a study of the origin and development of lung cancer
TRANSCRIPT

Thorax (1953), 8, 1.
A STUDY OF THE ORIGIN AND DEVELOPMENTOF LUNG CANCER
BY
C. RAEBURN AND H. SPENCERFrom the Area Pathological Laboratory, Whipps Cross Hospital, London, and the Department of Pathology,
St. Thomas's Hospital Medical School, London
(RECEIVED FOR PUBLICATION JuNE 26, 1952)
During recent years increasing attention has beenpaid to the development and early stages of differentforms of malignant neoplasms. The failure of theusual forms of treatment to arrest most well-estab-lished malignant tumours focused interest on thediscovery of the earliest stages of development ofsuch neoplasms, as it is only in the earliest phasesthat present methods of treatment offer any hopeof effectual treatment. The study of the changesthat lead on to established malignant tumourformation also provides possible clues to aetiologicalfactors in some sites, and also enables some of thefundamental changes resulting in malignant tumourformation to be observed. It was with these objectsin view that the present investigation was undertaken.The terms "lung cancer" and "bronchial
carcinoma" have been used synonymously, and ithas been customary to consider that most lungcancers arise in the major bronchi near the hila ofthe lungs (Willis, 1948). Except for a few reportedcases of small, peripherally situated tumours (Grayand Cordonnier, 1929; Stewart and Allison, 1943;James and Pagel, 1944; Petersen, Hunter, andSneeden, 1949; Spain and Parsonnet, 1951; Priorand Jones, 1952) arnd one describing two minutegrowths in main bronchi (Aufses and Neuhof, 1952),very little attempt has been made to trace the originof this very common tumour by looking for theearliest stages in its development. Because thelarger bronchi are so frequently involved in thelater spread of the disease it is usually assumed thatmost growths started in the main bronchi. Thatthe epithelium and glands of the larger bronchi canand undoubtedly do provide the site of origin ofprimary carcinomata is certain, but the far greatersurface area of epithelium provided by the peripheralbronchi and bronchiolar trees might well be expectedto provide the site of origin for many more primarygrowths. Furthermore, the trachea and largebronchi undergo much of their development anddifferentiation in utero while the peripheral bronchiand bronchioles continue to develop during the
A
first eight years of extra-uterine existence. Thusthe peripheral air passages are the last parts of theair passages normally exposed to physiologicaldevelopmental stimuli (Geschickter and Denison,1934).In view of the great frequency with which car-
cinoma of the lung is encountered at routinepost-mortem examinations it might reasonably beexpected that from time to time an unsuspectedand early growth would be found somewhere in thelungs. Both of us for some years past have beenin the habit of exploring the main bronchi and theirimmediate branches at all'post-mortem examina-tions in the hope that such an early growth wouldbe discovered. So far only one such small car-cinoma has been found in 750 adult post-mortemexaminations.The absence of such growths in the larger air
passages prompted one of us to start sectioning thewhole of both lungs with great care, and all sus-picious nodules, particularly scars, were removedand sectioned as a routine. The results in the first400 necropsies (Raeburn, 1951) yielded four smallunsuspected carcinomata arising in the periphery ofthe lungs, mainly in association with scars. Sincethen our combined results of extensive searching inlungs obtained at routine post-mortem examinations,excluding infants, has revealed in a short period ofa year a further six cases, including the one in thelarge bronchus mentioned above, which, whencombined with three cases of small growths removedsurgically, has provided 13 specimens of small andearly growths (Cases 1-13), in which the mode andsite of origin of the neoplastic process could bedetermined with reasonable accuracy.
In addition to the above tumours a further twocases (Cases 14 and 15) have been added. These,though very considerably larger, had arisen in sitesother than main bronchi and appeared to have beenintimately related to pre-existing chronic inflamma-tory lesions in the lung.

C. RAEBURN and H. SPENCER
The following is a brief description of the 15 casesforming the series.
SUMMARIES OF 15 CASESCASE 1.-A man aged 68 died from renal failure due
to bilateral hydronephrosis. A second primary papillaryand transitional-celled bladder carcinoma had invadedand blocked both ureters. In addition there were
considerable enslight roughenirthe mucous meseparate noduldistance of 1.3CASE 2.-A v
pulmonary tub(and a small nc
We o' o 8 M;~~Mk~~~~~~
~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ 4. 1 t
AA
e
~~~4 4 4*i'j,,,
41~~ ~ ~ ~ ~ ~ ~
>:*we*v , ¢R #W~ ~ J* I
JJ-i ;t
X.,rt%X½A;,,,,,,S,,, 2,
FIG. 1.-Case 1 section of the upper lobar bronchus showing an intra-epithelialcarcinoma arising in respiratory epithelium still covered with ciliated epithelium(x 140)
lo]
A#t,t,~~~~~~~~F.,*-+ wP,, S~~~~~~~~~~~~~~~e4 #r ?' ;. }*geS
HP ,~~~~~~~~~~fo
ca
W]
4 in
w?'%J'-'*R''t'r**.*it mlu
; ;.z>**4srW9fJ'w<Sk n
1L
* ~ ~ ~~~i .&#, .*5
ei
FIG. 2.-Case 2: section of the main left upper lobar bronchus showing an intra- tiepithelial carcinoma arising in metaplastic squamous bronchial epithelium.The appearances very closely resemble Bowen's skin cancer (x 140). e.
