a randomized comparative study between neonatal …
TRANSCRIPT

A RANDOMIZED COMPARATIVE STUDY BETWEEN
NEONATAL OUTCOMES OF ECLAMPTIC MOTHERS
TREATED WITH LOW DOSE MAGNESIUM SULPHATE AND
STANDARD DOSE REGIMEN FOR MANAGEMENT OF
ECLAMPSIA IN MC GANN DISTRICT TEACHING HOSPITAL,
SHIVAMOGGA
By
Dr. Sriti Hegde
Post Graduate
Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Bengaluru,
Karnataka, in partial fulfillment of the requirements for the degree of
M.D. PHARMACOLOGY
Under the guidance of
Dr. Vedavathi H M.D.
Professor and Head
Department of Pharmacology
Shivamogga Institue of Medical Sciences
Shivamogga -577201
DEPARTMENT OF PHARMACOLOGY
SHIVAMOGGA INSTITUTE OF MEDICAL SCIENCES, SHIVAMOGGA
577201
2018

Scanned by CamScanner

Scanned by CamScanner

Scanned by CamScanner

Scanned by CamScanner

Acknowledgement
ACKNOWLEDGEMENT
Acknowledgement is made in an attempt to recognize the person’s contribution
towards the work. I whole heartedly thank all those people who have encouraged me
right from the conception of this work till its present form.
With humble gratitude and great respect, I would like to thank my beloved teacher
and guide, Dr.Vedavathi H M.D, Professor and Head of the Department of
Pharmacology, Shivamogga Institute of Medical Sciences, Shivamogga, for being a
source of inspiration. Her constant encouragement kept me active in the academics.
Her vast experience, simplicity, knowledge, supervision, guidance, constant
inspiration and valuable advices nurtured me in completing this study successfully. I
am deeply indebted and grateful to her.
I would like to express the deepest appreciation to my co-guide, Dr. Prashant
kumar H M.S OBG, Professor and Head, Department of Obstetrics and Gynaecology,
Shivamogga Institute of Medical Sciences, Shivamogga for encouraging me in
recruitment of the subjects, ensuring the completeness of work, rendering timely
suggestions, guiding me throughout this work with his fine clinical skills and
extensive experience.
I also thank Dr. Sreenivas P Revankar Associate professor and Dr. Nagaraja
Prasad S Associate professor Department of Pharmacology for healthy discussions
regarding my academics.
My cordial and humble thanks to Dr. Dharani Devangi R, Assistant Professor,
Department of Pharmacology, Shivamogga Institute of Medical Sciences,
Shivamogga, for her support, guidance and invaluable help at several times during
this work.

Acknowledgement
I also sincerely thank Dr.Shruthi SL and Dr. Anusha SJ, Tutors Department of
Pharmacology Shivamogga Institute of Medical Sciences, Shivamogga for their
constant support, advice and help which helped me to keep up my confidence in
completion of my work.
My sincere thanks to Dr. Anirudh, Department of Community Medicine,
Shivamogga Institute of Medical Sciences, Shivamogga, for her invaluable help and
effort in making me understand the statistical part of the thesis.
I extend my thanks to my senior post graduates Dr. Jean Lourdes Murray and
Dr. Harini Manjunath for always being there and lending a helping hand in
completion of my dissertation.
I also thank my fellow postgraduates Dr. Eshanu Shastry and Dr. Abhishek C P and
for helping me at peak times and making my dissertation a successful work.
I wish to thank the interns and staff of Department of Obstetrics and Gynaecology,
Shivamogga Institute of Medical Sciences, Shivamogga for their active involvement
in the collection of the data needed for my study.
I wish to thank the interns and staff of Department of Obstetrics and Gynaecology,
Shivamogga Institute of Medical Sciences, Shivamogga for their active involvement
in the collection of the data needed for my study.
I thank DR. Lepakshi B G M.S OBG, Director, for giving me an opportunity to
undertake the present study.
I also thank Shankar G C laboratory technician, Rajesh clerk, Ranganath, Rajeshwari,
Madhusudan Raghavendra and Vinodamma non-teaching staff of the department of
Pharmacology, Shivamogga Institute of Medical Sciences, Shivamogga for their help
and co-operation rendered during my entire study period.

Acknowledgement
I am also thankful to my husband Vinayak Hegde for always believing
me and supporting me in my academics. My heartfelt thanks to my parents
Mahabaleshwar Hegde and Veena Hegde for encouraging me in my studies,
without whom it would be impossible in completion of my post graduation.
I am thankful to all my patients for participating in my study without them this
dissertation study would not have been possible and I wish them a long life and good
health.
Date: 25-11-2017 Signature of the Candidate
Place: Shivamogga Name: DR. SRITI HEGDE

ABBREVATIONS
ARM Artificial rupture of membrane
AST Asparatate
BMI Body mass index
CAT Computerized axial tomography
CNS Central nervous system
CVP Central venous pressure
DTR Deep tenodon reflexes
DBP Diastolic blood pressure
DIC Disseminated intravascular coagulation
ECG Electrocardiography
EEG Electroencephalogram
EGTA Ethylene glycol
GFR Glomerular filteration rate
HELLP Hemolysis and elevate liver enzymes and low platelet count
HR Heart rate
IL Interleukins
IM Intramuscular
IUFD Intrauterine foetal death
IUGR Intrauterine growth retardation
IV Intravenous
LBW Low birth weight
LFT Liver function test
MgSO4 Magnesium sulphate

MRI Magnetic resonance imaging
NICU Neonatal intensive care unit
NMDA N-methyl-d-asparatate
NO Nitrous oxide
O2 Oxygen
OBG Obstetrics and Gynaecology
PGI2 Prostacyclin
RCOG Royal college of Gyanaecologists
RFT Renal function test
ROS Reactive oxygen species
SBP Systolic blood pressure
SIMS Shivamogga Institute of Medical Science
TNF Tumor necrosis factor
TXA2 Thromboxane
VLBW Very low birth weight
WHO World health organization

LIST OF TABLES USED
SL. NO.
TABLES
PAGE
NO.
1. Risk factors and etiopathological factors for eclampsia 16
2. Pathophysiology and oragan dysfunctions in eclampsia 20
3. The principles of management of eclampsia 22
4. Intramuscular regimen for management of eclampsia 24
5. Maternal complications of eclampsia 28
6. Regimens of magnesium sulphate for the management of
eclampsia
37
7. Randomized control trial of magnesium sulphate with
another anticonvulsants to prevent recurrent eclamptic
convulsions
41
8. Selective vs universal magnesium sulphate prophylaxis 43
9. Representation of age distribution of eclamptic mothers
in both groups
61
10. Representation of distribution of parity among eclamptic
mothers in both groups
63
11. Representation of distribution of eclamptic mothers who
received antenatal care in both groups
65
12. Representation of distribution of eclamptic mothers from
different areas among both groups
67
13. Representation of distribution of gestational age among
eclamptic mothers in both groups
69
14. Representation of distribution of body mass index among
eclamptic mothers in both groups
71
15. Representation of systolic blood pressure distribution
among eclamptic mothers in both groups
73
16. Representation of diastolic blood pressure distribution 75

among eclamptic mothers in both groups
17. Representation of distribution of no. of episodes if
seizures before the start of treatment in eclamptic
mothers among both groups
77
18. Representation of distribution of mode of delivery among
eclamptic mothers in both groups
79
19. Representation of birth weight distribution in neonates of
eclamptic mothers among both groups
81
20. Representation of distribution cord blood magnesium at
the time of delivery among neonates of eclamptic
mothers in both groups
83
21. Representation of distribution of APGAR scores at 5min
among the neonates of eclamptic mothers in both groups
85
22. Representation of NICU care requirement among the
neonates of eclamptic mothers in both groups
87
23. Representation of incidence of respiratory distress among
the neonates of eclamptic mothers in both groups
89
24. Representation of incidence of hypotonia among the
neonates of eclamptic mothers in both groups
91
25. Representation of incidence of bradycardia among the
neonates of eclamptic mothers in both groups
92
26. Representation of serum blood magnesium at the time of
delivery among the neonates of eclamptic mothers in
both groups
93
27. Neonatal adverse events in both the groups 95
28. Maternal adverse events in both the groups 95

LIST OF FIGURES
SL.
NO. TITLE
PAGE
NO.
1. Bar diagram showing incidence of eclampsia over a decade
in India
9
2. Schematic representation of normal implantation and
defective implantation in preeclampsia and eclampsia
11
3. Schematic representation showing glomerular capillary
endotheliosis
12
4. Etiopathology of pre-eclampsia and eclampsia 13
5. Illustration showing location of cerebral haemorhages and
petechiae in women with eclampsia
15
6. Illustration of signs of eclampsia 18
7. Illustration showing extensive tongue injury following
eclamptic convulsion.
25
8. Illustration of structure of magnesium sulphate 30
9. Illustration of mechanism of action of magnesium sulphate
on myometrial cell
31
10. Comparing of serum magnesium levels in mEq/L following
intravenous and intramuscular regimens
38
11. Flow chart representing the recruitment of the patient in the study 60
12. Graphical representation of distribution of age of eclamptic
mothers among both the groups
62
13. Graphical representation of parity distribution among eclamptic
mothers among both the groups
64
14. Graphical representation of distribution of antenatal care received
between both the groups
66
15. Graphical representation of distribution of eclamptic mothers in
rural and urban areas among both the groups
68
16. Graphical representation of distribution of gestational age in
weeks of eclamptic mothers among both the groups
70
17. Graphical representation of BMI distribution of eclamptic mothers
among both the groups
72
18. Graphical representation of distribution of systolic blood pressure
of eclamptic mothers among both the groups
74
19. Graphical representation of distribution of diastolic blood pressure
in eclamptic mothers among both the groups
76
20. Graphical representation of distribution of number of convulsions
in eclamptic mothers among both the groups
78
21. Graphical representation of distribution of mode of delivery in
eclamptic mothers among both the groups
80
22. Graphical representation of distribution of birth weight in neonates
of eclamptic mothers among both the groups
82
23. Graphical representation (line diagram)of distribution of cord
blood magnesium level at the time of delivery in neonates of
eclamptic mothers among both the groups
84
24. Graphical representation of distribution of APGAR scores among
the neonates of eclamptic mothers among both the groups
86
25. Graphical representation (line diagram) correlation of cord blood
magnesium level and APGAR scores in neonates of eclamptic
mothers in both the groups
86
26. Graphical representation of distribution of NICU care requirement
in neonates of eclamptic mothers among both the groups
88

27. Graphical representation (scatter plot) correlation of cord
blood magnesium level and NICU care requirement in
neonates of eclamptic mothers among both the groups
88
28. Graphical representation of distribution of incidence of respiratory
distress in neonates of eclamptic mothers among both the groups
90
29. Graphical representation (box plot) of distribution of incidence of
respiratory distress in neonates of eclamptic mothers among both
the groups
90
30. Graphical representation of distribution of incidence of hypotonia
in neonates of eclamptic mothers among both the groups
91
31. Graphical representation of distribution of incidence of
bradycardia in neonates of eclamptic mothers among both the
groups
92
32. Graphical representation (line diagram) of distribution of serum
magnesium levels of eclamptic mothers among both the groups
94
33. Graphical representation of distribution of adverse events among
both the groups
97
34. Graphical representation (line diagram) correlation of serum
magnesium level and adverse events in eclamptic mothers among
both the groups
98
35. Graphical representation (line diagram) correlation of serum
magnesium level and adverse events in eclamptic mothers among
both the groups
98
1
ABSTRACT
BACKGROUND AND OBJECTIVE - Eclampsia is one of the preventable cause of
maternal and neonatal mortality. Magnesium sulphate is the drug of choice to control
the convulsions and prevent them. The toxic effects of magnesium sulphate like
decreased urinary output and aspiration pneumonia has discouraged many primary
and secondary health centres to use the drug. Considering the low body mass index of
women in developing countries, the use of low dose magnesium sulphate regimen
may improve the safety profile of magnesium sulphate. The objective of this study is
to compare the neonatal outcome in eclamptic mothers treated with Low-dose
magnesium sulphate regimen and Standard dose magnesium sulphate regimen.
MATERIALS AND METHODS - This is a randomised prospective open labelled
comparative study between the neonates of eclamptic mothers treated with Low dose
magnesium sulphate regimen and Standard dose magnesium sulphate regimen. The
study included 100 patients with eclampsia and divided into two groups, where group
A received low dose magnesium sulphate regimen and group B received standard
regimen. Maternal and cord blood magnesium sulphate was measured. Neonatal
outcomes of all the eclamptic patients were recorded. Maternal complications was
also assessed.
RESULTS - In this present study, NICU care was required for 28(56%) neonates in
standard regimen group compared to 8(16%) neonates in low dose regimen group.
Bradycardia and Hypotonia was significantly increased in neonates of standard
regimen group (p<0.05). APGAR scores decreased with increase in cord blood
magnesium levels. Recurrence of seizure was seen in 10% of cases in low dose

2
regimen group compared to 5% in standard dose regimen group. There was no
maternal mortality.
CONCLUSION - Neonatal complication are significantly related to increasing serum
magnesium level. Low dose magnesium sulphate regimen showed better neonatal
outcome compared to Standard dose magnesium sulphate regimen. It also showed
effective seizure control in eclamptic mothers without significant seizure recurrence.
Hence, the low-dose magnesium sulphate regimen was found to be safe in
themanagement of eclamptic mothers, without toxicity to their neonates.
KEYWORDS - Low dose magnesium sulphate regimen; Eclampsia; Neonatal
outcome

TITLE - "A randomized comparative study between neonatal outcome of
eclamptic mothers treated with low dose magnesium sulphate and standard dose
regimen for management of eclampsia in McGann teaching district hospital,
Shivamogga"
INTRODUCTION
Eclampsia is an important cause of maternal and perinatal morbidity and mortality
worldwide. Incidence in developing countries is 1 in 500 deliveries. Perinatal
mortality rate in neonates of eclamptic mothers is 30 to 50% in India.1
Magnesium sulphate is anticonvulsant drug of choice for both prevention and
treatment of eclampsia.2 Magnesium causes cerebral vasodilatation and reduction of
cerebral ischemia by calcium antagonism and relaxation of smooth muscles. Also it
has its action on peripheral vasculature and uterus.2
Dose related toxicity of magnesium sulphate is a concern. Potential hazards include
maternal hypotension, respiratory depression, respiratory arrest and decreased tendon
reflexes, decreased urinary output.3
A significant percentage of perinatal and early neonatal morbidity and mortality is
attributed to magnesium toxicity like increased still birth early neonatal death, birth
asphyxia, bradycardia, hypotonia, hyporeflexia, gastrointestinal hypomotility and
meconium plug syndrome.4 Experience with Pritchard’s magnesium sulphate regimen
showed all the above mentioned multiple toxicity and needed dose omission.
Adoption of this treatment in primary and secondary level hospital has been delayed
due to fear of toxicity of drug linked to high serum magnesium levels and can be life
threatening to both mother and neonate.5
3

Previously, no dose adjustment of magnesium sulphate were made for maternal
weight even though maternal weight is very low in low income countries than high
income ones (i.e 65kg vs 45kg).6 So low dose regimens have been described
principally due to lower BMI of Indian women and concerns about toxicity in
circumstances where facility for measurement of serum magnesium levels are not
available.7
In this study we used Bankura regimen of low dose magnesium sulphate for
administration because study with this regimen showed efficacy similar to standard
Pritchard regimen with reduced maternal and perinatal mortality.6
Normal serum concentrations of magnesium for adults are 0.75-1.25 mmol/L.
Therapeutic magnesium serum concentration recommended for the treatment of
eclamptic convulsions are 1.5-3.5mmol/L, which can be obtained by both the low
dose and standard dose regimen.7,8
Monalisa Das et al, observed the serum magnesium levels and its outcome in neonates
of eclamptic mothers treated with low dose magnesium sulphate regimen. In this cross
sectional observational study on eclampsia patients and their neonates, loading dose
and maintenance doses of magnesium sulphate were administered to eclampsia
patients by combination of intravenous and intramuscular routes. Maternal serum and
cord blood magnesium levels were estimated. Neonatal outcome was assessed.
APGAR scores decreased with increase in cord blood magnesium levels and
increasing dose of magnesium sulphate. Also other parameters like hypotonia, birth
asphyxia, intubation in delivery room, NICU care requirement were increased with
increasing dose of magnesium sulphate.6
4

Latika Sahu et al, compared low dose magnesium sulphate and standard dose regimen
for management of eclampsia. In this prospective randomized study involving two
groups of patient with eclampsia receiving either low dose group or standard
dose/control group magnesium sulphate regimen. Convulsions were controlled in 96%
of eclampsia cases with low dose magnesium sulphate regimen. There was no
maternal mortality.7
Ruchira Nautiyal et al, compared low dose magnesium sulphate regimen with
Pritchard’s regimen for eclampsia. In this prospective cross sectional study, patients
were divided into two groups. Group A received low dose magnesium sulphate
regimen group B were managed with pritchard regimen of magnesium sulphate. The
recurrence of fits, toxicity profile and feto-maternal outcome was studied. Low dose
regimen was equally effective in controlling the seizures. Incidence of loss of deep
tendon reflex compared with standard dose. Mean values of serum magnesium in both
the groups was comparable.8
Mina Abbasi Ghanavati et al, observed Neonatal effects of magnesium sulphate given
to mother. In this retrospective cohort analysis of women who received magnesium
sulphate for prevention or treatment of eclampsia magnesium sulphate was given
intravenously 6gm dose, followed by 3gm/hour infusion. The neonates were
diagnosed with hypotonia lower APGAR scores, intubation in delivery room,
admission to special nursery care, and hypotonia were all significantly increased as
maternal serum magnesium concentrations increased before birth.9
Jana N et al , studied low dose magnesium sulphate regimen for the management of
eclampsia over a decade in Indian women. A low dose of magnesium sulphate of 3gm
intravenously and 5gm intramuscularly, followed by 2.5gm intramuscularly every 4
5
hours, for 24 hours beyond the last seizure. Second phase of the study included
retrospective analysis of eclamptic mothers treated by same regimen at the same
hospital. The low dose regimen was associated with a lower seizure recurrence and
slightly lower maternal mortality compared with collaborative eclampsia trial.10
Nassar AH et al, observed adverse maternal and neonatal outcome of prolonged
course of magnesium sulphate tocolysis. They found neonatal magnesium level was
significantly higher in cases and also abnormal bone mineralization was encountered.
Maternal morbidity rate was higher with prolonged intake of tocolytic magnesium
regimen.11
Begum R et al observed low dose Dhaka magnesium regimen for eclampsia. In this
cross sectional observation study on eclampsia convulsions were controlled in 97% of
eclampsia cases and toxicity profile was less among the Dhaka regimen group
compared with standard dose.12
Neonatal outcome of low dose magnesium sulphate has rarely been studied. So we
tried to find the safety of same. Prior studies were observational studies and have not
included all the parameters which we have included in the present study, also did not
consider the correlation with serum magnesium levels. This type of study has not been
done in this region. So we tried to find the efficacy of this low dose regimen which
can be tried in our institution and also can be informed to nearby primary and
secondary centres to implement this regimen without fear of magnesium toxicity as in
standard Pritchard's regimen which can reduce the complications of eclampsia
reaching our tertiary level hospital.
6

7
OBJECTIVES
1. To compare the neonatal outcome in eclamptic mothers treated with low-dose
magnesium sulphate regimen and standard dose magnesium sulphate regimen.
2. To determine the efficacy of low-dose magnesium sulphate regimen in
controlling and preventing the episodes of seizure.
3. To assess the maternal complications occurring due to magnesium sulphate
regimens.
4. To correlate the cord blood magnesium levels and the neonatal outcome in
eclamptic mothers.
5. To correlate the serum magnesium levels and the maternal complications in
patients of eclampsia.

