a simple trajectory guidance device that assists freehand and interactive image guided biopsy of...
TRANSCRIPT

Computer Aided Surgery 2:186–192 (1997)
Brief Technical Report
A Simple Trajectory Guidance Device that AssistsFreehand and Interactive Image Guided Biopsy
of Small Deep Intracranial TargetsNitin Patel, F.R.C.S., and David Sandeman, F.R.C.S.
Department of Neurological Surgery, Frenchay Hospital, Bristol, England
ABSTRACT Frameless image guided stereotactic systems are rapidly becoming incorporated intoroutine neurosurgical practice. In our unit, the Elekta Viewing Wand has been applied to a compre-hensive range of neurosurgical procedures, including pituitary, posterior fossa, skull base, atlantoax-ial, and epilepsy surgery. The system allows a minimally invasive surgical exposure and providesinstant and continual navigational information during surgery. Subjective studies have shown thisintraoperative information to facilitate the surgeon’s perception of anatomic relations and identifica-tion of structures, thus improving surgical safety. Furthermore, in comparison to traditional stereo-tactic frames, the frameless system has been reported to reduce operative time. The technologyinvolves the use of a localizing mechanical arm to which a pointer or biopsy probe is attached. Thislocalizing arm is hand-held and is therefore only as steady as the surgeon’s hand. This precludesthe use of the Viewing Wand for functional procedures and for the safe biopsy of small, deep-seatedintracranial lesions. Both types of procedures are very dependent on a steady linear approach to thetarget for a successful outcome. We have designed a simple guidance device that eliminates the riskof unwanted drift or angular movements of the probe as it is advanced toward the target. Whenused with the Viewing Wand, this device guides the wand biopsy probe along a predetermined, fixedlinear trajectory to the intracranial target. We report the successful use of the fixed trajectoryguidance device (FTGD) with the Elekta Viewing Wand in a series of 12 patients. Comp Aid Surg2:186–192 (1997) q1997 Wiley-Liss, Inc.
Key words: interactive image guided neurosurgery, frameless stereotaxy, device, intracranial target
INTRODUCTIONFreehand localization and biopsy of small, deep- stereotactic frames. The technique defines the po-
sition of an intracranial target by coordinates de-seated, intracranial targets, often in eloquentareas, is usually very difficult and unsafe, even rived from the frame that is rigidly fixed to the
skull during preoperative scanning and during thein skilled hands. However, since the 1950s, it hasbeen possible to define and correlate the exact surgical procedure.
Recent technological advances have led toposition of single or multiple points within thecranium to preoperative imaging by the use of the development of image guidance systems that