nphysematous changes in both lungs andng of the main right upper lobe bronchus,embrane of which was raised by several[es up to 2.0 mm. in diameter over acm. (Fig. 1).voman aged 62 was known to have active,erculosis. Bronchoscopy was performedAdular swelling approximately 3 mm. in
diameter was seen in the mucousmembrane of the orifice of the mainleft upper lobe bronchus. The noduleand a strip of mucous membrane wereremoved. No obstruction of thebronchus was seen and all the visiblegrowth was removed (Fig. 2).CASE 3.-A man aged 58 gave a
history of a chronic cough dating back25 years and recent slight haemoptysis.Bronchoscopy showed a raised nodu-lar growth in the right lower lobemain bronchus extending approxi-mately 1.3 cm. The growth wasremoved surgically together with fourhilar glands, two of which appeared tocontain growth. Section showed asquamous-celled carcinoma startingas an intra-epithelial cancer.
CASE 4.-A woman aged 50 hadcomplained of slight haemoptysis.Bronchoscopy revealed a few smallnodules, none of which exceeded 3mm. in diameter, in the mucous mem-brane of the right upper lobe mainbronchus. One was excised for histo-
gical examination and showed an intra-?ithelial carcinoma.CASE 5.-A woman aged 64 died ofneral peritonitis after a total gastrectomyr a columnar-celled adenocarcinoma.ost-mortem examination revealed an old,avitated, fibrous scar 1.5 cm. in diameter,rhich was considered to be tuberculousnature, occupying the apex of the right
ng. No growth was suspected on
aked-eye examination and it was onlyzund on microscopical examination (Figs.and 4).CASE 6.-A woman aged 68 died of a
iassive pulmonary embolism. Post-nortem examination showed a greyish.vedge-shaped scar beneath the pleura ofhe middle lobe of the right lung 0.3-m. in diameter. Fig. 5 shows the micro-copical appearance of the growth, whosexistence had not been suspected previously.CASE 7.-A man aged 81 died from con-
luent bronchopneumonia. The apex ofhe left lung was fibrosed, and only whenxamined microscopically was a small oat-
2

THE ORIGIN AND DEVELOPMENT OF LUNVG CANCER
and round-celled carcinoma ediscovered.
CASE 8.-A man aged 73died from myocardial infarc-tion. He was also found tohave syphilitic aortitis and achronic gastric ulcer. l heapex of the left lung wasscarred. Only following micro-scopical examination was a "'',very early carcinoma of a 'polygonal- and squamoid- 1 Icelled type (Fig. 6) discovered.
CASE 9.-A man aged 59 t *died from generalized purulent -bronchitis and emphysema. iEPost-mortem examination re- - Svealed a soft, greyish-whitenodule 1.2 cm. in diametersurrounding blood vessels inthe upper lobe of the leftlung. The nodule was closebeneath the pleura in the FIG 3--Case5 a low powparavertebral part of the lobe. arising in an apical scar.A solitary metastasis was foundin the left fifth rib. Microscopical exami- ,nation revealed a mixed polygonal and ,V!scluamous-celled growth arising in a pre- - $existing scar (Fig. 7). 1,
CASE 10.-A man of 76 died from confluent d- ibronchopneumonia. There was a patch ofpleural thickening on the surface of theright lower lobe 3 cm. in extent and '"4extending 0.6 cm. into the subjacent lung. ;q .Microscopical examination revealed old scartissue, reparative changes, and a polygonal- 4 'celled carcinoma developing in some places.