8
REVIEW OF LITERATURE
Eclampsia is a multisystem disorder of unknown aetiology characterized by
development of hypertension to the extent of 140/90mmHg or more with proteinuria
after the 20th week in a previously normotensive a non proteinuric patient
complicated with generalised tonic-clonic convulsions and/coma. The basic
underlying pathology is endothelial dysfunction and vasospasm, affecting almost all
vessels, particularly those of uterus, kidney, placental bed and brain.13
EPIDEMOLOGY
Eclampsia is one of the leading causes of high maternal mortality and morbidity and
also high perinatal mortality. According to WHO, eclampsia is the cause of 12 per
cent of all maternal death globally. It accounts for 50,000 maternal deaths worldwide.
In India, reported incidence of eclampsia varies from 0.179 to 3.7 per cent. And
maternal mortality varies from 2.2 to 23 per cent of all eclamptic women. . The
estimated incidence of eclampsia in Western countries is 1 in 2000 to 3448
deliveries.14
Maternal mortality in eclampsia is very high in India and varies from 2 to 30 per cent,
much more in ruralbased hospital than in the urban counterpart. However, if treated
early and adequately, the mortality should be even less than 2 per cent.15
In India, incidence of eclampsia is high. Observation has shown that the situation is
remaining same over the decades, though in certain places reports show declining
incidence. It is observed that during the last 40 to 50 years, i.e., from 1976 to 2015
(January– February), the incidence of eclampsia in India has not changed. This trend
is evident from figure no 1. Maternal mortality from eclampsia is also remaining
highthroughout the ages.In 1982 maternal mortality was 14.12 to17.28 % and in 1992

9
it was 8.06; a death rate of 11.54% was reported in 2002. In 2010, maternalmortality
from eclampsia ranged from 2.2 to 9 %.19
Figure no 1 : Bar diagram showing incidence of eclampsia over a decade in India.
Courtesy Nobis P.N, HajongAnupama. Eclampsia in India Through the DecadesThe
Journal of Obstetrics and Gynecology of India 2016;66(1):172–176
Perinatal mortality too shows the same gloomy picture overthe decades. In 1984 the
reported figure of perinatal deathwas 45 %, in 1988 it was 32 %, in 2007 it was39.3 %
and in 2010 it ranged from 24.5 to 48 %.16
ETIOPATHOLOGY OF ECLAMPSIA
The term eclampsia is derived from a Greek word, meaning “like a flash of
lightening”. It may occur quiteabruptly, without any warning manifestations. In
majority (over 80%); however, the disease is preceded byfeatures of severe pre-
eclampsia. Pre-eclampsia when complicated with generalized tonic–clonic
convulsions and/or coma is calledeclampsia.2
The underlying pathology is endothelial dysfunction and intense vasospasm.

10
The responsible agent for endothelial dysfunction and vasospasm, still has not been
isolated precisely but it is certain that the origin is humoral.17
The following are the consideration -
• Increased circulating pressor substances.
• Increased sensitivity of the vascular system to normally circulating pressor
substances.
Trophoblast invasion and Uterine Vascular Changes : Normally, there is invasion
of the endovascular trophoblasts into the walls of the spiral arterioles of the
uteroplacental bed. In the first trimester (10-12 weeks) endovascular trophoblasts
invades up to decidual segments and in second trimester (16-18 weeks) another wave
of trophoblasts invades upto the myometrial segments. This process replaces the
endothelial lining and the muscular arterial wall by fibrinoid formation. The spiral
arterioles thereby become distended, tortuous, and funnel-shaped. This physiological
change transforms the spiral arterioles into a low resistance, low pressure, high flow
system. In eclampsia, there is failure of the second wave of endovascular trophoblast
migration and there is reduction of blood supply to the fetoplacental unit. Figure no 2
shows defective implantation characterized by inconsistence of spiral arteriolar wall
by extravilloustrophoblasts. This results in a small-caliber vessel with high resistance
flow. The magnitude ofdefective trophoblastic invasion is thought to correlate with
severity of the hypertensive disorder. Nelson and colleagues completed
placentalexamination in more than 1200 women with preeclampsia.
Theseinvestigators reported that vascular lesions including spiral arteriolenarrowing,
atherosis, and infarcts were more common in placentasfrom women diagnosed with
preeclampsia before 34 weeks.18,19

11
Figure no 2 : It is schematic representation of normal implantation and defective
implantation in preeclampsia and eclampsia.
Courtesy: Cunningham FG. Obstetrical complication: Hypertensived disorders. In:
Leveno K, editor. Williams Obstetrics 24th edition. New York: Mc Graw Hill
Education 2014: p 732
(1) There is an imbalance in different components of prostaglandins—relative or
absolute deficiency of vasodilator prostaglandin (PGI2) from vascular endothelium
and increased synthesis ofthromboxane (TXA2), a potent vasoconstrictor in platelets.
(2) There is increased vascular sensitivity to thepressor agent angiotensin-II.
Angiotensinase activity is depressed, following proteinuria with elimination of α2
globulin.
(3) Nitric oxide (NO): It is synthesized in the vascular endotheliumand
syncytiotrophoblast from L-arginine. It significantly relaxes vascular smooth muscle,
inhibits plateletaggregation and prevents intervillous thrombosis.Deficiency of nitric
oxide contributes to the development ofhypertension.
spiral arteries

12
(4) Endothelin-1 is synthesized by endothelial cells, and it is a potent vasoconstrictor
compared to angiotensin-II. Endothelin-1 also contributes to the cause of
hypertension.
(5) Inflammatory mediators:Cytokines [tumour necrosis factor (TNF-α),
interleukins (IL-6) and others] derived from activated leukocytes cause endothelial
injury
(6) Abnormal lipid metabolism—results in more oxidative stress. Lipid peroxides,
reactive oxygen species (ROS) and superoxide anion radicals — cause endothelial
injury and dysfunction. Platelet and neutrophil activation, cytokines,
superoxideradical production and endothelial damage are in a vicious cycle.
(7) Others—mutation of factor V Leiden increases the risk.20
Figure no 3: Schemation showing glomerular capillary endotheliosis.
Courtesy: Cunningham FG. Obstetrical complication: Hypertensived disorders. In:
Leveno K, editor. Williams Obstetrics 24th edition. New York: Mc Graw Hill
Education 2014: p 732

13
EDEMA: The cause of excessive accumulation of fluids in the extracellular tissue
spaces is not clear. Probableexplanations are: Increased oxidative stress → endothelial
injury → increased capillary permeability. On thisbasis, the leaky capillaries and
decreased blood osmotic pressure are the probable explanations.
PROTEINURIA: The probable chain of events is as follows. Spasm of the afferent
glomerular arterioles →anoxic change to the endothelium of the glomerular tuft →
glomerular endotheliosis→ increased capillarypermeability → increased leakage of
proteins. Tubular reabsorption is simultaneously depressed. Albuminconstitutes 50–
60% and alpha globulin constitutes 10–15% of the total proteins excreted in the
urine.21
Figure no 4: Etiopathology of pre-eclamapsia and eclampsia.
Courtesy: Dutta DC. Hypertensive Disorders in Pregnancy. In: Konar H, editor. DC
Dutta’sText Book of Obstetrics. 8th ed. New Delhi: Jaypee Brothers Medical
Publishers(P) Ltd.; 2015. p. 268.

14
CEREBRAL PATHOLOGY:includes cortical or subcortical oedema, infarction and
haemorrhage. The neurological abnormalities areoften due to hypoxia, ischemia or
oedema. Several neurodiagnostic tests e.g. EEG, CAT, cerebral Doppler Velocimetry,
MRI, MRIangiography reveal presence of oedema and infarction. Findings are similar
to those as seen in hypertensive encephalopathy.Cerebral imaging is indicated when
there is focal neurologic deficits, prolonged coma, or atypical presentation for
eclampsia.13
CAUSE OF CONVULSION: The cause of cerebral irritation leading to convulsion is
not clear. The irritation may be provokedby:
(1) Anoxia — spasm of the cerebral vessels → increased cerebral vascular resistance
→ fall in cerebral oxygen consumption→ anoxia,
(2) Cerebral oedema — may contribute to irritation,
(3) Cerebral dysrhythmia — increases following anoxia oroedema. There is excessive
release of excitatory neurotransmitters (glutamate).

15
Figure no 5: Illustration showing location of cerebral haemorrhages and petechiae in
women with eclampsia.
Courtesy: Cunningham FG. Obstetrical complication: Hypertensived disorders. In:
Leveno K, editor. Williams Obstetrics 24th edition. New York: Mc Graw Hill
Education 2014: p 732
Pia Arachnoid

16
Table no 1: Risk factors and etiopathological factors for eclampsia.13
RISK FACTORS FOR ECLAMPSIA ETIOPATHOLOGICAL FACTORS
Primigravida: Young or elderly (first time
exposure to chorionic villi)
Failure of trophoblast invasion
(abnormal
Placentation)
Family history: Hypertension, pre-
eclampsia
Vascular endothelial damage
Placental abnormalities:
– Hyperplacentosis: Excessive exposure to
chorionicvilli—(molar pregnancy twins,
diabetes)
– Placental ischemia.
Inflammatory mediators (Cytokines)
Dietary deficiency or excess
Obesity: BMI >35 kg/m2, Insulin
resistance.
Immunological intolerance between
maternal andfoetal tissues
Pre-existing vascular disease Coagulation abnormalities
New paternity Increased oxygen free radicals
Thrombophilias(antiphospholipidsyndrome,
protein C, Sdeficiency, Factor V Leiden)
Genetic predisposition

17
CLINICAL FEATURES OF ECLAMPSIA
An eclamptic patient always shows previous manifestations of acute fulminating
pre-eclampsia — called premonitory symptoms.
ALARMING SYMPTOMS: The following are the ominous symptoms, which may
be evident either singly or incombination. These are usually associated with acute
onset of the syndrome.
(1) Headache — either locatedover the occipital or frontal region
(2) Disturbed sleep
(3) Diminished urinary output—Urinary output of lessthan 400 ml in 24 hours is very
ominous,
(4) Epigastric pain—acute pain in the epigastric region associated withvomiting, at
times coffee colour, is due to hemorrhagic gastritis or due to subcapsular haemorrhage
in the liver,
(5) Eye symptoms—there may be blurring, scotoma, dimness of vision or at times
complete blindness. Visionis usually regained within 4–6 weeks following delivery.
The eye symptoms are due to spasm of retinal vessels(retinal infarction), occipital
lobe damage (vasogenic oedema) or retinal detachment. Reattachment of the retina
occurs following subsidence of oedema and normalization of blood pressure after
delivery.22
SIGNS
1. Abnormal weight gain: Abnormal weight gain within a short span of time probably
appears even beforethe visible oedema. A rapid gain in weight of more than 5 lb a
month or more than 1 lb a week in later monthsof pregnancy is significant.

18
2. Rise of blood pressure: The rise of blood pressure is usually insidious but may be
abrupt. The diastolicpressure usually tends to rise first followed by the systolic
pressure.
Figure no 6 : Illustration of signs of eclampsia.
Courtesy:Dutta DC. Hypertensive Disorders in Pregnancy. In: Konar H, editor. DC
Dutta’sText Book of Obstetrics. 8th ed. New Delhi: Jaypee Brothers Medical
Publishers(P) Ltd.; 2015. p. 268.
3. Oedema: Visible oedema over the ankles on rising from the bed in the morning is
pathological. The oedemamay spread to other parts of the body in uncared cases
(Figno.6).
4. There is no manifestation of chronic cardiovascular or renal pathology.
5. Pulmonary oedema — due to leaky capillaries and low oncotic pressure.
6. Abdominal examination may reveal evidences of chronic placental insufficiency,
such as scanty liquoror growth retardation of the foetus.23
MARKED PEDAL OEDEMA MARKED VULVAL OEDEMA

19
Thus, the manifestations of pre-eclampsia usually appear in the following order—
rapid gain in weight →visible oedema and/or hypertension → proteinuria.
ECLAMPTIC CONVULSION OR FIT:The fits are epileptiform and consist of four
stages.
1.Premonitory stage: The patient becomes unconscious. There is twitching of the
muscles of the face,tongue, and limbs. Eyeballs roll or are turned to one side and
become fixed. This stage lasts for about 30 seconds.
2.Tonic stage: The whole body goes into a tonic spasm — the trunk-opisthotonus,
limbs are flexed andhands clenched. Respiration ceases and the tongue protrudes
between the teeth. Cyanosis appears. Eyeballsbecome fixed. This stage lasts for about
30 seconds.
3.Clonic stage: All the voluntary muscles undergo alternate contraction and
relaxation. The twitchings startin the face then involve one side of the extremities and
ultimately the whole body is involved in the convulsion.Biting of the tongue occurs.
Breathing is difficult and blood stained frothy secretions fill the mouth; cyanosis
gradually disappears. This stage lasts for 1–4 minutes.
4. Stage of coma: Following the fit, the patient passes on to the stage of coma. It may
last for a brief periodor in others deep coma persists till another convulsion. On
occasion, the patient appears to be in a confusedstate following the fit and fails to
remember the happenings.
Rarely, the coma occurs without prior convulsion.The fits are usually multiple,
recurring at varying intervals. When it occurs in quick succession, it is called

20
statuseclampticus. Following the convulsions, the temperature usually rises; pulse and
respiration rates areincreased and so also the blood pressure. The urinary output is
markedly diminished; proteinuria is pronounced,and the blood uric acid is raised.
CENTRAL NERVOUS SYSTEM ABNORMALITIES IN ECLAMPSIA
• Cerebral oedema
• Cerebral haemorrhage
• Posterior (parietal or occipital lobe) reversible encephalopathy syndrome
• Basal ganglia an brain stem lesion(rare)24
Table no 2: Pathophysiology and organ dysfunctions in eclampsia.2
ORGAN DYSFUNCTION IN PRE-ECLAMPSIA AND ECLAMPSIA
CARDIOVASCULAR
HAEMATOLOGICAL RENAL HEPATIC
Generalized vasospasm Plasma volume GFR Liver cell
damage
Peripheral vascular
resistance
Hemoconcentration Renal
plasma flow
Periportal
necrosis
CVP
Coagulation disorder Serum uric
acid
Subcapsular
haematoma
Pulmonary wedge
pressure
Blood viscosity

21
INVESTIGATIONS
Urine: Proteinuria is the last feature of pre-eclampsia to appear. It may be trace or at
times copious. There may be few hyaline casts, epithelial cells or even few red cells.
24 hours urine collection for protein measurement is done.
Ophthalmoscopic examination: In severe cases there may be retinal oedema,
constriction of the arterioles, alteration of normal ratio of vein: arteriole diameter
from 3 : 2 to 3 : 1 and nicking of the veins where crossed by the arterioles. There may
be haemorrhage.
Blood values: The blood changes are not specific and often inconsistent. A serum uric
acid level (biochemical marker of pre-eclampsia)of more than 4.5 mg/dL indicates the
presence of pre-eclampsia. Blood urea level remainsnormal or slightly raised. Serum
creatinine level may be more than 1 mg/dL. There may be thrombocytopenia
and abnormal coagulation profile of varying degrees. Hepatic enzyme levels may be
increased.
Antenatal foetal monitoring: Antenatal foetal well being assessment is done by
clinical examination, dailyfoetal kick count, ultrasonography for foetal growth and
liquor pockets, cardiotocography, umbilical artery flowvelocimetry and biophysical
profile.25
MANAGEMENT
PREDICTION AND PREVENTION: In majority of cases, eclampsia is preceded by
severe pre-eclampsia. Thus theprevention of eclampsia rests on early detection and
effective institutional treatment with judicious terminationof pregnancy during pre-
eclampsia. However, eclampsia can occur bypassing the preeclamptic state and as

22
such, it is not always a preventable condition. Eclampsia may present in atypical
ways; hence, it is at timesdifficult to predict. Use of antihypertensive drugs,
prophylactic anticonvulsant therapy and timely deliveryare important steps. Close
monitoring during labour and 24 hours’ postpartum, are also important in prevention
ofeclampsia. Magpie trial showed prophylactic use of magnesium sulphate lowers the
risk of eclampsia.Unfortunately, 30–85 percent of cases of eclampsia remained
unpreventable.26
FIRST AID TREATMENT OUTSIDE THE HOSPITAL: The patient at home or in
the peripheral healthcentres should be shifted urgently to the tertiary referral care
hospitals.Transport of an eclamptic patient to a tertiary care centre is important.27
HOSPITAL—THE PRINCIPLES OF MANAGEMENT ARE:
Table no 3 - The principles of management.28
Maintain: airway, breathing and
circulation
Hemodynamic stabilization
(control BP)
Oxygen administration 8–10 L/min Organize the investigations
Arrest convulsions Deliver by 6-8 hours
Ventilator support Prevention of complication
Prevention of injury Post partum care

23
GENERAL MANAGEMENT
Supportive care:
(i) to prevent serious maternal injury from fall, (ii) prevent aspiration, (iii) to maintain
airway and (iv) to ensure oxygenation.
Patient is kept in a railed cot and a tongue blade is inserted between the teeth. She is
kept in the lateraldecubitus position to avoid aspiration. Vomitus and oral secretions
are removed by frequent suctioning,oxygenation is maintained through a face mask
(8–10 L/min) to prevent respiratory acidosis. Oxygenation ismonitored using a
transcutaneous pulse oximeter. Arterial blood gas analysis is needed when O2
saturationfalls below 92 percent. Sodium bicarbonate is given when the pH is below
7.10. The patient should have adoctor or at least a trained midwife for constant
supervision.29
Detailed history is to be taken from the relatives, relevant to the diagnosis of
eclampsia, duration ofpregnancy, number of fits and nature of medication
administered outside.
Examination: Once the patient is stabilized, a thorough but quick general, abdominal
and vaginalexaminations are made. A self-retaining catheter is introduced and the
urine is tested for protein. The continuousdrainage facilitates measurement of the
urinary output and periodic urine analysis.
Monitoring:Half hourly pulse, respiration rates and blood pressure are recorded.
Hourly urinary outputis to be noted. If undelivered, the uterus should be palpated at
regular intervals to detect the progress of labourand the foetal heart rate is to be
monitored. Immediately after a convulsion, foetal bradycardia is common.

24
Fluid balance: Crystalloid solution (Ringer’s solution) is started as a first choice.
Total fluids shouldnot exceed the previous 24 hours urinary output plus 1000 ml
(insensible loss through lungs and skin). Infusion of balanced salt solution should be
at the rate of1 ml/kg per hour. In pre-eclampsia and eclampsia although there is
hypovolemia, the tissues are over loaded. Anexcess of dextrose or crystalline
solutions should not be used as it will aggravate the tissue overload leadingto
pulmonary oedema and adult respiratory distress syndrome. CVP monitoring is
needed for a patient with severe hypertension and reduced urineoutput.
Antibiotic: To prevent infection, Ceftriaxone 1 gm IV twice daily is given.30
SPECIFIC MANAGEMENT:
Anticonvulsant and sedative regime: The aim is to control the fits and to preventits
recurrence.
Magnesium sulphate is the drug of choice. It acts as a membrane stabilizer and
neuroprotector. It reducesmotor endplate sensitivity to acetylcholine. Magnesium
blocks neuronal calcium influx also. It induces cerebralvasodilatation, dilates uterine
arteries, increases production of endothelial prostacyclin and inhibits platelet
activation. It has no detrimental effects on the neonate within therapeutic level. It has
got excellentresult with maternal mortality of 3%. It does not control hypertension.
Table no 4: Intramuscular regimen for management of eclampsia.31
REGIMEN LOADING DOSE MAINTAINANCE DOSE
Intramuscular (Pritchard) 4 gm IV over 3–5 min
followed by 10
gm deep IM (5 gm in each
buttock)
5 gm IM 4 hourly in
alternate buttock

25
Antihypertensives and diuretics: Inspite of anticonvulsant and sedative regime, if
the blood pressureremains more than 160/110 mm Hg, antihypertensive drugs should
be administered. Drugs commonly usedare parenteral, hydralazine, labetalol, calcium
channel blockers or nitroglycerin.
Presence of pulmonary oedema requires diuretics. In such cases, the potent one
(frusemide) should beadministered in doses of 20–40 mg intravenously and to be
repeated at intervals.
Management during fit: (a) In the premonitory stage, a mouth gag is placed in
between the teeth to preventtongue bite and should be removed after the clonic phase
is over. (b) The air passage is to be cleared off themucus with a mucus sucker. The
patient’s head is to be turned to one side and the pillow is taken off. Raisingthe
footend of the bed, facilitates postural drainage of theupper respiratory tract. (c)
Oxygen is given until cyanosisdisappears.32
Figure no 7: Extensive tongue injury following an eclamptic convulsion. It occurs in
clonic stage.
Courtesy:Dutta DC. Hypertensive Disorders in Pregnancy. In: Konar H, editor. DC
Dutta’sText Book of Obstetrics. 8th ed. New Delhi: Jaypee Brothers Medical
Publishers(P) Ltd.; 2015. p. 268

26
OBSTETRIC MANAGEMENT: During pregnancy: In majority of cases with
antepartum eclampsia, labour startsoon after convulsions. But when labour fails to
start, the management depends on—(i) whether the fits arecontrolled or not and (ii)
the maturity of the foetus. The decision to deliver is made once the woman is stable.
• Fits controlled:
Baby mature:Delivery should be done. (a) If the cervix is favourable and there is no
contraindication of vaginaldelivery, surgical induction by low rupture of the
membranes is done. Oxytocin drip may be added, if needed.
(b) When the cervix is unfavourable, cervical ripening with PGE2 gel or pessary
could be achieved before ARM. (c)If the cervix is unfavourable and/or there is
obstetric contraindication of vaginal delivery, caesarean section is done.
Baby premature(<37 weeks): Delivery is recommended in a set up with neonatal
intensive care unit (NICU).The underlying disease process of pre-eclampsiaeclampsia
persists until the woman delivers. At times thedisease process may flare up.
Moreover, there lies the risk of recurrent convulsions and IUFD. Steroid therapy is
given when pregnancy is less than 34 weeks. Conservative management at very early
pregnancymay improve perinatal outcome but this must be carefully balanced with
maternal well-being.
Baby dead: The preeclamptic process gradually subsides and eventually expulsion of
the baby occurs.Otherwise medical method of induction is started.
Fits not controlled: If the fits are not controlled with anticonvulsant within a
reasonable period (6–8 hours),termination of pregnancy should be done. If vaginal
examination indicates a quick response to induction, lowrupture of the membranes is

27
done. Oxytocin infusion may be added. The uterus responds well to oxytocin insuch
cases. In presence of unfavourable factors, caesarean section gives a quick response.
During labour:In the absence of any contraindication to vaginal delivery, as soon as
the labour is well established,low rupture of the membranes is to be done to accelerate
the labour. The dose schedule of antihypertensive andanticonvulsant drugs may be
increased to quieten the patient. Second stage should be curtailed by forceps,
ventouseor craniotomy, if the baby is dead. Prophylactic intravenous ergometrine or
syntometrine following the deliveryof the anterior shoulder should not be given as it
may produce further rise of blood pressure. Instead, 10 units ofoxytocin IM or IV
slowly should be given.
Indications of caesarean section: (i) Uncontrolled fits in spite of therapy. (ii)
Unconscious patient and poorprospect of vaginal delivery. (iii) Obstetric indications
Follow up and prognosis: Patient should be followed up in the postnatal clinic by 6
weeks time. Persistenceof hypertension, proteinuria and abnormal blood biochemistry
necessitates further investigationand consultation with a physician.
Recurrence risk varies between 2 and 25%. 33

28
COMPLICATIONS
Table no 5 - Maternal complications of eclampsia.2
Injuries -
Tongue bite, injuries due to fallfrom bed,
bed sore.
Pulmonary complications:
Oedema—due to leaky bloodcapillaries
Pneumonia—due to aspiration,hypostatic
or infective
Adult respiratory distress syndrome
Embolism
Hyperpyrexia
Cardiac—Acute left ventricularfailure
Renalfailure
Hepatic—necrosis, Subcapsular
hematoma
Cerebral:Oedema
(vasogenic)haemorrhage
Neurologicaldeficits
Disturbed vision: Due to
retinaldetachment or occipital
lobeischemia.
Hematological
Thrombocytopenia
Disseminated intravascular
Coagulopathy
Postpartum
Shock
Sepsis
Psychosis
PROGNOSIS
MATERNAL: Immediate: Once the convulsion occurs, the prognosis becomes
uncertain. Prognosis depends on many factors and the ominous features are:
(1) Long interval between the onset of fit and commencementof treatment (late
referral).
(2) Antepartum eclampsiaespecially with long delivery interval.
(3) Number offits more than 10.

