a review of pain management choices, resources, and ... · pdf filea review of pain management...
TRANSCRIPT

A Review of Pain Management Choices, Resources, and Information Access

Patients consider pain as one of the worst
postoperative experiences Severe postoperative pain is detrimental to
recovery

Acute Pain management improves patient outcomes!
If severe pain is not controlled, it may:
negatively affect patient recovery
lead to development of chronic pain

Acute pain services have been developed as anesthesiologists working with nursing have been found to have the most interest in pain management Nursing education encouraging development
of critical thinking skills is central to optimizing individualized patient care
Nurse clinicians/nurse practitioners are being trained to support clinical pain management

Post surgical pain Trauma pain
Pain control (e.g. labour and delivery) Acute exacerbations of chronic conditions
e.g. acute on chronic pain

Past medical history Pre-injury/preoperative pain report and
medical management Patient response both past and present to
pain medications Type of injury/surgery Present pain assessment including patient
pain report and response to meds ordered Goals of therapy

The body reacts to external stimuli and has the ability to distinguish between minor
and substantial injury After tissue injury and the resulting
inflammatory response, a patient’s threshold to and perception of pain is altered
Desborough J. (2000). The Stress Response to Trauma and Surgery. British Journal of Anaesthesia, 85(1), 109-117.

This response promotes maximum chances
for survival because it: • Increases cardiovascular functions • Preserves body fluid • Supplies the body with increased energy generating molecules
Desborough J. (2000). The Stress Response to Trauma and Surgery. British Journal of Anaesthesia, 85(1), 109-117.

Prolonged response can lead to: exhaustion weight loss decreased immune response less enthusiasm and ability to perform
rehabilitation needed for recovery
Desborough J. (2000). The Stress Response to Trauma and Surgery. British Journal of Anaesthesia, 85(1), 109-117.

Pain affects: ventilation immune system (increasing infection) GI tract (decreased gastric emptying) endocrine system (altered hormone release causing
metabolic disturbances) The stress/inflammatory response to pain puts the
body into a prothrombotic (hypercoagulable) state increasing blood clotting risks
Joint Commission on Accreditation of Healthcare Organization (December 2001, p.14). Pain: Current Understanding of Assessment, Management, and Treatments. P.14
Anesthesiologists’ goals in managing pain is
to reduce this response with planned trauma and minimize the response after traumatic injury

An anesthesiologist is assigned to Acute Pain
Service at each site (UH and VH)
Nurse Clinician acute pain management – one for each site

• PAIN Consultant is listed at the top of the OR record
• Monday to Friday, excluding holidays there is an anesthesiologist assigned to the acute pain service

Communication Algorithm for Acute Pain Service, UH Daytime weekdays 0800 – 1600 hours
1st call - Anesthesiologist Pain Consultant – 13351 2nd call - Nurse Clinician Pain Management – 14227
After hours and on weekends Anesthesiologist on call for pain covers weekend clinical rounds
First call - Anesthesia Resident on call – 19855 Second call – Anesthesiologist on call – 13830
Third call – for difficult pain management issues only – Anesthesiologist Pain Consultant -
(e.g. epidural hematoma, acute on chronic pain management) – pager 13351 – contact should be made through anesthesia on call
Communication Algorithm for Acute Pain Service, VH.
Daytime weekdays (0800-1600 hours) APS Nurse Clinician: 14691
Anesthesia pain Consultant: 18954 For all pre-op consults during the day, please contact the APS consultant at –
pager #18954 For any pain issues or pain consults during the day 7:30 am - 15:30hrs, please
contact APS nurse Clinician at pager # 14691
After hours 1st Call Anesthesia Resident on Call: 13305 2nd Anesthesia Consultant on Call: 14206
Available on the APS website http://www.lhsc.on.ca/priv/pain/algorith.htm • UH anesthesia resident
on call carries a text pager

Helps you to remember essential pain assessment criteria: • P – provoking or precipitating factors • Q – quality of pain (what words does the person use to describe pain?) • R – radiation of pain (does the pain extend from the site?) • S – severity of pain (intensity, 0-10 scale) • T – timing (occassional, intermittent, constant)
Registered Nurses Association of Ontario (November 2002). Nursing Best Practice Guideline: assessment and management of pain. Toronto.
Nociceptive pain Innate, protective response to trauma. Injury activates pain sensing nerve fibers
sending communication of such pain to the CNS
Neuropathic pain Response to damage to the nervous system
related to disease or trauma
Pasero, C, McCaffery, M. (2011). Pain Assessment and Pharmacologic Management. Mosby, pp. 890.