Received original June 25, 1996; accepted June 2, 1997.
Address correspondence/reprint requests to Mr. Nitin Patel, F.R.C.S., Neurosurgical Registrar, Neuroscience Research,Academic Centre (Room 1), Frenchay Hospital, Bristol BS16 1LE, United Kingdom.
q1997 Wiley-Liss, Inc.
810C 96-009/ 810C$$6009 08-28-97 09:16:44 igsas W: IGS

Patel and Sandeman: Trajectory Guidance 187
do not require frame-based coordinates for target with a stereotactic frame is achieved by advanc-ing a probe along a predetermined linear trajec-localization. The first commercially available
‘‘frameless’’ interactive image guided system tory that is fixed relative to the brain. In contrast,frameless systems use a hand-held localizingwas the ISG/Elekta Viewing Wand (ISG Tech-
nologies, Inc., Toronto, Ontario, Canada). Its de- probe, the steadiness of which is dependent onthe surgeon’s hand. Understandably, therefore,scription and application to a wide range of intra-
cranial and skull base procedures have been pre- frameless systems have thus far been consideredunsuitable for functional surgery and for the safeviously reported.1,6,11,13 This system also has
potential applications outside the cranium, with biopsy of small, deep-seated intracranial lesions,which are often situated in functionally eloquentrecent publications describing its use in upper
cervical spine surgery.3,10 areas of the brain.We have devised a simple surgical instru-Frameless systems are proving to be more
versatile and less cumbersome than traditional ment, the fixed trajectory guidance device(FTGD), which overcomes this limitation. A spe-stereotactic frames. Moreover, phantom studies,
using a model of the skull.14 have found the inher- cially adapted biopsy probe, attached to the wandarm, is guided by the device along a predeter-ent mechanical accuracy of the ISG/Elekta View-
ing Wand to be within 2 mm. This translates into mined linear trajectory to the intracranial target.This trajectory remains fixed relative to the brainan application accuracy of 2–3 mm with 95%
confidence limits of between 0 and 3.5 mm.7–9 In during the procedure, thus eliminating the riskof misdirection or drift associated with freehanda recent series of 325 cases,6 the display cursor
was judged to be within 2 mm of the actual posi- wand-guided biopsy.tion of the wand probe in the surgical field in92% of cases. This compares favorably with ap- MATERIALS AND METHODSplication accuracy studies of standard frame-based stereotactic systems.5,8,14
The Elekta Viewing WandFrameless systems provide constant intraop-
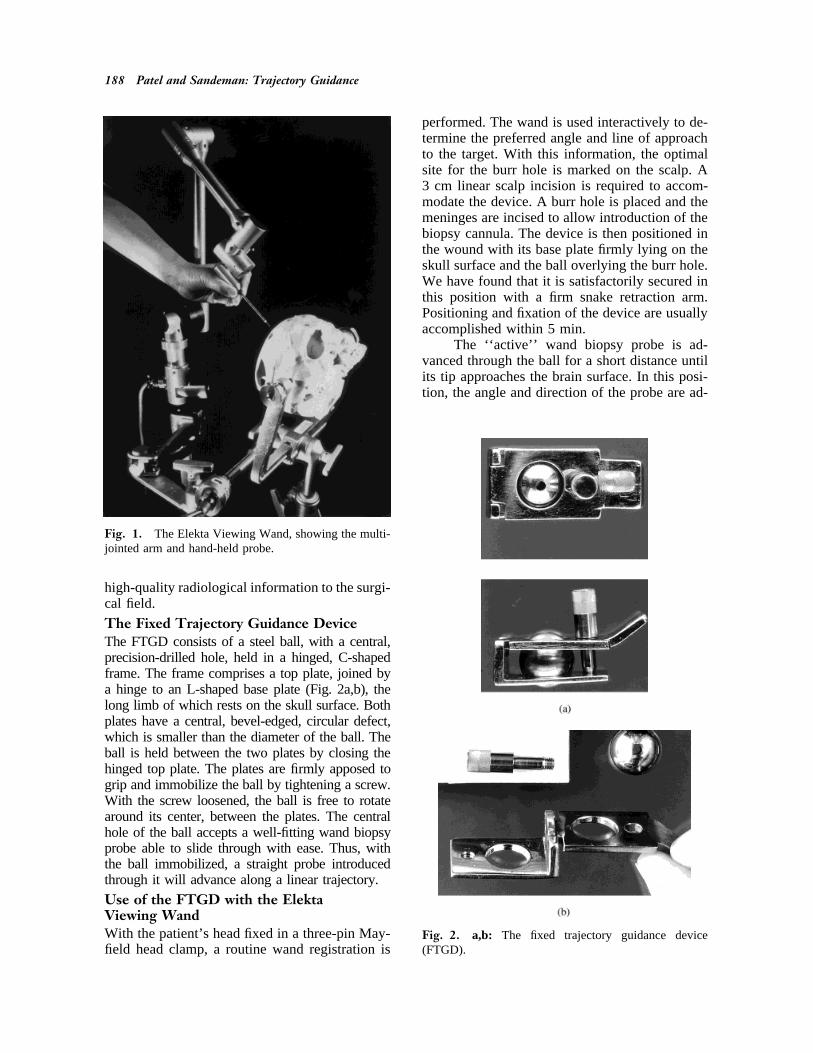
erative navigational information, which permits The Viewing Wand (Fig. 1) has been previouslydescribed.12 In brief, it comprises a ‘‘position-the surgeon to identify precisely the spatial posi-