29
(4) Coma in between fits.
(5) Temperature over 102°F with pulse rate above 120/minute.
(6)Blood pressure over 200 mm Hg systolic.
(7) Oliguria (< 400 mL/24 hours) with proteinuria > 5 gm/24 hours.
(8) Nonresponse to treatment.
(9) Jaundice.
Mortality:Maternal mortality in eclampsia is very high in India and varies from 2–
30%, much more in ruralbased hospital than in the urban counterpart. However, if
treated early and adequately, the mortality shouldbe even less than 2%.
Causes of maternal deaths: (1) Cardiac failure. (2) Pulmonary oedema(3) Aspiration
and/or septic pneumonia (4) Cerebral haemorrhage (5) Acute renal failure (6)
Cardiopulmonary arrest (7) Adult respiratory distress syndrome (ARDS) (8)
Pulmonary embolism (9) Postpartum shock (10) Puerperal sepsis.
Maternalcomplications are higher in antepartum eclampsia.
Remote: If the patient recovers from acute illness, she is likely to recover rapidly
within 2–3 weeks. Recurrenceof eclampsia in subsequent pregnancies is uncommon,
although chance of pre-eclampsia is about 30%.34
FETAL: The perinatal mortality is very high to the extent of about 30–50%. The
causes are: (1) Prematurity — spontaneous or induced, (2) Intrauterine asphyxia
due to placental insufficiency arising out of infarction,retroplacental haemorrhage and
spasm of uteroplacental vasculature, (3) Effects of the drugs used to
controlconvulsions, (4) Trauma during operative delivery.35

30
SPECIFIC PHARMACOTHERAPEUTIC MANAGEMENT OF ECLAMPSIA
MAGNESIUM SULPHATE
CHEMISTRY
Magnesium sulphate USP is MgSO4·7H2O and not simple MgSO4. It is heptahydrate
sulphate mineral epsomite (MgSO4.7H20), commonly called Epsom salt. It contains
8.12 mEqper 1 g. Molar mass is MgS04 heptahydrate is 246.47g/mol.36
The generic formula of Magnesium sulphate is
Figure no 8: Illustration of structure of magnesium sulphate.
BACKGROUND AND HISTORY
In 118 a farmer by the name of Henry Wicker at Epsom in England attempted to give
his cows water from a well. They refused to drink because bitter taste of the water.
However the farmer noticed that the water seemed to heal scratches and rashes.
Eventually it was recognized to be magnesium sulphate.
Joseph Black recognized magnesium as an element in 1755. It was isolated by Sir
Humphry Davy in 1808. The name magnesium comes from Magnesia, a district of
Greece were it was first found and to this present day a lot of magnesium ore is
present in the area.13
First used anecdotally for the control of eclamptic seizures in the early 1900s,
magnesium sulphate remains one of the most commonly used medications in obstetric
practice today. Over the past 95 years, there have been countless research studies

31
investigating the efficacy of magnesium sulphate for the management of eclampsia,
preeclampsia, preterm labour, and most recently for prevention of cerebral palsy.
MECHANISM OF ACTION
Some proposed mechanisms of action include:
(1) reduced presynaptic release of the neurotransmitter glutamate,
(2) Blockade of glutamatergicN-methyl-d-aspartate(NMDA) receptors,
(3) Potentiation of adenosine action,
(4)Improved calcium buffering by mitochondria, and
(5) Blockageof calcium entry via voltage-gated channels (Arango, 2006;Wang,
2012a).13
Magnesium sulphate acts as a membrane stabilizer and neuroprotector. It reduces
motor endplate sensitivity to acetylcholine. Magnesium blocks neuronal calcium
influx also.
Figure no 9: Illustration of Mechanism of action of Magnesium sulphate on
Myometrial cell.
Courtesy:Goodman, Louis S, 19.6-2000; Gilman, Alfred, 1908-1984;Hardman, JoelG
13th ed./ editor, Laurence L.Brunton; assosciate editors Bruce A. Chabner, The
pharmacological basis of Medicine.

32
PHARMACOLOGICAL ACTIONS
Central nervous system - It depresses CNS, blocks peripheral neuromuscular
transmission and hence produces anticonvulsant effects. It promotes movement of
calcium, potassium, and sodium in a out of cells and stabilizes excitable membranes.
It also decreases amount of acetylcholine released at end-plate by motor nerve
impulse. It induces cerebral vasodilatation.37
Cardiovascular system - Slows rate of SA node impulse formation in myocardium
and prolongs conduction time.Magnesiumdecreased systemic vascular resistance and
mean arterial pressure.At the same time, it increased cardiac output withoutevidence
of myocardial depression.
Uterus - It dilates uterine arteries, increases production of endothelial prostacyclin.
Blood - inhibits platelet activation.
Respiratory system - Bronchodilator
Gastrointestinal system - Promotes osmotic retention of fluid in colon, causing
distension and increased peristaltic activity, subsequently resulting in bowel
evacuation.38
PHARMACOKINETICS
Parenterally administered magnesium is cleared almost totally by renal excretion, and
magnesium intoxication is unusual when the glomerular filtration rate is normal or
only slightly decreased. Adequate urine output usually correlates with preserved
glomerular filtration rates. Magnesium excretion is not urine flow dependent, and
urinary volume per unit time does not, per se, predict renal function. Thus,

33
serumcreatinine levels must be measured to detect a decreased glomerularfiltration
rate.
Magnesium is cleared almost exclusively by renal excretion,the dosages described
will become excessive if glomerularfiltration is substantially decreased.
Protein bound - 30%
Extracellular distribution 1-2%.39
THERAPEUTIC EFFICACY- Eclamptic convulsions are almost always prevented
orarrested by plasma magnesium levels maintained at 4 to7 mEq/L, 4.8 to 8.4 mg/dL,
or 2.0 to 3.5 mmol/L.13
DRUG INTERACTION
Magnesium sulphate binds with tetracyclines like demeclocycline, doxycycline and
minocycline
Magnesium sulphate interacts with bisphosphonates
Magnesium sulphate interacts with levothyroxine
Magnesium sulphate interacts with fluoroquinolones
USES OTHER THAN ECLAMPSIA
1. Oral magnesium sulphate preparations is used as laxative or osmotic purgative.
2. Used in replacement therapy for hypomagnesimia
3. Magnesium sulphate is aantiarrhthmic agent for torsades de pointes in cardiac
arrest under the ECC guidelines and for managing quinidine-induced arrhythmias.
4. Used as a bronchodilator in severe exacerbations of asthma.
5. It is used in agriculture, food preparation, and aquariums.39

34

35
ADVERSE EFFECTS AND TOXICITY PROFILE
Patellar reflexes disappear when the plasma magnesium levelreaches 10 mEq/L—
about 12 mg/dL—presumably because ofa curariform action. This sign serves to warn
of impendingmagnesium toxicity.
When plasma levels rise above 10 mEq/L,breathing becomes weakened. At 12 mEq/L
or higher levels,respiratory paralysis and respiratory arrest follow.40,41
MAGNESIUM SULPHATE - TO CONTROL CONVULSIONS
In more severe cases of preeclampsia and in eclampsia, magnesium sulphate
administered parenterally is an effective anticonvulsant that avoids producing central
nervoussystem depression in either the mother or the infant.
It has no detrimental effects on the neonate within therapeutic level. It has got
excellent result with maternal mortality of 3%. It does not control hypertension.
It may begiven intravenously by continuous infusion or intramuscularly by
intermittent injections.42
DOSAGE REGIMEN
Continuous intravenous (IV) regimen
• Give 4- to 6-g loading dose of magnesium sulphate diluted in 100 mL of IV
fluid administered over 15–20 min
• Begin 2 g/hr in 100 mL of IV maintenance infusion. Some recommend 1 g/hr
• Monitor for magnesium toxicity:
• Assess deep tendon reflexes periodically

36
• Some measure serum magnesium level at 4–6 hr and adjust infusion to
maintain levels between 4 and 7 mEq/L (4.8to 8.4 mg/dL)
• Measure serum magnesium levels if serum creatinine ≥ 1.0 mg/dL
• Magnesium sulphate is discontinued 24 hr after delivery.34
Intermittent intramuscular regimen
• Give 4 g of magnesium sulphate (MgSO4·7H2O USP) as a 20% solution
intravenously at a rate not to exceed 1 g/min
• Follow promptly with 10 g of 50% magnesium sulphate solution, one half (5
g) injected deeply in the upper outerquadrant of each buttock through a 3-inch-
long 20-gauge needle. (Addition of 1.0 mL of 2% lidocaine
minimizesdiscomfort.)
• If convulsions persist after 15 min, give up to 2 g more intravenously as a
20% solution at a rate notto exceed 1 g/min.
• If the woman is large, up to 4 g may be given slowly
• Every 4 hr thereafter, give 5 g of a 50% solution of magnesium sulphate
injected deeply in the upper outer quadrant ofalternate buttocks, but only after
ensuring that:
• The patellar reflex is present,
• Respirations are not depressed, and
• Urine output the previous 4 hr exceeded 100 mL
• Magnesium sulphate is discontinued 24 hr after delivery.35
Becauselabour and delivery is a more likely time for convulsions todevelop, women
with preeclampsia-eclampsia usually aregiven magnesium sulphate during labour and
for 24 hourspostpartum.

37
Table no 6: Regimens of magnesium sulphate for the management of eclampsia.43
REGIMENS OF MGSO4 FOR THE MANAGEMENT OF SEVERE PRE-
ECLAMPSIA AND ECLAMPSIA
Other Regimens -
Dhaka regimen - The loading dose of magnesium sulphate 4gm IV in dilution and 3
gm IM in each buttock (10gms). Followed by a maintenance dose of 2.5gm
intramuscular every 4 hourly for 24 hours after administration of the first dose.
Padhar regimen - The loading dose of magnesium sulphate 4gm IV in dilution and
3gm IM in each buttock. Followed by a maintenance dose of 4g intramuscular every
4th hourly for 24 after administration of the first dose or till the delivery whichever
comes first.
Lytic cocktail regimen - Menon in India employed the regime using chlorpromazine,
phenargan and pethidine and has got satisfactory result with reduction of maternal
mortality to 2.2%
Lean regimen (Diazepam therapy) - Diazepam is used in initial dose of 40mg IV. A
further 40mg in 500ml in 5% dextrose is infused at 30 drops per min or adjusted as
per need. Maternal mortality rate using this regimen is 5%.
REGIMEN LOADING DOSE MAINTAINANCE
DOSE
INTRAMUSCULAR
(Pritchard)
4g IV over 3-5min
followed by 10g deep IM
(5g in each buttock)
5g IM 4 hourly in alternate
buttock
INTRAVENOUS
(Zuspan or Sibai)
4-6g IV over 15-20min 1-2gm/hr IV infusion

38
Phenytoin therapy - Phenytoin is also used to control convulsions. It is given by
slow IV with monitoring. Initial dose is 10mg/kg followed by 5mg/kg two hours
later.Thereafter 200mg is given orally after 12 hours and continued until 48hours after
delivery.44
Figure no 8: Comparision of serum magnesium levels in mEq/L following
intravenous and intramuscular regimen.
Courtesy :Sibai BM, Graham JM, McCubbin JH. A comparison of intravenous and
intramuscular magnesium sulfate regimens in preeclampsia. Am J ObstetGynecol
1984;150:728–33.
In only 5 of 245 women with eclampsia atParkland Hospital was it necessary to use
supplementaryanticonvulsant medication to control convulsions. For these, an
intravenous barbiturate is given slowly.Midazolam or lorazepam may be given in a
small single dose,but prolonged use is avoided because it is associated with ahigher
mortality rate.

39
Foetal and Neonatal Effects.
Magnesium administered parenterallypromptly crosses the placenta to achieve
equilibriumin foetal serum and less so in amniotic fluid.Levels in amniotic fluid
increase with duration of maternal infusion. Current evidence supports theview that
magnesium sulphate has small but significant effectson the foetal heart rate pattern—
specifically beat-to-beat variability. At high serum magnesium levels the CNS is
depressed, neonates have profound respiratory depression requiring mechanical
ventilation. It is also associated with failure to pass meconium (meconium plug
syndrome). Hallak and coworkerscompared an infusion ofmagnesium sulphate with a
saline infusion. These investigatorsreported that magnesium was associated with a
small and clinicallyinsignificant decrease in variability. Similarly, in a
retrospectivestudy, Duffy and associates reported a lowerheart rate baseline that was
within the normal range; decreasedvariability; and fewer prolonged decelerations.
They noted noadverse outcomes.45,46
Overall, maternal magnesium therapy appears safe forperinates. For example, a recent
MFMU Network study ofmore than 1500 exposed preterm neonates found no
associationbetween the need for neonatal resuscitation and cordblood magnesium
levels. Still, there area few neonatal adverse events associated with its use. In
aParkland Hospital study of 6654 mostly term exposed newborns,6 percent had
hypotonia.In addition, exposed neonates had lower 1 and 5minute APGAR scores, a
higher intubation rate, and more admissionsto the special care nursery. The study
showed that neonataldepression occurs only if there is severehypermagnesemia
atdelivery.Observational studies have suggested a protective effect ofmagnesium
against the development of cerebral palsy in verylow-birthweight infants. Nguyen and
colleagues expanded this possibility to include term newbornneuroprotection.They

40
performed a Cochrane Database review to compareterm neonatal outcomes with and
without exposure toperipartum magnesium therapy and reported that there
wereinsufficient data to draw conclusions. Several neonatal complications are
significantly related to increasing concentration of magnesium in maternal circulation.
Long-term useof magnesium, given for several days for tocolysis, has beenassociated
with neonatal osteopenia.47-49
Maternal Safety and Efficacy of Magnesium Sulphate.
The multinational Eclampsia Trial Collaborative Group study involved 1687 women
with eclampsia randomly allocated to different anticonvulsant regimens. In one
cohort, 453 women were randomly assigned to be given magnesium sulphate and
compared with 452 given diazepam. In a second cohort, 388 eclamptic women were
randomly assigned to be given magnesium sulphate and compared with 387 women
given phenytoin. The results of these and othercomparative studies that each enrolled
at least 50 women aresummarized in Table. In aggregate, magnesium sulphatetherapy
was associated with a significantly lower incidence ofrecurrent seizures compared
with women given an alternativeanticonvulsant - 9.7 versus 23 percent. Importantly,
thematernal death rate of 3.1 percent with magnesium sulphatewas significantly lower
than that of 4.9 percent for the otherregimens.
Magnesium safety and toxicity was recently reviewed by Smith and coworkers. In
more than 9500 treatedwomen, the overall rate of absent patellar tendon reflexes
was1.6 percent; respiratory depression 1.3 percent; and calciumgluconate
administration 0.2 percent. They reported only onematernal death due to magnesium
toxicity. Our anecdotalexperiences are similar—in the estimated 50 years of its use

41
inmore than 40,000 women, there has been only one maternaldeath from an
overdose.50
Table no 7: Randomised control trial of magnesium sulphate with another.51
anticonvulsants to prevent recurrent eclamptic convulsions.
STUDY Comparing
drug
Recurrent seizures
MgSO4 (%) Other drug
(%) RR (95%CI)
Crowther52
(1990)
Diazepam
5/24
7/27
0.80
(0.29-2.2)
Bhalla53 (1994) Lytic cocktail 1/45 11/45 0.09(0.1-0.68)
Eclampsia
Trial
Colloborative
group(1995)
Phenytoin
60/453 126/452 0.48
(0.36-0.63)
Diazepam 22/388 66/387 0.33
(0.21-0.53)
TOTAL 88/910
(9.7)
210/911
(23)
0.41
(0.32-0.51)
Who Should Be Given Magnesium Sulphate?
Magnesium will prevent proportionately more seizures in women with
correspondingly worse disease. As previously discussed,however, severity is difficult
to quantify, and thus itis difficult to decide which individual woman might
benefitmost from neuroprophylaxis. The 2013 Task Force recommends that women
with either eclampsia or severe preeclampsia should be given magnesium sulphate
prophylaxis.At the same time, however, the 2013 Task Force suggests thatall women
with “mild” preeclampsia do not need magnesiumsulphate neuroprophylaxis. The
conundrum is whether or not togive neuroprophylaxis to any of these women with
“nonsevere”gestational hypertension or preeclampsia.54
In many other countries, and principally following disseminationof the Magpie Trial
Collaboration Group studyresults, magnesium sulphate is now recommended for

42
womenwith severe preeclampsia. In some, however, debate continuesconcerning
whether therapy should be reserved for women whohave an eclamptic seizure. We are
of the opinion that eclamptic seizures are dangerous.Maternal mortality rates of up to
5 percent have been reported even in recent studies. Moreover, thereare substantially
increased perinatal mortality rates in both industrializedcountries and underdeveloped
ones. Finally, the possibility of adverse long-term neuropsychologicaland vision-
related sequel of eclampsia described byAukes, Postma, Wiegman, and
theircoworkers, have raised additionalconcerns that eclamptic seizures are not
“benign.”55
Selective versus Universal Magnesium Sulphate Prophylaxis
There is uncertainty around which women with non-severe gestational hypertension
should be given magnesium sulphate neuroprophylaxis. An opportunity to address
these questions was afforded by a change in our prophylaxis protocol for women
delivering at Parkland Hospital. Before this time, Lucas and associates had found that
the risk of eclampsia without magnesium prophylaxis was approximately 1 in 100 for
women with mild preeclampsia. Up until 2000, all women with gestational
hypertension were given magnesium prophylaxis intramuscularly as first described by
Pritchard in 1955. After 2000, we instituted a standardized protocol for intravenously
administered magnesium sulphate. At the same time, we also changed our practice of
universal seizure prophylaxis for all women with gestational hypertension toone of
selective prophylaxis given only to women who met ourcriteria for severe gestational
hypertension. These criteria, shown in Table, included women with ≥ 2+ proteinuria
measured by dipstick in a catheterized urine specimen. Following this protocol