Nociceptive pain responds well to
opioids
Neuropathic pain opioids are third line after:
1. Tricyclic antidepressants (e.g. Amitriptyline) and anticonvulsants (e.g.,Gabapentin)
2. Topical Lidocaine and SNRIs (serotonin/norepinephrine reuptake inhibitors)
(e.g. Duloxetine) Moulin D., et al. (2007). Pharmacological Management of Chronic Neuropathic Pain –
Consensus Statement and Guidelines from the Canadian Pain Society. Pain Res Manag., 12(1), 13-21.

Nociceptive Pain Quality descriptors might include achy, throbbing pain Neuropathic Pain Quality descriptors sound like electricity such
as stabbing, burning, shooting pain

Pain standards of the Joint Commission on Accreditation of Healthcare Organizations Recommendation: make pain assessment/management a
priority in daily practice
PQRST: Consider pain intensity or severity the fifth vital sign along the temperature, pulse, respiration, BP
Patient’s rights: full pain workup when pain is not easily characterized or treated
JCAHO 1999-2000.

From Key
From flow sheet
Documentation: revised generic LHSC Adult Graphic Record

Everything you want to know about acute pain management baseline knowledge base is an expectation
for practice See the APS website under pain management
strategies, education: http://www.lhsc.on.ca/priv/pain/slpacm.htm

All new nurses will review:
Acute Pain Management Self Directed Learning Package (SDLP) http://www.lhsc.on.ca/priv/pain/slpacm.htm
Intravenous PCA pump and website http://www.lhsc.on.ca/priv/pain/ivpca/index.htm
All new nurses who will be working with these modalities will also review: Neuraxial Pain Management SDLP
(epidural/intrathecal opioid analgesia) http://www.lhsc.on.ca/priv/pain/epidural/epstrat.htm
Regional Anesthesia/Analgesia SDLP (on line soon)
This site has been produced to help clinical staff with easy access to: Clinical reference
Clinical staff education material
Patient education material
Technology quick reference

Click intranet explorer icon on your desktop or under start menu
Select “Programs/Departments/Resources” located
near the top of the home page Select “Acute Pain Services”
Menu located on the left side of the page

Welcome
APS Communication Algorithm
Pain Management Strategies
Opioid Choices and Conversions
Order Forms
Monograph Index
IV PCA
Intrathecal Opioid Analgesic
Epidural
Regional Block
Technology
Duragesic
Methadone
Complementary Strategies
Links
Click on epidural

Staff education on the site
Patient safety assessment reviewed
Basic assessment information

Common concerns regarding the use of opioids include:
the potential for detrimental side effects
physical dependence
Addiction
opioid-induced hyperalgesia
Pasero, C, McCaffery, M. (2011). Pain Assessment and Pharmacologic Management. Mosby, pp.
291-300.

Located in the CNS, pituitary gland and the GI
tract
Especially abundant in the dorsal horn of the spinal cord
Pasero, C, McCaffery, M. (2011). Pain Assessment and Pharmacologic Management. Mosby, pp. 284

Opioid pain management decision making is influenced by:
Efficacy
Potency
Responsiveness
Resistance Pasero, C, McCaffery, M. (2011). Pain Assessment and Pharmacologic Management. Mosby, pp.290-291.

Efficacy optimal dose for each patient (considering
side effect profile and reported pain relief) Potency equivalent dosing of different opioids using a
conversion chart (see APS website)

Responsiveness is influenced by:
patient characteristics
the particular type of pain the patient is having e.g. opioid responsiveness is reduced when managing neuropathic pain

