a review of interstitial lung diseases - continuing … · 2009-06-18 · a review of interstitial...
TRANSCRIPT

A Review of Interstitial Lung Diseases
Paul J. Wolters, MDAssociate Professor
Department of MedicineUniversity of California San Francisco

Outline
• Overview of diagnosis in ILD– Why it is important
– Definition/Classification
– High‐resolution CT scan
– Multidisciplinary approach
• Cases– Interactive format (ARS)
– Review of radiology and pathology
• Questions/Discussion

Why it is Important to be Aware of ILD’s

Don’t stop with “pulmonary fibrosis”
• Reasons for a specific diagnosis:
– Many forms are treatable
– Treatments depend on diagnosis
– Prognosis varies
– Eligibility for clinical trials

Clinical Classification
Pulmonary Fibrosis
Exposure-related:- Occupational- Environmental- Avocational- Medication
Idiopathic interstitial
pneumonia (IIP)
Connective tissue disease:- Scleroderma- Rheum. arthritis- Sjogrens- UCTD
Other:- Sarcoidosis- Vasculitis/Diffuse alveolar
hemorrhage (DAH)- Langherhans cell histiocytosis
(LCH)- Lymphagioleiomyomatosis
(LAM)- Pulmonary alveolar
proteinosis (PAP)- Eosinophilic pneumonias- Neurofibromatosis- Inherited disorders- Chronic aspiration- Inflammatory bowel disease
Idiopathic pulmonary
fibrosis (IPF)
Desquamative interstitial pneumonia (DIP)
Acute interstitial pneumonia (AIP)
Nonspecific interstitial pneumonia (NSIP)
Respiratory bronchiolitis interstitial lung dis. (RBILD)
Cryptogenic organizing pneumonia (COP)
Lymphocytic interstitial pneumonia (LIP)

Clinical History
Idiopathicusual interstitial pneumonitis (UIP) = IPFnonspecific interstitial pneumonitis (NSIP)desquamative interstitial pneumonitis (DIP)respiratory bronchiolitis ILD (RBILD)acute interstitial pneumonitis (AIP)
Occupational/Environmental-Asbestos-Birds/Molds/Organic Material (HP)
DrugsUnclassified
Collagen VascularJoint c/oSicca sxSkin rashRaynaud’s

Exam: Clues to diagnosis
• Lung: Crackles on exam.• Findings c/w sarcoid: Uveitis, skin rash, erythema nodosum, hepatomegaly.
• Findings c/w CVD: Synovitis, rash, sclerodactaly.
• Findings c/w IPF: Clubbing

CXR is Not Useful for Differentiating ILD’s
HP
CVD-ILD
IPF
NSIP

High‐resolution CT (HRCT)
1‐1.5 mm collimation
Images taken every 10 mm
Supine, prone and expiratory images

HRCT is the Key to Diagnosing ILD’s
• Pattern of abnormality on HRCT scan may suggest a specific ILD.
• HRCT findings guide subsequent diagnostic tests.
• HRCT findings may be sufficient for diagnosis.

Usual Interstitial Pneumonia (UIP)
• Irregular lines in a patchy, basilar, subpleural distribution
• Traction bronchiectasis
• minimal Ground glass opacities.
• Honeycomb lung

Nonspecific Interstitial Pneumonitis (NSIP)
• Ground glass opacities (100%)• Consolidation (98%)• Nodules (96%)• Traction bronchiectasis (95%)• Intralobular reticulation (87%)• Lower lobe predominance

Desquamative Interstitial Pneumonia (DIP)
•Ground glass opacity with a basilar, subpleural, and lower lobe distribution
•Lower lobe reticular opacities

Hypersensitivity Pneumonitis
•Subacute phase :multifocal or diffuse GGO poorly definedcentrilobular nodules
•Subacute and chronic phases : mosaic perfusionair trapping on expiratory
images
•CT may be normal in some cases

Sarcoidosis
• Perilymphatic nodules• Peribronchial nodules• GGO• Upper lobe predominant,+/- fibrosis

Diagnostic AlgorithmSuspected PF
HRCTDetailed history,PE +
Non-diagnosticDiagnostic
Lung biopsy
1. IPF2. Sarcoidosis3. CV-ILD4. Hypersensitivity
pneumonitis5. Rare disease
(LAM, PAP)
PFTs/Labs+

1 2 3 4 50
0.10.20.30.40.50.60.70.80.91.0
Modified from: Flaherty KR, et al. Am J Respir Crit Care Med. 2004;170:904-910.
Agr
eem
ent(κ)
Step
Multidisciplinary approach
Step Assessment Method
Information Provided
1 Individual HRCT
2 Individual HRCT, clinical data
3Discussion
(clinician and radiologist)
HRCT, clinical data
4
Individual (clinician,
radiologist and pathologist)
HRCT, clinical data, SLB
5 Discussion HRCT, clinical data, SLB
• Agreement increased with multidisciplinary approach