43
change, 60 percent of 6518 women with gestational hypertension during a 4½-year
period were given magnesium sulphate neuroprophylaxis.56
Table no 8:Selective versus Universal MagnesiumSulphate Prophylaxis
Selective versus Universal MagnesiumSulphate Prophylaxis: Parkland
Hospital
Criteria to Define Severity of GestationalHypertension
In a woman with new-onset proteinuric hypertension,at least one of the
following criteria is required:
Systolic BP > 160mmHg
Diastolic BP >110mmHg
Proteinuria > 2+ dipstick in a catheterized specimen
Serum creatinine >1.2mg/dL
Platelet count < 100,000/uL
AST Elevated 2 times above upper limit of normal
response
Persistent headache or scotoma
Persistent mid epigastric or right-upper quadrant pain
The remaining 40 percent with nonsevere hypertension werenot treated, and of these,
27 women developed eclamptic seizures—1 in 92. The seizure rate was only 1 in 358
for 3935women with criteria for severe disease who were given magnesiumsulphate,
and thus these cases were treatment failures.To assess morbidity, outcomes in 87
eclamptic women werecompared with outcomes in all 6431 noneclamptic
hypertensivewomen. Although most maternal outcomes were similar,almost a fourth
of women with eclampsia who underwentemergent caesarean delivery required
general anaesthesia. This isa great concern because eclamptic women have

44
laryngotrachealoedema and are at a higher risk for failed intubation, gastric
acidaspiration. Neonatal outcomes were also a concernbecause the composite
morbidity which was significantly increased tenfold in eclamptic compared
withnoneclamptic women—12 versus 1 percent, respectively.Thus, if one uses the
Parkland criteria for nonsevere gestationalhypertension, about 1 of 100 such women
who are notgiven magnesium sulphate prophylaxis can be expected to have
aneclamptic seizure. A fourth of these women likely will requireemergent caesarean
delivery with attendant maternal and perinatalmorbidity and mortality from general
anaesthesia. From this, themajor question regarding management of nonsevere
gestational hypertension remains—whether it is acceptable to avoid
unnecessarytreatment of 99 women to risk eclampsia in one? Theanswer appears to be
yes as suggested by the 2013 Task Force.57
Management of Severe Hypertension
Dangerous hypertension can cause cerebrovascular haemorrhageand hypertensive
encephalopathy, and it can trigger eclampticconvulsions in women with preeclampsia.
Other complicationsinclude hypertensive afterload congestive heart failure and
placental abruption.Because of these sequel, the National High BloodPressure
Education Program Working Group (2000) and the2013 Task Force recommend
treatment to lower systolic pressuresto or below 160 mm Hg and diastolic pressures to
orbelow 110 mm Hg. Martin and associates (2005) reportedprovocative observations
that highlight the importance of treating systolic hypertension. They described 28
selectedwomen with severe preeclampsia who suffered an associatedstroke. Most of
these were haemorrhagic strokes - 93 percentand all women had systolic pressures >
160 mm Hgbefore suffering their stroke. By contrast, only 20 percent of these same

45
women had diastolic pressures > 110 mm Hg. Itseems likely that at least half of
serious haemorrhagic strokesassociated with preeclampsia are in women with chronic
hypertension. Long-standing hypertensionresults in development of Charcot-
Bouchard aneurysmsin the deep penetrating arteries of the lenticulostriate branchof
the middle cerebral arteries. These vessels supply the basalganglia, putamen,
thalamus, and adjacent deep white matter,as well as the pons and deep cerebellum.
These unique aneurysmalweakenings predispose these small arteries to ruptureduring
sudden hypertensive episodes.54
Antihypertensive Agents
Several drugs are available to rapidly lower dangerously elevatedblood pressure in
women with the gestational hypertensive disorders.The three most commonly
employed are hydralazine,labetalol, and nifedipine. For years, parenteral hydralazine
wasthe only one of these three available. But when parenteral labetalolwas later
introduced, it was considered to be equally effectivefor obstetrical use. Orally
administered nifedipine has sincethen gained some popularity as first-line treatment
for severegestational hypertension.
Hydralazine
This is probably still the most commonly used antihypertensiveagent for treatment of
women with severegestational hypertension. Hydralazine is administered
intravenouslywith a 5 mg initial dose, and this is followed by 5 to10mg doses at 15 to
20minute intervals until a satisfactory response is achieved. Some limit the total dose
to 30 mg per treatment cycle. The target response antepartumor intrapartum is a
decrease in diastolic blood pressure to 90 to110 mm Hg. Lower diastolic pressures

46
risk compromised placentalperfusion. Hydralazine has proven remarkably effective to
prevent cerebral haemorrhage. Its onset of action can be asrapid as 10 minutes.
Although repeated administration every15 to 20 minutes may theoretically lead to
undesirable hypotension,this has not been our experience when given in these5 to
10mg increments.At Parkland Hospital, between 5 and 10 percent of allwomen with
intrapartum hypertensive disorders are given aparenteral antihypertensive agent. Mo
As with any antihypertensive agent, the tendency to give alarger initial dose of
hydralazine if the blood pressure is highermust be avoided. The response to even 5 to
10mg doses cannotbe predicted by hypertension severity. Thus, protocolis to always
administer 5 mg as the initial dose.In some cases, this foetal response to
diminisheduterine perfusion may be confused with placental abruptionand may result
in unnecessary and potentially dangerous emergentcaesarean delivery.55
Labetalol
This effective intravenous antihypertensiveagent is an α1- and nonselective β blocker.
Some preferits use over hydralazine becauseof fewer side effect. 10mg intravenously
dose is given initially. If theblood pressure has not decreasedto the desirable level in
10 minutes,then 20 mg is given. The next 10 minute incremental dose is 40mg and is
followed by another40 mg if needed. If a salutaryresponse is not achieved, then
an80mg dose is given. Sibairecommends 20 to 40 mg every10 to 15 minutes as
needed anda maximum dose of 220 mg pertreatment cycle. The AmericanCollege of
Obstetricians andGynecologistsrecommends starting with a 20mgintravenous bolus. If
not effective within 10 minutes, this is followedby 40 mg, then 80 mg every 10
minutes. Administrationshould not exceed a 220mg total dose per treatment cycle.

47
Hydralazine versus Labetalol
Comparative studies of these two antihypertensive agents show equivalent results. In
an older trial, Mabie and colleagues compared intravenous hydralazine withlabetalol
for blood pressure control in 60 peripartum women.
Labetalol lowered blood pressure more rapidly, and associatedtachycardia was
minimal. However, hydralazine loweredmean arterial pressures to safe levels more
effectively. In a latertrial, Vigil-De Gracia and associates randomly assigned
200 severely hypertensive women intrapartum to be given either:
(1) Intravenous hydralazine—5 mg, which could be given every20 minutes and
repeated to a maximum of five doses, or
(2) Intravenous labetalol—20 mg initially, followed by 40 mgin 20 minutes and then
80 mg every 20 minutes if needed upto a maximum 300mg dose.
Maternal and neonatal outcomeswere similar. Hydralazine caused significantly more
maternaltachycardia and palpitations, whereas labetalol more frequentlycaused
maternal hypotension and bradycardia. Both drugs have been associated with a
reduced frequency of foetal heart rate accelerations.13
Nifedipine
This calcium-channel blocking agent has become popularbecause of its efficacy for
control of acute pregnancy-relatedhypertension. The Royal College of Obstetricians
and Gynaecologists recommenda 10mg initial oral dose to be repeated in 30 minutesif

48
necessary. Nifedipine given sublingually is no longer recommended. Randomized
trials that comparednifedipine withlabetalol found neither drug definitively superior to
the other.However, nifedipine lowered blood pressure more quickly.56
Other Antihypertensive Agents
A few other generally available antihypertensive agents have beentested in clinical
trials but are not widely used. Belfort and associates administered the calcium
antagonistverapamilby intravenous infusion at 5 to 10 mg per hour.Mean arterial
pressure was lowered by 20 percent. Belfort andcoworkers reported that
nimodipinegiven eitherby continuous infusion or orally was effective to lower
bloodpressure in women with severe preeclampsia. Bolte and colleaguesreported good
results in preeclampticwomen given intravenous ketanserin, a selective serotonergic
(5HT2A) receptor blocker. Nitroprussideor nitroglycerineis recommendedby some if
there is not optimal response to first-lineagents. With these latter two agents, foetal
cyanide toxicity maydevelop after 4 hours. There are experimental antihypertensive
drugs that maybecome useful for preeclampsia treatment. One is calcitoningene
related peptide (CGRP),a 37amino acid potent vasodilator.Another is antidigoxin
antibody Fab (DIF) directed against endogenous digitalis-like factors, also called
cardiotonic steroids.13
Diuretics
Potent loop diuretics can further compromise placental perfusion.Immediate effects
include depletion of intravascularvolume, which most often is already reduced
compared withthat of normal pregnancy. Therefore, before delivery,diuretics are not
used to lower blood pressure.

49
In a randomised control study by Bhattacharje N et al. evaluated the efficacy of
intravenous low-dose magnesium sulphate for the management of eclampsia. A total
of 144 women with eclampsia were divided into a study group and a control group of
72 women each. The study group received 0.75 g/h of magnesium sulphate
intravenously after a loading intravenous dose of 4g and the control group was given
the standard intramuscular regimen as advocated by Pritchard. The primary outcome
measure was recurrence rate of the seizures. The secondary outcome measures were
development of magnesium toxicity if any, and maternal and perinatal outcomes. The
difference in the incidence of fit recurrence was statistically insignificant when both
groups were compared (7.46% vs 8.57%, p = 0.939). The total dose of magnesium
sulphate was significantly lower in the intravenous group (p < 0.0001), in which no
patient developed magnesium toxicity. Low-dose intravenous magnesium sulphate
was found to be as effective as the standard intramuscular regimen, while maintaining
a high safety margin.56
A prospective randomized study by Sahu L et al. of fifty eclampsia cases, treated with
magnesium sulphate (25 each with low dose regime and Pritchard regime) was carried
out from October 2010 to January 2012 at MAMC & LNH, New Delhi, India. In the
study, convulsions were controlled in 96% of eclampsia cases with low dose
magnesium sulphate regimen. One case i.e. 4% had single episode of recurrence of
convulsion, which was controlled by giving additional drugs and shifted to standard
dose regimen. There was no maternal mortality. The maternal and perinatal morbidity
and mortality in the study were comparable to those of standard Pritchard’s regimen.
The study did not find a single case of magnesium related toxicity with low dose

51
METHODOLOGY
This is a prospective, interventional study conducted
• To compare the neonatal outcome in eclamptic mothers treated with low-dose
magnesium sulphate regimen and standard dose magnesium sulphate regimen,
and
• To determine the safety, efficacy and side effect profile of magnesium
sulphate regimens. Also to determine the predisposing risk factors associated
with eclampsia.
SOURCE OF DATA - This prospective study was conducted on patients
witheclampsia in the eclampsia ward of department of obstetrics and gynaecology at
MCGANN TEACHING DISTRICT HOSPITAL SIMS (Shivamogga institute of
medical sciences), SHIVAMOGGA.
STUDY DESIGN - This is a prospective randomised comparative open labelled
single centred study.
STUDY DURATION - This study was conducted for the duration of one year from
December 2016 to January 2018.
ETHICS CLEARANCE: Ethics clearance obtained from the IEC (Institutional
Ethics committee) With the ethics clearance Reference No: SIMS/IEC/272/2016-17
MATERIALS USED IN THE STUDY -
1) Injection magnesium sulphate 2 ml ampoule.

52
2) Automated clinical chemical analyzer - for the assessment of serum and cord
magnesium levels
3) Clinical examination kit - (knee hammer, stethoscope etc)
4) Standard case record form
INCLUSION CRITERIA
1. Mothers diagnosed with eclampsia- history of generalised tonic clonic seizure
with increased blood pressure more than 140/90 mmHg, proteinuria > 1+ by
dipstick method in the absence of underlying seizure disorder >20 weeks of
pregnancy.
2. All cases of antepartum, intrapartumeclampsia presenting in obstetric
emergency, labour rooms and eclamptic wards.
3. Those who gave informed consent to participate in the study.
EXCLUSION CRITERIA:
1. Eclampsia with complications like HELLP syndrome, renal failure, severe
pulmonary oedema, respiratory failure, cardiovascular diseases, and
disseminated intravascular coagulation.
2. Patients who received magnesium sulphate before coming to hospital.
3. Patients with known seizure disorder.
4. Neonates of multiple pregnancy, very low birth weight(<1500gm), congenital
malformations.
METHODOLOGY
Totally 110 patients diagnosed with eclampsia and their neonates were screened in
obstetrics and gynaecology department of MC GANN TEACHING DISTRICT

53
HOSPITAL, SHIVAMOGGA. Out of 110, 10 patients with eclampsia and their
neonates couldn't meet the eligibility criteria, hence were excluded from the study.The
patients who met the inclusion criteria then were randomised into two groups.
Method of randomization: Patients included in the study as per the inclusion
andexclusion criteria were randomised into two groups by using block randomization
with a fixed block size 4 and allocation ratio 1:1 having equal chance of equal
distribution of patients into two groups. Computer generated random numbers in
Microsoft Excel 2007was used for allocation of block randomization.
Study procedure
Patients diagnosed with eclampsia by Obstetrics faculty in the eclampsia ward or
labour room were approached. Patient were stabilized initially by keeping them on a
railed cot and a tongue blade inserted between the teeth. They were kept in the
lateraldecubitus position to avoid aspiration. Vomitus and oral secretions were
removed by frequent suctioning, oxygenation was maintained through a face mask (8–
10 L/min) to prevent respiratory acidosis. Oxygenation was monitored using a
transcutaneous pulse oximeter. To take informed consent, their legal guardian/blood
relative were informed about the purpose of the study, study procedure, hospital staff
involved in the study, protocol of the study and about the treatment options available
to them, information about the investigations that will be carried out and the
information about the drug regimen used and their adverse effects in their own
understandable language.

54
Once explained, Informed consent(Annexure I) was taken from the patients guardian
who were willing to let their daughter/wife to participate in the study.Also once the
patient was stabilized, she was also explained in detail about the nature, purpose and
protocol of the study and Informed consent was taken from the patient too.
Patients and their guardians were explained that they can refuse or withdraw from the
study at any time and that will not affect her treatment in the hospital.
After obtaining informed consent from the patient/legal guardian of the patient
detailed history was obtained and recorded in the standard case record form.
The patients prior to their allotment into the study groups were enquired about
detailed information regarding no. of episodes of seizure before coming to the
hospital, past history of seizure disorder, last menstrual period(LMP), headache,
blurring of vision, epigastric pain, past history of preeclampsia/eclampsia in previous
pregnancy if any, similar family history and treatment taken for management of
seizure before coming to the hospital. General physical examination was conducted
including blood pressure recordings, vital signs, pallor, oedema and cyanosis.
Systemic examination included central nervous system, respiratory system and
cardiovascular system. Obstetric and pelvic examination was done by obstetrics
faculty. Routine laboratory investigations were done which included blood group and
Rh type, haemogram, platelet count, liver function tests, renalfunction tests, serum
electrolytes, coagulation profile, andurinary protein concentration.
The eligible patients were randomised into two groups
Group A (n=50) - received low dose magnesium sulphate regimen (Bankura regimen)

55
Group B (n=50) - received standard dose magnesium sulphate regimen (Pritchard's
regimen)
The patient in both the groups were admitted in eclampsia ward and examined in
detail for any complication due to eclampsia by continuous monitoring.
Group ‘A’received low dose magnesium sulphate -Bankura regimen. This comprised
of a loading dose of 3 grams magnesium sulphate prepared from, 6ml of magnesium
sulphate solution diluted with 5% dextrose solution and made upto 15ml, given
intravenously slowly at the rate of 1ml/min and 2.5 grams(5ml) of magnesium
sulphategiven intramuscular in each buttock. Followed by a maintenance dose of
2.5grams given 4 hourly in alternate buttock.
Group B received magnesium sulphate as per Pritchard’s regimen. This included a
loading dose of 4 grams of magnesium sulphate prepared from 8ml of magnesium
sulphate solution diluted with 5% dextrose solution and made upto 20ml given slowly
intravenously at the rate of 1ml/min and 5 grams (10ml) of magnesium sulphate deep
intramuscularly in each buttock. Followed by maintenance dose of 5 grams given 4th
hourly in alternate buttock.
After stabilization of the patient, artificial rupture of membrane and oxytocin
administration was used to induce labour, in patients who did not have a spontaneous
onset of labour, with dinoprostone gel used only occasionally when cervix was
unfavourable. Steroid therapy was given when delivery was less than <34weeks
Caesarean section was performed for obstetrical indications.
All obstetrical interventions were at the discretion of attending obstetric faculty.

56
The patients were monitored every 4th hourly till the delivery for adverse effect due
to magnesium sulphate regimens like loss of deep tendon reflexes, urinary output,
pulmonary crepitations, pulse rate, and blood pressure.
Recurrence of seizure if occurred in Group A in low dose magnesium sulphate
regimen, the patient was given immediately standard dose magnesium sulphate
regimen. If seizure recurred in Group B, they were treated with another dose of
Magnesium sulphate also when it was refractory general anaesthetic was used.
Maternal serum was collected from eclamptic mothers after giving induction of labour
and serum magnesium level was assessed in the hospital laboratory by automated
chemical analyzer. The clinical chemical analyzer used dye binding assay method for
estimation of magnesium level in the sample. Magnesium ion reacted with xylidyl
blue in an alkaline medium to form a water soluble purple-red chelate, the colour
intensity of which was proportional to concentration of magnesium in the sample.
Interference of calcium was excluded from the reaction by complexing it with
ethylene glycol tetraacetic acid (EGTA).
After the delivery the cord blood was collected either by the nursing staff or by intern
and sent to the laboratory for the assessment of magnesium level.
Neonatal birth weight, APGAR scores at 5 min was recorded. Presence of respiratory
depression, requirement of intubation in delivery room, NICU care requirement,
bradycardia and hypotonia was recorded. Monitoring of all the above mentioned
parameters in neonates was done for 24 hours. Still births and early neonatal deaths
were also noted.

57
Neonatal birth weight, APGAR score at 1, 5 min wererecorded. A maximum score of
10 and minimum score of 0was assigned to the neonates. The respiratory depression
was defined as apnoea at birth for more than 20seconds, bradycardia was defined as <
90 beats/min for > 5 s in duration. Neonatal hypotonia was diagnosed if neonate was
limp or flaccid and exhibited reduced activity. Neonatal resuscitation in the labour
room and NICU was at the decision of attending paediatric and faculty. Early neonatal
death was defined as death during first 15 days of life.
Maternal height and weight was recorded on 3rd and 4th day after delivery or when
patient was ambulatory.
Phone number was taken from the patient and follow up was also done on the 16th
day of the neonate for any adverse drug reaction. Also to enquire about any
recurrence of seizure in the mother.
The investigators phone number was also given to the patient and their guardians for
they were asked to inform if any reactions occur or convulsions develop during the 15
days of study follow up period.
STATISTICAL ANALYSIS
The data collected from the study was tabulated in Microsoft excel Microsoft Excel
2007.
Few selected data were given codes for statistical analysis in SPSS software version
20.0. (Annexure-IV). The demographic data was analysed with descriptive statistics
and compared with chi square test. All the demographic data analysed was considered
significant with a p value ≤ 0.05.

58
Pearson Correlation Coefficient was used to determine correlation between
APGARscore and cord blood magnesium level.
The Chisquare/Fisher’s exact test was used to determine whether there was
statistically significant difference between the groups with respect to primary study
parameters.
P ≤ 0.05 were considered significant
SAMPLE SIZE CALCULATION
Sample size was calculated with power of 80%. Alpha as 0.05% and expecting the
largest mean difference between two groups with 0.22 and anticipated complication
rates 8% and 30% from previous studies.12,13 Thus the sample size "n" required per
group was n=49. But n=50 patients in each group will be recruited for the study. The
total participants recruited for the study will be N=100.