Resistance (tolerance)
is the body’s adjustment to constant dosing of opioid decreasing the effect. Patients , over time, will need higher dose of drug to maintain an effect
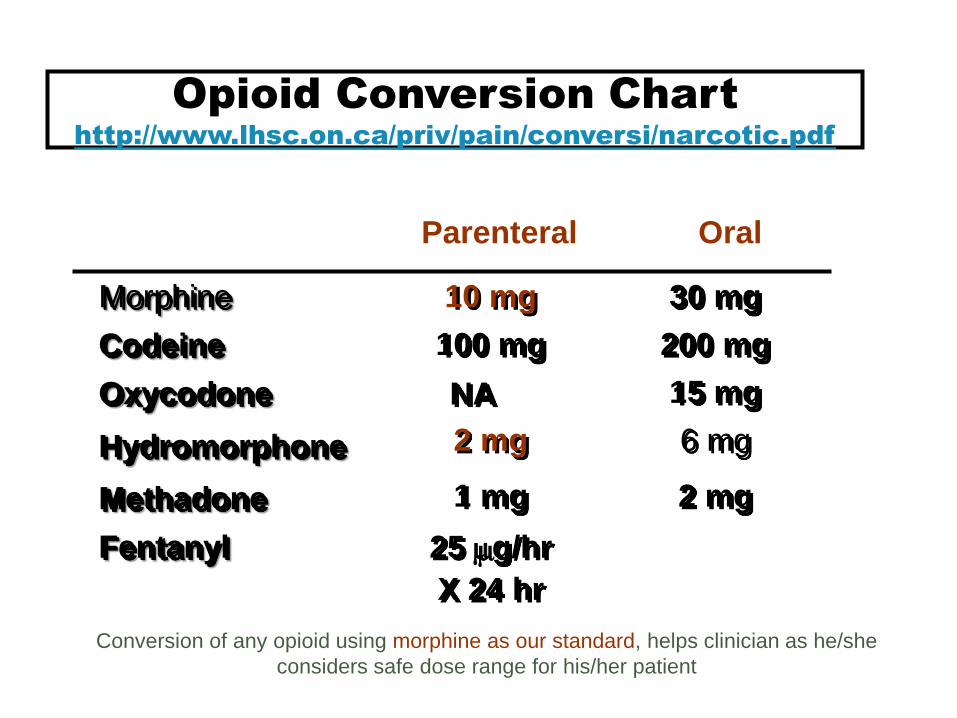
Opioid Conversion Chart
http://www.lhsc.on.ca/priv/pain/conversi/narcotic.pdf
Morphine
Codeine
Oxycodone
Hydromorphone
Methadone
Fentanyl
10 mg
100 mg
NA
2 mg
1 mg
25 mg/hr
X 24 hr
Parenteral Oral
30 mg
200 mg
15 mg
6 mg
2 mg
Conversion of any opioid using morphine as our standard, helps clinician as he/she
considers safe dose range for his/her patient

Neuroplasticity: “the ability of the peripheral and central nervous systems to change both structure and function as a result of noxious stimuli.”
If patient’s opioid receptors are “flooded” with high dose opioid, the body will reroute signals through other receptors (e.g. NMDA receptors) Opioids will be less effective in this
situation Pasero, C, McCaffery, M. (2011). Pain Assessment and Pharmacologic Management. Mosby, pp. 860.

Key points in management:
Consider opioid tolerance
Management of baseline pain
Be cognizant that the patient will have tolerance to most of the opioid induced adverse effects
Balanced analgesia strategy use is important Pasero, C, McCaffery, M. (2011). Pain Assessment and Pharmacologic Management. Mosby, pp. 293-294; 624.

Pain management administration choices:
1. IV Opioid Patient Controlled Analgesia (PCA)
2. Intrathecal Opioid one-shot
3. Epidural Analgesia
4. Regional Block Analgesia

Safety is our first priority in caring for our
patients
With our patient safe, excellent analgesia is our ultimate goal

PCA is associated with greater patient satisfaction compared with intermittent opioid injections.
The reasons for this include:
Patient driven small and frequent intravenous bolus doses of opioid
Flexibility in dosing
The intensity of acute pain is rarely constant Patients are able to titrate the amount of opioid
delivered against dose-related side effects

• Shaded area represents targeted analgesia concentration
• The aim to achieve analgesia
• When below targeted conc., the patient is likely to experience more pain

Advantage of this opioid administration route:
Quick access to opioid prior to team knowing opioid requirements of patient
Disadvantage
Drug is metabolized more quickly than parenteral or oral routes which sometimes affects patient sleep/effective pain control
Minimum IV rate may preclude use of PCA for patients with a fluid restriction (e.g. minimum is 50 ml/hr)
Pasero, C, McCaffery, M. (2011). Pain Assessment and Pharmacologic Management. Mosby, pp. 410.