tion of a hand-held probe in the surgical field sensing’’ articulated arm with six joints and sixdegrees of freedom, linked to an interactive imagewith reformatted computerized tomographic (CT)
or magnetic resonance (MR) images shown on a display computer loaded with the patient’s preop-erative CT or MRI data. The base of the arm ishigh-definition display monitor. Unlike stereotac-
tic frames, therefore, these systems allow the sur- rigidly fixed relative to the surgical field and aprobe is attached to its free end. Each joint ofgeon to localize rapidly any number of targets in
different planes. the localizing arm houses an electrogoniometer(FAROSurgicom), which constantly relays itsThere is, however, one notable disadvantage
of frameless systems. Their dependence on preop- angle to a host computer, where calculations de-termine the exact spatial position of the wanderative image data for intraoperative navigation
precludes their ability to compensate for shifts of probe tip relative to the fixed base. Either CT orMR images of the head, acquired preoperatively,intracranial contents during the procedure. How-
ever, significant brain shift tends to be limited to can be used for image guidance. Segmentation ofthe two-dimensional data allows accurate three-decompressive procedures of large tumors and
cystic lesions. In such cases, the surgeon can still dimensional (3D) reconstruction of the skin sur-face and other structures. In the operating theater,benefit from the system by obtaining the appro-
priate navigational information prior to the de- the actual position and contour of the patient’shead is then exactly matched with the 3D image.compressive procedure. Alternatively, intraopera-
tive ultrasound may be more useful insofar as it This process, termed registration, has alreadybeen described in detail.12 Upon completion ofprovides real-time navigation. It is important to
note, however, that ultrasound is difficult to apply registration, the surgeon can interactively use theWand probe tip as a pointer within the operatingto surgery of deep-seated lesions and that the im-
age quality is dependent on the echogenicity of field and simultaneously identify its exact posi-tion relative to the preoperative image. It there-tissue interfaces.13
The localization of an intracranial target fore allows direct and accurate transference of
810C 96-009/ 810C$$6009 08-28-97 09:16:44 igsas W: IGS
188 Patel and Sandeman: Trajectory Guidance
