: mean follow-up time less than
5 years.
Roos, J., Sennerby, L., Lekholm, U., Jemt, T.,
Grondahl, K. & Albrektsson, T. (1997) A qualitative
and quantitative method for evaluating implant
success: a 5-year retrospective analysis of the Brane-
mark implant. International Journal of Oral &
Maxillofacial Implants 12: 504–514.
Exclusion criteria: no detailed information on FPDs.
Saadoun, A.P. & Le Gall, M.G. (1996) An 8-year
compilation of clinical results obtained with steri-
oss endosseous implants. Compendium of Continu-
ing Education Dentistry 17: 669–674.
Exclusion criteria: mean follow-up time less than
5 years.
Salonen, M.A.M., Raustia, AM., Kainulainen,V. &
Oikarinen, KS. (1997) Factors related to Periotest
values in endosseal implants: a 9-year follow-up.
Journal of Clinical Periodontology 24: 272–227.Exclusion criteria: no detailed information on FPDs.
Sbordone, L., Barone, A., Ciaglia, R.N., Ramaglia,
L. & Iacono V.J. (1999) Longitudinal study of dental
implants in periodontally compromised population.
Journal of Periodontology 70: 1322–1329.
Exclusion criteria: mean follow-up time less than
5 years.
Schliephake, H., Neukam, F.W., Schmelzeisen, R.
& Wichmann, M. (1999) Long-term results of en-
dosteal implants used for restoration of oral function
after oncologic surgery. International Journal of
Oral & Maxillofacial Surgery 28: 260–265.
Exclusion criteria: mean follow-up time less than
5 years.Schliephake, H., Neukam, F.W. & Wichmann, M.
(1997) Survival analysis of endosseous implants in
bone grafts used for the treatment of severe alveolar
ridge atrophy. Journal of Oral and Maxillofacial
Sugery 55: 1227–1233.
Exclusion criteria: no detailed information on FPDs.
Schliephake, H., Schmelzeisen, R., Husstedt, H. &
Schmidt-Wondera, L-U. (1999) Comparison of the
late results of mandibular reconstruction using non-
vascularized or vascularizedgrafts and dental implant.
Journal of Oral and Maxillofacial Surgery 57:
944–950.
Exclusion criteria: mean follow-up time less than
5 years.
Schnitman, P.A., Wohrle, P.S., Rubenstein, J.E., Da
Silva, J.D. & Wang, N-H. (1997) Ten-year results for
Branemark implants immediately loaded with fixed
prostheses at implant placement. International Jour-
nal of Oral & Maxillofacial Implants 12: 495–503.
Exclusion criteria: no detailed information on FPDs.
Schwartz-Arad, D. & Chaushu, G. (1997) Place-
ment of implants into fresh extraction sites: 4 to 7
years retrospective evaluation of 95 immediate im-
plants. Journal of Periodontology 24: 272–277.
Exclusion criteria: no detailed information on FPDs.
Sethi, A. & Kaus, T. (2000) Maxillary ridge expan-
sion with simultaneous implant placement: 5-year
results of an ongoing clinical study. International
Journal of Oral & Maxillofacial Implants 15: 491–499.
Exclusion criteria: no detailed information on FPDs.
Sethi, A., Kaus, T., Sochor, P., Axmann-Krcmar, D.
& Chenavaz, M. (2002) Evolution of the concept
of angulated abutments in implant dentistry:
14-year clinical data. Implant Dentistry 11: 41–51.
Exclusion criteria: no detailed information on FPDs.
Smithloff, M. & Fritz, M.F. (1982) The use of bladeimplants in a selected population of partially eden-
tulous adults: a ten-year report. Journal of Perio-
dontology 53: 413–418.
Exclusion criteria: no information on the reconstruc-
tions.
Smithloff, M. & Fritz, M.F. (1987) The use of blade
implants in a selected population of partially eden-
tulous adults: a 15-year report. Journal of Perio-
dontology 58: 589–593.
Exclusion criteria: no information on the reconstruc-
tions.
Snauwaert, K., Duyck, J., van Steenbergh, D., Quir-
ynen, M. & Naert, I. (2000) Time dependent failure
rate and marginal bone loss of implants supported
prostheses: a 15-year follow-up study. Clinical Oral
Investigations 4: 13–20.