Safety: Assess for and identify early opioid - induced
respiratory depression (apply this strategy to all routes)
Monitor for sedation as an early sign of respiratory depression
Learn to assess unstimulated respiratory rate and pattern on patients who are sedated

Omnifuse PCA syringe pump http://www.lhsc.on.ca/priv/pain/ivpca/tech.htm

Given close to site of action – the Dorsal Horn of the Spinal Cord
Close proximity of injection avoids loss of drug as it travels to the receptors and thus means smaller doses are required to achieve analgesia
Morphine can be given in much smaller doses
(about 5 % of injectable dose) and will last 12-24 hours

Dose is given by an anesthesiologist in the Operating Room
Safety assessment is required related to
duration of action
Assessment of respiratory rate, sedation, oxygen saturation q1h x 24 hours
Horlocker et al (2009). Practice Guidelines for the Prevention, Detection, and Management of Respiratory Depression Associated with Neuraxial Opioid Administration. Anesthesiology, 110(2), 218-230. Pasero, C, McCaffery, M. (2011). Pain Assessment and Pharmacologic Management. Mosby, pp. 418-419.

Intrathecal, spinal, and subarachnoid are interchangeable terms. Epidural remains outside or on the dura
Intrathecal/spinal anesthesiologists insert a needle through the dura into the cerebrospinal fluid


Epidural analgesia (Neuraxial Pain Management Self Directed Learning Package)
http://www.lhsc.on.ca/priv/pain/epidural/index.htm
Regional block analgesia catheters (Peripheral Nerve Blocks) http://www.lhsc.on.ca/priv/pain/regional.htm

Postoperative pain management
As a sole technique for surgical procedures (e.g. cesarean section)
Analgesia alone (e.g. childbirth, knee manipulations)
Trauma pain
Chronic pain management

Reduced doses of local and opioid are used in combined dosing
Better activity pain control
Decreased incidence of ileus promoting early feeding
Preservation of pulmonary function
Provides cardiac protection = by reducing oxygen requirements and increasing blood supply

Taken from: http://www.webmm.ahrq.gov/case.aspx?caseID=90

Use low concentrations of local anesthetic drug in an attempt to block sensory fibers only (motor fibers unaffected)
This means that the patient will be able to move and walk normally while still receiving good pain relief
NOTE: dense motor blockade is not an expected effect of low dose epidural local infusions and indicates serious complications

Failure or poor analgesia Hypotension Post Dural puncture headache Epidural can slow labour Rare but potentially catastrophic catheter related
issues which include:
- Nerve root/spinal cord damage - Infection (epidural abscess) - Epidural hematoma - Catheter migration to blood vessel or CSF Pasero, C, McCaffery, M. (2011). Pain Assessment and Pharmacologic Management. Mosby, pp. 433, 437, 439.

Causes of hypovolemia after major surgery include: blood loss, bowel prep, 3rd spacing Heart conditions e.g.MI, valve disease, CHF Anemia Sepsis Anastomotic leak Cowling G, Haas R. (2002). Hypotension in the PACU: An Algorithmic Approach. Journal of PeriAnesthesia Nursing, 17(3), 159-163.

In the low concentrations used in combination with opioids for pain relief, significant hypotension is unlikely unless the patient is also hypovolemic.

Called “regional” block because:
the goal is to numb a specific area of the body
named after the anatomical location/nerve plexus targeted.
E.g. Femoral block = femoral nerve
Lower limb regional blocks are the most frequently done block at UH (e.g. femoral/sciatic)

Knowledge of anatomy helps you to trouble shoot potential catheter- related issues http://www.lhsc.on.ca/priv/pain/regional/femoral.pdf

Needle/catheter is placed in tissue in close proximity to targeted nerve/nerve plexus.
Dose/concentration of local anesthetic agent used determine the density of the block
anesthesia = full block analgesia = block to pain
Ultrasound and/or nerve stimulator is used to ensure safe and precise catheter placement

NOTE: pump number Quick reference and pump education material available at: http://www.lhsc.on.ca/priv/pain/epidural/tech.htm