performed. The wand is used interactively to de-termine the preferred angle and line of approachto the target. With this information, the optimalsite for the burr hole is marked on the scalp. A3 cm linear scalp incision is required to accom-modate the device. A burr hole is placed and themeninges are incised to allow introduction of thebiopsy cannula. The device is then positioned inthe wound with its base plate firmly lying on theskull surface and the ball overlying the burr hole.We have found that it is satisfactorily secured inthis position with a firm snake retraction arm.Positioning and fixation of the device are usuallyaccomplished within 5 min.
The ‘‘active’’ wand biopsy probe is ad-vanced through the ball for a short distance untilits tip approaches the brain surface. In this posi-tion, the angle and direction of the probe are ad-
Fig. 1. The Elekta Viewing Wand, showing the multi-jointed arm and hand-held probe.
high-quality radiological information to the surgi-cal field.
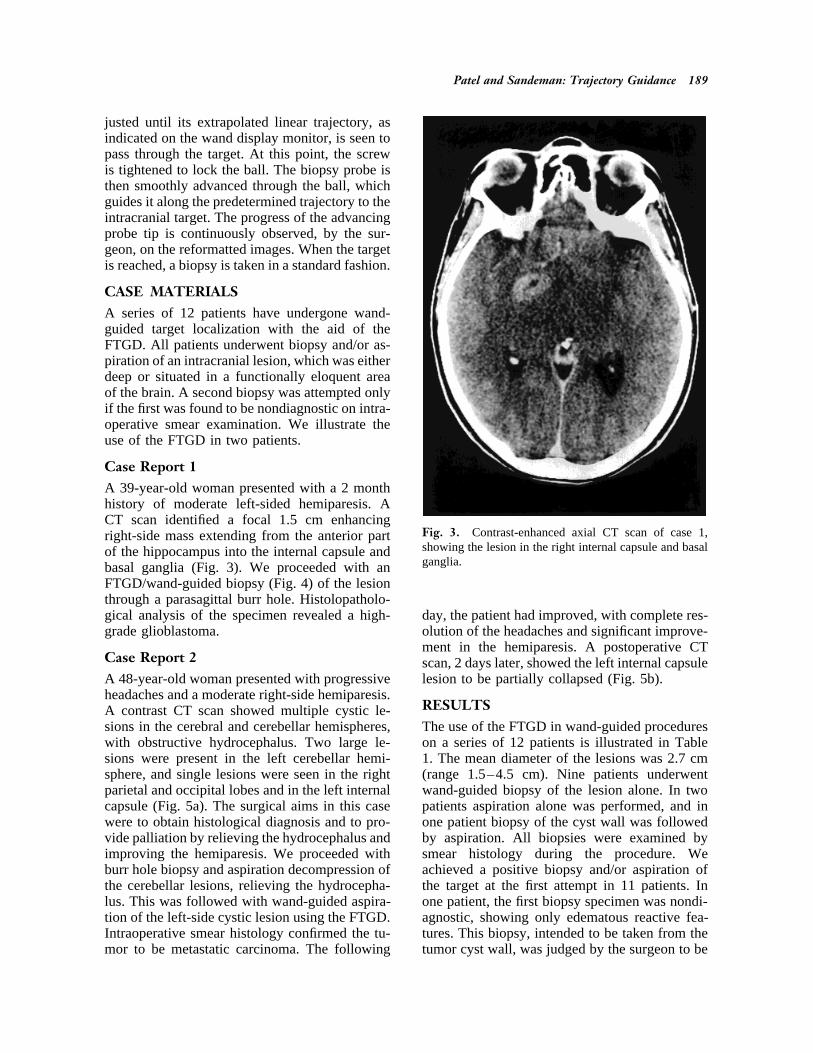
The Fixed Trajectory Guidance DeviceThe FTGD consists of a steel ball, with a central,precision-drilled hole, held in a hinged, C-shapedframe. The frame comprises a top plate, joined bya hinge to an L-shaped base plate (Fig. 2a,b), thelong limb of which rests on the skull surface. Bothplates have a central, bevel-edged, circular defect,which is smaller than the diameter of the ball. Theball is held between the two plates by closing thehinged top plate. The plates are firmly apposed togrip and immobilize the ball by tightening a screw.With the screw loosened, the ball is free to rotatearound its center, between the plates. The centralhole of the ball accepts a well-fitting wand biopsyprobe able to slide through with ease. Thus, withthe ball immobilized, a straight probe introducedthrough it will advance along a linear trajectory.
Use of the FTGD with the ElektaViewing WandWith the patient’s head fixed in a three-pin May- Fig. 2. a,b: The fixed trajectory guidance device
(FTGD).field head clamp, a routine wand registration is
810C 96-009/ 810C$$6009 08-28-97 09:16:44 igsas W: IGS
Patel and Sandeman: Trajectory Guidance 189
justed until its extrapolated linear trajectory, asindicated on the wand display monitor, is seen topass through the target. At this point, the screwis tightened to lock the ball. The biopsy probe isthen smoothly advanced through the ball, whichguides it along the predetermined trajectory to theintracranial target. The progress of the advancingprobe tip is continuously observed, by the sur-geon, on the reformatted images. When the targetis reached, a biopsy is taken in a standard fashion.
CASE MATERIALSA series of 12 patients have undergone wand-guided target localization with the aid of theFTGD. All patients underwent biopsy and/or as-piration of an intracranial lesion, which was eitherdeep or situated in a functionally eloquent areaof the brain. A second biopsy was attempted onlyif the first was found to be nondiagnostic on intra-operative smear examination. We illustrate theuse of the FTGD in two patients.