59
RESULTS
There were total 110 eclampsia cases were screened during the study period and after
exclusion only 100 cases met the inclusion criteria.
9 patients were excluded from the study due to the following reasons (Fig No):
• 6 neonates had low birth weight
• 2 mothers had eclampsia with elevated liver enzymes and complication
• 1 patient had received magnesium sulphate before coming to the hospital
• 1 patient had multiple pregnancy
100 patients were randomized into two groups of 50 patients each as follows:
GROUP ‘A’ (CASE): n=50 patients and their neonates were included in the group
and analyzed in the study
GROUP ‘B’ (CONTROL): n=50 patients and their neonates were included in the
group and analyzed in the study

60
Figure no 11 : Flow chart representing the recruitment of the patients in the study.
110 patients diagnosed with
eclampsia were screened
4 patients were excluded
from the study
2 mothers -eclampsia with
complication
1 patient - received
magnesium sulphate before
coming to the hospital
1 patient - multiplepregnancy
N = 106 were randomised in two
groups
n = 53 were included
Group A
n = 53 were included in
Group B
n = 50 mothers and neonates
were analyzed who received
low dose magnesium sulphate
regimen
n = 50 mothers and neonates
were analyzed who received
standard dose magnesium
sulphate regimen
4 patients were
excluded - VLBW
neonate
2 patients were
excluded - VLBW
neonate

61
DEMOGRAPHIC PROFILE OF THE PATIENTS IN BOTH GROUP
1. AGE DISTRIBUTION
Table no. 9 - Representation of age distribution of eclamptic mothers in both
groups
AGE IN
YEARS
GROUP ᵡ2 p-value
Standard dose
group
n (%)
Low dose
group
n (%)
df= 3
4.97
0.17
18-22 23 (46) 32 (64)
23-27 17 (50) 8 (16)
28-32 7 (14) 8 (16)
32-36 3 (6) 2 (4)
Mean (+)SD 24.36+3.48 24.1+3.89
Median 26 26
IQR 4.75 9.5
Table no 9 represents the age distribution of eclamptic mothers among the two
groups. The mean age of mother for the standard dose regimen group is 24.36+3.48
and low dose regimen group is 24.1+3.89. Proportion of patients were more in the age
group between 18-22 in the standard dose regimen group and low dose regimen group
with frequency of 23 and 32 constituting 46% and 64% respectively. The minimum
and maximum age distributed among standard dose regimen group and low dose
regimen group are 20, 33 and 19, 34 respectively. There was no significant difference
in the age distribution among groups with ᵡ2(chi-square value) = 4.97 and p value
of 0.17.

62
Figure No 12: Graphical representation of distribution of age of eclamptic mothers
among both the groups.
0
5
10
15
20
25
20 - 2425 - 29
30 - 35
NO
.OF
PA
TIEN
TS
AGE IN YEARS
Standard dose
Low dose group

63
2. PARITY DISTRIBUTION
Table no 10 - Representation of distribution of parity among the mothers of both
group
GRAVIDA
STATUS/PARITY
GROUP ᵡ2 p-value
Standard dose
group
n(%)
Low dose
group
n(%)
df = 1
1.08
0.29
Primigravida 39 (78) 43 (86)
Multigravida 11 (22) 7 (14)
Table no 10 represents the distribution of parity of eclamptic mothers between two
groups. The frequency (proportion) of Primigravida distributed among standard dose
regimen group and low dose regimen group is 39(78%) and 43(86%) respectively.
The frequency (proportion) of Multigravida distributed among standard dose regimen
group and low dose regimen group is 11(22%) and 7(14%) respectively. There was no
significant difference between parity distribution between groups with
x2 = 1.08 and p value of 0.29.

64
Figure No 13: Graphical representation of parity distribution among eclamptic
mothers in both the groups.
0
5
10
15
20
25
30
35
40
45
primi gravida
multigravida
NO
. OF
PATI
ENTS
GRAVIDA STATUS
Standard dose group
Low dose group

65
3. DISTRIBUTION OF ANTENATAL CARE
Table no 11 : Representation of distribution of mothers who received antenatal
care in both the groups
ANTENATAL
CARE
GROUP ᵡ2 p-value
Standard
dose group
n(%)
Low dose
group
n(%)
df = 1
0.21
0.63
Booked cases 13 (26) 11 (22)
Unbooked cases 37 (74) 39 (78)
Table no 11 represents the distribution of patients diagnosed with eclampsia who
received antenatal care in both standard dose regimen group and low dose regimen
group. The frequency of unbooked mothers in both the groups were higher with 37
patients constituting of 74% in standard dose regimen group and 39 patients in low
dose regimen group constituting of 78%. The frequency (proportion) of eclamptic
patients was least both in standard dose regimen group and low dose regimen group
with frequency of 13 patients constituting 26% and 11 patients constituting 22%
respectively. There was no significant difference in distribution of booked and
unbooked mothers between groups with x2 =0.21and p value of 0.63.

66
Figure no 14: Graphical representation distribution of antenatal care received between
both the groups.
0
5
10
15
20
25
30
35
40
Booked cases
Unbooked cases
NO
.OF
PATI
ENTS
Standard dose group
Low dose group

67
4. DISTRIBUTION OF AREAS
Table no 12: Representation of distribution of eclamptic mothers from the
different areas among both the groups
AREA
GROUP ᵡ2 p-value
Standard
dose group
n(%)
Low dose
group
n(%)
df = 1
0.79
0.37
RURAL 38(76) 34(68)
URBAN 12(24) 16(32)
Table no 12 represents the distribution of rural and urban population between two the
two groups. The frequency (proportion) of mothers from rural areas distributed among
standard dose regimen group and low dose regimen group is 38(76%) and 34(68%)
respectively. The frequency (proportion) of mothers from urban areas distributed
among standard dose regimen group and low dose regimen group is 12(24%) and
16(32%) respectively. There was no significant difference between rural and urban
population between groups with x2 = 0.79 and p value of 0.37.

68
Figure No 15: Graphical representation of distribution of eclamptic mothers in rural
and urban areas among both the groups.
0
5
10
15
20
25
30
35
40
Rural population Urban population
NO
.OF
PATI
ENTS
Standard dose regimen
Low dose regimen
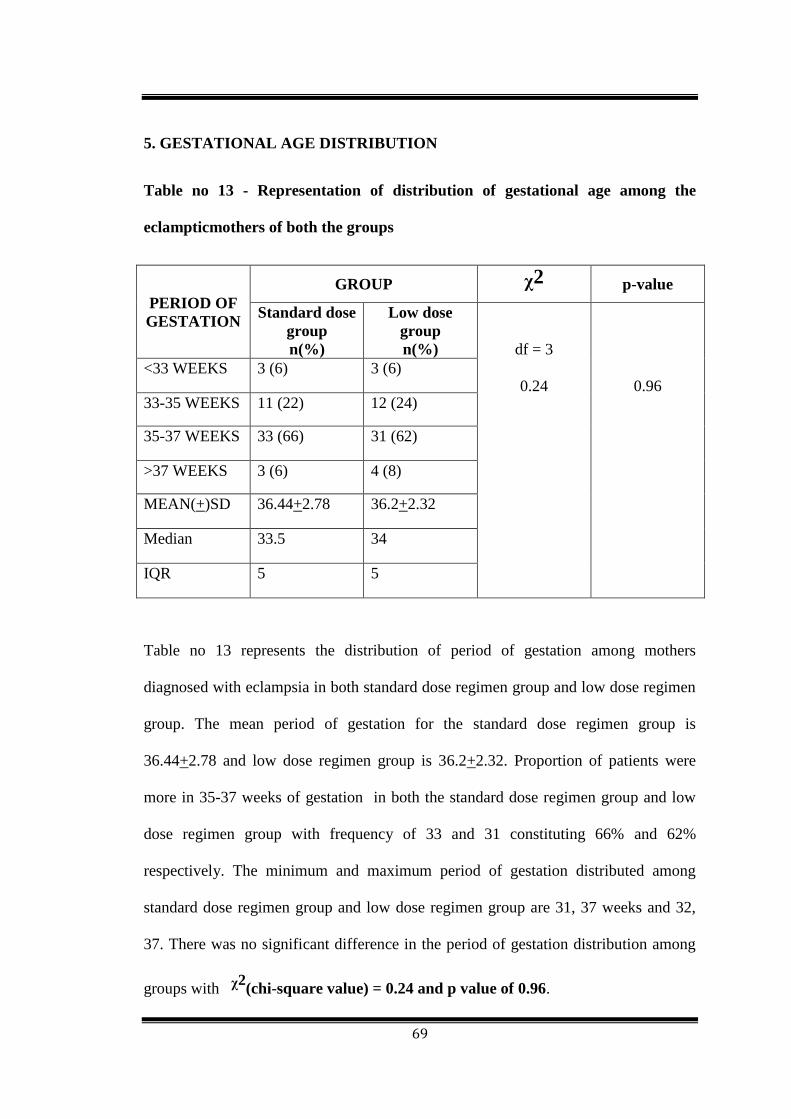
69
5. GESTATIONAL AGE DISTRIBUTION
Table no 13 - Representation of distribution of gestational age among the
eclampticmothers of both the groups
PERIOD OF
GESTATION
GROUP ᵡ2 p-value
Standard dose
group
n(%)
Low dose
group
n(%)
df = 3
0.24
0.96 <33 WEEKS 3 (6) 3 (6)
33-35 WEEKS 11 (22) 12 (24)
35-37 WEEKS 33 (66) 31 (62)
>37 WEEKS 3 (6) 4 (8)
MEAN(+)SD 36.44+2.78 36.2+2.32
Median 33.5 34
IQR 5 5
Table no 13 represents the distribution of period of gestation among mothers
diagnosed with eclampsia in both standard dose regimen group and low dose regimen
group. The mean period of gestation for the standard dose regimen group is
36.44+2.78 and low dose regimen group is 36.2+2.32. Proportion of patients were
more in 35-37 weeks of gestation in both the standard dose regimen group and low
dose regimen group with frequency of 33 and 31 constituting 66% and 62%
respectively. The minimum and maximum period of gestation distributed among
standard dose regimen group and low dose regimen group are 31, 37 weeks and 32,
37. There was no significant difference in the period of gestation distribution among
groups with ᵡ2(chi-square value) = 0.24 and p value of 0.96.

70
Figure No 16 : Graphical representation of distribution period of gestation in weeks of
eclamptic mothers among both the groups.
0
5
10
15
20
25
30
35
40
45
50
Standard dose group Low dose group
PR
OP
OR
TIO
N O
F P
ATI
ENTS
> 36 weeks
32 - 36 weeks
28 - 31 weeks
<28 weeks

71
6. BMI DISTRIBUTION
Table no 14 : Representation of distribution body mass index in both groups
among mothers
BODY MASS
INDEX
GROUP ᵡ2 p-value
Standard dose
group
n(%)
Low dose
group
n(%)
df = 2
1.63
0.44
<19 kg/m2 15 (30) 10 (20)
20 - 25kg/m2 32 (64) 35 (70)
>25kg/m2 3 (6) 5 (10)
MEAN(+)SD 20.97+2.72 19.42+2.80
Median 19.97 21.22
IQR 3.73 4.01
Table no 14 represents the distribution of body mass index among mothers diagnosed
with eclampsia in both standard dose regimen group and low dose regimen group. The
mean body mass index for the standard dose regimen group is 20.97+2.72 and low
dose regimen group is 19.42+2.80. Proportion of patients were more with BMI 20 to
22 kg/m2 in both the standard dose regimen group and low dose regimen group with
frequency of 32 and 35 constituting 64% and 70% respectively. The minimum and
maximum body mass index distributed among standard dose regimen group and low
dose regimen group are 18, 26 kg/m2 and 17, 28kg/m2 respectively. There was no
significant difference in the body mass index distribution among groups with
ᵡ2(chi-square value) = 0.51 and p value of 0.77.

72
Figure No 17: Graphical representation of body mass index distribution in eclamptic
mothers among both the groups.
0
5
10
15
20
25
30
35
< 19 kg/m2 20 - 25 kg/m2 >25 kg/m2
NO
.OF
PA
TIEN
TS
Standard dosegroup
Low dosegroup

73
7. SYSTOLIC BLOOD PRESSURE DISTRIBUTION
Table no 15 - Representation of systolic blood pressure distribution among
mothers of both group
SYSTOLIC
BLOOD
PRESSURE
GROUP ᵡ2 p-value
Standard dose
group
n(%)
Low dose
group
n(%)
df =2
2.31
0.31
130-150mmHg 8 (16) 10 (20)
150-170mmHg 35 (70) 28 (56)
>180mmHg 7 (14) 12 (24)
MEAN(+)SD 161.48+13.12 160+13.87
Median 159 160
IQR 7.74 6
Table no 15 represents the distribution of systolic blood pressure among mothers
diagnosed with eclampsia in both standard dose regimen group and low dose regimen
group. The mean systolic blood pressure for the standard dose regimen group is
161.48+13.12 and low dose regimen group is 160+13.87. Proportion of patients were
more with systolic blood pressure 150 to 170mmHg in both the standard dose regimen
group and low dose regimen group with frequency of 35 and 28 constituting 70% and
56% respectively. The minimum and maximum systolic blood pressure distributed
among standard dose regimen group and low dose regimen group are 150, 200mmHg
and 150, 180mmHg respectively. There was no significant difference in the systolic
blood pressure distribution among groups with ᵡ2(chi-square value) = 2.31 and p
value of 0.31

74
.
Figure No 18: Graphical representation of distribution of systolic blood pressure of
eclamptic mothers among both the groups.
0
5
10
15
20
25
30
35
130 - 150mmHg 150 - 170mmHg > 180mmHg
NO
OF
PA
TIEN
TS
Standard dosegroup

75
8. DIASTOLIC BLOOD PRESSURE DISTRIBUTION
Table no 16: Representation of distribution of diastolic blood pressure among
mothers of both groups
DIASTOLIC
BLOOD
PRESSURE
GROUP ᵡ2 p-value
Standard dose
group
n(%)
Low dose
group
n(%)
df = 2
0.72
0.69
<90mmHg 18 (36) 22 (44)
100mmHg 27 (54) 23 (46)
>110mmHg 5 (10) 5 (10)
MEAN(+)SD 97.4+6.32 100+6.58
Median 100 100
IQR 10 10
Table no 16 represents the distribution of diastolic blood pressure among mothers
diagnosed with eclampsia in both standard dose regimen group and low dose regimen
group. The mean diastolic blood pressure for the standard dose regimen group is
97.4+6.32 and low dose regimen group is 100+6.58. Proportion of patients were more
with diastolic blood pressure 100mmHg in both the standard dose regimen group and
low dose regimen group with frequency of 27 and 23 constituting 54% and 46%
respectively. The minimum and maximum diastolic blood pressure distributed among
standard dose regimen group and low dose regimen group are 90,100 mmHg and 90,
100mmHg respectively. There was no significant difference in the diastolic blood
pressure distribution among groups with ᵡ2(chi-square value) = 0.72 and p value
of 0.69.

76
Figure No 19: Graphical representation of distribution of diastolic blood pressure of
eclamptic mothers among both the groups.
0
5
10
15
20
25
30
<90mmHg100mmHg
>100mmHg
NO
. OF
PA
TIEN
TS
Standard doseregimen
Low doseregimen

77
9. EPISODES OF SEIZURE DISTRIBUTION
Table no 17 - Representation of distribution of no. of episodes of seizures before
the start of treatment in eclamptic mothers among both the groups
NO.OF
CONVULSSIONS
GROUP ᵡ2 p-value
Standard
dose group
n(%)
Low dose
group
n(%)
df = 3
2.24
0.52
<3 16 (32) 19 (38)
3 - 5 22 (44) 15 (30)
5 - 7 10 (20) 14 (28)
>7 2 (4) 2 (4)
Mean 4.3+1.59 4.24+2.0
Median 3 4
IQR 2 3
Table no 17 represents the distribution of number of seizures among mothers
diagnosed with eclampsia in both standard dose regimen group and low dose regimen
group. The mean number of seizures for the standard dose regimen group is 4.3+1.59
and low dose regimen group is 4.24+2.0. Proportion of patients were more with
number of seizures between 3 to 5 in both the standard dose regimen group and low
dose regimen group with frequency of 22 and 15 constituting 44% and 30%
respectively. The minimum and maximum number of episodes of seizure distributed
among standard dose regimen group and low dose regimen group are 1, 9 and 1, 8
respectively. There was no significant difference in the number of seizures before the
start of treatment distribution among groups with ᵡ2(chi-square value) = 2.24 and p
value of 0.52.

78
Figure No 20: Graphical representation of distribution of number of convulsions
before admission in eclamptic mothers among both the groups.
0
5
10
15
20
25
<3 3 to 5 5 to 7 > 7
Standard dosegroup

79
10. MODE OF DELIVERY DISTRIBUTION
Table no 18 : Representation of distribution of mode of delivery in mothers
among both groups
MODE OF
DELIVERY
GROUP ᵡ2 p-value
Standard
dose group
n(%)
Low dose
group
n(%)
df = 1
1.41
0.23
Vaginal delivery 36(72) 41(82)
Caesarean section 14 (28) 9 (18)
Table no 18 represents the distribution of mode of delivery in patients diagnosed with
eclampsia in both standard dose regimen group and low dose regimen group. The
frequency of vaginal delivery in eclamptic mothers in both the groups were higher
with 36 patients constituting of 72% in standard dose regimen group and 41 patients
in low dose regimen group constituting of 82%. The frequency (proportion) of
eclamptic patients who underwent caesarean section was least both in standard dose
regimen group and low dose regimen group with frequency of 14 patients constituting
28% and 9 patients constituting 18% respectively. There was no significant difference
in distribution of mode of delivery in eclamptic mothers between the groups with
x2 =1.41and p value of 0.23.

80
Figure No 21: Graphical representation of distribution of mode of delivery in
eclamptic mothers among both the groups.
0
10
20
30
40
50
60
Vaginal delivery Caesarean section
Standard dose regimen
Low dose regimen

81
OUTCOME MEASURES
1. BIRTH WEIGHT DISTRIBUTION
Table no 19 - Representation of distribution of birth weight among the neonates
of eclamptic mothers in both the groups
BIRTH
WEIGHT
(in grams)
GROUP ᵡ2 p-value
Standard
dose group
n(%)
Low dose
group
n(%)
df = 2
0.95
0.62
<2500 30(60) 31(62)
2500 - 3500 18(36) 15(30)
>3500 2(4) 4(8)
Mean 2624+505.30 2610+549.30
Median 2500 2500
IQR 700 700
Table no 19 represents the distribution of birth weight among mothers diagnosed with
eclampsia in both standard dose regimen group and low dose regimen group. The
mean birth weight for the standard dose regimen group is 2624+505.30 and low dose
regimen group is 2610+549.30. Proportion of patients were more with birth weight
less than 2500gm in both the standard dose regimen group and low dose regimen
group with frequency of 30 and 31 constituting 60% and 62% respectively. The
minimum and maximum birth weight distributed among standard dose regimen group
and low dose regimen group are 1800, 2000 and 3800, 3500 respectively. There was
no significant difference in the birth weight distribution among groups with
ᵡ2(chi-square value) = 0.95 and p value of 0.62.

82
Figure No 22: Graphical representation of distribution of birth weight in neonates of
eclamptic mothers among both the groups.
0
5
10
15
20
25
30
35
< 2500 2500 - 3500 > 3500
NO
.OF
NEO
NA
TES
BIRTH WEIGHT
Standard regimen
Low dose regimen

83
2. CORD BLOOD MAGNESIUM LEVEL DISTRIBUTION
Table no 20:Representation of distribution of cord blood magnesium at time of
delivery among the neonates of eclamptic mothers in both groups
CORD BLOOD
MAGNESIUM IN
MMOL/L
GROUP
Standard dose group
n(%)
Low dose group
n(%)
1.5 - 1.8 0 3(6)
1.8 - 2.1 0 10(20)
2.1 - 2.4 0 23(46)
2.4 - 2.7 3(6) 11(22)
2.7 - 3.0 7(14) 3(6)
3.0 -3.3 15(30) 0
3.3 - 3.6 21(42) 0
3.6 - 3.9 4(8) 0
MEAN(+)SD
3.28+0.16 2.20+0.26
MEDIAN
3.25 2.2
IQR
0.2 0.37
MIN
3.0 1.7
MAX
3.8 2.7
Table no 20 represents the distribution of cord blood magnesium level among mothers
diagnosed with eclampsia in both standard dose regimen group and low dose regimen
group. The mean cord blood magnesium level for the standard dose regimen group is
3.28+0.16 and low dose regimen group is 2.20+0.26. The minimum and maximum
level of cord blood magnesium distributed among standard dose regimen group and
low dose regimen group are 2.6, 3.8 mmol/l and 1.7, 2.8 mmol/l respectively.