Block assessment columns for local anesthetic infusions only >catheter site for epidural only
Opioid safety assessment columns
Pain Scores: Rest and activity
Pump number from previous slide charted here
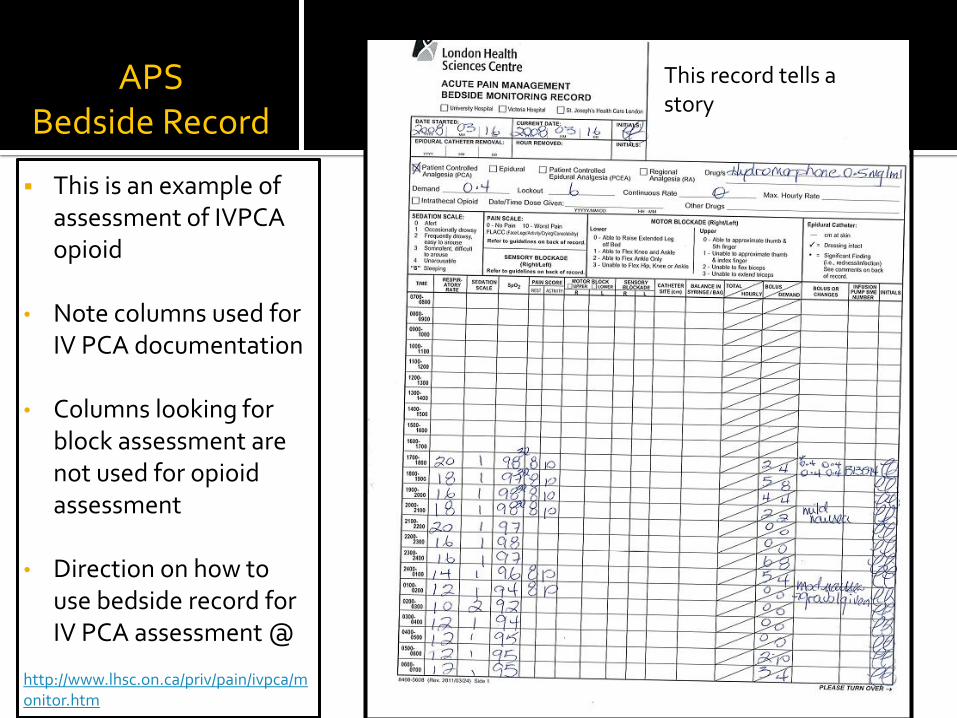
APS Bedside Record
This is an example of assessment of IVPCA opioid
• Note columns used for
IV PCA documentation
• Columns looking for block assessment are not used for opioid assessment
• Direction on how to use bedside record for IV PCA assessment @
http://www.lhsc.on.ca/priv/pain/ivpca/monitor.htm
This record tells a story

APS Bedside Record
Back of the bedside record (previous example continued) • Contains scales
for pain assessment
• an area to do narrative charting

Vital signs: Respiratory Rate (RR) Level of sedation
(sedation is an early sign of respiratory depression)
Oxygen saturation (SpO2)
NRS or appropriate pain score tool
Side effect profile
Assess respiratory pattern: Adult ⇒ q1h x 12 hours ⇒ q2h x 12 hours ⇒ q4h for remainder of therapy
Pediatrics ⇒q1h x 24 hours ⇒ q2h x 24 hours ⇒q4h for remainder of therapy Pain score q4h at rest and
with activity while patient is receiving analgesia
Side effect profile q4h See APS website

APS Bedside Record
This is an example of the bedside record used to assess epidural analgesia Remember that
the dermatome chart is located on the back of this record
Direction on how to use the monitoring record for epidural assessment
http://www.lhsc.on.ca/priv/pain/epidural/secg.pdf
What does this charting tell you??

Vital Signs: Respiratory rate Sedation score Oxygen saturation Blood pressure Pain score Sensory blockade Motor blockade Catheter monitoring Side effects
Assess respiratory pattern: the same as with IV PCA
Blood pressure q4h while on infusion
Pain score q4h(rest and activity) Sensory and motor blockade
q4h x 24 hours then q12h at the beginning of each shift
Infusion system – hub q1h Site with dressing checks Side effects q4h

Acute pain service now uses electronic
charting
APS power chart notes can be reviewed by all staff

Go to start menu and select information systems
Open power chart Prod Domain
Enter user name and password
Open the patient that you are caring for (you are in
the flow sheet view)

• Go to “All results flow
sheet”
• Click the down arrow
to reveal
selections there
• Scroll to the Acute
Pain Service View
• Pain service
documentation
including
procedure
records entered
will appear in this
view

Power chart view:
Procedure record for
epidural insertions
Nice concise
summary of
insertion which
includes location of
catheter at skin on
insertion

If not entered in power chart, documentation of the
procedure may be recorded on:
The anesthesia record (under the title Regional) or
Paper anesthesia procedure record located in the
OR section of the chart

Go to LHSC intranet;
Programs/Departments/Resources; Nursing; Nursing Grand Rounds; Videos
See presentations by Heather Fisher and Cindy Carnegie on Pain Management and Epidural Analgesia
http://www.lhsc.on.ca/priv/nursing/rounds/videos.htm