Exclusion criteria: mean follow-up time less than
5 years.
Sonoyama, W., Kuboki, T., Okamoto, S., Suzuki,
H., Kanyama, M., Yatani, H. & Yamashita, A.
(2002) Quality of life assessment in patients with
implant-supported and resin bonded fixed prosthesis
for bounded edentulous spaces. Clinical Oral I m-
plants Research 13: 359–364.
Exclusion criteria: no information on the reconstruc-
tions.
van Steenberghe, D. (1989) Retrospective multicen-
ter evaluation of the survival rate of osseointegrated
fixtures supporting fixed partial prostheses in thetreatment of partial edentulism. The Journal of
Prosthetic Dentistry 61: 217–223.
Exclusion criteria: mean follow-up time less than
5 years.
van Steenberghe, D., Klinge, B., Linden U., Quir-
ynen, M., Herrmann, I. & Garpland, C. (1993)
Periodontal indices around natural and titanium
abutments: a longitudinal multicenter study. Jour-
nal of Periodontology 64: 538–541.
Exclusion criteria: mean follow-up time less than
5 years.
van Steenberghe, D., Lekholm, U., Bolender, C.,
Folmer, T., Henry, P., Herrmann, I., Higuchi, K.,
Laney, W., Linden, U. & Astrand P. (1990) Theapplicability of osseointegrated oral implants in the
rehabilitation of partial edentulism: a prospective
multicenter study on 558 implants. International
Journal of Oral & Maxillofacial Implants 5: 272–281.
Exclusion criteria: mean follow-up time less than
5 years.
van Steenberghe, D., Sullivan, D.Y. & Listrom, R.
(1989) A retrospective multicenter evaluation of the
survival rate of osseointergrated fixture supporting
bridges in the treatment of partial edentulism. The
Journal of Prosthetic Dentistry 61: 217–223.
Exclusion criteria: mean follow-up time less than
5 years.
Stultz, E.R., Lofland, R., Sendax,V.I. & Hornbuckle
C. (1993) A multicenter 5-year retrospective survi-
val analysis of 6,200 Integral implants. Compen-
dium of Continuing Education Dentistry 14:
478–486.
Exclusion criteria: mean follow-up time less than
5 years.
Teixeira, E.R., Wadamoto, M., Akagawa, Y. &
Kimoto, T. (1997) Clinical application of short
hydroxylapatite-coated dental implants to the pos-
terior mandible: a five- year survival study. The
Journal of Prosthetic Dentistry 78: 166–171.
Exclusion criteria: no detailed information on FPDs.
Ten Bruggenkate, C., Asikainen, P., Foitzik, C.,
Krekeler, G. & Sutter, F. (1998) Short (6mm) non-
submerge dental implants: results of a multicenter
clinical trial of 1 to 7 years. International Journal of
Oral & Maxillofacial Implants 13: 791–798.
Exclusion criteria: no detailed information on FPDs.
Tinsley, D., Watson, C.J., Russell, J.L. (2001) A
comparison of hydroxylapatite coated implant re-
tained fixed and removable mandibular prostheses
over 4 to 6 years. Clinical Oral Implants Research
12: 159–166.
Exclusion criteria: totally edentulous patients.
Tolman, D.E. & Laney, W.R. (1992) Tissue-
integrated prosthesis comlications. International
Journal of Oral & Maxillofacial Implants 7:
477–484.
Exclusion criteria: mean follow-up time less than
5 years.
Vehemente, V.A., Chuang, S-K., Daher, S., Muftu,
A. & Dodson, T.B. (2002) Risk factors affecting
dental implant survival. Journal of Oral Implantol-
ogy 28: 74–81.
Exclusion criteria: no detailed information on FPDs.
Visch, L.L., van Waas, M.A.J., Schmitz, P.I.M. &Levendag, P.C. (2002) A clinical evaluation of im-
plants in irradiated oral cancer patients. Journal of
Dental Research 8: 856–859.
Exclusion criteria: no information on the reconstruc-
tions.
Walton, J.N. & MacEntee, M.I. (1994) Problems
with prostheses on implants: a retrospective study.
The Journal of Prosthetic Dentistry 71: 283–288.
Exclusion criteria: mean follow-up time less than
5 years.