CASE 11.-A man aged 72 died from 'rheumatic mitral stenosis and heart failure.A small greyish-white nodule 1.5 cm. in dia-meter was found in the upper part of the 49>4lower lobe of the right lung. There was Ysome scarring in the vicinity and an oldcalcified and caseous tuberculous focus in >*Athe apex of the right lung. Microscopicalexamination showed an adenocarcinoma ' 4Zarising in the edges of an old fibro-
;W
anthracotic scar. FIG. 4.-(noma
CASE 12.-A woman of 69 died of coronary of theartery occlusion. A greyish nodule, 0.2 cm. tumouin diameter 2 cm. beneath the pleurawas found in the lower lobe of the left lung.Microscopically it proved to be an oat- and round-celled carcinoma with evidence of surrounding fibrosisdue to previous damage of a lung.CASE 13.-A man aged 64 died from a paraplegia
complicated by acute pyelonephritis. Post-mortemexamination showed that the upper lobe of the left lungwas adherent to the chest wall over a circular area ofapproximately 2 cm. Beneath the fibrous adhesions
fer view of the entire oat- and round-celled carcinoma found by accidentThe growth was only detected by microscopical examination ( x 42).
-ED lr" ,,,",.' '.9-~ ~ ~ I--.' '9
Case 5: a high-power view of the minute round- and oat-celled carci-.seen in Fig. 3. The spindle shape, hyperchromatism, and arrangemente cells differentiate this type of growth from a benign adenomatousur ( x 140).
there was an indurated superficial scar in the lung, anddeep to this was a greyish-white nodule 1 cm. in diameter.The superficial scar and the deeper nodule togetherresembled a collar stud in shape. There was secondarygrowth in the lymph glands lying immediately externalto the main lobar bronchus, and in a further glandbehind the left clavicle. Examination of the spinalcord showed an area of softening at the level ofD3-4, but no secondary growth to account for this
3

C. RAEBURN and H. SPENCER
:\ *t='> # *'f> ;
jo
<*8v~~ ~ ~9,.ts t\8
I~~I
,*-;~~~-.Ni'- J
*'-J*eF.R*Ai '
JU~~~~~~*2.O2
FIG. 5.-Case 6: A, a further example of a very small oat- and round( x 140); B shows the same growth within a lympha
was found in the cord. Microscopical examinationshowed an anaplastic predominantly round- and oat-celled carcinoma which had almost certainly arisen inconnexion with the subpleural scar, and which hadspread along the perivascular and peribronchial lym-phatic to the central regional glands. From theseglands, retrograde lymphatic spread into the submucousplexus of the lymphatic spaces of the upper lobe mainbronchus had occurred, but there was no break of thesurface mucosa that could be identified.CASE 14.-A man aged 49 was found to have a shadow
in the upper lobe of the right lung following mass
radiological examination. He had no symptoms referableto the growth. The right lung was removed, and therewas a deep puckered scar on the interlobar surface ofthe upper lobe. The middle lobe was adherent at thispoint. On cutting the lung there was a dense anthracoticscar extending inwards from the pleural surface sur-
rounded by translucent growth approximately 2.5 cm.
in diameter. On microscopical examination it was foundto be a mucus-secreting carcinoma arising in and aboutan old fibro-anthracotic lung scar. There was growthin one hilar gland with no detectable intermediatelysituated deposits.CASE 15.-A man aged 50 complained of increasing
dyspnoea, loss of weight, and a chronic cough. Ashadow suggestive of a growth was seen in the lowerlobe of the right lung. The right lung was removed,and on the posterior part of the lower lobe 5 cm. abovethe diaphragm there was a dense scar extending into thelung from the pleural surface, the whole 3 cm. in depth.The centre of this area was dark grey, the periphery
pale and more translucent.Microscopical examinationshowed a polygonal-celledcarcinoma arising in andabout a chronic fibro-anthracotic scar.
-#xtw Histological examina-tion of the four growths
Oi ^ s * F found arising in the mainlobar bronchi (Cases1-4) showed that in
'#;:i3aevery case they were
squamous-celled carci-AA* Al* nomata, and all four
cases appeared to havestarted as intra-epithelial cancer ana-Iogous to Bowen's intra-epithelial skin cancer.The bronchial epitheliumin some of the cases hadundergone metaplasticsquamous-celled changein sharply defined zones,
l-celled carcinoma arising in a scar and in these areas theLtiCvessel (x 280).
epithelial cells were
hyperplastic, hyperchromatic, and some of thecells had enlarged, resembling the cells seen inPaget's disease of the breast, a condition probablyanalogous to that under discussion (Figs. 1 and 2).The ducts of the mucous glands had undergonesquamous metaplastic change as in an intra-epithelial ecto-cervical uterine cancer. The changesdescribed above were multifocal, and it appeared asthough a whole field of cells had undergone malig-nant change simultaneously. So far no otherhistological variety of lung cancer has been incon-trovertibly proved to have arisen in a main bronchus.In the many other cases which we have examined,and where the larger bronchi were involved ingrowth, the appearances might equally well havebeen explained on a basis of secondary spread.