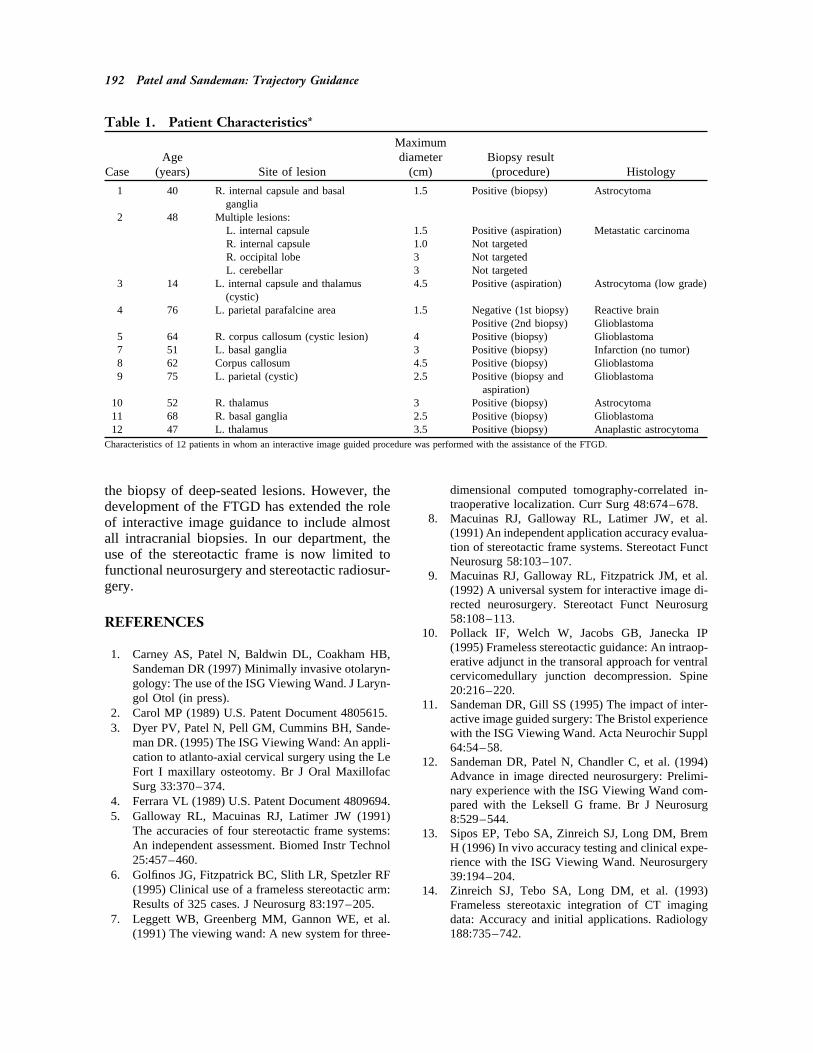
Case Report 1A 39-year-old woman presented with a 2 monthhistory of moderate left-sided hemiparesis. ACT scan identified a focal 1.5 cm enhancing
Fig. 3. Contrast-enhanced axial CT scan of case 1,right-side mass extending from the anterior partshowing the lesion in the right internal capsule and basalof the hippocampus into the internal capsule andganglia.basal ganglia (Fig. 3). We proceeded with an
FTGD/wand-guided biopsy (Fig. 4) of the lesionthrough a parasagittal burr hole. Histolopatholo-gical analysis of the specimen revealed a high- day, the patient had improved, with complete res-
olution of the headaches and significant improve-grade glioblastoma.ment in the hemiparesis. A postoperative CT
Case Report 2 scan, 2 days later, showed the left internal capsulelesion to be partially collapsed (Fig. 5b).A 48-year-old woman presented with progressive
headaches and a moderate right-side hemiparesis.RESULTSA contrast CT scan showed multiple cystic le-
sions in the cerebral and cerebellar hemispheres, The use of the FTGD in wand-guided procedureson a series of 12 patients is illustrated in Tablewith obstructive hydrocephalus. Two large le-
sions were present in the left cerebellar hemi- 1. The mean diameter of the lesions was 2.7 cm(range 1.5–4.5 cm). Nine patients underwentsphere, and single lesions were seen in the right
parietal and occipital lobes and in the left internal wand-guided biopsy of the lesion alone. In twopatients aspiration alone was performed, and incapsule (Fig. 5a). The surgical aims in this case
were to obtain histological diagnosis and to pro- one patient biopsy of the cyst wall was followedby aspiration. All biopsies were examined byvide palliation by relieving the hydrocephalus and
improving the hemiparesis. We proceeded with smear histology during the procedure. Weachieved a positive biopsy and/or aspiration ofburr hole biopsy and aspiration decompression of
the cerebellar lesions, relieving the hydrocepha- the target at the first attempt in 11 patients. Inone patient, the first biopsy specimen was nondi-lus. This was followed with wand-guided aspira-
tion of the left-side cystic lesion using the FTGD. agnostic, showing only edematous reactive fea-tures. This biopsy, intended to be taken from theIntraoperative smear histology confirmed the tu-
mor to be metastatic carcinoma. The following tumor cyst wall, was judged by the surgeon to be
810C 96-009/ 810C$$6009 08-28-97 09:16:44 igsas W: IGS

190 Patel and Sandeman: Trajectory Guidance
Fig. 4. Viewing Wand images of the biopsy procedure in case 1.