84
Figure no 23: Graphical representation (Line diagram) of distribution of cord blood
magnesium level at the time of delivery of neonates of eclamptic mothers among both
the groups.
0
5
10
15
20
25
1.5 1.8 2.1 2.4 2.7 3 3.3 3.6 3.9
DISTRIBUTION OF CORD BLOOD MAGNESIUM LEVEL AMONG BOTH THE GROUPS
Standard dose regimen group Low dose regimen group
x axis - No. of neonates
y axis - Cord blood magnesium level

85
Table no 21 - Representation of APGAR scores at 5 min among the neonates of
eclamptic mothers in both groups
APGAR
SCORE
GROUP ᵡ2 p-value
Standard dose
group
n(%)
Low dose
group
n(%)
df = 2
7.56
0.02
<3 6 (12) 1 (2)
3 - 7 17 (34) 10 (20)
>7 27 (54) 39 (78)
MEAN(+)SD 6.62+2.23 8.9+1.46
Median 8 9
IQR
3.75 1
MIN
3 3
MAX
10 10
As per Table no 21 Chi square test showed that over all there is statistically
significant difference in APGAR score at 5 min between the two groups with
χ2 = 7.56 and p = 0.02, with a mean APGAR score at 5 min in standard dose regimen
group 6.62+2.23 and in low dose regimen group 8.9+1.46. The Interquartile range
between the standard dose regimen group is 3.75 and in low dose regimen group is
1.APGAR scores decreased significantly with increase in cord blood magnesium
levels. Cord blood magnesium level of severely depressed neonates (APGAR score ≤
3), was in the range of 3.5–3.9 mmol/L. This is depicted in figure no. which shows
spikes (APGAR score < 3) at cord blood magnesium level of 3.5 to 3.9 and another
spikes (APGAR score between 3-7) at cord blood magnesium level of 3.3 to
3.5mmol/L. The pearson correlation coefficient for cord blood magnesium level and
APGAR score was = -0.79, which is statistically significant.

86
Figure No 24: Graphical representation of distribution of APGAR scores of neonates
of eclamptic mothers among both the groups.
Figure No 25: Graphical representation (line diagram) of correlation of cord blood
magnesium level and APGAR scores in neonates of eclamptic mother in both the
groups
0
5
10
15
20
25
30
35
40
< 3 3 to 7
> 7
NO
. OF
NEO
NA
TES
APGAR SCORES
Standard doseregimen group
Low dose regimengroup
0
1
2
3
4
5
6
7
8
9
10
1.5 1.7 1.9 2.1 2.3 2.5 2.7 2.9 3.1 3.3 3.5 3.7 3.9
No
. of
ne
on
ate
s
CORRELATION
< 3
3 TO 7

87
4. NICU CARE DISTRIBUTION
Table no : 22 - Representation of requirement of NICU care among the neonates
of eclamptic mothers in both groups
INCIDENCE
GROUP ᵡ2 p-value
Standard dose
group
n(%)
Low dose
group
n(%)
df = 1
17.36
<0.001
NICU care
required 28(56) 8(16)
NICU care not
required 22(44) 42(84)
As per Table no 22 The Chi square test showed that over all there is statistically
significant difference in NICU care requirement between the two groups with
χ2 = 17.36 and p = <0.001, with a proportion of neonates who required NICU care in
standard dose regimen group were 56% and low dose regimen group were 16%.
NICU care requirement increased significantly with increase in cord blood
magnesium levels. The number of neonates who required NICU care were more when
they had cord blood magnesium level in the range of 3.5 to 3.8 mmol/l. This is
depicted in the figure no. which shows a scatter plot, where the neonates admission in
the NICU is seen to be scattered more with the higher level of cord blood
magnesium. Proportion of neonates admitted in NICU varied from 70 - 100% at the
cord blood magnesium level between 3.5 - 3.8mmol/l.

88
Figure No 26 : Graphical representation of distribution of NICU care requirement in
neonates of eclamptic mothers among both the groups.
Figure No 27: Graphical representation of distribution of NICU care requirement in
neonates of eclampticmothers scattered among both the groups.
0
5
10
15
20
25
30
35
40
45
50
Standard dose groupLow dose group
NICU care not required
NICU care required
0
20
40
60
80
100
120
0 1 2 3 4 5
Pe
rce
nta
ge o
f ad
mis
sio
n
Cord blood magnesium level
NICU care requirement
NICU care requirement

89
5. RESPIRATORY DISTRESS DISTRIBUTION
Table no 23 - Representation of incidence of respiratory distress among the
neonates of eclamptic mothers in both groups
GROUP ᵡ2 p-value
Standard dose
group
n(%)
Low dose
group
n(%)
df = 1
5.74
0.01 Respiratory
distress
13(26) 4(8)
No respiratory
distress
37(74) 46(92)
As per Table no 23 Chi square test showed that over all there is statistically
significant difference in incidence of respiratory distress between the two groups with
χ2 = 5.74 and p = 0.01, with a proportion of neonates who had respiratory distress in
standard dose regimen group was 26% and low dose regimen group was 8%.

90
Figure No 28: Graphical representation of distribution of incidence of respiratory
distress in neonates of eclamptic mothers among both the groups.
Figure No 29: Graphical representation (box plot) of distribution of incidence of
respiratory distress in neonates of eclamptic mothers in the box plot form among both
the groups.
0
5
10
15
20
25
30
35
40
45
50
Respiratory distress Normal breathing
NO
.OF
PA
TIEN
TS
StandardDose group
Low dosegroup
0
10
20
30
40
50
60
Standard dose regimen Low dose regimen

91
6. HYPOTONIA DISTRIBUTION
Table no 24 - Representation of incidence of hypotonia among the neonates of
eclamptic mothers in both groups
GROUP ᵡ2 p-value
Standard dose
group
n(%)
Low dose
group
n(%)
df = 1
13.22
0.0002
Presence of
Hypotonia
27 4
No Hypotonia 23 46
As per Table no 24 Chi square test showed that over all there is statistically
significant difference in incidence of hypotonia between the two groups with
χ2 = 17.36 and p = <0.001, with a proportion of neonates who had hypotonia in
standard dose regimen group was 54% and low dose regimen group was 8%.
Figure No 30: Graphical representation of distribution of incidence of hypotonia in
neonates of eclamptic mothers among both the groups.
0
5
10
15
20
25
30
35
40
45
50
Hypotonia Normal muscle tone
Standard dose regimen
Low dose regimen

92
7. BRADYCARDIA DISTRIBUTION
Table no 25 - Representation of incidence of bradycardia among the neonates of
eclamptic mothers in both groups
INCIDENCE
GROUP ᵡ2 p-value
Standard dose
group
n(%)
Low dose
group
n(%)
df = 1
9.49
0.002 Bradycardia 13(26) 2(4)
No
Bradycardia
37(74) 44(88)
As per Table no 25 Chi square test showed that over all there is statistically
significant difference in incidence of bradycardia between the two groups with
χ2 = 9.49 and p = 0.002, with a proportion of neonates who had bradycardia in
standard dose regimen group was 26% and low dose regimen group was 4%.
Figure No 31: Graphical representation of distribution of incidence of bradycardia in
neonates of eclamptic mothers among both the groups.
0
5
10
15
20
25
30
35
40
45
Bradycardia
Normal heart rate
NO
. OF
PA
TIEN
TS
Standard dosegroup
Low dosegroup

93
SAFETY PARAMETERS
1. SERUM MAGNESIUM LEVEL DISTRIBUTION
Table no 26 - Representation of serum magnesium level at the time of delivery in
eclamptic mothers among both groups
SERUM MAGNESIUM
LEVEL IN M MOL/L
GROUP
Standard dose group
n(%)
Low dose group
n(%)
1.8 - 2.1 0 10(20)
2.1 - 2.4 0 21(42)
2.4 - 2.7 0 11(22)
2.7 - 3.0 0 19(38)
3.0 -3.3 6(12) 0
3.3 - 3.6 38(76) 0
3.6 - 3.9 6(12) 0
MEAN(+)SD
3.40+0.16 2.31+0.26
MEDIAN
3.4 2.3
IQR
0.2 0.3
MIN
3.1 1.8
MAX
3.9 2.8
Table no 26 represents the distribution of serum magnesium level among mothers
diagnosed with eclampsia in both standard dose regimen group and low dose regimen
group. The mean serum magnesium level for the standard dose regimen group is
3.40+0.16 and low dose regimen group is 2.31+0.26. The minimum and maximum
level of cord blood magnesium distributed among standard dose regimen group and
low dose regimen group are 3.1, 3.9 mmol/l and 1.8, 2.8 mmol/l respectively.
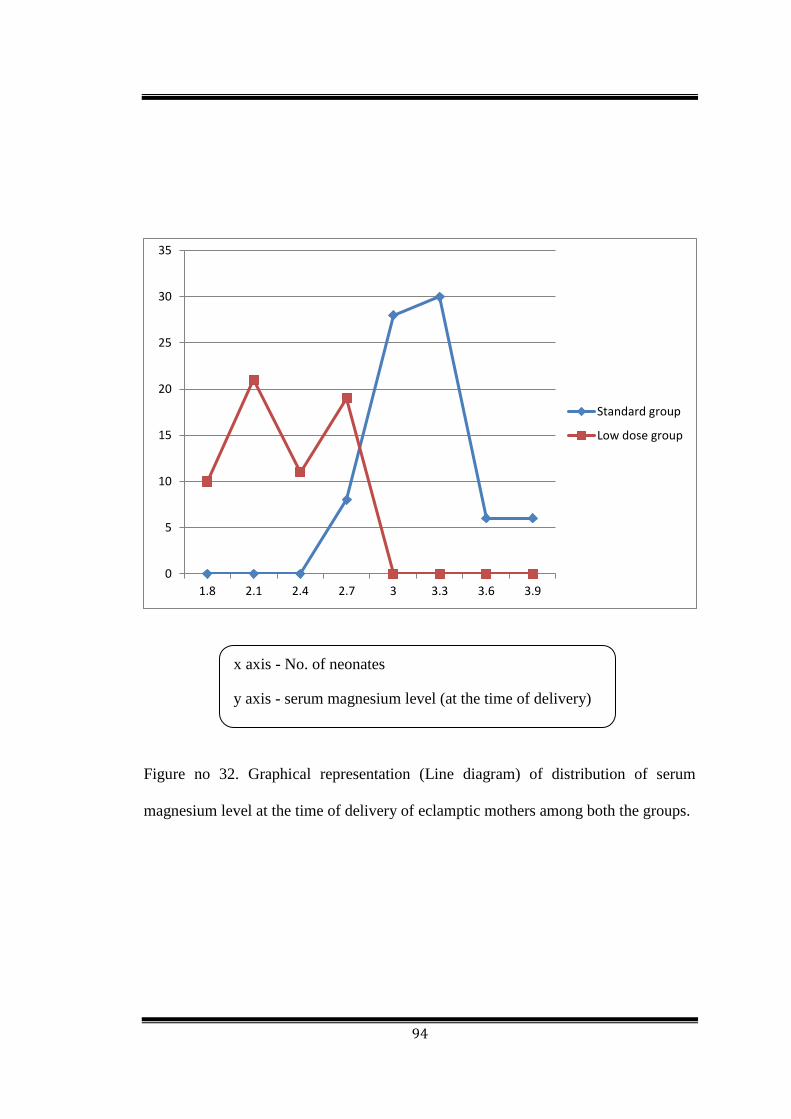
94
Figure no 32. Graphical representation (Line diagram) of distribution of serum
magnesium level at the time of delivery of eclamptic mothers among both the groups.
0
5
10
15
20
25
30
35
1.8 2.1 2.4 2.7 3 3.3 3.6 3.9
Standard group
Low dose group
x axis - No. of neonates
y axis - serum magnesium level (at the time of delivery)
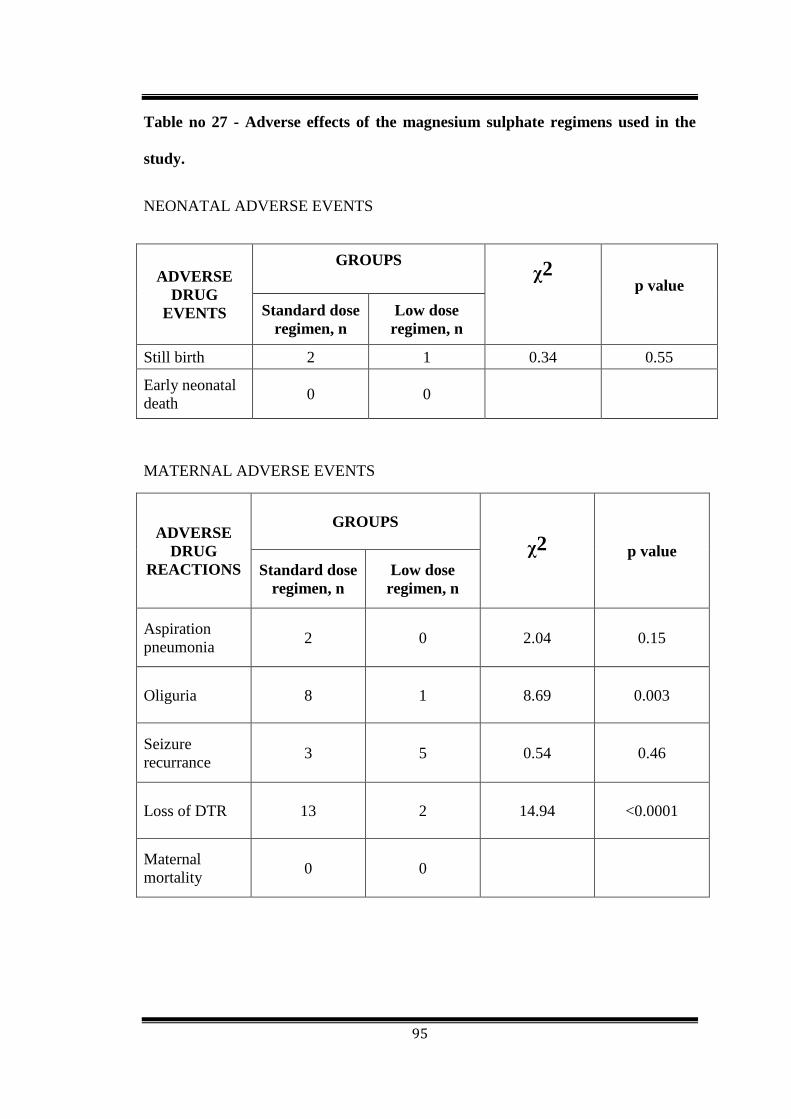
95
Table no 27 - Adverse effects of the magnesium sulphate regimens used in the
study.
NEONATAL ADVERSE EVENTS
ADVERSE
DRUG
EVENTS
GROUPS
ᵡ2 p value
Standard dose
regimen, n
Low dose
regimen, n
Still birth 2 1 0.34 0.55
Early neonatal
death 0 0
MATERNAL ADVERSE EVENTS
ADVERSE
DRUG
REACTIONS
GROUPS
ᵡ2 p value
Standard dose
regimen, n
Low dose
regimen, n
Aspiration
pneumonia 2 0 2.04 0.15
Oliguria 8 1 8.69 0.003
Seizure
recurrance 3 5 0.54 0.46
Loss of DTR 13 2 14.94 <0.0001
Maternal
mortality 0 0

96
In the study the neonatal adverse drug event observed was still birth, which was seen
in one case in low dose magnesium sulphate group compared to two cases in standard
dose regimen group, and the result did not show any statistical significance. There
was no early neonatal mortality documented in the study.
In the study the adverse drug events observed in mothers were loss/decreased deep
tendon reflexes, oliguria, seizure recurrence and aspiration pneumonia. In low dose
magnesium sulphate regimen group the proportion of adverse event observed were
loss of deep tendon reflex (4%), oliguria (2%), seizure recurrence(10%). There was
no aspiration pneumonia and maternal mortality reported in the low dose group. In the
standard dose magnesium sulphate regimen group the proportion of adverse event
observed were loss of deep tendon reflex (26%), oliguria (16%), seizure recurrence
(6%) and aspiration pneumonia (4%). There was no maternal mortality reported in the
standard dose regimen group. Low dose magnesium sulphate regimen group showed
statistical significant less number of adverse events loss/decreased deep tendon reflex
and oliguria.
The figure no depicts correlation between serum magnesium level in mothers at the
time of delivery and adverse events loss of DTR and oliguria. Both show statistical
significant higher adverse events at the range of 3.3-3.9mmol/l. The graphs no depicts
spikes at the serum magnesium level of 3.4 to 3.9mmol/l representing higher number
of cases with adverse events.
The figure no depicts correlation between serum magnesium level in mothers at the
time of delivery and adverse events aspiration pneumonia and seizure recurrence.
Both did not show statistical significant higher or lower adverse events.

97
Figure no 33. Graphical representation of distribution of adverse events in eclamptic
mothers among both the groups.
0
2
4
6
8
10
12
14
Standard doseregimenLow doseregimen

98
Figure no 34. Graphical representation of correlation of serum magnesium level and
adverse events in eclamptic mothers among both the groups.
Figure no 35. Graphical representation of correlation of serum magnesium level and
adverse events in eclamptic mothers among both the groups.
0
1
2
3
4
5
6
7
8
1.5 1.7 1.9 2.1 2.3 2.5 2.7 2.9 3.1 3.3 3.5 3.7 3.9
loss of DTR
Oliguria
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
1.5 1.7 1.9 2.1 2.3 2.5 2.7 2.9 3.1 3.3 3.5 3.7 3.9
Aspiration pneumonia
Seizure recurrance

99
DISCUSSION
The present study was conducted among the neonates of eclamptic mothers in the
Obstetrics and Gynaecology department at Mc Gann Teaching District Hospital,
Shivamogga Institute of Medical Sciences, Shivamogga. Total 110 patients were
screened out of which 100 patients and their neonates were included and analyzed in
the study.
In our study 100 patients with eclampsia were analyzed for neonatal outcome who
were treated with magnesium sulphate regimens. The two regimens of magnesium
sulphate used in the study are Standard dose magnesium sulphate regimen (Pritchard's
regimen) and Low dose magnesium sulphate regimen (Bankura regimen). The study
was done to compare and assess safety of Low dose magnesium sulphate regimen and
Standard dose magnesium sulphate regimen in neonates of eclamptic mothers treated
with this regimen.58
In the present study the mean age of mothers included in the study was 24.36+3.48 in
Standard dose magnesium sulphate regimen group and 24.1+3.89 in Low dose
magnesium sulphate regimen group which is in accoradance with Mahajan N et al
where the mean age of mothers diagnosed with eclampsia was 23.64. WhereasBangal
V et al. Shilva et al. reported that 44% and 46% of cases respectively below 20 years
of age which is much lower age group than our study. In our study primigravida
constituted larger proportions of patients in both the groups with 78% of primigravida
in Standard dose magnesium sulphate regimen group and 86% primigravida in Low
dose magnesium sulphate regimen group. Similar studies by Sardesai et al. Pritchard
et al. and Begum R et al. observed 80%, 75%, and 79% of eclampsia cases in
primigravidas respectively. These observations are similar to our study.59

100
In the present study the number of eclamptic mothers who got antenatal care were
very less with only 26% in Standard dose magnesium sulphate regimen group and
22% in Low dose magnesium sulphate regimen group. In a similar study by Sardesai
et al. shows 23.4% of eclamptic mothers got antenatal care which is similar to our
study. In another identical study by Stone S R et al. shows only 8% of mothers who
were diagnosed with eclampsia had got antenatal care which is much lower than our
study. This difference may be due to larger middle class and educated population in
our area who are eager to receive antenatal care. Eclampsia is a sequel of
preeclampsia with uncontrolled blood pressure hence regular antenatal checkups,
screening and treatment of preeclampsia are major factors that contributes to prevent
the morbidity and mortality associated with eclampsia. So lesser the mothers receives
the antenatal care more chances of incidence of eclampsia.60
In our study majority of patients diagnosed with eclampsia were from rural areas with
76% in Standard dose magnesium sulphate regimen group and 68% in Low dose
magnesium sulphate regimen group. This implies there was very little accessibility for
antenatal care and continuous monitoring of the blood pressure, and even many of the
patients were not diagnosed with preeclampsia. Our observations are similar to the
study done by Shamsuddin L et al. who reported 80% of patients diagnosed with
eclampsia were from rural communities in their study.61
The average period of gestation of mothers who presented with eclampsia at our
hospital was 36.44+2.78 weeks in Standard dose magnesium sulphate regimen group
and 36.2+2.32 weeks in Low dose magnesium sulphate regimen group. In an
identical study by LatikaSahu et al. observed the mean weeks of gestation in mothers
who presented with eclampsia was 34 weeks which is very similar to our study. Also