Although the aetiological factors concerned inmost forms of human malignant disease are stillunknown, the association of chronic irritation andinflammation as a precursor condition of carcino-matous growths in several situations is a well-established fact, and has been suggested as a causefor lung cancer (Wolf, 1895; Weller, 1929). Thefinding of unusual areas of hyperplasia and evenmalignant tumours associated with damage andfibrosis in the lungs might therefore be expected.The investigation was also undertaken to deter-
mine whether there was any relationship betweenchronic inflammation in the lung and the subsequent
.4
I

THE ORIGIN AND DEVELOPMENT OF LUNG CANCER
A B C
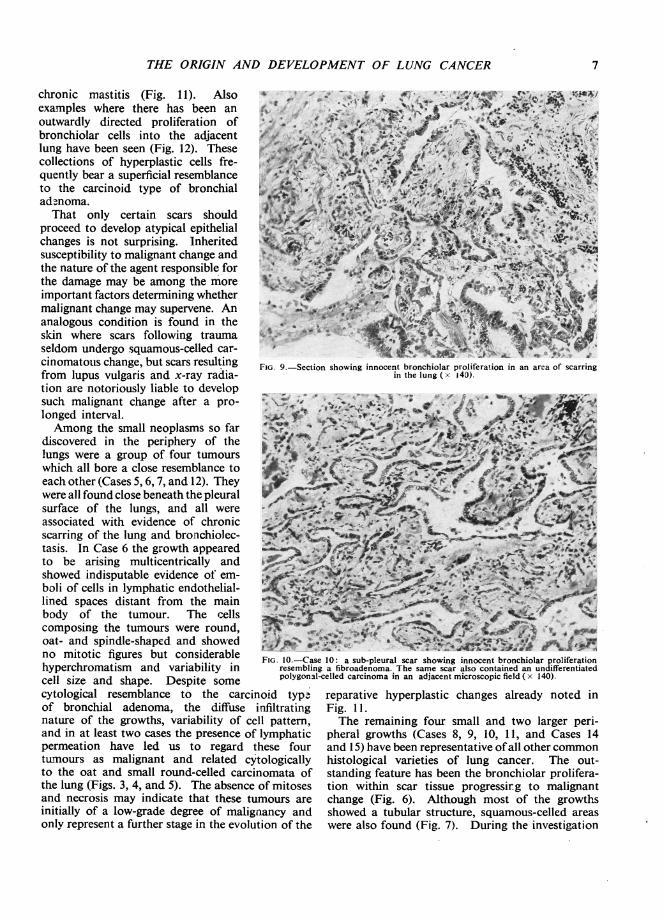
FIG. 6.-Case 8: a composite photomicrograph of a scar cancer in the lung; A, normal bronchiolar proliferationat the edge of a small scar; B slightly deeper in the scar showing solid atypical bronchiolar outgrowths;C still deeper in the scar showing a polygonal-celled carcinoma (all x 140).
A B
FIG. 7.-Case 9: A, bronchioles invading a lung scar (one of the bronchioles shows carcinomatouschange); B, an adjacent microscopic field showing an area of squamoid carcinoma. An exampleof a scar cancer producing different histological varieties of growth in the same tumour ( x 140).
5
C. RAEBURN and H. SPENCER
development of malignant change. As stated above,all scarred areas have been removed from bothlungs at post-mortem examinations, includingobvious tuberculous fibrocaseous and calcifiednodules. Particular attention has lately been paidto lung tissue adjacent to scarred hilar lymph glands.Such material removed from 750 necropsies hasenabled us to study the process of repair in a largenumber of scars in damaged lung, and has producedatypical areas of regenerative hyperplasia which weconsider may be pre-cancerous, as well as 10 actualsmall or microscopical carcinomata.The reaction of lung tissue to injury may be
conveniently divided into the changes which occurin main bronchi and the changes which occur whenbronchioles and alveoli are damaged. Macroscopicevidence of scarring in the larger bronchi is uncom-mon, and if the damage to the bronchial wall hasinvolved the basement germinal layer of cells itfrequently leads to destruction of the whole thicknessof the bronchial wall. This is well demonstratedin suppurative bronchiectasis, where the bronchialwall may be destroyed and the surrounding lungbecomes implicated in the destructive process. Thewall of the resulting cavity is lined by fibrous tissueand may eventually become covered by squamousepithelium.
Lesser degrees of damage to the main bronchi,provided the basement layer of epithelial cellsremains intact, is repaired by simple regenerationfrom the germinal layer of cells. The resulting
..