just superficial to the cyst surface, and a second applicable to a wider range of neurosurgical pro-cedures. Moreover, its accuracy is comparable todeeper biopsy along the same trajectory proved
to be positive. There were no intraoperative prob- that of traditional stereotactic frames.6,14 A funda-mental advantage of stereotactic frames over thelems associated with use of the FTGD. Postopera-
tive examination of patients showed no evidence hand-held localizing probes of the Viewing Wandis the facility of allowing precise linear advance-of worsening neurological function. In two pa-
tients (cases 2 and 3), significant improvement in ment of the surgical probe to the target, thus elim-inating potential errors associated with handneurological function was seen following tumor
cyst aspiration. In one of these patients (case 2), movement. This is essential, particularly for func-tional procedures and the biopsy of small, deep-subsequent imaging confirmed a reduction in the
size of the large peritumoral cyst. seated lesions, which are often situated in func-tionally eloquent areas of the brain. This report
DISCUSSION constitutes a simple assessment of a device de-signed to fixate the linear trajectory of a hand-Stereotactic frames accurately direct an instru-
ment along a linear trajectory, which is fixed rela- held probe as it is advanced toward an intracranialtarget.tive to the brain, to a predetermined intracranial
target. The Elekta Viewing Wand represents the The basic principle of the design is not new.Similar devices have been described2,4 for usenew concept of intracranial navigation by inter-
active image guidance. This ‘‘frameless’’ system in neurosurgical operations, including stereotacticprocedures. Although the form and complexity ofis more versatile than stereotactic frames and is
810C 96-009/ 810C$$6009 08-28-97 09:16:44 igsas W: IGS

Patel and Sandeman: Trajectory Guidance 191
Fig. 5. a: Preoperative CT image of case 2, showing multiple cystic lesions. b: The postoperative image shows adecrease in the size of a cystic lesion (arrow) following wand/FTGD aspiration.
their designs vary, the common underlying func- the device to allow direct fixation to the skullwith bone screws through an enlarged base plate.tion of these devices is to guide neurosurgical
tools in a predetermined trajectory relative to the Second, the process of intraoperative reformattingof contrast-enhancing lesions by the Viewingpatient’s skull. The application of this type of
device to interactive image guided procedures has Wand can be associated with a small reductionin the delineating signal of the lesion. If the lesionnot been previously described.
The use of the FTGD in conjunction with is very small or enhances poorly, any diminutionin contrast enhancement during the reformattingthe Viewing Wand has allowed safe and accurate
image guided biopsies of intracranial lesions that process can make it difficult to identify the lesionon reformatted images. In this instance the sur-are small, deep, or located in functionally im-
portant regions of the brain. The smallest lesion geon might not reliably identify the target. Incontrast, a frame-based stereotactic biopsy that isbiopsied with this method was 1.5 cm in diameter.