Case 1

Case 1
• 57 year old man
• Abnormal CXR 3 months prior to presentation (notes “normal” CXR from 5 years ago)
• Mild dyspnea on exertion, no cough
• PMH: GERD for 30 years
• Meds: omeprazole 40mg daily

Case 1
• Social: lifetime non‐smoker, some mold in home, pharmacist
• Family: no history of ILD
• 114/73 hr 70 rr 16 96% RA (93% walking)• Dry inspiratory crackles at both bases• Normal cardiac examination• No clubbing, joint deformities, rashes

Case 1
• PFTs– FVC 5.10 (83%)
– FEV1 4.42 (90%)
– FEV1/FVC 0.87
– TLC 7.40 (88%)
– DLCO 23.41 (57%)

CXR

What additional testing would you perform next in this patient?
1. Bronchoalveolar lavage (BAL)
2. BAL and transbronchial biopsy
3. Serological evaluation
4. High resolution CT scan
5. Surgical lung biopsy
6. No additional testing; diagnosis is clear

HRCT

HRCT

HRCT

HRCT

HRCT

HRCT

HRCT

Serological evaluation
• ANA negative
• RF = 4

What additional testing would you perform next in this patient?
1. Bronchoalveolar lavage (BAL)
2. BAL and transbronchial biopsy
3. Surgical lung biopsy
4. No additional testing; diagnosis is clear
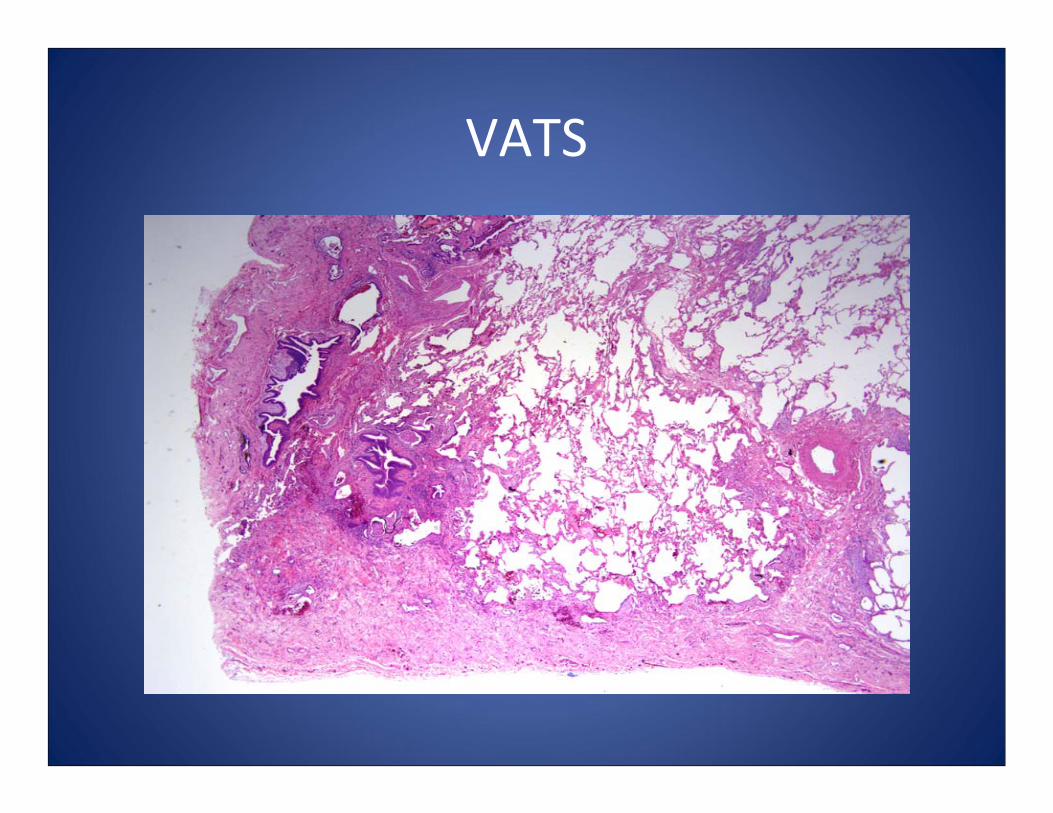
VATS

VATS

Usual Interstitial Pneumonia (UIP)
• Temporal heterogeneity– Subpleural accentuation of fibrosis
– Regions of normal lung
• Microscopic honeycombing
• Fibroblast Foci

Diagnosis of IPF
Management
• Enrolled in clinical trial
• Pulmonary rehabilitation
• Weight loss (if overweight)
• Lung transplant referral

• “A specific form of chronic fibrosing interstitial pneumonia limited to the lung and associated with the histologic appearance of usual interstitial pneumonia on surgical lung biopsy.”
ATS/ERS. Am J Respir Crit Care Med. 2000;161:646-664.
IPF: Published Definition