9
~~~ ~ ~ ~ ~ ~ ~ ~ ~ 7
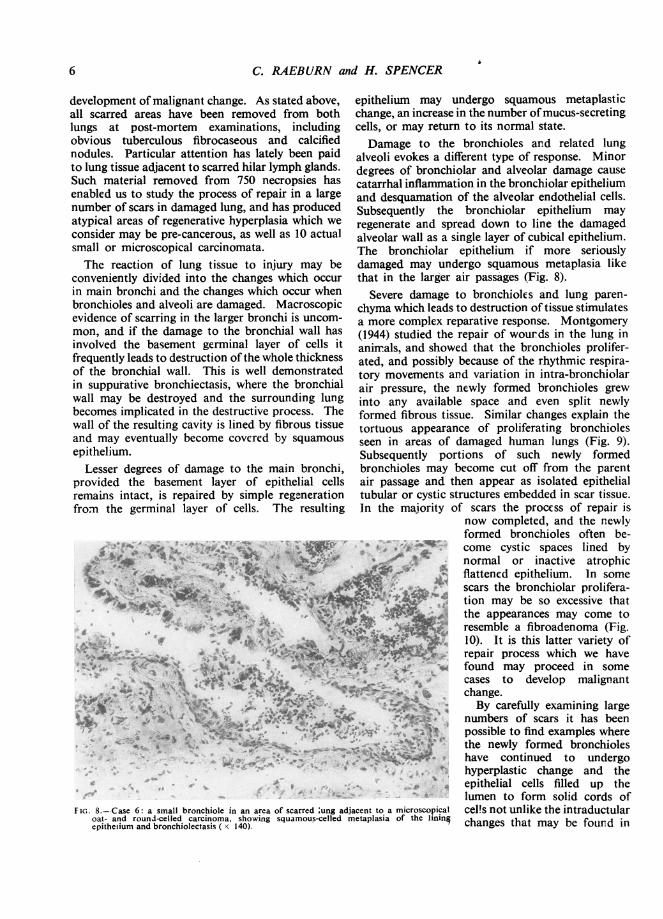
Fi.. 8.--Case 6: a small bronchiole in an area of scarred :ung adjacent to a microscopicaloat- and round-celled carcinoma, showing squamous-celled metaplasia of the liningepitheiium and bronchiolectasis ( x 140).
epithelium may undergo squamous metaplasticchange, an increase in the number ofmucus-secretingcells, or may return to its normal state.Damage to the bronchioles and related lung
alveoli evokes a different type of response. Minordegrees of bronchiolar and alveolar damage causecatarrhal inflammation in the bronchiolar epitheliumand desquamation of the alveolar endothelial cells.Subsequently the bronchiolar epithelium mayregenerate and spread down to line the damagedalveolar wall as a single layer of cubical epithelium.The bronchiolar epithelium if more seriouslydamaged may undergo squamous metaplasia likethat in the larger air passages (Fig. 8).
Severe damage to bronchioles and lung paren-chyma which leads to destruction of tissue stimulatesa more complex reparative response. Montgomery(1944) studied the repair of wounds in the lung inanimrals, and showed that the bronchioles prolifer-ated, and possibly because of the rhythmic respira-tory movements and variation in intra-bronchiolarair pressure, the newly formed bronchioles grewinto any available space and even split newlyformed fibrous tissue. Similar changes explain thetortuous appearance of proliferating bronchiolesseen in areas of damaged human lungs (Fig. 9).Subsequently portions of such newly formedbronchioles may become cut off from the parentair passage and then appear as isolated epithelialtubular or cystic structures embedded in scar tissue.In the majority of scars the proecss of repair is
now completed, and the newlyformed bronchioles often be-come cystic spaces lined bynormal or inactive atrophicflattened epithelium. In somescars the bronchiolar prolifera-tion may be so excessive thatthe appearances may come toresemble a fibroadenoma (Fig.10). It is this latter variety ofrepair process which we havefound may proceed in somecases to develop malignantchange.By carefully examining large
numbers of scars it has beenpossible to find examples wherethe newly formed bronchioleshave continued to undergohyperplastic change and theepithelial cells filled up thelumen to form solid cords ofcel!s not unlike the intraductularchanges that may be found in
6
MkVV.t
AO.