Weber, H.P., Crohin, C.C., & Fiorellini, J.P. (2000)
A 5-year prospective clinical and radiographic study
of non-submerged dental implants. Clinical Oral
Implants Research 11: 144–153.Exclusion criteria: no detailed information on FPDs.
Weyant, R.J. (1994) Characteristics associated with
the loss and peri-implant tissue health of endosseous
dental implants. International Journal of Oral &
Maxillofacial Implants 9: 95–102.
Exclusion criteria: no detailed information on FPDs.
Wheeler, S.L. (1996) Eight-year clinical retrospec-
tive study of titanium plasma-sprayed and hydro-
xyapatite-coated cylinder implants. International
Journal of Oral & Maxillofacial Implants 11:
340–350.
Exclusion criteria: mean follow-up time less than
5 years.
Pjetursson et al . Systematic review of FPDs
641 | Clin. Oral Impl. Res. 15, 2004 / 625–642

8/8/2019 A Systematic Review of the Survival FDP_I_Implant Supported FDP
http://slidepdf.com/reader/full/a-systematic-review-of-the-survival-fdpiimplant-supported-fdp 18/18
Willer, J., Noack, N. & Hoffmann, J. (2003) Suvival
rate of IMZ implants: a prospective 10-year
analysis. Journal of Oral and Maxillofacial Surgery
61: 691–695.
Exclusion criteria: no detailed information on FPDs.
Winkler, F., Morris, H.F. & Spray, J.R. (2001)
Stability of implants andnatural teeth as determined
by periotest over 60 months of function. Journal of
Oral Implantology 27: 198–203.
Exclusion criteria: no detailed information on FPDs.
Wyatt, C.C.L. & Zarb, G.A. (2002) Bone level
changes proximal to oral implants supporting fixed
partial prostheses. Clinical Oral Implants Research
13: 162–168.
Exclusioncriteria: no information on the reconstruc-
tions.
Yoshida, K., Takamatsu, Y., Adachi, Y., Kishi, M.,
Sekine, H.& Shigematsu,T. (1996) Functioning sur-
vival rate of fixtures and superstructures of osseoin-
tegrated implants. The Bulletin of Tokyo Dental
College 37: 55–62.
Exclusion criteria: mean follow-up time less than
5 years.
Zarb, G.A. & Schmitt, A. (1989) The longitudinal
clinical effectiveness of osseointegrated dental im-
plants: the Toronto study. Part II: the prosthetic
results. The Journal of Prosthetic Dentistry 64: 53–61.
Exclusion criteria: totally edentulous patients.
Zarb, G.A. & Schmitt, A. (1990) The longitudinal
clinical effectiveness of osseointegrated dental im-
plants: the Toronto study. Part II: problems and
complication encountered. The Journal of Prosthetic
Dentistry 64: 185–194.
Exclusion criteria: totally edentulous patients.
Zarb, G.A. & Schmitt, A. (1990) The longitudinal
clinical effectiveness of osseointegrated dental im-
plants: the Toronto study. Part III: problems and
complications encountered. The Journal of Prosthe-
tic Dentistry 64: 185–194.
Exclusion criteria: totally edentulous patients.
Zarb, G.A. & Schmitt, A. (1993) The longitudinal
clinical Effectiveness of osseointegrated dental im-
plants in posterior partially edentulous patients.
International Journal of Prosthodontics 6: 189–196.
Exclusion criteria: multiple publications on the
same patient cohort.
Zarb, G.A. & Schmitt, A. (1993) The longitud-
inal clinical effectiveness of osseointegrated
dental implants in anterior partially edentulous
patients. International Journal of Prosthodontics 6:
180–188.
Exclusion criteria: mean follow-up time less than
5 years.
Zinsli, B., Sagesser, T., Mericske, E. & Mericske-
Stern, R. (2004) Clinical evaluation of small-dia-
meter ITI implants: a prospective study. Interna-
tional Journal of Prosthodontics 19: 92–99.
Exclusion criteria: mean follow-up time less than
5 years.
Zitzman, N.U., Scharer, P. & Marinello, C.P.
(2001) Long-term results of implants treatment
with guided bone regeneration: a 5-year prospective
study. International Journal of Oral & Maxillofa-
cial Implants: 16: 355–366.
Exclusion criteria: no detailed information
on FPDs.
Pjetursson et al . Systematic review of FPDs