• Median survival for IPF is 2–3 years
• No proven therapy
Modified from Bjoraker JA. Am J Respir Crit Care Med. 1998;157:199-203.
IPF
Survival

Case 2

Case 2
• 63‐year‐old woman
• 5‐month history of shortness of breath and nonproductive cough
• PMH: hypertension, treated for TB exposure in 1980, arthritis
• Medications: diltiazem

Case 2
• Social: former smoker (18 pk/yrs); office worker.
• Family: No history of ILD
• 135/80 hr 90 rr 14 94% RA (90% walking)• Dry inspiratory crackles at both bases• Normal cardiac examination• No clubbing, joint deformities, rashes

CXR

What additional testing would you perform next in this patient?
1. Bronchoalveolar lavage (BAL)
2. BAL and transbronchial biopsy
3. Serological evaluation
4. High resolution CT scan
5. Surgical lung biopsy
6. No additional testing; diagnosis is clear

HRCT

HRCT

HRCT

HRCT

HRCT

HRCT

Serological evaluation
• ANA 1:80, speckled
• RF = 18, cyclic citrullinated antibody (CCP) negative

What additional testing would you perform next in this patient?
1. Bronchoalveolar lavage (BAL)
2. BAL and transbronchial biopsy
3. Surgical lung biopsy
4. No additional testing; diagnosis is clear

VATS

VATS

VATS

Nonspecific Interstitial Pneumonitis (NSIP)
• Uniform involvement of the lung with– Septal thickening
– Interstitial inflammation (lymphocytes)
– +/‐ Fibrosis

What additional testing would you perform next in this patient?
1. Bronchoalveolar lavage (BAL)
2. BAL and transbronchial biopsy
3. Additional serologies
4. No additional testing; diagnosis is clear

Additional serologies
• RNP negative
• Scl70 negative
• SSA, SSB negative
• Jo‐1 negative, CPK 104

Diagnosis of NSIP
Management
• Treated with prednisone and mycophenolate (CellCept)
• Pulmonary rehabilitation

• Distinguishing NSIP from UIP is a challenge!– Patients usually younger, more likely to be women
– Honeycombing on HRCT is uncommon in NSIP
– Surgical biopsy shows diffuse thickening of alveolar septae and few if any fibroblast foci
NSIP

IPF NSIP

IPF NSIP

IPF NSIP

• The diagnosis of NSIP should prompt you to go back to look for an etiology
– Occult connective tissue disease
– Drug reaction
– Hypersensitivity pneumonitis
NSIP

Case 3

Case 3
• 43 year old man
• Subacute progressive dyspnea
• PMH: mild obstructive sleep apnea on CPAP 6 cm H20, seasonal allergies
• Meds: cetirizine , multivitamin

Case 3
• Social: non‐smoker, banker, no known exposures, no pets.
• Family: no history of ILD
• BP 116/56, hr 60, rr16, 98% RA (88% walking)• Moderately obese• Lungs clear to auscultation

Case 3
• PFTs:– FVC 3.17 (73%)
– FEV1 2.43 (77%)
– FEV1/FVC 0.77
– TLC 4.65 (82%)
– DLCO 15.1 (58%)

CXR

What additional testing would you perform next in this patient?
1. Bronchoalveolar lavage (BAL)
2. BAL and transbronchial biopsy
3. Echocardiogram
4. High resolution CT scan
5. Surgical lung biopsy
6. No additional testing; diagnosis is clear

HRCT

HRCT

HRCT

HRCT

HRCT

HRCT

HRCT – expiratory views

HRCT – expiratory views

HRCT – expiratory views

Serological Evaluation
• ANA negative
• RF 12
• SS‐A, SS‐B negative

What additional testing would you perform next in this patient?
1. Bronchoalveolar lavage (BAL)
2. BAL and transbronchial biopsy
3. Surgical lung biopsy
4. No additional testing; diagnosis is clear

VATS Biopsy: Low Power

VATS Biopsy: High Power

VATS Biopsy: High Power

Hypersensitivity Pneumonitis
• Airwaycentric inflammation
• Poorly formed granuloma (giant cell)
• Areas of organizing pneumonia

What additional testing would you perform next in this patient?
1. Bronchoalveolar lavage (BAL)
2. Sputum culture
3. Serum precipitins
4. Additional history
5. No additional testing; diagnosis is clear

Additional history
• Patient recently moved to a new home built on the site of a former pigeon farm. There is ongoing construction of new units around his home and lots of dust.

Hypersensitivity Pneumonitis
Management
• Remove antigen (Relocated from new home)
• Treat with prednisone
• Pulmonary rehabilitation

Thank you!

Clinical Coordinator: (415) 353-8764Clinic fax: (415) 353-2568
http://www.ucsfhealth.org/adult/medical_services/pulmonary/ild/index.html
UCSF Interstitial Lung Disease Clinic