4".M..e,
..J
THE ORIGIN AND DEVELOPMENT OF LUNG CANCER
chronic mastitis (Fig. 11). Alsoexamples where there has been an 4outwardly directed proliferation ofbronchiolar cells into the adjacentlung have been seen (Fig. 12). Thesecollections of hyperplastic cells fre- ' "quently bear a superficial resemblance ' *to the carcinoid type of bronchial .ad-noma. fThat only certain scars should
proceed to develop atypical epithelial 'cfchanges is not surprising. Inherited %susceptibility to malignant change andthe nature of the agent responsible forthe damage may be among the moreimportant factors determining whether 4malignant change may supervene. Ananalogous condition is found in theskin where scars following trauma '. :eseldom undergo squamous-celled car-cinomatous change, but scars resulting FIG. 9.-Secti(from lupus vulgaris and x-ray radia-tion are notoriously liable to developsuch malignant change after a pro- .41longed interval.Among the small neoplasms so far s% .
discovered in the periphery of thelungs were a group of four tumourswhich all bore a close resemblance toeach other (Cases 5, 6, 7, and 12). Theywere all found close beneath the pleuralsurface of the lungs, and all wereassociated with evidence of chronic * ^scarring of the lung and bronchiolec- tNOtasis. In Case 6 the growth appearedto be arising multicentrically and tshowed indisputable evidence of em-boli of cells in lymphatic endothelial-lined spaces distant from the main :'% ,body of the tumour. The cellscomposing the tumours were round, ;oat- and spindle-shaped and showed j %,5no mitotic figures but considerable FIG. 1hyperchromatism and variability in resemblincell size and shape. Despite some polygonalcytological resemblance to the carcinoid typeof bronchial adenoma, the diffuse infiltratingnature of the growths, variability of cell pattern,and in at least two cases the presence of lymphaticpermeation have led us to regard these fourtumours as malignant and related cytologicallyto the oat and small round-celled carcinomata ofthe lung (Figs. 3, 4, and 5). The absence of mitosesand necrosis may indicate that these tumours areinitially of a low-grade degree of malignancy andonly represent a further stage in the evolution of the
p , 4> 4','
*-. ..4b
* -s.
.M 4b"
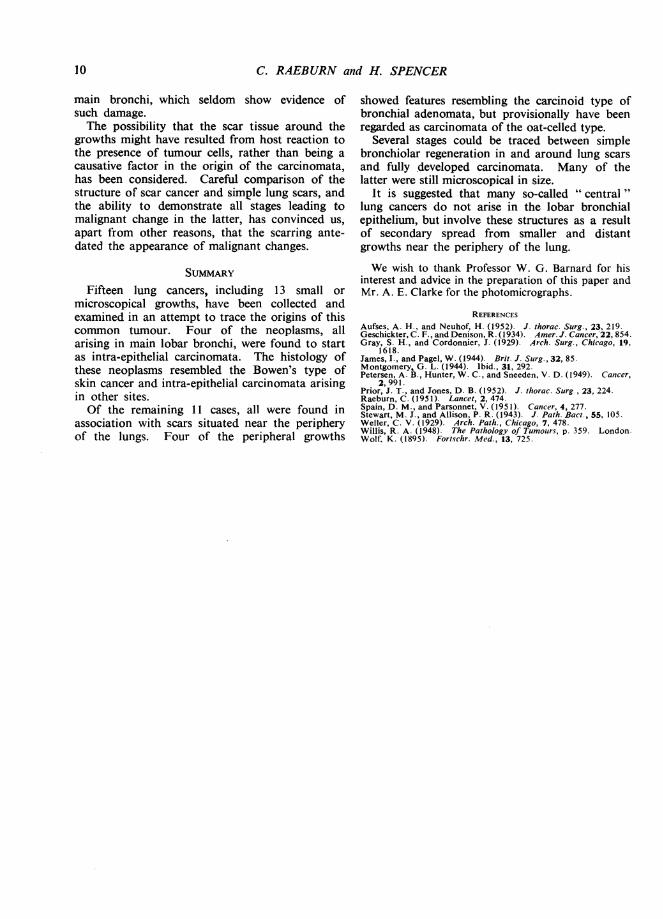
"x% fiW7* -: _ # .4- s J-ion showing innocent bronchiolar proliferation in an area of scarring
in the lung ( x j40).
4 e-. *
_ vty- -..fbIj
p~~~~~~i
W.,AAi;4
se 10: a sub-pleural scar showing innocent bronchiolar proliferationrig a fibroadenoma. The same scar also contained an undifferentiated1Lcelled carcinoma in an adjacent microscopic field ( x 140).
reparative hyperplastic changes already noted inFig. 1 1.The remaining four small and two larger peri-
pheral growths (Cases 8, 9, 10, 11, and Cases 14and 15) have been representative ofall other commonhistological varieties of lung cancer. The out-standing feature has been the bronchiolar prolifera-tion within scar tissue progressir.g to malignantchange (Fig. 6). Although most of the growthsshowed a tubular structure, squamous-celled areaswere also found (Fig. 7). During the investigation
7

C. RAEBURN and H. SPENCER
Aw.
A'~~~A
%61k
.i >~~~~~~~~~~i
.:"o
..
V...
2.i." .m.:
4 .,
;*
V., :%
llWs .. .
46(*.}
eS & 'S
t
%. .4, a
*0,*.