101
other studies by Altman D et al. and Begum R et al. observed mean weeks of
gestation to be 33.3 weeks and 35.8 weeks respectively.62
In the present study mean body mass index of eclamptic mothers was 20.97+2.72 in
Standard dose magnesium sulphate regimen group and 19.42+2.80 in low dose
magnesium sulphate regimen group. These values are indicating towards the lower
range of BMI in our study area among mothers. This indicates the lower body mass
index in developing communities which warrants usage of magnesium sulphate in
lower dose to prevent the toxicity due to hypermagnesimia. In resembling studies by
Sibai B M et al, Bangal V et al and Sardesai et al. the mean BMI of the eclamptic
mothers was 20.64 ± 1.24, 20.75 ± 1.33 and 22.83 ± 2.53 respectively which is similar
to our study. All the above studies done in developing countries are therefore
indicating lower range of BMI among mothers receiving less antenatal care.63
In our study we found the mean systolic blood pressure of the mothers with eclampsia
was 161.48 +13.12 in Standard dose magnesium sulphate regimen group and
160+13.87 in the Low dose magnesium sulphate regimen group. The elevated blood
pressure shows the need of administering the magnesium sulphate regimen as
mentioned in the treatment of eclampsia is recommended (MAGPIE Trial-2002). In a
similar study by Duley et al. the mean systolic blood pressure among the eclamptic
mothers was 164 ± 14.14 which corresponds to our study value. The severe
hypertension (>160mmHg) among the mothers indicates that delivery should be
considered irrespective of the gestational age, which was done accordingly in our
study.64
In our study we observed the mean of diastolic blood pressure of eclamptic mothers
was 97.4+6.32 in Standard dose magnesium sulphate regimen group and 100+6.58 in

102
Low dose magnesium sulphate regimen group. These values are little higher than
normal showing the fulminant eclamptic state of the mother. Both systolic blood
pressure and diastolic blood pressure are showing the need of treating the mother
immediately with anticonvulsants to prevent recurrent seizures and to start appropriate
antihypertensive. In similar study by Jana N et al. and Mahajan N et al the mean
diastolic blood pressure was 118.8 ± 4.01 and 104.8 ± 9.48 respectively which is in
accordance to our study.65
In the present study the average number of convulsions the mother suffered before the
admission in our hospital was 4.3+1.59 in Standard dose magnesium sulphate regimen
group and 4.24+2.0 in Low dose magnesium sulphate regimen group. This indicating
the potential morbidity and mortality in both mother and the foetus. In identical
studies by Malapaka S V et al. and Bangal V et al. show the higher numbers with
average number of convulsions before admissions 6.08+2.81 and 6.83+1.33. This is
due to better use of transportation facility by the nearby population of our hospital
under jananisurakshayojana and also the awareness among the community for better
healthcare facility.66
In the present study the proportion of caesarean section done among eclamptic
mothers was 28% in Standard dose magnesium sulphate regimen group and 18% in
Low dose magnesium sulphate regimen group which was comparable with similar
studies by Nautiyal R et al. and Seth S et al. who showed proportion to be 16% and
20% respectively. There was no maternal mortality seen in our study among both the
groups. The patient with complications before admission were not included in the
study which might be the reason for better outcome in our study. If complication
developed the both treating gynaecologist and physician shifted the patient to

103
intensive care unit (ICU) and managed accordingly. And mother who developed
complications due to eclampsia were also excluded from the study. This is similar to
the study by Sardesai et al. and Shilva et al which also reported no maternal mortality.
In the present study the mean birth weight of neonates was found to be 2624+505.30
grams in Standard dose magnesium sulphate regimen group and 2610+549.30 grams
in Low dose magnesium sulphate regimen group. The neonatal birth weight did not
vary significantly among the groups in our study which is in accordance with the
study by Das M et al. Also similar studies by Stone S R et al. and Donovan E F et al.
showed similar observations.67,68
In the present study the mean cord blood magnesium level was 3.28+0.16 mmol/l in
Standard dose magnesium sulphate regimen and 2.20+0.26mmol/l in Low dose
magnesium sulphate regimen. The greater proportion of cord blood magnesium levels
were in the desired therapeutic range of 2.0-3.5mmol/l. Only 4(8%) neonates had
levels exceeding 3.8mmol/l. These findings are in accordance with identical studies
by Riaz M et al and Rasch D K et al which reported the mean cord blood magnesium
level to be 3.36 and 3.19mmol/l respectively. The dose of magnesium sulphate in Low
dose magnesium sulphate regimen group was 40% lower than in
ColloborativeEclampsia Trial, using standard Pritchard regimen (40g vs 23.9g, p <
0.001).6,7
In the present study the APGAR score of the neonates at 5 min was primary endpoint
and it showed a statistical significance between the groups. The mean APGAR score
was 6.62+2.23 in Standard dose magnesium sulphate regimen group and 8.9+1.46 in
Low dose magnesium sulphate regimen group. Neonates with severely depressed
APGAR score were significantly more in Standard dose magnesium sulphate regimen

104
group compared to Low dose magnesium sulphate regimen group. There was
significant decrease in APGAR scores with corresponding increase in the cord blood
magnesium level. APGAR scores were decreased as the cord blood magnesium level
increased from 2.5 to 3.5 mmol/l. The neonatal effects of magnesiumion that we
observed occurred primarily within the therapeuticrange of magnesium sulphate in
mothers. Similar studies by Das M et al. and Green K W et al showed significant
correlation between the APGAR scores and cord blood magnesium level. They found
higher proportion of neonates had severely depressed APGAR scores where in
mothers were treated with Prtichard regimen compared to Low dose regimen.
However identical studies by Regmi M C et al. and Bhattacharjee et al. did not show
statistical significance in decrease of APGAR scores between neonates of eclamptic
mothers in Standard dose magnesium sulphate regimen group and Low dose
magnesium sulphate regimen groups. This may be due to the lesser sample size and
less emphasis on neonatal parameters.8
In the present study neonates who required NICU care were significantly more in
Standard dose magnesium sulphate regimen group compared to Low dose magnesium
sulphate regimen group. Also there was significant correlation between the number of
NICU admissions and cord blood magnesium level. Number of NICU admission
increased with the cord blood magnesium level increase. Higher proportion of
neonates were admitted with cord blood magnesium level in the range of 3.5-3.8
mmol/l compared to lower range <3.5mmol/l of cord blood magnesium level. These
findings are in accordance with similar studies by Latikasahu and Monalisa Das who
showed significant increase in rate of admission in NICU among neonates of mothers
treated with standard dose regimen group compared to lower dose regimens. However

105
other identical studies by Mahajan NN and Jana N showed no significance in neonatal
parameters among neonates of eclamptic mothers.9
In our study we found incidence of respiratory distress, hypotonia and bradycardia to
be significantly more among neonates of eclamptic mother who were treated with
Standard dose magnesium sulphate regimen compared to neonates of eclamptic
mothers who were treated with Low dose magnesium sulphate regimen. These
findings are in accordance with similar studies by Abbassi-Ghanavati and Das M who
showed significant increase in rate of admission in NICU among neonates of mothers
treated with Standard dose magnesium regimen compared to lower dose regimens.
However other identical studies by Shilva andBangal V there was no significance in
neonatal parameters among neonates of eclamptic mothers.10
In the present study the proportion of still birth among eclamptic mothers was 1% in
Standard dose magnesium sulphate regimen group and 0.5% in Low dose magnesium
sulphate regimen group which was much lower compared to similar studies by Begum
R et al. and Sardesai et al. who showed proportion to be 30% and 15% respectively.
This might be due to the exclusion criteria considered in our study which excluded
eclamptic mothers with complication. Our results did not show any statistical
significance in still births among both the groups which is in accordance with Begum
R et al which showed no significance difference in still births among both the groups.
In an identical study by Das M et al. there was statistical significance difference in
still births among both the groups which is in contrast to our study.11
There was no early neonatal death in our study. If complication developed in the
neonates attending paediatric faculty shifted the neonate to neonatal intensive care

106
unit (NICU) and managed accordingly. This is similar to the study by Sardesai et al.
and Shilva et al which also reported no early neonatal mortality.12
In the present study the seizure recurrence after administration of magnesium sulphate
regimens was seen in 6% among eclamptic mothers in Standard dose magnesium
sulphate regimen group and 10% in Low dose magnesium sulphate regimen group.
There was no statistical significance in seizure recurrence in both the groups. The
eclamptic mothers with seizure recurrence were treated accordingly with the protocol
decided in the study. Our findings were in accordance with the study by Sahu L et al.
where the seizure recurrence in the low dose regimen group was 4% and zero cases in
standard dose regimen group.62
In the present study significant less number of adverse effects or adverse events were
observed in Low dose magnesium sulphate regimen group which wereloss of deep
tendon reflexes, aspiration pneumonia and oliguria. In Standard dose magnesium
sulphate regimen group higher number of adverse events reported compared to Low
dose regimen group such as ,n (%) loss of deep tendon reflexes 13(26%), constituting
the highest adverse effect, which lasted for hours, followed by oliguria 8(16%) and
aspiration pneumonia 2(4%). Adverse events in mothers were statistically related to
higher serum magnesium levels. Standard dose magnesium sulphate regimen safety
and efficacy have been documented in study by Pritchard J A et al. who evaluated 245
cases of eclampsia and found magnesium sulphate alone effectively controlled
convulsions in great majority of cases with very few and rare adverse events like renal
failure, pulmonary oedema and only one case of respiratory arrest.63
In our study we have evaluated the neonatal outcomes of eclamptic mothers treated
with Low dose magnesium sulphate regimen and Standard dose magnesium sulphate
107
regimen for management of eclampsia. Our results highlighted the largely forgotten
observations on neonatal outcome of eclamptic mothers treated with magnesium
sulphate which was made several decades ago. Further studies with larger size needed
for documentation of neonatal adverse events due to hypermagnesimia. The results
are clinically relevant to health care facilities in developing countries, where maternal
height and weight are almost always low.64
The present study results have implications -
• Firstly, following the Low dose magnesium sulphate regimen decreases the
risk of magnesium toxicity to mothers and newborns and hence increased
safety of the drug.
• Secondly with a lesser toxicity, magnesium sulphate treatment is likely to
become acceptable at primary health centres. Recent similar studies in
Bangladesh by Shamshuddin L et al. suggests that administering the drug at
primary health centres significantly reduces the recurrence of seizures,
maternal deaths and improves perinatal outcome.

108
CONCLUSION
This study was conducted to compare the neonatal outcome in eclamptic
mothers treated with low-dose magnesium sulphate regimen and standard dose
magnesium sulphate regimen. We concluded that
• Neonatal outcome were better in eclamptic mothers treated with low dose
magnesium sulphate regimen compared to the eclamptic mothers treated with
standard dose magnesium sulphate regimen.
• Low dose magnesium sulphate regimen has comparable efficacy as standard
dose magnesium sulphate regimen to control convulsions in management of
eclampsia.
• Low dose magnesium sulphate regimen had less magnesium toxicity and fewer
maternal adverse events and achieved serum magnesium levels within
therapeutic range for control of convulsons in eclampsia compared to standard
dose magnesium sulphate regimen.
• APGAR scores decreased with increase in cord blood magnesium levels and
NICU care requirement increased with increase in cord blood magnesium
levels.
• Our analysis indicates that several neonatal outcomes are significantly related
to increasing concentration of magnesium ion in the maternal circulation.
• Maternal adverse events increased with increase in serum magnesium levels of
the eclamptic mothers after loading dose.

109
STRENGTHS
• This was a comparative study on neonatal outcomes of eclamptic mothers were
assessed who were treated with magnesium sulphate regimens.
• Several neonatal and maternal parameters which were not considered in the
previous studies were highlighted in this study.
• The correlation of neonatal parameters with cord blood magnesium level were
done and correlation of maternal parameters with serum magnesium level was
done. So the results could be elaborated to the health facilities were no facilities
for monitoring the therapeutic concentration of magnesium level were present.
• The result of the study can be can be implemented in the nearby primary and
secondary centres without fear of magnesium toxicity as in standard Pritchard's
regimen which can reduce the complications of eclampsia while reaching our
tertiary care hospital.
LIMITATIONS
• Larger sample size, including multi institution would give more power to the
study and would help in assessment of several other neonatal and maternal
parameters.
• Facilities for continuous electrocardiographic monitoring of all newborn not
available in our hospital, so bradycardia and subtle ECG changes due to
neonatal hypermagnesimia could not be monitored.

110
SUMMARY
• This interventional prospective randomized open labelled study was done
between neonatal outcomes of eclamptic mothers treated with low dose
magnesium sulphate regimen treated with standard dose magnesium sulphate
regimen for management of eclampsia.
• Eclampsia is a multisystem disorder of unknown aetiology characterized by
development of hypertension to the extent of 140/90mmHg or more with
proteinuria after the 20th week in a previously normotensive an non
proteinuric patient complicated with generalised tonic-clonic convulsions
and/coma.
• In severe cases of preeclampsia and in eclampsia,magnesium sulphate
administered parenterally is an effectiveanticonvulsant that avoids producing
central nervoussystem depression in either the mother or the infant.
• Magnesium sulphate acts as a membrane stabilizer and neuroprotector. . It
reduces motor endplate sensitivity to acetylcholine. Magnesium blocks
neuronal calcium influx also byblockadeof calcium entry via voltage-gated
channels.
• Magnesium sulphate may begiven intravenously by continuous infusion or
intramuscularlyby intermittent injection.
• Magnesium sulphate is attributed to dose related toxicity which is a major
concern. Possible maternal adverse effects include reduced urinary output,
respiratory depression, aspiration pneumonia, hypotension, decreased or loss
of deep tendon reflexes. A significant percentage of perinatal and early

111
neonatal morbidity and mortality has been recorded due to neonatal
hypermagnesimia.
• Pritchard in 1984 suggested that the dose of magnesium sulphate may be
reduced for women with low BMI in Asia as administering Pritchard’s
regimen might prove to be hazardous for them due to dose related toxicity.
Various low dose magnesium sulphate regimens have been described
principally because of low BMI of Indian women & concern about toxicity in
circumstances where facility for measurement of serum level of magnesium is
not available. Low dose magnesium sulphate regimen has shown promise in
terms of decrease in side effects without a significant decrease in its
therapeutic benefits.
• Low-dosemagnesium sulphate for administration, showed efficacy similar to
standard Pritchardregimen with reduced maternal and perinatal mortality in
previous studies. However, neonatal outcome has rarely been studied
withlowdose magnesium sulphate regimen.
• The primary end point of the study was to assess the neonatal outcome by the
assessment of APGAR scores at 5min. Secondary end points of the study were
to assess neonatal parameters in terms of birth weight, respiratory depression,
NICU care requirement, bradycardia and hypotonia. Also to study the
correlation of neonatal outcomes with cord blood magnesium level. And to
assess the safety and efficacy of low dose magnesium sulphate regimen.
• In the present study the neonates with severely depressed APGAR score were
significantly more in standard dose regimen group compared to low dose
regimen group. There was significant decrease in APGAR scores with
corresponding increase in the cord blood magnesium level.

112
• Neonatal parameters like NICU care requirement, incidence of respiratory
distress, bradycardia and hypotonia showed significant decrease in Low dose
magnesium sulphate regimen group compared to Standard dose magnesium
sulphate regimen group.
• Low dose magnesium sulphate regimen had less number of adverse events
reported among eclamptic mothers and it had decreased maternal morbidity
compared to standard dose magnesium sulphate regimen. Also it was effective
in controlling convulsion in eclamptic mothers similar to Pritchard's regimen.
• Low dose magnesium sulphate regimen can be used by nearby primary and
secondary centres and implement this regimen without fear of magnesium
toxicity as in standard Pritchard's regimen which can reduce the complications
of eclampsia while reaching our tertiary care hospital.
• Larger trials with multiple institutional trials should be undertaken to find the
lowest effective dose of magnesium sulphate for convulsion control.

113
REFERENCES
1. World Health Organisation International. Collaborative Study of Hypertensive
Disorders of pregnancy. Geographic Variation in the incidence of hypertension in
pregnancy. Am J ObstetGynecol1958;158:80-3.
2. Dutta DC. Hypertensive Disorders in Pregnancy. In: Konar H, editor. DC Dutta’s
Text Book of Obstetrics. 8th ed. New Delhi: Jaypee Brothers Medical
Publishers(P) Ltd.; 2015. p. 268.
3. Altura BM, Altura BT, Carella A, Gebrewold A, Murakawa T, Nishio A. Mg2+-
Ca2+ interaction in contractility of vascular smooth muscle: Mg2+ versus organic
calcium channel blockers on myogenic tone and agonist-induced responsiveness
of blood vessels. Can J PhysiolPharmacol 1987;65:729-45.
4. Idama TO, Lindow SW. Magnesium sulphate: A review of clinical pharmacology
applied to obstetrics. Br J ObstetGynaecol1998;105:260-8.
5. Pritchard JA, Cunningham FG, Pritchard SA. The Parkland Memorial Hospital
protocol for treatment of eclampsia: Evaluation of 245 cases. Am J
ObstetGynecol1984;148:951-63.
6. Das M, Patralekha Ray Choudri, Badal C. Assessment of serum magnesium levels
and its outcome in neonates of eclamptic mothers treated with low dose
magnesium sulphate regimen. Indian journal of pharmacology 2015:55(4):757-
761.
7. Sahu L, Singh S, Tempe A, Koner BC. A randomized comparative study between
low-dose magnesium sulphate and standard dose regimen for management of
eclampsia. International Journal Reproduction Contraception Obstetrics and
Gynaecology 2014;3:79-86.

114
8. RuchiraNautiyal, Akansha Srivastava, Nidhi Chauhan, Hemant Kumar Nautiyal,
Feasibility of low dose magnesium sulphate for eclampsia – a randomized study
Indian Journal of Obstetrics and Gynaecology Research 2016;3(2):121-125.
9. Abbassi-Ghanavati M, Alexander JM, McIntire DD, Savani RC, Leveno KJ.
Neonatal effects of magnesium sulphate given to the mother. American Journal of
Perinatolgy2012;29:795-9.
10. Jana N, Dasgupta S, Das AK, Santra D, Samanta B. Experience of a low-dose
magnesium sulphate regimen for the management of eclampsia over a decade.
International Journal of Gynaecology and Obstetrics 2013;122:13-7.
11. Nassar AH, Sakhel K, Maarouf H, Naassan GR, Usta IM. Adverse maternal and
neonatal outcome of prolonged course of magnesium sulfatetocolysis.
ActaObstetGynecolScand2006;85:1099-103.
12. Begum R, Begum A, Johanson R, Ali MN, Akhter S. A low dose ("Dhaka")
magnesium sulphate regime for eclampsia. ActaObstetGynecolScand
2001;80:998-1002.
13. Cunningham FG, Leveno KJ, Bloom SL, Spong CY, Dashe JS, Hoffman BL, et
al., editors. Hypertensive Disorders. In: Williams Obstetrics. 24th ed. New York:
McGraw–Hill Education; 2014. p. 728-9.
14. K.Park.Preventive medicine in obstetrics, pediatrics and geriatrics. Park textbook
of Preventive and Social Medicine. 23rd edition. Jabalpur: M/s BanarsidasBhanot
Publishers.2015; 532-5.
15. Nobis P N, Hajong A et al. Eclampsia in India Through Decades.The Journal of
Obstetrics and Gynaecology of India (September–October 2016) 66(S1):S172–
S176.

115
16. Ministry of Health and Family Welfare, India. Annual Report. New Delhi: 2005:
105-111. Available at:
http://mohfw.nic.in/WriteReadData/l892s/6960144509Annual%20Report%20to%
20the%20People%20on%20Health.pdf. Accessed December 2011.
17. Chesley LC. Hypertensive Disorders in Pregnancy. New York: Appleton-Century-
Crofts; 1978.
18. Fernando Arias. Hypertensive disorder in pregnancy; Practical Guide to High
Risk pregnancy and delivery.3rd ed. New Delhi: Elsevier publishers;2008:397-
437.
19. Bhargava A, Pant R, Chutani I, Singh S R. In search for accelerated recovery from
eclampsia. J Obstet and Gynecol India. 2006;56:402-5.
20. Duley L. The Eclampsia Trial collaborative Group. Which Anticonvulsant for
women with Eclampsia? Evidence from the Collaborative Eclampsia Trial. Lancet
1995;345:1455-63.
21. Euser AG, Bullinger L, Cipolla MJ. Magnesium sulphate treatment decreases
blood-brain barrier permeability during acute hypertension in pregnant rats.
ExpPhysiol2008;93:254-61.
22. American College of Obstetricians and Gynecologists: Diagnosis and
management of preeclampsia and eclampsia. Practice Bulletin No. 33, January
2002.
23. Shokry M, Elsedfy GO, Bassiouny MM, Anmin M, Abozid H. Effects of antenatal
magnesium sulphate therapy on cerebral and systemic hemodynamics in preterm
newborns. ActaObstetricaetGynaecologica. 2010;8(6)9:801-6.