Although the FTGD might allow accurate tar- independent of such intraoperative image re-format remains the technique of choice in suchgeting of much smaller lesions, this optimism
must remain guarded for two main reasons. First, cases. The other instance in which frame-basedstereotactic technique may be preferable is in thethe current design precludes absolute rigid fixa-
tion of the FTGD to the skull, so the device is biopsy of lesions less than 1 cm in diameter forthe reasons discussed above.susceptible to accidental movement during the
procedure. However, we have found that, withCONCLUSIONSattention to surgical method, a firm retraction arm
provides satisfactory fixation. If necessary, rigid The initial experience with the freehand ViewingWand suggested that its use would be limited infixation is also feasible by simple modification of
810C 96-009/ 810C$$6009 08-28-97 09:16:44 igsas W: IGS
192 Patel and Sandeman: Trajectory Guidance
Table 1. Patient Characteristics*Maximum
Age diameter Biopsy resultCase (years) Site of lesion (cm) (procedure) Histology
1 40 R. internal capsule and basal 1.5 Positive (biopsy) Astrocytomaganglia
2 48 Multiple lesions:L. internal capsule 1.5 Positive (aspiration) Metastatic carcinomaR. internal capsule 1.0 Not targetedR. occipital lobe 3 Not targetedL. cerebellar 3 Not targeted
3 14 L. internal capsule and thalamus 4.5 Positive (aspiration) Astrocytoma (low grade)(cystic)
4 76 L. parietal parafalcine area 1.5 Negative (1st biopsy) Reactive brainPositive (2nd biopsy) Glioblastoma
5 64 R. corpus callosum (cystic lesion) 4 Positive (biopsy) Glioblastoma7 51 L. basal ganglia 3 Positive (biopsy) Infarction (no tumor)8 62 Corpus callosum 4.5 Positive (biopsy) Glioblastoma9 75 L. parietal (cystic) 2.5 Positive (biopsy and Glioblastoma
aspiration)10 52 R. thalamus 3 Positive (biopsy) Astrocytoma11 68 R. basal ganglia 2.5 Positive (biopsy) Glioblastoma12 47 L. thalamus 3.5 Positive (biopsy) Anaplastic astrocytoma
Characteristics of 12 patients in whom an interactive image guided procedure was performed with the assistance of the FTGD.
dimensional computed tomography-correlated in-the biopsy of deep-seated lesions. However, thetraoperative localization. Curr Surg 48:674–678.development of the FTGD has extended the role
8. Macuinas RJ, Galloway RL, Latimer JW, et al.of interactive image guidance to include almost(1991) An independent application accuracy evalua-all intracranial biopsies. In our department, thetion of stereotactic frame systems. Stereotact Functuse of the stereotactic frame is now limited to Neurosurg 58:103–107.
functional neurosurgery and stereotactic radiosur- 9. Macuinas RJ, Galloway RL, Fitzpatrick JM, et al.gery. (1992) A universal system for interactive image di-
rected neurosurgery. Stereotact Funct Neurosurg58:108–113.REFERENCES
10. Pollack IF, Welch W, Jacobs GB, Janecka IP(1995) Frameless stereotactic guidance: An intraop-
1. Carney AS, Patel N, Baldwin DL, Coakham HB,erative adjunct in the transoral approach for ventral
Sandeman DR (1997) Minimally invasive otolaryn-cervicomedullary junction decompression. Spine
gology: The use of the ISG Viewing Wand. J Laryn-20:216–220.
gol Otol (in press). 11. Sandeman DR, Gill SS (1995) The impact of inter-2. Carol MP (1989) U.S. Patent Document 4805615. active image guided surgery: The Bristol experience3. Dyer PV, Patel N, Pell GM, Cummins BH, Sande- with the ISG Viewing Wand. Acta Neurochir Suppl
man DR. (1995) The ISG Viewing Wand: An appli- 64:54–58.cation to atlanto-axial cervical surgery using the Le 12. Sandeman DR, Patel N, Chandler C, et al. (1994)Fort I maxillary osteotomy. Br J Oral Maxillofac Advance in image directed neurosurgery: Prelimi-Surg 33:370–374. nary experience with the ISG Viewing Wand com-
4. Ferrara VL (1989) U.S. Patent Document 4809694. pared with the Leksell G frame. Br J Neurosurg5. Galloway RL, Macuinas RJ, Latimer JW (1991) 8:529–544.
The accuracies of four stereotactic frame systems: 13. Sipos EP, Tebo SA, Zinreich SJ, Long DM, BremAn independent assessment. Biomed Instr Technol H (1996) In vivo accuracy testing and clinical expe-25:457–460. rience with the ISG Viewing Wand. Neurosurgery
6. Golfinos JG, Fitzpatrick BC, Slith LR, Spetzler RF 39:194–204.(1995) Clinical use of a frameless stereotactic arm: 14. Zinreich SJ, Tebo SA, Long DM, et al. (1993)Results of 325 cases. J Neurosurg 83:197–205. Frameless stereotaxic integration of CT imaging
7. Leggett WB, Greenberg MM, Gannon WE, et al. data: Accuracy and initial applications. Radiology188:735–742.(1991) The viewing wand: A new system for three-
810C 96-009/ 810C$$6009 08-28-97 09:16:44 igsas W: IGS