FIG. 11.-Bronchiolar proliferation in a scar in lung. The bronchiolar epithelium isforming solid nests of cells. The change was localized and was due toinnocent regenerative hyperplasia ( x 280).
true malignant change. Only caseswhich have shown obvious malignantchange have been included in thisseries. Unfortunately, post-mortemexaminations on patients dying fromestablished lung cancer rarely affordmuch useful information, as the sizeof the growths precludes any attemptto determine their point of origin.The rapidity with which many lung
carcinomata metastasize and the occa-sional difficulty which a pathologistmay experience in finding the site of asmall primary growth are two featuresof the condition, both of which arewell recognized. One of the minutescar cancers included in this series(Case 9), a mixed squamous-celledand adenocarcinon'a (Fig. 7), hadalready metastasized to a rib withoutany evidence of distant lymphaticpermeation, and Case 13 showedwidespread lymphatic permeationwhich had reached the hilar lymphglands and the lymphatic channels inthe lobar bronchial wall.A further growth, while still fairly
small and confined to the periphery ofthe lung, had already spread by thelymphatic channels to a central hilargland which was adherent to theouter wall of the main upper lobebronchus (Case 14). The possibilityof further spread of growth from sucha central lymph gland into the wallof the adjacent main lobar bronchuscould lead to the mistaken impressionthat the growth had originated in thelaige bronchus.
DIscussIoN*Koe.^+->-.v * i F <S -t,Hitherto it has been customary tok.i>-D'regard most lung carcinomata as
> b ~ /orto; ; l having arisen from main bronchi%$-:-*a# Ji i............ S and their immediate divisions, largely*-->xt-< B because the main bronchi so fre-
quently become involved in a mass
of growth. Although main bronchiFIG. 12.-A localized area of bronchiolar epithelial hyperplasia in a sub-pleural
scar, but showing no evidence of true malignant change (x 140). undoubtedly can be the seat of
origin of primary lung carcinomata,
many lung scars have been found which have shown where we have been able to procure veryall degrees of bronchiolar proliferation, many re- small early growths before spread has occurredsembling fibroadenomata, and great difficulty has the growths have in every case been of thebeen experienced in determining the borderline intra-epithelial variety analogous to Bowen'sbetween innocent reparative proliferation and disease of the skin, intra-epithelial cancer of the
fi=-.Au
k . % ''s'#*
8
:
,

THE ORIGIN AND DEVELOPMENT OF LUNG CANCER
cervix uteri and oesophagus, ard Paget's intra-epithelial cancer of the breast. Such carcinomataundoubtedly can metastasize and then usuallybehave as a fairly rapidly spreading variety ofsquamous-celled carcinoma. Apart from this typeof growth, which starts ab initio as multiple areasof epithelial hyperplasia, all the other small growthswhich have been obtained from lungs show unmis-takable evidence of having arisen in and aboutdamaged lung tissue. In these cases the wholeprocess leading up to malignant tumour formationappears to pursue a different course from thosearising in the main bronchi. To appreciate thechanges it is necessary to study the response ofbronchiolar and alveolar tissue to damage. Thebronchioles appear to play an important part in thehealing process both by downgrowth of bronchiolarepithelium to line the partly damaged alveolar wallsand by the formation of new bronchioles resemblingthe formation of new bile ducts following damageto the liver.
In most cases in which lung is damaged thebronchiolar changes described above take place, butafter an initial period of hyperplasia the newlyformed epithelium becomes flattened and atrophicand all evidence of active growth ceases. In a fewcases, however, possibly over a long period, regenera-tive hyperplasia continues and results in atypicalareas of epithelial proliferation. The bronchiolarepithelium becomes heaped up both within thelumen of damaged alveoli and new bronchioles,and the resulting condition resembles an innocenttumour. The border-line between innocency andmalignancy, as in so many other situations, is veryindeterminate, and other cases show unmistakablefeatures of being true carcinomata.Among the group of peripherally arising tumours,
four showed a very close resemblance to each otherand to other similar tumours recently reviewed byPrior and Jones (1952). Although for the reasonsalready stated, namely local infiltration, lymphaticpermeation, and cytological structure, we haveincluded these growths as early carcinomata andnot among the adenomata, our cases in commonwith other similar cases previously reported in theliterature show certain unusual features. Of the19 cases collected by the authors we have cited,14 occurred in women and only five in men, areversal of the usual sex incidence found in lungcancer. This unusual sex incidence has been foundalso in our four cases, with three female and onemale case. The sub-pleural localization, and theassociation of these tumours with lung fibrosis andbronchiolectasis also noted by the same authors,was also common to our four cases. As in the case
reported by Gray and Cordonnier, one of ourtumours (Case 6) was multicentric in its points oforigin. Unfortunately the future course of thepatients found harbouring these growths wasimpossible to assess, although the patient who wasreported by Stewart and Allison in 1943 as showinga similar tumoar in a brochiectatic lung hasremained alive and well.