116
24. Fisher S, Roberts JM: The placenta in normal pregnancy and preeclampsia.
InTaylor RN, Roberts JM, Cunningham FG (eds): Chesley’s Hypertensive
Disorders in Pregnancy, 4th ed. Amsterdam, Academic Press, 2014
25. Hallak M, Berman RF, Irtenkauf SM, Janusz CA, Cotton DB. Magnesium sulfate
treatment decreases N-methyl-D-aspartate receptor binding in the rat brain: An
autoradiographic study. J SocGynecolInvestig 1994;1:25-30.
26. Montan S. Medical prevention of pre-eclampsia. ActaObstetGynaecolScand
Suppl. 1997;76(164):111-5.
27. Witlin AG: Prevention and treatment of eclamptic convulsions.
ClinObstetGynecol1999;42:507–518.
28. Helmin R H J. Prevention of eclampsia and preeclampsia. Lancet 1952;1:64.
29. Altman D, Carroli G, Duley L, Farrell B, Moodley J, Neilson J, et al. Do women
with pre-eclampsia, and their babies, benefit from magnesium sulphate? The
magpie trial: A randomised placebo-controlled trial. Lancet 2002;359:1877-90.
30. Lipsitz PJ. The clinical and biochemical effects of excess magnesium in the
newborn. Pediatrics1971;47:501-9.
31. Sibai BM. Magnesium sulfate is the ideal anticonvulsant in preeclampsia –
eclampsia. Am J Obstet Gynecol. 1990;162(5):1141-5.
32. Chinayon P. Clinical management and outcome of eclampsia at Rajavithi
Hospital. J Med Assoc Thai.1998;81(8):579-85.
33. Bhargava A, Pant R, Chutani I, Singh SK: In search for accelerated recovery from
eclampsia. J ObstetGynecol India 2006;56:402–405.

117
34. Regmi MC, Aggrawal A, Pradhan T, Rijal P, Sabdi A. Loading dose versus
standard regimen of magnesium sulphate in eclampsia-a randomized trial. Nepal
Med Coll J. 2010;12(4):244-7.
35. Chowdhury JR, Chaudhuri S, Bhattacharyya N, et al: Comparison ofintramuscular
magnesium sulfate with low dose intravenous magnesiumsulfate regimen for
treatment of eclampsia. J ObstetGynaecol Res 35:119, 2009
36. Ekele BA, Muhammed D, Bello L N, Namadina IM. Magnesium sulfate therapy
in Eclampsia : the Sokoto (ultra short) regimen. BMC Res Notes. 2009;2:165.
37. Duley LW, Crowther CA, Middleton P, Marret S, Rouse D. Magnesium sulphate
for women at risk of preterm birth for neuroprotection of the fetus. Cochrane
Database Syst Rev. 2009 Jan;21(1):CD004661.
38. Ekele BA, Muhammed D, Bello LN, Namadina IM. Magnesium sulphate therapy
in eclampsia: the Sokoto (ultra short) regimen. BMC Res Notes. 2009;2:165-8.
39. Magpie Trial Collaboration Group: Do women with pre-eclampsia, and
theirbabies, benefit from magnesium sulphate? The Magpie Trial: a
randomisedplacebo-controlled trial. Lancet 359:1877, 2002
40. Laurence L, Bruton. Antiarrhytmic drugs In: Goodman and Gilman’s The
Pharmacological Basis of Therapeutics.13th edition. New York: McGraw-Hill
Education; 2011.p.842.
41. Maternal anthropometry and pregnancy outcomes. A WHO Collaborative Study:
Introduction. Bull World Health Organ 1995;73 Suppl:1-6.
42. Duley L. Magpie Trial Follow up Collaborative group. The Magpie Trial: A
randomized trial comparing magnesium sulphate with placebo for preeclampsia:
Outcome for children at 18 months. Br J ObstetGynaecol. 2007;114(3):289-99.
118
43. Duley L. Maternal mortality associated with hypertensive disorders of pregnancy
in Africa, Asia, Latin America and the Carribean. Br J ObstetGynaecol
1992;99(7):547-53.
44. The Eclampsia Trial Collaborative Group. Which anticonvulsant for women with
eclampsia? Evidence from the Collaborative Eclampsia Trial. Lancet
1995;345:1455-63.
45. Gastrich MD, Gandhi SK, Pantazopoulos J, et al: Cardiovascular outcomesafter
preeclampsia or eclampsia complicated by myocardial infarction or stroke.
ObstetGynecol120(4), 823, 2012
46. Kleigman, Behram, Jenson, Stanton et al, editors. Electrolytes and acid base
disorders. In: Nelson textbook of Pediatrics Volume 1. 18th edition. New Delhi:
Reed Elsevier India Private Limited 2010.p.287.
47. Stone SR, Pritchard JA. Effect of maternally administered magnesium sulfate on
the neonate. ObstetGynecol 1970;35:574-7.
48. Donovan EF, Tsang RC, Steichen JJ, Strub RJ, Chen IW, Chen M. Neonatal
hypermagnesemia: Effect on parathyroid hormone and calcium homeostasis.
JPediatr1980;96:305-10.
49. Lipsitz PJ, English IC. Hypermagnesemia in the newborn infant.
Pediatrics1967;40:856-62.
50. Rasch DK, Huber PA, Richardson CJ, L'Hommedieu CS, Nelson TE, Reddi
R.Neurobehavioral effects of neonatal hypermagnesemia. J Pediatr
1982;100:272-6.
51. Green KW, Key TC, Coen R, Resnik R. The effects of maternally administered
magnesium sulfate on the neonate. Am J ObstetGynecol 1983;146:29-33.

119
52. Riaz M, Porat R, Brodsky NL, Hurt H. The effects of maternal magnesium sulfate
treatment on newborns: A prospective controlled study. J Perinatol 1998;18:449-
454.
53. Alexander JM, McIntire DD, Leveno KJ, et al: Selective magnesium sulfate
prophylaxis for the prevention of eclampsia in women with
gestationalhypertension. ObstetGynecol 108:826, 2006
54. Crowther CA, Bouwmeester AM, Ashurst HM: Does admission to hospitalfor bed
rest prevent disease progression or improve fetal outcome in pregnancy
complicated by non-proteinuric hypertension? Br J ObstetGynaecol 99:13, 1992
55. Abalos E, Duley L, Steyn DW, et al: Antihypertensive drug therapy for mild to
moderate hypertension during pregnancy. Cochrane Database Syst Rev
1:CD002252, 2007
56. Duffy CR, Odibo AO, Roehl KA, et al: Effect of magnesium sulfate on fetalheart
rate patterns in the second stage of labor. ObstetGynecol 119(6):1129, 2012
57. Hallak M, Martinez-Poyer J, Kruger ML, et al: The effect of magnesium sulfateon
fetal heart rate parameters: a randomized, placebo-controlled trial. Am J
ObstetGynecol 181:1122, 1999
58. Sardesai S, Maira S, Patil A. Low dose Magnesium Sulphate therapy for
Eclampsia and imminent Eclampsia ─ regimen tailored for Indian women. J
ObstetGynecol India 2003;53:546-550.
59. Shilva, Saha SC, Kalra J, Prasad R. Safety and efficacy of low-dose MgSO4 in the
treatment of eclampsia. Int J GynaecolObstet 2007;97:150-1.
60. Bangal V, Kwatra A, Raghav S, Jadhav S. Low dose magnesium sulphate regime
for Eclampsia. Pravara Med Rev 2009;4:13-5.

INFORMED CONSENT (GUARDIAN)
SHIVAMOGGA INSTITUTE OF MEDICAL SCIENCES
I have been briefed on the foregoing study being conducted by Dr. Sriti Hegde and it has
been conveyed to me about the treatment regimen, need for the blood test and the need for the
observation of new born in my own language. I have had the opportunity to ask questions
about it and any questions that I have asked have been answered to my satisfaction. I consent
on behalf of my ________________( relation ) _____________ (name).
Name :
Relation with the participant :
Signature :
Date:
If illiterate
I have accurately read the consent form to the relative of the participant and the individual
has had the opportunity to ask questions. I confirm that the individual has given the consent.
Sign :
Name of the relative of the participant
Relation with the participant
Left thumb impression :
Date :

INFORMED CONSENT
SHIVAMOGGA INSTITUTE OF MEDICAL SCIENCES
I have been briefed on the foregoing study being conducted by Dr. Sriti Hegde and it has
been conveyed to me about the treatment regimen, need for the blood test and the need for the
observation of new born in my own language. I have had the opportunity to ask questions
about it and any questions that I have asked have been answered to my satisfaction. I consent
voluntarily to participate.
Name of the participant :
Signature :
Date:
If illiterate
I have accurately read the consent form to the relative of the participant and the individual
has had the opportunity to ask questions. I confirm that the individual has given the consent.
Sign :
Name of the participant
Left thumb impression :
Date :

M¦àUÉ ¥ÀvÀæ (¸ÀA§A¢üPÀgÀÄ) ²ªÀªÉÆUÀÎ ªÉÊzÀQÃAiÀÄ «eÁÕ£ÀUÀ¼À ¸ÀA¸ÉÜ ²ªÀªÉÆUÀÎ
(ªÉÄðéZÁgÀPÀgÀÄ eÉÆÃ¥Á£À ªÀiÁqÀĪÀÅzÀÄ)
qÁ. ±ÀÈw ºÉUÀqÉ gÀªÀgÀ G£ÀßvÀ ªÉÊzÀåQÃAiÀÄ ªÁå¸ÀAUÀPÉÌ ¸ÀºÀPÀj¸À®Ä M¦àUÉ ¤ÃrgÀÄvÉÛ£É F PÀÄjvÀÄ CªÀgÀÄ £À£Àß
ªÀiÁvÀÈ ¨sÁµÉAiÀÄ°è G¥ÀAiÉÆÃV¸ÀÄwÛgÀĪÀ OµÀ¢ü ¥ÀzÀÞwÛAiÀÄ §UÉÎ CzÀjAzÀ ¸ÁzsÀåªÁUÀ§ºÀÄzÁzÀ ¥ÀæAiÉÆÃd£ÀUÀ¼ÀÄ
ºÁUÀÄ CqÀØ¥ÀjuÁªÀÄUÀ¼À §UÉÎ gÀPÀÛ ¥ÀjÃPÉëAiÀÄ CUÀvÀåvÉ ºÁUÀÄ ªÀÄUÀĪÀ£ÀÄß ¤UÁzÀ°è EqÀĪÀ CUÀvÀåvÉAiÀÄ §UÉÎ
«ªÀj¹gÀÄvÁÛgÉ £Á£ÀÄ F PÀÄjvÀÄ PÉýzÀ ¥ÀæwAiÉÆÃAzÀÄ ¥Àæ±ÉßUÀ½UÉ £À£ÀUÉ vÀȦÛAiÀiÁUÀĪÀ jÃwAiÀÄ°è GvÀÛgÀUÀ¼À£ÀÄß
¤ÃrgÀÄvÁÛgÉ.
F §UÉÎ £Á£ÀÄ AiÀiÁgÀ MvÁÛAiÀÄ«®èzÉ À̧é-EZÉѬÄAzÀ £À£Àß ……………… CzÀ …………………………………………………… ¥ÀgÀªÁV
M¦àUÉ ¤ÃrgÀÄvÉÛãÉ.
ºÉ¸ÀgÀÄ:
D¨sÀåyðAiÉÆA¢UÉ ¸ÀA§AzsÀ:
¸À»
¢£ÁAPÀ:
C£ÀPÀëgÀ¸ÀÜgÁzÀgÉ
£Á£ÀÄ M¦àUÉ ¥ÀvÀæzÀ°ègÀĪÀ J¯Áè ªÀiÁ»wUÀ¼À£ÀÄß C¨sÀåyðAiÀÄ ¸ÀA§A¢üUÉ «ªÀgÀªÁV w½¹gÀÄvÉÛãÉ. CzÀgÀ §UÉÎ
¥Àæ±ÉßUÀ¼À£ÀÄß PÉüÀĪÀÅzÀPÉÌ CªÀPÁ±À PÀ°à¹zÀÄÝ, CzÀgÀ §UÉÎ ªÀiÁ»wAiÀÄ£ÀÄß w½zÀÄ, D¨sÀåyðAiÀÄ ¸ÀA§A¢ü
M¦àUÉAiÀÄ£ÀÄß ¤Ãr ºÉ̈ ÉânÖ£À À̧» ºÁQgÀÄvÁÛgÉ.
ºÉ¸ÀgÀÄ:
D¨sÀåyðAiÉÆA¢UÉ ¸ÀA§AzsÀ:
ºÉ̈ ÉânÖ£À UÀÄgÀÄvÀÄ :
¢£ÁAPÀ:
M¦àUÉ ¥ÀvÀæ
²ªÀªÉÆUÀÎ ªÉÊzÀQÃAiÀÄ «eÁÕ£ÀUÀ¼À ¸ÀA¸ÉÜ ²ªÀªÉÆUÀÎ
(ªÉÄðéZÁgÀPÀgÀÄ eÉÆÃ¥Á£À ªÀiÁqÀĪÀÅzÀÄ)
qÁ. ±ÀÈw ºÉUÀqÉ gÀªÀgÀ G£ÀßvÀ ªÉÊzÀåQÃAiÀÄ ªÁå À̧AUÀPÉÌ À̧ºÀPÀj¸À®Ä M¦àUÉ ¤ÃrgÀÄvÉÛ£É F PÀÄjvÀÄ CªÀgÀÄ £À£Àß
ªÀiÁvÀÈ s̈ÁµÉAiÀÄ°è G¥ÀAiÉÆÃV¸ÀÄwÛgÀĪÀ OµÀ¢ü ¥ÀzÀÞwÛAiÀÄ §UÉÎ CzÀjAzÀ ¸ÁzsÀåªÁUÀ§ºÀÄzÁzÀ ¥ÀæAiÉÆÃd£ÀUÀ¼ÀÄ
ºÁUÀÄ CqÀØ¥ÀjuÁªÀÄUÀ¼À §UÉÎ gÀPÀÛ ¥ÀjÃPÉëAiÀÄ CUÀvÀåvÉ ºÁUÀÄ ªÀÄUÀĪÀ£ÀÄß ¤UÁzÀ°è EqÀĪÀ CUÀvÀåvÉAiÀÄ §UÉÎ
«ªÀj¹gÀÄvÁÛgÉ £Á£ÀÄ F PÀÄjvÀÄ PÉýzÀ ¥ÀæwAiÉÆÃAzÀÄ ¥Àæ±ÉßUÀ½UÉ £À£ÀUÉ vÀȦÛAiÀiÁUÀĪÀ jÃwAiÀÄ°è GvÀÛgÀUÀ¼À£ÀÄß
¤ÃrgÀÄvÁÛgÉ. F §UÉÎ £Á£ÀÄ AiÀiÁgÀ MvÁÛAiÀÄ«®èzÉ ¸Àé-EZÉѬÄAzÀ s̈ÁUÀªÀ»¸ÀÄvÉÛ£É ºÁUÀÄ M¦àUÉ ¤ÃrÃgÀÄvÉÛãÉ.
ºÉ¸ÀgÀÄ :
¸À» ;
¢£ÁAPÀ :
C£ÀPÀëgÀ¸ÀÜgÁzÀgÉ £Á£ÀÄ M¦àUÉ ¥ÀvÀæzÀ°ègÀĪÀ J¯Áè ªÀiÁ»wUÀ¼À£ÀÄß C¨sÀåyðUÉ «ªÀgÀªÁV w½¹gÀÄvÉÛãÉ. CzÀgÀ §UÉÎ ¥Àæ±ÉßUÀ¼À£ÀÄß
PÉüÀĪÀÅzÀPÉÌ CªÀPÁ±À PÀ°à¹zÀÄÝ, CzÀgÀ §UÉÎ ªÀiÁ»wAiÀÄ£ÀÄß w½zÀÄ, D¨sÀåyðAiÀÄÄ M¦àUÉAiÀÄ£ÀÄß ¤Ãr ºÉ¨ÉânÖ£À
¸À» ºÁQgÀÄvÁÛgÉ.
¸À» : ºÉ¸ÀgÀÄ : ºÉ¨ÉânÖ£À UÀÄgÀÄvÀÄ : ¢£ÁAPÀ :

Scanned by CamScanner

ANNEXURE III
CASE REPORT FORM
DATE -
NAME :
AGE
GENDER MALE / FEMALE
IP/OP NO.
PHONE NUMBER
OCCUPATION
ADDRESS
INFORMANT
RELATION OF INFORMANT WITH THE PATIENT
SOCIOECONOMIC STATUS
HISTORY OF PRESENT ILLNESS:
G__P__L__A__D__ with ________ weeks of amenorrhea with history of generalised tonic clonic seizures

LMP
EDD
HISTORY OF PRESENT PREGNANCY
I TRIMESTER
II TRIMESTER
III TRIMESTER
OBSTETRICS HISTORY
YEAR PREGNANCY LABOUR PEURPERIUM BABY
MENSTRUAL HISTORY
AGE OF MENARCHE DURATION
CYCLE AMOUNT OF BLOOD FLOW

PAST HISTORY
CONVULSION HISTORY
HYPERTENSION
ENDOCRINE DISORDERS (DIABETES/THROID ABNORMALITY)
CHRONIC KIDNEY DISEASE
CORTICOSTEROID MEDICATION
OTHERS SPECIFY
FAMILY HISTORY
SIMILAR HISTORY IN THE FAMILY
OTHERS
PERSONAL HISTORY -
CONTRACEPTIVE USE
IMMUNIZATION STATUS
SMOKING
ALCOHOL
ALLERGY

GENERAL PHYSICAL EXAMINATION
GLASSGOW COMA SCALE
(GCS)
HEIGHT
HR WEIGHT
BP BREAST
RR PALLOR
TEMP ICTERUS
BUILD CYANOSIS
NUTRITION PEDAL OEDEMA
OBSTETRICS EXAMINATION
ABDOMEN
CERVIX
LABORATORY VALUES -
Hb gm% ALT IU/L
RBC million/mL ALP IU/L
PLATELET thousands/mL AST IU/L
TLC thousands/mL S. sodium
BLOOD GROUP S. potassium
RBS gm/dL S.creatinine
BILLIRUBIN TOTAL
mg/dL

REGIMEN USED
0 hour
at time of delivery
cord blood
serum magnesium
MONITORING OF MAGNESIUM TOXICITY
DTR Urine output
Pedal oedema
Pulmonary crepitations
Blood pressure
Oxygen saturation
4 h
8h
12h
16h
20h
24h
CONTROL OF SEIZURE BY THE ABOVE REGIMEN
RECURRENCE OF SEIZURE
SHIFTED TO PRITCHARD'S REGIMEN
TERMINATION OF PREGNANCY
METHOD USED
OUTCOME OF PRESENT PREGNANCY

NEONATAL PARAMETERS
BIRTH WEIGHT
APGAR SCORE (1min)
APGAR SCORE (5min)
RESPIRATORY DISTRESS
INTUBATION IN DELIVERY ROOM
BRADYCARDIA
HYPOTONIA
NICU care requirement
TIME TO FIRST STOOL
TIME TO FIRST VOID
FEEDING INTOLERANCE
STILL BIRTH
EARLY NEONATAL DEATH

ANNEXURE IV
KEY TO MASTER CHART
COLUMN HEADING CODE
A Patient ID number
B Age in years
C Gravida status of mother 0 - multigravida
1 - primigravida
D Antenatal care required 0 - booked cases
1 - unbooked cases
E Areas 0 - rural
1 - urban
F Gestation period in weeks
G Body mass index in kg/m2
H Systolic blood pressure
I Diastolic blood pressure
J No. of seizures before admission
K Mode of delivery 0 - Vaginal delivery
1 - Caesarean section
L Deep tendon reflexes 0 - Deep tendon reflex
1 - Loss of DTR
M Pulmonary crepitations 0 - Normal breathing
1 - Pulmonary crepitation
N Urinary output 0 - Normal urine output
1 - Oliguria

O Seizure recurrence 0 - No recurrence of
seizure
1 - Recurrence of seizure
P Birth weight
Q APGAR scores at 5 min
R NICU admissions 0 - NICUcare not required
1 - NICU care required
S Respiratory distress 0 - Respiratory distress
1 - Normal breathing
T Hypotonia 0 - Normal muscle tone
1 - Hypotonia
U Bradycardia 0 - Normal heart rate
1 - Bradycardia
V Still birth 0 - Live birth
1 - Still birth
W Early neonatal death 0 - Healthy neonates
1 - Neonatal death
X Regimen followed 0 - Low dose regimen
1 - Standard dose regimen
Y Maternal serum magnesium level
Z Cord blood magnesium level

Scanned by CamScanner

Scanned by CamScanner
Scanned by CamScanner

ANNEXURE V
IMAGES
Illustration of automated clinical chemical analyzer for estimation of serum and cord
blood magnesium
Illustration of reagents used for estimation of serum and cord blood magnesium