Future study of this distinctive group of tumoursmay show that in fact they belong to a group ofrelatively benign adenomatous tumours or hyper-plasias and should not be included among themalignant lung tumours.Of the remaining seven undoubted peripherally
situated scar cancers, all were found in males andthree were almost entirely of an adenocarcinomatouspattern. This conforms to the almost universalfinding of male preponderance in true lung cancerand to the observed greater frequency of origin ofadenocarcinomata in the periphery of the lung.The growth found in Case 8 and shown in Fig. 7is very similar to that in the two cases describedby James and Pagel (1944), and the description oftheir cases leaves little doubt that their two caseswere but further examples of malignant changesupervening in lung scar tissue at the apices oflungs.
This latter group of tumours showed localinfiltration, lymphatic permeation, and even blood-borne metastases at a very early stage in theirdevelopment.The relationship of previous lung damage to
primary malignant disease of the lung has beennoted before, but the present tendency is to regardmost lung tumours as having arisen from the lobarbronchial epithelium or glands. From our experi-ence it would appear possible that some growthsstart in the lung substance from bronchiolar tissuein areas of chronic fibrosis and thence spread to theregional hilar glands. From the regional hilarglands subsequent backspread into the lymphaticchannels in the adjacent lobar bronchial wall maythen occur.The almost universal finding of at least one or
two scarred areas in the lung substance at post-mortem examination contrasts with the rarity ofnaked-eye and even microscopical evidence ofchronic damage to the main bronchi and theirsurface epithelium. This fact, combined with theknown tendency in many situations for chronicinflammation and fibrosis to precede malignantchange, agrees more closely with our observedfindings of malignant growths and atypical areasof epithelial hyperplasia arising in fibrotic andchronically inflamed lung tissue rather than in the
9
C. RAEBURN and H. SPENCER
main bronchi, which seldom show evidence ofsuch damage.The possibility that the scar tissue around the
growths might have resulted from host reaction tothe presence of tumour cells, rather than being acausative factor in the origin of the carcinomata,has been considered. Careful comparison of thestructure of scar cancer and simple lung scars, andthe ability to demonstrate all stages leading tomalignant change in the latter, has convinced us,apart from other reasons, that the scarring ante-dated the appearance of malignant changes.
SUMMARYFifteen lung cancers, including 13 small or
microscopical growths, have been collected andexamined in an attempt to trace the origins of thiscommon tumour. Four of the neoplasms, allarising in main lobar bronchi, were found to startas intra-epithelial carcinomata. The histology ofthese neoplasms resembled the Bowen's type ofskin cancer and intra-epithelial carcinomata arisingin other sites.Of the remaining 11 cases, all were found in
association with scars situated near the peripheryof the lungs. Four of the peripheral growths
showed features resembling the carcinoid type ofbronchial adenomata, but provisionally have beenregarded as carcinomata of the oat-celled type.
Several stages could be traced between simplebronchiolar regeneration in and around lung scarsand fully developed carcinomata. Many of thelatter were still microscopical in size.
It is suggested that many so-called " central"lung cancers do not arise in the lobar bronchialepithelium, but involve these structures as a resultof secondary spread from smaller and distantgrowths near the periphery of the lung.
We wish to thank Professor W. G. Barnard for hisinterest and advice in the preparation of this paper andMr. A. E. Clarke for the photomicrographs.
REFERENCESAufses, A. H., and Neuhof, H. (1952). J. thorac. Surg., 23, 219.Geschickter,C. F., and Denison, R.(1934). Amer.J. Cancer, 22,854.Gray, S. H., and Cordonnier, J. (1929). Arch. Surg., Chicago, 19,
1618.James, 1., and Pagel, W. (1944). Brit. J. Surg.,32, 85.Montgomery, G. L. (1944). Ibid., 31, 292.Petersen, A. B., Hunter, W. C., and Sneeden, V. D. (1949). Cancer,
2,991.Prior, J. T., and Jones, D. B. (1952). J. thorac. Surg., 23, 224.Raeburn, C. (1951). Lancet, 2, 474.Spain, D. M., and Parsonnet, V. (1951). Cancer, 4, 277.Stewart, M. J., and Allison, P. R. (1943). J. Path. Bact., 55, 105.Weller, C. V. (1929). Arch. Path., Chicago, 7, 478.Willis, R. A. (1948). The Pathology of Tumours, p. 359. London.Wolf, K. (1895). Fortschr. Med., 13, 725.
10